
Efficacy of Sensory and Motor Interventions for Children with Autism
27
lish language for the past 30 years with a focus on the past 10 years. Also, manual searches of key references from articles were completed. In a few noted cases, studies of individuals with related disorders (e.g., men- tal retardation), or slightly older children (over 8 years) were included provided the results had implications for young children with autism. LITERATURE REVIEW OF SENSORY AND MOTOR DEVELOPMENT Empirical studies about sensory and motor devel- opment in children with autism are limited compared to studies of other aspects of development. Those that exist often suffer from a variety of methodological limitations; however, these studies provide both a foundation of sci- entific knowledge critical for understanding the early development of children with autism and guidance for intervention planning. Empirical evidence converges to confirm the existence of sensory and motor difficulties for many children with autism at some point in their early development (Adrien et al., 1987; 1992; 1993; Baranek, 1999; Dahlgren & Gilberg, 1989; Hoshino et al., 1982; Ohta, Nagai, Hara, & Sasaki, 1987; Ornitz, Guthrie, & Farley, 1977; Scharre & Creedon, 1992), although much PURPOSE, SEARCH PROCEDURES, AND SCOPE The purpose of this paper is threefold: (1) briefly summarize the empirical literature with respect to sen- sory and motor development/abnormalities in children with autism, (2) evaluate the scientific basis of sensory and motor interventions used with children with autism, and (3) describe implications of these findings for edu- cation and further research. Subject headings and key- words were searched for terms related to sensory and motor deficits (e.g., arousal, sensory reactivity/pro- cessing, habituation, posture, praxis, gross/fine/oral motor development, etc.), and categorical terms spe- cific to sensory and motor interventions (e.g., sensory integration, prism lenses, etc.). Searches were con- ducted using MEDLINE, CINAHL, & PSYCINFO data- bases to find empirical studies specific to children with autism spectrum disorders (i.e., autistic disorder, per- vasive developmental disorder) available in the Eng- Efficacy of Sensory and Motor Interventions for Children with Autism Grace T. Baranek 1 Idiosyncratic responses to sensory stimuli and unusual motor patterns have been reported clin- ically in young children with autism. The etiology of these behavioral features is the subject of much speculation. Myriad sensory- and motor-based interventions have evolved for use with children with autism to address such issues; however, much controversy exists about the efficacy of such therapies. This review paper summarizes the sensory and motor difficulties often manifested in autism, and evaluates the scientific basis of various sensory and motor interventions used with this population. Implications for education and further research are described. KEY WORDS: Sensorimotor therapies; evidence-based treatments; sensory integration. Journal of Autism and Developmental Disorders, Vol. 32, No. 5, October 2002 (© 2002) 397 0162-3257/02/1000-0397/0 © 2002 Plenum Publishing Corporation 1 The Clinical Center for the Study of Development and Learning, Room 111 Medical School Wing E—CB # 7120 University of North Carolina at Chapel Hill, Chapel Hill, NC 27599-7120; e-mail: [email protected]
Transcript of Efficacy of Sensory and Motor Interventions for Children with Autism

lish language for the past 30 years with a focus on thepast 10 years. Also, manual searches of key referencesfrom articles were completed. In a few noted cases,studies of individuals with related disorders (e.g., men-tal retardation), or slightly older children (over 8 years)were included provided the results had implications foryoung children with autism.
LITERATURE REVIEW OF SENSORY ANDMOTOR DEVELOPMENT
Empirical studies about sensory and motor devel-opment in children with autism are limited compared tostudies of other aspects of development. Those that existoften suffer from a variety of methodological limitations;however, these studies provide both a foundation of sci-entific knowledge critical for understanding the earlydevelopment of children with autism and guidance forintervention planning. Empirical evidence converges toconfirm the existence of sensory and motor difficultiesfor many children with autism at some point in their earlydevelopment (Adrien et al.,1987; 1992; 1993; Baranek,1999; Dahlgren & Gilberg, 1989; Hoshino et al.,1982;Ohta, Nagai, Hara, & Sasaki, 1987; Ornitz, Guthrie, &Farley, 1977; Scharre & Creedon, 1992), although much
PURPOSE, SEARCH PROCEDURES, ANDSCOPE
The purpose of this paper is threefold: (1) brieflysummarize the empirical literature with respect to sen-sory and motor development/abnormalities in childrenwith autism, (2) evaluate the scientific basis of sensoryand motor interventions used with children with autism,and (3) describe implications of these findings for edu-cation and further research. Subject headings and key-words were searched for terms related to sensory andmotor deficits (e.g., arousal, sensory reactivity/pro-cessing, habituation, posture, praxis, gross/fine/oralmotor development, etc.), and categorical terms spe-cific to sensory and motor interventions (e.g., sensoryintegration, prism lenses, etc.). Searches were con-ducted using MEDLINE, CINAHL, & PSYCINFO data-bases to find empirical studies specific to children withautism spectrum disorders (i.e., autistic disorder, per-vasive developmental disorder) available in the Eng-
Efficacy of Sensory and Motor Interventions for Children with Autism
Grace T. Baranek1
Idiosyncratic responses to sensory stimuli and unusual motor patterns have been reported clin-ically in young children with autism. The etiology of these behavioral features is the subjectof much speculation. Myriad sensory- and motor-based interventions have evolved for usewith children with autism to address such issues; however, much controversy exists about theefficacy of such therapies. This review paper summarizes the sensory and motor difficultiesoften manifested in autism, and evaluates the scientific basis of various sensory and motorinterventions used with this population. Implications for education and further research aredescribed.
KEY WORDS: Sensorimotor therapies; evidence-based treatments; sensory integration.
Journal of Autism and Developmental Disorders, Vol. 32, No. 5, October 2002 (© 2002)
3970162-3257/02/1000-0397/0 © 2002 Plenum Publishing Corporation
1 The Clinical Center for the Study of Development and Learning,Room 111 Medical School Wing E—CB # 7120 University of NorthCarolina at Chapel Hill, Chapel Hill, NC 27599-7120; e-mail:[email protected]

variability is present in specific symptoms or patternsexpressed. These types of behaviors appear neither uni-versal nor specific to the disorder of autism; however,qualitative aspects of these patterns have not been wellstudied, and prospective, longitudinal investigations thatsystematically document developmental trajectories frominfancy through childhood are yet to be accomplished.The majority of evidence stems from parental reports,which themselves are prone to some biases and method-ological weaknesses. Empirical data from retrospectivevideo studies (Adrien et al., 1992; Baranek, 1999) andclinical evaluations (Gillberg et al.,1990) are emergingto suggest that patterns of sensory and motor featuresin autism may differ qualitatively from those in other de-velopmental disorders. Furthermore, unusual sensory-perceptual features appear to be manifest quite early inthe development of children with autism (i.e., by 9 to12 months of age). Though not well understood, sensoryprocessing and motor patterns may be related to core fea-tures, development of other aberrant behaviors, and laterprognosis; thus these patterns have implications for earlydiagnosis and intervention.
Unusual sensory responses (e.g., hypo- and hyper-responses; preoccupations with sensory features of ob-jects, perceptual distortions; paradoxical responses tosensory stimuli) have been reported in 42 to 88% ofolder children with autism in various studies (Kientz &Dunn, 1997; LeCouteur et al.,1989; Ornitz et al.,1977;Volkmar, Cohen, & Paul, 1986), indicating that theseare common concerns in this population. Percentagesvary depending on how specifically items were sam-pled. Auditory processing problems are particularlynoted, with one study (Greenspan & Weider, 1997) pur-porting that 100% of subjects demonstrated these dif-ficulties. Visual spatial skills are often more advancedthan other areas of development, although individualdifferences are noted. Sensory processing abilities alsoappear to be uneven and of a fluctuating nature inautism, such that both hyper- and hypo-responses areevident in the same child. These aberrant sensory re-actions are thought to reflect poor sensory integrationand/or arousal modulation in the central nervous sys-tem, although the underlying nature of these symptomsremains speculative (e.g., neurological structures andsystems involving the cerebellum, limbic system, cor-tical mechanisms, etc). Both patterns of under- andover-arousal have been reported (Hutt, Hutt, Lee, &Ounsted, 1964; James & Barry, 1984; Kinsbourne,1987; Kootz & Cohen, 1981; Kootz, Marinelli, &Cohen, 1982; Rimland, 1964; Zentall & Zentall, 1983).Children with autism tend to show these abnormal sen-sory responses to both social and nonsocial stimuli and
398 Baranek
in the absence of known peripheral dysfunction (e.g.,hearing acuity, visual defect) per se.Thus some re-searchers have suggested shifting toward the investi-gation of more complex levels of informationprocessing including attentional control mechanismsand executive functions to help explain some of theseunusual sensory features or motor deficits (e.g., Lin-coln et al.,1995; Minshew, Goldstein, & Seigel, 1997;Wainwright & Bryson, 1996). Given that many con-ventional educational environments are sensorily com-plicated and unpredictable, interventions likely need toconsider the individualized sensory processing needsof children demonstrating such difficulties to optimizesuccessful participation in such programs.
With respect to developmental milestones, uneven-ness between domains is often reported, indicating a rel-ative sparing of general motor skills compared tolanguage or social skills in children with autism (Klin,Volkmar, & Sparrow, 1992; Stone et al., 1999). How-ever, not all children with autism demonstrate prowessin motor skills and considerable variability exists (Amato& Slavin, 1998; DeMyer et al., 1972; Jones & Prior,1985; Johnson, Siddons, Frith, & Morton, 1992; Ohtaet al.,1987; Ornitz et al.,1977; Rapin, 1997; Rinehart,Bradshaw, Brereton, & Tonge, 2001). Many demonstrateatypical features (e.g., low muscle tone, oral-motor prob-lems, repetitive motor movements, dyspraxia) or test inthe delayed ranges on standardized motor assessmentsparticularly as the complexity of tasks increases.Whether or not these difficulties are purely motoric isunclear, because other areas also affect test-taking abil-ities. Furthermore, delayed motor development is nota unique characteristic of children with autism, becauseit is often associated with the level of mental retarda-tion in general. However, because more than 75% ofchildren with autism have concomitant mental retarda-tion, the presence of motoric concerns, regardless ofwhether they are primary or secondary to autism, stillhas substantial implications for individualized educa-tional interventions. Developmental motor delays, al-though only minimally different during infancy, maybecome magnified with progressive age (e.g., Ohtaet al.,1987). Especially during early foundational years,motor skills provide a means for learning importantskills in other domains (e.g., social skills, academics)and thus motor-related difficulties may need to be ad-dressed in the educational curricula or through relatedtherapy services. At least one study (Perez & Sevilla,1993) demonstrates a predictive relationship betweenmotor skills in children with autism to functional out-comes in other domains such as vocational and leisureskills 5 years later.

Motor planning deficits are an area of particular in-terest, given that several studies point out that bothyounger and older children with autism may demonstratedifficulties with aspects of praxis (Adams, 1998; Jones& Prior, 1985; Rinehart et al.,2001; Rogers et al.,1996;Smith & Bryson, 1998; Stone et al.,1990). These diffi-culties are certainly exaggerated in tasks that require ex-ecution of a social imitation, either motor or objectrelated, but may also be present in nonimitated simplegoal-directed motor tasks (e.g., reaching, grasping, andplacing) (Hughes & Russell, 1993). Motor planningdeficits are sometimes mistaken for general clumsiness;however, Rinehart et al. (2001) separated out two com-ponents of action and found that highly functioning chil-dren with autism spectrum disorders, ages 5 to 19 years,had intact movement executionbut atypical movementpreparationduring a simple motor reprogramming taskcompared with typical, IQ-matched controls. Specifi-cally, children with autistic disorder were characterizedby a lack of anticipation during movement preparationphases, findings suggestive of difficulties in motivationalaspects of behavior or attention for action. Children withAsperger’s disorder showed slower preparations formovement at phases in which movement should beoptimal—implicating additional dysfunction in thefrontal-striatal system, according to the authors.
Although it is possible that the formulation of motorplans is deficient, it is also possible that simple motorplanning is intact but that the use of externally guided vi-sual feedback is diminished, affecting the quality of motorperformance, postural stability, and the lack of effectivesequencing of actions (Masterton & Biederman, 1983;Gepner, Mestre, Masson, & de Schonen, 1995; Smith &Bryson, 1998; Stone et al.,1990; Kohen-Raz, Volkmar,& Cohen, 1992). Thus, perceptually challenging tasksthat require smooth integration of visual with vestibular-proprioceptive information, for example, may be partic-ularly difficult to perform and could result in poor qualityof motor performance on complex tasks. These findingstaken together with evidence that motor imitation skillsin young children with autism predict later expressivelanguage skills and play skills (Stone et al.,1997), havesignificant implications for educational interventions andfuture research.
EFFICACY OF SENSORY AND MOTORINTERVENTIONS
Because “interventions for sensory and motordeficits” are not synonymous with “sensory and motorinterventions,” the following inclusion criteria were
Efficacy of Sensory and Motor Interventions for Children with Autism 399
used to define the parameters for the review: (a) re-medial interventions that target specific sensory ormotor components per se,broader performance out-comes that are thought to be the result of the sensory-motor treatment, or both; (b) compensatory skillstraining approaches; and/or (c) task/environmentalmodifications targeted for sensory and motor difficul-ties. A variety of other interventions exist that may beat least partially aimed at improving sensory and motorskills; however, only those interventions that have aprimary basis in sensory processing or motor theorieswere included. Traditional behavioral interventions andpsychopharmacological treatments were excluded.Likewise, comprehensive educational models (e.g.,Greenspan—DIR Model; TEACCH) were excluded,even though these programs frequently include a sen-sory processing or motor development component. Al-though a variety of professionals (e.g., occupationaltherapists, adaptive physical educators, physical ther-apists, speech pathologists, etc.) may utilize varioussensory-motor strategies listed within the context ofany given child’s individualized educational plan, thispaper is not intended to be a critique of the efficacy ofthose related services. Sensory-motor interventions arenot presumed to represent the full scope of therapeutic/educational services offered by specialized profes-sionals. Sensory or motor treatments often are used asan adjunct to a more holistic intervention plan. Forexample, the occupational therapist provides therapeu-tic interventions aimed at improving a child’s occupa-tional performance (e.g., play, school functional skills,self-care) within the educational context. Remediationof sensory or motor deficits (as well as other compo-nents including cognitive or psychosocial functions)may occur if indicated, but only within the larger con-text of occupational performance problems within thelearning environment. Compensatory interventions andenvironmental adaptations are also utilized and oftenpreferred because of the more immediate effects onmeaningful participation.
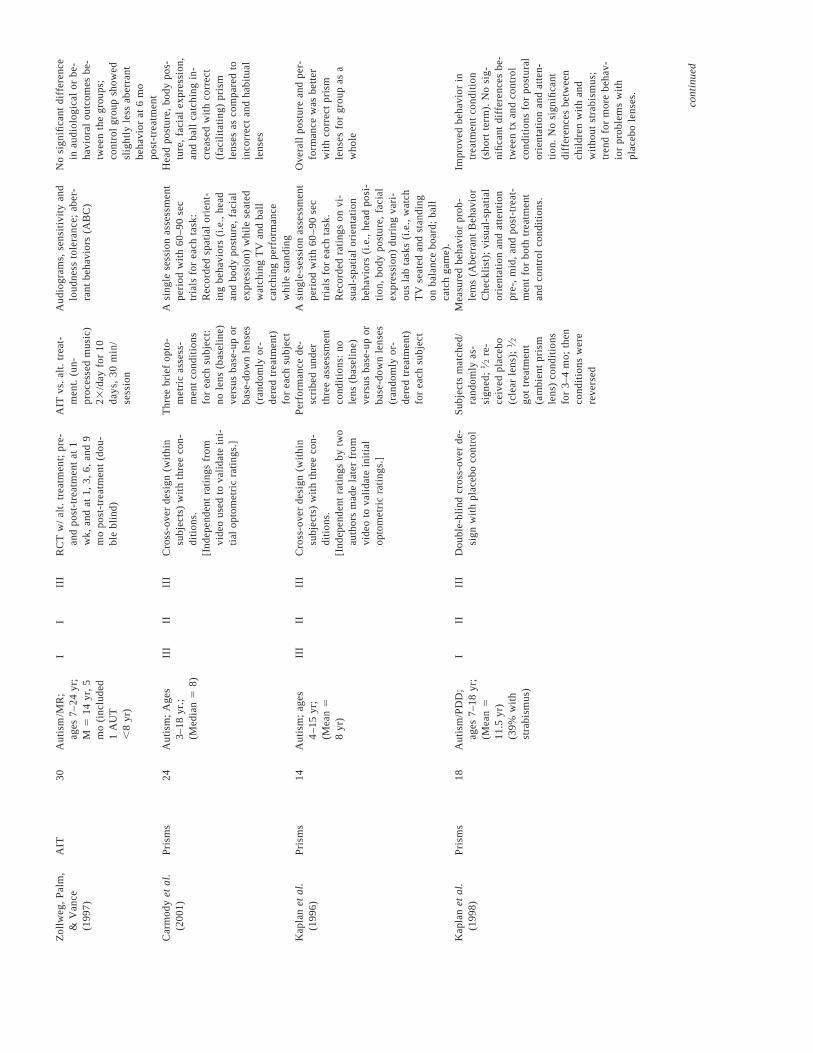
To judge the validity of each category of inter-ventions, first a description of each intervention ap-proach is provided that includes the underlyingassumptions of the intervention, proposed mechanismsthought to be responsible for the therapeutic changespurported, and the service delivery model utilized toprovide the intervention. In addition, the scientific evi-dence (i.e., efficacy research from peer-reviewedsources) of each intervention category is reviewed.Table I provides a comparative summary of the empir-ical studies reviewed for children with autism spectrumdisorders.

