EHLERS-DANLOS SYNDROME PHYSICAL THERAPY AND...
12
PHYSICAL THERAPY AND EHLERS-DANLOS SYNDROME From a Structural Approach to a Process Approach Jan Dommerholt, PT, DPT, DAAPM O NLY 10% of physicians referring EDS-HT patients to rheumatology clinics realized that their joint hypermobility was the underlying cause of their patient’s pain Adib et al. Joint hypermobility syndrome in childhood. A not so benign multisystem disorder? Rheumatology. 2005 PHYSICAL THERAPY A lack of awareness of the condition amongst health professionals, patients and wider society Palmer S, Terry R, Rimes KA, Clark C, Simmonds J, Horwood J, Physiotherapy management of joint hypermobility syndrome - a focus group study of patient and health professional perspectives Physiotherapy (2015) http://dx.doi.org/10.1016/j.physio.2015.05.001 SUBJECTIVE HEALTH COMPLAINTS The complaints reported were Musculoskeletal (98%) Pseudoneurological (96%) Gastrointestinal (94%) Allergic (73%) and Influenza-like (58%) Maenad S, Assmus J & Berglund B. International Journal of Nursing Studies 48 (2011) 720–724 EDS-HT: A CHARACTERIZATION OF THE PATIENT’S LIVED EXPERIENCE Joints (99%) Cardiovascular system (96%) Gastrointestinal system (96%) Skin (95%) Neurological/psychological manifestations (88%) Genitourinary system (67%) Murray B et al. EDSHT: A characterization of the patients’ lived experience. AJOMG. 2013 Physical therapy is generally accepted as an efficient treatment for some musculoskeletal complications of EDS Keer R, Simmonds J. 2011. Joint protection and physical rehabilitation of the adult with hypermobility syndrome. Curr Opin Rheumatol 23: 131–136 Physical therapy has limits especially concerning time spent (by both the practitioner and the patient), inter-operator variability, and long-term efficacy Castori M et al.2012. Management of pain and fatigue in the joint hypermobility syndrome (a.k.a. Ehlers– Danlos syndrome, hypermobility type): Principles and proposal for a multidisciplinary approach. Am J Med Genet Part A 158A:2055–2070.
Transcript of EHLERS-DANLOS SYNDROME PHYSICAL THERAPY AND...
PHYSICAL THERAPY AND EHLERS-DANLOS SYNDROME
From a Structural Approach to a Process Approach
Jan Dommerholt, PT, DPT, DAAPM
ONLY 10%of physicians referring EDS-HT patients to rheumatology clinics realized that their joint hypermobility was the underlying cause of their patient’s pain
Adib et al. Joint hypermobility syndrome in childhood. A not so benign multisystem disorder? Rheumatology. 2005
PHYSICAL THERAPY
A lack of awareness of the condition amongst health professionals, patients and wider societyPalmer S, Terry R, Rimes KA, Clark C, Simmonds J, Horwood J, Physiotherapy management of joint hypermobility syndrome - a focus group study of patient and health professional perspectives
Physiotherapy (2015) http://dx.doi.org/10.1016/j.physio.2015.05.001
SUBJECTIVE HEALTH COMPLAINTS
The complaints reported were Musculoskeletal (98%) Pseudoneurological (96%) Gastrointestinal (94%) Allergic (73%) and Influenza-like (58%)Maenad S, Assmus J & Berglund B. International Journal of Nursing Studies 48 (2011) 720–724
EDS-HT: A CHARACTERIZATION OF THE PATIENT’S LIVED EXPERIENCE
Joints (99%) Cardiovascular system (96%) Gastrointestinal system (96%) Skin (95%) Neurological/psychological manifestations (88%) Genitourinary system (67%)
Murray B et al. EDS-‐HT: A characterization of the patients’ lived experience. AJOMG. 2013
Physical therapy is generally accepted as an efficient treatment for some musculoskeletal
complications of EDS
Keer R, Simmonds J. 2011. Joint protection and physical rehabilitation of the adult with hypermobility syndrome. Curr Opin Rheumatol 23: 131–136
Physical therapy has limits especially concerning time spent (by both the practitioner and the
patient), inter-operator variability, and long-term efficacy
Castori M et al.2012. Management of pain and fatigue in the joint hypermobility syndrome (a.k.a. Ehlers–Danlos syndrome, hypermobility type): Principles and proposal for a multidisciplinary approach. Am J
Med Genet Part A 158A:2055–2070.
