EFFICIENCY OF PROSTHETIC TREATMENT WITH … · POST RESECTION PROSTHESES WITH SOLID SUBSTITUTE PART...
4
/ J of IMAB. 2016, vol. 22, issue 3/ http://www.journal-imab-bg.org 1265 EFFICIENCY OF PROSTHETIC TREATMENT WITH POST RESECTION PROSTHESES WITH SOLID SUBSTITUTE PART Ivan Gerdzhikov 1 , Mariana Dimova 2 , Tihomir Georgiev 3 1) Department of Prosthetic dentistry, Faculty of Dental Medicine, Medical University -Sofia, Bulgaria 2) Department of Prosthetic dentistry, Faculty of Dental Medicine, Medical University-Sofia, Bulgaria 3) Department of Oral and Maxillofacial Surgery, Faculty of Dental Medicine, Medical University-Varna, Bulgaria Journal of IMAB - Annual Proceeding (Scientific Papers) 2016, vol. 22, issue 3 Journal of IMAB ISSN: 1312-773X http://www.journal-imab-bg.org ABSTRACT Aim: The aim of this study is to track the effective- ness of prosthetic treatment with post resection dentures with solid substitute part and their role in the restoration of damaged functions. Materials and methods: The study included 14 pa- tients (9 men and 5 women) with different size and loca- tion of defects in the upper jaw treated in the period 2010- 2016 with post resection prostheses with a solid substitute part. The impressions were taken with irreversible hydro- colloid impression material. The prostheses were com- pleted by heat-curing acrylic with low quantity residual monomer. The effectiveness of prosthetics was evaluated by the method of Mihaylov for both oral-nasal examination of the pressure with the device “Oronasopneumotest.” For objectifying and assess the occlusal-articulation ratios was held computerized occlusal analysis with the sys- tem T-SCAN 8. Results: The results showed successful obturation and sealing of defects in all patients. It was found satisfactory recovery of the speaking function and normalization of occlusal-articulation ratios. Conclusion: The prosthetic treatment with post re- section prostheses with a solid substitute part allows suc- cessful recovery of the lost speech and chewing functions, helping to restore self esteem and social rehabilitation of patients. Key words: palatal defects, maxillary resection, ob- turator, post resection prostheses. Damage in the maxillofacial area, occurring after maxillary resection, inflicts serious aesthetical changes, mental problems and functional disabilities in respect of impaired mastication, swallowing, speech and breathing [1, 2]. A common opinion [3, 4, 5, 6] is that the degree of func- tional damage depends on the size and location of the de- fect. This is also confirmed by a research of Usui et al. [7, 8], who discovered lesser functional impairment in patients with smaller defects, a greater number of intact teeth and mouth opening greater than 20mm. Analogous is Devlin et Barker [9] position, who found that the localization of the defect, it’s size, and the condition of the remaining denti- tion are crucial for determining the degree of functional damage and for the prognosis the treatment. Prosthetic methods of treatment are of prime impor- tance in complex treatment and rehabilitation in patients with maxillary resection (10, 11). According to the volume of the maxillofacial area engaged, treatment has its specif- ics, with respect to the degree of disability [12]. Scientific literature describes a multitude of methods and modifications for treatment of patients with maxillary resection [13, 14, 15]. Some of these advocate treatment with closed obturators and others prefer hollow bulb obturators [16, 17]. Whatever the clinical approach, the main point of the treatment is to restore the masticatory function [18, 19]. For its improvement and for heightening of the masticatory function Umino et al. [20] suggest restoring of the occlusal contacts of first and second molars. Through videofluoroscopic analysis Yonthcev et al. [5] visualize the leading role of these molars in the masticatory cycle along with the negligible contribution of incisors and the teeth on the side of the defect. In a similar research before and after prosthetic treatment of patients with single-sided defects Xing et al. [21] found a 59,98% raise in masticatory effec- tiveness one month after the end of treatment. Similar re- sults were obtained by Vergo et Chapman [4], who improve nutrition by distributing the masticatory stress. MATERIALS AND METHODS With the method applied, a prosthetic rehabilitation of 14 patients (9 men and 5 women) with oncologic opera- tions of the maxilla, treated between 2011 and 2016 with closed post resection prostheses was carried out. The pas- sageway defects which occurred, were unilateral and en- gaged only the hard palate and the alveolar crest, with the natural teeth preserved (Fig. 1). http://dx.doi.org/10.5272/jimab.2016223.1265
Transcript of EFFICIENCY OF PROSTHETIC TREATMENT WITH … · POST RESECTION PROSTHESES WITH SOLID SUBSTITUTE PART...

