E/M: Coding Opportunities- Documentation is key€¦ · E/M: Coding Opportunities-Documentation is...
35
E/M: Coding Opportunities- Documentation is key Compiled and Presented by: Suzan Berman CPC, CEMC, CEDC The duplication of this presentation, all or in part, without the expression permission of the presenter, is strictly prohibited.
Transcript of E/M: Coding Opportunities- Documentation is key€¦ · E/M: Coding Opportunities-Documentation is...
E/M: Coding Opportunities-Documentation is key
Compiled and Presented by:Suzan Berman CPC, CEMC, CEDC
The duplication of this presentation, all or in part, without the expression permission of the presenter, is strictly prohibited.
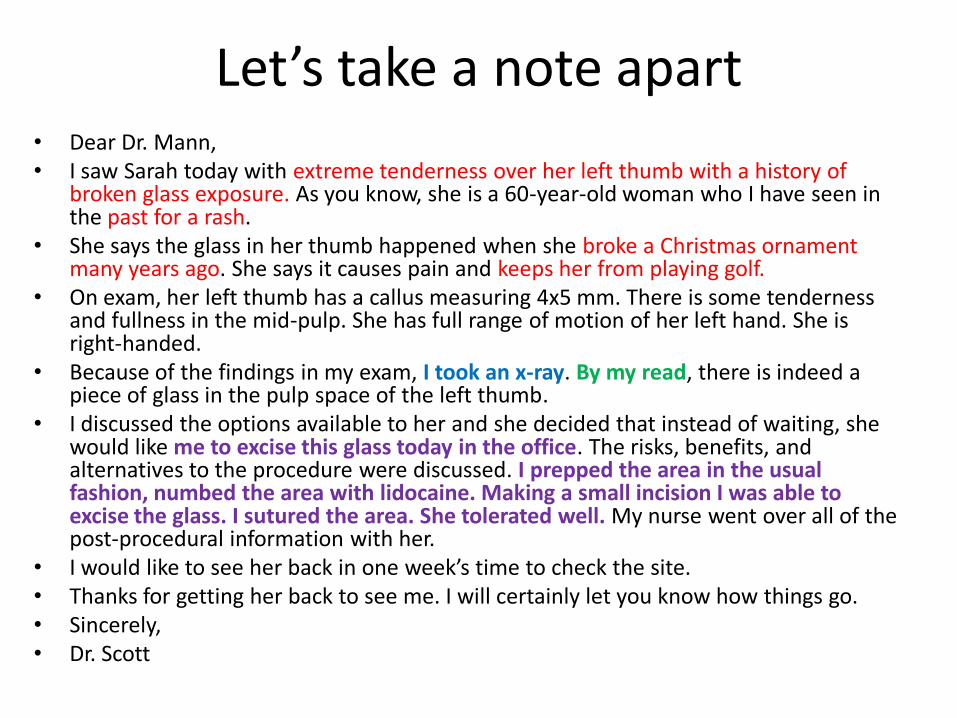
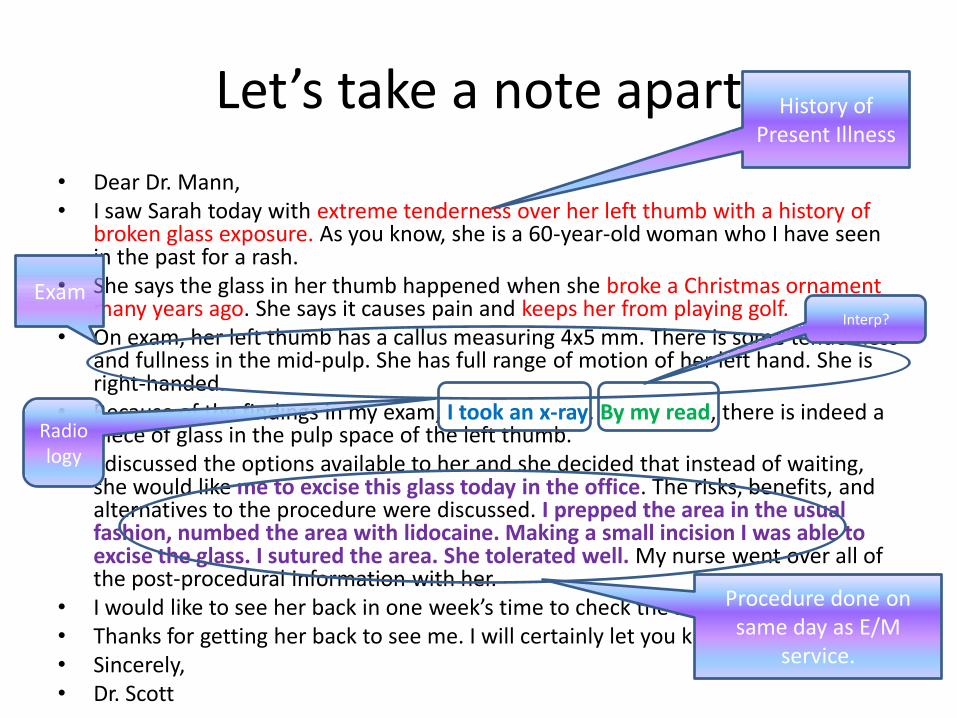
Let’s take a note apart• Dear Dr. Mann,• I saw Sarah today with extreme tenderness over her left thumb with a history of
broken glass exposure. As you know, she is a 60-year-old woman who I have seen in the past for a rash.
• She says the glass in her thumb happened when she broke a Christmas ornament many years ago. She says it causes pain and keeps her from playing golf.
• On exam, her left thumb has a callus measuring 4x5 mm. There is some tenderness and fullness in the mid-pulp. She has full range of motion of her left hand. She is right-handed.
• Because of the findings in my exam, I took an x-ray. By my read, there is indeed a piece of glass in the pulp space of the left thumb.
• I discussed the options available to her and she decided that instead of waiting, she would like me to excise this glass today in the office. The risks, benefits, and alternatives to the procedure were discussed. I prepped the area in the usual fashion, numbed the area with lidocaine. Making a small incision I was able to excise the glass. I sutured the area. She tolerated well. My nurse went over all of the post-procedural information with her.
• I would like to see her back in one week’s time to check the site.• Thanks for getting her back to see me. I will certainly let you know how things go.• Sincerely,• Dr. Scott
