
Effect of Conditioning on Visceral Organs during Indirect Ischemia/Reperfusion Injury
8
Effect of Conditioning on Visceral Organs during Indirect Ischemia/Reperfusion Injury A. Tulga Ulus, 1 Soner Yavas, 1 Ali Sapmaz, 2 Ziysan Sakao gullari, 3 Erdal Simsek, 1 Siyar Ersoz, 2 and Cuneyt Koksoy, 2 Ankara, Turkey Background: The mortality and morbidity rates of even extensive thoracoabdominal replace- ment have improved markedly in recent years. We investigated the effects of a temporary occlu- sion of the aorta as a direct precondition and temporary occlusion of the axillary artery for remote preconditioning to determine any effects that preconditioning may have on indirect (nonische- mic) injuries to visceral organs (indirect effects of remote ischemia/reperfusion injury). Methods: Thirty-seven New Zealand white rabbits were divided into five groups: controls (sham-operated; group 1); direct ischemia to the infrarenal aorta without preconditioning (group 2); direct ischemic preconditioning to the infrarenal aorta (group 3); remote ischemic precondi- tioning before clamping the infrarenal aorta (group 4); and simultaneous direct aortic and remote ischemic preconditioning before the clamping and during clamping of the infrarenal aorta (group 5). We used a 30-minute ischemia period for aortic occlusion for spinal cord ischemia/reperfu- sion. The axillary artery was used for remote preconditioning. After 24 hours, tissue specimens of the internal organs were obtained. Results: Myocardial congestion was the main pathology detected in all groups. Histopathologic evaluation of tissue samples taken from the hearts showed no significant differences in terms of the degree of polymorphonuclear leukocyte (PMNL) infiltration and edema between the groups. Lung congestion and pneumonic cell infiltration were detected in all the groups. Pneumonic cell infiltration was significantly high in groups 2 and 3. Cell infiltration was lowest in group 4 at 71.4% of normal values, which differed from the normal values of 25e33.3% in the other groups (P < 0.05). Although there is a difference between the groups in case of renal congestion, there is not any difference as tubular damage and PMN. There was a significant difference with regard to renal congestion between groups 2 and 3. Renal congestion was normal in 80% of the kidneys in group 3. This differed from the normal values observed in the other groups (14.3e57.1%, P < 0.05). Liver congestion was detected in all groups. Conclusions: Different preconditioning methods may play an important role in distinct organ injuries during aortic cross-clamping. The visceral organs that exhibited positive and construc- tive results with direct and remote preconditioning included the lungs and kidneys during indirect ischemia/reperfusion injury. Remote ischemic conditioning was determined to be especially advantageous as a protection method, due to the fact that it is easy to use and effective for indi- rect ischemia/reperfusion injury. INTRODUCTION The mortality and morbidity rates of even extensive thoracoabdominal replacements have improved markedly in recent years. 1 Visceral organ dysfunc- tion, however, is still associated with a significant risk of postoperative mortality or morbidity after thoracabdominal aortic aneurysm (TAAA) repair. In 1986, the concept of ischemic preconditioning was first introduced as a potent, endogenous form of cardioprotection against ischemia/reperfusion (I/R) injuries. 2 Ischemic preconditioning (IPC) is 1 Cardiovascular Surgery Clinic, Turkiye Yuksek Ihtisas Education and Research Hospital, Ankara, Turkey. 2 Department of General Surgery, University of Ankara, Ankara, Turkey. 3 Department of Pathology, Turkiye Yuksek Ihtsas Education and Research Hospital, Ankara, Turkey. Correspondence to: Erdal Simsek, MD, Department of Cardiovas- cular Surgery, Yuksek Ihtisas Training and Research Hospital, Kızılay Street, Altinda g, Ankara, Turkey; E-mail: [email protected] Ann Vasc Surg 2014; 28: 437–444 http://dx.doi.org/10.1016/j.avsg.2013.06.027 Ó 2014 Elsevier Inc. All rights reserved. Manuscript received: December 2, 2012; manuscript accepted: June 14, 2013. 437
Transcript of Effect of Conditioning on Visceral Organs during Indirect Ischemia/Reperfusion Injury
1Cardiovasand Research
2DepartmeTurkey.
3DepartmeResearch Hosp
Correspondcular Surgery,Street, Altinda
Ann Vasc Surghttp://dx.doi.or� 2014 Elsevi
Manuscript rec
2013.
