Elbow Trauma. 6% of all fractures and dislocations involve elbow Most common fractures differ...
18
Elbow Trauma
-
Upload
richard-fletcher -
Category
Documents
-
view
219 -
download
0
Transcript of Elbow Trauma. 6% of all fractures and dislocations involve elbow Most common fractures differ...

Elbow Trauma

Elbow Trauma
• 6% of all fractures and dislocations involve elbow• Most common fractures differ between adults
and children – M.C. in adults- radial head and neck fxs.– M.C. in children- supracondylar fxs.
• Complex anatomy requires 4 views for adequate interpretation – AP in extension, medial oblique, lateral and axial
olecranon (Jones view)
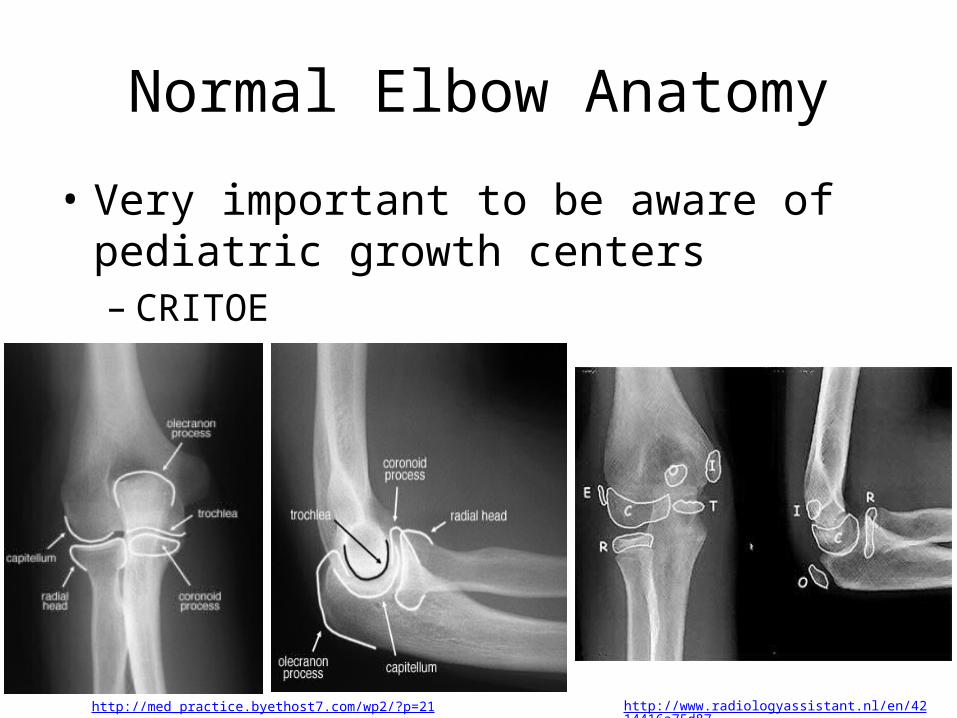
Normal Elbow Anatomy
• Very important to be aware of pediatric growth centers– CRITOE
http://med_practice.byethost7.com/wp2/?p=21 http://www.radiologyassistant.nl/en/4214416a75d87
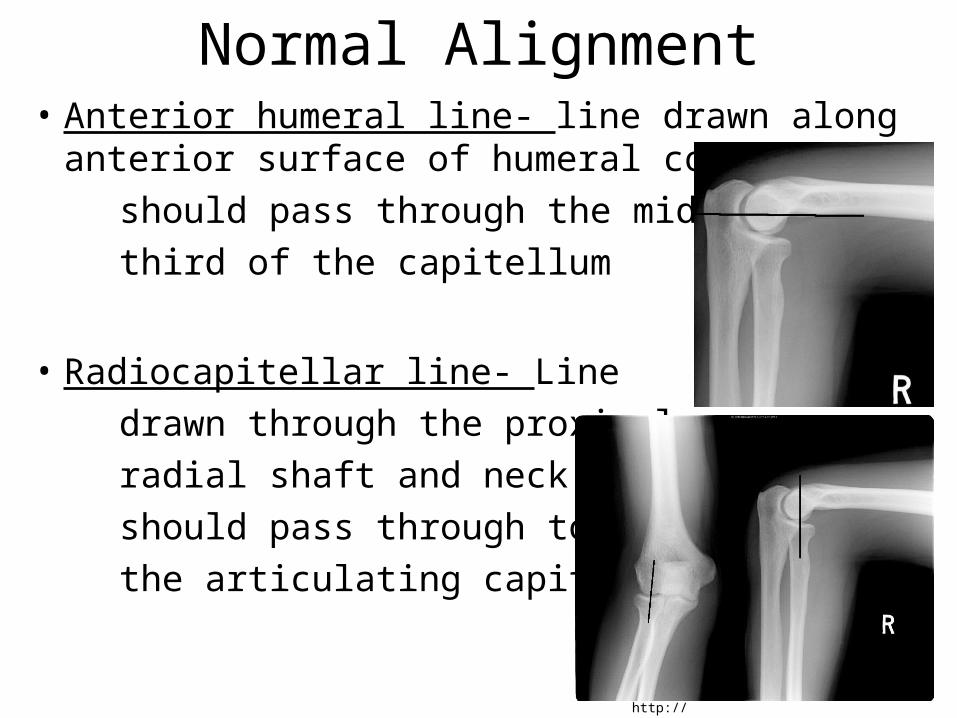
Normal Alignment• Anterior humeral line- line drawn along anterior
surface of humeral cortex should pass through the middle third of the capitellum
• Radiocapitellar line- Line drawn through the proximal radial shaft and neck should pass through to the articulating capitellum
http://imageinterpretation.co.uk/elbow.html

