Efficacy and side effects of botulinum toxin treatment for blepharospasm and hemifacial spasm
6
~ ~ ~~ - Original Articles Efficacy and side effects of botulinurn toxin treatment for blepharospasm and hemifacial spasm Jane Price, DipAppSci(Orth)* Justin O’Day, FRACO, FRACS, FRACPt Abstract Purpose: To analyse the effectiveness and rate of side effects of botulinum toxin treatment for blepharospasmand hemifacial spasm. Methods: In a prospective trial, 81 patients with blepharospasm and 70 with hemifacial spasm were treated with botulinum toxin A in the neuro- ophthalmology clinic at St Vincent’s Hospital, Melbourne. Some 989 treatments were given and the mean follow-up time was 28.7 months. Results: The duration of action was longer for patients with hemifacial spasm than for those with blepharospasm (median 12.0 weeks compared with 7.0 weeks, f<O.OOOI). There was no change in the duration of effect over time with repeated treatments of the same dose (F=0.4, b0.05). Once an effective dosage was reached, increasing the dose further did not prolong the duration of effect. There were no systemic side effects, but there were a number of local transient side effects. The most significant side effect was ptosis, which occurred in 12% of treatments given to those patients with blepharospasm and hemifacial spasm. Conclusion: Botulinum toxin is an effective treat- ment for blepharospasm and hemifacial spasm, but there are a number of side effects, the most signifi- cant being ptosis. Key words: Blepharospasm, botulinum toxin, hemifacial spasm, ptosis. Botulinum toxin A is one of several neurotoxins produced by the bacterium Clostridium botulinum. When injected locally, it causes progressive muscular paralysis by inhibiting the release of acetylcholine at the neuromuscular junction.’z2 The paralytic effect of botulinum toxin is tempo- rary and this effect lessens as there is resprouting at the neuromuscular junction.’ Botulinum toxin is quickly bound to the tissue surrounding the injection site and therefore there is little chance of producing systemic side effects, but a number of local side effects can occur.’-“ The first investigation of botulinum toxin for ocular complaints was by Scott in 1973.’ After injections of botulinum toxin into the extraocular muscle of monkeys, he noted that there were significant alterations in ocular alignment. From these observations, he proposed that botulinum toxin could be used as an alternative to stra- From St Vincent’s Hospital, Melbourne, Victoria. *Orthoptist. j-Head of Eye Department. Rfprints: Dr Justin O’Day, 55 Victoria Parade, Fitzroy, Victoria 3065. 255 Efficacy and side effects of botulinum toxin treattnent for blepharospasrn and hemifacial spasm
-
Upload
jane-price -
Category
Documents
-
view
212 -
download
0
Transcript of Efficacy and side effects of botulinum toxin treatment for blepharospasm and hemifacial spasm

~ ~ ~~ -
Original Articles
Efficacy and side effects of botulinurn toxin treatment for blepharospasm and hemifacial spasm
Jane Price, DipAppSci(Orth)* Justin O’Day, FRACO, FRACS, FRACPt
Abstract
Purpose: To analyse the effectiveness and rate of side effects of botulinum toxin treatment for blepharospasm and hemifacial spasm.
Methods: In a prospective trial, 81 patients with blepharospasm and 70 with hemifacial spasm were treated with botulinum toxin A in the neuro- ophthalmology clinic at St Vincent’s Hospital, Melbourne. Some 989 treatments were given and the mean follow-up time was 28.7 months.
Results: The duration of action was longer for patients with hemifacial spasm than for those with blepharospasm (median 12.0 weeks compared with 7.0 weeks, f<O.OOOI). There was no change in the duration of effect over time with repeated treatments of the same dose (F=0.4, b0 .05 ) . Once an effective dosage was reached, increasing the dose further did not prolong the duration of effect. There were no systemic side effects, but there were a number of local transient side effects. The most significant side effect was ptosis, which occurred in 12% of treatments given to those patients with blepharospasm and hemifacial spasm.
