
EFIM Summer School 2015 - esim2015summer.org · EFIM Summer School 2015. SCD as emerging problem of...
51
Acute Sickle Cell Crisis M. Domenica Cappellini Fondazione “Ca Granda” Policlinico Università di Milano Muravera 8-12 june 2015 EFIM Summer School 2015
Transcript of EFIM Summer School 2015 - esim2015summer.org · EFIM Summer School 2015. SCD as emerging problem of...

Acute Sickle Cell Crisis
M. Domenica CappelliniFondazione “Ca Granda” Policlinico
Università di Milano
Muravera8-12 june 2015
EFIM Summer School 2015

SCD as emerging problem of public health in non endemic areas
Weatherall DJ et al. Bulletin WHO 79: 704, 2001; Modell B et al Bulletin WHO 86: 480, 2008


Sickle cell mutation Falciparum malaria
Eaton JW, et al., eds. Sickle cell disease: basic principles andclinical practice. New York: Raven Press Ltd. 1994.
Selection of the sickle cell traitHbS mutation protects against
Plasmodium falciparum infections
HbS = sickle cell haemoglobin.

SCD is now a global diseaseSCD is now a global disease

Worldwide Status of Hemoglobin disorders
• 270 million carriers of Hb disorders:80000 of Thalassaemia, most of Sickle Cell Disease.
• 300000 affected births per year total.• 60-70000 births of Thalassaemics: most
of these die in early life, often with no diagnosis and no or inadequate treatment.
• About 200000 new cases of SCD per year.
Agastiniotis M. WHO Report 2004

Hemoglobinopathies are Emerging Problem of Public Health based on YLD and DALYs (1999-2010; 2010-2055)
YLDs: years lived with disability for hemoglobinopathies (β-thal and SCD): 10.197 vs 21.342 cardiovascular disorders
DALYs: disability adjusted life years for hemoglobinopathies (β-thal and SCD): 15.640 vs 75.000 diabetes Murray CJ et al Lancet 380: 2197, 2012; Kassebaum NJ Blood 123: 615, 2014

50 million heterozygous HbSindividuals in the world
• Africa– 10–40% HbS mutation carriers in the population – 200,000–300,000 SCD newborns/year
• USA– 1 SCD newborn/600 births in Afro-American population – 60,000–70,000 SCD patients
• France– 405 SCD newborns in 2007 – 10,000 SCD patients
de Montalembert M. Br Med J. 2008;337:a1397.

Case 1• Female, 34 yrs, Nurse, from Sicily leaving in Milan • Admitted at ER on 19/4/2011• Since 3 days she complained left back pain
unresponsive to pain killer. • Since 2 days fever, cough, worsening dyspnea.• Past History: diagnosis of Sickle/thal in childood. She
had pregnacy at 32yrs (cesarean delivery). Bladder stones
• She uses NSAIDs whenever she has pain, She was occasionally transfused in the past, she was admitted to hospital in several occasions because of back pain

Physical Examination
• She was well oriented, suffering, with shortness of breath (dyspnea)
• pale, without cyanosis• BP 140/90, HR110 r, RR 28-30/min,
O2sat. 94% , T 36.8°C• Heart sounds normal but frequent• Reduced left chest expansion• Vescicular breath sounds reduced at lower
left fields

Lab tests
• WBC 11.9;GR 3.87, Hb 8.7g/dl , Ht 27%, MCV 70fl, MCH 22.5, MCHC 32.1, Plt 359
• Crea 0.6, Na 139, K 3.6, Alt 15, Bil. tot. 3.0 PT 83% (inr 1.12), PTT 30”, D Dimer 0.44 ( v.n 0.29 microg/ml)
• ECG: tachycardia • Rx thorax


ER therapy
• Oxygen delivery• NSAIDs e.v.• Hydration e.v.• Antibiotics (Macrolide e.v.)

