Effect of distraction on simulated anterior segment surgical performance
6
Effect of distraction on simulated anterior segment surgical performance Jonathan Park, MBChb, BSc, Salman Waqar, MRCSEd, BSc, Thomas Kersey, MRCOphth, Neil Modi, MBChb, Chin Ong, MRCOphth, Tamsin Sleep, FRCOphth, MA PURPOSE: To determine the effect of distraction on anterior segment surgical performance using a virtual reality simulator in expert and novice surgeons. SETTING: Horizon Suite Simulation Centre, South Devon Foundation NHS Trust, Devon, England. DESIGN: Cohort study. METHODS: Expert and novice ophthalmic surgeons completed a standardized and validated surgical task 10 times on a virtual reality simulator (EyeSi). They then completed a cognitive task (arithmetic questions), after which they completed 10 attempts on the simulator module while also completing the cognitive task. RESULTS: For experts (n Z 7), the distracting cognitive task had no statistically significant effect on operating scores. The rate of correctly answered questions decreased from 12.3 per minute G 2.1 (SD) while single tasking to 8.6 G 3.1 per minute while dual tasking (PZ.018). For novices (n Z 14), the distracting cognitive task had no effect on any operating score except a small reduc- tion in the penalty odometer score. The rate of correctly answered questions decreased from 11.5 G 4.1 per minute while single tasking to 7.0 G 3.2 per minute while dual tasking (PZ.001). CONCLUSION: A distractive cognitive task reduced the ability of novice surgeons and expert surgeons to deal with that cognitive task, although their simulated surgical performance was not overtly compromised. Financial Disclosure: No author has a financial or proprietary interest in any material or method mentioned. J Cataract Refract Surg 2011; 37:1517–1522 Q 2011 ASCRS and ESCRS It is not uncommon for surgeons to be distracted while operating. The degree and frequency of distraction de- pends on multiple factors including the presence of trainees, the operating room environment, and exter- nal factors, such as regional on-call responsibilities. In general surgery, operating surgeons are interrupted on average more than 10 times per case, including calls from the ward or emergency department, pagers, door opening, and conversations not pertinent to the surgi- cal case. 1 Distractions for the operating surgeon are cognitive in nature. This requires surgeons to dual-task because they not only continue their psychomotor surgical task (the operation) but also simultaneously respond to a cognitive task (the distraction). It is important to con- sider the ability of surgeons to perform both the surgi- cal task and the cognitive task when distracted while operating because both are likely to be of importance and should receive a competent response. The effect of distraction on surgical performance and the ability to deal with the distraction are poorly understood because it is a variable that is potentially unsafe to evaluate in a real operating environment. The distractive effect has, however, been investigated using virtual reality simulators for laparoscopic sur- gery; no detrimental effect on surgical performance was observed after distractions consisting of noise and music. 2 In contrast, laparoscopic surgical simula- tor studies have shown that more complex cognitive tasks can increase the duration of operating 3 and can have detrimental effects on the ability to deal with the surgical and cognitive tasks, depending on the experience of the operating surgeon. 4 The aim of this study was to determine the effect of distraction on anterior segment surgical performance using a virtual reality simulator in both expert and novice surgeons. To our knowledge, this is the first study to consider the effect of distraction on the ability Q 2011 ASCRS and ESCRS Published by Elsevier Inc. 0886-3350/$ - see front matter 1517 doi:10.1016/j.jcrs.2011.01.031 ARTICLE
-
Upload
jonathan-park -
Category
Documents
-
view
214 -
download
0
Transcript of Effect of distraction on simulated anterior segment surgical performance

ARTICLE
Effect of distraction
on simulated anteriorsegment surgical performanceJonathan Park, MBChb, BSc, Salman Waqar, MRCSEd, BSc, Thomas Kersey, MRCOphth,Neil Modi, MBChb, Chin Ong, MRCOphth, Tamsin Sleep, FRCOphth, MA
Q 2011 A
Published
SCRS an
by Elsev
PURPOSE: To determine the effect of distraction on anterior segment surgical performance usinga virtual reality simulator in expert and novice surgeons.
SETTING: Horizon Suite Simulation Centre, South Devon Foundation NHS Trust, Devon, England.
DESIGN: Cohort study.
METHODS: Expert and novice ophthalmic surgeons completed a standardized and validatedsurgical task 10 times on a virtual reality simulator (EyeSi). They then completed a cognitivetask (arithmetic questions), after which they completed 10 attempts on the simulator modulewhile also completing the cognitive task.