900 females and 46 males
81% (755/942) had received exercise advice from a physiotherapist
77% (701/940) agreed or strongly agreed that exercise was important for management
ATTITUDES, BELIEFS AND BEHAVIOURS TOWARDS EXERCISE AMONGST INDIVIDUALS WITH JOINT HYPERMOBILITY SYNDROME/
EHLERS DANLOS SYNDROME – HYPERMOBILITY TYPE J. Simmonds, M. Cairns, N. Ninis, W. Lever, Q. Aziz, A. Hakim
Swimming 28% (261/946)
Walking 24% (233/946) and
Pilates 22% (221/496)
ATTITUDES, BELIEFS AND BEHAVIOURS TOWARDS EXERCISE AMONGST INDIVIDUALS WITH JOINT HYPERMOBILITY SYNDROME/
EHLERS DANLOS SYNDROME – HYPERMOBILITY TYPE J. Simmonds, M. Cairns, N. Ninis, W. Lever, Q. Aziz, A. Hakim
Diagnosis and subsequent referral to physiotherapy services is often difficult and convoluted
Referral was often for acute single joint injury, failing to recognize the long-term multi-joint nature of the condition
PHYSICAL THERAPY
Palmer S, Terry R, Rimes KA, Clark C, Simmonds J, Horwood J, Physiotherapy management of joint hypermobility syndrome - a focus group study of patient and health professional perspectives
Physiotherapy (2015) http://dx.doi.org/10.1016/j.physio.2015.05.001
Health professionals and patients felt that if left undiagnosed, EDS was more difficult to treat because of its chronic nature
When EDS was treated by health professionals with knowledge of the condition, patients reported satisfactory outcomes
PHYSICAL THERAPY
Palmer S, Terry R, Rimes KA, Clark C, Simmonds J, Horwood J, Physiotherapy management of joint hypermobility syndrome - a focus group study of patient and health professional perspectives
Physiotherapy (2015) http://dx.doi.org/10.1016/j.physio.2015.05.001
ONLY ABOUT 4% OF PHYSICAL THERAPISTS ADMIT LIKING THE MANAGEMENT OF PATIENTS WITH PERSISTENT (CHRONIC)
PAIN
Wolff MS et al 1991 Physical Therapy 71:207-‐214
POSTURE CORRECTION
Perceived asymmetry, imbalances, misalignments, or postural deviations are usually normal biological variations and not pathology, even in many cases of EDS