Admission in emergency medicine ward
• 19/4 • Pain and polipnea, fever,
repeated blood cultures• 1 unit of RBC • NSAIDs not efficacious• Transient benefit by
oppioid • Early antigens: negative
• 20/4• Clinical status was
worsening• O2 , 1 unit RBC• Increase of antibiotic
spectrum analgesia, (cefalosporine III gen)
• Increase analgesia • esami, rx thorax, CT
thorax • Admitted to intensive
care room


Admission to Intensive Care• Sedation, intubation, analgesia• Blood transfusion/ antibiotics(+ Bactrim
ev)• Cultures: negative• Fever: 37.4°C• Improvment of xray thorax• extubated 24/4• Back to emergency medicine room


From 26/4 recurrence of pain and fever PCR decreasing, CVC removed (culture neg).
Reintroduction of FANS and oppioid.Respiratory status stable
Treatment: IMIPENEM + TEICOPLANINANo active hemolysis
Pregressive improvment Discharged on 6/5

Case 2
• Female 45 yrs, well educated, english teacher• In childood diagnosis of SCD• Colecistectomy in 1984, twin pregnancy in1986
cesarean delivery• Anemia (9-10g/dl), LDH >1000, Bil. Ind. > 4mg/dl• 3-4 sickling crises/year well controlled with
analgesics and hydration

Caso clinico 2• From 1995 on blood transfusions
(approximately every 3 months to keep HbS< 40%)
• End of june 2006, good general conditions, she transfused and she went on holidays
• 20.8.06: 2 days cough, moderate thorax pain• Fever38.7°• A GP of the area was consulted and he
prescribed oral antibiotics
Caso clinico 2• 21.8.06: fever 39.4. The GP visited the
patient again and found a worsed situation: the pt was well oriented however suffering; poli/dysponoic
• They call the ambulance for transfer in ER• The ambulance arrived after 1 hour• The patient arrived in ER with Acute Chest
syndrome• At 6pm she died

Waiting at Sickle Cell Clinic, KATHGhana

Courtesy of Dr H. Wajcman.
Haemoglobin S [β6 (A3)Glu→Val]
H. Wajcman

De-oxygenate SLOW
Oxygenate FAST

Therefore
• The pathophysiology of SCD is explained – either by a decrease in the time needed for
polymerization• red cell dehydration • HbF%
– or by an increase in the time during which the red cell is in transit in the capillary
HbF% = percent fetal haemoglobin.

PS exposure
HaemolysisNO
Platelet activation
Hypoxia reoxygenationInflammation
Endothelial activationCEC
Overexpression TF
Red celldehydration
CEC = circulating endothellial cells; NO = nitric oxide; PS = phosphatidylserine; TF = tissue factor.
Reproduced from Stuart MJ, Nagel RL. Lancet. 2004;364:1343-60 © 2004, with permission from Elsevier.
Modified by M de Montalembert.
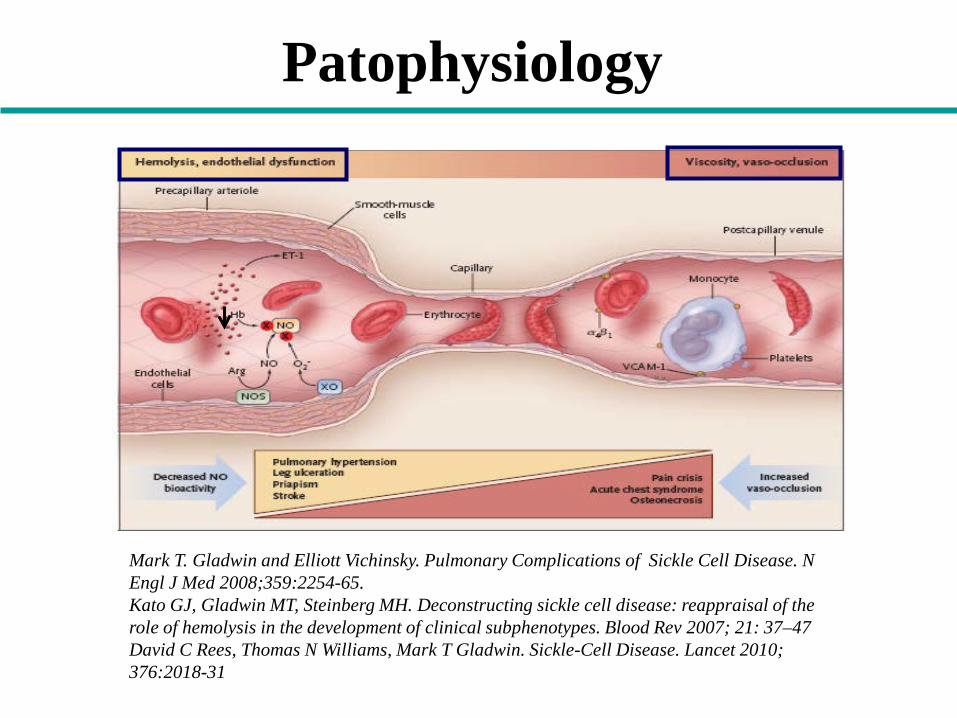
Patophysiology
Mark T. Gladwin and Elliott Vichinsky. Pulmonary Complications of Sickle Cell Disease. N Engl J Med 2008;359:2254-65.Kato GJ, Gladwin MT, Steinberg MH. Deconstructing sickle cell disease: reappraisal of the role of hemolysis in the development of clinical subphenotypes. Blood Rev 2007; 21: 37–47David C Rees, Thomas N Williams, Mark T Gladwin. Sickle-Cell Disease. Lancet 2010; 376:2018-31

