
Effect of Statin Therapy on the Progression of Common ... · Effect of Statin Therapy on the...
14
108 Journal of Atherosclerosis and Thrombosis Vol. 20, No. 1 Original Article Effect of Statin Therapy on the Progression of Common Carotid Artery Intima-Media Thickness: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials Yubei Huang 1 , Weiqin Li 2 , Lili Dong 3 , Ruilai Li 4 and Yangfeng Wu 4, 5 1 Department of Epidemiology and Biostatistics, Tianjin Medical University Cancer Institute and Hospital, Tianjin, China 2 Tianjin Women’s and Children’s Health Center, Tianjin, China 3 Tianjin University of Traditional Chinese Medicine, Tianjin, China 4 The George Institute for Global Health, Beijing, China 5 Department of Epidemiology and Biostatistics, School of Public Health, Peking University Health Science Center, Beijing, China Aim: To evaluate the effect of statin therapy on the decrease of common carotid artery intima-media thickness (CCA-IMT) compared to placebo or usual care. Methods: A systematic search of electronic databases (MEDLINE, EMBASE, and Cochrane Center Register) up to December 2011 was performed. Two reviewers independently determined the eligi- bility of randomized controlled trials (RCTs) comparing statin therapy with a placebo or usual care with a minimum follow-up of 6 months. Results: Twenty-one RCTs involving 6317 individuals were included in this review. The pooled weighted mean difference (WMD) between statin therapy and placebo or usual care on CCA-IMT was −0.029 mm (95%CI: −0.045, −0.013). Subgroup analyses showed significant effects of lovas- tatin (WMD: −0.077; 95%CI: −0.082, −0.073) and simvastatin (WMD: −0.069; 95%CI: −0.094, −0.045), followed by pravastatin and rosuvastatin, but no significant benefits of atorvastatin, fluvas- tatin, or cerivastatin. A greater decrease in mean CCA-IMT was observed in the setting of secondary prevention versus primary prevention (WMD: −0.045 vs. −0.004), in younger patients versus older patients (WMD: −0.057 vs. −0.041), and in studies where the patient proportion was males ≥ females ( −0.044 vs. −0.008). Meta-regression analysis showed a significant association between changes in mean CCA-IMT with decreasing triglyceride levels. A similar, but not statistically significant trend was also found between CCA-IMT decrease and the decrease in LDL-C levels or increase in HDL-C levels. Conclusion: Statin therapy is associated with a favorable decrease in CCA-IMT, an effect that seems to be mainly driven by the CCA-IMT at baseline and the extent of lipid decrease, specifically triglyc- erides. J Atheroscler Thromb, 2013; 20:108-121. Key words; Statin, IMT, Systematic review, Meta-analysis, Trials Introduction The PLAC Ⅱ (Pravastatin, Lipids, and Atheroscle- Address for correspondence: Yangfeng Wu, Room 334, Department of Epidemiology and Biostatistics, School of Public Health, Peking University Health Science Center, No. 38, Xueyuan Road, Haidian District, Beijing, 100191 China E-mail: [email protected]. Received: March 28, 2012 Accepted for publication: July 24, 2012 rosis in the Carotids) study in 1995 was the first trial to demonstrate pravastatin’s role in reducing common carotid artery intima-media thickness (CCA-IMT) in hypercholesterolemic patients with coronary heart dis- ease 1) . Several other randomized controlled trials that followed further demonstrated statins’ beneficial effect on progression of CCA-IMT in a wide range of indi- viduals 2-6) . However, other trials soon emerged show- ing conflicting results 7-12) , including the Regression Growth Evaluation Statin Study (REGRESS), which Yubei Huang and Weiqin Li contributed equally to this work.
Transcript of Effect of Statin Therapy on the Progression of Common ... · Effect of Statin Therapy on the...

108 Journal of Atherosclerosis and Thrombosis Vol.20, No.1
Original Article
Effect of Statin Therapy on the Progression of Common Carotid Artery Intima-Media Thickness: An Updated Systematic Review and Meta-Analysis of Randomized Controlled Trials
Yubei Huang1, Weiqin Li2, Lili Dong3, Ruilai Li4 and Yangfeng Wu4, 5
1Department of Epidemiology and Biostatistics, Tianjin Medical University Cancer Institute and Hospital, Tianjin, China2Tianjin Women’s and Children’s Health Center, Tianjin, China3Tianjin University of Traditional Chinese Medicine, Tianjin, China4The George Institute for Global Health, Beijing, China5Department of Epidemiology and Biostatistics, School of Public Health, Peking University Health Science Center, Beijing, China
Aim: To evaluate the effect of statin therapy on the decrease of common carotid artery intima-media thickness (CCA-IMT) compared to placebo or usual care.Methods: A systematic search of electronic databases (MEDLINE, EMBASE, and Cochrane Center Register) up to December 2011 was performed. Two reviewers independently determined the eligi-bility of randomized controlled trials (RCTs) comparing statin therapy with a placebo or usual care with a minimum follow-up of 6 months.Results: Twenty-one RCTs involving 6317 individuals were included in this review. The pooled weighted mean difference (WMD) between statin therapy and placebo or usual care on CCA-IMT was −0.029 mm (95%CI: −0.045, −0.013). Subgroup analyses showed significant effects of lovas-tatin (WMD: −0.077; 95%CI: −0.082, −0.073) and simvastatin (WMD: −0.069; 95%CI: −0.094, −0.045), followed by pravastatin and rosuvastatin, but no significant benefits of atorvastatin, fluvas-tatin, or cerivastatin. A greater decrease in mean CCA-IMT was observed in the setting of secondary prevention versus primary prevention (WMD: −0.045 vs. −0.004), in younger patients versus older patients (WMD: −0.057 vs. −0.041), and in studies where the patient proportion was males ≥ females (−0.044 vs. −0.008). Meta-regression analysis showed a significant association between changes in mean CCA-IMT with decreasing triglyceride levels. A similar, but not statistically significant trend was also found between CCA-IMT decrease and the decrease in LDL-C levels or increase in HDL-C levels.Conclusion: Statin therapy is associated with a favorable decrease in CCA-IMT, an effect that seems to be mainly driven by the CCA-IMT at baseline and the extent of lipid decrease, specifically triglyc-erides.
J Atheroscler Thromb, 2013; 20:108-121.
Key words; Statin, IMT, Systematic review, Meta-analysis, Trials
Introduction
The PLAC Ⅱ (Pravastatin, Lipids, and Atheroscle-
Address for correspondence: Yangfeng Wu, Room 334, Department of Epidemiology and Biostatistics, School of Public Health, Peking University Health Science Center, No. 38, Xueyuan Road, Haidian District, Beijing, 100191 ChinaE-mail: [email protected]: March 28, 2012Accepted for publication: July 24, 2012
rosis in the Carotids) study in 1995 was the first trial to demonstrate pravastatin’s role in reducing common carotid artery intima-media thickness (CCA-IMT) in hypercholesterolemic patients with coronary heart dis-ease1). Several other randomized controlled trials that followed further demonstrated statins’ beneficial effect on progression of CCA-IMT in a wide range of indi-viduals2-6). However, other trials soon emerged show-ing conflicting results7-12), including the Regression Growth Evaluation Statin Study (REGRESS), which
Yubei Huang and Weiqin Li contributed equally to this work.

109Statin Therapy and the Common Carotid Artery Intima-Media Thickness
at the end of the trial; and (3) follow-up was at least 6 months.
Data Sources and Searching StrategyTo identify relevant trials, searches in the follow-
ing 3 databases (from inception to October 25, 2011), MEDLINE (OVID), EMBASE, and Cochrane Cen-tral Register of Controlled Trials, were performed by two reviewers working independently and in parallel. References of related published major systematic reviews on the subject were also obtained and reviewed. Finally, the authors of possibly relevant trials were contacted when more information or clarification was needed.
Searches were not limited by language. Studies were obtained using the two groups of key terms as Medical Subject Headings in the searching strategies: 1) HMG-COA reductase inhibitor, hydroxymethylgl-utaryl-CoA reductase inhibitors, atorvastatin, fluvas-tatin, lovastatin, pravastatin, rosuvastatin and simvas-tatin; 2) carotid artery plaque, carotid artery diseases, carotid artery injuries, and carotid stenosis. (for details refer to Appendix 1).
Study SelectionTwo review authors (Huang and Li) working inde-
pendently and in parallel, scanned related abstracts and obtained the full text reports of studies when the abstract indicated or suggested the study was a RCT evaluating statin therapy based on the outcome of interest. After obtaining full reports of the candidate trials (either in full peer-reviewed publications or press articles), the same review authors independently assessed the eligibility of the studies for inclusion in the review. Any disagreement in study selection was adjudicated by a third reviewer (Wu).
Data CollectionThe same two review authors extracted data from
the eligible trials independently using standardized forms. Information about the statin, the type of inter-vention being tested, the baseline characteristics of the population being studied [age, sex, body mass index (BMI), current smoking, hypertension, history of myocardial infarction (MI), history of diabetes melli-tus (DM)], the baseline lipid levels [total cholesterol (TC), low density lipoprotein cholesterol (LDL-C), high density lipoprotein cholesterol (HDL-C), and triglycerides (TG)], the measurement and mean CCA-IMT in each arm, and the length of follow-up were collected.
When studies did not report baseline characteris-tics for the whole population, we re-calculated the
concluded that pravastatin had no effect on the far wall of CCA-IMT in male patients with coronary artery disease13).
