Elsevier items and derived items © 2005 by Mosby, Inc. 0 CHAPTER 24 Dissociative Disorders.
Upload
oliver-freemanCategory
view
249download
0
Elsevier items and derived items © 2005 by Elsevier Inc. Slide 1Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 1
Fluids and Electrolytes
Fluids and Electrolytes

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 2Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 2
Fluids and ElectrolytesFluids and Electrolytes
Dr. Efren N. AquinoDr. Efren N. AquinoMarch 7, 2008March 7, 2008
Fluids and ElectrolytesFluids and Electrolytes
Dr. Efren N. AquinoDr. Efren N. AquinoMarch 7, 2008March 7, 2008

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 3Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 3
Fluids (Water)Fluids (Water)
FunctionsFunctions Provides an extracellular transportation
route to deliver nutrients to the cells and carry waste products from the cells
Provides a medium in which chemical reactions, or metabolism, can occur within the cell
Acts as a lubricant for tissues Aids in the maintenance of acid-base
balance Assists in heat regulation via evaporation

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 4Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 4
Fluids (Water)Fluids (Water)
• Percentage of body weight that is water depends on several factors. Age
• Premature infant: 90%
• Newborn: 70-80%
• Twelve years to adult: 50-60%
• Older adults: 45-55%

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 5Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 5
Proportion of body weight Proportion of body weight represented by water.represented by water.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 6Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 6
Fluids (Water)Fluids (Water)
• Amount of Fat Fat contains relatively little water. The female has proportionately more body
fat than the male, which means that the female has less body fluid.
The more obese an individual, the lesser is the percentage of body water.
• Extracellular Fluid Is Lost from the Body More Rapidly than Intracellular Fluid

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 7Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 7
Fluid CompartmentsFluid CompartmentsFluid CompartmentsFluid Compartments
• Intracellular Fluid Largest of the two compartments Contains the fluid inside the billions of
cells within the body
• Extracellular Fluid Contains any fluid outside the cell Divided into interstitial and intravascular
compartments

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 8Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 8
Fluid CompartmentsFluid CompartmentsFluid CompartmentsFluid Compartments
• Extracellular Fluid Interstitial fluid
• Between the cells or in the tissue
• Accounts for approximately 27% of the fluid in the body
• Examples: lymph, cerebrospinal fluid, and gastrointestinal secretions
Intravascular fluid
• Plasma within the vessels
• Makes up 7% of fluid volume

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 9Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 9
Volumes of body fluids in each fluid Volumes of body fluids in each fluid compartment.compartment.
(Redrawn from Long, B.C., Phipps, W.J., Cassmeyer, V.L. (1993). Medical surgical nursing: a nursing process approach. [3rd ed.]. St. Louis: Mosby.)

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 10Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 10
Fluids Fluids and and ElectrolyElectrolytestes
Fluids Fluids and and ElectrolyElectrolytestesA Relative
volume of three body fluids compartmentsin a young adult male.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 11Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 11
Sources of fluid intake:
1. Water we drink
2. Water in food we eat
3. Product of catabolism
Fluid output:
1. Lungs – expired air
2. Skin – perspiration and insensible loss
3. Kidneys - urine
4. Large intestine - feces

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 12Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 12
Sources of Sources of fluid intake fluid intake and output.and output.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 13Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 13
Water Intake and Output in mLWater Intake and Output in mLWater Intake and Output in mLWater Intake and Output in mL
1. Water we drink = 1500
2. Water in foods = 700
3. Catabolism = 200
Total: 2,400 mL
1. Lungs = 350
2. Sweat = 100
3. Insensible loss = 350
4. Urine = 1400
5. Feces = 200
Total: 2,400

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 14Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 14
Homeostasis of the total volume of body water.
• A basic mechanism for adjusting intake to compensate for excess output of body fluid

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 15Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 15

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 16Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 16
Aldosterone Mechanism.
• Aldosterone restores normal extracellular fluid (ECF) volume when such levels decrease below normal.
• Excess aldosterone, however, leads to excess ECF volume, that is, excess blood volume (hypervolemia) and excess interstitial fluid volume (edema), and also to an excess of the total Na+ content of the body.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 17Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 17

