
Effects of patch or gel estrogen therapies on auditory brainstem response in surgically...
6
Effects of patch or gel estrogen therapies on auditory brainstem response in surgically postmenopausal women: a prospective, randomized study Salvatore Caruso, M.D., a Luigi Maiolino, M.D., b Carmela Agnello, M.D., a Aldo Garozzo, M.D., b Lucia Di Mari, M.D., a and Agostino Serra, M.D. b Department of Microbiological Science and Gynecological Science, University of Catania School of Medicine, Catania, Italy Objective: To study the effects of gonadal steroids on the nongenital audiological target in surgically postmenopausal women treated with patch or gel transdermal estrogen therapy (ET). Design: Prospective randomized study. Setting: Research Group for Sexology, University of Catania, Italy. Patient(s): One hundred twenty-two surgically postmenopausal women. Intervention(s): Transdermal E 2 by patch or gel, and evaluation of auditory brainstem response by auditory- evoked potentials for waves I, III, and V latencies, and for interpeak I–III, I–V, and III–V intervals. Main Outcome Measure(s): Changes in auditory wave latencies and in interpeak intervals during treatment with ET with respect to baseline levels. Result(s): One hundred two women completed the study. Forty-eight subjects used E 2 patches and 54 E 2 gel. No significant difference was observed in plasma E 2 improvement and in auditory brainstem response values with the two estrogen (E) formulations. The wave latencies and the interpeak intervals showed lower values during the E treatment than at baseline. Conclusion(s): Auditory brainstem response seems to depend on the type of E given. Our data suggest that fluctuating E levels act on waves, even if the exact mechanism of the gonadal steroids is not clear. However, we believe that E could influence neuronal plasticity, the metabolic levels of neurotransmitters, and thus, the neuronal conduction time into the audiological system. (Fertil Steril 2003;79:556 – 61. ©2003 by American Society for Reproductive Medicine.) Key Words: Auditory brainstem response, estrogen therapy (ET), hearing, surgically induced menopause After natural and surgically induced meno- pause, the subjective and objective complaints, as well as organic and metabolic organ dam- age, depend on estrogen (E) deficiency syn- drome (1). The changes that occur during menopausal transition and the postmenopausal period are a result of decreasing ovarian func- tion with a reduction in ovarian hormones, mainly E (2). Menopause transition is a time of changing hormone secretion and a time of in- creasing health and situational concerns, but it can also be a time for feeling well while chang- ing one’s lifestyle and possibly adding thera- pies to delay and reduce other diseases of later life (3). Menopause, as an E deficiency disease, if left untreated, might impair the health and well-being of climacteric and postmenopausal women (4 – 6). Hormone therapy (HT) may reduce the incidence of menopausal symptoms in women, and also have other important ben- efits on different nongenital targets, namely reducing postmenopausal bone loss and the incidence of cardiovascular disease (7, 8). Clinical observations strongly suggest that premenopausal and postmenopausal changes in gonadal function modify auditory (9, 10), ol- factory (11, 12), and taste (13) thresholds, and the trophic aspect of the larynx (14). However, the direct role of gonadal hormones on sensory processing, including the auditory system, has not been fully studied (9, 15). The influence of E on other gonadal steroid substances may Received January 15, 2002; revised and accepted September 11, 2002. Reprint requests: Salvatore Caruso, M.D., Ospedale S. Bambino, Via Torre del Vescovo, 95124 Catania, Italy (FAX: 39-095-312001; E-mail: [email protected]). a Research Group for Sexology, Department of Microbiological Science and Gynecological Science, University of Catania School of Medicine. b Department of Otorhinolaryngology, University of Catania School of Medicine. FERTILITY AND STERILITY VOL. 79, NO. 3, MARCH 2003 Copyright ©2003 American Society for Reproductive Medicine Published by Elsevier Science Inc. Printed on acid-free paper in U.S.A. 0015-0282/03/$30.00 doi:10.1016/S0015-0282(02) 04763-5 556
-
Upload
salvatore-caruso -
Category
Documents
-
view
214 -
download
1
Transcript of Effects of patch or gel estrogen therapies on auditory brainstem response in surgically...

Effects of patch or gel estrogen therapieson auditory brainstem response insurgically postmenopausal women: aprospective, randomized study
Salvatore Caruso, M.D.,a Luigi Maiolino, M.D.,b Carmela Agnello, M.D.,a
Aldo Garozzo, M.D.,b Lucia Di Mari, M.D.,a and Agostino Serra, M.D.b
Department of Microbiological Science and Gynecological Science, University of Catania School of Medicine,Catania, Italy
Objective: To study the effects of gonadal steroids on the nongenital audiological target in surgicallypostmenopausal women treated with patch or gel transdermal estrogen therapy (ET).