Although previous systematic reviews have explored the effects of statin therapy on the progres-sion of CCA-IMT to make sense of the existing evi-dence, several critical concerns in the study designs of these reviews likely biased the pooled results. Ama-renco (2004) and Kang (2004) identified only 9 and 10 trials, respectively14, 15). The latest review (2010) included 11 trials16), but a few large-scale trials, such as the FAST (Fukuoka Atherosclerosis Trial)6), HYRIM (Hypertension High Risk Management trial)17), LiSA (Lescol in Severe Atherosclerosis trial)18), and PRE-VEND IT (Prevention of REnal and Vascular ENd-stage Disease Intervention Trial), were not included8). Each of these three reviews also included at least 2 of the following 4 trials, ARBITER (ARterial Biology for the Investigation of the Treatment Effects of Reducing cholesterol), ASAP (Atorvastatin versus Simvastatin on Atherosclerosis Progression), Van and VYCTOR (The VYtorin on Carotid intima-media Thickness and Overall arterial Rigidity), which compared the effects of different statins but not statins with a placebo and/or usual care19-22). These selection choices undoubtedly caused heterogeneity among the included trials and biased the pooled results. Furthermore, none of the three reviews explored the effect of statin therapy on the progression of CCA-IMT in different subgroups with respect to the demographic characteristics of the participants, the duration of follow-up, and the type and dose of statin used.
In order to update the current evidence on statin therapy and its effect on CCA-IMT progression, we undertook this systematic review and meta-analysis to help resolve these uncertainties and further define statins’ effect on CCA-IMT.
Method
We conducted this systematic review according to the PRISMA statement23).
Eligibility CriteriaAll potential randomized controlled trials (RCTs)
and cluster-RCTs were considered for review, exclud-ing quasi-RCTs (trials with little or no randomiza-tion), and trials comparing different statins or differ-ent doses of the same statin on CCA-IMT. Only eligi-ble RCTs fulfilling the following criteria were included in this systematic review: (1) the RCT compares a statin with either a placebo or usual care (including diet control); (2) the RCT provides mean CCA-IMT
110 Huang et al.
plots of the WMD versus its standard error25, 26). The I2 statistic was calculated as a measure of the propor-tion of the overall variation that is attributable to between-study heterogeneity27, 28). Because cerivastatin was withdrawn from the market in 2001 due to reports of fatal rhabdomyolysis29), sensitivity analysis excluding the trials evaluating the effect of cerivastatin was conducted.
Pre-specified subgroup meta-analysis was used to explore potential sources of between-study heteroge-neity according to the type of statin, patient’s condi-tion (primary prevention or secondary prevention), study quality (JADAD scored as low or high), dura-tion of follow-up (≥2 years or <2 years), mean age of participants (≥60 years or <60 years) and gender pro-portion (male ≥ female or male < female). Univariate meta-regression analysis was used to explore the dose response relationship between the change in CCA-IMT and baseline level of CCA-IMT, as well as the change in CCA-IMT and between-group differences in lipid level decrease30, 31).
All statistical analyses were performed with STATA (version 12.0).
arithmetical means. Any disagreement in data collec-tion was adjudicated by the same third reviewer (Wu).
Jadad scoring was used to assess the methodolog-ical quality of the studies24). Based on this system, studies are scored according to the presence of three key methodological features: randomization, blinding, and withdrawals/dropouts, with scores ranging from 0-5. Studies with a Jadad score of 4 or 5 are consid-ered high quality, while those receiving a score of 3 or less, low quality.
Data AnalysisWe calculated the weighted mean difference
(WMD) and appropriate 95% confidence intervals [CIs] using a random-effect model according to the number of patients based on intention-to-treat analy-sis when possible. The weight given to each study was equal to the inverse of the variance. In cases where studies did not report results based on intention-to-treat, we analyzed outcomes based on the randomized population.
Potential publication bias was assessed with the Begg test and represented graphically with funnel
229 reports identified using Medline,
EMBASE and Cochrane Center
181 reports excluded
- not randomized controlled trials (RCT)
- RCT with non-statin intervention
- RCT did not use intima-media thickness
(IMT) as outcome
46 reports identified from 35 potentially
relevant trials 14 trials excluded
- PLAS-II, KAPS, PHYLLIS, CAIUS did not
have enough data for meta-analysis
- Watanabe, OSACA-2, Yamada used
integrated backscatter values or plaque
thickness rather than IMT as outcome
- ARBITER, ASAP, Van, and VYCTOR
compared different statins
- Yu’s trial compared different doses of the
same statin
- Nakamura’s trial had a follow-up of less than
6 months
- Lorenzo’s trial was still ongoing
21 studies fulfilled the criteria and were
included
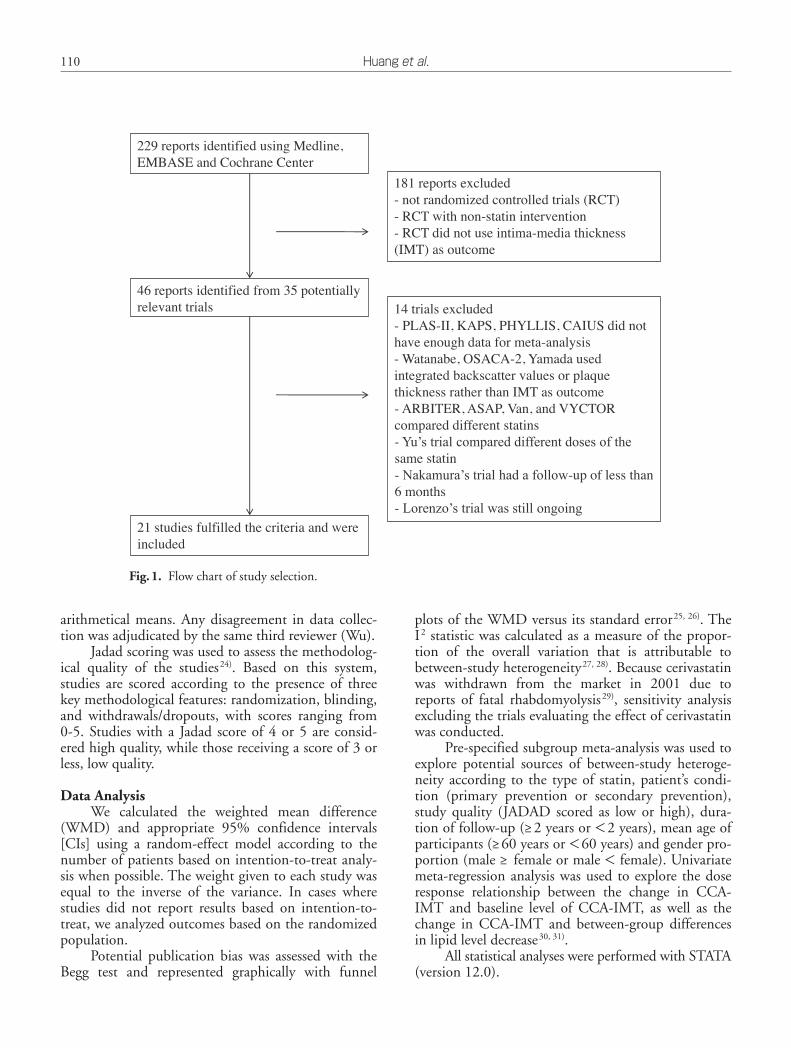
Fig.1. Flow chart of study selection.

111Statin Therapy and the Common Carotid Artery Intima-Media ThicknessTa
ble
1.C
hara
cter
isti
cs o
f inc
lude
d st
udie
s
Tria
l Pa
tient
s’ m
ajor
co
nditi
onD
esig
nJA
DA
D
Stat
inC
ontr
olFo
llow
Up,
yr
sPa
tient
s, T
(I/C
)A
ge,
yrs
Men
, %
PMI,
%
PDM
, %
H
P, %
c-SM
K,
%
BMI
ACA
PS, 1
994
Bae,
200
4
BCA
PS, 2
001
Beish
uize
n 20
04
FAST
, 200
2
HYR
IM, 2
004
LIPI
D, 1
998
LiSA
, 199
9
MA
RS,
199
3
MET
EOR
200
7
Peng
200
6
PREV
END
IT 2
005
REG
RES
S, 1
998
Rei
d 20
05
Sprin
g 20
08
Taka
hash
i 200
5-1
Taka
hash
i 200
5-2
Wie
gman
200
4
Wu
2007
-1
Wu
2007
-2
Zha
ng 2
004
Ito 2
004-
1
Ito 2
004-
2
Yoko
yam
a 20
05
Car
otid
AS
(S)
CH
D (S
)
Car
otid
AS
(S)
DM
(P)
HC
ho (P
)
HP(
P)
CH
D (S
)
CH
D (S
)
CA
D (S
)
Subc
linic
al A
S (S
)
HP +
caro
tid A
S (S
)
Mic
roal
bum
inur
ia(P
)
CH
D (S
)
CA
D (S
)
PAD
(P)
DM
and
HC
ho (P
)
DM
and
HC
ho (P
)
Fam
ilial
HC
ho (P
)
HP
(P)
HP
(P)
Car
otid
AS
(S)
HC
ho (P
)
HC
ho (P
)
HC
ho (P
)
DB
NR
DB
DB
NR
DB
DB
DB
DB
TB
NR
DB
DB
DB
O NR
NR
DB
O O NR
O O O
BR R R BR MR
R R R R BR R R BR BR BR R R BR R R R R R R
3 1 3 4 3 3 4 4 2 5 1 3 3 4 3 1 1 4 1 1 1 2 2 2
L A* F S P F P F L R S**
P P P A S P P A A S C P F
20-4
0
10 40 20 10 40 40 40 80 40 20 40 40 40 80 5-10
10-2
0
20-4
0
10 20 5
0.3
20 40
PLA
UC
PLA
PLA
UC
PLA
PLA
PLA
PLA
PLA
anti-
HP
PLA
PLA
PLA
PLA
PLA
PLA
PLA
PLA
PLA
PLA
UC
UC
UC
3 0.5 3 2 2 4 4 1 4 2 3 3.8 2
0.75 0.5 1 1 2 1 1 3 0.5
0.5 1
461
(230
/231
)
205
(105
/100
)
793
(395
/398
)
250
(125
/125
)
164
(83/
81)
568
(283
/285
)
522
(273
/249
)
365
(187
/178
)
188
(99/
89)
984
(702
/282
)
162
(82/
80)
642
(317
/325
)
255
(131
/124
)
54 (2
8/26
)
100
(48/
52)
30 (1
5/15
)
30 (1
5/15
)
214
(106
/108
)
90 (5
0/40
)
101
(61/
40)
52 (2
4/28
)
24 (1
3/11
)
23 (1
2/11
)
40 (2
0/20
)
61.6
60.0
61.9
58.5
66.3
57.1
61.0
59.8
58.0
57.0
62.0
50.8
56.2
70.5
67.0
58.1
57.5
13.0
71.0
71.0
57.0
64.0
64.5
61.0
51.3
67.8
45.5
47.2
31.7
100.
