Effect of Adding Motolimod to Standard Combination … · ActiveS A Randomized, Double-Blind,...
307
Active8 Title: Version: Sponsor: Study Chairs: Contract Research Organization: vTX-2337 CLINICAL PROTOCOL VRXP.A2O2 ActiveS A Randomized, Double-Blind, Placebo-Controlled Study of Chemotherapy Plus Cetuximab in Combination with VTX-2337 in Patients with Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck Original Issue: 3l-May-2013 Amendment No.: Version 1.1 l4-Jun-2013 VentiRx Pharmaceuticals, Incorporated 1301 Second Avenue Suite 2800 Seattle, WA 98101 (206) 689-22s9 Ezra Cohen, MDI and Robert Ferris, MD, PhD2 PRA Intemational 4130 Parklake Avenue Suite 400 Raleigh, NC27612 I 14-Jun-2013 CONFIDENTIAI- This document contains proprietary and confidential information of VentiRx Pharmaceuticals, Inc. Acceptance of this document constitutes agreement by the recipient that no previously unpublished information contained herein will be published or disclosed without the prior written approval of VentiRx Pharmaceuticals, Inc., except disclosure to study personnel and appropriate Institutional Review Boards (IRB)/Independent Ethics Committees (IEC) under the condition that thepersonnel have agreed to keep this information confidential. The foregoing shall not apply to disclosure required by govemmental regulations or laws; however, VentiRx Pharmaceuticals, Inc. shall be promptly notif,red ofany such disclosure. I Associate Professor of Medicine, University of Chicago Comprehensive Cancer Center ? Professor of Otolaryngology, Cancer Immunology Prõgram, University of Pittsburgh Cancer Institute VentiRx Ph armaceuticals Incorporated Confidential Information Approved by: James Kylelryan, MD Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020
Transcript of Effect of Adding Motolimod to Standard Combination … · ActiveS A Randomized, Double-Blind,...

Active8
Title:
Version:
Sponsor:
Study Chairs:
Contract Research Organization:
vTX-2337
CLINICAL PROTOCOL VRXP.A2O2
ActiveS
A Randomized, Double-Blind, Placebo-Controlled Study of ChemotherapyPlus Cetuximab in Combination with VTX-2337 in Patients with Recurrent orMetastatic Squamous Cell Carcinoma of the Head and Neck
Original Issue: 3l-May-2013
Amendment No.: Version 1.1 l4-Jun-2013
VentiRx Pharmaceuticals, Incorporated
1301 Second Avenue
Suite 2800
Seattle, WA 98101
(206) 689-22s9
Ezra Cohen, MDI and Robert Ferris, MD, PhD2
PRA Intemational
4130 Parklake Avenue
Suite 400
Raleigh, NC27612
I14-Jun-2013
CONFIDENTIAI-This document contains proprietary and confidential information of VentiRx Pharmaceuticals, Inc. Acceptance ofthis document constitutes agreement by the recipient that no previously unpublished information contained hereinwill be published or disclosed without the prior written approval of VentiRx Pharmaceuticals, Inc., except disclosureto study personnel and appropriate Institutional Review Boards (IRB)/Independent Ethics Committees (IEC) underthe condition that thepersonnel have agreed to keep this information confidential. The foregoing shall not apply todisclosure required by govemmental regulations or laws; however, VentiRx Pharmaceuticals, Inc. shall be promptlynotif,red ofany such disclosure.
I Associate Professor of Medicine, University of Chicago Comprehensive Cancer Center? Professor of Otolaryngology, Cancer Immunology Prõgram, University of Pittsburgh Cancer Institute
VentiRx Ph armaceuticals IncorporatedConfidential Information
Approved by:
James Kylelryan, MD
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 2 Confidential Information 14-Jun-2013
VentiRx Pharmaceuticals Protocol No. VRXP-A202
PRINCIPAL INVESTIGATOR PROTOCOL AGREEMENT
A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED STUDY OF CHEMOTHERAPY PLUS CETUXIMAB IN COMBINATION WITH VTX 2337 IN
PATIENTS WITH RECURRENT OR METASTATIC SQUAMOUS CELL CARCINOMA OF THE HEAD AND NECK
Version Date: 14-Jun-2013
I attest that I have read this protocol and the Investigator Brochure (IB) for VTX-2337. I agree to conduct the trial in accordance with the provisions herein, U.S. Food and Drug Administration (FDA) regulations, applicable Competent Authorities, International Conference on Harmonization (ICH) guidelines for Good Clinical Practice (GCP), state and local regulations and the requirements of the IRB/IEC.
I will provide copies of the current protocol and access to all information provided by VentiRx Pharmaceuticals, Inc. to the study personnel under my supervision. I will discuss this material with them to ensure that they are fully informed about the investigational drug and the study protocol.
Principal Investigator Signature Date
Principal Investigator Printed Name
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 3 Confidential Information 14-Jun-2013
TABLE OF CONTENTS 1.0 STUDY SYNOPSIS ...........................................................................................................5
2.0 BACKGROUND ................................................................................................................8
2.1 Investigational Agent ...............................................................................................9
2.2 Nonclinical Data ......................................................................................................9
2.3 Clinical Data ..........................................................................................................11
2.4 Risks/Benefits ........................................................................................................14
2.5 Dose Rationale .......................................................................................................15
2.6 Population ..............................................................................................................16
3.0 TRIAL RATIONALE AND OBJECTIVES ..................................................................16
3.1 Rationale ................................................................................................................16
3.2 Objectives ..............................................................................................................17
4.0 TRIAL DESIGN...............................................................................................................17
4.1 Study Design/Type.................................................................................................17
4.2 Endpoints ...............................................................................................................18
4.3 Procedures to Minimize Bias .................................................................................19
4.4 Maintenance of Blinding Procedures .....................................................................19
4.5 Trial Treatment ......................................................................................................20
4.6 Duration .................................................................................................................21
4.7 Discontinuation ......................................................................................................22
5.0 SELECTION OF SUBJECTS ........................................................................................22
5.1 Inclusion Criteria ...................................................................................................22
5.2 Exclusion Criteria ..................................................................................................23
6.0 CLINICAL TRIAL PROCESSES AND PROCEDURES ...........................................24
6.1 Subject Screening and Randomization (Day -14 to -1) .........................................24
6.2 Treatment Period ....................................................................................................26
6.3 End of Treatment ...................................................................................................29
6.4 Follow Up Period ...................................................................................................30
6.5 Early Treatment Discontinuation ...........................................................................32
6.6 Assessments ...........................................................................................................32
6.7 Monitoring for Subject Compliance ......................................................................38
7.0 TREATMENT ..................................................................................................................39
7.1 Packaging, Labeling and Storage ...........................................................................39
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 4 Confidential Information 14-Jun-2013
7.2 Preparation of Investigational Product ...................................................................39
7.3 Administration of Investigational Product and Study Treatment(s) ......................40
7.4 Dose Modifications ................................................................................................42
7.5 Emergency Unblinding ..........................................................................................48
7.6 Concomitant Medications and Supportive Care ....................................................48
7.7 Investigational Product Accountability ..................................................................51
8.0 ADVERSE EVENTS .......................................................................................................51
8.1 Definitions..............................................................................................................51
8.2 Reporting Requirements ........................................................................................53
8.3 Criteria for Determining Adverse Event Severity .................................................54
8.4 Criteria for Determining Adverse Event Expectedness .........................................55
8.5 Criteria for Determining Adverse Event Causality ................................................55
8.6 Expedited Reporting of Serious Adverse Events ...................................................56
9.0 STATISTICAL PLAN .....................................................................................................56
9.1 Statistical Considerations .......................................................................................56
9.2 Statistical Methods .................................................................................................58
9.3 Schedule of Analyses .............................................................................................62
9.4 Termination Criteria...............................................................................................62
9.5 Deviation Reporting ...............................................................................................62
10.0 REGULATORY, QUALITY, AND ADMINISTRATIVE REQUIREMENTS .........63
10.1 Trial Conduct .........................................................................................................63
10.2 Ethical Considerations ...........................................................................................63
10.3 Investigator Responsibilities and Requirements ....................................................64
10.4 Data Identification, Handling, and Record Keeping ..............................................65
10.5 Quality Control and Quality Assurance .................................................................66
11.0 SUPPLEMENTS ..............................................................................................................67
11.1 ECOG Performance Status Assessment.................................................................68
11.2 Baseline Tumor Evaluation and Categorization: RECIST v1.1 ............................69
11.3 Response Assessment: immune-related RECIST (irRECIST) ..............................71
11.4 List of CYP3A4 Inhibitors and/or Inducers ...........................................................75
11.5 List of Abbreviations .............................................................................................76
12.0 LITERATURE AND REFERENCES............................................................................80
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 5 Confidential Information 14-Jun-2013
1.0 STUDY SYNOPSIS
Protocol Number VRXP-A202
Protocol Title A Randomized, Double-Blind, Placebo-Controlled Study of Chemotherapy Plus Cetuximab in Combination with VTX-2337 in Patients with Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck
Investigational Phase II
Investigational Product VTX-2337, a subcutaneously-administered Toll-like receptor 8 agonist
Study Sites Approximately 60 sites in North America
Study Duration Enrollment Period: Approximately 18 months Duration of Study: Approximately 36 months; following completion of accrual, all subjects will be followed for 12 months
Study Population Adults who have not previously received treatment for recurrent or metastatic squamous cell carcinoma of the head and neck
Study Design Randomized, double-blind, placebo-controlled, parallel group
Primary Objectives To compare the progression-free survival of subjects treated with cisplatin or carboplatin + fluorouracil (5-FU) + cetuximab combined with VTX-2337 to those treated with cisplatin or carboplatin + 5-FU + cetuximab alone (standard-of-care; SOC).
Secondary Objectives To compare the safety of subjects treated with SOC in combination with VTX-2337 to those treated with SOC alone. To compare the overall survival between the two treatment groups. To compare the best objective response rate (ORR), duration of best response (DOBR), disease control rate (DCR), and duration of disease control (DDC) between the two treatment groups.
Sample Size n=175
Inclusion Criteria Summary
1. Ability and willingness to provide written informed consent and to comply with the study’s visit and assessment schedule
2. Prior documentation of histologically or cytologically confirmed squamous cell carcinoma of the head and neck
3. Locoregionally recurrent or metastatic disease 4. At least one measurable lesion on screening CT or MRI 5. 18 years of age or older 6. ECOG performance status of 0 or 1 7. Acceptable bone marrow, renal, and hepatic function based upon screening
lab tests 8. Willingness to use medically acceptable contraception 9. For females with reproductive potential: a negative serum pregnancy test
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 6 Confidential Information 14-Jun-2013
Exclusion Criteria Summary
1. Disease which is amenable to curative local therapy 2. Nasopharyngeal, salivary gland, lip, or sinonasal carcinoma 3. Surgery or irradiation ≤ 4 weeks prior to randomization 4. Prior systemic anti-cancer therapy, unless administered for locally advanced
disease and completed ≥ 6 months prior to randomization 5. Treatment with an investigational agent ≤ 30 days prior to randomization 6. Treatment with oral or parenteral corticosteroids ≤ 2 weeks prior to
randomization or a requirement for chronic systemic immunosuppressive therapy for any reason
7. Prior serious infusion reaction to cetuximab 8. Treatment with an immunotherapy ≤ 30 days prior to randomization 9. Known brain metastases, unless stable for ≥ 28 days prior to randomization 10. Active autoimmune disease, defined as any autoimmune condition currently
requiring therapy 11. Known infection with HIV 12. Clinically significant cardiac disease ≤ 6 months prior to randomization 13. Pregnant or breast-feeding females 14. Any other condition or circumstance that could interfere with adherence to
the study requirements, or otherwise compromise the study’s objectives
Study Drug Dose and Administration
VTX-2337 or placebo (investigational product; IP) will be administered as a subcutaneous injection on Day 8 and Day 15 of a 21-day cycle at a dose level of 3.0 mg/m2 for 6 cycles, followed by dosing on Days 8 and 22 of a 28-day cycle for cycles 7 and beyond. IP will be administered until disease progression. Standard-of-Care will consist of the following:
1. Cisplatin (100 mg/m2) OR carboplatin (AUC 5 mg/mL/min) administered as an IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles.
2. 5-FU (1000 mg/m2) administered as a continuous IV infusion on Days 1–4 of a 21-day cycle for a maximum of 6 cycles.
3. Cetuximab (initial dose: 400 mg/m2; remaining doses: 250 mg/m2) administered weekly until disease progression.
On days when investigational product and cetuximab are both dosed, IP will be administered first, followed by the cetuximab infusion.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 7 Confidential Information 14-Jun-2013
Study Overview This is a randomized, double-blind, placebo-controlled, parallel group study to evaluate the safety and efficacy of VTX-2337 in combination with cisplatin or carboplatin, 5-FU and cetuximab in prolonging the progression-free survival in subjects with recurrent or metastatic squamous cell carcinoma of the head and neck. Subjects will be screened for eligibility and qualified subjects will be randomized 1:1 to 1 of 2 treatment groups:
− SOC + VTX-2337 − SOC + placebo
Tumor assessments will be by CT or MRI starting at Week 12 (± 3 days), then at Week 18 (± 3 days) and every 8 weeks (± 7 days) thereafter. Response will be evaluated by immune-related RECIST criteria (irRECIST) and confirmed by an independent radiologist. Upon independent confirmation of disease progression, active participation in the study is complete and subjects will undergo the End of Treatment evaluations. Subjects will be followed for survival until ~12 months after the last subject is randomized. Adverse events and safety will be evaluated throughout the study by an independent Data Safety Monitoring Board (DSMB). The DSMB will also conduct an assessment of the safety and tolerability of the starting dose.
Primary Outcome Measures
Progression-free survival will be assessed by serial imaging studies (CT or MRI) performed at baseline (Screening), Week 12 (± 3 days), Week 18 (± 3 days) and every 8 weeks (± 7 days) thereafter. Tumor response as evaluated by irRECIST. All tumor responses will be reviewed and confirmed by a central, independent radiologist. Whenever medically feasible and appropriate, suspected disease progression events should be confirmed by central review prior to completing the End of Treatment assessments and initiating new anti-cancer therapy.
Secondary Outcome Measures
Safety will be assessed by physician or subject report of adverse events. Overall survival will be determined by report of subject vital status. Objective response rate, duration of best response, disease control rate, and duration of disease control will be assessed by irRECIST and evaluated by independent radiologist.
Statistical Considerations Randomization of all subjects will be stratified by prior chemotherapy (yes or no), ECOG performance status (0 or 1), and platinum therapy as assigned by the investigator at the time of randomization (cisplatin or carboplatin). Sample size: n=175 subjects. Power, alpha and hazard ratio assumptions: see full protocol.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 8 Confidential Information 14-Jun-2013
2.0 BACKGROUND
Head and neck carcinomas (HNC) are the fifth most common cancer in the world, with increasing incidence.[1, 2] In the United States, 40,000 to 50,000 new cases are diagnosed and approximately 12,000 deaths due to this cause occur yearly.[2] HNCs describe malignancies of the upper aerodigestive tract which include squamous cell carcinomas of the oral cavity, nasopharynx, pharynx and larynx. While tobacco and alcohol use are the most common risk factors for HNCs, Epstein-Barr virus and human papilloma virus (HPV) may also play a role in the development of carcinomas of the nasopharynx and squamous cell carcinomas of the oropharynx, respectively.[1–6]
The majority of squamous cell carcinoma of the head and neck (SCCHN) cases (up to 75%) are diagnosed in its late stages (stages III or IV).[7, 8] Metastatic and recurrent SCCHN that is no longer amenable to local surgical/radiation therapy causes substantial morbidity and high mortality, with a median progression free survival (PFS) of ≤ 6 months due to the lack of effective therapeutic options.[9, 10, 11] Recurrent or metastatic disease has traditionally been managed with cytotoxic chemotherapies such as methotrexate, organoplatinum compounds, fluorouracil (5-FU), or taxanes—either alone or in combination. More recently, cetuximab (Erbitux®), the IgG1 monoclonal antibody which targets epidermal growth factor receptor (EGFR) was approved by FDA and Health Canada for use in combination with radiation therapy for the initial treatment of locally or regionally advanced SCCHN and by FDA for use as monotherapy in patients with recurrent or metastatic SCCHN who have progressed after platinum-based therapy and in combination with platinum-based therapy with 5-FU in patients with recurrent or metastatic SCCHN. Approval was based on clinical benefit and tolerability in the phase 3 setting.[12, 13] Namely, the addition of cetuximab to first-line platinum-based therapy with 5-FU resulted in an improvement of median overall survival (OS) from of 10.1 months compared to 7.4 months for patients treated with platinum/5-FU alone. As more than 90% of SCCHNs express the EGFR, targeting EGFR and its signaling pathway significantly advanced the treatment of SCCHN.[14] However, in this difficult-to-treat SCCHN population, the overall prognosis remains poor and the observed responses of 36% and a median time to progression of 5.6 months for cetuximab in combination with platinum and 5-FU are not ideal.[12, 13] Therefore, combinations that enhance response and provide clinical benefit, without significantly increasing toxicity, are still urgently needed.
One approach to enhance the efficacy of treatment with cetuximab plus chemotherapy in SCCHN is to add an immunomodulatory agent that would promote an anti-tumor immune response. Ideally, this agent would enhance both the effects of cetuximab (e.g., by augmenting antibody-dependent cellular cytotoxicity; ADCC) and chemotherapy (e.g., by modulating the tumor microenvironment and increasing T cell responses to antigenic debris generated by tumoricidal activity). One such candidate is VTX-2337, a modulator of Toll-like receptor 8
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 9 Confidential Information 14-Jun-2013
(TLR8). Activation of TLR8 enhances natural killer (NK) cells, myeloid-derived dendritic dendritic cells (mDC), and monocytes. VTX-2337 has demonstrated enhanced killing of SCCHN cells in combination with cetuximab, and synergistic activity with chemotherapy.[15]
The current study tests the hypothesis that the addition of VTX-2337 to the cetuximab plus platinum/5-FU regimen in locally recurrent and/or metastatic SCCHN patients will provide clinical benefit and will be reasonably well tolerated.
2.1 Investigational Agent
VTX-2337 is comprised of an active pharmaceutical ingredient (API) formulated at neutral pH in Captisol® (a cyclodextrin-based solubilizing agent). The API of VTX-2337 is VTX-378: a novel, small, organic molecule TLR8 agonist with a molecular weight of 458.6. VTX-2337 a lyophilized cake is supplied in sterile, single-use vials and is administered via subcutaneous injection.
The selectivity of this compound has been assessed in peripheral mononuclear cells (PBMC) and in cells engineered to express only a single TLR. In both PBMC and cell transfectants, VTX-2337 is highly selective for TLR8 with an EC50 of approximately 70 nM. VTX-2337 shows minimal activity for TLR7 (with an EC50 of approximately 3 μM), but does not stimulate other TLRs.[16]
Placebo contains Captisol and citric acid, the same excipient ingredients of the VTX-2337 formulation, but does not include the API VTX-378.
2.2 Nonclinical Data
Nonclinical studies have included in vitro and in vivo assessments of the pharmacologic, pharmacokinetic (PK), metabolism and toxicologic characteristics of VTX-2337. Extensive information regarding the pre-clinical evaluation of VTX-2337 may be found in the Investigator’s Brochure (IB).
2.2.1 Pharmacokinetics and Pharmacology
The PK and pharmacology of VTX-2337 have been broadly evaluated in non-human primates (cynomologus monkeys). The compound shows linear pharmacokinetics over a wide dose range, with a half-life (t1/2) of approximately 2–4 hours. VTX-2337 elicits the production of multiple inflammatory mediators—chemokines (e.g., MCP-1, MIP-1β), cytokines (e.g., IL-6, IL-1, TNFα, IL 12), acute phase proteins and shed cell surface antigens—which are consistent with activation of the innate immune system and can be readily measured in plasma. A clear pharmacokinetic-pharmacodynamic (PK/PD) relationship is observed for many of these inflammatory markers.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 10 Confidential Information 14-Jun-2013
Refer to §2.3 for information regarding PK/PD data in patients.
2.2.2 In Vitro ADCC and NK Observations
To characterize the potential for VTX-2337 to modulate immune function beyond the characterization in PD studies, immunophenotyping of peripheral blood and NK cell cytotoxic activity was assessed. These in vivo studies demonstrated that administration of VTX-2337 results in transient changes in blood cell populations consistent with cellular activation of neutrophils, NK cells, and T cells and may result in the transient extravasation of these latter cell populations from the blood compartment.[16]
In addition, VTX-2337 stimulates the production of cytokines from mDC, monocytes, and NK cells in vitro.[17] VTX-2337 stimulates ADCC when used in combination with a variety of monoclonal antibodies of the IgG1 subclass including rituximab and traztuzumab.[17] More recently, in collaboration with Dr. Robert Ferris at the University of Pittsburgh, it was demonstrated that VTX-2337 increases the cetuximab-mediated killing of SCCHN targets in an NK-dependent manner.[18] The TLR8 and NK-dependent enhancement of ADCC occurs in samples from patients of all three FcRγ3a genotypes, including those with the allele encoding the homozygous F/F variant that is associated with lower affinity for the Fc receptor.
In addition, the stimulation of mDC and monocytes concurrent with cetuximab administration was tested to determine the promotion of development of EGFR-specific T cells via a mechanism referred to as ‘cross-priming’. Using a mixed culture model in vitro, tetramer analysis (using a molecular reagent that detects human leucocyte antigen-specific, EGFR peptide specific CD8+ T cells) demonstrated that VTX-2337 stimulates cross-priming and increases the number of EGFR-specific CD8+ T cells following cetuximab treatment.
Taken together, the ability of VTX-2337 to stimulate the production of inflammatory cytokines (including IL-1, IL-18, TNFα, IL-12, and IFNg), the activation and stimulation of NK cells and ADCC, and the activation of the antigen processing and presentation of mDC and monocytes provide a strong rationale that this TLR8 agonist may enhance the activity of cetuximab in clinical studies.
2.2.3 Toxicology
In conjunction with FDA requirements, standard toxicology studies were performed with the aim of inducing and identifying drug-related toxicities. The clinically relevant toxicities observed in these studies were mechanistically based; that is, attributed to activation of the innate immune system via TLR8. The most frequent of these included transient constitutional symptoms consistent with the influenza-like response frequently seen with immunomodulatory agents. As noted in §2.3, these flu-like symptoms identified in preclinical toxicology studies have
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 11 Confidential Information 14-Jun-2013
subsequently been observed in clinical trials of VTX-2337, and include pyrexia, chills, myalgia, and fatigue.
As detailed in the VTX-2337 IB, organ-based toxicity was also observed in preclinical toxicology studies. Organ-based toxicities have not been observed in any clinical trial of VTX-2337 to date, and are not described herein.
2.3 Clinical Data 2.3.1 Phase I Solid Tumor: VTX-2337 Monotherapy (VRXP-A101)
VTX-2337 was first evaluated clinically as a stand-alone agent in a Phase I standard dose-escalation study to assess the safety, tolerability and biological activity of the compound in late-stage cancer patients. At doses ranging from 0.1–3.9 mg/m2, VTX-2337 was well tolerated overall, with the predominant adverse events being transient grade 1 or 2 fever, chills, flu-like symptoms, nausea and vomiting, anorexia, and injection site reaction. No significant drug-related hematologic, gastrointestinal, neurologic or cardiac toxicities were observed. At the highest dose evaluated, 3.9 mg/m2 (cohort 8; n=8) a single subject experienced a dose-limiting toxicity (DLT) of grade 3 hypotension associated with grade 2 cytokine release syndrome (CRS), from which the subject recovered completely. Accordingly, the maximum dose evaluated in this study (3.9 mg/m2) was adequately well tolerated. Overall, VTX-2337 was found to be well tolerated when administered subcutaneously weekly for 3 weeks of a 4-week cycle.
The PK of VTX-2337 were assessed in all subjects (n=33) and demonstrated dose-dependent exposure. With subcutaneous administration, VTX-2337 was rapidly absorbed into systemic circulation as well as rapidly cleared, with mean Tmax ranging from 0.5–0.7 hours and t½ ranging from 1.7–7.1 hours. Peak plasma levels and total systemic exposure were generally dose-proportional.
The biological activity (cytokines, chemokines and other inflammatory markers, including those indicative of TLR8 activation) of VTX-2337 was assessed in all subjects. Biological activity of VTX-2337 was shown to be dose dependent, with the robust induction of multiple inflammatory markers in all subjects receiving doses ≥ 2.0 mg/m2.
Clinical responses were assessed by response evaluation criteria in solid tumors (RECIST) at 8 weeks. No complete responses (CR) or partial responses (PR) were seen in the study, but approximately 25% of subjects had evidence of stable disease (SD) at 8 weeks. It should be noted that VTX-2337 is anticipated to have stand-alone biological activity, but is not anticipated to induce a CR or PR as a single agent.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 12 Confidential Information 14-Jun-2013
The doses selected from this study to be used in combination studies were 2.5, 3.0, and 3.5 mg/m2. All of these doses are expected to be biologically active based on the biomarker data from VRXP-A101.
2.3.2 Phase 1 SCCHN: VTX-2337 with Cetuximab (VRXP-A103)
This ongoing, single-center phase 1b protocol at Seattle Cancer Care Alliance (Seattle, WA) is being conducted as an Investigator Sponsored Trial, with Laura Chow, MD as the Sponsor-Investigator.
VRXP-A103 assesses the safety and tolerability of VTX-2337 in combination with cetuximab. Cetuximab is administered weekly and VTX-2337 is administered weekly for three weeks of a four-week cycle. Three dose levels of VTX-2337 will be evaluated in a standard dose-escalation schema: 2.5 mg/m2, 3.0 mg/m2 and 3.5 mg/m2.
Ten subjects with recurrent or metastatic SCCHN have been enrolled. The study regimen has been safe and adequately tolerated to date. There have been no dose-limiting toxicities; no serious, unexpected drug-related adverse events; and no evidence of synergistic toxicities between cetuximab and VTX-2337. Clinical tolerability data indicate that long-term dosing at 3.0 mg/m2 will be better tolerated than 3.5 mg/m2.
Preliminary translational medicine results are available from the first two cohorts of SCCHN subjects who received VTX-2337 (2.5 and 3.0 mg/m2) in combination with cetuximab. Consistent with the data from the Phase 1 VRXP-A101 study, serum biomarkers consistent with TLR8 activation were readily measured at both dose levels. In additional, ex vivo analysis of NK cells collected pre-dose and 24 hours after dosing demonstrate NK cell activation. Given the proposed mechanism of VTX-2337 enhancing ADCC with cetuximab in an NK-dependent manner, these data provide important correlative information and suggest the doses of 2.5 or 3.0 mg/m2 are sufficient from a pharmacologic perspective.
Based on preliminary efficacy data, eight of the 10 subjects have been eligible for evaluation of tumor response: one subject achieved a partial response, 2 subjects experienced disease stabilization, 3 subjects had disease progression, two subjects have not yet had a response assessment, and 2 subjects discontinued the study prematurely and were unevaluable for response assessment.
2.3.3 Phase 1 Ovarian Cancer (VTX-2337 with Chemotherapy)
Study VRXP-A102 (GOG-9925) was a phase I study conducted in collaboration with Gynecologic Oncology Group (GOG). The study separately assessed two treatment regimens containing VTX-2337 in women with recurrent ovarian cancer. Regimen 1 evaluated pegylated
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 13 Confidential Information 14-Jun-2013
liposomal doxorubicin (PLD, Doxil®; 40 mg/m2) plus VTX-2337 at three dose levels: 2.5 mg/m2, 3.0 mg/m2, and 3.5 mg/m2. Regimen 2 consisted of weekly paclitaxel (80 mg/m2) plus VTX-2337 (3.0 mg/m2).
In both of the regimens evaluated, there were no dose-limiting toxicities; no serious, unexpected drug-related adverse events; and no evidence of synergistic toxicities between PLD plus VTX-2337 or paclitaxel plus VTX-2337. PD data confirm the biological activity of VTX-2337 in both regimens at all dose levels, with biomarker responses indicative of TLR8 stimulation and immune activation.
To date, 20 subjects have been treated: 13 on Regimen 1 and 7 on Regimen 2. On Regimen 1, one subject enrolled based on biochemical evidence of recurrent disease achieved a complete biochemical response, one subject with non-measureable disease achieved a complete response, 7 subjects had stable disease, and 3 subjects had progressive disease (including one subject with non-target disease [biochemical recurrence only] who had biochemical progression). One subject did not complete the first cycle and was not evaluable for efficacy. On Regimen 2, four of the 7 subjects had disease progression, while 3 experienced disease stabilization (including 1 subject who remains on study).
Two of the 7 subjects enrolled in Regimen 1 at the 3.5 mg/m2 dose level of VTX-2337 withdrew from treatment or had a dose reduction due to grade 2 or 3 drug-related events (e.g., chills, fatigue, nausea, vomiting, fever). These events suggest that long-term dosing of VTX 2337 at 3.5 mg/m2 is not clinically optimal. Based on this information, and the adequate biological activity of VTX-2337 at 2.5 and 3.0 mg/m2, the selection of 3.0 mg/m2 of VTX-2337 was recommended as the optimal dose for the randomized, Phase 2 study.
2.3.4 Phase 2 Ovarian Cancer (VTX-2337 with Chemotherapy)
GOG-3003 is a randomized, placebo-controlled, ongoing Phase 2 study designed to evaluate VTX-2337 (3.0 mg/m2) in combination with PLD in patients with recurrent or persistent epithelial ovarian, fallopian tube, or primary peritoneal cancer. The study will evaluate the overall survival of VTX-2337 in combination with PLD compared to PLD alone in approximately 210 subjects. PFS, response rate, and safety of the combination are key secondary endpoints. This multicenter study is being conducted in approximately 80 clinical sites in the United States, in collaboration with the GOG. Enrollment in this study is currently ongoing.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 14 Confidential Information 14-Jun-2013
2.4 Risks/Benefits 2.4.1 Potential Risks
In previously published trials of platinum, 5-FU, and cetuximab the most common adverse events (AE) overall were skin reactions, headache, diarrhea, infection, and nausea. The most common grade 3 or 4 adverse events were anemia, neutropenia, and thrombocytopenia. Less commonly, dosing with cetuximab may result in a serious infusion reaction requiring medical intervention and immediate, permanent discontinuation with cetuximab.[12]
The most common AE associated with VTX-2337 when administered as a single-agent is grade 1 or 2 injection site reaction. The most common systemic drug-related adverse events are transient grade 1 or 2 chills, flu-like symptoms, fever, nausea, and vomiting; these transient symptoms typically last < 48 hours. Less commonly, dosing with VTX-2337 may result in CRS, which is most likely to be grade 1, but more severe reactions are possible. Similarly, the most common AEs reported in patients receiving VTX-2337 in combination with cetuximab were grade 1 and 2 injection site reactions, flu-like symptoms, nausea, fatigue, vomiting, cough, malaise, and dyspnea.
Potential long-term clinical effects of VTX-2337 are unknown and cannot be reliably predicted. However, several subjects in clinical trials have received up to 8 cycles (24 individual weekly doses) of VTX-2337 without unanticipated problems. Investigators will be informed of any newly-identified risks associated with VTX-2337, if they occur.
Although the combinations of VTX-2337 plus chemotherapy (PLD, paclitaxel) and VTX-2337 plus cetuximab did not demonstrate any dose-limiting or synergistic toxicities, VTX-2337 has not previously been studied in combination with platinum plus 5-FU plus cetuximab. While no new or unexpected or synergistic toxicities are anticipated, the safety of this combination will be carefully evaluated by an independent data safety monitoring board (DSMB) (see also §9.2.2).
Overall, at the dose level to be administered in this clinical trial (≤ 3.0 mg/m2), VTX-2337 treatment-related toxicities are expected to be transient and consistent with those events commonly associated with an activated immune response. This includes symptoms of chills, fever, flu-like syndrome, headache, nausea, vomiting, and local injection site reaction.
2.4.2 Potential Benefits
The efficacy of VTX-2337 has not been formally evaluated in clinical trials to date. However, exploratory data from study VRXP-A101 showed 25% of the 33 subjects enrolled had disease stabilization at 8 weeks. In addition, preliminary data from a phase 1b study of VTX-2337 in combination with cetuximab in patients with advanced SCCHN (n=10) included 1 subject who
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 15 Confidential Information 14-Jun-2013
experienced a partial response, 2 subjects who experienced disease stabilization; two subjects were not evaluable and 2 subjects have not yet had a tumor evaluation. Furthermore, a phase 1b study of VTX-2337 with chemotherapy in women with recurrent, platinum-resistant ovarian cancer (n=20) included 2 subjects who experienced complete response (one of which was a biochemical CR) and 10 subjects who experienced disease stabilization (2–8 months).
The current study of VTX-2337 is a multi-dose study to assess the safety, tolerability and efficacy of the investigational drug in combination with cisplatin or carboplatin, 5-FU, and cetuximab. The clinical efficacy of this combination has not yet been evaluated; however, the addition of VTX-2337 to the standard-of-care (SOC) treatment regimen may be more effective than SOC alone.
Participating subjects may also benefit from the personal satisfaction of participating in an investigative process that will contribute information regarding the investigational product (IP) that may help patients afflicted with SCCHN.
2.5 Dose Rationale
The selection of the starting dose for this study, as well as the Phase 2 study in ovarian cancer (3.0 mg/m2) was based on data from the initial phase 1 study of VTX-2337 used as a single agent, and data from the two Phase 1b studies combining VTX-2337 with cetuximab in SCCHN patients and with PLD or paclitaxel in ovarian cancer patients, respectively. These studies showed that VTX-2337 is biologically active in some subjects at doses as low as 0.4 mg/m2 based on biomarker data as previously described. Biological activity of VTX-2337 was shown to be dose dependent. At VTX-2337 doses ≥ 2.0 mg/m2, nearly all subjects evaluated have a robust biological response, as indicated by the induction of multiple inflammatory markers consistent with activation of TLR8. In study VRXP-A103, where cellular responses were assessed, VTX-2337 in combination with cetuximab at doses ≥ 2.5 mg/m2 (the lowest dose tested) was associated with cellular responses including NK cell activation.
While no DLTs have been observed at 3.5 mg/m2 in either the cetuximab or chemotherapy combination studies, treating investigators have reported reduced tolerability at 3.5 mg/m2 compared to 3.0 mg/m2. This has included higher fevers, more intense flu-like symptoms, and more persistent injection site reactions. Based on its clear biological activity and improved long-term tolerability, as well as the lack of dose-limiting or synergistic toxicities, 3.0 mg/m2 has been selected as the appropriate dose for Phase 2 studies of VTX-2337 in combination with chemotherapy.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 16 Confidential Information 14-Jun-2013
2.6 Population
This study will be conducted in adult subjects with recurrent or metastatic SCCHN who have not previously received treatment for their recurrent or metastatic disease. Eligible subjects will have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 and adequate hematologic, renal and hepatic function. This study will not include subjects with disease which is amenable to local therapy or who have received recent treatment for their disease.
Refer to §5.0 for specific eligibility requirements for subjects.
3.0 TRIAL RATIONALE AND OBJECTIVES 3.1 Rationale
Recurrent or metastatic SCCHN is an aggressive disease with few treatment options with proven clinical benefit. The use of the EGFR-specific monoclonal antibody cetuximab in combination with platinum and 5-FU based chemotherapy has demonstrated clinical benefit in these patients. Still, the response rate (30-40%), delay in disease progression (overall PFS of approximately 6 months) and OS (approximately 11-12 months in this treated population) leave room for considerable improvement. Ideally, an agent could be added to this regimen that would provide additive or synergistic clinical benefit without dramatically increasing the toxicity of this drug combination. In this regard, an immunomodulatory agent that increases the activity of cetuximab and/or the chemotherapy backbone would be potentially beneficial.
VTX-2337 is a small molecule agonist of TLR8 that stimulates specific immune cell populations including mDC, monocytes, and NK cells. In a variety of cell culture based and animal studies, VTX-2337 has been shown to enhance ADCC in the context of a variety of IgG1-isotype monoclonal antibodies including cetuximab. The enhancement of ADCC occurs across all FcRg3a genotypes—including those associated with lower affinity to FcR and associated lower clinical responses in patients. Via the stimulation of various antigen presenting cells, VTX-2337 enhances the generation of tumor-antigen specific CD8+ T cells and has been found to enhance the tumoricidal activity of certain chemotherapy regimens. In addition, VTX-2337 stimulates the production of a variety of inflammatory cytokines and chemokines that would be expected to modulate the tumor microenvironment. These functions of VTX-2337 are consistent with the role of its receptor—TLR8—as a sentinel of viral infection and the expression of a ‘danger’ signal to rid the host of an unwanted intruder.
VTX-2337 has been evaluated as a single-agent in cancer patients (n=33) to determine the biological activity and safety profile of this novel compound. VTX-2337 has also been evaluated in several combination studies with cetuximab (n=10), PLD (n=13), and paclitaxel (n=7) to address the safety and activity of this agent in combination with SOC anticancer regimens.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 17 Confidential Information 14-Jun-2013
Collectively, these data provide a rationale for continued study of VTX-2337 at the selected dose in larger, randomized clinical trials to determine if this compound provides clinical benefit.
As of yet, the anti-tumor effects of VTX-2337 in combination with platinum-based therapy with 5-FU and cetuximab have not been evaluated. However, as VTX-2337 may enhance therapeutic responses to platinum-5-FU chemotherapy with cetuximab; this combination is a promising combination that should be explored for its potential for improved anti-tumor effects in this patient population.
3.2 Objectives
The purpose of this study is to compare the safety and efficacy of SOC in combination with VTX-2337 to those treated with SOC alone in subjects with recurrent or metastatic SCCHN. Efficacy objectives include comparing the PFS, OS, objective response rate (ORR), duration of best response (DOBR), disease control rate (DCR), and duration of disease control (DDC) of the two treatment groups. The PD of VTX-2337 will also be evaluated.
4.0 TRIAL DESIGN 4.1 Study Design/Type
This is a randomized, double-blind, placebo-controlled, parallel-group study. The study consists of screening (≤ 14 days1), initial treatment (cycles 1–6), subsequent treatment (cycles 7+), and long-term follow-up. Following the screening period, qualified subjects will be randomized in a 1:1 ratio to receive SOC plus placebo or SOC plus VTX-2337. Randomization of all subjects will be stratified by receipt of prior chemotherapy (yes or no), ECOG performance status (0 or 1), and platinum therapy as assigned by the investigator at the time of randomization (cisplatin or carboplatin).
Subjects will then be administered cisplatin or carboplatin—as assigned by the investigator prior to randomization—5-FU, cetuximab, and IP (i.e., VTX-2337 or placebo) on pre-specified days of a 21-day cycle for 6 cycles (§6.0). Thereafter, subjects will continue on study for cycles 7+ for dosing of weekly cetuximab and biweekly IP in 28-day cycles.
Subjects will be evaluated for PFS according to immune-related Response Evaluation Criteria In Solid Tumors (irRECIST; §6.6.1.2) at Week 12 (± 3 days), Week 18 (± 3 days), and every 8 weeks (± 7 days) thereafter. Treatment will be discontinued for subjects with independently-confirmed radiographic disease progression. Upon discontinuation of treatment, subjects will complete the End of Treatment visit and will be followed for survival.
1 Baseline imaging may be performed within 28 days of randomization.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 18 Confidential Information 14-Jun-2013
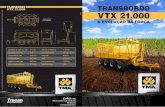
Figure 1: Study Schema
4.2 Endpoints 4.2.1 Primary Endpoint(s)
The primary endpoint of the study is to compare the PFS of patients with recurrent or metastatic SCCHN treated with VTX-2337 plus SOC versus patients treated with SOC alone using irRECIST evaluated by independent radiology review.
4.2.2 Secondary Endpoint(s)
The secondary endpoints of the study are to compare the following between the two treatment groups:
• Safety as measured by adverse events, including clinically significant changes in physical examination, peripheral blood hematology, serum chemistry, urinalysis, and ECG.
• The OS of patients with recurrent or metastatic SCCHN.
• The ORR, DOBR, DCR, and DDC of patients with recurrent or metastatic SCCHN using irRECIST evaluated by independent radiology review.
4.2.3 Exploratory Endpoint(s)
The exploratory endpoints of this study are as follows:
• To compare genetic polymorphisms that may impact the response of patients to a TLR8 agonist or to cetuximab between the two treatment groups.
• To compare immune biomarker response as measured by a multiplexed panel of cytokines, chemokines, and inflammatory markers between the two treatment groups.
Subsequent Treatment Cycles 7+
Initial Treatment 6 Cycles (18 Weeks)
Screening< 14 Days
Screening
SOC + VTX-2337
SOC + Placebo
Rand
omiza
tion
Cetuximab + Placebo
Cetuximab + VTX-2337
Follow Up
Dise
ase
Prog
ress
ion
Survival Follow-Up
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 19 Confidential Information 14-Jun-2013
• To compare the effect of immune cell subsets within the tumor on response to treatment and/or clinical outcome, as measured by immunohistochemistry in primary tumor tissue between the two treatment groups.
• To assess the PK of VTX-2337.
4.3 Procedures to Minimize Bias
The study design and methods were selected to minimize bias. This is a randomized, double-blind, placebo-controlled study.
All subjects will receive SOC treatment; in addition, subjects will be randomly assigned in a 1:1 ratio to one of two treatment arms: SOC + VTX-2337 or SOC + placebo. To ensure that both known and unknown confounding factors are evenly distributed between treatment groups randomization of all subjects will be stratified by prior chemotherapy (yes or no), ECOG performance status (0 or 1), and platinum therapy, as assigned by the investigator at the time of randomization (cisplatin or carboplatin). Neither the investigators nor the subjects know to which treatment group a subject is assigned.
The labeling, packaging, and distribution of VTX-2337 and placebo will be identical so that the clinical site personnel remain blinded to study treatment. Placebo will be utilized to ensure that subjects, investigators, and all other study personnel will remain blinded to the study treatment.
In order to minimize potential bias and variability from individual radiology reviewers, radiologic assessment of tumor response will be performed via central radiology review. The central reviewers are blinded to study treatment and are independent from the clinical sites.
4.4 Maintenance of Blinding Procedures
All clinical, regulatory, and safety personnel at the contract research organization (CRO) and sponsor, as well as all investigators and clinical site staff, will remain blinded to the study treatment assignment. Members of the data safety monitoring board (DSMB) may be unblinded; an unblinded statistician, independent from the project team, will provide support to the DSMB. Additionally, individuals with access to the randomization schema and IP kit assignments will remain separate from the study personnel responsible for day-to-day operations and evaluation of the clinical data. Refer to §7.5 for emergency unblinding procedures.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 20 Confidential Information 14-Jun-2013
4.5 Trial Treatment
Subjects randomized in the study will be administered all of the following:
• IP (i.e., VTX-2337 or placebo)
• Cetuximab
• Cisplatin or carboplatin (as assigned by the investigator)
Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent should be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject.
• Fluorouracil (5-FU)
When cetuximab is administered on the same day as chemotherapy, cetuximab administration will be completed ≥ 1 hour prior to administration of platinum and 5-FU. When cetuximab is administered on the same day as IP, the dose of IP will be given prior to cetuximab.
Please refer to §7.0 for additional information regarding subject treatment procedures.
4.5.1 Investigational Product Treatment
Subjects will receive IP at a dose of 3.0 mg/m2 (see also §9.2.2) given as a subcutaneous injection on Days 8 and 15 of a 21-day cycle for up to 6 cycles. Following the 6th cycle, subjects will continue to receive IP on Days 8 and 22 of a 28-day cycle until disease progression. (§7.3.1)
4.5.2 Cetuximab Treatment
On Cycle 1 Day 1, subjects will receive an initial cetuximab dose of 400 mg/m2 given as a 2-hour intravenous (IV) infusion. This will be followed by weekly cetuximab doses of 250 mg/m2 given as a 1-hour IV infusion. Weekly treatment with cetuximab will continue until disease progression. (§7.3.2)
Cetuximab will be administered in a manner consistent with the current labeled dosing regimen. Please refer to the cetuximab label for additional information.
4.5.3 Platinum Treatment
The platinum therapy (cisplatin or carboplatin) is assigned to each subject at the discretion of the investigator. Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent must be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject. Reasonable efforts
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 21 Confidential Information 14-Jun-2013
should be made to keep the subject on the platinum therapy originally assigned; however, the platinum therapy may be changed if clinically necessary. (§7.3.3)
Cisplatin Treatment
Subjects will receive 100 mg/m2 of cisplatin as a 1-hour IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles. Cisplatin administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the cisplatin label for additional information.
Carboplatin Treatment
Subjects will receive carboplatin at an AUC of 5 mg/mL/min as a 1-hour IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles. The carboplatin dose will be based upon the subject’s screening glomerular filtration rate (GFR) in mL/min. The Calvert formula will be used for carboplatin dosing:
Total Dose (mg) = (target AUC) x (GFR + 25)
Carboplatin administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the carboplatin label for additional information.
4.5.4 5-FU Treatment
Subjects will receive a continuous IV infusion of 5-FU at a dose of 1000 mg/m2/day on Days 1–4 of a 21-day cycle for a maximum of 6 cycles. 5-FU administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the 5-FU label for additional information.
4.6 Duration
The enrollment period of the study is expected to be approximately 18 months, followed by a 12-month follow up period.
The duration of participation will vary among individual subjects due to factors such as disease progression and time of enrollment. After providing written informed consent, subjects will be screened for eligibility within 14 days of randomization (28 days for imaging) according to the procedures outlined in §6.1. Eligible subjects will be randomized into the study and will receive treatment as described in §6.2 and §7.0. Subjects will receive therapy until independently-confirmed disease progression per irRECIST. Thereafter, subjects will be followed long-term for survival.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 22 Confidential Information 14-Jun-2013
4.7 Discontinuation
Enrollment in the study will end when approximately 175 subjects have been randomized and have received at least one dose of IP. The sponsor may terminate enrollment in the study at any time for any reason.
Whenever possible, enrolled subjects should complete the study per protocol. However, individual subjects may withdraw from the study prematurely at any time, (e.g., subject decides to discontinue participation due to an adverse event, whether or not related to IP). Subjects who are noncompliant with the study’s requirements may also be removed from the study at any time by the investigator or study sponsor. Regardless of reason for discontinuing the study prematurely, the End of Treatment evaluations should be completed and the subject should be followed for survival, whenever feasible.
Please refer to §6.5 for early discontinuation of individual subjects.
5.0 SELECTION OF SUBJECTS
This study will enroll adult male and female subjects with recurrent or metastatic SCCHN who have not previously received treatment for their recurrent or metastatic SCCHN. All patients considered for enrollment and the reason(s) any screened subject is determined to be ineligible, must be documented. Written informed consent with an IRB/IEC-approved Informed Consent Form (ICF) must be obtained from all subjects prior to undergoing any study-specific procedures, including the discontinuation of any medication(s).
Subjects must meet all of the following eligibility criteria at the time of randomization.
5.1 Inclusion Criteria
1) Ability and willingness to provide written informed consent and to comply with the study’s visit and assessment schedule
2) Prior documentation of histologically or cytologically confirmed squamous cell carcinoma of the head and neck
Patients with squamous cell carcinoma of an unknown primary are eligible provided they previously received treatment for their locoregional head and neck cancer
3) Locoregionally recurrent or metastatic disease
4) At least one measurable lesion as defined by RECIST v1.1 (§11.1) on screening computed tomography (CT) or magnetic resonance imaging (MRI)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 23 Confidential Information 14-Jun-2013
5) 18 years of age or older
6) ECOG performance status of 0 or 1
7) Acceptable bone marrow, renal, and hepatic function based upon screening lab tests as demonstrated by the following:
− White blood cell (WBC) count > 2,500 cells/Μl
− Absolute neutrophil count (ANC) > 1,500 cells/μL
− Platelet count ≥ 100,000 cells/μL
− Hemoglobin ≥ 9 g/dL
− Creatinine WNL OR Creatinine Clearance > 60 mL/min
− Total bilirubin ≤ 2.0 x ULN
− SGOT (AST), SGPT (ALT) ≤ 2.5 x ULN or
≤ 5 x ULN in presence of liver metastases
− Potassium ≥ LLN
8) Willingness to use medically acceptable contraception throughout the study period and for 4 weeks after the final administration of IP
9) For female subjects with reproductive potential: a negative serum pregnancy test
5.2 Exclusion Criteria
1) Disease which is amenable to curative local therapy
2) Nasopharyngeal, salivary gland, lip, or sinonasal carcinoma
3) Surgery or irradiation within 4 weeks of randomization
4) Prior systemic anti-cancer therapy, unless administered for locally advanced disease and completed at least 6 months prior to randomization
5) Treatment with an investigational agent within 30 days of randomization
6) Treatment with oral or parenteral corticosteroids within 2 weeks of randomization or a requirement for chronic systemic immunosuppressive therapy for any reason
7) Prior serious infusion reaction to cetuximab
8) Treatment with an immunotherapy within 30 days of randomization
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 24 Confidential Information 14-Jun-2013
9) Known brain metastases, unless stable for at least 28 days prior to randomization
10) Active autoimmune disease, defined as any autoimmune condition currently requiring therapy (e.g., systemic lupus erythematosus, multiple sclerosis, inflammatory bowel disease, rheumatoid arthritis)
11) Known infection with HIV
12) Clinically significant cardiac disease (e.g., congestive heart failure, unstable or uncontrolled angina, myocardial infarction) within 6 months of randomization
13) Pregnant or breast-feeding females
14) Any other condition or circumstance that could interfere with adherence to the study’s procedures or requirements, or otherwise compromise the study’s objectives
6.0 CLINICAL TRIAL PROCESSES AND PROCEDURES
The schedules of study visits, procedures and assessments are in Table 1.
Subjects will receive study treatment, as described in §7.0. Please refer to §6.5 for requirements for individual subjects who discontinue study treatment prematurely. Unscheduled evaluations may be done at the discretion of the investigator as needed to assess the subject’s clinical status. All scheduled visits and procedures must be conducted at the study site of the Principal Investigator as indicated on the FDA Form 1572.
The imaging technique used for each subject (CT or MRI) is at the discretion of the investigator, but the same technique must be used for each individual subject throughout the study. Imaging should not be delayed in case of missed doses or dose delays.
All study-required laboratory evaluations must be performed by the central laboratories using the provided kits. All visit windows should be calculated from Cycle 1 Day 1.
6.1 Subject Screening and Randomization (Day -14 to -1) 6.1.1 Screening Procedures
Subjects with recurrent or metastatic SCCHN may be screened for this study. Prior to the initiation of screening procedures, informed consent will be obtained from each subject as described in §10.2.1.
Upon completion of the informed consent process, sites will register the subject in the interactive voice/web response system (IXRS); IXRS will assign a unique screening number to each subject. The screening number will be comprised of the three-digit site number followed by a three-digit,
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 25 Confidential Information 14-Jun-2013
sequential number (e.g., 123901, 123902). Upon randomization, a unique randomization number will be assigned by IXRS; the randomization number will be used as the subject number for the duration of the study.
The following procedures are required for screening and may be done at any time in the 14 days prior to randomization, unless otherwise specified:
• Complete medical history, including
— Concomitant medications and history of prior anticancer interventions
— Histological or cytological confirmation of SCCHN1
— Tumor staging according to the TNM Classification of Malignant Tumors
— HPV status for patients with oropharyngeal carcinoma only
If HPV status is not available in the subject’s medical history, testing for HPV status by p16 immunohistochemistry should be conducted at the time of screening
• Complete physical exam (PE), including vital signs (temperature, T; blood pressure, BP; respiration rate, RR; heart rate, HR), assessment of ECOG performance status (§11.1), weight and height
• Obtain 12-lead electrocardiogram (ECG)
• Collect blood samples for the following analyses:
— Complete blood count (CBC)
— Serum chemistry
— Serum pregnancy test (females with reproductive potential2 only)
— Pharmacogenetics
• Collect urine for urinalysis
• CT or MRI of the neck, chest, upper abdomen, and other anatomic region(s) of disease according to the requirements delineated in the VRXP-A202 Imaging Manual within 28 days of randomization
1 For patients with unknown primary who have previously received treatment for locoregional head and neck cancer, histological or cytological confirmation of squamous cell carcinoma is acceptable. 2 Females who are premenopausal or ≤ 2 years postmenopausal and not surgically sterile
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 26 Confidential Information 14-Jun-2013
• Submit a tissue sample from the primary tumor for all randomized subjects. When possible, re-biopsy at screening of primary tumor or metastatic tissue is preferred; however, archive tumor tissue may be used in absence of re-biopsy. If a tumor tissue sample is not available, sites should notify the sponsor or its representative prior to study entry.
A representative paraffin-embedded block of tissue from the original (diagnostic) biopsy and/or repeat biopsies will be submitted. If blocks cannot be submitted, 20 unstained slides plus one H&E stained 5-micron sections mounted on positively-charged glass slides are acceptable.
6.1.2 Randomization (Enrollment) Procedures
Subjects who have completed all screening assessments and are deemed eligible may be randomized (enrolled) up to 1 business day prior to Cycle 1 Day 1. Randomization of all subjects will be stratified by the receipt of prior chemotherapy (yes or no), ECOG performance status (0 or 1), and platinum therapy, as assigned by the investigator at the time of randomization (cisplatin or carboplatin).
Upon randomization, sites will be provided the subject’s randomization number and medication ID number. Randomization will also prompt an order for IP to be placed. A subject specific kit of IP will arrive approximately 3–4 business days after randomization.
6.2 Treatment Period
The treatment period is split into two phases: initial treatment and subsequent treatment. Initial treatment consists of six 21-day cycles where subjects receive the following per cycle:
• A single dose of cisplatin or carboplatin (Day 1)
• A continuous infusion of 5-FU (Days 1–4)
• Three doses of cetuximab (Days 1, 8 and 15)
• Two doses of IP (Days 8 and 15)
Cycles 7+ consist of 28-day cycles where subjects receive the following per cycle:
• Four weekly doses of cetuximab (Days 1, 8, 15, and 22)
• Two doses of IP (Days 8 and 22)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 27 Confidential Information 14-Jun-2013
Treatment continues until the subject has PD. Upon independent confirmation of radiographic disease progression and completion of treatment, subjects will complete the End of Treatment visit (§6.3) and begin long-term follow-up.
6.2.1 Initial Treatment (Cycles 1–6)
Study Cycles 1–6, Day 1 (CX.D1) (±2 days)
• Within 72 hours prior to treatment, collect blood samples for the following analyses:
— CBC
— Serum chemistry
• Problem-oriented PE, including vital signs (T, BP, RR, HR), ECOG performance status assessment and weight
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
— Cisplatin or carboplatin
— 5-FU
• Assess adverse events1 and update concomitant medications
Study Cycles 1–6, Days 2–4 (CX.D2-4) (±0 days)
• Continue 5-FU infusion according to the procedures in §7.3
Study Cycles 1–6, Days 8 and 15 (CX.D8; CX.D15) (±1 day)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
On Cycle 1 Day 8 and Cycle 3 Day 8 Only the assessments noted below will be completed. PK samples will only be collected on C1D8, not C3D8. Cetuximab administration will begin AFTER the 1 hour post-dose ECG and blood collection are completed.
1 DLTs will be assessed for all subjects, until at least six subjects randomized to receive VTX-2337 have received one cycle of treatment and the DSMB has completed the assessment of the starting dose. (§9.2.2)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 28 Confidential Information 14-Jun-2013
• Pre-dose
— Collect blood sample for PK assessment (C1D8 only)
— Collect blood sample for immune biomarker assessment
• 45 minutes post IP dose (±15 min)
— Collect blood samples for PK assessment (C1D8 only)
• 1 hour post IP dose (±15 min)
— Obtain 12-lead ECG
• 8 hours post IP dose (±15 min)
— Collect blood sample for PK assessment (C1D8 only)
— Collect blood sample for immune biomarker assessment
Study Cycles 1–6, Week 12 (± 3 days) and Week 18 (± 3 days)
• Perform CT / MRI of neck, chest, upper abdomen, and other anatomical region(s) of disease using the same technique as baseline and in accordance with the Imaging Manual
Imaging should not be delayed in case of missed doses or dose delays.
6.2.2 Subsequent Treatment (Cycles 7+)
Study Cycles 7+, Day 1 (CX.D1) (±2 days)
• Within 72 hours prior to treatment, collect blood samples for the following analyses:
— CBC
— Serum chemistry
• Problem-oriented PE, including vital signs (T, BP, RR, HR), ECOG performance status assessment, and weight
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 29 Confidential Information 14-Jun-2013
Study Cycles 7+, Day 8 (CX.D8) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 15 (CX.D15) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 22 (CX.D22) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Every 8 Weeks (± 7 days)
• Perform CT / MRI of neck, chest, upper abdomen, and other anatomical region(s) of disease using the same technique as baseline and in accordance with the Imaging Manual
Imaging should not be delayed in case of missed doses or dose delays.
6.3 End of Treatment
Subjects will receive therapy until independently-confirmed disease progression per irRECIST. In the absence of significant clinical deterioration requiring intervention, disease progression identified at Week 12 should be confirmed with a repeat scan ≥ 4 weeks later and the subject should continue treatment until independent confirmation of PD based on the confirmation scan.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 30 Confidential Information 14-Jun-2013
The End of Treatment visit will be completed within 14 days of independent confirmation of radiologic PD as assessed by irRECIST (§11.3) and prior to initiation of other anti-cancer therapy.
• Complete PE, including vital signs (T, BP, RR, HR), ECOG performance status assessment and weight if not completed within the previous 14 days
• Collect blood samples for the following analyses if not completed within the previous 14 days:
— CBC
— Serum chemistry
• Collect urine for urinalysis if not completed within the previous 14 days
• 12-lead ECG
• Assess adverse events and update concomitant medications
• Perform CT/MRI for subjects who have not had an imaging study within the previous 4 weeks
6.4 Follow Up Period
Following the End of Treatment visit, subjects will be followed for survival. During the follow-up period, subjects will be contacted every 8 weeks to assess vital status and disease state, including the initiation of any new anticancer interventions.
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 31 Confidential Information 14-Jun-2013
Table 1: Schedule of Procedures and Assessments
Screen Cycles 1–6 Cycles 7+
EOT
FU
Study Week: -2 to -1 1–18 19+ Q8 weeks Day: -14 to -1 1 2 3 4 8 15 1 8 15 22
Informed Consent X
Medical History & Eligibility1 X
VTX-2337 or Placebo (IP) X X X X
Cetuximab2 X X X X X X X
Cisplatin or Carboplatin X
Fluorouracil (5-FU) X X X X
Physical Examination X X X X
12-Lead ECG3 X X X
CBC with differential4 X X X X
Serum Chemistry4 X X X X
Biomarkers5 2X
PK6 3X
Urinalysis X X
Pharmacogenetics X
Serum Pregnancy7 X
Submit Tumor Tissue X
CT or MRI8 X X X
AE/CRx9 X X X X X X X X
Assess Vital Status X 1 HPV status for patients with oropharyngeal carcinoma only 2 Cycle 1 Day 1 dose = 400 mg/m2; subsequent doses are 250 mg/m2 3 Screening, End of Treatment, and Cycle 1 Day 8 and Cycle 3 Day 8 only: perform 1 hour (±15 minutes) post-dose
of IP, when applicable 4 Obtain within 72 hours of each Day 1 dose 5 Cycle 1 Day 8 and Cycle 3 Day 8 only: perform pre-dose and 8 hours (±15 minutes) post-dose of IP 6 Cycle 1 Day 8 only: perform pre-dose, and 45 minutes and 8 hours (±15 minutes) post-dose of IP 7 Serum pregnancy to be collected on all females with reproductive potential 8 The same imaging modality must be used for each subject throughout the study. Assess tumor response at
Week 12 (± 3 days), Week 18 (± 3 days), and every 8 weeks (± 7 days) thereafter. Do not delay imaging if dosing/cycle is delayed
9 DLTs will be assessed for all subjects until the DSMB has completed the assessment of the starting dose (§9.2.2).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 32 Confidential Information 14-Jun-2013
6.5 Early Treatment Discontinuation
Treatment may be discontinued early for individual subjects for any of the following reasons:
• Subject decision / withdraw of consent
• Unacceptable toxicity related to the administration of the study required medications according to §7.4
• Subject lost to follow-up after repeated attempts to contact the subject
• Onset of an adverse event that would make ongoing treatment in the clinical trial inadvisable, as determined by the investigator, medical monitor, or study sponsor
• Subject non-compliance with the study’s requirements and/or procedures as determined by the investigator, medical monitor, or study sponsor
• Death
In the event a subject is withdrawn from treatment prematurely due to any of the reasons noted above, the End of Treatment evaluations should be completed, and the subject should be followed for survival.
In the rare event that a subject withdraws consent for all study-related activities, including follow-up for survival, this should be clearly documented in the medical record and eCRF.
6.6 Assessments 6.6.1 Assessment of Efficacy 6.6.1.1 Efficacy Parameters
The following efficacy parameters will be assessed by independent radiology review according to irRECIST (§11.3), and are defined as follows:
• Progression-free survival: the duration of time from randomization to the time of irPD or death, whichever comes first
• Objective response rate: the proportion of subjects who achieve complete or partial response
• Duration of best response: the duration of time from the date measurement criteria are first met for irCR, or irPR (if irCR is never met), until the first date that irPD is confirmed by independent radiology review or death, whichever comes first
• Disease control rate: the percentage of subjects who achieved irCR, irPR, or irSD
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 33 Confidential Information 14-Jun-2013
• Duration of disease control: the duration of time from the date measurement criteria are first met for irCR, irPR, or irSD, until the first date that irPD is confirmed by independent radiology review or death, whichever comes first
Overall survival is defined as the duration of time from randomization to the time of death due to any cause, or the date the subject was last confirmed to be alive.
6.6.1.2 Method and Timing
Imaging studies (CT or MRI) of the neck, chest, upper abdomen, and other anatomical region(s) of disease must be obtained at study Screening, Week 12, Week 18, and every 8 weeks thereafter until disease progression. Imaging studies will be completed at the End of Treatment visit for subjects who discontinue the study prematurely and have not had CT/MRI completed within the last 4 weeks (§6.5). For each subject, the same imaging method must be used at study screening and all follow-up assessments.
RECIST v1.1 is primarily designed to evaluate the early effects of cytotoxic agents and depends on tumor shrinkage to demonstrate biologic activity. However, clinical evidence of tumor responses seen with immunotherapeutic agents, such as VTX-2337, can take longer to achieve and may occur after a period of disease stabilization or following an initial increase in tumor burden. In light of the limitations of utilizing RECIST v1.1 to evaluate immunomodulatory agents, immune-related response criteria have been proposed as an alternative to conventional RECIST to systematically detect the novel response patterns observed with immunologic agents.[1819] This study will use RECIST v1.1 for the baseline tumor evaluation, and an immune-related modification of RECIST v1.1 (irRECIST) to determine tumor response.
As noted above, the immune-mediated responses expected from VTX-2337 require activation of the immune system prior to the observation of clinical responses, and such immune activation may take weeks to months to be clinically evident. Some subjects with advanced cancer may have objective increase of tumor burden within 12 weeks following the start of dosing on study. Such subjects may not have had sufficient time to develop the required immune activation or, in some subjects, tumor increases may represent infiltration of lymphocytes into the original tumor (often referred to as pseudo-progression). In traditional oncology studies, such increases in tumor burden during the first 12 weeks of the study would constitute progressive disease and lead to discontinuation of study treatment and imaging to detect response, thus disregarding the potential for subsequent immune-mediated clinical response. Therefore, in this study, the first imaging assessment will be performed at Week 12, followed by assessments at Week 18 and every 8 weeks thereafter.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 34 Confidential Information 14-Jun-2013
In addition, a key distinction between standard RECIST v1.1 criteria and irRECIST is that the latter requires early evidence of disease progression (i.e., an assessment of progressive disease ≤ 12 weeks after starting study treatment)—in the absence of rapid clinical deterioration—be confirmed by repeat, consecutive imaging ≥ 4 weeks after the initial assessment. During this interim ≥ 4 week period, subjects should continue to be followed per protocol, including continued dosing with study treatment. The key differences between RECIST v1.1 and irRECIST are outlined in Table 2.
irRECIST
Total Measured Tumor Burden
The total measured tumor burden (TMTB) is established at baseline as the sum of the longest diameters (SOD)—the shortest axes should be used for lymph nodes—of all target lesions (≤ 2 lesions per organ, ≤ 5 lesions total). At each subsequent tumor assessment (TA), the SOD of new, measurable lesions (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; ≤ 2 new lesions per organ, ≤ 5 new lesions total) is added to the SOD of the target lesions to provide the updated TMTB:
TMTB = SOD target lesions + SOD new, measurable lesions
Percentage changes in TMTB at each TA describe the size and growth kinetics of both old and new, measurable lesions as they appear. At each TA, the response in TMTB is defined as follows:
• Complete Response (irCR): Complete disappearance of all target and new, measurable lesions, with the exceptions of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
Response in Non-Target Lesions
The presence of non-target lesions is established at baseline; at each TA, the presence of any new, non-measurable lesions is assessed. The presence of new, non-measurable lesions will rule out an overall response of irCR. An increase in the size or number of new, non-measurable lesions does not necessarily imply an overall response of irPD; if these lesions become measurable (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; up to 2 new lesions per
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 35 Confidential Information 14-Jun-2013
organ, total 5 new lesions) at a subsequent TA, their measurement will, at that point, start to contribute to the TMTB.
The response in non-target lesions is defined as follows:
• Complete Response (irCR): Complete disappearance of all non-target lesions
• non-irCR/non-irPD: Non-target lesions do not meet the criteria for irCR or irPD
• Progressive Disease (irPD): Unequivocal increase in the number or size of non-target lesions. To achieve unequivocal progression of non-target lesions, there must be a substantial worsening of non-target disease of a magnitude that, according to the treating physician, warrants a change in anticancer therapy
NOTE: Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing lesions) should be considered irSD and treatment may continue until the next scheduled assessment.
Overall Response
The overall response according to irRECIST is derived from the responses in TMTB as well as the presence of any non-target lesions as follows:
• Complete Response (irCR): Complete disappearance of all lesions (whether measurable or not); lymph nodes must decrease to < 10 mm in shortest dimension
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
Comprehensive RECIST v1.1 and irRECIST guidelines can be found in §11.2 and §11.3, respectively.
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 36 Confidential Information 14-Jun-2013
Table 2: Tumor Response Evaluation: Comparison between RECIST v1.1 and irRECIST
Criteria RECIST v1.1 irRECIST
First tumor assessment (TA) Typically assessed at Week 8 Assessed at Week 12
New lesion(s)
New measurable lesions (≥ 10 mm [≥ 15 mm for lymph node short axis])
Always represents PD Included in TMTB if measurable
New non-measurable lesions (< 10 mm [< 15 mm for lymph node short axis])
Always represents PD Does not define progression but precludes irCR
Non-target lesions Changes contribute to defining best overall response (BOR), CR, PR, SD and PD
Changes contribute to defining irCR (complete disappearance required)
Unequivocal progression of non-target lesions
Always represents PD May represent irPD if there is a substantial worsening that warrants a change in anticancer therapy
CR Disappearance of all lesions Disappearance of all lesions
PR ≥ 30% decrease in the SOD of all target lesions compared with baseline, in absence of new lesions or unequivocal progression of non-target lesions
≥ 30% decrease in the TMTB compared with baseline
SD Neither CR, PR, or PD can be established
Neither irCR, irPR, or irPD can be established
PD ≥ 20% increase in SOD of target lesions compared with nadir. The SOD of target lesions must also demonstrate an absolute increase of ≥ 5 mm. The appearance of ≥ 1 new lesions is also considered progression
≥ 20% increase in TMTB compared with nadir. The TMTB must also demonstrate an absolute increase of ≥ 5mm*
*Subjects with an initial finding of progressive disease (irPD) before or at the 12 week imaging assessment, but without rapid clinical deterioration, require confirmation of irPD with a second, consecutive scan obtained ≥ 4 weeks from the initial documentation. Subjects will continue to receive study treatment until irPD is confirmed at this later time point. Best overall response (BOR) will therefore include responses occurring at any time before disease progression and after early progression (i.e., within the first 12 weeks of the study).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 37 Confidential Information 14-Jun-2013
6.6.2 Assessment of Safety 6.6.2.1 Safety Parameters
The primary safety parameters are the occurrence and severity of adverse events throughout the study treatment period. Refer to §8.2 for AE reporting requirements.
