Ehlers-Danlos syndrome has varied molecular … · generalised dermatochalasis (pendulous or...
11
40 Med Geniet 1997;34:400-410 Syndrome of the month Ehlers-Danlos syndrome has varied molecular mechanisms F Michael Pope, Nigel P Burrows Ehlers-Danlos syndrome (EDS) is a group of variable clinical entities which share a propen- sity to skin fragility, joint laxity, and ligamen- tous fragility or shortening. Tschernogobow,' Ehlers,2 and Danlos3 independently described unusual bruising, excessive cutaneous extensi- bility, and molluscoid pseudotumours. The eponym of Ehlers-Danlos syndrome (EDS) was first suggested by Poumeau-Delille and Soulie.4 Spectacular early examples were retro- spectively commented upon by Beighton.5 Morris' described a notable British patient who Beighton re-examined more than 60 years later. The proband had classical EDS. Beighton7 not only showed impressive pictures of the so-called "Elastic Lady" but also included the original lithograph of a Spaniard with unilateral cutaneous hyperextensibility investigated in Leyden almost 300 years before, who was very probably a somatic mosaic. In Ehlers's time there was considerable difficulty in distinguishing clearly between cutis hyper- elastica (overextensible skin), dermatorrhexis (easy splitting of skin), and both localised and generalised dermatochalasis (pendulous or redundant skin). To this day the similarities of such physical signs still cause confusion. In practice the designations hyperelastic, pendu- lous, and lax skin often overlap and can even occur at different times in the same patient. For example, EDS skin is hyperelastic early in life but later becomes lax or drooping, especially in old age. The systemic implications, complica- tions, and associations of EDS were largely unrecognised for many years although the association of congenital hip dislocations was described early. In 1960 Mories8 first described a four-fold increase in fetal prematurity. He also noticed that the dermis was collagen depleted and elastin rich. Thirdly, he described catastrophic lethal arterial bleeding in a 15 year old adolescent boy with a traumatic arterial tear which was surgically unrepairable because of the extreme venous and arterial fragility. Very probably the patients with prematurity had EDS I/II while the vascular fragility was caused by acrogeric EDS IV. Subsequent clini- cal, molecular, and genetic progress has been rapid. For example, Barabas9 first proposed three distinct subsets. These included classical forms with prematurity, a milder type with venous varicosity, and a third, potentially lethal, form with minor cutaneous and joint changes but extreme arterial fragility (which we now call EDS IV). Soon afterwards, Beighton' also clearly described the frequent prematurity. He added an X linked form,' while dividing Barabas's first group into "gravis" and "mitis" variants, which we now call EDS I and II respectively, to make five subtypes. He also delineated the wide clinical heterogeneity with various rheumatological, orthopaedic, surgical, and cutaneous complications and was also fully familiar with such surgical complications as arterial aneurysms, venous varicosities, arterio- venous fistulas, and inguinal, umbilical, and hiatus hernias. He also documented reflux hydronephrosis, bladder neck obstruction, co- lonic diverticulae with perforation, and pleu- roperitoneal rupture (leading to pneumo- or haemothorax). These complications are now recognised as particularly common in EDS types IV, VI, and VII. In 1972, McKusick'2 added two further subtypes (types VI and VII). We now know that the former is caused by lysyl underhydroxylation, while the latter results from the misprocessing of procollagen (to col- lagen). In 1988 Beighton et al'3 published an International Nosology of Connective Tissue Disease where nine subcategories of EDS were defined. Subsequently, he correlated the sub- types with the various biochemical and mo- lecular abnormalities (table 1) and also pub- lished the equivalent Molecular Nosology."' (Med Genet 1997;34:400-410) Keywords: Ehlers-Danlos syndrome; molecular mecha- nisms Genetics of EDS (table 1) Autosomal dominant or autosomal recessive inheritance occurs in EDS I, II, III, IV, VI, and VII. Compound heterozygosity (see later) is also very likely. X linked forms have been described but are highly unusual. Autosomal dominant inheritance was first mentioned by Kopp.'5 Wiener'" described 12 affected sub- jects in three generations. Stuart'7 and Coe and Silver'8 both described the vertical transmis- sion particularly of EDS type I. Johnson and Falls" published a very large five generation American family of British-Canadian extrac- tion with typical EDS I and with two separate MRC Connective Tissue Genetics Group, Strangeways Research Laboratory and Department of Clinical Genetics, Addenbrooke's NHS Trust, Cambridge, UK F M Pope N P Burrows Correspondence to: Dr Pope, Strangeways Research Laboratory, Worts Causeway, Cambridge CB1 4RN, UK. 400 on 5 October 2018 by guest. Protected by copyright. http://jmg.bmj.com/ J Med Genet: first published as 10.1136/jmg.34.5.400 on 1 May 1997. Downloaded from
Transcript of Ehlers-Danlos syndrome has varied molecular … · generalised dermatochalasis (pendulous or...

40 Med Geniet 1997;34:400-410
Syndrome of the month
Ehlers-Danlos syndrome has varied molecularmechanisms
F Michael Pope, Nigel P Burrows
Ehlers-Danlos syndrome (EDS) is a group ofvariable clinical entities which share a propen-sity to skin fragility, joint laxity, and ligamen-tous fragility or shortening. Tschernogobow,'Ehlers,2 and Danlos3 independently describedunusual bruising, excessive cutaneous extensi-bility, and molluscoid pseudotumours. Theeponym of Ehlers-Danlos syndrome (EDS)was first suggested by Poumeau-Delille andSoulie.4 Spectacular early examples were retro-spectively commented upon by Beighton.5Morris' described a notable British patient whoBeighton re-examined more than 60 yearslater. The proband had classical EDS.Beighton7 not only showed impressive picturesof the so-called "Elastic Lady" but alsoincluded the original lithograph of a Spaniardwith unilateral cutaneous hyperextensibilityinvestigated in Leyden almost 300 years before,who was very probably a somatic mosaic. InEhlers's time there was considerable difficultyin distinguishing clearly between cutis hyper-elastica (overextensible skin), dermatorrhexis(easy splitting of skin), and both localised andgeneralised dermatochalasis (pendulous orredundant skin). To this day the similarities ofsuch physical signs still cause confusion. Inpractice the designations hyperelastic, pendu-lous, and lax skin often overlap and can evenoccur at different times in the same patient. Forexample, EDS skin is hyperelastic early in lifebut later becomes lax or drooping, especially inold age. The systemic implications, complica-tions, and associations of EDS were largelyunrecognised for many years although theassociation of congenital hip dislocations wasdescribed early. In 1960 Mories8 first describeda four-fold increase in fetal prematurity. Healso noticed that the dermis was collagendepleted and elastin rich. Thirdly, he describedcatastrophic lethal arterial bleeding in a 15 yearold adolescent boy with a traumatic arterialtear which was surgically unrepairable becauseof the extreme venous and arterial fragility.Very probably the patients with prematurityhad EDS I/II while the vascular fragility wascaused by acrogeric EDS IV. Subsequent clini-cal, molecular, and genetic progress has beenrapid. For example, Barabas9 first proposedthree distinct subsets. These included classicalforms with prematurity, a milder type with
venous varicosity, and a third, potentiallylethal, form with minor cutaneous and jointchanges but extreme arterial fragility (which wenow call EDS IV). Soon afterwards, Beighton'also clearly described the frequent prematurity.He added an X linked form,' while dividingBarabas's first group into "gravis" and "mitis"variants, which we now call EDS I and IIrespectively, to make five subtypes. He alsodelineated the wide clinical heterogeneity withvarious rheumatological, orthopaedic, surgical,and cutaneous complications and was also fullyfamiliar with such surgical complications asarterial aneurysms, venous varicosities, arterio-venous fistulas, and inguinal, umbilical, andhiatus hernias. He also documented refluxhydronephrosis, bladder neck obstruction, co-lonic diverticulae with perforation, and pleu-roperitoneal rupture (leading to pneumo- orhaemothorax). These complications are nowrecognised as particularly common in EDStypes IV, VI, and VII. In 1972, McKusick'2added two further subtypes (types VI and VII).We now know that the former is caused by lysylunderhydroxylation, while the latter resultsfrom the misprocessing of procollagen (to col-lagen). In 1988 Beighton et al'3 published anInternational Nosology of Connective TissueDisease where nine subcategories of EDS weredefined. Subsequently, he correlated the sub-types with the various biochemical and mo-lecular abnormalities (table 1) and also pub-lished the equivalent Molecular Nosology."'(Med Genet 1997;34:400-410)
Keywords: Ehlers-Danlos syndrome; molecular mecha-nisms
Genetics ofEDS (table 1)Autosomal dominant or autosomal recessiveinheritance occurs in EDS I, II, III, IV, VI, andVII. Compound heterozygosity (see later) isalso very likely. X linked forms have beendescribed but are highly unusual. Autosomaldominant inheritance was first mentioned byKopp.'5 Wiener'" described 12 affected sub-jects in three generations. Stuart'7 and Coe andSilver'8 both described the vertical transmis-sion particularly of EDS type I. Johnson andFalls" published a very large five generationAmerican family of British-Canadian extrac-tion with typical EDS I and with two separate
MRC ConnectiveTissue GeneticsGroup, StrangewaysResearch Laboratoryand Department ofClinical Genetics,Addenbrooke's NHSTrust, Cambridge, UKF M PopeN P Burrows
Correspondence to:Dr Pope, StrangewaysResearch Laboratory, WortsCauseway, Cambridge CB14RN, UK.