0
88.0
61.6
92.0
59.5
58.6
65.0
100.
0
− 78.2
− − 46.0
60.3
60.3
− 32.0
52.1
37.5
− 12.2 − − − − 75.0
35.6 − − − − 51.2 − − − − − − − − 0.0
0.0
0.0
2.0
29.8 3.2
100.
0
25.0
− 5.0
5.5
− 9.5
− 4.3
− 14.0
29.0
100.
0
100.
0
− − − − 16.7
17.4
15.0
31.2
48.3
12.2
50.0
39.6
100.
0
− 29.4 − 20.5
100.
0
− 26.5 − − − − −
100.
0
100.
0
− 50.0
43.4
35.0
11.5
41.5
30.8
24.0
59.8
18.3
− 9.6
16.0 4.5
− 39.5
31.5
55.0
32.1 − − 11.0 − − − 20.8
21.7
22.5
25.8
− 25.5
31.0
23.2
29.2 − − − 27.3 − − 26.3 − 25.4
23.7
24.5
20.0 − − − 23.0
23.0
23.7
Not
e: P
atie
nts’
maj
or c
ondi
tion
: AS,
ath
eros
cler
osis
; CH
D, c
oron
ary
hear
t di
seas
e; D
M, d
iabe
tes
mel
litus
; HC
ho, h
yper
chol
este
role
mia
; HP,
hyp
erte
nsio
n; C
HD
, cor
onar
y ar
tery
dis
ease
; PA
D, p
erip
hera
l art
eria
l dis
ease
; (P)
, pri
mar
y pr
even
tion
; (S)
, sec
onda
ry p
reve
ntio
n.D
esig
n: D
B, d
oubl
e bl
ind;
NR
, not
rep
orte
d; T
B, t
ri-b
lind;
O, o
pen;
R, r
ando
miz
atio
n w
itho
ut d
etai
led
info
rmat
ion;
BR
, blo
ck r
ando
miz
atio
n; M
R, m
ulti
-cen
tere
d ra
ndom
izat
ion.
Stat
in: L
, Lov
asta
tin;
A, A
torv
asta
tin;
F, F
luva
stat
in; S
, Sim
vast
atin
; P, P
rava
stat
in; R
, Ros
uvas
tati
n; C
, cer
ivas
tati
n; P
LA
, pla
cebo
; UC
, usu
al c
are;
ant
i-H
P, a
nti-
hype
rten
sion
the
rapy
; *
, Ato
rvas
tati
n+U
C; **
, S+
aspi
rin +
anti
-hyp
erte
nsio
n.Pa
tien
ts, T
(I/
C):
T, T
otal
; I: i
nter
vent
ion;
C: c
ontr
ol;
PMI,
pre
viou
s m
yoca
rdia
l inf
arct
ion;
PD
M, p
ervi
ous
diab
etes
mel
litus
; c-S
MK
, cur
rent
sm
okin
g; B
MI,
bod
y m
ass
inde
x.

112 Huang et al.Ta
ble
2.M
ean
CC
A-I
MT
and
ser
um li
pid
at b
asel
ine
and
follo
w-u
p in
eac
h in
clud
ed s
tudy
Tria
lC
CA
-IM
T, m
mT
C, m
g/dL
TG
, mg/
dLLD
L-C
, mg/
dLH
DL-
C, m
g/dL
B (I
/C)
F (I
/C)
F (I
/C),
sdB
(I/C
)F
(I/C
)B
(I/C
)F
(I/C
)B
(I/C
)F
(I/C
)B
(I/C
)F
(I/C
)
ACA
PS, 1
994
Bae,
200
4
BCA
PS, 2
001
Beish
uize
n, 2
004
FAST
, 200
2
HYR
IM, 2
004
LIPI
D, 1
998
LiSA
, 199
9
MA
RS,
199
3
MET
EOR
, 200
7
Peng
, 200
6
PREV
END
IT, 2
005
REG
RES
S, 1
998
Rei
d, 2
005
Sprin
g, 2
008
Taka
hash
i, 20
05-1
Taka
hash
i, 20
05-2
Wie
gman
, 200
4
Wu,
200
7-1
Wu,
200
7-2
Zha
ng, 2
004
Ito, 2
004-
1
Ito, 2
004-
2
Yoko
yam
a, 2
005
1.15
0/1.
140
0.87
0/0.
870
0.89
5/0.
910
0.76
3/0.
780
1.26
7/1.
286
0.79
7/0.
801
0.80
4/0.
786
0.74
0/0.
720
0.75
7/0.
694
0.76
0/0.
760
1.00
0/1.
030
0.77
0/0.
770
0.86
0/0.
860
1.53
0/1.
520
0.76
0/0.
780
1.02
8/1.
017
1.07
9/1.
017
0.49
7/0.
492
1.05
0/1.
020
1.05
0/1.
020
0.87
0/0.
760
0.87
0/0.
890
1.09
0/0.
890
0.90
0/0.
870
1.12
3/1.
158
0.88
0/0.
890
0.90
5/0.
945
0.76
5/0.
774
1.09
1/1.
586
0.85
5/0.
864
0.79
0/0.
831
0.72
0/0.
690
0.66
2/0.
740
0.76
1/0.
778
0.80
0/1.
080
0.81
0/0.
810
0.83
1/0.
842
1.37
0/1.
470
0.73
0/0.
770
1.04
1/1.
045
1.09
9/1.
045
0.48
7/0.
487
1.04
0/1.
020
1.04
0/1.
020
0.91
0/0.
810
0.88
0/0.
900
1.11
0/0.
900
0.86
0/0.
920
0.19
0/0.
190
0.29
0/0.
150
0.20
5/0.
216
0.11
6/0.
124
0.64
2/0.
501
0.17
7/0.
190
0.00
9/0.
009
0.13
0/0.
110
0.01
2/0.
017
0.12
0/0.
120
0.18
0/0.
150
0.16
0/0.
170
0.05
1/0.
050
0.19
0/0.
310
0.09
0/0.
100
0.13
6/0.
167
0.15
3/0.
167
0.04
8/0.
044
0.11
0/0.
120
0.12
0/0.
120
0.30
0/0.
240
0.22
0/0.
240
0.38
0/0.
240
0.27
0/0.
270
236.
1/23
6.2
194.
0/18
9.0
237.
6/23
6.1
212.
5/21
6.7
251.
5/25
5.2
229.
5/23
1.0
217.
9/22
1.0
289.
0/28
4.0
230.
3/23
4.1
229.
0/23
0.0
236.
1/23
6.1
224.
5/22
4.5
239.
2/23
6.8
198.
9/20
8.6
181.
9/17
4.2
255.
9/19
1.7
256.
1/19
1.7
302.
0/30
0.0
− −
232.
2/19
3.5
251.
0/24
3.0
257.
0/24
3.0
247.
0/25
0.0
−
153.
0/18
3.0
−
173.
8/22
2.1
193.
7/24
0.0
−
177.
6/21
6.7
238.
7/27
0.1
155.
2/23
1.4
151.
0/23
0.0
193.
5/24
7.7
−
190.
4/23
7.6
162.
9/19
9.7
149.
0/17
4.2
− −
246.
0/29
8.0
− −
193.
5/19
3.5
201.
0/24
2.0
205.
0/24
2.0
202.
0/24
3.0
318.
6/32
7.5
193.
0/18
3.0
99.1
/105
.3
161.
1/16
6.4
168.
7/13
5.8
154.
0/16
2.0
157.
5/14
6.0
189.
0/18
3.0
157.
5/15
8.4
126.
0/13
4.0
203.
6/19
4.7
−
163.
7/16
1.1
−
147.
8/16
6.4
150.
4/12
9.1
184.
5/12
9.1
70.0
/64.
0
− −
150.
5/11
5.1
− −
189.
0/17
6.0
−
174.
0/19
0.0
−
141.
6/15
2.2
− −
140.
7/14
8.7
−
119.
5/16
1.1
98.0
/139
.0
132.
8/22
1.3
−
147.
8/17
2.6
−
126.
6/17
7.9
− −
58.0
/65.
0
− −
141.
6/11
5.1
− −
154.
0/16
7.0
157.
1/15
5.6
122.
0/11
3.0
162.
5/16
2.5
133.
1/13
7.4
160.
7/17
1.6
149.
8/15
0.2
149.
8/15
5.6
198.
0/19
3.0
156.
0/15
8.7
155.
0/15
4.0
127.
7/12
3.8
−
168.
7/16
7.6
−
97.9
/92.
1
− −
239.
0/23
7.0
138.
5/13
1.6
140.
5/13
1.6
135.
5/13
1.6
150.
0/16
0.0
148.
0/16
0.0
154.
