Effective strategies for
22
Effective Strategies for Implementing Clinical Guidelines; a systematic review A presentation of graduate research for the students, faculty and guests of Regis University December 01, 2007
-
Upload
casey-dills -
Category
Technology
-
view
294 -
download
8
Transcript of Effective strategies for

Effective Strategies for Implementing Clinical Guidelines;
a systematic review
A presentation of graduate research for the students, faculty and guests of Regis University December 01, 2007

“Clinical practice guidelines are systematically developed
statements to assist practitioner and patient decisions about appropriate health care for
specific clinical circumstances” (Institute of Medicine,
1990)

Importance
Reduce variation in clinical practices
Improve quality outcomes
Improve cost effectiveness

Criticisms
‘Cookbook Medicine’Not ReliableNot relevant to the presenting condition(s)Liability

A changing environment
• Increased emphasis on clinical quality
• Patient safety
• Cost effectiveness
• Transparency
• Payment structures (pay-for-performance)

Research Objective
Identify the most effective strategies ofimplementing clinical guidelines through an evidence based approach
Validate physician trustGuide health policyPresent opportunities to promote cost effective improvements in patient care

Methods
Endorsed by the Cochrane Effective Practice and Organization of Care (EPOC)
• Systematic review methodology has the ability to manage potentially unmanageable amounts of information (Torgeson, 2003)

Using qualitative research in systematic reviews
When is not appropriate to use meta-analysis?• Broad review question• Diverse studies (mixing apples with oranges)
Guidance on the Conduct of Narrative Synthesis in Systematic Reviews;
qualitative research methods from the Institute for health research at Lancaster University, London.
Steps for Conducting Narrative Synthesis
• Mapping
• Specify the Review Question
• Identify studies for inclusion
• Data Extraction and quality appraisal
• Synthesis
• Reporting conclusions

Inclusion Criteria using PICO
1) Study meets 4 PICO
2) Study meets 3 PICO
3) Study meets 2 PICO
4) Study meets 1 PICO
5) Study meets 0 PICO
Identify studies for inclusion

Data extraction and quality appraisal
EPPI centre approach
Trustworthiness Appropriateness Relevance Overall Weight A) HIGH
B) MEDIUM
C) LOW

Search Strategy
• Database search; EBSCOhost
• Full-texts published 1990-2007
• (clinical guidelines OR clinical practice guidelines OR evidence based guidelines) and (implement OR disseminate OR integrate) and/or (quality improvement OR process improvement)

Yield
• First search yielded 2727 abstracts for review
• Second screening evaluated 129 articles • Appraisal identified 56 articles for critical
review by first and second reviewer agreement
• Final appraisal identified 33 articles for synthesis