Severe formsof SCD
Asymptomatic patients
Intermediate forms
of SCD
Penicillin, folic acid, hydration
Hydroxyurea
Chronic blood transfusion
Bone marrow transplantation
PainACS
Stroke
ACS = acute chest syndrome.
Severity of SCD varies widely among patients

Red blood cellsHbFα-Thalassaemia
EndotheliumNO/ET1
Neutrophils/inflammationAdhesion molecules
Reproduced from Stuart MJ, Nagel RL. Lancet. 2004;364:1343-60 © 2004, with permission from Elsevier.
Modified by M de Montalembert.
Potential modifiers of disease severity
ET1 = endothelin 1.

Clinical manifestations in SCD
CNSInfarctive and hemorrhagic strokesSilent ischemic infarcts ultimately leading to neurological and neurocognitive impairment
Eyes Retinal ischemia, detachments – ‘sickle retinopathy’
CardiovascularAplastic crises lead to severe anemia and cardiac decompensationCardiomyopathy and/or premature coronary artery disease
PulmonaryRecurrent acute chest syndromePulmonary hypertensionChronic sickle lung disease
KidneysInability to concentrate urineProteinuria progressing to nephrotic syndrome and end-stage renal failure
Joints Osteonecrosis (avascular necrosis) of femoral and humeral heads
Legs Chronic ulcers, usually over the medial malleoli

Complications of SCD in children
Castro O, et al. Blood. 1994;84:643-9.Gill FM, et al. Blood. 1995;86:776-83.
Ohene-Frempong K, et al. Blood. 1998;91:288-94.
Polymerization of deoxy-HbS Endothelial dysfunction
Age (years)
Bacteraemia
Pain
ACS
ASS
Stroke
Chronic organ damage ?
1 2 43 65 7 13 14 158 129 10 11
highly variable
ASS = acute splenic sequestration.

Stroke subtype by age
● Ischaemic stroke– 54% of CVAs– highest in 1st decade and
after 30 years– peak at 2–5 years
● Haemorrhagic stroke– during 2nd decade– Risk factors: low Hb, high WBC,
hypertension and steroids use
● Silent stroke– radiological findings consistent
with white-matter disease– 10–30% (not characterized as
age-dependent)– associated with cognitive
deficiencies and higher stroke risk
Verduzco LA, Nathan DG. Blood. 2009;114:5117-25.
Age (years)
Haz
ard
func
tion
0.0010
0.0015
0.0020
0.0025
0.0030
0.0035
0.0040
10 20 30 40 50
Haemorrhagic stroke
Infarctive stroke
CVA = cerebrovascular accident.