Let’s look at the details
• History– HPI
– ROS
– PFSH
• Exam– 1995 vs. 1997
– Problem focused vs. Expanded Problem Focused
• Decision Making– New problem vs.
Established
– Risk level
• Code choices– New patient?
– Established patient?
– Consultation?
• Additional services?
History of Present Illness
Let’s take a note apart
• Dear Dr. Mann,• I saw Sarah today with extreme tenderness over her left thumb with a history of
broken glass exposure. As you know, she is a 60-year-old woman who I have seen in the past for a rash.
• She says the glass in her thumb happened when she broke a Christmas ornament many years ago. She says it causes pain and keeps her from playing golf.
• On exam, her left thumb has a callus measuring 4x5 mm. There is some tenderness and fullness in the mid-pulp. She has full range of motion of her left hand. She is right-handed.
• Because of the findings in my exam, I took an x-ray. By my read, there is indeed a piece of glass in the pulp space of the left thumb.
• I discussed the options available to her and she decided that instead of waiting, she would like me to excise this glass today in the office. The risks, benefits, and alternatives to the procedure were discussed. I prepped the area in the usual fashion, numbed the area with lidocaine. Making a small incision I was able to excise the glass. I sutured the area. She tolerated well. My nurse went over all of the post-procedural information with her.
• I would like to see her back in one week’s time to check the site.• Thanks for getting her back to see me. I will certainly let you know how things go.• Sincerely,• Dr. Scott
Exam
Radiology
Interp?
Procedure done on same day as E/M
service.
Clearly state Chief Complaint
• This can be written in the patient’s words.
• This is the reason for the encounter.
• A specific reason, not just a follow up is suggested.

Are these clear chief complaints?
• Patient is here for follow up.
• Mrs. Esher says her wound is still open.
• Patient is here to establish.
• No complaints.
• Patient presents for follow-up after hernia surgery.