Design: Prospective randomized study.
Setting: Research Group for Sexology, University of Catania, Italy.
Patient(s): One hundred twenty-two surgically postmenopausal women.
Intervention(s): Transdermal E2 by patch or gel, and evaluation of auditory brainstem response by auditory-evoked potentials for waves I, III, and V latencies, and for interpeak I–III, I–V, and III–V intervals.
Main Outcome Measure(s): Changes in auditory wave latencies and in interpeak intervals during treatmentwith ET with respect to baseline levels.
Result(s): One hundred two women completed the study. Forty-eight subjects used E2 patches and 54 E2 gel.No significant difference was observed in plasma E2 improvement and in auditory brainstem response valueswith the two estrogen (E) formulations. The wave latencies and the interpeak intervals showed lower valuesduring the E treatment than at baseline.
Conclusion(s): Auditory brainstem response seems to depend on the type of E given. Our data suggest thatfluctuating E levels act on waves, even if the exact mechanism of the gonadal steroids is not clear. However,we believe that E could influence neuronal plasticity, the metabolic levels of neurotransmitters, and thus, theneuronal conduction time into the audiological system. (Fertil Steril� 2003;79:556–61. ©2003 by AmericanSociety for Reproductive Medicine.)
Key Words: Auditory brainstem response, estrogen therapy (ET), hearing, surgically induced menopause
After natural and surgically induced meno-pause, the subjective and objective complaints,as well as organic and metabolic organ dam-age, depend on estrogen (E) deficiency syn-drome (1). The changes that occur duringmenopausal transition and the postmenopausalperiod are a result of decreasing ovarian func-tion with a reduction in ovarian hormones,mainly E (2). Menopause transition is a time ofchanging hormone secretion and a time of in-creasing health and situational concerns, but itcan also be a time for feeling well while chang-ing one’s lifestyle and possibly adding thera-pies to delay and reduce other diseases of laterlife (3). Menopause, as an E deficiency disease,if left untreated, might impair the health and
well-being of climacteric and postmenopausalwomen (4–6). Hormone therapy (HT) mayreduce the incidence of menopausal symptomsin women, and also have other important ben-efits on different nongenital targets, namelyreducing postmenopausal bone loss and theincidence of cardiovascular disease (7, 8).
Clinical observations strongly suggest thatpremenopausal and postmenopausal changes ingonadal function modify auditory (9, 10), ol-factory (11, 12), and taste (13) thresholds, andthe trophic aspect of the larynx (14). However,the direct role of gonadal hormones on sensoryprocessing, including the auditory system, hasnot been fully studied (9, 15). The influence ofE on other gonadal steroid substances may
Received January 15,2002; revised andaccepted September 11,2002.Reprint requests: SalvatoreCaruso, M.D., Ospedale S.Bambino, Via Torre delVescovo, 95124 Catania,Italy (FAX: 39-095-312001;E-mail:[email protected]).a Research Group forSexology, Department ofMicrobiological Scienceand GynecologicalScience, University ofCatania School ofMedicine.b Department ofOtorhinolaryngology,University of CataniaSchool of Medicine.
FERTILITY AND STERILITY�VOL. 79, NO. 3, MARCH 2003
Copyright ©2003 American Society for Reproductive MedicinePublished by Elsevier Science Inc.
Printed on acid-free paper in U.S.A.
0015-0282/03/$30.00doi:10.1016/S0015-0282(02)04763-5
556

have direct effects on the cochlea and various central audi-tory system pathways; they could indirectly influence centralprocessing through other pathways and they could modulateblood flow in the cochlea and brain (15). A decrease in E andmetabolism rates could influence the availability of neuro-transmitters at the synapse and in turn influence neuralconduction time (16–19).
Advances in electronic and computer technology andtheir physiological application have made the detection ofsmall biological signals arising from within the nervoussystem possible. Since the brainstem potentials were de-scribed by Sohmer and Feinmesser (20) and by Jewett andWilliston (21), interest has continued to increase, both in theaudiological and the neurological fields. The auditory brain-stem response (ABR) by auditory-evoked potentials is ameasurement of the electrical activities generated in thebrainstem auditory pathways after auditory stimulation andrecorded from the surface of the scalp. Classification of theseauditory-evoked potentials has been based primarily on theirlatencies in relation to a previous stimulus. The responseconsists of five waves, I–V (21). The preponderance ofexperimental and clinical evidence suggests that wave I isgenerated by action potentials of the cochlear nerve, wave IIby the cochlear nucleus, wave III by the superior olivarycomplex, wave IV by the nucleus of the lateral lemniscus,and wave V by the inferior colliculus (21).
