Emergency care in hemophilia - hemofilia.or.id Manado KEDARURATAN HEMOFILIA... · • deep hematoma...
34
Management of acute bleeding & emergency in hemophilia Novie Amelia Chozie , Fitri Primacakti, Djajadiman Gatot Divisi Hematologi-Onkologi Departemen Ilmu Kesehatan Anak FKUI/RSCM Jakarta
Transcript of Emergency care in hemophilia - hemofilia.or.id Manado KEDARURATAN HEMOFILIA... · • deep hematoma...

Management of acute bleeding & emergency in hemophilia
Novie Amelia Chozie, Fitri Primacakti, Djajadiman Gatot
Divisi Hematologi-Onkologi
Departemen Ilmu Kesehatan Anak FKUI/RSCM Jakarta

Perdarahan akut, kapan mulai terjadi ?
•Bayi/anak laki-laki
•Lebam atau memar saat bayi
mulai belajar merangkak
•Usia 1 – 2 tahun :
•Paling sering : sendi & otot
•Spontan atau karena trauma
ringan

Perdarahan akut, kapan mulai terjadi ?
•Perdarahan lain :
•perdarahan frenulum (pada bayi)
•Lebam kebiruan di kulit
•Perdarahan otak
•Perdarahan saluran kemih
•Mimisan
•Pada hemofilia ringan : perdarahan pascatrauma/kecelakaan/tindakan medik (cabut gigi, khitan)
Guidelines for the Management of Hemophilia, WFH 2012

Sites of bleeding
Guidelines for the Management of Hemophilia, WFH 2012

Perdarahan sendi (hemartrosis) akut
•Pertolongan pertama : RICE
•Faktor konsentrat sesegera mungkin
(< 2 jam)
•Analgetik : parasetamol, COX-2 inhibitor
•Fisioterapi segera setelah sakit dan bengkak hilang
Hoots WK. Emergency care issues in hemophilia. WFH, 2007

WFH Guidelines 2013Acute bleeds should be treated as quickly as possible, preferably within 2 (two) hours.
If in doubt, treat.

Fig. The cycle initiated by hemarthrosis, leading to
chronic synovitis and progressive arthropathy.
J Am Acad Orthop Surg. 2004;12:234-245. Pharmacological Research 2017;115:192–199
Hemarthrosis & hemophilic arthropathy

Synovitis
The goal of treatment is to deactivate the synovium as quickly as possible and preserve joint function.
• Factor concentrate replacement : short treatment courses (6-8 weeks) of secondary prophylaxis with intensive physiotherapy
• Daily exercise to improve muscle strength and maintain joint motion
• Antiinflamation : NSAIDs (COX-2 inhibitors)
• Functional bracing
• Synovectomy
Haemophilia. 2013:19; e1–47.

Chronic haemophilic arthropathy
The goals of treatment :
• To improve joint function
• Relieve pain
• Assist patient to continue/resume normal activities of daily living.
Haemophilia. 2013:19; e1–47.

On-demand treatment
• Treatment after bleeding has occurred
• The past standard of care in many developed countries
• Outcome : long term arthropathy• Poor quality of life
• Potential increase cost of healthcare (joint surgery, etc)
World Federation of Hemophilia

Prophylaxis
• Prophylaxis is the treatment by intravenous injection of factor concentrate to prevent anticipated bleeding.
• Ahlberg, 19651
• Moderate hemophilia (F VIII/IX 15%) vs Severe hemophilia (<1%)• Less joint bleed
• Less musculoskeletal complication (i.e. arthropathy)
• Better quality of life
• Nilsson, 19922
• Hypothesis : converting patient with severe hemophilia to moderate hemophilia will decrease musculoskeletal complication
Acta Orthop Scand. 1965:77;3-132
J Intern Med. 1992:232:25-32

Low dose prophylaxis study, RSCM
OutcomeProphylaxis
n = 22
On-demand
n = 18p CI# 95%
Total bleeding episodes 10,4 ± 6,4 17,3 ± 8,8 0,006* 2,08–11,87
Joint bleeding episodes 5 ± 4,3 8
(3–30)
0,009^ 0,9–6,99
*non paired T-test ^ Mann-Whitney #CI = confidence interval
• Prospective, randomized study
• Low dose prophylaxis (10 IU/kg 2x/week) versus On-demand
• Mean age in prophylaxis group was 12 ± 3.5 years and median age in on-demand group was 11.9 (6.518.2) years.
• No inhibitor F VIII found in both groups

Dose calculation :
F VIII (unit):
BW (kg) x % (plasma target –patient F VIII ) x 0,5
F IX (unit):
BW (kg) x % (plasma target –patient F IX )
Replacement therapy

Bleeding
Hemofilia A Hemofilia B
Plasma Target (%) Duration (day) Plasma Target (%) Duration (day)
Joint 10-20 1-2* 10-20 1-2*
Muscle (excl.iliopsoas) 10-20 2-3* 10-20 2-3*
Iliopsoas
-initial
-maintenance
20-40
10-20
1-2
3-5#
15-30
10-20
1-2
3-5#
CNS
-initial
-maintenance
50-80
30-50
20-40
1-3
4-7
8-14^
50-80
30-50
20-40
1-3
4-7
8-14^
Resp. tract
-initial
-maintenance
30-50
10-20
1-3
4-7
30-50
10-20
1-3
4-7
Gastrointestinal
-initial
-maintenance
30-50
10-20
1-3
4-7
30-50
10-20
1-3
4-7
Ginjal 20-40 3-5 15-30 3-5
Deep laceration 20-40 5-7 15-30 5-7
Operasi mayor
-pre-op
-post-op
60-80
30-40
20-30
10-20
1-3
4-6
7-14
50-70
30-40
20-30
10-20
1-3
4-6
7-14
Tooth extraction
-before procedure
-after procedure
50
20-40
1-3* 40
20-30
1-3*