The cause of many common musculoskeletal and pain complaints cannot be explained solely by biomechanics, structure or posture
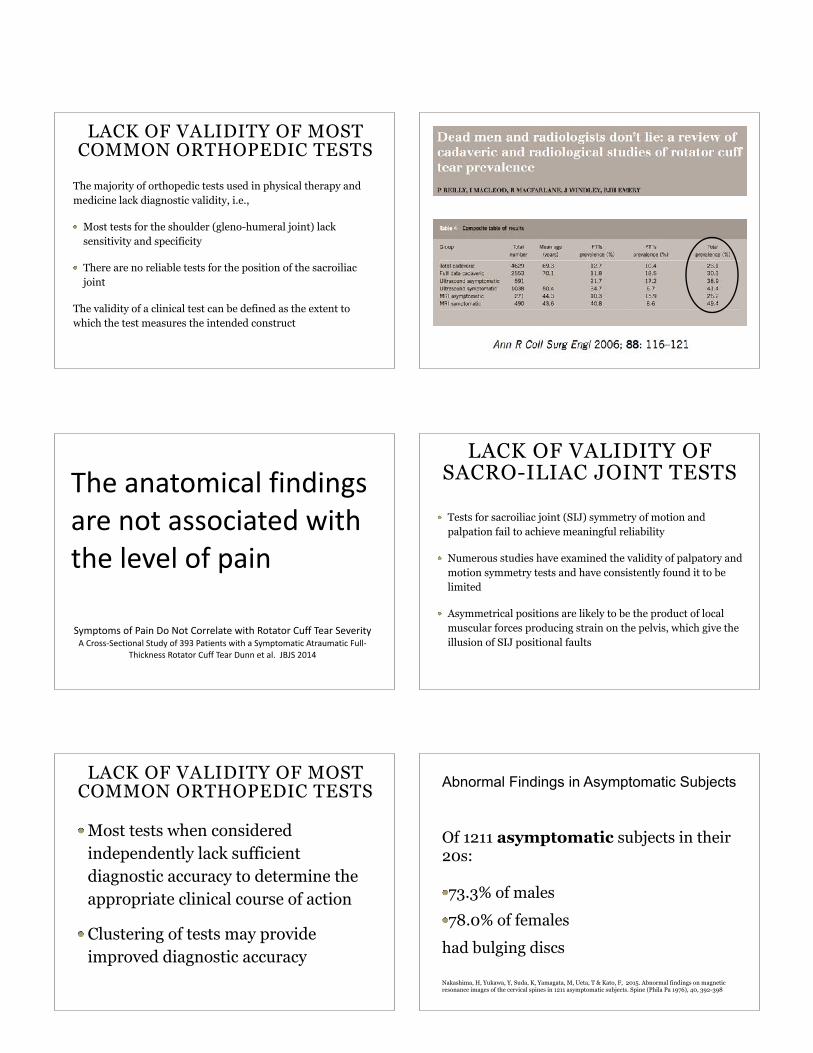
LACK OF VALIDITY OF MOST COMMON ORTHOPEDIC TESTS
The majority of orthopedic tests used in physical therapy and medicine lack diagnostic validity, i.e.,
Most tests for the shoulder (gleno-humeral joint) lack sensitivity and specificity
There are no reliable tests for the position of the sacroiliac joint
The validity of a clinical test can be defined as the extent to which the test measures the intended construct
Symptoms of Pain Do Not Correlate with Rotator Cuff Tear Severity A Cross-‐Sectional Study of 393 Patients with a Symptomatic Atraumatic Full-‐
Thickness Rotator Cuff Tear Dunn et al. JBJS 2014
The anatomical findings are not associated with the level of pain
LACK OF VALIDITY OF SACRO-ILIAC JOINT TESTS
Tests for sacroiliac joint (SIJ) symmetry of motion and palpation fail to achieve meaningful reliability
Numerous studies have examined the validity of palpatory and motion symmetry tests and have consistently found it to be limited
Asymmetrical positions are likely to be the product of local muscular forces producing strain on the pelvis, which give the illusion of SIJ positional faults
LACK OF VALIDITY OF MOST COMMON ORTHOPEDIC TESTS
Most tests when considered independently lack sufficient diagnostic accuracy to determine the appropriate clinical course of action
Clustering of tests may provide improved diagnostic accuracy
Abnormal Findings in Asymptomatic Subjects
Of 1211 asymptomatic subjects in their 20s:
73.3% of males 78.0% of females
had bulging discs
Nakashima, H, Yukawa, Y, Suda, K, Yamagata, M, Ueta, T & Kato, F, 2015. Abnormal findings on magnetic resonance images of the cervical spines in 1211 asymptomatic subjects. Spine (Phila Pa 1976), 40, 392-398
JOINT MANIPULATION
Many of our patients with EDS-HT have received joint manipulations to “correct stiff spinal segments”
It is, however, questionable whether EDS-HT patients ever need spinal manipulations
NO HANDS-ON PHYSICAL THERAPY??
