LOWERING YOUR CHOLESTEROL. PRESENTED BY RASGAS MEDICAL CENTRE.

of 7
Upload
mutiara-auliaCategory
view
215download
08/13/2019 Effect of a Cholesterol Lowering Diet
1/7
B A S I C S C I E N C E : O B S T E T R I C S
Effect of a cholesterol-lowering diet during pregnancy on
maternal and fetal Doppler velocimetry: the CARRDIP studyJanette Khoury, MD; Guttorm Haugen, MD, PhD; Serena Tonstad, MD, PhD; Kathrine Frey Frslie, MSc;
Tore Henriksen, MD, PhD
OBJECTIVE: The purpose of this study was to evaluate the effect of a low-cholesterol lowsaturated fat diet on Doppler indices in the fetus and mother.
STUDY DESIGN:Two hundred ninety nonsmoking white women, aged21-38 years, without previous pregnancy complications and carrying asingle fetus were assigned randomly to continue their usual diet (con-trol subjects; n 149) or to adopt a low-cholesterol lowsaturated fatdiet (intervention group; n 141) from gestational week 17-20 tobirth. Doppler velocimetry of the umbilical artery and both uterine ar-teries were assessed at gestational weeks 24, 30, and 36.
RESULTS:The physiologic gestational decrease in umbilical arterypulsatility index (PI) from week 24-30 was more pronounced in the
intervention group, compared with the control group, with median val-
ues (interquartile range) of 0.17 (0.29, 0.06) and 0.11
(0.25, 0.01), respectively (P .048). Assignment to the intervention
diet did not influence the changes in mean PI value of the 2 uterine
arteries (P .3). The change in umbilical artery PI and mean PI value
of the uterine arteries between weeks 24 and 36 were not significantly
different between the 2 groups (P 1.0 and .2 respectively).
CONCLUSION:Our study shows that a cholesterol-lowering diet during
pregnancy may modify fetoplacental circulation in mid pregnancy.
Key words:cholesterol-lowering diet, pregnancy, Doppler index
Cite this article as: Khoury J, Haugen G, Tonstad S, Frslie KF, Henriksen T. Effect of a cholesterol-lowering diet during pregnancy on maternal and fetal
Doppler velocimetry: the CARRDIP study. Am J Obstet Gynecol 2007;196:549.e1-549.e7.
Established risk factors for cardiovas-cular diseases and diabetes mellitusare more prevalent in pregnant womenwith placental insufficiency than in other
pregnant women.1-7The established asso-ciation between low birthweight and therisk of adult cardiovascular diseases thusmay indicate that the placentation is im-paired in women with cardiovascular riskfactors (for example, hyperlipidemia),whichresultsinplacentalinsufficiencyandsmall infants.1Several mechanisms may be
involved. Maternal hyperlipidemia mayreduce prostacyclin secretion and en-hance peroxidase production and resultin vasoconstriction and platelet aggrega-
tion and affect placental perfusion.8Moreover, dyslipidemia may induceacute atherosis that, together with coag-ulation disorders, result in local throm-bosisand placental infarctions, as seenincases with preeclampsia.1
In a randomized clinical trial, the Car-diovascular Risk ReductionDiet in Preg-
nancy (CARRDIP), we compared the ef-
fect of a low-cholesterol low-saturated
fat diet with the usual Norwegian diet
among white healthy women on mater-
nal cord and neonatal lipid concentra-tions and on pregnancy outcome. Ma-
ternal lipid concentrations were reduced
in the intervention group, and we ob-
served a prominent reduction in the in-
cidence of preterm delivery (37 weeks
of gestation) in this group. The diet had
no adverse effects, and there were no dif-
ferences between the intervention and
control groups with respect to other
pregnancy complications9or on biomar-
kersof endothelial activation, inflamma-
tion, and hemostasis, except for fetal tis-
sue plasminogen activator antigen
(tPAag), which were lower in the inter-
vention group.10The observed effects of
an antiatherogenic diet during preg-
nancy on maternal lipid profile could
lead hypothetically to local changes in
the fetomaternal interphase that were
not reflected in the systemic inflamma-
tory responses of pregnancy. This pre-
sumed localeffectof thediet may explain
the observed reductionin preterm deliv-eries in the diet group.