0/15
6.0
−
86.0
/109
.0
−
99.8
/146
.3
103.
0/15
7.0
130.
8/15
4.4
108.
0/14
7.8
144.
7/17
7.6
85.1
/154
.8
78.0
/152
.0
81.3
/127
.7
−
120.
4/16
6.4
−
72.0
/90.
2
− −
182.
0/23
7.0
97.1
/133
.5
84.0
/133
.5
123.
8/12
7.7
103.
0/15
3.0
108.
0/15
3.0
118.
0/15
6.0
52.2
/52.
0
37.6
/37.
3
53.4
/53.
4
47.6
/46.
8
56.7
/56.
5
49.1
/49.
5
36.8
/36.
4
53.0
/56.
0
43.0
/43.
3
50.0
/49.
0
52.2
/51.
1
−
38.3
/37.
5
−
48.4
/46.
1
51.5
/48.
3
49.0
/48.
3
47.0
/48.
0
− −
46.4
/50.
3
54.0
/60.
0
54.0
/60.
0
52.0
/57.
0
−
39.1
/36.
7
−
46.4
/47.
2
60.3
/59.
6
−
37.2
/35.
2
−
46.4
/44.
5
53.0
/50.
0
62.7
/50.
7
−
40.6
/36.
8
−
48.4
/47.
6
− −
50.0
/49.
0
− −
46.4
/46.
4
61.0
/62.
0
57.0
/62.
0
57.0
/55.
0
Not
e: B
: bas
elin
e; F
: end
of f
ollo
w-u
p; I
: int
erve
ntio
n; C
: con
trol
; sd,
sta
ndar
d de
viat
ion
of m
ean
CC
A-I
MT
at f
ollo
w-u
p.

113Statin Therapy and the Common Carotid Artery Intima-Media Thickness
IMT as the outcome measure35-37); (3) ARBITER, ASAP, Van, and VYCTOR compared different statins19-22); (4) Yu’s trial compared different doses of the same statin38); (5) Nakamura’s trial had a follow-up of less than 6 months39); and (6) Lorenzo’s trial was still ongoing at the time of our analysis40). Twenty-one studies met the inclusion criteria and were thus included in this systematic review (Fig.1).
Study CharacteristicsThe 21 trials (investigating 7 different statins) had
a sample size ranging from 36 to 984, and involved 6317 individuals2-13, 17, 18, 41-47). Twelve of the studies recruited participants with a previous history of car-diovascular disease or subclinical carotid atherosclero-sis (AS). The remaining 9 studies recruited partici-pants without an obvious diagnosis of carotid AS. The reported mean age of the participants ranged from 51 to 71 years old with the exception of Wiegman’s study
Role of the Funding SourceNo funding sources had a role in the study
design, data collection, analysis, interpretation or writ-ing of the report. The writing group had full access to all the data contained in the study and take final responsibility for the explanation of the results.
Results
Study SelectionA search of Medline, EMbase and Cochrane
Central provided 229 citations. Of these, 181 trials did not meet all the inclusion criteria based on a review of the abstracts and were discarded. Another 14 trials were excluded after reviewing the full papers: (1) PLAS-Ⅱ, KAPS, PHYLLIS, and CAIUS did not pro-vide enough data for meta-analysis1, 32-34); (2) Wata-nabe, OSACA-2, and Yamada used integrated back-scatter values or plaque thickness rather than CCA-
NOTE: Weights are from random effects analysis
Overall (I-squared = 95.7%, p = 0.000)
ID
Wu 2007-2
Ito 2004-2
METEOR 2007
ACAPS, 1994
Ito 2004-1
Wu 2007-1
LiSA, 1999
Wiegman 2004
BCAPS, 2001
REGRESS, 1998 PREVEND IT 2005
Reid 2005
Takahashi 2005-1
Beishuizen 2004
Peng 2006
Takahashi 2005-2
MARS, 1993
LIPID, 1998
Zhang 2004
FAST, 2002 HYRIM, 2004
Yokoyama 2005
Bae, 2004
Spring 2008
Study
-0.03 (-0.05, -0.01)
WMD (95% CI)
0.02 (-0.03, 0.07)
0.21 (-0.05, 0.47)
-0.02 (-0.03, -0.00)
-0.04 (-0.07, -0.00)
-0.02 (-0.21, 0.17)
0.02 (-0.03, 0.07)
0.03 (0.01, 0.05)
0.00 (-0.01, 0.01)
-0.04 (-0.07, -0.01)
-0.01 (-0.02, 0.00) 0.00 (-0.03, 0.03)
-0.10 (-0.24, 0.04)
-0.00 (-0.11, 0.10)
-0.01 (-0.04, 0.02)
-0.28 (-0.33, -0.23)
0.05 (-0.06, 0.17)
-0.08 (-0.08, -0.07)
-0.04 (-0.04, -0.04)
0.10 (-0.05, 0.25)
-0.50 (-0.67, -0.32) -0.01 (-0.04, 0.02)
-0.06 (-0.23, 0.11)
-0.01 (-0.07, 0.05)
-0.04 (-0.08, -0.00)
Statin
61, 1.040 (0.120)
12, 1.110 (0.380)
702, 0.761 (0.120)
230, 1.123 (0.190)
13, 0.880 (0.220)
50, 1.040 (0.110)
187, 0.720 (0.130)
106, 0.487 (0.048)
395, 0.905 (0.205)
131, 0.831 (0.051) 317, 0.810 (0.160)
28, 1.370 (0.190)
15, 1.041 (0.136)
125, 0.765 (0.116)
82, 0.800 (0.180)
15, 1.099 (0.153)
99, 0.662 (0.012)
273, 0.790 (0.009)
24, 0.910 (0.300)
83, 1.091 (0.642) 283, 0.855 (0.177)
20, 0.860 (0.270)
105, 0.880 (0.290)
48, 0.730 (0.090)
N, mean (SD);
2913
Control
40, 1.020 (0.120)
11, 0.900 (0.240)
282, 0.778 (0.120)
231, 1.158 (0.190)
11, 0.900 (0.240)
40, 1.020 (0.120)
178, 0.690 (0.110)
108, 0.487 (0.044)
398, 0.945 (0.216)
124, 0.842 (0.050) 325, 0.810 (0.170)
26, 1.470 (0.310)
15, 1.045 (0.167)
125, 0.774 (0.124)
80, 1.080 (0.150)
15, 1.045 (0.167)
89, 0.740 (0.017)
249, 0.831 (0.009)
28, 0.810 (0.240)
81, 1.586 (0.501) 285, 0.864 (0.190)
20, 0.920 (0.270)
100, 0.890 (0.150)
52, 0.770 (0.100)
N, mean (SD);
100.00
Weight
4.42
0.37
6.74
5.43
0.68
4.40
6.20
6.96
5.85
6.96 6.14
1.14
1.67
5.81
4.20
1.55
7.22
7.26
1.00
0.75 5.78
0.82
3.45
5.22
% WMD (95% CI)
3404
Statin reduces IMT Statin increases IMT 0 WMD (95% CI)
Fig.2. Meta-analysis of statin therapy on the progression of mean CCA-IMT.

114 Huang et al.
This was consistent across both the low and high qual-ity studies as identified by JADAD scoring. A signifi-cant decrease in mean CCA-IMT was observed in studies using statins for secondary prevention (WMD: −0.045; 95%CI: −0.046, −0.043), but not primary prevention (WMD: −0.004; 95%CI: −0.013, 0.006). The effect was also significant only after a duration of at least 2 or more years on statin therapy (WMD: −0.044; 95%CI: −0.045, −0.043). The effect was observed to be greater among a younger patient pop-ulation than an older patient population (WMD: −0.057 vs. −0.041), and in trials where males out-numbered females (−0.044 vs. −0.008) (Table 3).
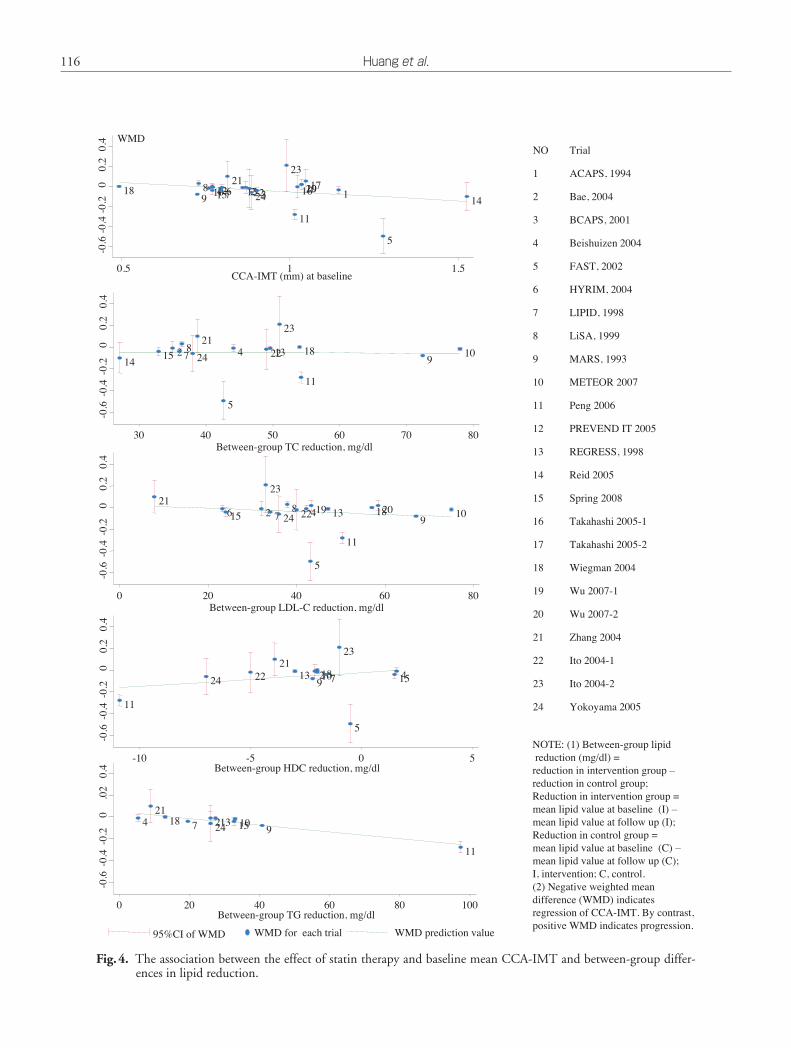
In an attempt to identify other sources of resid-ual difference between trials, we performed meta-regression analysis of baseline mean CCA-IMT and the net decrease (difference between decrease of inter-vention and control group) in lipid levels (TC, TG, LDL-C and HDL-C) (Fig.4). Of these variables, we found a significant association between decreases of mean CCA-IMT with net decrease in TG levels. A similar, but not statistically significant trend was also seen in mean CCA-IMT decrease and decrease in LDL-C levels and increase in HDL-C levels. No such association was found in regard to changes in TC levels.