If the goal of hands-on physical therapy is to correct asymmetry, imbalances, misalignments, or postural deviations, its value is questionable
ERGONOMICS
The best ergonomic chair is only as good as the behavior of the person who sits in that chair
ERGONOMICS
Ergonomic modifications are often indicated, but they are not the silver bullet to solve all problems
RING SPLINTS
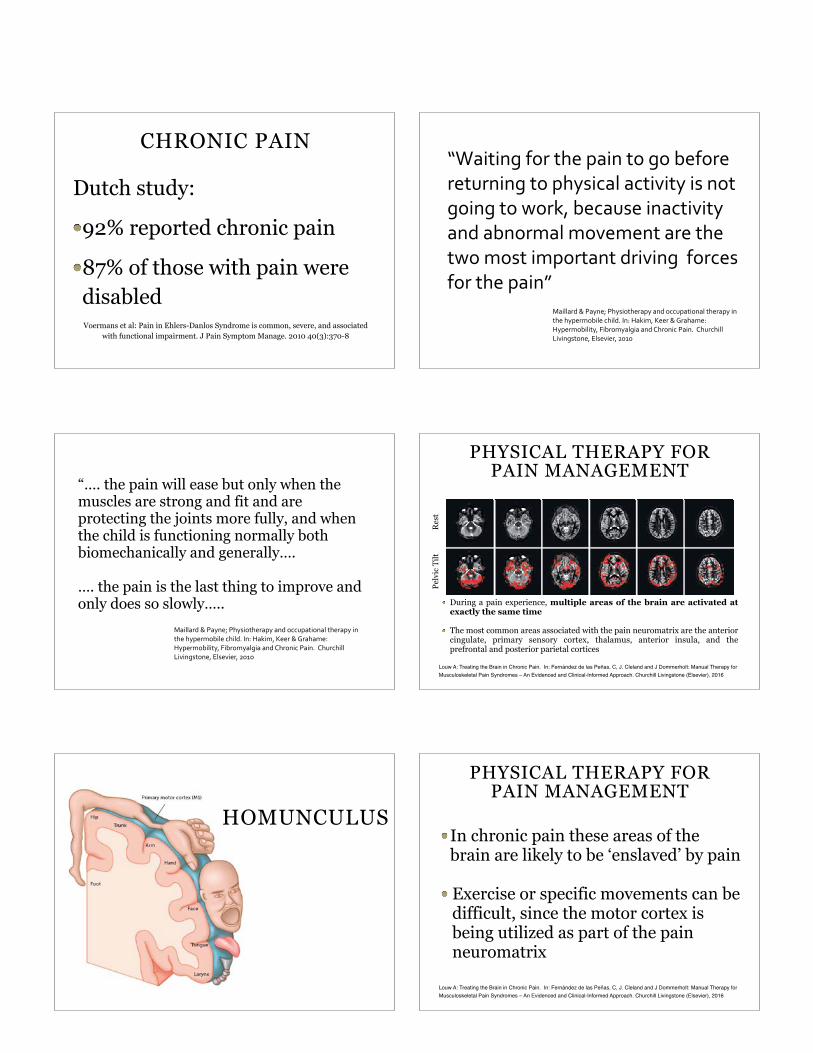
CHRONIC PAIN
Dutch study:
92% reported chronic pain
87% of those with pain were disabledVoermans et al: Pain in Ehlers-Danlos Syndrome is common, severe, and associated
with functional impairment. J Pain Symptom Manage. 2010 40(3):370-8
“Waiting for the pain to go before returning to physical activity is not going to work, because inactivity and abnormal movement are the two most important driving forces for the pain”
Maillard & Payne; Physiotherapy and occupational therapy in the hypermobile child. In: Hakim, Keer & Grahame: Hypermobility, Fibromyalgia and Chronic Pain. Churchill Livingstone, Elsevier, 2010
“…. the pain will ease but only when the muscles are strong and fit and are protecting the joints more fully, and when the child is functioning normally both biomechanically and generally….
…. the pain is the last thing to improve and only does so slowly…..