DeBaun MR, et al. Blood. 2012;119:4587-96.
Prevalence of silent infarcts60
Prev
alen
ce (%
)
Mean age (years)
0
10
20
30
40
50
0 5 10 15
11.86
27.7 28.2
37.4

Vichinsky E, et al. Pediatrics. 1988;81:749-55.
100
98
96
94
92
90
88
860 10 20 30 40 10
YearsMonths
Surv
ival
(%)
HbSS diagnosed in newborn period
HbSS diagnosed after newborn period
HbSS = haemoglobin SS.
Earlier diagnosis positively impacts survival

Prophylaxis with oral penicillin reduces morbidity and mortality of pneumoccocal
infections
• 125 SCD children aged 3–36 months• Randomly assigned to receive either 125 mg oral
penicillin or placebo
Gaston MH, et al. N Engl J Med. 1986;314:1593-9.
Placebo group
Penicillin group p
Streptococcus pneumoniaeinfections 13 2 0.0025
Death (S. pneumoniae) 3 0 0.003
Incidence of S. pneumoniaesepticaemia 0.09 0.02 < 0.05

Acute Painful Crisis in Sickle Cell Disease
• Acute painful crisis are the most common complication in SCD-> rate of 0.8 episodes per yr.
• Episodes of pain are sometimes trigger by infection, extreme temperatures or by physical, or emotional stress.
• The large part of the acute painful crisis are unprovoked and begin with little warning

Possible Causes of Acute Pain Interesting Bone-Muscle District(s) to be considered
in SCD patients
• Bone infarction
• Aseptic necrosis of bone: ephiphyseal segments of the humari and especially of the femora
• Osteoporosis and vertebral collapse
• Osteomelities
• If pain interests a joint, associated with fever and local signs of arthritis--> consider septic arthritis

Treatmentof complications
● PAIN
● Infections● Acute anaemia: ASS, aplastic crisis● Severe vaso-occlusive events: ACS, strokes, priapism,
organ failure● Pulmonary hypertension● Complications in high-risk pregnancies
Transfusion therapy is a cornerstone for management of SCD complications

ACUTE PAINFUL CRISIS Vaso-occlusion
Patient clinical examination• District identification• Pain pattern: MILD-MODERATE
•Injury•Inflammation•Ischemia•Infarction
Hydrate and
Observe
1st level analgesic therapy
Patient clinical re-examination: pain score at 12-24-48 hrs
Resolution of the acute
painful crisis
UNCHANGED or WORST
PAIN H

PAIN CONTROL STRATEGIES:combined treatments with different
pharmacological targets
• Nonsteroidal anti-inflammatory agents affect pain signal transduction.
• Oppiods influence transmission and modulation of nociception and if used in systemic form can influence pain-perception .
Rees DC. Br J Haematol 120: 744, 2003

PERSISTENT PAINOR SEVERE PAIN
Admission to IM/HematolDepartment
2nd level Analgesic Therapy
Patient clinical examination• District identification• Pain pattern
• CBC (WBC)• X Rays• Bone scan
TransfusionStrategies
pRBCs or TEA
Hydration(i.v.)
at least 2L/d
pRBCs: packed red blood cells; TEA: erythrocytoapheresis
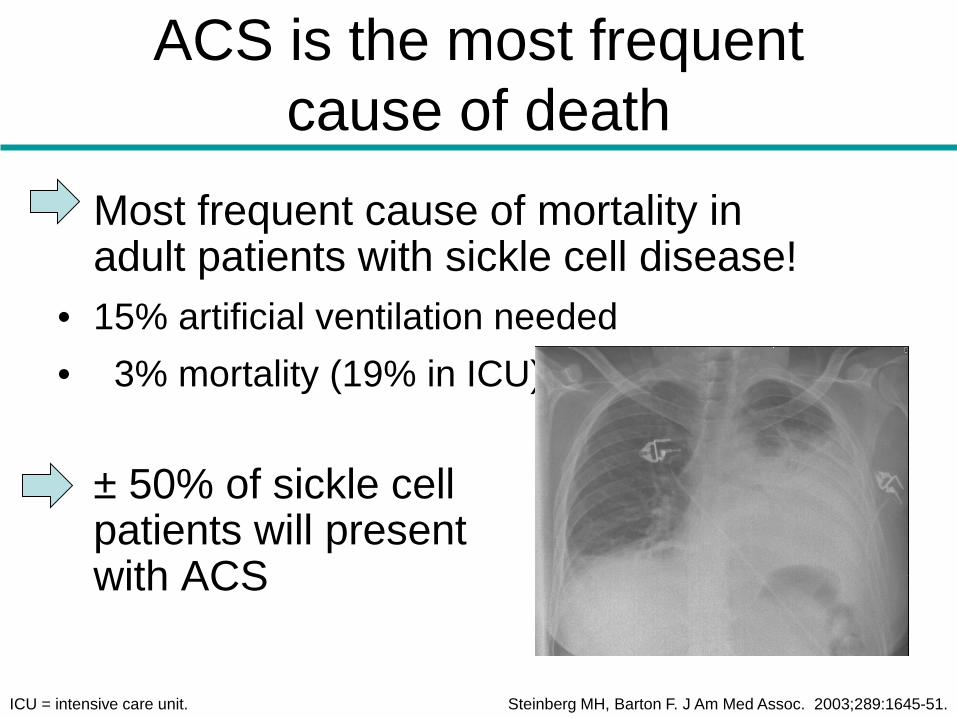
ACS is the most frequent cause of death
Most frequent cause of mortality in adult patients with sickle cell disease!
• 15% artificial ventilation needed• 3% mortality (19% in ICU)
± 50% of sickle cell patients will present with ACS
ICU = intensive care unit. Steinberg MH, Barton F. J Am Med Assoc. 2003;289:1645-51.