The pre-dose assessments performed on Day 1—including PE, vital signs, and laboratory assessments—will serve as the baseline and the standard for comparison of all follow-up examinations. All abnormal findings will be noted on follow-up and compared to baseline and clinically significant changes will be noted as adverse events.
6.6.2.2 Method and Timing
History and Physical Examination
A PE and medical history must be obtained at the Screening visit, on Day 1 of each cycle, and at End of Treatment.
Electrocardiograms
A 12-lead ECG will be performed at Screening, 1-hour post dose on Cycle 1 Day 8 and Cycle 3 Day 8, and End of Treatment.
Clinical Laboratory Evaluations
The clinical laboratory evaluations will be collected at Screening and on Day 1 of each cycle, and will include a complete set of clinical labs, including serum chemistry, complete blood count with differential, and urinalysis, as described in §6.2.
Subject-Reported Adverse Events
In addition to those adverse events noted by the study staff as determined through clinical evaluation, additional events may be elicited from the subject in a non-leading manner or volunteered by the subject at any time during the study. All adverse events, regardless of their severity or relationship to treatment with IP, will be recorded. All subjects experiencing adverse events will receive treatment if required for their event. Adverse events that are determined to be related to IP will be followed until resolution, or until resolved with sequelae.
6.6.3 Translational Research Assessments
Various immune and immunogenetic assessments will be performed on all subjects in the study. Exploratory analyses correlating data from these assessments will be performed to determine if
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 38 Confidential Information 14-Jun-2013
predictors of potential clinical benefit emerge. These predictors would be valuable in defining appropriate populations for study in subsequent trials of VTX-2337 in this patient group.
Pharmacogenomics
A single sample of genomic DNA will be collected on all subjects for analysis of genetic polymorphisms that may impact the response of patients to a TLR8 agonist or to cetuximab. These include defined single nucleotide polymorphisms (SNPs) in the TLR8 gene (most notably the A1G variant), and variants in the FcλRII and FcλRIII genes (most notably the 131 and 158 polymorphisms, respectively), that vary binding affinity for the FcR.
Immune Biomarker Analysis
TLR8 stimulates the production of a variety of cytokines and chemokines from immune cells. Serum samples will be collected pre-dose and 8 hours post-dose on C1D8 and C3D8 for analysis using a multiplexed panel of cytokines, chemokines, and inflammatory markers.
Tissue Biomarker Studies
Assessment of the effect of immune cell subsets, as measured by immunohistochemistry in primary tumor tissue (e.g., immune score) will be completed on tumor tissue obtained from the primary tumor site. This analysis includes but is not limited to an automated analysis of CD3, CD45, and FOXP3 staining of lymphocyte populations in the tumor using immunohistochemistry. Additional studies including gene signature analysis or detached somatic mutations will be performed, if indicated.
Pharmacokinetic Analysis
Plasma samples will be obtained on Cycle 1 Day 8 and quantitatively analyzed to support population PK and exposure-response analyses.
6.7 Monitoring for Subject Compliance
No specific measures for subject compliance are required for this study. IP must be administered in the clinic or hospital setting under the supervision of the investigator or clinical site staff. Subjects should be carefully evaluated prior to study entry to ensure they can comply with the study’s visit and assessment schedule.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 39 Confidential Information 14-Jun-2013
7.0 TREATMENT 7.1 Packaging, Labeling and Storage
IP is provided as an off-white, lyophilized cake in a 3 mL clear-glass, stoppered, single-use vial. Each vial is identified with a label similar to the following:
xx mg VTX-2337 or Placebo for subcutaneous injection
Subject #XXXXX
Prepare according to clinical protocol VRXP-A202
Store 2–8ºC
Caution: New drug—limited by federal law to investigational use.
VentiRx Pharmaceuticals, Inc.
xx mg VTX-2337 or Placebo for subcutaneous injection
Subject XXXXX for protocol VRXP-A202
Subject #: ________________
Date: ___________________
↑ This portion attached to vial ↑ Detach this portion for subject record
Upon randomization, a subject-specific kit containing a supply of IP will be shipped via traceable courier to the clinical site. Re-supply will be generated based on data provided by the site. Unopened vials of IP should be stored in the refrigerator at 2−8ºC (36−46ºF) and protected from light.
VTX-2337 and placebo will be labeled, packaged, and shipped by Fisher Clinical Services (Mount Prospect, IL).
7.2 Preparation of Investigational Product
Refer to the Pharmacy Manual for complete instructions regarding the storage and preparation of IP.
Before administration, IP must be reconstituted and prepared according to the Pharmacy Manual. Investigational drug solution should be prepared and transferred using aseptic technique in a biological safety cabinet. Vials of IP are intended for single use only.
IP will be supplied by VentiRx Pharmaceuticals. All other medications may be obtained through standard institutional practice.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 40 Confidential Information 14-Jun-2013
7.3 Administration of Investigational Product and Study Treatment(s) 7.3.1 Investigational Product Administration
IP (i.e., VTX-2337 or placebo) is administered as a subcutaneous injection of 3.0 mg/m2 (see also §9.2.2). Doses are given prior to cetuximab on Days 8 and 15 of a 21-day cycle for the first 6 cycles and on Days 8 and 22 for cycles 7+. Subjects will continue to receive bi-weekly doses of IP until independently-confirmed disease progression. See also §6.3 and §6.5.
Within 30 minutes prior to each dose of IP subjects will be administered 650–1000 mg acetaminophen by mouth to help mitigate potential adverse events commonly associated with the administration of VTX-2337 (e.g., fever, myalgia). Subjects will be given or instructed to take an additional dose of 650–1000 mg acetaminophen by mouth approximately 4–6 hours after administration of IP, and as needed thereafter for symptoms of fever and/or body aches. Acetaminophen is the preferred over-the-counter analgesic and antipyretic; due to their potentially immunosuppressive effects, administration of NSAIDS within 24 hours of dosing should be avoided if clinically feasible.
To potentially reduce the effects of injection site reaction that may be associated with the administration of IP, application of an ice pack to the injection site for approximately 30 minutes prior to injection is recommended. Additionally, at the discretion of the investigator, single doses of IP may be divided and administered at two different anatomical locations.
The dose of IP should be administered with a syringe suitable for subcutaneous injection. To administer the injection, 1–2 inches of fatty tissue should be pinched up to avoid injection into the muscle layer. The needle can be inserted at either 45 or 90 degrees; a 45 degree angle is recommended when less than 2 inches of tissue can be pinched. Appropriate anatomic areas for subcutaneous injection include the fatty tissue over the abdomen, triceps, thighs, or lower back. The injection site should be rotated among anatomically appropriate locations to help avoid injection site reaction.
Standard medications to treat possible hypersensitivity reactions and/or symptoms of CRS should be readily available at the time of treatment, including epinephrine, H1 antihistamines (e.g., diphenhydramine), H2 antihistamines (e.g., ranitidine), narcotics, IV fluids for volume expansion and supplemental oxygen.
Due to their immunosuppressive effect, administration of systemic corticosteroids (e.g., dexamethasone) should be avoided in this setting if other means of treatment are available and appropriate.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 41 Confidential Information 14-Jun-2013
7.3.2 Cetuximab Administration
The initial 400 mg/m2 dose of cetuximab is administered on Cycle 1 Day 1 as a 120-minute IV infusion (maximum infusion rate 10 mg/min).
The subsequent, weekly, 250 mg/m2 doses of cetuximab are administered as 60-minute IV infusions (maximum infusion rate 10 mg/min). Subjects will continue to receive weekly doses of cetuximab until independently-confirmed disease progression. See also §6.3 and §6.5.
Subjects will be premedicated with an H1 antagonist (e.g., 50 mg of diphenhydramine) intravenously 30–60 minutes prior to the first dose; premedication should be administered for subsequent cetuximab doses based upon clinical judgment and the presence/severity of prior infusion reactions.
Serious infusion reactions, requiring medical intervention and immediate, permanent discontinuation of cetuximab, include rapid onset of airway obstruction (e.g., bronchospasm, stridor, hoarseness), hypotension, shock, loss of consciousness, myocardial infarction and/or cardiac arrest. Subjects should be monitored for 1 hour following cetuximab infusions in a setting with resuscitation equipment and other agents necessary to treat anaphylaxis (e.g., epinephrine, intravenous antihistamines, bronchodilators, oxygen, and corticosteroids).
When cetuximab is administered on the same day as chemotherapy, cetuximab administration will be completed ≥ 1 hour prior to administration of platinum and 5-FU. When cetuximab is administered on the same day as IP, the dose of IP will be given prior to cetuximab.
For additional information please refer to the cetuximab label.
7.3.3 Platinum Administration
The platinum therapy should be assigned by the investigator prior to randomization. Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent should be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject. Reasonable efforts should be made to keep the subject on the platinum therapy originally assigned; however, the platinum therapy may be changed if clinically necessary.
Cisplatin
At least one hour after completion of cetuximab administration, subjects will receive a 100 mg/m2 dose of cisplatin administered as a 60-minute IV infusion. Cisplatin will be
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 42 Confidential Information 14-Jun-2013
administered on Day 1 of a 21-day cycle for a maximum of 6 cycles and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
Pretreatment hydration may be administered according to institutional standards.
For additional information regarding cisplatin administration, please refer to the label.
Carboplatin
At least one hour after completion of cetuximab administration, subjects will receive carboplatin at an AUC of 5 mg/mL/min administered as a 60-minute IV infusion. Carboplatin will be administered on Day 1 of a 21-day cycle for a maximum of 6 cycles, and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
For additional information regarding administration, please refer to the carboplatin label.
7.3.4 Fluorouracil (5-FU) Administration
At least one hour after completion of cetuximab administration, subjects will receive an intravenous infusion of 5-FU at a dose of 1000 mg/m2 per day for 4 days. 5-FU administration will begin on Day 1 of a 21-day cycle for a maximum of 6 cycles and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
For additional information regarding 5-FU administration please refer to the label.
7.4 Dose Modifications
In order to maintain dose-intensity and cumulative dose-delivery, reasonable efforts should be made to minimize dose reductions and treatment delays. Any subject whose treatment is delayed should be evaluated on a weekly basis until adequate hematologic and non-hematologic parameters have been met.
Toxicities may require the dose reduction of one or more of the study required medications. The investigator should carefully assess all treatment-associated toxicities and, whenever possible, determine if the toxicities can reasonably be attributed to a single agent or a causal relationship with one of the agents can reasonably be ruled out. If appropriate, dose reductions should not affect the dose of other products. For example, if the dose of cetuximab is reduced, cisplatin or carboplatin, 5-FU, and IP should be administered per protocol.
• Toxicity grades are defined using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 4.03
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 43 Confidential Information 14-Jun-2013
• Any subject who requires a dose reduction due to drug-related toxicity will continue to receive the reduced dose for the remainder of study treatment
• Dose escalations are not allowed
It is imperative that sequencing of chemotherapy and IP be maintained throughout the study. Specifically, platinum and 5-FU should be administered on the same day, if possible. If short delays are required that separate the administration of platinum and 5-FU, all attempts should be made to dose these agents on the same day in subsequent cycles. Due to the immunosuppressive effects associated with the dosing period of 5-FU, all attempts should be made to avoid co-administration of IP until 48 hours after completion of 5-FU administration.
In addition, the timing of imaging studies should not be affected by dose reductions or delays. Subjects should remain on study (i.e., continue receiving treatment with other agents and undergo all protocol-related assessments) until independently-confirmed disease progression. Thereafter, subjects should be followed for long-term survival per protocol.
7.4.1 Investigational Product Dose Modifications
Management of Injection Site Reactions
Acute symptoms of injection site reactions typically resolve within 48 hours of injection, but more persistent reactions are not unexpected. Grade 2 reactions may include a painful, raised, fluid-filled blister that mimics a sterile abscess. Injection site reactions do not typically warrant antibiotic intervention as they have been found to be sterile. A culture of the fluid can be obtained—using sterile technique—if infection is strongly suspected (i.e., associated with fever persisting more than 24 hours after injection).
Ice and acetaminophen should be administered prophylactically according to §7.3.1. Symptomatic treatment with ice, acetaminophen and narcotics is acceptable. Due to their potentially suppressive effects, the use of NSAIDs within 24 hours of dosing with IP should be avoided, if clinically feasible.
Management of Systemic Toxicities
The most common systemic drug-related adverse events—grade 1 or 2 chills, flu-like symptoms and fever—typically resolve in < 48 hours and do not require dose reductions or a delay in the dosing regimen. Less commonly, dosing with VTX-2337 may result in CRS, which is most likely to be grade 1, but more severe reactions are possible.
CRS is a symptom complex and is characterized by systemic symptoms which may include fever, nausea, chills, tachycardia, hypotension, dyspnea, asthenia, headache, and rash. VTX-2337
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 44 Confidential Information 14-Jun-2013
directly targets TLR8, which is expressed on immune cells. CRS may result from the release of cytokines from the activated immune cells, or from ‘downstream’ events that can be associated with cytokine production. Symptoms of CRS may be acute or delayed by several hours after dosing with IP.
Treatment of systemic drug-related events should be consistent with the severity of the reaction as well as institutional standards and may include: acetaminophen, H1- and H2-receptor antagonists, narcotics, IV fluids for volume expansion, and supplemental oxygen. Due to their potentially immunosuppressive effect, administration of NSAIDs and systemic steroids (e.g., dexamethasone) should be avoided if other means of treatment are available and medically appropriate.
In most cases the CRS will be no more than grade 1. However, a severe, life-threatening reaction resulting from a substantial release of cytokines is possible. Severe CRS is a medical emergency and urgent intervention must be taken to prevent life-threatening complications. This may include administration of sympathomimetic amines for pressor support and/or hospitalization for acute monitoring and intervention.
Investigational Product Dose Modifications
Table 3 and Table 4 outline dose delay and reduction requirements for IP. Delays in IP dosing should not delay or shift the timing of cetuximab, platinum, or 5-FU dosing (i.e., doses of IP are skipped and not made up). In the event of grade 3 or grade 4 toxicities attributed to IP, subsequent doses should be delayed until recovery to ≤ grade 1.
Table 3: Investigational Product Dose Reduction Schedule
IP Dose Level (mg/m2)
3.0
2.5
2.0
1.5
NOTE: Only two dose reductions are allowed. If a third dose reduction is required, IP should be discontinued.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 45 Confidential Information 14-Jun-2013
Table 4: Investigational Product Dose Modifications
Grade Action
Cytokine Release Syndrome
1 Dose reduction not required; consider prophylactic precautions—including volume expansion and treatment with oral or IV antihistamines—with next dose
2 Consider prophylactic precautions—including volume expansion and treatment with oral or IV antihistamines—with next dose Reduce dose by 1 level at investigator’s discretion
3 Use prophylactic precautions with next dose Reduce dose by 1 level
Injection Site Reaction
1 Dose reduction not required; consider administering subsequent injections at distal anatomic site(s)
2 Administer subsequent injections at distal anatomic site(s) until resolved to ≤ grade 1
Delay dosing for up to 2 weeks if needed
If > 2 week delay or > 2 delays are required with consecutive injections, reduce dose by 1 level
3 Delay dosing until resolved to ≤ grade 1 Reduce dose by 1 level
Non-Hematologic Drug-Related AEs
1–2 Dose reduction not required; manage per institutional standards
≥ 3 Reduce dose by 1 level
Hematologic Drug-Related AEs
1–3 Dose reduction not required; manage per institutional standards
≥ 4 Reduce dose by 1 level
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 46 Confidential Information 14-Jun-2013
7.4.2 Cetuximab Dose Modifications
Table 5 and Table 6 should be used as a guideline for cetuximab dose modifications. Please refer to the cetuximab label for additional information.
Table 5: Cetuximab Dose Modifications for Infusion Reactions
NCI-CTC Grade Dose Modification
1
Reduce infusion rate by 50% 2
Non-serious grade 3
Serious grade 3 (e.g., requiring hospitalization) or any grade 4 Immediately and permanently discontinue cetuximab
Table 6: Cetuximab Dose Modifications for Dermatologic Toxicity
Severe Acneiform Rash Cetuximab Delay/Discontinuation
Outcome Dose Modification
1st occurrence Delay infusion by 1–2 weeks Improvement Continue at 250 mg/m2
No improvement Discontinue cetuximab
2nd occurrence Delay infusion by 1–2 weeks Improvement Reduce dose to 200 mg/m2
No improvement Discontinue cetuximab
3rd occurrence Delay infusion by 1–2 weeks Improvement Reduce dose to 150 mg/m2
No improvement Discontinue cetuximab
4th occurrence Discontinue cetuximab
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 47 Confidential Information 14-Jun-2013
7.4.3 Chemotherapy Dose Modifications (cisplatin, carboplatin, and 5-FU)
Table 7 and Table 8 should be used as a guide for dose reductions of cisplatin, carboplatin, and 5-FU. The dose of each agent should be reduced by 25% in subjects with related toxicities ≥ grade 3.
Table 7: Dose Reduction Guidelines for Chemotherapeutic Agents
Grade ≥ 3 Toxicity Chemotherapy Delay/Discontinuation
Outcome Dose Modification
1st occurrence Delay infusion by 1–2 weeks Improvement Reduce dose by 25%
No improvement Discontinue agent
2nd occurrence Delay infusion by 1–2 weeks Improvement Reduce dose to 50%
No improvement Discontinue agent
3rd occurrence Discontinue agent
Table 8: Chemotherapy Dose Reduction Schedule
Agent Original Dose (100%) 25% Reduction 50% Reduction
Cisplatin 100 mg/m2 75 mg/m2 50 mg/m2
Carboplatin AUC of 5 mg/mL/min AUC of 3.75 mg/mL/min AUC of 2.5 mg/mL/min
5-FU 1000 mg/m2 750 mg/m2 500 mg/m2
Additional Considerations for Cisplatin
Repeat doses of cisplatin should not be administered until the following parameters have been met:
• serum creatinine < 1.5 mg/100 mL • platelets ≥ 100k/mm3 • WBC ≥ 2000/mm3
When clinically appropriate, subjects assigned to cisplatin should receive 2 dose reductions prior to discontinuation of cisplatin and/or being re-assigned to receive carboplatin. If clinically necessary, the investigator may change the platinum chemotherapy from cisplatin to carboplatin.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 48 Confidential Information 14-Jun-2013
Additional Considerations for Fluorouracil (5-FU)
If severe gastrointestinal or hematologic toxicity occurs with the first dose of 5-FU, consider dihydropyrimidine dehydrogenase (DPD) deficiency and discontinuation of 5-FU.
7.5 Emergency Unblinding
The treatment assignment of any individual subject may be accessed only in case of an emergency, such as a life-threatening serious adverse event (SAE) where knowledge of the treatment code is required for medical management of the event. The investigator should obtain approval from the medical monitor or sponsor prior to unblinding and should document the unblinding (including notification of sponsor/medical monitor and reason for unblinding) in the subject’s medical record.
Contact information for notification of unblinding:
PRA Oncology Call Center Toll Free: +1 (866) 326-5053 Direct: +1 (434) 951-4082 Fax: +1 (800) 280-7035 Email: [email protected]
After obtaining sponsor or medical monitor approval, to unblind the subject’s treatment assignment the investigator will log into IXRS and enter, at minimum, the subject’s randomization number; IXRS will then provide the treatment assignment. The treatment assignment should be maintained as confidential (i.e., only personnel essential for subject treatment should be informed of the treatment assigned) and placed in a sealed envelope.
The treatment code for an individual subject may also be broken at the discretion of the study sponsor to facilitate regulatory reporting of suspected unexpected serious adverse reactions (SUSAR).
7.6 Concomitant Medications and Supportive Care
Medications that must be discontinued prior to study entry are outlined in §5.2. The following medications and interventions, unless otherwise specified, are prohibited from the time of study screening until the End of Treatment visit:
• Systemic anti-cancer therapy, including chemotherapy, radiotherapy, or endocrine therapy other than those required per protocol
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 49 Confidential Information 14-Jun-2013
• Systemic—oral, IV, injectable—corticosteroids (e.g., dexamethasone) should be avoided (see below)
• Any investigational drug or device other than VTX-2337 or placebo
• NSAIDs within 24 hours of IP dosing should be avoided if clinically feasible, due to their potentially suppressive effects
• Any immunotherapy other than VTX-2337 or placebo
• Cytochrome P450 3A4 (CYP3A4) inducers and/or inhibitors may affect the metabolism of VTX-2337. Therefore, care should be exercised when drugs or other substances that affect CYP3A4 are administered concomitantly with VTX-2337 or placebo and, if possible, alternatives that do not affect CYP3A4 should be administered instead. A list of CYP3A4 inhibitors and inducers may be found in §11.4.
Subjects should be provided with full supportive care measures, as clinically indicated, and in accordance with institutional standards. Such care includes medication for pain control and symptom management, antibiotics, bisphosphonates, antiemetics, colony stimulating factors, and transfusions of blood or blood products. Treatment for drug-related adverse events should be administered at the discretion of the investigator.
Anaphylactic-like reactions have been reported with administration of cetuximab, cisplatin, carboplatin, and 5-FU. Epinephrine and/or antihistamines may be administered to alleviate symptoms. Due to their immunosuppressive effect, administration of systemic steroids (e.g., dexamethasone) should be avoided in this setting if other means of treatment are available and appropriate. For additional information on treatment of cetuximab infusion reactions refer to §7.3.
Localized radiotherapy is permitted for palliation of painful lesions at the investigator’s discretion. However, medical management in place of radiation therapy should be used if clinically appropriate.
7.6.1 Chemotherapy-induced nausea and vomiting
Corticosteroids (e.g., dexamethasone) are often used as the first-line treatment for chemotherapy-induced nausea and vomiting; however, the administration of systemic corticosteroids (oral, IV, injectable) broadly inhibits the production of multiple cytokines and chemokines and impairs cellular immunity, thus impeding the immunostimulatory and pharmacologic effects of VTX-2337. As such, a steroid-sparing approach to the management of adverse events during the treatment phase of this study is warranted.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 50 Confidential Information 14-Jun-2013
Marked nausea and vomiting commonly occur in patients treated with cisplatin, carboplatin, and 5-FU. Nausea and vomiting may be acute (onset 1–4 hours after infusion) or delayed (begins or persists ≥ 24 hours after infusion). To combat chemotherapy-induced nausea and vomiting, the following algorithm should be used:
a) Nonsteroidal anti-emetics, such as a 5-HT3 antagonist (e.g., ondansetron), should be utilized for first-line management of symptoms
b) In the event that symptoms cannot be adequately controlled with nonsteroidal medications, dexamethasone 20 mg may be administered on Day 1 of each cycle
c) If dexamethasone on Day 1 followed by nonsteroidal antiemetics on subsequent days does not sufficiently manage symptoms, dexamethasone 20 mg may be administered on Day 2 and/or Day 3. Every reasonable attempt should be made to discontinue dexamethasone use ≥ 72 hours prior to administration of IP
7.6.2 Fever with Neutropenia
Grade 1 or 2 transient pyrexia is a common side effect of VTX-2337, with typical onset 3–6 hours after dosing with the investigational product and lasting approximately 24 hours. Fever may or may not be accompanied by flu-like symptoms such as shaking, chills, and myalgia. In a Phase 3 study of cetuximab plus platinum-5-FU, more than 25% of subjects experienced grade 3 or 4 neutropenia and 6% of subjects experienced febrile neutropenia.(12) The nadir typically occurs 18–23 days after administration of platinum. It is therefore anticipated that grade 3 or 4 neutropenia will sometimes be present during the 24-hour window in which fever induced by VTX-2337 is anticipated. The following algorithm will be used to carefully evaluate subjects to help determine if the fever reflects the expected pharmacology of VTX-2337 or an infection related to chemotherapy-induced neutropenia.
For subjects who experience onset of fever within 8 hours of dosing with IP but are without symptoms or signs of infection, a complete blood count may be drawn.
• A: If the ANC is > 500 cells/µL, follow for resolution of fever (expected ≤ 36 hours)
— A1: If fever persists > 36 hours and the subject is still asymptomatic, draw blood cultures and repeat CBC. If ANC declined to <500 cells/µL, switch to algorithm B1 below
— A2: If fever persists > 36 hours and the subject develops additional symptoms and/or signs of infection, draw blood cultures and repeat CBC. Treat as appropriate, either as an outpatient with oral antibiotics or as inpatient with parenteral antibiotics
• B: If the ANC is < 500 cells/µL, draw blood cultures the same day
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 51 Confidential Information 14-Jun-2013
— B1: If fever persists > 36 hours and the subject is asymptomatic, start oral antibiotics
— B2: If fever persists > 36 hours and the subject has symptoms of infection, admit the subject to the hospital for parenteral antibiotics
7.7 Investigational Product Accountability
VentiRx Pharmaceuticals will provide an adequate supply of IP for the study population and protocol requirements. Drug supplies must be kept in an appropriate, secure area (e.g., locked pharmacy) and stored in accordance with the conditions specified in this protocol, the pharmacy manual, and on the IP labels.
Drug supplies are to be used only in accordance with this protocol, pharmacy manual, and under the personal supervision of the Principal Investigator or under the supervision of a sub-investigator who is responsible to the investigator. IP may be administered only to eligible subjects who are randomized in the study. The Principal Investigator is accountable for all used and unused investigational drug. The investigator agrees not to destroy any used, partially used, or unused investigational drug supplies unless otherwise directed by VentiRx Pharmaceuticals or its representatives. Upon written notification, the investigator will ship unused IP according to instructions provided.
A master drug log must be maintained for all IP vials received, dispensed (including the subject’s ID number, the subject’s initials, and the dates each vial is dispensed) and returned or destroyed. In addition, a subject-specific record of each vial administered, including the date and identification number of each vial, will be maintained with the case file for each subject. Any discrepancy in the drug distribution logs (master log and subject logs) must be explained in detail.
8.0 ADVERSE EVENTS
The following sections describe the minimum requirements for assessing and reporting AEs, including SAEs and serious suspected adverse reactions, for subjects participating in trial VRXP-A202. The investigator is additionally responsible for complying with all local institution and IRB/IEC requirements for reporting AEs.
8.1 Definitions 8.1.1 Adverse Event (AE)
An adverse event is defined as any untoward medical occurrence associated with the use of a drug in humans, whether or not considered drug-related. An AE can therefore be any unfavorable and unintended sign, symptom, or disease which is temporally associated with the use of the
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 52 Confidential Information 14-Jun-2013
investigational drug, whether or not considered related to (i.e., to have a causal relationship with) the IP.
AEs include exacerbation of a pre-existing illness, an increase in frequency or intensity of a pre-existing episodic event or condition, a condition detected or diagnosed after IP administration even though it may have been present prior to the start of the study, or a continuous persistent disease or symptom present at baseline that worsens following the start of the study.
Medical conditions and diseases that are present before Cycle 1 Day 1 are only considered AEs if they worsen after starting treatment with Cycle 1 Day 1. Any medical condition with an onset or diagnosis before Cycle 1 Day 1 will be included in the subject’s medical history. Abnormal laboratory values or test results constitute AES if they induce clinical signs or symptoms or if they require intervention or therapy.
8.1.2 Serious Adverse Event (SAE)
An AE or suspected adverse reaction is considered ‘‘serious’’ if, in the view of either the investigator or sponsor, it results in any of the following outcomes:
• Death
• A life-threatening1 adverse event
• Inpatient hospitalization or prolongation of existing hospitalization,
• A persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions
• A congenital anomaly/birth defect
Important medical events that may not result in death, be life-threatening, or require hospitalization may be considered serious when, based upon appropriate medical judgment, they may jeopardize the subject and may require medical or surgical intervention to prevent one of the outcomes listed in this definition. Examples of such medical events include allergic bronchospasm requiring intensive treatment in an emergency room or at home, blood dyscrasias or convulsions that do not result in inpatient hospitalization, or the development of drug dependency or drug abuse.
1 An AE or suspected adverse reaction is considered “life-threatening” if, in the view of either the investigator or sponsor, its occurrence places the patient or subject at immediate risk of death. It does not include an AE or suspected adverse reaction that, had it occurred in a more severe form, might have caused death.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 53 Confidential Information 14-Jun-2013
8.1.3 Dose-Limiting Toxicities (DLT)
A DLT is defined as any IP-related adverse event, occurring during Cycle 1 (Week 1–3), which meets the following criteria:
• Any ≥ grade 4 hematologic toxicity
• Any ≥ grade 3 non-hematologic toxicity (including injection-site reaction), with the exception of:
— Grade 3 dermatologic toxicities
— Grade 3 hypersensitivity reaction
• Diarrhea, nausea, or vomiting will only be considered a DLT when ≥ grade 3 toxicity occurs despite adequate anti-emetics or anti-diarrhea medications
• Treatment delay due to toxicity lasting greater than 21 days
• Death
“IP related” refers to events that are possibly or probably related to the administration of IP or the combined treatment regimen of IP, platinum, 5-FU, and cetuximab, and not clearly attributed to platinum, 5-FU, cetuximab alone, or other causes.
DLTs will be assessed for all subjects until at least six subjects randomized to receive VTX-2337 have received one cycle of treatment and the DSMB has completed the assessment of the starting dose. (§9.2.2) Individual subjects who experience DLTs may nevertheless receive additional doses of IP, following careful medical evaluation and appropriate treatment and/or a dose delay of 1 week, at the discretion of the investigator, with input from the medical monitor and study sponsor.
8.2 Reporting Requirements
Information regarding all AEs, whether volunteered by the subject, discovered via questioning by the investigator or clinical personnel, or identified through physical examination, laboratory test or other means will be collected from the first dose of study required medication administered on Cycle 1 Day 1 until 7 days after the last dose of any study medication. Suspected adverse reactions (i.e. AEs that are assessed as related to IP) which are ongoing will be followed until resolution or until grade ≤ 2 and stabilized. Suspected adverse reactions may be reported at any time.
Information collected regarding each AE will include, but is not limited to (1) duration (start and stop dates), (2) severity as delineated in §8.2.2, (3) relationship to the investigational drug (“causality”) as described in §8.5 (serious adverse events only), (4) any action taken and (5)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 54 Confidential Information 14-Jun-2013
outcome. Whenever possible, AEs should be described in terms of a change in the baseline status (e.g., “increased frequency of migraines”) or with a diagnosis or summary term in place of individual clinical signs or symptoms (e.g., “upper respiratory infection” vs. “runny nose”, “sneezing” and “cough”).
8.2.1 Serious Adverse Events
The investigator must immediately (≤ 24 hours of clinical site personnel becoming aware of the event) report to the study’s medical monitor any SAE—whether or not considered drug related, including those listed in the IB—and must include an assessment of whether there is a reasonable possibility that the investigational drug caused or otherwise contributed to the event. The site will provide the initial notification to PRA Drug Safety via fax or email on the required SAE Report Form, which must be signed by the investigator. Follow-up information or new information regarding an ongoing SAE must be provided promptly to PRA Drug Safety.
PRA Drug Safety Phone: +1 (800) 772-2215 +1 (434) 951-3489 Fax: +1 (888) 772-6919 +1 (434) 951-3482 email: [email protected]
The investigator is responsible for notifying the IRB/IEC or other appropriate committees of all SAEs in accordance with institutional and IRB/IEC policies.
8.2.2 Dose Limiting Toxicities
As described in §9.2.2, DLTs will be assessed for all subjects until the DSMB has completed the assessment of the starting dose. Once the investigator has determined a DLT has occurred, the DLT should be reported within 48 hours. This is necessary to allow the DSMB to review DLTs in a timely manner.
8.3 Criteria for Determining Adverse Event Severity
AEs will be categorized and severity will be graded according to the NCI-CTCAE version 4.03.
Note that “seriousness” and “severity” are distinct concepts. “Serious” is a term applied to an AE that meets specific regulatory requirements; it is typically associated with events that pose a threat to the subject’s life or functioning. “Severity” refers to the AE intensity classification. A severe AE may be of minor medical significance (e.g. grade 3 headache), while an AE that is
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 55 Confidential Information 14-Jun-2013
graded as mild in severity may be serious (e.g. grade 1 stroke requiring overnight hospitalization).
8.4 Criteria for Determining Adverse Event Expectedness
An AE (§8.4) or suspected adverse reaction is considered ‘‘unexpected’’ if it is not listed in the IB or is not listed at the specificity or severity that is observed. The sponsor or its representative will be responsible for determining the expectedness of adverse events.
For example, under this definition, hepatic necrosis would be unexpected (by virtue of greater severity) if the IB referred only to elevated hepatic enzymes or hepatitis. Similarly, cerebral thromboembolism and cerebral vasculitis would be unexpected (by virtue of greater specificity) if the IB listed only cerebral vascular accidents. ‘‘Unexpected’’—as used in this definition—also refers to AEs or suspected adverse reactions that are mentioned in the IB as occurring with a class of drugs or as anticipated from the pharmacological properties of the drug, but are not specifically mentioned as occurring with the particular drug under investigation.
Therefore, "unexpected" also refers to an AE or suspected adverse reaction that has not been previously observed (i.e. included in the IB) rather than from the perspective of such an experience not being unanticipated from the subject’s disease state.
8.5 Criteria for Determining Adverse Event Causality
The following categories for determining the relationship of an AE to the IP are as follows:
None: The AE is temporally independent of the administration of IP and/or can be readily attributed to other factors such as the subject’s clinical state, environmental factors, or concomitant drugs or therapies
Possible: The AE follows a reasonable temporal sequence from administration of IP and cannot readily be explained by the subject’s clinical state, environmental factors, or concomitant drugs or therapies
Probable: The AE follows a clear temporal sequence from administration of IP and is unlikely to be related to the subject’s clinical state, environmental factors, or concomitant drugs or therapies. The AE ceases with discontinuation of the drug and reoccurs after restarting, if applicable
Note that the term “suspected adverse reaction” is used to describe an AE for which there is a reasonable possibility that the IP caused the adverse event (i.e. an event that is assessed as ‘possibly’ or ‘probably’ caused by administration of IP).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 56 Confidential Information 14-Jun-2013
8.6 Expedited Reporting of Serious Adverse Events
Regulations require that VentiRx Pharmaceuticals or its representatives to report any suspected adverse reactions1 that are both serious (§8.1) and unexpected (§8.4). Such events must be reported to the FDA, applicable regulatory authorities, and all participating investigators (i.e., all investigators to whom VentiRx is providing drug under its INDs or under any investigator’s IND) within 15 calendar days after VentiRx or its representative receives the information and determines that it qualifies for reporting. Such notification must occur within 7 calendar days if the SUSAR was fatal or life-threatening.
Therefore, once the investigator has determined that an SAE has occurred, it is important to adhere to the reporting timeframes outlined in §8.2. After receiving the investigator’s SAE report, including the investigator’s assessment of causality, VentiRx or its representatives will also assess the event for seriousness and the relationship to IP and will determine if the event was unexpected.
Investigational New Drug Safety Reports (INDSRs), or equivalent, will be reported to FDA and applicable local regulatory authorities by VentiRx Pharmaceuticals or its representatives; copies of the report will be distributed to clinical investigators. The investigator is responsible for notifying the relevant IRB/IEC of all INDSRs in accordance with institutional and IRB/IEC policies.
9.0 STATISTICAL PLAN 9.1 Statistical Considerations
All analyses will use SAS® version 9.1.3 or higher (SAS Institute, Inc., Cary, NC). Summary tables will be organized by treatment group: Combination Arm (SOC plus VTX-2337) versus Control Arm (SOC plus placebo). All available scheduled data for the safety or efficacy populations will be used in the analyses. Important CRF data will be included in data listings for all subjects who are randomized on the study. Missing data will not be imputed, except via censoring in survival analyses.
In keeping with ICH E9, center effect will not be included in the analysis models as it is recognized that there will be limited numbers of subjects per center in this trial. However, randomization stratification factors and/or their interaction terms with treatment may be explored.
1 A suspected adverse reaction is an adverse event for which there is a reasonable possibility that the investigational drug caused the adverse event. For the purposes of investigational new drug (IND) safety reporting, “reasonable possibility” means there is evidence to suggest a causal relationship between the drug and the adverse event.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 57 Confidential Information 14-Jun-2013
Unless otherwise noted, categorical data will be presented using counts and percentages, with the number of subjects in the analysis population by treatment group as the denominator for percentages. Percentages will be rounded to one decimal place. Continuous data, unless otherwise noted, will be summarized using the number of observations (n), mean, standard deviation, median, minimum, and maximum. The primary test on PFS, secondary test on OS, and all other statistical tests will be conducted using a 1-sided significance level of 0.10.
9.1.1 Sample Size and Operating Characteristics
The total samples size is approximately 175 subjects (estimated 88 per treatment group). In the event the starting dose of VTX-2337 is reduced (see §9.2.2), the sample size for the trial will be adjusted so that 175 subjects will be treated at the modified starting dose. Subjects who discontinue the study prior to receiving their first dose of IP will be replaced. A dropout rate of approximately 10% over the life of the study is assumed.
The timing of the primary analysis will be event-driven. One hundred thirty-four (134) PFS events are required to detect a hazard ratio (HR) of 0.67 with 85% power at a 1-sided alpha of 0.10. This HR represents a 50% improvement in PFS, which translates to an increase in median PFS from 6 months (control arm) to 9 months (combination arm). It is estimated that a population of 175 evaluable subjects accrued over 18 months will need to be followed for an additional 9 months to provide the requisite number of PFS events.
The analysis of OS will be conducted when all randomized subjects (accrued over 18 months) have been followed for ≥ 12 months following enrollment of the final subject. It is estimated that 112 OS events will be accrued during this time, providing 72.8% power at a 1-sided alpha of 0.10 to detect a HR of 0.70. This HR represents a 30% reduction in the risk of death, and a 42.9% increase in the median OS. Assuming a median OS of 11 months in the control arm, the median OS in the combination arm will be 15.7 months.
9.1.2 Subject Population(s) for Analysis
The analysis populations are:
Intent to Treat (ITT) Population: The ITT population will include all randomized subjects in the study. This population will be used for efficacy analyses. If the randomized treatment arm differs from the actual treatment for a given subject, that subject will be analyzed according to the randomized treatment arm.
Per Protocol (PP) Population: The PP population will include all subjects who have at least one tumor assessment after receiving at least one dose of IP and have no major protocol deviations that could impact efficacy assessments. This population will be defined in detail in the
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 58 Confidential Information 14-Jun-2013
Statistical Analysis Plan (SAP) prior to final database lock and unblinding for the primary analysis.
Safety Population: The safety population will include all subjects who receive at least one dose of IP. This population will be used for safety analyses. If the randomized treatment arm differs from the actual treatment for a given subject, that subject will be analyzed according to the actual treatment arm.
Other analysis populations may be defined, if required, in the detailed SAP.
9.2 Statistical Methods
A detailed SAP will be finalized before the primary database lock and unblinding. This analysis plan may modify what is outlined in the protocol; however, any major modifications of the primary endpoint definition or its analysis will also be reflected in a protocol amendment.
9.2.1 Efficacy 9.2.1.1 Primary Efficacy Endpoint
Review by a central radiologist, blinded to subject treatment assignments and independent from the clinical sites, will assess all tumor responses. The resulting response data will serve as primary clinical efficacy data for the trial. Deaths on study will also contribute to the PFS endpoint. PFS is defined as the duration of time from randomization to time of irPD or death, whichever comes first, or the last tumor assessment date for censored subjects.
The primary efficacy endpoint, PFS, will be summarized and displayed by treatment group using Kaplan-Meier methods (SAS® PROC LIFETEST). Point estimates (25th, 50th, and 75th percentiles) will be provided, along with a 1-sided 90% confidence interval (CI). Treatments will be compared for the ITT population using a stratified log-rank test, with randomization stratification factors included, as the primary analysis. The HR between the 2 study arms, as well as the associated 90% CI, will be presented using Cox proportional hazards regression (SAS® PROC PHREG) controlling for randomization stratification factors. Kaplan-Meier plots will be presented.
The primary analysis will be a stratified log-rank test (using the randomization stratification factors) comparing PFS between the 2 randomized arms in the ITT population.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 59 Confidential Information 14-Jun-2013
9.2.1.2 Secondary Efficacy Endpoint
Secondary efficacy endpoints include:
• Overall survival (OS)
• Tumor response based on irRECIST v1.1[19]:
— Objective response rate (ORR)
— Duration of best response (DOBR)
— Disease control rate (DCR)
— Duration of disease control (DDC)
Overall Survival
OS will be measured from the date of subject randomization until death or the last follow up date for censored subjects. OS will be summarized and analyzed in the same manner as PFS.
Tumor response
For each secondary endpoint involving tumor responses, assessments per the central-radiology review will be presented and analyzed as primary.
The number and percent of subjects achieving objective response (irCR or irPR) will be tabulated for ITT population subjects treated with SOC plus VTX-2337 versus those treated with SOC plus placebo. The number and percent of subjects achieving disease control (irSD, irPR, or irCR) will be tabulated in the same manner. As well, the number and percent of subjects exhibiting each level of best tumor response (irCR, irPR, irSD, irPD, or missing) will be presented by treatment group for the ITT population. Stratified Cochran-Mantel-Haenszel mean scores tests (SAS® PROC FREQ) will be used to compare tumor response rates between the 2 study arms while controlling for randomization stratification factors. In addition, maximum change in TMTB from baseline in ITT population subjects will be presented graphically.
Duration of best response—measured in days—will be defined as the duration of time from the date measurement criteria are first met for irCR, or irPR (if irCR is never met), until the first date that irPD is confirmed by the central radiology review, or death, whichever comes first, or the last tumor assessment date for censored subjects. DOBR will be calculated only for responding subjects (irCR or irPR) as assessed by irRECIST. DOBR will be summarized and displayed by treatment group using Kaplan-Meier methods. Point estimates (25th, 50th, and 75th percentiles) will be provided, along with 1-sided 90% CIs.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 60 Confidential Information 14-Jun-2013
Duration of disease control—measured in days—will be defined as the duration of time from the date measurement criteria are first met for irCR, irPR, or irSD to the first date that irPD is confirmed by the central radiology review, or death, whichever comes first, or the last tumor assessment date for censored subjects. DDC will be calculated only for subjects who achieve disease control (irCR, irPR or irSD) as assessed by irRECIST. DDC will be summarized and displayed in the same manner as DBR.
9.2.1.3 Sensitivity Analysis
Analyses on the PP population will be performed for the primary and the secondary efficacy endpoints and serve as supportive analyses for the ITT analyses.
9.2.2 Safety
AEs, vital signs, ECG, and safety laboratory data (peripheral blood hematology, serum chemistry, and urinalysis) will be presented descriptively. All AEs, vital signs, ECGs, and clinical laboratory abnormalities will be presented. Safety data will be presented in tabular and/or graphical format and summarized descriptively by treatment group and time point, where appropriate. Descriptive statistics will be shown for baseline, scheduled visits, and the change from baseline to these visits, as applicable.
A DSMB of at least three independent members with expertise in the patient population, statistics, and/or clinical research will be appointed to monitor subject safety data while the trial is ongoing. The DSMB will meet at predetermined intervals set forth in the DSMB Charter—approximately every 6 months—to review toxicities and serious and/or unexpected adverse events. The DSMB will primarily evaluate safety data; efficacy data will only be reviewed in the event of a serious safety concern. Minutes for all meetings will be generated.
To address any new or unexpected safety issues, the first DSMB meeting will occur after an unblinded statistician has confirmed that 6 subjects, who have been randomized to receive VTX-2337, have completed one cycle of therapy. The purpose of this meeting is to evaluate any DLTs or any acute, unexpected, or synergistic toxicities associated with the combination of VTX-2337, platinum, 5-FU, and cetuximab. If > 1 of these first 6 subjects experiences a DLT or other unacceptable toxicity, the DSMB may recommend that the starting dose of VTX-2337/placebo be reduced by one dose level (§7.4). If a dose reduction is recommended, a similar analysis of 6 subjects treated at the reduced starting dose will occur. In the event the starting dose of VTX-2337/placebo is reduced, the sample size for the trial will be adjusted so that 175 subjects will be treated at the modified starting dose.
Refer to §8.1.3 for DLT definition.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 61 Confidential Information 14-Jun-2013
Adverse Events
AEs will be coded using the Medical Dictionary for Regulatory Activities (MedDRA). All AEs will be listed. Treatment-emergent AEs (TEAEs) are those which first occur or increase in severity or relationship to study drug after the first dose of study drug. AEs with missing date of onset will be considered treatment-emergent. The number and percent of patients reporting TEAEs will be tabulated by system organ class and preferred term and categorized by treatment group. AEs will be further classified by severity and relationship to treatment in tabulations. Tables and/or narratives of any on-study death, or SAE, as well as early withdrawals because of AEs, will be provided. The relationship between drug exposure and adverse events will be evaluated qualitatively.
Electrocardiogram
Descriptive statistics for QRS, QTc, QT and HR will be presented for baseline, End of Treatment visit, and the change from baseline to End of Treatment. The incidence of outliers in absolute QTcF and QTcB intervals (> 450 to ≤ 480, > 480 to ≤ 500, and > 500 msec) and the absolute uncorrected QT intervals (> 500 msec) at End of Treatment, as well as changes from baseline in QTcF and QTcB (> 30 to ≤ 60 and > 60 msec) will be summarized by treatment group.
Laboratory Values
Laboratory test results will be converted to International System of Units (SI) units. Abnormal laboratory results will be graded with the NCI-CTCAE (Version 4.03) standard. Descriptive statistics will be shown for baseline, scheduled visits, and the change from baseline to these visits. Shift summaries of NCI-CTCAE grade from baseline to worst post-baseline result will be provided by treatment group. In addition, selected parameters will be displayed graphically over time by treatment group.
9.2.3 Other Data
Demographics, Baseline Characteristics, and Disposition
Demographic information and baseline characteristics will be summarized for the ITT population. Demographic data will be summarized by treatment group and will include summary statistics for age, age group (≤ 60, > 60), race, sex, height, and weight. General medical history data and oncology history data will also be tabulated by treatment group using counts and percentages. Oncology history will include prior anticancer interventions, histological or cytological confirmation of SCCHN, tumor staging according to the TNM Classification of Malignant Tumors, HPV status (for patients with oropharyngeal carcinoma only), prior chemotherapy for SCCHN (Yes or No), and ECOG performance status (0 or 1).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 62 Confidential Information 14-Jun-2013
The disposition of all randomized subjects will be summarized. These data will include the number of subjects enrolled (randomized), receiving study treatment, assigned to each dose group, and prematurely discontinuing from the study and the reason(s) for premature discontinuation.
Extent of Exposure
Dosing data will be summarized by treatment group to include duration of treatment (days), cumulative dose and dose intensity, and number (%) of patients with dose modifications.
Concomitant Medications
Concomitant medications will be presented in data listings and coded using the WHODRUG dictionary. Concomitant medications will be summarized by treatment group and preferred drug names.
Translational Research Assessments
Statistical evaluation of translational research assessments will be described in SAP.
9.3 Schedule of Analyses
The primary analysis will be conducted when 134 PFS events have accrued on study. The secondary efficacy analysis (OS) will be conducted approximately 12 months following randomization of the last subject. It is anticipated that approximately 112 OS events will have occurred at the time of the secondary analysis on OS. Two database locks will be scheduled for the 2 analyses, at the time points described above. Additional analyses may be performed and will be outlined in the SAP.
9.4 Termination Criteria
Enrollment in the study will end when at least 175 subjects have been enrolled, to provide approximately 88 subjects per treatment group. Subjects who discontinue the study prior to receiving their first dose of IP will be replaced. A dropout rate of approximately 10% over the life of the study is assumed. The end of the trial is defined as the date when the final analysis of the OS endpoint is completed.
9.5 Deviation Reporting
Major protocol deviations will be presented in a listing.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 63 Confidential Information 14-Jun-2013
10.0 REGULATORY, QUALITY, AND ADMINISTRATIVE REQUIREMENTS 10.1 Trial Conduct
This study will be conducted in compliance with the protocol issued by VentiRx Pharmaceuticals and approved by the IRB/IEC and according to FDA regulations, applicable Competent Authorities and Guidelines for Good Clinical Practice (21 CFR §312 and ICH Guidance E6). No deviation from the protocol will be implemented without the prior approval from the study’s sponsor or its representative, as well as review and approval from the IRB/IEC except where it may be necessary to eliminate an immediate hazard to a research subject. In such cases, the deviation will be reported to the IRB/IEC and VentiRx Pharmaceuticals, or their respresentative, as soon as possible.
10.2 Ethical Considerations 10.2.1 Informed Consent
Patients meeting the criteria set forth in the protocol may be offered the opportunity to participate in this study. Candidate subjects or their legal guardians will receive a comprehensive explanation of the study, including the nature and investigational status of the IP, any known previously experienced adverse reactions, alternative therapies available and other factors which are part of obtaining appropriately informed consent. Patients will be given the opportunity to ask questions of qualified personnel who are knowledgeable about the study and provide adequate time to consider whether or not to participate.
Informed consent will be documented with an ICF that has been approved by the institution’s IRB/IEC. The ICF is to be signed and dated by the subject or subject’s legally authorized representative, by the person who conducts the consent process and any additional signatures required by the institution’s IRB/IEC. The original signed ICF will be filed in the subject’s medical record and a copy of the signed ICF will be given to the subject or the subject’s legally authorized representative. The subject’s medical record should contain a notation that written informed consent was obtained and a written description of the consent process.
Any changes to the ICF (e.g., in the event of a protocol amendment that changes the study’s procedures or alters its scope, or if significant new information regarding the safety or efficacy of the investigational drug becomes available) must be reviewed and approved by the IRB/IEC. The revised ICF must be used to re-consent any subject currently enrolled in the study who is affected by the change.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 64 Confidential Information 14-Jun-2013
10.2.2 Institutional Review Board/Ethics Committee Approval
The protocol and all relevant supporting materials, including the IB and Informed Consent Form, must be submitted to the appropriate IRB/IEC for review and approval. A copy of the IRB/IEC’s written approval must be provided to the study’s sponsor or its representative prior to initiation of the study and commencement of the subject screening and enrollment. The IRB/IEC should be informed by the investigator of the study’s progress and provide written documentation of the periodic review and ongoing approval according to IRB/IEC policies.
Any changes in the study protocol, revisions to the ICF, and all unanticipated problems involving risks to human subjects (e.g., SAEs occurring at the clinical site, INDSRs) must be reported promptly to the IRB/IEC and according to institutional and IRB/IEC requirements. Written approval from the IRB/IEC must be obtained prior to implementation of any change(s), if applicable.
10.2.3 Subject Privacy
The investigator, CRO, VentiRx Pharmaceuticals, and representatives of VentiRx Pharmaceuticals shall comply with all applicable local, state and federal privacy laws. The medical records of participating subjects are considered confidential and disclosure to third parties other than those noted below is prohibited.
The medical records of participating study subjects and all data generated as a result of participation in this study are to be available for review upon request by the FDA or other regulatory authorities, VentiRx Pharmaceutics or its representatives, and by the IRB/IEC. The IRB/IEC-approved ICF must clearly indicate that the subject’s medical records will be inspected by said parties and permission for such review is a requirement for study participation.
10.3 Investigator Responsibilities and Requirements
By agreeing to participate in this clinical trial, the Principal Investigator and all subinvestigators agree to perform the study in accordance with all stipulations of the protocol, the FDA Code of Federal Regulations (21 CFR Parts 11, 50, 54, 56 and 312), applicable local regulation(s) and ICH Guidelines for GCP (E6).
Prior to initiation of the study the Principal Investigator must, at minimum, provide VentiRx or its representative with the following documentation:
• Signed clinical trial agreement
• Signed Principal Investigator Protocol Agreement
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 65 Confidential Information 14-Jun-2013
• Signed FDA Form 1572 or equivalent
• Curriculum Vitae of the Principal Investigator
• Current medical license(s) for the Principal Investigator
• Copy of written IRB/IEC approval for the study and informed consent form
• Financial disclosure for the Principal Investigator
The Principal Investigator is responsible for complying with all commitments as delineated in Box 9 of FDA form 1572 and/or local regulations.
10.4 Data Identification, Handling, and Record Keeping 10.4.1 Source Documentation
Adequate and accurate case histories, which record all data and observations relevant to the clinical investigation, should be prepared and maintained for each subject screened or randomized in the study. Such source documentation includes all original documents or medical records regarding the subject’s participation in the study, including medical history, notes from the physician or nurse, the subject’s laboratory reports, imaging studies, electrocardiogram tracings, hospital records and details regarding the distribution of the investigational drug.
10.4.2 Case Report Forms and Electronic Data Capture
The investigator will be provided with access to a secure, web-based system that is compliant with 21 CFR §11 for capturing and reporting all study-related data ( EDC). Such data will be entered into the EDC system by the investigator and site personnel in a timely and accurate manner. The investigator must review all submitted data for accuracy and consistency with the protocol and authorize the data for each subject upon completion.
All required fields on the electronic case report forms (CRFs) must be filled in and 100% of the information collected on CRFs must be verifiable through review of the original source documentation.
10.4.3 Essential Documents
The Principal Investigator and clinical site personnel are responsible for maintaining an organized, comprehensive file of all essential documents required to demonstrate compliance with regulatory requirements. Such documents include, but are not limited to:
• Protocol with all amendments, signed Principal Investigator Protocol Agreement(s) and informed consent form(s)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 66 Confidential Information 14-Jun-2013
• IB, including all updates
• Copy of the signed FDA Form 1572
• CVs and medical licenses for the Principal Investigator and subinvestigators
• IRB/IEC approval of the protocol and amendment(s), informed consent form(s) and any other study-related materials
• IRB/IEC membership list or Letter of Assurance
• Subject Screening and Enrollment Log, which may be obtained from EDC
• IRB/IEC submissions of SAEs that have occurred at the institution and of INDSRs provided by the study’s sponsor
• Laboratory certifications and reference ranges
• Significant correspondence from VentiRx Pharmaceuticals or CRO
• Other documents as required by local regulatory authorities
These files must be available for inspection by VentiRx Pharmaceuticals, their representatives, the IRB/IEC, or regulatory authorities at any time.
10.4.4 Record Retention
All study related documentation noted in §10.4.1, §10.4.2 and §10.4.3 above must be maintained in accordance with FDA and local regulations. For sites in the US, as described in 21 CFR §312.62, the investigator will retain all such study records for a period of 2 years after marketing approval is received for VTX-2337, or for 2 years after all clinical and product development of VTX-2337 is discontinued. Investigators should not destroy any records relating to this study without prior approval from VentiRx Pharmaceuticals.
10.5 Quality Control and Quality Assurance 10.5.1 Site Training and Monitoring Procedures
Prior to the initiation of the study, personnel from the sponsor or its representatives will meet with the investigator and clinical staff to review and discuss the protocol, the investigational drug, study procedures, drug accountability, adverse event reporting, ICH/GCP guidelines, CRF completion guidelines, record keeping and administrative requirements, monitoring requirements, and the ability of the site to adequately conduct the protocol. During the course of the study, representatives from the sponsor will provide additional study-specific training to site staff upon request by the investigator, in response to a change in key clinical site staff, or if
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 67 Confidential Information 14-Jun-2013
issues with study conduct or GCP compliance are observed during the course of routine monitoring visits.
A representative from VentiRx Pharmaceuticals will visit the clinical site periodically to monitor adherence to the protocol, to review and retrieve study-related data, and/or documents. The frequency of monitoring visits depends on the rate of enrollment at the site and the investigator will permit the sponsor’s representative to monitor the study as frequently as the sponsor deems necessary to determine that protocol adherence and data collection are acceptable. The monitor will be permitted full access to subjects’ complete medical records. CRFs will be reviewed and compared to the subject’s case history to ensure the accuracy of the reported data and that key data are collected and recorded as specified by the protocol. Other study records, such as essential regulatory documents, subject screening log, and drug disposition logs will also be inspected.
10.5.2 Data Management Procedures
VentiRx Pharmaceuticals or its designee will prepare guidelines for database setup, data review, quality control, and database lock at the conclusion of the study—including procedures for electronic edit checks. CRF Completion Guidelines will be prepared to guide the data entry activities completed by the sites. The database will be validated following established procedures. Electronic databases that hold subject study data will conform to 21 CFR §11 requirements.
10.5.3 Auditing Procedures
VentiRx Pharmaceuticals and the applicable Competent Authorities maintain the right to conduct audit(s) at the clinical site.
11.0 SUPPLEMENTS Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 68 Confidential Information 14-Jun-2013
11.1 ECOG Performance Status Assessment
Grade ECOG 0 Fully active, able to carry on all pre-disease performance without restriction 1 Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or
sedentary nature, e.g., light house work, office work 2 Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about
more than 50% of waking hours. 3 Capable of only limited selfcare, confined to bed or chair more than 50% of waking hours. 4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or chair. 5 Dead
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 69 Confidential Information 14-Jun-2013
11.2 Baseline Tumor Evaluation and Categorization: RECIST v1.1 11.2.1 Categorization of Tumors
All tumor lesions will be categorized at baseline as either one of the following:
• Measurable: lesions that can be accurately measured in at least one dimension (longest diameter to be recorded) as ≥ 10 mm for soft tissue lesions and ≥ 15 mm in short axis for lymph nodes with CT or MRI scan. All tumor measurements must be recorded in decimal fractions of centimeters.
• Non-measurable: All other lesions (or sites of disease), including small lesions (longest diameter < 10 mm or pathological lymph nodes with ≥ 10 to < 15 mm short axis), are considered non-measurable disease. Leptomeningeal disease, ascites, pleural/pericardial effusions, lymphangitis cutis/pulmonitis, inflammatory breast disease, and abdominal/pelvic masses (identified by physical exam and not CT or MRI) are considered as non-measurable.
11.2.2 Special considerations regarding lesion measurability
Bone lesions: Lytic bone lesions or mixed lytic-blastic lesions, with identifiable soft tissue components, that can be evaluated by CT or MRI can be considered as measurable lesions if the soft tissue component meets the definition of measurability described above. Blastic bone lesions are non-measurable.
Cystic lesions that meet the criteria for radiographically defined simple cysts should not be considered as malignant lesions (neither measurable nor non-measurable) since they are, by definition, simple cysts. “Cystic lesions” thought to represent cystic metastases can be considered as measurable lesions, if they meet the definition of measurability described above. However, if non-cystic lesions are present in the same subject, these are preferred for selection as target lesions.
Lesions with prior local treatment (e.g., tumor lesions that are situated in a previously irradiated area) will not be considered measureable unless progression is documented or a biopsy is obtained to confirm persistence at least 90 days following completion of radiation therapy.
11.2.3 Methods of Assessment
The same method of assessment and the same technique should be used to characterize each identified and reported lesion at baseline and during follow-up.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 70 Confidential Information 14-Jun-2013
All measurements should be taken and recorded in metric notation using a ruler. All baseline evaluations should be performed as closely as possible to the beginning of treatment and never more than 28 days before the beginning of treatment.
Clinical lesions: Superficial clinical lesions measured by caliper or ruler will not be used to assess tumor response in this study.
Conventional CT and MRI: CT slice thickness should be ≤ 5 mm. MRI is also acceptable in certain situations (e.g., for body scans), but NOT lung.
Use of MRI remains a complex issue. MRI has excellent contrast, special and temporal resolution; however, there are many image acquisition variables involved in MRI, which greatly impact image quality, lesions conspicuity, and measurement. Furthermore, the availability of MRI is variable globally. As with CT, if an MRI is performed, the technical specifications of the scanning sequences used should be optimized for the evaluation of the type and site of disease. Furthermore, as with CT, the modality used at follow-up should be the same as was used at baseline and the lesions should be measured/assessed on the same pulse sequence parameters for all scanners, body parts, and diseases. Ideally, subsequent image acquisitions should use the same type of scanner and follow the baseline imaging protocol as closely as possible. If possible, body scans should be performed with breath-hold scanning techniques.
PET-CT: PET-CT is an acceptable means of imaging if the CT is of diagnostic quality and meets with the requirements in the Imaging Manual.
FDG-PET: FDG-PET will not be used to assess tumor response in this study.
Ultrasound: Ultrasound will not be used to assess tumor response in this study.
Endoscopy, Laparoscopy: Endoscopy, Laparoscopy will not be used to assess tumor response in this study.
Cytology, Histology: In rare cases, these techniques can be used to differentiate between PR and CR.
It is mandatory to obtain cytological confirmation of the neoplastic origin of any effusion that appears or worsens during treatment when measurable disease has met criteria for response or stable disease. This confirmation is necessary to differentiate response or stable disease versus progressive disease, as an effusion may be a side effect of the treatment.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 71 Confidential Information 14-Jun-2013
11.2.4 Baseline documentation of “Target” and “Non-Target” lesions
Target lesions: All measurable lesions, up to a maximum of 2 lesions per organ and 5 lesions in total—representative of all involved organs—should be identified as target lesions and recorded and measured at baseline. Target lesions should be selected on the basis of their size (lesions with the longest diameter), be representative of all involved organs and in addition should be those that lend themselves to reproducible repeated measurements. It may be the case that, on occasion, the largest lesion does not lend itself to reproducible measurement, in which circumstance the next largest lesion which can be reproducibly measured should be selected.
The sum of the diameters (long axis for non-nodal lesions, short axis for nodal lesions) of all target lesions will be calculated and reported as the baseline sum of diameters (baseline TMTB). If lymph nodes are to be included in the sum, then only the short axis is added into the sum. The baseline TMTB will be used as reference to further characterize any objective tumor regression in the measurable dimension of the disease.
Non-target lesions: All other lesions (or sites of disease), including any measurable lesions over and above the 5 target lesions, should be identified as non-target lesions and should also be recorded at baseline. Measurements of these lesions are not required, but the presence, absence, or in rare cases unequivocal progression of each should be noted throughout follow-up.
Malignant lymph nodes: To be considered pathologically enlarged and measurable, a lymph node must be ≥ 15 mm in short axis when assessed by CT scan (CT scan slice thickness ≥ 5 mm). At baseline and in follow-up, only the short axis will be measured and followed.
11.3 Response Assessment: immune-related RECIST (irRECIST)
As previously noted, this study will assess tumor response with an immune-related modification of RECIST v1.1 (referred to as irRECIST). The response criteria from standard RECIST v1.1 has, therefore, not been included in this protocol.
Determination of response via irRECIST will take into consideration all target and non-target lesions.
11.3.1 Total Measured Tumor Burden
TMTB is established at baseline as the sum of the longest diameters (SOD)—the shortest axes should be used for lymph nodes—of all target lesions (≤ 2 lesions per organ, ≤ 5 lesions total). At each subsequent TA, the SOD of new, measurable lesions (≥ 10 mm [lymph nodes ≥ 15 mm
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 72 Confidential Information 14-Jun-2013
in shortest diameter]; ≤ 2 new lesions per organ, ≤ 5 new lesions total) is added to the SOD of the target lesions to provide the updated TMTB:
TMTB = SOD target lesions + SOD new, measurable lesions
If there are more than 2 new lesions per organ or more than 5 new lesions total, the lesions added to the TMTB should be selected on the basis of their size (i.e., lesions with the longest diameter should be selected).
Percentage changes in TMTB at each TA describe the size and growth kinetics of both old and new, measurable lesions as they appear. At each TA, the response in TMTB is defined as follows:
• Complete Response (irCR): Complete disappearance of all target and new, measurable lesions, with the exceptions of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
11.3.2 Response in Non-Target Lesions
The presence of non-target lesions is established at baseline; at each TA, the presence of any new, non-measurable lesions is assessed. The presence of new, non-measurable lesions will rule out an overall response of irCR. An increase in the size or number of new, non-measurable lesions does not necessarily imply an overall response of irPD; if these lesions become measurable (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; up to 2 new lesions per organ, total 5 new lesions) at a subsequent TA, their measurement will, at that point, start to contribute to the TMTB.
The response in non-target lesions is defined as follows:
• Complete Response (irCR): Complete disappearance of all non-target lesions
• non-irCR/non-irPD: Non-target lesions do not meet the criteria for irCR or irPD
• Progressive Disease (irPD): Unequivocal increase in the number or size of non-target lesions. To achieve unequivocal progression of non-target lesions, there must be a substantial worsening of non-target disease of a magnitude that, according to the treating physician, warrants a change in anticancer therapy
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 73 Confidential Information 14-Jun-2013
NOTE: Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing lesions) should be considered irSD and treatment may continue until the next scheduled assessment.
11.3.3 Overall Response
The overall response (OR) according to irRECIST is derived from the responses in TMTB as well as the presence of any non-target lesions as follows:
• Complete Response (irCR): Complete disappearance of all lesions (whether measurable or not); lymph nodes must decrease to < 10 mm in shortest dimension
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
The immune-related best overall response (irBOR) is the best irRECIST OR over the study as a whole, recorded between the date of first dose until the last TA prior to subsequent anticancer therapy for individual subjects. An assessment of disease progression at or before week 12 (unconfirmed irPD at week 12) will not preclude an irBOR of irCR, irPR, or irSD. Conversely, an assessment of irPD at or after Week 12 (confirmed irPD at week 12), will preclude a subsequent irBOR of irCR, irPR, or irSD. However, any post-progression clinical activity in subjects with irBOR of irPD may be summarized for exploratory purposes.
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 74 Confidential Information 14-Jun-2013
Table 9: Best Overall Response (irBOR)
Target Lesions Baseline (Index) and New
Measurable Lesions Non-Target Lesions*
irRC Overall Response Total Measurable Tumor
Burden (TMTB) Baseline Lesions Unequivocal New Lesions
irCR irCR No irCR
irCR irSD No irPR
irPR irCR or irSD No irPR
irSD irCR or irSD No irSD
irPD Any Yes or No irPD
Any Unequivocal Progression Yes or No irPD
Any Any Yes irPD
*Any increase in the size or number of non-measurable lesions does not necessarily imply an overall response of irPD. If new lesions become measureable (≥ 10 mm) at a subsequent TA, their measurement will at that point start to contribute to the TMTB. To achieve unequivocal progression of non-target lesions, there must be an overall level of substantial worsening in non-target disease that is of a magnitude that the treating physician would feel it is important to change therapy. Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing locations) should be considered irSD and treatment may continue until the next schedule assessment.
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 75 Confidential Information 14-Jun-2013
11.4 List of CYP3A4 Inhibitors and/or Inducers
Table 10 includes example CYP3A4 inhibitors and inducers. CYP3A4 inducers and inhibitors should be administered with caution and, if possible, alternatives that do not affect CYP3A4 should be administered instead (§7.6).