Conclusion: Botulinum toxin is an effective treat- ment for blepharospasm and hemifacial spasm, but there are a number of side effects, the most signifi- cant being ptosis.
Key words: Blepharospasm, botulinum toxin, hemifacial spasm, ptosis.
Botulinum toxin A is one of several neurotoxins produced by the bacterium Clostridium botulinum. When injected locally, it causes progressive muscular paralysis by inhibiting the release of acetylcholine at the neuromuscular junction.’z2 The paralytic effect of botulinum toxin is tempo- rary and this effect lessens as there is resprouting at the neuromuscular junction.’ Botulinum toxin is quickly bound to the tissue surrounding the injection site and therefore there is little chance of producing systemic side effects, but a number of local side effects can occur.’-“
The first investigation of botulinum toxin for ocular complaints was by Scott in 1973.’ After injections of botulinum toxin into the extraocular muscle of monkeys, he noted that there were significant alterations in ocular alignment. From these observations, he proposed that botulinum toxin could be used as an alternative to stra-
From St Vincent’s Hospital, Melbourne, Victoria. *Orthoptist. j-Head of Eye Department. Rfprints: Dr Justin O’Day, 55 Victoria Parade, Fitzroy, Victoria 3065.
255 Efficacy and side effects of botulinum toxin treattnent for blepharospasrn and hemifacial spasm

bismus surgery or for other disorders such as blepharospasm or lid retraction in endocrine exophthalmos. It was not until 1984 that botulinum toxin was used for the treatment of facial ~ p a s m . ~ ' ~
Blepharospasm
Blepharospasm is characterised by involuntary spasms of the orbicularis oculi and can be associ- ated with other d y s t o n i a ~ . ~ , ~ ~ In most cases there is no known cause, but it may occur with dysfunction of basal ganglia or the rostra1 midbrain. It may occur with disorders such as Parkinson's disease, Huntington's disease or progressive supranuclear palsy and can be drug- induced in tardive dyskinesia.11,12
Blepharospasm has been treated with selective facial nerve avulsion, a major surgical procedure which often produces only temporary Orbicularis stripping is another option which often results in fewer complications. Centrally acting drugs have also been used for the treat- ment of blepharospasm. These have been reported to have variable responses but are often used in conjunction with botulinum toxin treat- ment. Other treatments such as hypnotherapy, acupuncture and relaxation therapy have been used .3,9,L0
Hemifacial spasm
Hemifacial spasm is characterised by unilateral contractions of the muscles innervated by the facial nerv~e.~,'~ In a recent study, magnetic reso- nance tomographic angiography showed that up to 65% of patients with hemifacial spasm have ipsilateral compression of the facial nerve or pons.'* Rare causes include aneurysms and tumours of the cerebello-pontine angle. 1 5 - 1 9
Hemifacial spasm has been treated with facial nerve decompression but the spasm often returns and hearing loss and facial weakness can be compl i~a t ions .~~~~ Other treatments have been used such as selective facial neurectomy, but aberrant regeneration can be a complication. Centrally acting drugs have been used with limited success.
Patients, materials and methods
In a prospective trial, 151 outpatients with blepharospasm or hemifacial spasm were treated
with a total of 989 treatments with botulinum toxin A. The number of treatments per patient ranged from one to 27 in patients with blepharospasm and one to 16 in those with hemi- facial spasm. The mean follow-up was 28.7 months (range 1.6 to 53.0 months).
Patients were reviewed in the neuro-ophthal- mology clinic at St Vincent's Hospital and were asked to rate, on a scale of 0-4, how debilitated they were by the eyelid or facial spasm. This was done before treatment and after the first treat- ment. 0 = No inconvenience 1 = Minor inconvenience 2 = Some interference with lifestyle, e.g., decreases time able to read, drive or socially diffi- cult. 3 = Significant interference with lifestyle, e.g., significantly affects reading, driving. 4 = Severely affects lifestyle, e.g., unable to read, drive.