400
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Ehlers-Danlos syndrome has varied molecular mechanisms
homozygotes. They also speculated upon auto-somal recessive inheritance while both Weberand Aitken"0 and Ronchese" separately de-scribed sporadic examples of EDS I withaffected first cousin parents.Autosomal recessive inheritance occurs in
EDS VI although compound allelic heterozy-gosity may be more common than homozygos-ity except in consanguineous or inbred popula-tions. Beighton5 first suggested autosomalrecessive inheritance in an affected brother andsister whose parents and children were normal.Convincing autosomal recessive inheritancealso occurs in procollagen peptidase deficiency.In humans this causes EDS VIIC and inanimals dermatosparaxis. While the animalskin is excessively fragile, in humans there isextreme joint laxity and blepharochalasis/cutislaxa (CL). The original EDS VII patient ofLichtenstein et al'2 had congenital hip disloca-tions and short stature. Skin from EDS VIICpatients, cattle, sheep, and cats show severelydisorganised and misassembled hieroglyphiccollagen fibrils when examined by transmissionelectron microscopy. Homozygosity or doubleheterozygosity has also been postulated in EDSIV." 23-2 The latter patient had a normal colla-gen III profile. The family of Beasley andCohen'6 with joint laxity, lop ears, and an unu-sual face may also be an example of autosomalrecessive inheritance but was unclassifiableclinically. Apparent X linked pedigrees weredocumented by Beighton" in two British fami-lies with a clinical phenotype resembling EDSII. One family contained six affected males andthree possible carrier females in four genera-
tions. Phenotypic variability is far outweighedby biochemical and molecular diversity so thatindividual families are (almost always) unique.An International Working Party was convenedto standardise the nosology"3 and EDS IX (theoccipital horn syndrome) and EDS XI (famil-ial joint instability) are now excluded from theclassification. Lysyl oxidase deficiency is asso-ciated with Menkes syndrome and X linkedcutis laxa which, while allelic, are not a form ofEDS. The lysyl oxidase dependent form ofEDS has not been confirmed.
Molecular abnormalities causing EDS(table 1)In keeping with recent rapid advances, themolecular mechanisms of many EDS subtypesare now well understood. Most disrupt colla-gen fibril assembly by altering certain crucialmolecular components, the anatomical distri-bution of which dictates the consequentmolecular pathology. Thus the molecular com-
position of regions such as skin, vasculature(arteries, veins, and capillaries), pleuroperito-neum, intestinal walls, ligaments, tendons, car-
tilage, and eyes (the cornea and vitreous) maybe severely weakened and disorganised.Many types of EDS have specific mutations,
while in others, such as EDS III, VIII, and X,the abnormality is either unknown or inconsist-ent. Generally, there are two classes ofmutations, one in which structural genes are
faulty and the other in which their processingenzymes are disturbed.'7 Examples of theformer are mutations of the COLlAl, 1A2,3A1, and 5A1 genes and of the latter lysyl
Table 1 Ehlers-Danlos syndrome (cutis hyperelastica) after Beighton et al'3
Histology electronType Synonym McKusick No Specialfeatures microscopy Basic defectEDS I Gravis type AD 130000 Widespread scarring and Cauliflower COL5A1 linked in some
bruising, especially forehead, fibrils families. Mutationschin, and shin. Molluscoid include exon skips and apseudotumours translocation and a
cysteine substitutionEDS II Mitis type AD 130010 Similar but less severe Cauliflower
fibrilsEDS III Hypermobile AD 130020 No cutaneous scars Non-specific Unknown
typeEDS IV Vascular type AD 130050 Nearly always type III collagen Collagen COL3A1 mutations.
IVA acrogeric deficient depletion, Numerous pointIVB acrogeric AR 22535 variation of fibre mutations and exon skips,
size rarely deletionsIVC ecchymotic AD 130050 Risk of arterial rupture highest in
acrogeric subtypesEDS V X linked type XL 305200 Very rare. Not lysyl oxidase
deficient. Resembles EDS I, II,and III
EDS VI Ocular scoliotic AR 225400 Muscular hypotonia, often Non-specific Lysyl hydroxylase pointVIA decreased muscular dystrophy suspected mutations or exon skipslysyl hydroxylase (slow motor milestones) (homozygosity andlevels double heterozygosity)VIB normal Persistent premature scoliosis.levels Arterial rupture in 30%
EDS VII Arthrochalasis AD 130060 Extremely lax joints with Fibrils vary from Types A & B specificA, B, C multiplex congenital hip dislocation. angular in A and exon 6 skips or deletions
congenita Occasionally mild facial cutis B, to of COLlAl, 1A2 eitherlaxa. Some types have skin hieroglyphic in C pNal (I) or pNa2(1)fragility, mandibular hyperplasia retained. Type C
AR 224510 Severe generalised cutis laxa in procollagen peptidasehumans; dermatosparaxis in deficiency. Both pNal (I)cattle, sheep, and cats and pNa2(I) extensions
retainedEDS VIII Periodontitis AD 130080 Allelic variation with variable Non-specific Some are COL3A1type expression others not
EDS IX VacantEDS X Fibronectin AR 225310 Fibronectin deficient Association with FN may
abnormality be coincidental
401
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Pope, Burrows
B
_-_W-W.~~~~.*
D
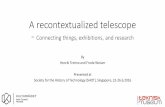
Figure 1 Typical clinicalfeatures ofEDS I; the clinical signs ofEDS II are similarmilder. Shown are the characteristic facial scars (A), extreme cutaneous extensibilityand patellar and pretibial scars (C). Broadened feet and hands are also a feature in s
families, as shown in this affected father and child (D).
hydroxylase or procollagen peptidaseciency. Defects of one or other mech-occur in EDS types I, II, IV, VI, and VII.III, in contrast, is highly heterogeneouscally and overlaps with osteogenesis impe(OI), pseudoxanthoma elasticum (PXE)Marfan syndrome (MFS). Candidateinclude COLlA1, 1A2, 3A1, 5A1, filelastin, lysyl oxidase, and lysyl hydroxylas
Clinical features ofEDS types I and ]
(fig 1)The five cardinal clinical elements ofinclude hyperextensible, doughy skin, atrscars, joint hypermobility, connectivefragility, and bruising (table 1). The c&phenotypes of EDS I and II overlap suttially and are probably allelic autosomalnant mutations with variable penetiCompound heterozygosity is also poEDS type I differs from type II only idegree of skin fragility and ligamentousThe skin splits over prominences suchforehead, chin, elbows, knees, andBroadened hands and feet and a widebuild (mesomorphism) are also con
Other notable clinical signs include epicfolds and fibrous nodules of the knees,and Achilles tendons. Even though mitraprolapse is common, aortic dilatation an
ture are not, and arterial fragility is viiunknown. Non-specific features includeneous varicosities, myopia, and late onsetarthritis (OA). Since collagen a (V) (
occur in cartilage and vitreous humour, t
is probably a direct complication rathe:primarily mechanical. In EDS II the c
phenotype is milder and skin fragility mu(
impressive; epicanthic folds, fibrous nodules,and mesomorphism are infrequent or evenabsent.
Collagen type V and the role ofCOLSA1/COL5A2 genesThere is now strong evidence to implicate typeV collagen c 1 chains in the aetiology of EDS Iand II. Clinical features include excessive skinfragility, ligamentous laxity, and relativelybenign prognosis. The collagen is disorganisedand forms so-called cauliflower fibrils.