/ J of IMAB. 2016, vol. 22, issue 3/ http://www.journal-imab-bg.org 1265
EFFICIENCY OF PROSTHETIC TREATMENT WITHPOST RESECTION PROSTHESES WITH SOLIDSUBSTITUTE PART
Ivan Gerdzhikov1, Mariana Dimova2, Tihomir Georgiev3
1) Department of Prosthetic dentistry, Faculty of Dental Medicine, MedicalUniversity -Sofia, Bulgaria2) Department of Prosthetic dentistry, Faculty of Dental Medicine, MedicalUniversity-Sofia, Bulgaria3) Department of Oral and Maxillofacial Surgery, Faculty of Dental Medicine,Medical University-Varna, Bulgaria
Journal of IMAB - Annual Proceeding (Scientific Papers) 2016, vol. 22, issue 3Journal of IMABISSN: 1312-773Xhttp://www.journal-imab-bg.org
ABSTRACTAim: The aim of this study is to track the effective-
ness of prosthetic treatment with post resection dentureswith solid substitute part and their role in the restorationof damaged functions.
Materials and methods: The study included 14 pa-tients (9 men and 5 women) with different size and loca-tion of defects in the upper jaw treated in the period 2010-2016 with post resection prostheses with a solid substitutepart.
The impressions were taken with irreversible hydro-colloid impression material. The prostheses were com-pleted by heat-curing acrylic with low quantity residualmonomer.
The effectiveness of prosthetics was evaluated bythe method of Mihaylov for both oral-nasal examinationof the pressure with the device “Oronasopneumotest.”
For objectifying and assess the occlusal-articulationratios was held computerized occlusal analysis with the sys-tem T-SCAN 8.
Results: The results showed successful obturationand sealing of defects in all patients.
It was found satisfactory recovery of the speakingfunction and normalization of occlusal-articulation ratios.
Conclusion: The prosthetic treatment with post re-section prostheses with a solid substitute part allows suc-cessful recovery of the lost speech and chewing functions,helping to restore self esteem and social rehabilitation ofpatients.
Key words: palatal defects, maxillary resection, ob-turator, post resection prostheses.
Damage in the maxillofacial area, occurring aftermaxillary resection, inflicts serious aesthetical changes,mental problems and functional disabilities in respect ofimpaired mastication, swallowing, speech and breathing [1,2]. A common opinion [3, 4, 5, 6] is that the degree of func-tional damage depends on the size and location of the de-fect. This is also confirmed by a research of Usui et al. [7, 8],
who discovered lesser functional impairment in patientswith smaller defects, a greater number of intact teeth andmouth opening greater than 20mm. Analogous is Devlin etBarker [9] position, who found that the localization of thedefect, it’s size, and the condition of the remaining denti-tion are crucial for determining the degree of functionaldamage and for the prognosis the treatment.
Prosthetic methods of treatment are of prime impor-tance in complex treatment and rehabilitation in patientswith maxillary resection (10, 11). According to the volumeof the maxillofacial area engaged, treatment has its specif-ics, with respect to the degree of disability [12].
Scientific literature describes a multitude of methodsand modifications for treatment of patients with maxillaryresection [13, 14, 15]. Some of these advocate treatmentwith closed obturators and others prefer hollow bulbobturators [16, 17]. Whatever the clinical approach, the mainpoint of the treatment is to restore the masticatory function[18, 19]. For its improvement and for heightening of themasticatory function Umino et al. [20] suggest restoring ofthe occlusal contacts of first and second molars. Throughvideofluoroscopic analysis Yonthcev et al. [5] visualize theleading role of these molars in the masticatory cycle alongwith the negligible contribution of incisors and the teeth onthe side of the defect. In a similar research before and afterprosthetic treatment of patients with single-sided defectsXing et al. [21] found a 59,98% raise in masticatory effec-tiveness one month after the end of treatment. Similar re-sults were obtained by Vergo et Chapman [4], who improvenutrition by distributing the masticatory stress.