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 18Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 18

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 19Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 19
Fluid and ElectrolytesFluid and ElectrolytesFluid and ElectrolytesFluid and Electrolytes
• 60% of body consists of fluid
• Intracellular space
• Extracellular space
• Electrolytes are active ions: positively and negatively charged

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 20Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 20
Gains and LossesGains and LossesGains and LossesGains and Losses
Water and electrolytes move in a variety of ways
1. Kidneys
2. Skin
3. Lungs
4. GI tract

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 21Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 21
Fluid Volume DisturbancesFluid Volume DisturbancesFluid Volume DisturbancesFluid Volume Disturbances
• Fluid Volume Deficit (Hypovolemia)
• Fluid Volume Excess (Hypervolemia)

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 22Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 22
Electrolyte ImbalancesElectrolyte ImbalancesElectrolyte ImbalancesElectrolyte Imbalances
1. Hypo and Hypernatremia
2. Hypo and Hyperkalemia
3. Hypo and Hypercalcemia
4. Hypo and Hypermagnesemia
5. Hypo and Hyperphosphatemia
6. Hypo and Hyperchloremia

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 23Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 23
Cells inCells in1. Hyponatremia1. Hyponatremia2. hypernatremia2. hypernatremia
Cells inCells in1. Hyponatremia1. Hyponatremia2. hypernatremia2. hypernatremia

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 24Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 24
EKG in 1. Hypokalemia2. Hyperkalemia
EKG in 1. Hypokalemia2. Hyperkalemia

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 25Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 25
Types of IV SolutionsTypes of IV SolutionsTypes of IV SolutionsTypes of IV Solutions
• Isotonic
• Hypotonic
• Hypertonic

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 26Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 26
• The normal daily loss of fluids must be met by the normal daily intake.
• Daily water intake and output is approximately 2500 ml.
• Fluid leaves the body through the kidneys, lungs, skin, and GI tract.
• Water loss is replenished by ingestion of liquids and foods and by metabolism of food and body tissues.
Intake and OutputIntake and Output

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 27Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 27
Intake and OutputIntake and OutputIntake and OutputIntake and Output
• Intake includes all fluids entering the body. Fluids can be liquids taken orally or
consumed in food, including foods that assume a liquid consistency at room temperature.
This also includes tube feedings and parenteral intake such as intravenous fluids, blood components, and total parenteral nutrition.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 28Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 28
Intake and OutputIntake and OutputIntake and OutputIntake and Output
• Output includes all fluids leaving the body. Examples are urine, diarrhea, vomitus,
nasogastric suction, and chest tube drainage.
Also included is drainage from surgical wounds and drainage collected in surgical receptacles such as the Jackson-Pratt, Davol, or Hemovac systems.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 29Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 29
Intake and OutputIntake and OutputIntake and OutputIntake and Output
• The kidneys play an extremely important role in fluid balance.
• If the kidneys are not functioning properly, the body has great difficulty in regulating fluid balance.
• Glomerular Filtration Rate an Nephrons filter blood at a rate of 125
ml per min, or about 180 L per day. This leads to output of 1 to 2 L of urine
per day.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 30Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 30
Intake and OutputIntake and OutputIntake and OutputIntake and Output
• The kidneys must excrete a minimum of 30 ml/hr of urine to eliminate waste products from the body.
• The kidneys react to fluid excesses by excreting a more dilute urine; this rids the body of excess fluid and conserves electrolytes.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 31Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 31
Intake and OutputIntake and OutputIntake and OutputIntake and Output
• A simple and accurate method of determining water balance is to weigh the patient under exact conditions. 1 L of fluid equals 1 kg (2.2 lb); a weight
change of 1 kg will reflect a loss or gain of 1 L of body fluid.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 32Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 32
Regulation of Body Fluid Regulation of Body Fluid CompartmentsCompartmentsRegulation of Body Fluid Regulation of Body Fluid CompartmentsCompartments
• Osmosis is the diffusion of water caused by fluid gradient
• Tonicity is the ability of solutes to cause osmotic driving forces
• Diffusion is the movement of a substance from area of higher concentration to one of lower concentration

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 33Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 33