Effect of Conditioning on Visceral Organsduring Indirect Ischemia/Reperfusion Injury
A. Tulga Ulus,1 Soner Yavas,1 Ali Sapmaz,2 Ziysan Sakao�gullari,3 Erdal Simsek,1
Siyar Ersoz,2 and Cuneyt Koksoy,2 Ankara, Turkey
Background: The mortality and morbidity rates of even extensive thoracoabdominal replace-ment have improved markedly in recent years. We investigated the effects of a temporary occlu-sion of the aorta as a direct precondition and temporary occlusion of the axillary artery for remotepreconditioning to determine any effects that preconditioning may have on indirect (nonische-mic) injuries to visceral organs (indirect effects of remote ischemia/reperfusion injury).Methods: Thirty-seven New Zealand white rabbits were divided into five groups: controls(sham-operated; group 1); direct ischemia to the infrarenal aorta without preconditioning (group2); direct ischemic preconditioning to the infrarenal aorta (group 3); remote ischemic precondi-tioning before clamping the infrarenal aorta (group 4); and simultaneous direct aortic and remoteischemic preconditioning before the clamping and during clamping of the infrarenal aorta (group5). We used a 30-minute ischemia period for aortic occlusion for spinal cord ischemia/reperfu-sion. The axillary artery was used for remote preconditioning. After 24 hours, tissue specimensof the internal organs were obtained.Results: Myocardial congestion was the main pathology detected in all groups. Histopathologicevaluation of tissue samples taken from the hearts showed no significant differences in terms ofthe degree of polymorphonuclear leukocyte (PMNL) infiltration and edema between the groups.Lung congestion and pneumonic cell infiltration were detected in all the groups. Pneumonic cellinfiltration was significantly high in groups 2 and 3. Cell infiltration was lowest in group 4 at 71.4%of normal values, which differed from the normal values of 25e33.3% in the other groups(P < 0.05). Although there is a difference between the groups in case of renal congestion, thereis not any difference as tubular damage and PMN. There was a significant difference with regardto renal congestion between groups 2 and 3. Renal congestion was normal in 80% of the kidneysin group 3. This differed from the normal values observed in the other groups (14.3e57.1%,P < 0.05). Liver congestion was detected in all groups.Conclusions: Different preconditioning methods may play an important role in distinct organinjuries during aortic cross-clamping. The visceral organs that exhibited positive and construc-tive results with direct and remote preconditioning included the lungs and kidneys during indirectischemia/reperfusion injury. Remote ischemic conditioning was determined to be especiallyadvantageous as a protection method, due to the fact that it is easy to use and effective for indi-rect ischemia/reperfusion injury.
cular Surgery Clinic, Turkiye Yuksek Ihtisas EducationHospital, Ankara, Turkey.
nt of General Surgery, University of Ankara, Ankara,
nt of Pathology, Turkiye Yuksek Ihtsas Education andital, Ankara, Turkey.
ence to: Erdal Simsek, MD, Department of Cardiovas-Yuksek Ihtisas Training and Research Hospital, Kızılay�g, Ankara, Turkey; E-mail: [email protected]
2014; 28: 437–444g/10.1016/j.avsg.2013.06.027er Inc. All rights reserved.
eived: December 2, 2012; manuscript accepted: June 14,
INTRODUCTION
The mortality and morbidity rates of even extensive
thoracoabdominal replacements have improved
markedly in recent years.1 Visceral organ dysfunc-
tion, however, is still associated with a significant
risk of postoperative mortality or morbidity after
thoracabdominal aortic aneurysm (TAAA) repair.
In 1986, the concept of ischemic preconditioning
was first introduced as a potent, endogenous form
of cardioprotection against ischemia/reperfusion
(I/R) injuries.2 Ischemic preconditioning (IPC) is
437

438 Ulus et al. Annals of Vascular Surgery
a counter intuitive phenomenon, involving induc-
tion of brief periods of ischemia, which protects
various organs from subsequent episodes of more
protracted or sustained ischemia. Initially described
by Murry et al. in a canine model of myocardial
ischemia, IPC occurs in many species, including
humans, and in various organs, including the liver,
lungs, intestine, and kidneys.2e6
Wepreviously investigated the effects of precondi-
tioning on the spinal cord using the same I/R model
with the same experimental setup to determine
spinal cord functional and pathologic outcomes.
Because I/R injury is thought to be a systemic
reaction, we investigated the effects of temporary
occlusion of the aorta as direct preconditioning
and the axillary artery for remote preconditioning
to determine the effects that preconditioning may
have on injury to visceral organs (indirect effects
of remote ischemia/reperfusion injury).
METHODS
The study was carried out according to the ‘‘Princi-
ples of Laboratory Animal Care’’ and The Guide for
the Care and Use of Laboratory Animals (NIH Publica-
tion No. 80-23, revised 1985), after approval from
the ethics committee of out institution. This investi-
gation was performed for the purpose of evaluating
distal organs and is the second part of this research is
related to spinal cord ischemia.
Thirty-sevenNewZealandwhite rabbitswereused
in the study and the (meanweight 2.7 ± 0.2 kg, range
2.5e3.5kg). Theanimalswere allowedaccess to stan-
dard rabbit chow and tap water ad libitum.
The Rabbits were divided into five groups as
follows:
Group 1: controls (sham-operated).
Group 2: direct ischemia to the infrarenal aorta
without preconditioning.
Group 3: direct ischemic preconditioning to the
infrarenal aorta.
Group 4: remote ischemic preconditioning,
before clamping of the infrarenal aorta.