Signs of Fracture
• Usual signs may not be readily visible– Fracture line, cortical disruption, etc.
• Soft tissue signs can indicate fracture– Fat pad sign
• On lateral, might see fat pad parallel to anterior humeral cortex, but should never see posterior fat pad
• With effusion, anterior may be displaced and will be shaped like a sail (sail sign)

Fat Pad Sign• Posterior fat pad is normally buried in olecranon fossa
and not visible– Becomes elevated and visible with joint uffusion
• Effusion (acute capsular swelling) can be from any origin (hemorrhagic, inflammatory, infectious, traumatic, etc.)
• Ant. fat pad may be obliterated, so post. Fat pad is more reliable when visible
http://www.radiologyassistant.nl/en/4214416a75d87 http://usmorthopaedic.blogspot.com/2009/06/how-to-read-elbow-x-ray-at-glance.html

Distal humerus fractures
• 95% extend to articular surface• Classified according to relationship with
condyle and shape of fracture line– Supracondylar, intercondylar, condylar and
epicondylar

Supracondylar Fractures• Most common elbow fracture in children (60%)• Fracture line extends transversely or obliquely
through distal humerus above the condyles • Distal fragment usually displaces posteriorly
http://imageinterpretation.co.uk/elbow.html
Normal
Intercondylar fracture
• Fracture line extends between medial and lateral condyles and extends to supracondylar region– Results and T or Y shaped configuration for
fracture
• Called trans-condylar if it extends through both condyles

Epicondylar fracture• Usually avulsion from traction of respective
common flexor (medial) or extensor (lateral) tendons
• Medial epicondyle avulsion common in sports with strong throwing motion (little leaguer’s elbow)
http://radiopaedia.org/images/445333

Fractures of Proximal Ulna• Olecranon fx.- direct trauma or avulsion by
triceps tendon• Coronoid process fx.- avulsion by brachialis or
impaction into trochlear fossa– Rarely isolated; usually associated with post. elbow dislocation
http://www.radiologyassistant.nl/en/4214416a75d87#a421500951381a

Fractures of Proximal Radius• M.C. adult elbow fx. (50%)• FOOSH transmits force causing impaction of
radial head into capitellum• Chisel fracture- incomplete fracture of radial
head that extends to center of articular surface• Usual rad. signs (fx. Line, articular disruption) may not be visible
– May be occult; fat pad sign is good indicator of occult fx.
http://learningradiology.com/mobile/msk/fxswithnames.htm
Fractures of the forearm
• Isolated ulnar fractures• Isolated radial fractures• Bony rings usually can't be fractured in one
place without disruption somewhere else in the ring
• 60% or forearm fractures involve both bones (BB fractures)
• These fractures usually have associated displacement with angulation and rotation

Isolated Ulnar Fractures• Distal shaft (Nightstick fx.)- direct trauma
• Proximal shaft (Monteggia’s fx.)- fx. of proximal ulna with dislocation of radius
http://www.wheelessonline.com/ortho/monteggias_fracture
http://radiographics.rsna.org/content/24/4/1009/F31.expansion.html

Isolated Radial Fractures• Most frequent is a Galeazzi’s fx. (reverse
Monteggia’s fx.) – Fracture of distal radial shaft with dislocation of distal radioulnar joint– Rare, but serious injury
http://www.learningradiology.com/archives05/COW%20157-Galeazzi%20Fx/galeazzicorrect.htm
Dislocations of Elbow
• 3rd m.c. dislocation in adults behind shoulder and interphalangeal joints– More common in children
• Classified according to displacement of radius an ulna relative to humerus– Posterior, posterolateral, anterior, medial and
anteromedial
• Posterior and posterolateral or more most common– 85-90% of all elbow locations– 50% have associated fractures
Pulled Elbow
• AKA nursemaid’s elbow• Occurs when child’s hand is pulled, tractioning arm
and causing radial head to slip out from under annular ligament and trapping the ligament in the radiohumeral articulation
• Immediate pain; stuck in mid-pronation due to pain• No radiographic pain• Supination reduces the dislocation and ends pain,
usually during positioning of lateral radiograph

References
• Yochum, T.R. (2005) Yochum and Rowe’s Essentials of Skeletal Radiology, Third Edition. Lippincott, Williams and Wilkins: Baltimore.