Maillard & Payne; Physiotherapy and occupational therapy in the hypermobile child. In: Hakim, Keer & Grahame: Hypermobility, Fibromyalgia and Chronic Pain. Churchill Livingstone, Elsevier, 2010
PHYSICAL THERAPY FOR PAIN MANAGEMENT
During a pain experience, multiple areas of the brain are activated at exactly the same time
The most common areas associated with the pain neuromatrix are the anterior cingulate, primary sensory cortex, thalamus, anterior insula, and the prefrontal and posterior parietal cortices
Louw A: Treating the Brain in Chronic Pain. In: Fernández de las Peñas, C, J. Cleland and J Dommerholt: Manual Therapy for Musculoskeletal Pain Syndromes – An Evidenced and Clinical-Informed Approach. Churchill Livingstone (Elsevier), 2016
Res
tPe
lvic
Tilt
HOMUNCULUS
PHYSICAL THERAPY FOR PAIN MANAGEMENT
In chronic pain these areas of the brain are likely to be ‘enslaved’ by pain
Exercise or specific movements can be difficult, since the motor cortex is being utilized as part of the pain neuromatrix
Louw A: Treating the Brain in Chronic Pain. In: Fernández de las Peñas, C, J. Cleland and J Dommerholt: Manual Therapy for Musculoskeletal Pain Syndromes – An Evidenced and Clinical-Informed Approach. Churchill Livingstone (Elsevier), 2016

PHYSICAL THERAPY FOR PAIN MANAGEMENT
Patients have been accused of malingering, or being lazy or not motivated
Yet from a neuroscience perspective there is a justified reason for their difficulty with these exercises
Louw A: Treating the Brain in Chronic Pain. In: Fernández de las Peñas, C, J. Cleland and J Dommerholt: Manual Therapy for Musculoskeletal Pain Syndromes – An Evidenced and Clinical-Informed Approach. Churchill Livingstone (Elsevier), 2016
PHYSICAL THERAPY FOR PAIN MANAGEMENT
Traditionally, clinicians have either followed a top-down (cognitive) or a bottom-up approach (such as manual therapy) to treat pain The two approaches are not mutually exclusive and clinicians are therefore urged to consider a combination of the two
Louw A: Treating the Brain in Chronic Pain. In: Fernández de las Peñas, C, J. Cleland and J Dommerholt: Manual Therapy for Musculoskeletal Pain Syndromes – An Evidenced and Clinical-Informed Approach. Churchill Livingstone (Elsevier), 2016
