EFFECT -...
14
THE EFFECT OF THYROID DISEASE ON CALCIUM METABOLISM IN MAN1 By STEPHEN M. KRANE, GORDON L BROWNELL, JOHN B. STANBURY, AND HELEN CORRIGAN (From the Medical Services of the Massachusetts General Hospital and the Department of Medicine of the Harvard Medical School, Boston, Mass.) (Submitted for publication October 31, 1955; accepted April 24, 1956) Abnormal thyroid function profoundly alters calcium metabolism. In 1929, Aub, Bauer, Heath, and Ropes (1) demonstrated in patients on con- stant low calcium diets that urinary and fecal ex- cretion of calcium and phosphorus is frequently increased in hyperthyroidism and lower than nor- mal in myxedema. These changes could not be ascribed to elevation of metabolism per se (1) acidosis (2) or vitarmin D deficiency (3); they were observed even in the absence of the para- thyroid glands (4, 5). In addition, roentgeno- graphic evidence of skeletal demineralization has been described in patients with thyrotoxicosis (6). The conventional balance techniques which have been used in the study of calcium metabolism in thyroid disease measure only net effects: they do not measure the processes of deposition and re- sorption of calcium. An indication of the skeletal turnover of calcium, however, can be obtained from serial observations of the specific activity of radioactive calcium (Ca45) in blood and urine after intravenous injection (7, 8). The present study was designed to define the alterations in calcium metabolism in thyroid dis- ease in man by using Ca45 and the technique of isotope dilution. Observations have been made in euthyroid, hyperthyroid, and myxedematous sub- jects, and, for purposes of comparison, in addi- tional euthyroid patients with Paget's disease and with hypoparathyroidism. MATERIALS AND METHODS All patients (Table I) were on the metabolic ward and were ambulatory throughout the study. Diets, which were constant and of neutral ash, contained from 0.08 to 0.23 grams of calcium per day (Table II). In order to avoid tetany, the two hypoparathyroid subjects were given 0.31 and 0.57 grams, respecfively, of calcium 1 Aided by grants AT (30-1) 667 and AT (30-1) 1755 from the Atomic Energy Commission and A(446) C from the United States Public Health Service. in their diets per day. Fluid intake was maintained at 2,000 to 2,500 ml. per day. Complete collections of urine and stool were begun after six days on the fixed diet. A three-day control collection of urine and feces was ob- tained prior to the administration of Ca. The stock solution of Ca"Cl, 2 was acidified with con- centrated HCI, added to 0.9 per cent NaCI solution to give a final concentration of approximately 0.5 j&c per ml. saline at a pH of 6, and autoclaved. Five to seven mi- crocuries were injected from a calibrated syringe into an antecubital vein one hour before breakfast. Blood samples were obtained by venipuncture from the op- posite arm at frequent intervals. Fractional urine col- lections were made for the first three days following in- jection, and daily thereafter. Stool collections were made TABLE I Clinical data Name R. P. Wa. ; F. W. L.S. C. L. J. B. W.W B. M A. W O. H. E. N. Age Sex Diagnosis 50 M Coronary heart disease; hyperurice- mia (A.S.H.D.)* V. 26 M Friedreich's ataxia (Fr.A.) (1) 18 M Hyperthyroid (diffuse goiter) (Thyr- tox.) (2) 19 Euthyroid, hypoparathyroid, 1 yr. following thyroidectomy (Hypo- parathyr. after Rx.) (1) 31 F Hyperthyroid (diffuse goiter) (Thyr- tox.) (2) 31 Early myxedema (4 months follow- ing thyroidectomy) (Myx. after Rx.) 38 F Hyperthyroid (diffuse goiter) (Thyr- tox.) 26 M Hyperthyroid (diffuse goiter) (Thyr- tox.) T. (1) 42 F Myxedema (Myx.) (2) 42 Euthyroid (4 months on treatment) (Normal after Rx.) (1) 39 F Myxedema (Myx.) (2) 39 Euthyroid (5 months on treatment) (Normal after Rx.) 67 F Paget's disease of bone (Osteitis De- formans) (Paget's dis. 59 F Paget's disease of bone (Osteitis De- formans) (Paget's dis.) 41 F Hypoparathyroid, 4 years following thyroidectomy (Hypoparathyr.) * Abbreviations to be used in all tables. 2 Obtained from Oak Ridge. Ca" has only a beta ray (M.E.V. = 0.26) and a half-life of 152 days. 874
-
Upload
trinhthien -
Category
Documents
-
view
216 -
download
0
Transcript of EFFECT -...

THE EFFECT OF THYROID DISEASE ON CALCIUM METABOLISMIN MAN1
By STEPHENM. KRANE, GORDONL BROWNELL,JOHN B. STANBURY, ANDHELENCORRIGAN
(From the Medical Services of the Massachusetts General Hospital and the Department ofMedicine of the Harvard Medical School, Boston, Mass.)
(Submitted for publication October 31, 1955; accepted April 24, 1956)
Abnormal thyroid function profoundly alterscalcium metabolism. In 1929, Aub, Bauer, Heath,and Ropes (1) demonstrated in patients on con-stant low calcium diets that urinary and fecal ex-cretion of calcium and phosphorus is frequentlyincreased in hyperthyroidism and lower than nor-mal in myxedema. These changes could not beascribed to elevation of metabolism per se (1)acidosis (2) or vitarmin D deficiency (3); theywere observed even in the absence of the para-thyroid glands (4, 5). In addition, roentgeno-graphic evidence of skeletal demineralization hasbeen described in patients with thyrotoxicosis (6).
The conventional balance techniques which havebeen used in the study of calcium metabolism inthyroid disease measure only net effects: they donot measure the processes of deposition and re-sorption of calcium. An indication of the skeletalturnover of calcium, however, can be obtainedfrom serial observations of the specific activity ofradioactive calcium (Ca45) in blood and urineafter intravenous injection (7, 8).
The present study was designed to define thealterations in calcium metabolism in thyroid dis-ease in man by using Ca45 and the technique ofisotope dilution. Observations have been made ineuthyroid, hyperthyroid, and myxedematous sub-jects, and, for purposes of comparison, in addi-tional euthyroid patients with Paget's disease andwith hypoparathyroidism.
