Embolia polmonare: ciò che le linee guida non dicono polmonare: ciò che le linee guida non dicono...
42
Embolia polmonare: ciò che le linee guida non dicono F. Numeroso, UO Pronto Soccorso e Medicina d'Urgenza Azienda Ospedaliero-Universitaria di Parma
Transcript of Embolia polmonare: ciò che le linee guida non dicono polmonare: ciò che le linee guida non dicono...

Emboliapolmonare:ciòchelelineeguidanondicono
F.Numeroso,UOProntoSoccorsoeMedicinad'UrgenzaAziendaOspedaliero-UniversitariadiParma

TEP,CIO’CHELEGLNONDICONO:MACOSANONDICONO?

TEP,CIO’CHELEGLNONDICONO:FONTIBIBLIOGRAFICHE
TEP,CIO’CHELEGLNONDICONO:FONTIBIBLIOGRAFICHE

TEP,CIO’CHELEGLNONDICONO:FONTIBIBLIOGRAFICHE

Ø Growingevidencesuggestingover-diagnosisofPE
Ø Diagnosticvalueandclinicalsignificanceofsub-segmentaldefects
Ø Incidental(unsuspected)PE
Ø Triplerule-out’CTangiographyforpatientswithchestpain
Ø Roleofreduced-doseiv.thrombolysis,catheter-directedtreatmentinintermediate-riskpatients
Ø UseofneworalanticoagulantsinthetreatmentofPEandsecondarypreventionofVTE
Ø Criteriaforearlydischargeandhometreatmentoflow-riskpatients
Ø Roleofmagneticresonanceimaging
Ø VTEinpregrancy
Ø Optimalmanagementofpatientswithcancer
Ø Follow-upafterPE:durationofanticoagulationandsearchCTPvasculardisease
TEP,CIO’CHELEGLNONDICONO:MACOSANONDICONO?
(ESCGL2014,JACC2016)

TEP,CIO’CHELEGLNONDICONO:OVERDIAGNOSISOFPE
• To compare incidence, mortality and treatment complications (GI tract or intracranialhemorrage or secondary thrombocytopenia) of PE before and after CTPAwas introduced