COMBINATION
TOP-DOWN: therapeutic neuroscience education (TNE)
BOTTOM-UP: manual therapy and exercise
HANDS-ON PHYSICAL THERAPY??
If the goal of hands-on physical therapy is to compliment “therapeutic neuroscience education”, hands-on therapy can be very useful
Manual therapy
Soft tissue mobilizations
Dry needling
Exercise
HANDS-ON PHYSICAL THERAPY??
Therapeutic neuroscience education works best if combined with movement-based therapies such as manual therapy and exercise
Feeding the brain information ‘from both ends’
Louw A: Treating the Brain in Chronic Pain. In: Fernández de las Peñas, C, J. Cleland and J Dommerholt: Manual Therapy for Musculoskeletal Pain Syndromes – An Evidenced and Clinical-Informed Approach. Churchill Livingstone (Elsevier), 2016
WHAT DOES THE RESEARCH SAY ABOUT PT, EDS AND EXERCISE?
Not much…….
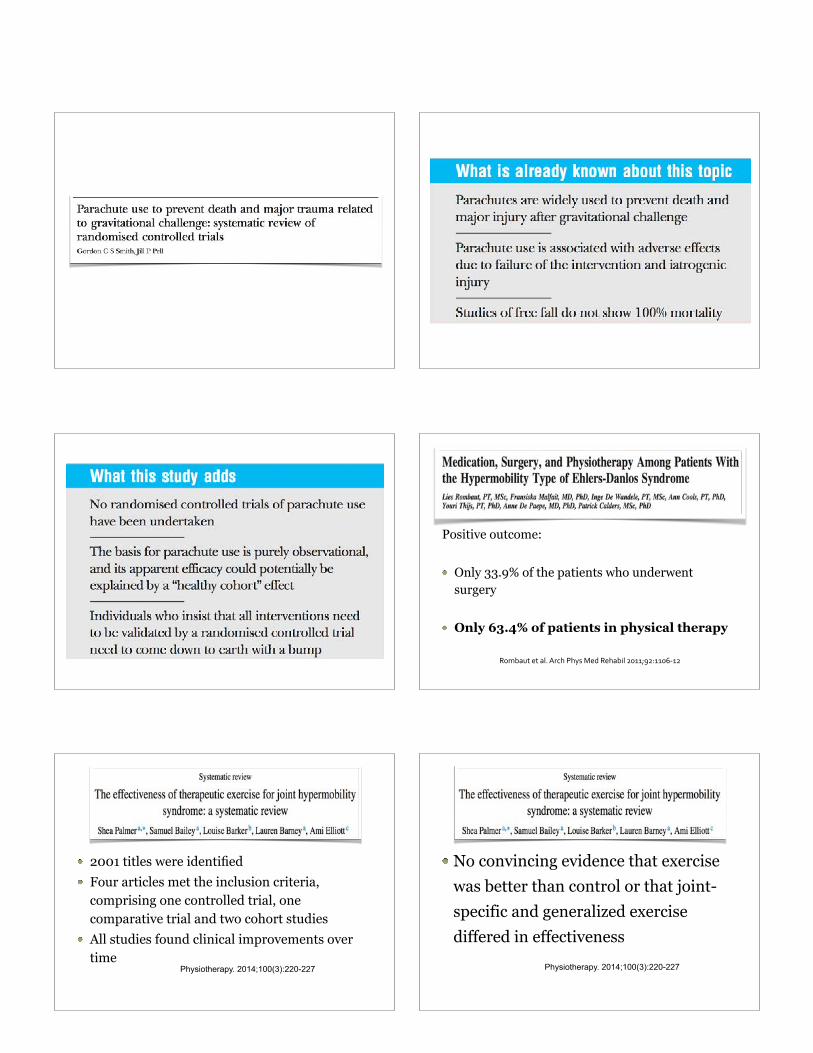
Rombaut et al. Arch Phys Med Rehabil 2011;92:1106-‐12
Positive outcome:
Only 33.9% of the patients who underwent surgery
Only 63.4% of patients in physical therapy
2001 titles were identified Four articles met the inclusion criteria, comprising one controlled trial, one comparative trial and two cohort studies All studies found clinical improvements over time
Physiotherapy. 2014;100(3):220-227
No convincing evidence that exercise was better than control or that joint-specific and generalized exercise differed in effectiveness
Physiotherapy. 2014;100(3):220-227
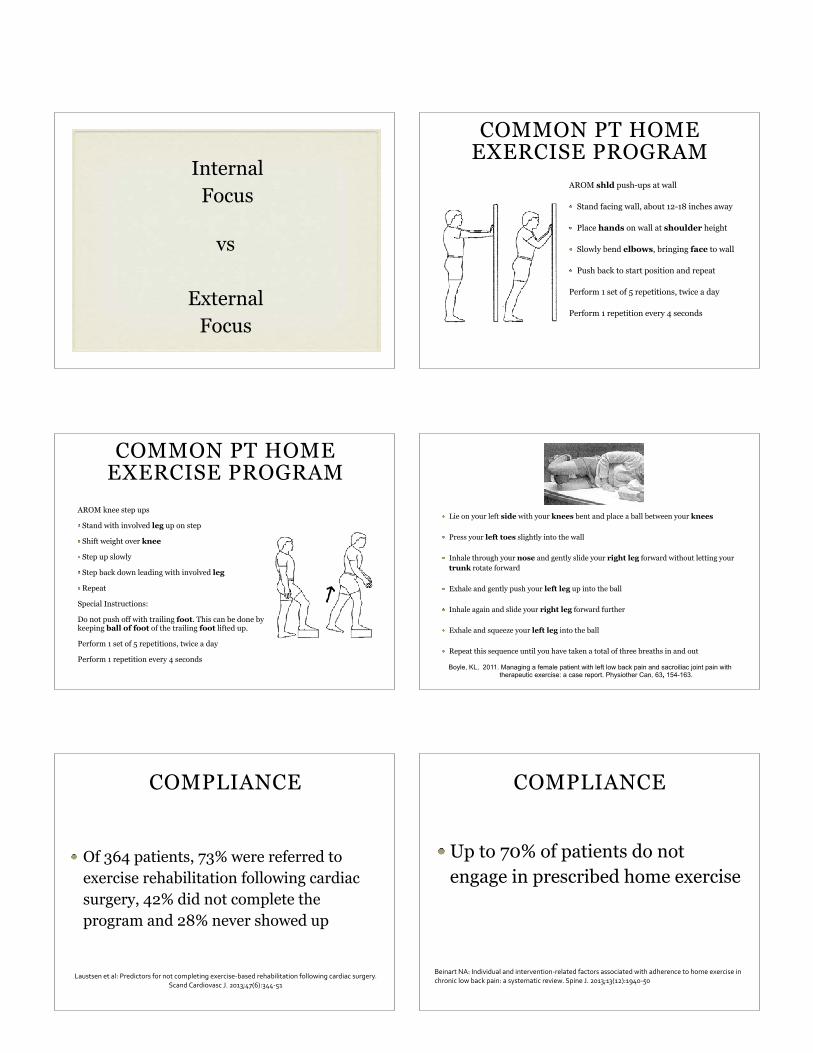
Internal Focus
vs
External Focus
COMMON PT HOME EXERCISE PROGRAM
AROM shld push-ups at wall
Stand facing wall, about 12-18 inches away
Place hands on wall at shoulder height
Slowly bend elbows, bringing face to wall
Push back to start position and repeat
Perform 1 set of 5 repetitions, twice a day
Perform 1 repetition every 4 seconds
COMMON PT HOME EXERCISE PROGRAM
AROM knee step ups
Stand with involved leg up on step
Shift weight over knee
Step up slowly
Step back down leading with involved leg
Repeat
Special Instructions:
Do not push off with trailing foot. This can be done by keeping ball of foot of the trailing foot lifted up.