World Federation of Haemophilia
https://www.wfh.org

Blood component replacement therapy
factor-VIII factor-IX
(unit/ml) (unit/ml) (ml)
Fresh-frozen plasma ~ 0,5 ~ 0,6 200
Cryoprecipitate ~ 4,0 - 20
Factor-VIII concentrate 25 - 100 - 10
Factor-IX concentrate - 25 - 35 20

Faktor pembekuan
•Faktor VIII • Setiap pemberian 1 unit F VIII akan menaikkan kadar
dalam plasma sebesar 2 %• Half life 8 – 12 jam : pemberian tiap 12 jam
•Faktor IX• Setiap pemberian 1 unit F IX akan menaikkan kadar dalam
plasma sebesar 1 %• Half life 24 jam : pemberian tiap 24 jam


Contoh :
• perdarahan sendi yang berat
• perdarahan otot luas
• deep hematoma
• Perdarahan saluran kemih



Pemberian faktor pembekuan
• Periksa kandungan faktor pembeku darah yang tersedia dalam kemasan, • 250/500/750/1000 IU, tergantung dari produk
yang digunakan.
• Tanggal kadaluarsa (expired date).
• Gunakan seluruh isi botol (vial), kecuali dokter atau tim hemofilia rumah sakit menganjurkan hallain.
• Jangan gunakan faktor pembeku darah jika : • Tidak dapat larut dengan baik
• Cairan berwarna atau berubah warna

Organ Deskripsi
Mata Konjungtiva tampak pucat, sklera tidak ikterik
Ekstremitas Akral hangat, CRT <2 cm, terdapat benjolan pada dorsal pedis sinistra, diameter
8x7x7cm, batas tidak tegas lingkar kaki terbesar 48 cm, dolor, kalor, tumor, rubor
Lain-lain Dalam batas normal
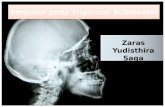
Keluhan utama: benjolan di punggung kaki kanan sejak 1 bulansebelum masuk rumah sakit (suspek osteosarcoma)
An. DA, Laki-laki, 16 tahun

Pemeriksaan Radiologis
• Destruksi tulang pada metatarsal
I, os cuneiforme intermedius & m
edial serta phalang proksimal di
giti I pedis kanan dengan pe
nipisan korteks & gambaran end
osteal scalopping
• Disused osteoporosis.

Pemeriksaan Laboratorium
Laboratorium Nilai
Rujukan
Hb (g/dl) 5 12,5 - 16,1
Hematokrit (%) 27,4 36,0 - 47,0
Leukosit (/UL) 6.780 4.00 - 1050
Trombosit (1000/UL) 520.000 150 - 400
MCV (fl)
MCH (pg)
MCHC (g/dL)
70,9
26
32
78,0 - 95,0
26,0 - 32,0
32,0 - 36,0
APTT (detik) >180 33,6
PT (detik) 12,4 10,4
SGOT/SGPT (U/L) 12/15 <20/<25
Ur/Cr (mg/dL) 20/0,5 15-40/0,5-1,5

Pemeriksaan yang diperlukan
• Pemeriksaan kadar faktor VIII dan IX
• Pemeriksaan kadar faktor pembekuan dapat dilakukan paling cepat 3 hari setelah pemberian faktor pembekuan darah atautransfusi darah
• Factor assay
– Faktor VIII : 176,1% (N: >50%)
– Faktor IX : 1% (N: >50%)
• Profil besi
– Ferritin : 23,5
– Serum iron : 27
– TIBC : 379
– Saturasi transferin : 7%

Pemeriksaan MRI
Sugestif gambaran pseudotumorhemofilia di phalang proksimal digiti I, metatarsal I, os cuneiform dan os talus dengan keterlibatan jaringan lunak di
sekitarnya. Osteopenia.

Resume Kasus
Riwayat Penyakit
* Perdarahan berulang:
(Memar, perdarahan
gusi)
* Riwayat perdarahan
dikeluarga
Pemeriksaan fisis
Benjolan pada dorsal pedis sinistra, diameter 8x7x7cm, batas tidaktegas lingkar kaki terbesar 48 cm, dolor, kalor, tumor, rubor :
PSEUDOTUMOR
Pemeriksaan Penunjang
Anemia
Pemanjangan APTT
Profil besi rendah
Pseudotumor

Diagnosis Kerja
✓Hemofilia B berat
✓Hematoma (pseudotumor) regio plantar pedis
✓Anemia defisiensi besi ec perdarahan

Kegawatan
Anemia: Hb 5 g/dL
Oksigen 1 ltr/mnt nasal
Transfusi
Target Hb 9 - 10 g/dL
Delta HbxBBx4
Transfusi I : 5 ml/KgBB dalam 4 jam
Transfusi II: sisa dari perhitungan
Preparat besi
Kadar Hb & ferritin normal

Tata Laksana Perdarahan
1. Konsentrat faktor pembekuan darah
gold standard (konsentrat F IX)
alternatif :
2. Transfusi komponen darah sesuai jenis
hemofilia yang dialami (FFP)

Comprehensive care
To be governed through multidiscipline approach involving experts in the field of:
• hematology • occupational therapy
• orthopedics • vocational therapy
• infectious disease • psychology
• nutrition • nursing
• dentistry • genetics

Panduan Home treatment
Perawatan Hemofilia Mandiri di Rumah
Tim Pelayanan Terpadu HemofiliaRSUPN Dr. Cipto Mangunkusumo
2017

Terima kasih