Effects of Dietary or Supplementary Micronutrients on Sex ... · via supplementation of vitamins...
21
nutrients Review Effects of Dietary or Supplementary Micronutrients on Sex Hormones and IGF-1 in Middle and Older Age: A Systematic Review and Meta-Analysis Ryan Janjuha 1 , Diane Bunn 2 , Richard Hayhoe 1 , Lee Hooper 1 , Asmaa Abdelhamid 1 , Shaan Mahmood 1 , Joseph Hayden-Case 1 , Will Appleyard 1 , Sophie Morris 1 and Ailsa Welch 1, * 1 Norwich Medical School, University of East Anglia, Norwich Research Park, Norwich, Norfolk NR4 7TJ, UK; [email protected] (R.J.); [email protected] (R.H.); [email protected] (L.H.); [email protected] (A.A.); [email protected] (S.M.); [email protected] (J.H.-C.); [email protected] (W.A.); [email protected] (S.M.) 2 School of Health Sciences, University of East Anglia, Norwich Research Park, Norwich, Norfolk NR4 7TJ, UK; [email protected] * Correspondence: [email protected]; Tel.: +44-1603591950 Received: 12 March 2020; Accepted: 6 May 2020; Published: 18 May 2020 Abstract: Observational research suggests that micronutrients may be protective for sarcopenia, a key health issue during ageing, potentially via effects on hormone synthesis and metabolism. We aimed to carry out a systematic review of RCTs investigating effects of increasing dietary or supplemental micronutrient intake on sex hormones and IGF-1 in individuals aged 45 years or older. We searched MEDLINE, EMBASE and Cochrane databases for RCTs reporting the effects of different micronutrients (vitamins A, C, D, or E; carotenoids; iron; copper; zinc; magnesium; selenium; and potassium) on sex hormones or IGF-1. Of the 26 RCTs identified, nine examined effects of vitamin D, nine of multi-nutrients, four of carotenoids, two of selenium, one of zinc, and one of vitamin E. For IGF-1 increasing vitamin D (MD: -0.53 nmol/L, 95% CI: -1.58, 0.52), multi-nutrients (MD: 0.60 nmol/L, 95% CI -1.12 to 2.33) and carotenoids (MD -1.32 nmol/L; 95% CI -2.76 to 0.11) had no significant effect on circulating concentrations. No significant effects on sex hormones of other micronutrients were found, but data were very limited. All trials had significant methodological limitations making effects of micronutrient supplementation on sex hormones unclear. Further high quality RCTs with physiological doses of micronutrients in people with low baseline intakes or circulating concentrations, using robust methodology, are required to assess effects of supplementation adequately. Keywords: micronutrients; sarcopenia; sex hormones; insulin-like growth factor 1; meta-analysis; randomized controlled trials 1. Introduction Sarcopenia is a major problem, involving loss of skeletal muscle mass and function with age, a process beginning at approximately 40 years in both men and women [1–3]. One mechanism for its onset, is the age-related decline in the endocrine system, including the secretion of sex hormones and insulin-like growth hormone-1 (IGF-1) [4]. Recent evidence suggests that certain micronutrients may be protective for sarcopenia, and also important for hormone synthesis and metabolism, particularly during the decrease in endogenous secretion that occurs during aging [4]. This decrease in hormone secretion is also associated with increases in risks of falls, osteoporosis, fractures, cardiovascular disease and all-cause mortality [5–16]. Nutrients 2020, 12, 1457; doi:10.3390/nu12051457 www.mdpi.com/journal/nutrients
Transcript of Effects of Dietary or Supplementary Micronutrients on Sex ... · via supplementation of vitamins...

nutrients
Review
Effects of Dietary or Supplementary Micronutrientson Sex Hormones and IGF-1 in Middle and OlderAge: A Systematic Review and Meta-Analysis
Ryan Janjuha 1, Diane Bunn 2, Richard Hayhoe 1, Lee Hooper 1 , Asmaa Abdelhamid 1,Shaan Mahmood 1, Joseph Hayden-Case 1, Will Appleyard 1, Sophie Morris 1 andAilsa Welch 1,*
1 Norwich Medical School, University of East Anglia, Norwich Research Park, Norwich, Norfolk NR4 7TJ, UK;[email protected] (R.J.); [email protected] (R.H.); [email protected] (L.H.);[email protected] (A.A.); [email protected] (S.M.);[email protected] (J.H.-C.); [email protected] (W.A.); [email protected] (S.M.)
2 School of Health Sciences, University of East Anglia, Norwich Research Park, Norwich,Norfolk NR4 7TJ, UK; [email protected]
* Correspondence: [email protected]; Tel.: +44-1603591950
Received: 12 March 2020; Accepted: 6 May 2020; Published: 18 May 2020�����������������
Abstract: Observational research suggests that micronutrients may be protective for sarcopenia,a key health issue during ageing, potentially via effects on hormone synthesis and metabolism.We aimed to carry out a systematic review of RCTs investigating effects of increasing dietary orsupplemental micronutrient intake on sex hormones and IGF-1 in individuals aged 45 years or older.We searched MEDLINE, EMBASE and Cochrane databases for RCTs reporting the effects of differentmicronutrients (vitamins A, C, D, or E; carotenoids; iron; copper; zinc; magnesium; selenium; andpotassium) on sex hormones or IGF-1. Of the 26 RCTs identified, nine examined effects of vitamin D,nine of multi-nutrients, four of carotenoids, two of selenium, one of zinc, and one of vitamin E. ForIGF-1 increasing vitamin D (MD: −0.53 nmol/L, 95% CI: −1.58, 0.52), multi-nutrients (MD: 0.60 nmol/L,95% CI −1.12 to 2.33) and carotenoids (MD −1.32 nmol/L; 95% CI −2.76 to 0.11) had no significanteffect on circulating concentrations. No significant effects on sex hormones of other micronutrientswere found, but data were very limited. All trials had significant methodological limitations makingeffects of micronutrient supplementation on sex hormones unclear. Further high quality RCTs withphysiological doses of micronutrients in people with low baseline intakes or circulating concentrations,using robust methodology, are required to assess effects of supplementation adequately.
Keywords: micronutrients; sarcopenia; sex hormones; insulin-like growth factor 1; meta-analysis;randomized controlled trials
1. Introduction
Sarcopenia is a major problem, involving loss of skeletal muscle mass and function with age,a process beginning at approximately 40 years in both men and women [1–3]. One mechanism for itsonset, is the age-related decline in the endocrine system, including the secretion of sex hormones andinsulin-like growth hormone-1 (IGF-1) [4]. Recent evidence suggests that certain micronutrients maybe protective for sarcopenia, and also important for hormone synthesis and metabolism, particularlyduring the decrease in endogenous secretion that occurs during aging [4]. This decrease in hormonesecretion is also associated with increases in risks of falls, osteoporosis, fractures, cardiovascular diseaseand all-cause mortality [5–16].
Nutrients 2020, 12, 1457; doi:10.3390/nu12051457 www.mdpi.com/journal/nutrients

Nutrients 2020, 12, 1457 2 of 21
The endocrine system decline with age [4] includes a decrease in testosterone concentrations of0.5%–1% per year in men, and of oestrogen in women, that begins around 30 years of age [17,18]. Thedecline in testosterone concentrations in men is associated with loss of muscle mass and strength [19,20],and furthermore testosterone/dihydrotestosterone (DHT) supplementation can increase musclestrength [21]. Similarly, oestrogen concentrations, which decline more rapidly during the menopausein women [22], are closely linked to muscle strength [23]. Evidence from randomised controlled trials(RCTs) suggests oestrogen replacement therapy reduces the decline in strength of post-menopausalwomen [22] via a reduction in ‘FOXO3’ activation and ‘MuRF1’ protein expression [24].
The concentration of other endocrine hormones, (Dehydroepiandrosterone, DHEAS; Sex-HormoneBinding Globulin, SHBG; and Insulin-like Growth Factor-1, IGF-1) are also associated with skeletalmuscle [25,26] and may be involved in the aetiology of sarcopenia since circulating concentrationschange with age. DHEAS [27] is converted into the active forms of testosterone and oestrogen,and stimulates production of IGF-1 [18], declines with age and relates to loss of muscle mass andstrength [17]. SHBG transports testosterone, oestrogen, and other steroids in the blood, and increaseswith age thus reducing free testosterone and oestrogen [28–30]. The age-related decline in IGF-1 [31] isrelevant due to its roles in promoting myoblast proliferation and differentiation, as well as formationof muscle fibres during normal growth, and in response to injury [32]. Alongside improving musclehypertrophy and strength, IGF-1 also suppresses muscle inflammation and fibrosis, and is associatedwith skeletal muscle mass and strength [32–36]. Therefore, increasing concentrations of circulatingIFG-1 and sex hormones may be potentially beneficial for preventing sarcopenia as well as certainnon-communicable diseases and conditions of aging.
Micronutrients are potentially important for sex hormone synthesis and metabolism, particularlyduring the age-related decline in the endocrine system. Previous research from in-vitro, in-vivoor observational studies found that certain micronutrients including vitamin D [37–47], vitaminE [48–50], vitamin A [51], lycopene [52], iron [53], magnesium [54–56], selenium [57–60] orzinc [58,60–67] were associated with either androgen metabolism, testosterone concentrations orSHBG. Associations have also been found between oestrogen and vitamins C, D, E, A, and carotenoids,including lycopene [48,68–71]. IGF-1 has also been associated with lycopene [72–75], magnesium [55],selenium [57] or zinc [61,62,76,77], iron/ferritin [78] and copper [79]. These studies indicate therelevance of micronutrients to the endocrine system, although many were in individuals in youngadulthood and their effects in older age have been less studied to date.
The mechanisms for the role of micronutrients in synthesis of sex hormones and IGF-1 includethe involvement in steroidogenesis, via the involvement of prostaglandins, on the precursors ofsex hormones, for vitamins D, E, the carotenoids, zinc and selenium, as well the effects of vitaminC [38–50,52,60,64,65,68,69,71,79–86], and effects on transporter proteins. Zinc is also an inhibitor oftwo enzymes, aromatase and 5α-reductase, that are involved in testosterone metabolism [60].
Intake of micronutrients, micronutrient deficiency, as well as protein intake, may be also importantin determining the onset of sarcopenia [38,76,77,87–96]. Recent observational and animal studiesfound that vitamins C, D, E, and carotenoids and the minerals magnesium, selenium, iron and zincare relevant to muscle mass and physical performance [76,77,88,89,92,97–99]. The mechanisms forthe action of these nutrients include involvement in collagen and carnitine synthesis, for vitamin C,activities on skeletal muscle cell differentiation and proliferation, for vitamin D [38] and synthesis ofprotein and mitochondrial function, for magnesium [38,76,77,87–97].
Further mechanisms for changes in hormones and the musculoskeletal system that occur duringaging are the associated increases in low grade circulating inflammatory cytokines and of ROS(Reactive Oxygen Species) [93]. A number of micronutrients act as endogenous antioxidants with thecapacity to reduce ROS and circulating inflammatory cytokines. These micronutrients include vitaminsA, C, E [100,101], the carotenoids [100–105], zinc [60,106], magnesium [55] and selenium [57,60].Therefore, improving intakes or rectifying micronutrient deficiency could potentially affect both theonset of sarcopenia as well as sex hormone and IGF-1 metabolism, via a number of mechanisms, during