From the Department of Obstetrics and Gynecology, Rikshospitalet-Radiumhospitalet
Medical Center (Drs Khoury, Haugen, and Henriksen); the Department of Preventive
Cardiology, Ullevl University Hospital (Drs Khoury and Tonstad); the Section of
Biostatistics, Rikshospitalet-Radiumhospitalet Medical Center (Ms Frslie); and theUniversity of Oslo (Drs Haugen, Tonstad, and Henriksen), Oslo, Norway.
Presented in part at the 35th Congress of the Nordic Federation of Societies of Obstetrics andGynecology, Gothenburg, Sweden, May 20-23, 2006, and at the 4th World Congress onDevelopmental Origins for Health and Disease (DOHaD), Utrecht, the Netherlands, Sept. 14-16,2006.
Received June 15, 2006; accepted Jan. 16, 2007.
Reprints not available from the authors.
Supported by the Norwegian Council on Cardiovascular Disease.
0002-9378/$32.00 2007 Mosby, Inc. All rights reserved.doi: 10.1016/j.ajog.2007.01.017
See related editorial, page 497
Research www.AJOG.org
JUNE 2007 American Journal of Obstetrics & Gynecology 549.e1
8/13/2019 Effect of a Cholesterol Lowering Diet
2/7
Placental development and functionmay affectthe fetus,even thoughthe pla-centa apparently is functioning nor-mally.1The specific role of maternal nu-tritional status before or duringpregnancy on placental circulation and
function hasbeen explored only sparselyin humans.Doppler ultrasound velocimetry is a
valuable tool to evaluatefeto- and utero-placental blood flow.11-18Umbilical arteryvelocimetryhasbecome a routinemethodfor fetal surveillance in high-risk pregnan-cies. An increased uteroplacental vascularresistance, by means of uterine arteryDoppler evaluation, is associated withcomplications such as preeclampsia, pre-term delivery, small-for-gestational age,
and operative delivery.
19
In consideration of the relation be-tween placental dysfunction and cardio-vascular disease, we investigated the ef-fect of an antiatherogenic diet on thefetoplacental and uteroplacental circula-tion using Doppler velocimetry in theCARRDIP study.
MATERIAL AND METHODS
Participants
The CARRDIP trial has been describedpreviously.9 Two hundred ninety non-smoking white women aged 21-38 yearswho were carrying a single fetus were as-signed randomly to either adopt a low-cholesterol low-saturated fat diet or tocontinue their usual diet from gesta-tionalweeks17-20to birth.Womenwithprevious pregnancy complications wereexcluded. The intervention group (n 141) were asked to consume fish, low-fatmeats, oils, low-fat dairy products,
whole grains, fruits, vegetables, and le-gumes. The intervention diet aimed tolimit dietary cholesterol and to reducethe intake of saturated fat by replacingsaturated fat with mono- andpolyunsat-urated fat. The control group (n 149)was asked to consume their usual dietthat was based on Norwegian foodstuffsand not to introducemore oils or low-fatmeat and dairy products than usual. Toassess dietary compliance, weighed di-etary records were assigned on a prede-
termined day weekly throughout preg-nancy. The diet was recorded on 4 days
during gestation weeks 19-24 (period 1),on 6 days during weeks 24-30 (period 2),and on 6 days during 30-36 of gestation(period 3). Both the intervention andcontrol groups followed the same sched-ule of blood sampling, physicianand di-
etician visits, and assessments.