Most patients were seen for review one week after the first treatment. For all subsequent treat- ments, the patients were requested to phone at one week after treatment. Patients were asked to rate as a percentage how much subjective improvement there was in the spasm and if there were any complications as outlined in the infor- mation sheet. If there were any complications, these were noted and if necessary the patient was asked to be seen for review to document the changes. When the patient returned for further treatment the duration of effect of the previous treatment was ascertained.
The botulinum toxin was diluted according to the concentration required. Unpreserved saline was used to dilute the botulinum to concentra- tions of 2.5 units/O.l mL, 5 unitd0.l mL or 10 unitd0.l mL. At each injection site, 0.1 mL of botulinum toxin was injected and therefore, when patients required a larger dose the vials of higher concentration were used. Each injection was given using a 1 mL syringe and a 30-gauge needle.
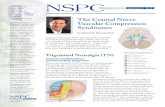
All patients were initially given a standard treatment regimen commencing with the lowest dose (2.5 units per site). For patients with blepharospasm, this was usually a total of 20 units. The injection sites can be seen in Figure 1. Initial standard treatment for blepharospasm is shown by sites denoted with 'A' with 2.5 units per site. If an increase in dose is required, sites
256 Australian and New Zealand Journal of Ophthalmology 1994; 22(4)

Y Figure 1 Injection sites for blepharospasm. Standard initial dose is represented by sites marked with ‘A’ with 2.5 units per site. For an increase in dose, sites marked with ‘B’ are included. If a further increase is necessary, sites marked ‘A’ are used but with 5 units per site and sites ‘B’
are included if this dose is not sufficient.
marked ‘By are included. For a further dose increase, sites marked with ‘A’ are used but with 5 units per site and sites ‘B’ are included if necessary. Each treatment is given twice before increasing the dose. A similar pattern of injection sites was used for patients with hemifacial spasm and the initial dose was 2.5 units per site and is shown by the site marked ‘A’ in Figure 2 . Extra injections into the upper cheek were used for persistent lower facial spasm.
If complications such as ptosis, facial weakness or diplopia arose, and this was disturbing to the patient or the side effect occurred for two succes- sive treatments, certain injection sites were omitted. For patients with hemifacial spasm who experienced facial weakness after treatment, the injection site in the upper cheek was omitted and if this persisted, further injections in the lower lid were also omitted.
For patients who experienced a ptosis which interfered with daily functioning or was cosmeti- cally unacceptable, the upper lid injection on the medial side was omitted and if ptosis still persisted, the upper lid injection on the lateral side was omitted. Ptosis was recorded as being present or absent, but was not graded according to severity. For cases where diplopia was experi- enced, the injection regimen varied according to which muscle was affected. In most cases this was the inferior oblique muscle or the superior rectus and the injections in those areas were omitted.
Figure 2 Injection sites for hemifacial spasm. Standard initial dose is represented by sites marked with ‘A’ with 2.5 units per site. Set pattern of increasing the dose is the same as for the blepharospasm patients. * Indicates additional
sites used for persistent facial spasm.
Results
There was a higher proportion of women to men in both groups, a ratio of 2.1:l for the blepharospasm group and 2.2: 1 in the hemifacial spasm group. In the blepharospasm group, there were seven patients with Meige’s syndrome and two patients with Parkinson’s disease. The average age of onset of disease was similar for the blepharospasm group (57.3f12.9 years) and the hemifacial spasm group (55.1f14.1 years).
Seven patients with blepharospasm and 13 with hemifacial spasm underwent surgery to alle- viate their eyelid or facial spasm. In the blepharospasm group, five had bilateral blepharoplasty and two had orbicularis stripping. In the hemifacial spasm group, nine had facial nerve decompression, two had selective facial nerve avulsion, one had a blepharoplasty and one had an orbicularis stripping procedure. Patients in both the blepharospasm and hemifa- cia1 spasm groups were less debilitated after treatment (Figures 3, 4).