TEP,CIO’CHELEGLNONDICONO:OVERDIAGNOSISOFPE
• PEisthequintessentialdiagnosisofmedicinebecouse itcapturesallthecomplexityofmedicinein
theevidence-basedera
• Thefactthatdeathratesremainstablewhereasincidencehasnearlydoubledsuggeststhatnearly
halfofthepts.diagnosedashavingPEexperienceonlytherisksoftherapywithout thebenefit
• Therearestrikinggapsinourknowledge.Whatevidencesupports anticoagulation?AreallPES
equallyconcerning?Whatisthenumberneededtotreattopreventerecurrenceordeath?
• Industry-sponsored studiescontinuestotesttrivialities.Instead,fundamentalquestionmustbe
answered.WichpatientwithVTEbenefitfromanticoagulationatall?
Arch Intern Med. 2012
TEP,CIO’CHELEGLNONDICONO:GESTIONETEPSUBSEGMENTARIA
• Difetti di riempimento a carico di arteriole di 2-3 mm di diametro
• Incidenza: 4.7-15% among positive CTPAs
• Bassa specificità CT (37-46%), scarso accordo inter-osservatori (51%)
• Il dolore toracico è il sintomo più comune ma spesso il riscontro è occasionale
• Rispetto ai casi di TEP prossimale: maggiori livelli di PaO2 e spO2, DVT meno
frequente, biomarcatori più bassi (ddimero), meno frequenti alterazioni ECG,
solitamente stabilità emodinamica e assenza di disfunzioneVDx
TEP,CIO’CHELEGLNONDICONO:GESTIONETEPSUBSEGMENTARIA
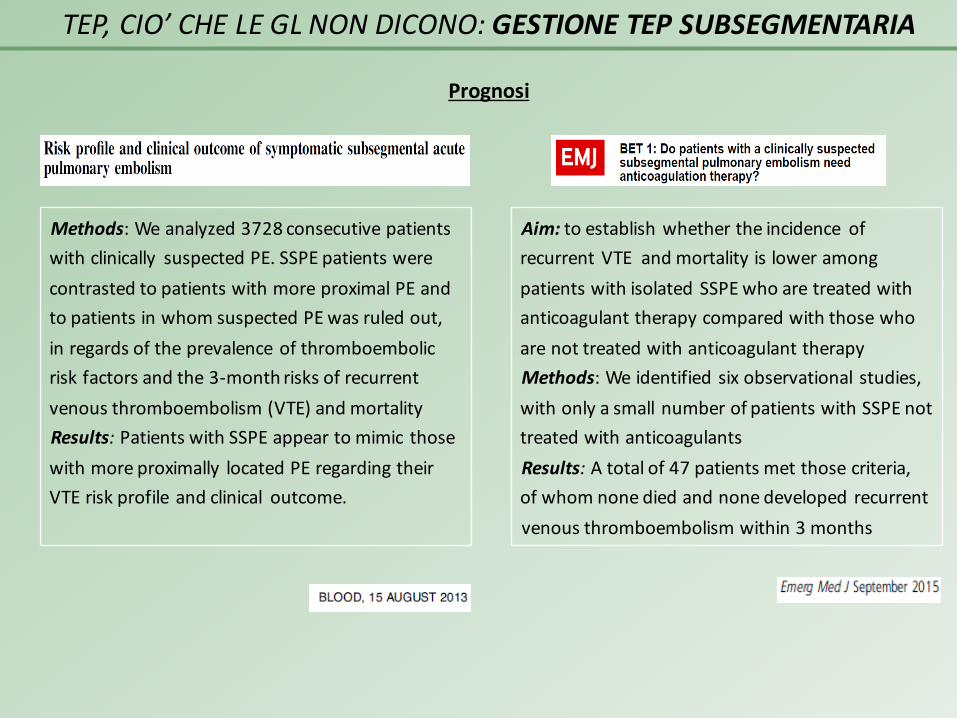
Methods:Weanalyzed3728consecutivepatientswithclinically suspectedPE. SSPEpatientswerecontrastedtopatientswithmoreproximalPEandtopatientsinwhomsuspectedPEwasruledout,inregardsoftheprevalenceofthromboembolicriskfactorsandthe3-monthrisksofrecurrentvenousthromboembolism(VTE)andmortalityResults:PatientswithSSPEappeartomimic thosewithmoreproximally locatedPEregardingtheirVTEriskprofileandclinical outcome.
Prognosi
Aim:toestablishwhethertheincidence ofrecurrentVTEandmortalityisloweramongpatientswithisolatedSSPEwhoaretreatedwithanticoagulanttherapycomparedwiththosewhoarenottreatedwithanticoagulanttherapyMethods:Weidentifiedsix observational studies,withonlyasmallnumberofpatientswithSSPE nottreatedwithanticoagulantsResults:Atotalof47patientsmetthosecriteria,ofwhomnonediedandnonedevelopedrecurrentvenousthromboembolismwithin3months

TEP,CIO’CHELEGLNONDICONO:GESTIONETEPSUBSEGMENTARIA
POSIZIONE DELLE LINEE GUIDA
Ø ESC Guidelines, 2014
• “The diagnostic value and clinical significance of sub-segmental defects on MDCT are
still under debate”
• “The definition of sub-segmental PE has yet to be standardized”
• “Further testing to confirm PE may be considered in case of isolated sub-segmental
clots (2b C)»
• “In a patient with isolated sub-segmental PE and non proximal DVT, the decision on
whether to treat should be made on an individual basis, taking into account the
clinical probability and the bleeding risk”