MATERIALSANDMETHODS
All patients (Table I) were on the metabolic wardand were ambulatory throughout the study. Diets,which were constant and of neutral ash, contained from0.08 to 0.23 grams of calcium per day (Table II). Inorder to avoid tetany, the two hypoparathyroid subjectswere given 0.31 and 0.57 grams, respecfively, of calcium
1 Aided by grants AT (30-1) 667 and AT (30-1) 1755from the Atomic Energy Commission and A(446) C fromthe United States Public Health Service.
in their diets per day. Fluid intake was maintained at2,000 to 2,500 ml. per day. Complete collections of urineand stool were begun after six days on the fixed diet. Athree-day control collection of urine and feces was ob-tained prior to the administration of Ca.
The stock solution of Ca"Cl, 2 was acidified with con-centrated HCI, added to 0.9 per cent NaCI solution togive a final concentration of approximately 0.5 j&c per ml.saline at a pH of 6, and autoclaved. Five to seven mi-crocuries were injected from a calibrated syringe intoan antecubital vein one hour before breakfast. Bloodsamples were obtained by venipuncture from the op-posite arm at frequent intervals. Fractional urine col-lections were made for the first three days following in-jection, and daily thereafter. Stool collections were made
TABLE I
Clinical data
Name
R. P.
Wa. ;F. W.
L.S.
C. L.
J. B.
W.W
B. M
A. W
O. H.
E. N.
Age Sex Diagnosis
50 M Coronary heart disease; hyperurice-mia (A.S.H.D.)*
V. 26 M Friedreich's ataxia (Fr.A.)(1) 18 M Hyperthyroid (diffuse goiter) (Thyr-
tox.)(2) 19 Euthyroid, hypoparathyroid, 1 yr.
following thyroidectomy (Hypo-parathyr. after Rx.)
(1) 31 F Hyperthyroid (diffuse goiter) (Thyr-tox.)
(2) 31 Early myxedema (4 months follow-ing thyroidectomy) (Myx. afterRx.)
38 F Hyperthyroid (diffuse goiter) (Thyr-tox.)
26 M Hyperthyroid (diffuse goiter) (Thyr-tox.)
T. (1) 42 F Myxedema (Myx.)(2) 42 Euthyroid (4 months on treatment)
(Normal after Rx.)(1) 39 F Myxedema (Myx.)(2) 39 Euthyroid (5 months on treatment)
(Normal after Rx.)67 F Paget's disease of bone (Osteitis De-
formans) (Paget's dis.59 F Paget's disease of bone (Osteitis De-
formans) (Paget's dis.)41 F Hypoparathyroid, 4 years following
thyroidectomy (Hypoparathyr.)
* Abbreviations to be used in all tables.2 Obtained from Oak Ridge. Ca" has only a beta ray
(M.E.V. = 0.26) and a half-life of 152 days.
874

CALCIUM METABOLISM IN THYROID DISEASE 875
|v]i#)t|q|fC°1'- > | 1+ |4 -+ + + + I +
- C~~ ~ 4 U) C4 WI) NOI cie'-U)1° 0 10I
0-~~~4tmB C-o b; m 04 GoW X b
co 0 eq - - io s iOO
% '0 @ 0~ t- - m '0 '0% eqN
P.c Noo.z C; ci CZosi Iso.i 4 S
v
o 0 0 o oA o o o O o o O0@o0 U) e#) 0% t 0 e4t 0tN$ '0
tg U) '0 U '0 0Ook- CK to 00 C1@0 ' 0% '0 0o%m %O l- t 0 - tX t- 00 0% . c0
-~~4~4 4.0' '~4 ~ 0e 0% 0 -1I - 1 eq 1- I - 1- 0 - - 1- 1 1-
co: j4 0ce O0 V) c@0 e 0ot- m %O 0 %C t- oo 0% co co ooeq Uoeq @0ooo co eq e 0 co t- 0% eq @0 0
o C; c C; C;O oo:tO O t. o O 06 00
*X td @0 eq 0 co co 0 eq 0 @oc)tW OO 0 _ O'0 eq t- O Ot. oo t4 0 0 eq t- '0 U U ) ) '
S 0N - - Nvo 0 0'. 0 40 0 0 0=, m WI %O "-I I
) n c NO _- t-_ _U%I) '0 1-4inU)1 14 0 0 m 0o0' - t'0o 0% @0 0 o eo o o - -
qt to in 0 11-1 ' t e t 'oo ft-I I$Id o 1Cs 14 1° C; lo lo C;lo C;lo g lo'0oo U) eq eqS eqo eqo 8 eq
co m eg (4 oo o s o o NO
I inlo 1' %o co °4 Neo q '°0s U)o 0 @0 e
N'to . eq '0M4o
~~~~~~~~W C4 s V- V- o 4N
I~~~~~~~~~C C;Cs1I';C; C; C; C;C;I1°1°° I 1
i4 cO0 0 O00 0 00 O 00O O0 O OCe i toC)+4 0
~0 - - 0D V- 0-4 0 -" - qC; a C; C;B i C;c; 5 C
'1 U4 C44' @0 ' 0 @0 t 4~
4 4)Co Z154%~ ~ ~ ~ ~ ~ w-OL
c
%_0.= Z CL, .. 0~~~~~~~~~~~~~
44T4H,; c co

S. M. KRANE, G. L. BROWNELL, J. B. STANBURY, AND H. CORRIGAN
in three-day periods. An aliquot of the solution usedfor injection was taken for the standard. The amountof stable calcium (Ca'5) included in each injection rangedfrom 1 to 6 mgm. After giving the Ca", collections weremade for times ranging from 9 to 22 days for the variouspatients. If a previous study had been done, control col-lections were assayed for radioactivity prior to the ad-ministration of the second tracer of Cae.
Stable calcium (Ca") was determined by the method ofFiske and Logan (9). The results of analysis of dupli-cate samples agreed within ±3 per cent of the mean.Phosphorus B was determined by the method of Fiske andSubbarrow (10) and nitrogen according to the macro-method of Kjeldahl. Aliquots of urine (200 ml.) wereacidified with 4 ml. of concentrated HC1. The 3-daystool collections (obtained without a marker) were mixedin a Waring Blendor, and made up to volume with dis-tilled water. For calcium and phosphorus analyses, du-plicate 200-ml. aliquots of the blended and diluted fecalsamples were dried for 2 to 3 days in a steam oven andthen ashed in an electric muffle furnace at 5500 C. over-night. The ash was dissolved in concentrated HCI anddistilled water. Nitrogen analyses of the feces were per-formed directly on unashed aliquots of the blended anddiluted fecal samples.