MATERIALS AND METHODSWith the method applied, a prosthetic rehabilitation
of 14 patients (9 men and 5 women) with oncologic opera-tions of the maxilla, treated between 2011 and 2016 withclosed post resection prostheses was carried out. The pas-sageway defects which occurred, were unilateral and en-gaged only the hard palate and the alveolar crest, with thenatural teeth preserved (Fig. 1).
http://dx.doi.org/10.5272/jimab.2016223.1265
1266 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 3/
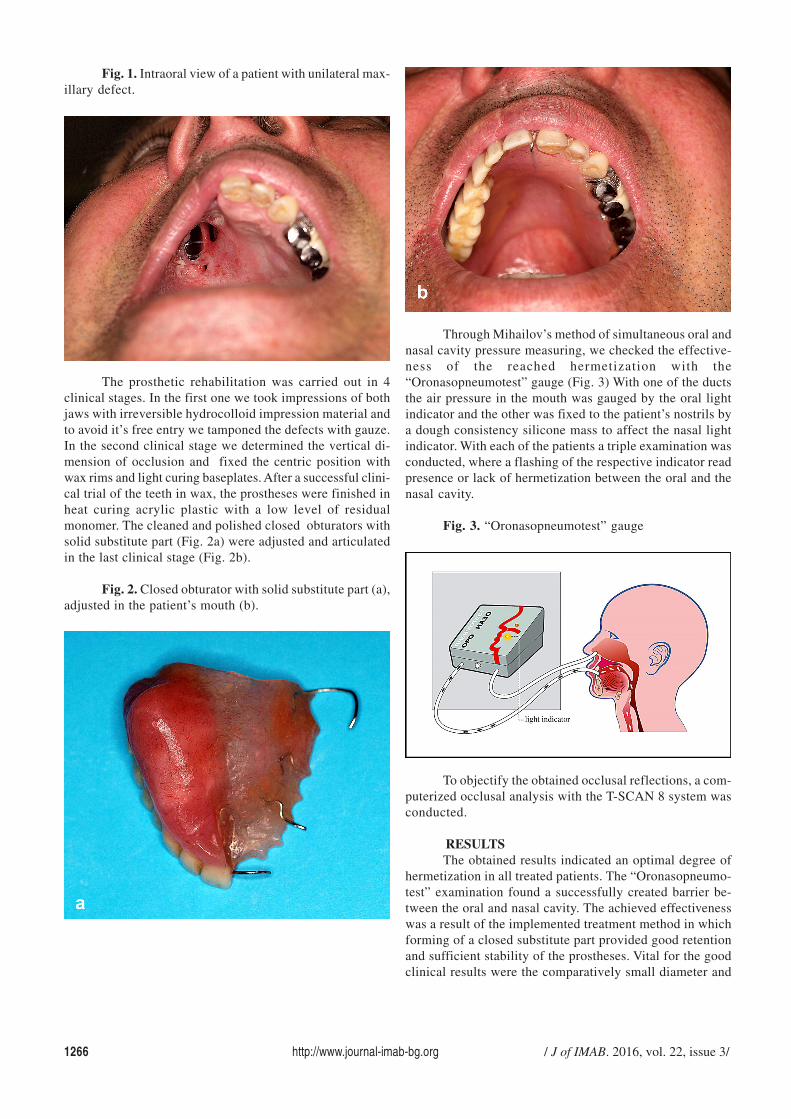
Fig. 1. Intraoral view of a patient with unilateral max-illary defect.
The prosthetic rehabilitation was carried out in 4clinical stages. In the first one we took impressions of bothjaws with irreversible hydrocolloid impression material andto avoid it’s free entry we tamponed the defects with gauze.In the second clinical stage we determined the vertical di-mension of occlusion and fixed the centric position withwax rims and light curing baseplates. After a successful clini-cal trial of the teeth in wax, the prostheses were finished inheat curing acrylic plastic with a low level of residualmonomer. The cleaned and polished closed obturators withsolid substitute part (Fig. 2a) were adjusted and articulatedin the last clinical stage (Fig. 2b).