Tab
le 1
.S
en
sory
an
d M
oto
r In
terv
en
tion
Stu
die
s
Tre
atm
en
tIn
t.E
xt.
Inte
rve
ntio
n
Ou
tco
me
sS
tud
yca
teg
orya
nS
ub
ject
sva
l.bva
l.cG
end
De
sig
n e
lem
en
tssp
eci
fica
tion
sm
ea
sure
dF
ind
ing
s
Ayr
es
&
Tic
kle
(1
98
0)
Ca
se-S
mith
&
Bry
an
(1
99
9)
Lin
de
rma
n &
S
tew
ard
(1
99
9)
La
rrin
gto
n
(19
87
)
Re
illy
et
al.
(19
83
)
Sta
gn
itti,
Ra
iso
n,
&
Rya
n
(19
99
)
Ed
els
on
et
al.
(19
99
)
SI-
cla
ssic
al
SI-
cla
ssic
al
SI-
cla
ssic
al
SI-
ba
sed
SI-
ba
sed
SI-
ba
sed
(Se
nso
ryD
iet)
SS
-to
uch
p
ress
ure
10
5 2 1 18
1 12
Mild
-se
vere
au
tism
; 3
–1
3 y
r
Au
tism
/MR
; 4
–5
yr
Au
tism
; 3
–4
yr
Au
tism
/se
vere
MR
; 1
5-y
r-o
ld b
oy
Au
tism
6–
11
yr
Se
nso
ry D
efe
n-
sive
ne
ss a
nd
Po
ssib
leA
utis
m s
pe
c-tr
um
; 5
-yr-
old
bo
y
Au
tism
4–
13
yr
III
IV IV IV III
IV I
IV II IV IV I IV I
III
I I III
III
II III
Re
tro
spe
ctiv
e c
ase
-co
ntr
ol
of
tre
atm
en
t re
spo
nd
ers
vers
us
no
nre
spo
nd
ers
Sin
gle
-su
bje
ct A
B d
esi
gn
;3
wk
ba
selin
e,
10
wk
tre
atm
en
t
Sin
gle
-su
bje
ct A
B d
esi
gn
;2
wk
ba
selin
e,
7 o
r 1
1 w
k tr
ea
tme
nt
De
scri
ptiv
e c
ase
stu
dy
Co
un
ter-
ba
lan
ced
alte
rna
ting
tre
atm
en
ts d
esi
gn
; ra
nd
om
ass
ign
me
nt
to a
ctiv
ityo
rde
r
De
scrr
iptiv
e c
ase
stu
dy
RC
T w
ith p
lace
bo
; P
re-
an
dp
ost
-tre
atm
en
t m
ea
sure
s
23w
k fo
r o
ne
ye
ar
30
min
tre
atm
en
tse
ssio
ns
plu
ste
ach
er
con
sulta
-tio
n
1 h
r/w
k in
clin
ic
Va
rie
d s
en
sory
tre
at-
me
nt
(ve
st./
pro
p/
ora
l m
oto
r) t
rea
t-m
en
t in
sch
oo
l a
nd
gro
up
ho
me
; 2
yr
2 s
ess
ion
s 3
0 m
inve
stib
ula
r tr
ea
t-m
en
t ve
rsu
s 2
se
s-si
on
s 3
0m
in fi
ne
mo
tor
tre
atm
en
t(a
ltern
atin
g);
pro
-vi
de
d w
ithin
a 3
wk
Bru
shin
g,
join
t co
m-
pre
ssio
n 3
–53
/da
yfo
r 2
wk
(oth
er
tech
niq
ue
s w
ere
als
o u
sed
); r
e-
pe
ate
d a
ga
in a
t 5
mo
po
st t
rea
tme
nt
Hu
g M
ach
ine
(p
res-
sure
) ve
rsu
sp
lace
bo
(n
o p
res-
sure
) 23
20
-min
sess
ion
s p
er
we
ek;
6 w
k to
tal
La
ng
ua
ge
, a
wa
ren
ess
of
en
-vi
ron
me
nt,
pu
rpo
sefu
l a
c-tiv
itie
s, s
elf-
stim
ula
tion
.,so
cia
l a
nd
em
otio
na
lb
eh
avi
or
Ma
ste
ry p
lay,
en
ga
ge
d b
e-
ha
vio
rs,
pe
er
an
d a
du
ltin
tera
ctio
ns
Fu
nct
ion
al
be
ha
vio
rm
ea
sure
s va
rie
d b
etw
ee
nsu
bje
cts
(e.g
., s
oci
al
inte
ract
ion
s,co
mm
un
ica
tion
)V
ari
ety
of
be
ha
vio
rs (
e.g
.,S
IB,
pla
y sk
ills,
so
cia
lin
tera
ctio
ns)
Qu
an
tity
an
d q
ua
lity
of
voca
liza
tion
s m
ea
sure
dd
uri
ng
tre
atm
en
t o
nly
.(N
o p
re-p
ost
me
asu
res)
.
An
ecd
ota
l re
po
rts
of
tact
ileto
lera
nce
, a
ffe
ct,
act
ivity
leve
l, te
mp
er
tan
tru
ms
at
ho
me
, sc
ho
ol/c
om
mu
nity
Be
ha
vio
ral
(te
nsi
on
, a
nxi
-e
ty,
hyp
era
ctiv
ity)
an
dp
hys
iolo
gic
al
(ga
lva
nic
skin
re
spo
nse
)
Su
bje
cts
with
hyp
er-
resp
on
sivi
ty t
o t
act
ilea
nd
ve
stib
ula
r st
imu
lih
ad
be
tte
r o
utc
om
es
tha
n h
ypo
-re
spo
nsi
vesu
bje
cts
Ge
ne
ral
imp
rove
me
nts
in
ma
ste
ry p
lay,
en
ga
ge
db
eh
avi
ors
, a
nd
ad
ult
inte
ract
ion
s. N
o s
ign
if-ic
an
t ch
an
ge
s in
pe
er
inte
ract
ion
sIn
cre
ase
in
so
cia
l in
ter-
act
ion
s, r
esp
on
se t
om
ove
me
nt
an
d a
ffe
c-tio
n,
an
d a
pp
roa
ch t
on
ew
act
iviti
es
Po
sitiv
e e
ffe
cts
rep
ort
ed
in m
an
y d
om
ain
s o
fb
eh
avi
or
Fin
e m
oto
r a
ctiv
itie
se
licite
d m
ore
va
rie
tyo
f sp
ee
ch a
nd
me
an
len
gth
of
voca
liza
tion
sa
nd
de
cre
ase
d a
utis
ticsp
ee
ch t
ha
n t
he
vest
ibu
lar
tre
atm
en
t
Imp
rove
me
nts
in a
ll a
rea
sfo
llow
ing
tre
atm
en
t;b
en
efit
s fa
de
d b
y5
mo
nth
s p
ost
-tre
at-
me
nt;
6-
an
d 9
-mo
as-
sess
me
nts
(fo
llow
ing
2n
d p
ha
se o
f tr
ea
tme
nt)
sho
we
d s
en
sory
de
fen
-si
ven
ess
cu
red
De
cre
ase
d t
en
sio
n a
nd
an
xie
ty f
or
tre
atm
en
tg
rou
p.
Su
bje
cts
with
initi
ally
hig
he
r a
nxi
ety
leve
l h
ad
be
tte
r o
ut-
com
es

Fie
ld e
ta
l.(1
99
7)
McC
lure
&
Ho
ltz-Y
otz
(1
99
0)
Ra
y e
ta
l.(1
98
8)
Zis
serm
an
(1
99
1)
Be
ttis
on
(1
99
6)
Bro
wn
(1
99
9)
Gill
be
rg e
ta
l.(1
99
7)
Lin
k (1
99
7)
SS
-to
uch
th
era
py
SS
-to
uch
p
ress
ure
SS
-ve
stib
ula
r
SS
-to
uch
p
ress
ure
AIT
(B
era
rd)
AIT
(B
era
rd)
AIT
(B
era
rd)
AIT
(B
era
rd)
22
1 1 1 80
2 9 3
Au
tism
; m
ea
na
ge
4.5
yr
Au
tism
/MR
;1
3-y
r-o
ld b
oy
in p
sych
iatr
icu
nit
Au
tism
; 9
-yr-
old
ma
le
Au
tism
; 8
-yr-
old
fe
ma
le
Au
tism
or
As-
pe
rge
r (s
ou
nd
hyp
ers
en
si-
tivity
), a
ge
s3
–1
7 y
r
Au
tism
; 3
.5 a
nd
5 y
r
Au
tism
(a
llw
ith M
R);
3
–1
6 y
r
Au
tism
; a
ge
s 6
,7
, a
nd
15
yr;
2 n
on
verb
al
I IV IV IV I IV III
IV
I IV IV IV I IV III
IV
III
III
II III
III
III
IV III
RC
T w
ith a
ltern
ativ
e t
rea
t-m
en
t; P
re-
an
d p
ost
-tre
at-
me
nt
me
asu
res
De
scri
ptiv
e c
ase
re
po
rt
De
scri
ptiv
e c
ase
re
po
rt;
Pre
-, m
id-,
an
d p
ost
-tre
at-
me
nt
me
asu
rem
en
t
De
scri
ptiv
e c
ase
re
po
rt
RC
T w
ith a
ltern
ativ
e t
rea
t-m
en
t; p
re-
an
d p
ost
me
a-
sure
s a
t 1
, 3
, 6
, 1
2 m
o
De
scri
ptiv
e c
ase
re
po
rts
Pre
- a
nd
po
st-d
esi
gn
(p
are
nts
/ra
ters
aw
are
of
tre
atm
en
t)
De
scri
ptiv
e c
ase
re
po
rts
(pre
- a
nd
po
st-m
ea
sure
s)
To
uch
th
era
py
ver-
sus
on
e-t
o-o
ne
qu
iet
pla
y (r
ea
d)
231
5-m
in s
es-
sio
ns
pe
r w
ee
k;4
wk
tota
lE
last
ic (
pre
ssu
re)
wra
pp
ing
s a
d-
min
iste
red
ove
r 4
tre
atm
en
t se
s-si
on
sS
elf-
initi
ate
dve
stib
ula
r st
imu
-la
tion
; 5
-min
se
s-si
on
s 23
we
ek
ove
r 4
wk
Pre
ssu
re g
arm
en
ts(v
est
an
d g
love
s)w
orn
in
cla
ss-
roo
m
Tre
atm
en
t g
rou
ph
ad
AIT
(filte
red
/mo
du
-la
ted
mu
sic)
;co
ntr
ol
gro
up
ha
dst
ruct
ure
d l
iste
n-
ing
tre
atm
en
t(u
np
roce
sse
dm
usi
c),
2 3
30
min
pe
r d
ay,
10
da
ysA
IT 2
33
0 m
inp
er
da
y, 1
0 d
ays
AIT
30
min
da
ily,
10
da
ys
AIT
30
min
da
ily,
10
da
ys
To
uch
ave
rsio
ns,
off
-ta
skb
eh
avi
ors
, o
rie
nta
tion
to
sou
nd
s, s
tere
oty
pic
be
-h
avi
or,
te
ach
er
rep
ort
Se
lf-st
imu
lato
ry b
eh
avi
ors
,se
lf-a
bu
se,
soci
al
inte
r-a
ctio
ns
Tim
e s
pe
nt
voca
lizin
g
Se
lf-st
imu
lato
ry b
eh
avi
or
(e.g
., h
an
d s
lap
pin
g)
Ab
err
an
t b
eh
avi
or
(AB
C),
sen
sory
pro
ble
ms,
so
un
dse
nsi
tivity
, IQ
, la
ng
ua
ge
,a
ud
iom
etr
ic t
est
s.
De
scri
ptio
ns
of
sen
sory
,m
oto
r, a
nd
fu
nct
ion
al
be
ha
vio
rs
Pre
an
d p
ost
-te
sts
of
au
tism
sym
pto
ms
on
CA
RS
an
dA
BC
De
scri
ptio
ns
of
he
ari
ng
acu
-ity
, so
un
d s
en
sitiv
ity,
an
db
eh
avi
or
at
ho
me
/sch
oo
lre
po
rte
d b
y ca
reg
ive
rs
Bo
th g
rou
ps
sho
we
dp
osi
tive
ch
an
ge
s;tr
ea
tme
nt
gro
up
im
-p
rove
d i
n r
esp
on
se t
oso
un
ds,
ste
reo
typ
ic b
e-
ha
vio
r, a
nd
so
cia
l b
e-
ha
vio
rsG
en
era
lly p
osi
tive
ou
t-co
me
s in
all
are
as
du
rin
g t
rea
tme
nt
Incr
ea
sed
vo
caliz
atio
ns
du
rin
g t
rea
tme
nt;
mo
stp
rom
ine
nt
in fi
rst
we
ek
De
cre
ase
in
se
lf-st
imu
la-
tory
be
ha
vio
rs w
ithg
love
s, s
ligh
t (n
on
-si
gn
ifica
nt)
de
cre
ase
with
ve
st
Sim
ilar
ga
ins
no
ted
in
bo
th g
rou
ps.
75
% o
fsu
bje
cts
imp
rove
d i
n1
st m
on
th.
Mu
ch v
ari
-a
bili
ty a
nd
att
en
ua
tion
of
imp
rove
me
nts
ove
rco
urs
e o
f 1
2-m
o f
ol-
low
-up
. T
wo
su
bje
cts
ha
d s
ign
ifica
nt
ad
vers
ee
ffe
cts
Ge
ne
ral
imp
rove
me
nts
no
ted
in
a v
ari
ety
of
do
ma
ins
(e.g
., a
tte
n-
tion
an
d s
pe
ech
)N
o s
ign
ifica
nt
diff
er-
en
ces
on
CA
RS
an
dA
BC
; se
nso
ry p
rob
-le
ms
de
clin
ed
slig
htly
On
e c
hild
im
pro
ved
; o
ne
child
ha
d m
ixe
d r
e-
sults
; o
ne
ch
ild d
ete
ri-
ora
ted
fo
llow
ing
ase
izu
re d
uri
ng
AIT
an
d w
as
D/C
on
da
y 5
con
tinu
ed