Data demonstrate that postmenopausal women showmore exaggerated ABR latencies and interpeak latenciesthan do younger women or men of all ages (22–24); there-fore, it has been hypothesized that this relationship couldchange with age (25–27). The source of these male–femalerelated differences could be factors such as hormones, headsize, skin thickness, or gender-dependent sizes of the exter-nal acoustic meatus (28), or even metabolic disorders (29). Ithas also been reported that there is a fluctuation in behavioralauditory thresholds during the menstrual cycle (17, 28–32).In a previous cross-sectional article of ours (9), we demon-strated that ABR wave and interpeak latencies in womenwho were treated with HT overlap those of younger women,and the postmenopausal women who did not take HT hadlonger wave latencies and interpeak intervals than the pre-menopausal women. Moreover, we noted that the averagesof wave and interpeak latencies were less in women whoused estrogen therapy (ET) than in women who used com-bined HT or sequential HT. To confirm our data, we wantedto study the changes in ABR in surgically induced post-menopausal women treated with ET by a prospective trial.
MATERIALS AND METHODS
The study was performed at the Research Group forSexology of the Department of Microbiological and Gyne-cological Science and at the Department of Otorhinolaryn-gology, University of Catania School of Medicine, Catania,
Italy. All subjects gave their written, informed consent be-fore participation in the study, which was conducted inaccordance with the Declaration of Helsinki and with theapproval of the institutional review board of the researchcommittees of both departments. The study was not adver-tised and no remuneration was offered.
SubjectsOne hundred twenty-two healthy hysterectomized women
ranging in age from 47 to 55 years (mean age, 52.6 years),who had been surgically menopausal for between 8 monthsand 5 years, and who were experiencing moderate to severemenopausal symptoms (Kupperman index �15, with �1 hotflushes with sweating per day) were screened for enrollmentinto the longitudinal study. Climacteric symptoms, for whichwomen required HT treatment, were hot flushes, nightsweating, sleep problems, vaginal dryness, and tiredness.Each subject had a surgical postmenopausal status by hys-terectomy and ovariectomy for benign gynecological diseasefor more than 6 months before inclusion in the study. Theplasma FSH levels were more than 40 IU/mL, and the serumE2 levels were less than 30 pg/mL. Inclusion criteria requireda normal gynecological history and examination, normalmammography result within 1 year, and no major abnormal-ity of serum glucose, lipids, or liver enzymes.
The following concomitant treatments were prohibited:any symptomatic treatment for climacteric symptoms, tran-quilizers, and antidepressant drugs. Any ear, nose, or throatproblem, any significant medical problem, or smoking anduse of drugs and alcohol excluded subjects from participa-tion. The body mass index of each woman was within thenormal range (mean � SD, 24.5 � 1.6 kg/m2).
Study DesignThe study was conducted as a randomized, two-treatment
arm study. The primary efficacy end point was the modifi-cations in the ABR during ET, and the secondary efficacyend point was the effects of each ET on wave latencies andinterpeak latencies. Before undergoing the audiometric tests,all women underwent ear, nose, and throat examinations tolook for inflammation of the upper airways. Subsequently,each woman underwent a pretreatment audiometric testingabout 4 weeks before enrollment, and then at the third monthof ET treatment. Measurements of plasma E2 levels wereperformed at the baseline and during the third month of ETtreatment.
ERTWomen were randomly allocated to one of two treatment
groups, and treatments were assigned to subjects in chrono-logical order of inclusion. Study therapy consisted of twomodalities of ET. Fifty-five women were treated with trans-dermal E2 patches and 55 women with transdermal E2 gel.The patches were changed once a week, and the gel was usedonce a day. The ET was used as a continuous regimen. Table1 shows the types of treatment used.
