Effect of Pre-LVAD PVR on Heart Transplant...
18
Effect of Pre-LVAD PVR on Heart Transplant Outcome Masaki Tsukashita, MD, PhD, Hiroo Takayama, MD, PhD, Koji Takeda, MD, PhD, Jiho Han, BS, Sowmyashree Sreekanth, BS, Lauren Truby, BS, Paolo C. Colombo, MD, Melana Yuzefpolskaya, MD, Veli K. Topkara, MD, Arthur Reshad Garan, MD, Donna M. Mancini, MD, Paul A. Kurlansky, MD, Yoshifumi Naka, MD, PhD Columbia University Medical Center Columbia University Medical Center Division of Cardiothoracic Surgery AATS 2015, VAD/ECMO Session
Transcript of Effect of Pre-LVAD PVR on Heart Transplant...

Effect of Pre-LVAD PVR on Heart Transplant Outcome
Masaki Tsukashita, MD, PhD, Hiroo Takayama, MD, PhD, Koji Takeda, MD, PhD,
Jiho Han, BS, Sowmyashree Sreekanth, BS, Lauren Truby, BS, Paolo C.
Colombo, MD, Melana Yuzefpolskaya, MD, Veli K. Topkara, MD, Arthur Reshad
Garan, MD, Donna M. Mancini, MD, Paul A. Kurlansky, MD, Yoshifumi Naka, MD,
PhD
Columbia University Medical Center
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
AATS 2015, VAD/ECMO Session

DISCLOSURE
Y. Naka has received consulting fees from Thoratec Corp. The
remaining authors have no conflicts of interest to disclose.

BACKGROUND
Fixed pulmonary hypertension (pHTN) is often considered a
contraindication to orthotopic heart transplantation (OHT).
Two-thirds of transplant candidates present with pHTN at the
time of OHT evaluation.
Several previous studies have demonstrated LVAD implantation
decreased PVR and rendered patients with pHTN eligible for
OHT.
These were mostly small studies varying in types of LVAD
devices used (pulsatile or continuous-flow [CF]).
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
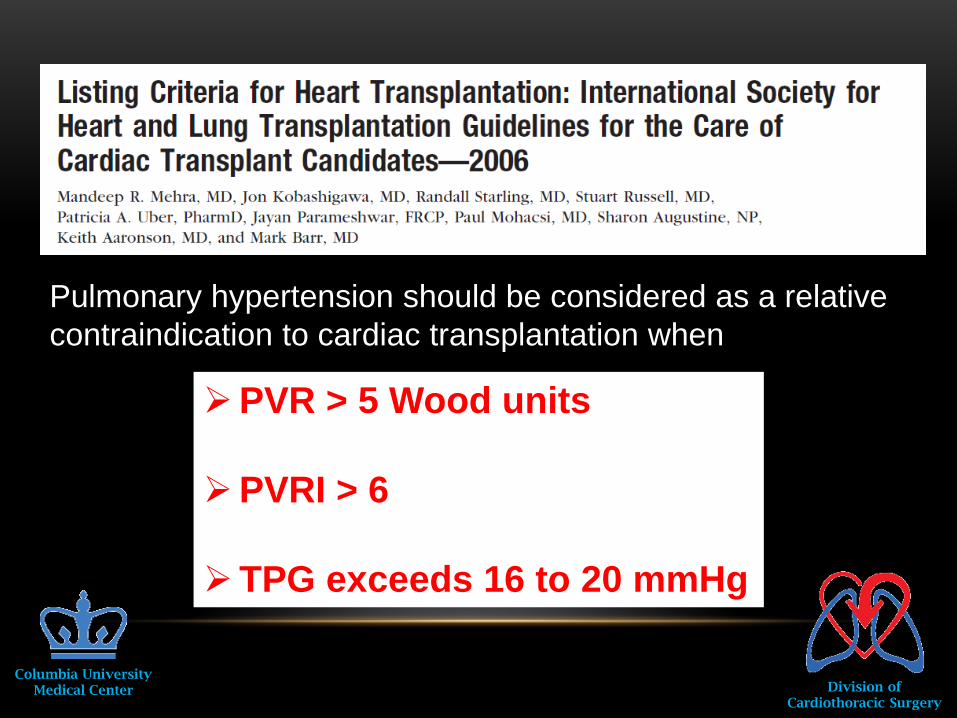
Pulmonary hypertension should be considered as a relative
contraindication to cardiac transplantation when
PVR > 5 Wood units
PVRI > 6
TPG exceeds 16 to 20 mmHg