In the blepharospasm group, 45% of the patients required an increase in dose from the standard treatment given on the first visit. A small proportion of the patients (8.6%) required more than 40 units in total to provide symp- tomatic relief. The range of dosages used is shown in Figure 5. For the hemifacial spasm group, most patients obtained symptomatic relief
Efficacy and side effects of botulinum toxin treatment for blepharospasm and hemifacial spasm 257

UI 3s
2 26
- 5 30 .- - e 0 20
5 15
z 5 10
S
0 20 30 40 60 80 0 1 2 3 4
Category
Figure 3 Debility rating for hemifacial spasm patients before and after treatment. n = 70 (1 not recorded).
on the standard dose (Figure 6). Only 8.6% required an increase in the dosage.
The duration of effect was significantly longer in the hemifacial spasm group compared with the blepharospasm patients using the Mann-Whitney test (median, 12.025.9 weeks compared with 7.0k5.5 weeks, W=154106, P<O.OOOl). There was a wide range of durations of effect from 0.5 to 64 weeks in the blepharospasm group and 0.5 to 41 weeks in the hemifacial spasm group.
There was no significant difference in the dura- tion of effect for 13 blepharospasm patients who received seven repeated treatments on the same dose (20 units) using a one-way ANOVA (F=0.4, -0.05). There was no linear correlation between the dose and duration (r= -0.1). Once an effective dosage was reached, increasing the dose further did not prolong the duration of effect.
The 13 hemifacial spasm patients who had previous surgery had 63 treatments with botulinum toxin. There was no difference in the duration of effect between the surgical group and
so 46 l P R E r n P O 8 1
d 40
.%! 3s 30
25
c)
5 20
E 15 3 z 10
6
0 0 1 2 3 4
Category
Figure 4 Debility rating for blepharospasm patients, before and after treatment. n = 81 (3 not recorded).
Total dose (units)
Figure 5 Current total dose of botulinum toxin used for blepharospasm patients. (n = 81 patients.)
the non-surgical group (T=0.9, -0.05). There was also no difference in the rate of side effects for the surgical group compared with the non- surgical group (x’ = 1.3, -0.05) and in partic- ular no significant increase in the rate of ptosis, which was 1 1 % for the surgical group and 9% for the non-surgical group (x’ = 0.2, -0.05).
There were a number of local side effects asso- ciated with the botulinum toxin treatment and these occurred in 38% of the treatments given to patients (Figure 7). Most side effects were minor, but ptosis and diplopia were quite debilitating in some cases. Other side effects included bruising, ectropion, photophobia, facial weakness, expo- sure keratitis, epiphora, dry eye and blurred vision. Ptosis occurred in 13% of treatments given to patients with blepharospasm and in 11% of treatments given to those with hemifacial spasm. Over all, ptosis occurred in 12% of treatments.
The major complication of botulinum toxin treatment was ptosis. After the first treatment, 12.2% of blepharospasm patients had a ptosis and by the sixth treatment, 46.3% of
I I
7.6 10 12.6 16 17.6 26 40
Total dose (units)
Figure 6 Current total dose of botulinum toxin used for hemifacial spasm patients. (n = 70 patients.)
258 Australian and New Zealand Journal of Ophthalmology 1994; 22(4)

None 62%
Blurred vision 3%
PtOSlS 12% Other 10%
Figure 7 Percentage of side effects for all treatments given to all patients.
blepharospasm patients had at least one episode of transient ptosis (Figure 8). Hemifacial spasm patients who had six consecutive treatments followed a similar pattern.
The rate of ptosis in the blepharospasm group remained the same (1 3%) for treatments given at doses of 40 units or greater (xz = 0.03, 130.05). Diplopia occurred in 2% of treatments for blepharospasm and hemifacial spasm patients.