FERTILITY & STERILITY� 557

InvestigationsThe subjective thresholds were measured in each woman
for pure tones at 250, 500, 1,000, 2,000, and 4,000 Hz in asilent cabin with the Amplaid 311 (Amplifon, Milan, Italy)audiometer. The compliance of the tympanic cavity wasevaluated to identify eventual inflammation of the middleear. The stapedial reflex threshold was then measured toevaluate the correct functioning of the neuronal arc—theacoustic nerve, the reticular formation, and the facialnerve—with an Amplaid 711 (Amplifon) impedance audi-ometer. Finally, each woman, with her eyes closed, wasawake in a dark room, electrically and acoustically shieldedwith Amplaid MK 12 (Amplifon), and underwent the audi-tory brainstem test by auditory-evoked potentials.
The ABR was recorded with three surface electrodes(impedance �5 k�). The first was placed on the forehead(20% of nasion–inion length), the second on the ipsilateralmastoid, and the ground electrode was on the controlateralmastoid. The activity received from these electrodes wasrecorded by a differential amplifier and a second stage am-plifier; filters on both amplifiers were set at 100 and 3,000Hz. The acoustic stimuli were 100-dB sound pressure levelpeak emissions, alternated with clicks at 11/s produced bydelivering a 100-�s electrical square wave to a TDH-49earphone (Amplifon). A 2,000-stimuli presentation was per-formed.
The positive peak latencies of waves I, III, and V weremeasured using visual overlay cursors, and the interwavesI–III, I–V, and III–V intervals were calculated for eachresponse. Waves II and IV were not evaluated because oftheir lesser importance in ABR.
Statistical AnalysisAlthough the Kupperman index scores were not an end
point of this study, hot flushes was the symptom for whichwomen were enrolled in this study, although the scores werenot used to perform statistical analyses. The intention-to-
treat population was based on the efficacy and safety of ETused, with the last observation carried forward for patientswho prematurely discontinued treatment. However, the pri-mary end point was the outcome of the ABR values obtainedduring ET.
The within-group change with time of ABR values—obtained during the third month of ET treatment with respectto baseline values—was studied using a two-way ANOVAt-test. The difference between the two treatments was esti-mated with the 95% confidence interval (CI). The differ-ences were considered statistically significant for P�.05. Allstatistical analyses were carried out using a software packagefor Windows 95 (Glantz, Primer of Biostatistics, McGraw-Hill, Inc., New York, 1997).
RESULTSOf the 122 women screened, 110 were randomized to one
of the two treatment arms, and 12 (9.8%) were excludedfrom treatment for medical reasons. The intention-to-treatpopulation was 102 women; 18 of 110 women (17.6%)discontinued treatment prematurely: eight of them (7.8%)did not receive any treatment after baseline screening for fearof the HT drug. Ten (9.8%) withdrew during ET treatmentfor adverse events due to local intolerance to the patch(5/110), for lack of efficacy of the drug (3/110), or becausethey did not wish to continue treatment (2/110). Finally, 92of 110 women (90.1%) completed each audiometric test.Table 2 shows their baseline values. There were no signifi-cant differences between the two groups for demographic orclinical characteristics (one-way ANOVA).
Figure 1 shows the levels of E2 at baseline and at the thirdmonth of ET treatment. Both E2 patch and E2 gel groups hadan improvement in plasma E2 level with respect to baseline(58 � 3.9 pg/mL and 56 � 4.1 pg/mL, respectively; P�.05).Moreover, there were no statistically significant differencesbetween the groups. The average wave and interpeak laten-
T A B L E 1
Types of ET used for surgically postmenopausal women.
No ofusers E2 patch E2 hemihydrate patch E2 hemihydrate gel
15 Esclima 50 (10 mg)a
20 Climara 50 (3.9 mg)b
20 Zerella 50 (3.9 mg)c
21 Sandrena (1 g)d
34 Estrodose (0.75 mg)e
a Takeda, Rome, Italy.b Schering, Milan, Italy.c Theramex, Milan, Italy.d Organon, Rome, Italy.e Wyeth Lederle, Aprilia-Latina, Italy.
Caruso. Estrogen therapy and auditory brainstem response. Fertil Steril 2003.
T A B L E 2
Baseline characteristics of the randomized subjects bytwo treatment arms.
E2 patch(n � 48)
E2 gel(n � 54)
Age (y) 50.2 � 3.1a 50.9 � 2.8Body mass index (kg/m2) 24.7 � 1.4 24.3 � 1.5Age at menopause (y) 49.8 � 6.1 49.5 � 6.6Daily incidence of hot flushesb 5.6 � 3.2 5.3 � 3.6FSH (IU/mL) 60 � 0.3 58 � 8.4E2 (pg/mL) 21 � 3.2 23 � 2.2a Mean � SD.b In the week before enrollment.P is not significant.