Group 5: simultaneous direct aortic ischemia
and remote ischemic perconditioning before
clamping and during clamping of the infrarenal
aorta.
Surgical Procedure
The animals were administered ketamine (50mg/kg)
and xylazine (10 mg/kg) intramuscularly for in-
duction of anesthesia and allowed to breathe
spontaneously without mechanical ventilation.
Intravenous xylazine was used for anesthesia main-
tenance, if needed. An ear vein catheter was placed
for the administration of intravenous fluids and addi-
tional medications. An ear arterial catheter was
placed to obtain blood samples.
After sterile surgical preparation, the abdomen
was opened with a 4-cm midline laparotomy inci-
sion and the retroperitoneal abdominal aorta was
exposed. In group 1 (sham, 6 animals), the abdomen
was provisionally closed to avoid excessive heat or
fluid loss and kept this way for 30 minutes without
clamping. In group 2 (9 animals), after positioning
of the abdominal aorta with tape, 50 IU/kg heparin
sodium was administered intravenously and the
aorta was cross-clamped using an atraumatic
vascular clamp immediately caudal to the origin of
the left renal artery and above the aortic bifurcation.
The use of application of 30 minutes of ischemic
insult is based on the results of previous experi-
ments using this model.7e9 After occluding the
aorta, the abdomen was provisionally closed to
avoid excessive heat or fluid loss. After removal
of the cross-clamp, distal reperfusion was observed
visually. In group 3 (6 animals), in this direct
preconditioning group, after the three 5-minute
periods of clamping of the aorta, 30 minutes of
clampingwas done. In group 4 (8 animals), the right
axillary artery was exposed via a 3-cm-long axillary
incision and controlled with vascular tape. The axil-
lary artery was clamped three times for 5-minute
periods with 5-minute clamp removal periods.
During these clamping periods, the abdomen was
opened with a 4-cm midline laparotomy incision
and the retroperitoneal abdominal aorta was
exposed and controlled with vascular tape. After
clamping and reperfusing the axillary artery a third
time, the abdominal aorta was cross-clamped using
an atraumatic vascular clamp immediately caudal
to the origin of the left renal artery and above the
aortic bifurcation, and the abdomen was provision-
ally closed to avoid excessive heat or fluid loss and
kept this way for 30minutes. In group 5 (8 animals),
the axillary artery and abdominal aorta were
clamped simultaneously. Although the axillary
arterywas clamped three times for 5-minute periods
with 5-minute clamp removal periods, the abdom-
inal aortawas clamped continuously for 30minutes.
Upon completion of the procedures, incisions
were closed with sutures and all catheters were
removed. The animals were allowed to recover
from anesthesia before they were returned to the
holding area, where they could move freely in their
cages, and were provided with food and water ad
libitum and permitted to remain alive for 24 hours.
Vol. 28, No. 2, February 2014 Conditioning of visceral organs in I/R 439
At that point, all animals were euthanized with
intravenous sodium pentobarbital (50 mg/kg) and
tissue specimens were obtained.
Histopathologic Assessment
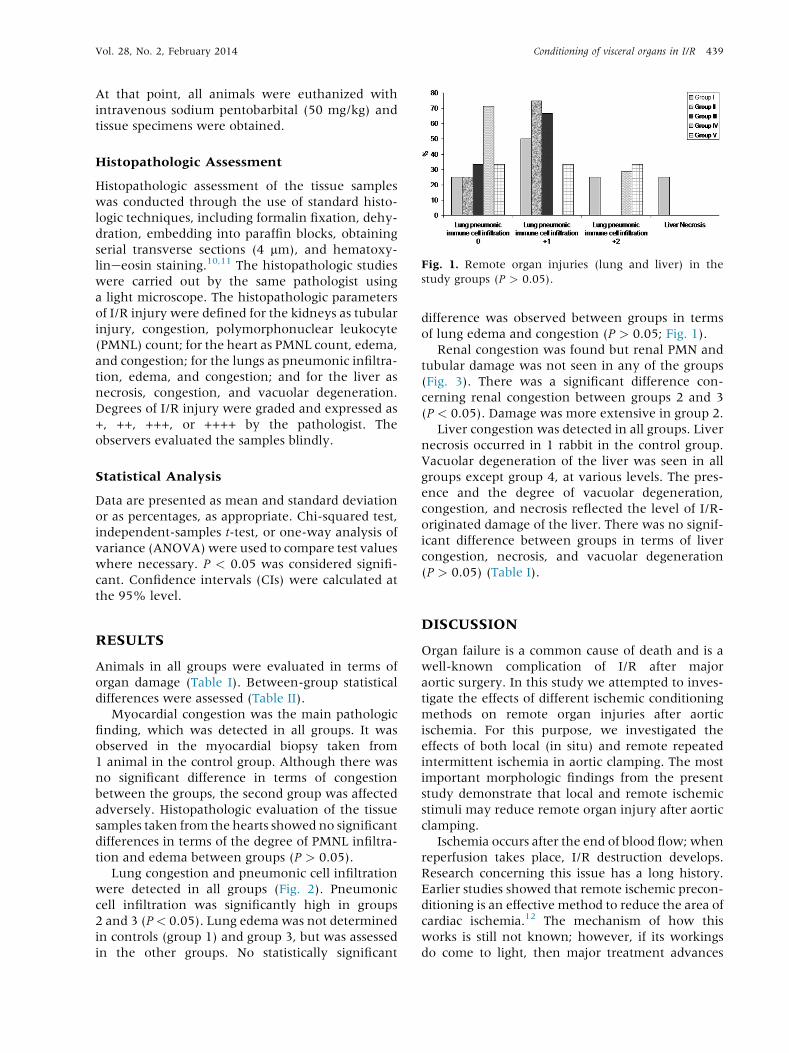
Fig. 1. Remote organ injuries (lung and liver) in the
study groups (P > 0.05).