9
The investigator (S.T.) who was notin touch with the pregnant women cre-ated the randomization list from a ta-ble of random numbers. The dieticianin charge for giving the dietary advicewas given sealed dark envelopes thatwere numbered serially and that con-tained the randomization number andcode (control or intervention). Eachenvelope was opened by the dieticianwho assigned the encoded diet group
to each screened and eligible woman ina serial sequence. A specialist in obstet-rics and gynecology (J.K.) conductedthe initial examination and all the fol-low-up examinations, according to thestudy protocol; usual antenatal carewas provided by the participants phy-sician and/or midwife. Blinding in-cluded all medical personnel, with theexception of the dietician. In addition,the participants were told not to dis-close their dietary assignment to any of
the study staff or other participants.Of the 290 women who were assignedrandomly, 269 women completed thestudy: 127 women in the interventiongroup and 142 women in the controlgroup.Fourteenwomen(10%)in thein-tervention group dropped out of thestudy (11 before gestational week 24 and3 after week 24). In the control group,the correspondingnumber was7women(5%), all before week 24.9
Doppler measurementsDoppler velocimetry of the umbilical ar-teryandtheuterinearteryoneachsideofthe uterus was performed at gestationweeks 24,30,and 36.Gestational agewasbased on the ultrasound examination atweek 17-18 of gestation. Missing valuesat each follow-up visit were due to drop-outs from the study (n 18, 20, 21, re-spectively) or from 1 specific examina-tion because of preterm delivery (n 0,
0, 12, respectively), practical reasons (n 9, 7, 9, respectively), or because of dif-
ficulties in obtaining adequate Dopplersignals, especially from 1 or both of theuterine arteries (n 4, 5, 14,respectively).
Flow velocity waveforms were ob-tained with an ultrasound machine
(XP128/10OB; Acuson Corp, MountainView, CA) equipped with a 5-MHz con-vex probe and a 100-Hz high-pass filter.The umbilical artery blood velocity sig-nals were obtained from a free-floatingcentral part of the cord. Care was takento include only measurements that wereobtained at an insonation angle of30degrees during fetal apnea. Uterine ar-tery blood flow velocity was imagedtransabdominally by color Doppler flowmapping. Doppler velocity waveforms
were obtained from the main uterine ar-tery. The transducer was placed in thelower lateral quadrant of the abdomenand angled medially until the apparentcrossover of the external iliac arteryand the main uterine artery could beidentified. The pulsatility index (PI) wasmeasured in 3 subsequent waveformsfrom both the umbilical artery and eachof the 2 uterine arteries. The mean of the3 measurements was used in the statisti-cal analyses. All Doppler examinations
were performedby thesame investigator(J.K.) For umbilical artery PI, the in-traobserver (J.K.) and interobserver(G.H.) coefficients of variation were3.6% and 5.1%, respectively. For themean PI value of the uterine arteries, theintraobserver and interobserver coeffi-cients of variation were 10.4% and12.5%, respectively.
PIisanindirectcrudemeasureforbloodflow impedance with large variations in-side the normal range. PI levels, especially
in the umbilical artery, decrease signifi-cantlywithincreasinggestational ageas anexpression of the decreasingplacental vas-cular resistance.20,21We explored the de-gree of thisphysiologicdecrease inPIasanindicator of the effect of maternal dietaryintervention during pregnancy on the fe-toplacental circulation.
Statistical analysesThe assessment of the effects of a cho-
lesterol-lowering diet on Doppler ve-locimetry in the umbilical cord and
Research Basic Science: Obstetrics www.AJOG.org
549.e2 American Journal of Obstetrics & Gynecology JUNE 2007
8/13/2019 Effect of a Cholesterol Lowering Diet
3/7
each of the uterine arteries was part ofthe secondary hypothesis of the CARR-
DIP study and is part of the originalprotocol. Power calculations were
done in regard to the primary hypoth-esis (ie, reducing maternal and neona-
tal total cholesterol levels).9 A samplesize of 130 women in each group was
required to detect a 5% reduction inmaternal total cholesterol and a changeof 15% (approximately 8 mg/dL) in
neonatal total cholesterol levels ( .05; .20) in the intervention vs the
control groups. Given an expected rateof adverse pregnancy outcome of 25%(data based on the Norwegian Birth
Register), this number of participantshad approximately 65% power, with
set at .05, to find a 50% increase in theoccurrence of any adverse pregnancy
outcome. To account for dropouts, weaimed to include a total of 300participants.
We have earlier published the mean( SD) of dietary intake in the control
and intervention group of fat, micronu-trients, macronutrients,9 and differentfood categories10 based on all weighed
dietary records during the whole studyperiod. In contrast inTable 1,we give the
mean (SD) dietary intake calculated
fromweighed records thatwerecollected
in each of the3 differentperiods through
gestation; correlations between dietary
intakeand the change in Doppler veloci-metry at different periods through gesta-
tion are given in Table 3.