Table 10: Examples of CYP3A4 Inhibitors and Inducers
Inhibitors Inducers
Amiodarone Indinavir Barbiturates
Aprepitant Itraconazole Carbamazepine
Chloramphenicol Ketoconazole Efavirenz
Cimetidine Mibefradil Glucocorticoids
Ciprofloxacin Mifepristone Modafinil
Clarithromycin Nefazodone Nevirapine
Delavirdine Nelfinavir Oxcarbazepine
Diethyl-dithiocarbamate Norfloxacin Phenobarbital
Diltiazem Norfluoxetine Phenytoin
Erythromycin Ritonavir Pioglitazone
Fluconazole Saquinavir Rifabutin
Fluvoxamine Star fruit Rifampin
Gestodene Telithromycin St. John’s wort
Grapefruit juice Verapamil Troglitazone
Imatinib Voriconazole --
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 76 Confidential Information 14-Jun-2013
11.5 List of Abbreviations
Abbreviation or Term Definition/Explanation
5-FU Fluorouracil
ADCC Antiobody-dependent cellular cytotoxicity
AE Adverse Event
ALT (SGPT) Alanine aminotransferase (Serum Glutamic Pyruvic Transaminase)
ANC Absolute neutrophil count
API Active pharmaceutical ingredient
AST (SGOT) Aspartate aminotransferase (Serum Glutamic Oxaloacetic Transaminase)
AUC Area under the curve
BOR Best overall response
BP Blood pressure
C Celsius
CBC Complete blood count
CI Confidence interval
CR Complete response
CRF Case report form
CRO Contract research organization
CRS Cytokine release syndrome
CRx Concomitant medication
CT Computed tomography
DCR Disease control rate
DDC Duration of disease control
DLT Dose-limiting toxicity
DOBR Duration of best response
DSMB Data safety monitoring board
EC50 Half maximal effective concentration
ECG Electrocardiogram
ECOG Eastern cooperative oncology group
EGFR Epidermal growth factor receptor
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 77 Confidential Information 14-Jun-2013
Abbreviation or Term Definition/Explanation
F Fahrenheit
FDA Food and Drug Administration
GCP Good Clinical Practice
GFR Glomerular Filtration Rate
GOG Gynecologic oncology group
HNC Head and neck carncioma
HPV Human papilloma virus
HR Heart rate
HR Hazard ration
IB Investigator’s Brochure
ICF Informed consent form
ICH International Conference on Harmonization
IEC Independent ethics committee
IND Investigational new drug
INDSR Investigational new drug safety report
IP Investigational product
IRB Institutional Review Board
irRECIST immune-related response evaluation criteria in solid tumors
IV Intravenous
IXRS Interactive voice/web response system
M Meter
mDC Myeloid Dendritic Cell
MedDRA Medical dictionary for regulatory activities
Mg Milligram
Min minute
mL Milliliter
MRI Magnetic resonance imaging
NK Natural killer
Nm Nano molar
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 78 Confidential Information 14-Jun-2013
Abbreviation or Term Definition/Explanation
ORR Objective response rate
OS Overall survival
PBMC Peripheral mononuclear cells
PD Pharmacodynamic
PD Progressive disease
PE Physical examination
pH Hydrogen ion concentration
PFS Progression free survival
PK Pharmacokinetic
PLD Pegylated liposomal doxorubicin
PR Partial response
RECIST Response evaluation criteria in solid tumors
RR Respiration rate
SAE Serious Adverse Event
SD Stable disease
SGOT (AST) Serum Glutamic Oxaloacetic Transaminase
SGPT (ALT) Serum Glutamic Pyruvic Transaminase
SC Subcutaneous
SI International system of units
SOC Standard-of-care
SOD Sum of diameters
SUSAR Suspected unexpected serious adverse reactions
t½ Terminal elimination phase half-life
T Temperature
t1/2 Mean half life
TA Tumor assessment
TEAE Treatment emergent adverse events
TLR Toll-like Receptor
TMTB Total measured tumor burden
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 79 Confidential Information 14-Jun-2013
Abbreviation or Term Definition/Explanation
ULN Upper Limit of Normal
µM micro molar
US United States
WBC White blood cell
WHO-DRUG World Health Organization-Drug Reference List
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 80 Confidential Information 14-Jun-2013
12.0 LITERATURE AND REFERENCES
1. Smith, E.M., et al., Tobacco and alcohol use increases the risk of both HPV-associated and HPV-independent head and neck cancers. Cancer Causes Control, 2010. 21:1369-1378.
2. Carvalho, A.L., et al., Trends in incidence and prognosis for head and neck cancer in the United States: a site-specific analysis of the SEER database. Int J Cancer, 2005. 114(5): p. 806-16.
3. Davies, L. and H.G. Welch, Epidemiology of head and neck cancer in the United States. Otolaryngol Head Neck Surg, 2006. 135(3): p. 451-7.
4. Curado, M.P. and M. Hashibe, Recent changes in the epidemiology of head and neck cancer. Curr Opin Oncol, 2009. 21(3): p. 194-200.
5. Hobbs, C.G., et al., Human papillomavirus and head and neck cancer: a systematic review and meta-analysis. Clin Otolaryngol, 2006. 31(4): p. 259-66.
6. Dobrossy, L., Epidemiology of head and neck cancer: magnitude of the problem. Cancer Metastasis Rev, 2005. 24(1): p. 9-17.
7. Argiris, A., et al., Head and neck cancer. Lancet, 2008. 371(9625): p. 1695-709.
8. Lango, M.N., Multimodal treatment for head and neck cancer. Surg Clin North Am, 2009. 89(1): p. 43-52, viii.
9. Ferrari, D., et al., A review on the treatment of relapsed/metastatic head and neck cancer. Expert Opin Pharmacother, 2009. 10(16): p. 2625-32.
10. Specenier, P.M. and J.B. Vermorken, Recurrent head and neck cancer: current treatment and future prospects. Expert Rev Anticancer Ther, 2008. 8(3): p. 375-91.
11. Ferlito, A., et al., Incidence and sites of distant metastases from head and neck cancer. ORL J Otorhinolaryngol Relat Spec, 2001. 63(4): p. 202-7.
12. Vermorken, J.B., et al., Platinum-Based chemotherapy plus Cetuximab in Head and Neck Cancer. N Engl J Med, 2008;359:1116-27.
13. Rivera, F., et al., Cetuximab in metastatic or recurrent head and neck cancer: the EXTREME trial. Expert Rev Anticancer Ther, 2009. 9(10): p. 1421-8.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 81 Confidential Information 14-Jun-2013
14. Boshoff, C. and M. Posner, Targeting EGFR in head and neck cancer: a decade of progress. Nat Clin Pract Oncol, 2009. 6(3): p. 123.
15. Lim, C., et al., VTX-2337, a Selective TLR8 Ligand, Enhances Cetuximab-mediated ADCC in Head and Neck Cancer, J Immunother, 2011. 34(9): p. 693.
16. Specenier, P.M. and J.B. Vermorken, Current concepts for the management of head and neck cancer: chemotherapy. Oral Oncol, 2009. 45(4-5): p. 409-15.
17. Lu, H., et al., VTX-2337 is a novel TLR8 agonist that activates NK cells and augments ADCC, Clin Cancer Res, 2012. 18(2):499-509
18. Stephenson, R., et al., TLR8 stimulation enhances cetuximab-mediated natural killer cell lysis of head and neck cancer cells and dendritic cell cross-priming of EGFR-specific CD8+ T cells, Cancer Immunol Immunother. May 2013.
19. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebbé C, Maio M, Binder M, Bohnsack O, Nichol G, Humphrey R, Hodi FS: Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria, Clin Cancer Res 2009, 15(23):7412–20
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 2 Confidential Information 03-Jun-2014
VentiRx Pharmaceuticals Protocol No. VRXP-A202
PRINCIPAL INVESTIGATOR PROTOCOL AGREEMENT
A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED STUDY OF CHEMOTHERAPY PLUS CETUXIMAB IN COMBINATION WITH VTX 2337 IN
PATIENTS WITH RECURRENT OR METASTATIC SQUAMOUS CELL CARCINOMA OF THE HEAD AND NECK
Version Date: 03-Jun-2014
I attest that I have read this protocol and the Investigator Brochure (IB) for VTX-2337. I agree to conduct the trial in accordance with the provisions herein, U.S. Food and Drug Administration (FDA) regulations, applicable Competent Authorities, International Conference on Harmonization (ICH) guidelines for Good Clinical Practice (GCP), state and local regulations and the requirements of the IRB/IEC.
I will provide copies of the current protocol and access to all information provided by VentiRx Pharmaceuticals, Inc. to the study personnel under my supervision. I will discuss this material with them to ensure that they are fully informed about the investigational drug and the study protocol.
Principal Investigator Signature Date
Principal Investigator Printed Name
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 3 Confidential Information 03-Jun-2014
TABLE OF CONTENTS 1.0 STUDY SYNOPSIS ...........................................................................................................5
2.0 BACKGROUND ..............................................................................................................10
2.1 Investigational Agent .............................................................................................11
2.2 Nonclinical Data ....................................................................................................11
2.3 Clinical Data ..........................................................................................................13
2.4 Risks/Benefits ........................................................................................................16
2.5 Dose Rationale .......................................................................................................17
2.6 Population ..............................................................................................................18
3.0 TRIAL RATIONALE AND OBJECTIVES ..................................................................18
3.1 Rationale ................................................................................................................18
3.2 Objectives ..............................................................................................................19
4.0 TRIAL DESIGN...............................................................................................................19
4.1 Study Design/Type.................................................................................................19
4.2 Endpoints ...............................................................................................................20
4.3 Procedures to Minimize Bias .................................................................................21
4.4 Maintenance of Blinding Procedures .....................................................................21
4.5 Trial Treatment ......................................................................................................22
4.6 Duration .................................................................................................................23
4.7 Discontinuation ......................................................................................................24
5.0 SELECTION OF SUBJECTS ........................................................................................24
5.1 Inclusion Criteria ...................................................................................................24
5.2 Exclusion Criteria ..................................................................................................25
6.0 CLINICAL TRIAL PROCESSES AND PROCEDURES ...........................................26
6.1 Subject Screening and Randomization (Day -14 to -1) .........................................27
6.2 Treatment Period ....................................................................................................28
6.3 End of Treatment ...................................................................................................32
6.4 Follow Up Period ...................................................................................................33
6.5 Early Treatment Discontinuation ...........................................................................35
6.6 Assessments ...........................................................................................................35
6.7 Monitoring for Subject Compliance ......................................................................41
7.0 TREATMENT ..................................................................................................................42
7.1 Packaging, Labeling and Storage ...........................................................................42
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 4 Confidential Information 03-Jun-2014
7.2 Preparation of Investigational Product ...................................................................42
7.3 Administration of Investigational Product and Study Treatment(s) ......................42
7.4 Dose Modifications ................................................................................................45
7.5 Emergency Unblinding ..........................................................................................53
7.6 Concomitant Medications and Supportive Care ....................................................53
7.7 Investigational Product Accountability ..................................................................56
8.0 ADVERSE EVENTS .......................................................................................................56
8.1 Definitions..............................................................................................................56
8.2 Reporting Requirements ........................................................................................58
8.3 Criteria for Determining Adverse Event Severity .................................................59
8.4 Criteria for Determining Adverse Event Expectedness .........................................60
8.5 Criteria for Determining Adverse Event Causality ................................................60
8.6 Expedited Reporting of Serious Adverse Events ...................................................61
9.0 STATISTICAL PLAN .....................................................................................................61
9.1 Statistical Considerations .......................................................................................61
9.2 Statistical Methods .................................................................................................63
9.3 Schedule of Analyses .............................................................................................67
9.4 Termination Criteria...............................................................................................67
9.5 Deviation Reporting ...............................................................................................67
10.0 REGULATORY, QUALITY, AND ADMINISTRATIVE REQUIREMENTS .........68
10.1 Trial Conduct .........................................................................................................68
10.2 Ethical Considerations ...........................................................................................68
10.3 Investigator Responsibilities and Requirements ....................................................69
10.4 Data Identification, Handling, and Record Keeping ..............................................70
10.5 Quality Control and Quality Assurance .................................................................71
11.0 SUPPLEMENTS ..............................................................................................................72
11.1 ECOG Performance Status Assessment.................................................................73
11.2 Baseline Tumor Evaluation and Categorization: RECIST v1.1 ............................74
11.3 Response Assessment: immune-related RECIST (irRECIST) ..............................77
11.4 Chemotherapy Dose Delay Algorithm...................................................................80
11.5 List of CYP3A4 Inhibitors and/or Inducers ...........................................................81
11.6 List of Abbreviations .............................................................................................82
12.0 LITERATURE AND REFERENCES............................................................................86
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 5 Confidential Information 03-Jun-2014
1.0 STUDY SYNOPSIS
Protocol Number VRXP-A202
Protocol Title A Randomized, Double-Blind, Placebo-Controlled Study of Chemotherapy Plus Cetuximab in Combination with VTX-2337 in Patients with Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck
Investigational Phase II
Investigational Product VTX-2337, a subcutaneously-administered Toll-like receptor 8 agonist
Study Sites Approximately 60 sites in North America
Study Duration Enrollment Period: Approximately 18 months Duration of Study: Approximately 36 months; following completion of accrual, all subjects will be followed for approximately 12 months
Study Population Adults who have not previously received systemic treatment for recurrent or metastatic squamous cell carcinoma of the head and neck
Study Design Randomized, double-blind, placebo-controlled, parallel group
Primary Objectives To compare the progression-free survival of subjects treated with cisplatin or carboplatin + fluorouracil (5-FU) + cetuximab combined with VTX-2337 to those treated with cisplatin or carboplatin + 5-FU + cetuximab alone (standard-of-care; SOC).
Secondary Objectives To compare the safety of subjects treated with SOC in combination with VTX-2337 to those treated with SOC alone. To compare the overall survival between the two treatment groups. To compare the best objective response rate (ORR), duration of best response (DOBR), disease control rate (DCR), and duration of disease control (DDC) between the two treatment groups.
Sample Size n=175
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 6 Confidential Information 03-Jun-2014
Inclusion Criteria Summary
1. Ability and willingness to provide written informed consent and to comply with the study’s visit and assessment schedule
2. Prior documentation of histologically or cytologically confirmed squamous cell carcinoma of the head and neck
3. Locoregionally recurrent or metastatic SCCHN that has not previously been treated with systemic therapy for recurrent or metastatic disease
4. At least one measurable lesion as defined by RECIST v1.1 (§11.1) on screening computed tomography (CT) or magnetic resonance imaging (MRI)
5. 18 years of age or older 6. ECOG performance status of 0 or 1 7. Acceptable bone marrow, renal, and hepatic function based upon screening
lab tests 8. Willingness to use medically acceptable contraception throughout the study
period and for 4 weeks after the final administration of IP 9. For female subjects with reproductive potential: a negative serum pregnancy
test
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 7 Confidential Information 03-Jun-2014
Exclusion Criteria Summary
1. Disease which is amenable to curative local therapy 2. Nasopharyngeal, salivary gland, lip, or sinonasal carcinoma 3. Major surgery or irradiation within 4 weeks of randomization 4. Prior systemic anti-cancer therapy, unless administered for localized SCCHN
and completed at least 6 months prior to disease recurrence 5. Treatment with an investigational agent within 30 days of randomization 6. Treatment with oral or parenteral corticosteroids within 2 weeks of
randomization or a requirement for chronic systemic immunosuppressive therapy for any reason
7. Prior serious infusion reaction to cetuximab 8. Treatment with an immunotherapy within 30 days of randomization 9. Known brain metastases, unless stable for at least 28 days prior to
randomization 10. Active autoimmune disease, defined as any autoimmune condition currently
requiring therapy (e.g., systemic lupus erythematosus, multiple sclerosis, inflammatory bowel disease, rheumatoid arthritis)
11. Known infection with HIV 12. Clinically significant cardiac disease (e.g., congestive heart failure, unstable
or uncontrolled angina, myocardial infarction) within 6 months of randomization
13. Pregnant or breast-feeding females 14. History of another primary malignancy, with the exception of the following:
• curatively resected non-melanoma skin cancer • curatively treated in situ cervical cancer • other malignancy curatively treated with no evidence of disease and
no anticancer therapy administered for at least 3 years prior to randomization, with the exception of adjuvant hormonal therapy for breast cancer
15. Any other condition or circumstance that could interfere with adherence to the study’s procedures or requirements, or otherwise compromise the study’s objectives
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 8 Confidential Information 03-Jun-2014
Study Drug Dose and Administration
VTX-2337 or placebo (investigational product; IP) will be administered as a subcutaneous injection on Day 8 and Day 15 of a 21-day cycle at a dose level of 3.0 mg/m2 for 6 cycles, followed by dosing on Days 8 and 22 of a 28-day cycle for cycles 7 and beyond. IP will be administered until disease progression. Standard-of-Care will consist of the following:
1. Cisplatin (100 mg/m2) OR carboplatin (AUC 5 mg/mL/min) administered as an IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles.
2. 5-FU (1000 mg/m2/day) administered as a continuous IV infusion on Days 1–4 of a 21-day cycle for a maximum of 6 cycles.
3. Cetuximab (initial dose: 400 mg/m2; remaining doses: 250 mg/m2) administered weekly until disease progression.
On days when investigational product and cetuximab are both dosed, IP will be administered first, followed by the cetuximab infusion.
Study Overview This is a randomized, double-blind, placebo-controlled, parallel group study to evaluate the safety and efficacy of VTX-2337 in combination with cisplatin or carboplatin, 5-FU and cetuximab in prolonging the progression-free survival in subjects with recurrent or metastatic squamous cell carcinoma of the head and neck. Subjects will be screened for eligibility and qualified subjects will be randomized 1:1 to 1 of 2 treatment groups:
− SOC + VTX-2337 − SOC + placebo
Tumor assessments will be by CT or MRI starting at Week 12 (± 3 days), then at Week 18 (± 3 days) and every 8 weeks (± 7 days) thereafter. Response will be evaluated by immune-related RECIST criteria (irRECIST) and confirmed by an independent radiologist. Upon independent confirmation of disease progression, active participation in the study is complete and subjects will undergo the End of Treatment evaluations. Subjects will be followed for survival until ~12 months after the last subject is randomized. Adverse events and safety will be evaluated throughout the study by an independent Data Safety Monitoring Board (DSMB). The DSMB will also conduct an assessment of the safety and tolerability of the starting dose.
Primary Outcome Measures
Progression-free survival will be assessed by serial imaging studies (CT or MRI) performed at baseline (Screening), Week 12 (± 3 days), Week 18 (± 3 days) and every 8 weeks (± 7 days) thereafter. Tumor response as evaluated by irRECIST. All tumor responses will be reviewed and confirmed by a central, independent radiologist. Whenever medically feasible and appropriate, suspected disease progression events should be confirmed by central review prior to completing the End of Treatment assessments and initiating new anti-cancer therapy.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 9 Confidential Information 03-Jun-2014
Secondary Outcome Measures
Safety will be assessed by physician or subject report of adverse events. Overall survival will be determined by report of subject vital status. Objective response rate, duration of best response, disease control rate, and duration of disease control will be assessed by irRECIST and evaluated by independent radiologist.
Statistical Considerations Randomization of all subjects will be stratified by prior systemic therapy for SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy as assigned by the investigator at the time of randomization (cisplatin or carboplatin). Sample size: n=175 subjects. Power, alpha and hazard ratio assumptions: see full protocol.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 10 Confidential Information 03-Jun-2014
2.0 BACKGROUND
Head and neck carcinomas (HNC) are the fifth most common cancer in the world, with increasing incidence.[1, 2] In the United States, 40,000 to 50,000 new cases are diagnosed and approximately 12,000 deaths due to this cause occur yearly.[2] HNCs describe malignancies of the upper aerodigestive tract which include squamous cell carcinomas of the oral cavity, nasopharynx, pharynx and larynx. While tobacco and alcohol use are the most common risk factors for HNCs, Epstein-Barr virus and human papilloma virus (HPV) may also play a role in the development of carcinomas of the nasopharynx and squamous cell carcinomas of the oropharynx, respectively.[1–6]
The majority of squamous cell carcinoma of the head and neck (SCCHN) cases (up to 75%) are diagnosed in its late stages (stages III or IV).[7, 8] Metastatic and recurrent SCCHN that is no longer amenable to local surgical/radiation therapy causes substantial morbidity and high mortality, with a median progression free survival (PFS) of ≤ 6 months due to the lack of effective therapeutic options.[9, 10, 11] Recurrent or metastatic disease has traditionally been managed with cytotoxic chemotherapies such as methotrexate, organoplatinum compounds, fluorouracil (5-FU), or taxanes—either alone or in combination. More recently, cetuximab (Erbitux®), the IgG1 monoclonal antibody which targets epidermal growth factor receptor (EGFR) was approved by FDA and Health Canada for use in combination with radiation therapy for the initial treatment of locally or regionally advanced SCCHN and by FDA for use as monotherapy in patients with recurrent or metastatic SCCHN who have progressed after platinum-based therapy and in combination with platinum-based therapy with 5-FU in patients with recurrent or metastatic SCCHN. Approval was based on clinical benefit and tolerability in the phase 3 setting.[12, 13] Namely, the addition of cetuximab to first-line platinum-based therapy with 5-FU resulted in an improvement of median overall survival (OS) from of 10.1 months compared to 7.4 months for patients treated with platinum/5-FU alone. As more than 90% of SCCHNs express the EGFR, targeting EGFR and its signaling pathway significantly advanced the treatment of SCCHN.[14] However, in this difficult-to-treat SCCHN population, the overall prognosis remains poor and the observed responses of 36% and a median time to progression of 5.6 months for cetuximab in combination with platinum and 5-FU are not ideal.[12, 13] Therefore, combinations that enhance response and provide clinical benefit, without significantly increasing toxicity, are still urgently needed.
One approach to enhance the efficacy of treatment with cetuximab plus chemotherapy in SCCHN is to add an immunomodulatory agent that would promote an anti-tumor immune response. Ideally, this agent would enhance both the effects of cetuximab (e.g., by augmenting antibody-dependent cellular cytotoxicity; ADCC) and chemotherapy (e.g., by modulating the tumor microenvironment and increasing T cell responses to antigenic debris generated by tumoricidal activity). One such candidate is VTX-2337, a modulator of Toll-like receptor 8
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 11 Confidential Information 03-Jun-2014
(TLR8). Activation of TLR8 enhances natural killer (NK) cells, myeloid-derived dendritic dendritic cells (mDC), and monocytes. VTX-2337 has demonstrated enhanced killing of SCCHN cells in combination with cetuximab, and synergistic activity with chemotherapy.[15]
The current study tests the hypothesis that the addition of VTX-2337 to the cetuximab plus platinum/5-FU regimen in locally recurrent and/or metastatic SCCHN patients will provide clinical benefit and will be reasonably well tolerated.
2.1 Investigational Agent
VTX-2337 is comprised of an active pharmaceutical ingredient (API) formulated at neutral pH in Captisol® (a cyclodextrin-based solubilizing agent). The API of VTX-2337 is VTX-378: a novel, small, organic molecule TLR8 agonist with a molecular weight of 458.6. VTX-2337 a lyophilized cake is supplied in sterile, single-use vials and is administered via subcutaneous injection.
The selectivity of this compound has been assessed in peripheral mononuclear cells (PBMC) and in cells engineered to express only a single TLR. In both PBMC and cell transfectants, VTX-2337 is highly selective for TLR8 with an EC50 of approximately 70 nM. VTX-2337 shows minimal activity for TLR7 (with an EC50 of approximately 3 μM), but does not stimulate other TLRs.[16]
Placebo contains Captisol and citric acid, the same excipient ingredients of the VTX-2337 formulation, but does not include the API VTX-378.
2.2 Nonclinical Data
Nonclinical studies have included in vitro and in vivo assessments of the pharmacologic, pharmacokinetic (PK), metabolism and toxicologic characteristics of VTX-2337. Extensive information regarding the pre-clinical evaluation of VTX-2337 may be found in the Investigator’s Brochure (IB).
2.2.1 Pharmacokinetics and Pharmacology
The PK and pharmacology of VTX-2337 have been broadly evaluated in non-human primates (cynomologus monkeys). The compound shows linear pharmacokinetics over a wide dose range, with a half-life (t1/2) of approximately 2–4 hours. VTX-2337 elicits the production of multiple inflammatory mediators—chemokines (e.g., MCP-1, MIP-1β), cytokines (e.g., IL-6, IL-1, TNFα, IL 12), acute phase proteins and shed cell surface antigens—which are consistent with activation of the innate immune system and can be readily measured in plasma. A clear pharmacokinetic-pharmacodynamic (PK/PD) relationship is observed for many of these inflammatory markers.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 12 Confidential Information 03-Jun-2014
Refer to §2.3 for information regarding PK/PD data in patients.
2.2.2 In Vitro ADCC and NK Observations
To characterize the potential for VTX-2337 to modulate immune function beyond the characterization in PD studies, immunophenotyping of peripheral blood and NK cell cytotoxic activity was assessed. These in vivo studies demonstrated that administration of VTX-2337 results in transient changes in blood cell populations consistent with cellular activation of neutrophils, NK cells, and T cells and may result in the transient extravasation of these latter cell populations from the blood compartment.[16]
In addition, VTX-2337 stimulates the production of cytokines from mDC, monocytes, and NK cells in vitro.[17] VTX-2337 stimulates ADCC when used in combination with a variety of monoclonal antibodies of the IgG1 subclass including rituximab and traztuzumab.[17] More recently, in collaboration with Dr. Robert Ferris at the University of Pittsburgh, it was demonstrated that VTX-2337 increases the cetuximab-mediated killing of SCCHN targets in an NK-dependent manner.[18] The TLR8 and NK-dependent enhancement of ADCC occurs in samples from patients of all three FcRγ3a genotypes, including those with the allele encoding the homozygous F/F variant that is associated with lower affinity for the Fc receptor.
In addition, the stimulation of mDC and monocytes concurrent with cetuximab administration was tested to determine the promotion of development of EGFR-specific T cells via a mechanism referred to as ‘cross-priming’. Using a mixed culture model in vitro, tetramer analysis (using a molecular reagent that detects human leucocyte antigen-specific, EGFR peptide specific CD8+ T cells) demonstrated that VTX-2337 stimulates cross-priming and increases the number of EGFR-specific CD8+ T cells following cetuximab treatment.
Taken together, the ability of VTX-2337 to stimulate the production of inflammatory cytokines (including IL-1, IL-18, TNFα, IL-12, and IFNg), the activation and stimulation of NK cells and ADCC, and the activation of the antigen processing and presentation of mDC and monocytes provide a strong rationale that this TLR8 agonist may enhance the activity of cetuximab in clinical studies.
2.2.3 Toxicology
In conjunction with FDA requirements, standard toxicology studies were performed with the aim of inducing and identifying drug-related toxicities. The clinically relevant toxicities observed in these studies were mechanistically based; that is, attributed to activation of the innate immune system via TLR8. The most frequent of these included transient constitutional symptoms consistent with the influenza-like response frequently seen with immunomodulatory agents. As noted in §2.3, these flu-like symptoms identified in preclinical toxicology studies have
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 13 Confidential Information 03-Jun-2014
subsequently been observed in clinical trials of VTX-2337, and include pyrexia, chills, myalgia, and fatigue.
As detailed in the VTX-2337 IB, organ-based toxicity was also observed in preclinical toxicology studies. Organ-based toxicities have not been observed in any clinical trial of VTX-2337 to date, and are not described herein.
2.3 Clinical Data 2.3.1 Phase I Solid Tumor: VTX-2337 Monotherapy (VRXP-A101)
VTX-2337 was first evaluated clinically as a stand-alone agent in a Phase I standard dose-escalation study to assess the safety, tolerability and biological activity of the compound in late-stage cancer patients. At doses ranging from 0.1–3.9 mg/m2, VTX-2337 was well tolerated overall, with the predominant adverse events being transient grade 1 or 2 fever, chills, flu-like symptoms, nausea and vomiting, anorexia, and injection site reaction. No significant drug-related hematologic, gastrointestinal, neurologic or cardiac toxicities were observed. At the highest dose evaluated, 3.9 mg/m2 (cohort 8; n=8) a single subject experienced a dose-limiting toxicity (DLT) of grade 3 hypotension associated with grade 2 cytokine release syndrome (CRS), from which the subject recovered completely. Accordingly, the maximum dose evaluated in this study (3.9 mg/m2) was adequately well tolerated. Overall, VTX-2337 was found to be well tolerated when administered subcutaneously weekly for 3 weeks of a 4-week cycle.
The PK of VTX-2337 were assessed in all subjects (n=33) and demonstrated dose-dependent exposure. With subcutaneous administration, VTX-2337 was rapidly absorbed into systemic circulation as well as rapidly cleared, with mean Tmax ranging from 0.5–0.7 hours and t½ ranging from 1.7–7.1 hours. Peak plasma levels and total systemic exposure were generally dose-proportional.
The biological activity (cytokines, chemokines and other inflammatory markers, including those indicative of TLR8 activation) of VTX-2337 was assessed in all subjects. Biological activity of VTX-2337 was shown to be dose dependent, with the robust induction of multiple inflammatory markers in all subjects receiving doses ≥ 2.0 mg/m2.
Clinical responses were assessed by response evaluation criteria in solid tumors (RECIST) at 8 weeks. No complete responses (CR) or partial responses (PR) were seen in the study, but approximately 25% of subjects had evidence of stable disease (SD) at 8 weeks. It should be noted that VTX-2337 is anticipated to have stand-alone biological activity, but is not anticipated to induce a CR or PR as a single agent.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 14 Confidential Information 03-Jun-2014
The doses selected from this study to be used in combination studies were 2.5, 3.0, and 3.5 mg/m2. All of these doses are expected to be biologically active based on the biomarker data from VRXP-A101.[19]
2.3.2 Phase 1 SCCHN: VTX-2337 with Cetuximab (VRXP-A103)
This ongoing, single-center phase 1b protocol at Seattle Cancer Care Alliance (Seattle, WA) is being conducted as an Investigator Sponsored Trial, with Laura Chow, MD as the Sponsor-Investigator.
VRXP-A103 assesses the safety and tolerability of VTX-2337 in combination with cetuximab. Cetuximab is administered weekly and VTX-2337 is administered weekly for three weeks of a four-week cycle. Three dose levels of VTX-2337 are being evaluated in a standard dose-escalation schema: 2.5 mg/m2, 3.0 mg/m2, and 3.5 mg/m2.
Enrollment is complete (n=13), and one subject remains on study. The study regimen has been safe and adequately tolerated. There have been no dose-limiting toxicities; no serious, unexpected drug-related adverse events; and no evidence of synergistic toxicities between cetuximab and VTX-2337. Clinical tolerability data indicate that long-term dosing at 3.0 mg/m2 will be better tolerated than 3.5 mg/m2.
Translational medicine results are available from the first twelve subjects who received VTX-2337 (2.5, 3.0, or 3.5 mg/m2) in combination with cetuximab. As expected based on data from the Phase 1 VRXP-A101 study, serum biomarkers consistent with TLR8 activation were readily measured at both dose levels. In addition, ex vivo analysis of NK cells collected pre-dose and 24 hours after dosing demonstrate NK cell activation. Given the proposed mechanism of VTX-2337 enhancing ADCC with cetuximab in an NK-dependent manner, these data provide important correlative information and suggest the doses of 2.5, 3.0, and 3.5 mg/m2 are biologically active from a pharmacologic perspective.
Based on preliminary efficacy data, 10 of the 13 subjects have been eligible for evaluation of tumor response: 2 subjects achieved a partial response, 4 subjects experienced disease stabilization, and 4 subjects had disease progression. One subject has not yet had a response assessment, and 2 subjects discontinued the study prematurely and were unevaluable for response assessment.[20]
2.3.3 Phase 1 Ovarian Cancer (VTX-2337 with Chemotherapy)
Study VRXP-A102 (GOG-9925) was a phase I study conducted in collaboration with Gynecologic Oncology Group (GOG). The study separately assessed two treatment regimens containing VTX-2337 in women with recurrent ovarian cancer. Regimen 1 evaluated pegylated
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 15 Confidential Information 03-Jun-2014
liposomal doxorubicin (PLD, Doxil®; 40 mg/m2) plus VTX-2337 at three dose levels: 2.5 mg/m2, 3.0 mg/m2, and 3.5 mg/m2. Regimen 2 consisted of weekly paclitaxel (80 mg/m2) plus VTX-2337 (3.0 mg/m2).
In both of the regimens evaluated, there were no dose-limiting toxicities; no serious, unexpected drug-related adverse events; and no evidence of synergistic toxicities between PLD plus VTX-2337 or paclitaxel plus VTX-2337. PD data confirm the biological activity of VTX-2337 in both regimens at all dose levels, with biomarker responses indicative of TLR8 stimulation and immune activation.
Twenty subjects were treated: 13 on Regimen 1 and 7 on Regimen 2. On Regimen 1, one subject enrolled based on biochemical evidence of recurrent disease achieved a complete biochemical response, 1 subject with non-measureable disease achieved a complete response, 7 subjects had stable disease, and 3 subjects had progressive disease (including 1 subject with non-target disease [biochemical recurrence only] who had biochemical progression). One subject did not complete the first cycle and was not evaluable for efficacy. On Regimen 2, one subject experienced a partial response, 2 subjects experienced disease stabilization, and 4 of the 7 subjects had disease progression.
Two of the 7 subjects enrolled in Regimen 1 at the 3.5 mg/m2 dose level of VTX-2337 withdrew from treatment or had a dose reduction due to grade 2 or 3 drug-related events (e.g., chills, fatigue, nausea, vomiting, fever). These events suggest that long-term dosing of VTX 2337 at 3.5 mg/m2 is not clinically optimal. Based on this information, and the adequate biological activity of VTX-2337 at 2.5 and 3.0 mg/m2, the selection of 3.0 mg/m2 of VTX-2337 was recommended as the optimal dose for the randomized, Phase 2 study.[21]
2.3.4 Phase 2 Ovarian Cancer (VTX-2337 with Chemotherapy)
GOG-3003 is a randomized, placebo-controlled, ongoing Phase 2 study designed to evaluate VTX-2337 (3.0 mg/m2) in combination with PLD in patients with recurrent or persistent epithelial ovarian, fallopian tube, or primary peritoneal cancer. The study will evaluate the overall survival of VTX-2337 in combination with PLD compared to PLD alone in approximately 290 subjects. PFS, response rate, and safety of the combination are key secondary endpoints. This multicenter study is being conducted in approximately 100 clinical sites in the United States, in collaboration with the GOG. Enrollment in this study is complete.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 16 Confidential Information 03-Jun-2014
2.4 Risks/Benefits 2.4.1 Potential Risks
In previously published trials of platinum, 5-FU, and cetuximab the most common adverse events (AE) overall were skin reactions, headache, diarrhea, infection, and nausea. The most common grade 3 or 4 adverse events were anemia, neutropenia, and thrombocytopenia. Less commonly, dosing with cetuximab may result in a serious infusion reaction requiring medical intervention and immediate, permanent discontinuation with cetuximab.[12]
The most common AE associated with VTX-2337 when administered as a single-agent is injection site reaction. Most often these have been grade 1 or 2; however, grade 3 injection site reactions have been reported. The most common systemic drug-related adverse events are transient grade 1 or 2 chills, flu-like symptoms, fever, nausea, and vomiting; these transient symptoms typically last < 48 hours. Less commonly, dosing with VTX-2337 may result in CRS, which is most likely to be grade 1 or 2, but grade 3 reactions have been reported. Similarly, the most common AEs reported in patients receiving VTX-2337 in combination with cetuximab were grade 1 and 2 injection site reactions, flu-like symptoms, nausea, fatigue, vomiting, cough, malaise, and dyspnea.
Potential long-term clinical effects of VTX-2337 are unknown and cannot be reliably predicted. However, several subjects in clinical trials have received up to 8 cycles (24 individual weekly doses) of VTX-2337 without unanticipated problems. Investigators will be informed of any newly-identified risks associated with VTX-2337, if they occur.
Although the combinations of VTX-2337 plus chemotherapy (PLD, paclitaxel) and VTX-2337 plus cetuximab did not demonstrate any dose-limiting or synergistic toxicities, VTX-2337 has not previously been studied in combination with platinum plus 5-FU plus cetuximab. While no new, unexpected, or synergistic toxicities are anticipated, the safety of this combination will be carefully evaluated by an independent data safety monitoring board (DSMB) (see also §9.2.2).
Overall, at the dose level to be administered in this clinical trial (3.0 mg/m2), VTX-2337 treatment-related toxicities are expected to be transient and consistent with those events commonly associated with an activated immune response. This includes symptoms of chills, fever, flu-like syndrome, headache, nausea, vomiting, and local injection site reaction.
2.4.2 Potential Benefits
The efficacy of VTX-2337 has not been formally evaluated in clinical trials to date. However, exploratory data from study VRXP-A101 showed 25% of the 33 subjects enrolled had disease stabilization at 8 weeks. In addition, preliminary data from a phase 1b study of VTX-2337 in
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 17 Confidential Information 03-Jun-2014
combination with cetuximab in patients with advanced SCCHN (n=13) included 2 subjects who experienced a partial response, 4 subjects who experienced disease stabilization; 2 subjects were not evaluable and 1 subject has not yet had a tumor evaluation. Furthermore, a phase 1b study of VTX-2337 with chemotherapy in women with recurrent, platinum-resistant ovarian cancer (n=20) included 2 subjects who experienced complete response (one of which was a biochemical CR), 1 subject who experienced a partial response, and 10 subjects who experienced disease stabilization (2–8 months).
The current study of VTX-2337 described herein is a multi-dose study to assess the safety, tolerability and efficacy of the investigational drug in combination with cisplatin or carboplatin, 5-FU, and cetuximab. The clinical efficacy of this combination has not yet been evaluated; however, the addition of VTX-2337 to the standard-of-care (SOC) treatment regimen may be more effective than SOC alone.
Participating subjects may also benefit from the personal satisfaction of participating in an investigative process that will contribute information regarding the investigational product (IP) that may help patients afflicted with SCCHN.
2.5 Dose Rationale
The selection of the starting dose for this study, as well as the Phase 2 study in ovarian cancer (3.0 mg/m2) was based on data from the initial phase 1 study of VTX-2337 used as a single agent, and data from the two Phase 1b studies combining VTX-2337 with cetuximab in SCCHN patients and with PLD or paclitaxel in ovarian cancer patients, respectively. These studies showed that VTX-2337 is biologically active in some subjects at doses as low as 0.4 mg/m2 based on biomarker data as previously described. Biological activity of VTX-2337 was shown to be dose dependent. At VTX-2337 doses ≥ 2.0 mg/m2, nearly all subjects evaluated have a robust biological response, as indicated by the induction of multiple inflammatory markers consistent with activation of TLR8. In study VRXP-A103, where cellular responses were assessed, VTX-2337 in combination with cetuximab at doses ≥ 2.5 mg/m2 (the lowest dose tested) was associated with cellular responses including NK cell activation.
While no DLTs have been observed at 3.5 mg/m2 in either the cetuximab or chemotherapy combination studies, treating investigators have reported reduced tolerability at 3.5 mg/m2 compared to 3.0 mg/m2. This has included higher fevers, more intense flu-like symptoms, and more persistent injection site reactions. Based on its clear biological activity and improved long-term tolerability, as well as the lack of dose-limiting or synergistic toxicities, 3.0 mg/m2 has been selected as the appropriate dose for Phase 2 studies of VTX-2337 in combination with chemotherapy.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 18 Confidential Information 03-Jun-2014
2.6 Population
This study will be conducted in adult subjects with recurrent or metastatic SCCHN who have not previously received systemic treatment for their recurrent or metastatic disease. Eligible subjects will have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 and adequate hematologic, renal, and hepatic function. This study will not include subjects with disease which is amenable to curative local therapy or who had disease recurrence within 6 months of completion of systemic therapy for localized SCCHN.
Refer to §5.0 for specific eligibility requirements for subjects.
3.0 TRIAL RATIONALE AND OBJECTIVES 3.1 Rationale
Recurrent or metastatic SCCHN is an aggressive disease with few treatment options with proven clinical benefit. The use of the EGFR-specific monoclonal antibody cetuximab in combination with platinum and 5-FU based chemotherapy has demonstrated clinical benefit in these patients. Still, the response rate (30-40%), delay in disease progression (overall PFS of approximately 6 months) and OS (approximately 11-12 months in this treated population) leave room for considerable improvement. Ideally, an agent could be added to this regimen that would provide additive or synergistic clinical benefit without dramatically increasing the toxicity of this drug combination. In this regard, an immunomodulatory agent that increases the activity of cetuximab and/or the chemotherapy backbone would be potentially beneficial.
VTX-2337 is a small molecule agonist of TLR8 that stimulates specific immune cell populations including mDC, monocytes, and NK cells. In a variety of cell culture based and animal studies, VTX-2337 has been shown to enhance ADCC in the context of a variety of IgG1-isotype monoclonal antibodies including cetuximab. The enhancement of ADCC occurs across all FcRg3a genotypes—including those associated with lower affinity to FcR and associated lower clinical responses in patients. Via the stimulation of various antigen presenting cells, VTX-2337 enhances the generation of tumor-antigen specific CD8+ T cells and has been found to enhance the tumoricidal activity of certain chemotherapy regimens. In addition, VTX-2337 stimulates the production of a variety of inflammatory cytokines and chemokines that would be expected to modulate the tumor microenvironment. These functions of VTX-2337 are consistent with the role of its receptor—TLR8—as a sentinel of viral infection and the expression of a ‘danger’ signal to rid the host of an unwanted intruder.
VTX-2337 has been evaluated as a single-agent in cancer patients (n=33) to determine the biological activity and safety profile of this novel compound. VTX-2337 has also been evaluated in several combination studies with cetuximab (n=13), PLD (n=13), and paclitaxel (n=7) to
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 19 Confidential Information 03-Jun-2014
address the safety and activity of this agent in combination with SOC anticancer regimens. Collectively, these data provide a rationale for continued study of VTX-2337 at the selected dose in larger, randomized clinical trials to determine if this compound provides clinical benefit.
As of yet, the anti-tumor effects of VTX-2337 in combination with platinum-based therapy with 5-FU and cetuximab have not been evaluated. However, as VTX-2337 may enhance therapeutic responses to platinum-5-FU chemotherapy with cetuximab; this combination is a promising combination that should be explored for its potential for improved anti-tumor effects in this patient population.
3.2 Objectives
The purpose of this study is to compare the safety and efficacy of SOC in combination with VTX-2337 to those treated with SOC plus placebo in subjects with recurrent or metastatic SCCHN. Efficacy objectives include comparing the PFS, OS, objective response rate (ORR), duration of best response (DOBR), disease control rate (DCR), and duration of disease control (DDC) of the two treatment groups. The PD of VTX-2337 will also be evaluated.
4.0 TRIAL DESIGN 4.1 Study Design/Type
This is a randomized, double-blind, placebo-controlled, parallel-group study. The study consists of screening (≤ 14 days1), initial treatment (cycles 1–6), subsequent treatment (cycles 7+), and long-term follow-up. Following the screening period, qualified subjects will be randomized in a 1:1 ratio to receive SOC plus placebo or SOC plus VTX-2337. Randomization of all subjects will be stratified by receipt of prior systemic therapy of SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy as assigned by the investigator at the time of randomization (cisplatin or carboplatin).
Subjects will then be administered cisplatin or carboplatin—as assigned by the investigator prior to randomization—5-FU, cetuximab, and IP (i.e., VTX-2337 or placebo) on pre-specified days of a 21-day cycle for 6 cycles (§6.0). Thereafter, subjects will continue on study for cycles 7+ for dosing of weekly cetuximab and biweekly IP in 28-day cycles.
Subjects will be evaluated for PFS according to immune-related Response Evaluation Criteria In Solid Tumors (irRECIST; §6.6.1.2) at Week 12 (± 3 days), Week 18 (± 3 days), and every 8 weeks (± 7 days) thereafter. Treatment will be discontinued for subjects with independently-confirmed radiographic disease progression. Upon discontinuation of treatment, subjects will complete the End of Treatment visit and will be followed for survival. 1 Baseline imaging may be performed within 28 days of randomization.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 20 Confidential Information 03-Jun-2014
Figure 1: Study Schema
4.2 Endpoints 4.2.1 Primary Endpoint(s)
The primary endpoint of the study is to compare the PFS of patients with recurrent or metastatic SCCHN treated with VTX-2337 plus SOC versus patients treated with SOC alone using irRECIST evaluated by independent radiology review.
4.2.2 Secondary Endpoint(s)
The secondary endpoints of the study are to compare the following between the two treatment groups:
• Safety as measured by adverse events, including clinically significant changes in physical examination, peripheral blood hematology, serum chemistry, urinalysis, and ECG.
• The OS of patients with recurrent or metastatic SCCHN.
• The ORR, DOBR, DCR, and DDC of patients with recurrent or metastatic SCCHN using irRECIST evaluated by independent radiology review.
4.2.3 Exploratory Endpoint(s)
The exploratory endpoints of this study are as follows:
• To compare genetic polymorphisms that may impact the response of patients to a TLR8 agonist or to cetuximab between the two treatment groups.
• To compare immune biomarker response as measured by a multiplexed panel of cytokines, chemokines, and inflammatory markers between the two treatment groups.
Subsequent Treatment Cycles 7+
Initial Treatment 6 Cycles (18 Weeks)
Screening< 14 Days
Screening
SOC + VTX-2337
SOC + Placebo
Rand
omiza
tion
Cetuximab + Placebo
Cetuximab + VTX-2337
Follow Up
Dise
ase
Prog
ress
ion
Survival Follow-Up
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 21 Confidential Information 03-Jun-2014
• To compare the effect of immune cell subsets within the tumor on response to treatment and/or clinical outcome, as measured by immunohistochemistry in primary tumor tissue between the two treatment groups.
• To assess the PK of VTX-2337.
4.3 Procedures to Minimize Bias
The study design and methods were selected to minimize bias. This is a randomized, double-blind, placebo-controlled study.
All subjects will receive SOC treatment; in addition, subjects will be randomly assigned in a 1:1 ratio to one of two treatment arms: SOC + VTX-2337 or SOC + placebo. To ensure that both known and unknown confounding factors are evenly distributed between treatment groups randomization of all subjects will be stratified by prior systemic therapy for SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy, as assigned by the investigator at the time of randomization (cisplatin or carboplatin). Neither the investigators nor the subjects know to which treatment group a subject is assigned.
The labeling, packaging, and distribution of VTX-2337 and placebo will be identical so that the clinical site personnel remain blinded to study treatment. Placebo will be utilized to ensure that subjects, investigators, and all other study personnel will remain blinded to the study treatment.
In order to minimize potential bias and variability from individual radiology reviewers, radiologic assessment of tumor response will be performed via central radiology review. The central reviewers are blinded to study treatment and are independent from the clinical sites.
4.4 Maintenance of Blinding Procedures
All clinical, regulatory, and safety personnel at the contract research organization (CRO) and sponsor, as well as all investigators and clinical site staff, will remain blinded to the study treatment assignment. Members of the data safety monitoring board (DSMB) may be unblinded; an unblinded statistician, independent from the project team, will provide support to the DSMB. Additionally, individuals with access to the randomization schema and IP kit assignments will remain separate from the study personnel responsible for day-to-day operations and evaluation of the clinical data. Refer to §7.5 for emergency unblinding procedures.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 22 Confidential Information 03-Jun-2014
4.5 Trial Treatment
Subjects randomized in the study will be administered all of the following:
• IP (i.e., VTX-2337 or placebo)
• Cetuximab
• Cisplatin or carboplatin (as assigned by the investigator)
Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent should be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject.
• Fluorouracil (5-FU)
When cetuximab is administered on the same day as chemotherapy, cetuximab administration will be completed ≥ 1 hour prior to administration of platinum and 5-FU. When cetuximab is administered on the same day as IP, the dose of IP will be given prior to cetuximab.
Please refer to §7.0 for additional information regarding subject treatment procedures.
4.5.1 Investigational Product Treatment
Subjects will receive IP at a dose of 3.0 mg/m2 (see also §9.2.2) given as a subcutaneous injection on Days 8 and 15 of a 21-day cycle for up to 6 cycles. Following the 6th cycle, subjects will continue to receive IP on Days 8 and 22 of a 28-day cycle until disease progression. (§7.3.1)
4.5.2 Cetuximab Treatment
On Cycle 1 Day 1, subjects will receive an initial cetuximab dose of 400 mg/m2 given as a 2-hour intravenous (IV) infusion1. This will be followed by weekly cetuximab doses of 250 mg/m2 given as a 1-hour IV infusion1. Weekly treatment with cetuximab will continue until disease progression. (§7.3.2)
Please refer to the cetuximab label for additional information.
4.5.3 Platinum Treatment
The platinum therapy (cisplatin or carboplatin) is assigned to each subject at the discretion of the investigator. Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent must be determined prior to randomization. Unless clinically necessary, the
1 The duration of infusion may be adjusted according to institutional standards.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 23 Confidential Information 03-Jun-2014
investigator should not change the platinum chemotherapy for each subject. Reasonable efforts should be made to keep the subject on the platinum therapy originally assigned; however, the platinum therapy may be changed if clinically necessary. (§7.3.3)
Cisplatin Treatment
Subjects will receive 100 mg/m2 of cisplatin as a 1-hour IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles1. Cisplatin administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the cisplatin label for additional information.
Carboplatin Treatment
Subjects will receive carboplatin at an AUC of 5 mg/mL/min as a 1-hour IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles1. The carboplatin dose will be based upon the subject’s Creatinine Clearance (CrCl) in mL/min as estimated by the Cockroft-Gault Formula. The Calvert formula will be used for carboplatin dosing:
Total Dose (mg) = (target AUC) x (CrCl + 25)
Carboplatin administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the carboplatin label for additional information.
4.5.4 5-FU Treatment
Subjects will receive a continuous IV infusion of 5-FU at a dose of 1000 mg/m2/day on Days 1–4 of a 21-day cycle for a maximum of 6 cycles. 5-FU administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the 5-FU label for additional information.
4.6 Duration
The enrollment period of the study is expected to be approximately 18 months, followed by a ~12-month follow up period.
The duration of participation will vary among individual subjects due to factors such as disease progression and time of enrollment. After providing written informed consent, subjects will be screened for eligibility within 14 days of randomization (28 days for imaging) according to the procedures outlined in §6.1. Eligible subjects will be randomized into the study and will receive treatment as described in §6.2 and §7.0. Subjects will receive therapy until independently- 1 The duration of infusion may be adjusted according to institutional standards.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 24 Confidential Information 03-Jun-2014
confirmed disease progression per irRECIST. Thereafter, subjects will be followed long-term for survival.
4.7 Discontinuation
Enrollment in the study will end when approximately 175 subjects have been randomized and have received at least one dose of IP. The sponsor may terminate enrollment in the study at any time for any reason.
Whenever possible, enrolled subjects should complete the study per protocol. However, individual subjects may withdraw from the study prematurely at any time, (e.g., subject decides to discontinue participation due to an adverse event, whether or not related to IP). Subjects who are noncompliant with the study’s requirements may also be removed from the study at any time by the investigator or study sponsor. Regardless of reason for discontinuing the study prematurely, the End of Treatment evaluations should be completed and the subject should be followed for survival, whenever feasible.
Please refer to §6.5 for early discontinuation of individual subjects.
5.0 SELECTION OF SUBJECTS
This study will enroll adult male and female subjects with recurrent or metastatic SCCHN who have not previously received systemic treatment for their recurrent or metastatic SCCHN. All patients considered for enrollment and the reason(s) any screened subject is determined to be ineligible, must be documented. Written informed consent with an IRB/IEC-approved Informed Consent Form (ICF) must be obtained from all subjects prior to undergoing any study-specific procedures, including the discontinuation of any medication(s).
Subjects must meet all of the following eligibility criteria at the time of randomization.
5.1 Inclusion Criteria
1) Ability and willingness to provide written informed consent and to comply with the study’s visit and assessment schedule
2) Prior documentation of histologically or cytologically confirmed squamous cell carcinoma of the head and neck
Patients with squamous cell carcinoma of an unknown primary are eligible provided they previously received treatment for their locoregional head and neck cancer
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 25 Confidential Information 03-Jun-2014
3) Locoregionally recurrent or metastatic SCCHN that has not previously been treated with systemic therapy for recurrent or metastatic disease
4) At least one measurable lesion as defined by RECIST v1.1 (§11.1) on screening computed tomography (CT) or magnetic resonance imaging (MRI)
5) 18 years of age or older
6) ECOG performance status of 0 or 1
7) Acceptable bone marrow, renal, and hepatic function based upon screening lab tests as demonstrated by the following:
− White blood cell (WBC) count > 2,500 cells/Μl
− Absolute neutrophil count (ANC) > 1,500 cells/μL
− Platelet count ≥ 100,000 cells/μL
− Hemoglobin ≥ 9 g/dL
− Creatinine ≤ ULN OR Creatinine Clearance ≥ 60 mL/min
− Total bilirubin ≤ 2.0 x ULN
− SGOT (AST), SGPT (ALT) ≤ 2.5 x ULN or
≤ 5 x ULN in presence of liver metastases
− Potassium ≥ LLN
8) Willingness to use medically acceptable contraception throughout the study period and for 4 weeks after the final administration of IP
9) For female subjects with reproductive potential: a negative serum pregnancy test
5.2 Exclusion Criteria
1) Disease which is amenable to curative local therapy
2) Nasopharyngeal, salivary gland, lip, or sinonasal carcinoma
3) Major surgery or irradiation within 4 weeks of randomization
4) Prior systemic anti-cancer therapy, unless administered for localized SCCHN and completed at least 6 months prior to disease recurrence
5) Treatment with an investigational agent within 30 days of randomization
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 26 Confidential Information 03-Jun-2014
6) Treatment with oral or parenteral corticosteroids within 2 weeks of randomization or a requirement for chronic systemic immunosuppressive therapy for any reason
7) Prior serious infusion reaction to cetuximab
8) Treatment with an immunotherapy within 30 days of randomization
9) Known brain metastases, unless stable for at least 28 days prior to randomization
10) Active autoimmune disease, defined as any autoimmune condition currently requiring therapy (e.g., systemic lupus erythematosus, multiple sclerosis, inflammatory bowel disease, rheumatoid arthritis)
11) Known infection with HIV
12) Clinically significant cardiac disease (e.g., congestive heart failure, unstable or uncontrolled angina, myocardial infarction) within 6 months of randomization
13) Pregnant or breast-feeding females
14) History of another primary malignancy, with the exception of the following:
− curatively resected non-melanoma skin cancer
− curatively treated in situ cervical cancer
− other malignancy curatively treated with no evidence of disease and no anticancer therapy administered for at least 3 years prior to randomization, with the exception of adjuvant hormonal therapy for breast cancer
15) Any other condition or circumstance that could interfere with adherence to the study’s procedures or requirements, or otherwise compromise the study’s objectives
6.0 CLINICAL TRIAL PROCESSES AND PROCEDURES
The schedules of study visits, procedures and assessments are in Table 1.
Subjects will receive study treatment, as described in §7.0. Please refer to §6.5 for requirements for individual subjects who discontinue study treatment prematurely. Unscheduled evaluations may be done at the discretion of the investigator as needed to assess the subject’s clinical status. All scheduled visits and procedures must be conducted at the study site of the Principal Investigator as indicated on the FDA Form 1572.
The imaging technique used for each subject (CT or MRI) is at the discretion of the investigator, but the same technique must be used for each individual subject throughout the study. Imaging should not be delayed in case of missed doses or dose delays.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 27 Confidential Information 03-Jun-2014
All study-required laboratory evaluations must be performed by the central laboratories using the provided kits.
6.1 Subject Screening and Randomization (Day -14 to -1) 6.1.1 Screening Procedures
Subjects with recurrent or metastatic SCCHN may be screened for this study. Prior to the initiation of screening procedures, informed consent will be obtained from each subject as described in §10.2.1.
Upon completion of the informed consent process, sites will register the subject in the interactive voice/web response system (IXRS); IXRS will assign a unique screening number to each subject. The screening number will be comprised of the three-digit site number followed by a three-digit, sequential number (e.g., 123901, 123902). Upon randomization, a unique randomization number will be assigned by IXRS; the randomization number will be used as the subject number for the duration of the study.
The following procedures are required for screening and may be done at any time in the 14 days prior to randomization, unless otherwise specified:
• Complete medical history, including
— Concomitant medications and history of prior anticancer interventions
— Histological or cytological confirmation of SCCHN1
— Tumor staging according to the TNM Classification of Malignant Tumors
— HPV status for patients with oropharyngeal carcinoma only
— If HPV status is not available in the subject’s medical history, testing for HPV status by p16 immunohistochemistry, in situ hybridization, or polymerase chain reaction should be conducted at the time of screening (knowledge of HPV status is not necessary prior to randomization)
• Complete physical exam (PE), including vital signs (temperature, T; blood pressure, BP; respiration rate, RR; heart rate, HR), assessment of ECOG performance status (§11.1), weight and height
• Obtain 12-lead electrocardiogram (ECG)
• Collect blood samples for the following analyses:
1 For patients with unknown primary who have previously received treatment for locoregional head and neck cancer, histological or cytological confirmation of squamous cell carcinoma is acceptable.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 28 Confidential Information 03-Jun-2014
— Complete blood count (CBC)
— Serum chemistry
— Serum pregnancy test (females with reproductive potential1 only)
— Pharmacogenetics
• Collect urine for urinalysis
• CT or MRI of the neck, chest, upper abdomen, and other anatomic region(s) of disease according to the requirements delineated in the VRXP-A202 Imaging Manual within 28 days of randomization
• Submit a tissue sample from the primary or metastatic tumor for all randomized subjects. When possible, re-biopsy at screening of primary tumor or metastatic tissue is preferred; however, archive tumor tissue may be used in absence of re-biopsy. If a tumor tissue sample is not available, sites should notify the sponsor or its representative prior to study entry.
A representative paraffin-embedded block of tissue from the original (diagnostic) biopsy and/or repeat biopsies will be submitted. If blocks cannot be submitted, 20 unstained slides plus one H&E stained 5-micron sections mounted on positively-charged glass slides are acceptable.
6.1.2 Randomization (Enrollment) Procedures
Subjects who have completed all screening assessments and are deemed eligible may be randomized (enrolled) up to 1 business day prior to Cycle 1 Day 1. Randomization of all subjects will be stratified by the receipt of prior systemic therapy for SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy, as assigned by the investigator at the time of randomization (cisplatin or carboplatin).
Upon randomization, sites will be provided the subject’s randomization number and medication ID number. Randomization will also prompt an order for IP to be placed. A subject specific kit of IP will arrive approximately 3–4 business days after randomization.
6.2 Treatment Period
The treatment period is split into two phases: initial treatment (Cycles 1–6) and subsequent treatment (Cycles 7+).
Cycles 1–6 consist of 21-day cycles where subjects receive the following per cycle:
1 Females who are premenopausal or ≤ 2 years postmenopausal and not surgically sterile
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 29 Confidential Information 03-Jun-2014
• A single dose of cisplatin or carboplatin (Day 1)
• A continuous infusion of 5-FU (Days 1–4)
• Three doses of cetuximab (Days 1, 8 and 15)
• Two doses of IP (Days 8 and 15)
Cycles 7+ consist of 28-day cycles where subjects receive the following per cycle:
• Four weekly doses of cetuximab (Days 1, 8, 15, and 22)
• Two doses of IP (Days 8 and 22)
Treatment continues until the subject has PD. Upon independent confirmation of radiographic disease progression and completion of treatment, subjects will complete the End of Treatment visit (§6.3) and begin long-term follow-up.
6.2.1 Initial Treatment (Cycles 1–6)
Study Cycles 1–6, Day 1 (CXD1) (±2 days)
• Within 72 hours prior to treatment, collect blood samples for the following analyses:
— CBC
— Serum chemistry
• Problem-oriented PE, including vital signs (T, BP, RR, HR), ECOG performance status assessment and weight
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
— Cisplatin or carboplatin
— 5-FU
• Assess adverse events and and update concomitant medications
Study Cycles 1–6, Days 2–4 (CXD2-4) (±0 days)
• Continue 5-FU infusion according to the procedures in §7.3
Study Cycles 1–6, Day 8 (CXD8) (±1 day)
• Administer the following study medications according to the procedures in §7.3
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 30 Confidential Information 03-Jun-2014
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
On Cycle 1 Day 8 and Cycle 3 Day 8 only the assessments noted below will be completed. PK samples will only be collected on C1D8, not C3D8. Cetuximab administration will begin AFTER the 1 hour post-dose ECG and blood collection are completed. If Day 8 of Cycle 1 or 3 is skipped for any reason, the following assessments should be completed the next day the subject receives IP:
• Pre-dose
— Collect blood sample for PK assessment (C1D8 only)
— Collect blood sample for immune biomarker assessment
• 45 minutes post IP dose (±15 min)
— Collect blood samples for PK assessment (C1D8 only)
• 1 hour post IP dose (±15 min)
— Obtain 12-lead ECG
• 8 hours post IP dose (±15 min)
— Collect blood sample for PK assessment (C1D8 only)
— Collect blood sample for immune biomarker assessment
Study Cycles 1–6, Day 15 (CXD15) (±1 day)
• Pre-dose
— Collect blood sample for CBC
• Collect vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 31 Confidential Information 03-Jun-2014
Study Cycles 1–6, Week 12 (± 3 days) and Week 18 (± 3 days)
• Perform CT / MRI of neck, chest, upper abdomen, and other anatomical region(s) of disease using the same technique as baseline and in accordance with the Imaging Manual
Imaging should not be delayed in case of missed doses or dose delays.
6.2.2 Subsequent Treatment (Cycles 7+)
Study Cycles 7+, Day 1 (CXD1) (±2 days)
• Within 72 hours prior to treatment, collect blood samples for the following analyses:
— CBC
— Serum chemistry
• Problem-oriented PE, including vital signs (T, BP, RR, HR), ECOG performance status assessment, and weight
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 8 (CXD8) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 15 (CXD15) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 22 (CXD22) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— IP
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 32 Confidential Information 03-Jun-2014
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Every 8 Weeks (± 7 days)
• Perform CT / MRI of neck, chest, upper abdomen, and other anatomical region(s) of disease using the same technique as baseline and in accordance with the Imaging Manual
Imaging should not be delayed in case of missed doses or dose delays.
6.3 End of Treatment
Subjects will receive therapy until independently-confirmed disease progression per irRECIST. In the absence of significant clinical deterioration requiring intervention, disease progression identified at or before Week 12 should be confirmed with a repeat scan ≥ 4 weeks later and the subject should continue treatment until independent confirmation of PD based on the confirmation scan.
The End of Treatment visit will be completed within 14 days of independent confirmation of radiologic PD as assessed by irRECIST (§11.3) and prior to initiation of other anti-cancer therapy.
• Complete PE, including vital signs (T, BP, RR, HR), ECOG performance status assessment and weight if not completed within the previous 14 days
• Collect blood samples for the following analyses if not completed within the previous 14 days:
— CBC
— Serum chemistry
• Collect urine for urinalysis if not completed within the previous 14 days
• 12-lead ECG
• Assess adverse events and update concomitant medications
• Perform CT/MRI for subjects who have not had an imaging study within the previous 4 weeks
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 33 Confidential Information 03-Jun-2014
6.4 Follow Up Period
Following the End of Treatment visit, subjects will be followed for survival. During the follow-up period, subjects will be contacted every 8 weeks to assess vital status and disease state, including the initiation of any new anticancer interventions.
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 34 Confidential Information 03-Jun-2014
Table 1: Schedule of Procedures and Assessments
Screen Cycles 1–6 Cycles 7+
EOT
FU
Study Week: -2 to -1 1–18 19+ Q8 weeks Day: -14 to -1 1 2 3 4 8 15 1 8 15 22
Informed Consent1 X
Medical History & Eligibility2 X
VTX-2337 or Placebo (IP) X X X X
Cetuximab3 X X X X X X X
Cisplatin or Carboplatin X
Fluorouracil (5-FU) X X X X
Physical Examination X X X X
Vital Signs X X X X X
12-Lead ECG4 X X X
CBC with differential5 X X X X X
Serum Chemistry5 X X X X
Biomarkers6 2X
PK7 3X
Urinalysis X X
Pharmacogenetics X
Serum Pregnancy8 X
Submit Tumor Tissue X
AE/CRx9 X X X X X X X X
Assess Vital Status X
Tumor Assessments
Screen Week 12 ± 3 Days
Week 18 ± 3 Days
Week 26 ± 7 Days
Every 8 Weeks ± Days
EOT FU
CT or MRI10 X X X X X X
1 Informed consent may be obtained any time prior to study related procedures (i.e., is not required to be within 14 days of randomization)
2 HPV status for patients with oropharyngeal carcinoma only 3 Cycle 1 Day 1 dose = 400 mg/m2; subsequent doses are 250 mg/m2 4 Cycle 1 Day 8 and Cycle 3 Day 8: perform 1 hour (±15 minutes) post-dose of IP 5 Obtain within 72 hours of each Day 1 dose 6 Cycle 1 Day 8 and Cycle 3 Day 8 only: perform pre-dose and 8 hours (±15 minutes) post-dose of IP 7 Cycle 1 Day 8 only: perform pre-dose, and 45 minutes and 8 hours (±15 minutes) post-dose of IP 8 Serum pregnancy to be collected on all females with reproductive potential 9 AEs will be collected from Cycle 1 Day 1 until 7 days after the last dose of any study medication or EOT visit, whichever is
later 10 The same imaging modality must be used for each subject throughout the study. Assess tumor response at Week 12 (± 3 days),
Week 18 (± 3 days), and every 8 weeks (± 7 days) thereafter. Do not delay imaging if dosing/cycle is delayed
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 35 Confidential Information 03-Jun-2014
6.5 Early Treatment Discontinuation
Treatment may be discontinued early for individual subjects for any of the following reasons:
• Subject decision / withdraw of consent
• Unacceptable toxicity related to the administration of the study required medications according to §7.4
• Cetuximab infusion reactions prior to administration of the first dose of IP (i.e., Cycle 1 Day 1) requiring (i) permanent discontinuation of cetuximab or (ii) administration of corticosteroids with each dose of cetuximab
• Subject lost to follow-up after repeated attempts to contact the subject
• Onset of an adverse event that would make ongoing treatment in the clinical trial inadvisable, as determined by the investigator, medical monitor, or study sponsor
• Subject non-compliance with the study’s requirements and/or procedures as determined by the investigator, medical monitor, or study sponsor
• Death
In the event a subject is withdrawn from treatment prior to/without independently-confirmed disease progression per irRECIST, the subject should continue to complete imaging assessments per protocol until another anti-cancer therapy is initiated, or death.
In addition, if a subject is withdrawn from treatment prematurely due to any of the reasons noted above, the End of Treatment evaluations should be completed, and the subject should be followed for survival.
Subjects should remain on study (i.e., be followed for survival) until death. In the rare event that a subject withdraws consent for all study-related activities, including follow-up for survival, this should be clearly documented in the medical record and eCRF.