Like collagens I, II, III, and XI, collagen Vhas an uninterrupted triple helix with N and Cterminal extensions. There are two or possiblythree forms of collagen V proteins, at least twoof which, ul (V) and a2(V), are coded by sepa-rate non-allelic genes. Firstly, on clinicalgrounds, there are very severely disorganisedcollagen fibrils (cauliflowers) (fig 2D). Sec-ondly, abnormalities of both collagen type V c 1chains and the COL5A1 gene have beendescribed in a sporadic EDS I/II patient withincreased skin fragility and joint laxity withcorneal flattening.21 29 Furthermore, transgenichomozygous mutant mice with an in frameexonic deletion in Col5a23° also had fragileskin, dermal thinning, and corneal disorganisa-
but tion as well as severe skeletal and ligamentous(B), deformities. An equivalent rabbit model showssonie similar pathology. Several independent groups
have detected linkage of human COL5A1defi- markers in families with EDS I or II which are
anism therefore allelic.3' 32 Other COL5A1 mutationsEDS have also recently been reported.33-35 In one, aclini- translocation interrupts the COL5A1 gene atrfecta intron 2433 and in the second an exon 65 skip), and was found in a three generation family.34 Agenes third had a mutation of a highly conserved C)rillin, terminal cysteine. There are therefore at leastse. three published COL5A1 mutations with
either EDS I or II phenotypes. In other similar[I families, linkage to COL5A1 has been
excluded36 (Burrows et al, unpublished data).EDS Somehow, collagen type V controls type I col-
rophic lagen fibril packing.37 ' This credibly explainstissue the gross fibrillar disorganisation which typifieslinical EDS I and II and implies that the disorganisa-bstan- tion is a direct effect of the mutant type V col-domi- lagen. Allegedly, collagen type XI analogouslyrance. regulates the thickness of collagen type II fibrilsssible. and collagen V and XI coassociate with or evenin the substitute for one another in vitreous humour.laxity. Corneal shape is also collagen V dependent.as the Mutations of either collagen type XI geneshins. (COLl lAl or COLl A2) can cause variantsbody of the Stickler syndrome (SS)42 43 in humansnmon. and mice.}+ Since COL lAl but not 11A2 isanthic expressed in the vitreous, only mutations of theshins, former cause vitreous pathology. Collagen
1 valve ci2(V) chains coassociate with ci2(XI) chains,43d rup- which may both coassociate with collagen typertually II. It is therefore not surprising that corneal or
cuta- vitreous abnormalities and high myopia coseg-osteo- regate with premature OA in some EDS fami-chains lies. Furthermore, COL5A2 mutations are a
he OA potential cause of arterial fragility,28 suggestingr than the possibility that c2(V) chains and collagenlinical type III interact analogously to ac(V) chainsch less and type I collagen chains. Lastly, several
402
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Ehlers-Danlos syndrome has varied molecular mechanisms
A. B
c
a
...
E F;- $
.-; ee -
:- A:
.S a,,,F fl0 i F.
-,. F,
s:X,_.4.^- E F
-:: t:>;
_... F.>,t.
S
Figure 2 Transmission electron micrographs showing variably angular and hiefibrils of (A) EDS VIM, (B) EDS VIIB, (C) EDS VIIC. The distortion ts greatest inEDS VIIC in which every collagen a chain has a persistent N terminal extension. (D)Cauliflowerfibres typical ofEDS IIII. (E) Irregularfibrils ofEDS IV (F) Normal controlshowing (to the left) a uniformly sized, transversely sectioned collagen fibril. Fig 2(A) and(B) are reproduced by permission of the authors8' and the Journal ofMedical Genetics,fig2(B)"' by permission of the British Journal of Dermatology. We thank Professor BrianLake of the Institute of Child Health for providingfig 2(C).
different collagen mutations cause disorderedfibrillogenesis in vivo.46 COL5A1 homozygotesare either exceptionally rare or genetic lethals.Good animal models for COL5A1 mutationwill be essential for the future detailed analysisof the chemical composition and 3Dorganisation of tissues such as articular carti-lage, ligament, cornea, vitreous humour, arter-ies, veins, and capillaries.
Clinical features ofEDS type IV (vascularEhlers-Danlos syndrome) (fig 3)Vascular/arterial EDS differs from other varie-ties by virtue of severe vascular fragility, bothvenous and arterial. It was originally describedby Barabas9 and Sack.47 In ecchymotic EDSthere are often post-haemorrhagic haemosi-derin deposits over the knees, shins, andelbows, which may also complicate EDS I/IIand VIII. Acrogeria is specific to EDS IV and ischaracterised by generally thinned skin; theextremities (hands, feet, and face) are prema-turely aged (fig 3A, B). Other suggestivefeatures include prominent capillaries and kel-
oidal or elastotic scars (often with elastosisperforans serpiginosa). Large eyes, lobelessears, and a Madonna-like face are also typical.48Although short stature is usual, occasional slimand tall people overlap with MFS. Other clini-cal features include acro-osteolysis, diffuse alo-pecia of the scalp, and certain orthopaediccomplications such as congenital talipes or hipdislocations and tendon contractures, particu-larly of the Achilles or extensor tendons of thefeet and toes. Pleuroperitoneal or colonic rup-ture are more non-specific (and may also com-plicate other EDS or MFS phenotypes).Vascular pathology includes aneurysms ofsmall to medium sized arteries such as renal,
* splenic, axillary, brachial, femoral, popliteal,* and internal carotid vessels. The internal
carotid system may be compromised by dilata-'.*** ^ tion, arteriovenous malformations, aneurysms,
or dissections caused by arterial thinning and*,|l -** ^ fragility from collagen III deficiency. Occasion-{ ally the general phenotype is EDS III/BHS.489
For example, we observed a Gly->Ser 637 sub-4 ''3 stitution in a large autosomal dominant
pedigree with generalised joint laxity andpremature osteoarthritis.48 4
In EDS IV, skin histology shows strikingdermal thinning (from one-third to two-thirdsof normal), collagen depletion, and elastin pro-liferation. The mechanism of the latter isunclear (and may be primary rather thansecondary to collagen depletion). Transmissionelectron microscopy typically shows collagenfibril disorganisation with irregularity and abimodal size distribution (fig 2E). Somehowcollagen III/I ratios influence collagen fibrildiameter and interactions and, if mutated or
46~A~ diminished, seriously impair long term arterialroglyphic strength and stability.
Protein chemistryThere is very strong clinical, histological,biochemical, and molecular evidence thatfaulty collagen III causes dermal atrophy andvascular and gastrointestinal fragility.23 24 27Firstly, collagen III predominates in skin bloodvessels and ligaments. It is a unique interstitialcollagen, analogous to types I, II, V, and XI. Ithas a specific role in the strength and stabilityof blood vessels where it exerts its maximumclinical effect. The protein is a homotrimer[cal(III)]3 with two intrachain cysteine crosslinks at the C terminus. Collagen III deficiency,in the main, causes vascular EDS but may alsocause other less specific phenotypes such asEDS III.Two patterns are usual. The first (group 1)
exhibits poorly secreted and overhydroxylatedcollagen III proteins caused by either helicalglycine substitutions or exon skips. Thestoichiometry dictates that only one-eighth ofthe triple helices are normal. The remainingseven-eighths contain either one, two, or threefaulty al1(III) chains which are consequentlyretained intracellularly or poorly secreted anddegraded. Not surprisingly, patients with suchsevere biochemical deficiencies have severelyabnormal clinical phenotypes. The secondabnormal pattern includes null alleles (group2). Here reduced collagen type III secretion
403
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

4Pope, Burrows
collagen III, although poorly secreted, is notovermodified. In other words the residualcollagen III molecules are usually normal.Thus, the clinical phenotype is milder, moredifficult to diagnose, and overlaps with EDSIII/BHS or even merges into normality. Simi-larly, the arterial phenotype varies; occasionallythere is premature aortic rupture, internalcarotid or cerebral arterial dilatation, or arterialrupture. In contrast, the more spectacularcarotid-cavernous-sinus aneurysms segregatewith group I mutations. The group 2 (nullallele) phenotype of arterial dilatation andcutaneous striae also overlaps clinically withatypical forms of MFS, from which it may beclinically indistinguishable.
..:
...
Figure 3 Various clinicalfeatures of vascular EDS IV (COL3AI mutations). Thin s(A), prematurely aged hands (B), andfacialfeatures typify the acrogeric subtype (D).Sometimes there is a characteristic circinate rash (elastosis perforans serpiginosa) althotthis can occasionally complicate other inherited connective tissue disorders (C).
without intracellular retention or overmol
cation is the norm. The other allele is usu
wild type but occasionally can be mutantcontrast to the secretory (group I) muta
Molecular pathology ofCOL3A1 mutants(fig 4)Since 1991, there have been rapid advances inphenotype/genotype correlations. Generally, 3'mutations are acrogeric whereas the pheno-
'( types of 5' or middle helical exon skips areharder to recognise. Unfortunately, even the
E latter are at risk of arterial rupture which isnevertheless much more frequent in mutationsat the 3' end. Arterial rupture is difficult, if notimpossible, to predict, occurring as early as thesecond decade (rare) to early or late middle age(very common). Like analogous COLlAl,1A2, or 2A1 mutations,7 they are virtuallyprivate to affected families. They include auto-somal dominant glycine substitutions or exonskips. So far, only three large in frame deletionsranging from 0.5 to 3 kb have beenreported.53.55 A smaller 27 bp intraexonic dele-tion was caused by spliced mispairing.56 Alldisrupt the collagen triple helix by a dominantnegative mechanism. Here, each trimer iseither wild type, or contains three, two, or oneabnormal chains in homotrimers such as colla-gens II and III or in heterotrimers such as col-lagen I. Thus, COL3A1 mutations cause severedisturbance with seven-eighths of the proteinmolecules abnormal compared to heterotrim-ers such as type I collagen where between halfand three-quarters are faulty,50 51 dependingwhether the mutation affects COLlAl orCOL1A2. Both homozygosity and heterozy-gosity for various COL3A1 mutations or com-pound heterozygosity with other collagen orextracellular matrix molecules are also theo-
07" retically possible, although to date there havebeen no published examples. Similar consid-erations also apply to COLlAl and COL1A2(OI mutants) in which only occasional doublemutations have been identified. Perhaps suchdouble hits would be catastrophic in wide-spread tissue components such as collagen I orIII. In contrast, double mutations of minoritycomponents like collagen VII are relatively
kin common. Thus, double glycine substitutionsugh cause severe recessive dystrophic epidermolysis
bullosa while in contrast single glycines areeither clinically silent or can cause minor auto-somal dominant epidermolysis bullosa.57
difi- Reliable genetic counselling and prenatalLally diagnosis are available for most vascular EDSIn patients. This requires a combination of histol-
ints, ogy, electron microscopy, and type III collagen
9
404
III-
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Ehlers-Danlos syndrome has varied molecular mechanisms
A
COL3A1 point mutations
100 200 300 400 500co
600 700rCCIO
80000CDor-r-.