TEP,CIO’CHELEGLNONDICONO:GESTIONETEPSUBSEGMENTARIA
POSIZIONE DELLE LINEE GUIDA
Ø ACCPGuidelines2012:questionnotaddressed
Ø ACCPGuidelines,Update2016
• “Becausetheabnormalitiesaresmall,adiagnosisofsubsegmentalPEismorelikelytobe
false-positivefindingthanadiagnosisofPEinthesegmentalormoreproximalpulmonary
arteries”
• “BecauseatruesubsegmentalPEislikelytohavearisenfromasmallDVT,theriskof
progressiveorrecurrentVTEwithoutanticoagulationisexpectedtobelowerthanin
patientswithalargerPE”
• “ForsubsegmentalPEandnoproximalDVT,wesuggestclinicalsurveillanceover
anticoagulationwithalowriskofrecurrentVTE(Grade2C),andanticoagulationover clinical
surveillancewithahighrisk(Grade2C) ”

TEP,CIO’CHELEGLNONDICONO:GESTIONETEPSUBSEGMENTARIA

TEP,CIO’CHELEGLNONDICONO:GESTIONETEPINCIDENTALE
• PEsilenticlinicamente,individuateinmanierainattesa,pre- opost-mortem
• NettoincrementodellafrequenzadopointroduzionediscannerCTmultidetector
• Interessanoarterielobariosegmentalimaanchesubsegmentalietalvolta“acavaliere”
• Circalametàdeicasisonoindividuatisolodallarivalutazionedelleimmagini(radiologi
nonpreparatiacercarli,lesionidistraenti,piccoledimensioni)
• Riportatainpazientioncologici(1-5%)maanchenononcologici,contrauma,patologie
polmonariacute,sottopostiaventilazionemeccanicaoinautopsiepost-mortem
• Perdefinizioneinsospettaticlinicamentemapoiconrivalutazioneanamnesticamirata
sintomiosegninel44-75%,secondoalcuniautori
Tex Heart Inst J. 2013; 40(1): 9–12.
Thrombosis Research 2016: 138: 55–60

TEP,CIO’CHELEGLNONDICONO:GESTIONETEPINCIDENTALE

• Ignota la storia naturale, varia con quella della malattia di base
• Dati contrastanti sul ruolo prognostico (mortalità e morbosità)
• Non definita la gestione terapeutica, anche se
! frequenti in autopsie e generalmente non contribuivano al decesso
! casi misconosciuti alla prima diagnosi e per questo non trattati non sono
risultati associati a prognosi avversa
• In assenza di dati sull’efficacia del trattamento, nella maggior parte dei casi
vengono gestiti al pari delle embolie sintomatiche e come tali trattate
TEP,CIO’CHELEGLNONDICONO:GESTIONETEPINCIDENTALE
Tex Heart Inst J. 2013; 40(1): 9–12.
TEP,CIO’CHELEGLNONDICONO:GESTIONETEPINCIDENTALE
POSIZIONE DELLE LINEE GUIDA
Ø ESC Guidelines, 2014
• Someexpertsbelievethatpatientswithincidental(unsuspected)PEonCTshouldbe
treated,especiallyiftheyhavecancerandaproximalclot,butsolidevidencein
supportofthisecommendationislacking.
• Theirsignificance,particularlyiflimitedtosegmentalorsub-segmentalarteries,is
unclear;however,inviewofthehighriskofanadverseoutcomereportedby
uncontrolledstudies,thetreatmentstrategiesrecommendedforsymptomaticPE
shouldbealsoconsideredforincidentalPEfoundinpatientswithmalignancy
• IncidentalPEinpatientswithcancershouldbemanagedinthesamemanneras
symptomaticPE.(gradeIIaC)

POSIZIONEDELLELINEEGUIDA
Ø ACCPGuidelines2012
• InpatientswhoareincidentallyfoundtohaveasymptomaticPE,we
suggestthesameinitialandlong-termanticoagulationasforcomparable
patientswithsymptomaticPE(grade2B)
TEP,CIO’CHELEGLNONDICONO:GESTIONETEPINCIDENTALE

TEP,CIO’CHELEGLNONDICONO:DIFFICOLTA’DIAGNOSTICHE
ACCURATEZZACTA- Sensibilità =83%- Specificità=96%- VPP=86%- VPN=95%
Conclusion: The predictive value of either CTA or CTA–CTV is high with a concordant
clinical assessment, but additional testing is necessary when clinical probability is
inconsistent with the imaging results.