Nutrients 2020, 12, 1457 3 of 21
aging. Improvements in micronutrient intake could be achieved through increased consumption ofdietary whole foods, e.g., oranges (rich in vitamin C); or via supplementation of vitamins and minerals,e.g., single component or multivitamin tablets.
A number of micronutrients have antioxidant activity with the capacity to reduce ROSand circulating inflammatory cytokines. These micronutrients are vitamin A [100,101], thecarotenoids [100,101], vitamin C [102,103], vitamin E [104,105], zinc [106], magnesium [55] andselenium [57]. Therefore, rectifying micronutrient deficiency could potentially affect both the onsetof sarcopenia as well as sex hormone and IGF-1 metabolism during aging. This can typically beachieved through increased consumption of dietary whole foods, e.g., oranges (rich in vitamin C); orvia supplementation of vitamins and minerals, e.g., single component or multivitamin tablets.
We are unaware of any previous systematic reviews that have investigated the importance ofmicronutrient intakes on sex hormones and IGF-1 in middle and older aged people at risk of sarcopenia.Therefore, given the potential role for micronutrients to influence secretion of these hormones duringaging, and the importance of these sex hormones to the aetiology of sarcopenia, we conducteda systematic review (SR) to investigate the effects of dietary or supplemental intake of specifiedmicronutrients and changes in concentration of sex hormones and IGF-1. We included adults aged45 years or older, since this is the age at which recognisable declines in muscle mass and function, sexhormones and IGF-1 start to occur [107].
2. Materials and Methods
The systematic review was conducted in accordance with the Cochrane collaborationguidelines and reported using the PRISMA 2009 checklist [108,109]. The protocol was registeredwith the International prospective register of systematic reviews (PROSPERO), registration ID:CRD42018098657 [110].
2.1. Search Methods
Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, and EMBASE weresearched to 2nd April 2019 using the ‘Population, intervention, comparators, outcomes, study design’(PICOS) Framework (see Table 1) without date restrictions. The search strategy can be viewed inSupplementary Appendix A, but in brief, a MEDLINE search was developed and adapted for EMBASEand Cochrane, and search limiters were used for RCTs as per the ‘Scottish Collegiate Network’ [111].
Table 1. PICO Framework for search strategy. See Supplementary Tables (Table S1, A–Table S5, E),for further details.
P Humans, adults only, aged >45 years.
I Micronutrients
C -
O Sex hormones and IGF-1
S Randomised controlled trials (RCTs)
2.2. Eligibility Criteria
We included randomised controlled trials (RCTs) that assessed the effects of additionalmicronutrients in adults aged at least 45 years on primary outcomes. The primary outcomeswere changes or differences in sex hormone concentrations, including: androgens (androstenediol,androstenedione, dihydrotestosterone and testosterone), oestrogens (E2, estradiol, estriol, and estrone),DHEAS, SHBG, and IGF-1 (see Supplementary Table S1, A). Relevant micronutrients were thosewith known or potential relevance to sex hormone or IGF-1 metabolism and physiology, as wellas sarcopenia, and included any one, or combination, of vitamin A [48,69]; vitamin C [76]; vitaminD [38–47]; vitamin E [48,50]; carotenoids [69]; or the minerals zinc [64,65], magnesium [54], selenium,potassium [76,77], iron/ferritin [78] and copper [79].

Nutrients 2020, 12, 1457 4 of 21
Where studies included groups of individuals with varying age ranges, they were included if themean age was greater than 45 years, or more than 75% of individuals were older than 45 years (in bothtreatment arms). We included studies that used any micronutrient or hormone extraction method,including biomarkers from blood, plasma, red blood cells, body fat, urine, hair, and nails. We excludedstudies where the age of the population was unclear, or where participants stopped, started, or changed,hormonal medication, during a study. Where RCTs examined micronutrients in conjunction withanother intervention, e.g., exercise, the study was included only if the comparator group receivedthe same non-dietary intervention. Studies that included participants on active dialysis, or withkidney or liver disease [112], were excluded as these are known to affect endogenous sex hormonesand IGF-1 [113,114]. In-vitro studies and studies that used foods as interventions without a reporteddose of an eligible nutrient were also excluded. We accepted trials of multivitamins or multi-nutrientstudies that included further compounds, other than the micronutrients previously listed. This isbecause some studies may have used combined vitamins for an intervention and provided information.Studies that fell into this category were reported separately, and were defined as two or more differentmulti-nutrients in the intervention group compared to placebo. We excluded non-English languagepapers that we were unable to translate within the research team.
2.3. Study Selection
Study selection was conducted in a two-phase process. Screening of titles and abstracts againstinclusion/exclusion criteria (Supplementary Table S2, B) was carried out independently by tworeviewers (RJ and one of DB, AA, RH, AW, SM, JC, WA). Potential titles and abstracts identified by anyreviewer were collected in full text and subsequently assessed against the inclusion/exclusion criteriaby at least 2 reviewers. Any disagreements were discussed, a third reviewer was not needed to clarifyconsensus on eligibility.
2.4. Data Extraction
We created and tested a data extraction form for this review (Supplementary Table S3, C).Data extracted included: publication details, aims, objectives, country, setting, design, dates,funding, recruitment method, ethical review, participant demographics, intervention descriptions(including: micronutrient type and extraction methods) and outcomes (method of extraction andhormone type). Data extraction and risk of bias assessment was completed independently in duplicateby RJ and another review team member. We were unable to contact authors on any queries regardingdata due to time constraints.
2.5. Risk of Bias (Quality Assessment)
Risk of bias assessment was based on the Cochrane Risk of Bias tool (https://handbook-5-1.cochrane.org/chapter_8/table_8_5_a_the_cochrane_collaborations_tool_for_assessing.htm) (SupplementaryTable S4, D) [115]. Alongside the typical seven standard domains, we included three further items:‘hormonal treatment’ bias, where participants may be taking medication(s) that influence sex hormones;‘sponsorship’ bias, where funding by companies may have influenced the outcome of results; and‘outcome measurement’ bias, which concerns the differences in accuracy of extraction methods. TheJournal of Clinical Endocrinology and Metabolism [116] recommends measurement of sex hormones tobe conducted using mass spectrometry, as this conveys the highest degree of accuracy, and lowest bias.Studies that used other (less reliable) methods of hormone extraction, e.g., direct immunoassay [117] orelectro chemiluminescent assay [118], were assessed to be at high risk of outcome measurement bias.
2.6. Data Synthesis and Statistical Analysis
Meta-analyses were performed only where at least two trials could be combined. We used arandom effects model in ‘Review Manager (RevMan) [Computer program] [119]. We produced theforest plots using ‘end data’ for intervention and placebo groups. Outcomes were ‘continuous’ and

Nutrients 2020, 12, 1457 5 of 21
data for IGF-1, testosterone, and SHBG, reported in non-standard units were converted using anonline tool (http://unitslab.com/node/230). Where meta-analysis was not possible or data could notbe converted or utilised, results were narratively reported. Some studies reported data as ‘median’values so could not be included in a meta-analysis, but have been included in some forest plots tohelp illustrate overall effects. Sensitivity analysis, using fixed-effects meta-analysis, was carried outwhere at least two trials were combined. Comparison between random and fixed effects meta-analysisallowed small study bias to be assessed [120]. We also intended to use funnel plots to assess smallstudy (publication) bias; but as no meta-analysis included at least 10 studies, this was not useful.
3. Results
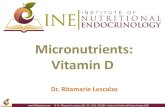
A total of 7623 titles and abstracts were identified from the three separate databases. After theremoval of duplicates, 5444 papers remained, of which 5043 were excluded based on title and abstractscreening. The remaining 400 studies were assessed in full text, leaving a total of 26 eligible studies.The majority of excluded studies (n = 374) were excluded due to the population age or study design.A summary overview of the selection process is provided in Figure 1.Nutrients 2020, 10, x FOR PEER REVIEW 6 of 23
Figure 1. PRISMA Flowchart.
Records identified through database searching
n = 647 (Cochrane)
n = 3460 (Embase)
n = 3516 (Medline)
Scre
enin
g Id
entif
icat
ion
Records after duplicates removed
(n =5444)
Records screened
(n =5444)
Records excluded based on title and
abstract.
(n = 5044)
Full-text articles assessed for
eligibility
(n =400)
Full-text articles excluded, with reasons
(n = 374)
Elig
ibili
ty
Incl
uded
Randomised Controlled Trials
(n = 26)
Vitamin D = 9;
Multi-nutrient = 9;
Carotenoids = 4;
Selenium = 2;
Zinc = 1;
Vitamin E = 1.
Figure 1. PRISMA Flowchart.
The 26 eligible RCTs examined a range of micronutrients: vitamin D (9, 35%), multi-nutrients(9, 35%), carotenoids (4, 15%), selenium (2, 8%), vitamin E (1, 4%) and zinc (1, 4%). Briefly, a total of

Nutrients 2020, 12, 1457 6 of 21
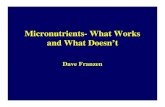
2443 participants were examined. Interventions ranged from 4 weeks to 48 months and participantswere mostly males (~64%). Some studies (9, 35%) included individuals who either had a histologicaldiagnosis of prostate cancer or colon cancer, evidence of increasing prostate specific antigen (PSA),or a family history of cancer. Other studies (8, 31%) examined individuals with metabolic syndrome(including obesity) and/or cardiovascular disease. Different races/ethnic groups were also studied,including: Asian, Black, Latino and White. Details of the study characteristics can be found inSupplementary Table S5, E. An overview of the risk of bias for RCTs is shown in Figure 2. We found notrials assessing effects of vitamins A or C, potassium, iron or copper on our outcomes.
Nutrients 2020, 10, x FOR PEER REVIEW 7 of 23
Figure 2. Risk of bias of included RCTs, assessed for each domain and each included trial, based on the Cochrane Risk of Bias tool [120]. +: low risk of bias ?: unclear risk of bias, -: high risk of bias. Carot, carotenoids; multi, multi-nutrient; vit D, vitamin D; vit E, vitamin E. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
Figure 2. Risk of bias of included RCTs, assessed for each domain and each included trial, based on theCochrane Risk of Bias tool [120]. +: low risk of bias, ?: unclear risk of bias, -: high risk of bias. Carot,carotenoids; multi, multi-nutrient; vit D, vitamin D; vit E, vitamin E. Please refer to SupplementaryTable S5, E to find detailed information on the studies and the reference number.

Nutrients 2020, 12, 1457 7 of 21
3.1. Risk of Bias of Included RCTs
Methods of minimising selection bias were poorly reported, with 54% (14/26) and 77% (20/26) ofRCT studies being unclear in methodology of ‘randomisation’ and ‘allocation concealment’, respectively(Figure 2). Many studies (58%, or 15/26) minimised performance bias by blinding participants andstudy personnel, and a smaller proportion (42%, or 11/26) successfully reported blinding of outcomes.Incomplete outcome data was minimised, as was the influence of hormonal treatments on sexhormones (mainly through comprehensive exclusion criteria). Only a small proportion of studies(~12%) advised participants to change their dietary habits in addition to any intervention or placebo.The majority of studies (88%, or 23/26) reported serum blood concentrations, with 12% (3/26) estimatingmicronutrient intake from dietary assessment questionnaires. Although extraction using serumanalysis for micronutrients may pick up coagulants and other trace elements, there appears to be anon-significant variation between plasma and serum values. It is unclear whether the coagulants ortrace elements would influence supplemented or non-supplemented cohorts differently. It is worthnoting, Olmedilla-Alonso et al. [121] found retinol, gamma- and alpha-tocopherol serum values werepositively biased (mean difference of less than: 0.05, 0.01 and 0.7 mol/L, respectively) when comparedto plasma values [121]. However, this is unlikely to influence our results as we only identified one trialwith vitamin E within our systematic review. Only 8% (2/26) of studies measured sex hormones usingthe gold standard recommendation of mass spectrometry [122].
3.2. Vitamin D
Nine studies assessed effects of vitamin D on relevant outcomes [116,123–130] but no studiesassessed effects on androstenediol, androstenedione, dihydrotestosterone, estriol, or DHEAS. Vitamin Ddoses varied from 100 IU [130], through 1000 IU [125], 4000 IU [129], 20,000 IU [128] up to 40,000 IU [123],and one was unclear [126]. Baseline vitamin D status was low in some trials [128,129], normal insome [127] and unknown in others [123,124]. Study duration ranged from 6 weeks [130] through1 year [116,123,125], up to 36 months [129].
3.2.1. Effects of Vitamin D on IGF-1
Four studies [123–125,131] assessed the effects of vitamin D supplementation on IGF-1 over 4 weeksto 12 months. We presented the Kamycheva trial [123] as two groups, severely obese (study participantswith >35 kg/m2) and non-severely obese (other participants), as results were presented this way inthe paper. Meta-analysis demonstrated no significant effects of the intervention (mean difference:−0.53 nmol/L, 95% CI: −1.58, 0.52, 3 RCTs, I2 0%, Figure 3). One trial [124] could not be included inthe meta-analysis because it was not possible to convert the units of IGF-1 used (µg/10E06 platelets)to nmol/L. This was a 4-week RCT that confirmed a statistically non-significant mean differenceof 0.007 µg/10E06 platelets, p = 0.413 between intervention and placebo post intervention. Thefour included trials randomised 447 participants (mean age: 55.2, 59% males, including dropouts)from Norway [123], USA [124,125] and Austria [131]. Studies used a variety of vitamin D dosages:400 IU [124] 1000 IU [125], 2800 IU [131] and 40,000 IU [123].
Major sources of bias within these studies included randomisation procedures (sequence generationand allocation concealment) and blinding (Figure 3). Only one trial was at low risk of attrition bias,and no studies used ‘mass spectrometry’ to measure sex hormone concentrations, so all were at highrisk of outcome assessment bias.
The lack of effect of increasing vitamin D on IGF-1 was confirmed in the set of trials whichsupplemented with vitamin D and other compounds (two or more micronutrients) (Figure 3).Combining all the trials increasing vitamin D (individually or as part of a broader intervention)suggests little or no effect on IGF-1 (MD: −0.27 nmol/L, 95% CI −1.20 to 0.67, I2 0%). This did not differin sensitivity analysis using fixed-effects meta-analysis (MD: −0.27 nmol/L, 95% CI −1.20 to 0.67, I2