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 34Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 34
Regulation of Body Fluid Compartments (cont’d)Regulation of Body Fluid Compartments (cont’d)
• Filtration is the movement of water and solutes from an area of high hydrostatic pressure to an area of low hydrostatic pressure
• Osmolality reflects the concentration of fluid that affects the movement of water between fluid compartments by osmosis
• Osmotic pressure is the amount of hydrostatic pressure needed to stop the flow of water by osmosis

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 35Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 35
Sodium-Potassium PumpSodium-Potassium PumpSodium-Potassium PumpSodium-Potassium Pump
• Sodium concentration is higher in ECF than ICF
• Sodium enters cell by diffusion
• Potassium exits cell into ECF

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 36Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 36
Movement of Fluid and ElectrolytesMovement of Fluid and ElectrolytesMovement of Fluid and ElectrolytesMovement of Fluid and Electrolytes
• Substances entering the body begin their journey in the extracellular fluid.
• To carry out their functions, they must cross the semipermeable membrane surrounding each body cell to enter the cell.
• The fat and protein molecules that make up the membrane are arranged so that some substances can enter the cells and others cannot.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 37Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 37
Movement of Fluid and ElectrolytesMovement of Fluid and ElectrolytesMovement of Fluid and ElectrolytesMovement of Fluid and Electrolytes
• Several methods are used by the body to move fluids, electrolytes and other solutes, or dissolved substances into and out of cells. Passive Transport Processes Active Transport Processes

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 38Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 38
Movement of Fluid and ElectrolytesMovement of Fluid and ElectrolytesMovement of Fluid and ElectrolytesMovement of Fluid and Electrolytes
Passive Transport Processes• No cellular energy is required to move
substances from a high concentration to a low concentration.
Active Transport Processes• Cellular energy is required to move
substances from a low concentration to a high concentration.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 39Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 39
Passive TransportPassive TransportPassive TransportPassive Transport
• Diffusion This is the movement of particles in all
directions through a solution or gas. Solutes move from an area of higher
concentration to an area of lower concentration, which eventually results in an equal distribution of solutes within the two areas.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 40Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 40
Passive TransportPassive TransportPassive TransportPassive Transport
• Osmosis This is the movement of water from an
area of lower concentration to an area of higher concentration.
It equalizes the concentration of ions or molecules on both sides of the membrane.
The flow of water will continue until the number of ions or molecules on both sides are equal.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 41Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 41
Passive TransportPassive TransportPassive TransportPassive Transport
• Osmosis Hypertonic Solutions Isotonic Solutions Hypotonic Solutions

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 42Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 42
Passive TransportPassive TransportPassive TransportPassive Transport
• Osmosis Hypertonic Solutions
• A solution of higher osmotic pressure
• Pulls fluid from the cells Isotonic Solutions
• A solution of same osmotic pressure
• Expands the body’s fluid volume without causing a fluid shift
Hypotonic Solutions

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 43Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 43
Passive TransportPassive TransportPassive TransportPassive Transport
• Osmosis Hypertonic Solutions Isotonic Solutions Hypotonic Solutions
• A solution of lower osmotic pressure.
• Moves into the cell, causing them to enlarge

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 44Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 44
Passive TransportPassive TransportPassive TransportPassive Transport
• Filtration This is the transfer of water and
dissolved substances from an area of higher pressure to an area of lower pressure.
A force behind filtration is called hydrostatic pressure, or the force pressing outward on a vessel wall.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 45Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 45
Passive TransportPassive TransportPassive TransportPassive Transport
• Filtration The pumping action of the heart is
responsible for the amount of force of the hydrostatic pressure that causes water and electrolytes to move from the capillaries to the interstitial fluid.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 46Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 46
Diffusion.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 47Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 47
Osmosis.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 48Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 48
Filtration.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 49Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 49
Active TransportActive TransportActive TransportActive Transport
• Requires energy
• Force that moves molecules into cells without regard for their positive or negative charge and against concentration factors that would prevent entry via diffusion