Histopathologic assessment of the tissue samples
was conducted through the use of standard histo-
logic techniques, including formalin fixation, dehy-
dration, embedding into paraffin blocks, obtaining
serial transverse sections (4 mm), and hematoxy-
lineeosin staining.10,11 The histopathologic studies
were carried out by the same pathologist using
a light microscope. The histopathologic parameters
of I/R injury were defined for the kidneys as tubular
injury, congestion, polymorphonuclear leukocyte
(PMNL) count; for the heart as PMNL count, edema,
and congestion; for the lungs as pneumonic infiltra-
tion, edema, and congestion; and for the liver as
necrosis, congestion, and vacuolar degeneration.
Degrees of I/R injury were graded and expressed as
+, ++, +++, or ++++ by the pathologist. The
observers evaluated the samples blindly.
Statistical Analysis
Data are presented as mean and standard deviation
or as percentages, as appropriate. Chi-squared test,
independent-samples t-test, or one-way analysis of
variance (ANOVA)were used to compare test values
where necessary. P < 0.05 was considered signifi-
cant. Confidence intervals (CIs) were calculated at
the 95% level.
RESULTS
Animals in all groups were evaluated in terms of
organ damage (Table I). Between-group statistical
differences were assessed (Table II).
Myocardial congestion was the main pathologic
finding, which was detected in all groups. It was
observed in the myocardial biopsy taken from
1 animal in the control group. Although there was
no significant difference in terms of congestion
between the groups, the second group was affected
adversely. Histopathologic evaluation of the tissue
samples taken from the hearts showed no significant
differences in terms of the degree of PMNL infiltra-
tion and edema between groups (P > 0.05).
Lung congestion and pneumonic cell infiltration
were detected in all groups (Fig. 2). Pneumonic
cell infiltration was significantly high in groups
2 and 3 (P< 0.05). Lung edema was not determined
in controls (group 1) and group 3, but was assessed
in the other groups. No statistically significant
difference was observed between groups in terms
of lung edema and congestion (P > 0.05; Fig. 1).
Renal congestion was found but renal PMN and
tubular damage was not seen in any of the groups
(Fig. 3). There was a significant difference con-
cerning renal congestion between groups 2 and 3
(P < 0.05). Damage was more extensive in group 2.
Liver congestion was detected in all groups. Liver
necrosis occurred in 1 rabbit in the control group.
Vacuolar degeneration of the liver was seen in all
groups except group 4, at various levels. The pres-
ence and the degree of vacuolar degeneration,
congestion, and necrosis reflected the level of I/R-
originated damage of the liver. There was no signif-
icant difference between groups in terms of liver
congestion, necrosis, and vacuolar degeneration
(P > 0.05) (Table I).
DISCUSSION
Organ failure is a common cause of death and is a
well-known complication of I/R after major
aortic surgery. In this study we attempted to inves-
tigate the effects of different ischemic conditioning
methods on remote organ injuries after aortic
ischemia. For this purpose, we investigated the
effects of both local (in situ) and remote repeated
intermittent ischemia in aortic clamping. The most
important morphologic findings from the present
study demonstrate that local and remote ischemic
stimuli may reduce remote organ injury after aortic
clamping.
Ischemia occurs after the end of blood flow; when
reperfusion takes place, I/R destruction develops.
Research concerning this issue has a long history.