RESULTS: For experts (n Z 7), the distracting cognitive task had no statistically significant effecton operating scores. The rate of correctly answered questions decreased from 12.3 per minuteG 2.1 (SD) while single tasking to 8.6G 3.1 per minute while dual tasking (PZ.018). For novices(nZ 14), the distracting cognitive task had no effect on any operating score except a small reduc-tion in the penalty odometer score. The rate of correctly answered questions decreased from 11.5G 4.1 per minute while single tasking to 7.0 G 3.2 per minute while dual tasking (PZ.001).
CONCLUSION: A distractive cognitive task reduced the ability of novice surgeons and expertsurgeons to deal with that cognitive task, although their simulated surgical performance was notovertly compromised.
Financial Disclosure: No author has a financial or proprietary interest in any material or methodmentioned.
J Cataract Refract Surg 2011; 37:1517–1522 Q 2011 ASCRS and ESCRS
It is not uncommon for surgeons to be distracted whileoperating. The degree and frequency of distraction de-pends on multiple factors including the presence oftrainees, the operating room environment, and exter-nal factors, such as regional on-call responsibilities.In general surgery, operating surgeons are interruptedon averagemore than 10 times per case, including callsfrom the ward or emergency department, pagers, dooropening, and conversations not pertinent to the surgi-cal case.1
Distractions for the operating surgeon are cognitivein nature. This requires surgeons to dual-task becausethey not only continue their psychomotor surgical task(the operation) but also simultaneously respond toa cognitive task (the distraction). It is important to con-sider the ability of surgeons to perform both the surgi-cal task and the cognitive task when distracted whileoperating because both are likely to be of importanceand should receive a competent response.
d ESCRS
ier Inc.
The effect of distraction on surgical performanceand the ability to deal with the distraction are poorlyunderstood because it is a variable that is potentiallyunsafe to evaluate in a real operating environment.The distractive effect has, however, been investigatedusing virtual reality simulators for laparoscopic sur-gery; no detrimental effect on surgical performancewas observed after distractions consisting of noiseand music.2 In contrast, laparoscopic surgical simula-tor studies have shown that more complex cognitivetasks can increase the duration of operating3 and canhave detrimental effects on the ability to deal withthe surgical and cognitive tasks, depending on theexperience of the operating surgeon.4
The aim of this study was to determine the effect ofdistraction on anterior segment surgical performanceusing a virtual reality simulator in both expert andnovice surgeons. To our knowledge, this is the firststudy to consider the effect of distraction on the ability
0886-3350/$ - see front matter 1517doi:10.1016/j.jcrs.2011.01.031

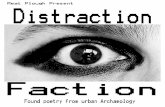
Figure 1. The intraocular surgical simulator. Note the phacoemulsi-fication and microscope pedals, instructor screen, head prop withelectronic eye, and viewing microscope on an adjustable platform.
1518 EFFECT OF DISTRACTION ON SURGICAL PERFORMANCE
of ophthalmic surgeons to manage both an intraocularsurgical task and a distracting cognitive task usinga virtual reality simulator. The use of intraocular sim-ulators is growing among training centers in theUnited Kingdom.
SUBJECTS AND METHODS
This study used the EyeSi virtual reality cataract surgerysimulator (VRmagic, Inc.) to measure intraocular surgicalperformance (Figure 1). The simulator comprises a manne-quin head with an eye that rotates and pivots when manip-ulated by the surgeon. Probes inserted into the eye simulatedifferent intraocular instruments with appropriate visualfeedback. The microscope provides stereoscopic imagesthat can be manipulated like a real operating room micro-scope using a footpedal.
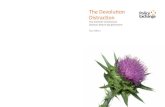
The simulator allows repeated measurements of a stan-dardized surgical task and provides feedback to the userin the following categories: surgeon efficiency, achievementof surgical goal, and tissue injury.A During the task, writ-ten prompts appear to give basic guidance after a surgicalerror (such as, “Do not rotate the eye”). The module usedfor this study was the forceps module, level 4 (Figure 2),because it has shown construct validity.5 The surgeon is re-quired to grasp 6 triangular objects from the periphery ofthe anterior chamber and place them in a net in the centerof the anterior chamber. This module was designed toteach surgeons how to accurately grasp the edge of a capsu-lorhexis flap while keeping the eye in the primary positionto maintain the red reflex and avoiding injury to the corneaor lens.