PURPOSE
Investigate the effect of CF-LVAD support on
pHTN
Analyze OHT outcomes in LVAD patients with
pre-existing elevated PVR.
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
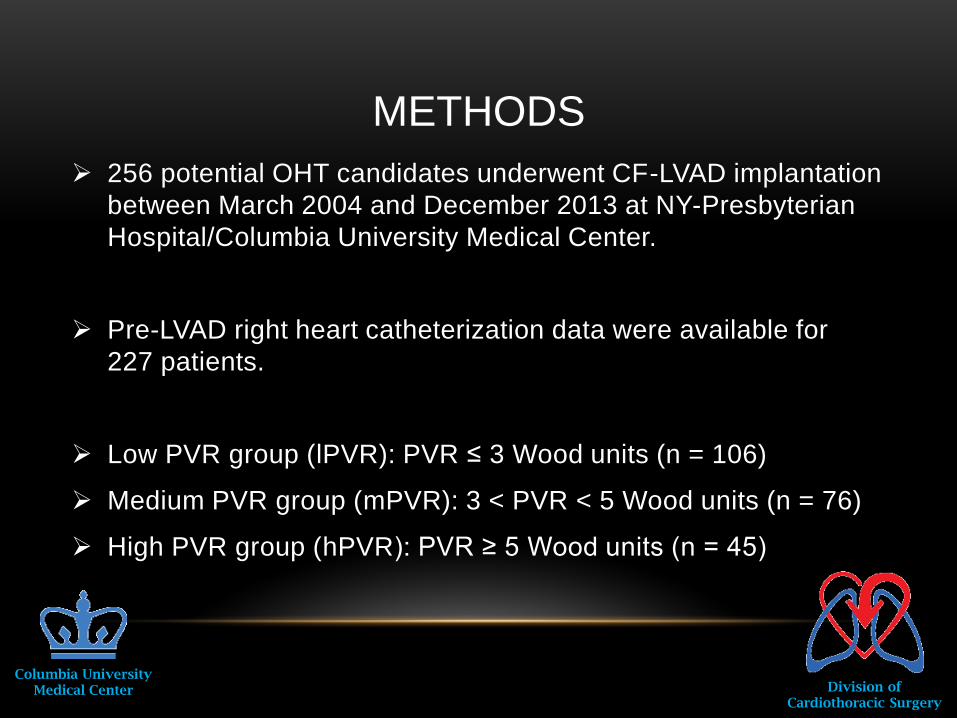
256 potential OHT candidates underwent CF-LVAD implantation
between March 2004 and December 2013 at NY-Presbyterian
Hospital/Columbia University Medical Center.
Pre-LVAD right heart catheterization data were available for
227 patients.
Low PVR group (lPVR): PVR ≤ 3 Wood units (n = 106)
Medium PVR group (mPVR): 3 < PVR < 5 Wood units (n = 76)
High PVR group (hPVR): PVR ≥ 5 Wood units (n = 45)
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
METHODS

Pre-LVAD patient characteristics
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
Variables All patients lPVR mPVR hPVR p value
Basic patient characteristics
Patients (n) 227 106 76 45
Age (years) 53.4 ± 12.5 51.7 ± 13.3 55.5 ± 11.1 53.8 ± 12.3 0.29
Female sex 41 (18.1%) 15 (14.2%) 13 (17.1%) 13 (28.9%) 0.09
BSA 1.97 ± 0.3 1.99 ± 0.26 1.99 ± 0.26 1.87 ± 0.25 0.02
Etiology of HF
ICM 83 (36.6%) 38 (35.9%) 30 (39.5%) 15 (33.3%)
0.71DCM 129 (56.8%) 62 (58.5%) 42 (55.3%) 25 (55.6%)
others 15 (6.6%) 6 (5.7%) 4 (5.3%) 5 (11.1%)

Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
Variables All patients lPVR mPVR hPVR p value
Preop MCS 22 (9.7%) 15 (14.2%) 3 (4.0%) 4 (8.9%) 0.07
Preop IABP 58 (25.6%) 31 (29.3%) 17 (22.4%) 10 (22.2%) 0.49
Previous cardiac
surgery
42 (18.5%) 15 (14.2%) 14 (18.4%) 13 (28.9%) 0.10
CABG 34 (15.0%) 11 (10.4%) 16 (21.1%) 7 (15.6%) 0.14
Mitral valve 13 (5.7%) 3 (2.8%) 3 (4.0%) 7 (15.6%) 0.006
Tricuspid valve 3 (1.3%) 0 (0.0%) 0 (0.0%) 3 (6.7%) 0.002
Aortic valve 4 (1.8%) 2 (1.9%) 2 (2.6%) 0 (0.0%) 0.6
Congenital 2 (0.90%) 1 (0.9%) 0 (0.0%) 1 (2.2%) 0.45