Discussion
Summary of EvidenceOverall, statins can significantly reduce CCA-
IMT compared to a placebo or usual care; however,
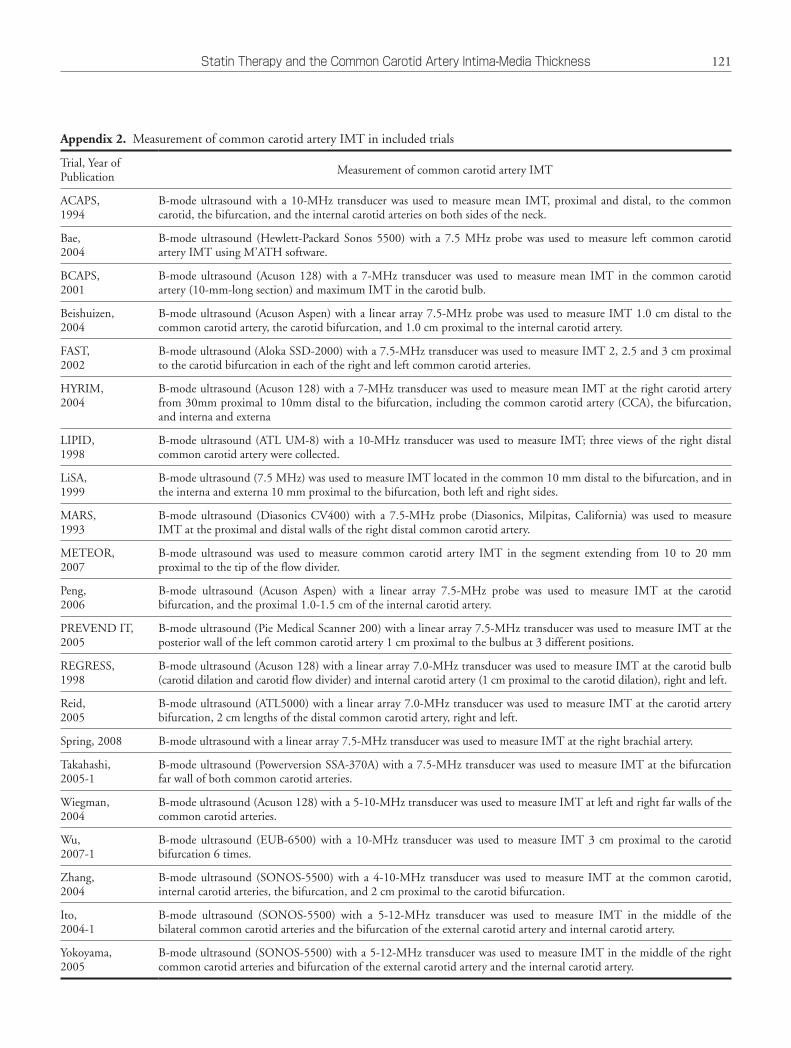
(mean age 13 years old)47), and the proportion of males in the included studies ranged from 32% to 100% (Table 1). CCA-IMT was measured with B- mode ultrasound in all included cases (for details refer to Appendix 2) and the mean CCA-IMT at baseline ranged from 0.495 mm to 1.525 mm (Table 2).
Syntheses of ResultsWe detected a significant weighted mean differ-
ence (WMD) in the decrease in mean CCA-IMT between statin therapy and placebo or usual care (WMD: −0.029; 95%CI: −0.045, −0.013). Strong evidence of heterogeneity (I2=95.7%, p<0.001) was observed (Fig.2). Sensitivity analyses excluding the trial evaluating the effect of cerivastatin resulted in a minor increase in the I2 from 95.7% to 95.9%, but no change in the pooled WMD46). Another sensitivity analysis excluding Wiegman’s trial resulted in a slight improvement in heterogeneity, but again no change in the pooled WMD47); however, both the Begg test (p=0.005) and funnel plots (Fig.3) demonstrated a significant publication bias when looking at all 21 tri-als.
Additional AnalysesSubgroup analyses showed significant effects of
lovastatin (WMD: −0.077; 95%CI: −0.082, −0.073) and simvastatin (WMD: −0.069; 95%CI: −0.094, −0.045) on the decrease of mean CCA-IMT, followed by pravastatin and rosuvastatin, but no significant benefits of atorvastatin, fluvastatin, or cerivastatin.
0
.05
.1
.15
S
E(W
MD
)
-0.6 -0.4 -0.2 0 0.2
Weighted mean difference (WMD)
Fig.3. Funnel plot of the weighted mean difference versus its SE.

115Statin Therapy and the Common Carotid Artery Intima-Media Thickness
showed that lowering serum cholesterol is effective in controlling the progression of CCA-IMT in a preven-tative setting and/or in patients whose presentation of atherosclerosis is still at an asymptomatic stage32, 33).
Thirdly, we found a significant relationship between CCA-IMT decrease and the net decrease in TG (Fig.5). We also found a strong, although not sta-tistically significant relationship between the magni-tude of CCA-IMT decrease and the net decrease in LDL-C levels. The role of hypertriglyceridemia in the pathogenesis of atherosclerotic disease has been con-troversial for many years48, 49), despite extensive inves-tigation by basic scientists, clinicians, and epidemiolo-gists. Because triglycerides do not accumulate in the vessel wall, its atherogenicity is thought to be based on the association between triglycerides and cholesterol50). Because of the multiple links between elevated triglyc-eride levels and risk for atherosclerotic cardiovascular disease, it seems prudent to screen for the presence of hypertriglyceridemia when determining a patient’s risk for atherosclerotic cardiovascular disease. A therapeu-tic program targeting a decrease of triglycerides is even more important in patients with hypertriglyceridemia than in persons with isolated hypercholesterolemia50).
Fourthly, findings from CAIUS and ACAPS sug-
this beneficial effect is not consistently seen in all statins, as insufficient evidence was found in the cases of atorvastatin, fluvastatin and cerivastatin. This is the first difference drawn from our systematic review compared with previous systematic reviews; however, further studies are needed to clarify the differential effects of statins on CCA-IMT.
Secondly, we found that the effect of lipid lower-ing on decreases in CCA-IMT was significant only in the setting of statin’s use in secondary prevention, namely in the presence of carotid AS or more advanced arterial diseases such as coronary artery dis-ease, but not in the setting of primary prevention. A possible explanation for this observation may be due to the larger IMT seen in more serious diseases, thus providing greater potential for decrease; however, this does not mean that statin therapy is unnecessary in the primary prevention of subclinical carotid AS. The lack of statin’s beneficial effect in a primary prevention setting may be due to the small sample size, because the pooled WMD was still negative at −0.004, although statistically insignificant. An included trial that looked at statin therapy in the setting of primary prevention, FAST6), showed it to be effective in reduc-ing CCA-IMT. Similar findings in CAIUS and KAPS
Table 3. Pre-specified subgroup analysis of statin therapy on the progression of mean CCA-IMT
Subgroup analysis Number of study Weighted mean difference (95%CI) p for test of WMD=0 I2
Type of statinLovastatinAtorvastatinFluvastatinSimvastatinPravastatinRosuvastatinCerivastatin
Patient conditionSecondary preventionPrimary prevention
Study qualityLowHigh
Duration of follow-upFollow up ≥2 yrsFollow up <2 yrs
Mean ageAge ≥60Age <60
GenderMale ≥FemaleMale <Female
2444811
1113
186
1311
1311
146
−0.077 (−0.082, −0.073)−0.008 (−0.031, 0.016)−0.002 (−0.018, 0.014)−0.069 (−0.094, −0.045)−0.040 (−0.041, −0.038)−0.017 (−0.034, 0.000)−0.020 (−0.206, 0.166)
−0.045 (−0.046, −0.043)−0.004 (−0.013, 0.006)
−0.067 (−0.070, −0.063)−0.040 (−0.041, −0.038)
−0.044 (−0.045, −0.043)0.009 (−0.007, 0.025)
−0.041 (−0.043, −0.040)−0.057 (−0.060, −0.053)
−0.044 (−0.046, −0.043)−0.008 (−0.019, 0.002)
<0.0010.5230.772
<0.001<0.001
0.0440.833
<0.0010.443
<0.001<0.001
<0.0010.274
<0.001<0.001
<0.0010.118
82.80%45.00%77.90%96.60%93.30%−
−
97.60%70.20%
94.10%94.10%
97.50%38.70%
90.60%97.10%
97.10%86.10%
116 Huang et al.
Fig.4. The association between the effect of statin therapy and baseline mean CCA-IMT and between-group differ-ences in lipid reduction.