900 1000 1100 1200
Ser la)-C CD
Arg llo00Cm 0 00O
Val l l iiCN N
ax °)oO
Asp l ll.
r-00t 00Gu. .
GIu l l l l
B
COL3A1 splicing and deletions
24
27
9 24
25
37x2 43
i 45
42@
41
7 20 25 34
16 27
SevereEhlers-Danlos IV
ModerateEhlers-Danlos IV
diagramatically in fig 4. Other mutants arereferred to in other studies.6 64 Opinions differas to the relevance of collagen III mutations inintracranial and aortic aneurysms.48 65-67 Thereis little doubt that COL3A1 mutations docause such defects but how frequently remainsto be determined.
Collagen type I mutations (fig 5)Collagen type I is a heterotrimer([al(I)]2a2(I)) of two different a chains. Thegenes COLlAl and COL1A2 are located onchromosomes 17 and 7 respectively. Both areinterstitial collagens with uninterrupted(GlyXY) triple helices and globular, removableN and C termini; other fibrillar collagensinclude types II, III, V, and XI, all with crossbanded fibrils. Mutations of COLlAl andCOL1A2 produce distinctive but overlappingclinical phenotypes which are position, type,and domain related.'1"2 Mutations of either Nterminal extensions each cause EDS VII (withdistinctive clinical features) while, in contrast,helical and C terminal mutations cause 01. Asexpected, OI and EDS VII overlap clinicallyand biochemically.68 69 In EDS VII, cutaneousfragility and ligamentous laxity predominate,while in OI the bones are abnormally fragile.OI families with loose ligaments and fragile,delicate blood vessels and skin are uncommon,while otherwise typical EDS families some-times have bone fragility/osteoporosis. Theclinical phenotype is strictly dictated by muta-tional position and EDS VII is an especiallyfocused example. Its mutations all causeskipping of exon 6 of either the COLlAl orCOL1A2 gene.27 5o51 By contrast, mutationswhich cause OI are more diffusely distributedbetween exons 7 and 52. In general the pheno-type worsens with higher exon numbers (3' endor C terminal locations). EDS VII is caused bytwo distinct but related mechanisms. Eitherthere is a structural abnormality of thepeptidase cleavage site or the cleaving enzymeis faulty.
14 24 37 Milder
-27/54 Ehlers-Danlos IV
33 48
5 10 20 25 30 35 40 45 50
Figure 4 Map of recently published COL3AI mutations. (A) Glycine substitutionsarranged by residue number and (B) exon skips or large deletions (studies ofKuivaniemi etal" and Pope et a8).
protein or COL3A1 gene analysis. Prenataldiagnosis by amniocentesis, chorionic villusbiopsy, or termination of pregnancy is poten-tially hazardous in affected females owing tothe inherent fragility of cervical, uterine, or
abdominal blood vessels. On the other hand,opinions vary as to the safety or dangers ofpregnancy in this subset.58 59
Two recent papers48 60 summarise the variouspublished COL3A1 mutations in vascular EDSIV. The 41 published mutations are illustrated
EDS type VII (fig 6E)There are two distinctive clinical phenotypes,one overlapping with EDS I/II and the otherwith congenital cutis laxa. The former is mildand autosomal dominant, while the latter issevere and autosomal recessive. EDS VIIA andB result from structural mutations of type Icollagen,22 while EDS VIIC is caused by theenzyme deficiency. Clinical signs include shortstature and excessive premature ligamentouslaxity (such as congenital dislocation of thehips). There may also be excessive cutaneousfragility reminiscent of EDS I/II, or mild cutislaxa (CL). Spinal and ligamentous deformitiessuch as kyphoscoliosis are relatively infrequent.In contrast to EDS I/II, in EDS VIIA and Bcollagen fibril morphology is only marginallyabnormal and the fibres are angular intransverse section rather than forming cauli-flowers (fig 2A, B). On the other hand, EDSVIIC shows grossly distorted, hieroglyphicfibrils.
405
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Pope, Burrows
Normal allele
{I AJ4 A
I.V.S.5 I.V.S.6
COLIA 1
GTAG exon 6'AG Weil et al 1989a
GT AG exon 6*A GT AG exon D'Alesslo et al 1991
COLIA 2
GTI-AG exon 6 |GC* AG exon 7 Weil et al 1988
exonGGT AG| exon 6 GC* AG exon7 Hoet al 1994
GTexon 6'A | Weil et
1989b
GT AG exon 6 ]*CT AG exon 7 Chlodo et al 1992
5GT- exon 6 'AT Weil 1990
OGT AG exon 6 *AT AG Nicholls et al 1991
exon5GT -AG exon 6 *AT AG axon Watson etal 1992
exonG5 GT AG exon 6 *AT- AG Lehman et al 1994
exon5GT -AG| exon 6 'AT -AG exon 7 Vasan et al 1990
Figure 5 Diagrammatical representation of various published exon 6 splice junctionmutations causing EDS VIIA or B. Coding sequences (exons) are boxed while non-codingsequences (introns) are shown as lines. The first two bases (splice donor) and last two bases(splice acceptor) of the intron sequence are always GT orAG respectively. Mutations are
denoted by asterisks.
Deletion of the peptidase cleavage siteSince collagen type I is a heterotrimer, loss ofeither the pNa 1 or pNa2 cleavage sites can
cause EDS VII. When pNal sequences are
uncleaved three-quarters of collagen type Iheterotrimers possess either one or two persist-ent pNa chains. With pNa2 defects, half thetype I collagen retains abnormal pNa2 se-
quences while the rest become normal a2chains. In both circumstances collagen fibrilassembly is compromised and normal head to
tail packing of individual triple helical mole-cules is severely disrupted. The persistent pNsequences seriously distort gap regions. Suchmisassembled fibrils are visible by transmissionelectron microscopy, which shows slightlyirregular to angulated structures in cross
section. When thicker than 10 nm, both initialnucleation and subsequent fibril growth are
seriously distorted by the presence of persistentpNa sequences374" 7' which are longer than theaggregating a chains. Exon skips also disrupttype I collagen a chains since both the pepsinand peptidase cleavage sites are deleted.Protein electrophoresis of pepsinised a chainstherefore shows elongated molecules withabnormally persistent pN sequences in addi-tion to the correctly cleaved normal a chains.Such abnormal pN proteins can also bepurified from NaCl extracted tissues. Procolla-gen "snapshots" also show inefficient process-ing patterns. Following the original descrip-tions of Lichtenstein et af22 of faulty conversionof procollagen to collagen in EDS VII, persist-ent pNa 1 and pNa2 components were sepa-rately demonstrated by Steinmann et ao0 71 andCole et al.72 73 Subsequently, various missplic-ing mutations of exon 6 sequences caused byfaulty splice acceptor or donor sequences havebeen discovered. Most are near to the obligate
G of the 5' intron acceptor GT sequence inintron 6 (fig 5).7484
Mutations ofprocollagen peptidase (PP)PP deficiency of cows was first described byLapiere et al.85 The animals had excessivelyfragile skin (dermatosparaxis), which was agenetic lethal. Transmission EM of the dermisshowed numerous bizarrely shaped collagenfibrils which formed flanged rods instead ofnormal cylinders. In transverse section theseappeared as hieroglyphs while in longitudinalsection they were severely disaggregated andtwisted. Biochemical analysis showed abnor-mally elongated collagen pNal and a2 chainswhich were extractable with salt or acidsolutions, implying abnormal cross linking. Atthe time, procollagen was thought to have sin-gle N terminal extensions and no C terminaladditions. In contrast to EDS type VIIA and B(see above), every component of type I triplehelix are abnormal, that is, contains bothpNal(l) and pNa2(1) chains. Consequently,no normal collagen triple helices are formed:instead fibrils assembled form [pNa(I)] 2pNa2(I) triple helices. Consequently, fibrillarpacking is very seriously disrupted (fig 2C).The equivalent human phenotype was notidentified until recently.85.89 Various otheranimal models such as sheep90 and Himalayancats9' were described previously, but includedvery convincing clinical and structural data,and the expected hieroglyphic fibrils andderanged biochemistry. The human clinicalphenotype unexpectedly showed prematurecutis laxa (CL) with blepharochalasis. So farthree examples have been published, two withexceptionally clear biochemical data and thethird with excellent illustrations of the clinicalphenotype.87.89 Both the French and Americandescriptions included disturbed procollagenprocessing, pNal (1) or a2(1) molecules, hiero-glyphic fibres, and deficient enzyme levels. Thephenotype of Smith et al88 included prematuredelivery, soft, fragile, and easily bruised skin,and patchily sagging skin, while in the patientof Nusgens et al,87 skin fragility, bruising, andgeneralised osteoporosis were notable. Rear-don et al,89 in contrast, described severe prema-ture generalised CL with blepharochalasis,redundant skin, and fragility. Every patient hadtypical hieroglyphic fibrils. Transient CL alsooccurs with the milder EDS VII type A and Bphenotypes in which skin fragility varies. Eventhough less disrupted than dermatosparaxis,the fibrils of EDS VII A and B can be manipu-lated to produce hieroglyphics under suitableexperimental conditions.92 Plainly the faultyangular fibrils characteristic of exon 6 deletions(which cause EDS VII A and B) are one step inthe progression from normal cylinders tohieroglyphs. Theoretically both more localisedand extensive mutations within and aroundexon 6 of the N propeptide coding region couldproduce a wider spectrum of fibrillar angularityand clinical features which are maximised inthe propeptidase enzyme deficiency of animalsand humans.