Box plots were used to illustrate the
pattern of PI levels for the intervention
and control group at the different time
points during the study period. We
used the Mann-Whitney test to evalu-
ate the differences in changes between
gestational weeks 24 and 30 or 36 be-
tween the intervention and control
group, because the distributions of the
differences were highly skewed. In cor-relation analysis, we used Pearsons
correlation coefficients to assess the as-
sociations between the dietary compo-
nents and Doppler velocimetry and be-
tween Doppler velocimetry and low-
density lipoprotein (LDL) cholesterol
in the control group and the interven-
tion group. Scatter plots were used to
illustrate the latter correlations. All
analyses were performed with SPSS
software (version 12.0; SPSS Inc, Chi-cago, IL). A 2-sided probability value
of .05 was considered statisticallysignificant.
RESULTS
Detailed characteristics of the interven-tion andcontrol group at randomizationare given elsewhere.9In brief, no differ-ences between the groups were observedin baseline characteristics such as age,parity, body mass index, other demo-graphic data, medical history, clinicaland laboratory examinations, and diet atrandomization.
Dietary compliance at differentperiods through the study
Weighed dietary records from baselineto gestation week 36 showed that theintervention group significantly re-duced their total mean intake of satu-rated fat and cholesterol and sig-nificantly increased their total meanintake of monosaturated oils, poly-saturated oils, fatty fish and fish prod-ucts, and vitaminsC, D, and E duringthe study period.9Table 1specifies di-etary intake at different gestation peri-ods and shows that compliance for
lowering the intake of dietary choles-terol and increasing the intake of vita-
TABLE 1
Dietary intake of fat, micronutrients, and fatty fish and fish products in the control and intervention groupsduring the different periods of weighed dietary record registration
Variable
Period 1 Period 2 Period 3
Control
group(n 141)
Intervention
group(n 127) Pvalue
Control
group(n 140)
Intervention
group(n 126) Pvalue
Control
group(n 137)
Intervention
group(n 124) Pvalue
Total fat* 32.5 4.7 29.6 5.2 31.9 4.3 30.0 5.0 32.5 4.1 30.2 4.8 ................................................................................................................................................................................................................................................................................................................................................................................
Saturated fat* 13.6 2.2 9.1 1.9 13.4 2.2 9.0 2.0 13.6 2.1 9.2 1.9 ................................................................................................................................................................................................................................................................................................................................................................................
Monounsaturated fat* 10.8 2.0 11.6 3.0 10.6 1.7 12.0 2.7 10.7 1.6 12.1 2.7 ................................................................................................................................................................................................................................................................................................................................................................................
Polyunsaturated fat* 5.6 1.5 6.3 1.6 5.4 1.5 6.5 1.7 5.6 1.4 6.5 1.7 ................................................................................................................................................................................................................................................................................................................................................................................
Cholesterol (mg/d) 271 102 210 88.3 263 77.4 214 74.1 265 77.4 224 77.4 ................................................................................................................................................................................................................................................................................................................................................................................
Fatty fish and products(g/d)
12.8 23.0 26.9 26.8 18.0 22.8 28.0 28.5 17.7 23.2 22.2 24.0 NS
................................................................................................................................................................................................................................................................................................................................................................................
Alpha-tocopherol(mg/d)
8.3 2.5 10.7 4.1 7.6 2.0 11.6 3.6 8.0 2.1 11.5 3.8
................................................................................................................................................................................................................................................................................................................................................................................
Vitamin C (mg/d) 154 63.0 182 80.0 158 61.7 178 72.3 154 66.7 179 81.8 ................................................................................................................................................................................................................................................................................................................................................................................
Period 1 (from randomization gestation weeks 17-20 to gestation week 24), period 2 (gestation weeks 24-30), and period 3 (gestation weeks 30-36). Data are given as mean SD. NS, notsignificant.
* Percent of energy. P .001, independent samples t-test for differences between the groups. P .05, independent samplest-test for differences between the groups.
www.AJOG.org Basic Science: Obstetrics Research
JUNE 2007 American Journal of Obstetrics & Gynecology 549.e3
8/13/2019 Effect of a Cholesterol Lowering Diet
4/7
min C was apparently better in the firstperiod after randomization than laterin the intervention group. Compliancefor higher intakes of fatty fish andproducts was low between gestationweeks 30 and 36 (period 3) in the in-tervention group.