Fig. 2. Closed obturator with solid substitute part (a),adjusted in the patient’s mouth (b).
Through Mihailov’s method of simultaneous oral andnasal cavity pressure measuring, we checked the effective-ness of the reached hermetization with the“Oronasopneumotest” gauge (Fig. 3) With one of the ductsthe air pressure in the mouth was gauged by the oral lightindicator and the other was fixed to the patient’s nostrils bya dough consistency silicone mass to affect the nasal lightindicator. With each of the patients a triple examination wasconducted, where a flashing of the respective indicator readpresence or lack of hermetization between the oral and thenasal cavity.
Fig. 3. “Oronasopneumotest” gauge
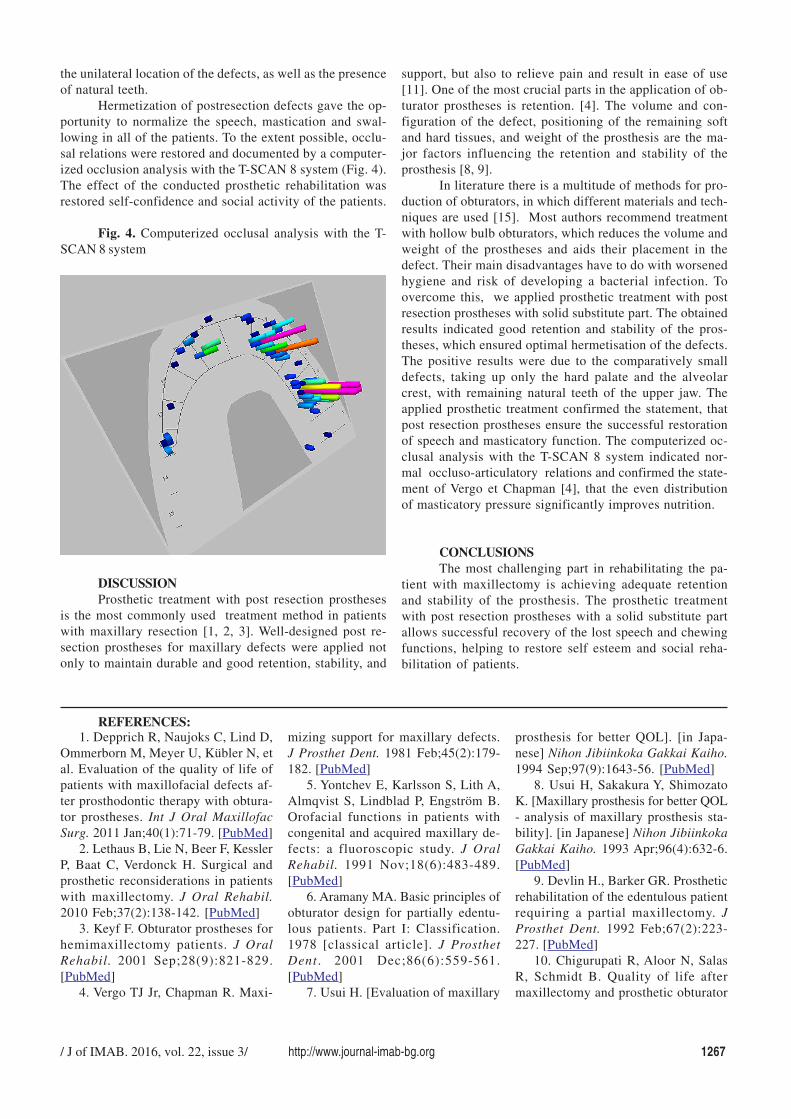
To objectify the obtained occlusal reflections, a com-puterized occlusal analysis with the T-SCAN 8 system wasconducted.