Tab
le 1
.S
en
sory
an
d M
oto
r In
terv
en
tion
Stu
die
s(C
on
tinu
ed
)
Tre
atm
en
tIn
t.E
xt.
Inte
rve
ntio
n
Ou
tco
me
sS
tud
yca
teg
orya
nS
ub
ject
sva
l.bva
l.cG
end
De
sig
n e
lem
en
tssp
eci
fica
tion
sm
ea
sure
dF
ind
ing
s
AIT
(B
era
rd)
AIT
(T
om
a-
tis)
AIT
(B
era
rd)
AIT
Mu
dfo
rd e
ta
l.(2
00
0)
Ne
ysm
ith-
Ro
y (2
00
1)
Rim
lan
d &
E
de
lso
n
(19
94
)
Rim
lan
d &
E
de
lso
n
(19
95
)
16
6 44
5
18
Au
tism
(lo
wfu
nct
ion
ing
);a
ge
s 5
–1
4 y
r (M
59
.4)
Se
vere
Au
tism
;a
ge
s 4
–1
1 y
r
Au
tism
; p
ri-
ma
ry o
r se
c-o
nd
ary
dx;
4
–4
1yr
(M
51
0.7
)
Au
tism
; 4
–2
1 y
r
II II III
I
I III
II I
I IV III
III
Ba
lan
ced
cro
ss-o
ver
exp
eri
-m
en
tal
de
sig
n (
pa
ren
tsb
lind
to
tre
atm
en
t co
nd
i-tio
ns)
Pre
- a
nd
po
st-d
esi
gn
with
ind
ep
en
de
nt
evl
ua
tion
(re
pe
ate
d a
cro
ss s
ub
ject
s)
[Pa
rt 1
:C
om
pa
red
3 A
ITd
evi
ces
usi
ng
RC
T.]
Pa
rt2
:R
etr
osp
ect
ive
ca
seco
ntr
ol
(tre
atm
en
t g
rou
pco
mp
are
d t
o n
o t
rea
t-m
en
t, c
on
tro
l g
rou
p o
f 9
sub
ject
fro
m a
pre
vio
us
pilo
t st
ud
y).
Fo
llow
-up
fro
m 1
to
9 m
o i
n 1
91
sub
ject
s.
RC
T w
/ a
lt. t
rea
tme
nt;
Pre
-,m
id-,
an
d p
ost
-tre
atm
en
tm
ea
sure
s a
t 2
wk
an
d a
t1
, 2
, 3
mo
po
st-t
rea
tme
nt.
(ra
ters
an
d p
are
nts
blin
dto
co
nd
itio
ns)
AIT
ve
rsu
s p
lace
bo
(dis
en
ga
ge
dh
ea
dp
ho
ne
s),
30
min
23
/da
y,1
0 d
ays
; 3
–5
mo
ba
selin
e;
tre
at-
me
nt
an
d c
on
tro
lp
ha
ses
in r
an
do
mo
rde
r fo
r a
ll su
b-
ject
s2
0 (
30
-min
) se
s-si
on
s re
pe
ate
dfo
r 4
–8
blo
cks.
Tre
atm
en
t p
ha
ses
follo
we
d b
y 3
–8
we
eks
of
no
tre
atm
en
t/e
valu
a-
tion
ph
ase
sA
IT 2
33
0 m
in p
er
da
y fo
r 1
0 d
ays
;o
ne
of
thre
e A
ITd
evi
ce c
on
diti
on
s(E
ER
S,
Au
dio
-ki
ne
tro
n,
or
Au
dio
To
ne
En
-h
an
cer)
.
AIT
ve
rsu
s a
lter-
na
tive
tre
atm
en
t(u
np
roce
sse
dm
usi
c) 2
33
0m
in p
er
da
y fo
r1
0 d
ays
Ab
err
an
t b
eh
avi
or
(AB
C,
Nis
on
ge
r; o
bse
rva
tion
al
reco
rdin
gs)
, IQ
, a
da
ptiv
eb
eh
avi
or
(Vin
ela
nd
), l
an
-g
ua
ge
me
asu
re (
Re
yne
ll)
CA
RS
sco
res
(fro
m i
nd
e-
pe
nd
en
t ra
ting
s o
f vi
de
o-
tap
ed
pla
y o
bse
rva
tion
sa
nd
te
ach
er/
pa
ren
t in
ter-
vie
ws)
Au
dio
gra
ms,
be
ha
vio
ral
re-
act
ion
s to
so
un
d,
pa
ren
tre
po
rts
of
sou
nd
se
nsi
tiv-
ity,
ab
err
an
t b
eh
avi
or,
an
d b
eh
avi
or
pro
ble
ms
che
cklis
ts
Au
dio
gra
ms;
pa
ren
tal
re-
po
rts
of
hyp
ers
en
sitiv
ityto
so
un
d a
nd
ab
err
an
t b
e-
ha
vio
r (s
tere
oty
py,
hyp
er-
act
ivity
, sp
ee
ch,
etc
)
Se
vera
l d
rop
-ou
ts d
ue
to
pro
ble
ms
tole
ratin
gtr
ea
tme
nt;
pla
ceb
osl
igh
tly m
ore
be
ne
fi-ci
al
(le
ss a
be
rra
nt
be
-h
avi
or)
th
an
AIT
fo
rsu
bje
cts
tha
t co
m-
ple
ted
tre
atm
en
t
Pre
-tre
atm
en
t, a
ll su
b-
ject
s w
ere
“se
vere
lya
utis
tic”
on
CA
RS
;A
fte
r tr
ea
tme
nt
3(y
ou
ng
er)
ch
ildre
n h
ad
red
uce
d s
eve
rity
of
au
tism
; 3
old
er
chil-
dre
n h
ad
fe
w c
ha
ng
es
No
sig
nifi
can
t d
iffe
r-e
nce
s a
mo
ng
3 A
ITd
evi
ces.
Slig
htly
im
-p
rove
d s
ou
nd
se
nsi
tiv-
ity &
acu
ity.
De
cre
ase
da
ud
iog
ram
va
ria
bili
tya
sso
cia
ted
wit
h i
m-
pro
ved
be
ha
vio
r.A
ge
an
d d
eg
ree
of
sou
nd
se
nsi
tivi
ty n
ot
rela
ted
to
be
ha
vio
ral
imp
rove
me
nt.
Tre
atm
en
t g
rou
p h
ad
de
-cr
ea
sed
au
dito
ry p
rob
-le
m b
eh
avi
ors
an
da
be
rra
nt
be
ha
vio
rs 3
mo
nth
s p
ost
-tre
atm
en
t.N
o s
ign
ifica
nt
cha
ng
es
in s
ou
nd
se
nsi
tivity
;h
ow
eve
r, s
ub
ject
sw
ere
no
t n
ece
ssa
rily
hyp
er-
sen
sitiv
e p
re-
tre
atm
en
t
Zo
llwe
g,
Pa
lm,
& V
an
ce
(19
97
)
Ca
rmo
dy e
ta
l.(2
00
1)
Ka
pla
n e
ta
l.(1
99
6)
Ka
pla
n e
ta
l.(1
99
8)
AIT
Pri
sms
Pri
sms
Pri
sms
30
24
14
18
Au
tism
/MR
;a
ge
s 7
–2
4 y
r;M
51
4 y
r,5
mo
(in
clu
de
d1
AU
T
,8
yr)
Au
tism
; A
ge
s3
–1
8 y
r.;
(Me
dia
n 5
8)
Au
tism
; a
ge
s 4
–1
5 y
r;(M
ea
n 5
8 y
r)
Au
tism
/PD
D;
ag
es
7–
18
yr;
(Me
an
51
1.5
yr)
(39
% w
ithst
rab
ism
us)
I III
III
I
I II II II
III
III
III
III
RC
T w
/ a
lt. t
rea
tme
nt;
pre
-a
nd
po
st-t
rea
tme
nt
at
1w
k, a
nd
at
1,
3,
6,
an
d 9
mo
po
st-t
rea
tme
nt
(do
u-
ble
blin
d)
Cro
ss-o
ver
de
sig
n (
with
insu
bje
cts)
with
th
ree
co
n-
diti
on
s.
[In
de
pe
nd
en
t ra
ting
s fr
om
vid
eo
use
d t
o v
alid
ate
in
i-tia
l o
pto
me
tric
ra
ting
s.]
Cro
ss-o
ver
de
sig
n (
with
insu
bje
cts)
with
th
ree
co
n-
diti
on
s.
[In
de
pe
nd
en
t ra
ting
s b
y tw
oa
uth
ors
ma
de
la
ter
fro
mvi
de
o t
o v
alid
ate
in
itia
lo
pto
me
tric
ra
ting
s.]
Do
ub
le-b
lind
cro
ss-o
ver
de
-si
gn
with
pla
ceb
o c
on
tro
l
AIT
vs.
alt.
tre
at-
me
nt.
(u
n-
pro
cess
ed
mu
sic)
23/d
ay
for
10
da
ys,
30
min
/se
ssio
n
Th
ree
bri
ef
op
to-
me
tric
ass
ess
-m
en
t co
nd
itio
ns
for
ea
ch s
ub
ject
:n
o l
en
s (b
ase
line
)ve
rsu
s b
ase
-up
or
ba
se-d
ow
n l
en
ses
(ra
nd
om
ly o
r-d
ere
d t
rea
tme
nt)
for
ea
ch s
ub
ject
Pe
rfo
rma
nce
de
-sc
rib
ed
un
de
rth
ree
ass
ess
me
nt
con
diti
on
s: n
ole
ns
(ba
selin
e)
vers
us
ba
se-u
p o
rb
ase
-do
wn
le
nse
s(r
an
do
mly
or-
de
red
tre
atm
en
t)fo
r e
ach
su
bje
ct
Su
bje
cts
ma
tch
ed
/ra
nd
om
ly a
s-si
gn
ed
; 1 ⁄2
re-
ceiv
ed
pla
ceb
o(c
lea
r le
ns)
; 1 ⁄2
go
t tr
ea
tme
nt
(am
bie
nt
pri
smle
ns)
co
nd
itio
ns
for
3–
4 m
o;
the
nco
nd
itio
ns
we
rere
vers
ed
Au
dio
gra
ms,
se
nsi
tivity
an
dlo
ud
ne
ss t
ole
ran
ce;
ab
er-
ran
t b
eh
avi
ors
(A
BC
)
A s
ing
le s
ess
ion
ass
ess
me
nt
pe
rio
d w
ith 6
0–
90
se
ctr
ials
fo
r e
ach
ta
sk:
Re
cord
ed
sp
atia
l o
rie
nt-
ing
be
ha
vio
rs (
i.e.,
he
ad
an
d b
od
y p
ost
ure
, fa
cia
le
xpre
ssio
n)
wh
ile s
ea
ted
wa
tch
ing
TV
an
d b
all
catc
hin
g p
erf
orm
an
cew
hile
sta
nd
ing
A s
ing
le-s
ess
ion
ass
ess
me
nt
pe
rio
d w
ith 6
0–
90
se
ctr
ials
fo
r e
ach
ta
sk.
Re
cord
ed
ra
ting
s o
n v
i-su
al-
spa
tial
ori
en
tatio
nb
eh
avi
ors
(i.e
., h
ea
d p
osi
-tio
n,
bo
dy
po
stu
re,
faci
al
exp
ress
ion
) d
uri
ng
va
ri-
ou
s la
b t
ask
s (i
.e.,
wa
tch
TV
se
ate
d a
nd
sta
nd
ing
on
ba
lan
ce b
oa
rd;
ba
llca
tch
ga
me
).M
ea
sure
d b
eh
avi
or
pro
b-
lem
s (A
be
rra
nt
Be
ha
vio
rC
he
cklis
t);
visu
al-
spa
tial
ori
en
tatio
n a
nd
att
en
tion
pre
-, m
id,
an
d p
ost
-tre
at-
me
nt
for
bo
th t
rea
tme
nt
an
d c
on
tro
l co
nd
itio
ns.
No
sig
nifi
can
t d
iffe
ren
cein
au
dio
log
ica
l o
r b
e-
ha
vio
ral
ou
tco
me
s b
e-
twe
en
th
e g
rou
ps;
con
tro
l g
rou
p s
ho
we
dsl
igh
tly l
ess
ab
err
an
tb
eh
avi
or
at
6 m
o
po
st-t
rea
tme
nt
He
ad
po
stu
re,
bo
dy
po
s-tu
re,
faci
al
exp
ress
ion
,a
nd
ba
ll ca
tch
ing
in
-cr
ea
sed
with
co
rre
ct(f
aci
lita
ting
) p
rism
len
ses
as
com
pa
red
to
inco
rre
ct a
nd
ha
bitu
al
len
ses
Ove
rall
po
stu
re a
nd
pe
r-fo
rma
nce
wa
s b
ett
er
with
co
rre
ct p
rism
len
ses
for
gro
up
as
aw
ho
le
Imp
rove
d b
eh
avi
or
intr
ea
tme
nt
con
diti
on
(sh
ort
te
rm).
No
sig
-n
ifica
nt
diff
ere
nce
s b
e-
twe
en
tx
an
d c
on
tro
lco
nd
itio
ns
for
po
stu
ral
ori
en
tatio
n a
nd
att
en
-tio
n.
No
sig
nifi
can
td
iffe
ren
ces
be
twe
en
child
ren
with
an
dw
itho
ut
stra
bis
mu
s;tr
en
d f
or
mo
re b
eh
av-
ior
pro
ble
ms
with
pla
ceb
o l
en
ses.
con
tinu
ed

Tab
le 1
.S
en
sory
an
d M
oto
r In
terv
en
tion
Stu
die
s(C
on
tinu
ed
)
Tre
atm
en
tIn
t.E
xt.
Inte
rve
ntio
n
Ou
tco
me
sS
tud
yca
teg
orya
nS
ub
ject
sva
l.bva
l.cG
end
De
sig
n e
lem
en
tssp
eci
fica
tion
sm
ea
sure
dF
ind
ing
s
Pa
tte
rnin
g
Pa
tte
rnin
g
Exe
rcis
e
Exe
rcis
e
66
12
7 3
Inst
itutio
na
lize
dsu
bje
cts
with
MR
; (M
5
15
yr)
Va
rio
us
DD
—C
P,
MR
,a
utis
m/
seiz
ure
(M
58
yr)
Au
tism
4–
14
yr
Au
tism
7–
11
yr
I III
II II
I II II II
III
III
III
IV
RC
T w
ith a
lt tr
ea
tme
nt
(ph
ysic
al
act
iviti
es
with
sen
sory
stim
ula
tion
an
da
tte
ntio
n)
an
d n
o-t
rea
t-m
en
t co
ntr
ol
gro
up
Pro
spe
ctiv
e c
oh
ort
de
sig
n(n
on
ran
do
m g
rou
p a
s-si
gn
me
nts
); p
re,
mid
-(3
an
d 6
mo
) a
nd
po
st-
tre
atm
en
t m
ea
sure
me
nts
(at
10
mo
)
Re
pe
ate
d r
eve
rsa
l d
esi
gn
(AB
AB
); 4
5 r
eve
rsa
ls;
Mu
ltip
le p
re-
an
d p
ost
-tr
ea
tme
nt
me
asu
res
Co
un
ter-
ba
lan
ced
, a
ltern
at-
ing
tre
atm
en
ts d
esi
gn
.B
ase
line
an
d m
ulti
ple
po
st-t
rea
tme
nt
me
asu
res
Do
ma
n-D
elc
ato
me
tho
d p
att
ern
ing
tre
atm
en
t 2
hr/
da
y 53
pe
rw
ee
k fo
r 2
.5 m
o,
the
n 7
3p
er
wk
for
4 m
o
Do
ma
n-D
elc
ato
me
tho
d p
att
ern
ing
8 h
r p
er
da
y; c
on
-tr
ol
gro
up
re
-ce
ive
d S
pe
cia
lE
du
catio
n s
er-
vice
s; 1
0 m
o5
–2
0 m
in s
tru
ctu
red
ind
ivid
ua
l jo
g-
gin
g s
ess
ion
s;va
ria
ble
se
ttin
gs
(e.g
., c
linic
an
dh
om
e)
an
d v
ari
-a
ble
du
ratio
n o
ftr
ea
tme
nt
4–
17
da
ys1
5 m
in v
igo
rou
s a
c-tiv
ity (
jog
gin
g)
follo
we
d b
y 1
5m
in m
ild a
ctiv
ity(b
all
pla
yin
g)
an
dre
turn
to
1st
co
n-
diti
on
; co
nd
itio
no
rde
r re
vers
ed
on
seco
nd
da
y
Co
gn
itive
pe
rfo
rma
nce
,d
eve
lop
me
nta
l te
sts
for
voca
bu
lary
, vi
sua
l-p
erc
ep
tua
l, a
nd
mo
tor
skill
s
De
velo
pm
en
tal
pro
file
, IQ
with
Ba
yle
y m
en
tal
sca
leo
r S
tan
ford
-Bin
et
(me
a-
sure
me
nts
no
t u
nifo
rmly
ap
plie
d)
Pe
rce
nt
of
self-
stim
ula
tion
as
we
ll a
s n
um
be
r o
f co
r-re
ct r
esp
on
ses
on
aca
de
-m
ic (
ma
tch
ing
ta
sk)
an
db
all
pla
yin
g (
catc
hin
gta
sk).
Tim
e s
am
plin
g o
f st
ere
o-
typ
ed
be
ha
vio
rs
No
dra
ma
tic c
ha
ng
es
inin
div
idu
als
; n
o s
ign
ifi-
can
t ch
an
ge
s in
IQ
or
mo
tor
skill
s. S
ign
ifi-
can
t in
cre
ase
s fo
rtr
ea
tme
nt
gro
up
in
tw
oca
teg
ori
es
mo
st r
ela
ted
to t
rea
tme
nt
skill
sta
ug
ht;
vis
ua
l co
mp
e-
ten
ce a
nd
mo
bili
ty.
No
tre
atm
en
t co
ntr
ol
fare
dw
ors
t o
n m
ost
me
a-
sure
sT
rea
tme
nt
gro
up
slig
htly
be
tte
r in
la
ng
ua
ge
an
dso
cia
liza
tion
at
3 m
ob
ut
find
ing
s w
ere
sho
rt-l
ive
d a
nd
no
sig
-n
ifica
nt
diff
ere
nce
sfo
un
d a
t 1
0 m
o.
Co
nsi
ste
nt
de
cre
ase
in
self-
stim
ula
tory
be
ha
v-io
rs a
nd
im
pro
vem
en
tsin
aca
de
mic
an
d p
lay
resp
on
ses
follo
win
gtr
ea
tme
nt
Re
du
ctio
n i
n s
elf-
stim
u-
lato
ry b
eh
avi
ors
aft
er
vig
oro
us
jog
gin
ge
xerc
ise
.
Ne
ma
n et
al.
(19
74
)
Bri
dg
ma
n e
ta
l.(1
98
5)
Ke
rn e
ta
l.(1
98
2)
Ke
rn e
ta
l.(1
98
4)