Doppler velocimetry and dietaryinterventionThe number of women with availableDoppler indices in the control and inter-
vention group atweeks 24, 30, and 36aregiven in Table 2.The physiologic gesta-
tional decrease in umbilical artery PIfrom weeks 24-30 was more pronounced
in the intervention group, comparedwith the control group (Figure 1A; me-dian,0.17 [interquartile range,0.29,0.06] vs 0.11 [interquartile range,0.25, 0.01], respectively; P .048).The change in the mean PI value of bothuterine arteries, however, was not signif-
icantly different between thegroups dur-ing the same period (Figure 1B; median,0.09 [interquartile range,0.25, 0.01]
vs 0.08 [interquartile range, 0.19,0.03], respectively; P .303).
The change in umbilical artery PI andmean PI value of the uterine arteries be-tween weeks 24 and 36 and betweenweeks 30 and 36 did not differ betweenthe groups (Figure 1).
There were no casesof reversed abnor-
mal blood flow in the umbilical artery atthe assigned visits in either group. Nodifferences in the number of womenwith the presence of unilateral or bilat-eral uterine artery notching were seenbetween the groups at the assigned visits(data not shown).
Correlations between Dopplervelocimetry and dietaryinterventionThere was a significant negative correla-
tion between thedietary intakeof choles-terol from baseline to gestation week 30and the change in umbilical artery PI be-tween weeks 24 and 30 in the interven-tion group (Table 3). In addition, therewas a weak negative correlation betweenenergy from total fat intake and satu-rated fat intake and the change in umbil-ical artery PI in the same period only inthe intervention group. From gestationweeks 30-36, a significantnegativecorre-lation persisted between the dietary in-
take of cholesterolandthe changein um-bilical artery PI in the intervention
TABLE 2
Number of women in the control and intervention groups atrandomization (gestation weeks 17-20) and women with availableDoppler indices at the assigned visits at which the Dopplermeasurements were performed
Variable
Diet group
Week 17-20 Week 24 Weeks 17-30 Week 36
PI umbilical artery.....................................................................................................................................................................................................................................
Control group 149 141 138 131.....................................................................................................................................................................................................................................
Intervention group 141 125 127 123..............................................................................................................................................................................................................................................
Mean PI of the uterine arteries.....................................................................................................................................................................................................................................
Control group 149 140* 134* 120*.....................................................................................................................................................................................................................................
Intervention group 141 119* 124* 114*..............................................................................................................................................................................................................................................
* Number of women with available Doppler blood flow of both uterine arteries.
TABLE 3
Correlations between mean dietary intake of macro- and micronutrients in the control and interventiongroups from baseline (right after randomization gestation weeks 17-20) to week 30 and from weeks30-36 and the change in PI of the umbilical artery from weeks 24-30 and weeks 30-36, respectively
Mean dietary intake
PI weeks 24-30 >PI weeks 30-36
Control group Intervention group Control group Intervention group
Pearsonscorrelation
coefficient (r) Pvalue
Pearsonscorrelation
coefficient (r) Pvalue
Pearsonscorrelation
coefficient (r) Pvalue
Pearsonscorrelation
coefficient (r) Pvalue
Total fat* 0.01 1.0 0.16 .09 0.10 1.0 0.01 .9................................................................................................................................................................................................................................................................................................................................................................................
Saturated fat* 0.06 .5 0.17 .07 0.11 .2 0.01 1.0................................................................................................................................................................................................................................................................................................................................................................................
Monounsaturated fat* 0.09 .3 0.01 .9 0.09 .3 0.9 1.0................................................................................................................................................................................................................................................................................................................................................................................
Polyunsaturated fat* 0.02 .8 0.00 1.0 0.01 1.0 0.00 1.0................................................................................................................................................................................................................................................................................................................................................................................
Cholesterol (mg/d) 0.13 .1 0.22 .02 0.12 .2 0.25 .007................................................................................................................................................................................................................................................................................................................................................................................