Ca' was determined as follows: 4 44ml. of trichloraceticacid (20 per cent) and 8 ml. of distilled water wereadded to 2.4 ml. of serum, the sample centrifuged, andthe Ca' determination performed on the supernatant.Complete recovery of Cae added to human serum in vitrowas achieved. Analyses of Cae in urine and feces weremade on acidified specimens which had been dried andashed, and the ash dissolved in HCI and distilled water.After analysis for the stable calcium of the sample, stablecalcium was added as CaCl2 to give a final concentrationof 6.0 mgm. per sample in all specimens. From a self-ab-sorption curve this concentration was found to be optimalfor sensitivity and reproducibility of sample measure-ments. Calcium was then precipitated as calcium oxa-late by the addition of saturated ammonium oxalate solu-tion. The solution was made alkaline by the addition ofdilute ammonium hydroxide and then adjusted to a pHof 5.4 with 2.5 per cent oxalic acid, using an alcoholicsolution of methyl red as indicator. After adding TritonX-1005 (0.1 per cent) as a detergent, the samples werefiltered over sintered glass on filter paper discs, 24 mm.diameter (Schleicher and Schuell No. 576), which werecemented to copper discs with polystyrene coil dope.
The discs from initial studies were assayed for Ca4 u-der a thin (< 1.9 mgm. per cm.') mica end-window G.M.tube connected to an automatic sample changer (Tracer-lab). In later studies, a gas-flow counter was used which
S The authors are indebted to the hospital chemistrylaboratory under Dr. Charles Dutoit and Miss G. Mar-garet Rourke for the phosphorus and nitrogen analyses.
4 This method was developed by Dr. C. J. Maletskos ofthe Massachusetts Institute of Technology.
5 Obtained from Rohm and Haas Co., Philadelphia 5,Pennsylvania.
increased sensitivity from 250,000 to 500,000 counts perminute per microcurie. Each of the duplicate sampleswas measured three times to an accumulation of 4,096counts. The standard was assayed with each run. Themaximum variation in accumulated counts of duplicatesamples was ± 6 per cent of the mean. The usual varia-tion was ± 3 per cent. Recorded radioactivity of thesamples was at least twice background.
The data for Ca'5 are expressed as per cent adminis-tered dose. Specific activity, as per cent of administereddose of labeled calcium per gram of calcium, was calcu-lated for each sample.6
METHODSOF ANALYSIS
Inspection of the semi-logarithmic plot of specific ac-tivities in urine and serum against time suggested thatthe curves could be resolved into a series of three orpossibly more decreasing exponential functions. Thiswas of interest because of the possibility that each func-tion represented a discrete calcium compartment withinthe body. The data were treated with this assumptionin view.
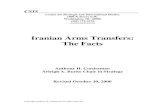
Analysis of exponents: The method of curve analysisis illustrated in Figure 1 where serum and urine specificactivities of an hyperthyroid subject are plotted againsttime in days. Serum specific activities are plotted forthe first day. Since the radioactivity of many serumsamples was low by 24 hours following the administra-tion of Ca, urine specific activities are plotted from thesecond day onward. The data of all subjects have beentreated in an identical manner. In Figure 1 (A) areplotted the observed specific activities from 0 to 9 days.The data from 1.25 to 8.5 days appeared to follow asingle exponential function. By the method of leastsquares a fit of this range of the data to the functionA,e-st yielded the solid line of Figure 1 (A) (A, isspecific activity extrapolated to zero time, k. is the rateconstant in fraction per day, and t is time in days).When this function was subtracted from the observeddata, the values in Figure 1 (B) were derived. Ananalysis by least squares of the data between 0.13and 0.67 days yielded the solid line in Figure 1 (B).When this line of slope k2 was extrapolated to zero time,the specific activity value of A2 was obtained. This linesubtracted from the remaining data of Figure 1 (B)yielded the points in Figure 1 (C). The solid line inFigure 1 (C) is the least squares fit of those data withslope k,, and when extrapolated to zero time gives A,.Thus, the data are analyzed in the form:
Specific activity = Ale-,it + A2e-k2t + Aae-k3t.Compartments: The size of each "compartment" (Q)
was obtained by dividing 100 per cent (the quantity oflabeled calcium at zero time) by the extrapolated specific
s The term "labeled calcium" refers to that quantityof calcium which was initially given to the patient as atracer dose marked with radioactive calcium. Thisquantity is independent of radioactive decay.
876

CALCIUM METABOLISM IN THYROID DISEASE
HYPERTHYROID pt. L.S.
(A)
o SFRUAI0 URINE
I' 0 K-0.279+ a
I I . I2 4 46
Tl ME(DAYSJ5-L
D.-I5
0.1 0.2 0.3 0.4 0.5rIME tDA YS,
100soso
tt 40
2
4.
'I)'
t*
2I
II0 0.01 0.02 0.03 0.04 0.05 0.06 0.07
TIME(DATS)
FIG. 1. ILLUSTRATION OF THE METHODOF ANALYSIS OF EXPONENTIAL FUNCTIONS OF
SPECIFIC ACTIVITY CURVEPLOTTED SEMI-LOGARITHMICALLY VmEsus TIMEThe data obtained from subject L. S. (i (hyperthyroid) are used as examples.
Note the different time scale for (A), (B) and (C). The specific activity values on
the ordinate are the same for (A), (B) and (C). The solid line in (A) has theslope k, which extrapolated to zero time yields A,; the solid line in (B) has the slopekI2 and intercept A2; the solid line in (C) has the slope k, and intercept A1. For fur-ther explanation, see the text.
activity value (A) for each function. For the third com-
partment (Q,) this equals A°; for the second (Q),As
100%A ; for the first (Qj, 100% This analy-As + A2 fArthefirst,sis is rigorously correct only when the size of the com-
partments (Q) increases and the flow (kQ) decreasesfrom one to the next compartment.
Calcium "pool': If specific activity
%administered dose Ca"6\gram Ca0
is known at time t, and the quantity retained in the body(100 per cent of administered Ca4 minus per cent ex-
creted) is known, the per cent retained at time t dividedby the specific activity at time t is the calcium "pool" attime t. The concept of a calcium "pool" makes no as-
sumption based on the shape of the curves, but reflects thefact that a lower specific activity at any time means a
larger mass of dilution. Calcium "pool" curves were de-rived from the ratio between the curve of labeled calciumretention and the specific activity curve for the variouspatients.