Nutrients 2020, 12, 1457 8 of 21
0%). The difference in effect size between fixed- and random-effects meta-analysis suggests that theremay be some small study bias present.
The effect of differing baseline vitamin D status, doses and study duration were assessedin sub-grouping. There were no differences between subgroups in any analysis (p ≥ 0.85 for allsubgroupings, not shown).Nutrients 2020, 10, x FOR PEER REVIEW 9 of 23
Figure 3. Forest plot assessing effects of increasing vitamin D intake and vitamin D amongst other nutrients, on IGF-1 (nmol/L). Multi, multi-nutrient; vit D, vitamin D. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
The effect of differing baseline vitamin D status, doses and study duration were assessed in sub-grouping. There were no differences between subgroups in any analysis (p ≥ 0.85 for all subgroupings, not shown).
3.2.2. Effects of Vitamin D on Testosterone
Five trials reported effects of vitamin D on testosterone. They included 754 participants (54% male) from China [126], The Netherlands [127], Austria [128], Germany [129] and USA [116]. All included women were post-menopausal. Only two studies could be combined in meta-analysis, suggesting no effect of vitamin D on free testosterone (MD 0.00, 95% CI -0.00 to 0.00, I2 0%, Figure 4). The effect did not differ in sensitivity analysis using fixed-effects meta-analysis, suggesting a lack of small study bias, although with only two trials this is difficult to assess. The other trials (shown in Figure 4 though not combined in meta-analysis) reported data as medians and interquartile ranges [127,128]. One study did not specify which type of testosterone was measured and did not provide enough data to be included [126].
The two trials that could be combined appeared to have adequate randomisation and blinding, though only one had adequate allocation concealment. Neither was at a low risk of outcome measurement bias.
Figure 4. Forest plot assessing effects of increasing vitamin D on free testosterone (nmol/L). Vit D, vitamin D. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
Figure 3. Forest plot assessing effects of increasing vitamin D intake and vitamin D amongst othernutrients, on IGF-1 (nmol/L). Multi, multi-nutrient; vit D, vitamin D. Please refer to SupplementaryTable S5, E to find detailed information on the studies and the reference number.
3.2.2. Effects of Vitamin D on Testosterone
Five trials reported effects of vitamin D on testosterone. They included 754 participants (54% male)from China [126], The Netherlands [127], Austria [128], Germany [129] and USA [116]. All includedwomen were post-menopausal. Only two studies could be combined in meta-analysis, suggesting noeffect of vitamin D on free testosterone (MD 0.00, 95% CI −0.00 to 0.00, I2 0%, Figure 4). The effectdid not differ in sensitivity analysis using fixed-effects meta-analysis, suggesting a lack of small studybias, although with only two trials this is difficult to assess. The other trials (shown in Figure 4 thoughnot combined in meta-analysis) reported data as medians and interquartile ranges [127,128]. Onestudy did not specify which type of testosterone was measured and did not provide enough data to beincluded [126].
Nutrients 2020, 10, x FOR PEER REVIEW 9 of 23
Figure 3. Forest plot assessing effects of increasing vitamin D intake and vitamin D amongst other nutrients, on IGF-1 (nmol/L). Multi, multi-nutrient; vit D, vitamin D. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
The effect of differing baseline vitamin D status, doses and study duration were assessed in sub-grouping. There were no differences between subgroups in any analysis (p ≥ 0.85 for all subgroupings, not shown).
3.2.2. Effects of Vitamin D on Testosterone
Five trials reported effects of vitamin D on testosterone. They included 754 participants (54% male) from China [126], The Netherlands [127], Austria [128], Germany [129] and USA [116]. All included women were post-menopausal. Only two studies could be combined in meta-analysis, suggesting no effect of vitamin D on free testosterone (MD 0.00, 95% CI -0.00 to 0.00, I2 0%, Figure 4). The effect did not differ in sensitivity analysis using fixed-effects meta-analysis, suggesting a lack of small study bias, although with only two trials this is difficult to assess. The other trials (shown in Figure 4 though not combined in meta-analysis) reported data as medians and interquartile ranges [127,128]. One study did not specify which type of testosterone was measured and did not provide enough data to be included [126].
The two trials that could be combined appeared to have adequate randomisation and blinding, though only one had adequate allocation concealment. Neither was at a low risk of outcome measurement bias.
Figure 4. Forest plot assessing effects of increasing vitamin D on free testosterone (nmol/L). Vit D, vitamin D. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
Figure 4. Forest plot assessing effects of increasing vitamin D on free testosterone (nmol/L). Vit D,vitamin D. Please refer to Supplementary Table S5, E to find detailed information on the studies andthe reference number.

Nutrients 2020, 12, 1457 9 of 21
The two trials that could be combined appeared to have adequate randomisation and blinding,though only one had adequate allocation concealment. Neither was at a low risk of outcomemeasurement bias.
3.2.3. Effects of Vitamin D on Oestradiol
Two trials assessed effects of vitamin D on oestradiol, but could not be combined in meta-analysis.Individually, neither found a statistically significant effect of supplementation [116,126].
3.2.4. Effects of Vitamin D on SHBG
Three studies reported effects of vitamin D on SHBG, randomising 445 participants(51% male) [116,128,129]. Meta-analysis of two RCTs suggested a small though non-statisticallysignificant increase in SHBG with vitamin D (MD 4.18 nmol/L, 95% CI −1.28 to 9.64, I2 0%, Figure 5),but data from the third trial contradicted this finding. Two of the three trials were at low risk ofselection bias, and all were well blinded, and one used a low risk method of outcome assessment(Figure 5).
Nutrients 2020, 10, x FOR PEER REVIEW 11 of 23
3.2.3. Effects of Vitamin D on Oestradiol
Two trials assessed effects of vitamin D on oestradiol, but could not be combined in meta-analysis. Individually, neither found a statistically significant effect of supplementation [116,126].
3.2.4. Effects of vitamin D on SHBG
Three studies reported effects of vitamin D on SHBG, randomising 445 participants (51% male) [116,128,129]. Meta-analysis of two RCTs suggested a small though non-statistically significant increase in SHBG with vitamin D (MD 4.18 nmol/L, 95% CI -1.28 to 9.64, I2 0%, Figure 5), but data from the third trial contradicted this finding. Two of the three trials were at low risk of selection bias, and all were well blinded, and one used a low risk method of outcome assessment (Figure 5).
Figure 5. Forest plot showing effects of increasing vitamin D on SHBG (nmol/L). Vit D, vitamin D. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
3.3. Multi-Nutrients
Nine studies assessed effects of multi-nutrients (defined as two or more different micronutrients in the intervention group) on relevant outcomes, but no studies assessed effects on androstenediol, androstenedione, E2, estradiol, estriol, estrone, or DHEAS. Those studies that also included vitamin D within the multi-nutrient interventions are also covered in Section 3.2.
3.3.1. Effects of Multi-Nutrient Supplements on IGF-1
Seven of the nine studies identified as multi-nutrient interventions [130,132–137] reported on IGF-1, suggesting little or no effect (MD: 0.60 nmol/L, 95% CI-1.12 to 2.33, I2 0%, 519 participants, figure 6). Effects did not differ in fixed-effects meta-analysis (MD: 0.60 nmol/L, 95% CI-1.12 to 2.33), suggesting that small study bias is not an issue here.
The Jensen et al. study [137] analysed data using a ‘per-protocol’ method which introduced potential bias [138], since the 20% of study participants withdrew. All seven studies measured micronutrient concentrations from blood samples, but none used mass-spectrometry to measure sex hormone concentrations, and many were unclear on selection bias and blinding.
3.3.2. Effects of multi-nutrients on testosterone
Two trials carried out in the Netherlands reported effects of multi-nutrient interventions on testosterone in men with rising levels of prostate-specific antigen (117 males, mean age: 72), and reported opposing findings (Figure 6). We were unable to meta-analyse these findings as Kranse did not provide any measure of variance. However, Hoenjet, 2005 [139] suggested no effect on testosterone concentrations (p = 0.28), while Kranse, 2005 [140] (cross-over trial) suggested significant reductions in testosterone but reported different numbers in different places in their paper, so the effect size was unclear (p = 0.02). Both trials were at unclear risk of selection bias and low risk of blinding problems.
Figure 5. Forest plot showing effects of increasing vitamin D on SHBG (nmol/L). Vit D, vitamin D. Pleaserefer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
3.3. Multi-Nutrients
Nine studies assessed effects of multi-nutrients (defined as two or more different micronutrientsin the intervention group) on relevant outcomes, but no studies assessed effects on androstenediol,androstenedione, E2, estradiol, estriol, estrone, or DHEAS. Those studies that also included vitamin Dwithin the multi-nutrient interventions are also covered in Section 3.2.
3.3.1. Effects of Multi-Nutrient Supplements on IGF-1
Seven of the nine studies identified as multi-nutrient interventions [130,132–137] reported onIGF-1, suggesting little or no effect (MD: 0.60 nmol/L, 95% CI −1.12 to 2.33, I2 0%, 519 participants,Figure 6). Effects did not differ in fixed-effects meta-analysis (MD: 0.60 nmol/L, 95% CI −1.12 to 2.33),suggesting that small study bias is not an issue here.
The Jensen et al. study [137] analysed data using a ‘per-protocol’ method which introducedpotential bias [138], since the 20% of study participants withdrew. All seven studies measuredmicronutrient concentrations from blood samples, but none used mass-spectrometry to measure sexhormone concentrations, and many were unclear on selection bias and blinding.
3.3.2. Effects of Multi-Nutrients on Testosterone
Two trials carried out in the Netherlands reported effects of multi-nutrient interventions ontestosterone in men with rising levels of prostate-specific antigen (117 males, mean age: 72), andreported opposing findings (Figure 6). We were unable to meta-analyse these findings as Kranse didnot provide any measure of variance. However, Hoenjet, 2005 [139] suggested no effect on testosterone