Fatty fish and products(g/d)
0.03 .7 0.14 .1 0.06 .5 0.11 .2
................................................................................................................................................................................................................................................................................................................................................................................
Alpha-tocopherol(mg/d)
0.00 1.0 0.07 .5 0.15 .1 0.77 .4
................................................................................................................................................................................................................................................................................................................................................................................
Vitamin C (mg/d)
0.02 .9
0.00 1.0
0.29 .001
0.07 .5................................................................................................................................................................................................................................................................................................................................................................................* Percent of energy.
Research Basic Science: Obstetrics www.AJOG.org
549.e4 American Journal of Obstetrics & Gynecology JUNE 2007
8/13/2019 Effect of a Cholesterol Lowering Diet
5/7
group. No correlations were found forthe dietary intake of vitamins C and E orthe intake of fatty fish and products andthe change in umbilical artery PI in ei-ther group at the mentioned gestationperiods, except for vitamin C intake be-
tween weeks 30 and 36, which was corre-lated negatively with the change in um-bilical artery PI in the same period in thecontrol group (Tables 3). No correla-tions were found between the change inthe mean PI values of both uterine arter-ies and the dietary variables that were re-ferred to earlier in either group at thementioned gestation periods (data notshown)
Correlations between Doppler
velocimetry and LDL cholesterolin maternal and cord bloodThere was a significant lower increase inmaternal plasma LDL cholesterol levelsin the intervention group, comparedwith the control group from baseline(weeks 17-20) to week 36.9In the currentanalysis, there was a significant positivecorrelation between the change in ma-ternal plasma LDL cholesterol (weeks24-30) and the change in umbilical ar-tery PI under the same period in the in-
tervention group (ie, the lower the in-crease in LDL cholesterol the larger thegestational decrease in umbilical arteryPI; Figure 2A). No such correlation wasfound in the control group (Figure 2B).The change in umbilical artery PI fromweeks 30- 36 did not exhibit such corre-lation (data not shown). The change inthe mean PI values of both uterine arter-ies in the same periods that were men-tioned (Figure 2) did not show such cor-relation in either groups (data not
shown). There was no correlation be-tween fetal plasma LDLlevels (mixed ar-terialand venouscord blood)and Dopp-ler changes in the umbilical artery fromweeks 24-30 and 30-36 or changes in themean PI valuesof both uterine arteries inthe same periods.
Correlations between Dopplervelocimetry and tPAag incord blood
There was a tendency towards lowerconcentrations of tPAag in cord blood in
the intervention group, compared withthe control group (median, 5.4 ng/mL[interquartile range, 3.1, 7.7 ng/mL] vs
5.8 ng/mL [interquartile range, 3.5, 11.8ng/mL];P.0510). No correlations were
found between the change in umbilicalartery PI between weeks 24 and 30 or 36and tPAag in cord blood in either group.
However, in thecontrol group, there wasa tendency towards a negative correla-
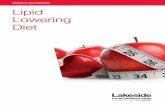
FIGURE 1
PI of the umbilical artery and mean PI of both uterine arteries at theassigned visits in the control and intervention groups
InterventionControl
1,75
1,50
1,25
1,00
0,75
0,50
0,25
UmbilicalarteryPI
wk 36
wk 30
wk 24
InterventionControl
2,10
1,80
1,50
1,20
0,90
0,60
0,30MeanPIvaluesofbothuterinearteries
wk 36
wk 30
wk 24
P = 0.048 P = 0.303
A B
Box plot for A, PI of the umbilical artery and B, the mean PI of both uterine arteries in the control
and intervention groups during the study period. The Y-axis represents PI values. The X-axis
represents the time at which the Doppler measurements were obtained. The circlesindicate outliers;
the stars indicate cases with extreme values. Probability values (Mann-Whitney test) refer to group
differences that are expressed as changes from gestation week 24 (start of Doppler measurements)
to gestation week 30.