6.6 Assessments 6.6.1 Assessment of Efficacy 6.6.1.1 Efficacy Parameters
The following efficacy parameters will be assessed by independent radiology review according to irRECIST (§11.3), and are defined as follows:
• Progression-free survival: the duration of time from randomization to the time of irPD or death, whichever comes first
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 36 Confidential Information 03-Jun-2014
• Objective response rate: the proportion of subjects who achieve complete or partial response
• Duration of best response: the duration of time from the date measurement criteria are first met for irCR, or irPR (if irCR is never met), until the first date that irPD is confirmed by independent radiology review or death, whichever comes first
• Disease control rate: the percentage of subjects who achieved irCR, irPR, or irSD
• Duration of disease control: the duration of time from the date measurement criteria are first met for irCR, irPR, or irSD, until the first date that irPD is confirmed by independent radiology review or death, whichever comes first
Overall survival is defined as the duration of time from randomization to the time of death due to any cause, or the date the subject was last confirmed to be alive.
6.6.1.2 Method and Timing
Imaging studies (CT or MRI) of the neck, chest, upper abdomen, and other anatomical region(s) of disease must be obtained at study Screening, Week 12, Week 18, and every 8 weeks thereafter until disease progression. Imaging studies will be completed at the End of Treatment visit for subjects who discontinue the study prematurely and have not had CT/MRI completed within the last 4 weeks (§6.5). For each subject, the same imaging method must be used at study screening and all follow-up assessments.
RECIST v1.1 is primarily designed to evaluate the early effects of cytotoxic agents and depends on tumor shrinkage to demonstrate biologic activity. However, clinical evidence of tumor responses seen with immunotherapeutic agents, such as VTX-2337, can take longer to achieve and may occur after a period of disease stabilization or following an initial increase in tumor burden. In light of the limitations of utilizing RECIST v1.1 to evaluate immunomodulatory agents, immune-related response criteria have been proposed as an alternative to conventional RECIST to systematically detect the novel response patterns observed with immunologic agents.[18, 19] This study will use RECIST v1.1 for the baseline tumor evaluation, and an immune-related modification of RECIST v1.1 (irRECIST) to determine tumor response.
As noted above, the immune-mediated responses expected from VTX-2337 require activation of the immune system prior to the observation of clinical responses, and such immune activation may take weeks to months to be clinically evident. Some subjects with advanced cancer may have objective increase of tumor burden within 12 weeks following the start of dosing on study. Such subjects may not have had sufficient time to develop the required immune activation or, in some subjects, tumor increases may represent infiltration of lymphocytes into the original tumor (often referred to as pseudo-progression). In traditional oncology studies, such increases in tumor
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 37 Confidential Information 03-Jun-2014
burden during the first 12 weeks of the study would constitute progressive disease and lead to discontinuation of study treatment and imaging to detect response, thus disregarding the potential for subsequent immune-mediated clinical response. Therefore, in this study, the first imaging assessment will be performed at Week 12, followed by assessments at Week 18 and every 8 weeks thereafter.
In addition, a key distinction between standard RECIST v1.1 criteria and irRECIST is that the latter requires early evidence of disease progression (i.e., an assessment of progressive disease ≤ 12 weeks after starting study treatment)—in the absence of rapid clinical deterioration—be confirmed by repeat, consecutive imaging ≥ 4 weeks after the initial assessment. During this interim ≥ 4 week period, subjects should continue to be followed per protocol, including continued dosing with study treatment. The key differences between RECIST v1.1 and irRECIST are outlined in Table 2.
irRECIST
Total Measured Tumor Burden
The total measured tumor burden (TMTB) is established at baseline as the sum of the longest diameters (SOD)—the shortest axes should be used for lymph nodes—of all target lesions (≤ 2 lesions per organ, ≤ 5 lesions total). At each subsequent tumor assessment (TA), the SOD of new, measurable lesions (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; ≤ 2 new lesions per organ, ≤ 5 new lesions total) is added to the SOD of the target lesions to provide the updated TMTB:
TMTB = SOD target lesions + SOD new, measurable lesions
Percentage changes in TMTB at each TA describe the size and growth kinetics of both old and new, measurable lesions as they appear. At each TA, the response in TMTB is defined as follows:
• Complete Response (irCR): Complete disappearance of all target and new, measurable lesions, with the exceptions of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 38 Confidential Information 03-Jun-2014
Response in Non-Target Lesions
The presence of non-target lesions is established at baseline; at each TA, the presence of any new, non-measurable lesions is assessed. The presence of new, non-measurable lesions will rule out an overall response of irCR. An increase in the size or number of new, non-measurable lesions does not necessarily imply an overall response of irPD; if these lesions become measurable (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; up to 2 new lesions per organ, total 5 new lesions) at a subsequent TA, their measurement will, at that point, start to contribute to the TMTB.
The response in non-target lesions is defined as follows:
• Complete Response (irCR): Complete disappearance of all non-target lesions
• non-irCR/non-irPD: Non-target lesions do not meet the criteria for irCR or irPD
• Progressive Disease (irPD): Unequivocal increase in the number or size of non-target lesions. To achieve unequivocal progression of non-target lesions, there must be a substantial worsening of non-target disease of a magnitude that, according to the treating physician, warrants a change in anticancer therapy
NOTE: Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing lesions) should be considered irSD and treatment may continue until the next scheduled assessment.
Overall Response
The overall response according to irRECIST is derived from the responses in TMTB as well as the presence of any non-target lesions as follows:
• Complete Response (irCR): Complete disappearance of all lesions (whether measurable or not); lymph nodes must decrease to < 10 mm in shortest dimension
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
Comprehensive RECIST v1.1 and irRECIST guidelines can be found in §11.2 and §11.3, respectively.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 39 Confidential Information 03-Jun-2014
Table 2: Tumor Response Evaluation: Comparison between RECIST v1.1 and irRECIST
Criteria RECIST v1.1 irRECIST
First tumor assessment (TA) Typically assessed at Week 8 Assessed at Week 12
New lesion(s)
New measurable lesions (≥ 10 mm [≥ 15 mm for lymph node short axis])
Always represents PD Included in TMTB if measurable
New non-measurable lesions (< 10 mm [< 15 mm for lymph node short axis])
Always represents PD Does not define progression but precludes irCR
Non-target lesions Changes contribute to defining best overall response (BOR), CR, PR, SD and PD
Changes contribute to defining irCR (complete disappearance required)
Unequivocal progression of non-target lesions
Always represents PD May represent irPD if there is a substantial worsening that warrants a change in anticancer therapy
CR Disappearance of all lesions Disappearance of all lesions
PR ≥ 30% decrease in the SOD of all target lesions compared with baseline, in absence of new lesions or unequivocal progression of non-target lesions
≥ 30% decrease in the TMTB compared with baseline
SD Neither CR, PR, or PD can be established
Neither irCR, irPR, or irPD can be established
PD ≥ 20% increase in SOD of target lesions compared with nadir. The SOD of target lesions must also demonstrate an absolute increase of ≥ 5 mm. The appearance of ≥ 1 new lesions is also considered progression
≥ 20% increase in TMTB compared with nadir. The TMTB must also demonstrate an absolute increase of ≥ 5mm*
*Subjects with an initial finding of progressive disease (irPD) before or at the 12 week imaging assessment, but without rapid clinical deterioration, require confirmation of irPD with a second, consecutive scan obtained ≥ 4 weeks from the initial documentation. Subjects will continue to receive study treatment until irPD is confirmed at this later time point. Best overall response (BOR) will therefore include responses occurring at any time before disease progression and after early progression (i.e., within the first 12 weeks of the study).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 40 Confidential Information 03-Jun-2014
6.6.2 Assessment of Safety 6.6.2.1 Safety Parameters
The primary safety parameters are the occurrence and severity of adverse events throughout the study treatment period. Refer to §8.2 for AE reporting requirements.
The pre-dose assessments performed on Day 1—including PE, vital signs, and laboratory assessments—will serve as the baseline and the standard for comparison of all follow-up examinations. All abnormal findings will be noted on follow-up and compared to baseline and clinically significant changes will be noted as adverse events.
6.6.2.2 Method and Timing
History and Physical Examination
A complete physical exam and medical history, including detailed cancer history, must be obtained within 14 days prior to randomization.
Complete physical exams and problem-oriented physical exams are subsequently required as described in §6.0. Vital signs should be monitored as shown in Table 1.
Electrocardiograms
A 12-lead ECG will be performed at Screening, 1-hour post dose on Cycle 1 Day 8 and Cycle 3 Day 8, and End of Treatment.
Clinical Laboratory Evaluations
The clinical laboratory evaluations will be collected at Screening and within 72 hours of Day 1 of each cycle, and will include a complete set of clinical labs, including serum chemistry, complete blood count with differential, and urinalysis, as described in §6.2.
Subject-Reported Adverse Events
In addition to those adverse events noted by the study staff as determined through clinical evaluation, additional events may be elicited from the subject in a non-leading manner or volunteered by the subject at any time during the study. All adverse events, regardless of their severity or relationship to treatment with IP, will be recorded. All subjects experiencing adverse events will receive treatment if required for their event. Adverse events that are determined to be related to IP will be followed until resolution, or until resolved with sequelae.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 41 Confidential Information 03-Jun-2014
6.6.3 Translational Research Assessments
Various immune and immunogenetic assessments will be performed on all subjects in the study. Exploratory analyses correlating data from these assessments will be performed to determine if predictors of potential clinical benefit emerge. These predictors would be valuable in defining appropriate populations for study in subsequent trials of VTX-2337 in this patient group.
Pharmacogenomics
A single sample of genomic DNA will be collected on all subjects for analysis of genetic polymorphisms that may impact the response of patients to a TLR8 agonist or to cetuximab. These include defined single nucleotide polymorphisms (SNPs) in the TLR8 gene (most notably the A1G variant), and variants in the FcγRII and FcγRIII genes (most notably the 131 and 158 polymorphisms, respectively), that vary binding affinity for the FcR.
Immune Biomarker Analysis
TLR8 stimulates the production of a variety of cytokines and chemokines from immune cells. Serum samples will be collected pre-dose and 8 hours post-dose on C1D8 and C3D8 for analysis using a multiplexed panel of cytokines, chemokines, and inflammatory markers.
Tissue Biomarker Studies
Assessment of the effect of immune cell subsets, as measured by immunohistochemistry in primary tumor tissue (e.g., immune score) will be completed on tumor tissue obtained from the primary tumor site. This analysis includes but is not limited to an automated analysis of CD3, CD45, and FOXP3 staining of lymphocyte populations in the tumor using immunohistochemistry. Additional studies including gene signature analysis or detached somatic mutations will be performed, if indicated.
Pharmacokinetic Analysis
Plasma samples will be obtained on Cycle 1 Day 8 and quantitatively analyzed to support population PK and exposure-response analyses.
6.7 Monitoring for Subject Compliance
No specific measures for subject compliance are required for this study. IP must be administered in the clinic or hospital setting under the supervision of the investigator or clinical site staff. Subjects should be carefully evaluated prior to study entry to ensure they can comply with the study’s visit and assessment schedule.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 42 Confidential Information 03-Jun-2014
7.0 TREATMENT 7.1 Packaging, Labeling and Storage
IP is provided as an off-white, lyophilized cake in a 3-mL clear-glass, stoppered, single-use vial. Each vial is identified with a label similar to the following:
8.4 mg VTX-2337 or Placebo for subcutaneous injection
Subject #XXXXX
Prepare according to clinical protocol VRXP-A202
Store 2–8ºC
Caution: New drug—limited by federal law to investigational use.
VentiRx Pharmaceuticals, Inc.
8.4 mg VTX-2337 or Placebo for subcutaneous injection
Subject XXXXX for protocol VRXP-A202
Subject #: ________________
Date: ___________________
↑ This portion attached to vial ↑ Detach this portion for subject record
Upon randomization, a subject-specific kit containing a supply of IP will be shipped via traceable courier to the clinical site. Sites will order re-supply kits through the IXRS. Unopened vials of IP should be stored in the refrigerator at 2−8ºC (36−46ºF) and protected from light.
VTX-2337 and placebo will be labeled, packaged, and shipped by Fisher Clinical Services (Mount Prospect, IL).
7.2 Preparation of Investigational Product
Refer to the Pharmacy Manual for complete instructions regarding the storage and preparation of IP.
Before administration, IP must be reconstituted and prepared according to the Pharmacy Manual. Investigational drug solution should be prepared and transferred using aseptic technique in a biological safety cabinet. Vials of IP are intended for single use only.
IP will be supplied by VentiRx Pharmaceuticals. All other medications may be obtained through standard institutional practice.
7.3 Administration of Investigational Product and Study Treatment(s) 7.3.1 Investigational Product Administration
IP (i.e., VTX-2337 or placebo) is administered as a subcutaneous injection of 3.0 mg/m2 (see also §9.2.2). Doses are given prior to cetuximab on Days 8 and 15 of a 21-day cycle for the first
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 43 Confidential Information 03-Jun-2014
6 cycles and on Days 8 and 22 for cycles 7+. Subjects will continue to receive bi-weekly doses of IP until independently-confirmed disease progression. See also §6.3 and §6.5.
Within 30 minutes prior to each dose of IP subjects will be administered 650–1000 mg acetaminophen by mouth to help mitigate potential adverse events commonly associated with the administration of VTX-2337 (e.g., fever, myalgia). Subjects will be given or instructed to take an additional dose of 650–1000 mg acetaminophen by mouth approximately 4–6 hours after administration of IP, and as needed thereafter for symptoms of fever and/or body aches. Acetaminophen is the preferred over-the-counter analgesic and antipyretic; due to their potentially immunosuppressive effects, administration of NSAIDS within 24 hours of dosing should be avoided if clinically feasible.
To potentially reduce the effects of injection site reaction that may be associated with the administration of IP, an ice pack may be applied to the injection site for approximately 30 minutes prior to injection, immediately following injection, and throughout the day of injection. Additionally, at the discretion of the investigator, single doses of IP may be divided and administered at two different anatomical locations.
The dose of IP should be administered with a syringe suitable for subcutaneous injection. To administer the injection, 1–2 inches of fatty tissue should be pinched up to avoid injection into the muscle layer. The needle can be inserted at either 45 or 90 degrees; a 45 degree angle is recommended when less than 2 inches of tissue can be pinched. Appropriate anatomic areas for subcutaneous injection include the fatty tissue over the abdomen, triceps, thighs, or lower back. The injection site should be rotated among anatomically appropriate locations to help avoid injection site reaction.
Standard medications to treat possible hypersensitivity reactions and/or symptoms of CRS should be readily available at the time of treatment, including epinephrine, H1 antihistamines (e.g., diphenhydramine), H2 antihistamines (e.g., ranitidine), narcotics, IV fluids for volume expansion and supplemental oxygen.
Due to their immunosuppressive effect, administration of systemic corticosteroids (e.g., dexamethasone) should be avoided in this setting if other means of treatment are available and appropriate.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 44 Confidential Information 03-Jun-2014
7.3.2 Cetuximab Administration
The initial 400 mg/m2 dose of cetuximab is administered on Cycle 1 Day 1 as a 120-minute IV infusion (maximum infusion rate 10 mg/min).1
The subsequent, weekly, 250 mg/m2 doses of cetuximab are administered as 60-minute IV infusions (maximum infusion rate 10 mg/min).1 Subjects will continue to receive weekly doses of cetuximab until independently-confirmed disease progression. See also §6.3 and §6.5.
Subjects will be premedicated with an H1 antagonist (e.g., 50 mg of diphenhydramine) intravenously 30–60 minutes prior to the first dose; premedication should be administered for subsequent cetuximab doses based upon clinical judgment and the presence/severity of prior infusion reactions. Premedication with steroids may be administered on Cycle 1 Day 1, if required by institutional standards. However, due to their immunosuppressive effect, steroids should be discontinued 72 hours prior to dosing with IP. See also §7.6.
Serious infusion reactions, requiring medical intervention and immediate, permanent discontinuation of cetuximab, include rapid onset of airway obstruction (e.g., bronchospasm, stridor, hoarseness), hypotension, shock, loss of consciousness, myocardial infarction and/or cardiac arrest. Subjects should be monitored for 1 hour following cetuximab infusions in a setting with resuscitation equipment and other agents necessary to treat anaphylaxis (e.g., epinephrine, intravenous antihistamines, bronchodilators, oxygen, and corticosteroids).
When cetuximab is administered on the same day as chemotherapy, cetuximab administration will be completed ≥ 1 hour prior to administration of platinum and 5-FU. When cetuximab is administered on the same day as IP, the dose of IP will be given prior to cetuximab.
For additional information please refer to the cetuximab label.
7.3.3 Platinum Administration
The platinum therapy should be assigned by the investigator prior to randomization. Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent should be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject. Reasonable efforts should be made to keep the subject on the platinum therapy originally assigned; however, the platinum therapy may be changed if clinically necessary.
1 The duration of infusion may be adjusted according to institutional standards.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 45 Confidential Information 03-Jun-2014
Cisplatin
At least one hour after completion of cetuximab administration, subjects will receive a 100 mg/m2 dose of cisplatin administered as a 60-minute IV infusion.1 Cisplatin will be administered on Day 1 of a 21-day cycle for a maximum of 6 cycles and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
Pretreatment hydration may be administered according to institutional standards.
For additional information regarding cisplatin administration, please refer to the label.
Carboplatin
At least one hour after completion of cetuximab administration, subjects will receive carboplatin at an AUC of 5 mg/mL/min administered as a 60-minute IV infusion.1 Carboplatin will be administered on Day 1 of a 21-day cycle for a maximum of 6 cycles, and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
For additional information regarding administration, please refer to the carboplatin label.
7.3.4 Fluorouracil (5-FU) Administration
At least one hour after completion of cetuximab administration, subjects will receive an intravenous infusion of 5-FU at a dose of 1000 mg/m2 per day for 4 days. 5-FU administration will begin on Day 1 of a 21-day cycle for a maximum of 6 cycles and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
For additional information regarding 5-FU administration please refer to the label.
7.4 Dose Modifications
In order to maintain dose-intensity and cumulative dose-delivery, reasonable efforts should be made to minimize dose reductions and treatment delays. Any subject whose treatment is delayed due to treatment-related toxicity should be evaluated on a weekly basis until adequate hematologic and non-hematologic parameters have been met.
Toxicities may require reduction or discontinuation of one or more of the study required-medications (refer to §7.4.3). The investigator should carefully assess all treatment-associated toxicities and, whenever possible, determine if the toxicities can reasonably be attributed to a single agent, or, conversely, if a causal relationship with an agent can reasonably be ruled out. If
1 The duration of infusion may be adjusted according to institutional standards.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 46 Confidential Information 03-Jun-2014
appropriate, dose reductions and discontinuations should not affect the dose or administration of the other agents.
• Toxicity grades are defined using the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 4.03
• Any subject who requires a dose reduction due to drug-related toxicity will continue to receive the reduced dose for the remainder of study treatment
• Prior to dose reduction, supportive care should be maximized at the investigator’s discretion for adverse events such as nausea, vomiting, diarrhea, and electrolyte imbalances
• Dose escalations are not allowed
• If study-required therapy is delayed by more than 6 weeks for any reason, the site should contact the medical monitor
It is anticipated that toxicities attributed to the cytotoxic agents (cisplatin, carboplatin, and/or 5-FU) may require a delay in the Day 1 dose of the next scheduled treatment cycle while awaiting subject recovery. In such a case, platinum and 5-FU chemotherapy should be delayed together in order to ensure that they are administered together at the next Day 1 treatment. During a treatment delay, subjects should be evaluated weekly. If toxicity leads to a delay in cytotoxic chemotherapy for greater than 3 consecutive weeks (i.e., > 21 days), one or both of the chemotherapeutic agents (at the discretion of the investigator, depending upon the cause of toxicity) should be permanently discontinued. This should not impact the continuation of the other study treatments, including platinum in the absence of 5-FU or vice versa.
During the ≤ 3-week delay, the previous cycle should be extended to include treatment on Day 22 and potentially Days 29 and 36 (see below). Please refer to §11.4 for additional information.
Extended Cycles 1–5, Day 22 (CXD22) (±1day)
• If evaluations performed by the local laboratory are required to assess ongoing toxicities (e.g., decreased neutrophils), also send samples to the central laboratory
• Problem-oriented PE, including vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 47 Confidential Information 03-Jun-2014
Extended Cycles 1–5, Day 29 (CXD29) (±1day)
• If evaluations performed by the local laboratory are required to assess ongoing toxicities (e.g., decreased neutrophils), also send samples to the central laboratory
• Problem-oriented PE, including vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Extended Cycles 1–5, Day 36 (CXD36) (±1day)
• If evaluations performed by the local laboratory are required to assess ongoing toxicities (e.g., decreased neutrophils), also send samples to the central laboratory
• Problem-oriented PE, including vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
It is possible that a subject may require a dose to be held due to toxicities related to cetuximab or IP. Those doses should be considered missed and will not be made up. For example, if on Day 15, a subject is unable to receive the scheduled dose of cetuximab, IP should be given as appropriate, and the next week the subject would proceed with Day 1 of the next cycle.
The timing of imaging studies should not be affected by dose reductions or delays. Subjects should remain on study (i.e., continue receiving treatment with other agents and undergo all protocol-related assessments) until independently-confirmed disease progression. Thereafter, subjects should be followed for long-term survival per protocol.
7.4.1 Investigational Product Dose Modifications
Management of Injection Site Reactions
Acute symptoms of injection site reactions typically resolve within 48 hours of injection, but more persistent reactions are not unexpected. Grade 2 and 3 reactions may include a painful, raised, fluid-filled blister that mimics a sterile abscess. Injection site reactions do not typically warrant antibiotic intervention as they have been found to be sterile. A culture of the fluid can be
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 48 Confidential Information 03-Jun-2014
obtained—using sterile technique—if infection is strongly suspected (i.e., associated with fever persisting more than 24 hours after injection).
Ice and acetaminophen should be administered prophylactically according to §7.3.1. Symptomatic treatment with ice, acetaminophen and narcotics is acceptable. Due to their potentially suppressive effects, the use of NSAIDs within 24 hours of dosing with IP should be avoided, if clinically feasible.
Management of Systemic Toxicities
The most common systemic drug-related adverse events—grade 1 or 2 chills, flu-like symptoms and fever—typically resolve in < 48 hours and do not require dose reductions or a delay in the dosing regimen. Less commonly, dosing with VTX-2337 may result in CRS, which is most likely to be grade 1 or 2, but more severe reactions have been reported.
CRS is a symptom complex and is characterized by systemic symptoms which may include fever, nausea, chills, tachycardia, hypotension, dyspnea, asthenia, headache, and rash. VTX-2337 directly targets TLR8, which is expressed on immune cells. CRS may result from the release of cytokines from the activated immune cells, or from ‘downstream’ events that can be associated with cytokine production. Symptoms of CRS may be acute or delayed by several hours after dosing with IP.
Treatment of systemic drug-related events should be consistent with the severity of the reaction as well as institutional standards and may include: acetaminophen, H1- and H2-receptor antagonists, narcotics, IV fluids for volume expansion, and supplemental oxygen. Due to their potentially immunosuppressive effect, administration of NSAIDs and systemic steroids (e.g., dexamethasone) should be avoided if other means of treatment are available and medically appropriate.
In most cases the CRS will be grade 1 or 2. However, a severe, life-threatening reaction resulting from a substantial release of cytokines is possible. Severe CRS is a medical emergency and urgent intervention must be taken to prevent life-threatening complications. This may include administration of sympathomimetic amines for pressor support and/or hospitalization for acute monitoring and intervention.
Investigational Product Dose Modifications
Table 3 and Table 4 outline dose delay and reduction requirements for IP. Delays in IP dosing should not delay or shift the timing of cetuximab, platinum, or 5-FU dosing (i.e., doses of IP are skipped and not made up). In the event of grade 3 or grade 4 toxicities attributed to IP, subsequent doses should be delayed until recovery to ≤ grade 1.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 49 Confidential Information 03-Jun-2014
Table 3: Investigational Product Dose Reduction Schedule
IP Dose Level (mg/m2)
3.0
2.5
2.0
NOTE: Only two dose reductions are allowed. If a third dose reduction is required, IP should be discontinued.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 50 Confidential Information 03-Jun-2014
Table 4: Investigational Product Dose Modifications
Grade Action
Cytokine Release Syndrome
1 Dose reduction not required; consider prophylactic precautions—including volume expansion and treatment with oral or IV antihistamines—with next dose
2 Consider prophylactic precautions—including volume expansion and treatment with oral or IV antihistamines—with next dose Reduce dose by 1 level at investigator’s discretion
3 Use prophylactic precautions with next dose Reduce dose by 1 level
Injection Site Reaction
1 Dose reduction not required; consider administering subsequent injections at distal anatomic site(s)
2 Administer subsequent injections at distal anatomic site(s) until resolved to ≤ grade 1
Delay dosing for up to 2 weeks if needed
If > 2 week delay or > 2 delays are required with consecutive injections, reduce dose by 1 level
3 Delay dosing until resolved to ≤ grade 1 Reduce dose by 1 level
Non-Hematologic Drug-Related AEs
1–2 Dose reduction not required; manage per institutional standards
≥ 3 Reduce dose by 1 level
Hematologic Drug-Related AEs
1–3 Dose reduction not required; manage per institutional standards
≥ 4 Reduce dose by 1 level
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 51 Confidential Information 03-Jun-2014
7.4.2 Cetuximab Dose Modifications
Table 5 and Table 6 should be used as a guideline for cetuximab dose modifications. Please refer to the cetuximab label for additional information.
Table 5: Cetuximab Dose Modifications for Infusion Reactions
NCI-CTC Grade Dose Modification
1
Reduce infusion rate by 50% 2
Non-serious grade 3
Serious grade 3 (e.g., requiring hospitalization) or any grade 4 Immediately and permanently discontinue cetuximab
Table 6: Cetuximab Dose Modifications for Dermatologic Toxicity
Severe Acneiform Rash Cetuximab Delay/Discontinuation
Outcome Dose Modification
1st occurrence Delay infusion by 1–2 weeks Improvement Continue at 250 mg/m2
No improvement Discontinue cetuximab
2nd occurrence Delay infusion by 1–2 weeks Improvement Reduce dose to 200 mg/m2
No improvement Discontinue cetuximab
3rd occurrence Delay infusion by 1–2 weeks Improvement Reduce dose to 150 mg/m2
No improvement Discontinue cetuximab
4th occurrence Discontinue cetuximab
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 52 Confidential Information 03-Jun-2014
7.4.3 Chemotherapy Dose Modifications (cisplatin, carboplatin, and 5-FU)
Table 7 and Table 8 should be used as a guide for dose reductions of cisplatin, carboplatin, and 5-FU. The dose of each agent should be reduced by 25% in subjects with related toxicities ≥ grade 3. Primary or secondary prophylaxis with granulocyte colony growth factor (G-CSF) is permitted in order to manage the neutropenia expected from platinum-5-FU therapy.
Table 7: Dose Reduction Guidelines for Chemotherapeutic Agents
Grade ≥ 3 Toxicity Chemotherapy Delay/Discontinuation
Outcome Dose Modification
1st occurrence Delay infusion by 1–3 weeks Improvement Reduce dose by 25%
No improvement Discontinue agent
2nd occurrence Delay infusion by 1–3 weeks Improvement Reduce dose to 50%
No improvement Discontinue agent
3rd occurrence Discontinue agent
Table 8: Chemotherapy Dose Reduction Schedule
Agent Original Dose (100%) 25% Reduction 50% Reduction
Cisplatin 100 mg/m2 75 mg/m2 50 mg/m2
Carboplatin AUC of 5 mg/mL/min AUC of 3.75 mg/mL/min AUC of 2.5 mg/mL/min
5-FU 1000 mg/m2/day 750 mg/m2/day 500 mg/m2/day
Additional Considerations for Chemotherapy Dosing
Investigators should follow their institutional standards for repeat dosing criteria (i.e., serum creatinine and hematologic thresholds for dosing).
When clinically appropriate, subjects assigned to cisplatin should receive 2 dose reductions prior to discontinuation of cisplatin and/or being re-assigned to receive carboplatin. If clinically necessary, the investigator may change the platinum chemotherapy from cisplatin to carboplatin.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 53 Confidential Information 03-Jun-2014
7.5 Emergency Unblinding
The treatment assignment of any individual subject may be accessed only in case of an emergency, such as a life-threatening serious adverse event (SAE) where knowledge of the treatment code is required for medical management of the event. The investigator should obtain approval from the medical monitor or sponsor prior to unblinding and should document the unblinding (including notification of sponsor/medical monitor and reason for unblinding) in the subject’s medical record.
Contact information for notification of unblinding:
PRA Oncology Call Center Toll Free: +1 (866) 326-5053 Direct: +1 (434) 951-4082 Fax: +1 (800) 280-7035 Email: [email protected]
After obtaining sponsor or medical monitor approval, to unblind the subject’s treatment assignment the investigator will log into IXRS and enter, at minimum, the subject’s randomization number; IXRS will then provide the treatment assignment. The treatment assignment should be maintained as confidential (i.e., only personnel essential for subject treatment should be informed of the treatment assigned) and placed in a sealed envelope.
The treatment code for an individual subject may also be broken at the discretion of the study sponsor to facilitate regulatory reporting of suspected unexpected serious adverse reactions (SUSAR).
7.6 Concomitant Medications and Supportive Care
Medications that must be discontinued prior to study entry are outlined in §5.2. The following medications and interventions, unless otherwise specified, are prohibited from the time of study screening until the End of Treatment visit:
• Systemic anti-cancer therapy, including chemotherapy, radiotherapy, or endocrine therapy other than those required per protocol
• Systemic—oral, IV, injectable—corticosteroids (e.g., dexamethasone, prednisone) within 72 hours of dosing with IP (see also §7.6.1)
• Any investigational drug or device other than VTX-2337 or placebo
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 54 Confidential Information 03-Jun-2014
• NSAIDs, including aspirin, within 24 hours of IP dosing should be avoided if clinically feasible, due to their potentially suppressive effects Any immunotherapy other than VTX-2337 or placebo
• Cytochrome P450 3A4 (CYP3A4) inducers and/or inhibitors may affect the metabolism of VTX-2337. Therefore, care should be exercised when drugs or other substances that affect CYP3A4 are administered concomitantly with VTX-2337 or placebo and, if possible, alternatives that do not affect CYP3A4 should be administered instead. A list of CYP3A4 inhibitors and inducers may be found in §11.5.
Subjects should be provided with full supportive care measures, as clinically indicated, and in accordance with institutional standards. Such care includes medication for pain control and symptom management, antibiotics, bisphosphonates, antiemetics, colony stimulating factors, and transfusions of blood or blood products. Treatment for drug-related adverse events should be administered at the discretion of the investigator.
Anaphylactic-like reactions have been reported with administration of cetuximab, cisplatin, carboplatin, and 5-FU. Epinephrine and/or antihistamines may be administered to alleviate symptoms. Due to their immunosuppressive effect, administration of systemic steroids (e.g., dexamethasone) should be avoided in this setting if other means of treatment are available and appropriate. For additional information on treatment of cetuximab infusion reactions refer to §7.3.
Localized radiotherapy is permitted for palliation of painful lesions at the investigator’s discretion. However, medical management in place of radiation therapy should be used if clinically appropriate.
7.6.1 Chemotherapy-induced nausea and vomiting
Corticosteroids (e.g., dexamethasone) are often used as the first-line treatment for chemotherapy-induced nausea and vomiting (CINV); however, the administration of systemic corticosteroids (oral, IV, injectable) broadly inhibits the production of multiple cytokines and chemokines and impairs cellular immunity, thus impeding the immunostimulatory and pharmacologic effects of VTX-2337. For this reason, a steroid-sparing approach to toxicity management is ideal—particularly in terms of steroid frequency and proximity to IP administration.
The nausea and vomiting associated with high-dose cisplatin and 5-FU may be acute (onset 1–4 hours after infusion) or delayed (begins or persists ≥ 24 hours after infusion). Prophylactic use of steroids on Day 1 to combat the acute nausea and vomiting are allowed. Alternatives to steroid
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 55 Confidential Information 03-Jun-2014
use on days 2–4 should be employed, if possible. However, use of steroids within 72 hours of IP administration is prohibited.
Non-steroidal antiemetic treatment options include both short- and long-acting 5-HT3 antagonists (e.g., ondansetron, palonosetron), short- and long-acting NK1 receptor antagonists (e.g., Emend/aprepitant, fosaprepitant), benzodiazapines, diphenhydramine, and metoclopramide.
7.6.2 Fever with Neutropenia
VTX-2337 has not been associated with hematologic toxicity such as myelosuppression or neutropenia. Transient, aseptic grade 1 and grade 2 (up to 40°C/104°F) pyrexia driven by cytokines is a common side effect of VTX-2337, occurring in approximately 50% of treated subjects. Grade 3 fever (> 40°C/104°F) has been observed in approximately 8% of treated subjects. The characteristic VTX-2337-related fever has an onset 3–8 hours after dosing, lasts approximately 24 hours, and is typically experienced following each dose. This fever may or may not be accompanied by flu-like symptoms such as shaking, chills, and myalgia. In contrast, in a Phase 3 study of cetuximab plus platinum-5-FU, more than 25% of subjects experienced grade 3 or 4 neutropenia and 6% of subjects experienced febrile neutropenia.[12] As the neutrophil nadir from platinum-5-FU therapy typically occurs between days 10 and 23 of the treatment cycle, it is expected that a fever induced by VTX-2337 may overlap with a period of grade 3–4 neutropenia induced by platinum-5-FU.
It may be difficult to differentiate between IP-related aseptic fever in a patient with incidental neutropenia and the presumed infectious state of classic febrile neutropenia. The former would be expected to involve the characteristics of VTX-2337-related fever noted above (i.e., fever following each dose with an onset and resolution within 24 hours) and would not be associated with findings of active infection.
Ultimately, investigators should rely upon clinical judgment and follow institutional guidelines when dealing with fever in the setting of neutropenia. Primary or secondary prophylaxis with granulocyte colony growth factor (G-CSF) is permitted in order to manage the neutropenia expected from platinum-5-FU therapy. Recommendations for evaluation and standard antibiotic therapy found in guidelines for inpatient or outpatient management of neutropenic fever may be utilized.
The reporting of adverse events with respect to fever in the setting of neutropenia should accurately reflect the investigator’s assessment of the etiology. If the investigator determines that the events most likely represent the presumed infectious state of classic febrile neutropenia, the single event term of “febrile neutropenia” should be used. However, if the investigator determines that the events most likely represent IP-related aseptic fever in a patient with
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 56 Confidential Information 03-Jun-2014
incidental neutropenia, the event should be reported using the two event terms of “fever” and “neutrophil count decreased”.
7.7 Investigational Product Accountability
VentiRx Pharmaceuticals will provide an adequate supply of IP for the study population and protocol requirements. Drug supplies must be kept in an appropriate, secure area (e.g., locked pharmacy) and stored in accordance with the conditions specified in this protocol, the pharmacy manual, and on the IP labels.
Drug supplies are to be used only in accordance with this protocol, pharmacy manual, and under the personal supervision of the Principal Investigator or under the supervision of a sub-investigator who is responsible to the investigator. IP may be administered only to eligible subjects who are randomized in the study. The Principal Investigator is accountable for all used and unused investigational drug. The investigator agrees not to destroy any used, partially used, or unused investigational drug supplies unless otherwise directed by VentiRx Pharmaceuticals or its representatives. Upon written notification, the investigator will ship unused IP according to instructions provided or will destroy unused IP according to institutional standards.
A master drug log must be maintained for all IP vials received, dispensed (including the subject’s ID number, the subject’s initials, and the dates each vial is dispensed) and returned or destroyed. In addition, a subject-specific record of each vial administered, including the date and identification number of each vial, will be maintained with the case file for each subject. Any discrepancy in the drug distribution logs (master log and subject logs) must be explained in detail.
8.0 ADVERSE EVENTS
The following sections describe the minimum requirements for assessing and reporting AEs, including SAEs and serious suspected adverse reactions, for subjects participating in trial VRXP-A202. The investigator is additionally responsible for complying with all local institution and IRB/IEC requirements for reporting AEs.
8.1 Definitions 8.1.1 Adverse Event (AE)
An adverse event is defined as any untoward medical occurrence associated with the use of a drug in humans, whether or not considered drug-related. An AE can therefore be any unfavorable and unintended sign, symptom, or disease which is temporally associated with the use of the investigational drug, whether or not considered related to (i.e., to have a causal relationship with) the IP.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 57 Confidential Information 03-Jun-2014
AEs include exacerbation of a pre-existing illness, an increase in frequency or intensity of a pre-existing episodic event or condition, a condition detected or diagnosed after IP administration even though it may have been present prior to the start of the study, or a continuous persistent disease or symptom present at baseline that worsens following the start of the study.
Medical conditions and diseases that are present before Cycle 1 Day 1 are only considered AEs if they worsen after starting treatment with Cycle 1 Day 1. Any medical condition with an onset or diagnosis before Cycle 1 Day 1 will be included in the subject’s medical history. Abnormal laboratory values or test results constitute AEs if they induce clinical signs or symptoms or if they require intervention or therapy.
8.1.2 Serious Adverse Event (SAE)
An AE or suspected adverse reaction is considered ‘‘serious’’ if, in the view of either the investigator or sponsor, it results in any of the following outcomes:
• Death
• A life-threatening1 adverse event
• Inpatient hospitalization or prolongation of existing hospitalization,
• A persistent or significant incapacity or substantial disruption of the ability to conduct normal life functions
• A congenital anomaly/birth defect
Important medical events that may not result in death, be life-threatening, or require hospitalization may be considered serious when, based upon appropriate medical judgment, they may jeopardize the subject and may require medical or surgical intervention to prevent one of the outcomes listed in this definition. Examples of such medical events include allergic bronchospasm requiring intensive treatment in an emergency room or at home, blood dyscrasias or convulsions that do not result in inpatient hospitalization, or the development of drug dependency or drug abuse.
8.1.3 Dose-Limiting Toxicities (DLT)
DLTs were assessed for all subjects until six subjects randomized to receive VTX-2337 received one cycle of treatment and the DSMB completed the assessment of the starting dose. (§9.2.2)
1 An AE or suspected adverse reaction is considered “life-threatening” if, in the view of either the investigator or sponsor, its occurrence places the patient or subject at immediate risk of death. It does not include an AE or suspected adverse reaction that, had it occurred in a more severe form, might have caused death.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 58 Confidential Information 03-Jun-2014
Results from the initial DSMB evaluation concluded that the study can continue as planned at the dose level of 3.0 mg/m2 and that DLT recording criteria could be lifted.
A DLT is defined as any IP-related adverse event, occurring during Cycle 1 (Week 1–3), which meets the following criteria:
• Any ≥ grade 4 hematologic toxicity
• Any ≥ grade 3 non-hematologic toxicity (including injection-site reaction), with the exception of:
— Grade 3 dermatologic toxicities
— Grade 3 hypersensitivity reaction
• Diarrhea, nausea, or vomiting will only be considered a DLT when ≥ grade 3 toxicity occurs despite adequate anti-emetics or anti-diarrhea medications
• Treatment delay due to toxicity lasting greater than 21 days
• Death
“IP related” refers to events that are possibly or probably related to the administration of IP or the combined treatment regimen of IP, platinum, 5-FU, and cetuximab, and not clearly attributed to platinum, 5-FU, cetuximab alone, or other causes.
8.2 Reporting Requirements
Information regarding all AEs, whether volunteered by the subject, discovered via questioning by the investigator or clinical personnel, or identified through physical examination, laboratory test or other means will be collected from the first dose of study required medication administered on Cycle 1 Day 1 until the End of Treatment visit or 7 days after the last dose of any study medication, whichever is later. Suspected adverse reactions (i.e. AEs that are assessed as related to IP) which are ongoing will be followed until resolution or until grade ≤ 2 and stabilized. Suspected adverse reactions may be reported at any time.
Information collected regarding each AE will include, but is not limited to (1) duration (start and stop dates), (2) severity as delineated in §8.3, (3) relationship to the investigational drug (“causality”) as described in §8.5 (serious adverse events only), (4) any action taken and (5) outcome. Whenever possible, AEs should be described in terms of a change in the baseline status (e.g., “increased frequency of migraines”) or with a diagnosis or summary term in place of individual clinical signs or symptoms (e.g., “upper respiratory infection” vs. “runny nose”, “sneezing” and “cough”).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 59 Confidential Information 03-Jun-2014
8.2.1 Serious Adverse Events
The investigator must immediately (≤ 24 hours of clinical site personnel becoming aware of the event) report to the study’s medical monitor any SAE—whether or not considered drug related, including those listed in the IB—and must include an assessment of whether there is a reasonable possibility that the investigational drug caused or otherwise contributed to the event. The site will provide the initial notification to PRA Drug Safety via fax or email on the required SAE Report Form, which must be signed by the investigator. Follow-up information or new information regarding an ongoing SAE must be provided promptly to PRA Drug Safety.
PRA Drug Safety Phone: +1 (800) 772-2215 +1 (434) 951-3489 Fax: +1 (888) 772-6919 +1 (434) 951-3482 email: [email protected]
The investigator is responsible for notifying the IRB/IEC or other appropriate committees of all SAEs in accordance with institutional and IRB/IEC policies.
8.2.2 Dose Limiting Toxicities
As described in §9.2.2, DLTs were assessed for all subjects until the DSMB has completed the assessment of the starting dose. During this DLT assessment period, once the investigator has determined a DLT has occurred, the DLT required reporting within 48 hours to allow the DSMB to review DLTs in a timely manner.
8.3 Criteria for Determining Adverse Event Severity
AEs will be categorized and severity will be graded according to the NCI-CTCAE version 4.03.
Note that “seriousness” and “severity” are distinct concepts. “Serious” is a term applied to an AE that meets specific regulatory requirements; it is typically associated with events that pose a threat to the subject’s life or functioning. “Severity” refers to the AE intensity classification. A severe AE may be of minor medical significance (e.g. grade 3 headache), while an AE that is graded as mild in severity may be serious (e.g. grade 1 stroke requiring overnight hospitalization).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 60 Confidential Information 03-Jun-2014
8.4 Criteria for Determining Adverse Event Expectedness
An AE or suspected adverse reaction is considered ‘‘unexpected’’ if it is not listed in the IB or is not listed at the specificity or severity that is observed. The sponsor or its representative will be responsible for determining the expectedness of adverse events.
For example, under this definition, hepatic necrosis would be unexpected (by virtue of greater severity) if the IB referred only to elevated hepatic enzymes or hepatitis. Similarly, cerebral thromboembolism and cerebral vasculitis would be unexpected (by virtue of greater specificity) if the IB listed only cerebral vascular accidents. ‘‘Unexpected’’—as used in this definition—also refers to AEs or suspected adverse reactions that are mentioned in the IB as occurring with a class of drugs or as anticipated from the pharmacological properties of the drug, but are not specifically mentioned as occurring with the particular drug under investigation.
Therefore, "unexpected" also refers to an AE or suspected adverse reaction that has not been previously observed (i.e. included in the IB) rather than from the perspective of such an experience not being unanticipated from the subject’s disease state.
8.5 Criteria for Determining Adverse Event Causality
The following categories for determining the relationship of an AE to the IP are as follows:
None: The AE is temporally independent of the administration of IP and/or can be readily attributed to other factors such as the subject’s clinical state, environmental factors, or concomitant drugs or therapies
Possible: The AE follows a reasonable temporal sequence from administration of IP and cannot readily be explained by the subject’s clinical state, environmental factors, or concomitant drugs or therapies
Probable: The AE follows a clear temporal sequence from administration of IP and is unlikely to be related to the subject’s clinical state, environmental factors, or concomitant drugs or therapies. The AE ceases with discontinuation of the drug and reoccurs after restarting, if applicable
Note that the term “suspected adverse reaction” is used to describe an AE for which there is a reasonable possibility that the IP caused the adverse event (i.e. an event that is assessed as ‘possibly’ or ‘probably’ caused by administration of IP).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 61 Confidential Information 03-Jun-2014
8.6 Expedited Reporting of Serious Adverse Events
Regulations require that VentiRx Pharmaceuticals or its representatives to report any suspected adverse reactions1 that are both serious (§8.1) and unexpected (§8.4). Such events must be reported to the FDA, applicable regulatory authorities, and all participating investigators (i.e., all investigators to whom VentiRx is providing drug under its INDs or under any investigator’s IND) within 15 calendar days after VentiRx or its representative receives the information and determines that it qualifies for reporting. Such notification must occur within 7 calendar days if the SUSAR was fatal or life-threatening.
Therefore, once the investigator has determined that an SAE has occurred, it is important to adhere to the reporting timeframes outlined in §8.2.1. After receiving the investigator’s SAE report, including the investigator’s assessment of causality, VentiRx or its representatives will also assess the event for seriousness and the relationship to IP and will determine if the event was unexpected.
Investigational New Drug Safety Reports (INDSRs), or equivalent, will be reported to FDA and applicable local regulatory authorities by VentiRx Pharmaceuticals or its representatives; copies of the report will be distributed to clinical investigators. The investigator is responsible for notifying the relevant IRB/IEC of all INDSRs in accordance with institutional and IRB/IEC policies.
9.0 STATISTICAL PLAN 9.1 Statistical Considerations
All analyses will use SAS® version 9.1.3 or higher (SAS Institute, Inc., Cary, NC). Summary tables will be organized by treatment group: Combination Arm (SOC plus VTX-2337) versus Control Arm (SOC plus placebo). All available scheduled data for the safety or efficacy populations will be used in the analyses. Important CRF data will be included in data listings for all subjects who are randomized on the study. Missing data will not be imputed, except via censoring in survival analyses.
In keeping with ICH E9, center effect will not be included in the analysis models as it is recognized that there will be limited numbers of subjects per center in this trial. However, randomization stratification factors and/or their interaction terms with treatment may be explored.
1 A suspected adverse reaction is an adverse event for which there is a reasonable possibility that the investigational drug caused the adverse event. For the purposes of investigational new drug (IND) safety reporting, “reasonable possibility” means there is evidence to suggest a causal relationship between the drug and the adverse event.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 62 Confidential Information 03-Jun-2014
Unless otherwise noted, categorical data will be presented using counts and percentages, with the number of subjects in the analysis population by treatment group as the denominator for percentages. Percentages will be rounded to one decimal place. Continuous data, unless otherwise noted, will be summarized using the number of observations (n), mean, standard deviation, median, minimum, and maximum. The primary test on PFS, secondary test on OS, and all other statistical tests will be conducted using a 1-sided significance level of 0.10.
9.1.1 Sample Size and Operating Characteristics
The total samples size is approximately 175 subjects (estimated 88 per treatment group). In the event the starting dose of VTX-2337 is reduced (see §9.2.2), the sample size for the trial will be adjusted so that 175 subjects will be treated at the modified starting dose. Subjects who discontinue the study prior to receiving their first dose of IP will be replaced. A dropout rate of approximately 10% over the life of the study is assumed.
The timing of the primary analysis will be event-driven. One hundred thirty-four (134) PFS events are required to detect a hazard ratio (HR) of 0.67 with 85% power at a 1-sided alpha of 0.10. This HR represents a 50% improvement in PFS, which translates to an increase in median PFS from 6 months (control arm) to 9 months (combination arm). It is estimated that a population of 175 evaluable subjects accrued over 18 months will need to be followed for an additional 9 months to provide the requisite number of PFS events.
The analysis of OS will be conducted when all randomized subjects (accrued over 18 months) have been followed for ≥ 12 months following enrollment of the final subject. It is estimated that 112 OS events will be accrued during this time, providing 72.8% power at a 1-sided alpha of 0.10 to detect a HR of 0.70. This HR represents a 30% reduction in the risk of death, and a 42.9% increase in the median OS. Assuming a median OS of 11 months in the control arm, the median OS in the combination arm will be 15.7 months.
9.1.2 Subject Population(s) for Analysis
The analysis populations are:
Intent to Treat (ITT) Population: The ITT population will include all randomized subjects in the study. This population will be used for efficacy analyses. If the randomized treatment arm differs from the actual treatment for a given subject, that subject will be analyzed according to the randomized treatment arm.
Per Protocol (PP) Population: The PP population will include all subjects who have at least one tumor assessment after receiving at least one dose of IP and have no major protocol deviations that could impact efficacy assessments. This population will be defined in detail in the
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 63 Confidential Information 03-Jun-2014
Statistical Analysis Plan (SAP) prior to final database lock and unblinding for the primary analysis.
Safety Population: The safety population will include all subjects who receive at least one dose of IP. This population will be used for safety analyses. If the randomized treatment arm differs from the actual treatment for a given subject, that subject will be analyzed according to the actual treatment arm.
Other analysis populations may be defined, if required, in the detailed SAP.
9.2 Statistical Methods
A detailed SAP will be finalized before the primary database lock and unblinding. This analysis plan may modify what is outlined in the protocol; however, any major modifications of the primary endpoint definition or its analysis will also be reflected in a protocol amendment.
9.2.1 Efficacy 9.2.1.1 Primary Efficacy Endpoint
Review by a central radiologist, blinded to subject treatment assignments and independent from the clinical sites, will assess all tumor responses. The resulting response data will serve as primary clinical efficacy data for the trial. Deaths on study will also contribute to the PFS endpoint. PFS is defined as the duration of time from randomization to time of irPD or death, whichever comes first, or the last tumor assessment date for censored subjects.
The primary efficacy endpoint, PFS, will be summarized and displayed by treatment group using Kaplan-Meier methods (SAS® PROC LIFETEST). Point estimates (25th, 50th, and 75th percentiles) will be provided, along with a 1-sided 90% confidence interval (CI). Treatments will be compared for the ITT population using a stratified log-rank test, with randomization stratification factors included, as the primary analysis. The HR between the 2 study arms, as well as the associated 90% CI, will be presented using Cox proportional hazards regression (SAS® PROC PHREG) controlling for randomization stratification factors. Kaplan-Meier plots will be presented.
The primary analysis will be a stratified log-rank test (using the randomization stratification factors) comparing PFS between the 2 randomized arms in the ITT population.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 64 Confidential Information 03-Jun-2014
9.2.1.2 Secondary Efficacy Endpoint
Secondary efficacy endpoints include:
• Overall survival (OS)
• Tumor response based on irRECIST v1.1[19]:
— Objective response rate (ORR)
— Duration of best response (DOBR)
— Disease control rate (DCR)
— Duration of disease control (DDC)
Overall Survival
OS will be measured from the date of subject randomization until death or the last follow up date for censored subjects. OS will be summarized and analyzed in the same manner as PFS.
Tumor response
For each secondary endpoint involving tumor responses, assessments per the central-radiology review will be presented and analyzed as primary.
The number and percent of subjects achieving objective response (irCR or irPR) will be tabulated for ITT population subjects treated with SOC plus VTX-2337 versus those treated with SOC plus placebo. The number and percent of subjects achieving disease control (irSD, irPR, or irCR) will be tabulated in the same manner. As well, the number and percent of subjects exhibiting each level of best tumor response (irCR, irPR, irSD, irPD, or missing) will be presented by treatment group for the ITT population. Stratified Cochran-Mantel-Haenszel mean scores tests (SAS® PROC FREQ) will be used to compare tumor response rates between the 2 study arms while controlling for randomization stratification factors. In addition, maximum change in TMTB from baseline in ITT population subjects will be presented graphically.
Duration of best response—measured in days—will be defined as the duration of time from the date measurement criteria are first met for irCR, or irPR (if irCR is never met), until the first date that irPD is confirmed by the central radiology review, or death, whichever comes first, or the last tumor assessment date for censored subjects. DOBR will be calculated only for responding subjects (irCR or irPR) as assessed by irRECIST. DOBR will be summarized and displayed by treatment group using Kaplan-Meier methods. Point estimates (25th, 50th, and 75th percentiles) will be provided, along with 1-sided 90% CIs.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 65 Confidential Information 03-Jun-2014
Duration of disease control—measured in days—will be defined as the duration of time from the date measurement criteria are first met for irCR, irPR, or irSD to the first date that irPD is confirmed by the central radiology review, or death, whichever comes first, or the last tumor assessment date for censored subjects. DDC will be calculated only for subjects who achieve disease control (irCR, irPR or irSD) as assessed by irRECIST. DDC will be summarized and displayed in the same manner as DBR.
9.2.1.3 Sensitivity Analysis
Analyses on the PP population will be performed for the primary and the secondary efficacy endpoints and serve as supportive analyses for the ITT analyses.
9.2.2 Safety
AEs, vital signs, ECG, and safety laboratory data (peripheral blood hematology, serum chemistry, and urinalysis) will be presented descriptively. All AEs, vital signs, ECGs, and clinical laboratory abnormalities will be presented. Safety data will be presented in tabular and/or graphical format and summarized descriptively by treatment group and time point, where appropriate. Descriptive statistics will be shown for baseline, scheduled visits, and the change from baseline to these visits, as applicable.
A DSMB of at least three independent members with expertise in the patient population, statistics, and/or clinical research will be appointed to monitor subject safety data while the trial is ongoing. The DSMB will meet at predetermined intervals set forth in the DSMB Charter—approximately every 6 months—to review toxicities and serious and/or unexpected adverse events. The DSMB will primarily evaluate safety data; efficacy data will only be reviewed in the event of a serious safety concern. Minutes for all meetings will be generated.
To address any new or unexpected safety issues, the first DSMB meeting occured after an unblinded statistician confirmed that 6 subjects, who had been randomized to receive VTX-2337, had completed one cycle of therapy. The purpose of this meeting was to evaluate any DLTs or any acute, unexpected, or synergistic toxicities associated with the combination of VTX-2337, platinum, 5-FU, and cetuximab. Results from the initial DSMB evaluation concluded that the study can continue as planned at the dose level of 3.0 mg/m2 and that DLT recording criteria could be lifted.
Refer to §8.1.3 for DLT definition.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 66 Confidential Information 03-Jun-2014
Adverse Events
AEs will be coded using the Medical Dictionary for Regulatory Activities (MedDRA). All AEs will be listed. Treatment-emergent AEs (TEAEs) are those which first occur or increase in severity or relationship to IP after the first dose of IP. AEs with missing date of onset will be considered treatment-emergent. The number and percent of patients reporting TEAEs will be tabulated by system organ class and preferred term and categorized by treatment group. AEs will be further classified by severity and relationship to treatment in tabulations. Tables and/or narratives of any on-study death, or SAE, as well as early withdrawals because of AEs, will be provided. The relationship between drug exposure and adverse events will be evaluated qualitatively.
Electrocardiogram
Descriptive statistics for QRS, QTc, QT and HR will be presented for baseline, End of Treatment visit, and the change from baseline to End of Treatment. The incidence of outliers in absolute QTcF and QTcB intervals (> 450 to ≤ 480, > 480 to ≤ 500, and > 500 msec) and the absolute uncorrected QT intervals (> 500 msec) at End of Treatment, as well as changes from baseline in QTcF and QTcB (> 30 to ≤ 60 and > 60 msec) will be summarized by treatment group.
Laboratory Values
Laboratory test results will be converted to International System of Units (SI) units. Abnormal laboratory results will be graded with the NCI-CTCAE (Version 4.03) standard. Descriptive statistics will be shown for baseline, scheduled visits, and the change from baseline to these visits. Shift summaries of NCI-CTCAE grade from baseline to worst post-baseline result will be provided by treatment group. In addition, selected parameters will be displayed graphically over time by treatment group.
9.2.3 Other Data
Demographics, Baseline Characteristics, and Disposition
Demographic information and baseline characteristics will be summarized for the ITT population. Demographic data will be summarized by treatment group and will include summary statistics for age, age group, race, sex, height, and weight. General medical history data and oncology history data will also be tabulated by treatment group using counts and percentages. Oncology history will include prior anticancer interventions, histological or cytological confirmation of SCCHN, tumor staging according to the TNM Classification of Malignant Tumors, HPV status (for patients with oropharyngeal carcinoma only), prior systemic therapy for SCCHN (Yes or No), and ECOG performance status (0 or 1).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 67 Confidential Information 03-Jun-2014
The disposition of all randomized subjects will be summarized. These data will include the number of subjects enrolled (randomized), receiving study treatment, assigned to each dose group, and prematurely discontinuing from the study and the reason(s) for premature discontinuation.
Extent of Exposure
Dosing data will be summarized by treatment group to include duration of treatment (days), cumulative dose and dose intensity, and number (%) of patients with dose modifications.
Concomitant Medications
Concomitant medications will be presented in data listings and coded using the WHODRUG dictionary. Concomitant medications will be summarized by treatment group and preferred drug names.
Translational Research Assessments
Statistical evaluation of translational research assessments (§4.2.3) will be described in SAP.
9.3 Schedule of Analyses
The primary analysis will be conducted when 134 PFS events have accrued on study. The secondary efficacy analysis (OS) will be conducted approximately 12 months following randomization of the last subject. It is anticipated that approximately 112 OS events will have occurred at the time of the secondary analysis on OS. Two database locks will be scheduled for the 2 analyses, at the time points described above. Additional analyses may be performed and will be outlined in the SAP.
9.4 Termination Criteria
Enrollment in the study will end when at least 175 subjects have been randomized, to provide approximately 88 subjects per treatment group. Subjects who discontinue the study prior to receiving their first dose of IP will be replaced. A dropout rate of approximately 10% over the life of the study is assumed. The end of the trial is defined as the date when the final analysis of the OS endpoint is completed.
9.5 Deviation Reporting
Major protocol deviations will be presented in a listing.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 68 Confidential Information 03-Jun-2014
10.0 REGULATORY, QUALITY, AND ADMINISTRATIVE REQUIREMENTS 10.1 Trial Conduct
This study will be conducted in compliance with the protocol issued by VentiRx Pharmaceuticals and approved by the IRB/IEC and according to FDA regulations, applicable Competent Authorities and Guidelines for Good Clinical Practice (21 CFR §312 and ICH Guidance E6). No deviation from the protocol will be implemented without the prior approval from the study’s sponsor or its representative, as well as review and approval from the IRB/IEC except where it may be necessary to eliminate an immediate hazard to a research subject. In such cases, the deviation will be reported to the IRB/IEC and VentiRx Pharmaceuticals, or their respresentative, as soon as possible.
10.2 Ethical Considerations 10.2.1 Informed Consent
Patients meeting the criteria set forth in the protocol may be offered the opportunity to participate in this study. Candidate subjects or their legal guardians will receive a comprehensive explanation of the study, including the nature and investigational status of the IP, any known previously experienced adverse reactions, alternative therapies available and other factors which are part of obtaining appropriately informed consent. Patients will be given the opportunity to ask questions of qualified personnel who are knowledgeable about the study and provide adequate time to consider whether or not to participate.
Informed consent will be documented with an ICF that has been approved by the institution’s IRB/IEC. The ICF is to be signed and dated by the subject or subject’s legally authorized representative, by the person who conducts the consent process and any additional signatures required by the institution’s IRB/IEC. The original signed ICF will be filed in the subject’s medical record and a copy of the signed ICF will be given to the subject or the subject’s legally authorized representative. The subject’s medical record should contain a notation that written informed consent was obtained and a written description of the consent process.
Any changes to the ICF (e.g., in the event of a protocol amendment that changes the study’s procedures or alters its scope, or if significant new information regarding the safety or efficacy of the investigational drug becomes available) must be reviewed and approved by the IRB/IEC. The revised ICF must be used to re-consent any subject currently enrolled in the study who is affected by the change.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 69 Confidential Information 03-Jun-2014
10.2.2 Institutional Review Board/Ethics Committee Approval
The protocol and all relevant supporting materials, including the IB and Informed Consent Form, must be submitted to the appropriate IRB/IEC for review and approval. A copy of the IRB/IEC’s written approval must be provided to the study’s sponsor or its representative prior to initiation of the study and commencement of the subject screening and enrollment. The IRB/IEC should be informed by the investigator of the study’s progress and provide written documentation of the periodic review and ongoing approval according to IRB/IEC policies.
Any changes in the study protocol, revisions to the ICF, and all unanticipated problems involving risks to human subjects (e.g., SAEs occurring at the clinical site, INDSRs) must be reported promptly to the IRB/IEC and according to institutional and IRB/IEC requirements. Written approval from the IRB/IEC must be obtained prior to implementation of any change(s), if applicable.
10.2.3 Subject Privacy
The investigator, CRO, VentiRx Pharmaceuticals, and representatives of VentiRx Pharmaceuticals shall comply with all applicable local, state and federal privacy laws. The medical records of participating subjects are considered confidential and disclosure to third parties other than those noted below is prohibited.
The medical records of participating study subjects and all data generated as a result of participation in this study are to be available for review upon request by the FDA or other regulatory authorities, VentiRx Pharmaceutics or its representatives, and by the IRB/IEC. The IRB/IEC-approved ICF must clearly indicate that the subject’s medical records will be inspected by said parties and permission for such review is a requirement for study participation.
10.3 Investigator Responsibilities and Requirements
By agreeing to participate in this clinical trial, the Principal Investigator and all subinvestigators agree to perform the study in accordance with all stipulations of the protocol, the FDA Code of Federal Regulations (21 CFR Parts 11, 50, 54, 56 and 312), applicable local regulation(s) and ICH Guidelines for GCP (E6).
Prior to initiation of the study the Principal Investigator must, at minimum, provide VentiRx or its representative with the following documentation:
• Signed clinical trial agreement
• Signed Principal Investigator Protocol Agreement
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 70 Confidential Information 03-Jun-2014
• Signed FDA Form 1572 or equivalent
• Curriculum Vitae of the Principal Investigator
• Current medical license(s) for the Principal Investigator
• Copy of written IRB/IEC approval for the study and informed consent form
• Financial disclosure for the Principal Investigator
The Principal Investigator is responsible for complying with all commitments as delineated in Box 9 of FDA form 1572 and/or local regulations.
10.4 Data Identification, Handling, and Record Keeping 10.4.1 Source Documentation
Adequate and accurate case histories, which record all data and observations relevant to the clinical investigation, should be prepared and maintained for each subject screened or randomized in the study. Such source documentation includes all original documents or medical records regarding the subject’s participation in the study, including medical history, notes from the physician or nurse, the subject’s laboratory reports, imaging studies, electrocardiogram tracings, hospital records and details regarding the distribution of the investigational drug.
10.4.2 Case Report Forms and Electronic Data Capture
The investigator will be provided with access to a secure, web-based system that is compliant with 21 CFR §11 for capturing and reporting all study-related data ( EDC). Such data will be entered into the EDC system by the investigator and site personnel in a timely and accurate manner. The investigator must review all submitted data for accuracy and consistency with the protocol and authorize the data for each subject upon completion.
All required fields on the electronic case report forms (CRFs) must be filled in and 100% of the information collected on CRFs must be verifiable through review of the original source documentation.
10.4.3 Essential Documents
The Principal Investigator and clinical site personnel are responsible for maintaining an organized, comprehensive file of all essential documents required to demonstrate compliance with regulatory requirements. Such documents include, but are not limited to:
• Protocol with all amendments, signed Principal Investigator Protocol Agreement(s) and informed consent form(s)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 71 Confidential Information 03-Jun-2014
• IB, including all updates
• Copy of the signed FDA Form 1572
• CVs and medical licenses for the Principal Investigator and subinvestigators
• IRB/IEC approval of the protocol and amendment(s), informed consent form(s) and any other study-related materials
• IRB/IEC membership list or Letter of Assurance
• Subject Screening and Enrollment Log, which may be obtained from EDC
• IRB/IEC submissions of SAEs that have occurred at the institution and of INDSRs provided by the study’s sponsor
• Laboratory certifications and reference ranges
• Significant correspondence from VentiRx Pharmaceuticals or CRO
• Other documents as required by local regulatory authorities
These files must be available for inspection by VentiRx Pharmaceuticals, their representatives, the IRB/IEC, or regulatory authorities at any time.
10.4.4 Record Retention
All study related documentation noted in §10.4.1, §10.4.2 and §10.4.3 above must be maintained in accordance with FDA and local regulations. For sites in the US, as described in 21 CFR §312.62, the investigator will retain all such study records for a period of 2 years after marketing approval is received for VTX-2337, or for 2 years after all clinical and product development of VTX-2337 is discontinued. Investigators should not destroy any records relating to this study without prior approval from VentiRx Pharmaceuticals.
10.5 Quality Control and Quality Assurance 10.5.1 Site Training and Monitoring Procedures
Prior to the initiation of the study, personnel from the sponsor or its representatives will meet with the investigator and clinical staff to review and discuss the protocol, the investigational drug, study procedures, drug accountability, adverse event reporting, ICH/GCP guidelines, CRF completion guidelines, record keeping and administrative requirements, monitoring requirements, and the ability of the site to adequately conduct the protocol. During the course of the study, representatives from the sponsor will provide additional study-specific training to site staff upon request by the investigator, in response to a change in key clinical site staff, or if
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 72 Confidential Information 03-Jun-2014
issues with study conduct or GCP compliance are observed during the course of routine monitoring visits.
A representative from VentiRx Pharmaceuticals will visit the clinical site periodically to monitor adherence to the protocol, to review and retrieve study-related data, and/or documents. The frequency of monitoring visits depends on the rate of enrollment at the site and the investigator will permit the sponsor’s representative to monitor the study as frequently as the sponsor deems necessary to determine that protocol adherence and data collection are acceptable. The monitor will be permitted full access to subjects’ complete medical records. CRFs will be reviewed and compared to the subject’s case history to ensure the accuracy of the reported data and that key data are collected and recorded as specified by the protocol. Other study records, such as essential regulatory documents, subject screening log, and drug disposition logs will also be inspected.
10.5.2 Data Management Procedures
VentiRx Pharmaceuticals or its designee will prepare guidelines for database setup, data review, quality control, and database lock at the conclusion of the study—including procedures for electronic edit checks. CRF Completion Guidelines will be prepared to guide the data entry activities completed by the sites. The database will be validated following established procedures. Electronic databases that hold subject study data will conform to 21 CFR §11 requirements.
10.5.3 Auditing Procedures
VentiRx Pharmaceuticals and the applicable Competent Authorities maintain the right to conduct audit(s) at the clinical site.
11.0 SUPPLEMENTS Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 73 Confidential Information 03-Jun-2014
11.1 ECOG Performance Status Assessment
Grade ECOG 0 Fully active, able to carry on all pre-disease performance without restriction 1 Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or
sedentary nature, e.g., light house work, office work 2 Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about
more than 50% of waking hours. 3 Capable of only limited selfcare, confined to bed or chair more than 50% of waking hours. 4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or chair. 5 Dead
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 74 Confidential Information 03-Jun-2014
11.2 Baseline Tumor Evaluation and Categorization: RECIST v1.1 11.2.1 Categorization of Tumors
All tumor lesions will be categorized at baseline as either one of the following:
• Measurable: lesions that can be accurately measured in at least one dimension (longest diameter to be recorded) as ≥ 10 mm for soft tissue lesions and ≥ 15 mm in short axis for lymph nodes with CT or MRI scan. All tumor measurements must be recorded in decimal fractions of centimeters.
• Non-measurable: All other lesions (or sites of disease), including small lesions (longest diameter < 10 mm or pathological lymph nodes with ≥ 10 to < 15 mm short axis), are considered non-measurable disease. Leptomeningeal disease, ascites, pleural/pericardial effusions, lymphangitis cutis/pulmonitis, inflammatory breast disease, and abdominal/pelvic masses (identified by physical exam and not CT or MRI) are considered as non-measurable.
11.2.2 Special considerations regarding lesion measurability
Bone lesions: Lytic bone lesions or mixed lytic-blastic lesions, with identifiable soft tissue components, that can be evaluated by CT or MRI can be considered as measurable lesions if the soft tissue component meets the definition of measurability described above. Blastic bone lesions are non-measurable.