a r t i c l e p d f # Population (setting)
Intervention (Implementation factors present)
Comaprisons (pre/post design)
Outcomes (identified supported)
A Trustworthiness
B Appropriateness
C Relevance
D Overall weight comments
1211980.pdfHospitals yes yes yes 1 b high medium medium medium research does not provide conlcusive evidence to support review question
2444820.pdfclinicical alliance yes no yes 2 b medium medium medium medium clinical focus, lacks appropriateness to answer review question
3009671.pdfPeds Clinics yes yes yes 1 b high mdium high medium controled study, lacks strong approprateness of review question, topical relevance high
3740011.pdfclinicians yes no yes 2 c medium low medium low qualitative desing of guidleine use, lacks significance to review question, offers theoretical and evidenced based topical relevance
3970231.pdfGP yes yes Yes 1 a high high high high controlled study with strong appropriateness to review question
3970284.pdfPCP/GP yes yes yes 2 b medium medium low medium qualitative aevaluation of use of guidelines lacks relevance to review question,
3972072.pdfHospitals Hungry yes yes yes 1 a high medium high high trustworthy study methods, strong topical relevance, lacks some key componants of review question, but offers strong appropriateness to the relevance of the review question
4460579.pdfSingle practice yes yes yes 1 a medium high high high not scholorly, strong appropriateness to review quesiton, strong relevance
4997435.pdfNursing no no yes 3 c medium low low low research based opinion
5172083.pdfno no no no 5 c low low low low commercial proposoal
5184270.pdfGP Austraila no yes no 3 c medium low low low lacks appropriateness to answer review question
5184435.pdfPractice no no no 4 c low low low low lacks appropriateness to answer review question
5186676[1].pdfFP Canada yes yes yes 1 b high medium medium medium qualitative evaluation with componants appropriate to answer review question
5277923.pdfUrban GP yes yes yes 1 b high medium medium medium qaulitative desing, lacks appropriateness to asnwering review question
5302024.pdfHospital yes yes yes 1 b high medium low medium trustworthy research, lacks appropriateness to answering review question
5333208.pdfhospital units yes no yes 2 c medium low medium low lacks approrpiateness to answer review question
5383238.pdfpractices yes yes yes 1 a high high high high trustoworthy research design, appropriate to answering review question
53832385520966.pdfAlliances yes no yes 2 c low low medium low consensus, lacks appropriateness to answer review question
5608247.pdfclinics yes yes yes 1 a high medium high high qualitaive research design, lacks appropriateness to review question, offers strong relevance to review question
5661963[1].pdfno no no no 5 c low low low low has no appropriateness to asnwering review question
5801733[1].pdfclinics Finland yes yes yes 1 b medium medium low medium qualitative desing lacking in appropriateness to answering review question
5861964.pdfhospital units yes yes yes 1 b medium medium medium medium qaulitative research desing, moderate approriateness and relevence toanswer review queistion
5928424.pdfSNF 10 yes yes yes 1 a high high high high experimental design, strong appropriateness to asnwer review quation
6071232.pdfhospital yes no yes 2 c low low medium low non research, lacks approrpiateness to review question, offers moderade relevance to review question
6433398.pdfHealth Trusts yes yes yes 1 b medium medium high medium trustworthy research design, moderate appropriateness with high relevacne to review question
6494343.pdfCommunity RN yes yes yes 1 b medium high high high action research with appropriateness to review question, strong relevance to answer review question
6697833[1].pdfno no no no 5 c low low low low no relevance or appropriateness to review question
6712275[1].pdfBirth Center yes no yes 2 b medium medium medium medium moderate appropriatness to answer review question identified
6725285[1].pdfnone yes no yes 3 c low low medium low opinion based, moderate relevance to answering review question
6756415.pdfno no no no 5 b low medium high medium opinion based, with a strong relevance to answering review question
6756432.pdfhospital China yes yes yes 1 a high high high hgih trustworthy research desing, supports appropriateness to answer review question
6756432[1].pdf6822903[1].pdfhospital yes yes yes 1 b low medium high medium lacks research design, has componants of appropriateness to review question, high releveance to review question
6823752.pdfhospital yes no yes 2 b medium medium emdium medium lacks research design, has noted appropriateness and relevance to answer review question
6879242.pdfperinatal unit yes no yes 2 b medium medium low medium lacks research design, moderate appropriateness
6879246.pdfneonate unit yes no yes 2 b medium medium low medium lacks research design
6906180.pdfHMO clinics yes no yes 2 a high high medium high trustworthy qualitative design, strong appropriateness to review question
6910687.pdfhospital yes yes yes 1 a high high high high mixed method reserch, appropriateness and relevance to review question
6985898[1].pdfhospitals 4 yes yes yes 1 c high low low low controled study, lacks appropriateness to review question
6987359.pdfhospital yes yes yes 1 a high medium high high controlled study, has appropriateness and relevance to answer review question