Local research and ethical committee approval was ob-tained, and all subjects gave their written informed consentto participate in the study.
The expert surgeons in this study were classified assurgeons who had completed more than the 350 phaco-emulsification procedures that the Royal College of
Submitted: December 21, 2010.Final revision submitted: January 29, 2011.Accepted: January 31, 2011.
From the Ophthalmology Department, South Devon FoundationNHS Trust, Torbay, Devon, United Kingdom.
Mr. Park and Mr. Waqar contributed equally to this study.
Rod Taylor, PhD, professor of health services research and scien-tific director of the Peninsula Clinical Trials Unit, Peninsula MedicalSchool, Universities of Exeter and Plymouth, Exeter, United King-dom, and Ophthalmology Department, South Devon FoundationNHS Trust, Torbay, Devon, United Kingdom, helped with the statis-tical analysis.
Presented at the Symposia on Leading Advances in Ophthalmology,Bristol Eye Hospital Bicentenary Meeting, Bristol, England, June2010, and the 15th European Society of Cataract & RefractiveSurgeons Winter Meeting, Istanbul, Turkey, February 2011.
Corresponding author: JonathanPark,MBChb, BSc, OphthalmologyDepartment, South Devon Foundation NHS Trust, Torbay, Devon,TQ2 7AA, United Kingdom. E-mail: [email protected].
J CATARACT REFRACT SURG -
Ophthalmologists requires as the minimum criteria for com-pletion of training.6 The novice surgeons were classified asphysicians or student physicians who had not performed in-traocular surgery before.
Each surgeon received a standardized orientation to thesimulator with 2 practice sessions (level 1 and level 2 forcepsmodule), similar to previously reported validity studies.7
Scores for these sessions were not recorded. All surgeonsthen completed 10 attempts on the level 4 forceps module,and a mean plateau score was calculated for various surgicalparameters (total score, total time, lens injury, corneal injury,odometer score, operatingwithout red reflex score). This pla-teau score was the mean of the final 4 attempts and wasa practical attempt to reduce the effect of the steeper partof the performance curve (where initially with practice per-formance improves and then settles to a plateau) while pre-venting excessive practice that would result in fatigue. Theseattempts were completed with no distraction (single task-ing). The surgical parameters recorded allowed an overallforceps module score to be calculated automatically by thesoftware using the following formula: Forceps module totalscoreZ number remaining objects (0Z 100 points)� exces-sive task time score� corneal injury score� lens injury score� odometer score (measuring distance traveled by instru-ments in the anterior chamber) � operating without red re-flex score � interacting out of focus score � nonhorizontalinsertion/removal of instruments score.
VOL 37, AUGUST 2011

Figure 2. The anterior segment forceps module, level 4. Note thetriangular objects in the peripheral anterior chamber that have tobe grasped with the forceps and placed in a central net.
Table 1. Characteristics of surgeons.
Characteristic Expert Surgeons Novice Surgeons
Surgeons (n) 7 14Mean age (y) 47 22Intraocular surgicalexperience (y)
20.3 0
Real phacoprocedures (n)
3800 0
Table 2. Results for expert surgeons when single tasking (notdistracted) and dual tasking (distracted).
Parameter Single Tasking Dual Tasking P Value
Total scoreMean G SD 97.3 G 2.3 95.9 G 3.84 .17695% CI 95.6, 98.9 93.0, 98.7
Total rime (s)Mean G SD 44 G 12 49 G 14 .06395% CI 36, 52 39, 59
Lens injury scoreMean G SD �0.013 G 0.031 �0.017 G 0.029 .89395% CI �0.033, �0.009 �0.031, �0.003
Odometer scoreMean G SD �1.78 G 4.56 �0.37 G 0.52 1.000
1519EFFECT OF DISTRACTION ON SURGICAL PERFORMANCE
The subjects then completed a cognitive task while notoperating that involved answering arithmetic questions ofmoderate difficulty. The numbers were randomly generated,and the sum typically involved carrying a digit (for example,7 C 5); this method has been used as a distractive cognitivetask in other studies.4 The task lasted 2minutes, and the totalnumber of questions and number of correct answers permin-ute were calculated.
The surgeons then performed 10 further attempts on thelevel 4 forceps module, but this time they were distractedby the arithmetic cognitive task (dual tasking). They were in-formed that the surgical task and cognitive task were ofequal importance. A mean plateau score for this dual-tasking session was recorded for the same surgical parame-ters as described above, and similarly, the total number ofquestions and correct answers per minute were recordedwhile dual tasking.