Caruso. Estrogen therapy and auditory brainstem response. Fertil Steril 2003.
558 Caruso et al. Estrogen therapy and auditory brainstem response Vol. 79, No. 3, March 2003
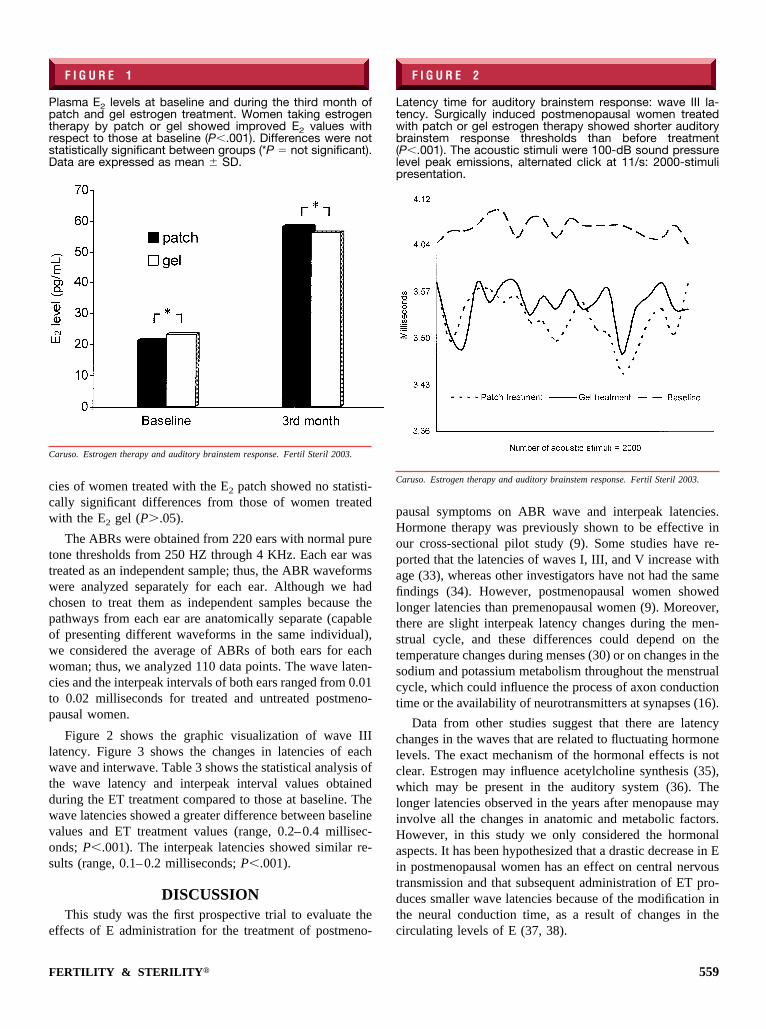
cies of women treated with the E2 patch showed no statisti-cally significant differences from those of women treatedwith the E2 gel (P�.05).
The ABRs were obtained from 220 ears with normal puretone thresholds from 250 HZ through 4 KHz. Each ear wastreated as an independent sample; thus, the ABR waveformswere analyzed separately for each ear. Although we hadchosen to treat them as independent samples because thepathways from each ear are anatomically separate (capableof presenting different waveforms in the same individual),we considered the average of ABRs of both ears for eachwoman; thus, we analyzed 110 data points. The wave laten-cies and the interpeak intervals of both ears ranged from 0.01to 0.02 milliseconds for treated and untreated postmeno-pausal women.