The analysis of calcium metabolism presented hereassumes that the calcium is first present in a small com-
partment with a rapid flow to and from a larger secondcompartment. This flow accounts for the initial rapid
877
10060
a 60
3. 40
~," 20
tO3 :i
6
2
(B)
0
a. 3.196 ±0.049
I I I I I I I0.6 0.7
(C)o
K* 36.60± 9.31
. . a a a a.
E
r-I I L
10 0

S. M. KRANE, G. L. BROWNELL, J. B. STANBURY, AND H. CORRIGAN
ME) -V ' 0o U) 00 k- 0 t- o4 t- 0 M o 4 U)'.4 mE Ce4 - 04 en co C4 0 Co 0 M E '. 0O 6 o V + 6 o o o o 6 6 o % 6
%O 0 E
o6
* *
00 t
ui el;o
*
co r-U) E)
V-
- b
)
*l *.
VO 0% q0 %*O *4 .*
U) 0 00 E -40 ei 4-
00 O n 4 c0
C4i V- NW 04 -. 04 4 4 t-. C4 -..
V- V- 0 CE9- CE
0* 0 W- C04 V- 0%1U) CE) U) o6 CE6 C-4
-4 0 CEV- CE
U)CEi
CIA C% 0
(DI Cl4 Cl
6i N6.~~~~V-
Vo VO t- -4 U) - 00o O 0 EVO U)i E) C ON U) It
%6 (9i el; V6 el; 00 V6000* 00 00 -. -. 00 t-. 0* 0. t
mE o tU 0 LO '4 0o It t-o Vo )
0 t- l4 Cl4 00 "I0 in _
eC C E)" V6 C4 V- (i Ce)
<6 CE) CEi %6 '-4e-~~~~~~~~~~~~1 elq V- Cl
t4 U)d4 U)
CE 0vC6 C9
00 eC U) 02%E U) WIE 0 U) 1 00 0
00*- .
el* ;*;*4*4* * .
V- co 0 9- t44..t- E '-a 00 - Cl 0 0% 0
- 0000 t-: _ 5_" _I_ *l .4
C14 ~ ~ ~ ~ -..~ S.@5s" 0 0.co
~ ~ ~*4h ~w
'U0o6
Y
. .c R4
o6
44
Ul U
=-CIO
W u
MD
cd -c,
Cd C
*
u
878
0% S4c4I
U) 00oo tr.
- 4
o U) 00 0 U) 0
q; 46 1; 6
"-
m b
*!
800
00
00
In0%
0%
NO
;Z4)
a,
U.
0
_44-

CALCIUM METABOLISM IN THYROID DISEASE
R.P d AGE50 CORONARYMGHa 819278 HEART
DISEASEII"Iv
- 0_ * v v_ ~ ~~~*
A__ o
_
0 * T v v
SERUM
* FECESURINE
I I I I I I I I I. I
0 2 4 6 8 10 12
TIME (DAYS)FIG. 2. SEMI-LOGARITHMIC PLoT OF SPECIFIC ACTIVITY VERSUSTIME FOR THE DATA
FROMCONTROLSUBJECT R. P. WITH CORONARYHEARTDISEASEIn this figure and Figures 3 to 5 the serum specific activity values for the first 30
minutes are not plotted.
decline in the specific activity curve. The analysis con-
tinues in the same manner into a third and, in some cases,a fourth compartment. The basic assumption of equalspecific activities after equilibrium can be made in an
open system (i.e., a system involving excretion of thesubstance) only when the amount being excreted is smallcompared to the other routes of flow to and from thecompartments being studied. The data appear to vali-date these assumptions over the time interval studied.However, at longer times, the specific activity of theurine and blood may diverge markedly from that of thebone compartments because the flow from the large bonecompartments may be small compared to the ingestionand excretion of unlabeled calcium.
RESULTS
Ca45 data
The concentration of labeled calcium in the se-rum declined rapidly following injection and couldnot be measured in most patients in the sampletaken seven days after administration of the radio-active calcium. Within the first hour after injec-tion, Ca45 appeared in the urine. Urine radio-
activity was readily measurable throughout theperiod of study (9 to 21 days). There was no cor-relation between the total labeled calcium and thetotal stable calcium excreted over a 9-day periodof observation (Table III).
Urine and serum specific activities yieldedcurves of characteristic form when plotted againsttime on semi-logarithmic paper (Figures 2-5).The specific activity of calcium in the serum was inall cases the same as that of the urine collectioncorresponding to the serum sample. Fecal specificactivity was almost always less than that of theurine or serum sample in the midpoint of the col-lection period and fell off at a rate similar to thatof urine.
In Figure 2 are plotted the data of a control sub-ject (R. P.). An initial rapid fall in specific ac-tivity of blood and urine was followed by a slower,linear decline from the second to the eighteenthday after administration of Ca 5. In contrast, thecurve of specific activity of the hyperthyroid sub-
o00.80.60.
40.
20.
N % 10.Q48
% 6.
<3 ft 4.
14t 2.
C 1.0.8.6
.4
.2
14 16 1 8 20 22
879

S. M. KRANE, G. L. BROWNELL, J. B. STANBURY, AND H. CORRIGAN
ject (F. W., Figure 3) showed a more rapid fallto lower levels. In the subject with myxedema(W. W., Figure 4) there was a very slow fall inspecific activity following the rapid initial decline.In subject A. W. (Figure 5) with Paget's disease,the drop in specific activity was very fast for thefirst eight days. The curve declined more slowlyduring the remaining 14-day period of observation.
Values for coefficients, rate constants and theirstandard deviations appear in Table IV. Differ-ences among patients were most marked in thethird slope which appeared by the second day.The small standard deviation of the slope and in-tercept of this function derived by least squaressupports the supposition that the data are expo-nential in nature. In the two control patients(R. P. and Wa. W.) this slope was 0.081 per day,and 0.164 per day, respectively. Blau, Spencer,Swernov, and Laszlo (11) studied two patientswithout bone disease with radiocalcium in whomthe slope of the function corresponding to k5 wascalculated to be 0.092 per day. In the hyperthy-
100.80.60.
40.
20.
I4*
I 4J
I.(
10.8.6.
4.
2.
I.C
.1
0 2 4 6 8 10 12
TrAmE(DArS)
roid subjects, k3 ranged from 0.215 to 0.288 perday. Whenone of the thyrotoxic subjects was re-studied four months after thyroidectomy, this thirdslope had decreased to 0.150 per day. In two fe-male patients with myxedema of several years'duration, these values were 0.063 and 0.072 perday. Then metabolic rates were returned to nor-mal with desiccated thyroid. Five months later,the values for k3 were found to have risen to 0.150and 0.174, respectively.
