
Effectiveness of the current dominant approach to integrated care in the NHS
19
Greater Manchester Primary Care Patient Safety Translational Research Centre Effectiveness of the current dominant approach to integrated care in the NHS: A systematic review of case management Jonathan Stokes This presentation summarises independent research funded by the NIHR Greater Manchester PSTRC. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
-
Upload
nuffield-trust -
Category
Healthcare
-
view
41 -
download
0
Transcript of Effectiveness of the current dominant approach to integrated care in the NHS
Greater ManchesterPrimary Care Patient SafetyTranslational Research Centre
Effectiveness of the current dominant approach to integrated care in the NHS: A systematic review of case management
Jonathan Stokes
This presentation summarises independent research funded by the NIHR Greater Manchester PSTRC. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.

BackgroundHealth system challenges
Greater Manchester Primary Care Patient Safety Translational Research Centre
Cost
Complexity
Barnettetal,2012
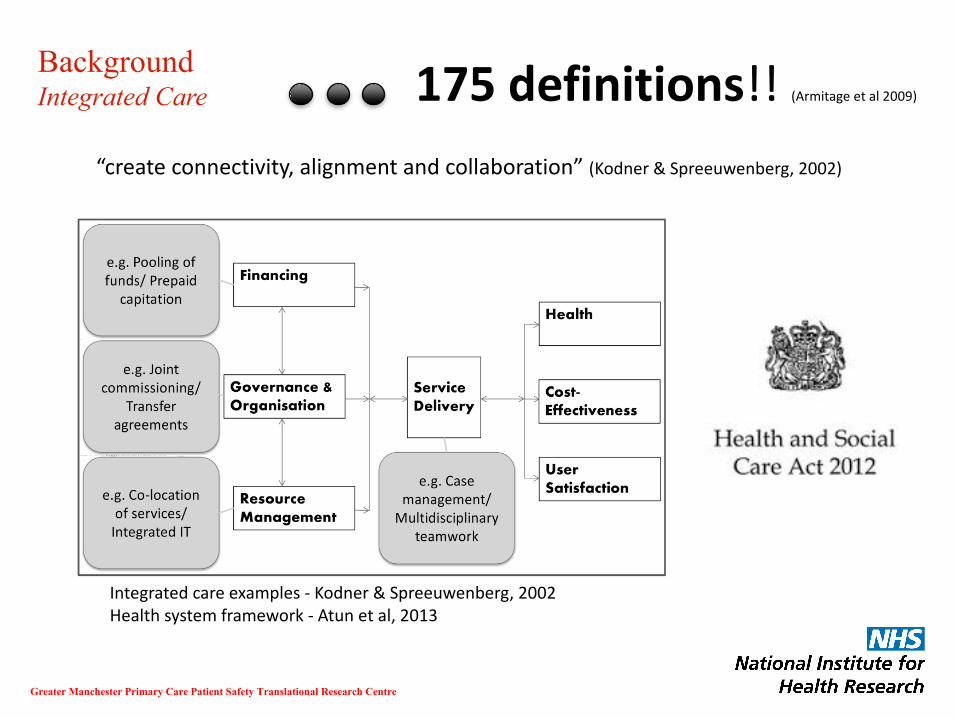
BackgroundIntegrated Care
Greater Manchester Primary Care Patient Safety Translational Research Centre
“createconnectivity,alignmentandcollaboration”(Kodner &Spreeuwenberg,2002)
Integratedcareexamples- Kodner &Spreeuwenberg,2002Healthsystemframework- Atun etal,2013
175definitions!!(Armitageetal2009)

Integrated care in the English NHS
Greater Manchester Primary Care Patient Safety Translational Research Centre
Effectivenessofthismodelnotbeensubjectedtorigorousquantitativesynthesisacrossallhealthsystemgoals
Integrated care emphasis Percentage of CCGs
Multidisciplinaryteamcasemanagement(MDT):Identificationofhighriskgroups(usuallyusingarisk-stratificationtool),implementationofastructuredcareplan,andregularmonitoringbyamultidisciplinaryteambasedattheprimarycarelevel(ofteninvolvingasocialworker)
81%
Othercasemanagement:Similartotheabovemodel,butthecareplanisimplementedandregularlymonitoredbyasingle,dedicatedcasemanager(oftenapracticenurse,oranintensivecasemanager)
14%
Jointplanningandcommissioning:IntegratedcareemphasisplacedonestablishingbetterlinkswiththeLocalAuthorityandotherorganisationallinkse.g.throughjoinedupplansandmulti-agencyboards
5%
10%randomsampleof211CCGs(2013)Publicallyavailabledocumentsreviewed– whateachbrandingasintegratedcare?