KE
Y:
a Tre
atm
en
t C
ate
go
ry C
od
es
●S
I, S
en
sory
In
teg
ratio
n T
he
rap
y (c
lass
ica
l)●
SI-
ba
sed
, S
en
sory
-In
teg
ratio
n B
ase
d A
pp
roa
ch●
SS
, S
en
sory
Stim
ula
tion
Te
chn
iqu
e●
Pa
tte
rnin
g,
Se
nso
rim
oto
r P
att
ern
ing
●A
IT,
Au
dito
ry I
nte
gra
tion
Tra
inin
g●
Pri
sm,
Am
bie
nt
Pri
sm L
en
ses
(Vis
ua
l T
he
rap
y)●
Exe
rcis
e,
Exe
rcis
e T
he
rap
yb I
nte
rna
l V
alid
ity C
lass
ifica
tion
Cri
teri
a:
●I:
Pro
spe
ctiv
e s
tud
y co
mp
ari
ng
tre
atm
en
t to
alte
rna
tive
or
pla
ceb
o (
e.g
., R
CT
) w
he
re e
valu
ato
rs a
re b
lind
to
tre
atm
en
t st
atu
s.●
II:
Mu
ltip
le b
ase
line
, A
BA
B,
reve
rsa
l/with
dra
wa
l w
ith m
ea
sure
me
nt
of
ou
tco
me
blin
d t
o t
rea
tme
nt
con
diti
on
s, o
r p
rep
ost
de
sig
n w
ith i
nd
ep
. e
valu
atio
n.
●II
I: P
rep
ost
or
his
tori
cal
de
sig
ns
or
mu
ltip
le b
ase
line
, A
BA
B,
reve
rsa
l/with
dra
wa
l (n
ot
“blin
d”)
.●
IV:
Oth
er
(e.g
., s
ing
le s
ub
ject
[A
B o
r A
BA
] d
esi
gn
s w
itho
ut
mu
ltip
le b
ase
line
s; c
ase
stu
dy
rep
ort
s).
c Ext
ern
al
Va
lidity
Cla
ssifi
catio
n C
rite
ria
:●
I: R
an
do
m a
ssig
nm
en
t o
f w
ell-
de
fine
d c
oh
ort
s a
nd
ad
eq
ua
te s
am
ple
siz
e f
or
com
pa
riso
ns.
●II
: N
on
ran
do
m a
ssig
nm
en
t, b
ut
we
ll-d
efin
ed
co
ho
rts
with
in
clu
sio
n/e
xclu
sio
n c
rite
ria
an
d d
ocu
me
nta
tion
of
att
ritio
n/f
ailu
res.
In
ad
diti
on
, a
de
qu
ate
sa
mp
le s
ize
fo
r g
rou
p d
esi
gn
s o
r re
pli-
catio
n a
cro
ss t
hre
e o
r m
ore
sin
gle
su
bje
cts.
●II
I: W
ell-
de
fine
d p
op
ula
tion
of
thre
e o
r m
ore
su
bje
cts
in s
ing
le-s
ub
ject
de
sig
ns
or
sam
ple
of
ad
eq
ua
te s
ize
in
gro
up
de
sig
ns.
●IV
: O
the
r.d G
en
era
liza
tion
Cla
ssifi
catio
n C
rite
ria
:●
I: D
ocu
me
nte
d c
ha
ng
es
(i.e
., g
en
era
liza
tion
) in
at
lea
st o
ne
na
tura
l se
ttin
g o
uts
ide
of
tre
atm
en
t se
ttin
g.
●II
: G
en
era
liza
tion
to
on
e o
the
r se
ttin
g o
r m
ain
ten
an
ce b
eyo
nd
exp
eri
me
nta
l in
terv
en
tion
in
na
tura
l se
ttin
g i
n w
hic
h i
nte
rve
ntio
n t
oo
k p
lace
.●
III:
In
terv
en
tion
occ
urr
ed
in
na
tura
l se
ttin
g o
r u
se o
f o
utc
om
e m
ea
sure
s w
ith d
ocu
me
nte
d r
ela
tion
ship
to
fu
nct
ion
al
ou
tco
me
.●
IV:
No
t a
dd
ress
ed
or
oth
er.
Le
vin
son
&
Re
id
(19
93
)
Wa
tte
rs &
W
att
ers
(1
98
0)
Exe
rcis
e
Exe
rcis
e
3 5
Au
tism
(lo
wfu
nct
ion
ing
) 1
1 y
r
Au
tism
; a
ge
s 9
–1
1 y
r
II II
II II
IV IV
Co
un
terb
ala
nce
d,
alte
rna
t-in
g t
rea
tme
nts
de
sig
n;
mu
ltip
le p
re-,
du
rin
g,
po
st-t
rea
tme
nt
me
asu
re-
me
nts
Alte
rna
ting
tre
atm
en
ts d
e-
sig
n w
ith t
hre
e p
re-t
ask
con
diti
on
s in
ra
nd
om
ize
do
rde
r. P
re-
an
d p
ost
-tre
at-
me
nt
me
asu
res
15
min
gro
up
w
alk
ing
(m
ild
exe
rcis
e)
for
5 s
ess
ion
s ve
rsu
s1
5 m
in i
nd
ivid
ua
ljo
gg
ing
(vi
go
rou
se
xerc
ise
) 34
ses-
sio
ns
acr
oss
9 w
kC
om
pa
red
th
ree
con
diti
on
s: 8
–1
0m
in j
og
gin
g v
er-
sus
15
min
TV
vie
win
g v
ers
us
vari
ed
aca
de
mic
task
s; g
ive
n1
sess
ion
pe
r d
ay,
1–
4 3
pe
r w
ee
k(t
ota
l w
ee
ks v
ar-
ied
)
He
art
ra
tes,
in
div
idu
aliz
ed
me
asu
res
of
self-
stim
ula
-to
ry b
eh
avi
ors
Ra
tes
of
self-
stim
ula
tory
be
ha
vio
rs a
nd
aca
de
mic
pe
rfo
rma
nce
du
rin
g a
la
n-
gu
ag
e t
rain
ing
se
ssio
np
ost
tre
atm
en
t
Re
du
ctio
n i
n s
elf-
stim
u-
lato
ry b
eh
avi
ors
aft
er
vig
oro
us
exe
rcis
etr
ea
tme
nt.
Eff
ect
s w
ea
ro
ff a
fte
r 9
0 m
in
De
cre
ase
in
se
lf-st
imu
la-
tory
be
ha
vio
rs f
ollo
w-
ing
exe
rcis
e c
on
diti
on

Sensory Integration Therapy
Description and Assumptions
Sensory integration (SI) therapy, based on thework of Dr. A. Jean Ayres, is intended to focus directlyon the neurological processing of sensory informationas a foundation for learning of higher-level (motor oracademic) skills. Some of the neurological assumptionsupon which this model is based (i.e., hierarchically or-ganized nervous system) have received criticism asbeing outdated; recent theorists are reconceptualizingthis theory (Bundy & Murray, 2002). The assumptionthat sensory experiences have an effect on learning isless controversial, although the mechanisms throughwhich this occurs are somewhat ambiguous and oftendebated. Disruptions in subcortical (sensory integra-tive) functions are treated by providing controlled ther-apeutically designed sensory experiences for a child torespond to with adaptive motor actions. Through so-matosensory and vestibular activities actively con-trolled/sought out by the child, the nervous system isthought to be able to better modulate, organize, and in-tegrate information from the environment, which in turnprovides a foundation for further adaptive responsesand higher-order learning. Other necessary componentsof the classical SI model include a child-centered ap-proach, providing a just-right challenge (scaffolding),facilitating progressively more sophisticated adaptivemotor responses, and engaging the child in affectivelymeaningful and developmentally appropriate play in-teractions. The child’s focus is intended to be placedon the occupation of play (intrinsically motivated) andnot on cognitive-behavioral strategies or repetitivedrills—as is the focus of other sensorimotor and be-havioral approaches. Treatment goals may center onimproving sensory processing to either (a) develop bet-ter sensory modulation as related to attention and be-havioral control, or (b) integrate sensory informationto form better perceptual schemas and practic abilitiesas a precursor for academic skills, social interactions,or more independent functioning.
Service Delivery Model and Approach
SI therapy is classicallyprovided utilizing a directone-on-one intervention model in a clinic environmentthat requires specialized equipment (e.g., suspendedswings). Treatment plans are designed individually andcarried out by a trained therapist (OT) approximately1 to 3 times per week, 1-hour sessions. Duration typi-cally entails several months and in some cases years.Consultative services, home/school programs, or task/
406 Baranek
environmental adaptations are often provided in tan-dem with the direct intervention. Cost varies depend-ing on the location, frequency, and duration of thetreatment, but it is comparable to hourly rates of othertherapy services. Equipment is generally low-tech, butcan be moderately expensive. The feasibility of doingclassical SI in a school setting is low because of theneed for specialized equipment and the “pull-out”model that may conflict with inclusionary principles.
Empirical Studies
Three studies investigated interventions thatmatched the criteria of classical SI therapy. Two utilizedprospective AB designs with several subjects and ade-quate controls to look at SI treatment efficacy (Case-Smith & Bryan, 1999; Linderman & Steward, 1999); oneutilized a retrospective design to identify predictors ofpositive outcomes within a group of children with autismreceiving SI (Ayres & Tickle, 1980). Although outcomemeasures included aspects of proximate (sensory pro-cessing/modulation) functions and/or broader outcomes(e.g., play skills, social interactions), none of the studiesdirectly attempted to remediate deficits in praxis.
Case-Smith & Bryan (1999) studied five boysacross a 3-week baseline phase and a 10-week inter-vention that consisted of a combination of classical SItreatment and consultation with teachers. Independentcoding of videotaped observations of free play indi-cated that three of the five boys demonstrated signi-ficant improvements in mastery play, and four of fivedemonstrated less “nonengaged” play. Only 1 subjecthad significant improvements with adult interactions,and none changed in level of peer interaction. Outcomemeasures more directly related to intrinsic features ofthe intervention (e.g., individual mastery play) ap-peared more improved than measures that were notdirectly addressed in treatment (e.g., peer interaction).Although it is possible that the positive results couldbe attributed to factors other than the intervention it-self (i.e., maturation, caregiving effects), the authorsnote that the behaviors did not change systematicallyacross all outcome measures. However, because sen-sory processing variables were not directly assessed, itis not known whether the positive outcomes are directlydue to improvements in sensory processing mechanismsper se,as would be purported by sensory integrationtheory. It is also possible that the improvements evi-denced are a function of other components of the in-tervention (e.g., play coaching, motivational strategies).
Linderman & Steward (1999) also utilized a sin-gle subjects AB design with two 3-year-olds with per-

vasive developmental disorder (mild autism) to trackthe functional behavioral changes in the home envi-ronment associated with classical SI (clinic-based1 hour per week for 7 to 11 weeks). Subject 1 (who wasnoted to have tactile hypersensitivity) demonstratedgains in all intended outcomes (social interactions, ap-proach to new activities, response to holding). Subject2 (who had both hypo-responsiveness to vestibular andhyper-responsiveness to tactile sensations) made gainsin activity level and social interaction, but not in func-tional communication. This study purports that SI mayresult in some functional gains that generalize to natu-ralistic contexts. However, given the limitations inher-ent in this single subject design, it is also possible thatother co-occurring interventions (e.g., education), mat-urational effects, and parent participation in evaluationprocedures may have also contributed to the positiveoutcomes, thus limiting definitive conclusions aboutthe efficacy of the treatment.
The last study by Ayres and Tickle (1980) utilizeda retrospective (within group) design to explore variablesthat predicted positive or negative outcomes followingone year of SI therapy in 10 children (mean age 7.4 years)with autism. They found that subjects who tended tohave average to hyper-responsive patterns to the vari-ous stimuli (e.g., touch, movement, gravity, and airpuff) showed better outcomes than those with a hypo-responsive pattern. Numerous limitations (i.e., small sam-ple size, variability of the outcome measures used, lackof control over maturational effects, retrospective natureof the study) make conclusive statements difficult; how-ever, the study raises the possibility that differences inoutcomes may be partially dependent on specific subjectattributes including patterns of sensory processing.
Numerous efficacy studies of SI exist with otherpopulations (e.g., children with MR or LD) (e.g., Arendt,Maclean, & Baumeister, 1988; Ayres, 1972; Clark et al.,1978; Hoehn & Baumeister, 1994; Humphries et al.,1990; 1992; 1993; Kanter, Kanter, & Clark, 1982; Po-latajko et al.,1991; 1992; Wilson et al.,1992). Althoughthese are excluded from this review, it is noteworthythat these studies have sparked much controversy, giventhe lack of consistent empirical support. Some difficultissues surround the nature of the intervention andwhether or not these studies were truly representativeof SI therapy versus some other variation of sensori-motor or perceptual-motor treatments. Several meta-analyses (Ottenbacher, 1982; Vargas & Camilli, 1999)are also available; these report that effect sizes vary fromlow to moderately high depending on the populationsstudied, recency of the studies, and specific parametersmeasured. Outcomes in psychoeducational and motor
Efficacy of Sensory and Motor Interventions for Children with Autism 407
categories are stronger than in other areas, at least forSI studies compared to no treatment conditions; how-ever, effects appeared to be equivocal when comparedwith alternative treatments.
Other Sensory Integration-Based Approaches
Description and Assumptions
This section groups several types of approachesthat are based on the foundations of SI theory, but de-viate from classical SI in one or more criteria: (a) so-matosensory and vestibular activities are provided butsuspended equipment is not used; (b) treatment is moreadult-structured or passively applied (i.e., not con-ducive to child-directed play), and/or (c) treatment ismore cognitively focused than found in classical SI.For example, structured perceptual-motor training ap-proaches may fall into this category. Although thesewere popular 10 to 30 years ago, they are less oftenused today with children with autism.
One example of a popular modernized version of anSI-based program is the “Sensory Diet” (or sometimesreferred to as a sensory summation approach), in whichthe child is provided with a home or classroom programof sensory-based activities aimed at fulfilling the child’ssensory needs. A schedule of frequent and systematicallyapplied somatosensory stimulation (i.e., brushing with asurgical brush and joint compressions) is followed by aprescribed set of activities designed to meet the child’ssensory needs are integrated into the child’s daily rou-tine. Another example that melds together aspects of sen-sory integration theory with a cognitive-behavioralapproach is the “Alert Program,” in which a child (usu-ally with a higher functioning level and verbal abilities)is given additional cognitive strategies to assist withhis/her arousal modulation.
Service Delivery Model and Approach
These models often utilize a direct intervention (one-on-one or group). Consultative/collaborative models arecommon; caregivers under the supervision of a thera-pist may carry out school programs. Treatments gen-erally require less equipment than classical SI and canoften be provided in an inclusive setting. Cost is com-parable to SI, depending on the length and duration ofintervention.
Empirical Studies
No studies of specific perceptual-motor treatmentsfor autism were found. Two studies (Larrington, 1987;Reilly, Nelson, & Bundy, 1983) using structured

sensorimotor interventions based on SI principles werefound. Despite documenting numerous positive out-comes, the descriptive case study by Larrington (1987)provides limited internal validity as a result of multi-ple methodological weaknesses, probable maturationeffects, and a focus on an older age-group (teenager)that has limited generalizability to young children. Themore rigorous study by Reilly et al., (1983) utilized acounter-balanced alternating treatments design with18 children diagnosed with autism (ages 6 to 11 years)to measure the comparative effects of two interventionson production of vocalizations. The authors expectedthat structured vestibular-based activities would facil-itate higher amounts of language in their subjects duringthe intervention than the table-top fine motor activities.Order of the two treatment conditions was randomlyassigned, and each subject received two 30-minute ses-sions of each type. No significant differences werefound with respect to function of speech, articulation,total language, or rate of vocalizations during the in-tervention sessions. In contrast to the hypotheses, sig-nificant differences in favor of the fine motor groupwere found for variety of speech, length of vocaliza-tions, and amount of autistic speech. Limitations ofthese findings included: (a) the children’s vocalizationshad been previously reinforced by teachers during finemotor activities in the classroom—which may haveproved in favor of the alternative therapy; (b) a shortduration of the intervention period may not have beensufficient to provide an adequate sampling of behav-iors, and (c) outcome measures outside of the treatmentsessions were not provided, thus it is not known if thevocalizations generalized to other contexts.
Although the Sensory Diet interventions are com-monly used, only one study of a child suspected of hav-ing an autistic spectrum disorder was found (Stagnitti,Raison, & Ryan, 1999). This case report described a5-year-old boy with severe sensory defensiveness whounderwent a treatment program consisting of brushing(i.e., sensory summation) followed by joint compres-sions an average of 3 to 5 times daily for 2 weeks. Theprogram included integration of appropriate sensory ac-tivities interspersed throughout the child’s daily activ-ities and routines (i.e., sensory diet) and was carried outby the parents at home under the supervision of a thera-pist trained in these methods. Following initial im-provements, the treatment program was repeated severalmonths later when the child’s behaviors seemed to againdeteriorate. Post-treatment parental reports suggestedimprovements in tolerance of tactile stimulation, fewertemper tantrums, an increase in activity level, and bet-ter coordination. The authors concluded that the child
408 Baranek
was cured of his sensory defensiveness, and autisticsymptoms appeared to resolve. These anecdotal claimsappear unfounded given that no systematic data werecollected and that adequate methodological controlswere not instituted (e.g., a variety of competing treat-ments were implemented during the 9-month period).
No empirical studies on the Alert Program werefound for children with autism or related populations. Itmay be that some of these programs have been too re-cently developed to have been subjected to empiricaltests; more likely they are utilized by clinicians who re-port outcomes via individualized education plans (IEPs)and not through the peer-reviewed research literature.
Sensory Stimulation Techniques
Description and Assumptions
These approaches are varied and usually involvepassively providing one type of sensory stimulationthrough a circumscribed modality (e.g., touch pressure,vestibular stimulation) with a prescribed regimen. Some-times these techniques are incorporated within thebroader sensory-integration–based programs describedabove; other times they are used in isolation. The as-sumptions vary with the treatment, but most are basedon neurophysiological principles stipulating that a givensensory experience may provide facilitatory or inhibitoryinfluences on the nervous system that result in behav-ioral changes such as arousal modulation. An exampleof a commonly used technique is “deep pressure” (i.e.,firm touch pressure providing calming input), which canbe applied via therapeutic touch (e.g., massage; jointcompression), or an apparatus (e.g., Hug Machine, pres-sure garments, weighted vests). Vestibular stimulation,another example, is often used to modulate arousal, fa-cilitate postural tone, or increase vocalizations. Auditoryintegration training and visual therapies will be discussedin separate sections.
Service Delivery Model and Approach
The service delivery models vary, depending onthe intervention provided. Both direct and consultativeapproaches are used, although the direct interventionapproach is more often described in research. Costvaries depending on the equipment used (e.g., minimalcost of brushes vs. moderate to significant costs of HugMachine) and staff time allocated.
Empirical Studies
Five studies specific to children with autism werefound in this category. Three of the studies utilized case