Dimensions of the various compartments alsoappear in Table IV. The size of all compartments,especially the third, was greatest in the hyperthy-roid subjects and those with Paget's disease. Com-parttments were smallest in the subjects with un-treated myxedema and in subject E. N. with hypo-parathyroidism.
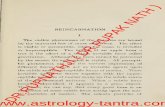
The values for the calcium "pool" at nine daysafter administration of Ca45 are in Table III. Hy-perthyroid subjects and those with Paget's diseasehad the largest "pools". These ranged from 47 to333 grams. The myxedematous subjects and the
14 16 Is 20 22
FIG. 3. SEMI-LoGARITHMIC PLOT OF SPECIFIC ACTIVITY VERSUS TIME FOR
SUBJECT F. W.(1) WITH HYPERTHYROIDISMObservations were made for nine days following the administration of Ca'5.
F.W. g AGE 19MGH* 519840
o SERUM.* FECESY URINE
_0
- 0 0
Y
V
* vV0
VV
8 -
5 -
4
2 -
IL
880
HYPERTHYROID
.2

CALCIUM METABOLISM IN THYROID DISEASE
0 2 4 6 a 10 12
TImE (DAYS)14 16 18 20
FIG. 4. SEMI-LOGARITHMIC PLOT OF SPECIFIC ACTIVITY VERSUSTIME FOR THE DATAFROMSUBJECT W. W.(i) WITH MYXEDEMABEFORETREATMENT
patient with long-standing hypoparathyroidismhad the smallest, 5.1, 5.0, and 4.4 grams, respec-tively. After treatment of the myxedema, thecalcium "pool" rose to 13 and 18 grams. Therapidity and extent to which labeled calcium en-ters body calcium spaces in hyperthyroid, euthy-roid, and myxedematous subjects is illustrated inthe calcium "pool" curves of Figure 6.
Balance data
Metabolic balance data for calcium, phosphorus,and nitrogen are given in Table II. Two of thefour hyperthyroid patients (F. W. and J. B.) werein a distinctly more negative calcium and phos-phorus balance than is normal for a low calciumintake. Both had high levels of calcium in thefeces as well as in the urine. Both had elevatedurinary excretion of nitrogen, but their intakeswere high in nitrogen and calories. They re-mained almost in nitrogen equilibrium and main-tained their body weight. The other two hyper-thyroid subjects, both female, had normal urinarycalcium values and were in only slightly negative
calcium balance.7 Alkaline phosphatase values inthe serum were significantly elevated in patientF. W.(1), but there was no clinical evidence of liverdisease, and there was no retention of bromsulpha-lein in the serum.
Urinary calcium excretion was low in bothwomenwith myxedema of long standing (B. M.(1,)and W. W.(1)). The amount of calcium in thefeces was normal. These subjects were in slightlynegative calcium balance. Both were restudiedfive months after treatment with desiccated thy-roid. Urinary calcium excretion had increasedalmost threefold, and total calcium excretion ap-proximately doubled. The concentration of cal-cium and phosphorus in the serum was normal be-fore and after treatnent.
Subject L. S. went from negative calcium bal-ance when she was hyperthyroid to positive bal-ance five months after thyroidectomy, when signsof early myxedema were present. Urinary cal-cium, which had been 0.13 gm. per day when she
7 Normal subjects are in slightly negative calcium bal-ance on a low calcium intake (12).
100.80.60.
40.
20.
10.8.6.
4.
2.
eiA.11k :k
;Z,ta 4.IRt3 "uniz izi.C:4
C4qq6e
W.W. AGE42 MYXEDEMAMGH* 819735 (BEFORE PX)
y00
v~~~~~~~~~0
Y0
o SERUM
0 FECES
v URINE8B
lB
I .4
.4
22
881
*

S. M. KRANE, G. L. BROWNELL, J. B. STANBURY, AND H. CORRIGAN
was hyperthyroid, averaged 0.02 gm. per day inthe myxedematous state.
Patient E. N, with untreated surgical hypopara-thyroidism of four years' duration had low urinarycalcium levels. Fecal calcium values were high,presumably because during the period of study shecontinued to take eight enteric coated aspirin tab-lets per day. These were found subsequently tocontain a total of 0.254 gm. calcium. It is possiblethat this calcium was not available for absorption.Patient F. W., the hyperthyroid subject who dem-onstrated the most marked calcium losses, be-came parathyroid following thyroid surgery. Al-though euthyroid when studied one year later,he still had evidence of parathyroid underactivity.He was in positive calcium balance of considerabledegree at this time.
DISCUSSION
The nature of the processes governing uptakeby the skeleton of labeled calcium and phosphorushas been studied by microradioautography andcomparative x-ray photography. Engfeldt, Eng-
str6m, and Zetterstrom (13) have shown that P'2is deposited in cortical bone in discrete locationscorresponding to individual Haversian systems.Radioactivity was most intense in those osteons ofleast density by x-ray and therefore of most re-cent origin. In similar studies employing Ca ,Lacroix (14) also demonstrated that radioactivityis detected in compact bone only where osteogene-sis is taking place, i.e., in the absorption cavitieswhich are being filled by concentric lamellae ofnew bone. Lacroix (14) also demonstrated thatin this regard cancellous bone behaves like com-pact bone. In addition, there is evidence that invitro ion exchange and recrystallization processesoccur to a greater extent in bone crystals fromareas of recent origin than in older establishedbone (15).
The present study provides further informationon the mobility and deposition of the calcium storesof the body as disclosed by observations on theprogressive dilution of administered labeled cal-cium into the calcium compartments. Mixing inthe first compartment (Ql) of dilution accounts
A.W. g AGE67MGH* 649107
OSTEITISDEFORMANS
o SERUM* FECESv URINE
-v- v
- V
- V
V Vyv v
0 2 4 6 8 10 12
TIME (DAYS)
V Vv v * Y
14 16 18 20 22
FIG. 5. SEMI-LOGARITHMIC PLOT OF SPECnac Acmvy VERsus TIME FOR THE DATAFROMSUBJECTA. W. WITH EXTENSMPAGET'S DISESE OF BONE
100.80.60.
40.
20.
ftC-3
k zt11;z v
.a V3IR .a
t.) tuiz U;)--,. Q%ak-4
I
% w
10.8.6.