MethodsStudy Selection
Greater Manchester Primary Care Patient Safety Translational Research Centre
Population: Adults (18+) with long-term conditionsIntervention:Identifying ‘at-risk’ patients to case manageCase management Primary care/community-basedComparison:Usual care or no-case management
Outcomes:Health – self-assessed health status, mortality;Cost – total cost of care, healthcare utilisation (primary and non-specialistcare and secondary care separately), and; Satisfaction – patient satisfactionStudy design:Cochrane EPOC methodology (RCT, nRCT, CBA, ITS)
Search strategy
DatabasesMEDLINE EMBASECINAHL Cochrane (CENTRAL) HMICCAB Global Health
Blocks of search terms1. Case management2. EPOC methodology filter3. Primary care filter
Exclusions
• Mental health only• Hospital discharge
planning• Non-English
language/ grey literature
QualityEPOC Risk of bias tool
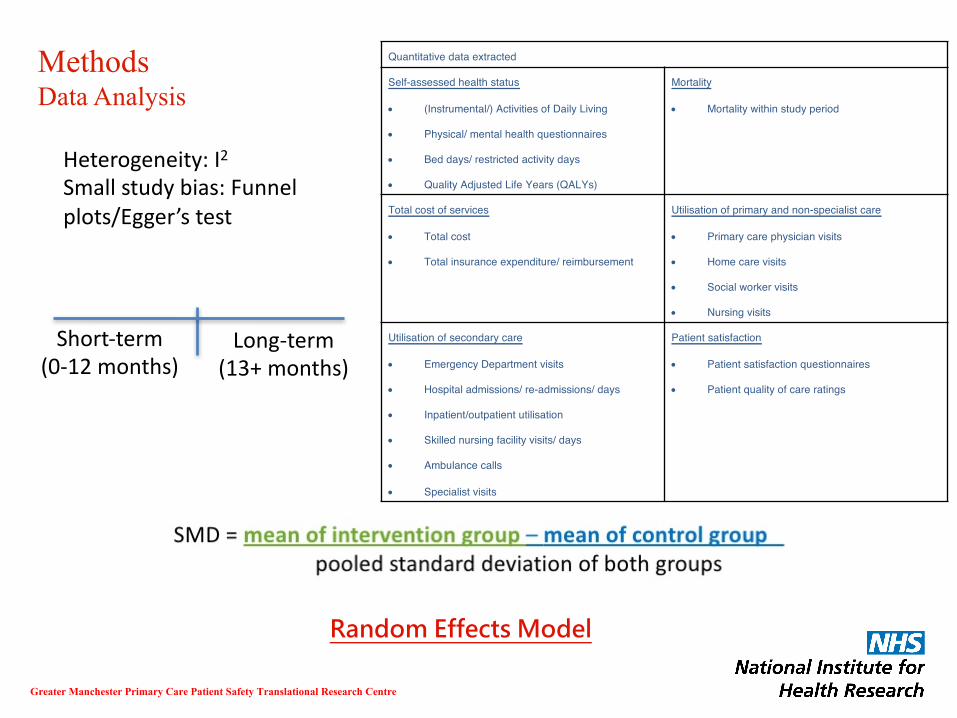
MethodsData Analysis
Greater Manchester Primary Care Patient Safety Translational Research Centre
Quantitative data extracted
Self-assessed health status
• (Instrumental/) Activities of Daily Living
• Physical/ mental health questionnaires
• Bed days/ restricted activity days
• Quality Adjusted Life Years (QALYs)
Mortality
• Mortality within study period
Total cost of services
• Total cost
• Total insurance expenditure/ reimbursement
Utilisation of primary and non-specialist care