406
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Ehlers-Danlos syndrome has varied molecular mechanisms
A V. C
IE
Figure 6 Various physicalfeatures ofEDS III (A, B), EDS VI (C, D), and EDS VII (E). In practice a degree of laxity(A, B) can complicate any of the EDS subtypes but is a sole feature in EDS III. Scoliosis is a consistent feature ofEDS VI,sometimes complicates EDS VII, and rarely occurs in EDS I, II, and III. The criss cross lines shown in (D) are typical ofeither EDS VI or EDS VII and a slight facial cutis laxa is particularly characteristic ofEDS VII (E). At other times thelatter shows cutaneous fragility very similar to that offig 1.
Other enzyme abnormalities causingEDSOther crucial post-translational modificationsof fibrillar collagen triple helices include enzy-matic hydroxylation of certain lysines and exci-sion of the C propeptides in addition totrimming by the specific N propeptidases.Lysyl oxidase then promotes cross links bydecondensing hydroxylysines to aldehydes.Mutated enzymes cause very specific forms ofEDS. Thus, lysyl hydroxylase (LH) deficiencycauses EDS VIA93-'04 while procollagen pepti-dase deficiency causes EDS VIIC85-87 (see alsoabove). The role of lysyl oxidase is morecontroversial'05 106 and so far the diseasescaused by C terminal propeptidase mutationsare unknown. Since the C propeptide is essen-tial for chain association, homozygous enzymemutations might be genetically lethal. Bonemorphogenic protein 1 (BMP1) and the Cpropeptidase are now known to beidentical.'O7 108
Ehlers-Danlos syndrome type VI (lysylhydroxylase deficiency) (fig 6C)The disorder was first recognised as unique byMcKusick,'2 although Beighton et all3 hadobserved autosomal recessive inheritance in afamily with severe spinal deformities, ligamen-tous laxity, ocular fragility, and retinal detach-ment. There is extreme ligamentous laxity withsevere ocular fragility, retinal detachment, andscleromalacia. The severe ligamentous prob-lems present in early infancy usually withmotor delay caused by severe muscular hypoto-
nia. Sometimes muscular dystrophy is(wrongly) suspected but nearly all affectedchildren eventually walk normally. The diffi-culties are caused by excessive ligamentouslaxity which young muscles cannot adequatelycontrol. In adult life or middle age, there maybe aortic dilatation or arterial rupture.Krane et al3 and Pinnell et al4 then
discovered underhydroxylation of lysine anddeficient collagen lysyl hydroxylase in twoaffected sisters with severe infantile hypotonia,premature scoliosis, and ocular fragility. Othersignificant features included soft, hyperextensi-ble, easily scarred skin and premature ruptureof the membranes. There are two similar clini-cal phenotypes, type VIA with enzyme defi-ciency and type VIB with normal enzyme.There may also be a third, predominantly ocu-lar, variant.
Biochemistry and molecular pathology(table 2)Krane et at3 and Pinnell et al4 measuredenzyme activity using tritium labelled chickprocollagen as substrate. Nearly 20 years later,both the chick and human genes were clonedand sequenced.95 96 LH or procollagen lysyl 2oxoglutarate 5 dioxygenase requires copper,Fe", and 02 as cofactors. EDS VI is caused byeither deficient or faulty enzymes with variableKm or V max.97 98 The mutations are oftencomplex and include Alu-Alu compoundrecombinations and homozygous or doubleheterozygous exon skips.98-'02 Homozygousdeletions tend to cluster in inbred families. The
407
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

4Pope, Burrows
Table 2 Lysyl hydroxylase mutations (the gene has 19 exons)
Ha et al 9 Double heterozygote 3 base pair deletion Glu (-) 532 andGly 678 to Arg
Hautala et al 9 Homozygous 7 exon duplication rearrangement at Alu/Alu in two sibs
Hyland et al 1'0 Homozygous stop codon Arg 319-X:CGA-TGAPousi et al "' As for Hautala et al9 but in an unrelated female
hydroxylysine content of defective tissuesvaries between 5% and 50% being lowest inskin, bone, and tendon. Collagen I is more
underhydroxylated than collagen III, while col-lagens II, IV, and V are normally hydroxylated.This implies more than one hydroxylase withvariable specificity for other collagen types, so
that other clinical phenotypes are also likely.Underhydroxylation of collagen al (1) anda2(1) chains causes overmigration and impairscondensation cross linking of adjacent hy-droxylysines which can be measured inurine.'03 104 Urine sampling and type I collagena chain electrophoresis are simple and usefulscreens for enzyme deficiency.
The C terminal propeptide (BMPI)deficiencyIt is now apparent that the C terminalpropeptidase (CPP) is identical to bonemorphogenetic protein 1 (BMP 1). The latter ishomologous to the Drosophila pattern forma-tion genes TLD and TRI with analogues ininsects and sea urchins, such as the BP 10 andSpAN genes which are TGFO activators.'07Homozygous enzyme deficiencies would eitherbe genetic lethals or severely crippling inmechanical terms. Persistence ofpC extensionswould severely impair collagen triple formationjust as persistent pN sequences interfere withmolecular packing. Errors of the pC extensionswould seriously disrupt both helical windingand chain association; quite possibly collagentriple helices would not form at all. The effectsof C propeptidase deficiency should be worse
than N propeptidase deficiency which causes
EDS VIIA-C. Holmes et ar' studied thestepwise removal of pC or pN propeptidesbefore collagen fibrillogenesis. Retention ofeither extension by faulty processing inhibitsfibril formation as do helical mutations of thefully processed molecule.
Heterozygotes for CPP deficiency might alsohave impaired fibrillogenesis. Homozygositycould easily cause severe clinical phenotypes,such as lethal 01, and certain severe chondro-dysplasias or EDS variants either as allelichomozygotes or as double heterozygotes incombination with other ECM propeptidemutations such as pC I, II, III, V, or XI abnor-malities respectively.
EDS variants ofunknown cause
This applies to EDS types III, VIII, and X inwhich the causes are non-specific (EDS III),variable (EDS VIII), or represented by a singleone-off example (EDS VIII).
EDS type III (fig 6 A, B)Unlike EDS types I and II there is no
significant cutaneous scarring despite obviousjoint hypermobility and doughy skin. This
clinical subtype merges with the so-calledbenign hypermobile syndrome (BHS) butwhich has normal skin texture. This milderclinical phenotype can also segregate in typicalEDS I/II families probably owing to incom-plete penetrance. Similar clinical features mayalso accompany COL3A1 mutations," suchas MFS and SS. Heterozygotes for autosomalrecessive disorders such as PXE and lysylhydroxylase deficiency (EDS VI) have verysimilar clinical phenotypes.109 There can also beoverlap (clinical and biochemical) with vascu-lar EDS (see above).