4.
2.
1.0.8.6
.4
.V y0 vIVVY
.2
882
0

CALCIUM METABOLISM IN THYROID DISEASE
mm mcqc"FoO
-H -H Ui -H
coo o- cc-t-o v-00 -0eq140e40
-H 4H 41-H1
'00 oq 0%'O
t- cctif; c o614cooo 0 C)O -o
eqOd4 '1)0 ON#
-H i -H
C1)o% C%,- 0 0 Mt Ot- ) m 0%'o I ) NOw - t- -- eqCso'-
-Hl -H 41-H-4H 4 -H
0%ot0oo co in et-- _)- .4 eqeO 0C4eO o0
464141
0v08
U)0'0 0)
-H -H
cot- r 0 'O -0_ oo ) t-- %011)p10% co0o 011) C4' -o " -d4_| -H _
-H " 4i 41"'4 `- q
Nior41
b0 seq004in00
-H N-H
1"0 %4o
41 -H
cO- eqoWI)0 ) 11
Tl -H
0a )
oo~9-0 0-04- 0-
''l-H -H00 00D -
-)- H4O1O 0-en m oO
*4 1. .l 114_ M_
OeC11)In0 144 - t- M In t- cc -,. V-t - In ON k- - eqOCw- Wcoo eq Cq C0- co, W-eq Odo -c c0tr-i6 ooo -CC oC -fo o_-6 W6 e'itoo r-o
+ + + ++-H -H41 1 1 - 41 -HC0-O) e0C4 D0NO - - 0t- Oe 0 0-tNOt 0C-O
cqo 0%'- u1) 'N -4 00o t-e _- , en in em q"-_t-0o _o -6 - e-iC W 56c_io W_o o6_o e 6
-H + 41 4141+ -H -H -H
t-%0I o cm 0I
-HNO0N
0
* cc
eq t~-0% oo6 6
oo - m - 04 0%0
-H -H H4-H
o66 oo oe
eqH "-H-,CDq c-to to-' ci oo_- r4_+ _+-4- 'Il
No1-) qc- oo t-- 'O _ n0 d40o %oo 0 NO0 vL t- 0%r coo '0 1 u)
* . *.: .6 *
el *r *;*:c .
Il`4- ffi c_ -H eq -H_-H oH c4 -H
o- 0 0 to) t-r t-- 0o '0
o
eq
oo C% oo 0 0% t- (I cc 'O cc 'OC;66 6-06C;C566666C
eq cc66Ns-H
d4 I t- 114 t-eq k-'0t-cc t- (D,c eqt - eq -4m- d'- t-- cc- t o 00 0e 'tN) c-oW-
-6C664C;C;C 666 6 -46 66C;C .4 66641 41 - H-H -H -H
NO Nco 1' 0' 0%1*00_ 00
soCD N
m-H -H Hm
t-C1)qdJ4 0- %
e0 t--ui ec-i `-Hc-H
1.1-:1 -%.= 0--.,q .i ,.:, ;::. M 04
0 %-., m1:4 z -
< , ,W-I - P4g. U5 co &; .: ;-, .: &.
.4 w..- E5%.-- .4 &. .4 >l- Cd
z
_- -- '0eq '0% ') 0 -cc V-- '_ It in) in e')'0 ~lC1) f
-0 ~4 Il t-0% 4C ciu0c1)t) 1t '0 -i 06 '0eqr11H11) _o oH 000-H eqH cH1)cc cc-H_o
'
o0 O oo t-- c oo U '6c6to-oo' m
r
'0 e c 0 e t-looo '0-C;o oo e e6 uoOeq t 11 "t .11 r- c- %OCS k- 'tt 11 00 c- %N- % 0-
4i -11 11 -H -H -H -H
-
4; X
. -, . J
.- . 4-
ll'.%k
104C4 1'.,.-.o 4),
9.0.4
.i co
.j e0z
1-7
.-% -%l%-. -
*g w, *
*4 C4* E
0m
z
14-)
ui-m:I, 0 I...
-< & O & r &1-
883
4I.. E
aU
., 80
cU,s
U
.%a
r,
1.b..
ac-4z
"Or'.0
-:ir.s4nr.
1~0
II-ocU (z'+cduU6
Ua4 -
4)
Cd

S. M. KRANE, G. L. BROWNELL, J. B. STANBURY, AND H. CORRIGAN
1000.800.600.
400.
200.
100.80.60.0 / ,' C.L. C. L. THYROT40. /~~
t / ,.- L. S. (2). R THYR420. _ / S/ - Wa.W. FRIEDR
.4 / / - B.M.(2) EUTHYF/i/~~~~~~~~'-~~~~W. W. (2) EUTHYF
80. // / R.P. EUTHYF
I6 B.M. (1) MYXEDE~~6.g/~~~~~~~~~/-~~~W.W.(I) MYXEDE
4.~ ~ -E. N. HYPOPA
2. /
1.00.80.6
0.4
0.2
0.1lll3 6 9TIME (DA YS)
1%0 REMAINING IN BODYAT TIMEtFIG. 6. CALCIUM "POOL" IN GRAMS REMAININ iVITY AT TIME t/SPECIFIC ACTIVITY AT TIME tLOGARITHMICALLY VERSUSTIME
It is apparent that Ca' in the hyperthyroid subjects exchanges with acalcium and more rapidly than normal.
for the initial rapid fall in serum specific activityof labeled calcium after intravenous administration.In view of the small size of this compartment andits high rate constant it probably represents extra-cellular fluid. In support of this assumption is theclose agreement of the calculated values of calciumcontent of the extracellular fluid and those obtainedfrom analysis of the curve of isotope dilution(Table IV). An insufficient number of bloodsamples were drawn in the first 30 minutes afterinjection of labeled calcium to distinguish be-tween serum and interstitial fluid distribution.
The second and third compartments reflect re-versible processes. Flow rates from the first to thesecond (k1Q,) and from the second to the third(k2 [Q1 + Q2]) are of too great a magnitude tobe explained by an irreversible skeletal depositionof calcium salts, but are in keeping with ion ex-
IS PLOTTED SEMI-
larger quantity of
change at the surface of bone crystals and equili-bration of surface ions with those in the crystalinterior, i.e., recrystallization (15). Formationof new bone crystals incorporating the labeled cal-cium is consistent with flow (k8 [Q1 + Q2 + Q8])from the third compartment. Whatever their ex-act significance, the compartments and flow ratesobserved were sensitive to varying levels of thy-roid gland function.