TEP,CIO’CHELEGLNONDICONO:DIFFICOLTA’DIAGNOSTICHE
• PIOPED II investigators recommend stratification of all patients with suspected PEaccording to an objective probability assessment. In patients with discordant findings onclinical assessment and CT imaging, further evaluation depends on clinical judgment

TEP,CIO’CHELEGLNONDICONO:DIFFICOLTA’DIAGNOSTICHE
Technical
Breathing
Rippling
Bolus-related
Streakartifacts
Windowssetting
Anatomical
Volumeaveragingartifacts
Vessel orientation
Bronchovascularanatomy
Lymphnodesandperibronchovasculartissue
Mucous-filledbronchus
Patient-related
Obesity
Pulmonarydieases
Vascularvasoconstriction
Arteryobstructionduetoextrinsiccompression
Pulmonaryarterialcatheters
PitfallsinCTdiagnosisofacutePE
SeminarsinRoentgenology,2015

TEP,CIO’CHELEGLNONDICONO:DIFFICOLTA’DIAGNOSTICHE
Aim:ToquestiontheconventionaltheorythatPEareabnormalandtotestthehypothesisthatsmallperipheralPEareafunctionoflife
Methods:Thestudygroupincluded26womenand24menwithPEandalower-extremityvenousUSperformedwithin7daysoftheCT.ThelocationsofthePEwereplottedonapulmonaryarterialdiagram,andwidthofthemostproximalclotforeachpatientwasmeasured
Results:33(66%)patientshadPEinthecentralpulmonaryarteries,ofwhich19(58%)hadDVT.17(34%)patientshadperipheralPE;DVTwasdetected in0(0%)patients.Theperipheral clotsmeasured1.0–3.8mm(mean2.5mm),theyappearedfocalandroundedwitha“dotlike”appearance.
Conclusion:Peripheral,focalfillingdefectsinthepulmonaryarteries,whichwetermed“dots,”arenottraditionalembolicclots,arenotassociatedwithdetectable lower-extremityclot loadandmayrepresent“normal”embolicactivityoriginating fromthelowerextremityvenousvalvesinaphysiologicprocesswiththelungcapillary bedstrappinganddissolvingtheembolibyendogenousfibrinolysis,therebyprotectingthesistemiccirculation