RESULTSThe obtained results indicated an optimal degree of
hermetization in all treated patients. The “Oronasopneumo-test” examination found a successfully created barrier be-tween the oral and nasal cavity. The achieved effectivenesswas a result of the implemented treatment method in whichforming of a closed substitute part provided good retentionand sufficient stability of the prostheses. Vital for the goodclinical results were the comparatively small diameter and
/ J of IMAB. 2016, vol. 22, issue 3/ http://www.journal-imab-bg.org 1267
the unilateral location of the defects, as well as the presenceof natural teeth.
Hermetization of postresection defects gave the op-portunity to normalize the speech, mastication and swal-lowing in all of the patients. To the extent possible, occlu-sal relations were restored and documented by a computer-ized occlusion analysis with the T-SCAN 8 system (Fig. 4).The effect of the conducted prosthetic rehabilitation wasrestored self-confidence and social activity of the patients.
Fig. 4. Computerized occlusal analysis with the T-SCAN 8 system
support, but also to relieve pain and result in ease of use[11]. One of the most crucial parts in the application of ob-turator prostheses is retention. [4]. The volume and con-figuration of the defect, positioning of the remaining softand hard tissues, and weight of the prosthesis are the ma-jor factors influencing the retention and stability of theprosthesis [8, 9].
In literature there is a multitude of methods for pro-duction of obturators, in which different materials and tech-niques are used [15]. Most authors recommend treatmentwith hollow bulb obturators, which reduces the volume andweight of the prostheses and aids their placement in thedefect. Their main disadvantages have to do with worsenedhygiene and risk of developing a bacterial infection. Toovercome this, we applied prosthetic treatment with postresection prostheses with solid substitute part. The obtainedresults indicated good retention and stability of the pros-theses, which ensured optimal hermetisation of the defects.The positive results were due to the comparatively smalldefects, taking up only the hard palate and the alveolarcrest, with remaining natural teeth of the upper jaw. Theapplied prosthetic treatment confirmed the statement, thatpost resection prostheses ensure the successful restorationof speech and masticatory function. The computerized oc-clusal analysis with the T-SCAN 8 system indicated nor-mal occluso-articulatory relations and confirmed the state-ment of Vergo et Chapman [4], that the even distributionof masticatory pressure significantly improves nutrition.
CONCLUSIONSThe most challenging part in rehabilitating the pa-
tient with maxillectomy is achieving adequate retentionand stability of the prosthesis. The prosthetic treatmentwith post resection prostheses with a solid substitute partallows successful recovery of the lost speech and chewingfunctions, helping to restore self esteem and social reha-bilitation of patients.
DISCUSSIONProsthetic treatment with post resection prostheses
is the most commonly used treatment method in patientswith maxillary resection [1, 2, 3]. Well-designed post re-section prostheses for maxillary defects were applied notonly to maintain durable and good retention, stability, and
REFERENCES:1. Depprich R, Naujoks C, Lind D,
Ommerborn M, Meyer U, Kübler N, etal. Evaluation of the quality of life ofpatients with maxillofacial defects af-ter prosthodontic therapy with obtura-tor prostheses. Int J Oral MaxillofacSurg. 2011 Jan;40(1):71-79. [PubMed]
2. Lethaus B, Lie N, Beer F, KesslerP, Baat C, Verdonck H. Surgical andprosthetic reconsiderations in patientswith maxillectomy. J Oral Rehabil.2010 Feb;37(2):138-142. [PubMed]
3. Keyf F. Obturator prostheses forhemimaxillectomy patients. J OralRehabil. 2001 Sep;28(9):821-829.[PubMed]