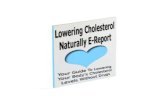
FIGURE 2
The relation between the change in LDL-cholesterol concentrationsand the change in umbilical artery
1209060300-30-60
Change in LDL-C mg/dlwk 30 minus wk 24
0,75
0,50
0,25
0,00
-0,25
-0,50
-0,75
Changeinumb
ilicalarteryPI
wk30minuswk24
Intervention r = 0.19
P= .04
1209060300-30-60
Change in LDL-C mg/dlwk 30 minus wk 24
0,75
0,50
0,25
0,00
-0,25
-0,50
-0,75
Changeinumb
ilicalarteryPI
wk30minuswk24
Control r = - 0.06
P=.5
A B
Scatter plot for the change in LDL-cholesterol concentrations ( LDL-C; milligrams per deciliters)
between weeks 24 and 30 and the change in umbilical artery PI during the same period in A, the
intervention andB, the control group. Correlation coefficients and corresponding probability values
are referred to in text boxesin the right-hand corner within each scatter plot.
www.AJOG.org Basic Science: Obstetrics Research
JUNE 2007 American Journal of Obstetrics & Gynecology 549.e5
8/13/2019 Effect of a Cholesterol Lowering Diet
6/7
8/13/2019 Effect of a Cholesterol Lowering Diet
7/7
pregnant women.26Notably, there wereno cases of idiopathic spontaneous pre-term delivery in the intervention group.Intheentirecohort,wefoundatendencytowards a lesser gestational decrease inumbilical artery PI from weeks 24-30 in
the preterm delivery group, comparedwith the term group: median, 0.02(25th, 75th percentile, 0.24, 0.12) inthe preterm group vs 0.15 (25th, 75thpercentile, 0.29, 0.02 in the termgroup; P .08). No other pregnancycomplication exhibited this tendency(data not shown). This may explain thereason that women who were prone togive birth to a premature baby (37weeksof gestation) were theonly womenwith adverse pregnancy outcome who
profited from the intervention diet. Wesuggest that the decrease in umbilical ar-tery resistance in the intervention groupmay have contributed to the differencein idiopathic spontaneous preterm de-livery between the groups. By achievingdecreased resistance in the umbilical ar-tery at mid gestation, the interventiondiet could have been associated with aless stressed fetus,which in turn mighthave delayed the onset of labor.27
Wehave demonstratedthat dietary in-
tervention can modify fetoplacental cir-culation in mid pregnancy. Specifically,the use of a low-cholesterol low-satu-rated fat diet during pregnancy may re-inforce the physiologic gestational de-creasein umbilical arteryPI levels in midgestation. f
ACKNOWLEDGMENTS
We thank the obstetric staff at the ultrasoundoutpatient clinic at the National University Hos-pital, Rikshospitalet in Oslo for their help in therecruitment process.
REFERENCES
1.Henriksen T, Clausen T. The fetal origins hy-pothesis: placental insufficiency and inheritanceversus maternal malnutrition in well-nourished
populations. Acta Obstet Gynecol Scand
2002;81:112-4.
2.Ray JG, Vermeulen MJ, Schull MJ, Re-
delmeier DA. Cardiovascular health after mater-
nal placental syndromes (CHAMPS): popula-
tion-based retrospective cohort study. Lancet
2005;366:1797-803.
3.Wikstrom AK, Haglund B, Olovsson M, Lin-
deberg SN. The risk of maternal ischaemic
heartdisease after gestational hypertensive dis-
ease. BJOG 2005;112:1486-91.
4.Pell JP, Smith GC, Dominiczak A, et al. Fam-
ily history of premature death from ischaemic
heart disease is associated with an increased
risk of delivering a low birth weight baby. Heart
2003;89:1249-50.
5.Sattar N, Ramsay J, Crawford L, Cheyne H,
Greer IA. Classic and novel risk factor parame-
ters in women with a history of pre-eclampsia.
Hypertension 2003;42:39-42.
6.Kaaja R, Tikkanen MJ, Viinikka L, Ylikorkala O.
Serum lipoproteins, insulin, and urinary prostanoid
metabolites in normal and hypertensive pregnant
women. Obstet Gynecol 1995;85:353-6.
7.Lorentzen B, Henriksen T. Plasma lipids and
vascular dysfunction in pre-eclampsia. Semin
Reprod Endocrinol 1998;16:33-9.
8.de Onis M, Villar J, Gulmezoglu M. Nutritional
interventions to prevent intrauterine growth re-
tardation: evidence from randomized controlled
trials. Eur J Clin Nutr 1998;52(suppl):S83-93.