Earlier studies showed that remote ischemic precon-
ditioning is an effective method to reduce the area of
cardiac ischemia.12 The mechanism of how this
works is still not known; however, if its workings
do come to light, then major treatment advances
Table I. Comparison of remote organ injuries and mortality between groups
Group 1 Group 2 Group 3 Group 4 Group 5 P
Exitus % (n) 0 22.2 (2) 0 0 0 0.160
Myocardial congestion 0.839
0 75.0 (3) 42.9 (3) 60.0 (3) 62.5 (5) 57.1 (4)
1+ 25.0 (1) 42.9 (3) 40.0 (2) 37.5 (3) 42.9 (3)
2+ 0 14.3 (1) 0 0 0
Myocardial PMN -
0 100.0 (4) 100.0 (7) 100.0 (5) 100.0 (8) 100.0 (7)
1+ 0 0 0 0 0
Myocardial edema -
0 100.0 (4) 100.0 (7) 100.0 (5) 100.0 (8) 100.0 (7)
1+ 0 0 0 0 0
Lung congestion 0.830
0 50.0 (2) 75.0 (3) 50.0 (3) 28.6 (2) 40.0 (2)
1+ 50.0 (2) 25.0 (1) 33.3 (2) 57.1 (4) 60.0 (3)
2+ 0 0 16.7 (1) 14.3 (1) 0
Lung pneumonic
immune cell
infiltration
0.234
0 25.0 (1) 25.0 (1) 33.3 (2) 71.4 (5) 33.3 (2)
1+ 50.0 (2) 75.0 (3) 66.7 (4) 0 33.3 (2)
2+ 25.0 (1) 0 0 28.6 (2) 33.3 (2)
Lung edema 0.638
0 100.0 (4) 75.0 (3) 100.0 (6) 85.7 (6) 66.7 (4)
1+ 0 25.0 (1) 0 14.3 (1) 16.7 (1)
2+ 0 0 0 0 16.7 (1)
Renal congestion 0.152
0 25.0 (1) 14.3 (1) 80.0 (4) 33.3 (2) 57.1 (4)
1+ 50.0 (2) 85.7 (6) 0 66.7 (4) 28.6 (2)
2+ 25.0 (1) 0 20.0 (1) 0 14.3 (2)
Renal PMN -
0 100.0 (4) 100.0 (7) 100.0 (5) 100.0 (6) 100.0 (7)
1+ 0 0 0 0 0
Renal tubular injury -
0 100.0 (4) 100.0 (7) 100.0 (5) 100.0 (6) 100.0 (7)
1+ 0 0 0 0 0
Liver congestion 0.633
0 40.0 (2) 57.1 (4) 80.0 (4) 50.0 (2) 33.3 (2)
1+ 40.0 (2) 42.9 (3) 20.0 (1) 25.0 (1) 50.0 (3)
2+ 0 0 0 0 16.7 (1)
3+ 20.0 (1) 0 0 25.0 (1) 0
Liver necrosis 0.242
0 75.0 (3) 100.0 (7) 100.0 (5) 100.0 (4) 100.0 (5)
1+ 25.0 (1) 0 0 0 0
Liver vacuolar
degeneration
0.516
0 60.0 (3) 57.1 (4) 60.0 (3) 100.0 (4) 66.7 (4)
1+ 20.0 (1) 42.9 (3) 40.0 (2) 0 33.3 (2)
2+ 20.0 (1) 0 0 0 0
440 Ulus et al. Annals of Vascular Surgery
may be developed.13 According to one theory, aden-
osine and bradykinin are secreted from the other
tissues and, accordingly, catecholamine secretion,
sympatheticnerve stimulation, andfinallyprotection
is provided.13 According to the neural hypothesis,
adenosine, bradykinin, and calcitonin-generated
peptide (CGRP) provide protection by stimulating
the regional afferent neural pathway; in the humoral
hypothesis, adenosine, bradykinin, opioids, CGRP,
endocannabinoids, and other humoral factors
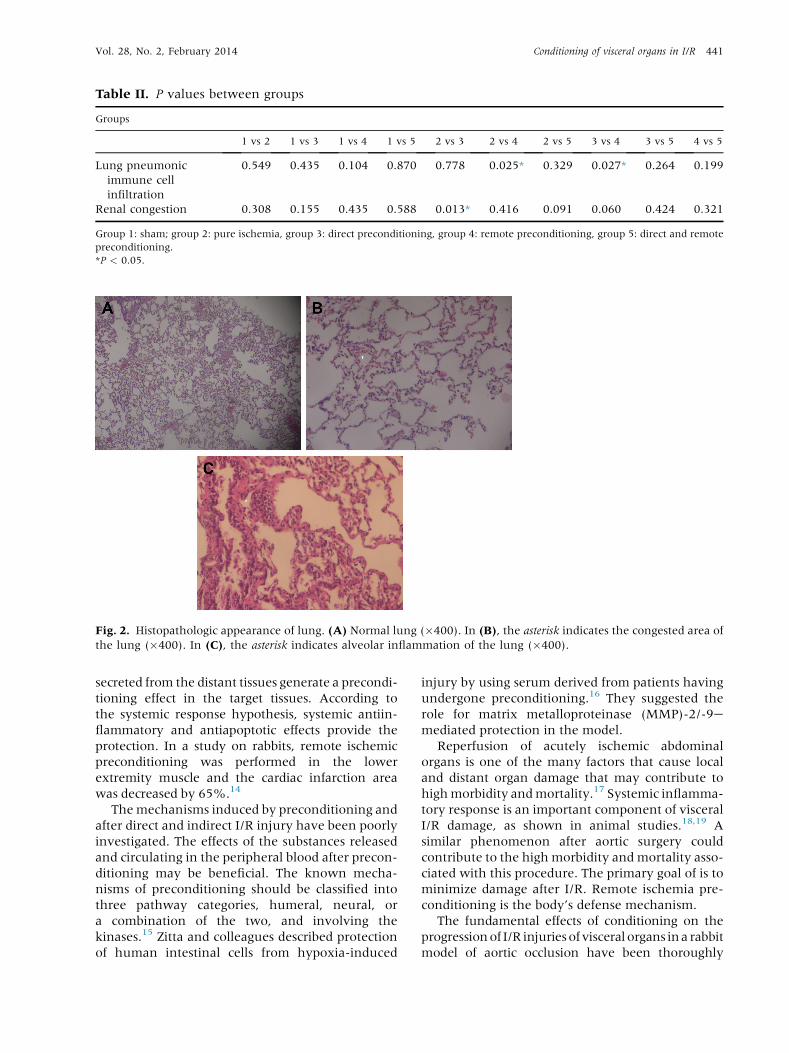
Table II. P values between groups
Groups
1 vs 2 1 vs 3 1 vs 4 1 vs 5 2 vs 3 2 vs 4 2 vs 5 3 vs 4 3 vs 5 4 vs 5
Lung pneumonic
immune cell
infiltration
0.549 0.435 0.104 0.870 0.778 0.025* 0.329 0.027* 0.264 0.199
Renal congestion 0.308 0.155 0.435 0.588 0.013* 0.416 0.091 0.060 0.424 0.321
Group 1: sham; group 2: pure ischemia, group 3: direct preconditioning, group 4: remote preconditioning, group 5: direct and remote
preconditioning.
*P < 0.05.
Fig. 2. Histopathologic appearance of lung. (A) Normal lung (�400). In (B), the asterisk indicates the congested area of
the lung (�400). In (C), the asterisk indicates alveolar inflammation of the lung (�400).