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 50Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 50
Active TransportActive TransportActive TransportActive Transport
• Requires energy
• Moves fluid and electrolytes from an area of low concentration to an area of high concentration
• Substances actively transported through the cell membrane include sodium, potassium, calcium, iron, hydrogen, amino acids, and glucose.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 51Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 51
Active TransportActive TransportActive TransportActive Transport
• Electrolytes Electrolytes develop tiny electrical
charges when they dissolve in water and break up into particles known as ions.
Ions develop either a positive or negative electrical charge.
• Cations have a positive charge.
• Anions have negative charge.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 52Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 52
Active TransportActive TransportActive TransportActive Transport
• Electrolytes A balance exists between the
electrolytes; for each positively charged cation, there must be a negatively charged anion.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 53Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 53
Active TransportActive TransportActive TransportActive Transport
• Sodium A cation Most abundant electrolyte in the body Normal level: 134 to 142 mEq/L Major source is from the diet; frequently
must be limited

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 54Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 54
Active TransportActive TransportActive TransportActive Transport
• Sodium Functions of sodium: regulates water
balance, controls extracellular fluid volume, increases cell membrane permeability, stimulates conduction of nerve impulses and helps maintain neuromuscular irritability, controls contractility of muscles

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 55Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 55
Active TransportActive TransportActive TransportActive Transport
• Sodium (continued) Hyponatremia
• Less than normal concentration of sodium in the blood
• Sodium level less than 134 mEq/L
• Can occur when there is a sodium loss or a water excess

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 56Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 56
Active TransportActive TransportActive TransportActive Transport
• Sodium (continued) Hyponatremia
• Body attempts to compensate by decreasing water excretion
• Patient likely to also have a potassium imbalance due to fluid being moved into the cells and potassium shifting out of the cells

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 57Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 57
Active TransportActive TransportActive TransportActive Transport
• Sodium Hypernatremia
• Greater than normal concentration of sodium in the blood
• Sodium level greater than 145 mEq/L
• Can occur when there is a sodium excess or a water loss

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 58Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 58
Active TransportActive TransportActive TransportActive Transport
• Sodium Hypernatremia
• Body attempts to correct the imbalance by conserving water through renal reabsorption
• Causes fluid to shift from the cells to the interstitial spaces, resulting in cellular dehydration

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 59Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 59
Active TransportActive TransportActive TransportActive Transport
• Potassium Dominant intracellular cation Normal level is 3.5 to 5 mEq/L Well-balanced diet usually provides
adequate potassium; approximately 65 mEq is required each day.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 60Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 60
Active TransportActive TransportActive TransportActive Transport
• Potassium The routes of potassium excretion are
the kidneys, in the feces, and through perspiration.
The kidneys control the excretion of potassium.
The main function is regulation of water and electrolyte content within the cell.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 61Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 61
Active TransportActive TransportActive TransportActive Transport
• Potassium Hypokalemia
• Decrease in body’s potassium to a level below 3.5 mEq/L
• The major cause of loss is renal excretion.
• The kidneys do not conserve potassium and excrete it even when the body needs it.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 62Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 62
Active TransportActive TransportActive TransportActive Transport
• Potassium Hypokalemia
• Potassium can be depleted due to excessive GI losses from gastric suctioning or vomiting and the use of diuretics.
• This can affect skeletal and cardiac function.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 63Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 63
Active TransportActive TransportActive TransportActive Transport
• Potassium Hyperkalemia
• Increase in the body’s serum potassium level above 5 mEq/L
• Gained through intake and lost by excretion
• The major cause of excess potassium is renal disease; severe tissue damage causes potassium to be released from the cell.
• Excessive increase in foods high in potassium can cause serum levels to increase.
• This can cause cardiac arrest.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 64Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 64
Active TransportActive TransportActive TransportActive Transport
• Chloride An extracellular anion. Normal level is 96 to 105 mEq/L. It is the chief anion in interstitial and intravascular
fluid. It has the ability to diffuse quickly between the
intracellular and extracellular compartments and combines easily with sodium to form sodium chloride or with potassium to form potassium chloride.
Daily requirement is equal to that of sodium. The main route of excretion is the kidneys.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 65Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 65
Active TransportActive TransportActive TransportActive Transport
• Chloride Hypochloremia
• It usually occurs when sodium is lost, because sodium and chloride are frequently paired.
• The most common causes of hypochloremia are vomiting and prolonged nasogastric or fistula drainage.
Hyperchloremia• It rarely occurs but may be seen when bicarbonate
levels fall.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 66Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 66
Active TransportActive Transport
• Calcium A positively charged ion. Normal level is 4.5 mEq/L. Of calcium in the body, 99% is concentrated in the
bones and teeth. Calcium is deposited in the bones and mobilized as
needed to help keep the blood level constant during any period of insufficient intake.
Vitamin D, calcitonin, and parathyroid hormone are necessary for absorption and utilization of calcium.
The best food sources are milk and cheese.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 67Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 67
Active TransportActive Transport
• Calcium Hypocalcemia
• Develops when the serum level is below 4.5 mEq/L
• A deficiency may be caused by infusion of excess amounts of citrated blood, excessive loss through diarrhea, inadequate dietary intake, surgical removal of parathyroid function, pancreatic disease, or small bowel disease.
• Signs and symptoms are neuromuscular irritation and increased excitability and tetany.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 68Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 68
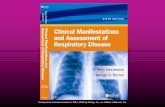
Tests for hypocalcemia. C, inflating a blood pressure cuff above the systolic pressure for a few minutes.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 69Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 69
Tests for hypocalcemia. B, Trousseau's sign is a carpal spasm induced by inflating a blood pressure cuff a little above the systolic pressure for a few minutes