There was one patient with hemifacial spasm who had selective facial nerve avulsion who subsequently went on to develop aberrant regeneration of the facial nerve. He developed prolonged weakness of the facial muscles after eyelid injection. This caused him to bite his oral mucosa when chewing.
Patients discontinued treatment for a number of different reasons. Nine patients from interstate continued treatment by an investigator in their State and six patients continued treatment with another investigator in Victoria. Eighteen patients (12%) discontinued treatment for reasons outlined in Table 1.
Discussion
Botulinum toxin A is an effective treatment for blepharospasm and hemifacial spasm. Most patients are less debilitated after treatment with botulinum toxin and the success of the treatment is reflected in the number of patients who return for repeated treatments. Only 12% of patients discontinued treatment over a 53-month period.
The duration of relief is temporary and the effect is longer in the hemifacial spasm group compared with the blepharospasm group. This is
E UI ’-1 80
0
f K ‘oo 20
0 1 2 3 4 8 8
Treatment number
Figure 8 Percentage of blepharospasm patients with at least one ptosis after six consecutive treatments (n = 41
patients.)
comparable with other s t u d i e ~ . ~ ~ - ~ ’ There is a wide variation in the duration of effect among patients in both groups. Forty-five per cent of the blepharospasm patients required an increase in the dose from the initial standard dose given on the first visit. Most hemifacial spasm patients experienced symptomatic relief on the standard dose given on the initial visit.
There was no significant change in the effect of botulinum toxin after seven repeated treatments with the same dose for the blepharospasm patients and this has been documented previ- ~ u s l y . ~ ~ ~ ~ ~ There was no linear correlation between the dosage and the duration of effect and therefore increasing the dose after an
Table 1. Reasons for 18 patients (12%) discontinuing treatment during the trial
Reason for discontinuing Number of treatment patients
Distance to travel outweighed benefit of
Side effects treatment 5
Ptosis 3 Rash 1
Wanted more definitive treatment 2 Surgery
Orbicularis stripping 1 Blepharoplasty 1
Other illnesses 2 Not debilitated by spasm, didn’t want
further treatment 2 Lost to follow-up 1
Efficacy and side effects Of botulinum toxin treatment for blepharospasm and hemifacial spasm 259

effective dosage was reached did not prolong the duration of effect.
The effect of botulinum toxin on the hemifacial spasm patients who had previous surgery was not
3. Osako M, Keltner JL. Botulinum A toxin (Oculinum) in ophthalmology. Surv Ophthalmol 199 1;36:28-46.
4. Patrinely JR, Whiting AS, Anderson RL. Local side effects of botulinum toxin injections. Adv Neurol 1988;49:493-9. - -
significantly different from those in the non 5. Dutton JJ, Buckley EG. Long-term results and complica- tions of botulinum A toxin in the treatment of blepharospasm. Ophthalmology 1988;95: 1529-34.
surgical group. There was also no increase in the number of side effects, in particular no increase 6. B~~~ CL, Gammon JA, Gemmill MC. Ptosis associated in the rate of ptosis. with botulinum toxin treatment of strabismus and
There were no systemic side effects from
number of local temporary side effects. The most
blepharospasm. Ophthalmology 1986;93: 1621-7. 7. Scott AB, Rosenbaum A, Collins CC. Pharmacologic
weakening of extraocular muscles. Invest Ophthalmol 1973; 12:924-7.
botulinum toxin injections but there were a
significant was ptosis which occurred in 12% of treatments given to blepharospasm patients and hemifacial spasm patients. Other studies have shown varying incidences of ptosis.4~”3J”*?2 The rate of ptosis did not increase with increasing doses in the blepharospasm patients. Diplopia was quite debilitating in some cases and this occurred in 2% of treatments. Other side effects included epiphora, local bruising, facial weak- ness, exposure keratitis, ectropion and other minor complications.
The blepharospasm patients in this trial were found to have dry eyes compared to the hemifa- cia1 spasm patients and this has been reported re~ently.’~ Therefore, it may be necessary to use artificial tears as a supplement to botulinum toxin treatment.