Perform 1 set of 5 repetitions, twice a day
Perform 1 repetition every 4 seconds
Lie on your left side with your knees bent and place a ball between your knees
Press your left toes slightly into the wall
Inhale through your nose and gently slide your right leg forward without letting your trunk rotate forward
Exhale and gently push your left leg up into the ball
Inhale again and slide your right leg forward further
Exhale and squeeze your left leg into the ball
Repeat this sequence until you have taken a total of three breaths in and out
Boyle, KL, 2011. Managing a female patient with left low back pain and sacroiliac joint pain with therapeutic exercise: a case report. Physiother Can, 63, 154-163.
COMPLIANCE
Of 364 patients, 73% were referred to exercise rehabilitation following cardiac surgery, 42% did not complete the program and 28% never showed up
Laustsen et al: Predictors for not completing exercise-‐based rehabilitation following cardiac surgery. Scand Cardiovasc J. 2013;47(6):344-‐51
COMPLIANCE
Up to 70% of patients do not engage in prescribed home exercise
Beinart NA: Individual and intervention-‐related factors associated with adherence to home exercise in chronic low back pain: a systematic review. Spine J. 2013;13(12):1940-‐50
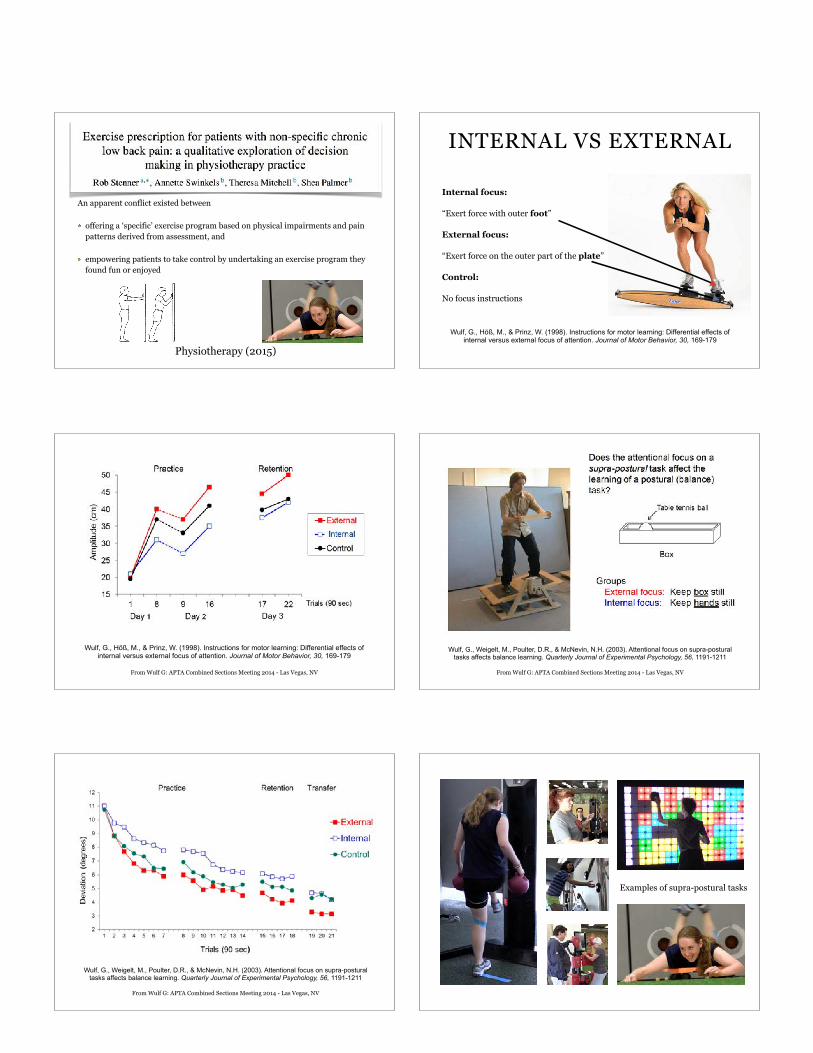
An apparent conflict existed between
offering a ‘specific’ exercise program based on physical impairments and pain patterns derived from assessment, and
empowering patients to take control by undertaking an exercise program they found fun or enjoyed
Physiotherapy (2015)
INTERNAL VS EXTERNAL
Internal focus:
“Exert force with outer foot”
External focus:
“Exert force on the outer part of the plate”
Control:
No focus instructions
Wulf, G., Höß, M., & Prinz, W. (1998). Instructions for motor learning: Differential effects of internal versus external focus of attention. Journal of Motor Behavior, 30, 169-179
Wulf, G., Höß, M., & Prinz, W. (1998). Instructions for motor learning: Differential effects of internal versus external focus of attention. Journal of Motor Behavior, 30, 169-179
From Wulf G: APTA Combined Sections Meeting 2014 - Las Vegas, NV From Wulf G: APTA Combined Sections Meeting 2014 - Las Vegas, NV
Wulf, G., Weigelt, M., Poulter, D.R., & McNevin, N.H. (2003). Attentional focus on supra-postural tasks affects balance learning. Quarterly Journal of Experimental Psychology, 56, 1191-1211
From Wulf G: APTA Combined Sections Meeting 2014 - Las Vegas, NV
Wulf, G., Weigelt, M., Poulter, D.R., & McNevin, N.H. (2003). Attentional focus on supra-postural tasks affects balance learning. Quarterly Journal of Experimental Psychology, 56, 1191-1211