Very good Chief Compliant and beginning of HPI
I saw Sarah today with extreme tenderness over her left thumb with a history of broken glass exposure.

History of Present Illness
• …with extreme tenderness over her left thumb with a history of broken glass exposure. As you know, she is a 60-year-old woman who I have seen in the past for a rash. She says the glass in her thumb happened when she broke a Christmas ornament many years ago. She says it causes pain and keeps her from playing golf.
• Extreme-Severity
• Tenderness-Sign/ Symptom
• Broke a Christmas ornament-Context
• Many years ago-Duration
• Keeps her from playing golf-Severity
• This is an extended HPI

As compared to this HPI…
• The patient’s wound is open, oozing, odorous, and red. It’s been like this for two days. She denies pain in this area.
• Location?
• Quality?
• Severity?
• Duration or Timing?
• Signs/Symptoms?
• Post op?
ROS and PFSH
• …I have seen in the past for a rash.
• No Review of systems was noted.
• Past history
– Prior illness-rash
Review of systems tips
• If a patient completes a compliant patient information sheet, when reviewed by the physicians, this information can be used toward the billed level of service.– Make certain it is
complete
– Sign and date the form
• Past, Family and Social history elements can also be included on this form.
What’s included in Past, Family, and Social Histories
• Past History
Allergies
Current Medications
Immunizations
Previous Trauma
Surgeries
Previous Illness
Previous Hospitalizations
• Social History Drug Use Alcohol
Consumption Tobacco Use Employment Sexual HistoryMarital Status Education Occupational
history
Past? Social?
• Patient denies any prior illnesses.
• Patient is a vegetarian.
• Patient is on OTC vitamins.
• Mr. Frank is on no medications.
• Patient has 2 dogs and 1 cat.
• G10 P8 A2
• Patient is a retired coal miner.
• Previous Illnesses?
• Dietary Status?
• Medications?
• Medications?
• Living arrangements?
• Sexual History?
• Occupational History? Employment?

• Health of Parents or cause and age of death
• Health of Siblings and Children
• Family Members with disease related to the Chief Complaint
Family History
• Non-contributory• Unremarkable
• What do these words really mean?
• Patient is adopted.• Patient has dementia
and doesn’t recall having a mother.

Review of Systems-14 systems• Constitutional• Eyes• Ears, Nose, Mouth/Throat• Cardiovascular• Respiratory• Gastrointestinal• Genitourinary• Allergic/Immunologic• Integumentary• Neurological• Endocrine• Psychiatric• Hematologic/ Lymphatic• Musculoskeletal• All others reviewed and
negative
• Review of systems is non-contributory.– Was it reviewed?
• ROS was unobtainable.– Why?
• All systems are negative.– What brought the
patient in to the office?
• See as above in HPI, ROS unremarkable.– Is there enough
information?
What if the history components are unobtainable?
• In order to get the proper credit for the history retrieval, you must document the following:– Any attempts you made to get the history
• “I spoke with the resident/nurse/family to gather the patient’s medications.”
– Why weren’t these details obtainable?• “The patient’s condition was of an urgent nature. Gathering the
social history was not warranted at this time.”
• “Gathering the patient’s family history was not pertinent to the patient’s emergent condition.”
• “Patient suffers from dementia and is a poor historian.”