EDS type VIIIFirst described by Stewart et all'" this pheno-type is clinically, biochemically, and allelicallyheterogeneous. Distinguishing clinical featuresinclude chronically inflamed, heavily pig-mented, discrete, pretibial plaques and prema-ture periodontal recession. There is collagendegradation as judged by gum resorption andthe cutaneous inflammation. In EDS VIII noconsistent biochemical or structural changesare detectable...... Certain mutant collagensmay be abnormally proteinase susceptible.Alternatively, faulty collagenase inhibitors suchas TIMP might be implicated, although all ofour EDS VIII patients have normal TIMP pro-files. We have observed both vertical and hori-zontal transmission of early adult gum reces-sion, sometimes accompanied by collagen IIIdeficiency. Similar features may accompanyEDS I, II, and IV. Others have also noted thisphenotype.111-114 The distinctive clinicalphenotype'06 is therefore biochemically andgenetically heterogeneous. Histology of theskin lesions shows a granulomatous collagendegeneration resembling necrobiosislipoidica. '15
Ehlers-Danlos syndrome with fibronectindeficiency (EDS X)Only one family with this phenotype has beendescribed."6 This included four affected sibs inone generation but with normal parents, whichMcKusick later classified as autosomal reces-sive. The phenotype includes thin, fragile, eas-ily scarred skin, joint hypermobility, and exces-sive bruising and therefore resembles EDSII/III. Platelet aggregation was abnormal butcorrectable with normal fibronectin. In otherEDS families a variety of clotting abnormalitieshave been described which are too inconsistentto be directly related."7 118
1 Tschernogobow A. Cutis laxa (presentation at the FirstMeeting of the Moscow Dermatological and VenereologicSociety, November 13, 1891). Mscht Prakt Derm1892;14:76.
2 Ehlers E. Cutis Laxa neigung zu haemorrhagien in der haut,lockerung mehrerer artikulationen. DermatologischeZeitschrifte 1901;8:173-5.
3 Danlos M. Un cas de cutis laxis avec tumeures parcontusion chronique des coudes et des genoux (xanthomejuvenile pseudo-diabetique) de MM Hallopeau et Mace deLkpinay. Bull Soc Franc Derm Syph 1908;19:70-2.
4 Poumeau-Delille GA, Soulie P. Un cas d'hyperlaxitecutanee et articulaire avec cicatrices atrophiques etpseudo-tumeurs molluscoides (syndrome d'Ehlers-Danlos). Bull Soc Med Hopitaux de Paris 1934;50:593-5.
5 Beighton P. Ehlers-Danlos syndrome. London: HeinemannMedical Books, 1970.
6 Morris M. Diseases of the skin. 4th ed. Plate XL. London:Cassell & Co, 1908.
408
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Ehlers-Danlos syndrome has varied molecular mechanisms
7 Beighton P. McKusick's heritable disorders of connective tissue.5th ed. St Louis: Mosby, 1993.
8 Mories A. Ehlers-Danlos syndrome, with the report of afatal case. Scot Med]3 1960;5:269-72.
9 Barabas AP. Heterogeneity of the Ehlers-Danlos syndrome:description of three clinical types and a hypothesis toexplain the basic defect(s). BM3 1967;ii:612-13.
10 Beighton P. Lethal complications of the Ehlers-Danlos syn-drome. BM3 1968;ii:656-60.
11 Beighton P. X-linked recessive inheritance in the Ehlers-Danlos syndrome. BM3 1968;ii:409-1 1.
12 McKusick VA. Ehlers-Danlos syndrome. In: Heritable disor-ders of connective tissue. 4th ed. St Louis: Mosby, 1972:292-371.
13 Beighton P, De Paepe A, Danks D, et al. Internationalnosology of heritable disorders of connective tissue, Berlin1986. Am _Med Genet 1988;29:581-4.
14 Beighton P, De Paepe A, Hall JG, et al. Molecular nosologyof heritable disorders of connective tissue. Am _Med Genet1992;42:431-48.
15 Kopp J. Demonstration zweier Falle im "Cutis Laxis."Munchen Med Wochenshrift 1888;135:259.
16 Wiener K. Gummihaut (Cutix Laxa) mit diminantervererbung. Arch Dermatol Syph 1924;148:559-6 1.
17 Stuart AM. Three cases exhibiting the Ehlers-Danlossyndrome. Proc R Soc Med Lond 1937;30:984-6.
18 Coe M, Silver SH. Ehlers-Danlos syndrome (cutis hyper-elastica). Am Dis Child 1940;59: 129-35.
19 Johnson SAM, Falls HF. Ehlers-Danlos syndrome: a clinicaland genetic study. Arch Dermatol Syph 1949;60:82-105.
20 Weber FP, Aitken J. Nature of the subcutaneous spherules insome cases of Ehlers-Danlos syndrome. Lancet 1938;i: 198-200.
21 Ronchese F. Dermatorrhexis with dermatochalasis andarthrochalasis (the so called Ehlers-Danlos syndrome). AmDis Child 1936;5:1403-10.
22 Lichenstein JR, Martin GR, Kohn LD, et al. Defect in con-
version of procollagen to collagen in a form of Ehlers-Danlos syndrome. Science 1973;182:292-300.
23 Pope FM, Martin GR, Lichtenstein JR, et al. Patients withEhlers-Danlos syndrome type IV lack type III collagen.Proc Nat Acad Sci USA 1975;72:1314-16.
24 Pope FM, Martin GR, McKusick VA. Inheritance ofEhlers-Danlos syndrome type IV syndrome. Arch Dis Child1977;63: 1016-25.
25 Suhl HMB, Steinmann B, Rao VH, et al. Ehlers-Danlossyndrome type IVD: an autosomal recessive disorder. ClinGenet 1984;25:278-87.
26 Beasley R, Cohen MM Jr. A new presumably autosomalrecessive form of Ehlers Danlos syndrome. Clin Genet1979;16: 19-24.
27 Pope FM. Ehlers-Danlos syndrome. Rheumatic manifesta-tions of haematological disease. Ballieres Clin Rheumatol199 1;5:321-49.
28 Nicholls AC, McCarron S, Narcisi P, et al. Molecularabnormalities of type V collagen in Ehlers-Danlos syn-drome. Am] Hum Genet 1994;55:A233.
29 Nicholls AC, Oliver JE, McCarron S, et al. An exon skippingmutation of a type V collagen gene (COL5AI) inEhlers-Danlos syndrome. IMed Genet 1996;33:940-6.
30 Andrikopoulos K, Liu X, Keene DR, et al. Targetedmutation in the colSa2 gene reveals a regulatory role fortype V collagen gene during matrix assembly. Nat Genet1995;9:31-6.
31 Loughlin J, Irwen C, Butcher S, et al. Linkage of the gene
that encodes the aI chain of type V collagen (COL5AI) totype II Ehlers-Danlos syndrome (EDS II). Hum Mol Genet1995;4:1649-51.
32 Burrows NP, Nicholls AC, Yates JRW, et al. The gene
encoding collagen al(V) (COL5Al) is linked to mixedEhlers-Danlos syndrome type I/II. Invest Dermatol 1996;106:1273-6.
33 Toriello HV, Glover TW, Takahara K, et al. A translocationinterrupts the COL5Al gene in a patient with Ehlers-Danlos syndrome and hypomelanosis of Ito. Nat Genet1996;13:361-5.
34 Wenstrup RJ, Langland G, Willing MC, et al. A splice-junction mutation in the region of COL5A1 that codes forthe carboxyl propeptide of pro-cal (V) chains results in thegravis form of the Ehlers-Danlos syndrome (type 1). HumMol Genet 1996;5:1733-6.
35 De Paepe A, Nuytinck L, Naeyart JM. Substitution of a
highly conserved cysteine in the C-propeptide of the pro
a2 1(V) collagen chain causes Ehlers-Danlos syndrometype I. Am] Hum Genet 1996;59:A255.
36 Greenspan DS, Northrup H, McAllister KA, et al.COL5A1: fine genetic mapping and exclusion as candidategene in families with nail-patella syndrome, tuberous scle-rosis, hereditary haemorrhagic telangiectasia and Ehlers-Danlos syndrome type II. Genomics 1995;25:737-9.
37 Birk DE, Fitch JM, Babiarz JP, et al. Collagen fibrillogenesisin vitro: interaction of types I and V collagen regulates fibrildiameter. Cell Sci 1990;95:649-57.
38 Birk DE, Fitch JM, Babiarz JP, etal. Collagen I and V arepresent in the same fibril in the avian corneal stroma. ]tCellBiol1988;106:999-1008.
39 Linsenmayer TF, Gibney E, Igoe F, et al. Type V collagen:molecular structure and fibrillar organisation of chickenal (V) NH,-terminal domain, a putative regulator ofcorneal fibrillogenesis.] Cell Biol1993;121:1181-9.
40 Moradi-Ameli M, Rousseau JC, Klemen JP, et al. Diversityin the processing events at the N terminus of collagen V.Eur] Biochem 1994;221:987-95.
41 Broek DL, Madri J, Eikenberry EF, et al. Characterisation ofthe tissue form of type V collagen from chick bone. J BiolChem, 1985;260:555-62.