Examples of supra-postural tasks
The focus of attention clearly has significant effects on the accuracy with which subjects can generate force and significant effects of motor planning in force production
Human Movement Science 31 (2012) 12–25
Training with an external focus of attention leads to improved performance when no attentional focus instructions are given
Human Movement Science 31 (2012) 12–25
An external focus of attention increases the automaticity of control
Human Movement Science 31 (2012) 12–25
Competitive cyclists performed significantly faster during a 16.1-km competitive trial than when performing maximally, without a competitor
The improvement in performance was elicited due to a greater external distraction, deterring perceived exertion
Journal of Science and Medicine in Sport 18 (2015) 486–491
The advantages of an external focus of attention may not be immediate, but often emerge only later in practice (but the research is not consistent….)
Human Movement Science 33 (2014) 120–134
An external focus of attention does not only improve performance, but could improve learning as well
Human Movement Science 33 (2014) 120–134
An internal focus of attention
can hinder learning
relative to an external focusHuman Movement Science 33 (2014) 120–134
APPLIES TO
Sports performance: Golf Basketball Volleyball Soccer Dart throwing American Football Jumping
APPLIES TO
Parkinson’s disease CVA (stroke) Autism Balance in older adults Pediatrics Multiple Sclerosis
Wulf, G., Landers, M., Lewthwaite, R., & Töllner, T. (2009). External focus instructions reduce postural instability in individuals with Parkinson disease.
Physical Therapy, 89, 162-168.
MULTIPLE SCLEROSIS
MS patients with balance problems
(1) conventional balance training (control),
(2) exergame training (playing exergames on an unstable platform)
(3) single-task (ST) exercises on the unstable platform
Playing exergames on an unstable surface had superior outcomes in balance and adherence
DOES IT WORK?
Ehlers Danlos Syndrome?? POTS??
There is no research yet, that demonstrates superior outcomes
From a Structural Approach to a Process Approach
DOES IT WORK?
Eileen - Ehlers Danlos Syndrome
DOES IT WORK?
Molly - Postural Orthostatic Tachycardia Syndrome
DOES IT WORK?
Molly - Postural Orthostatic Tachycardia Syndrome
DOES IT WORK?
Cassidy - Ehlers Danlos Syndrome and Postural Orthostatic Tachycardia Syndrome
THANKS TO
EILEEN MOLLY
CASSIDY DR. MARIA ARINI, PT, DPT
EDNF OUR OTHER PATIENTS