• Primary care physician visits
• Home care visits
• Social worker visits
• Nursing visits
Utilisation of secondary care
• Emergency Department visits
• Hospital admissions/ re-admissions/ days
• Inpatient/outpatient utilisation
• Skilled nursing facility visits/ days
• Ambulance calls
• Specialist visits
Patient satisfaction
• Patient satisfaction questionnaires
• Patient quality of care ratings
Short-term(0-12months)
Long-term(13+months)
Heterogeneity:I2Smallstudybias:Funnelplots/Egger’stest
Random Effects Model

ResultsStudies included
Greater Manchester Primary Care Patient Safety Translational Research Centre
• meanage:75.7(49.0to87.3)
• setting:64%LowPHCstrength
• patients:8%Specificconditions
• intervention:58%MDTcasemanagement;33%Socialworkerinvolved
• design:78%RCT
• follow-up:6to60months
• quality(9criteria):64%7+;30%4-6;6%3-

ResultsMeta-analysis
Greater Manchester Primary Care Patient Safety Translational Research Centre
Health
No. of studies:
Self-assessed health status
14
9
Mortality
1213
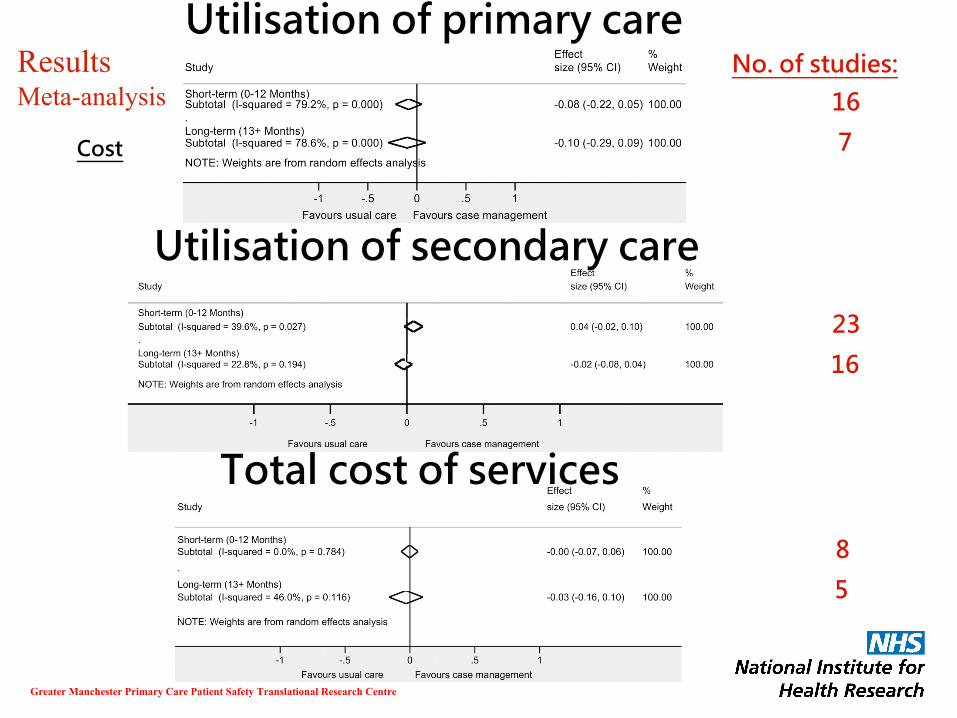
ResultsMeta-analysis
Greater Manchester Primary Care Patient Safety Translational Research Centre
Cost
No. of studies:
Utilisation of primary care
16
7
Utilisation of secondary care
23
16
Total cost of services
8
5

ResultsMeta-analysis
Greater Manchester Primary Care Patient Safety Translational Research Centre