Nutrients 2020, 12, 1457 10 of 21
concentrations (p = 0.28), while Kranse, 2005 [140] (cross-over trial) suggested significant reductions intestosterone but reported different numbers in different places in their paper, so the effect size wasunclear (p = 0.02). Both trials were at unclear risk of selection bias and low risk of blinding problems.
Nutrients 2020, 10, x FOR PEER REVIEW 12 of 23
3.3.3. Effects of multi-nutrients on Dihydrotestosterone and SHBG
The same two trials (Kranse, 2005; and Hoenjet, 2005) also assessed the effect of multi-nutrient supplementation on Dihydroteststerone and SHBG (Figure 6), but again Kranse provided no measure of variance and two different effect sizes, so could not be pooled. Multi-nutrient supplementation in Kranse, 2005, reportedly significantly decreased Dihydrotestosterone, but the effect size was unclear (p = 0.005), whereas, in Hoenjet 2005, non-significant findings were reported (MD: 0.1 nmol/L, 95% CI −0.1 to 0.2, p = 0.72). After supplementation with multi-nutrients, both studies reported non-significant decreases in SHBG.
Figure 6. Forest plot assessing the effects of multi-nutrient interventions on sex hormones and IGF-1 (nmol/L). Multi, multi-nutrient. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
3.4. Carotenoids
Four trials assessed the effects of carotenoids on relevant outcomes, but none assessed the effects on androgens (androstenediol, androstenedione, dihydrotestosterone or testosterone), oestrogens (E2, estradiol, estriol, or estrone), DHEAS or SHBG.
Effects of Carotenoids on IGF-1
Four studies [52,80–82] examined the effects of lycopene, all using ‘Lyco-O-Mato’ (containing ~15mg lycopene, plus 1.5mg phytoene, 1.4mg phytofluene, 0.4mg beta-carotene, and 5mg alpha tocopherol). Meta-analysis of 278 randomised participants (mean age: 63.0, 75% male) showed a non-significant decrease in IGF-1 as a result of the added carotenoids (MD −1.32nmol/L; 95% CI −2.76 to 0.11, I2 0%, Figure 6). None of the trials were at low risk of selection bias, but two were at low risk from issues around blinding (performance and detection bias), and none used mass-spectrometry to measure hormone concentrations (Figure 7).
Figure 6. Forest plot assessing the effects of multi-nutrient interventions on sex hormones and IGF-1(nmol/L). Multi, multi-nutrient. Please refer to Supplementary Table S5, E to find detailed informationon the studies and the reference number.
3.3.3. Effects of Multi-Nutrients on Dihydrotestosterone and SHBG
The same two trials (Kranse, 2005; and Hoenjet, 2005) also assessed the effect of multi-nutrientsupplementation on Dihydroteststerone and SHBG (Figure 6), but again Kranse provided no measureof variance and two different effect sizes, so could not be pooled. Multi-nutrient supplementation inKranse, 2005, reportedly significantly decreased Dihydrotestosterone, but the effect size was unclear(p = 0.005), whereas, in Hoenjet 2005, non-significant findings were reported (MD: 0.1 nmol/L, 95% CI−0.1 to 0.2, p = 0.72). After supplementation with multi-nutrients, both studies reported non-significantdecreases in SHBG.
3.4. Carotenoids
Four trials assessed the effects of carotenoids on relevant outcomes, but none assessed the effectson androgens (androstenediol, androstenedione, dihydrotestosterone or testosterone), oestrogens(E2, estradiol, estriol, or estrone), DHEAS or SHBG.
Effects of Carotenoids on IGF-1
Four studies [52,80–82] examined the effects of lycopene, all using ‘Lyco-O-Mato’ (containing~15 mg lycopene, plus 1.5 mg phytoene, 1.4 mg phytofluene, 0.4 mg beta-carotene, and 5 mg alphatocopherol). Meta-analysis of 278 randomised participants (mean age: 63.0, 75% male) showed anon-significant decrease in IGF-1 as a result of the added carotenoids (MD −1.32 nmol/L; 95% CI −2.76to 0.11, I2 0%, Figure 6). None of the trials were at low risk of selection bias, but two were at low risk

Nutrients 2020, 12, 1457 11 of 21
from issues around blinding (performance and detection bias), and none used mass-spectrometry tomeasure hormone concentrations (Figure 7).
Nutrients 2020, 10, x FOR PEER REVIEW 13 of 23
Trials of carotenoids as part of multi-nutrient supplementation (Figure 7), confirmed a small non-significant decrease in IGF-1 (MD: −0.39, 95% CI −2.90 to 0.11, I2 0%). These trials also demonstrated significant sources of bias (see earlier).
Overall effects of carotenoids (in either individual or multi-nutrient studies) suggested no important effect of carotenoids on IGF-1 (MD: −1.09, 95% CI −2.34 to 0.16, I2 0%), which did not differ in sensitivity analysis using fixed effects meta-analysis (MD: -1.09, 95% CI −2.34 to 0.16). This suggested minimal small study bias.
Figure 7. Forest plot assessing effects of increasing carotenoids (lycopene) and carotenoids amongst other nutrients on IGF-1 (nmol/L). Carot, carotenoids; multi, multi-nutrient. Please refer to Supplementary Table S5, E to find detailed information on the studies and the reference number.
3.5. Selenium
Two studies assessed effects of selenium on testosterone, but no studies assessed effects on oestrogens (E2, estradiol, estriol, or estrone), DHEAS, SHBG, IGF-1 or androgens other than testosterone.
Effects of Selenium on Testosterone
Two studies in the Czech Republic examined the effects of 240μg of selenium (as selenomethionine) on testosterone. Both intervention and placebo also received 570mg of silymarin, an extract of milk thistle [141,142]. Both suggested no significant effects on testosterone.
3.6. Vitamin E
One study assessed the effects of Vitamin E on DHEAS, but no studies assessed the effects on androgens (androstenediol, androstenedione, dihydrotestosterone and testosterone), oestrogens (E2, estradiol, estriol, and estrone), SHBG, or IGF-1.
Effects of Vitamin E on DHEAS
Amsterdam 2005 [143] found that 200mg vitamin E (as dl-alpha-tocopheryl acetate) over 15 months lead to a significant decrease in DHEAS in the supplemented group (p<0.02) but not the placebo group (p>0.05). The authors concluded there was no overall significant benefit to vitamin E supplementation.
3.7. Zinc
Figure 7. Forest plot assessing effects of increasing carotenoids (lycopene) and carotenoids amongst othernutrients on IGF-1 (nmol/L). Carot, carotenoids; multi, multi-nutrient. Please refer to SupplementaryTable S5, E to find detailed information on the studies and the reference number.
Trials of carotenoids as part of multi-nutrient supplementation (Figure 7), confirmed a smallnon-significant decrease in IGF-1 (MD:−0.39, 95% CI−2.90 to 0.11, I2 0%). These trials also demonstratedsignificant sources of bias (see earlier).
Overall effects of carotenoids (in either individual or multi-nutrient studies) suggested noimportant effect of carotenoids on IGF-1 (MD: −1.09, 95% CI −2.34 to 0.16, I2 0%), which did notdiffer in sensitivity analysis using fixed effects meta-analysis (MD: −1.09, 95% CI −2.34 to 0.16). Thissuggested minimal small study bias.
3.5. Selenium
Two studies assessed effects of selenium on testosterone, but no studies assessed effects onoestrogens (E2, estradiol, estriol, or estrone), DHEAS, SHBG, IGF-1 or androgens other than testosterone.
Effects of Selenium on Testosterone
Two studies in the Czech Republic examined the effects of 240 µg of selenium (as selenomethionine)on testosterone. Both intervention and placebo also received 570 mg of silymarin, an extract of milkthistle [141,142]. Both suggested no significant effects on testosterone.
3.6. Vitamin E
One study assessed the effects of Vitamin E on DHEAS, but no studies assessed the effectson androgens (androstenediol, androstenedione, dihydrotestosterone and testosterone), oestrogens(E2, estradiol, estriol, and estrone), SHBG, or IGF-1.
Effects of Vitamin E on DHEAS
Amsterdam 2005 [143] found that 200 mg vitamin E (as dl-alpha-tocopheryl acetate) over 15 monthslead to a significant decrease in DHEAS in the supplemented group (p < 0.02) but not the placebo group(p > 0.05). The authors concluded there was no overall significant benefit to vitamin E supplementation.

Nutrients 2020, 12, 1457 12 of 21
3.7. Zinc
One study assessed effects of zinc on IGF-1, but no studies assessed effects on androgens(androstenediol, androstenedione, dihydrotestosterone and testosterone), oestrogens (E2, estradiol,estriol, and estrone), DHEA or SHBG.
Effects of Zinc on IGF-1
A Swiss trial by Rodondi, 2009 [61] (n = 69, mean age 85, 86% female) reported that supplementationof 30 mg/day of zinc (alongside 15 g whey protein + 5 g amino acids) increased serum IGF-1 overa week compared to protein alone (+48.2% vs. +22.4%, respectively; p < 0.027), but there was nostatistically significant difference between groups at 4 weeks (+29.2% vs. +45.8%; p > 0.05).
4. Discussion
We found 26 trials assessing effects of micronutrient supplementation, but no trials assessing effectsof vitamins A or C, potassium, iron, or copper, on our outcomes. Data from nine trials suggested thatsupplementation with vitamin D had little or no effect on IGF-1, with or without other micronutrientcompounds. Vitamin D also failed to significantly alter testosterone or oestradiol, and the effects onSHBG and other outcomes were unclear. The multinutrient trials did not suggest statistically significantincreases in IGF-1, and the effects on testosterone, dihydrotestosterone and SHBG were unclear. Datawere very limited for effects of other micronutrients. Four trials suggested that carotenoids slightlyreduce IGF-1 and this was reinforced with the inclusion of other micronutrients (though none ofthe relationships were statistically significant). Selenium appears to have little effect on testosterone(2 trials), vitamin E had no effect on DHEAS, and zinc had little or no effect on IGF-1 (a single trial each).
Despite our systematic search including a large range of relevant micronutrients and hormones,we only identified studies that investigated effects of vitamin D, multi-nutrients, the carotenoids,selenium, vitamin E, and zinc, on sex hormones and IGF-1. To the best of our knowledge, this is thefirst systematic review examining the relationship between this range of micronutrients, sex hormonesand IGF-1 in people of middle and older age. We conducted the review using established Cochranemethodology [115].
Despite the biochemical, physiological and mechanistic roles of micronutrients for hormonesynthesis in older age our review found a paucity of trials and little direct evidence of significant effectsof micronutrient supplementation [38–50,52,60,64,65,68,69,71,79–86]. Since the age-related decline insex-hormones and IGF-1 not only increases the risk of sarcopenia, but also a number of conditions ofaging, including falls, osteoporosis, fractures, cardiovascular disease and all-cause mortality, this isunfortunate [5–16].
Limitations of the Available Data
Whilst we identified 26 RCTs of adults aged at least 45 years that met our eligibility criteria,when grouped by micronutrient and sex-hormone, the number of studies in each category was small(between one and nine studies per nutrient), and many had methodological limitations. A number of thestudies had small sample sizes or lack of control for dietary or lifestyle determinants in the interventionand control groups [52,80,82] and one study [137,138] also analysed data using a ‘per-protocol’ methodwhich may have introduced bias elements of bias [138].
For multi-nutrient interventions the composition of the nutrients varied substantially [130,132–136]with some containing more than 20 different micronutrients [132,137], making it difficult to attributebenefit to any specific micronutrient. A number of studies also included additional protein making itdifficult to isolate any specific effects of micronutrients from those of protein [61,132,137,144,145]. Thebaseline nutritional status of participants was not taken into account in a number of studies despitebaseline status or deficiency being likely to determine the response to interventions. Some studies

Nutrients 2020, 12, 1457 13 of 21
also included dietary advice to increase sources of calcium, which may have affected the results ofthe intervention.
Whilst we found no significant effect of the supplementation of micronutrients on circulatingsex hormones and IGF-1, the scale of effects for the few studies that included IGF-1 ranged betweenmean differences for vitamin D of −0.53 nmol/L (95% CI: −1.58, 0.52), for multi-nutrients of 0.60 nmol/L(95% CI −1.12 to 2.33) and carotenoids of −1.32 nmol/L (95% CI −2.76 to 0.11). This compares with thedifference for IGF-1 between age groups 50–54 years to 70–74 years of −3.4 nmol/L [146,147]. Althoughthe effect sizes found with micronutrients and IGF-1 in our analysis were non-significant, and smallerthan with age, these differences may have potential importance if found to be significant in futurewell-designed trials.
5. Recommendations for Future Studies
Although our systematic review demonstrated no conclusive effects of the supplementation ofmicronutrients on sex hormones in middle- and older-aged people, we recommend that larger RCTsare conducted specifically targeting the micronutrients where we found little or no existing research(magnesium, zinc, vitamin A, E, iron, copper, and potassium). Future RCTs should be of sufficientsize and include baseline and follow-up measures of dietary intake (such as with food frequencyquestionnaires), as well as using blood concentrations of the relevant micronutrients. This wouldclarify whether micronutrient supplementation is only beneficial to depleted individuals or whether itcan provide additional benefit to those with adequate micronutrient status. Direct measurements ofmicronutrient status have advantages as they are independent of potential reporting bias, are integratedmeasurements of intake and other physiological and lifestyle influences on status, such as smokinghabit, and can be used to determine whether supplementation results in improved micronutrientstatus [148–150]. Furthermore, dosages of micronutrients should be designed to rectify any pre-existingmicronutrient deficiency. Additionally, extraction of hormones should be performed using massspectrometry, and SHBG should be measured to account for changes to free oestrogen and testosteronethat may occur during the intervention. Other known lifestyle factors that affect circulating sexhormones and IGF-1, such as smoking habit and BMI should also be recorded [146,147]. An optimalfollow-up time has yet to be elucidated but we would recommend a minimum of 6 months, and thatendocrine and nutritional measurements be taken at 3 month intervals until the study is complete.
6. Conclusions
Effects of micronutrient supplementation on sex hormones and IGF-1 are unclear. Further highquality RCTs with physiological doses of micronutrients in people with low baseline intakes orcirculating concentrations, using robust methodology, are required to assess effects adequately.
Supplementary Materials: The following are available online at http://www.mdpi.com/2072-6643/12/5/1457/s1,Table S1, E: Search Strategy Form, Table S2, B: Inclusion/Exclusion Form, Table S3, C: Data Extraction Form,Table S4, D: Systematic review Cochrane Risk of Bias Form, Table S5, E: Table of Characteristics of RCTs (n = 26).
Author Contributions: Conceptualization, A.W.; methodology, A.W., L.H., D.B., A.A., R.J.; formal analysis, L.H.,R.J., A.A., D.B.; writing—original draft preparation, R.J., A.W., D.B., A.A.; writing—review and editing, A.W., D.B.,A.A., L.H., R.H.; data extraction and screening, R.J., D.B., A.A., A.W., R.H., L.H., S.M., J.H.-C., W.A. All authorshave read and agreed to the published version of the manuscript.
Funding: This research received no external funding but was partly funded by MRES funding to R.J. fromNorwich Medical School.
Conflicts of Interest: The authors declare no conflict of interest.
References
1. Epidemiologic and methodologic problems in determining nutritional status of older persons. Proceedingsof a conference. Albuquerque, New Mexico, October 19–21, 1988. Am. J. Clin. Nutr. 1989, 50 (Suppl. 5),1121–1235.