Conclusion
Botulinum toxin is an effective treatment for blepharospasm and hemifacial spasm. The effect is temporary and patients require repeated injections to maintain symptomatic relief. There are a number of local transient side effects which occur as a result of treatment which are minor in most cases, but complications such as ptosis and diplopia can be quite debilitating. Patients were likely to develop at least one ptosis the more treatments they had. Further evaluation of injection sites would be beneficial to provide an effective treatment with a reduced incidence of ptosis.
References 1. Melling J, Hambleton P, Shone CC. Clostridium
botulinum toxins: Nature and preparation for clinical use. Eye 1988;2;16-23.
2. Mackenzie I, Burnstock G. The effects of purified botulinum neurotoxin rype A on cholinergic, adrenergic and non-adrenergic, atropine resistant autonomic neuro- muscular transmission. Neuroscience 1982;7:997-1006.
8. Frueh BR, Felt DP, Wojno TH, Musch DC. Treatment of blepharospasm with botulinum toxin. A preliminary report. Arch Ophthalmol 1984;102: 1464-8.
9. Scott AB, Kennedy RA, Stubbs HA. Botulinum A toxin injection as a treatment for blepharospasm. Arch Ophthalmol 1985; 103:347-50.
10. Dutton JJ, Buckley EG. Botulinum toxin in the manage- ment of blepharospasm. Arch Neurol 1986;43:380-2.
11. Elston JS, Russell RW. Effect of treatment with botulinum toxin on neurogenic blepharospasm. BMJ 1985;99: 176-9.
12. Fahn S. Blepharospasm: a form of focal dystonia. Adv Neurol 1988;49:125-33.
13. Elston JS. Long-term results of treatment of idiopathic blepharospasm with botulinum toxin injections. Br J Ophthalmol 1987;7 1 :664-8.
14. Adler CH, Zimmerman RA, Savino PJ, Bernardi B, Bosley TM, Sergott RC. Hemifacial spasm: evaluation by magnetic resonance imaging and magnetic resonance tomographic angiography. Ann Neurol 1992;32:502-6.
15. Westra I, Drummond GT. Occult pontine glioma in a patient with hemifacial spasm. Can J Ophthalmol 199 1;26: 148-5 1.
Hemifacial spasm due to intracranial tumour. An international survey of botulinum toxin investigators. Ophthalmology 1988;95: 1042-5.
Hemifacial spasm associated with epidermoid tumours of the cerebellopontine angle. Neurology 1989;39:577-80.
18. Digre KB, Corbett JJ, Smoker WRK, McKusker S. C T and hemifacial spasm. Neurology 1988;38:1111-13.
19. Levin JM, Lee JE. Hemifacial spasm due to cerebello- pontine angle lipoma: Case report. Neurology 1987;37:337-9.
20. Moller M, Moller A. Loss of auditory function in microvascular decompression for hemifacial spasm. Neurosurgery 1985;63: 17-20.
2 1. Taylor J, Kraft S, et al. Treatment of blepharospasm and hemifacial spasm with botulinum toxin A: a Canadian multicentre study. Can J Ophthalmol 199 1;26: 133-8.
22. Mauriello JA, Aljian J. Natural history of treatment of facial dyskinesias with botulinum toxin: a study of 50 consecutive patients over seven years. Br J Ophthalmol 1991;75:737-9.
23. Mauriello JA, Coniaris H, Haupt EJ. Use of botulinum toxin in the treatment of one hundred patients with facial dyskinesias. Ophthalmology 1987;94:976-9.
24. Price J, O’Day J. A comparative study of tear secretion in blepharospasm and hemifacial spasm patients treated with botulinum toxin A. J Clin Neuro-ophthalmol 1993;13:67- 71.
16. Sprik C, Wirtschafter JD.
17. Auger RG, Piegras DG.
260 Australian and New Zealand Journal of Ophthalmology 1994; 22(4)