study descriptions (McClure & Holtz-Yotz, 1990;Ray, King, & Grandin, 1988; Zisserman, 1991), andtwo provided more rigorous and controlled methodo-logies with randomization of subjects to two alterna-tive treatment conditions (Edelson, Goldberg, Edelson,Kerr, & Grandin, 1999; Field et al., 1997). One studyreviewed the effects of vestibular stimulation (Rayet al., 1988), and four studies investigated the effectsof somatosensory stimulation on a variety of behaviors.All of these studies report effects of some type of touchpressure/deep pressure.
Although several limitations (e.g., a tendency touse numerous measures with small sample sizes) existin the majority of these studies, they yield some usefulinformation that may guide educational planning. Thetwo prospective controlled studies provide preliminaryevidence that touch pressure may have a calming ef-fect on children with autism (Edelson et al.,1999; Fieldet al., 1997). Field et al. (1997) measured the effectsof touch therapy (massage) on attentiveness and re-sponsivity in 22 preschool children with autism. Mas-sage was provided for 15 minutes per day, 2 days perweek for 4 weeks (i.e., eight sessions). Results indi-cated that both groups showed positive changes withrespect to all the observational variables (i.e., touchaversion, off-task behavior, orienting to sounds; stereo-typies) post-treatment; the touch therapy group demon-strated significantly greater changes in responsivenessto sound and stereotypies and significant improvementson measures of social communication. Although hy-pothetically links were made to changes in autonomic(vagal) activity, these claims are unsubstantiated, be-cause no physiological measures were taken.
Edelson et al., (1999) investigated the efficacy ofthe Hug Machine—a touch pressure device designedby Temple Grandin to decrease arousal and anxiety byself-administration of lateral body pressure—in 12 chil-dren with autism that had varying levels of anxiety. Thetreatment group (Hug Machine twice for 20 minutesper week for 6 weeks) showed a significant reductionon a tension scale and a marginally significant changeon anxiety. Physiological measures (galvanic skin re-sponses) were not significantly different betweengroups overall; however, variability in the experimen-tal group increased over the course of treatment. Theauthors concluded that children in the treatment groupwith higher initial levels of arousal/anxiety were morelikely to benefit from the intervention. Although thesmall sample size and marginally significant findingslimit the conclusions in this study, there is some con-vergence of findings with the Ayres and Tickle (1980)study that children with hyper-responsive patterns may
Efficacy of Sensory and Motor Interventions for Children with Autism 409
benefit more from these types of sensory-based inter-ventions than those who are under-responsive.
Both McClure and Holtz-Yotz (1990) and Zisser-man (1991) provide interesting but methodologicallyweak case reports using variations of touch pressuregarments to diminish self-stimulatory behaviors.Neither study provided a functional analysis of the self-stimulatory behaviors prior to the interventions, but bothassumed the function of the behaviors was sensationseeking and/or arousal modulation based and hypo-thesized that providing a sensory substitute would yieldcalming effects and decreased stereotypy. Zisserman(1991) described clinical improvements using pressuregloves (overall 46% decrease) but not for pressure vest(11.8% decrease). Additionally, no carry-over effectscould be demonstrated once the gloves were removed.Similarly, McClure & Holtz-Yotz (1990) using elasticwraps to effect behavioral changes (i.e., social inter-actions, self-stimulation) reported some positive effectsin an institutionalized 13-year-old boy with autism/mental retardation; however, investigator biases, co-interventions (medication, physical agent modalities),and poor reliability/validity for the measures used sig-nificantly limited conclusive statements. The final casestudy by Ray et al. (1988) describes the effects ofvestibular stimulation on speech sounds in a 9-year-oldlow-functioning boy with autism and dyspraxia. Self-controlled vestibular stimulation (i.e., spinning in circles5 minutes for 17 days across a 4-week period). Speechsounds were greater in the treatment (17% time) than thepre- (2% time) or post-intervention (1.3% time) phases.Because no measures of vestibular processing were di-rectly collected, it is unclear whether the increasedspeech production was directly linked to vestibular pro-cessing changes. The child was simultaneously receiv-ing other SI treatments in school, which may haveconfounded results.
Auditory Integration Training (AIT) and RelatedAcoustic Interventions
Description and Assumptions
AIT is based on the concept that electronicallymodulated/filtered music provided through earphonesmay be helpful in remediating hypersensitivities andoverall auditory processing ability that is thought to beproblematic in children with autism. Although exact neu-rological mechanisms underlying AIT and other listen-ing therapies are not known, various hypotheses havebeen proposed (e.g., improved functioning of the retic-ular activating system, reorganization of the cerebellar-vestibular system, modification of brain serotonin levels).

AIT is said to “massage” the middle ear (hair cells in thecochlea) and enhance auditory perception. Methods andequipment vary depending on the specific philosophicalapproach (i.e., Tomatis or Berard); the most commonlyused approach for children with autism in the UnitedStates is the Berard method, developed by the Frenchotolaryngologist during the 1960s–1990s. In the Berardmethod, a modulating and filtering device (e.g., Ears Ed-ucation & Retraining System [EERS], Audiokinetron orAudio Tone Enhancer [ATE]) accepts music input fromCDs and transforms sounds by (a) randomly modulatinghigh and low frequencies and (b) filtering out selectedfrequencies in accordance with the child’s performanceon an audiogram (test of auditory thresholds to a seriesof frequencies that measures hearing ability). Sound fre-quencies that are 5 to 10 dB different from their adjacentfrequencies (i.e., “peaks”) are filtered out for the listen-ing sessions. Volume level for the left ear is sometimesreduced in order to stimulate language development inthe left hemisphere. Although improved sound modula-tion is one goal of treatment, other goals include en-hancement of generalized behaviors (attention, arousal,language, social skills, etc.).
The Tomatis method is similar, but integrates apsychodynamic with a psychophysiological perspec-tive. In the passive phase, the individual listens to fil-tered sounds of the maternal voice, as well as preparedmusic through a modulating apparatus (i.e., ElectronicEar that attenuates low frequencies and amplifies higherfrequencies). The earphones have an attached bone con-ductor to facilitate sounds through vibration and airconduction methods. Later, in the active phase, the sub-ject is introduced to language and audio vocal exercisesthat provide feedback of his/her own voice throughheadphones to reinforce more normal auditory percep-tion and overall quality of life.
Variations of listening programs applied to chil-dren with autism include Stephen Porges’ AcousticIntervention. This treatment is based on Porges’ (1998)Polyvagal Theory—a phylogenetic theory of autonomicnervous system control that is the substrate for emo-tional and affective experiences. By providing filteredsounds of the human voice (as opposed to any filteredmusic), the listening stimulation is designed to alter-natively challenge and relax the middle ear muscles toenhance speech perception.
Service Delivery Model and Approach
The Berard AIT treatments are usually providedindividually in a small sound-quiet room for 30 min-utes 2 times per day for 10 to 20 days (i.e., minimum
410 Baranek
of 10 hours) by a professional trained in the techniques.Fees can range from $1000 to $3000 for the 2-weektreatment. The equipment itself is highly technical andexpensive. The Tomatis method is performed in simi-lar ways but often with repeated blocks of interventionwith longer overall durations, sometimes spanningyears of treatment. The Porges acoustic interventionuses five sessions at 45 minutes each. Occasionally,such auditory treatments are provided within a schoolsetting if the trainer brings the equipment to the school.
Empirical Studies
Nine studies were found using various methods ofAIT with children with autism. Eight of these studieswere utilized the Berard AIT method (Bettison, 1996;Brown, 1999; Gillberg, Johansson, Steffenburg, &Berlin, 1997; Link, 1997; Mudford, et al., 2000; Rim-land & Edelson, 1994; 1995; Zollweg, Palm, & Vance,1997). The Tomatis AIT approach was used in onestudy (Neysmith-Roy, 2001) for the population of in-terest. An additional study of the Tomatis AIT methoddemonstrating no positive benefits for children withsignificant learning disabilities is also published (Ker-shner et al., 1990) but is not included in this review.Although Porges’ acoustic intervention is currently un-dergoing some scientific experiments with childrenwith autism, no published studies in peer-reviewedjournals were found.
Of the nine AIT studies reviewed in total, threeused randomized, controlled methods with either notreatment or an alternate treatment/placebo, (Bettison,1996; Rimland & Edelson, 1995; Zollweg et al.,1997),two utilized other methodological designs with variouslevels of control (Neysmith-Roy, 2001; Mudford, et al.,2000), one was a pre-post open trial (Gillberg et al.,1997), two were descriptive case reports (Brown, 1999;Link, 1997), and one compared various types of AITdevices (Rimland & Edelson, 1994). These are sum-marized below.
Bettison (1996) utilized a randomized controlledtrials design with AIT as the treatment condition andan alternative structured listening task for the controlcondition for 80 children with autism (ages 3 to 17 years)with concomitant sound sensitivities. At 1 month post-treatment, both groups demonstrated significant butequal amounts of improvement for all measures show-ing nonspecific treatment effects. Significant improve-ments were maintained for the audiogram scores only;patterns of change across other behavioral measures(behavior checklist; development, sensory checklist,and sound sensitivity questionnaire) was so variable

that it is difficult to interpret clinically, even though someof the changes were positive. By 12 months, most ofthe improvements seen reverted to initial post-treatmentlevels taken at 1 month. It is not clear what aspect ofthe interventions was responsible for the outcomes—maturation, practice effects, or other aspects of thetreatment may have also influenced the results. More-over, this study documents negative side effects for twosubjects who had documented psychiatric problems.
Rimland & Edelson (1995) present some positiveeffects with 18 subjects (4 to 21 yrs of age) in a ran-domized controlled trial using AIT (EERS) versus un-filtered music. Results indicated that the treatmentgroup demonstrated fewer auditory problem behaviorsand aberrant behaviors than the control; these im-provements were maintained across 3 months. How-ever, neither the pure tone discomfort test nor thehearing sensitivity questionnaire provided evidence ofreduction in sound sensitivity post-treatment. Treat-ment and control groups did not significantly differ intheir hearing acuity at any of the six points tested. Posi-tive results were not limited to those with hyper-sensitive hearing. In a large scale study, these sameauthors (Rimland & Edelson, 1994) investigated thedifferential effectiveness of three types of auditoryfiltering devices for 445 subjects with primary orsecondary diagnoses of autism (CA 5 4 to 41 years;M 5 10.73 years). Because no differences were foundacross the three devices, data were collapsed across treat-ment conditions. Results indicated a significant but smallimprovement in hearing sensitivity, as well as decreasedvariability in audiograms for some subjects, mostlyduring the first 3 months. Lower-functioning individu-als seemed to make greater gains. However, there wasno significant relationship between level of sensitivitypre-AIT and the behavioral outcomes post-treatment.
Zollweg, Palm, & Vance (1997) used a well-controlled, double-blind design with an alternative treat-ment to study the effects of AIT on 30 low-functioning,multihandicapped, institutionalized residents. Nine ofthe 30 residents had autism; only 1 of the 9 with autismwas a child under the age of 8 years. Participants wereassigned randomly to treatment (filtered/modulatedmusic) or control (unfiltered/unmodulated music) groupsand provided with twenty 30-minute sessions by trainedpractitioners who were blind to the treatment conditions.Participants were allowed to engage in other activities(e.g., eating, toy play, magazine browsing) simultane-ously with treatment to facilitate cooperation. Subjectswere assessed for hearing sensitivity and tolerancefor loud sounds pre- and post-treatment (1- 3-, 6-, and9-month time periods) by a licensed audiologist, also
Efficacy of Sensory and Motor Interventions for Children with Autism 411
blind to treatment conditions. Results of audiological as-sessments demonstrated that there was a small magni-tude change of 200 Hz on pure tone thresholds betweenthe two groups at only one of seven frequencies tested.This finding was likely spurious given the number ofcomparisons and was not deemed clinically significantby the authors. No significant group differences werefound with respect to loudness discomfort levels at anyfrequency for any of the follow-up time points; in fact,only one subject demonstrated an increased tolerance be-tween the pre-AIT and the 9 month, post-AIT condition.Behavioral data indicated that both groups were reportedto improve over time; slight differences favored the con-trol group at 6 months post-treatment for overall scoreson the Aberrant Behavior Checklist (ABC), but groupshad similar levels of improvement on this measure at9-months after treatment. No significant differences be-tween groups were noted for any of the subscales of theABC at any of the post-treatment time points. Althoughboth groups were reported to improve over time, notablefluctuations across the subscales of aberrant behavior onpost-treatment assessment phases were not easily inter-pretable. These findings are similar to those of Bettison(1996) suggesting that factors other than AIT (e.g., extraattention; caregiver expectations, etc.) could be respon-sible for reductions in aberrant behaviors.
Mudford et al. (2000) used a balanced cross-overdesign to assess the effects of AIT (twenty 30-minutesessions) with 16 children with autism ages 5 to 14years. Four were girls; all of the subjects were low-functioning. Parents and AIT practitioners were blindto the treatment conditions that included either AIT(modulated music) without the filtering component, orthe placebo control (headphones disengaged, musicplaying in background of room). Baseline and follow-up assessments were used for each condition, includ-ing standardized measures of aberrant behavior,cognitive functioning, adaptive levels, language levels,and observational data. Notably, several childrendropped out of the study as a result of inability to tol-erate the procedures and/or severe behavioral difficul-ties. Of the 16 children completing the study, there wereno positive findings in favor of the AIT condition, de-spite a liberal alpha level used in the statistical tests.In fact, small but significant differences on measuresof aberrant behavior favored the control condition forthis low-functioning group.
Neysmith-Roy (2001) describes outcomes of theTomatis AIT method with six children with severeautism ranging from 4 to 11 years. Several blocks of“Intensives” (i.e., twenty 30-minute sessions repeatedfrom four to eight times) were each followed by a 3- to