Cystic lesions that meet the criteria for radiographically defined simple cysts should not be considered as malignant lesions (neither measurable nor non-measurable) since they are, by definition, simple cysts. “Cystic lesions” thought to represent cystic metastases can be considered as measurable lesions, if they meet the definition of measurability described above. However, if non-cystic lesions are present in the same subject, these are preferred for selection as target lesions.
Lesions with prior local treatment (e.g., tumor lesions that are situated in a previously irradiated area) will not be considered measureable unless progression is documented or a biopsy is obtained to confirm persistence at least 90 days following completion of radiation therapy.
11.2.3 Methods of Assessment
The same method of assessment and the same technique should be used to characterize each identified and reported lesion at baseline and during follow-up.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 75 Confidential Information 03-Jun-2014
All measurements should be taken and recorded in metric notation using a ruler. All baseline evaluations should be performed as closely as possible to the beginning of treatment and never more than 28 days before the beginning of treatment.
Clinical lesions: Superficial clinical lesions measured by caliper or ruler will not be used to assess tumor response in this study.
Conventional CT and MRI: CT slice thickness should be ≤ 5 mm. MRI is also acceptable in certain situations (e.g., for body scans), but NOT lung.
Use of MRI remains a complex issue. MRI has excellent contrast, special and temporal resolution; however, there are many image acquisition variables involved in MRI, which greatly impact image quality, lesions conspicuity, and measurement. Furthermore, the availability of MRI is variable globally. As with CT, if an MRI is performed, the technical specifications of the scanning sequences used should be optimized for the evaluation of the type and site of disease. Furthermore, as with CT, the modality used at follow-up should be the same as was used at baseline and the lesions should be measured/assessed on the same pulse sequence parameters for all scanners, body parts, and diseases. Ideally, subsequent image acquisitions should use the same type of scanner and follow the baseline imaging protocol as closely as possible. If possible, body scans should be performed with breath-hold scanning techniques.
PET-CT: PET-CT is an acceptable means of imaging if the CT is of diagnostic quality and meets with the requirements in the Imaging Manual.
FDG-PET: FDG-PET will not be used to assess tumor response in this study.
Ultrasound: Ultrasound will not be used to assess tumor response in this study.
Endoscopy, Laparoscopy: Endoscopy, Laparoscopy will not be used to assess tumor response in this study.
Cytology, Histology: In rare cases, these techniques can be used to differentiate between PR and CR.
It is mandatory to obtain cytological confirmation of the neoplastic origin of any effusion that appears or worsens during treatment when measurable disease has met criteria for response or stable disease. This confirmation is necessary to differentiate response or stable disease versus progressive disease, as an effusion may be a side effect of the treatment.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 76 Confidential Information 03-Jun-2014
11.2.4 Baseline documentation of “Target” and “Non-Target” lesions
Target lesions: All measurable lesions, up to a maximum of 2 lesions per organ and 5 lesions in total—representative of all involved organs—should be identified as target lesions and recorded and measured at baseline. Target lesions should be selected on the basis of their size (lesions with the longest diameter), be representative of all involved organs and in addition should be those that lend themselves to reproducible repeated measurements. It may be the case that, on occasion, the largest lesion does not lend itself to reproducible measurement, in which circumstance the next largest lesion which can be reproducibly measured should be selected.
The sum of the diameters (long axis for non-nodal lesions, short axis for nodal lesions) of all target lesions will be calculated and reported as the baseline sum of diameters (baseline TMTB). If lymph nodes are to be included in the sum, then only the short axis is added into the sum. The baseline TMTB will be used as reference to further characterize any objective tumor regression in the measurable dimension of the disease.
Non-target lesions: All other lesions (or sites of disease), including any measurable lesions over and above the 5 target lesions, should be identified as non-target lesions and should also be recorded at baseline. Measurements of these lesions are not required, but the presence, absence, or in rare cases unequivocal progression of each should be noted throughout follow-up.
Malignant lymph nodes: To be considered pathologically enlarged and measurable, a lymph node must be ≥ 15 mm in short axis when assessed by CT scan (CT scan slice thickness ≤ 5 mm). At baseline and in follow-up, only the short axis will be measured and followed.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 77 Confidential Information 03-Jun-2014
11.3 Response Assessment: immune-related RECIST (irRECIST)
As previously noted, this study will assess tumor response with an immune-related modification of RECIST v1.1 (referred to as irRECIST). The response criteria from standard RECIST v1.1 has, therefore, not been included in this protocol.
Determination of response via irRECIST will take into consideration all target and non-target lesions.
11.3.1 Total Measured Tumor Burden
TMTB is established at baseline as the sum of the longest diameters (SOD)—the shortest axis should be used for lymph nodes—of all target lesions (≤ 2 lesions per organ, ≤ 5 lesions total). At each subsequent TA, the SOD of new, measurable lesions (≥ 10 mm [lymph nodes ≥ 15 mm
in shortest diameter]; ≤ 2 new lesions per organ, ≤ 5 new lesions total) is added to the SOD of the target lesions to provide the updated TMTB:
TMTB = SOD target lesions + SOD new, measurable lesions
If there are more than 2 new lesions per organ or more than 5 new lesions total, the lesions added to the TMTB should be selected on the basis of their size (i.e., lesions with the longest diameter should be selected).
Percentage changes in TMTB at each TA describe the size and growth kinetics of both old and new, measurable lesions as they appear. At each TA, the response in TMTB is defined as follows:
• Complete Response (irCR): Complete disappearance of all target and new, measurable lesions, with the exceptions of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
11.3.2 Response in Non-Target Lesions
The presence of non-target lesions is established at baseline; at each TA, the presence of any new, non-measurable lesions is assessed. The presence of new, non-measurable lesions will rule out an overall response of irCR. An increase in the size or number of new, non-measurable
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 78 Confidential Information 03-Jun-2014
lesions does not necessarily imply an overall response of irPD; if these lesions become measurable (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; up to 2 new lesions per organ, total 5 new lesions) at a subsequent TA, their measurement will, at that point, start to contribute to the TMTB.
The response in non-target lesions is defined as follows:
• Complete Response (irCR): Complete disappearance of all non-target lesions
• non-irCR/non-irPD: Non-target lesions do not meet the criteria for irCR or irPD
• Progressive Disease (irPD): Unequivocal increase in the number or size of non-target lesions. To achieve unequivocal progression of non-target lesions, there must be a substantial worsening of non-target disease of a magnitude that, according to the treating physician, warrants a change in anticancer therapy
NOTE: Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing lesions) should be considered irSD and treatment may continue until the next scheduled assessment.
11.3.3 Overall Response
The overall response (OR) according to irRECIST is derived from the responses in TMTB as well as the presence of any non-target lesions as follows:
• Complete Response (irCR): Complete disappearance of all lesions (whether measurable or not); lymph nodes must decrease to < 10 mm in shortest dimension
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
The immune-related best overall response (irBOR) is the best irRECIST OR over the study as a whole, recorded between the date of first dose until the last TA prior to subsequent anticancer therapy for individual subjects. An assessment of disease progression at or before week 12 (unconfirmed irPD at week 12) will not preclude an irBOR of irCR, irPR, or irSD. Conversely, an assessment of irPD at or after Week 12 (confirmed irPD at week 12), will preclude a subsequent irBOR of irCR, irPR, or irSD. However, any post-progression clinical activity in subjects with irBOR of irPD may be summarized for exploratory purposes.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 79 Confidential Information 03-Jun-2014
Table 9: Best Overall Response (irBOR)
Target Lesions Baseline (Index) and New
Measurable Lesions Non-Target Lesions*
irRC Overall Response Total Measurable Tumor
Burden (TMTB) Baseline Lesions Unequivocal New Lesions
irCR irCR No irCR
irCR irSD No irPR
irPR irCR or irSD No irPR
irSD irCR or irSD No irSD
irPD Any Yes or No irPD
Any Unequivocal Progression Yes or No irPD
Any Any Yes irPD
*Any increase in the size or number of non-measurable lesions does not necessarily imply an overall response of irPD. If new lesions become measureable (≥ 10 mm) at a subsequent TA, their measurement will at that point start to contribute to the TMTB. To achieve unequivocal progression of non-target lesions, there must be an overall level of substantial worsening in non-target disease that is of a magnitude that the treating physician would feel it is important to change therapy. Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing locations) should be considered irSD and treatment may continue until the next schedule assessment.
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 80 Confidential Information 03-Jun-2014
11.4 Chemotherapy Dose Delay Algorithm
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 81 Confidential Information 03-Jun-2014
11.5 List of CYP3A4 Inhibitors and/or Inducers
Table 10 includes example CYP3A4 inhibitors and inducers. CYP3A4 inducers and inhibitors should be administered with caution and, if possible, alternatives that do not affect CYP3A4 should be administered instead (§7.6).
Table 10: Examples of CYP3A4 Inhibitors and Inducers
Inhibitors Inducers
Amiodarone Indinavir Barbiturates
Aprepitant/Fosaprepitant Itraconazole Carbamazepine
Chloramphenicol Ketoconazole Efavirenz
Cimetidine Mibefradil Glucocorticoids
Ciprofloxacin Mifepristone Modafinil
Clarithromycin Nefazodone Nevirapine
Delavirdine Nelfinavir Oxcarbazepine
Diethyl-dithiocarbamate Norfloxacin Phenobarbital
Diltiazem Norfluoxetine Phenytoin
Erythromycin Ritonavir Pioglitazone
Fluconazole Saquinavir Rifabutin
Fluvoxamine Star fruit Rifampin
Gestodene Telithromycin St. John’s wort
Grapefruit juice Verapamil Troglitazone
Imatinib Voriconazole --
Note that aprepitant/fosaprepitant is a CYP3A4 inhibitor recommended for use in managing CINV (§7.6.1). Given the specific pharmacology of aprepitant/fosaprepitant and VTX-2337 (e.g., short half life), as well as the number of intervening days between their administration, there is no contraindication to employing aprepitant or fosaprepitant for prevention of nausea and vomiting.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 82 Confidential Information 03-Jun-2014
11.6 List of Abbreviations
Abbreviation or Term Definition/Explanation
5-FU Fluorouracil
ADCC Antiobody-dependent cellular cytotoxicity
AE Adverse Event
ALT (SGPT) Alanine aminotransferase (Serum Glutamic Pyruvic Transaminase)
ANC Absolute neutrophil count
API Active pharmaceutical ingredient
AST (SGOT) Aspartate aminotransferase (Serum Glutamic Oxaloacetic Transaminase)
AUC Area under the curve
BOR Best overall response
BP Blood pressure
C Celsius
CBC Complete blood count
CI Confidence interval
CR Complete response
CRF Case report form
CRO Contract research organization
CRS Cytokine release syndrome
CRx Concomitant medication
CT Computed tomography
DCR Disease control rate
DDC Duration of disease control
DLT Dose-limiting toxicity
DOBR Duration of best response
DSMB Data safety monitoring board
EC50 Half maximal effective concentration
ECG Electrocardiogram
ECOG Eastern cooperative oncology group
EGFR Epidermal growth factor receptor
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 83 Confidential Information 03-Jun-2014
Abbreviation or Term Definition/Explanation
F Fahrenheit
FDA Food and Drug Administration
GCP Good Clinical Practice
GFR Glomerular Filtration Rate
GOG Gynecologic oncology group
HNC Head and neck carncioma
HPV Human papilloma virus
HR Heart rate
HR Hazard ration
IB Investigator’s Brochure
ICF Informed consent form
ICH International Conference on Harmonization
IEC Independent ethics committee
IND Investigational new drug
INDSR Investigational new drug safety report
IP Investigational product
IRB Institutional Review Board
irRECIST immune-related response evaluation criteria in solid tumors
IV Intravenous
IXRS Interactive voice/web response system
M Meter
mDC Myeloid Dendritic Cell
MedDRA Medical dictionary for regulatory activities
Mg Milligram
Min minute
mL Milliliter
MRI Magnetic resonance imaging
NK Natural killer
Nm Nano molar
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 84 Confidential Information 03-Jun-2014
Abbreviation or Term Definition/Explanation
ORR Objective response rate
OS Overall survival
PBMC Peripheral mononuclear cells
PD Pharmacodynamic
PD Progressive disease
PE Physical examination
pH Hydrogen ion concentration
PFS Progression free survival
PK Pharmacokinetic
PLD Pegylated liposomal doxorubicin
PR Partial response
RECIST Response evaluation criteria in solid tumors
RR Respiration rate
SAE Serious Adverse Event
SD Stable disease
SGOT (AST) Serum Glutamic Oxaloacetic Transaminase
SGPT (ALT) Serum Glutamic Pyruvic Transaminase
SC Subcutaneous
SI International system of units
SOC Standard-of-care
SOD Sum of diameters
SUSAR Suspected unexpected serious adverse reactions
t½ Terminal elimination phase half-life
T Temperature
t1/2 Mean half life
TA Tumor assessment
TEAE Treatment emergent adverse events
TLR Toll-like Receptor
TMTB Total measured tumor burden
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 85 Confidential Information 03-Jun-2014
Abbreviation or Term Definition/Explanation
ULN Upper Limit of Normal
µM micro molar
US United States
WBC White blood cell
WHO-DRUG World Health Organization-Drug Reference List
Remainder of page intentionally left blank.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 86 Confidential Information 03-Jun-2014
12.0 LITERATURE AND REFERENCES
1. Smith, E.M., et al., Tobacco and alcohol use increases the risk of both HPV-associated and HPV-independent head and neck cancers. Cancer Causes Control, 2010. 21:1369-1378.
2. Carvalho, A.L., et al., Trends in incidence and prognosis for head and neck cancer in the United States: a site-specific analysis of the SEER database. Int J Cancer, 2005. 114(5): p. 806-16.
3. Davies, L. and H.G. Welch, Epidemiology of head and neck cancer in the United States. Otolaryngol Head Neck Surg, 2006. 135(3): p. 451-7.
4. Curado, M.P. and M. Hashibe, Recent changes in the epidemiology of head and neck cancer. Curr Opin Oncol, 2009. 21(3): p. 194-200.
5. Hobbs, C.G., et al., Human papillomavirus and head and neck cancer: a systematic review and meta-analysis. Clin Otolaryngol, 2006. 31(4): p. 259-66.
6. Dobrossy, L., Epidemiology of head and neck cancer: magnitude of the problem. Cancer Metastasis Rev, 2005. 24(1): p. 9-17.
7. Argiris, A., et al., Head and neck cancer. Lancet, 2008. 371(9625): p. 1695-709.
8. Lango, M.N., Multimodal treatment for head and neck cancer. Surg Clin North Am, 2009. 89(1): p. 43-52, viii.
9. Ferrari, D., et al., A review on the treatment of relapsed/metastatic head and neck cancer. Expert Opin Pharmacother, 2009. 10(16): p. 2625-32.
10. Specenier, P.M. and J.B. Vermorken, Recurrent head and neck cancer: current treatment and future prospects. Expert Rev Anticancer Ther, 2008. 8(3): p. 375-91.
11. Ferlito, A., et al., Incidence and sites of distant metastases from head and neck cancer. ORL J Otorhinolaryngol Relat Spec, 2001. 63(4): p. 202-7.
12. Vermorken, J.B., et al., Platinum-Based chemotherapy plus Cetuximab in Head and Neck Cancer. N Engl J Med, 2008;359:1116-27.
13. Rivera, F., et al., Cetuximab in metastatic or recurrent head and neck cancer: the EXTREME trial. Expert Rev Anticancer Ther, 2009. 9(10): p. 1421-8.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Incorporated 87 Confidential Information 03-Jun-2014
14. Boshoff, C. and M. Posner, Targeting EGFR in head and neck cancer: a decade of progress. Nat Clin Pract Oncol, 2009. 6(3): p. 123.
15. Lim, C., et al., VTX-2337, a Selective TLR8 Ligand, Enhances Cetuximab-mediated ADCC in Head and Neck Cancer. J Immunother, 2011. 34(9): p. 693.
16. Specenier, P.M. and J.B. Vermorken, Current concepts for the management of head and neck cancer: chemotherapy. Oral Oncol, 2009. 45(4-5): p. 409-15.
17. Lu, H., et al., VTX-2337 is a novel TLR8 agonist that activates NK cells and augments ADCC. Clin Cancer Res, 2012. 18(2):499-509
18. Stephenson, R., et al., TLR8 stimulation enhances cetuximab-mediated natural killer cell lysis of head and neck cancer cells and dendritic cell cross-priming of EGFR-specific CD8+ T cells. Cancer Immunol Immunother. May 2013.
19. Northfelt, D., et al., A Phase 1 Dose-Finding Study of the Novel Toll-like Receptor 8 Agonist VTX-2337 in Adult Subjects with Advanced Solid Tumors or Lymphoma. Clin Cancer Res, Accepted for Publication.
20. Chow, L., et al., Phase 1 Clinical Trial of VTX-2337, a Small Molecule Toll-Like Receptor 8 (TLR8) Agonist in Combination with Cetuximab in Patients with Recurrent or Metastatic Squamous Cell Carconomas of the Head and Neck (SCCHN). Multidisciplinary Head and Neck Symposium; 2014 Feb 20–22; Scottsdale, AZ, USA.
21. Monk, B., et al., VTX-2337, a TLR8 Agonist, Plus Chemotherapy in Recurrent Ovarian Cancer: Preclinical and Phase 1 Data by the Gynecologic Oncology Group. American Society of Clinical Oncology, Annual Meeting; 2013 June 3–7; Chicago, IL, USA.
22. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebbé C, Maio M, Binder M, Bohnsack O, Nichol G, Humphrey R, Hodi FS. Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria. Clin Cancer Res 2009, 15(23):7412–20
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
CLINICAL PROTOCOL VRXP-A202
Active8
Title: A Randomized, Double-Blind, Placebo-Controlled Study of ChemotherapyPlus Cetuximab in Combination with VTX-2337 in Patients with Recurrent orMetastatic Squamous Cell Carcinoma of the Head and Neck
Version: Original Issue: 31-May-2013
Amendment No.: Version 1.1 14-Jun-2013
Version 2.0 03-Jun-2014 Version 3.0 25-Jan-2016
Sponsor: VentiRx Pharmaceuticals, Incorporated1191 Second AvenueSuite 1105Seattle, WA 98101(206) 689-2259
Study Chairs: Ezra Cohen, MD1 and Robert Ferris, MD, PhD2
Contract Research Organization:
Approved by:
PRA International 4130 Parklake Avenue Suite 400Raleigh, NC 27612
James Kyle Bryan, MD DateVentiRx Pharmaceuticals
CONFIDENTIALThis document contains proprietary and confidential information of VentiRx Pharmaceuticals, Inc. Acceptance of this document constitutes agreement by the recipient that no previously unpublished information contained herein will be published or disclosed without the prior written approval of VentiRx Pharmaceuticals, Inc., except disclosure to study personnel and appropriate Institutional Review Boards (IRB)/Independent Ethics Committees (IEC) under the condition that the personnel have agreed to keep this information confidential. The foregoing shall not apply to disclosure required by governmental regulations or laws; however, VentiRx Pharmaceuticals, Inc. shall be promptly notified of any such disclosure.
1 Associate Professor of Medicine, University of Chicago Comprehensive Cancer Center2 Professor of Otolaryngology, Cancer Immunology Program, University of Pittsburgh Cancer Institute
VentiRx Pharmaceuticals Incorporated 1Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
VentiRx Pharmaceuticals Protocol No. VRXP-A202
PRINCIPAL INVESTIGATORPROTOCOL AGREEMENT
A RANDOMIZED, DOUBLE-BLIND, PLACEBO-CONTROLLED STUDY OF CHEMOTHERAPY PLUS CETUXIMAB IN COMBINATION WITH VTX 2337 IN
PATIENTS WITH RECURRENT OR METASTATIC SQUAMOUS CELLCARCINOMA OF THE HEAD AND NECK
Version Date: 25-Jan-2016
I attest that I have read this protocol and the Investigator Brochure (IB) for VTX-2337. I agree to conduct the trial in accordance with the provisions herein, U.S. Food and Drug Administration (FDA) regulations, applicable Competent Authorities, International Conference on Harmonization (ICH) guidelines for Good Clinical Practice (GCP), state and local regulations and the requirements of the IRB/IEC.
I will provide copies of the current protocol and access to all information provided by VentiRx Pharmaceuticals, Inc. to the study personnel under my supervision. I will discuss this material with them to ensure that they are fully informed about the investigational drug and the study protocol.
Principal Investigator Signature Date
Principal Investigator Printed Name
VentiRx Pharmaceuticals Incorporated 2Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
TABLE OF CONTENTS1.0 STUDY SYNOPSIS ...........................................................................................................52.0 BACKGROUND ..............................................................................................................10
2.1 Investigational Agent .............................................................................................112.2 Nonclinical Data ....................................................................................................112.3 Clinical Data ..........................................................................................................132.4 Risks/Benefits ........................................................................................................162.5 Dose Rationale .......................................................................................................172.6 Population ..............................................................................................................18
3.0 TRIAL RATIONALE AND OBJECTIVES ..................................................................183.1 Rationale ................................................................................................................183.2 Objectives ..............................................................................................................19
4.0 TRIAL DESIGN.............................................................................................................. 194.1 Study Design/Type .................................................................................................194.2 Endpoints ...............................................................................................................204.3 Procedures to Minimize Bias .................................................................................214.4 Maintenance of Blinding Procedures .....................................................................214.5 Trial Treatment ......................................................................................................224.6 Duration .................................................................................................................234.7 Discontinuation ......................................................................................................24
5.0 SELECTION OF SUBJECTS ........................................................................................245.1 Inclusion Criteria ...................................................................................................255.2 Exclusion Criteria ..................................................................................................26
6.0 CLINICAL TRIAL PROCESSES AND PROCEDURES ...........................................276.1 Subject Screening and Randomization (Day -14 to -1) .........................................276.2 Treatment Period ....................................................................................................296.3 End of Treatment ...................................................................................................326.4 Follow Up Period ...................................................................................................336.5 Early Treatment Discontinuation ...........................................................................356.6 Assessments ...........................................................................................................356.7 Monitoring for Subject Compliance ......................................................................43
7.0 TREATMENT ..................................................................................................................447.1 Packaging, Labeling and Storage ...........................................................................447.2 Preparation of Investigational Product ...................................................................44
VentiRx Pharmaceuticals Incorporated 3Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
7.3 Administration of Investigational Product and Study Treatment(s) ......................447.4 Dose Modifications ................................................................................................477.5 Emergency Unblinding ..........................................................................................557.6 Concomitant Medications and Supportive Care ....................................................557.7 Investigational Product Accountability ..................................................................58
8.0 ADVERSE EVENTS .......................................................................................................588.1 Definitions..............................................................................................................588.2 Reporting Requirements ........................................................................................608.3 Criteria for Determining Adverse Event Severity .................................................618.4 Criteria for Determining Adverse Event Expectedness .........................................628.5 Criteria for Determining Adverse Event Causality ................................................628.6 Expedited Reporting of Serious Adverse Events ...................................................63
9.0 STATISTICAL PLAN .....................................................................................................639.1 Statistical Considerations .......................................................................................639.2 Statistical Methods .................................................................................................659.3 Schedule of Analyses .............................................................................................699.4 Termination Criteria...............................................................................................699.5 Deviation Reporting ...............................................................................................70
10.0 REGULATORY, QUALITY, AND ADMINISTRATIVE REQUIREMENTS .........7010.1 Trial Conduct .........................................................................................................7010.2 Ethical Considerations ...........................................................................................7010.3 Investigator Responsibilities and Requirements ....................................................7110.4 Data Identification, Handling, and Record Keeping ..............................................7210.5 Quality Control and Quality Assurance .................................................................73
11.0 SUPPLEMENTS ............................................................................................................. 7511.1 ECOG Performance Status Assessment .................................................................7511.2 Baseline Tumor Evaluation and Categorization: RECIST v1.1 ............................7511.3 Response Assessment: immune-related RECIST (irRECIST) ..............................7811.4 Response Assessment: RECIST v1.1 ....................................................................8111.5 Chemotherapy Dose Delay Algorithm ...................................................................8311.6 List of CYP3A4 Inhibitors and/or Inducers ...........................................................8411.7 List of Abbreviations .............................................................................................85
12.0 LITERATURE AND REFERENCES ...........................................................................89
VentiRx Pharmaceuticals Incorporated 4Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
1.0 STUDY SYNOPSIS
Protocol Number VRXP-A202
Protocol Title A Randomized, Double-Blind, Placebo-Controlled Study of Chemotherapy Plus Cetuximab in Combination with VTX-2337 in Patients with Recurrent or Metastatic Squamous Cell Carcinoma of the Head and Neck
Investigational Phase II
Investigational Product VTX-2337, a subcutaneously-administered Toll-like receptor 8 agonist
Study Sites Approximately 60 sites in North America
Study Duration Enrollment Period: Approximately 18 monthsDuration of Study: Approximately 36 months; following completion of accrual, all subjects will be followed for approximately 12 months
Study Population Adults who have not previously received systemic treatment for recurrent or metastatic squamous cell carcinoma of the head and neck
Study Design Randomized, double-blind, placebo-controlled, parallel group
Primary Objectives To compare the progression-free survival of subjects treated with cisplatin or carboplatin + fluorouracil (5-FU) + cetuximab combined with VTX-2337 to those treated with cisplatin or carboplatin + 5-FU + cetuximab alone (standard-of-care; SOC).
Secondary Objectives To compare the safety of subjects treated with SOC in combination with VTX-2337 to those treated with SOC alone.To compare the overall survival between the two treatment groups.To compare the best objective response rate (ORR), duration of best response (DOBR), disease control rate (DCR), and duration of disease control (DDC) between the two treatment groups.
Sample Size n=175
VentiRx Pharmaceuticals Incorporated 5Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Inclusion Criteria Summary
1. Ability and willingness to provide written informed consent and to complywith the study’s visit and assessment schedule
2. Prior documentation of histologically or cytologically confirmed squamouscell carcinoma of the head and neck
3. Locoregionally recurrent or metastatic SCCHN that has not previously beentreated with systemic therapy for recurrent or metastatic disease
4. At least one measurable lesion as defined by RECIST v1.1 (§11.1) onscreening computed tomography (CT) or magnetic resonance imaging (MRI)
5. 18 years of age or older6. ECOG performance status of 0 or 17. Acceptable bone marrow, renal, and hepatic function based upon screening
lab tests8. Willingness to use medically acceptable contraception throughout the study
period and for 4 weeks after the final administration of IP9. For female subjects with reproductive potential: a negative serum pregnancy
test
VentiRx Pharmaceuticals Incorporated 6Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Exclusion Criteria Summary
1. Disease which is amenable to curative local therapy2. Nasopharyngeal, salivary gland, lip, or sinonasal carcinoma3. Major surgery or irradiation within 4 weeks of randomization4. Prior systemic anti-cancer therapy, unless administered for localized SCCHN
and completed at least 6 months prior to disease recurrence5. Treatment with an investigational agent within 30 days of randomization6. Treatment with oral or parenteral corticosteroids within 2 weeks of
randomization or a requirement for chronic systemic immunosuppressive therapy for any reason
7. Prior serious infusion reaction to cetuximab8. Treatment with an immunotherapy within 30 days of randomization9. Known brain metastases, unless stable for at least 28 days prior to
randomization10. Active autoimmune disease, defined as any autoimmune condition currently
requiring therapy (e.g., systemic lupus erythematosus, multiple sclerosis, inflammatory bowel disease, rheumatoid arthritis)
11. Known infection with HIV12. Clinically significant cardiac disease (e.g., congestive heart failure, unstable
or uncontrolled angina, myocardial infarction) within 6 months of randomization
13. Pregnant or breast-feeding females14. History of another primary malignancy, with the exception of the following:
• curatively resected non-melanoma skin cancer• curatively treated in situ cervical cancer• other malignancy curatively treated with no evidence of disease and
no anticancer therapy administered for at least 3 years prior to randomization, with the exception of adjuvant hormonal therapy for breast cancer
15. Any other condition or circumstance that could interfere with adherence tothe study’s procedures or requirements, or otherwise compromise the study’s objectives
VentiRx Pharmaceuticals Incorporated 7Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Study Drug Dose and Administration
VTX-2337 or placebo (investigational product; IP) will be administered as a subcutaneous injection on Day 8 and Day 15 of a 21-day cycle at a dose level of 3.0 mg/m2 for 6 cycles, followed by dosing on Days 8 and 22 of a 28-day cycle for cycles 7 and beyond. IP will be administered until disease progression.Standard-of-Care will consist of the following:
1. Cisplatin (100 mg/m2) OR carboplatin (AUC 5 mg/mL/min) administered as anIV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles.
2. 5-FU (1000 mg/m2/day) administered as a continuous IV infusion on Days 1–4of a 21-day cycle for a maximum of 6 cycles.
3. Cetuximab (initial dose: 400 mg/m2; remaining doses: 250 mg/m2) administeredweekly until disease progression.
On days when investigational product and cetuximab are both dosed, IP will be administered first, followed by the cetuximab infusion.
Study Overview This is a randomized, double-blind, placebo-controlled, parallel group study to evaluate the safety and efficacy of VTX-2337 in combination with cisplatin or carboplatin, 5-FU and cetuximab in prolonging the progression-free survival in subjects with recurrent or metastatic squamous cell carcinoma of the head and neck.Subjects will be screened for eligibility and qualified subjects will be randomized 1:1 to 1 of 2 treatment groups:
− SOC + VTX-2337− SOC + placebo
Tumor assessments will be by CT or MRI starting at Week 12 (± 3 days), then at Week 18 (± 3 days) and every 8 weeks (± 7 days) thereafter. Response will be evaluated by immune-related RECIST criteria (irRECIST) and confirmed by an independent radiologist.Upon independent confirmation of disease progression, active participation in the study is complete and subjects will undergo the End of Treatment evaluations.Subjects will be followed for survival until ~12 months after the last subject is randomized.Adverse events and safety will be evaluated throughout the study by an independent Data Safety Monitoring Board (DSMB). The DSMB will also conduct an assessment of the safety and tolerability of the starting dose.
Primary Outcome Measures
Progression-free survival will be assessed by serial imaging studies (CT or MRI) performed at baseline (Screening), Week 12 (± 3 days), Week 18 (± 3 days) and every 8 weeks (± 7 days) thereafter.Tumor response as evaluated by irRECIST.All tumor responses for the primary endpoint will be reviewed and confirmed by a central, independent radiologist. Whenever medically feasible and appropriate, suspected disease progression events should be confirmed by central review prior to completing the End of Treatment assessments and initiating new anti-cancer therapy.
VentiRx Pharmaceuticals Incorporated 8Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Secondary Outcome Measures
Safety will be assessed by physician or subject report of adverse events.Overall survival will be determined by report of subject vital status.PFS will be assessed by RECIST v1.1 and evaluated by a central, independent radiologist. PFS will also be assessed by irRECIST and evaluated by the investigators.Objective response rate, duration of best response, disease control rate, and duration of disease control will be assessed by irRECIST, and by RECIST v1.1 and evaluated by a central, independent radiologist.
Statistical Considerations Randomization of all subjects will be stratified by prior systemic therapy for SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy as assigned by the investigator at the time of randomization (cisplatin or carboplatin).Sample size: n=175 subjects.Power, alpha and hazard ratio assumptions: see full protocol.
VentiRx Pharmaceuticals Incorporated 9Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
2.0 BACKGROUND
Head and neck carcinomas (HNC) are the fifth most common cancer in the world, with increasing incidence.[1, 2] In the United States, 40,000 to 50,000 new cases are diagnosed and approximately 12,000 deaths due to this cause occur yearly.[2] HNCs describe malignancies of the upper aerodigestive tract which include squamous cell carcinomas of the oral cavity, nasopharynx, pharynx and larynx. While tobacco and alcohol use are the most common risk factors for HNCs, Epstein-Barr virus and human papilloma virus (HPV) may also play a role in the development of carcinomas of the nasopharynx and squamous cell carcinomas of the oropharynx, respectively.[1–6]
The majority of squamous cell carcinoma of the head and neck (SCCHN) cases (up to 75%) are diagnosed in its late stages (stages III or IV).[7, 8] Metastatic and recurrent SCCHN that is no longer amenable to local surgical/radiation therapy causes substantial morbidity and high mortality, with a median progression free survival (PFS) of ≤ 6 months due to the lack of effective therapeutic options.[9, 10, 11] Recurrent or metastatic disease has traditionally been managed with cytotoxic chemotherapies such as methotrexate, organoplatinum compounds, fluorouracil (5-FU), or taxanes—either alone or in combination. More recently, cetuximab (Erbitux®), the IgG1 monoclonal antibody which targets epidermal growth factor receptor (EGFR) was approved by FDA and Health Canada for use in combination with radiation therapy for the initial treatment of locally or regionally advanced SCCHN and by FDA for use as monotherapy in patients with recurrent or metastatic SCCHN who have progressed after platinum-based therapy and in combination with platinum-based therapy with 5-FU in patients with recurrent or metastatic SCCHN. Approval was based on clinical benefit and tolerability in the phase 3 setting.[12, 13] Namely, the addition of cetuximab to first-line platinum-based therapy with 5-FU resulted in an improvement of median overall survival (OS) from of10.1 months compared to 7.4 months for patients treated with platinum/5-FU alone. As morethan 90% of SCCHNs express the EGFR, targeting EGFR and its signaling pathway significantly advanced the treatment of SCCHN.[14] However, in this difficult-to-treat SCCHN population, the overall prognosis remains poor and the observed responses of 36% and a median time to progression of 5.6 months for cetuximab in combination with platinum and 5-FU are not ideal.[12, 13] Therefore, combinations that enhance response and provide clinical benefit, withoutsignificantly increasing toxicity, are still urgently needed.
One approach to enhance the efficacy of treatment with cetuximab plus chemotherapy in SCCHN is to add an immunomodulatory agent that would promote an anti-tumor immune response. Ideally, this agent would enhance both the effects of cetuximab (e.g., by augmentingantibody-dependent cellular cytotoxicity; ADCC) and chemotherapy (e.g., by modulating thetumor microenvironment and increasing T cell responses to antigenic debris generated by tumoricidal activity). One such candidate is VTX-2337, a modulator of Toll-like receptor 8
VentiRx Pharmaceuticals Incorporated 10Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
(TLR8). Activation of TLR8 enhances natural killer (NK) cells, myeloid-derived dendritic dendritic cells (mDC), and monocytes. VTX-2337 has demonstrated enhanced killing of SCCHN cells in combination with cetuximab, and synergistic activity with chemotherapy.[15]
The current study tests the hypothesis that the addition of VTX-2337 to the cetuximab plus platinum/5-FU regimen in locally recurrent and/or metastatic SCCHN patients will provide clinical benefit and will be reasonably well tolerated.
2.1 Investigational Agent
VTX-2337 is comprised of an active pharmaceutical ingredient (API) formulated at neutral pH in Captisol® (a cyclodextrin-based solubilizing agent). The API of VTX-2337 is VTX-378: a novel, small, organic molecule TLR8 agonist with a molecular weight of 458.6. VTX-2337 a lyophilized cake is supplied in sterile, single-use vials and is administered via subcutaneous injection.
The selectivity of this compound has been assessed in peripheral mononuclear cells (PBMC) and in cells engineered to express only a single TLR. In both PBMC and cell transfectants, VTX-2337 is highly selective for TLR8 with an EC50 of approximately 70 nM. VTX-2337 shows minimal activity for TLR7 (with an EC50 of approximately 3 μM), but does not stimulate other TLRs.[16]
Placebo contains Captisol and citric acid, the same excipient ingredients of the VTX-2337 formulation, but does not include the API VTX-378.
2.2 Nonclinical Data
Nonclinical studies have included in vitro and in vivo assessments of the pharmacologic, pharmacokinetic (PK), metabolism and toxicologic characteristics of VTX-2337. Extensive information regarding the pre-clinical evaluation of VTX-2337 may be found in the Investigator’s Brochure (IB).
2.2.1 Pharmacokinetics and Pharmacology
The PK and pharmacology of VTX-2337 have been broadly evaluated in non-human primates (cynomologus monkeys). The compound shows linear pharmacokinetics over a wide dose range, with a half-life (t1/2) of approximately 2–4 hours. VTX-2337 elicits the production of multiple inflammatory mediators—chemokines (e.g., MCP-1, MIP-1β), cytokines (e.g., IL-6, IL-1, TNFα, IL 12), acute phase proteins and shed cell surface antigens—which are consistent with activation of the innate immune system and can be readily measured in plasma. A clear pharmacokinetic- pharmacodynamic (PK/PD) relationship is observed for many of these inflammatory markers.
VentiRx Pharmaceuticals Incorporated 11Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Refer to §2.3 for information regarding PK/PD data in patients.
2.2.2 In Vitro ADCC and NK Observations
To characterize the potential for VTX-2337 to modulate immune function beyond the characterization in PD studies, immunophenotyping of peripheral blood and NK cell cytotoxic activity was assessed. These in vivo studies demonstrated that administration of VTX-2337 results in transient changes in blood cell populations consistent with cellular activation of neutrophils, NK cells, and T cells and may result in the transient extravasation of these latter cell populations from the blood compartment.[16]
In addition, VTX-2337 stimulates the production of cytokines from mDC, monocytes, and NK cells in vitro.[17] VTX-2337 stimulates ADCC when used in combination with a variety of monoclonal antibodies of the IgG1 subclass including rituximab and traztuzumab.[17] More recently, in collaboration with Dr. Robert Ferris at the University of Pittsburgh, it was demonstrated that VTX-2337 increases the cetuximab-mediated killing of SCCHN targets in anNK-dependent manner.[18] The TLR8 and NK-dependent enhancement of ADCC occurs insamples from patients of all three FcRγ3a genotypes, including those with the allele encoding the homozygous F/F variant that is associated with lower affinity for the Fc receptor.
In addition, the stimulation of mDC and monocytes concurrent with cetuximab administration was tested to determine the promotion of development of EGFR-specific T cells via a mechanism referred to as ‘cross-priming’. Using a mixed culture model in vitro, tetramer analysis (using a molecular reagent that detects human leucocyte antigen-specific, EGFR peptide specific CD8+ T cells) demonstrated that VTX-2337 stimulates cross-priming and increases the number of EGFR-specific CD8+ T cells following cetuximab treatment.
Taken together, the ability of VTX-2337 to stimulate the production of inflammatory cytokines (including IL-1, IL-18, TNFα, IL-12, and IFNg), the activation and stimulation of NK cells and ADCC, and the activation of the antigen processing and presentation of mDC and monocytes provide a strong rationale that this TLR8 agonist may enhance the activity of cetuximab in clinical studies.
2.2.3 Toxicology
In conjunction with FDA requirements, standard toxicology studies were performed with the aim of inducing and identifying drug-related toxicities. The clinically relevant toxicities observed in these studies were mechanistically based; that is, attributed to activation of the innate immune system via TLR8. The most frequent of these included transient constitutional symptoms consistent with the influenza-like response frequently seen with immunomodulatory agents. As noted in §2.3, these flu-like symptoms identified in preclinical toxicology studies have
VentiRx Pharmaceuticals Incorporated 12Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
subsequently been observed in clinical trials of VTX-2337, and include pyrexia, chills, myalgia, and fatigue.
As detailed in the VTX-2337 IB, organ-based toxicity was also observed in preclinical toxicology studies. Organ-based toxicities have not been observed in any clinical trial of VTX-2337 to date, and are not described herein.
2.3 Clinical Data2.3.1 Phase I Solid Tumor: VTX-2337 Monotherapy (VRXP-A101)
VTX-2337 was first evaluated clinically as a stand-alone agent in a Phase I standard dose- escalation study to assess the safety, tolerability and biological activity of the compound in late- stage cancer patients. At doses ranging from 0.1–3.9 mg/m2, VTX-2337 was well tolerated overall, with the predominant adverse events being transient grade 1 or 2 fever, chills, flu-like symptoms, nausea and vomiting, anorexia, and injection site reaction. No significant drug-related hematologic, gastrointestinal, neurologic or cardiac toxicities were observed. At the highest dose evaluated, 3.9 mg/m2 (cohort 8; n=8) a single subject experienced a dose-limiting toxicity (DLT) of grade 3 hypotension associated with grade 2 cytokine release syndrome (CRS), from which the subject recovered completely. Accordingly, the maximum dose evaluated in this study(3.9 mg/m2) was adequately well tolerated. Overall, VTX-2337 was found to be well toleratedwhen administered subcutaneously weekly for 3 weeks of a 4-week cycle.
The PK of VTX-2337 were assessed in all subjects (n=33) and demonstrated dose-dependent exposure. With subcutaneous administration, VTX-2337 was rapidly absorbed into systemic circulation as well as rapidly cleared, with mean Tmax ranging from 0.5–0.7 hours and t½ ranging from 1.7–7.1 hours. Peak plasma levels and total systemic exposure were generally dose- proportional.
The biological activity (cytokines, chemokines and other inflammatory markers, including those indicative of TLR8 activation) of VTX-2337 was assessed in all subjects. Biological activity of VTX-2337 was shown to be dose dependent, with the robust induction of multiple inflammatory markers in all subjects receiving doses ≥ 2.0 mg/m2.
Clinical responses were assessed by response evaluation criteria in solid tumors (RECIST) at8 weeks. No complete responses (CR) or partial responses (PR) were seen in the study, but approximately 25% of subjects had evidence of stable disease (SD) at 8 weeks. It should be noted that VTX-2337 is anticipated to have stand-alone biological activity, but is not anticipated to induce a CR or PR as a single agent.
VentiRx Pharmaceuticals Incorporated 13Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
The doses selected from this study to be used in combination studies were 2.5, 3.0, and3.5 mg/m2. All of these doses are expected to be biologically active based on the biomarker data from VRXP-A101.[19]
2.3.2 Phase 1 SCCHN: VTX-2337 with Cetuximab (VRXP-A103)
This ongoing, single-center phase 1b protocol at Seattle Cancer Care Alliance (Seattle, WA) is being conducted as an Investigator Sponsored Trial, with Laura Chow, MD as theSponsor-Investigator.
VRXP-A103 assesses the safety and tolerability of VTX-2337 in combination with cetuximab. Cetuximab is administered weekly and VTX-2337 is administered weekly for three weeks of a four-week cycle. Three dose levels of VTX-2337 are being evaluated in a standard dose- escalation schema: 2.5 mg/m2, 3.0 mg/m2, and 3.5 mg/m2.
Enrollment is complete (n=13), and one subject remains on study. The study regimen has been safe and adequately tolerated. There have been no dose-limiting toxicities; no serious, unexpected drug-related adverse events; and no evidence of synergistic toxicities between cetuximab and VTX-2337. Clinical tolerability data indicate that long-term dosing at 3.0 mg/m2
will be better tolerated than 3.5 mg/m2.
Translational medicine results are available from the first twelve subjects who received VTX-2337 (2.5, 3.0, or 3.5 mg/m2) in combination with cetuximab. As expected based on data from the Phase 1 VRXP-A101 study, serum biomarkers consistent with TLR8 activation were readily measured at both dose levels. In addition, ex vivo analysis of NK cells collected pre-dose and 24 hours after dosing demonstrate NK cell activation. Given the proposed mechanism of VTX-2337 enhancing ADCC with cetuximab in an NK-dependent manner, these data provide important correlative information and suggest the doses of 2.5, 3.0, and 3.5 mg/m2 are biologically active from a pharmacologic perspective.
Based on preliminary efficacy data, 10 of the 13 subjects have been eligible for evaluation of tumor response: 2 subjects achieved a partial response, 4 subjects experienced disease stabilization, and 4 subjects had disease progression. One subject has not yet had a response assessment, and 2 subjects discontinued the study prematurely and were unevaluable for response assessment.[20]
2.3.3 Phase 1 Ovarian Cancer (VTX-2337 with Chemotherapy)
Study VRXP-A102 (GOG-9925) was a phase I study conducted in collaboration with Gynecologic Oncology Group (GOG). The study separately assessed two treatment regimens containing VTX-2337 in women with recurrent ovarian cancer. Regimen 1 evaluated pegylated
VentiRx Pharmaceuticals Incorporated 14Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
liposomal doxorubicin (PLD, Doxil®; 40 mg/m2) plus VTX-2337 at three dose levels: 2.5 mg/m2, 3.0 mg/m2, and 3.5 mg/m2. Regimen 2 consisted of weekly paclitaxel (80 mg/m2) plus VTX-2337 (3.0 mg/m2).
In both of the regimens evaluated, there were no dose-limiting toxicities; no serious, unexpecteddrug-related adverse events; and no evidence of synergistic toxicities between PLD plus VTX-2337 or paclitaxel plus VTX-2337. PD data confirm the biological activity of VTX-2337 in both regimens at all dose levels, with biomarker responses indicative of TLR8 stimulation and immune activation.
Twenty subjects were treated: 13 on Regimen 1 and 7 on Regimen 2. On Regimen 1, one subject enrolled based on biochemical evidence of recurrent disease achieved a complete biochemical response, 1 subject with non-measureable disease achieved a complete response, 7 subjects had stable disease, and 3 subjects had progressive disease (including 1 subject with non-target disease [biochemical recurrence only] who had biochemical progression). One subject did not complete the first cycle and was not evaluable for efficacy. On Regimen 2, one subject experienced a partial response, 2 subjects experienced disease stabilization, and 4 of the 7 subjects had disease progression.
Two of the 7 subjects enrolled in Regimen 1 at the 3.5 mg/m2 dose level of VTX-2337 withdrew from treatment or had a dose reduction due to grade 2 or 3 drug-related events (e.g., chills, fatigue, nausea, vomiting, fever). These events suggest that long-term dosing of VTX 2337 at 3.5 mg/m2 is not clinically optimal. Based on this information, and the adequate biological activity of VTX-2337 at 2.5 and 3.0 mg/m2, the selection of 3.0 mg/m2 of VTX-2337 was recommended as the optimal dose for the randomized, Phase 2 study.[21]
2.3.4 Phase 2 Ovarian Cancer (VTX-2337 with Chemotherapy)
GOG-3003 is a randomized, placebo-controlled, ongoing Phase 2 study designed to evaluate VTX-2337 (3.0 mg/m2) in combination with PLD in patients with recurrent or persistent epithelial ovarian, fallopian tube, or primary peritoneal cancer. The study will evaluate the overall survival of VTX-2337 in combination with PLD compared to PLD alone in approximately 290 subjects. PFS, response rate, and safety of the combination are key secondary endpoints. This multicenter study is being conducted in approximately 100 clinical sites in the United States, in collaboration with the GOG. Enrollment in this study is complete.
VentiRx Pharmaceuticals Incorporated 15Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
2.4 Risks/Benefits2.4.1 Potential Risks
In previously published trials of platinum, 5-FU, and cetuximab the most common adverse events (AE) overall were skin reactions, headache, diarrhea, infection, and nausea. The most common grade 3 or 4 adverse events were anemia, neutropenia, and thrombocytopenia. Less commonly, dosing with cetuximab may result in a serious infusion reaction requiring medical intervention and immediate, permanent discontinuation with cetuximab.[12]
The most common AE associated with VTX-2337 when administered as a single-agent is injection site reaction. Most often these have been grade 1 or 2; however, grade 3 injection site reactions have been reported. The most common systemic drug-related adverse events are transient grade 1 or 2 chills, flu-like symptoms, fever, nausea, and vomiting; these transient symptoms typically last < 48 hours. Less commonly, dosing with VTX-2337 may result in CRS, which is most likely to be grade 1 or 2, but grade 3 reactions have been reported. Similarly, the most common AEs reported in patients receiving VTX-2337 in combination with cetuximab were grade 1 and 2 injection site reactions, flu-like symptoms, nausea, fatigue, vomiting, cough, malaise, and dyspnea.
Potential long-term clinical effects of VTX-2337 are unknown and cannot be reliably predicted. However, several subjects in clinical trials have received up to 8 cycles (24 individual weekly doses) of VTX-2337 without unanticipated problems. Investigators will be informed of anynewly-identified risks associated with VTX-2337, if they occur.
Although the combinations of VTX-2337 plus chemotherapy (PLD, paclitaxel) and VTX-2337 plus cetuximab did not demonstrate any dose-limiting or synergistic toxicities, VTX-2337 has not previously been studied in combination with platinum plus 5-FU plus cetuximab. While no new, unexpected, or synergistic toxicities are anticipated, the safety of this combination will be carefully evaluated by an independent data safety monitoring board (DSMB) (see also §9.2.2).
Overall, at the dose level to be administered in this clinical trial (3.0 mg/m2), VTX-2337 treatment-related toxicities are expected to be transient and consistent with those events commonly associated with an activated immune response. This includes symptoms of chills, fever, flu-like syndrome, headache, nausea, vomiting, and local injection site reaction.
2.4.2 Potential Benefits
The efficacy of VTX-2337 has not been formally evaluated in clinical trials to date. However, exploratory data from study VRXP-A101 showed 25% of the 33 subjects enrolled had disease stabilization at 8 weeks. In addition, preliminary data from a phase 1b study of VTX-2337 in
VentiRx Pharmaceuticals Incorporated 16Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
combination with cetuximab in patients with advanced SCCHN (n=13) included 2 subjects who experienced a partial response, 4 subjects who experienced disease stabilization; 2 subjects were not evaluable and 1 subject has not yet had a tumor evaluation. Furthermore, a phase 1b study of VTX-2337 with chemotherapy in women with recurrent, platinum-resistant ovarian cancer (n=20) included 2 subjects who experienced complete response (one of which was a biochemical CR), 1 subject who experienced a partial response, and 10 subjects who experienced disease stabilization (2–8 months).
The current study of VTX-2337 described herein is a multi-dose study to assess the safety, tolerability and efficacy of the investigational drug in combination with cisplatin or carboplatin,5-FU, and cetuximab. The clinical efficacy of this combination has not yet been evaluated;however, the addition of VTX-2337 to the standard-of-care (SOC) treatment regimen may be more effective than SOC alone.
Participating subjects may also benefit from the personal satisfaction of participating in an investigative process that will contribute information regarding the investigational product (IP) that may help patients afflicted with SCCHN.
2.5 Dose Rationale
The selection of the starting dose for this study, as well as the Phase 2 study in ovarian cancer (3.0 mg/m2) was based on data from the initial phase 1 study of VTX-2337 used as a single agent, and data from the two Phase 1b studies combining VTX-2337 with cetuximab in SCCHN patients and with PLD or paclitaxel in ovarian cancer patients, respectively. These studies showed that VTX-2337 is biologically active in some subjects at doses as low as 0.4 mg/m2
based on biomarker data as previously described. Biological activity of VTX-2337 was shown to be dose dependent. At VTX-2337 doses ≥ 2.0 mg/m2, nearly all subjects evaluated have a robust biological response, as indicated by the induction of multiple inflammatory markers consistent with activation of TLR8. In study VRXP-A103, where cellular responses were assessed, VTX-2337 in combination with cetuximab at doses ≥ 2.5 mg/m2 (the lowest dose tested) was associated with cellular responses including NK cell activation.
While no DLTs have been observed at 3.5 mg/m2 in either the cetuximab or chemotherapy combination studies, treating investigators have reported reduced tolerability at 3.5 mg/m2
compared to 3.0 mg/m2. This has included higher fevers, more intense flu-like symptoms, and more persistent injection site reactions. Based on its clear biological activity and improved long- term tolerability, as well as the lack of dose-limiting or synergistic toxicities, 3.0 mg/m2 has been selected as the appropriate dose for Phase 2 studies of VTX-2337 in combination with chemotherapy.
VentiRx Pharmaceuticals Incorporated 17Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
2.6 Population
This study will be conducted in adult subjects with recurrent or metastatic SCCHN who have not previously received systemic treatment for their recurrent or metastatic disease. Eligible subjects will have an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1 and adequate hematologic, renal, and hepatic function. This study will not include subjects with disease which is amenable to curative local therapy or who had disease recurrence within 6 months of completion of systemic therapy for localized SCCHN.
Refer to §5.0 for specific eligibility requirements for subjects.
3.0 TRIAL RATIONALE AND OBJECTIVES3.1 Rationale
Recurrent or metastatic SCCHN is an aggressive disease with few treatment options with proven clinical benefit. The use of the EGFR-specific monoclonal antibody cetuximab in combination with platinum and 5-FU based chemotherapy has demonstrated clinical benefit in these patients. Still, the response rate (30-40%), delay in disease progression (overall PFS of approximately 6 months) and OS (approximately 11-12 months in this treated population) leave room for considerable improvement. Ideally, an agent could be added to this regimen that would provide additive or synergistic clinical benefit without dramatically increasing the toxicity of this drug combination. In this regard, an immunomodulatory agent that increases the activity of cetuximab and/or the chemotherapy backbone would be potentially beneficial.
VTX-2337 is a small molecule agonist of TLR8 that stimulates specific immune cell populations including mDC, monocytes, and NK cells. In a variety of cell culture based and animal studies, VTX-2337 has been shown to enhance ADCC in the context of a variety of IgG1-isotype monoclonal antibodies including cetuximab. The enhancement of ADCC occurs across all FcRg3a genotypes—including those associated with lower affinity to FcR and associated lower clinical responses in patients. Via the stimulation of various antigen presenting cells, VTX-2337 enhances the generation of tumor-antigen specific CD8+ T cells and has been found to enhance the tumoricidal activity of certain chemotherapy regimens. In addition, VTX-2337 stimulates the production of a variety of inflammatory cytokines and chemokines that would be expected to modulate the tumor microenvironment. These functions of VTX-2337 are consistent with the role of its receptor—TLR8—as a sentinel of viral infection and the expression of a ‘danger’ signal to rid the host of an unwanted intruder.
VTX-2337 has been evaluated as a single-agent in cancer patients (n=33) to determine the biological activity and safety profile of this novel compound. VTX-2337 has also been evaluated in several combination studies with cetuximab (n=13), PLD (n=13), and paclitaxel (n=7) to
VentiRx Pharmaceuticals Incorporated 18Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
address the safety and activity of this agent in combination with SOC anticancer regimens. Collectively, these data provide a rationale for continued study of VTX-2337 at the selected dose in larger, randomized clinical trials to determine if this compound provides clinical benefit.
As of yet, the anti-tumor effects of VTX-2337 in combination with platinum-based therapy with5-FU and cetuximab have not been evaluated. However, as VTX-2337 may enhance therapeutic responses to platinum-5-FU chemotherapy with cetuximab; this combination is a promising combination that should be explored for its potential for improved anti-tumor effects in this patient population.
3.2 Objectives
The purpose of this study is to compare the safety and efficacy of SOC in combination with VTX-2337 to those treated with SOC plus placebo in subjects with recurrent or metastatic SCCHN. Efficacy objectives include comparing the PFS, OS, objective response rate (ORR), duration of best response (DOBR), disease control rate (DCR), and duration of disease control (DDC) of the two treatment groups. The PD of VTX-2337 will also be evaluated.
4.0 TRIAL DESIGN4.1 Study Design/Type
This is a randomized, double-blind, placebo-controlled, parallel-group study. The study consists of screening (≤ 14 days1), initial treatment (cycles 1–6), subsequent treatment (cycles 7+), and long-term follow-up. Following the screening period, qualified subjects will be randomized in a 1:1 ratio to receive SOC plus placebo or SOC plus VTX-2337. Randomization of all subjects will be stratified by receipt of prior systemic therapy of SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy as assigned by the investigator at the time of randomization (cisplatin or carboplatin).
Subjects will then be administered cisplatin or carboplatin—as assigned by the investigator prior to randomization—5-FU, cetuximab, and IP (i.e., VTX-2337 or placebo) on pre-specified daysof a 21-day cycle for 6 cycles (§6.0). Thereafter, subjects will continue on study for cycles 7+ fordosing of weekly cetuximab and biweekly IP in 28-day cycles.
Subjects will be evaluated for PFS according to immune-related Response Evaluation Criteria In Solid Tumors (irRECIST; §6.6.1.2) at Week 12 (± 3 days), Week 18 (± 3 days), and every 8 weeks (± 7 days) thereafter. Treatment will be discontinued for subjects withindependently-confirmed radiographic disease progression. Upon discontinuation of treatment,subjects will complete the End of Treatment visit and will be followed for survival.
1 Baseline imaging may be performed within 28 days of randomization.
VentiRx Pharmaceuticals Incorporated 19Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Rand
omiza
tion
Dise
ase
Prog
ress
ion
Active8 VTX-2337
Figure 1: Study Schema
Screening
Screening< 14 Days
SOC +VTX-2337
SOC +Placebo
Initial Treatment6 Cycles (18 Weeks)
Cetuximab +VTX-2337
Cetuximab +Placebo
Subsequent TreatmentCycles 7+
Survival Follow-Up
Follow Up
4.2 Endpoints4.2.1 Primary Endpoint(s)
The primary endpoint of the study is to compare the PFS of patients with recurrent or metastatic SCCHN treated with VTX-2337 plus SOC versus patients treated with SOC alone using irRECIST evaluated by independent radiology review.
4.2.2 Secondary Endpoint(s)
The secondary endpoints of the study are to compare the following between the two treatment groups:
• Safety as measured by adverse events, including clinically significant changes in physicalexamination, peripheral blood hematology, serum chemistry, urinalysis, and ECG.
• The OS of patients with recurrent or metastatic SCCHN.
• The ORR, DOBR, DCR, and DDC of patients with recurrent or metastatic SCCHN usingirRECIST evaluated by independent radiology review.
• The ORR, DOBR, DCR, and DDC of patients with recurrent or metastatic SCCHN usingRECIST v1.1 evaluated by independent radiology review.
• PFS assessed by RECIST v1.1 and evaluated by independent radiology review.
• PFS assessed by irRECIST and evaluated by investigators.
VentiRx Pharmaceuticals Incorporated 20Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
4.2.3 Exploratory Endpoint(s)
The exploratory endpoints of this study are as follows:
• To compare genetic polymorphisms that may impact the response of patients to a TLR8agonist or to cetuximab between the two treatment groups.
• To compare immune biomarker response as measured by a multiplexed panel ofcytokines, chemokines, and inflammatory markers between the two treatment groups.
• To compare the effect of immune cell subsets within the tumor on response to treatment and/or clinical outcome, as measured by immunohistochemistry in primary tumor tissuebetween the two treatment groups.
• To assess the PK of VTX-2337.
4.3 Procedures to Minimize Bias
The study design and methods were selected to minimize bias. This is a randomized, double- blind, placebo-controlled study.
All subjects will receive SOC treatment; in addition, subjects will be randomly assigned in a 1:1 ratio to one of two treatment arms: SOC + VTX-2337 or SOC + placebo. To ensure that both known and unknown confounding factors are evenly distributed between treatment groups randomization of all subjects will be stratified by prior systemic therapy for SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy, as assigned by the investigator at the time of randomization (cisplatin or carboplatin). Neither the investigators nor the subjects know to which treatment group a subject is assigned.
The labeling, packaging, and distribution of VTX-2337 and placebo will be identical so that the clinical site personnel remain blinded to study treatment. Placebo will be utilized to ensure that subjects, investigators, and all other study personnel will remain blinded to the study treatment.
In order to minimize potential bias and variability from individual radiology reviewers, radiologic assessment of tumor response will be performed via central radiology review. The central reviewers are blinded to study treatment and are independent from the clinical sites.
4.4 Maintenance of Blinding Procedures
All clinical, regulatory, and safety personnel at the contract research organization (CRO) and sponsor, as well as all investigators and clinical site staff, will remain blinded to the study treatment assignment. Members of the data safety monitoring board (DSMB) may be unblinded; an unblinded statistician, independent from the project team, will provide support to the DSMB.
VentiRx Pharmaceuticals Incorporated 21Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Additionally, individuals with access to the randomization schema and IP kit assignments will remain separate from the study personnel responsible for day-to-day operations and evaluation of the clinical data. Refer to §7.5 for emergency unblinding procedures.
4.5 Trial Treatment
Subjects randomized in the study will be administered all of the following:
• IP (i.e., VTX-2337 or placebo)
• Cetuximab
• Cisplatin or carboplatin (as assigned by the investigator)
Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent should be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject.
• Fluorouracil (5-FU)
When cetuximab is administered on the same day as chemotherapy, cetuximab administration will be completed ≥ 1 hour prior to administration of platinum and 5-FU. When cetuximab is administered on the same day as IP, the dose of IP will be given prior to cetuximab.
Please refer to §7.0 for additional information regarding subject treatment procedures.
4.5.1 Investigational Product Treatment
Subjects will receive IP at a dose of 3.0 mg/m2 (see also §9.2.2) given as a subcutaneous injection on Days 8 and 15 of a 21-day cycle for up to 6 cycles. Following the 6th cycle, subjects will continue to receive IP on Days 8 and 22 of a 28-day cycle until disease progression. (§7.3.1)
4.5.2 Cetuximab Treatment
On Cycle 1 Day 1, subjects will receive an initial cetuximab dose of 400 mg/m2 given as a 2- hour intravenous (IV) infusion1. This will be followed by weekly cetuximab doses of 250 mg/m2
given as a 1-hour IV infusion1. Weekly treatment with cetuximab will continue until disease progression. (§7.3.2)
Please refer to the cetuximab label for additional information.
1 The duration of infusion may be adjusted according to institutional standards.
VentiRx Pharmaceuticals Incorporated 22Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
4.5.3 Platinum Treatment
The platinum therapy (cisplatin or carboplatin) is assigned to each subject at the discretion of the investigator. Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent must be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject. Reasonable efforts should be made to keep the subject on the platinum therapy originally assigned; however, the platinum therapy may be changed if clinically necessary. (§7.3.3)
Cisplatin Treatment
Subjects will receive 100 mg/m2 of cisplatin as a 1-hour IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles1. Cisplatin administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the cisplatin label for additional information.
Carboplatin Treatment
Subjects will receive carboplatin at an AUC of 5 mg/mL/min as a 1-hour IV infusion on Day 1 of a 21-day cycle for a maximum of 6 cycles1. The carboplatin dose will be based upon the subject’s Creatinine Clearance (CrCl) in mL/min as estimated by the Cockroft-Gault Formula. The Calvert formula will be used for carboplatin dosing:
Total Dose (mg) = (target AUC) x (CrCl + 25)
Carboplatin administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the carboplatin label for additional information.
4.5.4 5-FU Treatment
Subjects will receive a continuous IV infusion of 5-FU at a dose of 1000 mg/m2/day on Days 1–4 of a 21-day cycle for a maximum of 6 cycles. 5-FU administration should begin ≥ 1 hour following completion of cetuximab administration. Please refer to the 5-FU label for additional information.
4.6 Duration
The enrollment period of the study is expected to be approximately 18 months, followed by a~12-month follow up period.
1 The duration of infusion may be adjusted according to institutional standards.
VentiRx Pharmaceuticals Incorporated 23Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
The duration of participation will vary among individual subjects due to factors such as disease progression and time of enrollment. After providing written informed consent, subjects will be screened for eligibility within 14 days of randomization (28 days for imaging) according to the procedures outlined in §6.1. Eligible subjects will be randomized into the study and will receive treatment as described in §6.2 and §7.0. Subjects will receive therapy until independently- confirmed disease progression per irRECIST. Thereafter, subjects will be followed long-term for survival.
4.7 Discontinuation
Enrollment in the study will end when approximately 175 subjects have been randomized and have received at least one dose of IP. The sponsor may terminate enrollment in the study at any time for any reason.
Whenever possible, enrolled subjects should complete the study per protocol. However, individual subjects may withdraw from the study prematurely at any time, (e.g., subject decides to discontinue participation due to an adverse event, whether or not related to IP). Subjects who are noncompliant with the study’s requirements may also be removed from the study at any time by the investigator or study sponsor. Regardless of reason for discontinuing the study prematurely, the End of Treatment evaluations should be completed and the subject should be followed for survival, whenever feasible.
Please refer to §6.5 for early discontinuation of individual subjects.
5.0 SELECTION OF SUBJECTS
This study will enroll adult male and female subjects with recurrent or metastatic SCCHN who have not previously received systemic treatment for their recurrent or metastatic SCCHN. All patients considered for enrollment and the reason(s) any screened subject is determined to be ineligible, must be documented. Written informed consent with an IRB/IEC-approved Informed Consent Form (ICF) must be obtained from all subjects prior to undergoing any study-specific procedures, including the discontinuation of any medication(s).
Subjects must meet all of the following eligibility criteria at the time of randomization.
VentiRx Pharmaceuticals Incorporated 24Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
5.1 Inclusion Criteria
1) Ability and willingness to provide written informed consent and to comply withthe study’s visit and assessment schedule
2) Prior documentation of histologically or cytologically confirmed squamous cellcarcinoma of the head and neck
Patients with squamous cell carcinoma of an unknown primary are eligible provided they previously received treatment for their locoregional head and neck cancer
3) Locoregionally recurrent or metastatic SCCHN that has not previously beentreated with systemic therapy for recurrent or metastatic disease
4) At least one measurable lesion as defined by RECIST v1.1 (§11.2) on screeningcomputed tomography (CT) or magnetic resonance imaging (MRI)
5) 18 years of age or older
6) ECOG performance status of 0 or 1
7) Acceptable bone marrow, renal, and hepatic function based upon screening labtests as demonstrated by the following:
− White blood cell (WBC) count > 2,500 cells/Μl
− Absolute neutrophil count (ANC) > 1,500 cells/μL
− Platelet count ≥ 100,000 cells/μL
− Hemoglobin ≥ 9 g/dL
− Creatinine ≤ ULNORCreatinine Clearance ≥ 60 mL/min
− Total bilirubin ≤ 2.0 x ULN
− SGOT (AST), SGPT (ALT) ≤ 2.5 x ULN or
≤ 5 x ULN in presence of liver metastases
− Potassium ≥ LLN
8) Willingness to use medically acceptable contraception throughout the studyperiod and for 4 weeks after the final administration of IP
9) For female subjects with reproductive potential: a negative serum pregnancy test
VentiRx Pharmaceuticals Incorporated 25Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
5.2 Exclusion Criteria
1) Disease which is amenable to curative local therapy
2) Nasopharyngeal, salivary gland, lip, or sinonasal carcinoma
3) Major surgery or irradiation within 4 weeks of randomization
4) Prior systemic anti-cancer therapy, unless administered for localized SCCHN andcompleted at least 6 months prior to disease recurrence
5) Treatment with an investigational agent within 30 days of randomization
6) Treatment with oral or parenteral corticosteroids within 2 weeks of randomizationor a requirement for chronic systemic immunosuppressive therapy for any reason
7) Prior serious infusion reaction to cetuximab
8) Treatment with an immunotherapy within 30 days of randomization
9) Known brain metastases, unless stable for at least 28 days prior to randomization
10) Active autoimmune disease, defined as any autoimmune condition currentlyrequiring therapy (e.g., systemic lupus erythematosus, multiple sclerosis, inflammatory bowel disease, rheumatoid arthritis)
11) Known infection with HIV
12) Clinically significant cardiac disease (e.g., congestive heart failure, unstable oruncontrolled angina, myocardial infarction) within 6 months of randomization
13) Pregnant or breast-feeding females
14) History of another primary malignancy, with the exception of the following:
− curatively resected non-melanoma skin cancer
− curatively treated in situ cervical cancer
− other malignancy curatively treated with no evidence of disease and noanticancer therapy administered for at least 3 years prior to randomization, with the exception of adjuvant hormonal therapy for breast cancer
15) Any other condition or circumstance that could interfere with adherence to thestudy’s procedures or requirements, or otherwise compromise the study’s objectives
VentiRx Pharmaceuticals Incorporated 26Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
6.0 CLINICAL TRIAL PROCESSES AND PROCEDURES
The schedules of study visits, procedures and assessments are in Table 1.