Vol. 28, No. 2, February 2014 Conditioning of visceral organs in I/R 441
secreted from the distant tissues generate a precondi-
tioning effect in the target tissues. According to
the systemic response hypothesis, systemic antiin-
flammatory and antiapoptotic effects provide the
protection. In a study on rabbits, remote ischemic
preconditioning was performed in the lower
extremity muscle and the cardiac infarction area
was decreased by 65%.14
Themechanisms induced by preconditioning and
after direct and indirect I/R injury have been poorly
investigated. The effects of the substances released
and circulating in the peripheral blood after precon-
ditioning may be beneficial. The known mecha-
nisms of preconditioning should be classified into
three pathway categories, humeral, neural, or
a combination of the two, and involving the
kinases.15 Zitta and colleagues described protection
of human intestinal cells from hypoxia-induced
injury by using serum derived from patients having
undergone preconditioning.16 They suggested the
role for matrix metalloproteinase (MMP)-2/-9emediated protection in the model.
Reperfusion of acutely ischemic abdominal
organs is one of the many factors that cause local
and distant organ damage that may contribute to
highmorbidity andmortality.17 Systemic inflamma-
tory response is an important component of visceral
I/R damage, as shown in animal studies.18,19 A
similar phenomenon after aortic surgery could
contribute to the high morbidity and mortality asso-
ciated with this procedure. The primary goal of is to
minimize damage after I/R. Remote ischemia pre-
conditioning is the body’s defense mechanism.
The fundamental effects of conditioning on the
progressionof I/R injuriesof visceral organs ina rabbit
model of aortic occlusion have been thoroughly

Fig. 3. Histopathologic appearance of the kidney. (A)
Normal kidney (�400). In (B), the asterisk indicates the
severely congested kidney area (�400).
442 Ulus et al. Annals of Vascular Surgery
examined. It was identified that, in the aftermath of
aortic aneurysm repair, significant complications
may occur and visceral damage can be a severe,
even lethal pathology. One study showed a very
high rate (34.5%) of visceral organ damage (multi-
system organ failure) among 29 patients with thora-
coabdominal aortic aneurysm repair (TAAA).20 In
that study, the mortality rate was 17.2%, myocardial
infarction rate was 6.9%, pulmonary failure was
44.8%, renal failure was 34.5%, hepatic failure was
24.1%, hematopoietic failure was 41.4%, and spinal
cord injurywas 10.3%.20 Aortic aneurysm repair still
seems to be a great challenge. The most common
causes death include multisystem organ failure,
hemorrhagic shock, and cardiac damage. The most
overwhelming complication is paraplegia. It is
known that surgery for TAAA repair affects all major
organs, including the heart, lung, liver, kidneys,
intestines, and spinal cord.20,21
Throughout TAAA repair, the heart must regu-
late not only the immediate afterload augmentation
due to cross-clamping of the aorta but also the
inflammatory response due to visceral I/R injury.