Data tests of normality (histograms and Q-Q plots) wereapplied to determine data distribution. Parametric testing(paired t) was used for normally distributed data and non-parametric testing (Wilcoxon signed rank) for skewed data.Multiple comparison corrections were not required due tothe small sample size. A P value less than 0.05 was consid-ered statistically significant. All data were analyzed usingSPSS software (SPSS, Inc.).
95% CI �5.15, �1.59 �0.75, 0.02Operating withoutred reflex scoreMean G SD �0.77 G 0.59 �0.43 G 0.46 .24995% CI �1.20, �0.34 �0.73, �0.14
Correct answers(per min)Mean G SD 12.3 G 2.1 8.6 G 3.1 .01895% CI 10.8, 13.8 6.2, 10.9
CI Z confidence interval
RESULTS
Table 1 shows the characteristics of the 7 expert sur-geons and 14 novice surgeons recruited into the study.Table 2 and Table 3 show the results of the expert sur-geons and novice surgeons, respectively, when singletasking (no distraction) and dual tasking (with distrac-tion). The scores for corneal injury are not shown inTable 2 because at no point did the expert surgeonsinjure the cornea.
J CATARACT REFRACT SURG -
For expert surgeons, for all the surgical parametersrecorded, there was no statistically significant differ-ence in the operating scores between single tasking(no distraction) and dual tasking (with distraction).The rate of correctly answered questions was statisti-cally significantly lower when dual tasking thanwhen single tasking (PZ.018).
For novices, the distracting cognitive task had no ef-fect on any operating score except a small reduction inthe penalty odometer score (PZ.028). The rate of cor-rectly answered questions was statistically signifi-cantly lower when dual tasking than when singletasking (PZ.001).
The difference in the mean decrease in the numberof correct questions answered per minute was notstatistically significant between experts and novices(3.7 versus 4.5; PZ.317).
VOL 37, AUGUST 2011

Table 3. Results for novice surgeons when single tasking (notdistracted) and dual tasking (distracted).
Parameter Single Tasking Dual Tasking P Value
Total scoreMean G SD 68.9 G18.9 75.9 G 12.0 .05695% CI 58.9, 78.8 70.0, 82.2
Total time (s)Mean G SD 84 G 34 71 G 25 .06095% CI 67, 101 59, 84
Lens injury scoreMean G SD �0.9 G 1.1 �0.6 G 0.6 .30095% CI �1.5, �0.4 �0.9, �0.2
Corneal injury scoreMean G SD �6.0 G 9.0 �2.9 G 5.2 .05095% CI �10.7, �1.3 �5.6, �0.2
Odometer scoreMean G SD �14.0 G 7.4 �11.6 G 6.9 .02895% CI �17.9, �10.2 �15.1, �8.0
Operating withoutred reflex score
Mean G SD �4.5 G 5.5 �4.6 G 5.8 .73095% CI �7.3, �1.6 �7.7, �1.5
Correct answers(per min)
Mean G SD 11.5 G 4.1 7.0 G 3.2 .00195% CI 9.3, 13.6 5.3, 8.6
CI Z confidence interval
1520 EFFECT OF DISTRACTION ON SURGICAL PERFORMANCE
DISCUSSION
This study shows that a distractive cognitive task willreduce the ability of expert and novice surgeons todeal with that cognitive task, although their intraocu-lar simulated surgical performance will not be overtlycompromised. To our knowledge, this is the first studyto attempt to evaluate the effect of distraction on intra-ocular surgery.
The forceps module task was chosen because at thetime of this study, it was the only module to show con-struct validity.5 Recently, the capsulorhexis modulehas also been validated,7 suggesting that this simula-tor, which is becoming increasingly popular in oph-thalmic training departments, is quite realistic.
If this observed effect for a validated simulator task istransferred to a real-life operating session, it followsthat surgeons should ensure their operating room ses-sions are distraction free and that cognitive tasks aregiven appropriate attention at another time. For exam-ple, trainees should perhaps store questions that cometo their mind while observing operations and then askthe questions at the end of the operating list because thereply from their trainer is likely to be less than idealwhile they continue to operate. Similarly, cognitivetasks demanded of the surgeon from other sources,such as advice relating to other patients or
J CATARACT REFRACT SURG -
administrative issues, should be dealt with after theoperating session; if urgent, they should be dealt withby somebody else remote from the operating session.