42 Vikkula M, Mariman ECM, Liu VCH, et al. Autosomaldominant and recessive osteochondrodysplasias associatedwith the COLl 1A2 locus. Cell 1995;80:431-7.
43 Richards AJ, Yates JR, Williams R, et al. Stickler syndrometype 2 has a mutation in the COLI lAl gene resulting inthe substitution of glycine 97 by valine in al (XI) collagen.Hum Mol Genet 1996;5:1339-43.
44 Li Y, Laurda DA, Warman ML, et al. A fibrillar collagengene, Col 1 lal is essential for skeletal morphogenesis. Cell1995;80:423-30.
45 Mayne R, Brenton RG, Mayne PM, et al. Isolation andcharacteristics of the chains of type V/type XI collagenpresent in bovine vitreous. J Biol Chem 1993;268:9381-6.
46 Hausser I, Anton-Lamprecht I. Differential ultrastructuralalterations of collagen fibrils in Ehlers-Danlos syndrometypes I-IV as a means of diagnosis and classification. HumGenet 1994;3:394-407.
47 Sack G. Status dysvascularis: Ein falle von besondererZerreislichkeit de Blutgefasse. Deutsch Arch Kin Med1936;178:663-9.
48 Pope FM, Narcisi P, Nicholls AC, et al. COL3A1 mutationscause variable clinical phenotypes including acrogeria andvascular rupture. Br] Dermatol 1996;135:231-6.
49 Narcisi P, Richards AJ, Ferguson SD, et al. A family withEhlers-Danlos syndrome type III/articular hypermobilitysyndrome has a glycine 637 to serine in type III collagen.Hum Mol Genet 1994;3:1617-20.
50 Pope FM. Molecular abnormalities of collagen. In: Maddi-son PJ, Isenberg DA, Woo P, Glass D, eds. Oxford textbookof rheumatology. Vol I. Chapter 2.2. Oxford: Oxford Univer-sity Press, 1993.
51 Prockop DJ, Kivirrikko KI. Collagens: molecular biologydiseases and potentials for therapy. Annu Rev Biochem1995;64:403-34.
52 Cole WG, Dalgleish R. Perinatal lethal osteogenesis imper-fecta. ] Med Genet 1990;32:286-9.
53 Lee B, D'Alessio M, Vissing H, et al. Characteristics of alarge deletion associated with a polymorphic block ofreported dinucleotides in the type III procollagen gene(COL3A1) in a patient with Ehlers Danlos syndrome typeIV.AmJHum Genet 1991;48:511-17.
54 Vissing H, D'Alessio M, Lee B, et al. Multi exon deletion inthe procollagen III gene is associated with mild EDS typeIV. ] Biol Chem 1991;266:5644-8.
55 Milewicz DM, Witz AM, Smith AC, et al. Parental somaticand germline mosaicism for a multi exon deletion withunusual end points in a type III collagen which producesEhlers-Danlos syndrome type IV in the heterozygoteoffspring. Am _Hum Genet 1993;53:62-70.
56 Richards AJ, Lloyd JC, Narcisi P, et al A 27 base-pair dele-tion from one allele of the type III collagen gene(COL3A1) in a large family with a typical Ehlers-Danlossyndrome type IV. Hum Genet 1992; 88:325-30.
57 Christiano AM, Anton-Lamprecht I, Amano S, et al. Com-pound heterozygosity for COL7A1 mutations in twins withdystrophic epidermolysis bullosa; a recessive paternaldeletion/insertion mutation and dominant negative mater-nal glycine substitution results in a severe phenotype. Am ]fHum Genet 1996;58:682-93.
58 Rudd NL, Nimrod C, Holbrook KA, et al. Pregnancy com-plications in type IV Ehlers Danlos syndrome. Lancet1983;i:50-3.
59 Pope FM, Nicholls AC. Pregnancy and Ehlers-Danlos syn-drome type IV. Lancet 1983;i:249-50.
60 Kuivaniemi H, Tromp G, Bergfeld WF, et al. Ehlers-Danlossyndrome type IV: a single base substitution of the lastnucleotide of exon 34 in COL3A1 leads to exon skipping.]Invest Dermatol 1995;105:352-6.
61 Richards AJ, Narcisi P, Ferguson C, et al. Two newmutations affecting the donor splice site of COL3A1 IVS37 are causing skipping of exon 37 in patients with Ehlers-Danlos syndrome type IV. Hum Mol Genet 1994;3:1901-2.
62 Lloyd J, Narcisi P, Richards A, et al. T+6 to C+6 mutationin the donor splice of COL3A1 IVS7 causes exon skippingand results in Ehlers-Danlos syndrome type IV. _] MedGenet 1993;30:376-80.
63 Richards AJ, Narcisi P, Lloyd J, et al. The substitution ofglycine 661 by arginine in type III collagen producesmutant molecules with different thermal stabilities andcauses Ehlers-Danlos syndrome type IV. _] Med Genet1993;30:690-3.
64 Nuytinck L, De Paepe A, Pierard GE, et al. Single strandconformation polymorphism (SSCP). Analysis of theCOL3A1 gene detects a mutation that results in the substi-tution of glycine 1009 valine and causes severe Ehlers-Danlos syndrome type IV. Hum Mutat 1994;3:268-74.
65 Tromp G, Wu Y, Prockop DJ, et al. Sequencing of cDNAfrom 50 unrelated patients reveals that mutations in thetriple-helical domain of type III procollagen are aninfrequent cause of aortic aneurysms.
_Clin Invest
1993;91:2539-45.66 Kuivaniemi H, Prockop DJ, Wu Y, et al. Exclusion of muta-
tions in the gene for type III collagen (COL3A1) as a com-mon cause of intracranial aneurysms or cervical arterydissections: results from sequence analysis of the codingsequence of type III collagen from 55 unrelated patients.Neurology 1993;43:2652-8.
67 Pope FM, Kendall BE, Slapak GI, et al. Type III collagenmutations cause fragile cerebral arteries. Br 7 Neurosurg1991;5:537-57.
409
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from

Pope, Burrows
68 Hata R, Kurata SI, Shinkai H. Existence of malfunctioningpro alpha 2(I) collagen genes in a patient with a pro alpha
2(1) chain - defective variant of Ehlers-Danlos syndrome.EnirJ Biochenti 1988; 174:231-7.
69 Sasiki T, Gran K, Ono M, et al. Ehlers-Danlos syndrome: a
variant characterised by the deficiency of the pro alpha 2
chain of type I procollagen. Arch Dernatol 1987;123:76-9.70 Steinmann B, Tuderman L, Martin GR, et al. Evidence for
structural mutation of procollagen tvpe I in a patient withEhlers-Danlos syndrome type VII. EuirJ Pediatr 1979;130:
203-5.71 Steinmann B, Tuderman L, Peltonen L, et al. Evidence for a
structural mutation of procollagen type I in a patient withEhlers-Danlos syndrome type VII. Biol Chenm 1980;255:8887-93.
72 Cole WG, Chan D, Chambers GW, et al. Deletion of 24aminoacids from the pro alpha (I) chain of type I procol-lagen in a patient with Ehlers-Danlos syndrome type VII..Biol Che/so 1986;261:5496-503.
73 Cole WG, Evans R, Sillence DO. The clinical features ofEhlers-Danlos syndrome type VII due to a deletion of 24
amino acids from the pro alpha 1 (I) chain of type I procol-lagen. JMed Genet 1987;24:698-701.
74 Weil D, Bernard M, Combates N, et al. Identification of a
mutation that causes exon-skipping during collagen
pre-mRNA splicing in an EDS variant. .7 Biol Chein1980;263:8561-4.
75 Weil D, D'Alessio M, Ramirez F, et al. Base substitution in
the exon of a collagen gene causes alternative splicing andgenerates a structurally abnormal polypeptide in a patient
with Ehlers-Danlos syndrome type VII. EMBO .7 1989;8:1705-12.
76 Weil D, D'Alessio M, Ramirez F, et al. Structural and func-tional characterisation of a splicing mutation in the pro
alpha 2 (I) collagen gene of an Ehlers-Danlos svndrometype VII.JBiolChenm 1990;265:16007-1 1.
77 Weil D, D'Alessio M, Ramirez F, etal. Temperature-dependent expression of a collagen splicing defect infibroblasts of a patient with Ehlers-Danlos syndrome type
VII. BRio! Checot 1989;264: 16804-9.78 Nicholls AC, Oliver JE, Renouf DV, et al. Ehlers-Danlos
syndrome type VII. A single base change that causes exon
skipping in the type I collagen u2 (I) gene. Huon Genet199 1;87: 183-98.