We acknowledge the fact that aortic cross-
clamping clearly causes proximal systemic hyper-
tension and left ventricular distention. Increased
wall stress and decreased subendocardial perfusion
may also be observed due to left ventricular disten-
tion. Harward and colleagues reported a myocardial
infarction (MI) rate of 6.9% in this setting.20 Cam-
bria et al. evaluated 337 patients undergoing
TAAA repair over a 15-year period and described
a 13.8% rate of cardiac complications.22 In our
study, we observed no differences among groups
with regard to pathology of the heart.
Similar to the heart, although proximal to the
cross-clamp, pulmonary dysfunction after TAAA
repair is firmly associated with I/R injury and
systemic inflammatory response syndrome. The
incidence rates of pulmonary complications fol-
lowing TAAA repair varies between 20% and 50%.
Advanced age, longer aortic cross-clamp time,
number of packed red blood cells transfused, and
tobacco are considered common predictors of pro-
longed postoperative respiratory failure.23 Unlike
all other organs in the human body, the lung has
two blood supply networks with widespread anasto-
motic connections and a total of three likely sources
of lung tissue oxygenationdwhich has resulted in
comprehensive research into addressing the role of
neutrophils and other inflammatory mediators.24
However, these mediators seem to have only a
limited role in lung I/R injury.24,25 Another report
indicated that the rate of pulmonary dysfunction
was 44.8% after TAAA repair, 25% when cross-
clamp time was <40 minutes and 59% when cross-
clamp time was�40minutes.17 After aortic surgery,
a systemic inflammatory response, as detected by
a consistent increase in cytokine plasma concentra-
tion (tumor necrosis factor-a and interleukin-6),
was observed; nevertheless, there was no specific
evidence of a relationship between cytokine plasma
concentrations and clinical outcome after aortic
surgery. Thus, the clinical details associated with
the transient systemic inflammatory response re-
main unclear.26 In our investigation, according to
lung pneumonic immune cell infiltration findings,
the remote preconditioning group (group 4) showed
better results than groups 2 and 3. This may be
an important finding with regard to lung protec-
tion, although we studied only a small number of
animals.
Necrosis, congestion, and vacuolar degeneration
have been considered histopathologic parameters in
liver I/R injury.27 After 48 hours of reperfusion,
eminent microcirculatory destruction has been

Vol. 28, No. 2, February 2014 Conditioning of visceral organs in I/R 443
shown to take place, decreasing liver perfusion.26
Biopsies taken 24 hours postoperatively showed no
severe damage to liver tissues. Furthermore, we
observed no statistical difference between groups
with respect to biochemical or histopathologic
parameters, although vacuolar degeneration was
seen in 1 animal in group 3.
One of the most common complications of aortic
surgery is acute renal failure (ARF),28 with an inci-
dence rate of between 3% and 34.5%.13,18,26 It has
been asserted that the renal flow pattern diverts
the cortical nephrons even though the aorta is
cross-clamped infrarenally.29 Ultimately, regardless
of where the cross-clamp is placed, renal perfusion
decreases and the release of inflammatorymediators
leads to vasoconstriction, redistribution of the flow
pattern, and increased vascular permeability.
Finally, cytokines, forskolin, proteases, myeloper-
oxidase, and other enzymes that reduce damage
are absolved by the activated neutrophils.30 In our
study, the direct preconditioning group showed
the best results with regard to renal congestion.
There was a significant difference between groups,
particularly when comparing the ischemic group
and the direct preconditioning group. Precondition-
ing has major effect on renal injuries.
In conclusion, these present results suggest that
aortic cross-clamping causes remote organ injury.
Different ischemic conditioning methods may play
major roles in distinct organ injury during aortic
cross-clamping for aortic aneurysms. The organs
protected by direct and remote preconditioning
were the lungs and renal systems. Remote precondi-
tioning is considered an especially advantageous
protection method because it is easy to use and
effective during aortic surgery.
REFERENCES
1. Svensson LG. Paralysis after aortic surgery: in search of lost
cord function. Surgeon 2005;3:396e405.
2. Murry CE, Jennings RB, Reimer KA. Preconditioning with
ischemia: a delay of lethal cell injury in ischemic myocar-
dium. Circulation 1986;74:1124e36.
3. LIoris-Carsi JM, Cejalvo D, Toledo-Pereyra LH, et al. Precon-
ditioning: effect upon lesion modulation in warm liver
ischemia. Transplant Proc 1993;25:3303e4.4. Peralta C, Hotter G, Closa D, et al. Protective effect of pre-
conditioning on the injury associated to hepatic ischemia-
reperfusion in the rat: role of nitric oxide and adenosine.
Hepatology 1997;25:934e7.5. Lee HT, Emala CW. Protective effects of renal ischemic pre-
conditioning and adenosine pretreatment: role of A(1) and
A(3) receptors. Am J Physiol Renal Physiol 2000;278:380e7.
6. Hotter G, Closa D, Prados M, et al. Intestinal preconditioning
is mediated by a transient increase in nitric oxide. Biochem
Biophys Res Commun 1996;222:27e32.