8-week unsystematic evaluation period spanning 6 to21 months, depending on the individual child’s pro-gram. Pre- and post-measures of autistic symptoms onthe Childhood Autism Rating Scale (CARS) wererecorded on videotapes of two separate play conditionsand parent/teacher reports during both the interventionand evaluation phases. Videos were randomized andcoded by two raters who were blind to the conditionsof the study for each subject. Reductions in autisticsymptoms overall including an improvement in pre-linguistic behaviors were noted in three of the six boys(50%), who also happened to be among the youngestsubjects, but no improvements were seen in the otherthree (older) boys. Audiological/physiological mea-sures were not employed because the boys were unableto cooperate for the testing.
A case report by Brown (1999) on two preschool-age siblings with autism describes improvements insensory-motor functions, attention, social interest, praxis,eye control, and speech for two children who underwentAIT for two 30-minute sessions for 10 days. Similary,Link (1997) presented a case report for three childrenwith autism, documenting mixed findings. Sound sen-sitivity (using unvalidated measures) was noted to beunchanged for two of the three children and inconclu-sive for the third. Informal behavioral observationswere found to be improved for one child (across par-ent and teacher ratings) and mixed a second child. Onechild unfortunately suffered a psychomotor seizure dur-ing the AIT procedure and was removed from the pro-tocol on day 5. Parent and teacher reports on day 5indicated deterioration in behaviors possibly related tothe seizure. Both studies were weak methodologicallysuch that no systematic data was collected and pre- andpost-measures lacked independence, as well as valid-ity and reliability data; thus findings are speculative.
In summary, the nine available studies using var-ious methods of AIT with children with autism demon-strate mixed results. Studies with sample selectionbiases and unmasked evaluation processes would tendto favor outcomes for the treatment groups; however,this was not always the case. Some studies, using var-ious types of methodologies, reported improvements ineither behavior or audiological measures (e.g., Brown,1999; Link, 1997; Neysmith-Roy, 2001; Rimland,1994; 1995) at some points in time for some children.However, it is important to note that if changes are seenin behaviors without concomitant changes in hearingsensitivity, an alternative mechanism than that pro-posed by AIT theory may be responsible for the im-provements. Furthermore, significant fluctuations ofbehavior over time, and inconsistency of performance
412 Baranek
across measures seen in several studies (e.g., Bettison,1996; Zollweg et al., 1997) are difficult to interpret.Adverse effects (i.e., seizures, behavioral problems)and drop-out rates require special attention given thatthese are reported in several AIT studies.
Methodologically stronger studies (Bettison; 1996;Mudford et al., 2000; Zollweg et al., 1997) demon-strated that improvements in behavior often were notsignificantly different between treatment (AIT) andcontrol (unfiltered/unmodulated music) conditions(Bettison, 1996; Zollweg et al., 1997). In two studies(Mudford et al., 2000; Zollweg et al., 1997) the con-trol group showed a subtle advantage in reduction ofaberrant behaviors at at least one point in time. Simi-lar improvements for subjects in both treatment andcontrol conditions suggest that effects are due to fac-tors that are peripheral to the treatment (e.g., extra at-tention; caregiver expectations; compliance training)and/or other co-occurring treatments (i.e., behavioraland educational interventions) may be influencing out-comes. Future replication studies need to better controlfor such effects. Although the hypothesis that music ingeneral (filtered or unfiltered) may have a beneficialeffect on behavior is plausible, it is yet to be tested em-pirically. Gravel (1994) provided a detailed critique ofAIT studies, stressing the importance of distinguishingbetween statistical and clinical significance. She statesthat small differences between frequencies (i.e., 5 dB)or fluctuations in hearing sensitivity in some childrenwith autism may be attributable to attentional/behavioraldifficulties that preclude reliable responses on behav-ioral audiometry. Furthermore, electrophysiologicalmeasures (ABRs) fail to demonstrate differences inhearing sensitivity between children with autism andcontrols—a finding that may challenge the overallpremise of AIT.
Visual Therapies
Description and Assumptions
A variety of visual therapies including but not lim-ited to oculomotor exercises, ambient prism lenses, andcolored filters (i.e., Irlen lenses) have been applied tochildren with autism. These visual or behavioral opto-metric therapies and are aimed at improving visual pro-cessing or visual-spatial perception that may be relatedto autistic symptomatology (e.g., unusual visual stereo-typies, coordination problems, strabismus, attention,etc.). In particular, the ambient (i.e., visual-spatial sys-tem) as opposed to the focal (i.e., visual acuity system)is hypothesized to be dysfunctional in children with

autism. Thus prism lenses transform the light throughan angular displacement of 1 to 5 degrees (base up orbase down), producing a shift in the field of vision.These are thought to lead to more stable perception andimproved behavior or performance.
Service Delivery Model and Approach
Visual therapies and corrective lenses are pre-scribed individually through a licensed optometrist. Insome cases, programs are carried out by parents or otherprofessionals. Various visual treatments may also becombined, as in the case of ambient lenses and oculo-motor exercises. Costs may be moderate and includethe optometrist’s fees for the initial and follow-up eval-uations and cost of prescriptive eyewear.
Empirical Studies
Anecdotal data are plentiful; however, empiricalstudies regarding the efficacy of visual therapies specificto children with autism are limited. No published stud-ies were found on the use of Irlen lenses or independentuse of oculomotor therapies for children with autism.Three studies (all by the same group of researchers) in-vestigating prism lenses were found (Carmody, Kaplan,& Gaydos, 2001; Kaplan, Carmody, & Gaydos, 1996;Kaplan, Edelson, & Seip, 1998).
The study by Kaplan et al. (1998) used the mostrigorous methodological design (double-blind cross-over). It was an extension of the earlier pilot investi-gation (Kaplan et al.,1996) and used 18 children withautism (CA 5 7 to 18 years; M 5 11.53 yrs). Thirty-nine percent had strabismus. All subjects were pre-scribed prism lenses with modification determinedindividually for the visual direction (base up or basedown) and angular displacement. Five subjects were lostas a result of non-compliance with the eyewear. The re-maining 18 were matched and randomly assigned to oneof the two conditions (placebo lenses or treatment withprism lenses) for 3 months; then treatment conditionswere switched for the second phase (4 months). Pre-,mid-, and post-treatment measures were taken for pos-tural orientation, attention, and visual-spatial perfor-mance tasks, as well as ratings of behavioral problems.Results indicated short-term positive effects—behavioralfindings were most apparent at the mid-evaluation (11⁄2or 2 months), with less improvement at follow-up (3 or4 months). Performance on orientation and visual-spatial tasks was not significantly different betweenconditions. Given these findings, it is unclear what spe-cific mechanisms were responsible for the behavioralimprovements because the visual performance mea-
Efficacy of Sensory and Motor Interventions for Children with Autism 413
sures were unchanged, at least in the context of the lab-oratory tasks. Children were not engaged in simulta-neous visual training tasks that are usually prescribedin conjunction with prism lenses, which may have lim-ited long-term effects. Treatment effects did not appearrelated to whether or not the children had a prediag-nosed strabismus; however, a slight trend toward morebehavioral problems during the clear lens (placebo)condition for the strabismus subgroup was reported.
Unfortunately, the above results were less encour-aging than those from the original pilot study (Kaplanet al., 1996) and a more recent study (Carmody et al.2001), both of which demonstrated significantly bet-ter performance on orientation and visual-spatial per-formance when children with autism were wearingcorrect (“facilitating”) prism lenses. Carmody et al.(2001) assessed responses to prism lenses for a conve-nience sample of 24 children (2 girls, 22 boys) withautism, ages 3 to 18 years, in Hong Kong. Optometricevaluations revealed that 18 children had normal visualacuity, 3 were far-sighted, and 3 were near-sighted. Allchildren were assessed on measures of spatial orienta-tion/spatial management abilities with two functionaltasks (i.e., television viewing and ball catching) duringeach of three visual assessment conditions: (1) habit-ual viewing (nolenses), (2) eyeglasses with prisms usingbase-up condition, or (3) eyeglasses with prisms usingbase-down conditions. Both prism conditions used a milddisplacement of the visual scene (5.6 degrees); however,one condition was judged to be the child’s favored orcorrect condition (facilitating lenses) and one was judgedto be an incorrect condition (interfering lenses) based onobservational measures during the trials by the initialrater. Assessments were videotaped. The full perfor-mance assessments were then reviewed by an indepen-dent rater, and results were analyzed statistically tovalidate whether or not the facilitating condition was su-perior. Results validated the initial rater’s assessment thathead position, body posture, facial expressions, and ballcatching skills significantly improved in the “facilitatinglens” condition as opposed to the habitual or interferinglens conditions.
Differences in the ages of the samples and the rel-ative strength of the methodological designs across thethree studies could have contributed to the inconsis-tent findings. The Kaplan et al. (1996) and the Car-mody et al. (2001) studies used considerably weakerdesigns with relatively short trial periods across thethree assessment conditions (i.e., no lenses, incorrectprism lenses or correct prism lenses). Replication stud-ies by independent investigators, using well-controlleddesigns and longer-term follow-up are needed. Likewise,

outcome measures used in naturalistic contexts areneeded to demonstrate generalizability of these findings.
Sensorimotor Handling Techniques
Description and Assumptions
Several types of sensorimotor handling techniques(e.g., reflex integration, neurodevelopmental therapies,patterning, etc.) have been applied to children with de-velopmental disabilities. Neurodevelopmental therapy(NDT) is a specific sensorimotor (physiotherapy)treatment that originated with the Bobaths in Englandin the 1950s–1960s. Its focus is on normalization ofmuscle tone, integration of primitive reflexes, and fa-cilitation of more normal movement patterns throughspecific handling techniques. Sensorimotor patterningis a remedial technique that uses a series of very struc-tured, passively manipulated exercises to the limbs toreprogram the central nervous system. Originally de-signed by Doman and Delcato in the 1950s–1960s, thistreatment is based on an older and simplistic recapitu-lation theory. Developmental gross motor patterns thatmay have been “missed” (e.g., creeping or crawling)are patterned passively for neurological reorganization.Although it is not used extensively for children withautism, there has been a recent resurgence of interest,particularly as a last-resort therapy. Although cranio-sacral (C-S) therapy (Upledger, 1996) is not a sensori-motor treatment per se, it’s similarities to otherhandling techniques combined with recent anecdotaldata of its increased use with children with autism war-ranted inclusion in this paper. This osteopathic treat-ment involves physical manipulation (e.g, repeatedtreatments using gentle and noninvasive traction anddecompressions) to alleviate restrictions in the cranio-sacral system.
Service Delivery Model and Approach
These interventions are administered individuallyby persons trained in the procedures through attendancein specialized workshops. Contact with the child mustbe direct physical contact. Interventions may be shortor long term for NDT or C-S. Home programs for pat-terning therapies are eventually carried out by familiesand tend to be particularly long in duration (8 hours perday for several months or years). Cost of treatments isdependent on frequency and duration (therapists’ fees).
Empirical Studies
No empirical studies specific to autism or relateddisorders (e.g., mental retardation) were found for NDT.
414 Baranek
From a clinical perspective, it appears that this treat-ment is rarely applied in any systematic way for usewith children with autism unless other accompanyingand significant neuromotor problems are present (e.g.,cerebral palsy). No empirical studies were found in peer-reviewed journals for C-S. No empirical studies of sen-sorimotor patterning were found specific to autism.However, two older empirical studies with children withmental retardation were found (Bridgman, Cushen,Cooper, & Williams, 1985; Neman et al., 1974). Bothstudies provide similar findings and limitations. In themore rigorous study (Neman et al., 1974), the pattern-ing group out-performed the other groups in visual com-petence and mobility. On other measures, the patterninggroup out-performed the passive control but not the al-ternative intervention group; no measurable differenceswere found in IQ, and no case made dramatic im-provement on any measure. Results from methodolog-ically weaker study (Bridgman et al., 1985) indicatedthat the treatment group slightly out-performed the con-trol group on language and socialization, whereas thecontrol group fared better in self-help skills. Given thatin both studies improvements were more pronounced inthe earlier assessments, it appears that findings may re-flect early enthusiasm of participants. High drop-outrates are particularly noted with this treatment method.
Physical Exercise
Description and Assumptions
Although physical exercise is included in manyregular education curricula, it is not systematically orconsistently utilized with children with autism. Healthbenefits of various exercise programs have been touted,including changes in physical as well as mental well-being. Researchers have been interested in the appli-cation of physical exercise particularly as it effectsmaladaptive or self-stimulatory behaviors. Assumptionsfrequently made are that aerobic exercise would di-minish stress or modulate self-stimulatory or hyper-active behavior through physiological changes relatedto release of neurotransmitters such as acetylcholine orbeta-endorphins.
Service Delivery Model and Approach
Physical education programs are provided easilyvia individual or group methods by teachers within aneducational curriculum given adequate physical space.Frequency or interventions vary from multiple timesper day to not at all. The majority of research studiesconducted utilize approximately 15 minutes of treat-ment time per day. The cost of providing services is

usually modest, although larger physical spaces areoften necessitated (e.g., running track or gym) in lieuof expensive equipment (e.g., exercise bicycle).
Empirical Studies
Four studies of the efficacy of physical exercisefor children with autism were found (Kern, Koegel, &Dunlap, 1984; Kern et al., 1982; Levinson & Reid,1993; Watters & Watters, 1980). All of these studiedeffects of antecedent exercises on self-stimulatory/stereotyped behaviors using some variation of single-subject designs with controls (e.g., alternating treat-ments designs). Two of these studies also measuredaspects of academic and play tasks in children withautism (Kern et al., 1982; Watters & Watters, 1980).All studies found some beneficial, albeit short-lived,effects of exercise for decreasing self-stimulatory be-haviors and mixed findings for improving other simplecognitive/play tasks. Effects were greater for more in-tensive aerobic activity (relative to mild exertion). Amaximum effect was noted at about 1 to 11⁄2 hours withattenuation over time. Limitations of these studies in-cluded relatively small sample sizes, large variability inthe independent measures, and the potential confoundsof extra attention/social interaction that may have con-tributed to the beneficial effects of the program. TheWatters & Watters (1980) study also concluded thatthere was no evidence to support that decreases in self-stimulatory behavior would automatically generalize toimproved academic performance. Two additional stud-ies on general physical education effectiveness for chil-dren with autism were found (Schleien, Heyne, & Berken,1988; Weber & Thorpe, 1992). Weber & Thorpe (1992)found that for older children (ages 11 to 15) greaterlearning/retention of gross motor skills occurred in atask variation condition. Schleien et al., (1988) foundthat physical education activities in an integrated phys-ical education class with typical children did not ap-pear to significantly affect performance of motor orplay skills over a short term (9-week intervention).Short treatment length or poor sensitivity of motor mea-sures may have limited the findings. It is also possiblethat general physical exercise and recreational activi-ties do not necessarily generalize to improving socialplay without specific play skills being taught within thecontext of treatment.
Other Categories of Sensory or MotorInterventions
Although searches were attempted for many otherspecific sensory-motor intervention categories (e.g., de-velopmental motor therapies, motor skills training,
Efficacy of Sensory and Motor Interventions for Children with Autism 415
compensatory approaches, etc.), no empirical studieson autism were found. Clinical observation suggeststhat providing developmental motor training (i.e., skillstraining in hierarchically sequenced developmentalstages) and compensatory teaching strategies are com-monly utilized approaches in many educational andtherapeutic programs for children with various diag-noses; thus it was surprising to find so little. However,it appears that these strategies are being provided aspart of a broader therapeutic consultation program orvia comprehensive educational models; thus empiricaldata specific to these components may be obscured inthe literature. Future reviews may wish to address thesecomponents more specifically.
SUMMARY OF EFFICACY OF SENSORY ANDMOTOR INTERVENTIONS
The theoretical strength of many sensory andmotor interventions, particularly sensory integration(SI), rests on empirical findings that children withautism indeed have measurable deficits in various sen-sory processing and motor functions. Some of the treat-ments reviewed (e.g., sensorimotor handling) providea questionable rationale for their use with children withautism and have no empirical evidence to evaluate theirefficacy with this population. In particular, sensorimo-tor patterning is based on an older neurological theorythat has been essentially disproven; several other pro-grams based on sensory integration theory also sufferfrom partially outdated assumptions and are being mod-ernized. Although the sheer volume of studies was lowacross categories reviewed, it was encouraging that sev-eral new studies were conducted in recent years. Find-ings from these studies were often mixed. Severalstudies in the area of SI, sensory stimulation, auditoryintegration training, prism lenses, and physical exer-cise yielded some positive, albeit modest outcomes;however, methodological constraints (e.g., use of smalland convenience samples, weak/uncontrolled designs,observer bias, etc.) limit conclusive statements and gen-eralizability of much of this work. In some areas, suchas AIT, a few well-controlled studies have been re-cently conducted but with little overwhelming supportfor the treatment.
The biggest limiting factor is that many studiesfail to directly link changes in the purported dysfunc-tional mechanism (e.g., auditory sensitivity, visual dis-tortions, vestibular dysfunction) to the functionalchanges in behavior. Studies either provide outcomemeasures of the proximate sensory behaviors (e.g., au-ditory sensitivity, arousal, tactile defensiveness) or the