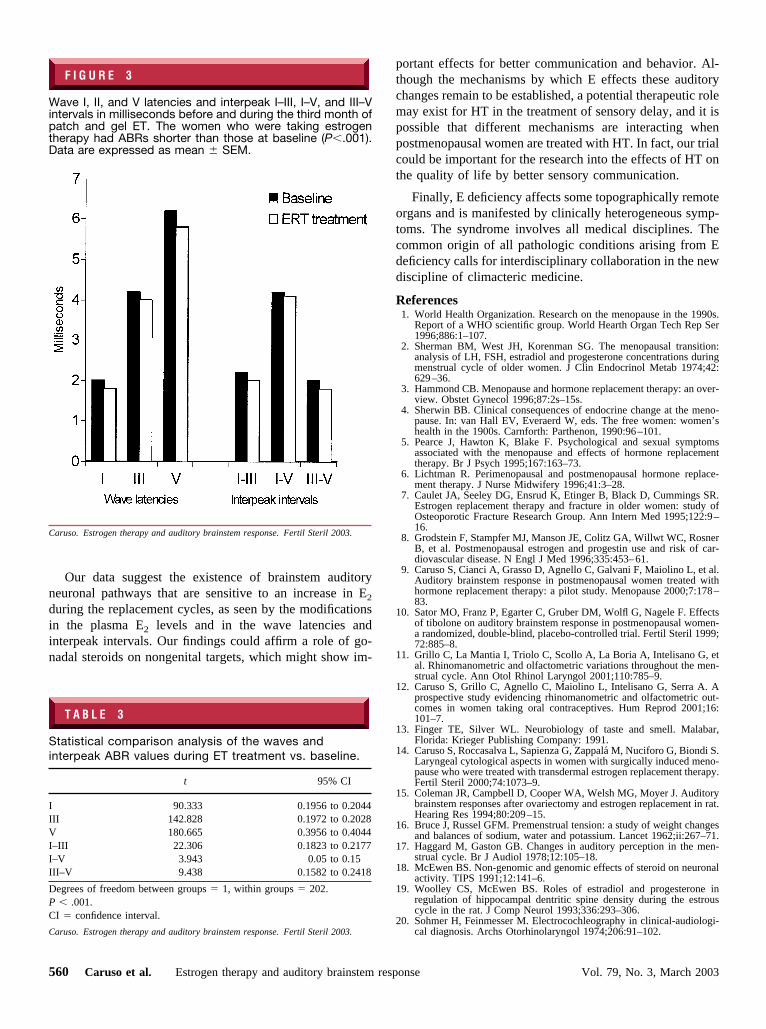
Figure 2 shows the graphic visualization of wave IIIlatency. Figure 3 shows the changes in latencies of eachwave and interwave. Table 3 shows the statistical analysis ofthe wave latency and interpeak interval values obtainedduring the ET treatment compared to those at baseline. Thewave latencies showed a greater difference between baselinevalues and ET treatment values (range, 0.2–0.4 millisec-onds; P�.001). The interpeak latencies showed similar re-sults (range, 0.1–0.2 milliseconds; P�.001).
DISCUSSIONThis study was the first prospective trial to evaluate the
effects of E administration for the treatment of postmeno-
pausal symptoms on ABR wave and interpeak latencies.Hormone therapy was previously shown to be effective inour cross-sectional pilot study (9). Some studies have re-ported that the latencies of waves I, III, and V increase withage (33), whereas other investigators have not had the samefindings (34). However, postmenopausal women showedlonger latencies than premenopausal women (9). Moreover,there are slight interpeak latency changes during the men-strual cycle, and these differences could depend on thetemperature changes during menses (30) or on changes in thesodium and potassium metabolism throughout the menstrualcycle, which could influence the process of axon conductiontime or the availability of neurotransmitters at synapses (16).
Data from other studies suggest that there are latencychanges in the waves that are related to fluctuating hormonelevels. The exact mechanism of the hormonal effects is notclear. Estrogen may influence acetylcholine synthesis (35),which may be present in the auditory system (36). Thelonger latencies observed in the years after menopause mayinvolve all the changes in anatomic and metabolic factors.However, in this study we only considered the hormonalaspects. It has been hypothesized that a drastic decrease in Ein postmenopausal women has an effect on central nervoustransmission and that subsequent administration of ET pro-duces smaller wave latencies because of the modification inthe neural conduction time, as a result of changes in thecirculating levels of E (37, 38).
F I G U R E 1
Plasma E2 levels at baseline and during the third month ofpatch and gel estrogen treatment. Women taking estrogentherapy by patch or gel showed improved E2 values withrespect to those at baseline (P�.001). Differences were notstatistically significant between groups (*P � not significant).Data are expressed as mean � SD.
Caruso. Estrogen therapy and auditory brainstem response. Fertil Steril 2003.
F I G U R E 2
Latency time for auditory brainstem response: wave III la-tency. Surgically induced postmenopausal women treatedwith patch or gel estrogen therapy showed shorter auditorybrainstem response thresholds than before treatment(P�.001). The acoustic stimuli were 100-dB sound pressurelevel peak emissions, alternated click at 11/s: 2000-stimulipresentation.
Caruso. Estrogen therapy and auditory brainstem response. Fertil Steril 2003.