In all patients studied the exchange betweenthe calcium in the extracellular fluid and that inbone was very rapid. Nevertheless, the concen-tration of stable calcium in the blood (and extra-cellular fluid) remained quite constant. The quan-tity of calcium exchanged was far greater than thenet quantity of calcium transferred from the boneto the extracellular fluid. In those subjects innegative balance, the net calcium lost (excreted)
884

CALCIUM METABOLISM IN THYROID DISEASE
from the extracellular fluid was then rapidly re-
placed from the larger bone pools. This suggestspart of the mechanism whereby serum levels can
be maintained and controlled.In all four hyperthyroid subjects the size of the
calcium compartments and the rates of flow fromthese compartments were distinctly greater thanin the euthyroid controls. This indicates increasedosteogenesis. Calculation of the rate of calcium"accretion" from the data obtained in the presentstudy by the method of Bauer, Carlsson, andLindquist (16) supports this concept. Since thesepatients were in negative calcium balance on a
low calcium intake, bone destruction as well as
bone formation was proceeding at an increasedrate. In myxedema, there was a slower rate ofthese processes. When myxedema was treated,the rate of fall of specific activity and the size ofthe compartments increased.
In hyperthyroidism, excessive destruction ofbone may be the primary event. In addition, un-
der the conditions of the present study, there may
have been increased bone resorption in response
to the low dietary intake of calcium. However,the weakened bones were able to respond with an
increase in osteoblastic activity followed by depo-sition of mineral. This is what is pictured to oc-
cur in "osteitis fibrosa." Askanazy and Rutis-hauser (17) and, later, Follis (18) reported mi-croscopic evidence of bone destruction in patientsdying with hyperthyroidism. In Follis' series of20 patients, osteitis fibrosa was found in the verte-bral bodies of all, whereas osteoporosis was ob-served only in four subjects. These findings are
thus not compatible with the concept that the pri-mary bone disease of thyrotoxicosis is osteoporosis,defined as decreased bone formation from a failureof matrix formation, with bone destruction pro-
ceeding at a normal rate (19). The elevated con-
centration of alkaline phosphatase in the serum ofpatient F. W. when thyrotoxic also supports theconcept of increased bone formation and is con-
sistent with reported observations in other hyper-thyroid patients (20) and the finding of increasedbone phosphatase. in animals given excessive dosesof thyroid (21).
It is possible that nutritional or other factorsmay adversely affect bone formation in other pa-
tients with hyperthyroidism. All in the presentstudy were adults. Those females with abnormal
thyroid function were pre-menopausal. Age mayhave been a factor in that the younger individualsstudied here conceivably had a greater capacity torespond with an increase in osteogenesis. Thetwo hyperthyroid subjects, F. W. and J. B., whowere in the most negative calcium balance, werenearly in nitrogen equilibrium. This fact is con-trary to the view that the hypercalcuria of hyper-thyroidism is directly related to nitrogen losses(22).
The turnover of calcium in the bones may berelated to blood flow. For this reason, two pa-tients with Paget's disease of bone were studied.Often in osteitis deformans there is an increase incardiac output and bone blood flow (23). Theincrease in vascularity could involve a greater ex-posure of bone crystals to Ca" in circulating fluidsand thereby increase the exchangeable surface.Both patients demonstrated an increased skeletalturnover of calcium. Both had extensive diseaseand elevation of the serum concentration of alka-line phosphatase. Increase in the vascularity ofthe skeleton in hyperthyroidism could influenceskeletal uptake in the same direction, whereas de-creased vascularity could have the opposite effectin myxedema. Blood flow in other organs isknown to be decreased in myxedema (24).
Relief of the hypothyroid state was followed bya decreased turnover of skeletal calcium. PatientF. W., who demonstrated marked calcium lossesand rapid turnover of skeletal calcium when hy-perthyroid, still showed a rapid fall in specific ac-tivity one year 'after thyroidectomy, when euthy-roid but hypoparathyroid. At the time of the sec-ond study, the size of the calcium compartmentswas much smaller and the calcium "pool" at ninedays considerably decreased compared to the ini-tial study. Nevertheless, the values were higherthan expected by comparison to other subjectsstudied. It is possible that this patient had notremineralized his bones completely at the time ofthe second study.
Similarly, the hyperthyroid subject, L. S., re-studied when myxedematous four months afterthyroidectomy, showed a decrease by a factor oftwo in rates of flow of calcium in and out of theosseous compartments, but the values were thenabout the same as the euthyroid controls. At thesame time, urinary and fecal calcium excretionwere reduced by a factor of four. This implies
885

S. M. KRANE, G. L. BROWNELL, J. B. STANBURY, AND H. CORRIGAN
that after withdrawal of the thyroid hormone, adecrease in the rate of bone destruction occurssooner than a decrease in osteogenesis.
The effects of thyroid hormone are probablynot mediated by the parathyroids. Aub, Albright,Bauer, and Rossmeisl (4) demonstrated that thy-roid increases the serum and urinary calcium inpatients with idiopathic and surgical hypopara-thyroidism. Cope and Donaldson (5) reported apatient who developed hypocalcemia and tetanyfollowing an inadequate subtotal thyroidectomy forhyperthyroidism. Whenhyperthyroidism recurred,tetany was relieved and the concentration of cal-cium in the serum rose. Hypocalcemia and tetanyagain appeared after treatment with potassiumiodide.
Increased fecal calcium in two patients with hy-perthyroidism and the very low fecal calcium inone of the myxedematous subjects (L. S.(2,)) arein keeping with the earlier reports of Aub, Bauer,Heath, and Ropes (1) and are contrary to theconcept proposed by Robertson (25) that the pri-mary effect of the thyroid hormone on calciummetabolism is on the kidney alone. The findingof hypercalcuria, often extreme in some patientswith hyperthyroidism, in the presence .of normalserum calcium suggests either an increase in fil-tered load or decreased tubular reabsorption.
SUMMARYAND CONCLUSIONS
1. Radioactive calcium (Ca45) was given in-travenously to patients with hyperthyroidism andmyxedema. Euthyroid subjects and patients withPaget's disease of bone, and others with hypo-parathyroidism were similarly studied. Severalpatients were studied before and after appropriatetreatment. Total quantities of the isotope excretedand specific activities of the serum, urine, andfeces were determined frequently for 9 to 22 days.In addition, stable calcium, phosphorus, and ni-trogen balances were performed on each subject.