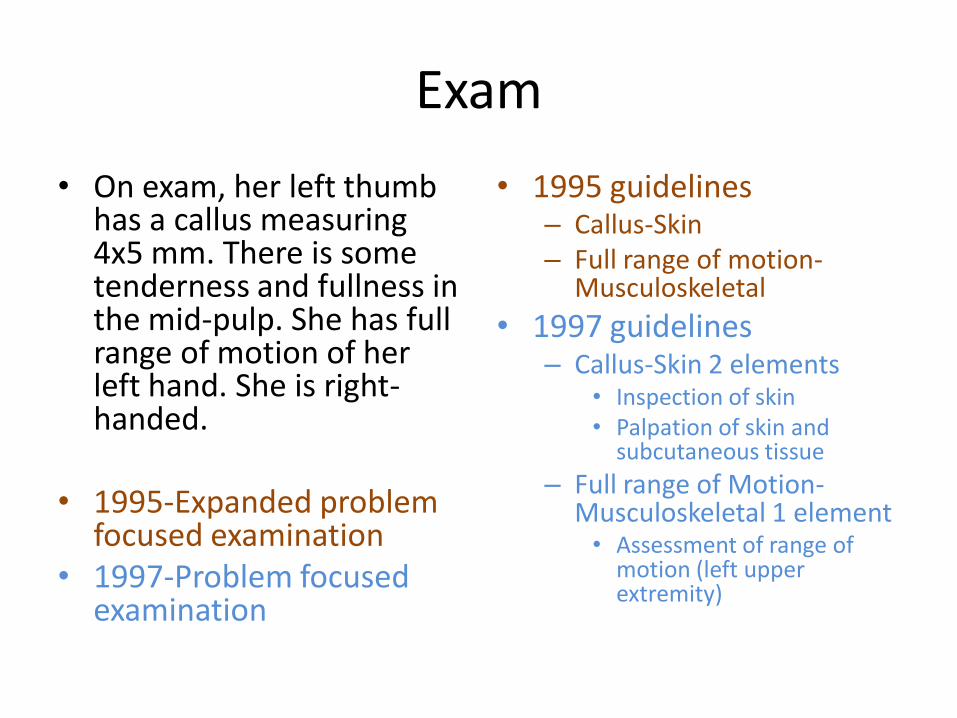
Exam
• On exam, her left thumb has a callus measuring 4x5 mm. There is some tenderness and fullness in the mid-pulp. She has full range of motion of her left hand. She is right-handed.
• 1995-Expanded problem focused examination
• 1997-Problem focused examination
• 1995 guidelines– Callus-Skin– Full range of motion-
Musculoskeletal
• 1997 guidelines– Callus-Skin 2 elements
• Inspection of skin• Palpation of skin and
subcutaneous tissue
– Full range of Motion-Musculoskeletal 1 element• Assessment of range of
motion (left upper extremity)
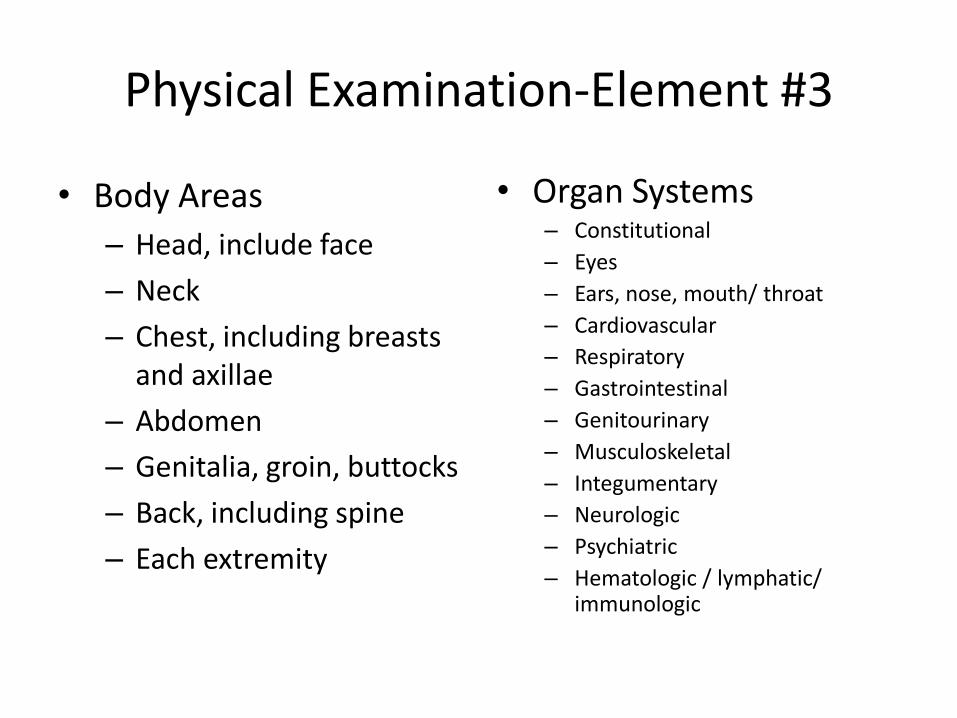
Physical Examination-Element #3
• Body Areas
– Head, include face
– Neck
– Chest, including breasts and axillae
– Abdomen
– Genitalia, groin, buttocks
– Back, including spine
– Each extremity
• Organ Systems– Constitutional
– Eyes
– Ears, nose, mouth/ throat
– Cardiovascular
– Respiratory
– Gastrointestinal
– Genitourinary
– Musculoskeletal
– Integumentary
– Neurologic
– Psychiatric
– Hematologic / lymphatic/ immunologic
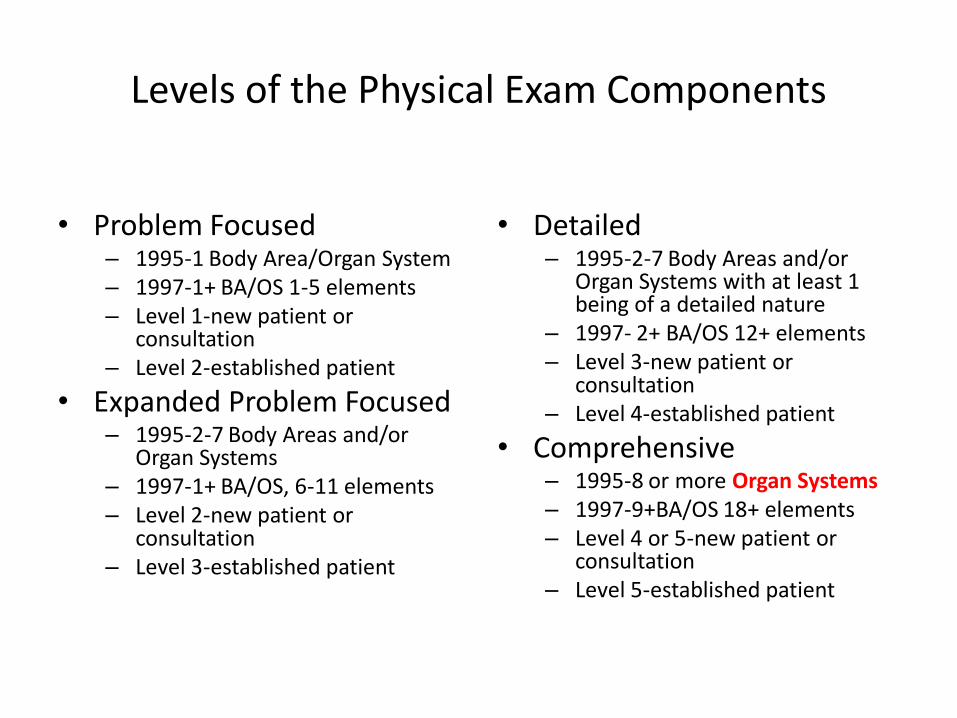
Levels of the Physical Exam Components
• Problem Focused– 1995-1 Body Area/Organ System– 1997-1+ BA/OS 1-5 elements– Level 1-new patient or
consultation– Level 2-established patient
• Expanded Problem Focused– 1995-2-7 Body Areas and/or
Organ Systems– 1997-1+ BA/OS, 6-11 elements– Level 2-new patient or
consultation– Level 3-established patient
• Detailed– 1995-2-7 Body Areas and/or
Organ Systems with at least 1 being of a detailed nature
– 1997- 2+ BA/OS 12+ elements– Level 3-new patient or
consultation– Level 4-established patient
• Comprehensive– 1995-8 or more Organ Systems– 1997-9+BA/OS 18+ elements– Level 4 or 5-new patient or
consultation– Level 5-established patient

Some common questions concerning the exam portion of the visit.
• Can you combine Body Areas and Organ Systems?
• What’s the difference between Expanded Problem-Focused and Detailed examinations?
• What’s considered a complete single system examination under 1995 guidelines?

Can you combine Body Areas and Organ Systems?
• It depends on where you are.• Although the guidelines could
be interpreted as to combine these, you’ll want to check with your local Medicare carrier.