NO Trial
1 ACAPS, 1994
2 Bae, 2004
3 BCAPS, 2001
4 Beishuizen 2004
5 FAST, 2002
6 HYRIM, 2004
7 LIPID, 1998
8 LiSA, 1999
9 MARS, 1993
10 METEOR 2007
11 Peng 2006
12 PREVEND IT 2005
13 REGRESS, 1998
14 Reid 2005
15 Spring 2008
16 Takahashi 2005-1
17 Takahashi 2005-2
18 Wiegman 2004
19 Wu 2007-1
20 Wu 2007-2
21 Zhang 2004
22 Ito 2004-1
23 Ito 2004-2
24 Yokoyama 2005
NOTE: (1) Between-group lipid
reduction (mg/dl) =
reduction in intervention group –
reduction in control group;
Reduction in intervention group =
mean lipid value at baseline (I) –
mean lipid value at follow up (I);
Reduction in control group =
mean lipid value at baseline (C) –
mean lipid value at follow up (C);
I, intervention; C, control.
(2) Negative weighted mean
difference (WMD) indicates
regression of CCA-IMT. By contrast,
positive WMD indicates progression.95%CI of WMD WMD prediction valueWMD for each trial
1898 1012154 76
2113222243
23
11
161920171
5
14
-0.6
-0.4
-0.2
00
.20
.4
0.5 1 1.5 CCA-IMT (mm) at baseline
WMD
21615 2
23
7 248
224
5
19 13
11
18209
10
-0.6
-0.4
-0.2
00
.20
.4
0 20 40 60 80Between-group LDL-C reduction, mg/dl
1415 27
824
21
5
4 2213
23
18
11
910
-0.6
-0.4
-0.2
00
.20
.4
30 40 50 60 70 80Between-group TC reduction, mg/dl
11
24 22
2113
9218107
23
5
154
-0.6
-0.4
-0.2
00
.20
.4
-10 -5 0 5Between-group HDC reduction, mg/dl
421
18 7 24213 1510
9
11
-0.6
-0.4
-0.2
0.0
20
.4
0 20 40 60 80 100 Between-group TG reduction, mg/dl

117Statin Therapy and the Common Carotid Artery Intima-Media Thickness
ues could not be calculated. Although we can still use the data from the remaining studies with complete baseline and follow-up lipid values, the results may lead to lower power for the conclusion.
Conclusions
Statins can significantly reduce the common carotid intima-media thickness when compared with a placebo or usual care, and this effect is mainly driven by baseline CCA-IMT and the extent of between-group lipid decrease.
Conflict of Interest
None.
References
1) Byington RP, Furberg CD, Crouse Iii JR, Espeland MA, Bond MA: Pravastatin, Lipids, and Atherosclerosis in the Carotid Arteries (PLAC-Ⅱ). The American Journal of Cardiology, 1995; 76: 54c-59c
2) Crouse JR, Raichlen JS, Riley WA, Evans GW, Palmer MK, O’Leary DH, Grobbee DE, Bots ML: Effect of rosu-vastatin on progression of carotid intima-media thickness in low-risk individuals with subclinical atherosclerosis: The METEOR Trial. JAMA, 2007; 297: 1344-1353
3) Hedblad B, Wikstrand J, Janzon L, Wedel H, Berglund G: Low-dose metoprolol CR/XL and fluvastatin slow pro-gression of carotid intima-media thickness: Main results from the (beta)-blocker cholesterol-lowering asymptom-atic plaque study (BCAPS). Circulation, 2001; 103: 1721-1726
4) Hodis HN, Mack WJ, LaBree L, Selzer RH, Liu C, Alau-povic P, Kwong-Fu H, Azen SP: Reduction in carotid arterial wall thickness using lovastatin and dietary therapy: a randomized controlled clinical trial. Ann Intern Med, 1996; 124: 548-556
5) MacMahon S, Sharpe N, Gamble G, Hart H, Scott J, Simes J, White H: Effects of lowering average of below-average cholesterol levels on the progression of carotid atherosclerosis: results of the LIPID Atherosclerosis Sub-study. LIPID Trial Research Group. Circulation, 1998; 97: 1784-1790
6) Sawayama Y, Shimizu C, Maeda N, Tatsukawa M, Kinu-kawa N, Koyanagi S, Kashiwagi S, Hayashi J: Effects of probucol and pravastatin on common carotid atheroscle-rosis in patients with asymptomatic hypercholesterolemia. Fukuoka Atherosclerosis Trial (FAST). J Am Coll Cardiol, 2002; 39: 610-616
7) Bae JH, Bassenge E, Kim KY, Synn YC, Park KR, Schwemmer M: Effects of low-dose atorvastatin on vascu-lar responses in patients undergoing percutaneous coro-nary intervention with stenting. J Cardiovasc Pharmacol Ther, 2004; 9: 185-192
8) Asselbergs FW, Van Roon AM, Hillege HL, De Jong PE,
gested that there may be an “efficacy window”, i.e., a carotid IMT range, during which progression may be slowed and/or stabilized, but above which lipid-lower-ing treatment is less effective32, 51). The results of our systematic review showed that lowering lipid levels can reduce atherosclerotic progression within a broad range of baseline IMT and cholesterol levels (results not shown). More interestingly, as baseline IMT increased, the decrease in CCA-IMT also increased. This finding further supports the use of lipid-lowering therapy in symptomatic or worse stages of AS, as lipid-lowering treatment may lead to greater stabiliza-tion in the progression of AS.
Risk of Bias Across StudiesSpecifically, four trials, PLAS-Ⅱ, KAPS, PHYL-
LIS and CAIUS, involving about 1400 participants, either did not report mean CCA-IMT or only reported the maximum IMT at the end of their stud-ies1, 32-34). Undoubtedly, omission of these trials may be the source of the asymmetry seen in the funnel plot. The demographic characteristics of the partici-pants, the duration of follow-up, and the type and dose of statin used can also lead to heterogeneity. Despite these potential biases, sensitivity analyses and subgroup analysis revealed nearly consistent results.
Limitations
The present study has some potential limitations that should be considered. First, a meta-analysis is ret-rospective research that is subject to the methodologi-cal deficiencies of the studies included, although we tried to minimize the likelihood of bias by developing a detailed protocol and using explicit criteria for study selection, data extraction, and analysis. Second, as in other meta-analyses, these results should be inter-preted with caution, since individual studies varied considerably with respect to the demographic charac-teristics of the participants, the duration of follow-up, and the type and dose of statin used. The benefits of statin therapy on CCA-IMT depend on the baseline risk of the populations treated. In primary prevention trials, the benefits of statins remain unclear. Third, we had insufficient data to analyze the effects of statins on mean CCA-IMT in different subgroups (e.g., men and women). Such analyses are more informative when performed using individual participant data rather than cohort level data. Similar approaches are also needed to determine whether there is a significant correlation between decreasing LDL-C and decreases in mean CCA-IMT. Fourth, as shown in Table 2, in several studies, changes in lipid and lipoproteins val-