It is not practical to expect all distractions to be re-moved from an operating theater, so it is reassuringthat our findings suggest that expert surgeons arecapable of maintaining a high level of surgical perfor-mance despite distraction. However, because the abil-ity of the operating surgeon to respond to a cognitivetask while operating is reduced, this study providesevidence that clinicians should attempt to ensurethat their surgery-room environment is free fromunnecessary distractions.
In agreement with other simulator studies,laparoscopic-simulated surgery studies4 found thatcognitive distractive tasks do not reduce the surgicalperformance of expert surgeons. However, such dis-traction can reduce the surgical performance in novicesurgeons on laparoscopic simulators,4 so the degree ofsurgical experience is likely to be relevant. Experimen-tal psychology studies suggest that a slowing of per-formance, known as the psychological refractoryperiod, exists in most dual-task situations.8,9 It hasbeen suggested that experience with a task can resultin automatism, in which the task is performed withrelatively little effort; thus, a distracting task maynot necessarily have a detrimental effect on the pri-mary task because the manifestation of psychologicalrefractory period is reduced.10 In this study, the mag-nitude of the drop in the cognitive task score wasgreater in novices than experts; however, this trenddid not reach statistical significance. No detrimentalchange in operating scores were noted in novices orexperts, so it would appear that with this particularsurgical task, even novices are capable of prioritizingtheir surgical task ahead of the distracting cognitivetask.
There are some limitations to this study. First, oursample size was limited by the number of availableexperienced surgeons in our department. Acquisitionof similar simulators by more hospitals around thecountry could provide a larger sample through multi-center collaboration, although at present a limitednumber of these simulators are available. However,our sample is larger than that in 2 previously pub-lished studies of ophthalmic surgical simulators relat-ing to validation5 (12 novices, 3 experts) and the effectof fatigue on surgical performance11 (7 experts) andlarger than that in other laparoscopic simulator stud-ies relating to distraction (13 subjects).3 Furthermore,this sample size managed to yield statistically signif-icant changes in the cognitive task score for bothexpert and novice surgeons; therefore, conclusionsabout the effect of distraction on cognitive functionwhile operating can be made.
VOL 37, AUGUST 2011

1521EFFECT OF DISTRACTION ON SURGICAL PERFORMANCE
Second, it remains difficult to remove the effect ofthe learning curve surgeons experience as they repeatan identical task on the simulator. This learning effectwill always be present in any study assessing the per-formance of novice surgeons. Despite distraction,some novice score parameters improved, althoughonly the odometer score and corneal injury scorereached statistical significance. This suggests that theresults obtained while the novice surgeon was dis-tracted were confounded by a learning effect. Thestudy protocol (standardized introduction to the sim-ulator followed by repeating the task 10 times and us-ing only the final 4 scores) resulted in each novicespending 2 to 3 hours on the simulator. It was believedthat granting further practice to remove the learningeffect would have resulted in significant fatigue thatwould have compromised performance and con-founded the results. The current study protocol istherefore a reasonable way of reducing the learningcurve effect without compromising performancewith fatigue, although it would be interesting to ex-plore these features in future studies.
Third, our expert surgeons were considerably moreexperienced (mean 3800 procedures) than our expertrequirement of 350 procedures, which was chosen torelate to the Royal College of Ophthalmologists’ re-quirement as the minimum criteria for completion oftraining.6 There may be differences between these ex-pert groups, so care must be taken when relating theresults to expert surgeons with less surgical experi-ence. However, because the detrimental effect of dis-traction on the cognitive score occurred with bothnovices and experienced experts, it would be feasibleto expect a similar pattern in experts with less experi-ence than those in our study group.
Finally, it is important to appreciate that variousforms of distraction may have different effects on dif-ferent surgeons. Previous studies of laparoscopic sim-ulators2 found no detrimental effect on surgicalperformance after distractions consisting of noiseand music.2 Other laparoscopic simulator studies4
found that cognitive tasks in the form of arithmeticquestions have a detrimental effect on surgical andcognitive tasks, depending on the experience of the op-erating surgeon. We chose to assess the effect of cogni-tive tasks in the form of arithmetic questions to allowcomparison with previous studies in other special-ties3,4 and because arithmetic questions providea task not that dissimilar to cognitive tasks that sur-geons in a real operating room are challenged with,such as questions relating to other patients or queriesrelating to their surgical practice. It would also be in-teresting for future studies to evaluate other forms ofdistraction, such as the emotional state of the surgeonand his or her team.