• Some will allow the mix– Trailblazers Health
• Some specifically state that this is not acceptable.– Highmark Medicare Services
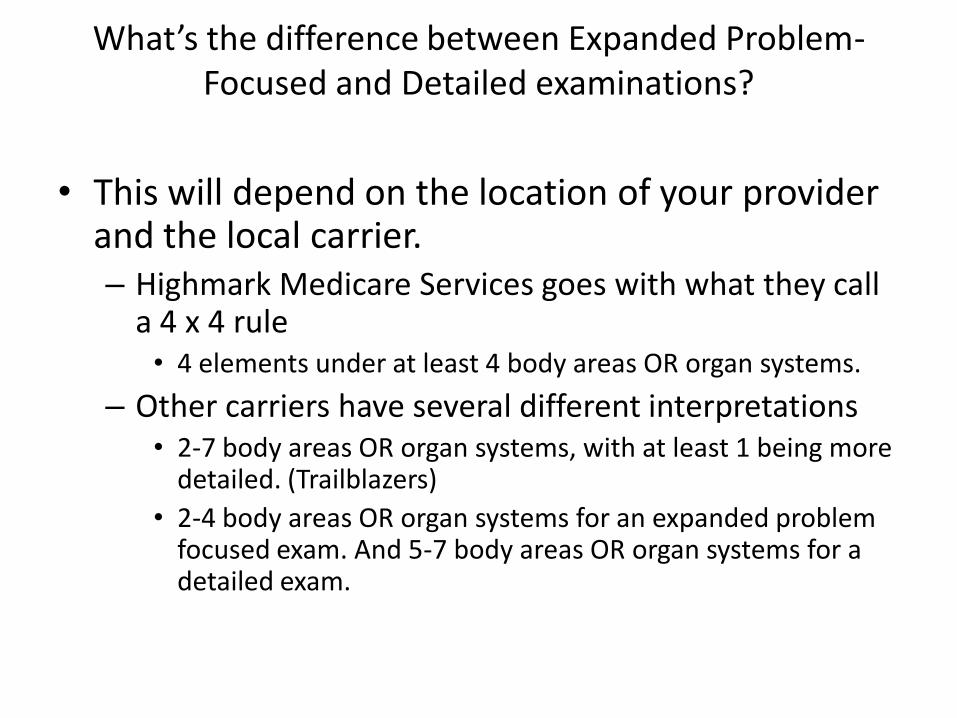
What’s the difference between Expanded Problem-Focused and Detailed examinations?
• This will depend on the location of your provider and the local carrier.– Highmark Medicare Services goes with what they call
a 4 x 4 rule• 4 elements under at least 4 body areas OR organ systems.
– Other carriers have several different interpretations• 2-7 body areas OR organ systems, with at least 1 being more
detailed. (Trailblazers)
• 2-4 body areas OR organ systems for an expanded problem focused exam. And 5-7 body areas OR organ systems for a detailed exam.
What’s considered a complete single system examination under 1995 guidelines?
• The guidelines do not stipulate what would constitute a complete single organ examination.
– Specialty societies as well as physician colleges may have suggestions on how to fulfill this requirement.
– It has also been said it is self-defined by the physician.
Where can this count?
• HEENT-Normal
• Abdomen-small scar from prior appendectomy
• No jaundice or pallor
• Breast exam is completely benign.

Exam elements explained
• H, E, ENT-what’s normal?– Highmark Medicare
Services says you can credit each of these body areas/organ systems.
– Best practice might be to indicate normal for each recognized element.
• Abdomen-small scar from prior appendectomy– Remember that the
category in which the element is mentioned might not be the category to which credit should be given.
– In this case, the element describes the skin of the abdomen and therefore should be counted under SKIN, not GI.
Other Exam elements
• Breast exam is completely benign.
– Skin?
– Genitourinary?
– Body Area of Breast only?
• No jaundice or pallor
– Skin vs. Eyes?
• The answer is:
– Either-look at the further description of the examination.
Medical decision-making or other service
• I took an x-ray. By my read…
• If you are billing for the x-ray, both the technical and professional component can be billed.