2. In four subjects with hyperthyroidism, spe-cific activity of serum and urine declined morerapidly and to lower levels than in euthyroid con-trols. In contrast, two myxedematous patientsdemonstrated the least fall in specific activity.After five months of treatment of the myxedemaspecific activity curves were found to decline atthe same rate as in the control patients.
3. Observation of all the specific activity curvessuggests that they can be analyzed into a series ofdecreasing exponential functions. It is proposedthat each function represents a discrete calciumcompartment within the body.
4. Changing thyroid function modifies the sizeof the calcium compartments and the rate of flowto and from these compartrnents. Compartmentsizes and flow rates are greatest in hyperthyroid-ism and Paget's disease of bone and least inmyxedema.
5. Two of four hyperthyroid subjects were innitrogen equilibrium, despite which they showedmarked losses of calcium in the urine and feces.
6. The findings indicate that bone formation aswell as destruction are proceeding at increasedrates in thyrotoxicosis.
REFERENCES
1. Aub, J. C., Bauer, W., Heath, C., and Ropes, M.,Studies of calcium and phosphorus metabolism.III. The effects of the thyroid hormone and thy-roid disease. J. Clin. Invest., 1929, 7, 97.
2. Albright, F., Bauer, W., and Aub, J. C., Studies ofcalcium and phosphorus metabolism. VIII. Theinfluence of the thyroid gland and the parathyroidhormone upon the total acid-base metabolism. 3.Clin. Invest., 1931, 10, 187.
3. Tibbetts, D. M., McLean, R., and Aub, J. C., Studiesof calcium and phosphorus metabolism. XX. Thehigh calcium excretion in exophthalmic goiter isnot due to vitamine D deficiency. J. Clin. Invest.,1932, 11, 1273.
4. Aub, J. C., Albright, F., Bauer, W., and Rossmeisl,E., Studies of calcium and phosphorus metabolism.VI. In hypoparathyroidism and chronic steatorrheawith tetany with special consideration of the thera-peutic effect of thyroid. J. Clin. Invest., 1932, 11,211.
5. Cope, O., and Donaldson, G. A., Relation of thyroidand parathyroid glands to calcium and phosphorusmetabolism. Study of a case with coexistent hy-poparathyroidism and hyperthyroidism. J. Clin.Invest., 1937, 16, 329.
6. Golden, R., and Abbott, H., The relation of the thy-roid, the adrenals and the islands of Langerhansto malacic diseases of bone. Am. J. Roentgenol.,1933, 30, 641.
7. Armstrong, W. D., Radiotracer studies of hard tis-sues. Ann. New York Acad. Sc., 1955, 60, 670.
8. Bronner, F., Harris, R. S., Maletskos, C. J., andBenda, C. E., Studies in calcium metabolism.The fate of intravenously injected radiocalcium inhuman beings. J. Clin. Invest., 1956, 35, 78.
9. Fiske, C. H., and Logan, M. A., The determinationof calcium by alkalimetric titration. II. The pre-
886

CALCIUM METABOLISM IN THYROID DISEASE
cipitation of calcium in the presence of magnesium,phosphate, and sulfate, with applications to theanalysis of urine. J. Biol. Chem., 1931, 93, 211.
10. Fiske, C. H., and Subbarrow, Y., The colorimetricdetermination of phosphorus. J. Biol. Chem., 1925,66, 375.
11. Blau, M., Spencer, H., Swernov, J., and Laszlo, D.,Utilization and intestinal excretion of calcium inman. Science, 1954, 120, 1029.
12. Bauer, W., Albright, F., and Aub, J. C., Studies ofcalcium and phosphorus metabolism. II. The cal-cium excretion of normal individuals on a lowcalcium diet, also data on a case of pregnancy.J. Clin. Invest., 1929, 7, 75.
13. Engfeldt, B., Engstr6m, A., and Zetterstrom, R., Re-newal of phosphate in bone minerals. II. Radio-autographic studies of the renewal of phosphate indifferent structures of bone. Biochim. et Biophys.Acta, 1952, 8, 375.
14. Lacroix, P., Radiocalcium and radiosulphur in thestudy of bone metabolism at the histological levelin Proceedings of 2nd Radioisotope Conference,Oxford, 1954, New York, Academic Press, 1954,N. 1, p. 134.
15. Neuman, W. F., and Newman, M. W., The natureof the mineral phase of bone. Chem. Rev., 1953,53, 1.
16. Bauer, G. C. H., Carlsson, A., and Lindquist, B.,Evaluation of accretion, resorption, and exchangereactions in the skeleton. Kungl. FysiografiskaSallskapet, Lund Forhandlingar, 1955, 25, 1.
17. Askanazy, M., and Rutishauser, E., Die Knochen derBasedow-Kranken. Beitrag zur latenten Osteo-
dystrophia fibrosa. Virchows Arch. f. path. Anat.,1933, 291, 653.
18. Follis, R. H., Jr., Skeletal changes associated withhyperthyroidism. Bull. Johns Hopkins Hosp., 1953,92, 405.
19. Albright, F., and Reifenstein, E. C., Jr., The Para-thyroid Glands and Metabolic Bone Disease; Se-lected Studies. Baltimore, Williams & WilkinsCo., 1948.
20. Nielsen, H., The bone system in hyperthyroidism. Aclinical and experimental study. Acta med. Scan-dinav., 1952, 142, Supp. 266, 783.
21. Williams, H. L., and Watson, E. M., Influence ofhormones upon phosphatase content of rat femurs.II. Effects of sex hormones, thyroxin, and thymusextract. Endocrinology, 1941, 29, 258.
22. Kinsell, L. W., Hertz, S., and Reifenstein, E. C., Jr.,The effect of testosterone compounds upon the ni-trogen balance and the creatine excretion in pa-tients with thyrotoxicosis. J. Clin. Invest., 1944,23, 880.
23. Edholm, 0. G., and Howarth, S., Studies on theperipheral circulation in osteitis deformans. Clin.Sc., 1953, 12, 277.
24. Rawson, R. W., and Rall, J. E., Diseases of the Thy-roid in Duncan, G. G., Ed., Diseases of Metabo-lism, Detailed Methods of Diagnosis and Treat-ment, 3rd ed., Philadelphia, W. B. Saunders Com-pany, 1952, p. 957.
25. Robertson, J. D., Calcium and phosphorus excretionin thyrotoxicosis and myxoedema. Lancet, 1942, 1,672.
887