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 70Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 70
Figure 22-4, A & BFigure 22-4, A & B
Tests for hypocalcemia. A, Chvostek’s sign. B, Trousseau’s sign.
(From Lewis, S.M., Heitkemper, M.M., Dirksen, S.R. [2004]. Medical-surgical nursing: assessment and management of clinical problems. [6th ed.]. St. Louis: Mosby.)

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 71Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 71
Active TransportActive Transport
• Calcium Hypercalcemia
• It occurs when calcium levels exceed 5.8 mEq/L.
• It may occur when calcium stored in the bones enters the circulation; occurs with immobilization.
• An increased intake of calcium or vitamin D also may be a cause.
• Neuromuscular activity is depressed and renal calculi may develop.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 72Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 72
Active TransportActive Transport
• Phosphorus Chiefly an intracellular anion Normal level is 4 mEq/L. Phosphorus and calcium have an inverse relationship
in the body; an increase in one causes a decrease in the other.
The majority is found in bones and teeth combined with calcium.
Dietary intake is usually 800 to 1500 mg per day. An adequate intake of vitamin D is necessary for the
absorption of both calcium and phosphorus.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 73Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 73
Active TransportActive Transport
• Phosphorus Hypophosphatemia
• Can occur from a dietary insufficiency, impaired kidney function, or maldistribution of phosphate
• Muscle weakness possible Hyperphosphatemia
• Most commonly occurs as a result of renal insufficiency; also can occur with increased intake of phosphate or vitamin D
• Signs and symptoms: tetany, numbness and tingling around the mouth, and muscle spasms

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 74Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 74
Active TransportActive Transport
• Magnesium The second most abundant cation in the intracellular
fluid. Normal level is 1.5 to 2.4 mEq/L. Although only small amounts are in the blood, it is
important in maintaining normal body function. The majority is found in bone, muscle, and soft tissue. Dietary intake is usually 200 to 400 mg per day. It is commonly distributed in foods: whole grains,
fruits, vegetables, meat, fish, legumes, and dairy products.
The major route of excretion is the kidneys.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 75Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 75
Active TransportActive Transport
• Magnesium Hypomagnesemia
• Develops when blood levels fall below 1.5 mEq/L
• A decreased level often parallels decreased potassium.
• Signs and symptoms: increased neuromuscular irritability similar to those observed with hypocalcemia
• Major causes are increased excretion by the kidneys, impaired absorption from the GI tract, and prolonged malnutrition.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 76Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 76
Active TransportActive Transport
• Magnesium Hypermagnesemia
• Develops when blood levels exceed 2.5 mEq/L
• It rarely occurs when kidney function is normal.
• Major causes are impaired renal function, excess magnesium administration, and diabetic ketoacidosis when there is severe water loss.
• An excess of magnesium severely restricts nerve and muscle activity.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 77Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 77
Active TransportActive Transport
• Bicarbonate A main anion of the extracellular fluid. Normal level is 22 to 24 mEq/L. It is an alkaline electrolyte whose major function is the
regulation of the acid-base balance. It acts as a buffer to neutralize acids in the body and
maintain the 20:1 bicarbonate/carbonic acid ratio needed to keep the body in homeostasis.
The kidneys selectively regulate the amount of bicarbonate retained or excreted.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 78Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 78
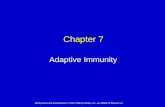
Regulation of acid-base balance. H2CO3, Carbonic acid; H2O, water;
CO2, carbon dioxide; HCO3-, bicarbonate.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 79Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 79
Acid-Base DisturbancesAcid-Base DisturbancesAcid-Base DisturbancesAcid-Base Disturbances
• Buffer Systems
• Acute and chronic metabolic acidosis
• Acute and chronic metabolic alkalosis
• Acute and chronic respiratory acidosis
• Acute and chronic respiratory alkalosis
• Blood Gas Analysis