TEP,CIO’CHELEGLNONDICONO:QUANDOCERCAREUNATEP?
• “Fishing” is rampant. By fishing, I mean scanning the body part thought to be the source of the
patient's complaint or problem, hoping thereby to reel in some sort of diagnosis. This sport
typically takes place in the emergency department
• In this scenario, a primary diagnosis of PE occasionally turns out to be right. Much more
commonly, however, critical review of the pre-test evidence clearly points to a different diagnosis
that could and should have been made presentation Nevertheless once these defects are
detected all thinking stops and anticoagulation automatically ensues
• I wonder how many normal, asymptomatic volunteers would have filling defects in their
pulmonary arteries if they were to undergo conventional pulmonary arteriography or contrast-
enhanced multidetector chest CTTex Heart Inst J. 2013; 40(1): 9–12.
TEP,CIO’CHELEGLNONDICONO:QUANDOCERCAREUNATEP?
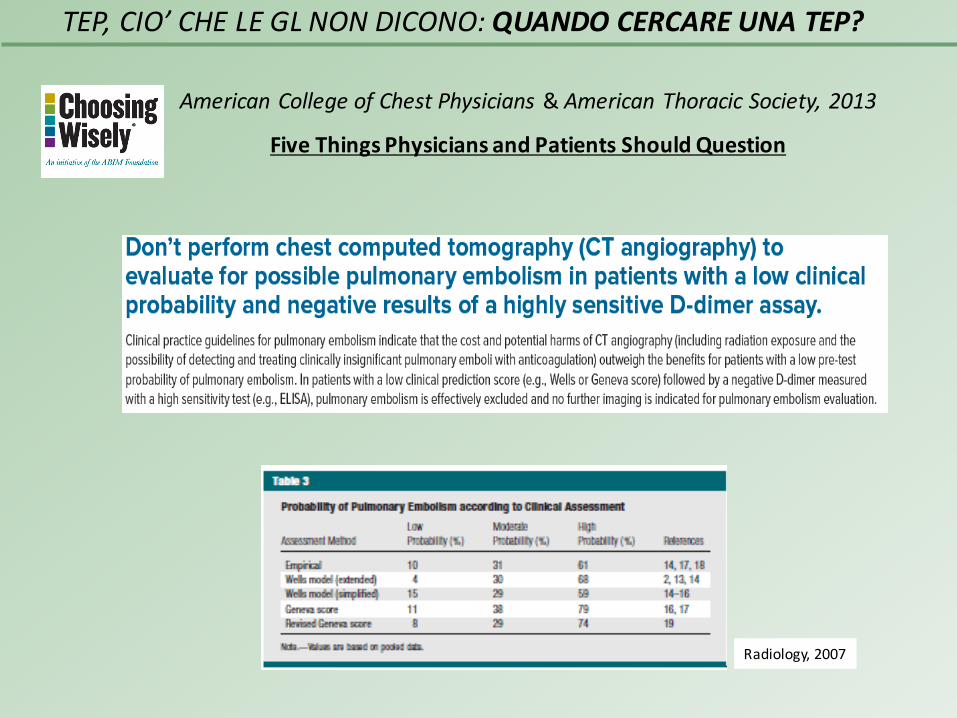
AmericanCollegeofChestPhysicians&AmericanThoracicSociety,2013
FiveThingsPhysiciansandPatientsShouldQuestion
Radiology,2007

TEP,CIO’CHELEGLNONDICONO:QUANDOCERCAREUNATEP?
In caso di TVP: SI'!
AIM:Todetermine,bysystematicreviewoftheliterature, theprevalenceofsilentPEinpatientswithdeepvenousthrombosisRESULTS:SilentPEwasdiagnosedin1665of5233patients(32%)withdeepvenousthrombosis.Theincidence ofsilentPEwashigherwithproximaldeepvenousthrombosisthanwithdistaldeepvenousthrombosis.SilentPEseemedtoincreasetheriskofrecurrentPE:25of488(5.1%)withversus7of1093(0.6%)withoutsilentPE

TEP,CIO’CHELEGLNONDICONO:QUANDOCERCAREUNATEP?
In caso di TVP: NO!
Methods:Aprospectiveandconsecutiveassessmentof103hospitalizedpatientswithlowerlimb
DVTintheabsenceofPEsymptoms,usingCTscan.D-dimerwasquantifiedbefore
anticoagulation.
Results: Theincidence ofS-PEwas66%.In77%ofthesecases,themainandlobarpulmonary
arterieswereaffected.IliacandfemoralDVTsmostoftenproducedS-PE.Diagnosisentailedhigher
hospitalizationexpenses.Nosignificant recurrence rateofthromboticeventswasobservedinthe
S-PEgroupduringthefollow-up.
Conclusions:Theincidence ofS-PEinlower-limbDVTishigh,butintheabsenceofsymptoms,
diagnosisdoesnotappeartobenecessary,astherearenoshort- orlong-termclinical or
therapeuticconsequences.