Nutrients 2020, 12, 1457 14 of 21
2. Boss, G.R.; Seegmiller, J.E. Age-Related Physiological Changes and Their Clinical Significance. West. J. Med.1981, 135, 434–440. [PubMed]
3. Marzetti, E.; on behalf of the SPRINTT Consortium; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.;Cherubini, A.; Collamati, A.; D’Angelo, E.; Pahor, M.; et al. Sarcopenia: An overview. Aging Clin. Exp. Res.2017, 29, 11–17. [CrossRef] [PubMed]
4. Marty, E.; Liu, Y.; Samuel, A.; Or, O.; Lane, J. A review of sarcopenia: Enhancing awareness of an increasinglyprevalent disease. Bone 2017, 105, 276–286. [CrossRef] [PubMed]
5. Vandenput, L.; Mellström, D.; A Laughlin, G.; Cawthon, P.M.; A Cauley, J.; Hoffman, A.R.; Karlsson, M.K.;Rosengren, B.E.; Ljunggren, Ö.; Nethander, M.; et al. Low Testosterone, but Not Estradiol, Is Associated WithIncident Falls in Older Men: The International MrOS Study. J. Bone Min. Res. 2017, 32, 1174–1181. [CrossRef]
6. Roddam, A.W.; Appleby, P.; Neale, R.E.; Dowsett, M.; Folkerd, E.; Tipper, S.; Allen, N.E.; Key, T.J. Associationbetween endogenous plasma hormone concentrations and fracture risk in men and women: The EPIC-Oxfordprospective cohort study. J. Bone Min. Metab. 2009, 27, 485–493. [CrossRef]
7. Khaw, K.-T.; Dowsett, M.; Folkerd, E.; Bingham, S.; Wareham, N.; Luben, R.N.; Welch, A.; Day, N. Endogenoustestosterone and mortality due to all causes, cardiovascular disease, and cancer in men: European prospectiveinvestigation into cancer in Norfolk (EPIC-Norfolk) Prospective Population Study. Circulation 2007, 116,2694–2701. [CrossRef]
8. Guadalupe-Grau, A.; Carnicero, J.A.; Losa-Reyna, J.; Tresguerres, J.; Gomez-Cabrera, M.C.; Castillo, C.;Alfaro-Acha, A.; Rosado-Artalejo, C.; Rodríguez-Mañas, L.; Garcia-Garcia, F.J. Endocrinology of Aging Froma Muscle Function Point of View: Results from the Toledo Study for Healthy Aging. J. Am. Med. Dir. Assoc.2017, 18, 234–239. [CrossRef]
9. Clegg, D.; Hevener, A.L.; Moreau, K.L.; Morselli, E.; Criollo, A.; Van Pelt, R.E.; Vieira-Potter, V.J. SexHormones and Cardiometabolic Health: Role of Estrogen and Estrogen Receptors. Endocrinology 2017, 158,1095–1105. [CrossRef]
10. Diamanti-Kandarakis, E.; Dattilo, M.; Macut, Đ.; Duntas, L.H.; Gonos, E.S.; Goulis, D.G.;Kanaka-Gantenbein, C.; Kapetanou, M.; Koukkou, E.G.; Lambrinoudaki, I.; et al. MECHANISMS INENDOCRINOLOGY: Aging and anti-aging: A Combo-Endocrinology overview. Eur. J. Endocrinol. 2017, 176,R283–R308. [CrossRef]
11. Horstman, A.M.; Dillon, E.L.; Urban, R.J.; Sheffield-Moore, M. The role of androgens and estrogens onhealthy aging and longevity. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 1140–1152. [CrossRef]
12. Yeap, B.B.; Alfonso, H.; Chubb, S.A.P.; Center, J.R.; Beilin, J.; Hankey, G.J.; Almeida, O.P.; Golledge, J.;Norman, P.; Flicker, L. U-Shaped Association of Plasma Testosterone, and no Association of Plasma Estradiol,with Incidence of Fractures in Men. J. Clin. Endocrinol. Metab. 2020, 105. [CrossRef] [PubMed]
13. Moreau, K.L.; Babcock, M.C.; Hildreth, K.L. Sex differences in vascular aging in response to testosterone.Biol. Sex Differ. 2020, 11, 18. [CrossRef] [PubMed]
14. Karlamangla, A.S.; Burnett-Bowie, S.M.; Crandall, C.J. Bone Health during the Menopause Transition andBeyond. Obstet. Gynecol. Clin. N. Am. 2018, 45, 695–708. [CrossRef] [PubMed]
15. Hidayat, K.; Du, X.; Shi, B.M. Sex hormone-binding globulin and risk of fracture in older adults: Systematicreview and meta-analysis of observational studies. Osteoporos Int. 2018, 29, 2171–2180. [CrossRef]
16. Brundle, C.; Heaven, A.; Brown, L.; Teale, E.; Young, J.; West, R.; Clegg, A. Convergent validity of theelectronic frailty index. Age Ageing 2019, 48, 152–156. [CrossRef]
17. Morley, J.E. Hormones and Sarcopenia. Curr. Pharm. Des. 2017, 23, 4484–4492. [CrossRef]18. Maggio, M.; Lauretani, F.; Ceda, G.P. Sex hormones and sarcopenia in older persons. Curr. Opin. Clin. Nutr.
Metab. Care 2013, 16, 3–13. [CrossRef]19. Baumgartner, R.N.; Waters, D.L.; Gallagher, D.; Morley, J.E.; Garry, P.J. Predictors of skeletal muscle mass in
elderly men and women. Mech. Ageing Dev. 1999, 107, 123–136. [CrossRef]20. Mouser, J.G.; Loprinzi, P.D.; Loenneke, J.P. The association between physiologic testosterone levels, lean
mass, and fat mass in a nationally representative sample of men in the United States. Steroids 2016, 115,62–66. [CrossRef]
21. Ottenbacher, K.J.; Ottenbacher, M.E.; Ottenbacher, A.J.; Acha, A.A.; Ostir, G.V. Androgen Treatment andMuscle Strength in Elderly Males: A Meta-Analysis. J. Am. Geriatr. Soc. 2006, 54, 1666–1673. [CrossRef]

Nutrients 2020, 12, 1457 15 of 21
22. Tiidus, P.M. Benefits of Estrogen Replacement for Skeletal Muscle Mass and Function in Post-MenopausalFemales: Evidence from Human and Animal Studies. Eurasian J. Med. 2011, 43, 109–114. [CrossRef][PubMed]
23. Samson, M.M.; Meeuwsen, I.B.; Crowe, A.; Dessens, J.A.; Duursma, S.A.; Verhaar, H.J. Relationships betweenphysical performance measures, age, height and body weight in healthy adults. Age Ageing 2000, 29, 235–242.[CrossRef] [PubMed]
24. Park, Y.-M.; Keller, A.C.; Runchey, S.S.; Miller, B.F.; Kohrt, W.M.; Van Pelt, R.E.; Kang, C.; Jankowski, C.M.;Moreau, K.L. Acute estradiol treatment reduces skeletal muscle protein breakdown markers in early- but notlate-postmenopausal women. Steroids 2019, 146, 43–49. [CrossRef] [PubMed]
25. Velders, M.; Diel, P. How sex hormones promote skeletal muscle regeneration. Sports Med. 2013, 43,1089–1100. [CrossRef]
26. Taekema, D.G.; Ling, C.H.; Blauw, G.J.; Meskers, C.G.; Westendorp, R.G.J.; De Craen, A.J.M.; Maier, A.B.Circulating levels of IGF1 are associated with muscle strength in middle-aged- and oldest-old women. Eur. J.Endocrinol. 2011, 164, 189–196. [CrossRef]
27. Warner, M.; Gustafsson, J.A. DHEA-a precursor of ERbeta ligands. J. Steroid Biochem. Mol. Biol. 2015, 145,245–247. [CrossRef]
28. Selby, C. Sex hormone binding globulin: Origin, function and clinical significance. Ann. Clin. Biochem. 1990,27 Pt 6, 532–541. [CrossRef]
29. Liu, P.Y.; Beilin, J.; Nguyen, T.V.; Center, J.R.; Meier, C.; Leedman, P.J.; Seibel, M.; A Eisman, J.; Handelsman, D.J.Age-Related Changes in Serum Testosterone and Sex Hormone Binding Globulin in Australian Men:Longitudinal Analyses of Two Geographically Separate Regional Cohorts. J. Clin. Endocrinol. Metab. 2007,92, 3599–3603. [CrossRef]
30. Longcope, C.; Goldfield, S.R.; Brambilla, D.J.; McKinlay, J. Androgens, estrogens, and sex hormone-bindingglobulin in middle-aged men. J. Clin. Endocrinol. Metab. 1990, 71, 1442–1446. [CrossRef]
31. Pang, A.L.-Y.; Chan, W.-Y. Chapter 22-Molecular Basis of Diseases of the Endocrine System. In EssentialConcepts in Molecular Pathology; Coleman, W.B., Tsongalis, G.J., Eds.; Academic Press: San Diego, CA, USA,2010; pp. 289–307.
32. Philippou, A.; Barton, E.R. Optimizing IGF-I for skeletal muscle therapeutics. Growth Horm. IGF Res. 2014,24, 157–163. [CrossRef]
33. Secco, M.; Bueno, C.; Vieira, N.M.; Almeida, C.; Pelatti, M.; Zucconi, E.; Bartolini, P.; Vainzof, M.; Miyabara, E.;Okamoto, O.K.; et al. Systemic delivery of human mesenchymal stromal cells combined with IGF-1 enhancesmuscle functional recovery in LAMA2 dy/2j dystrophic mice. Stem Cell Rev. 2013, 9, 93–109. [CrossRef][PubMed]
34. Rybalko, V.Y.; Pham, C.B.; Hsieh, P.-L.; Hammers, D.W.; Merscham-Banda, M.; Suggs, L.J.; Farrar, R.P.Controlled delivery of SDF-1alpha and IGF-1: CXCR4(+) cell recruitment and functional skeletal musclerecovery. Biomater. Sci. 2015, 3, 1475–1486. [CrossRef] [PubMed]
35. Bucci, L.; Yani, S.L.; Fabbri, C.; Bijlsma, A.Y.; Maier, A.B.; Meskers, C.G.; Narici, M.; Jones, D.A.; McPhee, J.S.;Seppet, E.; et al. Circulating levels of adipokines and IGF-1 are associated with skeletal muscle strength ofyoung and old healthy subjects. Biogerontology 2013, 14, 261–272. [CrossRef] [PubMed]
36. Mohamad, M.I.; Khater, M.S. Evaluation of insulin like growth factor-1 (IGF-1) level and its impact on muscleand bone mineral density in frail elderly male. Arch. Gerontol. Geriatr. 2015, 60, 124–127. [CrossRef]
37. Harrison, P. Low Vitamin D Tied to Testosterone Dip in Healthy Men 2015 [Vitamin D and Testosterone].Available online: https://www.medscape.com/viewarticle/845483 (accessed on 4 March 2020).
38. Ceglia, L.; Harris, S.S. Vitamin D and its role in skeletal muscle. Calcif Tissue Int. 2013, 92, 151–162. [CrossRef]39. Azadi-Yazdi, M.; Nadjarzadeh, A.; Khosravi-Boroujeni, H.; Salehi-Abargouei, A. The Effect of Vitamin D
Supplementation on the Androgenic Profile in Patients with Polycystic Ovary Syndrome: A SystematicReview and Meta-Analysis of Clinical Trials. Horm. Metab. Res. 2017, 49, 174–179. [CrossRef]
40. Zhao, D.; Ouyang, P.; De Boer, I.H.; Lutsey, P.L.; Farag, Y.M.; Guallar, E.; Siscovick, D.S.; Post, W.S.;Kalyani, R.R.; Billups, K.L.; et al. Serum vitamin D and sex hormones levels in men and women:The Multi-Ethnic Study of Atherosclerosis (MESA). Maturitas 2017, 96, 95–102. [CrossRef]
41. Rafiq, R.; Van Schoor, N.; Sohl, E.; Zillikens, M.; Oosterwerff, M.; Schaap, L.; Lips, P.; De Jongh, R. Associationsof vitamin D status and vitamin D-related polymorphisms with sex hormones in older men. J. Steroid Biochem.Mol. Boil. 2016, 164 (Suppl. C), 11–17. [CrossRef]