Subjects will receive study treatment, as described in §7.0. Please refer to §6.5 for requirements for individual subjects who discontinue study treatment prematurely. Unscheduled evaluations may be done at the discretion of the investigator as needed to assess the subject’s clinical status. All scheduled visits and procedures must be conducted at the study site of the Principal Investigator as indicated on the FDA Form 1572.
The imaging technique used for each subject (CT or MRI) is at the discretion of the investigator, but the same technique must be used for each individual subject throughout the study. Imaging should not be delayed in case of missed doses or dose delays.
All study-required laboratory evaluations must be performed by the central laboratories using the provided kits.
6.1 Subject Screening and Randomization (Day -14 to -1)6.1.1 Screening Procedures
Subjects with recurrent or metastatic SCCHN may be screened for this study. Prior to the initiation of screening procedures, informed consent will be obtained from each subject as described in §10.2.1.
Upon completion of the informed consent process, sites will register the subject in the interactive voice/web response system (IXRS); IXRS will assign a unique screening number to each subject. The screening number will be comprised of the three-digit site number followed by a three-digit, sequential number (e.g., 123901, 123902). Upon randomization, a unique randomization number will be assigned by IXRS; the randomization number will be used as the subject number for the duration of the study.
The following procedures are required for screening and may be done at any time in the 14 days prior to randomization, unless otherwise specified:
• Complete medical history, including
— Concomitant medications and history of prior anticancer interventions
— Histological or cytological confirmation of SCCHN1
1 For patients with unknown primary who have previously received treatment for locoregional head and neck cancer, histological or cytological confirmation of squamous cell carcinoma is acceptable.
VentiRx Pharmaceuticals Incorporated 27Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020
Dena.Jacob
Highlight

Active8 VTX-2337
— Tumor staging according to the TNM Classification of Malignant Tumors
— HPV status for patients with oropharyngeal carcinoma only
— If HPV status is not available in the subject’s medical history, testing for HPV statusby p16 immunohistochemistry, in situ hybridization, or polymerase chain reaction should be conducted at the time of screening (knowledge of HPV status is not necessary prior to randomization)
• Complete physical exam (PE), including vital signs (temperature, T; blood pressure, BP;respiration rate, RR; heart rate, HR), assessment of ECOG performance status (§11.1), weight and height
• Obtain 12-lead electrocardiogram (ECG)
• Collect blood samples for the following analyses:
— Complete blood count (CBC)
— Serum chemistry
— Serum pregnancy test (females with reproductive potential1 only)
— Pharmacogenetics
• Collect urine for urinalysis
• CT or MRI of the neck, chest, upper abdomen, and other anatomic region(s) of diseaseaccording to the requirements delineated in the VRXP-A202 Imaging Manual within 28 days of randomization
• Submit a tissue sample from the primary or metastatic tumor for all randomized subjects.When possible, re-biopsy at screening of primary tumor or metastatic tissue is preferred; however, archive tumor tissue may be used in absence of re-biopsy. If a tumor tissue sample is not available, sites should notify the sponsor or its representative prior to study entry.
A representative paraffin-embedded block of tissue from the original (diagnostic) biopsy and/or repeat biopsies will be submitted. If blocks cannot be submitted, 20 unstained slides plus one H&E stained 5-micron sections mounted on positively-charged glass slides are acceptable.
6.1.2 Randomization (Enrollment) Procedures
Subjects who have completed all screening assessments and are deemed eligible may be randomized (enrolled) up to 1 business day prior to Cycle 1 Day 1. Randomization of all subjects
1 Females who are premenopausal or ≤ 2 years postmenopausal and not surgically sterile
VentiRx Pharmaceuticals Incorporated 28Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
will be stratified by the receipt of prior systemic therapy for SCCHN (yes or no), ECOG performance status (0 or 1), and platinum therapy, as assigned by the investigator at the time of randomization (cisplatin or carboplatin).
Upon randomization, sites will be provided the subject’s randomization number and medication ID number. Randomization will also prompt an order for IP to be placed. A subject specific kit of IP will arrive approximately 3–4 business days after randomization.
6.2 Treatment Period
The treatment period is split into two phases: initial treatment (Cycles 1–6) and subsequent treatment (Cycles 7+).
Cycles 1–6 consist of 21-day cycles where subjects receive the following per cycle:
• A single dose of cisplatin or carboplatin (Day 1)
• A continuous infusion of 5-FU (Days 1–4)
• Three doses of cetuximab (Days 1, 8 and 15)
• Two doses of IP (Days 8 and 15)
Cycles 7+ consist of 28-day cycles where subjects receive the following per cycle:
• Four weekly doses of cetuximab (Days 1, 8, 15, and 22)
• Two doses of IP (Days 8 and 22)
Treatment continues until the subject has PD. Upon independent confirmation of radiographic disease progression and completion of treatment, subjects will complete the End of Treatment visit (§6.3) and begin long-term follow-up.
6.2.1 Initial Treatment (Cycles 1–6)
Study Cycles 1–6, Day 1 (CXD1) (±2 days)
• Within 72 hours prior to treatment, collect blood samples for the following analyses:
— CBC
— Serum chemistry
• Problem-oriented PE, including vital signs (T, BP, RR, HR), ECOG performance statusassessment and weight
VentiRx Pharmaceuticals Incorporated 29Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
— Cisplatin or carboplatin
— 5-FU
• Assess adverse events and and update concomitant medications
Study Cycles 1–6, Days 2–4 (CXD2-4) (±0 days)
• Continue 5-FU infusion according to the procedures in §7.3
Study Cycles 1–6, Day 8 (CXD8) (±1 day)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
On Cycle 1 Day 8 and Cycle 3 Day 8 only the assessments noted below will be completed. PK samples will only be collected on C1D8, not C3D8. Cetuximab administration will begin AFTER the 1 hour post-dose ECG and blood collection are completed. If Day 8 of Cycle 1 or 3 is skipped for any reason, the following assessments should be completed the next day the subject receives IP:
• Pre-dose
— Collect blood sample for PK assessment (C1D8 only)
— Collect blood sample for immune biomarker assessment
• 45 minutes post IP dose (±15 min)
— Collect blood samples for PK assessment (C1D8 only)
• 1 hour post IP dose (±15 min)
— Obtain 12-lead ECG
• 8 hours post IP dose (±15 min)
— Collect blood sample for PK assessment (C1D8 only)
— Collect blood sample for immune biomarker assessment
VentiRx Pharmaceuticals Incorporated 30Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Study Cycles 1–6, Day 15 (CXD15) (±1 day)
• Pre-dose
— Collect blood sample for CBC
• Collect vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 1–6, Week 12 (± 3 days) and Week 18 (± 3 days)
• Perform CT / MRI of neck, chest, upper abdomen, and other anatomical region(s) ofdisease using the same technique as baseline and in accordance with the Imaging Manual
Imaging should not be delayed in case of missed doses or dose delays.
6.2.2 Subsequent Treatment (Cycles 7+)
Study Cycles 7+, Day 1 (CXD1) (±2 days)
• Within 72 hours prior to treatment, collect blood samples for the following analyses:
— CBC
— Serum chemistry
• Problem-oriented PE, including vital signs (T, BP, RR, HR), ECOG performance statusassessment, and weight
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 8 (CXD8) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
VentiRx Pharmaceuticals Incorporated 31Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 15 (CXD15) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Day 22 (CXD22) (±1 days)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Study Cycles 7+, Every 8 Weeks (± 7 days)
• Perform CT / MRI of neck, chest, upper abdomen, and other anatomical region(s) ofdisease using the same technique as baseline and in accordance with the Imaging Manual
Imaging should not be delayed in case of missed doses or dose delays.
6.3 End of Treatment
Subjects will receive therapy until independently-confirmed disease progression per irRECIST. In the absence of significant clinical deterioration requiring intervention, disease progression identified at or before Week 12 should be confirmed with a repeat scan ≥ 4 weeks later and the subject should continue treatment until independent confirmation of PD based on the confirmation scan.
The End of Treatment visit will be completed within 14 days of independent confirmation of radiologic PD as assessed by irRECIST (§11.3) and prior to initiation of other anti-cancer therapy.
• Complete PE, including vital signs (T, BP, RR, HR), ECOG performance statusassessment and weight if not completed within the previous 14 days
• Collect blood samples for the following analyses if not completed within the previous 14days:
— CBC
VentiRx Pharmaceuticals Incorporated 32Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
— Serum chemistry
• Collect urine for urinalysis if not completed within the previous 14 days
• 12-lead ECG
• Assess adverse events and update concomitant medications
• Perform CT/MRI for subjects who have not had an imaging study within the previous 4weeks
6.4 Follow Up Period
Following the End of Treatment visit, subjects will be followed for survival. During thefollow-up period, subjects will be contacted every 8 weeks to assess vital status and disease state, including the initiation of any new anticancer interventions.
Remainder of page intentionally left blank.
VentiRx Pharmaceuticals Incorporated 33Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Table 1: Schedule of Procedures and Assessments
Screen Cycles 1–6 Cycles 7+
Study Week: -2 to -1 1–18 19+ EOT
Day: -14 to -1 1 2 3 4 8 15 1 8 15 22
Informed Consent1 X
FU
Q8weeks
Medical History & Eligibility2 X
VTX-2337 or Placebo (IP) X X X X
Cetuximab3 X X X X X X X
Cisplatin or Carboplatin X
Fluorouracil (5-FU) X X X X
Physical Examination X X X X
Vital Signs X X X X X
12-Lead ECG4 X X X
CBC with differential5 X X X X X
Serum Chemistry5 X X X X
Biomarkers6 2X
PK7 3X
Urinalysis X X
Pharmacogenetics X
Serum Pregnancy8
Submit Tumor Tissue
X
X
AE/CRx9 X X X X X X X X
Assess Vital Status X
Tumor Assessments
Screen Week 12 ± 3 Days
Week 18 ± 3 Days
Week 26 ± 7 Days
Every 8Weeks EOT FU± Days
1
CT or MRI10 X X X X X X
Informed consent may be obtained any time prior to study related procedures (i.e., is not required to be within 14 days of randomization)
2 HPV status for patients with oropharyngeal carcinoma only3 Cycle 1 Day 1 dose = 400 mg/m2; subsequent doses are 250 mg/m2
4 Cycle 1 Day 8 and Cycle 3 Day 8: perform 1 hour (±15 minutes) post-dose of IP5 Obtain within 72 hours of each Day 1 dose6 Cycle 1 Day 8 and Cycle 3 Day 8 only: perform pre-dose and 8 hours (±15 minutes) post-dose of IP7 Cycle 1 Day 8 only: perform pre-dose, and 45 minutes and 8 hours (±15 minutes) post-dose of IP8 Serum pregnancy to be collected on all females with reproductive potential9 AEs will be collected from Cycle 1 Day 1 until 7 days after the last dose of any study medication or EOT visit, whichever is
later10 The same imaging modality must be used for each subject throughout the study. Assess tumor response at Week 12 (± 3 days),
Week 18 (± 3 days), and every 8 weeks (± 7 days) thereafter. Do not delay imaging if dosing/cycle is delayed
VentiRx Pharmaceuticals Incorporated 34Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
6.5 Early Treatment Discontinuation
Treatment may be discontinued early for individual subjects for any of the following reasons:
• Subject decision / withdraw of consent
• Unacceptable toxicity related to the administration of the study required medicationsaccording to §7.4
• Cetuximab infusion reactions prior to administration of the first dose of IP (i.e., Cycle 1Day 1) requiring (i) permanent discontinuation of cetuximab or (ii) administration of corticosteroids with each dose of cetuximab
• Subject lost to follow-up after repeated attempts to contact the subject
• Onset of an adverse event that would make ongoing treatment in the clinical trialinadvisable, as determined by the investigator, medical monitor, or study sponsor
• Subject non-compliance with the study’s requirements and/or procedures as determinedby the investigator, medical monitor, or study sponsor
• Death
In the event a subject is withdrawn from treatment prior to/without independently-confirmed disease progression per irRECIST, the subject should continue to complete imaging assessments per protocol until irPD confirmation by the independent radiologist, or death.
In addition, if a subject is withdrawn from treatment prematurely due to any of the reasons noted above, the End of Treatment evaluations should be completed, and the subject should be followed for survival.
Subjects should remain on study (i.e., be followed for survival) until death. In the rare event that a subject withdraws consent for all study-related activities, including follow-up for survival, this should be clearly documented in the medical record and eCRF.
6.6 Assessments6.6.1 Assessment of Efficacy6.6.1.1 Efficacy Parameters
The following efficacy parameters will be assessed by independent radiology review according to irRECIST (§11.3) and RECIST v1.1, and are defined as follows:
• Progression-free survival: the duration of time from randomization to the time of PD ordeath, whichever comes first
VentiRx Pharmaceuticals Incorporated 35Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
• Objective response rate: the proportion of subjects who achieve complete or partialresponse
• Duration of best response: the duration of time from the date measurement criteria arefirst met for CR, or PR (if CR is never met), until the first date that PD is confirmed by independent radiology review or death, whichever comes first
• Disease control rate: the percentage of subjects who achieved CR, PR, or SD
• Duration of disease control: the duration of time from the date measurement criteria arefirst met foCR, PR, or SD, until the first date that PD is confirmed by independent radiology review or death, whichever comes first
In addition, PFS—as defined above—assessed by irRECIST and evaluated by investigators will also be included in the efficacy parameters.
Overall survival is defined as the duration of time from randomization to the time of death due to any cause, or the date the subject was last confirmed to be alive.
6.6.1.2 Method and Timing
Imaging studies (CT or MRI) of the neck, chest, upper abdomen, and other anatomical region(s) of disease must be obtained at study Screening, Week 12, Week 18, and every 8 weeks thereafter until disease progression. Imaging studies will be completed at the End of Treatment visit for subjects who discontinue the study prematurely and have not had CT/MRI completed within the last 4 weeks (§6.5). For each subject, the same imaging method must be used at study screening and all follow-up assessments.
RECIST v1.1 is primarily designed to evaluate the early effects of cytotoxic agents and depends on tumor shrinkage to demonstrate biologic activity. However, clinical evidence of tumor responses seen with immunotherapeutic agents, such as VTX-2337, can take longer to achieve and may occur after a period of disease stabilization or following an initial increase in tumor burden. In light of the limitations of utilizing RECIST v1.1 to evaluate immunomodulatory agents, immune-related response criteria have been proposed as an alternative to conventional RECIST to systematically detect the novel response patterns observed with immunologic agents.[18, 19] This study will use RECIST v1.1 for the baseline tumor evaluation, and an immune-related modification of RECIST v1.1 (irRECIST) in addition to RECIST v1.1 to determine tumor response .
As noted above, the immune-mediated responses expected from VTX-2337 require activation of the immune system prior to the observation of clinical responses, and such immune activation may take weeks to months to be clinically evident. Some subjects with advanced cancer may
VentiRx Pharmaceuticals Incorporated 36Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
have objective increase of tumor burden within 12 weeks following the start of dosing on study. Such subjects may not have had sufficient time to develop the required immune activation or, in some subjects, tumor increases may represent infiltration of lymphocytes into the original tumor (often referred to as pseudo-progression). In traditional oncology studies, such increases in tumor burden during the first 12 weeks of the study would constitute progressive disease and lead to discontinuation of study treatment and imaging to detect response, thus disregarding the potential for subsequent immune-mediated clinical response. Therefore, in this study, the first imaging assessment will be performed at Week 12, followed by assessments at Week 18 and every 8 weeks thereafter.
In addition, a key distinction between standard RECIST v1.1 criteria and irRECIST is that the latter requires early evidence of disease progression (i.e., an assessment of progressive disease ≤ 12 weeks after starting study treatment)—in the absence of rapid clinical deterioration—be confirmed by repeat, consecutive imaging ≥ 4 weeks after the initial assessment. During this interim ≥ 4 week period, subjects should continue to be followed per protocol, including continued dosing with study treatment. The key differences between RECIST v1.1 and irRECIST are outlined in Table 2.
irRECIST
Total Measured Tumor Burden
The total measured tumor burden (TMTB) is established at baseline as the sum of the longest diameters (SOD)—the shortest axes should be used for lymph nodes—of all target lesions(≤ 2 lesions per organ, ≤ 5 lesions total). At each subsequent tumor assessment (TA), the SOD ofnew, measurable lesions (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; ≤ 2 new lesions per organ, ≤ 5 new lesions total) is added to the SOD of the target lesions to provide the updated TMTB:
TMTB = SOD target lesions + SOD new, measurable lesions
Percentage changes in TMTB at each TA describe the size and growth kinetics of both old and new, measurable lesions as they appear. At each TA, the response in TMTB is defined as follows:
• Complete Response (irCR): Complete disappearance of all target and new, measurablelesions, with the exceptions of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
VentiRx Pharmaceuticals Incorporated 37Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
Response in Non-Target Lesions
The presence of non-target lesions is established at baseline; at each TA, the presence of any new, non-measurable lesions is assessed. The presence of new, non-measurable lesions will rule out an overall response of irCR. An increase in the size or number of new, non-measurable lesions does not necessarily imply an overall response of irPD; if these lesions become measurable (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; up to 2 new lesions per organ, total 5 new lesions) at a subsequent TA, their measurement will, at that point, start to contribute to the TMTB.
The response in non-target lesions is defined as follows:
• Complete Response (irCR): Complete disappearance of all non-target lesions
• non-irCR/non-irPD: Non-target lesions do not meet the criteria for irCR or irPD
• Progressive Disease (irPD): Unequivocal increase in the number or size of non-targetlesions. To achieve unequivocal progression of non-target lesions, there must be a substantial worsening of non-target disease of a magnitude that, according to the treating physician, warrants a change in anticancer therapy
NOTE: Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing lesions) should be considered irSD and treatment may continue until the next scheduled assessment.
Overall Response
The overall response according to irRECIST is derived from the responses in TMTB as well as the presence of any non-target lesions as follows:
• Complete Response (irCR): Complete disappearance of all lesions (whether measurableor not); lymph nodes must decrease to < 10 mm in shortest dimension
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
VentiRx Pharmaceuticals Incorporated 38Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
RECIST v1.1
Evaluate Target Lesions
• Complete Response (CR): Complete disappearance of all target lesions, with theexception of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (PR): Decrease in sum of diameters of target lesions ≥ 30% relative tobaseline
• Stable Disease (SD): Not meeting criteria for CR or PR, in absence of PD
• Progressive Disease (PD): Increase in sum of diameters of target lesions ≥ 20% with anabsolute increase of ≥ 5 mm relative to nadir
Evaluate Non-Target Lesions
• Complete Response (CR): Disappearance of all non-target lesions and normalization oftumour marker level. All lymph nodes must be non-pathological in size (<10 mm short axis).
• Non-CR/Non-PD: Persistence of one or more non-target lesion(s) and/or maintenance oftumour marker level above the normal limits.
• Progressive Disease (PD): Unequivocal progression of existing non-target lesions.(Note: the appearance of one or more new lesions is also considered progression).
New Lesions
The appearance of new malignant lesions denotes disease progression.
Overall Response
The overall response according to RECIST v1.1 is derived from the responses in sum of diameters in target lesions, the presence of any non-target lesions, as well as new lesions as noted in Table 3 and Table 4.
VentiRx Pharmaceuticals Incorporated 39Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Table 2: Tumor Response Evaluation: Comparison between RECIST v1.1 andirRECIST
Criteria RECIST v1.1 irRECIST
First tumor assessment (TA) Typically assessed at Week 8 Assessed at Week 12
New lesion(s)
New measurable lesions(≥ 10 mm [≥ 15 mm for lymph node short axis])
Always represents PD Included in TMTB if measurable
New non-measurable lesions (< 10 mm [< 15 mm for lymph node short axis])
Always represents PD Does not define progression but precludes irCR
Non-target lesions Changes contribute to defining best overall response (BOR), CR, PR, SD and PD
Changes contribute to defining irCR (complete disappearance required)
Unequivocal progression ofnon-target lesions
Always represents PD May represent irPD if there is a substantial worsening that warrants a change in anticancer therapy
CR Disappearance of all lesions Disappearance of all lesions
PR ≥ 30% decrease in the SOD of all target lesions compared with baseline, in absence of new lesions or unequivocal progression of non-target lesions
≥ 30% decrease in the TMTB compared with baseline
SD Neither CR, PR, or PD can be established
Neither irCR, irPR, or irPD can be established
PD ≥ 20% increase in SOD of target lesions compared with nadir. The SOD of target lesions must also demonstrate an absolute increase of ≥ 5 mm.The appearance of ≥ 1 new lesions is also considered progression
≥ 20% increase in TMTB compared with nadir. The TMTB must also demonstrate an absolute increase of ≥ 5mm*
*Subjects with an initial finding of progressive disease (irPD) before or at the 12 week imaging assessment, but without rapidclinical deterioration, require confirmation of irPD with a second, consecutive scan obtained ≥ 4 weeks from the initial documentation. Subjects will continue to receive study treatment until irPD is confirmed at this later time point. Best overall response (BOR) will therefore include responses occurring at any time before disease progression and after early progression (i.e., within the first 12 weeks of the study).
VentiRx Pharmaceuticals Incorporated 40Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Table 3: Time Point Response for Patients with Measurable Disease at Baseline(i.e., Target Disease)
TargetLesions
Non-Target Lesions NewLesions
Time PointResponse
CR CR No CRCR Non-CR/Non-PD No PRCR Not Evaluated No PRPR Non-PD or
Not EvaluatedNo PR
SD Non-PD orNot Evaluated
No SD
Not Evaluated Non-PD No Not EvaluatedPD Any Yes or No PDAny PD Yes or No PDAny Any Yes PD
Table 4: Time Point Response for Patients with only Non-Measurable Diseaseat Baseline (ie, Non-Target Disease)
Non-Target Lesions New Lesions Time Point ResponseCR No CR
Non-CR/non-PD No Non-CR/non-PD*Not Evaluated No NE
Unequivocal PD Yes or No PDAny Yes PD
*‘Non-CR/non-PD’ is preferred over ‘stable disease’ for non-targetdisease since SD is increasingly used as an endpoint for assessment of efficacy in some trials so to assign this category when no lesions can be measured is not advised
Comprehensive RECIST v1.1 and irRECIST guidelines can be found in §11.2 - §11.4.
VentiRx Pharmaceuticals Incorporated 41Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
6.6.2 Assessment of Safety6.6.2.1 Safety Parameters
The primary safety parameters are the occurrence and severity of adverse events throughout the study treatment period. Refer to §8.2 for AE reporting requirements.
The pre-dose assessments performed on Day 1—including PE, vital signs, and laboratory assessments—will serve as the baseline and the standard for comparison of all follow-up examinations. All abnormal findings will be noted on follow-up and compared to baseline and clinically significant changes will be noted as adverse events.
6.6.2.2 Method and Timing
History and Physical Examination
A complete physical exam and medical history, including detailed cancer history, must be obtained within 14 days prior to randomization.
Complete physical exams and problem-oriented physical exams are subsequently required as described in §6.0. Vital signs should be monitored as shown in Table 1.
Electrocardiograms
A 12-lead ECG will be performed at Screening, 1-hour post dose on Cycle 1 Day 8 and Cycle 3 Day 8, and End of Treatment.
Clinical Laboratory Evaluations
The clinical laboratory evaluations will be collected at Screening and within 72 hours of Day 1 of each cycle, and will include a complete set of clinical labs, including serum chemistry, complete blood count with differential, and urinalysis, as described in §6.2.
Subject-Reported Adverse Events
In addition to those adverse events noted by the study staff as determined through clinical evaluation, additional events may be elicited from the subject in a non-leading manner or volunteered by the subject at any time during the study. All adverse events, regardless of their severity or relationship to treatment with IP, will be recorded. All subjects experiencing adverse events will receive treatment if required for their event. Adverse events that are determined to be related to IP will be followed until resolution, or until resolved with sequelae.
VentiRx Pharmaceuticals Incorporated 42Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
6.6.3 Translational Research Assessments
Various immune and immunogenetic assessments will be performed on all subjects in the study. Exploratory analyses correlating data from these assessments will be performed to determine if predictors of potential clinical benefit emerge. These predictors would be valuable in defining appropriate populations for study in subsequent trials of VTX-2337 in this patient group.
Pharmacogenomics
A single sample of genomic DNA will be collected on all subjects for analysis of genetic polymorphisms that may impact the response of patients to a TLR8 agonist or to cetuximab. These include defined single nucleotide polymorphisms (SNPs) in the TLR8 gene (most notably the A1G variant), and variants in the FcγRII and FcγRIII genes (most notably the 131 and 158 polymorphisms, respectively), that vary binding affinity for the FcR.
Immune Biomarker Analysis
TLR8 stimulates the production of a variety of cytokines and chemokines from immune cells. Serum samples will be collected pre-dose and 8 hours post-dose on C1D8 and C3D8 for analysis using a multiplexed panel of cytokines, chemokines, and inflammatory markers.
Tissue Biomarker Studies
Assessment of the effect of immune cell subsets, as measured by immunohistochemistry in primary tumor tissue (e.g., immune score) will be completed on tumor tissue obtained from the primary tumor site. This analysis includes but is not limited to an automated analysis of CD3, CD45, and FOXP3 staining of lymphocyte populations in the tumor using immunohistochemistry. Additional studies including gene signature analysis or detached somatic mutations will be performed, if indicated.
Pharmacokinetic Analysis
Plasma samples will be obtained on Cycle 1 Day 8 and quantitatively analyzed to support population PK and exposure-response analyses.
6.7 Monitoring for Subject Compliance
No specific measures for subject compliance are required for this study. IP must be administered in the clinic or hospital setting under the supervision of the investigator or clinical site staff. Subjects should be carefully evaluated prior to study entry to ensure they can comply with the study’s visit and assessment schedule.
VentiRx Pharmaceuticals Incorporated 43Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
7.0 TREATMENT7.1 Packaging, Labeling and Storage
IP is provided as an off-white, lyophilized cake in a 3-mL clear-glass, stoppered, single-use vial. Each vial is identified with a label similar to the following:
8.4 mg VTX-2337 or Placebo for subcutaneous injection
Subject #XXXXX
Prepare according to clinical protocol VRXP-A202
Store 2–8ºC
Caution: New drug—limited by federal law to investigational use.
VentiRx Pharmaceuticals, Inc.
8.4 mg VTX-2337 or Placebo for subcutaneous injection
Subject XXXXX for protocol VRXP-A202
Subject #: ________________
Date: ___________________
↑ This portion attached to vial ↑ Detach this portion for subject record
Upon randomization, a subject-specific kit containing a supply of IP will be shipped via traceable courier to the clinical site. Sites will order re-supply kits through the IXRS. Unopened vials of IP should be stored in the refrigerator at 2−8ºC (36−46ºF) and protected from light.
VTX-2337 and placebo will be labeled, packaged, and shipped by Fisher Clinical Services (Mount Prospect, IL).
7.2 Preparation of Investigational Product
Refer to the Pharmacy Manual for complete instructions regarding the storage and preparation of IP.
Before administration, IP must be reconstituted and prepared according to the Pharmacy Manual. Investigational drug solution should be prepared and transferred using aseptic technique in a biological safety cabinet. Vials of IP are intended for single use only.
IP will be supplied by VentiRx Pharmaceuticals. All other medications may be obtained through standard institutional practice.
7.3 Administration of Investigational Product and Study Treatment(s)7.3.1 Investigational Product Administration
IP (i.e., VTX-2337 or placebo) is administered as a subcutaneous injection of 3.0 mg/m2 (see also §9.2.2). Doses are given prior to cetuximab on Days 8 and 15 of a 21-day cycle for the first
VentiRx Pharmaceuticals Incorporated 44Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
6 cycles and on Days 8 and 22 for cycles 7+. Subjects will continue to receive bi-weekly doses of IP until independently-confirmed disease progression. See also §6.3 and §6.5.
Within 30 minutes prior to each dose of IP subjects will be administered 650–1000 mg acetaminophen by mouth to help mitigate potential adverse events commonly associated with the administration of VTX-2337 (e.g., fever, myalgia). Subjects will be given or instructed to take an additional dose of 650–1000 mg acetaminophen by mouth approximately 4–6 hours after administration of IP, and as needed thereafter for symptoms of fever and/or body aches. Acetaminophen is the preferred over-the-counter analgesic and antipyretic; due to their potentially immunosuppressive effects, administration of NSAIDS within 24 hours of dosing should be avoided if clinically feasible.
To potentially reduce the effects of injection site reaction that may be associated with the administration of IP, an ice pack may be applied to the injection site for approximately 30 minutes prior to injection, immediately following injection, and throughout the day of injection. Additionally, at the discretion of the investigator, single doses of IP may be divided and administered at two different anatomical locations.
The dose of IP should be administered with a syringe suitable for subcutaneous injection. To administer the injection, 1–2 inches of fatty tissue should be pinched up to avoid injection into the muscle layer. The needle can be inserted at either 45 or 90 degrees; a 45 degree angle is recommended when less than 2 inches of tissue can be pinched. Appropriate anatomic areas for subcutaneous injection include the fatty tissue over the abdomen, triceps, thighs, or lower back. The injection site should be rotated among anatomically appropriate locations to help avoid injection site reaction.
Standard medications to treat possible hypersensitivity reactions and/or symptoms of CRS should be readily available at the time of treatment, including epinephrine, H1 antihistamines (e.g., diphenhydramine), H2 antihistamines (e.g., ranitidine), narcotics, IV fluids for volume expansion and supplemental oxygen.
Due to their immunosuppressive effect, administration of systemic corticosteroids (e.g., dexamethasone) should be avoided in this setting if other means of treatment are available and appropriate.
VentiRx Pharmaceuticals Incorporated 45Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
7.3.2 Cetuximab Administration
The initial 400 mg/m2 dose of cetuximab is administered on Cycle 1 Day 1 as a 120-minute IV infusion (maximum infusion rate 10 mg/min).1
The subsequent, weekly, 250 mg/m2 doses of cetuximab are administered as 60-minute IV infusions (maximum infusion rate 10 mg/min).1 Subjects will continue to receive weekly doses of cetuximab until independently-confirmed disease progression. See also §6.3 and §6.5.
Subjects will be premedicated with an H1 antagonist (e.g., 50 mg of diphenhydramine) intravenously 30–60 minutes prior to the first dose; premedication should be administered for subsequent cetuximab doses based upon clinical judgment and the presence/severity of prior infusion reactions. Premedication with steroids may be administered on Cycle 1 Day 1, if required by institutional standards. However, due to their immunosuppressive effect, steroids should be discontinued 72 hours prior to dosing with IP. See also §7.6.
Serious infusion reactions, requiring medical intervention and immediate, permanent discontinuation of cetuximab, include rapid onset of airway obstruction (e.g., bronchospasm, stridor, hoarseness), hypotension, shock, loss of consciousness, myocardial infarction and/or cardiac arrest. Subjects should be monitored for 1 hour following cetuximab infusions in a setting with resuscitation equipment and other agents necessary to treat anaphylaxis (e.g., epinephrine, intravenous antihistamines, bronchodilators, oxygen, and corticosteroids).
When cetuximab is administered on the same day as chemotherapy, cetuximab administration will be completed ≥ 1 hour prior to administration of platinum and 5-FU. When cetuximab is administered on the same day as IP, the dose of IP will be given prior to cetuximab.
For additional information please refer to the cetuximab label.
7.3.3 Platinum Administration
The platinum therapy should be assigned by the investigator prior to randomization. Because cisplatin or carboplatin administration is a stratification factor, the choice of platinum agent should be determined prior to randomization. Unless clinically necessary, the investigator should not change the platinum chemotherapy for each subject. Reasonable efforts should be made to keep the subject on the platinum therapy originally assigned; however, the platinum therapy may be changed if clinically necessary.
1 The duration of infusion may be adjusted according to institutional standards.
VentiRx Pharmaceuticals Incorporated 46Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Cisplatin
At least one hour after completion of cetuximab administration, subjects will receive a100 mg/m2 dose of cisplatin administered as a 60-minute IV infusion.1 Cisplatin will be administered on Day 1 of a 21-day cycle for a maximum of 6 cycles and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
Pretreatment hydration may be administered according to institutional standards.
For additional information regarding cisplatin administration, please refer to the label.
Carboplatin
At least one hour after completion of cetuximab administration, subjects will receive carboplatin at an AUC of 5 mg/mL/min administered as a 60-minute IV infusion.1 Carboplatin will be administered on Day 1 of a 21-day cycle for a maximum of 6 cycles, and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
For additional information regarding administration, please refer to the carboplatin label.
7.3.4 Fluorouracil (5-FU) Administration
At least one hour after completion of cetuximab administration, subjects will receive an intravenous infusion of 5-FU at a dose of 1000 mg/m2 per day for 4 days. 5-FU administration will begin on Day 1 of a 21-day cycle for a maximum of 6 cycles and should be discontinued if the subject has independently-confirmed disease progression. See also §6.3 and §6.5.
For additional information regarding 5-FU administration please refer to the label.
7.4 Dose Modifications
In order to maintain dose-intensity and cumulative dose-delivery, reasonable efforts should be made to minimize dose reductions and treatment delays. Any subject whose treatment is delayed due to treatment-related toxicity should be evaluated on a weekly basis until adequate hematologic and non-hematologic parameters have been met.
Toxicities may require reduction or discontinuation of one or more of the study required- medications (refer to §7.4.3). The investigator should carefully assess all treatment-associated toxicities and, whenever possible, determine if the toxicities can reasonably be attributed to a single agent, or, conversely, if a causal relationship with an agent can reasonably be ruled out. If
1 The duration of infusion may be adjusted according to institutional standards.
VentiRx Pharmaceuticals Incorporated 47Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
appropriate, dose reductions and discontinuations should not affect the dose or administration of the other agents.
• Toxicity grades are defined using the National Cancer Institute Common TerminologyCriteria for Adverse Events (NCI-CTCAE) version 4.03
• Any subject who requires a dose reduction of investigational product due to drug-relatedtoxicity will continue to receive the reduced dose for the remainder of study treatment
• Prior to dose reduction, supportive care should be maximized at the investigator’sdiscretion for adverse events such as nausea, vomiting, diarrhea, and electrolyte imbalances
• Dose escalations are not allowed
• If study-required therapy is delayed by more than 6 weeks for any reason, the site shouldcontact the medical monitor
It is anticipated that toxicities attributed to the cytotoxic agents (cisplatin, carboplatin, and/or 5- FU) may require a delay in the Day 1 dose of the next scheduled treatment cycle while awaiting subject recovery. In such a case, platinum and 5-FU chemotherapy should be delayed together in order to ensure that they are administered together at the next Day 1 treatment. During a treatment delay, subjects should be evaluated weekly. If toxicity leads to a delay in cytotoxic chemotherapy for greater than 3 consecutive weeks (i.e., > 21 days), one or both of the chemotherapeutic agents (at the discretion of the investigator, depending upon the cause of toxicity) should be permanently discontinued. This should not impact the continuation of the other study treatments, including platinum in the absence of 5-FU or vice versa.
During the ≤ 3-week delay, the previous cycle should be extended to include treatment on Day 22 and potentially Days 29 and 36 (see below). Please refer to §11.5 for additional information.
Extended Cycles 1–5, Day 22 (CXD22) (±1day)
• If evaluations performed by the local laboratory are required to assess ongoing toxicities(e.g., decreased neutrophils), also send samples to the central laboratory
• Problem-oriented PE, including vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
VentiRx Pharmaceuticals Incorporated 48Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Extended Cycles 1–5, Day 29 (CXD29) (±1day)
• If evaluations performed by the local laboratory are required to assess ongoing toxicities(e.g., decreased neutrophils), also send samples to the central laboratory
• Problem-oriented PE, including vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— IP
— Cetuximab
• Assess adverse events and update concomitant medications
Extended Cycles 1–5, Day 36 (CXD36) (±1day)
• If evaluations performed by the local laboratory are required to assess ongoing toxicities(e.g., decreased neutrophils), also send samples to the central laboratory
• Problem-oriented PE, including vital signs (T, BP, RR, HR)
• Administer the following study medications according to the procedures in §7.3
— Cetuximab
• Assess adverse events and update concomitant medications
It is possible that a subject may require a dose to be held due to toxicities related to cetuximab or IP. Those doses should be considered missed and will not be made up. For example, if on Day 15, a subject is unable to receive the scheduled dose of cetuximab, IP should be given as appropriate, and the next week the subject would proceed with Day 1 of the next cycle.
The timing of imaging studies should not be affected by dose reductions or delays. Subjects should remain on study (i.e., continue receiving treatment with other agents and undergo all protocol-related assessments) until independently-confirmed disease progression. Thereafter, subjects should be followed for long-term survival per protocol.
7.4.1 Investigational Product Dose Modifications
Management of Injection Site Reactions
Acute symptoms of injection site reactions typically resolve within 48 hours of injection, but more persistent reactions are not unexpected. Grade 2 and 3 reactions may include a painful, raised, fluid-filled blister that mimics a sterile abscess. Injection site reactions do not typically warrant antibiotic intervention as they have been found to be sterile. A culture of the fluid can be
VentiRx Pharmaceuticals Incorporated 49Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
obtained—using sterile technique—if infection is strongly suspected (i.e., associated with fever persisting more than 24 hours after injection).
Ice and acetaminophen should be administered prophylactically according to §7.3.1. Symptomatic treatment with ice, acetaminophen and narcotics is acceptable. Due to their potentially suppressive effects, the use of NSAIDs within 24 hours of dosing with IP should be avoided, if clinically feasible.
Management of Systemic Toxicities
The most common systemic drug-related adverse events—grade 1 or 2 chills, flu-like symptoms and fever—typically resolve in < 48 hours and do not require dose reductions or a delay in the dosing regimen. Less commonly, dosing with VTX-2337 may result in CRS, which is most likely to be grade 1 or 2, but more severe reactions have been reported.
CRS is a symptom complex and is characterized by systemic symptoms which may include fever, nausea, chills, tachycardia, hypotension, dyspnea, asthenia, headache, and rash. VTX-2337 directly targets TLR8, which is expressed on immune cells. CRS may result from the release of cytokines from the activated immune cells, or from ‘downstream’ events that can be associated with cytokine production. Symptoms of CRS may be acute or delayed by several hours after dosing with IP.
Treatment of systemic drug-related events should be consistent with the severity of the reaction as well as institutional standards and may include: acetaminophen, H1- and H2-receptor antagonists, narcotics, IV fluids for volume expansion, and supplemental oxygen. Due to their potentially immunosuppressive effect, administration of NSAIDs and systemic steroids (e.g., dexamethasone) should be avoided if other means of treatment are available and medically appropriate.
In most cases the CRS will be grade 1 or 2. However, a severe, life-threatening reaction resulting from a substantial release of cytokines is possible. Severe CRS is a medical emergency and urgent intervention must be taken to prevent life-threatening complications. This may include administration of sympathomimetic amines for pressor support and/or hospitalization for acute monitoring and intervention.
Investigational Product Dose Modifications
Table 5 and Table 6 outline dose delay and reduction requirements for IP. Delays in IP dosing should not delay or shift the timing of cetuximab, platinum, or 5-FU dosing (i.e., doses of IP are skipped and not made up). In the event of grade 3 or grade 4 toxicities attributed to IP, subsequent doses should be delayed until recovery to ≤ grade 1.
VentiRx Pharmaceuticals Incorporated 50Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Table 5: Investigational Product Dose Reduction Schedule
IP Dose Level (mg/m2)
3.0
2.5
2.0
NOTE: Only two dose reductions are allowed. If a third dose reduction is required, IP should be discontinued.
VentiRx Pharmaceuticals Incorporated 51Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Table 6: Investigational Product Dose Modifications
Grade Action
Cytokine Release Syndrome
1 Dose reduction not required; consider prophylactic precautions—including volume expansion and treatment with oral or IV antihistamines—with next dose
2 Consider prophylactic precautions—including volume expansion and treatment with oral or IV antihistamines— with next doseReduce dose by 1 level at investigator’s discretion
3 Use prophylactic precautions with next doseReduce dose by 1 level
Injection Site Reaction
1 Dose reduction not required; consider administering subsequent injections at distal anatomic site(s)
2 Administer subsequent injections at distal anatomic site(s) until resolved to ≤ grade 1
Delay dosing for up to 2 weeks if needed
If > 2 week delay or > 2 delays are required with consecutive injections, reduce dose by 1 level
3 Delay dosing until resolved to ≤ grade 1Reduce dose by 1 level
Non-Hematologic Drug-Related AEs
1–2 Dose reduction not required; manage per institutional standards
≥ 3 Reduce dose by 1 level
Hematologic Drug-Related AEs
1–3 Dose reduction not required; manage per institutional standards
≥ 4 Reduce dose by 1 level
VentiRx Pharmaceuticals Incorporated 52Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
7.4.2 Cetuximab Dose Modifications
Table 7 and Table 8 should be used as a guideline for cetuximab dose modifications. Please refer to the cetuximab label for additional information.
Table 7: Cetuximab Dose Modifications for Infusion Reactions
NCI-CTC Grade Dose Modification
1
Reduce infusion rate by 50%2
Non-serious grade 3
Serious grade 3 (e.g., requiring hospitalization) or any grade 4 Immediately and permanently discontinue cetuximab
Table 8: Cetuximab Dose Modifications for Dermatologic Toxicity
Severe Acneiform Rash CetuximabDelay/Discontinuation
Outcome Dose Modification
1st occurrence Delay infusion by 1–2 weeks Improvement Continue at 250 mg/m2
No improvement Discontinue cetuximab
2nd occurrence Delay infusion by 1–2 weeks Improvement Reduce dose to 200 mg/m2
No improvement Discontinue cetuximab
3rd occurrence Delay infusion by 1–2 weeks Improvement Reduce dose to 150 mg/m2
No improvement Discontinue cetuximab
4th occurrence Discontinue cetuximab
VentiRx Pharmaceuticals Incorporated 53Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
7.4.3 Chemotherapy Dose Modifications (cisplatin, carboplatin, and 5-FU)
Table 9 and Table 10 should be used as a guide for dose reductions of cisplatin, carboplatin, and5-FU. The dose of each agent should be reduced by 25% in subjects with related toxicities≥ grade 3. Primary or secondary prophylaxis with granulocyte colony growth factor (G-CSF) is permitted in order to manage the neutropenia expected from platinum-5-FU therapy.
Table 9: Dose Reduction Guidelines for Chemotherapeutic Agents
Grade ≥ 3 Toxicity ChemotherapyDelay/Discontinuation
Outcome Dose Modification
1st occurrence Delay infusion by 1–3 weeks Improvement Reduce dose by 25%
No improvement Discontinue agent
2nd occurrence Delay infusion by 1–3 weeks Improvement Reduce dose to 50%
No improvement Discontinue agent
3rd occurrence Discontinue agent
Table 10: Chemotherapy Dose Reduction Schedule
Agent Original Dose (100%) 25% Reduction 50% Reduction
Cisplatin 100 mg/m2 75 mg/m2 50 mg/m2
Carboplatin AUC of 5 mg/mL/min AUC of 3.75 mg/mL/min AUC of 2.5 mg/mL/min
5-FU 1000 mg/m2/day 750 mg/m2/day 500 mg/m2/day
Additional Considerations for Chemotherapy Dosing
Investigators should follow their institutional standards for repeat dosing criteria (i.e., serum creatinine and hematologic thresholds for dosing).
When clinically appropriate, subjects assigned to cisplatin should receive 2 dose reductions prior to discontinuation of cisplatin and/or being re-assigned to receive carboplatin. If clinically necessary, the investigator may change the platinum chemotherapy from cisplatin to carboplatin.
VentiRx Pharmaceuticals Incorporated 54Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
7.5 Emergency Unblinding
The treatment assignment of any individual subject may be accessed only in case of an emergency, such as a life-threatening serious adverse event (SAE) where knowledge of the treatment code is required for medical management of the event. The investigator should obtain approval from the medical monitor or sponsor prior to unblinding and should document the unblinding (including notification of sponsor/medical monitor and reason for unblinding) in the subject’s medical record.
Contact information for notification of unblinding:
PRA Oncology Call CenterToll Free: +1 (866) 326-5053Direct: +1 (434) 951-4082Fax: +1 (800) 280-7035Email: [email protected]
After obtaining sponsor or medical monitor approval, to unblind the subject’s treatment assignment the investigator will log into IXRS and enter, at minimum, the subject’s randomization number; IXRS will then provide the treatment assignment. The treatment assignment should be maintained as confidential (i.e., only personnel essential for subject treatment should be informed of the treatment assigned) and placed in a sealed envelope.
The treatment code for an individual subject may also be broken at the discretion of the study sponsor to facilitate regulatory reporting of suspected unexpected serious adverse reactions (SUSAR).
7.6 Concomitant Medications and Supportive Care
Medications that must be discontinued prior to study entry are outlined in §5.2. The following medications and interventions, unless otherwise specified, are prohibited from the time of study screening until the End of Treatment visit:
• Systemic anti-cancer therapy, including chemotherapy, radiotherapy, or endocrinetherapy other than those required per protocol
• Systemic—oral, IV, injectable—corticosteroids (e.g., dexamethasone, prednisone) within72 hours of dosing with IP (see also §7.6.1)
• Any investigational drug or device other than VTX-2337 or placebo
VentiRx Pharmaceuticals Incorporated 55Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
• NSAIDs, including aspirin, within 24 hours of IP dosing should be avoided if clinicallyfeasible, due to their potentially suppressive effects Any immunotherapy other than VTX- 2337 or placebo
• Cytochrome P450 3A4 (CYP3A4) inducers and/or inhibitors may affect the metabolismof VTX-2337. Therefore, care should be exercised when drugs or other substances that affect CYP3A4 are administered concomitantly with VTX-2337 or placebo and, if possible, alternatives that do not affect CYP3A4 should be administered instead. A list of CYP3A4 inhibitors and inducers may be found in §11.6.
Subjects should be provided with full supportive care measures, as clinically indicated, and in accordance with institutional standards. Such care includes medication for pain control and symptom management, antibiotics, bisphosphonates, antiemetics, colony stimulating factors, and transfusions of blood or blood products. Treatment for drug-related adverse events should be administered at the discretion of the investigator.
Anaphylactic-like reactions have been reported with administration of cetuximab, cisplatin, carboplatin, and 5-FU. Epinephrine and/or antihistamines may be administered to alleviate symptoms. Due to their immunosuppressive effect, administration of systemic steroids (e.g., dexamethasone) should be avoided in this setting if other means of treatment are available and appropriate. For additional information on treatment of cetuximab infusion reactions refer to §7.3.
Localized radiotherapy is permitted for palliation of painful lesions at the investigator’s discretion. However, medical management in place of radiation therapy should be used if clinically appropriate.
7.6.1 Chemotherapy-induced nausea and vomiting
Corticosteroids (e.g., dexamethasone) are often used as the first-line treatment for chemotherapy-induced nausea and vomiting (CINV); however, the administration of systemic corticosteroids (oral, IV, injectable) broadly inhibits the production of multiple cytokines and chemokines and impairs cellular immunity, thus impeding the immunostimulatory and pharmacologic effects of VTX-2337. For this reason, a steroid-sparing approach to toxicity management is ideal—particularly in terms of steroid frequency and proximity to IP administration.
The nausea and vomiting associated with high-dose cisplatin and 5-FU may be acute (onset 1–4 hours after infusion) or delayed (begins or persists ≥ 24 hours after infusion). Prophylactic use of steroids on Day 1 to combat the acute nausea and vomiting are allowed. Alternatives to steroid
VentiRx Pharmaceuticals Incorporated 56Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
use on days 2–4 should be employed, if possible. However, use of steroids within 72 hours of IP administration is prohibited.
Non-steroidal antiemetic treatment options include both short- and long-acting 5-HT3 antagonists (e.g., ondansetron, palonosetron), short- and long-acting NK1 receptor antagonists (e.g., Emend/aprepitant, fosaprepitant), benzodiazapines, diphenhydramine, and metoclopramide.
7.6.2 Fever with Neutropenia
VTX-2337 has not been associated with hematologic toxicity such as myelosuppression or neutropenia. Transient, aseptic grade 1 and grade 2 (up to 40°C/104°F) pyrexia driven by cytokines is a common side effect of VTX-2337, occurring in approximately 50% of treated subjects. Grade 3 fever (> 40°C/104°F) has been observed in approximately 8% of treated subjects. The characteristic VTX-2337-related fever has an onset 3–8 hours after dosing, lasts approximately 24 hours, and is typically experienced following each dose. This fever may or may not be accompanied by flu-like symptoms such as shaking, chills, and myalgia. In contrast, in a Phase 3 study of cetuximab plus platinum-5-FU, more than 25% of subjects experienced grade 3 or 4 neutropenia and 6% of subjects experienced febrile neutropenia.[12] As the neutrophil nadir from platinum-5-FU therapy typically occurs between days 10 and 23 of the treatment cycle, it is expected that a fever induced by VTX-2337 may overlap with a period of grade 3–4 neutropenia induced by platinum-5-FU.
It may be difficult to differentiate between IP-related aseptic fever in a patient with incidental neutropenia and the presumed infectious state of classic febrile neutropenia. The former would be expected to involve the characteristics of VTX-2337-related fever noted above (i.e., fever following each dose with an onset and resolution within 24 hours) and would not be associated with findings of active infection.
Ultimately, investigators should rely upon clinical judgment and follow institutional guidelines when dealing with fever in the setting of neutropenia. Primary or secondary prophylaxis with granulocyte colony growth factor (G-CSF) is permitted in order to manage the neutropenia expected from platinum-5-FU therapy. Recommendations for evaluation and standard antibiotic therapy found in guidelines for inpatient or outpatient management of neutropenic fever may be utilized.
The reporting of adverse events with respect to fever in the setting of neutropenia should accurately reflect the investigator’s assessment of the etiology. If the investigator determines that the events most likely represent the presumed infectious state of classic febrile neutropenia, the single event term of “febrile neutropenia” should be used. However, if the investigator determines that the events most likely represent IP-related aseptic fever in a patient with
VentiRx Pharmaceuticals Incorporated 57Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
incidental neutropenia, the event should be reported using the two event terms of “fever” and “neutrophil count decreased”.
7.7 Investigational Product Accountability
VentiRx Pharmaceuticals will provide an adequate supply of IP for the study population and protocol requirements. Drug supplies must be kept in an appropriate, secure area (e.g., locked pharmacy) and stored in accordance with the conditions specified in this protocol, the pharmacy manual, and on the IP labels.
Drug supplies are to be used only in accordance with this protocol, pharmacy manual, and under the personal supervision of the Principal Investigator or under the supervision of a sub- investigator who is responsible to the investigator. IP may be administered only to eligible subjects who are randomized in the study. The Principal Investigator is accountable for all used and unused investigational drug. The investigator agrees not to destroy any used, partially used, or unused investigational drug supplies unless otherwise directed by VentiRx Pharmaceuticals or its representatives. Upon written notification, the investigator will ship unused IP according to instructions provided or will destroy unused IP according to institutional standards.
A master drug log must be maintained for all IP vials received, dispensed (including the subject’s ID number, the subject’s initials, and the dates each vial is dispensed) and returned or destroyed. In addition, a subject-specific record of each vial administered, including the date and identification number of each vial, will be maintained with the case file for each subject. Any discrepancy in the drug distribution logs (master log and subject logs) must be explained in detail.
8.0 ADVERSE EVENTS
The following sections describe the minimum requirements for assessing and reporting AEs, including SAEs and serious suspected adverse reactions, for subjects participating in trial VRXP-A202. The investigator is additionally responsible for complying with all local institution and IRB/IEC requirements for reporting AEs.
8.1 Definitions8.1.1 Adverse Event (AE)
An adverse event is defined as any untoward medical occurrence associated with the use of a drug in humans, whether or not considered drug-related. An AE can therefore be any unfavorable and unintended sign, symptom, or disease which is temporally associated with the use of the investigational drug, whether or not considered related to (i.e., to have a causal relationship with) the IP.
VentiRx Pharmaceuticals Incorporated 58Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
AEs include exacerbation of a pre-existing illness, an increase in frequency or intensity of a pre- existing episodic event or condition, a condition detected or diagnosed after IP administration even though it may have been present prior to the start of the study, or a continuous persistent disease or symptom present at baseline that worsens following the start of the study.
Medical conditions and diseases that are present before Cycle 1 Day 1 are only considered AEs if they worsen after starting treatment with Cycle 1 Day 1. Any medical condition with an onset or diagnosis before Cycle 1 Day 1 will be included in the subject’s medical history. Abnormal laboratory values or test results constitute AEs if they induce clinical signs or symptoms or if they require intervention or therapy.
8.1.2 Serious Adverse Event (SAE)
An AE or suspected adverse reaction is considered ‘‘serious’’ if, in the view of either the investigator or sponsor, it results in any of the following outcomes:
• Death
• A life-threatening1 adverse event
• Inpatient hospitalization or prolongation of existing hospitalization,
• A persistent or significant incapacity or substantial disruption of the ability to conductnormal life functions
• A congenital anomaly/birth defect
Important medical events that may not result in death, be life-threatening, or require hospitalization may be considered serious when, based upon appropriate medical judgment, they may jeopardize the subject and may require medical or surgical intervention to prevent one of the outcomes listed in this definition. Examples of such medical events include allergic bronchospasm requiring intensive treatment in an emergency room or at home, blood dyscrasias or convulsions that do not result in inpatient hospitalization, or the development of drug dependency or drug abuse.
8.1.3 Dose-Limiting Toxicities (DLT)
DLTs were assessed for all subjects until six subjects randomized to receive VTX-2337 received one cycle of treatment and the DSMB completed the assessment of the starting dose. (§9.2.2)
1 An AE or suspected adverse reaction is considered “life-threatening” if, in the view of either the investigator or sponsor, its occurrence places the patient or subject at immediate risk of death. It does not include an AE or suspected adverse reaction that, had it occurred in a more severe form, might have caused death.
VentiRx Pharmaceuticals Incorporated 59Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Results from the initial DSMB evaluation concluded that the study can continue as planned at the dose level of 3.0 mg/m2 and that DLT recording criteria could be lifted.
A DLT is defined as any IP-related adverse event, occurring during Cycle 1 (Week 1–3), which meets the following criteria:
• Any ≥ grade 4 hematologic toxicity
• Any ≥ grade 3 non-hematologic toxicity (including injection-site reaction), with theexception of:
— Grade 3 dermatologic toxicities
— Grade 3 hypersensitivity reaction
• Diarrhea, nausea, or vomiting will only be considered a DLT when ≥ grade 3 toxicityoccurs despite adequate anti-emetics or anti-diarrhea medications
• Treatment delay due to toxicity lasting greater than 21 days
• Death
“IP related” refers to events that are possibly or probably related to the administration of IP or the combined treatment regimen of IP, platinum, 5-FU, and cetuximab, and not clearly attributed to platinum, 5-FU, cetuximab alone, or other causes.
8.2 Reporting Requirements
Information regarding all AEs, whether volunteered by the subject, discovered via questioning by the investigator or clinical personnel, or identified through physical examination, laboratory test or other means will be collected from the first dose of study required medication administered on Cycle 1 Day 1 until the End of Treatment visit or 7 days after the last dose of any study medication, whichever is later. Suspected adverse reactions (i.e. AEs that are assessed as related to IP) which are ongoing will be followed until resolution or until grade ≤ 2 and stabilized. Suspected adverse reactions may be reported at any time.
Information collected regarding each AE will include, but is not limited to (1) duration (start and stop dates), (2) severity as delineated in §8.3, (3) relationship to the investigational drug (“causality”) as described in §8.5 (serious adverse events only), (4) any action taken and (5) outcome. Whenever possible, AEs should be described in terms of a change in the baseline status (e.g., “increased frequency of migraines”) or with a diagnosis or summary term in place of individual clinical signs or symptoms (e.g., “upper respiratory infection” vs. “runny nose”, “sneezing” and “cough”).
VentiRx Pharmaceuticals Incorporated 60Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
8.2.1 Serious Adverse Events
The investigator must immediately (≤ 24 hours of clinical site personnel becoming aware of the event) report to the study’s medical monitor any SAE—whether or not considered drug related, including those listed in the IB—and must include an assessment of whether there is a reasonable possibility that the investigational drug caused or otherwise contributed to the event. The site will provide the initial notification to PRA Drug Safety via fax or email on the required SAE Report Form, which must be signed by the investigator. Follow-up information or new information regarding an ongoing SAE must be provided promptly to PRA Drug Safety.
PRA Drug SafetyPhone: +1 (800) 772-2215
+1 (434) 951-3489Fax: +1 (888) 772-6919
+1 (434) 951-3482email: [email protected]
The investigator is responsible for notifying the IRB/IEC or other appropriate committees of all SAEs in accordance with institutional and IRB/IEC policies.
8.2.2 Dose Limiting Toxicities
As described in §9.2.2, DLTs were assessed for all subjects until the DSMB has completed the assessment of the starting dose. During this DLT assessment period, once the investigator has determined a DLT has occurred, the DLT required reporting within 48 hours to allow the DSMB to review DLTs in a timely manner.
8.3 Criteria for Determining Adverse Event Severity
AEs will be categorized and severity will be graded according to the NCI-CTCAE version 4.03.
Note that “seriousness” and “severity” are distinct concepts. “Serious” is a term applied to an AE that meets specific regulatory requirements; it is typically associated with events that pose a threat to the subject’s life or functioning. “Severity” refers to the AE intensity classification. A severe AE may be of minor medical significance (e.g. grade 3 headache), while an AE that is graded as mild in severity may be serious (e.g. grade 1 stroke requiring overnight hospitalization).
VentiRx Pharmaceuticals Incorporated 61Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
8.4 Criteria for Determining Adverse Event Expectedness
An AE or suspected adverse reaction is considered ‘‘unexpected’’ if it is not listed in the IB or is not listed at the specificity or severity that is observed. The sponsor or its representative will be responsible for determining the expectedness of adverse events.
For example, under this definition, hepatic necrosis would be unexpected (by virtue of greater severity) if the IB referred only to elevated hepatic enzymes or hepatitis. Similarly, cerebral thromboembolism and cerebral vasculitis would be unexpected (by virtue of greater specificity) if the IB listed only cerebral vascular accidents. ‘‘Unexpected’’—as used in this definition—also refers to AEs or suspected adverse reactions that are mentioned in the IB as occurring with a class of drugs or as anticipated from the pharmacological properties of the drug, but are not specifically mentioned as occurring with the particular drug under investigation.
Therefore, "unexpected" also refers to an AE or suspected adverse reaction that has not been previously observed (i.e. included in the IB) rather than from the perspective of such an experience not being unanticipated from the subject’s disease state.
8.5 Criteria for Determining Adverse Event Causality
The following categories for determining the relationship of an AE to the IP are as follows:
None: The AE is temporally independent of the administration of IP and/or canbe readily attributed to other factors such as the subject’s clinical state, environmental factors, or concomitant drugs or therapies
Possible: The AE follows a reasonable temporal sequence from administration of IPand cannot readily be explained by the subject’s clinical state, environmental factors, or concomitant drugs or therapies
Probable: The AE follows a clear temporal sequence from administration of IP andis unlikely to be related to the subject’s clinical state, environmental factors, or concomitant drugs or therapies. The AE ceases with discontinuation of the drug and reoccurs after restarting, if applicable
Note that the term “suspected adverse reaction” is used to describe an AE for which there is a reasonable possibility that the IP caused the adverse event (i.e. an event that is assessed as ‘possibly’ or ‘probably’ caused by administration of IP).
VentiRx Pharmaceuticals Incorporated 62Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
8.6 Expedited Reporting of Serious Adverse Events
Regulations require that VentiRx Pharmaceuticals or its representatives to report any suspected adverse reactions1 that are both serious (§8.1) and unexpected (§8.4). Such events must be reported to the FDA, applicable regulatory authorities, and all participating investigators (i.e., all investigators to whom VentiRx is providing drug under its INDs or under any investigator’s IND) within 15 calendar days after VentiRx or its representative receives the information and determines that it qualifies for reporting. Such notification must occur within 7 calendar days if the SUSAR was fatal or life-threatening.
Therefore, once the investigator has determined that an SAE has occurred, it is important to adhere to the reporting timeframes outlined in §8.2.1. After receiving the investigator’s SAE report, including the investigator’s assessment of causality, VentiRx or its representatives will also assess the event for seriousness and the relationship to IP and will determine if the event was unexpected.
Investigational New Drug Safety Reports (INDSRs), or equivalent, will be reported to FDA and applicable local regulatory authorities by VentiRx Pharmaceuticals or its representatives; copies of the report will be distributed to clinical investigators. The investigator is responsible for notifying the relevant IRB/IEC of all INDSRs in accordance with institutional and IRB/IEC policies.
9.0 STATISTICAL PLAN9.1 Statistical Considerations
All analyses will use SAS® version 9.1.3 or higher (SAS Institute, Inc., Cary, NC). Summary tables will be organized by treatment group: Combination Arm (SOC plus VTX-2337) versus Control Arm (SOC plus placebo). All available scheduled data for the safety or efficacy populations will be used in the analyses. Important CRF data will be included in data listings for all subjects who are randomized on the study. Missing data will not be imputed, except via censoring in survival analyses.
In keeping with ICH E9, center effect will not be included in the analysis models as it is recognized that there will be limited numbers of subjects per center in this trial. However, randomization stratification factors and/or their interaction terms with treatment may be explored.
1 A suspected adverse reaction is an adverse event for which there is a reasonable possibility that the investigational drug caused the adverse event. For the purposes of investigational new drug (IND) safety reporting, “reasonable possibility” means there is evidence to suggest a causal relationship between the drug and the adverse event.
VentiRx Pharmaceuticals Incorporated 63Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Unless otherwise noted, categorical data will be presented using counts and percentages, with the number of subjects in the analysis population by treatment group as the denominator for percentages. Percentages will be rounded to one decimal place. Continuous data, unless otherwise noted, will be summarized using the number of observations (n), mean, standard deviation, median, minimum, and maximum. The primary test on PFS, secondary test on OS, and all other statistical tests will be conducted using a 1-sided significance level of 0.10.
9.1.1 Sample Size and Operating Characteristics
The total sample size is approximately 175 subjects (estimated 88 per treatment group). In the event the starting dose of VTX-2337 is reduced (see §9.2.2), the sample size for the trial will be adjusted so that 175 subjects will be treated at the modified starting dose. Similarly, in the event there are subjects who discontinue the study prior to receiving their first dose of IP, the sample size will be adjusted so that 175 subjects who receive at least one dose of VTX-2337/Placebo are enrolled. A dropout rate of approximately 10% over the life of the study is assumed.
The timing of the primary analysis will be event-driven. One hundred thirty-four (134) PFS events are required to detect a hazard ratio (HR) of 0.67 with 85% power at a 1-sided alpha of 0.10. This HR represents a 50% improvement in PFS, which translates to an increase in median PFS from 6 months (control arm) to 9 months (combination arm). It is estimated that a population of 175 subjects accrued over 18 months will need to be followed for an additional 9 months to provide the requisite number of PFS events. The primary analysis will occur when 134 PFS events have accumulated or earlier, provided that the number of PFS events is sufficient for at least 80% power to detect a hazard ratio (HR) of 0.67 at a 1-sided alpha of 0.10.
The analysis of OS will be conducted when all randomized subjects have been followed for ≥ 12 months following enrollment of the final subject. It is estimated that 112 OS events will be accrued during this time, providing 72.8% power at a 1-sided alpha of 0.10 to detect a HR of 0.70. This HR represents a 30% reduction in the risk of death, and a 42.9% increase in the median OS. Assuming a median OS of 11 months in the control arm, the median OS in the combination arm will be 15.7 months.
9.1.2 Subject Population(s) for Analysis
The analysis populations are:
Intent to Treat (ITT) Population: The ITT population will include all randomized subjects in the study. This population will be used for efficacy analyses. If the randomized treatment arm differs from the actual treatment for a given subject, that subject will be analyzed according to the randomized treatment arm.
VentiRx Pharmaceuticals Incorporated 64Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Per Protocol (PP) Population: The PP population will include all subjects who have at least one tumor assessment after receiving at least one dose of IP and have no major protocol deviations that could impact efficacy assessments. This population will be defined in detail in the Statistical Analysis Plan (SAP) prior to final database lock and unblinding for the primary analysis.
Safety Population: The safety population will include all subjects who receive at least one dose of IP. This population will be used for safety analyses. If the randomized treatment arm differs from the actual treatment for a given subject, that subject will be analyzed according to the actual treatment arm.
Other analysis populations may be defined, if required, in the detailed SAP.
9.2 Statistical Methods
A detailed SAP will be finalized before the primary database lock and unblinding. This analysis plan may modify what is outlined in the protocol; however, any major modifications of the primary endpoint definition or its analysis will also be reflected in a protocol amendment.
9.2.1 Efficacy9.2.1.1 Primary Efficacy Endpoint
Review by a central radiologist, blinded to subject treatment assignments and independent from the clinical sites, will assess all tumor responses according to irRECIST. The resulting response data will serve as primary clinical efficacy data for the trial. Deaths on study will also contribute to the PFS endpoint. PFS is defined as the duration of time from randomization to time of PD or death, whichever comes first, or the last tumor assessment date for censored subjects.
The primary efficacy endpoint, PFS, will be summarized and displayed by treatment group using Kaplan-Meier methods (SAS® PROC LIFETEST). Point estimates (25th, 50th, and 75th percentiles) will be provided, along with a 1-sided 90% confidence interval (CI). Treatments will be compared for the ITT population using a stratified log-rank test, with randomization stratification factors included, as the primary analysis. The HR between the 2 study arms, as well as the associated 90% CI, will be presented using Cox proportional hazards regression (SAS® PROC PHREG) controlling for randomization stratification factors. Kaplan-Meier plots will be presented.
The primary analysis will be a stratified log-rank test (using the randomization stratification factors) comparing PFS between the 2 randomized arms in the ITT population.
VentiRx Pharmaceuticals Incorporated 65Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
9.2.1.2 Secondary Efficacy Endpoints
Secondary efficacy endpoints include:
• Overall survival (OS)
• PFS as assessed by independent central review based on RECIST v1.1: defined as theduration of time from randomization to time of progressive disease or death, whichever comes first, or the last tumor assessment date for censored subjects.
• PFS as assessed by investigators based on irRECIST.
• Tumor response based on irRECIST [19] and based on RECIST v1.1:
— Objective response rate (ORR)
— Duration of best response (DOBR)
— Disease control rate (DCR)
— Duration of disease control (DDC)
Overall Survival
OS will be measured from the date of subject randomization until death or the last follow up date for censored subjects. OS will be summarized and analyzed in the same manner as PFS.
Tumor response
For each secondary endpoint involving tumor responses, assessments per the central-radiology review will be presented and analyzed as primary.
The number and percent of subjects achieving objective response (CR or PR) will be tabulated for ITT population subjects treated with SOC plus VTX-2337 versus those treated with SOC plus placebo. The number and percent of subjects achieving disease control (SD, PR, or CR) will be tabulated in the same manner. As well, the number and percent of subjects exhibiting each level of best tumor response (CR, PR, SD, PD, or missing) will be presented by treatment group for the ITT population. Stratified Cochran-Mantel-Haenszel mean scores tests (SAS® PROC FREQ) will be used to compare tumor response rates between the 2 study arms while controlling for randomization stratification factors. In addition, maximum change in TMTB from baseline in ITT population subjects will be presented graphically.
Duration of best response—measured in days—will be defined as the duration of time from the date measurement criteria are first met for CR, or PR (if CR is never met), until the first date that PD is confirmed by the central radiology review, or death, whichever comes first, or the last
VentiRx Pharmaceuticals Incorporated 66Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
tumor assessment date for censored subjects. DOBR will be calculated only for responding subjects (CR or PR) as assessed by irRECIST and by RECIST v1.1. DOBR will be summarized and displayed by treatment group using Kaplan-Meier methods. Point estimates (25th, 50th, and 75th percentiles) will be provided, along with 1-sided 90% CIs.