Satisfaction
No. of studies:
Patient satisfaction
8
4
DiscussionSummary of findings
Greater Manchester Primary Care Patient Safety Translational Research Centre
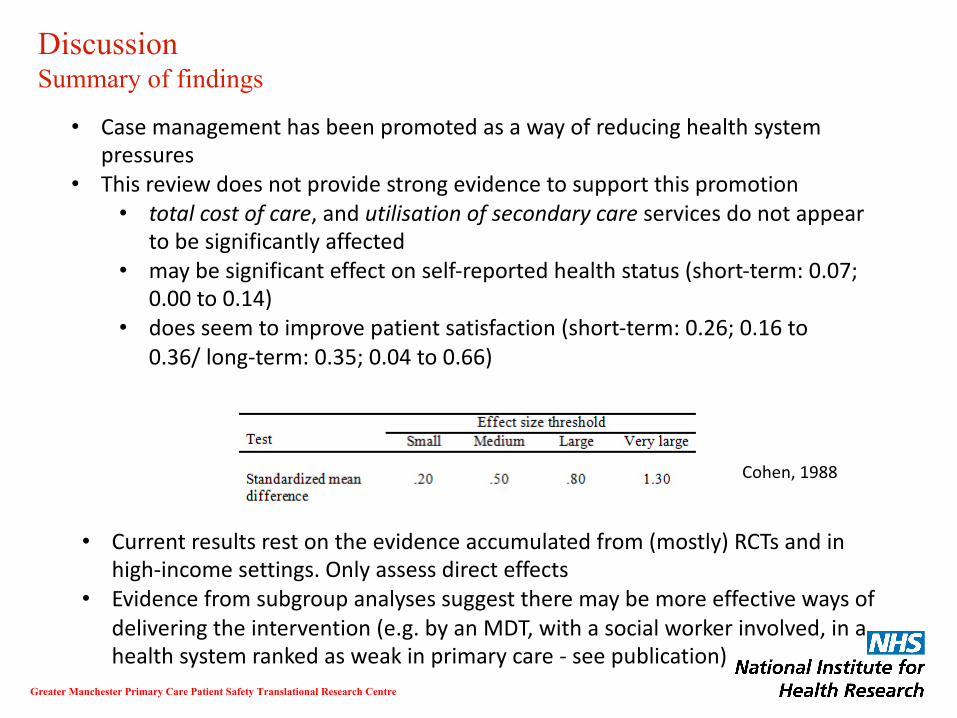
• Casemanagementhasbeenpromotedasawayofreducinghealthsystempressures
• Thisreviewdoesnotprovidestrongevidencetosupportthispromotion• totalcostofcare,andutilisationofsecondarycareservicesdonotappear
tobesignificantlyaffected• maybesignificanteffectonself-reportedhealthstatus(short-term:0.07;
0.00to0.14)• doesseemtoimprovepatientsatisfaction(short-term:0.26;0.16to
0.36/long-term:0.35;0.04to0.66)
Cohen,1988
• Currentresultsrestontheevidenceaccumulatedfrom(mostly)RCTsandinhigh-incomesettings.Onlyassessdirecteffects
• Evidencefromsubgroupanalysessuggesttheremaybemoreeffectivewaysofdeliveringtheintervention(e.g.byanMDT,withasocialworkerinvolved,inahealthsystemrankedasweakinprimarycare- seepublication)

DiscussionAim of integration
Greater Manchester Primary Care Patient Safety Translational Research Centre
• Noevidencethatcurrentlyintegratedcarewillbethemagicbullethopedtobe:• Cost/utilisation• Healthbenefits• Satisfaction
• ConflictbetweenNHS‘patient-centered’definition(aim!)ofintegratedcareandwhatcommissionerswantittoachieve?• Satisfaction(patientexperienceofcare)vCost• E.g.Fentonetal,2012– ‘Thecostofsatisfaction’
• Whatdowewantintegratedcaretoachieve?...Andisitableto?