Nutrients 2020, 12, 1457 16 of 21
42. Chin, K.Y.; Ima-Nirwana, S.; Wan Ngah, W.Z. Vitamin D is significantly associated with total testosteroneand sex hormone-binding globulin in Malaysian men. Aging Male 2015, 18, 175–179. [CrossRef]
43. Lerchbaum, E.; Pilz, S.; Trummer, C.; Rabe, T.; Schenk, M.; Heijboer, A.C.; Obermayer-Pietsch, B. Serumvitamin D levels and hypogonadism in men. Andrology 2014, 2, 748–754. [CrossRef]
44. Anic, G.M.; Albanes, D.; Rohrmann, S.; Kanarek, N.; Nelson, W.G.; Bradwin, G.; Rifai, N.; McGlynn, K.A.;Platz, E.A.; Mondul, A.M. Association between serum 25-hydroxyvitamin D and serum sex steroid hormonesamong men in NHANES. Clin. Endocrinol. 2016, 85, 258–266. [CrossRef] [PubMed]
45. Chang, E.M.; Kim, Y.S.; Won, H.J.; Yoon, T.K.; Lee, W.S. Association between Sex Steroids, Ovarian Reserve,and Vitamin D Levels in Healthy Nonobese Women. J. Clin. Endocrinol. Metab. 2014, 99, 2526–2532.[CrossRef] [PubMed]
46. Jorde, R.; Grimnes, G.; Hutchinson, M.S.; Kjaergaard, M.; Kamycheva, E.; Svartberg, J. Supplementation withvitamin D does not increase serum testosterone levels in healthy males. Horm. Metab. Res. 2013, 45, 675–681.[CrossRef] [PubMed]
47. Hammoud, A.O.; Wayne Meikle, A.; Matthew Peterson, C.; Stanford, J.; Gibson, M.; Carrell, D.T. Associationof 25-hydroxy-vitamin D levels with semen and hormonal parameters. Asian J. Androl. 2012, 14, 855–859.[CrossRef]
48. Mumford, S.L.; Browne, R.W.; Schliep, K.C.; Schmelzer, J.; Plowden, T.C.; A Michels, K.; Sjaarda, L.;Zarek, S.M.; Perkins, N.; Messer, L.; et al. Serum Antioxidants Are Associated with Serum ReproductiveHormones and Ovulation among Healthy Women. J. Nutr. 2016, 146, 98–106. [CrossRef]
49. Barella, L.; Rota, C.; Stocklin, E.; Rimbach, G. Alpha-tocopherol affects androgen metabolism in male rat.Ann. New York Acad. Sci. 2004, 1031, 334–336. [CrossRef]
50. Hartman, T.J.; Dorgan, J.F.; Woodson, K.; Virtamo, J.; A Tangrea, J.; Heinonen, O.P.; Taylor, P.R.; Barrett, M.J.;Albanes, D. Effects of long-term alpha-tocopherol supplementation on serum hormones in older men. Prostate2001, 46, 33–38. [CrossRef]
51. Hogarth, C.A.; Griswold, M.D. The key role of vitamin A in spermatogenesis. J. Clin. Investig. 2010, 120,956–962. [CrossRef]
52. Kucuk, O.; Sarkar, F.H.; Sakr, W.; Djuric, Z.; Pollak, M.N.; Khachik, F.; Li, Y.W.; Banerjee, M.; Grignon, D.;Bertram, J.S.; et al. Phase II randomized clinical trial of lycopene supplementation before radical prostatectomy.Cancer Epidemiol. Biomark. Prev. 2001, 10, 861–868.
53. Rotter, I.; Kosik-Bogacka, D.I.; Dolegowska, B.; Safranow, K.; Kuczynska, M.; Laszczynska, M. Analysis of therelationship between the blood concentration of several metals, macro- and micronutrients and endocrinedisorders associated with male aging. Environ. Geochem. Health 2016, 38, 749–761. [CrossRef]
54. Rotter, I.; Kosik-Bogacka, D.; Dolegowska, B.; Safranow, K.; Karakiewicz, B.; Laszczynska, M. Relationshipbetween serum magnesium concentration and metabolic and hormonal disorders in middle-aged and oldermen. Magnes. Res. 2015, 28, 99–107. [CrossRef] [PubMed]
55. Maggio, M.; Ceda, G.; Lauretani, F.; Cattabiani, C.; Avantaggiato, E.; Morganti, S.; Ablondi, F.; Bandinelli, S.;Dominguez, L.-J.; Barbagallo, M.; et al. Magnesium and anabolic hormones in older men. Int. J. Androl. 2011,34 Pt 2, e594–e600. [CrossRef]
56. Cinar, V.; Polat, Y.; Baltaci, A.K.; Mogulkoc, R. Effects of magnesium supplementation on testosterone levelsof athletes and sedentary subjects at rest and after exhaustion. Biol. Trace Elem. Res. 2011, 140, 18–23.[CrossRef] [PubMed]
57. Maggio, M.; Ceda, G.; Lauretani, F.; Bandinelli, S.; Dall’Aglio, E.; Guralnik, J.M.; Paolisso, G.; Semba, R.D.;Nouvenne, A.; Borghi, L.; et al. Association of plasma selenium concentrations with total IGF-1 among oldercommunity-dwelling adults: The InCHIANTI study. Clin. Nutr. 2010, 29, 674–677. [CrossRef] [PubMed]
58. Oluboyo, A.; Adijeh, R.U.; Onyenekwe, C.C.; O Oluboyo, B.; Mbaeri, T.C.; Odiegwu, C.N.; O Chukwuma, G.;Onwuasoanya, U.F. Relationship between serum levels of testosterone, zinc and selenium in infertile malesattending fertility clinic in Nnewi, south east Nigeria. Afr. J. Med. Med. Sci. 2012, 41, 51–54. [PubMed]
59. Hawkes, W.C.; Turek, P.J. Effects of dietary selenium on sperm motility in healthy men. J. Androl. 2001, 22,764–772.
60. Darago, A.; Klimczak, M.; Stragierowicz, J.; Stasikowska-Kanicka, O.; Kilanowicz, A. The Effect of Zinc,Selenium, and Their Combined Supplementation on Androgen Receptor Protein Expression in the ProstateLobes and Serum Steroid Hormone Concentrations of Wistar Rats. Nutrients 2020, 12, 153. [CrossRef]

Nutrients 2020, 12, 1457 17 of 21
61. Rodondi, A.; Ammann, P.; Ghilardi-Beuret, S.; Rizzoli, R. Zinc increases the effects of essential aminoacids-whey protein supplements in frail elderly. J. Nutr. Health Aging 2009, 13, 491–497. [CrossRef]
62. Blostein-Fujii, A.; DiSilvestro, R.A.; Frid, D.; Katz, C.; Malarkey, W. Short-term zinc supplementationin women with non-insulin-dependent diabetes mellitus: Effects on plasma 5’-nucleotidase activities,insulin-like growth factor I concentrations, and lipoprotein oxidation rates in vitro. Am. J. Clin. Nutr. 1997,66, 639–642. [CrossRef]
63. Vivoli, G.; Fantuzzi, G.; Bergomi, M.; Tonelli, E.; Gatto, M.; Zanetti, F.; Del Dot, M. Relationship between zincin serum and hair and some hormones during sexual maturation in humans. Sci. Total Environ. 1990, 95,29–40. [CrossRef]
64. Shafiei Neek, L.; Gaeini, A.A.; Choobineh, S. Effect of zinc and selenium supplementation on serumtestosterone and plasma lactate in cyclist after an exhaustive exercise bout. Biol. Trace Elem. Res. 2011, 144,454–462. [CrossRef] [PubMed]
65. Kilic, M.; Baltaci, A.K.; Gunay, M.; Gokbel, H.; Okudan, N.; Cicioglu, I. The effect of exhaustion exercise onthyroid hormones and testosterone levels of elite athletes receiving oral zinc. Neuro Endocrinol. Lett. 2006, 27,247–252. [PubMed]
66. Ebisch, I.M.; Thomas, C.M.; Peters, W.H.; Braat, D.D.; Steegers-Theunissen, R.P. The importance of folate,zinc and antioxidants in the pathogenesis and prevention of subfertility. Hum. Reprod. Update 2007, 13,163–174. [CrossRef] [PubMed]
67. Ebisch, I.M.W.; Pierik, F.H.; De Jong, F.H.; Thomas, C.M.G.; Steegers-Theunissen, R.P.M. Does folic acid andzinc sulphate intervention affect endocrine parameters and sperm characteristics in men? Int. J. Androl. 2006,29, 339–345. [CrossRef] [PubMed]
68. Vihtamaki, T.; Parantainen, J.; Koivisto, A.M.; Metsa-Ketela, T.; Tuimala, R. Oral ascorbic acid increasesplasma oestradiol during postmenopausal hormone replacement therapy. Maturitas 2002, 42, 129–135.[CrossRef]
69. Maggio, M.; De Vita, F.; Lauretani, F.; Bandinelli, S.; Semba, R.D.; Bartali, B.; Cherubini, A.; Cappola, A.R.;Ceda, G.; Ferrucci, L. Relationship between Carotenoids, Retinol, and Estradiol Levels in Older Women.Nutrients 2015, 7, 6506–6519. [CrossRef] [PubMed]
70. Lerchbaum, E. Vitamin D and menopause—A narrative review. Maturitas 2014, 79, 3–7. [CrossRef]71. Lerchbaum, E.; Obermayer-Pietsch, B. Vitamin D and fertility: A systematic review. Eur. J. Endocrinol. 2012,
166, 765–778. [CrossRef]72. Karas, M.; Amir, H.; Fishman, D.; Danilenko, M.; Segal, S.; Nahum, A.; Koifmann, A.; Giat, Y.; Levy, J.;
Sharoni, Y. Lycopene interferes with cell cycle progression and insulin-like growth factor I signaling inmammary cancer cells. Nutr. Cancer 2000, 36, 101–111. [CrossRef]
73. Liu, C.; Lian, F.; Smith, D.E.; Russell, R.M.; Wang, X.D. Lycopene supplementation inhibits lung squamousmetaplasia and induces apoptosis via up-regulating insulin-like growth factor-binding protein 3 in cigarettesmoke-exposed ferrets. Cancer Res. 2003, 63, 3138–3144.
74. Hirsch, K.; Atzmon, A.; Danilenko, M.; Levy, J.; Sharoni, Y. Lycopene and other carotenoids inhibit estrogenicactivity of 17beta-estradiol and genistein in cancer cells. Breast Cancer Res. Treat. 2007, 104, 221–230.[CrossRef] [PubMed]
75. Kanagaraj, P.; Vijayababu, M.R.; Ravisankar, B.; Anbalagan, J.; Aruldhas, M.M.; Arunakaran, J. Effect oflycopene on insulin-like growth factor-I, IGF binding protein-3 and IGF type-I receptor in prostate cancercells. J. Cancer Res. Clin. Oncol. 2007, 133, 351–359. [CrossRef] [PubMed]
76. Welch, A.A. Nutritional influences on age-related skeletal muscle loss. Proc. Nutr. Soc. 2014, 73, 16–33.[CrossRef]
77. Van Dronkelaar, C.; van Velzen, A.; Abdelrazek, M.; van der Steen, A.; Weijs, P.J.M.; Tieland, M. Minerals andSarcopenia; The Role of Calcium, Iron, Magnesium, Phosphorus, Potassium, Selenium, Sodium, and Zinc onMuscle Mass, Muscle Strength, and Physical Performance in Older Adults: A Systematic Review. J. Am. Med.Dir. Assoc. 2018, 19, 6–11. [CrossRef]
78. Liu, Z.; Ye, F.; Zhang, H.; Gao, Y.; Tan, A.; Zhang, S.; Xiao, Q.; Zhang, B.; Huang, L.; Ye, B.; et al. Theassociation between the levels of serum ferritin and sex hormones in a large scale of Chinese male population.PLoS ONE 2013, 8, e75908. [CrossRef] [PubMed]