• If these are billed, then the read cannot be counted again in the MDM section

Medical Decision-Making
• Management options– Self limited/minor
– Established problem
– Worsening problem
– New problem
– Work up for new problem
• Amount and complexity of data– review/order of clinical labs– review/order tests in radiology
section– review/order tests in medicine
section– discussion of test results with
performing physician– independent review of image,
tracing or specimen– decision to obtain old records– obtain history from someone
other than patient– review AND summarize old
records
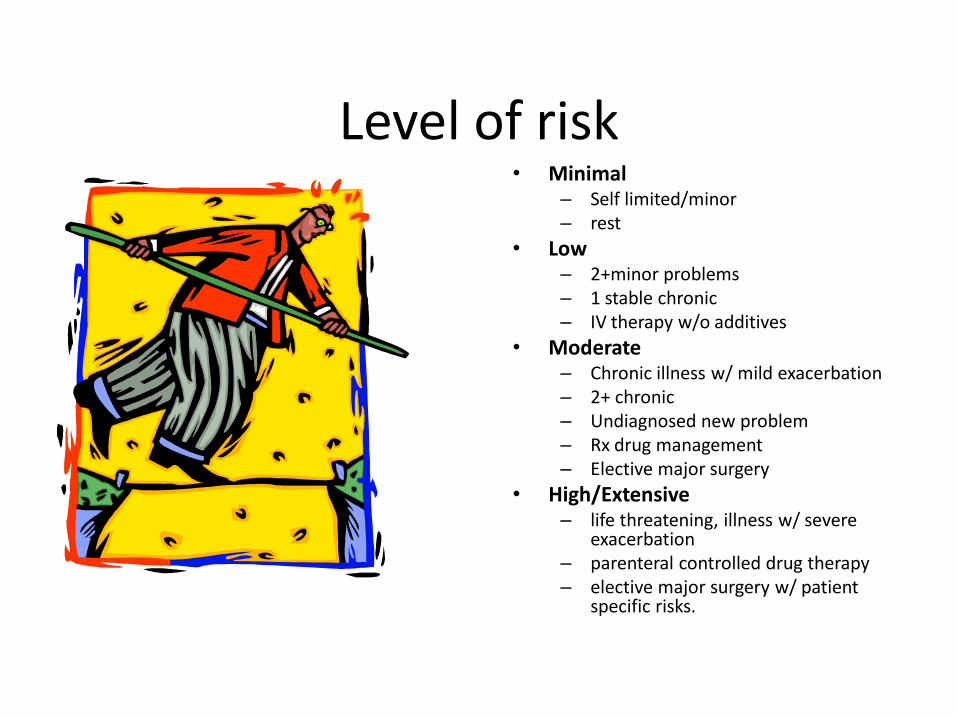
Level of risk• Minimal
– Self limited/minor– rest
• Low– 2+minor problems– 1 stable chronic– IV therapy w/o additives
• Moderate– Chronic illness w/ mild exacerbation– 2+ chronic– Undiagnosed new problem– Rx drug management– Elective major surgery
• High/Extensive– life threatening, illness w/ severe
exacerbation– parenteral controlled drug therapy – elective major surgery w/ patient
specific risks.

When is a patient considered new?
• If you have never seen the patient either in your office or the hospital.
• When the patient has never been seen by anyone within your group in the same specialty within the last 3 years.
…As you know, she is a 60-year-old woman who I have seen in the past for a rash.We can’t tell from the note how long ago this was.
What is a consult?• A consult involves
meeting the following criteria:– Another physician has
asked your opinion on a particular aspect of the care of his/her patient.
– There is documentation in the patient’s medical record that this request has been made
– The service is rendered by you in your office or the hospital.
– You, then, document your findings and/or recommendations in a written report back to the requesting physician.
• There are two types of consultations– Office or other out-patient
facility (99241-99245)
– In-house (99251-99255)
• Medicare no longer recognizes these code sets
I saw Sarah today with extreme tenderness over her left thumb with a history of broken glass exposure. As you know, she is a 60-year-old woman who I have seen in the past for a rash….
…Thanks for getting her back to see me. I will certainly let you know how things go.
Does this verbiage satisfy the consultation criteria?