118 Huang et al.
conventional lipid lowering on atherosclerosis progression in familial hypercholesterolaemia (ASAP): a prospective, randomised, double-blind trial. Lancet, 2001; 357: 577-581
21) Van Tits LJH, Smilde TJ, Van Wissen S, De Graaf J, Kastelein JJP, Stalenhoef AFH: Effects of atorvastatin and simvastatin on low-density lipoprotein subfraction profile, low-density lipoprotein oxidizability, and antibodies to oxidized low-density lipoprotein in relation to carotid intima media thickness in familial hypercholesterolemia. J Investig Med, 2004; 52: 177-184
22) Meaney A, Ceballos G, Asbun J, Solache G, Mendoza E, Vela A, Meaney E: The vytorin on carotid intima-media thickness and overall arterial rigidity (VYCTOR) study. J Clin Pharmacol, 2009; 49: 838-847
23) Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D: The PRISMA statement for reporting system-atic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ, 2009; 339: b2700
24) Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ: Assessing the quality of reports of randomized clinical trials: is blinding neces-sary ? Control Clin Trials, 1996; 17: 1-12
25) Begg CB, Mazumdar M: Operating characteristics of a rank correlation test for publication bias. Biometrics, 1994; 50: 1088-1101
26) Egger M, Davey Smith G, Schneider M, Minder C: Bias in meta-analysis detected by a simple, graphical test. BMJ, 1997; 315: 629-634
27) Higgins JP, Thompson SG: Quantifying heterogeneity in a meta-analysis. Stat Med, 2002; 21: 1539-1558
28) Higgins JP, Thompson SG, Deeks JJ, Altman DG: Mea-suring inconsistency in meta-analyses. BMJ, 2003; 327: 557-560
29) Staffa JA, Chang J, Green L: Cerivastatin and reports of fatal rhabdomyolysis. N Engl J Med, 2002; 346: 539-540
30) Higgins JP, Thompson SG: Controlling the risk of spuri-ous findings from meta-regression. Stat Med, 2004; 23: 1663-1682
31) Knapp G, Hartung J: Improved tests for a random effects meta-regression with a single covariate. Stat Med, 2003; 22: 2693-2710
32) Mercuri M, Bond MG, Sirtori CR, Veglia F, Crepaldi G, Feruglio FS, Descovich G, Ricci G, Rubba P, Mancini M, Gallus G, Bianchi G, D’Alo G, Ventura A: Pravastatin reduces carotid intima-media thickness progression in an asymptomatic hypercholesterolemic mediterranean popu-lation: the Carotid Atherosclerosis Italian Ultrasound Study. Am J Med, 1996; 101: 627-634
33) Salonen R, Nyssonen K, Porkkala-Sarataho E, Salonen JT: The Kuopio Atherosclerosis Prevention Study (KAPS): effect of pravastatin treatment on lipids, oxidation resis-tance of lipoproteins, and atherosclerotic progression. Am J Cardiol, 1995; 76: 34C-39C
34) Zanchetti A, Crepaldi G, Bond MG, Gallus G, Veglia F, Mancia G, Ventura A, Baggio G, Sampieri L, Rubba P, Sperti G, Magni A: Different effects of antihypertensive regimens based on fosinopril or hydrochlorothiazide with
Gans ROB, Smit AJ, Van Gilst WH: Effects of fosinopril and pravastatin on carotid intima-media thickness in sub-jects with increased albuminuria. Stroke, 2005; 36: 649-653
9) Reid JA, Wolsley C, Lau LL, Hannon RJ, Lee B, Young IS, Soong CV: The effect of pravastatin on intima media thickness of the carotid artery in patients with normal cholesterol. Eur J Vasc Endovasc Surg, 2005; 30: 464-468
10) Wu J, Wu G, Wang MP, Liu DL, Hu ZJ, Xu GY: Effect of atorvastatin on carotid intima-medial of thickness of pri-mary hypertension patients of Han nationality. Natl Med J China, 2007; 87: 2215-2218
11) Yokoyama H, Kawasaki M, Ito Y, Minatoguchi S, Fuji-wara H: Effects of fluvastatin on the carotid arterial media as assessed by integrated backscatter ultrasound compared with pulse-wave velocity. J Am Coll Cardiol, 2005; 46: 2031-2037
12) Zhang M, Zhang Y, Zhang W, Zhao YX, Gao YH, Zhang YY: [Study of diagnostic criteria of intima-media thicken-ing and effects of drugs on peripheral arteries]. Zhong Hua Yi Xue Za Zhi, 2004; 84: 1252-1256
13) de Groot E, Jukema JW, Montauban van Swijndregt AD, Zwinderman AH, Ackerstaff RG, van der Steen AF, Bom N, Lie KI, Bruschke AV: B-mode ultrasound assessment of pravastatin treatment effect on carotid and femoral artery walls and its correlations with coronary arterio-graphic findings: a report of the Regression Growth Eval-uation Statin Study (REGRESS). J Am Coll Cardiol, 1998; 31: 1561-1567
14) Amarenco P, Labreuche J, Lavallee P, Touboul PJ: Statins in stroke prevention and carotid atherosclerosis: system-atic review and up-to-date meta-analysis. Stroke, 2004; 35: 2902-2909
15) Kang S, Wu Y, Li X: Effects of statin therapy on the pro-gression of carotid atherosclerosis: a systematic review and meta-analysis. Atherosclerosis, 2004; 177: 433-442
16) Bedi US, Singh M, Singh PP, Bhuriya R, Bahekar A, Mol-nar J, Khosla S, Arora R: Effects of statins on progression of carotid atherosclerosis as measured by carotid intimal-medial thickness: a meta-analysis of randomized con-trolled trials. J Cardiovasc Pharmacol Ther, 2010; 15: 268-273
17) Anderssen SA, Hjelstuen AK, Hjermann I, Bjerkan K, Holme I: Fluvastatin and lifestyle modification for reduc-tion of carotid intima-media thickness and left ventricular mass progression in drug-treated hypertensives. Athero-sclerosis, 2005; 178: 387-397
18) Riegger G, Abletshauser C, Ludwig M, Schwandt P, Widimsky J, Weidinger G, Welzel D: The effect of fluvas-tatin on cardiac events in patients with symptomatic coro-nary artery disease during one year of treatment. Athero-sclerosis, 1999; 144: 263-270
19) Taylor AJ, Kent SM, Flaherty PJ, Coyle LC, Markwood TT, Vernalis MN: ARBITER: Arterial biology for the investigation of the treatment effects of reducing choles-terol: A randomized trial comparing the effects of atorvas-tatin and pravastatin on carotid intima medial thickness. Circulation, 2002; 106: 2055-2060
20) Smilde TJ, van Wissen S, Wollersheim H, Trip MD, Kastelein JJ, Stalenhoef AF: Effect of aggressive versus

119Statin Therapy and the Common Carotid Artery Intima-Media Thickness
without manifest cardiovascular disease. Diabetes Care, 2004; 27: 2887-2892
43) Peng HS, Sun CY, Lv HX: Efficacy of intervention with simvastatin and aspirin for carotid arteriosclerosis in patients with hypertension. Chinese Journal of Cerebro-vascular Diseases, 2006; 3: 15-18
44) Spring S, Simon R, van der Loo B, Kovacevic T, Brockes C, Rousson V, Amann-Vesti B, Koppensteiner R: High-dose atorvastatin in peripheral arterial disease (PAD): Effect on endothelial function, intima-media-thickness and local progression of PAD. An open randomized con-trolled pilot trial. Thromb Haemost, 2008; 99: 182-189
45) Takahashi T, Ishii N, Itai K, Goto R, Higashi K, Kobori S: HMG-CoA reductase inhibitors suppress the develop-ment and progression of carotid artery intimal-medial thickening in hypercholesterolemic type 2 diabetic patients. J Atheroscler Thromb, 2005; 12: 149-153
46) Ito Y, Kawasaki M, Yokoyama H, Okubo M, Sano K, Arai M, Nishigaki K, Uno Y, Takemura G, Minatoguchi S, Fujiwara H: Different effects of pravastatin and cerivas-tatin on the media of the carotid arteries as assessed by integrated backscatter ultrasound. Circulation Journal, 2004; 68: 784-790
47) Wiegman A, Hutten BA, de Groot E, Rodenburg J, Bak-ker HD, Büller HR, Sijbrands EJ, Kastelein JJ: Efficacy and safety of statin therapy in children with familial hypercholesterolemia: a randomized controlled trial. JAMA, 2004; 292: 331-337
48) Austin MA: Plasma triglyceride and coronary heart dis-ease. Arterioscler Thromb, 1991; 11: 2-14
49) Hulley SB, Rosenman RH, Bawol RD, Brand RJ: Epide-miology as a guide to clinical decisions. The association between triglyceride and coronary heart disease. N Engl J Med, 1980; 302: 1383-1389
50) Ginsberg HN: Is hypertriglyceridemia a risk factor for atherosclerotic cardiovascular disease ? A simple question with a complicated answer. Ann Intern Med, 1997; 126: 912-914
51) Byington RP, Evans GW, Espeland MA, Applegate WB, Hunninghake DB, Probstfield J, Furberg CD: Effects of lovastatin and warfarin on early carotid atherosclerosis: sex-specific analyses. Asymptomatic Carotid Artery Pro-gression Study (ACAPS) Research Group. Circulation, 1999; 100: e14-e17
or without lipid lowering by pravastatin on progression of asymptomatic carotid atherosclerosis: Principal results of PHYLLIS - A randomized double-blind trial. Stroke, 2004; 35: 2807-2812
35) Yamagami H, Sakaguchi M, Furukado S, Hoshi T, Abe Y, Hougaku H, Hori M, Kitagawa K: Statin therapy increases carotid plaque echogenicity in hypercholesterolemic patients. Ultrasound Med Biol, 2008; 34: 1353-1359
36) Watanabe K, Sugiyama S, Kugiyama K, Honda O, Fuku-shima H, Koga H, Horibata Y, Hirai T, Sakamoto T, Yoshimura M, Yamashita Y, Ogawa H: Stabilization of carotid atheroma assessed by quantitative ultrasound anal-ysis in nonhypercholesterolemic patients with coronary artery disease. J Am Coll Cardiol, 2005; 46: 2022-2030
37) Yamada K, Yoshimura S, Kawasaki M, Enomoto Y, Asano T, Minatoguchi S, Iwama T: Effects of atorvastatin on carotid atherosclerotic plaques: a randomized trial for quantitative tissue characterization of carotid atheroscle-rotic plaques with integrated backscatter ultrasound. Cerebrovasc Dis, 2009; 28: 417-424
38) Yu CM, Zhang Q, Lam L, Lin H, Kong SL, Chan W, Fung JW, Cheng KK, Chan IH, Lee SW, Sanderson JE, Lam CW: Comparison of intensive and low-dose atorvas-tatin therapy in the reduction of carotid intimal-medial thickness in patients with coronary heart disease. Heart, 2007; 93: 933-939
39) Nakamura T, Obata JE, Kitta Y, Takano H, Kobayashi T, Fujioka D, Saito Y, Kodama Y, Kawabata K, Mende A, Yano T, Hirano M, Sano K, Nakamura K, Kugiyama K: Rapid stabilization of vulnerable carotid plaque within 1 month of pitavastatin treatment in patients with acute coronary syndrome. J Cardiovasc Pharmacol, 2008; 51: 365-371
40) De Lorenzo F, Boffito M, Collot-Teixeira S, Gazzard B, McGregor JL, Shotliff K, Xiao H: Prevention of athero-sclerosis in patients living with HIV. Vasc Health Risk Manag, 2009; 5: 287-300
41) Probstfield JL, Margitic SE, Byington RP, Espeland MA, Furberg CD: Results of the primary outcome measure and clinical events from the Asymptomatic Carotid Artery Progression Study. Am J Cardiol, 1995; 76: 47c-53c
42) Beishuizen ED, van de Ree MA, Jukema JW, Tamsma JT, van der Vijver JC, Meinders AE, Putter H, Huisman MV: Two-year statin therapy does not alter the progression of intima-media thickness in patients with type 2 diabetes