Nutrients 2020, 12, 1457 18 of 21
79. Aihara, K.; Nishi, Y.; Hatano, S.; Kihara, M.; Ohta, M.; Sakoda, K.; Uozumi, T.; Usui, T. Zinc, copper,manganese, and selenium metabolism in patients with human growth hormone deficiency or acromegaly.J. Pediatr. Gastroenterol. Nutr. 1985, 4, 610–615. [CrossRef]
80. Walfisch, S.; Walfisch, Y.; Kirilov, E.; Linde, N.; Mnitentag, H.; Agbaria, R.; Sharoni, Y.; Levy, J. Tomatolycopene extract supplementation decreases insulin-like growth factor-I levels in colon cancer patients. Eur. J.Cancer Prev. 2007, 16, 298–303. [CrossRef]
81. Vrieling, A.; Voskuil, D.W.; Bonfrer, J.M.; Korse, C.M.; Van Doorn, J.; Cats, A.; Depla, A.C.; Timmer, R.;Witteman, B.J.; E Van Leeuwen, F.; et al. Lycopene supplementation elevates circulating insulin-like growthfactor binding protein-1 and -2 concentrations in persons at greater risk of colorectal cancer. Am. J. Clin.Nutr. 2007, 86, 1456–1462. [CrossRef]
82. Gann, P.H.; Deaton, R.J.; Rueter, E.E.; Van Breemen, R.B.; Nonn, L.; Macias, V.; Han, M.; Ananthanarayanan, V.A Phase II Randomized Trial of Lycopene-Rich Tomato Extract Among Men with High-Grade ProstaticIntraepithelial Neoplasia. Nutr. Cancer 2015, 67, 1104–1112. [CrossRef]
83. Darago, A.; Sapota, A.; Matych, J.; Nasiadek, M.; Skrzypinska-Gawrysiak, M.; Kilanowicz, A. The correlationbetween zinc and insulin-like growth factor 1 (IGF-1), its binding protein (IGFBP-3) and prostate-specificantigen (PSA) in prostate cancer. Clin. Chem. Lab. Med. 2011, 49, 1699–1705. [CrossRef]
84. Lerchbaum, E.; Trummer, C.; Schwetz, V.; Pachernegg, O.; Heijboer, A.C.; Pilz, S.; Obermayer-Pietsch, B.Vitamin D and Testosterone in Healthy Men: A Randomized Controlled Trial. J. Clin. Endocrinol. Metab.2017, 102, 4292–4302. [CrossRef] [PubMed]
85. Lerchbaum, E.; Rabe, T. Vitamin D and female fertility. Curr. Opin. Obstet. Gynecol. 2014, 26, 145–150.[CrossRef] [PubMed]
86. Lundqvist, J.; Norlin, M.; Wikvall, K. 1alpha,25-Dihydroxyvitamin D3 affects hormone production andexpression of steroidogenic enzymes in human adrenocortical NCI-H295R cells. Biochim. Biophys. Acta 2010,1801, 1056–1062. [CrossRef] [PubMed]
87. Sayer, A.A. Sarcopenia. BMJ 2010, 341, 1. [CrossRef]88. Hayhoe, R.P.G.; Lentjes, M.A.H.; Mulligan, A.A.; Luben, R.N.; Khaw, K.T.; Welch, A.A. Cross-sectional
associations of dietary and circulating magnesium with skeletal muscle mass in the EPIC-Norfolk cohort.Clin. Nutr. 2019, 38, 317–323. [CrossRef]
89. Welch, A.A.; Jennings, A.; Kelaiditi, E.; Skinner, J.; Steves, C.J. Cross-sectional associations between dietaryantioxidant vitamins C,E and carotenoid intakes and sarcopenic indices in women aged 18–79 years. Calcif.Tissue Int. 2020, 106, 331–342. [CrossRef]
90. Cameron, D.; Welch, A.A.; Adelnia, F.; Bergeron, C.M.; Reiter, D.A.; Dominguez, L.J.; Ferrucci, L. Age andfunction are more closely associated with intracellular magnesium as assessed by 31P Magnetic ResonanceSpectroscopy, than with serum mangesium. Front. Physiol. 2019, 10, 1454. [CrossRef]
91. Landi, F.; Camprubi-Robles, M.; E Bear, D.; Cederholm, T.; Malafarina, V.; Welch, A.A.; Cruz-Jentoft, A.J.;Landi, F. Muscle loss: The new malnutrition challenge in clinical practice. Clin. Nutr. 2019, 38, 2113–2120.[CrossRef]
92. Welch, A.A.; Skinner, J.; Hickson, M. Dietary Magnesium May Be Protective for Aging of Bone and SkeletalMuscle in Middle and Younger Older Age Men and Women: Cross-Sectional Findings from the UK BiobankCohort. Nutrients 2017, 9, 1189. [CrossRef]
93. Welch, A.A.; Kelaiditi, E.; Jennings, A.; Steves, C.J.; Spector, T.D.; MacGregor, A. Dietary Magnesium IsPositively Associated With Skeletal Muscle Power and Indices of Muscle Mass and May Attenuate theAssociation Between Circulating C-Reactive Protein and Muscle Mass in Women. J. Bone Min. Res. 2016, 31,317–325. [CrossRef]
94. Semba, R.D.; Lauretani, F.; Ferrucci, L. Carotenoids as protection against sarcopenia in older adults.Arch. Biochem. Biophys. 2007, 458, 141–145. [CrossRef] [PubMed]
95. Cermak, N.M.; Res, P.T.; de Groot, L.C.; Saris, W.H.; van Loon, L.J. Protein supplementation augments theadaptive response of skeletal muscle to resistance-type exercise training: A meta-analysis. Am. J. Clin. Nutr.2012, 96, 1454–1464. [CrossRef] [PubMed]
96. Hickson, M. Nutritional interventions in sarcopenia: A critical review. Proc. Nutr. Soc. 2015, 74, 378–386.[CrossRef] [PubMed]
97. Chung, E.; Mo, H.; Wang, S.; Zu, Y.; Elfakhani, M.; Rios, S.R.; Chyu, M.-C.; Yang, R.-S.; Shen, C.-L. Potentialroles of vitamin E in age-related changes in skeletal muscle health. Nutr. Res. 2018, 49, 23–36. [CrossRef]

Nutrients 2020, 12, 1457 19 of 21
98. Takisawa, S.; Funakoshi, T.; Yatsu, T.; Nagata, K.; Aigaki, T.; Machida, S.; Ishigami, A. Vitamin C deficiencycauses muscle atrophy and a deterioration in physical performance. Sci. Rep. 2019, 9, 4702. [CrossRef]
99. Demirbag, R.; Yilmaz, R.; Erel, O. The association of total antioxidant capacity with sex hormones.Scand Cardiovasc. J. 2005, 39, 172–176. [CrossRef]
100. Van Poppel, G.; Goldbohm, R.A. Epidemiologic evidence for beta-carotene and cancer prevention. Am. J.Clin. Nutr. 1995, 62 (Suppl. 6), 1393s–1402s. [CrossRef]
101. Sharoni, Y.; Danilenko, M.; Dubi, N.; Ben-Dor, A.; Levy, J. Carotenoids and transcription. Arch. Biochem.Biophys. 2004, 430, 89–96. [CrossRef]
102. Davison, G.W.; Ashton, T.; George, L.; Young, I.S.; McEneny, J.; Davies, B.; Jackson, S.K.; Peters, J.R.;Bailey, D.M. Molecular detection of exercise-induced free radicals following ascorbate prophylaxis in type 1diabetes mellitus: A randomised controlled trial. Diabetologia 2008, 51, 2049. [CrossRef]
103. Alessio, H.M.; Goldfarb, A.H.; Cao, G. Exercise-induced oxidative stress before and after vitamin Csupplementation. Int. J. Sport Nutr. 1997, 7, 1–9. [CrossRef]
104. Rokitzki, L.; Logemann, E.; Huber, G.; Keck, E.; Keul, J. alpha-Tocopherol supplementation in racing cyclistsduring extreme endurance training. Int. J. Sport Nutr. 1994, 4, 253–264. [CrossRef] [PubMed]
105. McAnulty, S.R.; McAnulty, L.S.; Nieman, D.C.; Morrow, J.D.; Shooter, L.A.; Holmes, S.; Heward, C.;Henson, D.A. Effect of alpha-tocopherol supplementation on plasma homocysteine and oxidative stress inhighly trained athletes before and after exhaustive exercise. J. Nutr. Biochem. 2005, 16, 530–537. [CrossRef][PubMed]
106. De Oliveira Kde, J.; Donangelo, C.M.; de Oliveira, A.V., Jr.; da Silveira, C.L.; Koury, J.C. Effect of zincsupplementation on the antioxidant, copper, and iron status of physically active adolescents. Cell Biochem.Funct. 2009, 27, 162–166. [CrossRef] [PubMed]
107. Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Fusco, D.; Sisto, A.; Ortolani, E.; Savera, G.;Salini, S.; Marzetti, E. Age-Related Variations of Muscle Mass, Strength, and Physical Performance inCommunity-Dwellers: Results From the Milan EXPO Survey. J. Am. Med. Dir. Assoc. 2017, 18, 88 e17–88 e24.[CrossRef]
108. Reviews, C.S. Cochrane Handbook for Systematic Reviews of Interventions. Available online: http://community.cochrane.org/handbook (accessed on 4 March 2020).
109. Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred reporting items for sytematic reviewsand meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e100009. [CrossRef] [PubMed]
110. PRISMA. The PRISMA Checklist: Prisma-statement.org. 2009. Available online: http://prisma-statement.org/documents/PRISMA%202009%20checklist.pdf (accessed on 4 March 2020).
111. Network SIG. SIGN 50: A Guideline Developers Handbook 2019. Available online: https://www.sign.ac.uk/
sign-50 (accessed on 4 March 2020).112. Schmidt, A.; Luger, A.; Hörl, W.H. Sexual hormone abnormalities in male patients with renal failure. Nephrol.
Dial. Transplant. 2002, 17, 368–371. [CrossRef]113. Moller, S.; Becker, U. Insulin-like growth factor 1 and growth hormone in chronic liver disease. Dig. Dis.
1992, 10, 239–248. [CrossRef]114. Oh, Y. The insulin-like growth factor system in chronic kidney disease: Pathophysiology and therapeutic
opportunities. Kidney Res. Clin. Pract. 2012, 31, 26–37. [CrossRef]115. Cochrane. Cochrane Handbook 2017. Available online: http://handbook-5-1.cochrane.org/ (accessed on 4
March 2020).116. Handelsman, D.J.; Wartofsky, L. Requirement for Mass Spectrometry Sex Steroid Assays in the Journal of
Clinical Endocrinology and Metabolism. J. Clin. Endocrinol. Metab. 2013, 98, 3971–3973. [CrossRef]117. Stanczyk, F.Z.; Cho, M.M.; Endres, D.B.; Morrison, J.L.; Patel, S.; Paulson, R.J. Limitations of direct estradiol
and testosterone immunoassay kits. Steroids 2003, 68, 1173–1178. [CrossRef]118. Vieira, J.G.H.; Nakamura, O.H.; Ferrer, C.M.; Tachibana, T.T.; Endo, M.H.K.; Carvalho, V.M. The importance
of methodology in serum testosterone measurement: Comparison between a direct immunoassay and amethod based on high performance liquid chromatography and tandem mass spectrometry (HPLC/MS-MS).Arq. Bras. Endocrinol. Metabol. 2008, 52, 1050–1055. [CrossRef] [PubMed]
119. Cochran. Review Manager 5 (ReVMan5) [Computer Program]. Version 5.3: Copenhagen: The NordicCochrane Centre, The Cochran Collaboration. 2014. Available online: http://Community.cochrane.org/
(accessed on 4 March 2020).