Variables All patients lPVR mPVR hPVR p value
LVEF (%) 15.2 ± 6.1 14.7 ± 5.5 15.8 ± 7.2 15.2 ± 5.2 0.7
Mean PAP
(mmHg)
36.2 ± 10.4 31.9 ± 8.9 38.5 ± 9.8 42.3 ± 10.4 0.0001
PCWP (mmHg) 24.1 ± 8.5 24.0 ± 8.5 24.8 ± 8.9 23.0 ± 7.9 0.82
TPG (mmHg) 12.1 ± 6.5 7.98 ± 3.80 13.5 ± 5.2 19.2 ± 6.4 0.0001
C.O. (L/min) 3.30 ± 1.02 3.71 ± 0.99 3.17 ± 0.89 2.57 ± 0.83 0.0001
PVR (WU) 3.59 ± 2.23 1.91 ± 0.63 3.86 ± 0.55 7.13 ± 2.09 0.0001
Hemodynamic Data

DEVICE TYPES
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
total lPVR mPVR hPVR
Jarvik 2000
Dura Heart
DeBakey
Ventrassist
HeartWare
HeartMate II
p=0.03
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery

Kaplan-Meier survival curve during LVAD support
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
p=0.24

Changes over time in pulmonary vascular resistance
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
0
1
2
3
4
5
6
7
8
9
10
Pre-LVAD Post-LVAD OHT 1y OHT 5y
PV
R (
Wo
od
un
its)
lPVR
mPVR
hPVR

Donor/recipient data for OHT
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
Variables All patients
(n = 148)
lPVR
(n = 72)
mPVR
(n = 47)
hPVR
(n = 29)
p value
Donor data
Age (year) 29.4 ± 9.2 28.2 ± 9.7 31.0 ± 8.2 30.4 ± 9.6 0.33
ABO identical 89.1% 88.9% 89.1% 89.7% 0.99
ABO compatible 10.9% 11.1% 10.9% 10.3%
Donor/recipient
weight
0.99 ± 0.17 0.98 ± 0.17 0.99 ± 0.15 1.03 ± 0.18 0.36
Recipient data
LVAD support
duration (days)
345 ± 343 328 ± 309 358 ± 372 362 ± 379 0.89