In caso di TVP: SI’, MA SOLO IN ALCUNE OCCASIONI
TEP,CIO’CHELEGLNONDICONO:QUANDOCERCAREUNATEP?
Purpose: The purpose of this investigationwas to determine the prevalence of silent PE in
patients with deep venous thrombosis (DVT) limited to the calf veins.
Results: The prevalence of silent PE in patients with DVT limited to the calf veins was
described in 6 investigations. Pooled data showed a prevalence of 24 of 183 (13.1%)
Conclusion: Silent PE in patients with DVT limited to the calf veins is not rare. Imaging at
the time of diagnosis of calf vein DVT, typically with a perfusion scan alone, may be useful,
but there is an economic cost and exposure to radiation.
TEP,CIO’CHELEGLNONDICONO:RISOLUZIONEDELTROMBOEOSTRUZIONERESIDUA
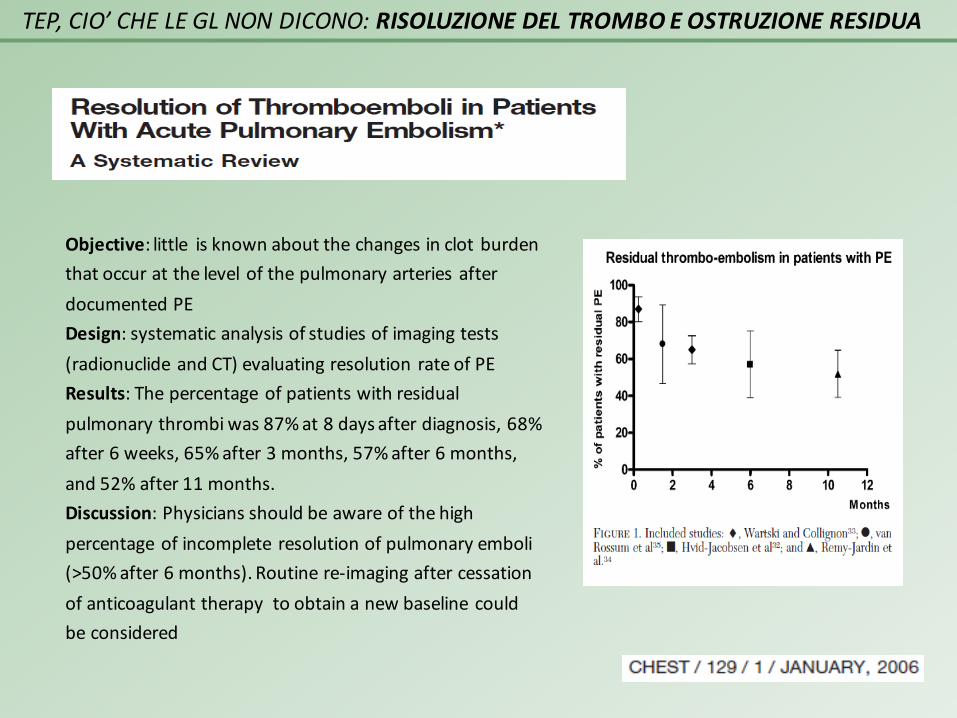
Objective:little isknownaboutthechangesinclotburdenthatoccuratthelevelofthepulmonaryarteriesafterdocumentedPEDesign:systematicanalysisofstudiesofimagingtests(radionuclideandCT)evaluatingresolution rateofPEResults:Thepercentageofpatientswithresidualpulmonarythrombiwas87%at8daysafterdiagnosis,68%after6weeks,65%after3months,57%after6months,and52%after11months.Discussion:Physiciansshouldbeawareofthehighpercentageofincomplete resolutionofpulmonaryemboli(>50%after6months).Routinere-imagingaftercessationofanticoagulanttherapytoobtainanewbaselinecouldbeconsidered

TEP,CIO’CHELEGLNONDICONO:RISOLUZIONEDELTROMBOEOSTRUZIONERESIDUA
Fonte Fattorepredittivo
AmJRoentgenol,2010 Calibrodellearteriecoinvolte(primase>)
InternEmergMed,2011 Età;coesistentepneumopatia
EurJInternMed,2012 Burdentromboticoiniziale;alterazioneemogasanalitica;precedentiepisodi diTVE
AmJRoentgenol,2013 Calibrodellearteriecoinvolte(primase<)
BloodCoagulFibrinolysis, 2015 Dimensionedell’embolo
Risoluzionedeltrombo:fattoripredittivi