broader functional behaviors (e.g., social interactions,play skills, academic performance), and rarely do theylink both in systematic and measurable ways. A fewpreliminary studies of AIT and sensory stimulationtreatments have attempted this; however, the results arestill tenuous and inconsistent across studies, indicatingneed for replications. Furthermore, it is still unclearwhat specific processes may be responsible for thegains reported, even in the studies that had reasonablecontrols and sample sizes. Are treatment effects trulyreflective of the intervention, or are there other non-treatment effects (e.g., parent’s expectations, matura-tion, imposed structure, added attention, practice, etc.)that influenced the results? Other aspects of the tasks,not central to the treatment protocol, may also be pro-ducing beneficial effects. For example, children in oneAIT study (Bettison, 1996) responded favorably underboth the treatment and the alternative condition, thus,processed (filtered/modulated) music did not appear tobe the critical treatment component. Although music“in general” may prove to be beneficial, an alternativeexplanation could involve the repeated demands forcompliance and structured attention to task that are notspecific to auditory processing. Another AIT study(Zollweg et al., 1997) demonstrated that both groupsimproved but the control group outperformed the treat-ment group on some measures, further questioning theefficacy of the treatment. Similarly, one of the coreprinciples and strengths of classical sensory integrationis that the therapy is child-directed and based in an in-dividualized play context. Thus, purported gains in en-gagement and functional play skills may be influencedby play coaching techniques employed by an experttherapist as much as they are by improvements in sen-sory processing per se.Only further research with ad-equate specificity and controls (e.g., multiple baselineconditions in single-subject designs) can tease apart theeffective from the noneffective components of theseinterventions.
Given that autistic symptoms are manifested dif-ferently across development and that heterogeneityexists within the autism spectrum, it is likely that indi-vidualized patterns of reactivity may be associated withdifferential treatment outcomes irrespective of the in-tervention category reviewed. Although outcomes forindividual children have been mixed, it is possible thatsignificant individual differences in subject character-istics may be masking significant group effects. That is,we don’t know which children will benefit the mostfrom which treatments and under which specific condi-tions. Several studies in the areas of SI and sensorystimulation indicated that specific sensory processing
416 Baranek
subtypes (e.g., hyper- versus hypo-responsive) and othersubject variables (e.g., age, developmental levels) mayaffect prognosis for treatment outcomes. Though smallsample sizes and retrospective designs limit generaliz-ability, there appeared to be some converging evidenceto suggest that a hyper-responsive pattern (i.e., high anx-iety, arousal, or sensitivities) may be more amenable tosensory techniques aimed at arousal modulation and re-sultant gains in performance. Physiological studies ofarousal indicate that younger (or less mature) childrenmay have a higher tendency to display hypersensitivereactions and reject sensory stimuli that interfere withother aspects of functioning. If so, one implication ofthese findings may be that perhaps beginning sometypes of sensory-motor interventions at earlier ageswould be more beneficial. Some studies have only beenconducted with older children and adults (e.g., exercisetreatments), and these results cannot be generalized topreschool populations. We cannot know the answers tothese types of questions until more systematic researchwith increased specificity of subject variables is con-ducted to help distinguish various levels of response totreatments; however, these findings indicate that whenprovided, sensory and motor interventions need to beindividualized for a given child with autism.
A further concern of this area of intervention is thatmost of the studies provide limited follow-up afterintervention, and so it is not known whether positiveeffects are sustained in the longterm. A few better-controlled follow-ups have been included in some of theAIT studies; however, in those studies in which positiveeffects were noted initially, an attenuation of responsesoccurred over time (over the course of 9 to 12 months).These types of findings were also true for one study onprism lenses and two on exercise treatments. This couldindicate that either the treatments were not useful in thelong term or, conversely, that more frequent applicationof treatment is needed to maintain such effects. Repeatedtreatments were certainly useful with exercise therapieswhere physiological and behavior changes were sus-tained for approximately 90 minutes following eachtreatment. The effects of treatment frequency, duration,and intensity on both short- and long-term outcomesneed to be further addressed.
Finally, issues of generalizability and feasibilityof sensory and motor interventions need to be addressedmore fully. The majority of studies across sensory andmotor treatment categories, particularly those con-ducted less recently, have not attempted to investigatebroader issues of generalizability. Two SI studies wereconducted in naturalistic contexts and documentedsome functional gains outside of the treatment context.

Others have been unable to prove that the interventionhas substantial effects on academic performance, beyondthe scope or context of the treatment per se.For exam-ple, several exercise studies have demonstrated positiveeffects on primary reduction of aberrant behaviors, butmore limited improvements in secondary effects onacademic skills, play, and recreation. AIT studiesdemonstrate much variability across studies and lack ofreplication for broader behavioral effects—in somecases, control treatments produced stronger reductionsin aberrant behaviors. Gains in areas of mastery play andengagement as a result of SI (i.e., Case-Smith & Bryan,1999) are interesting to note; however, it is not sur-prising that behaviors less directly addressed in the con-text of therapy (e.g., peer interactions and functionalcommunication) show the least improvement. Withoutdirect practice in generalizing to functional tasks andin naturalistic environments, the effects of therapeuticgains in sensory processing or motor components maybe limited. Studies of motor development in typicalchildren have demonstrated that behaviors emerge fromthe confluence of multiple dynamic systems; thus, task-relevant information and perceptions of affordances inthe environment can substantially alter movement pat-terns (Connolly & Elliott, 1989; Thelen & Ulrich,1991), and motor skills learned in one context may notautomatically generalize to naturalistic functional ac-tivities (Case-Smith, 1995). In fact, several studies havefound that performance of children with autism on goal-directed motor and imitation tasks appears to be betterin meaningful and purposeful contexts than in decon-textualized situations (e.g., Hughes & Russell, 1993;Rogers, et al., 1996; Stone, et al., 1997). Thus onewould expect that difficulties in applying newly ac-quired sensory or motor components to functional tasksand/or generalizing motor skills learned out of contextwould be magnified for children with autism.
The feasibility of carrying out specific sensory andmotor interventions varies tremendously and is depen-dent upon such variables as cost, qualifications ofneeded professionals, and congruence with the philo-sophical orientation of the broader educational pro-gram. With respect to cost, all treatments requirespecialized training and varying amounts of staff time;however, some require much more technologically so-phisticated and expensive equipment (e.g., AIT, HugMachine, prism lenses) than do others (e.g., massage,C-S). Some treatments (e.g., exercise therapies, someSI-based approaches, prism lenses) are certainly moreeasily administered within the context of inclusive ed-ucational programs than other treatments (e.g., senso-rimotor patterning). Of all the treatments summarized,
Efficacy of Sensory and Motor Interventions for Children with Autism 417
classical SI provides the strongest child-centered andplayful approach; this type of approach is often ap-pealing to even the most unmotivated or disengagedchild. In the case of sensory stimulation treatments(e.g., brushing, massage), AIT, patterning, and C-S, thechild must be able to tolerate various sensory applica-tions or physical manipulations provided by the thera-pist and usually in a restricted space. For some childrenwith autism, however, structure and repetition are notnecessarily aversive, although passive application ofstimulation may be; the effects on stress need to be doc-umented better in future studies. No negative side ef-fects have been reported in most of the literaturereviewed, with the exception of AIT, in which two stud-ies documented increased behavior problems and someadverse health effects with some children. In addition,compliance has been an issue in several treatments,such as limited tolerance for eyewear or headphones,causing drop-outs from treatment.
Feasibility solutions, however, must go beyondease of integration and cost effectiveness, they mustalso answer questions of best practice within the scopeof educational goals. Because most of these interven-tions are used to augment comprehensive educationalprograms, it is important to know whether or not thesetreatments actually facilitate progress or hinder it bytaking away valuable instruction time. The effects ofspecific sensory and motor interventions combined withvarious types of educational models need to be furtherinvestigated in large outcome studies. At least one casestudy report of three preschool children (Schwartzet al.,1998) indicates that there may be multiple meansto achieving promising outcomes in young childrenwith autism. Various combinations of specific inter-vention strategies (including SI in one case) were in-tegrated into the curriculum and produced positiveeffects. Although classical SI therapy originated witha clinic based, noninclusive model, newer approachesare attempting to utilize a more naturalistic context withsensory-based activities integrated into the classroomroutine. However, it will be important to investigate towhat degree specific treatments can be “altered” to fitan inclusive education model while still retaining theiressential therapeutic elements and purported benefits.Comparisons of such treatments need to be systemati-cally investigated in future efficacy research.
As Rogers (1998) eloquently summarized in her re-view of comprehensive educational programs, we mustkeep in mind that a lack of empirical data does not inferthat the treatment is ineffective, but rather that efficacyhas not been objectively demonstrated. Funding willbe critical to this increasingly urgent investigation.

Relying on nonharmful but potentially ineffective treat-ments can squander valuable time that could be used inmore productive educational or therapeutic ways. Giventhat at least some positive findings are noted with re-spect to the sensory and motor interventions reviewed,future research must move from the current level ofsmall-scale, poorly controlled, unsystematic studies ofeffectiveness, to a level that demands scientific rigorand well-controlled large-scale designs. Only such re-search can provide answers to important questions ofnot only what is effective but with whom and underwhat conditions.
RECOMMENDATIONS FOR EDUCATION
1. Although not all children with autism displaysensory processing and motor dysfunction,these types of difficulties are prevalent in thepopulation and are reported to interfere withperformance in many broader developmentaland functional domains. Therefore, at a mini-mum, “best practice” guidelines would indicatethat educational programs for young childrenwith autism need to incorporate appropriatelystructured physical and sensory environmentsthat accommodate these unique sensory pro-cessing patterns and provide opportunities fordevelopmentally appropriate sensory-motorexperiences within the context of functionaleducational goals.
2. Comprehensive educational programs may ben-efit from consultation with knowledgeable pro-fessionals (e.g., occupational therapists, speechand language therapists, physical therapists,adaptive physical educators, etc.) to provideguidance about potential interventions for chil-dren whose sensory processing or motoric diffi-culties interfere with educational performance,as well as to provide support for families strug-gling with these issues. It is important to notethat related services may provide many mean-ingful interventions that go well beyond thescope of this paper. Thus sensory and motor in-terventions are not synonymous with the termsfor professionals employing these interventions(e.g, occupational therapy, physical therapy, orspeech pathology); these terms should not be in-terchanged when making decisions for provisionof therapeutic services.
3. It is important to note that none of the specificinterventions reviewed claim to be a substitute
418 Baranek
for core educational curricula. If and when uti-lized, these should be viewed as supplementaryinterventions integrated at various levels into thebroader individualized educational program.
4. Specific task/environmental modifications forsensory processing or motoric deficits tend to bedescribed within the context of broader educa-tional approaches or in combination with spe-cific interventions more so than they are reportedin the empirical literature. For example, adapta-tions may take the form of changing performanceexpectations, modifying classroom activities tominimize negative sensory reactions, perceptualdistortions or motoric difficulties, teaching com-pensatory strategies, and/or maximizing thechild’s strengths to bypass sensory and motordifficulties and facilitate fuller participation.Such adaptations for sensory processing or motordifficulties would be feasible in many educa-tional programs and could be used in tandemwith other interventions.
5. Given the limited scientific basis of many of theremedial sensory and motor intervention ap-proaches reviewed in this paper, a conservativeapproach is recommended for prescribing spe-cific sensory or motor treatments. Best practicewould suggest that decisions be made on an in-dividualized clinical basis by expert profession-als. If indicated, it behooves the professional toprovide treatments in shorter-term increments(e.g., 6 to 12 weeks) and document progress ina systematic manner. Treatments need to be dis-continued if effects are not apparent within anexpected time frame or if negative reactions aredocumented. Certainly, regression in skills fol-lowing discontinuation of services merits specialattention.
6. With respect to specific interventions, the fol-lowing points are made:a. Most categories of sensory and motor inter-
ventions, including SI, sensory stimulationapproaches, AIT, and prism lenses haveshown mixed effects for children with autismprimarily through uncontrolled, descriptivestudies; large-scale experimental studies areoften lacking. Furthermore, beneficial effectsof sensory and motor treatments on atypicalbehaviors in some children have been shownto be short-lived in several studies that fol-lowed children longitudinally.
b. There is no available empirical evidence tosupport the use of sensorimotor handling

therapies for general educational purposesin young children with autism.
c. Potential risks of AIT (adverse side effects insome cases, lack of safeguards for hearingloss) need to be seriously weighed against thepotential benefits for each individual caseundergoing such an intervention.
d. SI and SI-based approaches appear to be rel-atively safe and anecdotally have shownsome benefits in a few children with autism.However, given the mixed findings acrossuncontrolled, small sample studies, thesetreatments need to be individually deter-mined and carefully monitored until better-controlled replication studies are completedwith children with autism.
e. Deciding how much to pull a child away fromhis or her educational program is a difficultdecision, and thus providing treatments withinthe context of an inclusive environment needsto be addressed.
7. Given the variability in developmental profilesof children with autism, it should be expectedthat not all children benefit equally from sen-sory or motor interventions. There is not a“one-size-fits-all” treatment for a diagnosis ofautism. Thus the indiscriminate use of any sen-sory- or motor-based intervention is unethical.Comprehensive assessments should be the basisfor service decisions, and, if necessary, sensoryand motor interventions must be prescribed inan individualized manner consistent with thefunctional goals for each child.
8. Although, in general, intervention strategiesneed to be developmentally appropriate, reme-diation of component-level sensory processingfunctions or developmental motor skills may notautomatically result in functional gains or gen-eralize to relevant contexts. Thus, best practicewould suggest that functional activities inte-grated into daily routines within naturalisticcontexts increase retention and generalizationof skills.
9. The paucity of available scientific research inthis area leaves many questions yet to be an-swered. However, these preliminary findingsmay provide direction for future studies. Thefollowing are recommended:a. Cross-sectional and longitudinal studies are
needed to document the developmental pro-gressions of unusual sensory processing fea-tures and qualitative motor functions and
Efficacy of Sensory and Motor Interventions for Children with Autism 419
their relationships to broader behavioral andeducational outcomes.
b. Replication studies by independent investi-gators are needed for all sensory and motortreatment categories that have shown posi-tive effects.
c. Methodologically more rigorous designs (e.g,multiple baseline single-subject designs; ran-domized controlled trials) with better-definedintervention components (duration/course,stimulus type/intensity/frequency, contextualconditions) and more reliable/valid and sys-tematic outcome measures are recommendedto directly test effects of a given treatment.
d. Studies that identify specific behavioral andphysiological patterns (individual differ-ences) that differentiate responders fromnonresponders to specific treatments arewarranted.
e. Studies linking the purported neurologicalmechanisms with both proximate measuresof the phenomenon and functional measuresof performance in broader domains (e.g., playskills, social skills, academic performance,independent functioning) are needed.
f. Studies providing information on earlier in-tervention, preventive benefits of sensoryand motor interventions, and/or long-termimpact on educational programming andfunctional outcomes of children in natural-istic contexts should be encouraged.
g. Studies documenting the relative contribu-tions of sensory or motor interventionswithin comprehensive educational curriculaare needed because it is unknown whethereducational goals are facilitated or inhibitedby these various interventions.
ACKNOWLEDGMENTS
I extend my gratitude to Alice Blair, Angela Suratt,and Lorin McGuire for their assistance in preparationof this manuscript. I also thank Ruth Humphry, LinnWakeford, Cathy Lord, Sally Rogers, and Pauline Fil-ipek for their helpful reviews. An earlier draft of thismanuscript was commissioned by the National Acad-emy of Sciences, National Research Council’s Com-mittee on Educational Interventions for Children withAutism, and presented at the first committee meetingin December of 1999.