4. Vergo TJ Jr, Chapman R. Maxi-
mizing support for maxillary defects.J Prosthet Dent. 1981 Feb;45(2):179-182. [PubMed]
5. Yontchev E, Karlsson S, Lith A,Almqvist S, Lindblad P, Engström B.Orofacial functions in patients withcongenital and acquired maxillary de-fects: a fluoroscopic study. J OralRehabil. 1991 Nov;18(6):483-489.[PubMed]
6. Aramany MA. Basic principles ofobturator design for partially edentu-lous patients. Part I: Classification.1978 [classical article]. J ProsthetDent . 2001 Dec;86(6):559-561.[PubMed]
7. Usui H. [Evaluation of maxillary
prosthesis for better QOL]. [in Japa-nese] Nihon Jibiinkoka Gakkai Kaiho.1994 Sep;97(9):1643-56. [PubMed]
8. Usui H, Sakakura Y, ShimozatoK. [Maxillary prosthesis for better QOL- analysis of maxillary prosthesis sta-bility]. [in Japanese] Nihon JibiinkokaGakkai Kaiho. 1993 Apr;96(4):632-6.[PubMed]
9. Devlin H., Barker GR. Prostheticrehabilitation of the edentulous patientrequiring a partial maxillectomy. JProsthet Dent. 1992 Feb;67(2):223-227. [PubMed]
10. Chigurupati R, Aloor N, SalasR, Schmidt B. Quality of life aftermaxillectomy and prosthetic obturator

1268 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 3/
15. Ariani N, Visser A, van Oort RP,Kusdhany L, Rahardjo TB, Krom BP,et al. Current state of craniofacial pros-thetic rehabilitation. Int J Prostho-dont. 2013 Jan-Feb;26(1):57- 67.[PubMed]
16. Cotert HS, Cura C, KeserciogluA. Modified flasking technique forprocessing a maxillary resection obtu-rator with continuous pressure injec-tion. J Prosthet Dent. 2001 Oct;86(4):438-440. [PubMed]
17. Elangovan S, Loibi E. Two-piece hollow bulb obturator. Indian JDent Res. 2011 May-Jun;22(3):486-488. [PubMed]
18. El Fattah H, Zaghloul A,Pedemonte E, Escuin T. Pre-prostheticsurgical alterations in maxillectomy toenhance the prosthetic prognoses aspart of rehabilitation of oral cancer pa-
rehabilitation. J Oral Maxillofac Surg.2013 Aug;71(8):1471-1478. [PubMed]
11. Chen C, Ren W, Gao L, ChengZ, Zhang L, Li S, et al. Function of ob-turator prosthesis after maxillectomyand prosthetic obturator rehabilitation.Braz J Otorhinolaryngol. 2016 Mar-Apr;82(2):177-183. [PubMed]
12. Borlase G. Use of obturators inrehabilitation of maxillectomy defects.Ann R Australas Coll Dent Surg. 2000Oct;15:75-79. [PubMed]
13. Anandakrishna GN, SivaranjaniG. Management of VelopharyngealDisorders. A Case Series. J Prostho-dont. 2010 Jul;19(5):397-402.[PubMed]
14. Patil PG. New technique to fab-ricate an immediate surgical obturatorrestoring the defect in original ana-tomical form. J Prosthodont. 2011Aug;20(6):494-498. [PubMed]
tient. Med Oral Patol Oral Cir Bucal.2012 Mar;17(2):262-70. [PubMed]
19. Kreeft AM, Krap M, WismeijerD, Speksnijder CM, Smeele LE, BoschSD, et al. Oral function after maxille-ctomy and reconstruction with an ob-turator. Int J Oral Maxillofac Surg.2012 Nov;41(11):1387-1392.[PubMed]
20. Umino S, Masuda G, Fujita K.Masticatory performance with a pros-thesis following maxillectomy: ananalysis of 43 cases. J Oral Rehabil.2003 Jun;30(6):642-645. [PubMed]
21. Xing GF, Jiao T, Sun J, JiangYL. [The analysis of masticatory effi-ciency after maxillofacial prosthetictreatment for unilateral maxillary de-fect]. [in Chinese] Shanghai KouQiang Yi Xue. 2003 Dec;12(6):422-423. [PubMed].
Address for correspondence:Dr. Ivan GerdzhikovDepartment of Prosthetic dentistry, Faculty of Dental Medicine, MedicalUniversity - Sofia1, St. George Sofiyski blvd., 1431 Sofia, Bulgaria.E-mail: [email protected]
Please cite this article as: Gerdzhikov I, Dimova M, Georgiev T. Efficiency of prosthetic treatment with post resectionprostheses with solid substitute part. J of IMAB. 2016 Jul-Sep;22(3):1265-1268.DOI: http://dx.doi.org/10.5272/jimab.2016223.1265
Received: 21/05/2016; Published online: 12/08/2016