Duration of disease control—measured in days—will be defined as the duration of time from the date measurement criteria are first met for CR, PR, or SD to the first date that PD is confirmed by the central radiology review, or death, whichever comes first, or the last tumor assessment date for censored subjects. DDC will be calculated only for subjects who achieve disease control (CR, PR or SD) as assessed by irRECIST and by RECIST v1.1. DDC will be summarized and displayed in the same manner as DBR.
9.2.1.3 Sensitivity Analysis
Analyses on the PP population will be performed for the primary and the secondary efficacy endpoints and serve as supportive analyses for the ITT analyses.
9.2.2 Safety
AEs, vital signs, ECG, and safety laboratory data (peripheral blood hematology, serum chemistry, and urinalysis) will be presented descriptively. All AEs, vital signs, ECGs, and clinical laboratory abnormalities will be presented. Safety data will be presented in tabular and/or graphical format and summarized descriptively by treatment group and time point, where appropriate. Descriptive statistics will be shown for baseline, scheduled visits, and the change from baseline to these visits, as applicable.
A DSMB of at least three independent members with expertise in the patient population, statistics, and/or clinical research will be appointed to monitor subject safety data while the trial is ongoing. The DSMB will meet at predetermined intervals set forth in the DSMB Charter— approximately every 6 months—to review toxicities and serious and/or unexpected adverse events. The DSMB will primarily evaluate safety data; efficacy data will only be reviewed in the event of a serious safety concern. Minutes for all meetings will be generated.
To address any new or unexpected safety issues, the first DSMB meeting occured after an unblinded statistician confirmed that 6 subjects, who had been randomized to receive VTX-2337, had completed one cycle of therapy. The purpose of this meeting was to evaluate any DLTs or any acute, unexpected, or synergistic toxicities associated with the combination of VTX-2337, platinum, 5-FU, and cetuximab. Results from the initial DSMB evaluation concluded that the study can continue as planned at the dose level of 3.0 mg/m2 and that DLT recording criteria could be lifted.
VentiRx Pharmaceuticals Incorporated 67Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Refer to §8.1.3 for DLT definition.
Adverse Events
AEs will be coded using the Medical Dictionary for Regulatory Activities (MedDRA). All AEs will be listed. Treatment-emergent AEs (TEAEs) are those which first occur or increase in severity or relationship to IP after the first dose of IP. AEs with missing date of onset will be considered treatment-emergent. The number and percent of patients reporting TEAEs will be tabulated by system organ class and preferred term and categorized by treatment group. AEs will be further classified by severity and relationship to treatment in tabulations. Tables and/or narratives of any on-study death, or SAE, as well as early withdrawals because of AEs, will be provided. The relationship between drug exposure and adverse events will be evaluated qualitatively.
Electrocardiogram
Descriptive statistics for QRS, QTc, QT and HR will be presented for baseline, End of Treatment visit, and the change from baseline to End of Treatment. The incidence of outliers in absolute QTcF and QTcB intervals (> 450 to ≤ 480, > 480 to ≤ 500, and > 500 msec) and the absolute uncorrected QT intervals (> 500 msec) at End of Treatment, as well as changes from baseline in QTcF and QTcB (> 30 to ≤ 60 and > 60 msec) will be summarized by treatment group.
Laboratory Values
Laboratory test results will be converted to International System of Units (SI) units. Abnormal laboratory results will be graded with the NCI-CTCAE (Version 4.03) standard. Descriptive statistics will be shown for baseline, scheduled visits, and the change from baseline to these visits. Shift summaries of NCI-CTCAE grade from baseline to worst post-baseline result will be provided by treatment group. In addition, selected parameters will be displayed graphically over time by treatment group.
9.2.3 Other Data
Demographics, Baseline Characteristics, and Disposition
Demographic information and baseline characteristics will be summarized for the ITT population. Demographic data will be summarized by treatment group and will include summary statistics for age, age group, race, sex, height, and weight. General medical history data and oncology history data will also be tabulated by treatment group using counts and percentages. Oncology history will include prior anticancer interventions, histological or cytological confirmation of SCCHN, tumor staging according to the TNM Classification of Malignant
VentiRx Pharmaceuticals Incorporated 68Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Tumors, HPV status (for patients with oropharyngeal carcinoma only), prior systemic therapy for SCCHN (Yes or No), and ECOG performance status (0 or 1).
The disposition of all randomized subjects will be summarized. These data will include the number of subjects enrolled (randomized), receiving study treatment, assigned to each dose group, and prematurely discontinuing from the study and the reason(s) for premature discontinuation.
Extent of Exposure
Dosing data will be summarized by treatment group to include duration of treatment (days), cumulative dose and dose intensity, and number (%) of patients with dose modifications.
Concomitant Medications
Concomitant medications will be presented in data listings and coded using the WHODRUG dictionary. Concomitant medications will be summarized by treatment group and preferred drug names.
Translational Research Assessments
Statistical evaluation of translational research assessments (§4.2.3) will be described in SAP.
9.3 Schedule of Analyses
The primary analysis will be conducted when 134 PFS events have accrued on study. The secondary efficacy analysis (OS) will be conducted approximately 12 months following randomization of the last subject. It is anticipated that approximately 112 OS events will have occurred at the time of the secondary analysis on OS. Two database locks will be scheduled for the 2 analyses, at the time points described above. Additional analyses may be performed and will be outlined in the SAP.
9.4 Termination Criteria
Enrollment in the study will end when at least 175 subjects have been randomized, to provide approximately 88 subjects per treatment group. Subjects who discontinue the study prior to receiving their first dose of IP will be replaced. A dropout rate of approximately 10% over the life of the study is assumed. The end of the trial is defined as the date when the final analysis of the OS endpoint is completed.
VentiRx Pharmaceuticals Incorporated 69Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
9.5 Deviation Reporting
Major protocol deviations will be presented in a listing.
10.0 REGULATORY, QUALITY, AND ADMINISTRATIVE REQUIREMENTS10.1 Trial Conduct
This study will be conducted in compliance with the protocol issued by VentiRx Pharmaceuticals and approved by the IRB/IEC and according to FDA regulations, applicable Competent Authorities and Guidelines for Good Clinical Practice (21 CFR §312 and ICH Guidance E6). No deviation from the protocol will be implemented without the prior approval from the study’s sponsor or its representative, as well as review and approval from the IRB/IEC except where it may be necessary to eliminate an immediate hazard to a research subject. In such cases, the deviation will be reported to the IRB/IEC and VentiRx Pharmaceuticals, or their respresentative, as soon as possible.
10.2 Ethical Considerations10.2.1 Informed Consent
Patients meeting the criteria set forth in the protocol may be offered the opportunity to participate in this study. Candidate subjects or their legal guardians will receive a comprehensive explanation of the study, including the nature and investigational status of the IP, any known previously experienced adverse reactions, alternative therapies available and other factors which are part of obtaining appropriately informed consent. Patients will be given the opportunity to ask questions of qualified personnel who are knowledgeable about the study and provide adequate time to consider whether or not to participate.
Informed consent will be documented with an ICF that has been approved by the institution’s IRB/IEC. The ICF is to be signed and dated by the subject or subject’s legally authorized representative, by the person who conducts the consent process and any additional signatures required by the institution’s IRB/IEC. The original signed ICF will be filed in the subject’s medical record and a copy of the signed ICF will be given to the subject or the subject’s legally authorized representative. The subject’s medical record should contain a notation that written informed consent was obtained and a written description of the consent process.
Any changes to the ICF (e.g., in the event of a protocol amendment that changes the study’s procedures or alters its scope, or if significant new information regarding the safety or efficacy of the investigational drug becomes available) must be reviewed and approved by the IRB/IEC. The revised ICF must be used to re-consent any subject currently enrolled in the study who is affected by the change.
VentiRx Pharmaceuticals Incorporated 70Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
10.2.2 Institutional Review Board/Ethics Committee Approval
The protocol and all relevant supporting materials, including the IB and Informed Consent Form, must be submitted to the appropriate IRB/IEC for review and approval. A copy of the IRB/IEC’s written approval must be provided to the study’s sponsor or its representative prior to initiation of the study and commencement of the subject screening and enrollment. The IRB/IEC should be informed by the investigator of the study’s progress and provide written documentation of the periodic review and ongoing approval according to IRB/IEC policies.
Any changes in the study protocol, revisions to the ICF, and all unanticipated problems involving risks to human subjects (e.g., SAEs occurring at the clinical site, INDSRs) must be reported promptly to the IRB/IEC and according to institutional and IRB/IEC requirements. Written approval from the IRB/IEC must be obtained prior to implementation of any change(s), if applicable.
10.2.3 Subject Privacy
The investigator, CRO, VentiRx Pharmaceuticals, and representatives of VentiRx Pharmaceuticals shall comply with all applicable local, state and federal privacy laws. The medical records of participating subjects are considered confidential and disclosure to third parties other than those noted below is prohibited.
The medical records of participating study subjects and all data generated as a result of participation in this study are to be available for review upon request by the FDA or other regulatory authorities, VentiRx Pharmaceutics or its representatives, and by the IRB/IEC. The IRB/IEC-approved ICF must clearly indicate that the subject’s medical records will be inspected by said parties and permission for such review is a requirement for study participation.
10.3 Investigator Responsibilities and Requirements
By agreeing to participate in this clinical trial, the Principal Investigator and all subinvestigators agree to perform the study in accordance with all stipulations of the protocol, the FDA Code of Federal Regulations (21 CFR Parts 11, 50, 54, 56 and 312), applicable local regulation(s) and ICH Guidelines for GCP (E6).
Prior to initiation of the study the Principal Investigator must, at minimum, provide VentiRx or its representative with the following documentation:
• Signed clinical trial agreement
• Signed Principal Investigator Protocol Agreement
VentiRx Pharmaceuticals Incorporated 71Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
• Signed FDA Form 1572 or equivalent
• Curriculum Vitae of the Principal Investigator
• Current medical license(s) for the Principal Investigator
• Copy of written IRB/IEC approval for the study and informed consent form
• Financial disclosure for the Principal Investigator
The Principal Investigator is responsible for complying with all commitments as delineated in Box 9 of FDA form 1572 and/or local regulations.
10.4 Data Identification, Handling, and Record Keeping10.4.1 Source Documentation
Adequate and accurate case histories, which record all data and observations relevant to the clinical investigation, should be prepared and maintained for each subject screened or randomized in the study. Such source documentation includes all original documents or medical records regarding the subject’s participation in the study, including medical history, notes from the physician or nurse, the subject’s laboratory reports, imaging studies, electrocardiogram tracings, hospital records and details regarding the distribution of the investigational drug.
10.4.2 Case Report Forms and Electronic Data Capture
The investigator will be provided with access to a secure, web-based system that is compliant with 21 CFR §11 for capturing and reporting all study-related data ( EDC). Such data will be entered into the EDC system by the investigator and site personnel in a timely and accurate manner. The investigator must review all submitted data for accuracy and consistency with the protocol and authorize the data for each subject upon completion.
All required fields on the electronic case report forms (CRFs) must be filled in and 100% of the information collected on CRFs must be verifiable through review of the original source documentation.
10.4.3 Essential Documents
The Principal Investigator and clinical site personnel are responsible for maintaining an organized, comprehensive file of all essential documents required to demonstrate compliance with regulatory requirements. Such documents include, but are not limited to:
• Protocol with all amendments, signed Principal Investigator Protocol Agreement(s) andinformed consent form(s)
VentiRx Pharmaceuticals Incorporated 72Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
• IB, including all updates
• Copy of the signed FDA Form 1572
• CVs and medical licenses for the Principal Investigator and subinvestigators
• IRB/IEC approval of the protocol and amendment(s), informed consent form(s) and anyother study-related materials
• IRB/IEC membership list or Letter of Assurance
• Subject Screening and Enrollment Log, which may be obtained from EDC
• IRB/IEC submissions of SAEs that have occurred at the institution and of INDSRsprovided by the study’s sponsor
• Laboratory certifications and reference ranges
• Significant correspondence from VentiRx Pharmaceuticals or CRO
• Other documents as required by local regulatory authorities
These files must be available for inspection by VentiRx Pharmaceuticals, their representatives, the IRB/IEC, or regulatory authorities at any time.
10.4.4 Record Retention
All study related documentation noted in §10.4.1, §10.4.2 and §10.4.3 above must be maintained in accordance with FDA and local regulations. For sites in the US, as described in 21 CFR §312.62, the investigator will retain all such study records for a period of 2 years after marketing approval is received for VTX-2337, or for 2 years after all clinical and product development of VTX-2337 is discontinued. Investigators should not destroy any records relating to this study without prior approval from VentiRx Pharmaceuticals.
10.5 Quality Control and Quality Assurance10.5.1 Site Training and Monitoring Procedures
Prior to the initiation of the study, personnel from the sponsor or its representatives will meet with the investigator and clinical staff to review and discuss the protocol, the investigational drug, study procedures, drug accountability, adverse event reporting, ICH/GCP guidelines, CRF completion guidelines, record keeping and administrative requirements, monitoring requirements, and the ability of the site to adequately conduct the protocol. During the course of the study, representatives from the sponsor will provide additional study-specific training to site staff upon request by the investigator, in response to a change in key clinical site staff, or if
VentiRx Pharmaceuticals Incorporated 73Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
issues with study conduct or GCP compliance are observed during the course of routine monitoring visits.
A representative from VentiRx Pharmaceuticals will visit the clinical site periodically to monitor adherence to the protocol, to review and retrieve study-related data, and/or documents. The frequency of monitoring visits depends on the rate of enrollment at the site and the investigator will permit the sponsor’s representative to monitor the study as frequently as the sponsor deems necessary to determine that protocol adherence and data collection are acceptable. The monitor will be permitted full access to subjects’ complete medical records. CRFs will be reviewed and compared to the subject’s case history to ensure the accuracy of the reported data and that key data are collected and recorded as specified by the protocol. Other study records, such as essential regulatory documents, subject screening log, and drug disposition logs will also be inspected.
10.5.2 Data Management Procedures
VentiRx Pharmaceuticals or its designee will prepare guidelines for database setup, data review, quality control, and database lock at the conclusion of the study—including procedures for electronic edit checks. CRF Completion Guidelines will be prepared to guide the data entry activities completed by the sites. The database will be validated following established procedures. Electronic databases that hold subject study data will conform to 21 CFR §11 requirements.
10.5.3 Auditing Procedures
VentiRx Pharmaceuticals and the applicable Competent Authorities maintain the right to conduct audit(s) at the clinical site.
VentiRx Pharmaceuticals Incorporated 74Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
11.0 SUPPLEMENTS11.1 ECOG Performance Status Assessment
Grade ECOG0 Fully active, able to carry on all pre-disease performance without restriction1 Restricted in physically strenuous activity but ambulatory and able to carry out work of a light or
sedentary nature, e.g., light house work, office work2 Ambulatory and capable of all selfcare but unable to carry out any work activities. Up and about
more than 50% of waking hours.3 Capable of only limited selfcare, confined to bed or chair more than 50% of waking hours.4 Completely disabled. Cannot carry on any selfcare. Totally confined to bed or chair.5 Dead
11.2 Baseline Tumor Evaluation and Categorization: RECIST v1.111.2.1 Categorization of Tumors
All tumor lesions will be categorized at baseline as either one of the following:
• Measurable: lesions that can be accurately measured in at least one dimension (longestdiameter to be recorded) as ≥ 10 mm for soft tissue lesions and ≥ 15 mm in short axis for lymph nodes with CT or MRI scan. All tumor measurements must be recorded in decimal fractions of centimeters.
• Non-measurable: All other lesions (or sites of disease), including small lesions (longestdiameter < 10 mm or pathological lymph nodes with ≥ 10 to < 15 mm short axis), are considered non-measurable disease. Leptomeningeal disease, ascites, pleural/pericardial effusions, lymphangitis cutis/pulmonitis, inflammatory breast disease, and abdominal/pelvic masses (identified by physical exam and not CT or MRI) are considered as non-measurable.
11.2.2 Special considerations regarding lesion measurability
Bone lesions: Lytic bone lesions or mixed lytic-blastic lesions, with identifiable soft tissue components, that can be evaluated by CT or MRI can be considered as measurable lesions if the soft tissue component meets the definition of measurability described above. Blastic bone lesions are non-measurable.
Cystic lesions that meet the criteria for radiographically defined simple cysts should not be considered as malignant lesions (neither measurable nor non-measurable) since they are, by definition, simple cysts. “Cystic lesions” thought to represent cystic metastases can be
VentiRx Pharmaceuticals Incorporated 75Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
considered as measurable lesions, if they meet the definition of measurability described above. However, if non-cystic lesions are present in the same subject, these are preferred for selection as target lesions.
Lesions with prior local treatment (e.g., tumor lesions that are situated in a previously irradiated area) will not be considered measureable unless progression is documented or a biopsy is obtained to confirm persistence at least 90 days following completion of radiation therapy.
11.2.3 Methods of Assessment
The same method of assessment and the same technique should be used to characterize each identified and reported lesion at baseline and during follow-up.
All measurements should be taken and recorded in metric notation using a ruler. All baseline evaluations should be performed as closely as possible to the beginning of treatment and never more than 28 days before the beginning of treatment.
Clinical lesions: Superficial clinical lesions measured by caliper or ruler will not be used to assess tumor response in this study.
Conventional CT and MRI: CT slice thickness should be ≤ 5 mm. MRI is also acceptable in certain situations (e.g., for body scans), but NOT lung.
Use of MRI remains a complex issue. MRI has excellent contrast, special and temporal resolution; however, there are many image acquisition variables involved in MRI, which greatly impact image quality, lesions conspicuity, and measurement. Furthermore, the availability of MRI is variable globally. As with CT, if an MRI is performed, the technical specifications of the scanning sequences used should be optimized for the evaluation of the type and site of disease. Furthermore, as with CT, the modality used at follow-up should be the same as was used at baseline and the lesions should be measured/assessed on the same pulse sequence parameters for all scanners, body parts, and diseases. Ideally, subsequent image acquisitions should use the same type of scanner and follow the baseline imaging protocol as closely as possible. If possible, body scans should be performed with breath-hold scanning techniques.
PET-CT: PET-CT is an acceptable means of imaging if the CT is of diagnostic quality and meets with the requirements in the Imaging Manual.
FDG-PET: FDG-PET will not be used to assess tumor response in this study.
Ultrasound: Ultrasound will not be used to assess tumor response in this study.
VentiRx Pharmaceuticals Incorporated 76Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Endoscopy, Laparoscopy: Endoscopy, Laparoscopy will not be used to assess tumor response in this study.
Cytology, Histology: In rare cases, these techniques can be used to differentiate between PR and CR.
It is mandatory to obtain cytological confirmation of the neoplastic origin of any effusion that appears or worsens during treatment when measurable disease has met criteria for response or stable disease. This confirmation is necessary to differentiate response or stable disease versus progressive disease, as an effusion may be a side effect of the treatment.
11.2.4 Baseline documentation of “Target” and “Non-Target” lesions
Target lesions: All measurable lesions, up to a maximum of 2 lesions per organ and 5 lesions intotal—representative of all involved organs—should be identified as target lesions and recorded and measured at baseline. Target lesions should be selected on the basis of their size (lesions with the longest diameter), be representative of all involved organs and in addition should be those that lend themselves to reproducible repeated measurements. It may be the case that, on occasion, the largest lesion does not lend itself to reproducible measurement, in which circumstance the next largest lesion which can be reproducibly measured should be selected.
The sum of the diameters (long axis for non-nodal lesions, short axis for nodal lesions) of all target lesions will be calculated and reported as the baseline sum of diameters (baseline TMTB). If lymph nodes are to be included in the sum, then only the short axis is added into the sum. The baseline TMTB will be used as reference to further characterize any objective tumor regression in the measurable dimension of the disease.
Non-target lesions: All other lesions (or sites of disease), including any measurable lesions over and above the 5 target lesions, should be identified as non-target lesions and should also be recorded at baseline. Measurements of these lesions are not required, but the presence, absence, or in rare cases unequivocal progression of each should be noted throughout follow-up.
Malignant lymph nodes: To be considered pathologically enlarged and measurable, a lymph node must be ≥ 15 mm in short axis when assessed by CT scan (CT scan slice thickness≤ 5 mm). At baseline and in follow-up, only the short axis will be measured and followed.
VentiRx Pharmaceuticals Incorporated 77Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
11.3 Response Assessment: immune-related RECIST (irRECIST)
As previously noted, this study will assess tumor response with an immune-related modification of RECIST v1.1 (referred to as irRECIST) as well as by RECIST v1.1.
Determination of response via irRECIST will take into consideration all target and non-target lesions.
11.3.1 Total Measured Tumor Burden
TMTB is established at baseline as the sum of the longest diameters (SOD)—the shortest axis should be used for lymph nodes—of all target lesions (≤ 2 lesions per organ, ≤ 5 lesions total). At each subsequent TA, the SOD of new, measurable lesions (≥ 10 mm [lymph nodes ≥ 15 mm
in shortest diameter]; ≤ 2 new lesions per organ, ≤ 5 new lesions total) is added to the SOD of the target lesions to provide the updated TMTB:
TMTB = SOD target lesions + SOD new, measurable lesions
If there are more than 2 new lesions per organ or more than 5 new lesions total, the lesions added to the TMTB should be selected on the basis of their size (i.e., lesions with the longest diameter should be selected).
Percentage changes in TMTB at each TA describe the size and growth kinetics of both old and new, measurable lesions as they appear. At each TA, the response in TMTB is defined as follows:
• Complete Response (irCR): Complete disappearance of all target and new, measurablelesions, with the exceptions of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
11.3.2 Response in Non-Target Lesions
The presence of non-target lesions is established at baseline; at each TA, the presence of any new, non-measurable lesions is assessed. The presence of new, non-measurable lesions will rule out an overall response of irCR. An increase in the size or number of new, non-measurable lesions does not necessarily imply an overall response of irPD; if these lesions become
VentiRx Pharmaceuticals Incorporated 78Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
measurable (≥ 10 mm [lymph nodes ≥ 15 mm in shortest diameter]; up to 2 new lesions per organ, total 5 new lesions) at a subsequent TA, their measurement will, at that point, start to contribute to the TMTB.
The response in non-target lesions is defined as follows:
• Complete Response (irCR): Complete disappearance of all non-target lesions
• non-irCR/non-irPD: Non-target lesions do not meet the criteria for irCR or irPD
• Progressive Disease (irPD): Unequivocal increase in the number or size of non-targetlesions. To achieve unequivocal progression of non-target lesions, there must be a substantial worsening of non-target disease of a magnitude that, according to the treating physician, warrants a change in anticancer therapy
NOTE: Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing lesions) should be considered irSD and treatment may continue until the next scheduled assessment.
11.3.3 Overall Response
The overall response (OR) according to irRECIST is derived from the responses in TMTB as well as the presence of any non-target lesions as follows:
• Complete Response (irCR): Complete disappearance of all lesions (whether measurableor not); lymph nodes must decrease to < 10 mm in shortest dimension
• Partial Response (irPR): Decrease in TMTB ≥ 30% relative to baseline
• Stable Disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD
• Progressive Disease (irPD): Increase in TMTB ≥ 20% relative to nadir
The immune-related best overall response (irBOR) is the best irRECIST OR over the study as a whole, recorded between the date of first dose until the last TA prior to subsequent anticancer therapy for individual subjects (Table 11). An assessment of disease progression at or before week 12 (unconfirmed irPD at week 12) will not preclude an irBOR of irCR, irPR, or irSD. Conversely, an assessment of irPD at or after Week 12 (confirmed irPD at week 12), will preclude a subsequent irBOR of irCR, irPR, or irSD. However, any post-progression clinical activity in subjects with irBOR of irPD may be summarized for exploratory purposes.
VentiRx Pharmaceuticals Incorporated 79Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Table 11: Best Overall Response (irBOR)
Target Lesions Baseline(Index) and New
Measurable LesionsNon-Target Lesions*
irRC Overall ResponseTotal Measurable Tumor
Burden (TMTB) Baseline Lesions Unequivocal New Lesions
irCR irCR No irCR
irCR irSD No irPR
irPR irCR or irSD No irPR
irSD irCR or irSD No irSD
irPD Any Yes or No irPD
Any Unequivocal Progression Yes or No irPD
Any Any Yes irPD
*Any increase in the size or number of non-measurable lesions does not necessarily imply an overall response of irPD. If new lesions become measureable (≥ 10 mm) at a subsequent TA, their measurement will at that point start to contribute to the TMTB. To achieve unequivocal progression of non-target lesions, there must be an overall level of substantial worsening in non-target disease that is of a magnitude that the treating physician would feel it is important to change therapy. Equivocal findings of progression of non-target lesions (e.g., small and uncertain new lesions; cystic changes or necrosis in existing locations) should be considered irSD and treatment may continue until the next schedule assessment.
Remainder of page intentionally left blank.
VentiRx Pharmaceuticals Incorporated 80Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
11.4 Response Assessment: RECIST v1.1
This study will assess tumor response with RECIST v1.1 as well as irRECIST.
Determination of response via RECIST v1.1 will take into consideration all target, non-target, and new lesions.
11.4.1 Establish of Sum of Diameters of Target Lesions and Response in Target Lesions
The presence of target lesions is established at baseline. A sum of the diameters, SOD (longest for non-nodal lesions, short axis for nodal lesions) for all target lesions (≤ 2 lesions per organ,≤ 5 lesions total), will be calculated and reported as the baseline SOD. At each subsequent tumorassessment (TA), the SOD of the target lesions identified at baseline is measured to provide the updated SOD.
Percentage changes in SOD of target lesions at each tumor assessment describe the size and growth kinetics of the target lesions. The presence of any new target lesions denote PD. At each tumor assessment, the response in SOD of target lesions is defined as follows:
• Complete Response (CR): Complete disappearance of all target lesions, with theexceptions of lymph nodes which must decrease to < 10 mm in short axis
• Partial Response (PR): Decrease in SOD of target lesions ≥ 30% relative to baseline
• Stable Disease (SD): Not meeting criteria for CR or PR, in absence of PD
• Progressive Disease (PD): Increase in SOD of target lesions ≥ 20% relative to nadir withan absolute increase of ≥ 5 mm; or an appearance of one or more new lesions
11.4.2 Response in Non-Target Lesions
The presence of non-target lesions is established at baseline; at each TA, the presence of any new, non-measurable lesions is assessed. The presence of new, non-measurable lesions denotes PD.
The response in non-target lesions is defined as follows:
• Complete Response (CR): Disappearance of all non-target lesions. All lymph nodesmust be non-pathological in size (<10 mm short axis)
• Non-CR/Non-PD: Persistence of one or more non-target lesion(s)
• Progressive Disease (PD): Unequivocal progression of existing non-target lesions.(Note: the appearance of one or more new lesions is also considered progression)
VentiRx Pharmaceuticals Incorporated 81Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
11.4.3 New Lesions
The appearance of new malignant lesions denotes disease progression.
11.4.4 Overall Response
The overall response according to RECIST v1.1 is derived from the response in target lesion(s), in non-target lesions, as well as new lesions. Table 3 and Table 4 are a summary of the overall timepoint responses.
The best overall response (BOR) is defined as the best RECIST v1.1 response over the study as a whole, recorded between the date of first dose until the last TA prior to subsequent anticancer therapy for individual subjects. An assessment of disease progression at or before week 12 will preclude a BOR of CR, PR, or SD.
VentiRx Pharmaceuticals Incorporated 82Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
11.5 Chemotherapy Dose Delay Algorithm
VentiRx Pharmaceuticals Incorporated 83Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
11.6 List of CYP3A4 Inhibitors and/or Inducers
Table 12 includes example CYP3A4 inhibitors and inducers. CYP3A4 inducers and inhibitors should be administered with caution and, if possible, alternatives that do not affect CYP3A4 should be administered instead (§7.6).
Table 12: Examples of CYP3A4 Inhibitors and Inducers
Inhibitors Inducers
Amiodarone Indinavir Barbiturates
Aprepitant/Fosaprepitant Itraconazole Carbamazepine
Chloramphenicol Ketoconazole Efavirenz
Cimetidine Mibefradil Glucocorticoids
Ciprofloxacin Mifepristone Modafinil
Clarithromycin Nefazodone Nevirapine
Delavirdine Nelfinavir Oxcarbazepine
Diethyl-dithiocarbamate Norfloxacin Phenobarbital
Diltiazem Norfluoxetine Phenytoin
Erythromycin Ritonavir Pioglitazone
Fluconazole Saquinavir Rifabutin
Fluvoxamine Star fruit Rifampin
Gestodene Telithromycin St. John’s wort
Grapefruit juice Verapamil Troglitazone
Imatinib Voriconazole --
Note that aprepitant/fosaprepitant is a CYP3A4 inhibitor recommended for use in managing CINV (§7.6.1). Given the specific pharmacology of aprepitant/fosaprepitant and VTX-2337 (e.g., short half life), as well as the number of intervening days between their administration, there is no contraindication to employing aprepitant or fosaprepitant for prevention of nausea and vomiting.
VentiRx Pharmaceuticals Incorporated 84Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
11.7 List of Abbreviations
Abbreviation or Term Definition/Explanation
5-FU Fluorouracil
ADCC Antiobody-dependent cellular cytotoxicity
AE Adverse Event
ALT (SGPT) Alanine aminotransferase (Serum Glutamic Pyruvic Transaminase)
ANC Absolute neutrophil count
API Active pharmaceutical ingredient
AST (SGOT) Aspartate aminotransferase (Serum Glutamic Oxaloacetic Transaminase)
AUC Area under the curve
BOR Best overall response
BP Blood pressure
C Celsius
CBC Complete blood count
CI Confidence interval
CR Complete response
CRF Case report form
CRO Contract research organization
CRS Cytokine release syndrome
CRx Concomitant medication
CT Computed tomography
DCR Disease control rate
DDC Duration of disease control
DLT Dose-limiting toxicity
DOBR Duration of best response
DSMB Data safety monitoring board
EC50 Half maximal effective concentration
ECG Electrocardiogram
ECOG Eastern cooperative oncology group
EGFR Epidermal growth factor receptor
VentiRx Pharmaceuticals Incorporated 85Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Abbreviation or Term Definition/Explanation
F Fahrenheit
FDA Food and Drug Administration
GCP Good Clinical Practice
GFR Glomerular Filtration Rate
GOG Gynecologic oncology group
HNC Head and neck carncioma
HPV Human papilloma virus
HR Heart rate
HR Hazard ration
IB Investigator’s Brochure
ICF Informed consent form
ICH International Conference on Harmonization
IEC Independent ethics committee
IND Investigational new drug
INDSR Investigational new drug safety report
IP Investigational product
IRB Institutional Review Board
irRECIST immune-related response evaluation criteria in solid tumors
IV Intravenous
IXRS Interactive voice/web response system
M Meter
mDC Myeloid Dendritic Cell
MedDRA Medical dictionary for regulatory activities
Mg Milligram
Min Minute
mL Milliliter
MRI Magnetic resonance imaging
NK Natural killer
Nm Nano molar
VentiRx Pharmaceuticals Incorporated 86Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Abbreviation or Term Definition/Explanation
ORR Objective response rate
OS Overall survival
PBMC Peripheral mononuclear cells
PD Pharmacodynamic
PD Progressive disease
PE Physical examination
pH Hydrogen ion concentration
PFS Progression free survival
PK Pharmacokinetic
PLD Pegylated liposomal doxorubicin
PR Partial response
RECIST Response evaluation criteria in solid tumors
RR Respiration rate
SAE Serious Adverse Event
SD Stable disease
SGOT (AST) Serum Glutamic Oxaloacetic Transaminase
SGPT (ALT) Serum Glutamic Pyruvic Transaminase
SC Subcutaneous
SI International system of units
SOC Standard-of-care
SOD Sum of diameters
SUSAR Suspected unexpected serious adverse reactions
t½ Terminal elimination phase half-life
T Temperature
t1/2 Mean half life
TA Tumor assessment
TEAE Treatment emergent adverse events
TLR Toll-like Receptor
TMTB Total measured tumor burden
VentiRx Pharmaceuticals Incorporated 87Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
Abbreviation or Term Definition/Explanation
ULN Upper Limit of Normal
µM micro molar
US United States
WBC White blood cell
WHO-DRUG World Health Organization-Drug Reference List
Remainder of page intentionally left blank.
VentiRx Pharmaceuticals Incorporated 88Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
12.0 LITERATURE AND REFERENCES
1. Smith, E.M., et al., Tobacco and alcohol use increases the risk of both HPV-associatedand HPV-independent head and neck cancers. Cancer Causes Control, 2010. 21:1369-1378.
2. Carvalho, A.L., et al., Trends in incidence and prognosis for head and neck cancer in theUnited States: a site-specific analysis of the SEER database. Int J Cancer, 2005. 114(5): p. 806-16.
3. Davies, L. and H.G. Welch, Epidemiology of head and neck cancer in the United States.Otolaryngol Head Neck Surg, 2006. 135(3): p. 451-7.
4. Curado, M.P. and M. Hashibe, Recent changes in the epidemiology of head and neckcancer. Curr Opin Oncol, 2009. 21(3): p. 194-200.
5. Hobbs, C.G., et al., Human papillomavirus and head and neck cancer: a systematicreview and meta-analysis. Clin Otolaryngol, 2006. 31(4): p. 259-66.
6. Dobrossy, L., Epidemiology of head and neck cancer: magnitude of the problem. CancerMetastasis Rev, 2005. 24(1): p. 9-17.
7. Argiris, A., et al., Head and neck cancer. Lancet, 2008. 371(9625): p. 1695-709.
8. Lango, M.N., Multimodal treatment for head and neck cancer. Surg Clin North Am,2009. 89(1): p. 43-52, viii.
9. Ferrari, D., et al., A review on the treatment of relapsed/metastatic head and neck cancer.Expert Opin Pharmacother, 2009. 10(16): p. 2625-32.
10. Specenier, P.M. and J.B. Vermorken, Recurrent head and neck cancer: current treatmentand future prospects. Expert Rev Anticancer Ther, 2008. 8(3): p. 375-91.
11. Ferlito, A., et al., Incidence and sites of distant metastases from head and neck cancer.ORL J Otorhinolaryngol Relat Spec, 2001. 63(4): p. 202-7.
12. Vermorken, J.B., et al., Platinum-Based chemotherapy plus Cetuximab in Head and NeckCancer. N Engl J Med, 2008;359:1116-27.
13. Rivera, F., et al., Cetuximab in metastatic or recurrent head and neck cancer: theEXTREME trial. Expert Rev Anticancer Ther, 2009. 9(10): p. 1421-8.
VentiRx Pharmaceuticals Incorporated 89Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 VTX-2337
14. Boshoff, C. and M. Posner, Targeting EGFR in head and neck cancer: a decade ofprogress. Nat Clin Pract Oncol, 2009. 6(3): p. 123.
15. Lim, C., et al., VTX-2337, a Selective TLR8 Ligand, Enhances Cetuximab-mediatedADCC in Head and Neck Cancer. J Immunother, 2011. 34(9): p. 693.
16. Specenier, P.M. and J.B. Vermorken, Current concepts for the management of head andneck cancer: chemotherapy. Oral Oncol, 2009. 45(4-5): p. 409-15.
17. Lu, H., et al., VTX-2337 is a novel TLR8 agonist that activates NK cells and augmentsADCC. Clin Cancer Res, 2012. 18(2):499-509
18. Stephenson, R., et al., TLR8 stimulation enhances cetuximab-mediated natural killer celllysis of head and neck cancer cells and dendritic cell cross-priming of EGFR-specific CD8+ T cells. Cancer Immunol Immunother. May 2013.
19. Northfelt, D., et al., A Phase 1 Dose-Finding Study of the Novel Toll-like Receptor 8Agonist VTX-2337 in Adult Subjects with Advanced Solid Tumors or Lymphoma. Clin Cancer Res, 2014, 20:3683-3691.
20. Chow, L., et al., Phase 1 Clinical Trial of VTX-2337, a Small Molecule Toll-LikeReceptor 8 (TLR8) Agonist in Combination with Cetuximab in Patients with Recurrent or Metastatic Squamous Cell Carconomas of the Head and Neck (SCCHN). Multidisciplinary Head and Neck Symposium; 2014 Feb 20–22; Scottsdale, AZ, USA.
21. Monk, B., et al., VTX-2337, a TLR8 Agonist, Plus Chemotherapy in Recurrent OvarianCancer: Preclinical and Phase 1 Data by the Gynecologic Oncology Group. American Society of Clinical Oncology, Annual Meeting; 2013 June 3–7; Chicago, IL, USA.
22. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebbé C, Maio M, Binder M,Bohnsack O, Nichol G, Humphrey R, Hodi FS. Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria. Clin Cancer Res 2009, 15(23):7412–20
23. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, Dancey J,Arbuck S, Gwyther S, Mooney M, Rubinstein L, Shankar L, Dodd L. Kaplan R, Lacombe D, Verweij J. Revised RECIST guideline (version 1.1). European Journal of Cancer 2009, 45:228-247
VentiRx Pharmaceuticals Incorporated 90Confidential Information 25-Jan-2016
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 1 of 33
Statistical Analysis Plan
Sponsor VentiRx Pharmaceuticals, Incorporated
Protocol No VRXP-A202
PRA Project ID VTX2337X-VT2337
Version Date 25-MAY-2016
Version Number 2.0
Approvals
Sponsor Name VentiRx Pharmaceuticals, Incorporated
Name of Sponsor Representative/Title
Kristi Manjarrez, Vice President, Clinical Affairs VentiRx Pharmaceuticals, Incorporated
Signature of Sponsor Representative /Date
Name of Sponsor Representative/Title
James Kyle Bryan, MD, Chief Medical Officer VentiRx Pharmaceuticals, Incorporated
Signature of Sponsor Representative /Date
Name of Project Manager/Title
Denise Wall, Project Manager PRA Health Sciences
Signature of Project Manager/Date
Name of Biostatistician /Title Eric Bissonette, Senior Principal Biostatistician PRA Health Sciences
Signature of Biostatistician /Date
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 2 of 33
TABLE OF CONTENTS
TABLE OF CONTENTS ........................................................................................................................... 2
1. INTRODUCTION ............................................................................................................................ 4 1.1 Changes from Protocol ............................................................................................................................. 4 1.2 Clarifications ............................................................................................................................................ 4
2. STUDY OBJECTIVES ..................................................................................................................... 5
3. STUDY DESIGN .............................................................................................................................. 5 3.1 Sample Size Considerations ...................................................................................................................... 7 3.2 Randomization ......................................................................................................................................... 7
4. STUDY ENDPOINTS ..................................................................................................................... 8 4.1 Primary Endpoint ..................................................................................................................................... 8 4.2 Secondary Endpoints ................................................................................................................................ 8
4.2.1 Safety Endpoints 8 4.2.2 Efficacy Endpoints 8
4.3 Exploratory Endpoints .............................................................................................................................. 9 4.4 Subgroup Analyses ................................................................................................................................... 9
5. DEFINITIONS ............................................................................................................................... 10
6. ANALYSIS POPULATIONS ........................................................................................................ 20 6.1 Safety Population.................................................................................................................................... 20 6.2 Intent to Treat Population ....................................................................................................................... 20 6.3 Per Protocol Population .......................................................................................................................... 20
7. INTERIM ANALYSES .................................................................................................................. 20
8. DATA REVIEW ............................................................................................................................. 20 8.1 Data Handling and Transfer ..................................................................................................................... 20 8.2 Data Screening ........................................................................................................................................ 21
9. STATISTICAL METHODS .......................................................................................................... 21 9.1 Subject Disposition ................................................................................................................................. 22 9.2 Protocol Deviations ................................................................................................................................. 22 9.3 Treatments ............................................................................................................................................. 23
9.3.1 Extent of Study-required Treatment Exposure 23 9.3.2 Concomitant Medications 23
9.4 Demographic and Baseline Characteristics ............................................................................................... 23 9.5 Efficacy Analyses ..................................................................................................................................... 24
9.5.1 Primary Efficacy Endpoint 24 9.5.2 Secondary Efficacy Endpoints 25 9.5.3 Sensitivity Analyses 26
9.6 Safety Analyses ....................................................................................................................................... 26 9.6.1 Adverse Events 26 9.6.2 Laboratory Data 28 9.6.3 Vital Signs 28 9.6.4 ECOG Performance Status 28 9.6.5 Electrocardiograms 29
9.7 Analyses for Exploratory Endpoints ......................................................................................................... 29 9.7.1 Genetic Polymorphisms Affecting Response to TLR8 Agonist or to Cetuximab 29 9.7.2 Immune Biomarker Response 29 9.7.3 Effect of Tumor Immune Cell Subsets on Response to Treatment and/or Clinical Outcome 29 9.7.4 PK Profile of Motolimod 29
10. QUALITY CONTROL AND VALIDATION ............................................................................... 30
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 3 of 33
11. REFERENCES ................................................................................................................................ 30
APPENDIX 1 GLOSSARY OF ABBREVIATIONS ......................................................................... 31
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 4 of 33
1. INTRODUCTION
This statistical analysis plan (SAP) describes the statistical methods to be used during the
reporting and analyses of data collected under VentiRx Protocol VRXP-A202.
This SAP should be read in conjunction with the study protocol and case report form (CRF).
This version of the plan has been developed using Protocol Amendment 3.0 dated 25JAN2016
and CRF dated 08JAN2015. Any further changes to the protocol or CRF may necessitate updates
to the SAP.
The SAP is to be developed in two stages. The purpose is to “finalize” a SAP so that we can start
programming earlier in the process. Versions of the SAP up to initial sponsor approval will be
known as SAP1. Changes following approval of SAP1 will be tracked in the SAP Change Log
and final versions of the SAP, known as SAP2 and SAP3, will be issued for VentiRx approval
prior to the first and second database lock, respectively.
1.1 CHANGES FROM PROTOCOL
Shift tables from baseline to worst post-baseline in National Cancer Institute (NCI) Common
Terminology Criteria for Adverse Events (CTCAE) grade for hematology and chemistry are
discussed in the protocol Section 9.2.2; however, these are not planned and are not discussed in
the SAP.
Progression-free survival (PFS), overall response rate (ORR), duration of objective response
(DOOR), disease control rate (DCR), and duration of disease control (DDC) as evaluated by
independent radiology review according to Response Evaluation Criteria In Solid Tumors
(RECIST) 1.1 will be included as secondary objectives of the study as described in Protocol
Amendment 3.0.
1.2 CLARIFICATIONS
VTX-2337 is replaced with motolimod.
DCR is defined as the percentage of subjects with complete response (CR), partial response
(PR), or stable disease (SD) per protocol; however, it is clarified as the percentage of subjects
with best overall response (BOR) of CR, PR, SD, or NN (Non-CR/Non-PD) in the SAP.
Per the intent to treat principle, all randomized subjects, including those who discontinue the
study prior to investigational product (IP) administration, will be included in the intent to treat
(ITT) population. Over the duration of the study, approximately 20 subjects were randomized but
discontinued the study prior to receiving a dose of IP. In order to ensure that at least 175 IP-
treated subjects are included in the efficacy analysis of the study, the sample size was expanded
to account for these 20 subjects (see Section 3.1).
The primary efficacy endpoint of the study is PFS as assessed by blinded central radiology
review according to immune-related RECIST (irRECIST). As a secondary objective, PFS will
also be assessed by RECIST 1.1. For simplicity, tumor response outcomes and endpoints will be
referenced throughout this SAP in generic terms: PFS, CR, PR, SD, PD, etc. However, these will
encompass both the assessments according to irRECIST and RECIST 1.1.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 5 of 33
2. STUDY OBJECTIVES
The primary objective of the study is to compare PFS of subjects treated with standard-of-care
(SoC, ie, cisplatin or carboplatin + fluorouracil [5-FU] + cetuximab) + Motolimod (Combination
Arm) to those treated with SoC + Placebo (Control Arm) according to irRECIST criteria.
The secondary objectives are to compare:
1) The safety between the two treatment arms.
2) The overall survival (OS) between the two treatment arms.
3) The PFS according to RECIST 1.1.
4) The ORR, DOOR, DCR, and DDC between the 2 treatment arms according to both
irRECIST and RECIST 1.1.
The exploratory objectives are:
1) To compare genetic polymorphisms that may impact the response of patients to a Toll-
like receptor 8 (TLR8) agonist or to cetuximab between the two treatment groups.
2) To compare immune biomarker response as measured by a multiplexed panel of
cytokines, chemokines, and inflammatory markers between the two treatment groups.
3) To compare the effect of immune cell subsets within the tumor on response to treatment
and/or clinical outcome, as measured by immunohistochemistry in primary tumor tissue
between the two treatment groups.
4) To assess the pharmacokinetics (PK) of motolimod.
3. STUDY DESIGN
This is a randomized, double-blind, placebo-controlled, parallel group study which consists of
the following:
1) Screening and randomization (Days -14 to -1): Following the screening period, qualified
subjects will be randomized in a 1:1 ratio to receive SoC + Placebo or SoC + Motolimod.
Treatment assignment will be blinded.
2) Initial treatment (Cycles 1–6, study Weeks 1–18): Once randomized, subjects will then be
administered the following on pre-specified days of a 21-day cycle for 6 cycles:
o Intravenous (IV) infusion of platinum therapy, cisplatin or carboplatin as assigned
by investigator, on Day 1
o A continuous IV infusion of 5-FU on Days 1, 2, 3, and 4
o IV infusion of cetuximab on Days 1, 8, and 15
o Subcutaneous injection of IP, motolimod or placebo, on Days 8 and 15
Note that “IP” (ie, study drug) refers to motolimod or placebo only. “Study-required
treatment” refers to IP or SoC medication.
If chemotherapy is delayed, the previous cycle (Cycle 1–5) should be extended for up to
3 weeks (Days 22, 29, and 36). Per protocol, IP and cetuximab may be administered on
Days 22 and 29, and cetuximab alone on Day 36. Missed doses of cetuximab and/or IP
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 6 of 33
are considered skipped and will not be made up. Refer to the protocol for additional
information about dose delays.
3) Subsequent treatment (Cycles 7+, study Weeks 19+): After initial treatment, subjects will
continue on study and receive the following on pre-specified days of a 28-day cycle for
cycles 7+:
o IV infusion of cetuximab on Days 1, 8, 15, and 22
o Subcutaneous injection of IP on Days 8 and 22
4) End of treatment (EOT) visit: Treatment will be discontinued for subjects with
independently-verified radiographic disease progression. Subjects may discontinue
treatment for other reasons (eg, death, withdrawn consent, unacceptable toxicity, non-
compliance with study-required medications, etc; see protocol Section 6.5). Upon
discontinuation of treatment, subjects will complete EOT visit and will be followed for
survival.
5) Survival follow-up: During the survival follow-up period, subjects will be contacted
every 8 weeks to assess vital status and disease state, including the initiation of any new
anticancer interventions. Subjects will be followed for survival for at least 12 months
after the last subject is randomized.
6) End of study (EOS): Upon completion or discontinuation of study, the EOS CRF will be
completed for all subjects who participated in survival follow up.
Subjects will be evaluated for PFS by computed tomography (CT) or magnetic resonance
imaging (MRI) at Week 12 (± 3 days), Week 18 (± 3 days), Week 26 (± 7 days) and every 8
weeks (± 7 days) thereafter. Response will be verified by an independent radiologist.
Figure 1: Study Schema
To address any new or unexpected safety issues, the first Data Safety Monitoring Board (DSMB)
meeting occurred after an unblinded statistician confirmed that 6 subjects, who had been
randomized to receive motolimod, had completed one cycle of therapy. The purpose of this
meeting was to evaluate any dose-limiting toxicities (DLTs) or any acute, unexpected, or
synergistic toxicities associated with the combination of motolimod, platinum, 5-FU, and
cetuximab. Results from the initial DSMB evaluate concluded that the study could continue as
planned at the dose level of 3.0 mg/m2.
Subsequent Treatment Cycles 7+
Initial Treatment 6 Cycles (18 Weeks)
Screening< 14 Days
Screening
SOC + VTX-2337
SOC + Placebo
Ran
do
miz
atio
n
Cetuximab + Placebo
Cetuximab + VTX-2337
Follow Up
Dis
ease
P
rogr
essi
on
Survival Follow-Up
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 7 of 33
In addition, adverse events and safety will be evaluated throughout the study by the DSMB. The
DSMB will meet at predetermined intervals set forth in the DSMB Charter—approximately
every 6 months—to review toxicities and serious and/or unexpected adverse events.
Please refer to Table 1 of the protocol for the full Schedule of Procedures and Assessments.
3.1 SAMPLE SIZE CONSIDERATIONS
The original sample size per protocol was approximately 175 subjects (estimated 88 per
treatment group) randomized and treated with at least one dose of IP. A dropout rate of 10% was
assumed over the duration of the study.
The total sample size was expanded to approximately 195 randomized subjects (estimated 97 per
treatment arm). This extension of randomization from the original projection of 175 subjects
was to account for approximately 20 subjects who discontinued treatment without receiving IP
(ie, 10% dropouts), in order to achieve approximately 175 randomized and IP-treated subjects.
The timing of the primary analysis is event-driven. One hundred thirty-four (134) PFS events are
required to detect a hazard ratio (HR) of 0.67 with 85% power with a one-sided alpha of 0.10.
This HR represents a 50% improvement in PFS, which translates to an increase in median PFS
from 6 months (Control Arm) to 9 months (Combination Arm). It was originally estimated that a
population of 175 IP-treated subjects accrued over 18 months would need to be followed for an
additional 9 months (27 months total) to provide the requisite number of PFS events.
The primary endpoint analysis will occur when approximately 134 PFS have been accumulated,
ensuring that the number of PFS events is sufficient for at least 80% power.
The analysis of OS will be conducted when all randomized subjects have been followed for ≥ 12
months following enrollment of the final subject. Given the 22-month actual accrual period, it is
estimated that 126 OS events will be accrued during 35 months of follow-up, providing 76%
power at a one-sided alpha of 0.10 to detect a HR of 0.70. This HR represents a 30% reduction in
the risk of death, and a 42.9% increase in the median OS. Assuming a median OS of 11 months
in the Control Arm, the median OS in the Combination Arm will be 15.7 months.
3.2 RANDOMIZATION
All subjects will be randomly assigned in a 1:1 ratio to one of 2 treatment arms: SoC +
Motolimod or SoC + Placebo. To ensure that both known and unknown confounding factors are
evenly distributed between treatment arms randomization of all subjects will be stratified by the
following factors:
• Prior systemic therapy for squamous cell carcinoma of the head and neck (SCCHN; yes or
no)
• Eastern Cooperative Oncology Group (ECOG) performance status (0 or 1)
• Platinum therapy, as assigned by investigators at randomization (cisplatin or carboplatin)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 8 of 33
4. STUDY ENDPOINTS
4.1 PRIMARY ENDPOINT
• PFS based on irRECIST and independent central assessment: defined as the duration of time
from randomization to time of progressive disease as defined by irRECIST (irPD) verified by
central, blinded and independent radiology review or death, whichever comes first, or the last
tumor assessment date for censored subjects. For the primary endpoint, PFS will be assessed
according to irRECIST.
4.2 SECONDARY ENDPOINTS
4.2.1 Safety Endpoints
• Adverse events
• Vital signs: pulse rate, respiration, systolic and diastolic blood pressure, temperature, height
and weight
• Clinical laboratory parameters:
o Hematology: red blood cell count (RBC), white blood cell count (WBC), platelet
count, hemoglobin (HGB), hematocrit (HCT), red blood cell distribution width
(RDW), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH),
mean corpuscular hemoglobin concentration (MCHC), and count differential tests
which include neutrophils, lymphocytes, monocytes, eosinophils, basophils, absolute
neutrophils count, absolute basophils count, absolute lymphocytes count, absolute
monocytes count, and absolute eosinophils count
o Serum chemistry: albumin (ALB), alkaline phosphatase (ALP), alanine
aminotransferase (ALT), aspartate aminotransferase (AST), blood urea nitrogen
(BUN), serum creatinine, potassium (K), sodium (Na), total bilirubin, bicarbonate,
chloride, lactate dehydrogenase (LDH)
o Urinalysis: glucose, ketones, pH, protein, bilirubin, blood nitrite, leukocyte esterase,
specific gravity
• 12-lead electrocardiogram (ECG): heart rate, PR interval, QRS duration, QT interval,
incidence of outliers and changes from baseline in QT interval corrected with Fridericia’s
formula (QTcF) and with Bazett’s formula (QTcB), RR interval
• ECOG performance status
4.2.2 Efficacy Endpoints
• PFS based on irRECIST and investigator assessment: defined as the duration of time from
randomization to time of progressive disease as defined by irRECIST (irPD) assessed by
local investigators or death, whichever comes first, or the last tumor assessment date for
censored subjects.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 9 of 33
• PFS based on RECIST 1.1 and independent central assessment: defined as the duration of
time from randomization to time of progressive disease as defined by RECIST 1.1 (PD)
verified by central, blinded and independent radiology review or death, whichever comes
first, or the last tumor assessment date for censored subjects.
• OS: defined as the duration of time from randomization to the time of death due to any cause,
or the date the subject was last confirmed to be alive for censored subjects.
• Tumor response as evaluated by irRECIST and RECIST version 1.1:
o Number and percent of subjects exhibiting each level of best tumor response
according to RECIST (complete response [CR], partial response [PR], stable disease
[SD], non-CR/non-PD [NN], progressive disease [PD], or not evaluable [NE])
assessed by the independent central reviewer and investigator will be presented by
treatment arm, respectively.
o ORR: defined as the proportion of subjects who achieve BOR of CR or PR.
o DOOR: defined as the duration of time from the date measurement criteria are first
met for CR or PR (if CR is never met), until the first date that PD is verified by
independent radiology review or death, whichever comes first.
o DCR: defined as the percentage of subjects with CR, PR, SD, or NN.
o DDC: defined as the duration of time from the date measurement criteria are first met
for CR, PR, SD, or NN, until the first date that PD is verified by central, independent
radiology review or death, whichever comes first.
4.3 EXPLORATORY ENDPOINTS
• Comparison of genetic polymorphisms that may impact the response of subjects to TLR8
agonist or to cetuximab between the two treatment arms.
• Comparison of immune biomarker response as measured by a multiplexed panel of
cytokines, chemokines, and inflammatory markers between the two treatment arms.
• Comparison of the effect of immune cell subsets within the tumor on response to treatment
and/or clinical outcome, as measured by immunohistochemistry in primary tumor tissue
between the two treatment arms.
• Population PK profile of motolimod.
4.4 SUBGROUP ANALYSES
The following factors may be analyzed:
• Prior systemic therapy for SSCHN (yes or no)
• Prior cetuximab (yes or no)
• Prior neoadjuvant systemic treatment (yes or no)
• Prior surgery (yes or no)
• Prior radiotherapy only (yes or no)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 10 of 33
• Prior chemoradiotherapy, including radiotherapy with cetuximab (yes or no)
• ECOG 1 or 0
• Metastatic disease (de novo vs. recurrent metastatic vs. none)
• Cisplatin vs. carboplatin
• HPV status (positive or negative or missing/unknown) for subjects with oropharyngeal
cancer
5. DEFINITIONS
AE leading to discontinuation of study-required treatment
AE leading to discontinuation of study-required treatment is defined as an AE with action taken
for any study-required treatment = dose discontinued.
Age
The following SAS® code will be used to calculate subject age (years):
Age = floor ([intck{‘month’, birth date, screen Date} - {day(randomization date) < day(birth
date)}] / 12),
where intck is a SAS® function counting integer days.
Baseline, change from baseline
Baseline is defined as the last non-missing value before the initial administration of study
required medication. Change from baseline will be defined as (value at post-baseline visit –
value at baseline).
Post-baseline values for tabulations generally will exclude unscheduled visit values, but
unscheduled visit values will be included in listings.
Body Surface Area
Body surface area (BSA) will be calculated by Mosteller formula:
BSA (m2) = ( [Height(cm) x Weight(kg) ]/ 3600 ) (1/2)
Concomitant medications
Concomitant medications are defined as any medications taken at or after the date of first dose of
study-required treatment (see definition of study-required treatment in this section). All
medications recorded on the Concomitant Medication CRF page are concomitant as this page
will only collect non-study medications (includes over-the-counter and prescription drugs) taken
from Cycle 1 Day 1 and during the course of the study.
Completed treatment phase
A subject who discontinues the treatment phase with independent verification of irPD or due to
death will be considered to have completed treatment. Such subjects will have “irPD (centrally
confirmed)” or “Death” as the primary reason for EOT on the EOT CRF page. The centrally
verified irPD date (scan date) will be included in the electronic data transfer from the central
radiology vendor. The death date will be on the death record CRF page.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 11 of 33
Completed survival follow-up
Subjects will be followed for survival for at least 12 months after the last subject is randomized.
A subject who dies anytime through survival follow-up (including death during treatment phase)
or who is still alive and on study at the time of the final OS analysis will be defined as having
completed survival follow-up (ie, the primary reason on EOS page is “Death” or “Study closed
by sponsor” or last confirmed to be alive date ≥ EOS date).
Currentness of follow-up
Currentness of follow-up in months is defined as (data cutoff date or study end date – last
confirmed alive date + 1)/30.42.
Discontinued early in treatment phase
A subject who discontinues the treatment phase in the absence of death or independent
verification of irPD will be considered an early discontinuation of treatment. Such subjects will
have any primary reason for treatment discontinuation except “Death” or “irPD (centrally
confirmed)” on the EOT CRF page. The discontinuation of treatment date will be the date of
EOT visit on the EOT CRF page. If an early discontinuation of treatment subject does not have
an EOT visit, the discontinuation of treatment date will be the date of the last study
procedure/assessment.
Discontinued survival follow-up early
A subject who discontinues survival follow-up in the absence of death or closure of the study by
the sponsor will be considered an early discontinuation of survival follow-up. Such subjects will
have any primary reason for study discontinuation except “Death” or “Study closed by sponsor”
on the EOS CRF page. The discontinuation of study date will be the date of EOS visit on the
EOS CRF page. If an early discontinuation of study subject does not have an EOS visit, then the
discontinuation of study date will be the last confirmed to be alive date.
Disease state at study entry
All patients with an initial diagnosis stage of M0 would be considered recurrent disease. If the
diagnosis stage at screening is also M0, then the recurrent disease is local only; otherwise if the
diagnosis stage at screening is M1, then the recurrent disease is metastatic.
All patients with an initial diagnosis stage of M1 would be considered de novo metastatic disease
unless they have received prior systemic therapy with curative intent.
All patients with an initial diagnosis stage of M1 who have received prior systemic therapy with
curative intent would be considered metastatic recurrent disease.
Stage at initial diagnosis Stage at screening Prior systemic therapy Disease state
M1 M1 No De novo metastatic disease M1 M1 Yes Recurrent disease (metastatic) M0 (or not present) M0 Yes/No Recurrent disease (local only) M0 M1 Yes/No Recurrent disease (metastatic)
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 12 of 33
Dose discontinuation, reduction, dose delay, or dose interruption of study required
treatment due to AE
Study required treatment dose discontinuation, reduction, dose delay, or dose interruption due to
AE is defined as an AE with action taken for study drug = dose discontinued, dose reduced, dose
delayed, or dose interrupted.
Duration from initial SCCHN diagnosis to randomization
Duration from initial diagnosis to randomization in days is defined as (randomization date –
initial diagnosis date).
Duration from recurrent or metastatic diagnosis to randomization
Duration from recurrent or metastatic diagnosis to randomization in days is defined as
(randomization date – recurrent or metastatic diagnosis date).
Duration of follow-up
Duration of follow-up in months is defined as (last confirmed alive date – randomization date +
1)/30.4375.
Evaluable subject
All randomized subjects (ie, ITT population) will be considered evaluable for the primary
endpoint.
Exposure, duration of
Duration of exposure for each of the following treatments is defined as (end date of the week of
last dose – first dose date + 1)/7 for the corresponding treatment expressed in weeks.
• Cetuximab
• IP
Duration of exposure for each of the following treatments is defined as (end date of the 3rd week
of last dose – first dose date + 1)/7 for the corresponding treatment expressed in weeks.
• Platinum therapy - cisplatin
• Platinum therapy - carboplatin
• 5-FU
Exposure, total
Total exposure for each of the above treatments, except for platinum therapy – carboplatin,
relative to body surface area is defined as the total mg/m2 of the corresponding treatment
administered during the study. Total exposure for carboplatin is defined as the total mg of
corresponding treatment administered during the study.
Total exposure (in mg/m2) for each of the above treatments, except for platinum therapy –
carboplatin, is calculated for each cycle and overall according to the corresponding dosing data
(ie, dose in mg/m2). Total exposure (in mg) for carboplatin is calculated for each cycle and
overall according to the corresponding dosing data.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 13 of 33
Exposure, dose intensity
Dose intensity (mg/m2/week) for each of the above treatments, except for platinum therapy –
carboplatin, is calculated as the total exposure (mg/m2)/duration of exposure (weeks). Dose
intensity (mg/week) for carboplatin is calculated as the total exposure (mg)/duration of exposure
(weeks).
Exposure, percent relative dose intensity
Percent relative dose intensity is total dose received (mg/m2) / planned dose (mg/m2) *100%. For
carboplatin, dose intensity is total dose received (mg) / planned dose (mg) * 100%.
Hematology tests results, automated and manual
The hematology panel tests listed in Section 4.2.1 will be run on automated equipment.
However, if the automated WBC count or differential is flagged as abnormal, a technologist will
perform a manual differential on the sample. If upon review, the technologist agrees with the
automated differential findings, the automated differential is released. If the technologist does
not agree or abnormal cells are noted, the manual differential results are released. Table 1 (see
below) lists the automated count differential tests and the corresponding matching/equivalent
manual tests. For statistical summary tables, the invalid values of automated results will be
replaced by the corresponding manual tests (the conversion factor of units 103/µL to 103/cumm =
1). The other hematology tests listed in Section 4.2.1 (ie, HCT, HGB, MCH, MCHC, MCV,
PLATELET COUNT, RBC, RDW and WBC) are stand-alone automated tests. They have no
matching tests in the manual differential panel.
In addition to the manual tests listed in Table 1, the manual differential panel contains the stand -
alone tests listed in Table 2 below that help the investigators to interpret the results. These tests
will not be displayed in the summary tables but will be presented where appropriate in the
listings.
Table 1 Equivalent Automated and Manual Hematology Count Differential Tests
Automated Tests Manual Tests
Test Name Units Test Name Units
Abs.basophil count 103/uL Calc.abs.basophil count 103/cumm
Abs.eosinophil count 103/uL Calc.abs.eosinophil count 103/cumm
Abs.lymphocyte count 103/uL Calc.abs.lymphocyte count 103/cumm
Abs.monocyte count 103/uL Calc.abs.monocyte count 103/cumm
Abs.neutrophil count 103/uL Calc.abs.neutrophil count 103/cumm
Basophils % Basos %
Eosinophils % Eos %
Lymphocytes % Lymphs %
Monocytes % Monos %
Neutrophils % Segs %
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 14 of 33
Table 2 Stand-alone Tests in the Manual Differential Panel
Manual Test Name Units
Atypical lymphs None (Results: Occasional, 10%, 25%, 50%, 75%, 100%)
Blasts %
Bands %
Bizarre platelets None (Results: 0, Occasional, Moderate, Many)
Diff comment NA
Giant platelets None (Results: 0, Occasional, Moderate, Many)
Hyperseg. neutrophils
None (Results: 0 - defined as <1/hpf, Few - defined as 1-2/hpf, Moderate - defined as 3-5/hpf, Many - defined as >5/hpf)
Metamyelocytes %
Myelocytes %
Nucleated rbcs %
Platelet estimate None (Adequate, Decreased, Increased)
Promyelocytes %
Reactive lymphs
None (Results: 0 – defined as <10% total lymphocyte count, Few – defined as 10%-30% of total lymphocyte count, Moderate – defined as 30%-60% of total lymphocyte count, Many – defined as >60% total lymphocyte count)
Smudge cells
None (Results: 0 - defined as <5/hpf, Few - defined as 6-10/hpf, Moderate - defined as 11-15/hpf, Many - defined as >15/hpf)
Toxic granulation None (Results: 0, Slight, Moderate, Marked)
Unclassified %
Investigational product
Motolimod or placebo.
Last confirmed alive date
The last confirmed alive date is the latest of the following: study visit date, telephone contact
date, EOS last confirmed alive date, follow-up systemic (anticancer) therapy end date or start
date (if ongoing or end date is missing), local or central radiologist scan date, or other date in the
clinical data.
Last cycle on chemotherapy
Last cycle on chemotherapy will be derived for each subject, including any part of an
uncompleted cycle as the last cycle.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 15 of 33
Last cycle on IP
Last cycle on IP will be derived for each subject, including any part of an uncompleted cycle as
the last cycle.
Primary reason for EOS
Primary reason for EOS will be collected on the EOS CRF page.
Primary reason for EOT
Primary reason for EOT will be collected on the EOT CRF page.
Protocol deviation, important protocol deviation
Potential planned or unplanned protocol deviations noted during clinical monitoring will be
documented by category (ie, inclusion criteria, exclusion criteria, IP, safety assessment, efficacy
assessment, visit window, informed consent, prohibited medication, regulatory compliance,
stratification error, archival tumor tissue, or other). Per PRA processes, planned or unplanned
protocol deviations will be entered into PRA’s Clinical Trials Management System (CTMS).
The study team and VentiRx will conduct ongoing reviews of the protocol deviations from
CTMS throughout the study, adjusting the protocol deviation criteria as appropriate. All protocol
deviations will be reviewed, categorized, designated important or not important, and finalized
prior to each of the database locks. Important protocol deviations will be defined as potentially
impacting safety or efficacy assessment following regulatory guidance criteria (International
Conference for Harmonization [ICH] E3).
Randomized subject
A randomized subject is defined as one who has a randomization number corresponding to a
treatment arm assigned by the interactive voice/web response system (IXRS).
Randomized subjects are also collected on the Enrolled CRF page with a randomization date.
Screen date
For this study, a subject’s screen status will be collected on the Screened CRF page with a screen
date.
Study day
Study day is defined relative to the date of the first administration of study-required treatment.
For assessments that occur after this visit date, study day is calculated as (assessment date –
study-required treatment first dose date + 1). For assessments that occur prior to study-required
treatment first dose date, study day will be calculated as (assessment date –study-required
treatment first dose date); there is no Study Day 0.
Study drug
Study drug will refer to IP, ie, motolimod or placebo, only.
Study-required treatment
Study required treatment will refer to SoC medication, ie, cisplatin, carboplatin, 5-FU,
cetuximab, and IP, ie, motolimod or placebo.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 16 of 33
Treatment arm, actual
A subject’s actual treatment arm (SoC + Motolimod/Combination Arm or SoC +
Placebo/Control Arm) will be determined by whether the subject is administered or placebo by
merging the Dosing (IP) CRF data, the Drug Dispensation CRF data and the Medication Packs
List using the Medication ID Number. If the subject receives one or more dose of motolimod,
then the subject’s actual treatment arm will be SoC + Motolimod/Combination Arm. If the
subject receives only placebo, then the subject’s actual treatment arm will be SoC +
Placebo/Control Arm.
Treatment arm, randomized
A subject’s randomized treatment arm (SoC + Motolimod/Combination Arm or SoC + Placebo/
Control Arm) will be the treatment arm associated with that subject’s randomization number in
the IXRS randomization schedule.