J CATARACT REFRACT SURG -
In the past few years, we have found the simulatorto be very useful for surgical training, and this studyshows that such simulators also have a role in researchthat cannot be performed in a real-life environment.The initial monetary expense associated with simula-tors is prohibitive for many units. At present, the EyeSisimulator basic setup cost is approximately £80 000and approximately a further £20 000 required for 3years of updates and maintenance support. This costis a significant factor in limiting the widespread adop-tion of this helpful technology.
To conclude, a distractive cognitive task will re-duce the ability of both novice and expert surgeonsto deal with that cognitive task, although their simu-lated surgical performance is not overtly compro-mised. It is important to consider what real-lifeimplications this could have on a daily basis in all op-erating rooms, and even for live surgery at meetings.This study also shows the valuable role simulatorscan play in evaluating a surgeon’s performance undervarying conditions without compromising patientsafety.
REFERENCES1. Healey AN, Sevdalis N, Vincent CA. Measuring intra-operative
interference from distraction and interruption observed in the
operating theatre. Ergonomics 2006; 49:589–604. Available at:
http://hfrp.umm.edu/ergonomics/Healy%20distraction%20in%20
OR%20Ergonomics%202006l.pdf. Accessed February 22,
2011
2. Moorthy K, Munz Y, Undre S, Darzi A. Objective evaluation of
the effect of noise on the performance of a complex laparoscopic
task. Surgery 2004; 136:25–30; invited commentary by DW
Rattner, 31
3. Goodell KH, Cao CGL, Schwaitzberg SD. Effects of cognitive
distraction on performance of laparoscopic surgical tasks.
J Laparoendosc Adv Surg Tech A 2006; 16:94–98. Available
at: http://engineering.tufts.edu/me/erel/documents/pubs/2006_
EffectsOfCognitiveDistraction.pdf. Accessed February 22, 2011
4. Hsu KE, Man F-Y, Gizicki RA, Feldman LS, Fried GM. Experi-
enced surgeons can do more than one thing at a time: effect
of distraction on performance of a simple laparoscopic and cog-
nitive task by experienced and novice surgeons. Surg Endosc
2008; 22:196–201
5. MahrMA,HodgeDO.Construct validity of anterior segment anti-
tremor and forceps surgical simulator training modules; attend-
ing versus resident surgeon performance. J Cataract Refract
Surg 2008; 34:980–985
6. Royal College of Ophthalmologists. Ophthalmology Specialty
Training. Workplace Based Assessment Handbook for Stages
4 to 7 of OST. May, 2008. Available at: http://www.rcophth.ac.
uk/documents.asp?sectionZ39§ionTitleZPublications&
letZW. Accessed February 22, 2011
7. Privett B, Greenlee E, Rogers G, Oetting TA. Construct validity
of a surgical simulator as a valid model for capsulorhexis train-
ing. J Cataract Refract Surg 2010; 36:1835–1838
8. Pashler H, Johnston JC, Ruthruff E. Attention and performance.
Annu Rev Psychol 2001; 52:629–651. Available at: http://www.
pashler.com/Articles/Pashler_etal_AnnualReview2001.pdf. Ac-
cessed February 22, 2011
VOL 37, AUGUST 2011

1522 EFFECT OF DISTRACTION ON SURGICAL PERFORMANCE
9. VanSelstM,Ruthruff E, Johnston JC. Can practice eliminate the
psychological refractory period effect? J Exp Psychol 1999;
25:1268–1283. Available at: http://human-factors.arc.nasa.
gov/ihi/cognition/publications/VanSelst.Ruthruff.Johnston.1999.
pdf. Accessed February 22, 2011
10. Schneider W, Shriffrin RM. Controlled and automatic human
information processing: I. Detection, search, and attention.
Psychol Rev 1977; 84:1–66
11. Waqar S, Park J, Kersey TL, Modi N, Ong C, Sleep TJ. Assess-
ment of fatigue in intraocular surgery: analysis using a virtual re-
ality simulator. Graefes Arch Clin Exp Ophthalmol 2011;
249:77–81
J CATARACT REFRACT SURG -
OTHER CITED MATERIALA. EyeSi Ophthalmic Surgery Simulator User Guide. Mannheim,
Germany, VRmagic, Inc, 2006
VOL
37, AUGUST 2011First author:Jonathan Park, MBChb, BSc
Ophthalmology Department, SouthDevon Foundation NHS Trust,Torbay, Devon, United Kingdom