7254449.pdforganization group hospitals yes no yes 2 a high high high high trusworthy study desing, strong appropriateness and relevance to review question
7296678.pdfhospital yes no yes 2 a high medium high high trustworthy study design, has componants of approrpirateness to review question, strong relevance to review question
7296678[1].pdf
Synthesis
• Thematic Analysis GroupingGrouping by common metaphors, concepts and themes
differentiated by effective vs. non-effective strategy
• Reciprocal TranslationExplores relationships within and between studies
Meta-ethnography approach to derive a constant comparison of themes to deduce primary conclusions
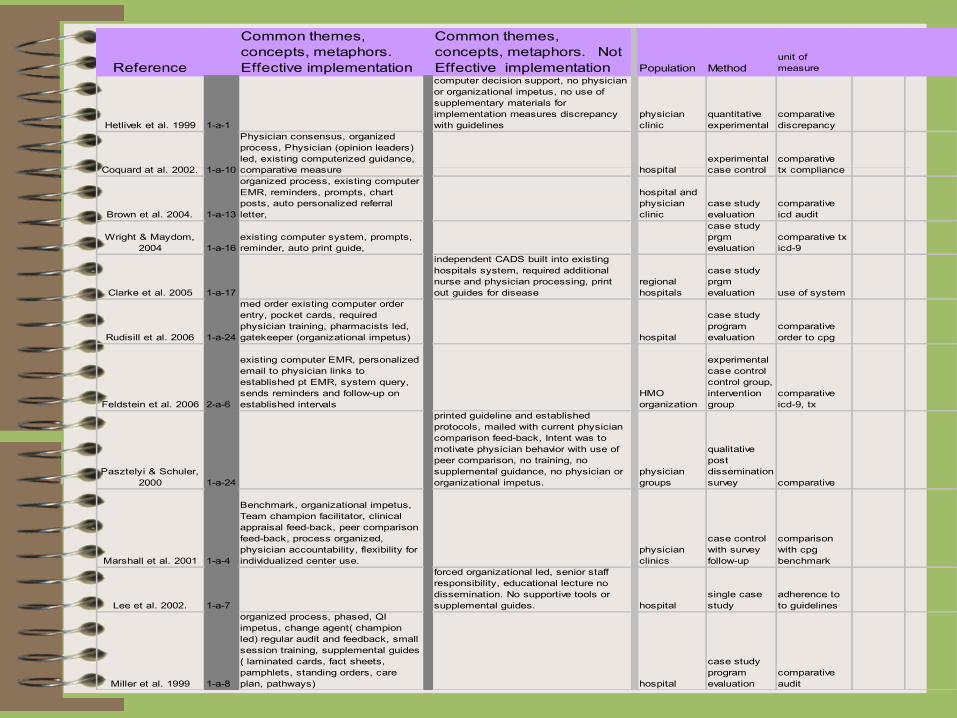
Reference
Common themes, concepts, metaphors. Effective implementation
Common themes, concepts, metaphors. Not Effective implementation Population Method
unit of measure
Hetlivek et al. 1999 1-a-1
computer decision support, no physician or organizational impetus, no use of supplementary materials for implementation measures discrepancy with guidelines
physician clinic
quantitative experimental
comparative discrepancy
Coquard at al. 2002. 1-a-10
Physician consensus, organized process, Physician (opinion leaders) led, existing computerized guidance, comparative measure hospital
experimental case control
comparative tx compliance
Brown et al. 2004. 1-a-13
organized process, existing computer EMR, reminders, prompts, chart posts, auto personalized referral letter,
hospital and physician clinic
case study evaluation
comparative icd audit
Wright & Maydom, 2004 1-a-16
existing computer system, prompts, reminder, auto print guide,
case study prgm evaluation
comparative tx icd-9
Clarke et al. 2005 1-a-17
independent CADS built into existing hospitals system, required additional nurse and physician processing, print out guides for disease
regional hospitals
case study prgm evaluation use of system
Rudisill et al. 2006 1-a-24
med order existing computer order entry, pocket cards, required physician training, pharmacists led, gatekeeper (organizational impetus) hospital
case study program evaluation
comparative order to cpg
Feldstein et al. 2006 2-a-6
existing computer EMR, personalized email to physician links to established pt EMR, system query, sends reminders and follow-up on established intervals
HMO organization
experimental case control control group, intervention group
comparative icd-9, tx
Pasztelyi & Schuler, 2000 1-a-24
printed guideline and established protocols, mailed with current physician comparison feed-back, Intent was to motivate physician behavior with use of peer comparison, no training, no supplemental guidance, no physician or organizational impetus.
physician groups
qualitative post dissemination survey comparative
Marshall et al. 2001 1-a-4
Benchmark, organizational impetus, Team champion facilitator, clinical appraisal feed-back, peer comparison feed-back, process organized, physician accountability, flexibility for individualized center use.
physician clinics
case control with survey follow-up
comparison with cpg benchmark
Lee et al. 2002. 1-a-7
forced organizational led, senior staff responsibility, educational lecture no dissemination. No supportive tools or supplemental guides. hospital
single case study
adherence to to guidelines
Miller et al. 1999 1-a-8
organized process, phased, QI impetus, change agent( champion led) regular audit and feedback, small session training, supplemental guides ( laminated cards, fact sheets, pamphlets, standing orders, care plan, pathways) hospital
case study program evaluation
comparative audit

Results non-effective
• Implementation strategy was passive • Guidelines are not generally accepted
• Guidelines are to long or complex • Implementation lacks accountability and
ownerships • Implementation process was unorganized or
required competing organizational values

Results Effective • Implementation is effective when applied to
structured quality improvements• Implementation is effective when guidelines are
are used as a benchmark or other comparative measure
• Regular feedback is critical to successful implementation
• Assistive supports in real-time help facilitate implementation
• Organizational setting must be supportive

Conceptual findings
• Quality Improvement facilitates social influencing behavior by acting as its vehicle
• Feedback and use of other comparative measures promotes group and individual competition & facilitating social influence through perceived intention.
• Knowledge translation; The use of assistive supports in real time that promote guidelines implementation presents a social influence at the level of interpersonal cognitive processing
• Organizational cultures are a construct to social influence where the organizations social structure has the most ability to influence either positively or negatively to the desired implementation.

Conclusion
Evidence Based Protocols for implementing clinical guidelines
Future Research
Limitations
Acknowledgements
Special thanks to Cassidy Smith from the Colorado Clinical Guidelines Collaborative
Jennie Popay and the teams for the providing the methods group Guidance on the conduct of Narrative Synthesis
My friends family and colleagues for their patients and support in helping me make this happen

THE END