Procedure on the same day as a visit
• …me to excise this glass today in the office. The risks, benefits, and alternatives to the procedure were discussed. I prepped the area in the usual fashion, numbed the area with lidocaine. Making a small incision I was able to excise the glass. I sutured the area. She tolerated well.
• Add the -25 modifier to the E/M service
• The E/M service, the procedure, and the x-ray can all be billed for the services rendered at this visit.
And then there’s modifiers…
• -25• Consultation in the ER
with a simple Incision and Drainage to follow
• A floor consultation for a chest tube insertion
• Procedure done in the office on the same day as a visit
– Both are separately identifiable
• -57• Consultation in the ER for
rupture appendix
• Motor vehicle accident with unknown injuries-exploratory laporotomy
• Office visit with immediate admission to hospital for surgery the next morning
– Major procedure done on the same day or the next calendar day after a visit

How it all adds up!Must meet or exceed 3 out of 3 for new patients and all consultsE&M Code History Exam DecisionMaking
Level 1- Problem Focused Problem Focused Straightforward Level 2- Expanded PF Expanded Problem Focused Straightforward Level 3- Detailed Detailed Low Level 4- Comprehensive Comprehensive Moderate Level 5- Comprehensive Comprehensive High
Must meet or exceed 2 out of 3 for established pts./ subsequent visitsLevel 1- Present problem minimal. May not require the presence of a physician. Typically 5minutes. Level 2- Problem Focused Problem Focused Straightforward Level 3- Expanded PF Expanded Problem Focused Low Level 4- Detailed Detailed Moderate Level 5- Comprehensive Comprehensive High
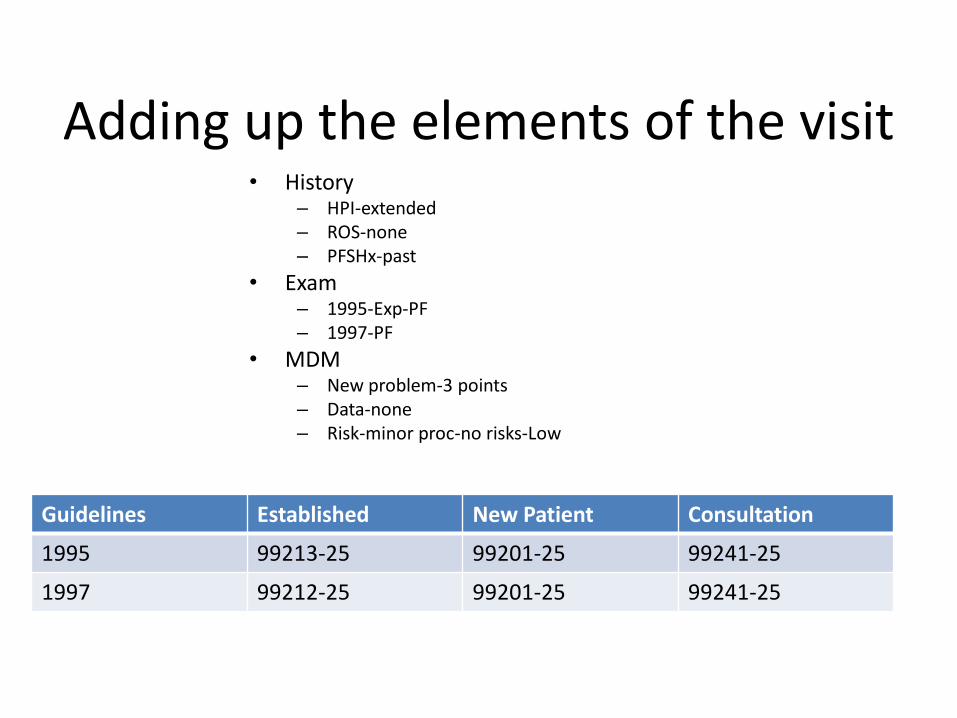
Adding up the elements of the visit• History
– HPI-extended– ROS-none– PFSHx-past
• Exam– 1995-Exp-PF– 1997-PF
• MDM– New problem-3 points– Data-none– Risk-minor proc-no risks-Low
Guidelines Established New Patient Consultation
1995 99213-25 99201-25 99241-25
1997 99212-25 99201-25 99241-25
The End
Questions