79 Vasan N, Kuivaniemi H, Vogel BE, etal. Mutation in the pro
u2 (I) gene (COLIA2) for type I procollagen in
Ehlers-Danlos syndrome type VII. Evidence suggesting
that skipping of exon 6 in RNA splicing may be a common
cause of the phenotype. AntJ Hunt GeCet 1991;148: 305-17.80 Watson RB, Wallis GA, Holmes DF, et al. Ehlers-Danlos
syndrometype VII B; incomplete cleavage of abnormaltype I procollagen by N-proteinase in vitro results in theformation of copolymers of collagen and partially cleavedpNcollagen that are near-circular in cross-section. .7BiolCheCn 1996;257:9093.
81 Carr AJ, Chiodo AA, Hilton JM, etal. The clinical featuresof Ehlers-Danlos syndrome type VIIB resulting from a basesubstitution at the splice acceptor site of intron V of theCOL Al gene. 7 MedGeCtet 1994;31:306-1 1.
82 Chiodo A, Hockey A, Cole WG. A base substitution at thesplice acceptor site of intron 5 of the COL1A2 gene
activates a cryptic splice site within exon 6 and generates
abnormal type I procollagen in a patient with Ehlers-Danlos syndrome type VII. Biol Chent 1991;267:6361-9.
83 Ho KK, Kong RY, Kuffner T, etal. Further evidence thatthe failure to cleave the minor amino propeptide of type Iprocollagen is the cause of Ehlers-Danlos syndrometypeVII. Hant Muitat 1994;3:358-64.
84 Lehmann HW, MandlosS, Winterpacht A, etal. Ehlers-Danlos syndrome type VII: phenotype and genotype. ArcliDerntiatot Res 1994;286:425-8.
85 Lapie&e CM, Lenaers A, Kohn LD. Procollagen peptidase:an enzyme excising the co-ordination peptides of procolla-gen. Proc NatlAcad Sci USA 197 1;68:3054-8.
86 Lapiere CM, Nusgens BV. Ehlers-Danlos syndrome type
VIIC or human dermatosparaxis. The offspring of a union
between basic and clinical research. Arch Dcrtnato!1993;129:1316-19.
87 Nusgens BV, Verellen-Dumoulin CW, Hermanns-Le T,eta!. Evidence for a relationship between Ehlers-Danlos syn-
drome type VII C in humans and bovine dermatosparaxis.Nat Gcttct 1992;1:214-17.
88 Smith LT, Wertelecki W, Milstone LM, et a!. Humandermatosparaxis: a form of Ehlers-Danlos syndrome thatresults ftom failure to remove the amino-terminal propep-tide type I procollagen. Anti 7 Hwon Genet 1992;51:235-44.
89 Reardon W, Wintet RM, Smith LT, et a!. The natural historyof human dermatosparaxis (Ehlers-Danlos syndrome type
VII C). C/itt Dstntrphto! 1995;4:1-1 1.90 Fjolstad M, Helle 0. A hereditary dysplasia of collagen in
sheep.77 Patho!1974;112:183-8.91 Counts D, Byets PH, Holbrook K<A, et al. Dermatosparaxis
in a Himalayan cat. Biochemical studies of dermal
collagen.7 Invcst Dertato! 1980;-74:96-9.92 Holmes DF, Watson RB, Steinmann B, et a!. Ehlers-Danlos
syndrome type VII B: morphology of type I collagen fibrils
formed in vivo and in vitro is determined by the conforma-tion of the retained N propeptide. Y7 Biol Chctmt 1993;68:15758-65.
93 Krane SM, Pinnell SR, Erbe RW. Lysvl procollagenhydroxylase deficiencv in fibroblasts from siblings withhydroxylysine deficient collagen. Proc Natl Acad Sci USA1 972;69:2899-903.
94 Pinnell SR, Krane SM, Kenzora JE, ct a!. A heritable disor-der of connective tissue: hydroxvlysine deficient collagen. NEtigl7Med 1972;286:1013-20.
95 Myllyla R, Pihlajaniemi T, Pajunen R, ct al. Molecular clon-ing of the chick lysyl hydroxylase: little homology inprimary structure to the two types of subunit of prolyl4-hydroxylase 7 Biol Chent 1991 ;266:2805-1 0.
96 Hautala T, Byers MG, Eddy RI, et al. Cloning of human lyslhydroxylase: complete DNA-derived amino acid sequenceand assignment of the gene (PLOD) to chromosomelp36.3-36.2. Gnoni7ics 1992;13:62-9.
97 Yeowell HN, Walker LC, Marshall MK, et al. The mRNAand activity of lysyl hydroxylase are upregulated by theadministration of ascorbate and hydroxlysine to humanskin fibroblasts from a patient with EDS VI. Arch BiochCntBiophvs 1995;321:510-16.
98 Ha VT, Marshal MK, ElsasLJ, ct al. A patient with Ehlers-Danlos syndrome type VI is a compound heterozygote formutations in the LOH gene. 7Cli'; Ittvest 1993;93:1716-2 1.
99 Hautala T, HeikkinenJ, Kivirikko KI,et al. A large duplica-tion in the gene for lysyl hydroxylase accounts for the typeVI variant of Ehlers-Danlos syndrome in two siblings.Getiontics 1993;15:399-405.
100 HylandJ, Ala-Kokko L, Royce P,etal. A homozygous stopcodon in the lysyl hydroxylase gene in two siblings withEhlers-Danlos syndrome type VI. Nat GCet 1992;2:228-31.
101 Pousi B, Hautala T, Hakkinen J,et al. Alu-Alu recombina-tion results in a duplication of seven exons in the lysylhydroxylase gene in a patient with the type VI variant ofEhlers-Danlos syndrome. Attt .7 Htot Geiet 1994;55:899-906.
102 Heikkinen J, Hautala T,Kivirikko KI,et al. Structure andexpression of the humanlysyl hydroxylase gene (PLOD):introns 9 and 16 contain Alu sequences at the sites ofrecombination in EDS VI patients. Gettttttics 1994;24:464-71.
103 Steinmann B, Eyre DR, Shao P. Urinarv pyridinolinecross-links in Ehlers-Danlos syndrome tvpe VI. At.7Y HtottGetlet 1995;57:1505-8.
104 Pasquali M, Dembure PP, Still MT,et al. Urinary pyridin-ium cross-links: a non invasive diagnostic test forEhlers-Danlos syndrome type VI. N Engl _7 Mcd 1994;331:132-3.
105 Siegel R, Black CM, BaileyAJ. Cross-linking of collagen inthe X-linked Ehlers-Danlos syndrometype V. BiochCtBio-phys Res Contnimn 1979;88:281-7.
106 Di Ferrante N, Leachman RD, Angelini P,ct al.Ehlers-Danlos type V (X-linked form) alysyl oxidase defi-ciency.Cowtitect TisstieRes 1975;3:49-53.
107 Kessler E, Takahara K, Biniaminov L,ct al. Bone morpho-genetic protein 1: thetype I procollagen C-proteinase. Sci-cenc 1996;271:360-2.
108 Reddi AH. BMP I: resurrection as procollagen C protein-ase. Sciceitce(Perspectizes) 1996;271:463.
109 Pope FM, Smith R. A coloIII atlas ofittlheritedcottttectivetis-site disorders. New York: Mosby-Wolfe, 1996.
110 StewartRE, Hollister DW, Rimoin DL. A new variant ofEhlers-Danlos syndrome: an autosomal dominant disorderof fragile skin, abnormal scarring and generalisedperi-odontitis.Birth Dcfccs 1977;XIII(3b):85-93.
111 Dyne1KM, Vitellaro-Zuccarello L, Bacchella L,et a!.Ehlers-Danlos syndrome type VIII: biochemical, stere-ological and immunocytochemical studies on dermis froma child with clinical signs of Ehlers-Danlos syndrome and afamily history of premature loss of permanent teeth. Br_7Dcrntatol 1993;128:458-63.
112 Hartsfield JK Jr, Kousseff BG. Phenotypic overlap ofEhlers-Danlos syndrome types IV and VIII. Anti 7 McdGcitct1990;37:465-70.
113Lapiere CM, Nusgens BV. Ehlers-Danlos syndrome (ED)type VIII skin has a reduced proportion of collagen III..7Invcst Dcrniatol 1981 ;76:422A.
114 Nelson DL, King RA. Ehlers-Danlos syndrome type VIII.Y7Ant Acad Dcrntatol 198 1;5:297-303.
115 Lever WF. Histopathologv of titeskiin. 4th ed. London:Pitman, 1967.
116 Arneson MA, Hammerschmidt DE, Furcht LT, et a!. Anew form of Ehlers-Danlos syndrome. _7 Anti Mcd Assoc1 980;244:144-7.
117 Anstey A, Mayne K, Winter M,et a!. Platelet and coagula-tion studies in Ehlers-Danlos syndrome. Br 7 Dcrtiatot!1 992;125:1555-63.
118 Pope FM, Nicholls AC, Palan A, ct a!. Clinical features ofan affected father and daughter with Ehlers-Danlossyndrome type VII B. Rr_7Dcrniatol 1992;126:77-82.
410
on 5 October 2018 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.5.400 on 1 May 1997. D
ownloaded from