DiscussionFocus on high-risk groups
Greater Manchester Primary Care Patient Safety Translational Research Centre
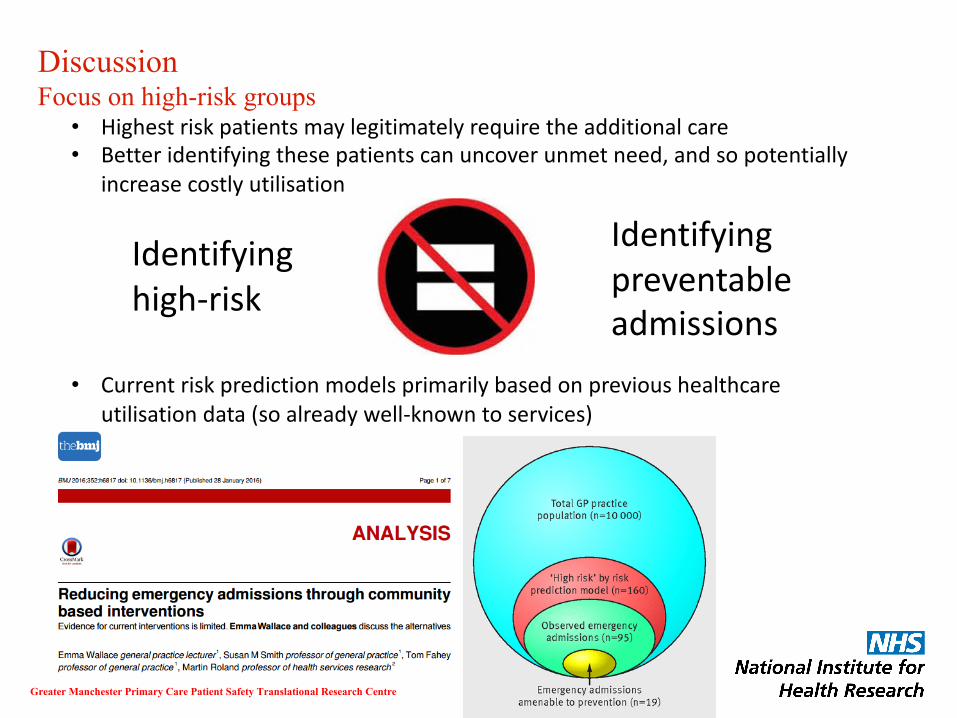
• Highestriskpatientsmaylegitimatelyrequiretheadditionalcare• Betteridentifyingthesepatientscanuncoverunmetneed,andsopotentially
increasecostlyutilisation
• Currentriskpredictionmodelsprimarilybasedonprevioushealthcareutilisationdata(soalreadywell-knowntoservices)
Identifyinghigh-risk
Identifyingpreventableadmissions

DiscussionAlternative means of integration
Greater Manchester Primary Care Patient Safety Translational Research Centre
Integratedcareexamples- Kodner &Spreeuwenberg,2002Healthsystemframework- Atun etal,2013
DiscussionOrganisational integration – e.g. ACOs
Greater Manchester Primary Care Patient Safety Translational Research Centre
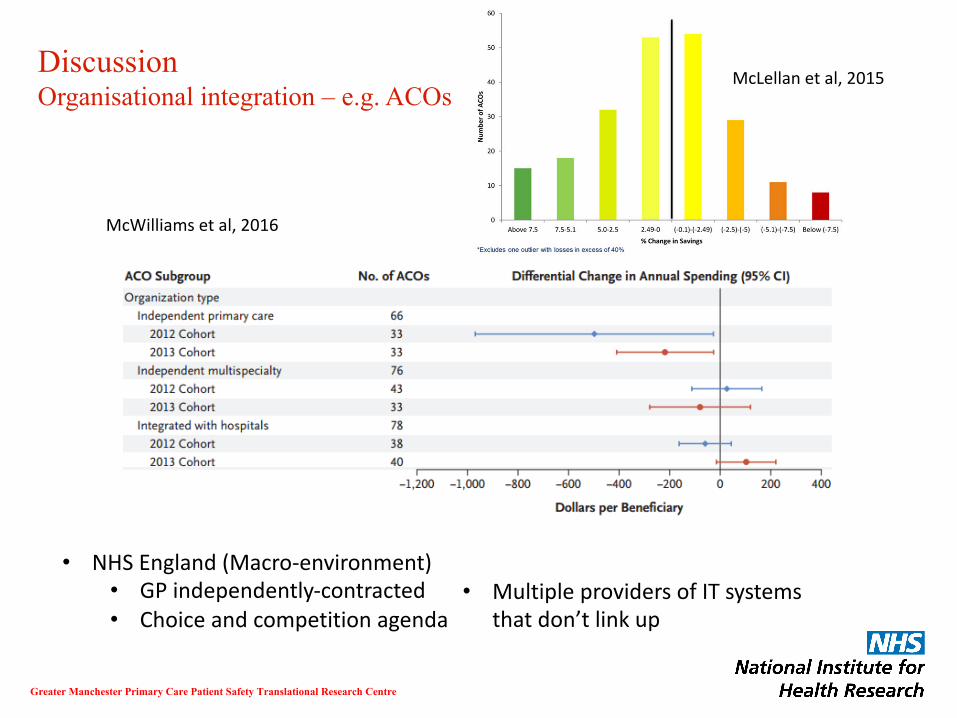
• NHSEngland(Macro-environment)• GPindependently-contracted• Choiceandcompetitionagenda
McLellanetal,2015
McWilliamsetal,2016
• MultipleprovidersofITsystemsthatdon’tlinkup
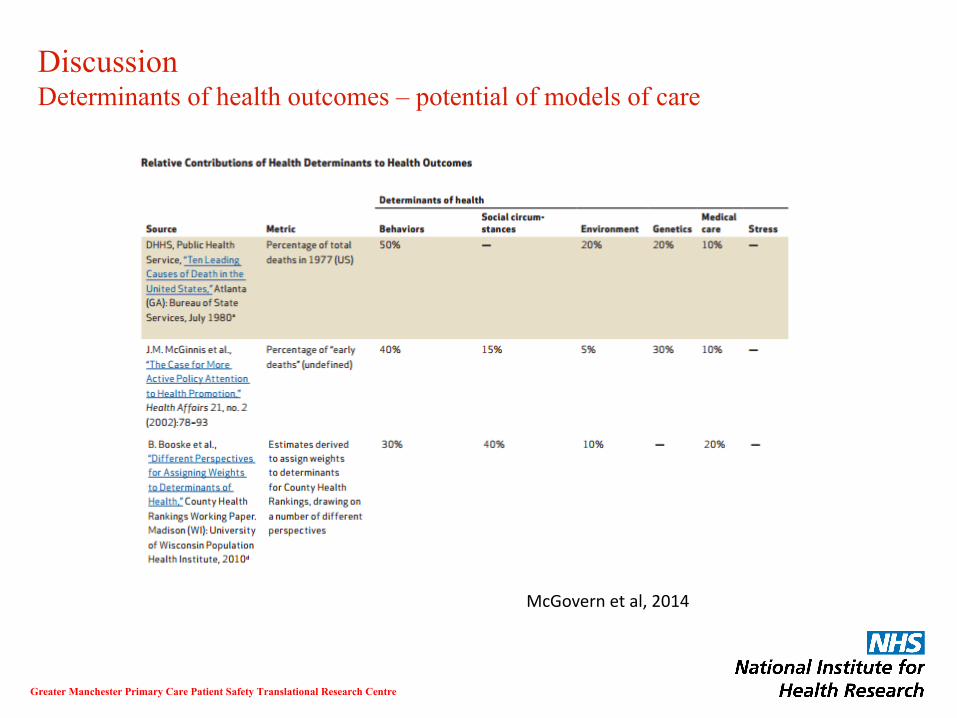
DiscussionDeterminants of health outcomes – potential of models of care
Greater Manchester Primary Care Patient Safety Translational Research Centre