9. Khoury J, Henriksen T, Christophersen B,
Tonstad S. Effect of a cholesterol-lowering diet
on maternal, cord, and neonatal lipids, and
pregnancy outcome: a randomized clinical trial.
Am J Obstet Gynecol 2005;193:1292-301.10.Khoury J, Henriksen T, Seljeflot I, Mrkerid
L, Frslic K, Tonstad S. Effects of an antiathero-
genic diet during pregnancy on markers of ma-
ternal and fetal endothelial activation and in-
flammation: the CARRDIP study. BJOG
2007;114:279-288.
11.Campbell S, Diaz-Recasens J, Griffin DR,et
al. New Doppler technique for assessing utero-
placental blood flow. Lancet 1983;1:675-7.
12.Laurin J, Marsal ??, Persson PH, Lingman
G. Ultrasound measurement of fetal blood flow
in predicting fetal outcome. BJOG 1987;
94:940-8.
13.Laurini R, Laurin J, Marsal K. Placental his-tology andfetalblood flowin intrauterinegrowth
retardation. Acta Obstet Gynecol Scand
1994;73:529-34.
14.Olofsson P, Olofsson H, Molin J, Marsal K.
Low umbilical artery vascular flow resistance
and fetal outcome. Acta Obstet Gynecol Scand
2004;83:440-2.15.Papageorghiou AT, Yu CK, Nicolaides KH.
The role of uterine artery Doppler in predictingadverse pregnancy outcome. Best Pract Res
Clin Obstet Gynaecol 2004;18:383-96.16.Pirhonen J, Erkkola R. Flow velocity wave-forms in the uterine artery in high risk pregnan-
cies. Ann Chir Gynaecol Suppl 1994;208:98-9.17.Strigini FA, Lencioni G, De Luca G, Lom-
bardo M, Bianchi F, Genazzani AR. Uterine ar-tery velocimetry and spontaneous preterm de-
livery. Obstet Gynecol 1995;85:374-7.18.van AsseltK, Gudmundsson S, Lindqvist P,
Marsal K. Uterine and umbilical artery velocim-etry in pre-eclampsia. Acta Obstet Gynecol
Scand 1998;77:614-9.19.Hofstaetter C, Dubiel M, Gudmundsson S,Marsal K. Uterine artery color Doppler assisted
velocimetry and perinatal outcome. ActaObstetGynecol Scand 1996;75:612-9.20.Arstrom K, Eliasson A, Hareide JH, Marshal
K. Fetal blood velocity waveforms in normalpregnancies: a longitudinal study. Acta Obstet
Gynecol Scand 1989;68:171-8.21.Voigt HJ, Becker V. Doppler flow measure-
ments and histomorphology of the placentalbed in uteroplacental insufficiency. J Perinat
Med 1992;20:139-47.22.Geppert A,GrafS, Beckmann R, etal. Con-
centration of endogenous tPA antigen in coro-nary artery disease: relation to thromboticevents, aspirin treatment, hyperlipidemia, and
multivessel disease. Arterioscler Thromb VascBiol 1998;18:1634-42.
23.Rush D, Kristal A, Navarro C, et al. The ef-
fects of dietary supplementation during preg-nancy on placentalmorphology, pathology,andhistomorphometry. Am J Clin Nutr 1984;39:
863-71.24.Mayhew TM. Fetoplacental angiogenesis
during gestation is biphasic, longitudinal andoccurs by proliferation and remodeling of vas-cular endothelial cells. Placenta 2002;23:
742-50.25.Kaufmann P, Mayhew TM, Charnock-
Jones DS. Aspects of human fetoplacental vas-culogenesis and angiogenesis: II, changes dur-
ing normal pregnancy. Placenta 2004;125:14-26.
26.Hvilsom GB, Thorsen P, Jeune B,Bakketeig LS. C-reactive protein: a serological
marker for preterm delivery? Acta Obstet Gy-necol Scand 2002;81:424-9.27.Lockwood CJ. Testing for risk of pretermdelivery. Clin Lab Med 2003;23:345-60.
www.AJOG.org Basic Science: Obstetrics Research
JUNE 2007 American Journal of Obstetrics & Gynecology 549.e7