REFERENCES
Adams, L. (1998). Oral-motor and motor-speech characteristics ofchildren with autism. Focus on Autism and Other Developmen-tal Disabilities, 13,108–112.
Adrien, J. L., Lenoir, P., Martineau, J., Perrot, A., Haneury, L., Lar-mande, C., & Sauvage, D. (1993). Blind ratings of early symp-toms of autism based upon family home movies. Journal of theAmerican Academy of Child and Adolescent Psychiatry, 33,617–626.
Adrien, J. L., Ornitz, E., Barthelemy, C., Sauvage, D., & Lelord, G.(1987). The presence or absence of certain behaviors associatedwith infantile autism in severely retarded autistic and nonautis-tic retarded children and very young normal children. Journalof Autism and Developmental Disorders, 17,407–416.
Adrien, J. L., Perrot, A., Sauvage, D., Leddet, I., Larmande, C.,Hameury, L., & Barthelemy, C. (1992). Early symptoms inautism from family home movies: Evaluation and comparisonbetween 1st and 2nd year of life using I.B.S.E. Scale. Acta Pae-dopsychiatrica: International Journal of Child and AdolescentPsychiatry, 55,71–75.
Amato, J., & Slavin, D. (1998). A preliminary investigation of oro-motor function in young verbal and nonverbal children withautism. Infant-Toddler Intervention 8,175–184.
Arendt, R. E., Maclean, W. E., & Baumeister, A. A. (1988). Critiqueof sensory integration therapy and its application in mental retar-dation. American Journal of Mental Retardation, 92,401–429.
Ayres, J. (1972). Improving academic scores through sensory inte-gration. Journal of Learning Disabilities, 5,338–343.
Ayres, A. J., & Tickle, L. S. (1980). Hyper-responsivity to touch andvestibular stimuli as a predictor of positive response to sensoryintegration procedures by autistic children. American Journalof Occupational Therapy, 34,375–381.
Baranek, G. T. (1999). Autism during infancy: A retrospective videoanalysis of sensory-motor and social behaviors at 9–12 monthsof age. Journal of Autism and Developmental Disorders, 29,213–224.
Baranek, G. T., Foster, L. G., & Berkson, G. (1997). Tactile defen-siveness and stereotyped behaviors. American Journal of Occu-pational Therapy, 51,91–95.
Bettison, S. (1996). The long-term effects of auditory training onchildren with autism. Journal of Autism and Developmental Dis-orders, 26,361–374.
Bridgman, G. D., Cushen, W., Cooper, D. M., & Williams, R. J. (1985).The evaluation of sensorimotor patterning and the persistence ofbelief. British Journal of Mental Subnormality, 31,67–79.
Brown, M. M. (1999). Auditory integration training and autism: Twocase studies. British Journal of Occupational Therapy, 62,13–17.
Bundy, A. C., & Murray, E. A. (2002). Sensory Integration: A. JeanAyre’s Theory Revisited. In A. C. Bundy, E. A. Murray & S.Lane (Eds.), Sensory integration: Theory and practice.Philadel-phia: F.A. Davis.
Carmody, D. P., Kaplan, M., & Gaydos, A. M. (2001). Spatial ori-entation adjustments in children with autism in Hong Kong.Child Psychiatry and Human Development, 31,233–247.
Case-Smith J. (1995). The relationships among sensorimotor com-ponents, fine motor skills, and functional performance inpreschool children. American Journal of Occupational Therapy,49, 645–652.
Case-Smith, J., & Bryan, T. (1999). The effects of occupational ther-apy with sensory integration emphasis on preschool-age chil-dren with autism. American Journal of Occupational Therapy,53, 489–497.
Clark, F. A., Miller, L. R., Kucherawy, D. A., & Azen, S. P. (1978).A comparison of operant and sensory integrative methods ondevelopmental parameters in profoundly retarded adults. Amer-ican Journal of Occupational Therapy, 32,86–92.
Connolly, K., & Elliott, J. (1989). The emergence of a tool-usingskill in infancy. Developmental Psychology, 25,894–912.
420 Baranek
Dahlgren, S. O., & Gillberg, C. (1989). Symptoms in the first twoyears of life. European Archives of Psychiatry and Neurologi-cal Science, 238,169–174.
DeMyer, M., Barton, S., & Norton, J. A. (1972). A comparison ofadaptive, verbal and motor profiles of psychotic and non-psychotic subnormal children. Journal of Autism and ChildhoodSchizophrenia, 2,359–377.
Edelson, S. M., Goldberg, M., Edelson, M. G., Kerr, D. C., &Grandin, T. (1999). Behavioral and physiological effects of deeppressure on children with autism: A pilot study evaluating theefficacy of Grandin’s Hug Machine. American Journal of Oc-cupational Therapy, 53,145–152.
Field, T., Lasko, P. M., Henteleff, T., Kabat, S., Talpins, S., & Dowl-ing, M. (1997). Brief report: Autistic children’s attentivenessand responsivity improve after touch therapy. Journal of Autismand Developmental Disorders, 27,333–339.
Gepner, B., Mestre, D., Masson, G., & de Schonen, S. (1995). Pos-tural effects of motion vision in young autistic children. Neuro-report, 6(8), 1211–1124.
Gillberg, C., Ehlers, S., Schaumann, H., Jakobsson, G., Dahlgren,S. O., Lindblom, R., Bagenholm, A., Tjuus, T., & Blidner, E.(1990). Autism under age 3 years: A clinical study of 28 casesreferred for autistic symptoms in infancy. Child Psychology andPsychiatry, 31,921–934.
Gillberg, C., Johansson, M., Steffenburg, S., & Berlin, O. (1997).Auditory integration training in children with autism: Brief re-port of an open pilot study. Autism, 1(1), 97–100.
Gravel, J. S. (1994). Auditory integrative training: Placing the bur-den of proof. American Journal of Speech and Language Pathol-ogy, 3,25–29.
Greenspan, S., & Weider, S. (1997). Developmental patterns and out-comes in infants and children with disorders in relating andcommunicating. A chart review of 200 cases of children withautistic spectrum diagnoses. Journal of Developmental andLearning Disorders, 1,87–141.
Hoehn, T. P., & Baumeister, A. A. (1994). A critique of the appli-cation of sensory integration therapy to children with learningdisabilities. Journal of Learning Disabilities, 27,338–350.
Hoshino, Y., Kumashiro, H., Yashima, Y., Tachibana, R., Watanabe,M., & Furukawa, H. (1982). Early symptoms of autistic chil-dren and its diagnostic significance. Folia Psychiatrica et Neu-rologica Japonica, 36,367–374.
Hughes, C., & Russell, J. (1993). Autistic children’s difficultywith mental disengagement from an object: Its implica-tions for theories of autism. Developmental Psychology, 29,498–510.
Humphries, T. W., Snider, L., & McDougall, B. (1993). Clinical eval-uation of the effectiveness of sensory integrative and perceptualmotor therapy in improving sensory integrative function in chil-dren with learning disabilities. Occupational Therapy Journalof Research, 13,163–182.
Humphries, T. W., Wright, M., McDougall, B., & Vertes, J. (1990).The efficacy of sensory integration therapy for children withlearning disability. Physical and Occupational Therapy in Pe-diatrics, 10,1–17.
Humphries, T. W., Wright, M., Snider, L., & McDougall, B. (1992).A comparison of the effectiveness of sensory integrative ther-apy and perceptual-motor training in treating children with learn-ing disabilities. Journal of Developmental and BehavioralPediatrics, 13,31–40.
Hutt, C., Hutt, S. J., Lee, D., & Ounsted, C. (1964). Arousal andchildhood autism. Nature, 204,909–919.
James, A. L., & Barry, R. J. (1984). Cardiovascular and electro-dermal responses to simple stimuli in autistic, retarded andnormal children. International Journal of Psychophysiology, 1,179–193.
Johnson, M. H., Siddons, F., Frith, U., & Morton, J. (1992). Canautism be predicted on the basis of infant screening tests? De-velopmental Medicine and Child Neurology, 34,316–320.

Jones, V., & Prior, M. (1985). A comparison of adaptive, verbaland motor profiles of psychotic and non-psychotic subnormalchildren. Journal of Autism and Childhood Schizophrenia, 2,359–377.
Kanter, R. M., Kanter, B., & Clark, D. L. (1982). Vestibular stimu-lation effect on language development in mentally retarded chil-dren. American Journal of Occupational Therapy, 36,46–41.
Kaplan, M., Carmody, D. P., & Gaydos, A. (1996). Postural orien-tation modifications in autism in response to ambient lenses.Child Psychiatry and Human Development, 2781–91.
Kaplan, M., Edelson, S. M., & Seip, J. L. (1998). Behavioral changesin autistic individuals as a result of wearing ambient transitionalprism lenses. Child Psychiatry and Human Development, 29,65–76.
Kern, L., Koegel, R. L., & Dunlap, G. (1984). The influence of vig-orous versus mild exercise on autistic stereotyped behaviors.Journal of Autism and Developmental Disorders, 14,57–67.
Kern, L., Koegel, L. R., Dyer, K., Blew, P. A., & Fenton, L. R.(1982). The effects of physical exercise on self-stimulation andappropriate responding in autistic children. Journal of Autismand Developmental Disorders, 12,399–419.
Kershner, J. R., Cummings, R. L., Clarke, K. A., Hadfield, A. J., &Kershner, B. A. (1990). Two year evaluation of the Tomatis lis-tening training program with learning disabled children. Learn-ing Disability Quarterly, 13,43–53.
Kientz, M. A., & Dunn, W. (1997). A comparison of the performanceof children with and without autism on the Sensory Profile.American Journal of Occupational Therapy, 51,530–537.
Kinsbourne, M. (1987). Cerebral-brainstem relations in infantileautism. In E. Schopler & G. B. Mesibov (Eds.), Neurobiologi-cal issues in autism(pp. 107–125). New York: Plenum Press.
Klin, A., Volkmar, F. R., & Sparrow, S. S. (1992). Autistic socialdysfunction: Some limitations of the theory of mind hypothe-sis. Journal of Child Psychology and Psychiatry, 33,861–876.
Kohen-Raz, R., Volkmar, F. R., & Cohen, D. (1992). Postural con-trol in children with autism. Journal of Autism and Develop-mental Disorders,22, 419–432.
Kootz, J. P., & Cohen, D. J., (1981). Modulation of sensory intakein autistic children: Cardiovascular and behavioral indices. Jour-nal of the American Academy of Child Psychiatry 20,692–701.
Kootz, J. P., Marinelli, B., & Cohen, D. J. (1982). Modulation of re-sponse to environmental stimulation in autistic children. Jour-nal of Autism and Developmental Disorders, 12,185–193.
Larrington, G. G. (1987). A sensory integration based program witha severely retarded/autistic teenager: An occupational therapycase report. In Z. Mailloux (Ed.), Sensory Integration Ap-proaches(pp. 101–117). New York: Hawthorn Press.
Le Couteur, A., Rutter, M., Lord, C., Rios, P., Robertson, S., Hold-grafer, M., & McLennan, J. (1989). Autism Diagnostic Inter-view: A standardized investigator-based instrument. Journal ofAutism and Developmental Disorders, 19,363–387.
Levinson, L. J., & Reid, G. (1993). The effects of exercise intensityon the stereotypic behaviors of individuals with autism. AdaptedPhysical Activity Quarterly, 10,(3), 255–268.
Lincoln, A. J., Courchesne, E., Harms, L., & Allen, M. (1995). Sen-sory modulation of auditory stimuli in children with autism andreceptive developmental language disorder: Event-related brainpotential evidence. Journal of Autism and Developmental Dis-orders, 25,521–539.
Linderman, T. M., & Steward, K. B. (1999). Sensory integrative-basedoccupational therapy and functional outcomes in young childrenwith pervasive developmental disorders: A single subject study.American Journal of Occupational Therapy, 53,207–213.
Link, H. M. (1997). Auditory integration training (AIT): Sound ther-apy—Case studies of three boys with autism who received AIT.British Journal of Learning Disabilities, 25,106–110.
Masterton, B. A., & Biederman, G. B. (1983). Proprioceptive versusvisual control in autistic children. Journal of Autism and Devel-opmental Disorders, 13,141–152.
Efficacy of Sensory and Motor Interventions for Children with Autism 421
McClure, M. K., & Holtz-Yotz, M. (1990). The effects of sensorystimulatory treatment on an autistic child. American Journal ofOccupational Therapy, 45,1138–1145.
Minshew, N. J., Goldstein, G., & Siegel, D. J. (1997). Neuropsycho-logic functioning in autism: Profile of a complex informationprocessing disorder. Journal of the International Neuro-psychological Society, 3,303–316.
Mudford, O. C., Cross, B. A., Breen, S., Cullen, C., Reeves, D.,Gould, J., & Douglas, J. (2000). Auditory integration trainingfor children with autism: No behavioral benefits detected. Amer-ican Journal on Mental Retardation, 105,118–129.
Neman, R., Roos, P., McCann, R. M., Menolascino, F. J., & Heal,L. W. (1974). Experimental evaluation of sensorimotor pat-terning used with mentally retarded children. American Journalof Mental Deficiency, 79,372–384.
Neysmith-Roy, J. M. (2001). The Tomatis method with severelyautistic boys: Individual case studies of behavioral changes.South African Journal of Psychology, 31,19–28.
Ohta, M., Nagai, Y., Hara, H., & Sasaki, M. (1987). Parental per-ception of behavioral symptoms in Japanese autistic children.Journal of Autism and Developmental Disorders, 17,549–563.
Ornitz, E. M., Guthrie, D., & Farley, A. H. (1977). The early devel-opment of autistic children. Journal of Autism and Develop-mental Disorders, 7,207–229.
Ottenbacher, K. (1982). Sensory integration therapy: Affect of effect.American Journal of Occupational Therapy, 36,571–578.
Perez, J. M., & Sevilla, M. (1993). Psychological assessment of ado-lescents and adults with autism. Journal of Autism and Devel-opmental Disorders, 23,653–664.
Polatajko, H. J., Kaplan, B. J., & Wilson, B. N. (1992). Sensory in-tegration treatment for children with learning disabilities: Itsstatus 20 years later. Occupational Therapy Journal of Research,12, 323–341.
Polatajko, H. J., Law, M., Miller, J., Schaffer, R., & Macnab, J.(1991). The effect of a sensory integration program on acade-mic achievement, motor performance, and self-esteem in chil-dren identified as learning disabled. Occupational TherapyJournal of Research, 11,155–176.
Porges, S. W. (1998). Love and the evolution of the autonomic ner-vous system: The Polyvagal theory of intimacy. Psychoneuro-endocrinology, 23,837–861.
Rapin, I. (1997). Autism. New England Journal of Medicine, 337,97–104.
Ray, T. C., King, L. J., & Grandin, T. (1988). The effectiveness ofself-initiated vestibular stimulation in producing speech soundsin an autistic child. Occupational Therapy Journal of Research,8, 187–190.
Reilly, C., Nelson, D. I., & Bundy, A. C. (1983). Sensorimotor ver-sus fine motor activities in eliciting vocalizations in autistic chil-dren. Occupational Therapy Journal of Research, 3,199–212.
Rimland, B. (1964). Infantile autism: The syndrome and its impli-cations for a neural theory of behavior.New York City:Appleton Century Crofts.
Rimland, B., & Edelson, R. (May, 1994). The effects of auditory in-tegration training on autism. American Journal of Speech andLanguage Pathology,18–24.
Rimland, B., & Edelson, S. (1995). Brief report: A pilot study of au-ditory integration training in autism. Journal of Autism and De-velopmental Disorders, 25,61–70.
Rinehart, N. J. Bradshaw, J. L., Brereton, A. V., & Tonge, B. J.(2001). Movement preparation in high-functioning autism andAsperger disorder: A serial choice reaction time task involvingmotor reprogramming. Journal of Autism and DevelopmentalDisorders, 31,79–88.
Rogers, S. J. (1998). Empirically supported comprehensive treat-ments for young children with autism Journal of Clinical ChildPsychology, 27,138–45.
Rogers, S. J., Bennetto, L., McEvoy, R., & Pennington, B. F.(1996). Imitation and pantomime in high-functioning adoles-

cents with autism spectrum disorders. Child Development, 67,2060–2073.
Scharre, J. E., & Creedon, M. P. (1992). Assessment of visual func-tion in autistic children. Optometry and Vision Science, 69,433–439.
Schleien, S. J., Heyne, L. A., & Berken, S. B. (1988). Integratingphysical education to teach appropriate play skills to learnerswith autism: A pilot study. Adapted Physical Activity Quarterly,5, 182–192.
Schwartz, I. S., Sandall, S. R., Garfinkle, A. N., & Bauer, J. (1998).Outcomes for children with autism: Three case studies. Topicsin Early Childhood Special Education, 18,132–143.
Smith, I. M., & Bryson, S. E. (1998). Gesture imitation in autism I:Nonsymbolic postures and sequences. Cognitive Neuropsycho-logy, 15,747–770.
Stagnitti, K., Raison, P., & Ryan, P. (1999). Sensory defensivenesssyndrome: A paediatric perspective and case study. AustralianOccupational Therapy Journal, 46,175–187.
Stone, W. L., Lemanek, K. L., Fishel, P. T., Fernandez, M. C., &Altemeier, W. A. (1990). Play and imitation skills in thediagnosis of autism in young children. Pediatrics, 86,267–272.
Stone, W. L., Ousley, O. Y., Hepburn, S. L., Hogan, K. L., & Brown,C. (1999). Patterns of adaptive behavior in very young childrenwith autism. American Journal of Mental Retardation, 104,187–199.
Stone, W. L., Ousley, O. Y., Littleford, C. D. (1997). Motor imita-tion in young children with autism: What’s the object? Journalof Abnormal Child Psychology, 25,475–485.
Thelen, E., & Ulrich, B. D. (1991). Hidden skills.Monograph of theSociety for Research in Child Development, 56 (pp. 1–98).Chicago: University of Chicago Press.
422 Baranek
Upledger, JE. (1996). An overview of craniosacral therapy: Its ori-gin and its applications for newborns and infants. Infants andYoung Children, 9,59–68.
Vargas, S., & Camilli, G. (1999). A meta-analysis of research on sen-sory integration treatment. American Journal of OccupationalTherapy, 53,189–198.
Volkmar, F. R., Cohen, D. J., & Paul, R. (1986). An evaluation ofDSM-III criteria for infantile autism. Journal of the AmericanAcademy of Child Psychiatry, 25,190–197.
Wainwright, J. A., & Bryson, S. E. (1996). Visual-spatial orientingin autism. Journal of Autism and Developmental Disorders, 26,423–438.
Watters, R. G., & Watters, W. E. (1980). Decreasing self-stimula-tory behavior with physical exercise in a group of autistic boys.Journal of Autism and Developmental Disorders, 10,379–387.
Weber, R. C., & Thorpe, J. (1992). Teaching children with autismthrough task variation in physical education. Exceptional Chil-dren, 59,77–86.
Wilson, B. N., Kaplan, B. J., Fellowes, S., Gruchy, C., & Faris, P.(1992). The efficacy of sensory integration treatment comparedto tutoring. Physical and Occupational Therapy in Pediatrics,12, 1–36.
Zentall, S. S., & Zentall, T. R. (1983). Optimal stimulation: A modelof disordered activity and performance in normal and deviantchildren. Psychological Bulletin, 94,446–471.
Zisserman, L. (1991). The effects of deep pressure on self-stimulatingbehaviors in a child with autism and other disabilities. AmericanJournal of Occupational Therapy, 46,547–551.
Zollweg, W., Palm, D., & Vance, V. (1997). The efficacy of auditoryintegration training: A double-blind study. American Journal ofAudiology, 6,39–47.

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.








![Temple Grandin Autism and my sensory based world[1].pdf](https://static.fdocuments.net/doc/165x107/577cd8791a28ab9e78a14915/temple-grandin-autism-and-my-sensory-based-world1pdf.jpg)