TEP,CIO’CHELEGLNONDICONO:RISOLUZIONEDELTROMBOEOSTRUZIONERESIDUA

TEP,CIO’CHELEGLNONDICONO:RISOLUZIONEDELTROMBOEOSTRUZIONERESIDUA
Aim: to investigate the rate of clot resolutionover time and identify risk factors of residualemboli in PE patientsMethods: We retrospectively analyzed 764 PEpatients with follow-up CT scans between day 3and 90. They were classified into 3 cohorts,based on the time of scan: day 3–7, 8–21, 22–90Results: The rate of complete resolution ofpulmonary emboli was 24% at 3–7 days, 47% at8–21 days and 78% at 22–90 days. Regardless ofthe time interval, larger pulmonary arteryinvolvement was only independent predictor ofresidual emboli. The presence of residual emboliwas not associated with an adverse outcome ofPE and rate of VTE recurrence
Aim: to assess the impact of RPO on the
development of recurrent symptomatic
VTE episodes and/or CTPH
Methods: The long-term follow-up was
obtained in 16 patients with and in 89
without RPO.
Results: We did not find any correlation
between RPO, assessed by CT scanning six
months after PE, and the development of
late complications

TEP,CIO’CHELEGLNONDICONO:RISOLUZIONEDELTROMBOEOSTRUZIONERESIDUA
POSIZIONE DELLE LINEE GUIDA
Ø ESCGuidelines, 2014
Chronic thromboembolic pulmonaryhypertension is a debilitating disease causedby chronic obstruction of major pulmonaryarteries. CTPH has been reported to be along-term complication of PE, with areported cumulative incidence of 0.1–9.1%within the first two years after asymptomatic PE event

TEP,CIO’CHELEGLNONDICONO:DIMISSIONEPRECOCE
Chest 2016 Feb 18
ActualmanagementofPE

TEP,CIO’CHELEGLNONDICONO:DIMISSIONEPRECOCE
POSIZIONE DELLE LINEE GUIDA
Ø ACCPGuidelines,2012
Ø ESC Guidelines, 2014
Ø ACCP Guidelines, Update 2016

TEP,CIO’CHELEGLNONDICONO:DIMISSIONEPRECOCE
Evidenzedisponibiliinletteratura

TEP,CIO’CHELEGLNONDICONO: DIMISSIONEPRECOCE
Evidenzedisponibiliinletteratura
Introduction:StudiesofoutpatientcareafterPEwererestrictedbysmall samplesizes,retrospectivedesignsandtheabsenceofarandomisedcontrolgroupforcomparisonwithinpatientcareMethods344patientswithacute,symptomaticPEalowriskofdeath(PESIriskclasses IorII)assignedtoinitialoutpatient(discharged≤24h)orinpatient treatmentwithsubcutaneousenoxaparin(≥5days)followedbyoralanticoagulation (≥90days).Theprimaryoutcomewassymptomatic,recurrentVTEwithin90days;safetyoutcomesincludedmajorbleedingwithin14or90daysandmortalitywithin90days.Findings 1(0,6%)of171outpatientsdevelopedrecurrentvenousthromboembolismwithin90dayscomparedwithnoneof168inpatient.Only1(0,6%)patientineach treatmentgroupdiedwithin90days,and2(1,2%)of171outpatientsandnoinpatientshadmajorbleedingwithin14days.By90days,3(1,8%)outpatientsbutnoinpatientshaddevelopedmajorbleedingMeanlengthofstaywas0,5daysforoutpatientsand3,9daysforinpatients.InterpretationInselected low-riskpatientswithPE,outpatientcarecansafelyandeffectivelybeusedinplaceofinpatientcare