FERTILITY & STERILITY� 559
Our data suggest the existence of brainstem auditoryneuronal pathways that are sensitive to an increase in E2
during the replacement cycles, as seen by the modificationsin the plasma E2 levels and in the wave latencies andinterpeak intervals. Our findings could affirm a role of go-nadal steroids on nongenital targets, which might show im-
portant effects for better communication and behavior. Al-though the mechanisms by which E effects these auditorychanges remain to be established, a potential therapeutic rolemay exist for HT in the treatment of sensory delay, and it ispossible that different mechanisms are interacting whenpostmenopausal women are treated with HT. In fact, our trialcould be important for the research into the effects of HT onthe quality of life by better sensory communication.
Finally, E deficiency affects some topographically remoteorgans and is manifested by clinically heterogeneous symp-toms. The syndrome involves all medical disciplines. Thecommon origin of all pathologic conditions arising from Edeficiency calls for interdisciplinary collaboration in the newdiscipline of climacteric medicine.
References1. World Health Organization. Research on the menopause in the 1990s.
Report of a WHO scientific group. World Hearth Organ Tech Rep Ser1996;886:1–107.
2. Sherman BM, West JH, Korenman SG. The menopausal transition:analysis of LH, FSH, estradiol and progesterone concentrations duringmenstrual cycle of older women. J Clin Endocrinol Metab 1974;42:629–36.
3. Hammond CB. Menopause and hormone replacement therapy: an over-view. Obstet Gynecol 1996;87:2s–15s.
4. Sherwin BB. Clinical consequences of endocrine change at the meno-pause. In: van Hall EV, Everaerd W, eds. The free women: women’shealth in the 1900s. Carnforth: Parthenon, 1990:96–101.
5. Pearce J, Hawton K, Blake F. Psychological and sexual symptomsassociated with the menopause and effects of hormone replacementtherapy. Br J Psych 1995;167:163–73.
6. Lichtman R. Perimenopausal and postmenopausal hormone replace-ment therapy. J Nurse Midwifery 1996;41:3–28.
7. Caulet JA, Seeley DG, Ensrud K, Etinger B, Black D, Cummings SR.Estrogen replacement therapy and fracture in older women: study ofOsteoporotic Fracture Research Group. Ann Intern Med 1995;122:9–16.
8. Grodstein F, Stampfer MJ, Manson JE, Colitz GA, Willwt WC, RosnerB, et al. Postmenopausal estrogen and progestin use and risk of car-diovascular disease. N Engl J Med 1996;335:453–61.
9. Caruso S, Cianci A, Grasso D, Agnello C, Galvani F, Maiolino L, et al.Auditory brainstem response in postmenopausal women treated withhormone replacement therapy: a pilot study. Menopause 2000;7:178–83.
10. Sator MO, Franz P, Egarter C, Gruber DM, Wolfl G, Nagele F. Effectsof tibolone on auditory brainstem response in postmenopausal women-a randomized, double-blind, placebo-controlled trial. Fertil Steril 1999;72:885–8.
11. Grillo C, La Mantia I, Triolo C, Scollo A, La Boria A, Intelisano G, etal. Rhinomanometric and olfactometric variations throughout the men-strual cycle. Ann Otol Rhinol Laryngol 2001;110:785–9.
12. Caruso S, Grillo C, Agnello C, Maiolino L, Intelisano G, Serra A. Aprospective study evidencing rhinomanometric and olfactometric out-comes in women taking oral contraceptives. Hum Reprod 2001;16:101–7.
13. Finger TE, Silver WL. Neurobiology of taste and smell. Malabar,Florida: Krieger Publishing Company: 1991.
14. Caruso S, Roccasalva L, Sapienza G, Zappala M, Nuciforo G, Biondi S.Laryngeal cytological aspects in women with surgically induced meno-pause who were treated with transdermal estrogen replacement therapy.Fertil Steril 2000;74:1073–9.
15. Coleman JR, Campbell D, Cooper WA, Welsh MG, Moyer J. Auditorybrainstem responses after ovariectomy and estrogen replacement in rat.Hearing Res 1994;80:209–15.
16. Bruce J, Russel GFM. Premenstrual tension: a study of weight changesand balances of sodium, water and potassium. Lancet 1962;ii:267–71.
17. Haggard M, Gaston GB. Changes in auditory perception in the men-strual cycle. Br J Audiol 1978;12:105–18.
18. McEwen BS. Non-genomic and genomic effects of steroid on neuronalactivity. TIPS 1991;12:141–6.
19. Woolley CS, McEwen BS. Roles of estradiol and progesterone inregulation of hippocampal dentritic spine density during the estrouscycle in the rat. J Comp Neurol 1993;336:293–306.