Imaging→ Bilateral lower lobes infiltrates more prominent on the right side compatible with ACS
syndrome

Progression of pneumonia in the face of treatment

Acute chest syndrome• A new pulmonary infiltrate involving at least one
complete lung segment not consistent with atelectasis• One or more of
– Chest pain– Fever– Tachypnea, wheezing, cough– Hypoxemia compared with baseline
• Complicates 30% of admissions for painful vaso-occlusive crises
• Most common post operative complication in patients with sickle cell disease

Pathophysiology of ACS in SCD patients
• Causes– infection*– fat embolism– vaso-
occlusion
Rees DC, et al. Lancet. 2010;376:2018-31.RSV = respiratory syncytial virus; Staph. = Staphylococcus; S.pn = Streptococcus pneumoniae.
Vaso-occlusion: increased HbS polymerization
Hypoventilation and atelectasis secondary to rib
and vertebral infarction
ACSPulmonary infection*
Erythrocyte rigidity
Regional hypoxia
Decreased oxygen delivery
Desaturated haemoglobin
Shunting of blood veins to
arteries
VCAM-1
α4β1 integrin
Increased endothelial VCAM-1 expression and adhesion
Increased erythrocyte adhesion in lung-pulmonary infarction
Microvasculature occlusion and bone marrow infarction
Fat embolism
Inflammation: secretory
phospholipase A2
NO
NO
*InfectionChlamydia: 29% Mycoplasma: 20% Staph. aureus: 5%S.pn: 4%Legionella: 2%RSV: 10%

Causes of ACS (1)
• Definite cause was established in 38% of cases– Infection 29%– Pulmonary infarction 16%– Pulmonary fat embolism 9%
• Most common post operative complication• Occurs in 30% of patients hospitalized for
pain– Incentive spirometry effective prevention
ACS clinical course
• Mean length of hospitalization 10.5 days• Patients >20 years of age had a more
severe course than those 20 years of age • Thirteen percent of patients required
mechanical ventilation; 81% recovered • Neurologic events occurred in 11%,
among whom 46% had respiratory failure • One fifth of the patients treated with
bronchodilators had clinical improvement

Causes of death
• Three percent of patients died. The most common causes of death were pulmonary emboli and infectious bronchopneumonia

Management of ACS
• Hydration – Do not over hydrate, use D5 ½ NS– Avoid boluses and overload
• Antibiotics– Third generation cephalosporine: ceftriaxone
or cefotaxime (Clinda for allergic patients)– Macrolide: azythromycin– Consider vancomycin
• Bronchodilators– Asthmatic patients with SCD do poorly

Management of ACS
• Transfusions– Simple transfusions 10 mL/kg packed cells
• Improve oxygenation for hypoxic patients• Anemia• Progression by CXR
– Exchange transfusion for severe patients who have poor response to oxygen
• Pain management• Oxygen


