Nutrients 2020, 12, 1457 20 of 21
120. Page, M.J.; Higgins, J.P.T.; Sterne, J.A.C. Chapter 13: Assessing risk of bias due to missing results in asynthesis. In Cochrane Handbook for Systematic Reviews of Interventions Version 60; Higgins, J.P.T., Thomas, J.,Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ,USA, 2019.
121. Olmedilla-Alonso, B.; Granado-Lorencio, F.; Blanco-Navarro, I. Carotenoids, retinol and tocopherols in blood:Comparability between serum and plasma (Li-heparin) values. Clin. Biochem. 2005, 38, 444–449. [CrossRef][PubMed]
122. Kamycheva, E.; Berg, V.; Jorde, R. Insulin-like growth factor I, growth hormone, and insulin sensitivity:The effects of a one-year cholecalciferol supplementation in middle-aged overweight and obese subjects.Endocrine 2013, 43, 412–418. [CrossRef] [PubMed]
123. Gee, J. Phase II Open Label, Multi-Center Clinical Trial of Modulation of Intermediate Endpoint Biomarkersby 1α-Hydroxyvitamin D2 in Patients With Clinically Localized Prostate Cancer and High Grade Pin. Prostate2013, 73, 970–978. [CrossRef]
124. Sinha-Hikim, I.; Duran, P.; Shen, R.; Lee, M.; Friedman, T.C.; Davidson, M.B. Effect of long term vitamin Dsupplementation on biomarkers of inflammation in Latino and African-American subjects with pre-diabetesand hypovitaminosis D. Horm. Metab. Res. 2015, 47, 280–283. [CrossRef]
125. Mason, C.; Tapsoba, J.D.D.; Duggan, C.; Imayama, I.; Wang, C.-Y.; Korde, L.A.; Stanczyk, F.; McTiernan, A.Effects of vitamin D supplementation during weight loss on sex hormones in postmenopausal women.Menopause 2016, 23, 645–652. [CrossRef]
126. Zhang, R.H.; Chen, K.J.; Lu, D.X.; Zhu, X.F.; Ma, X.C. A clinical study of Yigu capsule in treatingpostmenopausal osteoporosis. Chin. J. Integr. Med. 2005, 11, 97–103.
127. Heijboer, A.C.; Oosterwerff, M.; Schroten, N.F.; Eekhoff, E.M.; Chel, V.G.; De Boer, R.A.; Blankenstein, M.;Lips, P. Vitamin D supplementation and testosterone concentrations in male human subjects. Clin. Endocrinol.2015, 83, 105–110. [CrossRef]
128. Lerchbaum, E.; Trummer, C.; Theiler-Schwetz, V.; Kollmann, M.; Wölfler, M.; Heijboer, A.C.; Pilz, S.;Obermayer-Pietsch, B. Effects of vitamin D supplementation on androgens in men with low testosteronelevels: A randomized controlled trial. Eur. J. Nutr. 2018, 58, 3135–3146. [CrossRef]
129. Zittermann, A.; Ernst, J.B.; Prokop, S.; Fuchs, U.; Dreier, J.; Kuhn, J.; Knabbe, C.; Berthold, H.;Gouni-Berthold, I.; Gummert, J.F.; et al. Vitamin D supplementation does not prevent the testosterone declinein males with advanced heart failure: The EVITA trial. Eur. J. Nutr. 2019, 58, 673–680. [CrossRef]
130. Bonjour, J.P.; Benoit, V.; Pourchaire, O.; Rousseau, B.; Souberbielle, J.C. Nutritional approach for inhibitingbone resorption in institutionalized elderly women with vitamin D insufficiency and high prevalence offracture. J. Nutr. Health Aging 2011, 15, 404–409. [CrossRef] [PubMed]
131. Trummer, C.; Theiler-Schwetz, V.; Pandis, M.; Grübler, M.R.; Verheyen, N.; Gaksch, M.; Zittermann, A.;März, W.; Aberer, F.; Lang, A.; et al. Effects of Vitamin D Supplementation on IGF-1 and Calcitriol:A Randomized-Controlled Trial. Nutrients 2017, 9, 623. [CrossRef] [PubMed]
132. Persson, M.; Hytter-Landahl, A.; Brismar, K.; Cederholm, T. Nutritional supplementation and dietary advicein geriatric patients at risk of malnutrition. Clin. Nutr. 2007, 26, 216–224. [CrossRef] [PubMed]
133. Holick, M.F.; Lamb, J.; Lerman, R.H.; Konda, V.R.; Darland, G.; Minich, D.M.; Desai, A.; Chen, T.; Austin, M.;Kornberg, J.; et al. Hop rho iso-alpha acids, berberine, vitamin D3 and vitamin K1 favorably impactbiomarkers of bone turnover in postmenopausal women in a 14-week trial. J. Bone Miner. Metab. 2010, 28,342–350. [CrossRef]
134. Lamb, J.; Holick, M.F.; Lerman, R.H.; Konda, V.R.; Minich, D.M.; Desai, A.; Chen, T.; Austin, M.; Kornberg, J.;Chang, J.-L.; et al. Nutritional supplementation of hop rho iso-alpha acids, berberine, vitamin D(3),and vitamin K(1) produces a favorable bone biomarker profile supporting healthy bone metabolism inpostmenopausal women with metabolic syndrome. Nutr. Res. 2011, 31, 347–355. [CrossRef]
135. Alehagen, U.; Johansson, P.; Aaseth, J.; Alexander, J.; Brismar, K. Increase in insulin-like growth factor 1(IGF-1) and insulin-like growth factor binding protein 1 after supplementation with selenium and coenzymeQ10. A prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens.PLoS ONE 2017, 12, e0178614. [CrossRef]
136. Torbergsen, A.C.; Watne, L.O.; Frihagen, F.; Wyller, T.B.; Mowe, M. Effects of nutritional intervention uponbone turnover in elderly hip fracture patients. Randomized controlled trial. Clin. Nutr. ESPEN 2019, 29,52–58. [CrossRef]

Nutrients 2020, 12, 1457 21 of 21
137. Jensen, C.; Holloway, L.; Block, G.; Spiller, G.; Gildengorin, G.; Gunderson, E.; Butterfield, G.; Marcus, R.Long-term effects of nutrient intervention on markers of bone remodeling and calciotropic hormones inlate-postmenopausal women. Am. J. Clin. Nutr. 2002, 75, 1114–1120. [CrossRef]
138. Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Intention-to-treatversus per-protocol analysis. Perspect. Clin. Res. 2016, 7, 144–146. [CrossRef]
139. Hoenjet, K.M.; Dagnelie, P.C.; Delaere, K.P.; Wijckmans, N.E.; Zambon, J.V.; Oosterhof, G.O. Effect of anutritional supplement containing vitamin E, selenium, vitamin c and coenzyme Q10 on serum PSA inpatients with hormonally untreated carcinoma of the prostate: A randomised placebo-controlled study.Eur. Urol. 2005, 47, 433–439. [CrossRef]
140. Kranse, R.; Dagnelie, P.C.; Van Kemenade, M.C.; De Jong, F.H.; Blom, J.H.; Tijburg, L.B.; Weststrate, J.A.;Schröder, F.H. Dietary intervention in prostate cancer patients: PSA response in a randomized double-blindplacebo-controlled study. Int. J. Cancer 2005, 113, 835–840. [CrossRef] [PubMed]
141. Vidlar, A.; Vostálová, J.; Ulrichová, J.; Student, V.; Krajicek, M.; Vrbkova, J.; Simanek, V. The safety and efficacyof a silymarin and selenium combination in men after radical prostatectomy-a six month placebo-controlleddouble-blind clinical trial. Biomed. Pap. 2010, 154, 239–244. [CrossRef] [PubMed]
142. Vostalova, J.; Vidlar, A.; Ulrichova, J.; Vrbkova, J.; Simanek, V.; Student, V. Use of selenium-silymarin mixreduces lower urinary tract symptoms and prostate specific antigen in men. Phytomedicine 2013, 21, 75–81.[CrossRef] [PubMed]
143. Van Amsterdam, J.; van der Horst-Graat, J.; Bischoff, E.; Steerenberg, P.; Opperhuizen, A.; Schouten, E. Theeffect of vitamin E supplementation on serum DHEA and neopterin levels in elderly subjects. Int. J. Vitam.Nutr. Res. 2005, 75, 327–331. [CrossRef] [PubMed]
144. Zhu, K.; Meng, R.; A Kerr, D.; Devine, A.; Solah, V.; Binns, C.W.; Prince, R.L. The effects of a two-yearrandomized, controlled trial of whey protein supplementation on bone structure, IGF-1, and urinary calciumexcretion in older postmenopausal women. J. Bone Miner. Res. 2011, 26, 2298–2306. [CrossRef] [PubMed]
145. Larouche, D.; Hanna, M.; Chang, S.L.; Jacob, S.; Têtu, B.; Diorio, C. Evaluation of Antioxidant Intakes inRelation to Inflammatory Markers Expression within the Normal Breast Tissue of Breast Cancer Patients.Integr. Cancer Ther. 2017, 16, 485–495. [CrossRef]
146. Watts, E.L.; Appleby, P.N.; Albanes, D.; Black, A.; Chan, J.M.; Chen, C.; Cirillo, P.M.; Cohn, B.A.; Cook, M.B.;Donovan, J.L.; et al. Circulating sex hormones in relation to anthropometric, sociodemographic andbehavioural factors in an international dataset of 12,300 men. PLoS ONE 2017, 12, e0187741. [CrossRef]
147. Watts, E.L.; Perez-Cornago, A.; Appleby, P.N.; Albanes, D.; Ardanaz, E.; Black, A.; Bueno-De-Mesquita, H.B.;Chan, J.M.; Chen, C.; Chubb, S.P.; et al. The associations of anthropometric, behavioural and sociodemographicfactors with circulating concentrations of IGF-I, IGF-II, IGFBP-1, IGFBP-2 and IGFBP-3 in a pooled analysisof 16,024 men from 22 studies. Int. J. Cancer 2019, 145, 3244–3256. [CrossRef]
148. Bingham, S.A.; Cassidy, A.; Cole, T.J.; Welch, A.; Runswick, S.A.; Black, A.E.; Thurnham, D.; Bates, C.;Khaw, K.T.; Key, T.J.A.; et al. Validation of weighed records and other methods of dietary assessment usingthe 24 h urine nitrogen technique and other biological markers. Br. J. Nutr. 1995, 73, 531–550. [CrossRef]
149. A Bingham, S.; Luben, R.N.; Welch, A.; Low, Y.L.; Khaw, K.T.; Wareham, N.; Day, N. Associations betweendietary methods and biomarkers, and between fruits and vegetables and risk of ischaemic heart disease,in the EPIC Norfolk Cohort Study. Int. J. Epidemiol. 2008, 37, 978–987. [CrossRef]
150. Hayhoe, R.P.G.; Lentjes, M.A.H.; Mulligan, A.A.; Luben, R.N.; Khaw, K.T.; Welch, A.A. Carotenoid dietaryintakes and plasma concentrations are associated with heel bone ultrasound attenuation and osteoporoticfracture risk in the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk cohort.Br. J. Nutr. 2017, 117, 1439–1453. [CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open accessarticle distributed under the terms and conditions of the Creative Commons Attribution(CC BY) license (http://creativecommons.org/licenses/by/4.0/).