Intra- and postoperative data for OHT
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
Variables All patients
(n = 148)
lPVR
(n = 72)
mPVR
(n = 47)
hPVR
(n = 29)
p value
Intraoperative data
CPB time (min) 176 ± 54 175 ± 50 173 ± 43 184 ± 75 0.94
Ischemic time (min) 189 ± 51 187 ± 53 189 ± 46 195 ± 52 0.88
Postoperative data
iNO usage 49 (33.6%) 25 (35.2%) 12 (25.5%) 12 (42.9%) 0.28
In-hosp mortality 13 (8.8%) 5 (6.9%) 2 (4.3%) 6 (20.7%) 0.036
HD/CVVH 24 (16.4%) 8 (11.3%) 11 (23.9%) 5 (17.2%) 0.20
Primary graft failure 12 (8.2%) 7 (9.9%) 1 (2.2%) 4 (13.8%) 0.16
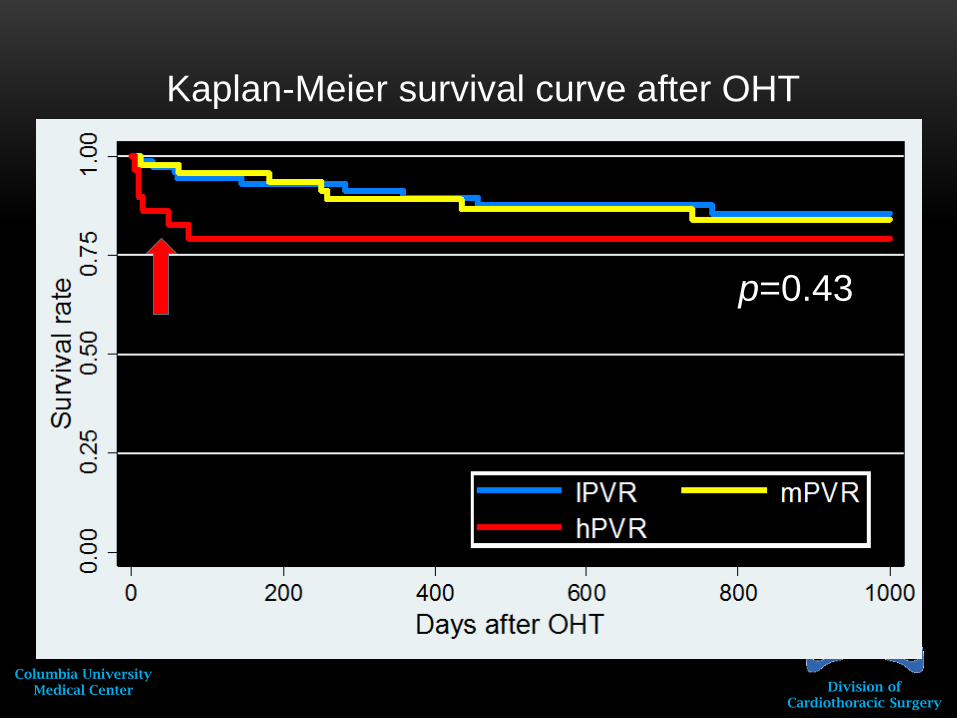
Kaplan-Meier survival curve after OHT
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
p=0.43
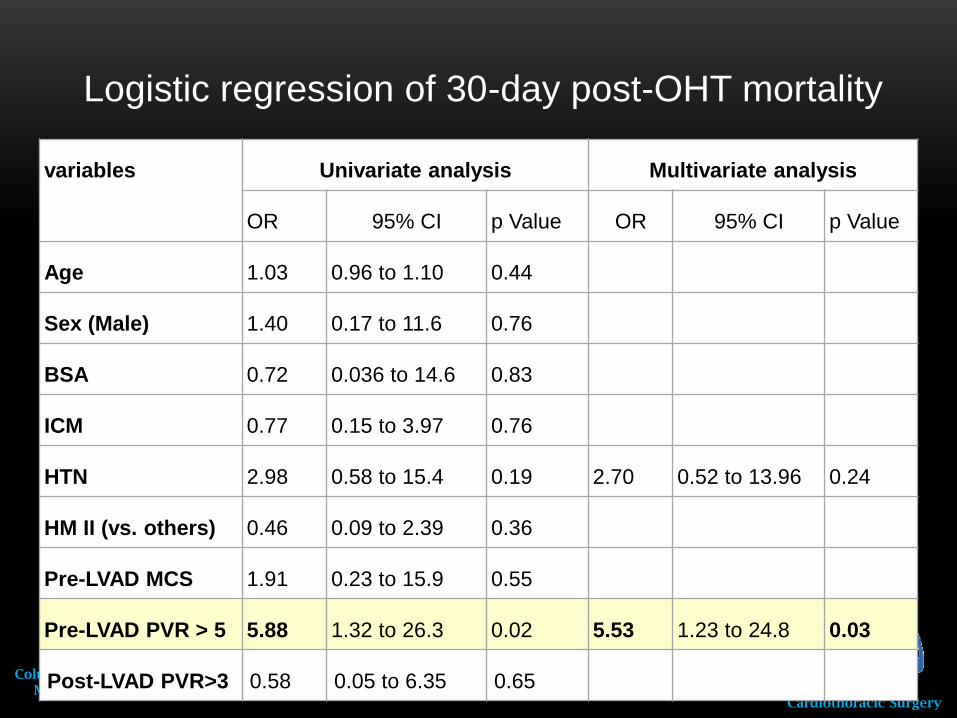
Logistic regression of 30-day post-OHT mortality
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
variables Univariate analysis Multivariate analysis
OR 95% CI p Value OR 95% CI p Value
Age 1.03 0.96 to 1.10 0.44
Sex (Male) 1.40 0.17 to 11.6 0.76
BSA 0.72 0.036 to 14.6 0.83
ICM 0.77 0.15 to 3.97 0.76
HTN 2.98 0.58 to 15.4 0.19 2.70 0.52 to 13.96 0.24
HM II (vs. others) 0.46 0.09 to 2.39 0.36
Pre-LVAD MCS 1.91 0.23 to 15.9 0.55
Pre-LVAD PVR > 5 5.88 1.32 to 26.3 0.02 5.53 1.23 to 24.8 0.03
Post-LVAD PVR>3 0.58 0.05 to 6.35 0.65
CONCLUSION
Columbia UniversityMedical Center Division of
Cardiothoracic Surgery
LVAD therapy significantly reduced PVR even in patients
with severely elevated PVR.
Early post-OHT mortality in LVAD patients with pre-
existing high PVR was high.
However, their long-term survival appeared comparable
to that for patients with lower PVR.

Columbia UniversityMedical Center
Division ofCardiothoracic Surgery