20. Sohmer H, Feinmesser M. Electrocochleography in clinical-audiologi-cal diagnosis. Archs Otorhinolaryngol 1974;206:91–102.
F I G U R E 3
Wave I, II, and V latencies and interpeak I–III, I–V, and III–Vintervals in milliseconds before and during the third month ofpatch and gel ET. The women who were taking estrogentherapy had ABRs shorter than those at baseline (P�.001).Data are expressed as mean � SEM.
Caruso. Estrogen therapy and auditory brainstem response. Fertil Steril 2003.
T A B L E 3
Statistical comparison analysis of the waves andinterpeak ABR values during ET treatment vs. baseline.
t 95% CI
I 90.333 0.1956 to 0.2044III 142.828 0.1972 to 0.2028V 180.665 0.3956 to 0.4044I–III 22.306 0.1823 to 0.2177I–V 3.943 0.05 to 0.15III–V 9.438 0.1582 to 0.2418
Degrees of freedom between groups � 1, within groups � 202.P � .001.CI � confidence interval.
Caruso. Estrogen therapy and auditory brainstem response. Fertil Steril 2003.
560 Caruso et al. Estrogen therapy and auditory brainstem response Vol. 79, No. 3, March 2003

21. Jewett DL, Williston JS. Auditory evoked far fields averaged from thescalp of human. Brain 1971;94:681–96.
22. Wharton JA, Church GT. Influence of menopause on the auditorybrainstem response. Audiology 1990;29:196–201.
23. Jerger J, Hall JW. Effect of age and sex on the auditory brainstemresponse. Arch Otolaryngol 1980;106:387–91.
24. Dehan CP, Jerger J. Analysis of gender differences in the auditorybrainstem response. Laryngoscope 1990;100:18–24.
25. Jerger J, Johnson K. Interaction of age, gender, and sensorineuralhearing loss on ABR latency. Ear Hear 1988;9:168–75.
26. O’Donovan CA, Beagley HA, Shaw M. Latency of brainstem responsein children. Br J Audiol 1980;14:23–9.
27. Rosenhamer HJ, Lindstrom B, Lundborg T. On the use of click-evokedelectrical brainstem responses in audiological diagnosis. II. The influenceof sex and age upon the normal response. Scand Audiol 1980;9:93–100.
28. Trune DN, Miehell C, Phillips DS. The relative importance of headsize, gender and age on auditory brainstem response. Hearing Res1988;32:165–74.
29. Baker MA, Weiler EM. Sex of listener and hormonal correlated ofaudiotory thresholds. Br J Audiol 1977;11:65–8.
30. Fagan PA, Church GT. Effect of the menstrual cycle on the auditorybrainstem response. Audiology 1986;25:321–8.
31. Elkin-Hirsch KE, Stoner WR, Stach BA, Jerger JF. Estrogen influencesauditory brainstem response during the normal menstrual cycle. Hear-ing Res 1992;60:143–8.
32. Elkind-Hirsch KE, Wallace E, Stach BA, Jerger JF. Cyclic steroidreplacement alters auditory brainstem response in young women pre-mature ovarian failure. Hearing Res 1992;64:93–8.
33. Patterson JV, Michalewski HJ, Thompson LW, Bowman TE, LitzelmanDK. Age and sex differences in the human auditory brainstem response.J Gerontol 1981;36:455–62.
34. Baegley HA, Sheldrake JB. Differences in brainstem response latencywith age and sex. Br J Audiol 1978;12:69–77.
35. Picton TW, Stapells DR, Campbell KB. Auditory evoked potentialsfrom the human cochlea and brainstem. J Otolaryngol (Suppl) 1981;9;1–41.
36. Weinberger NM, Bakin JS. Learning-induced physiological memory inadult primary auditory cortex: exceptive field plasticity, model, andmechanisms. Audiol Neurootol 1998;3:145–67.
37. Lagrange AH, Wagner EJ, Ronneklein OK, Kelly MJ. Estrogen rapidlyattenuates a GABAB response in hypothalamic neurons. Neuroendo-crinology 1996;64:114–23.
38. Murphy DD, Cole NB, Greenberger V, Segal M. Estradiol increasesdentritic spine density by reducing GABA neurotransmission in hip-pocampal neurons. J Neurosci 1998;18:2550–9.
FERTILITY & STERILITY� 561


