McGovernetal,2014

DiscussionAlternatives to integrated care?
Greater Manchester Primary Care Patient Safety Translational Research Centre
• Addressingcurrentfundinggapismostpressingchallenge• Prevention/earlyintervention?
• Someevidenceofabilitytoreducedemand(Purdy,2010)…butlikelytotakealongtime
• Expansionofprimarycare?• Someevidenceofreducedemergencyadmissionsforminor
conditions(Whittakeretal,2016)• Willonlyrealisecostsavingsifsecondarycareservices
decommissioned• Workforceproblems,e.g.lackofGPs
• Addressfundinggapdirectly?• Healthexpenditurepercapita
• Reverse‘self-inflicted’demandincreases?• Austeritychoices(e.g.publichealth,socialcarebudgets,etc.)• Privatisation• PFI,Consultancy/Agencystaff
Acknowledgements
Supervisors:
• Peter Bower
• Kath Checkland
• Søren Rud Kristensen
• Sudeh Cheraghi-Sohi
Other Co-authors:
• Maria Panagioti
• Rahul Alam
Greater Manchester Primary Care Patient Safety Translational Research Centre

A partnership between
The NIHR Greater Manchester Primary Care Patient Safety Translational Research Centre is funded by the National Institute for Health Research (NIHR) and is a partnership between the University of Manchester and Salford Royal NHS Foundation Trust


