7. Ulus AT, Saritas A, Yamak B, et al. ATP-MgCl2 utilization for
spinal cord protection during experimental thoracic aortic
occlusion. J Cardiovasc Surg 1999;40:495e9.
8. Nakano A, Cohen MV, Downey JM. Ischemic precondition-
ing: from basic mechanisms to clinical applications. Pharma-
col Ther 2000;86:263e75.
9. Ulus AT, Turan NN, Seren M, et al. In which period of injury
is resveratrol treatment effective: ischemia or reperfusion?
Ann Vasc Surg 2007;21:360e6.10. Beuk RJ, Heineman E, Tangelder GJ, et al. Effects of
different durations of total warm ischemia of the gut on
rat mesenteric microcirculation. J Surg Res 1997;73:14e23.
11. Quaedackers JS, Beuk RJ, Bennet L, et al. An evaluation of
methods for grading histologic injury following ischemia/
reperfusion of the small bowel. Transplant Proc 2000;32:
1307e10.12. Przyklenk K, Bauer B, Ovize M, et al. Regional ischemic ‘pre-
conditioning’ protects remote virgin myocardium from sub-
sequent sustained coronary occlusion. Circulation 1993;87:
893e9.13. Morita S. Remote ischemic preconditioning. Is it time to
introduce it in clinical practice? Circ J 2011;75:1821e2.
14. Birnbaum Y, Hale SL, Kloner RA. Ischemic preconditioning
at a distance: reduction of myocardial infarct size by partial
reduction of blood supply combined with rapid stimulation
of the gastrocnemius muscle in the rabit. Circulation 1997;
96:1641e6.
15. Zitta K, Meybohm P, Bein B, et al. Serum from patients
undergoing remote ischemic preconditioning protects
cultured human intestinal cells from hypoxia induced
damage: involvement of matrix metalloproteinase 2 and 9.
Mol Med 2012;18:29e37.
16. Tapuria N, Kumar Y, Habib MM, et al. Remote ischemic pre-
conditioning: a novel protective method from ischemia
reperfusion injury: a review. J Surg Res 2008;150:304e30.17. Welbourn R, Goldman G, O’Riordian M, et al. Role for
tumor necrosis factor as mediator of lung injury following
lower torso ischemia. J Appl Physiol 1991;70:2645e9.
18. Cambria RP, Clouse WD, Davison JK, et al. Thoracoabdomi-
nal aneurysm repair: results with 337 operations performed
over a 15-year interval. Ann Surg 2002;236:471e9.
19. Engle J, Safi HJ, Miller CC 3rd, et al. The impact of dia-
phragm management on prolonged ventilator support after
thoracoabdominal aortic repair. J Vasc Surg 1999;29:150e6.
20. Harward TR, Welborn MB 3rd, Martin TD, et al. Visceral
ischemia and organ dysfunction after thoracoabdominal
aortic aneurysm repair. A clinical and cost analysis. Ann
Surg 1996;223:729e34.
21. Johnston TD, Fischer R, Chen R, et al. Lung injury from gut
ischemia: insensitivity to portal blood flow diversion.
J Trauma 1993;35:508e11.
22. Ng CS, Wan S, Yim AP. Pulmonary ischaemiaereperfusion
injury: role of apoptosis. Eur Respir J 2005;25:356e63.23. Svensson LG, Hess KR, Coselli JS, et al. A prospective study
of respiratory failure after high-risk surgery on the thora-
coabdominal aorta. J Vasc Surg 1991;14:271e82.
24. Adembri C, Kastamoniti E, Bertolozzi I, et al. Pulmonary
injury follows systemic inflammatory reaction in infrarenal
aortic surgery. Crit Care Med 2004;32:1170e7.
25. Fondevila C, Busuttil RW, Kupiec-Weglinski JW. Hepatic
ischemia/reperfusion injury a fresh look. Exp Mol Pathol
2003;74:86e93.
26. Ikeda T, Yanaga K, KishikawaK, et al. Ischemic injury in liver
transplantation: difference in injury sites between warm and
cold ischemia in rats. Hepatology 1992;16:454e61.
444 Ulus et al. Annals of Vascular Surgery
27. Martin LF, Atnip RG, Holmes PA, et al. Prediction of post-
operative complications after elective aortic surgery using
stepwise logistic regression analysis. Am Surg 1994;60:
163e8.
28. Poulias GE, Doundoulakis N, Skoutas B, et al. Juxtarenal
abdominal aneurysmectomy. J Cardiovasc Surg (Torino)
1992;33:324e30.
29. Lauriat S, Linas SL. The role of neutrophils in acute renal
failure. Semin Nephrol 1998;18:498e504.
30. Svensson LG, Crawford ES, Hess KR, et al. Thoracoabdomi-
nal aortic aneurysms associated with celiac, superior mesen-
teric, and renal artery occlusive disease: methods and
analysis of results in 271 patients. J Vasc Surg 1992;16:
378e89.


