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 80Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 80
Acid-Base BalanceAcid-Base Balance
• Acid-base balance means homeostasis of the hydrogen ion concentration in the body fluids.
• The hydrogen ion concentration is determined by the ratio of carbonic acid to bicarbonate in the extracellular fluid.
• The ratio needed for homeostasis is 1 part carbonic acid to 20 parts bicarbonate.
• The symbol used to indicate hydrogen ion balance is pH.
• Arterial blood gases determine whether a solution is acid, neutral, or alkaline; the more hydrogen ions in a solution, the more acid is the solution, and the fewer hydrogen ions, the more alkaline is the solution.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 81Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 81
Acid-Base BalanceAcid-Base Balance
• The body has three systems that work to keep the pH in the narrow range of normal. Blood buffers: Buffers circulate throughout the body in
pairs, neutralizing excess acids or bases by contributing or accepting hydrogen ions.
Lungs: By speeding up or slowing down respirations, the lungs can increase or decrease the amount of carbon dioxide in the blood.
Kidneys: They excrete varying amounts of acid or base.
• The three systems work closely together to maintain a normal hydrogen ion concentration.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 82Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 82
• Respiratory Acidosis This is caused by any condition that impairs normal
ventilation. A retention of carbon dioxide occurs with a resultant
increase of carbonic acid in the blood. As the pH falls, the Pco2 level increases.
Shallow respirations result because of the retained carbon dioxide.
Treatment is aimed at improving ventilation; correcting the primary condition responsible for the imbalance.
Acid-Base ImbalanceAcid-Base Imbalance

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 83Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 83
• Respiratory Alkalosis This is caused by hyperventilation. Respirations that increase in rate, depth, or both can
result in loss of excessive amounts of carbon dioxide with a resultant lowering of the carbonic acid level in the blood.
The pH rises because of the decrease in carbonic acid being blown off with each exhalation.
Treatment is sedation and reassurance; breathing into a paper bag will cause rebreathing of the exhaled carbon dioxide.
Acid-Base ImbalanceAcid-Base Imbalance

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 84Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 84
• Metabolic Acidosis This can result from a gain of hydrogen ions or a loss
of bicarbonate: retaining too many acids or losing too many bases.
Without sufficient bases, the pH of the blood falls below normal; the bicarbonate level will also drop.
The effect is hyperventilation, as the lungs attempt to compensate by blowing off carbon dioxide to lower the Pco2 level.
Treatment is the administration of sodium bicarbonate.
Acid-Base ImbalanceAcid-Base Imbalance

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 85Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 85
Acid-Base ImbalanceAcid-Base Imbalance
• Metabolic Alkalosis This results when a significant amount of acid is lost
from the body or an increase in the bicarbonate level occurs.
The most common cause is vomiting gastric content, normally high in acid.
It can also occur in patients who ingest excessive amounts of alkaline agents, such as bicarbonate-containing antacids.
The central nervous system is depressed. Treatment is aimed at the cause.

Elsevier items and derived items © 2005 by Elsevier Inc. Slide 86Mosby items and derived items © 2006, 2003, 1999, 1995, 1991 by Mosby, Inc.Slide 86
DONE!!DONE!!