120 Huang et al.
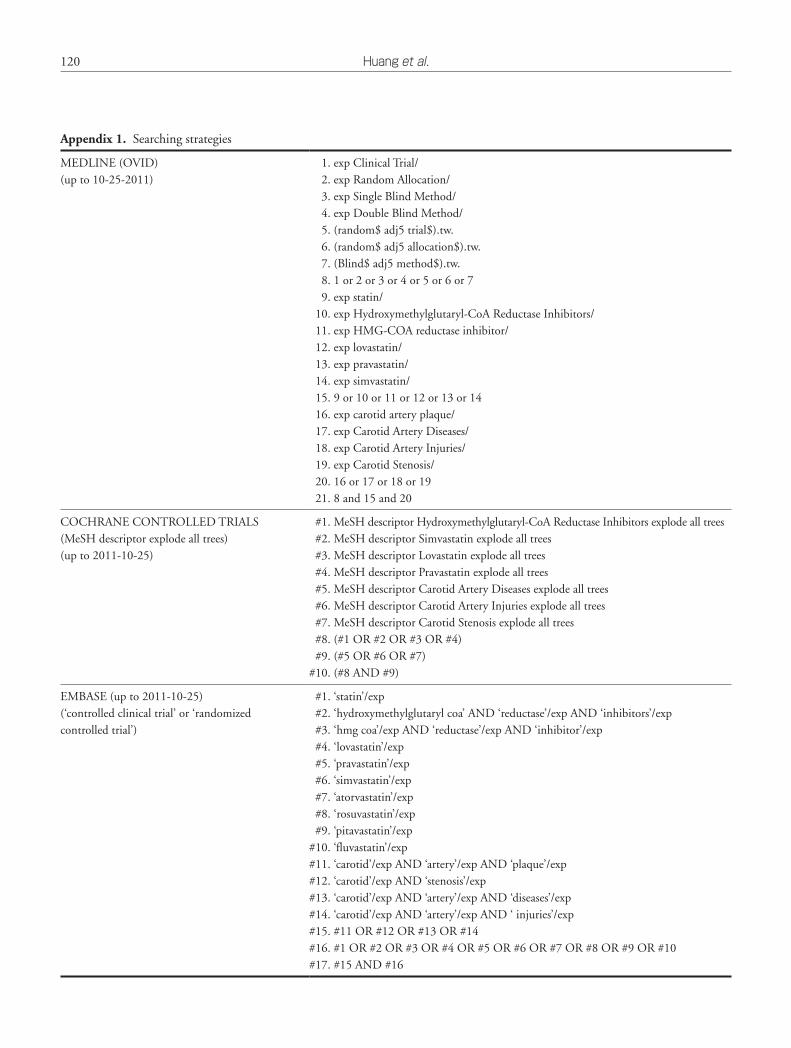
Appendix 1. Searching strategies
MEDLINE (OVID)(up to 10-25-2011)
1. exp Clinical Trial/2. exp Random Allocation/3. exp Single Blind Method/4. exp Double Blind Method/5. (random$ adj5 trial$).tw.6. (random$ adj5 allocation$).tw.7. (Blind$ adj5 method$).tw.8. 1 or 2 or 3 or 4 or 5 or 6 or 79. exp statin/
10. exp Hydroxymethylglutaryl-CoA Reductase Inhibitors/11. exp HMG-COA reductase inhibitor/12. exp lovastatin/13. exp pravastatin/14. exp simvastatin/15. 9 or 10 or 11 or 12 or 13 or 1416. exp carotid artery plaque/17. exp Carotid Artery Diseases/18. exp Carotid Artery Injuries/19. exp Carotid Stenosis/20. 16 or 17 or 18 or 1921. 8 and 15 and 20
COCHRANE CONTROLLED TRIALS(MeSH descriptor explode all trees)(up to 2011-10-25)
#1. MeSH descriptor Hydroxymethylglutaryl-CoA Reductase Inhibitors explode all trees#2. MeSH descriptor Simvastatin explode all trees#3. MeSH descriptor Lovastatin explode all trees#4. MeSH descriptor Pravastatin explode all trees#5. MeSH descriptor Carotid Artery Diseases explode all trees#6. MeSH descriptor Carotid Artery Injuries explode all trees#7. MeSH descriptor Carotid Stenosis explode all trees#8. (#1 OR #2 OR #3 OR #4)#9. (#5 OR #6 OR #7)
#10. (#8 AND #9)
EMBASE (up to 2011-10-25)(‘controlled clinical trial’ or ‘randomizedcontrolled trial’)
#1. ‘statin’/exp#2. ‘hydroxymethylglutaryl coa’ AND ‘reductase’/exp AND ‘inhibitors’/exp#3. ‘hmg coa’/exp AND ‘reductase’/exp AND ‘inhibitor’/exp#4. ‘lovastatin’/exp#5. ‘pravastatin’/exp#6. ‘simvastatin’/exp#7. ‘atorvastatin’/exp#8. ‘rosuvastatin’/exp#9. ‘pitavastatin’/exp
#10. ‘fluvastatin’/exp#11. ‘carotid’/exp AND ‘artery’/exp AND ‘plaque’/exp#12. ‘carotid’/exp AND ‘stenosis’/exp#13. ‘carotid’/exp AND ‘artery’/exp AND ‘diseases’/exp#14. ‘carotid’/exp AND ‘artery’/exp AND ‘ injuries’/exp#15. #11 OR #12 OR #13 OR #14#16. #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10#17. #15 AND #16
121Statin Therapy and the Common Carotid Artery Intima-Media Thickness
Appendix 2. Measurement of common carotid artery IMT in included trials
Trial, Year of Publication
Measurement of common carotid artery IMT
ACAPS, 1994
B-mode ultrasound with a 10-MHz transducer was used to measure mean IMT, proximal and distal, to the common carotid, the bifurcation, and the internal carotid arteries on both sides of the neck.
Bae, 2004
B-mode ultrasound (Hewlett-Packard Sonos 5500) with a 7.5 MHz probe was used to measure left common carotid artery IMT using M’ATH software.
BCAPS, 2001
B-mode ultrasound (Acuson 128) with a 7-MHz transducer was used to measure mean IMT in the common carotid artery (10-mm-long section) and maximum IMT in the carotid bulb.
Beishuizen, 2004
B-mode ultrasound (Acuson Aspen) with a linear array 7.5-MHz probe was used to measure IMT 1.0 cm distal to the common carotid artery, the carotid bifurcation, and 1.0 cm proximal to the internal carotid artery.
FAST, 2002
B-mode ultrasound (Aloka SSD-2000) with a 7.5-MHz transducer was used to measure IMT 2, 2.5 and 3 cm proximal to the carotid bifurcation in each of the right and left common carotid arteries.
HYRIM, 2004
B-mode ultrasound (Acuson 128) with a 7-MHz transducer was used to measure mean IMT at the right carotid artery from 30mm proximal to 10mm distal to the bifurcation, including the common carotid artery (CCA), the bifurcation, and interna and externa
LIPID, 1998
B-mode ultrasound (ATL UM-8) with a 10-MHz transducer was used to measure IMT; three views of the right distal common carotid artery were collected.
LiSA, 1999
B-mode ultrasound (7.5 MHz) was used to measure IMT located in the common 10 mm distal to the bifurcation, and in the interna and externa 10 mm proximal to the bifurcation, both left and right sides.
MARS, 1993
B-mode ultrasound (Diasonics CV400) with a 7.5-MHz probe (Diasonics, Milpitas, California) was used to measure IMT at the proximal and distal walls of the right distal common carotid artery.
METEOR, 2007
B-mode ultrasound was used to measure common carotid artery IMT in the segment extending from 10 to 20 mm proximal to the tip of the flow divider.
Peng, 2006
B-mode ultrasound (Acuson Aspen) with a linear array 7.5-MHz probe was used to measure IMT at the carotid bifurcation, and the proximal 1.0-1.5 cm of the internal carotid artery.
PREVEND IT, 2005
B-mode ultrasound (Pie Medical Scanner 200) with a linear array 7.5-MHz transducer was used to measure IMT at the posterior wall of the left common carotid artery 1 cm proximal to the bulbus at 3 different positions.
REGRESS, 1998
B-mode ultrasound (Acuson 128) with a linear array 7.0-MHz transducer was used to measure IMT at the carotid bulb (carotid dilation and carotid flow divider) and internal carotid artery (1 cm proximal to the carotid dilation), right and left.
Reid, 2005
B-mode ultrasound (ATL5000) with a linear array 7.0-MHz transducer was used to measure IMT at the carotid artery bifurcation, 2 cm lengths of the distal common carotid artery, right and left.
Spring, 2008 B-mode ultrasound with a linear array 7.5-MHz transducer was used to measure IMT at the right brachial artery.
Takahashi, 2005-1
B-mode ultrasound (Powerversion SSA-370A) with a 7.5-MHz transducer was used to measure IMT at the bifurcation far wall of both common carotid arteries.
Wiegman, 2004
B-mode ultrasound (Acuson 128) with a 5-10-MHz transducer was used to measure IMT at left and right far walls of the common carotid arteries.
Wu, 2007-1
B-mode ultrasound (EUB-6500) with a 10-MHz transducer was used to measure IMT 3 cm proximal to the carotid bifurcation 6 times.
Zhang, 2004
B-mode ultrasound (SONOS-5500) with a 4-10-MHz transducer was used to measure IMT at the common carotid, internal carotid arteries, the bifurcation, and 2 cm proximal to the carotid bifurcation.
Ito, 2004-1
B-mode ultrasound (SONOS-5500) with a 5-12-MHz transducer was used to measure IMT in the middle of the bilateral common carotid arteries and the bifurcation of the external carotid artery and internal carotid artery.
Yokoyama, 2005
B-mode ultrasound (SONOS-5500) with a 5-12-MHz transducer was used to measure IMT in the middle of the right common carotid arteries and bifurcation of the external carotid artery and the internal carotid artery.


