Treatment-emergent adverse events
TEAEs are those which first occur or increase in frequency or severity after the first dose of IP.
An adverse event (AE) with a missing start date which meets any of the following criteria will be
assumed to be a TEAE: 1) the start date of an AE is completely missing; 2) the start date of an
AE is partially missing and it cannot be determined whether the AE occurs prior to or after the
first dose of IP based on the partial date.
Tumor response via irRECIST and RECIST v1.1
Best overall response
BOR is defined as the best irRECIST or RECIST 1.1 response among all overall responses
(in the order of CR, PR, SD,NN, PD [including unconfirmed PD], and NE) during the study,
recorded from the date of randomization until PD verified by independent radiology review
or last tumor assessment, whichever is earlier/first.
For PD assessed according to irRECIST only:
If a subject has a finding of irPD assessed by the independent radiology review at or
before Week 12 (81-87 days post C1D1), the irPD is not confirmed by a repeat,
consecutive imaging assessment obtained at least 4 weeks later and verified by the
independent radiology review, and there are no other subsequent imaging assessments,
then his/her BOR is “unconfirmed irPD.” Unconfirmed irPD on or before Week 12 will
be considered irPD, and counts towards PFS.
If a subject has a finding of irPD assessed by the independent radiology review at or
before Week 12 (81-87 days post C1D1), and the irPD is confirmed by a repeat,
consecutive imaging assessment obtained at least 4 weeks later and verified by the
independent radiology review, the earlier irPD assessed by the independent radiology
review counts towards PFS. The subject’s BOR is irPD.
If a subject has a finding of irPD assessed by the independent radiology review at or
before Week 12 (81-87 days post C1D1) and the irPD is not confirmed by a repeat,
consecutive imaging assessment obtained at least 4 weeks later and verified by the
independent radiology review, but irPD is verified at a subsequent imaging assessment by
the independent radiology review, then the dearly, unconfirmed finding of irPD is
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 17 of 33
disregarded and the second irPD assessed by the independent radiology review counts
towards PFS. For example, the Week 12 independent radiology review result is irPD not
verified by repeat, consecutive imaging assessment obtained at least 4 weeks later, but
the Week 26 independent radiology review result is irPD, then the Week 26 result counts
towards PFS.
For PD assessed according to RECIST 1.1 only:
If a subject has a finding of PD assessed by the independent radiology review at or before
Week 12 (81–87 days post C1D1), it will be considered PD irrespective of confirmation
and regardless if a better tumor response is verified at a subsequent time point (ie,
confirmation ≥ 4 weeks later is not required).
If a subject has a finding of PD verified by an independent radiology review after Week 12,
then the BOR is the best response among all responses recorded from the date of
randomization until PD.
If a subject has post-treatment tumor assessment(s) but does not have a finding of PD
verified by an independent radiology review, then the BOR is the best response among all
responses recorded from the date of randomization until last tumor assessment.
If there is no post-treatment tumor assessment, the best overall response will be assigned as
NE.
BOR assessed by investigator will be collected on the BOR CRF page. For central review,
BOR will be determined from the independent radiology reviews at each time point.
Disease control rate
DCR is defined as the percentage of subjects with a BOR of CR, PR, SD, or NN.
Duration of objective response
DOOR, measured in days, is defined as the duration of time from the date measurement
criteria are first met for CR or PR (if CR is never met), until the first date that PD is verified
by independent radiology review or death due to any cause, whichever comes first.
If a subject is alive and without centrally verified PD at the time the total number of PFS
events by irRECIST is accrued, DOOR is defined as the time from the date measurement
criteria are first met for CR or PR (if CR is never met), to the date of the last tumor
assessment as a censored value.
DOOR will be calculated only for responding subjects (PR or CR) as assessed by central,
independent radiology review.
Duration of disease control
DDC, measured in days, is defined as the duration of time from the date measurement criteria
are first met for CR, PR, SD, or NN, until the first date that PD is verified by central,
independent radiology review or death due to any cause, whichever comes first.
If a subject is alive and without centrally verified PD at the time the total number of PFS
events is accrued, DDC is defined as the time from the date measurement criteria are first
met for CR, PR, SD, or NN to the date of the last tumor assessment as a censored value.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 18 of 33
DDC will be calculated only for subjects with PR, CR, SD, or NN as assessed by
independent radiology review.
Objective response
A subject who achieves objective response is one whose BOR is either PR or CR.
Objective response rate
ORR is defined as the percentage of subjects who achieved BOR of CR or PR.
Overall response, irRECIST
The overall response according to irRECIST is derived from the responses in total measured
tumor burden (TMTB; see definition in this section) as well as the presence of any non-target
lesions as follows:
• Complete response (irCR): Complete disappearance of all lesions (whether measurable or
not); lymph nodes must decrease to < 10 mm in shortest dimension;
• Partial response (irPR): Decrease in TMTB ≥ 30% relative to baseline;
• Stable disease (irSD): Not meeting criteria for irCR or irPR, in absence of irPD;
• Progressive disease (irPD): Increase in TMTB ≥ 20% relative to nadir.
Overall response, RECIST 1.1
The overall response according to RECIST 1.1 is derived from the responses in target
(measurable) and non-target (non-measurable and measurable) lesions as follows:
• Complete response (CR): Complete disappearance of all lesions (whether measurable or not);
lymph nodes must decrease to < 10 mm in shortest dimension;
• Partial response (PR): Decrease in TMTB ≥ 30% relative to baseline;
• Stable disease (SD): Not meeting criteria for CR or PR, in absence of PD;
• Progressive disease (PD): Increase in TMTB ≥ 20% with an absolute increase of ≥ 5 mm
relative to nadir, unequivocal progression of existing non-target lesions, or the appearance of
unequivocal new lesions.
Overall survival
OS is defined as the duration of time from randomization to the time of death due to any
cause, or the date the subject was last confirmed to be alive for censored subjects. See last
confirmed alive date definition in this section.
Progression-free survival
PFS, in days, will be measured from the date of randomization until the first date that irPD is
assessed by independent radiology review or death, whichever comes first.
If a subject is alive and without centrally verified irPD at the time the total number of PFS
events is accrued, PFS is defined as the time from the date of the randomization to the date of
the last tumor assessment as a censored value. In the event that the date of tumor assessment
is unavailable (ie, there is no tumor assessment after randomization), the randomization date
will serve as the censoring date instead.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 19 of 33
Progression-free survival rate
PFS rate for a certain time interval is defined as number of subjects having a PFS event or
censored during that interval. For subject having PFS events (i.e. disease progression per
independent radiology review or death), the month in which a PFS event occurred will be
determined using (PFS event date – randomization date + 1)/30.4375. For subjects without a
PFS event during the study (censored for PFS), the month in which the subject censored will
be determined using (censored date – randomization date + 1)/30.4375..
Progression-free survival – sensitivity analysis censored for alternative anticancer
therapy
The sensitivity analysis of PFS, in days, will be measured from the date of randomization
until the first date that PD is verified by independent radiology review or death, whichever
comes first.
If alternative anticancer therapy—not including therapy administered at sub-therapeutic
doses for symptom palliation only—was initiated prior to centrally verified PD or death, PFS
is defined as the time from the date of randomization to the start date of alternative anticancer
therapy as a censored value. Otherwise, if a subject is alive with no centrally verified PD and
no alternative anticancer therapy at the time the total number of PFS events is accrued, PFS
is defined as the time from the date of randomization to the date of the last tumor assessment
as a censored value. In the event that the date of tumor assessment is unavailable (ie, there is
no tumor assessment after randomization), the randomization date will serve as the censoring
date instead.
Sum of diameters
SOD = sum of long axis for non-nodal lesions and short axis for nodal lesions for target/new
lesions.
Total measured tumor burden
TMTB is established at baseline as the sum of the longest diameters (SOD)—the shortest
axes should be used for lymph nodes—of all target lesions (≤ 2 lesions per organ, ≤ 5 lesions
total).
At each subsequent tumor assessment (TA), the SOD of new, measurable lesions (≥ 10 mm
[lymph nodes ≥ 15 mm in shortest diameter]; ≤ 2 new lesions per organ, ≤ 5 new lesions
total) is added to the SOD of the target lesions to provide the updated TMTB:
TMTB = SOD target lesions + SOD new, measurable lesions
Percentage changes in TMTB at each TA describe the size and growth kinetics of both old
and new, measurable lesions as they appear.
TMTB, baseline and maximum decrease or minimum increase from baseline
Baseline TMTB is defined as the non-missing TMTB value at baseline prior to the initial
administration of study-required treatment.
Change in TMTB from baseline = (TMTB at post-baseline visit) – (TMTB at baseline).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 20 of 33
Maximum decrease or minimum increase is defined as the smallest value of change from
baseline in TMTB.
Unconfirmed irPD (irRECIST only)
“Unconfirmed irPD” is defined as a finding of irPD assessed by the independent radiology
review at or before Week 12 (81-87 days post C1D1) and not verified by a repeat,
consecutive imaging assessment obtained at least 4 weeks later and verified by independent
radiology review. Unconfirmed irPD after Week 12 will be considered irPD.
Week 12
Week 12 is defined as 81-87 days post C1D1.
6. ANALYSIS POPULATIONS
6.1 SAFETY POPULATION
The Safety population will include all subjects who receive at least one dose of IP. This
population will be used for safety analyses. If the randomized treatment arm differs from the
actual treatment, the subject will be analyzed according to the actual treatment arm. See Section
5 definitions of actual and randomized treatment arm.
6.2 INTENT TO TREAT POPULATION
The ITT population will include all randomized subjects in the study. This population will be
used for baseline and efficacy analyses. If the randomized treatment arm differs from the actual
treatment at any drug dispensed periods for a given subject, that subject will be analyzed
according to the randomized treatment arm.
6.3 PER PROTOCOL POPULATION
The Per Protocol (PP) population will include all ITT subjects who meet eligibility criteria, have
target lesion at baseline verified by the independent radiologist, have at least one tumor
assessment after receiving at least one dose of IP, and have no important protocol deviations that
could impact efficacy assessments. Since the PP population is a subset of the ITT population,
subjects will be analyzed according to the randomized treatment arm.
7. INTERIM ANALYSES
There will be no formal IA beyond the real-time analyses of safety data to support the safety
review by the DSMB.
8. DATA REVIEW
8.1 DATA HANDLING AND TRANSFER
Data will be entered by investigational sites into a clinical database built with DataLabs version
4 and exported as SAS® version 9.4 or higher datasets (SAS Institute, Inc., Cary, NC). Converted
datasets will be created using SAS® and following the standard Clinical Data Interchange
Standards Consortium (CDISC) Standard Data Tabulation Model (SDTM; version 1.2,
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 21 of 33
implementation guide version 3.1.2) conventions. Derived analysis datasets will be generated
using SAS® and following standard CDISC Analysis Dataset Model (ADaM) conventions. Data
analyses including summary tables, figures, and listings (TFLs) will be produced using SAS®.
Adverse events will be coded using the Medical Dictionary for Regulatory Activities (MedDRA
version 16.0) to assign a system organ class (SOC) and preferred term (PT) to each AE.
Concomitant medications will be coded to preferred drug names using the World Health
Organization Drug Dictionary (WHO-DD 2013MAR01DD [Basic]).
Clinical data from external vendors will be transferred electronically on a periodic basis.
Vendors include:
• ACM: Central Lab data
• Perceptive: Imaging and IXRS data
See the PRA Data Management Agreement for further details.
8.2 DATA SCREENING
Beyond the data review and cleaning built into the PRA Data Management Plan, the PRA
programming of analysis datasets and TFLs will provide additional data review.
Two database locks are planned for the study, one for the primary endpoint of PFS and the other
for the secondary endpoint of OS. For each of the 2 database locks, the review of an early TFL
dry run on clean subjects and a later TFL dry run on the nearly finalized database will allow for
further data review prior to finalization. The second dry run TFLs will be discussed with
VentiRx in a data review meeting to identify any final data issues and seek corrections prior to
finalization of the database.
In the event the OS analysis is triggered prior to the PFS analysis, that is, the requisite number of
PFS events will not be able to be accrued prior to the scheduled OS analysis (ie, 12 months after
the last subject is randomized), the OS analysis will be held and both PFS and OS will be
analyzed at the same time when the total number of PFS events is accrued, in which case only
one database lock will be planned.
In either case, the PRA statistician and VentiRx must approve database finalization.
9. STATISTICAL METHODS
All analyses will use SAS® version 9.4 or higher. Summary tables will be organized by treatment
arm: Combination Arm (SoC + Motolimod) versus Control Arm (SoC + Placebo). In the case of
a discrepancy between randomized and actual treatment, efficacy displays will use randomized
treatment arm and safety displays will use actual treatment arm. All available study data will be
used in the analyses. CRF data will be included in data listings for the ITT population. Missing
data will not be imputed, except via censoring in survival analyses.
In keeping with ICH E9, center effect will not be included in the analysis models as it is
recognized that there will be limited numbers of subjects per center in this trial. However,
randomization stratification factors and/or their interaction terms with treatment may be
explored. Actual (ie, corrected) values of stratification factors will be used in statistical models,
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 22 of 33
while randomized values may be used exploratory analysis, if applicable. If subjects switch
platinum therapy type, then the initial platinum therapy type will be used for subgroup analyses.
Unless otherwise noted, categorical data will be presented using counts and percentages, with the
number of subjects in the analysis population by treatment arm as the denominator for
percentages. Percentages will be rounded to one decimal place. Continuous data, unless
otherwise noted, will be summarized using the number of observations (n), mean, standard
deviation, median, minimum, and maximum. Minima and maxima will be rounded to the
precision of the original value, and means, standard deviations, medians, and confidence
intervals (CIs) will be rounded to one decimal place greater than the precision of the original
value, up to a maximum of 3 decimal places. P-values will be presented with 3 decimal places
(0.xxx), with values less than 0.001 presented as < 0.001. The primary test of PFS, secondary
test of OS, and all other statistical tests will be conducted using a one-sided significance level of
0.10. No multiplicity adjustments are planned.
9.1 SUBJECT DISPOSITION
Subject disposition of all randomized subjects will be summarized and will include the number
and percentage of subjects for the following categories (see Section 5 for definitions): Safety
population, ITT population, PP population, subjects with centrally verified irPD, subjects with
death without centrally verified irPD, subjects ongoing in the treatment phase, subjects who
discontinued early from the treatment phase, subjects with death any time through survival
follow-up, subjects alive and ongoing in survival follow-up, and subjects who discontinued early
from survival follow-up. Breakdowns of the corresponding reasons for treatment and study early
discontinuation will also be summarized. The reasons are those included on the CRF page for
EOT and EOS, respectively. Randomization assignments, subject population data, and subject
disposition and entry criteria data will be listed.
Completeness of follow-up will be examined in two ways. First, currentness (ie, recentness) of
follow-up in months (see definition in Section 5) will be examined relative to the data cutoff date
for intermediate analyses or the study end date at the end of the study. Number and percentage of
subjects with currentness of follow-up of < 3 months, 3 to < 6 months, 6 to <9 months, 9 to < 12
months, and ≥ 12 months will be summarized for the ITT population by treatment group and
overall. In addition, the number and percentage of subjects with EOS due to loss to follow-up or
withdrawn consent occurring in each interval will be tabulated. Secondly, duration of follow-up
in months (see definition in Section 5) will be described with summary statistics by treatment
group and overall for ITT population censored subjects with respect to the primary endpoint,
PFS by independent central assessment according to irRECIST.
9.2 PROTOCOL DEVIATIONS
See definition of protocol deviation in Section 5. Protocol deviations for the ITT population will
be imported into SAS® for inclusion in a table and a subject data listing. Important protocol
deviations will be summarized and include the number and percentage of subjects for the
following categories for the ITT population: inclusion criteria, exclusion criteria, IP, assessment
of safety, assessment of efficacy, informed consent, prohibited medication, stratification error, or
other.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 23 of 33
9.3 TREATMENTS
9.3.1 Extent of Study-required Treatment Exposure
Dosing data for IP will be summarized by treatment arm for the safety population to include
duration of exposure (in weeks), total exposure (in mg/m2), dose intensity (in mg/m2/week),
percent relative dose intensity (%), and number of cycles dosed. Total exposure (in mg/m2) will
be summarized by cycle.
Dosing data for cetuximab, cisplatin, and 5-FU will be summarized by treatment arm for the ITT
and safety population to include duration of exposure (in weeks), total exposure (in mg/m2), dose
intensity (in mg/m2/week), percent relative dose intensity (%), and number of cycles dosed. Total
exposure (in mg/m2) for each of the above treatments will be summarized by cycle.
Dosing data for carboplatin will be summarized by treatment arm for the ITT and safety
population to include duration of exposure (in weeks), total exposure (in mg), dose intensity (in
mg/week), percent relative dose intensity (%), and number of cycles dosed. Total exposure (in
mg) will be summarized by cycle.
See definitions in Section 5. Information regarding subjects’ dosing regimen will be listed.
In addition, number and percentage of subjects with dose delay or dose reduction of study-
required treatment will be tabulated by treatment arm and overall for the ITT population.
9.3.2 Concomitant Medications
Concomitant medications will be tabulated for the Safety population by treatment arm and
preferred drug name using counts and percentages. The number and percentage of subjects using
at least one medication within each treatment arm will also be displayed. See Section 5 for
definition of concomitant medications. Concomitant medications will be included in a by-subject
data listing.
9.4 DEMOGRAPHIC AND BASELINE CHARACTERISTICS
Demographic data will be summarized for the ITT population. Demographic data will include
summary statistics for age, age group (< 40, 40–49, 50–59, 60–69, 70–79, ≥ 80 years), gender,
race, ethnicity, height (m), and weight (kg). Baseline disease characteristics will include human
papilloma virus (HPV) status at screening (for subjects with oropharyngeal carcinoma only),
prior systemic therapy for SCCHN (yes, no), ECOG performance status (0, 1), and platinum
therapy assigned at randomization (cisplatin, carboplatin).
General medical history will be tabulated by SOC and PT using counts and percentages for the
ITT population.
Prior cancer treatment will be tabulated for the following categories using counts and
percentages for the ITT population: surgery (yes, no), radiotherapy (yes, no), setting of
radiotherapy (prophylactic, palliative, adjuvant, primary, other), chemotherapy (yes, no), setting
of chemotherapy (adjuvant, neoadjuvant, concomitant with radiotherapy, other), prior cetuximab
(yes, no), other systemic therapies (yes, no), and setting of other systemic therapies (adjuvant,
neoadjuvant, concomitant with radiotherapy, other).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 24 of 33
SCCHN history will be tabulated for the following categories using counts and percentages for
the ITT population: disease stage (T, N, and M and I, II, III, IV, IVA, IVB, or IVC) at initial
diagnosis and screening, histologic grade, and location of primary cancer. In addition, disease
state at study entry will be derived as de novo metastatic disease or recurrent disease (local only
or metastatic). Summary statistics for duration from initial diagnosis to randomization in days
and duration from recurrent or metastatic diagnosis to randomization in days (see definitions in
Section 5) will be provided.
Smoking and alcohol history will be tabulated for the ITT population. Smoking and alcohol
history will include summary statistics for the following: cigarette smoking status (never, current
[within last 30 days], former [over 30 days]), number of cigarettes per day, other forms of
tobacco status (never, current [within last 30 days], former [over 30 days]), number of days per
week of other smoked tobacco use, alcohol status (never, current [within last 30 days], former
[over 30 days]), and number of drinks per day.
Demographic, general medical history, prior cancer treatment, SCCHN history, and smoking and
alcohol history data will be listed by subject.
9.5 EFFICACY ANALYSES
Tumor responses assessed by a central radiologist who is blinded to subject treatment assignment
and independent from the clinical sites will serve as primary clinical efficacy data for the trial.
The primary efficacy analysis will be performed on the ITT population. If randomized treatment
arm differs from actual treatment arm for a given subject, that subject will be analyzed according
to randomized treatment arm (see definition of randomized treatment arm in Section 5).
9.5.1 Primary Efficacy Endpoint
PFS Based on Independent Central Assessment According to irRECIST
The primary efficacy endpoint, PFS based on central assessment by a blinded independent
radiologist, will be summarized and displayed by treatment arm using Kaplan-Meier methods
(SAS® PROC LIFETEST). Point estimates (25th, 50th, and 75th percentiles) will be provided,
along with a one-sided 90% CI with lower bound, i.e., (a, +∞), where (a, b) is two-sided 80%
confidence interval. In this way, the estimated lower bound might be available even though the
estimated percentile is not available. Treatments will be compared for the ITT population using a
stratified log-rank test controlling for randomization stratification factors as the primary analysis.
The one-sided stratified log-rank test p-value is calculated as
Prob(Z > z-score),
where
z-score is the ratio of rank statistics of the log-rank test for treatment group over its estimated
standard error and Z represents standard normal distribution.
The hazard ratio between the 2 treatment arms, as well as the associated one-sided 90% CI and
p-value, will be presented using a Cox proportional hazards regression (SAS® PROC PHREG)
model. A hazard ratio less than 1 indicates that subjects treated with motolimod achieve
improvement compared to those treated with placebo. Therefore, the corresponding one-sided
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 25 of 33
90% CI for hazard ratio will be (0, b), if a and b are the lower and upper confidence bounds
based on a two-sided 80% CI. The one-sided p-value derives based on the following hypothesis
H0: Hazard Ratio ≥ 1
vs Ha: Hazard Ratio < 1
The one-sided p-value is α/2 if the estimated hazard ratio is less than 1; 1-α/2 otherwise, where
α is the Wald chi-square p-value from the Cox proportional hazards regression (equivalent to the
two-sided p-value). The Cox regression model will be fitted to PFS with treatment arm and
randomization stratification factors as factors. Each randomization stratification factor by
treatment arm as interaction terms will be explored once the data are unblind. If the p-value for
interaction terms is smaller than 0.05, the interaction terms will be added as factors in the Cox
regression model for the unblind delivery. Subjects who do not have a PFS event during or after
the study will be censored as described in Section 5. A Kaplan-Meier plot will be presented.
As a supplementary analysis, number and percent of subjects PFS rate will be tabulated by
treatment arm and overall for the ITT population in 6-month time intervals (see definition of PFS
rate in Section 5).
9.5.2 Secondary Efficacy Endpoints
PFS Based on Investigators’ Assessment According to irRECIST
PFS based on investigator assessment according to irRECIST criteria will be summarized and
analyzed in the same manner as PFS based on independent central review by a blinded
radiologist.
PFS Based on Independent Central Assessment According to RECIST 1.1
PFS based on independent central assessment according to RECIST 1.1 criteria will be
summarized and analyzed in the same manner as PFS based on irRECIST, including analysis of
number and percentage of subjects PFS rate in 6-month time intervals.
Overall Survival
OS will be summarized and analyzed in the same manner as PFS. Subjects who do not die during
the study or during the follow-up period will be censored as described in Section 5.
Tumor Response Based on Independent Central Assessment and/or Investigators’
Assessment According to irRECIST or RECIST 1.1
For each secondary endpoint involving tumor response, assessments per the independent central
review according to irRECIST will be presented and analyzed foremost. Selected secondary
endpoints will have investigator assessment and/or assessment according to RECIST 1.1 criteria
analyzed as well.
The number and percentage of subjects achieving objective response (CR or PR) will be
tabulated for the ITT population by treatment arm. The number and percent of subjects achieving
disease control (SD, NN, PR, or CR) will be tabulated in the same manner. As well, the number
and percent of subjects exhibiting each level of best tumor response (CR, PR, SD, NN, PD
[including unconfirmed PD] or NE) will be presented by treatment arm for the ITT population.
Cochran-Mantel-Haenszel (CMH) tests (SAS® PROC FREQ) will be used to compare tumor
response rates between the 2 treatment arms while controlling for the randomization stratification
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 26 of 33
factors. In addition, maximum decrease or minimum increase in TMTB from baseline for ITT
population will be presented as a waterfall plot with vertical bars representing the sorted values
of changes.
DOOR measured in days will be summarized and displayed by treatment arm using Kaplan-
Meier methods, respectively. Subjects who do not have complete or partial response, as well as
those without an end date for complete or partial response will be censored as described in
Section 5. DDC measured in days will be summarized and displayed identically. Subjects who
do not have disease control (CR, PR, SD, or NN), as well as those without an end date for
disease control will be censored as described in Section 5. Point estimates (25th, 50th, and 75th
percentiles) will be provided, along with one-sided 80% CIs. Treatments will be compared for
the ITT population using a stratified log-rank test controlling for randomization stratification
factors as the primary analysis.
Efficacy data will be listed by subject.
9.5.3 Sensitivity Analyses
Sensitivity Analysis of PFS Based on Independent Central Assessment and Censored for
Alternative Anticancer Therapy
As a sensitivity analysis for the primary endpoint only, the PFS analysis based on central
assessment by a blinded independent radiologist according to irRECIST will be repeated using
an alternate set of censoring rules as described in Section 5.
Per Protocol Population
Analyses on the PP population will be performed for the primary efficacy endpoint and serve as
supportive analyses for the ITT analyses.
9.6 SAFETY ANALYSES
9.6.1 Adverse Events
Adverse events will be collected from the first dose of study-required medication administered
on Cycle 1 Day 1 until 7 days after the last dose of any study medication. TEAEs are those
which first occur or increase in severity after the first dose of IP.
Adverse events will be coded using MedDRA to assign a system organ class (SOC) and
preferred term (PT) to each adverse event. Each adverse event will also be given toxicity grade
defined using the NCI CTCAE version 4.03 grade for severity, ie, toxicity grade in CRF (1 =
Mild, 2 = Moderate, 3 = Severe, 4 = Life-threatening, 5 = Death).
Lower-level terms for injection site reactions (injection site reaction, erythema, redness,
irritation, nodule, itching, pain, tenderness, bruising, swelling, discoloration) will be included in
the higher-level term of Injection site reaction.
An overall summary of TEAEs including the following categories will be presented by actual
treatment arm for the Safety population:
• Total number of TEAEs reported
• Number and percentage of subjects reporting at least one TEAE
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 27 of 33
• Number and percentage of subjects with at least one TEAE occuring in at least 5% of
subjects
• Number and percentage of subjects with at least one Grade 3 or higher TEAE
• Number and percentage of subjects with at least one serious TEAE
• Number of subjects with a TEAE with outcome of death
• Number and percentage of subjects with at least one TEAE leading to discontinuation of
study-required treatment (IP, 5-FU, cetuximab, and/or platinum therapy)
The number and percentages of subjects reporting TEAEs, categorized by MedDRA body
system and PT, will be presented by actual treatment arm and overall. Note that counting will be
by subject, not event, and subjects are only counted once within each SOC or PT. Similarly, the
following tables will be provided:
• Number and percentage of subjects with TEAEs occurring in at least 5% of subjects
• Number and percentage of subjects with Grade 3 or higher TEAEs
• Number and percentage of subjects reporting serious TEAEs
• Number and percentage of subjects with TEAEs leading to death
• Number and percentage of subjects with TEAEs leading to discontinuation of study-
required treatment (IP, 5-FU, cetuximab, and/or platinum therapy)
• Number and percentage of subjects with TEAEs leading to dose reduction of study-
required treatment (IP, 5-FU, cetuximab, and/or platinum therapy)
• Number and percentage of subjects with TEAEs leading to dose delay of study-required
treatment (IP, 5-FU, cetuximab, and/or platinum therapy)
• Number and percentage of subjects with TEAEs leading to dose interruption of study-
required treatment (IP, 5-FU, cetuximab, and/or platinum therapy)
Tabulations will be sorted alphabetically by SOC and by preferred term within each SOC.
A summary of TEAEs, categorized by severity, will be provided by treatment arm and overall.
Subjects with multiple events within a particular SOC or PT will be counted under the category
of their most severe event within that body system or PT. For a given subject, if the severity
grade is missing for all TEAEs with the same preferred term, the AEs will be counted only once
for that term under the “Missing” severity category. If a subject has both missing and non-
missing severity grades for TEAEs with the same preferred term, the missing severity of the
TEAE will be treated as the lowest severity grade.
TEAEs will also be reported by preferred term only by treatment group (alphabetically) and for
just the SoC + Motolimod arm (by descending frequency of the number of subjects reporting the
TEAE).
A summary of deaths including the following categories will be presented by actual treatment
arm for the Safety population:
• Number and percentage of subjects who died by cause of death
• Number and percentage of subjects who died within 120 days of randomization by cause
of death
• Number and percentage of subjects who died on study-required treatment or within 30
days of last study-required treatment dose by cause of death
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 28 of 33
• Number and percentage of subjects who died more than 30 days after last study-required
treatment dose by cause of death
TEAEs, non-TEAEs, serious TEAEs, DLTs and deaths will be listed separately for subjects.
9.6.2 Laboratory Data
Blood samples for hematology and chemistry laboratory tests will be obtained at screening and
within 72 hours prior to each Day 1 dose and at the EOT if not completed within the previous 14
days. Urinalysis samples will be obtained at screening and at the EOT if not completed within
the previous 14 days.
Laboratory data will include parameter values, normal ranges, and out-of-range flags. Laboratory
parameters are listed in Table 2 in Section 5, and will be sorted by the order listed in the table.
Laboratory test results will be converted and reported in International System of Units (SI) units.
Clinical laboratory data summaries for safety analyses will include the following tables by
treatment arm for the Safety population:
• Hematology and chemistry results and changes from baseline by cycle and study day
• Urinalysis results and changes from baseline for continuous variables
• Urinalysis results at baseline and post-baseline for categorical variables
For change from baseline tables, descriptive statistics will be shown for baseline, specific
scheduled post-baseline time points, and the change from baseline to each of these post-baseline
time points.
In addition, continuous parameters for hematology, chemistry, and urinalysis will be displayed
graphically over time by treatment arm.
9.6.3 Vital Signs
Vital signs will be assessed at screening, Day 1 of each cycle, Day 15 of cycles 1–6, and EOT if
not completed within the previous 14 days. Vital signs parameters will include pulse rate,
respiration, systolic and diastolic blood pressure, temperature and weight.
Change from baseline by cycle will be summarized for vital signs parameters for the Safety
population. Descriptive statistics will be shown for baseline, EOT, and the change from baseline
to EOT visit. Vital signs data will also be listed by subject.
9.6.4 ECOG Performance Status
ECOG performance status will be assessed at screening, Day 1 of each cycle and EOT if not
completed within the previous 14 days.
The number and percentage of subjects by ECOG performance status will be summarized at
screening, baseline, last cycle of chemotherapy, and EOT for the Safety population.
ECOG status data will be listed by subject.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 29 of 33
9.6.5 Electrocardiograms
12-lead ECG results will be assessed locally at screening, one hour post IP dose (±15 min) on
Day 8 of Cycles 1 and 3 and EOT. ECG parameters will include heart rate, PR interval, QRS
duration, QT interval, and RR interval. The QT intervals will be corrected for heart rate by the
Bazett’s and Fridericia’s formula (QTcB = QT/[RR]1/2 and QTcF = QT/[RR]1/3 respectively).
A change from baseline summary will be displayed for ECG parameters for the Safety
population. Descriptive statistics will be shown for baseline, scheduled visits, and the change
from baseline to these visits. The incidence of outliers in maximum absolute QTcF and QTcB
intervals (> 450 to ≤ 480, > 480 to ≤ 500, and > 500 msec) and the maximum absolute
uncorrected QT intervals (> 500 msec) over all post-treatment evaluations, as well as in QTcF
and QTcB maximum changes from baseline (> 30 to ≤ 60 and > 60 msec) over all post-treatment
evaluations will be summarized by treatment arm.
ECG data will be listed by subject.
9.7 ANALYSES FOR EXPLORATORY ENDPOINTS
9.7.1 Genetic Polymorphisms Affecting Response to TLR8 Agonist or to
Cetuximab
9.7.2 Immune Biomarker Response
9.7.3 Effect of Tumor Immune Cell Subsets on Response to Treatment and/or
Clinical Outcome
9.7.4 PK Profile of Motolimod
A sparse blood sampling schedule to evaluate motolimod levels in the plasma of study subjects
was included in the design of study A-202. Blood was collected predose (time t=0), and at
approximately 0.75 and 8.0 hours (h) following the initial dose of motolimod (Cycle 1, Day 8).
The 0.75 h sampling time point was selected as it corresponds to maximum plasma
concentrations (Cmax) of motolimod following subcutaneous (SC) administration at a dose level
of 3.0 mg/m2. The 8.0 h sampling time point occurs between 1 and 2 plasma half-lives (t1/2),
when levels of motolimod are readily quantified following a 3.0 mg/m2 SC dose. The three
collection time points of 0, 0.75 and 8.0 h allow an approximation of motolimod exposures, or
area under the plasma concentration time curve from 0 to 8 h (AUC0-8) to be assessed for each
subject randomized to the motolimod treatment.
For subjects randomized to the motolimod treatment arm, an AUC0-8 will derive from motolimod
plasma levels measured in the three collection samples (0, 0.75 and 8 h). Descriptive statistics
including: n, mean, geometric mean, standard error (SE), std, coefficient of variation (CV),
median, minimum, and maximum will be determined for both Cmax (observed plasma
concentration at 0.75 h) and AUC0-8 from the subjects that received motolimod. This population
pharmacokinetic assessment will provide an estimate of motolimod exposures in SCCHN
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 30 of 33
patients given a 3.0 mg/m2 SC dose, as well as provide information on the inter-subject
variability of Cmax and AUC0-8 parameters in this study.
10. QUALITY CONTROL AND VALIDATION
PRA's goal is to ensure that each TFL delivery is submitted to the highest level of quality. Our
quality control and validation procedures will be documented separately in the study specific
quality control plan.
11. REFERENCES
[1] Jedd D. Wolchok, Axel Hoos, Steven O'Day, et al. Guidelines for the Evaluation of Immune
Therapy Activity in Solid Tumors: Immune-Related Response Criteria. Clin Cancer Res
2009;15:7412-7420. Published OnlineFirst November 24, 2009.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 31 of 33
APPENDIX 1 GLOSSARY OF ABBREVIATIONS
5-FU Fluorouracil
ADaM Analysis Dataset Model
AE Adverse event
ALB Albumin
ALP Alkaline phosphatase
ALT (SGPT) Alanine aminotransferase (serum glutamic pyruvic transaminase)
ANC Absolute neutrophil count
AST (SGOT) Aspartate aminotransferase (serum glutamic oxaloacetic transaminase)
AUC0-8 Area under the plasma concentration time curve from 0 to 8 h
BOR Best overall response
BUN Blood urea nitrogen
CBC Complete blood count
CDISC Clinical Data Interchange Standards Consortium
CI Confidence interval
Cmax Maximum concentration
CMH Cochran-Mantel-Haenszel
CR Complete response
CRF Case report form
CT Computed tomography
CTCAE Common Terminology Criteria for Adverse Events
CTMS Clinical Trials Management System
CV Coefficient of variation
DCR Disease control rate
DDC Duration of disease control
DLT Dose-limiting toxicity
DOOR Duration of objective response
DSMB Data and Safety Monitoring Board
ECG Electrocardiogram
ECOG Eastern Cooperative Oncology Group
EOS End of study
EOT End of treatment
h Hours
HCT Hematocrit
HGB Hemoglobin
HPV Human papilloma virus
HR Hazard ratio
IA Interim analysis
ICH International Conference on Harmonization
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 32 of 33
IP Investigational product
irRECIST Immune-related Response Evaluation Criteria in Solid Tumors
ITT Intent to Treat (population)
IV Intravenous
IXRS Interactive voice/web response system
K Potassium
LDH Lactate dehydrogenase
m Meter
MCH Mean corpuscular hemoglobin
MCHC Mean corpuscular hemoglobin concentration
MCV Mean corpuscular volume
MedDRA Medical Dictionary for Regulatory Activities
Mg Milligram
Min Minute
mL Milliliter
MRI Magnetic resonance tomography
Na Sodium
NCI National Cancer Institutes
NE Not evaluable
ORR Objective response rate
OS Overall survival
PD Progressive disease
PFS Progression free survival
PK Pharmacokinetic
PP Per protocol (population)
PR Partial response
PT Preferred term
QTcB QT corrected (Bazett’s formula)
QTcF QT corrected (Fridericia’s formula)
RBC Red blood cell
RDW Red blood cell distribution width
RECIST Response Evaluation Criteria in Solid Tumors
SAE Serious adverse event
SAP Statistical analysis plan
SC Subcutaneous
SCCHN Squamous cell carcinoma of the head and neck
SD Stable disesase
SDTM Standard Data Tabulation Model
SE Standard error
SGOT (AST) Serum glutamic oxaloacetic transaminase
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Sponsor: VentiRx Pharmaceuticals, Incorporated Statistical Analysis Plan Protocol No: VRXP-A202 25-MAY-2016/ Version 2.0
Page 33 of 33
SGPT (ALT) Serum glutamic pyruvic transaminase
SI International system of units
SoC Standard of care
SOC System organ class
SOD Sum of diameters
STD Standard deviation
SC Subcutaneous
t1/2 Time at which concentration is half maximum
TA Tumor assessment
TEAE Treatment emergent adverse event
TMTB Total measured tumor burden
TLR8 Toll-like receptor 8
TFL Tables, figures, and listings
WBC White blood cell
WHO-DD World Health Organization Drug Dictionary
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 Statistical Analysis Plan
Version 0.2 CONFIDENTIAL Page 1 of 4
Appendix 2
1.0 INTRODUCTION
This appendix to the Active8 statistical analysis plan describes the primary analyses for the study’s exploratory endpoints relating to translational research (TR). All Active8 TR assessments are exploratory endpoints of the study; as such, multiple investigative and hypothesis-generating analyses may be conducted in addition to those described herein.
2.0 EXPLORATORY ENDPOINT RATIONALE AND OBJECTIVES:
The primary goal of the TR analyses is to identify a biomarker or biomarkers that will predict clinical response to the investigational treatment (EXTREME [cetuximab + platinum + 5FU] + motolimod). Specifically, we seek to identify a baseline immune signature and/or an immune response that will predict the clinical outcome of irPFS, PFS1.1, OS, tumor response, disease control, or AEs in subjects receiving the investigational agent.
Additionally, the correlation between exploratory endpoints will be evaluated, and mixed-model approaches will be explored. The prognostic value of each translational research analysis will also be investigated.
2.1. Baseline Immune Status and Immune Response
The pharmacologic response to activation of TLR8 by motolimod can be measured in part by the qualitative and quantitative response of plasma cytokines and chemokines. In Active8, the response in >80 of these proteins (HumanMAP® panel; Myriad RBM) to subcutaneous dosing with investigational product (IP; motolimod or placebo) is assessed in vivo on Cycle 1 Day 8 and Cycle 3 Day 8 of study treatment.
A patient’s in vivo pharmacodynamic response to dosing with motolimod may predict clinical outcome following treatment with EXTREME + motolimod.
2.2. TLR8 Single Nucleotide Polymorphisms (SNPs)
An alteration in the gene encoding for Toll-like receptor 8, located on the X chromosome (Xp22.2), may modify an individual’s immune response to natural and synthetic TLR ligands, including motolimod. In turn, this may affect clinical outcome following study treatment.
Specimens were collected from Active8 participants who provided appropriate informed consent at the time of study entry. The specimens were genotyped for TLR8 SNPs.
2.3. Fc-Gamma Receptor (FcγR) Polymorphism
FcγRIIIA belongs to the FcγR family and is involved in antibody-dependent cell-mediated cytotoxicity (ADCC) in NK cells and in cytokine release by macrophages. The 3 FcγRIIIA genotypes may affect clinical outcome following study treatment. In addition, ADCC mediated through FcγRIIA, which also belongs to the same FcγR family, is carried mainly by macrophages. The 3 FcγRIIA genotypes may also affect clinical outcome following study treatment.
Specimens were collected from Active8 patients who provided appropriate informed consent at the time of study entry. The specimens were genotyped for FcγR polymorphisms.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 Statistical Analysis Plan
Version 0.2 CONFIDENTIAL Page 2 of 4
2.4. Immune Score and tissue marker expression
The type, density, and location of immune cell infiltrates in various kinds of tumors may be prognostic1,2,3 and may also predict response to therapy.
Archival tissue from Active8 subjects is analyzed by IHC with multiple immune markers. The density (positive cells/HPF) of the following markers will be assessed: CD3, CD8, CD45RO, PD-L1, CD68, and FOXP3 in 2 locations (tumor core vs invasive margin) for every sample. Additional analyses based on other relevant markers may be performed.
3.0 ANALYTIC PROCEDURES
3.1. Immune Response
Individual cytokines and chemokines are quantitatively assessed and reported for each patient. Analyte values below the limit of quantification will be replaced by the assay’s least detectable dose value. For the in vivo assay, the Cycle 1 Day 8 and Cycle 3 Day 8 response approximately 8 hours after dosing with motolimod will be compared to pre-dose levels.
The primary analyses will include analytes that are known to be induced by motolimod based on previous-completed non-clinical and clinical trials, and include but may not be limited to:
in vivo: IL-1ra, IL-6, IL-8, IL-10, MMP-9, G-CSF, MCP-1, MIP1-β, and GH
The identified analytes are significantly correlated within the assay, and thus will be evaluated in aggregate. The mean log-fold change across the selected analytes will be calculated for each subject, and modeled quantitatively and with the use of categories based on the median response (low vs high). Correlate analyses will be performed using traditional linear or generalized linear models, and may account for other potential clinical and demographic predictors.
As secondary analyses, the above analyses will be repeated with the analytes grouped according to biological function (e.g., innate, inflammatory, regulatory). Resulting p-values will be corrected for multiple testing using the false discovery rate approach of Benjamini and Hochberg4 with a threshold of 20%.
This step will also be repeated for each individual analyte used in the primary analyses. Due to the large number of variables, interaction effects will not be assessed here.
Additional analyses may include but are not limited to:
multivariate models based on all measured analytes using generalized linear regression models.
baseline predictors (i.e. analyte concentrations before drug treatment), to see if non-specific responses correlate with the clinical outcomes.
3.2. TLR8 SNPs
For each Active8 participant, TLR8 SNPs are reported as A only (AA), G only (GG), or both (AG).
The primary analysis will group patients with AA and AG genotypes and compare clinical outcomes to those of GG patients following treatment with EXTREME + motolimod.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 Statistical Analysis Plan
Version 0.2 CONFIDENTIAL Page 3 of 4
Additional analyses will compare AA vs AG + GG, as well as the 3 genotypes independently.
3.3. FcγR Polymorphisms
For each Active8 patient, FcγRIIIA polymorphisms are reported as FF, VV, and VF. The primary analysis will group patients with VV and VF genotypes and compare clinical outcomes to those of FF patients following treatment with EXTREME + motolimod. Additional analyses will compare VV vs VF + FF, as well as the 3 genotypes independently.
Additionally, FcγRIIA polymorphisms are reported as HH, RR, and HR. The primary analysis will group patients with HH and HR genotypes and compare clinical outcomes to those of RR patients following treatment with EXTREME + motolimod. Additional analyses will compare HH vs HR + RR, as well as the 3 genotypes independently.
3.4. Immune Score
For each Active8 tissue sample, scores (positive cells/HPF) for each marker tested will be reported as described in §2.4. The primary analysis will include CD3, CD8, and CD45RO. For each sample, an Immune Score will be derived from the 3 marker scores.
The primary analysis will compare clinical outcomes following treatment with EXTREME + motolimod in subjects with low Immune Score vs high Immune Score.
Additional analyses may be performed for the rest markers (PD-L1, CD68, and FOXP3).
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

Active8 Statistical Analysis Plan
Version 0.2 CONFIDENTIAL Page 4 of 4
Appendix References
1. Miecnik, B., et all. Histopathologic-Based Prognostic Factors of Colorectal Cancers Are Associated With the State of the Local Immune Reaction. Journal of Clinical Oncology (2011). doi: 10.1200/JCO.2010.30.5425.
2. Galon, J., et al. The Immune Score as a New Possible Approach for the Classification of Cancer. Journal of Translational Medicine (2012). doi: 10.1186/1479-5876-10-1.
3. Galon, J., et al. Towards the Introduction of the ‘Immunoscore’ in the Classification of Malignant Tumors. Journal of Pathology (2014). doi: 10.1002/path.4287.
4. Benjamini, Y. & Hochberg, Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the Royal Statistical Society Series B (1995). doi:10.2307/2346101.
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � ����
"�,������89:;�;<=>?�:;�@AB@:ABC�D=<�A@<�EFGE=:<:AB�HIE<:G:HIA<;JKH@A;@EL���������� � ���� ���M� ) NO:A:GIO8E:IO;JB@P�Q>FA<:R:FEL-����.�/��0S���������&(�T������0U�����V ���W�& �������&(�X �� ����U����/
Y=OO�8FZ<�[:F\ 8ID=OIE�[:F\ ]@�K<=>?�F;=O<;�_@;<F> �� � ���%,����� &� �"��&���� �&
�aF�IEF�=H>I<:AB�<9F�>F;:BA�@R�<9:;�;:<FJ�bFIEA�c@EFJ����������,������+������ �������(�� ���� ���� ��)*+���� ���� ���� �&�d�@R�d�$�(����-����.�/��0���+����"��&��e����������V����e�-����"��&�N9Fc@<9FEIH?�_O=;�NF<=Z:cID�:A�N@cD:AI<:@A�a:<9�[8fghiij�:A�_I<:FA<;�a:<9FG=EEFA<�@E�kF<I;<I<:G�Kl=Ic@=;�NFOO�NIEG:A@cI�@R�<9F�mFI>�IA>�]FGn������ $���� �&�� �����$� �+ ��&����$���������&�����������������������$��������&�������� �&��+����* ���)�V�����*� ����&��&������� ������ ��������+ �� ��&��������W)")�S�&�� �o+������)��� &����&�� � ����$��&�� ���)QAR@EcI<:@A�HE@P:>F>�D?�pF;H@A;:DOF�_IE<?qL���������� � ���� ���M� )��_=EH@;F�����������$���������&������� � ���������*�������$�������+�+ ��$�� �������,������ ����������� �� �� �#� ��� ���� � �� �$������� &� �&��� 4�r"��%-s���� ��&�,�������������t� ���� ������ ���� ����t�u�SW�t ����� ��+������� ���������� ��&�,���� ���� ������ ���� ����t�u�SW�t� ����� �� ����r�� �& �&�$� ��v�"w�s)" $���� �&�+�� ������+�+ ��,���� �������+ �� ��&)N@A>:<:@A QA<FEPFA<:@A _9I;F� � �� U�"#� ��������$�%� &� �&�-� 4 ��*(��������� �� ����
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � ����
8��*(�� ���� ���8��*(������ ���8��*(�9�$����� ��8��*(��� ��"��&������( :����+����� �"��&��8���*�( ;�� ���(�� �&�<�&�:����+������!&��(�� � �����;���*�����! �4��*(�=� &������>� ��� �� ��?�� �����+�&��?�:�+����* ��?�@�� ���;������A���� ���������(���� ����@$$� � �������( ;�� �&�<�&?�8�����B���&?��� ����������&�"��&��$�������� �������������� �������� ���������������������� �������������� ���������!�� �� �� �"#� �������� � �� �$�����%� &� �&�-� 4CDEFGHID�JKLME�NHFOKPDP�QR�STUVW����� ��%����$���� ����� ��&���� �(��� &� �&��� 4��#� ��� ���� � �� 8��*�:�$� ���� + �� ����$�(������� �X)")�Y8;������ ���ZGH[\DH�E[GPR�PD[]KJE�]E�NHFOKPDP�QR�DL[KC_�\]Ha]IDG[KI]JE�bLIcV��� ���@�� ��!� �����(�� � ��������$$� ��$���������������"@����"@�� �����������*��*������Y"�$�� �������,����� ����������� �� �� �"��%-)�d�����Y� �(� ����� �����0������ $��������� ���� ��������� �&�<�&�e�"� �& ���@�� ��!� �����(�� � �������� $����$���������������"@��+������"@�� ������� &+������+����?��� ��&��*� ���� �����*��$� ��� � �*����������� ���� �� ���?��������� ����&��� ��*�?������ �������?����� �����? �&�f�W)�d�����Y� �(�;����� �����0������ $��������� ���� ���������� �&�<�&�e��� � ��������$$� ��$���������������"@��+������"@�� �����������*��*�����@"�$�� �������,����� ����������� �� �� �"��%-)�d�����Y� �(�;����� ������������� $��������� ���� ��������� �&�<�&�e��� � ��������$$� ��$���������������"@����"@�� �������g� ��+����������� ��)d�����Y� �(�;����� �����0������ $��������� ���� ���������� �&�<�&�e�Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � ����
�� � ��������$$� ��$���������������"8����"8�� ������&�� ����$�������������)9�����:� �(�;����� �����0������ $��������� ���� ���������� �&�<�&)�=��� � ��������$$� ��$���������������"8����"8�� ������&��� ��� ������ ��)9�����:� �(�;����� �����0������ $��������� ���� ���������� �&�<�&)�=��� � ��������$$� ��$���������������"8����"8�� ������&�� ����$�&��� ��� ����)9�����:� �(�;����� �����0������ $��������� ���� ���������� �&�<�&)�=�8�����8�� ��!� �����(�� � ��������$$� ��$������ ������������,����������������������������� ����� �&��� ���� ��� �)�9�����:� �(�;����� �����0������ $��������� ���� ���������� �&�<�&�=��� � �������*����� ������������� �� ���� ��������������$�� ��������� ��>�.� *�������� ����� �����,���������,���� �����*����)�9�����:� �(�" ������*�=��� � �������������� �4����������� ��� ����&���� ����������&�� ����$� ��4����? ��4����?� �&���$� ���� �4�������,���������,���� �����*����)�9�����:� �(�" ������*?�� �����@ ��.?� �&��� �����@ ��.�=��� �������A�$����������9�����:� �(��� �����@ ��.�=�B��� ��&�B�������( ��C"��&��"� ���@ ��( D��������B��� ��&�"��&����������@ ��( "�����������/B��� ��&���� �����������@ ��( "�����������/�E:�� ��& � � ��� ����& ���$����� ����� �� ����FGHIJ GJJKLMNOPMQNHRNMQKSMJB�������� �(� ������ ��� �&� ����� ������������������������E�)��*��F�,������� &��������&���@ ��.� �&�@ ���C�$� ����& � � ���$��/� � ���?�$��,�&����&���*���@ ���.� �&����$��.�& �� � ���������&��� �����*������)����� ����E����*��F�8�� ���� ����E;T��C�*�>���F�,������� &��������&��@ ����$� ����& �� � ���$�� � ����$�/� � ���)C�:T�E�����*��F�,������� &��������&���@ �����U�$� ����& �� � ���$�� ����$�/� � ���)������ ��E����� ��&��(�U���*��V��� ����*�&���(��C��*��F�,������ &��������&�,��4���������&��� �����*������)@��*(����������>�.�;*����@��*(�� ���� ���8�����- �(� � �� ���@��*(������ ���8�����- �(�� ���@��*(�C�$����� ��8�����- ��(C�:T
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � 8���
9$�&��:����� ��; ��+���� � ��(� ������ ��� �&� ����� ��������� ���� ���<�)��*��=�,������� &��������&���> ��.� �&�> ���?�$� ����& �� � ��$��/� � ���@�$��,�&����&���*���> ���.� �&����$��.�& �� � ����������&��� ����*������)����� ����<����*��=�A�� ���� ����<;B��?�*�C���=�,������� &��������&��> ����$� ����& �� � ���$�� � ����$�/� � ���)?�:B�<�����*��=�,������� &��������&���> �����8�$� ����& �� � ���$�� ����$�/� � ���)������ ��<����� ��&��(�8���*��D��� ����*�&���(��?��*��=�,������ &��������&�,��4���������&��� �����*������)>��*(�� ���� ���A�����- �(� � �� ���>��*(������ ���A�����- �(�� ���>��*(�?�$����� ��A�����- ��(?�:B9$�&��:����� ��>��*(��� ��EFGHIJFK�EFLMNIOGIPQR�������� �� �&�S�&@�&���������&@��� ��� ������&@�� � �����*�������&�����+ �� �������� $���� �&�$$� ��$������������� ��� ����,���� ���� ������ ���� ���@�?�:B� �&� ����� ���������*��*������*�������$�������+�+ ��������T� ���,������ ����������� �� �� ��#� ��� ���� � �� �$������� &� �&�� 4)AUV9��W�9"(��� ���A�T� ��+�(�� � ��������$$� ��$���������������"A����"A�� �����������*��*������:"�$�� �������,����� ����������� �� �� �"��%-)"� �& ���A�T� ��+��(�� � �������$��,��*����,���������,���� �����*����(" $����$������������� &+������+����@��� ��&��*� ���� ������*��$� ��� � �*����������� ���� �� ���@�������� ����&��� ��*�@������ �������@����� �����@� �&�9�X)9$$� ��$���������������"A���������*��*�����A"�$�� �������,������ ����������� �� �� �"��%-)9$$� ��$���������������"A����A��@�>AU�@�>��@� �&�>>��������9�W"�� �&��+ �� ��������&����&����� &��*����+��,)9���� ����A�T� ��+��(
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � 8���
�� � ���*����� ������������� �� ���� ��������������$�� ��������� ��9�.� *�������� ����� �����,���������,���� �����*����)�� � ���������� �4���������������������������":�� ��� ����&���� ����������&�� ����$ ��4����;� ��4����;� �&���$� ���� �4�������,���������,���� �����*����)�� � ��������$$� ��$������ ������������,����������������������������������� �&��� ���� ��� �;� ��� ����&����������� �������������� �����������������,���������,���� ����*����)�� �����������<�$���������):=�9>-?("��@� ���,�������� �����&�$�����*��������A,�������B�& ��C� �&�#� ��$��&����@� ���,�������� �&�D�&��(������$����� �����*����(�":��E������������":��E��� ��)���� ����������,���������������!�>��� ����*� �����4����AF���& ��C;������ �����4��.�AF���& ��C� �&�+����.�,��4��AF���& ��C������ $���)���������,��������+ �� ��&������������ ��&��?�>"�� ������ A���?�>"�C� �&� �$���&���� ����&����&����� &��*���)=�����&����&���� �$�� ����$�&��� �����*������;� ��+��� ��� �� ��������������&����� ������ �&���@� ���,������&��*�����?�&�$���� ������+ �� ����)"��@� ���,�������$��,�&�$�����+�+ ��������G�������� $��������� ������@� ������ �&�D�&)��HIJKJLJIJMN�OPQRSTUMJRP�QSRT�MVW�XUMJRPUI�YJLSUSN�RQ�ZW[J\JPW] __abc�d_�efgdahaefdi�ab�f�djkl�a�fb�ame_gdfbd�eig_bfn�kihaa_bo�pfnq�rad�l_jgk_hd_g�fbk�sfmanl�mimtig�_g�sgaibk�ft_jd�kihakabc�d_�u_ab�f�djklo�p_�nifgb�m_gift_jd�da�djklv�l_j�_g�l_jg�k_hd_g�mfl�h_bdfhd�di�djkl�giifgh�dfss�jabc�dih_bdfhd�eg_wakik�tin_ro�x_g�cibigfn�abs_gmfda_bv�yifgb�zt_jd�]nabahfn�{djkaio|*���?��*�����$��"��&�(�� �.�6� ��� �&��&�����A|&���;�"����C"�����?��*�����$��"��&�(�� |��| �����%� ��������������(��-}SJMWSJU>� ������������� (|������� �&�,�����*���������+�&��,���������$��&� �����%����*� ������ ���*� ���� �$���&��#� ��� ���� � �� �$������� &� �&��� 4Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � /���
8 ��*�� ������ ����������� �� �� �&��� ����� ��� ��������+�������������� ��&�,���������� ���� ���$��� ����������� �� �� �&��� ��9���� ������� ��� ������������� ������*������!�:�.��� ���$� *�����&��;�<=����$� � ���� ����$������9 ��� �������� ��,>���� �>� �&���� �� �$�� ����� ��&������ ������*�� �������������*������������&� ���� ��� ���� ��� �����?��$� ����,��������&� ��+�������� �(� ���* ��+����������*� � ������;� ������������� (@��� ���,�� ����� �� ������ �� ��+��� ������ ��- ��� ���*� �>�� ��+ ���*� �&>����������� � �� � �� "��*��������� &� ����A�B�,��4���������� �&�C �������������� � ���� � ������� ��>�������� &��������&�$��� ��C�&�"��%-� �&� �����&� ���� ��/�������������&��� ����� ����� ���� �����,���� ����+����* ��� �� *����A����& ����������� �&�C ������ �����,���� ��� �����&��,��������,��4�9���#��������$�� ���� ������� �������������+������ ���$�� ����� ����������������$������� ������ ����� ���� �����,���� ��������� ���,���������& ��D�,���� ����� �� ���>���������� ����$�� ���� ����.�& ��9 ��+�� �������&��� ��� �����������#�����*����� ��D�,����$� ����,����%:�"�*��$� ��� �&� �&��� ���,������/��������*� �������� ���$��&��*�$� ���%������$� ��������� ��� ��*� � �>�,���������� ������$�E�F� �� ��+�������� ��&������ � �4��� � ��>�E��F� �� ��+������� ��&��������� ��+� �� � ��>���E���F������ ��*� � �� �� ��+������� ��&,�������+�&�� ��$�&��� ��� �&��� ��� � ������� ��� &��������&�$������ ���������� �&�C ���>�,���������� ������$� &G�+ ������ ������ ���$����� ��� � ��<����� �&�������� �� ��� � ����� �� ��&������$����,�����������&���HIJKLMKN�LJO�PIMLKQIJN�RJSITULKQIJ�STIU�KVW�XLKQIJLY�PQZTLT[�IS�\WOQMQJWDownloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � ����
89�:;<=>�?9=;�<@9AB�BCDE�EBAFGH�G9A�9=�G9A=�F9IB9=�?<G�I9>B<IB�BC;�EBAFG=;E;<=IC�EB<JJ�AED>K�BC;�I9>B<IB�D>J9=?<BD9>�L=9MDF;F�@G�BC;�EL9>E9=NO:;<E;�=;J;=�B9�BCDE�EBAFG�@G�DBE�P:D>DI<:8=D<:ENK9M�DF;>BDJD;=�QRP8�>A?@;=STUVWXYZ[\X]��_ab�cdeaf�ghijdhkl�ghijdhklmkdba�cdjdbln�opqjkljlr��+�������$�s�4 �� ��$��!�&� ��" ��� ��t������� 4u�s�4 �� �u�r����&�"� ���u�����vmkdba�cdjdbln�wjxyhpkj�,���%� ��*��z� �*��!�&� ��{���|�+�����%����u�� ��$��� u�r����&�"� ���u�0����� ��$��� �� � ���s�� � ����$������ � �� �&�}� ����� ��~��s�}�}� �&�&u�� ��$��� u�r����&�"� ���u�0���vr��+�������$�� ��$��� �" �����*�!����� � ���������t ���� u�� ��$��� u�r����&�"� ���u�0��0�r��+�������$�� ��$��� �-��������������+��� � ���������t��s�*����u�� ��$��� u�r����&�"� ���u�0����mkdba�cdjdbln�whxhpjahr��+�������$���� &�� � ���������s��� u���� &u�r����&�"� ���u�.���v�s�} ��������� &�%� ��� ���"�������+��u���� &u�r����&�"� ���u�.����mkdba�cdjdbln��bxj�jpb%������)�{� � �� � ���������-�, �4u���� , ��u�r����&�"� ���u��0���mkdba�cdjdbln��xhpaj!��s�&������ � ���������z�� �&u�����& u�r����&�"� ���u���.�/mkdba�cdjdbln��bhp�j-���� ���{��*� �� � ���� ��u�tt�s�����u�{��*� u�r����&�"� ���u���/��Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � .���
��������� � ���8��������9�� �� :�;��*� :�<����&�"� ���:������=>?@AB�C@D@AEF�GDHD??��������9���!�&� ��������%�����:�% , ��:�<����&�"� ���:�0/.I0=>?@AB�C@D@AEF�JKK?>L?E-���,�������<��+�������M������*�" ���$�!�&� ������ *:�8������:�<����&�"� ���:�/�/��� ����� � ���������<�� � :�8������:�<����&�"� ���:�/�.��=>?@AB�C@D@AEF�ND>EDE<��+�������$�O �� ��� � �������������,&:�O �� �:�<����&�"� ���:�//��I=>?@AB�C@D@AEF�PLQ?E?D>D���� ������������� � ���������:�RR�! ����:�R���� � :�<����&�"� ���:�������������)������:�!S:�RR�!�� ����:�R���� � :�<����&�"� ���:�����/��0�/=>?@AB�C@D@AEF�TD?>A! �����������$��� � ���!�&� ���" ����*�:�! ���:�<����&�"� ���:��U��U=>?@AB�C@D@AEF�TDVWKD>B����"�&����O�������������+��� � ���������� ��X���%�4���Y �����:�! ��� �&:�<����&�"� ���:������� ��������&�- ��� ��!���� ���!�&� ��������Y�����& :�! ��� �&:�<����&�"� ���:���..0=>?@AB�C@D@AEF�TDEEDZ[QEA@@ES � �M ������ � ���8��������Y���:�! �� �������:�<����&�"� ���:�����I=>?@AB�C@D@AEF�T?Z[?\D>O � ���� � ���8��������S�����:�!� ��* �:�<����&�"� ���:�U.���%�����M�&�%� ����"����S�����:�!� ��* �:�<����&�"� ���:�U.���Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � 0���
��+�&�� ��� � ���8��������"���$���&9�!� ��* �9�:����&�"� ���9�;.��<=>?@AB�C@D@AEF�G?EEHIJ?" ����K����� � ���� ��9�KK�L��&*���9�!������9�:����&�"� ���9�/��;;L �����M�,����%���� �"�)�K���9�!������9�:����&�"� ���9�/����=>?@AB�C@D@AEF�NAODBD-�+ & �� � ������� � ��P��& ���K ����* �9�-�+ & 9�:����&�"� ���9�.0��/=>?@AB�C@D@AEF�NAQ�RDSTEU?JAV ������%�� � 4�!�&� ��������K�� ��9�-�,�% ������9�:����&�"� ���9����</=>?@AB�C@D@AEF�NAQ�WAJEAXY� �*�� �&�%� ��*��"�� � �����9��)Z)V��+����9�-�,�M�����9�:����&�"� ���9���.�;% 4��� 4�:��+�������!�&� ��������% 4��� 49�-�,�M�����9�:����&�"� ���9���/��=>?@AB�C@D@AEF�NAQ�[HJ\!������ � ���������K 4��"� ���9�-�,�6�49�:����&�"� ���9����;�����L����+���%���� �-�,�6�49�-�,�6�49�:����&�"� ���9�����/!����"�� ��!�&� ��������-�,�6�49�-�,�6�49�:����&�"� ���9�����0"����L�4�:��+�������!�&� ��������"����L�49�-�,�6�49�:����&�"� ���9����0;=>?@AB�C@D@AEF�NHJ@U�]DJH?>D:��+�������$�-����� ���� � ���� ����%����� ����%���9�-����� ���� 9�:����&�"� ���9���<00� 4��P�����:��+�������L ������!�&� ���������������" ��9�-����� ���� 9�:����&�"� ���9������=>?@AB�C@D@AEF�_U?H:��+�������$���� ��� ��Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � �����
��� ��� ��8�9��8�:����&�"� ���8�;<�/���<��:��+�������%���� ���$����+�� �&���+�� �&8�9��8�:����&�"� ���8�;;��/���+�� �&������ ���+�� �&8�9��8�:����&�"� ���8�;;�0<=>?@AB�C@D@AEF�GHAIJ>" ������ �����!�&� ��������K��&8�9��*�8�:����&�"� ���8�0������+�&�� ��� � ������������� �&8�9��*�8�:����&�"� ���8�0����=>?@AB�C@D@AEF�LA>>EMNOD>?D" ����P�4���� � ���������Q ���8��������+ �� 8�:����&�"� ���8��.�;<�������+ �� �"� ���%�������� � ���R��������%������8��������+ �� 8�:����&�"� ���8������:��+�������$���������*��� � ���R����������������*�8��������+ �� 8�:����&�"� ���8��<���=>?@AB�C@D@AEF�CJS@T�UDHJN?>D%����*��� � ����������� ������8�"����� ���� 8�:����&�"� ���8��0;�<=>?@AB�C@D@AEF�VA>>AEEAA�������������� !�����8����������8�:����&�"� ���8��.���=>?@AB�C@D@AEF�VAWDE:��+�������$���� ��"���,�������!�&� ��������� ��X �� �X �� �8���� �8�:����&�"� ���8��<�0��..<�" ��Y�����!���� ���!�&� ��������Z���" �%����8���� �8�:����&�"� ���8��.��;=>?@AB�C@D@AEF�[?HI?>?D���*��� �� � ���"�� � �����8��XZ ��$ �8����*��� 8�:����&�"� ���8������=>?@AB�C@D@AEF�\DET?>I@J>!�&� ��9� �*��Y�� � ���8��""�4 ��8�� ����*��8�:����&�"� ���8�00��.Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � �����
! &�* ��8���!�&� ��������� 9�� ����*��9�:����&�"� ���9�0.;��<=>?@A�B?C?@DE�F>DGH=D>=!�&� ������*��$���� ����!��, �4��9���� ����9�:����&�"� ���9�I���/8��� �8&+ � �&�%� ��� ��9�J� )� �, �� 9���� ����9�:����&�"� ���9�I���/BKH=DHLD�C=A�MHNNCOHLC?HLD���������� � ���� ���J� )P=Q@D?>RC?HLD"��&���� ��( ST� �����9�!U :��+�������$���� *"��&���� ��( ������V�����9�!U9���U :��+�������$���������*���WHL@�P=XHLYC?>H=����� ����� �� �� ������&���&�����������&���������� ���� ��)*+�J&����$����Z-���-����[(-���$����U�9�� � �� ���\9�������89����%$$�UU9�������] 9�U���� ��]-9�! �_ ���T�\9�� �& ���U9�%�������*��!)�8��� ���J�&���$��&��*����&��$������+���������4���� �����.� *���������������� &�������_� ���,���� &+ � �&����&������������ )������� � ������)����;�����Ia��Z�;[(�/.��0�)&�(���)��I.����.��;��)�����;���0�)�S�������;�! ���)������������ ���( ���������� � ���� ���J� )����� ���� ��)*+�J&����$���( -����.�/��0�����%������$��� �*��b�����"��&��JU�-�����( �����8�����V�����"������&( 8�������9�����V���������&( 8������09����� ���:�& �������&( �� ����9����/ �������$��&( �� ������/\��,�&����+�&�&�������������� � ���� ���J� )("��%-�%-"���8&&���� ������+ ���!�"%�����(Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020

���������� ������� �������������� ��������� ���������������������� �������������� ���������!�� �� �� �"#� ��������� � �� �$�����%� &'
�����(�� ���� ���� ��)*+� �����,����&��-����.�/��01���2-����.�/��03� �42�3��,5� �267� � �����
� � �� �� � �� 8�"#� ��������%� &� �&�-� 4�-��� ���-��� ��8�9� �&�� �� �&�:������� ��-��� ������%����*� ������-��� ���-��� ��8�"#� ��������-��� ������"��������� ����� ���� ���������� ��;����� ���<������� ��� �<*�����<����� �������!�� �� ��!� � �����$��� � �*� ��< ����<����� ������8�<������� ��� �=�����������+��<*�����=���*� �; ����������*� ��:$$� ���$�>��*��
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 06/27/2020