TEP,CIO’CHELEGLNONDICONO:DIMISSIONEPRECOCE
Evidenzedisponibiliinletteratura

TEP,CIO’CHELEGLNONDICONO:DIMISSIONEPRECOCE
Lastratificazionedelrischio
Rulesbasedonasamplesetofclinical criteria
Erkens,2010;Kovacs,2010;Zondag,2010;Davies,2007;Rodriguez-Cerrillo,2009;Wells,2005
Parameters as:SBP,spO2,age>18,CrCl>30Clinicalconditionsas:nocontroindicationsforEPWH,nocomorbidities,noneedforparenteralnarcotics,nohighriskforhemorrage,noneedfortrombolysis,nopregnancy,noHF,norenalorliverimpairment,patientcompliance
Prognosticrulesbasedonclinical findings
PESI,2005 Variables:age;malegender;cancer; HF;COPD;HR>110;SBP<100;RR>30breaths/min;T<36C°;alteredmental status;spO2<90%
SimplifiedPESI,2010 Variables:age>80;cancer;HForCOPD;HR>110;SBP<100;spO2<90%
Spanishscore,2007 Variables:severebleeding;cancer;serumCr>2mg/dL; immobilization,nosurgeryinthepast2months,age>60
Geneva,2000 Variables:cancer;previousDVT;HF;SBP<100;DVTshownbyUS;PaO2<8.5kPa
Prognosticrulescombiningclinical data,biomarkersandimagingdata
ESCscore,2014 Variables:shockorhypotension;PESIIIIorIV; signsofRVdysfunction;biomarkers
LR-PEDscore,2012 Variables:age;chronicHF;AF;HR;troponinI;creatinin;glucoselevel;PCR
PREPscore,2010 Variables:cancer;cardiacorrespiratorydiseases; cardiogenicshock;alteredmentalstatus;BNP;righttoleftventriclediameterratio
PROTECT Variables:sPESI;troponinI;BNP;lowerlimbUS
FAST Variables:H-FABP;HR;syncope
Journal ofThrombosis andHaemostasis, 2015Journal ofThrombosis andHaemostasis, 2015
TEP,CIO’CHELEGLNONDICONO:CONCLUSIONI
l L’utilizzo di esami strumentali molto sensibili e di procedimenti diagnostici
spesso non basati sulla PPT comporta il rischio di overdiagnosis ed il
crescente riscontro di casi di PE subsegmentale o incidentale né è la
conferma. Nella quasi totalità di questi casi viene intrapresa terapia
anticoagulante ma questa è una pratica non basata sull’evidenza. Vi è uno
stringente bisogno di LG che consentano di selezionare pazienti a basso
rischio da destinare a regime di sola osservazione clinica, risparmiando i
rischi legati al trattamento. Diversamente i medici continueranno a
prescrivere terapia anticoagulante, anchepermotivi medico-legali

§ Non conoscendo in modo chiaro i meccanismi che presiedono alla
completa risoluzione del trombo né il suo significato prognostico, non
sembra giustificata la ripetizione sistematica di TC per ricerca di una
ostruzione vascolare residuamediante esami strumentali
§ Per identificare i pazienti a rischio per CTPH, sembra ragionevole
seguire l’iter suggerito dalle GL ESC (sospetto clinico > ECO > V/P scan
> conferma con angiografia, TC o RMN)
TEP,CIO’CHELEGLNONDICONO:CONCLUSIONI

§ Nel corso degli ultimi anni si è assistito ad una riduzione della durata
della degenza per PE anche se, almeno in Europa, l'ospedalizzazione
resta ancora mediamente prolungata (9-10 gg) ma non tutte le PE
sono uguali e talvolta in caso di pazienti a basso rischio appare
possibile una dimissione precoce
§ L'esecuzione di RCT da cui provengano evidenze forti nonché, forse,
l'utilizzo dei NAO potrebbero ottimizzare la gestione dei pazienti con
PE consentendo dimissione precoce dei pazienti a basso rischio con
notevole risparmio di risorse
TEP,CIO’CHELEGLNONDICONO:CONCLUSIONI

Grazieperl’attenzione!!
TEP,CIO’CHELEGLNONDICONO
![Stenosi polmonare Divulgativa [modalità compatibilità] · •L’arteria polmonare è il vaso sanguigno che ... •Persistenza del dotto arterioso ... Valvuloplastica polmonare](https://static.fdocuments.net/doc/165x107/5c694bea09d3f290788cdd77/stenosi-polmonare-divulgativa-modalita-compatibilita-larteria-polmonare.jpg)