Edward P. Sloan, MD, MPH, FACEP Basic Statistics for EM Research: Power Calculations.
Upload
lizbeth-rashCategory
view
236download
6
Edward P. Sloan, MD, MPH, FACEP
Hemophilia and Hemophilia and Rare Bleeding DisordersRare Bleeding Disorders

Edward P. Sloan, MD, MPH, FACEP
2007 EMA Advanced Emergency & Acute Care
Medicine Conference
Atlantic City, NJAtlantic City, NJSeptember 24, 2007September 24, 2007

Edward P. Sloan, MD, MPH, FACEP
Edward P. Sloan, MD, MPH FACEP
Professor
Department of Emergency MedicineUniversity of Illinois College of Medicine
Chicago, IL

Edward P. Sloan, MD, MPH, FACEP
Attending PhysicianEmergency Medicine
University of Illinois HospitalOur Lady of the Resurrection Hospital
Chicago, IL

Edward P. Sloan, MD, MPH, FACEP
DisclosuresDisclosures• Novo Nordisk grant to conferenceNovo Nordisk grant to conference• FERNE Chairman and PresidentFERNE Chairman and President• FERNE grants from Novo NordiskFERNE grants from Novo Nordisk• No financial disclosuresNo financial disclosures
• eMedicine source materialseMedicine source materials• Slide materials from Novo NordiskSlide materials from Novo Nordisk

Edward P. Sloan, MD, MPH, FACEP
www.ferne.orgwww.ferne.org

Edward P. Sloan, MD, MPH, FACEP
Global ObjectivesGlobal Objectives
• Maximize patient outcomeMaximize patient outcome• Utilize health care resources wellUtilize health care resources well
• Optimize evidence-based medicineOptimize evidence-based medicine• Enhance ED practiceEnhance ED practice

Edward P. Sloan, MD, MPH, FACEP
Sessions ObjectivesSessions Objectives
• Learn about hemophilia and RBDsLearn about hemophilia and RBDs• What are the diseases?What are the diseases?• How do patients present?How do patients present?• What are management principles?What are management principles?• What specific therapies?What specific therapies?• How to enhance pt outcomes?How to enhance pt outcomes?

Edward P. Sloan, MD, MPH, FACEP
Case Presentation
• 17 year old presents to ED • Known hemophilia A• Fell off of bicycle• Abdominal trauma• Hypotensive, tachycardic• Abdominal tenderness• What do you do?

Edward P. Sloan, MD, MPH, FACEP
ED Bleeding Disorder Patients: ED Bleeding Disorder Patients: Key ConceptsKey Concepts
• Identify the bleeding disorder
• Establish if bleeding is present
• Treat the bleeding
• Treat the bleeding disorder
• Establish endpoint for Rx success
• Disposition based on Dx, Rx, risk

Edward P. Sloan, MD, MPH, FACEP
Background
• Rare disorder: Affects fewer than 200,000 Americans
• (NIH office of Rare Diseases)
• Hemophilia• Other bleeding disorders• Rare Bleeding Disorders

Edward P. Sloan, MD, MPH, FACEP
Disease StatesDisease States

Edward P. Sloan, MD, MPH, FACEP
Hemophilia
• Hemophilia A • Congenital deficiency of factor VIII
(FVIII)
• Hemophilia B: Christmas Disease• Congenital deficiency of factor IX
(FIX)

Edward P. Sloan, MD, MPH, FACEP
Hemophilia
• Insufficient generation of thrombin by FVIIIa and FIXa complex
through the intrinsic pathway of the coagulation cascade

Edward P. Sloan, MD, MPH, FACEP
Coagulation CascadeCoagulation Cascade

Edward P. Sloan, MD, MPH, FACEP
Fibrin Clot StructureFibrin Clot Structure
Hemophilia A Normal Clot Structure

Edward P. Sloan, MD, MPH, FACEP
Hemophilia Severity
• Based on procoagulant levels or bleeding severity
• Severe: <1% clotting factor present Severe: <1% clotting factor present • Moderately severe: 1-5%Moderately severe: 1-5%• Mild: 5-40%Mild: 5-40%• Clinical bleeding severity may not Clinical bleeding severity may not
match amount of deficiency match amount of deficiency

Edward P. Sloan, MD, MPH, FACEP
Other Inherited Bleeding Disorders
• Congenital factor deficienciesCongenital factor deficiencies • von Willebrand’s Diseasevon Willebrand’s Disease• Other congenital platelet disorders Other congenital platelet disorders
• Glanzmann’s ThrombastheniaGlanzmann’s Thrombasthenia• Bernard Soulier SyndromeBernard Soulier Syndrome

Edward P. Sloan, MD, MPH, FACEP
von Willebrand’s Diseasevon Willebrand’s Disease
• Autosomally inherited bleeding disorder, mucocutaneous• Deficiency or dysfunction of the
protein termed von Willebrand factor (vWF)
• Primary hemostasis is impaired• Defective interaction between platelets and the vessel wall

Edward P. Sloan, MD, MPH, FACEP
Factor VII Deficiency
• Fewer than 200 cases of true Fewer than 200 cases of true factor VII deficiency have been factor VII deficiency have been reportedreported• Gene mutations, protein dysfunctionGene mutations, protein dysfunction• Factor VII coagulant activities Factor VII coagulant activities measured in the laboratory are measured in the laboratory are not not well correlated with bleeding well correlated with bleeding manifestationsmanifestations

Edward P. Sloan, MD, MPH, FACEP
Acquired Bleeding Disorders
• Vitamin K Deficiency• Severe Liver Disease
• Factors II, VII, IX and X are decreased• Platelets dysfunctional
• Renal Disease• Platelet dysfunction

Edward P. Sloan, MD, MPH, FACEP
Acquired Bleeding Disorders
• Oral Anticoagulant Therapy• Prolonged Use of Antibiotics
• Develop anti-platelet antibodies• Vitamin K deficiency
• Acquired Inhibitors (Antibodies)• Post malignancy• Related to pregnancy• Idiopathic• Elderly

Edward P. Sloan, MD, MPH, FACEP
Emergency Department Emergency Department EvaluationEvaluation

Edward P. Sloan, MD, MPH, FACEP
Patient Demographics
• Hemophilia • Present in childhood, esp with greater disease severity• All races• X-linked, recessive males

Edward P. Sloan, MD, MPH, FACEP
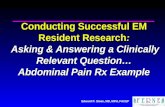
Patient PresentationsPatient Presentations
Mannucci et al. Blood 2004;104:1243-1252
15%
25%
13%
75%
81%
16%
75%70%
66% 65%
8%
30%
50%
38%
13%
25%
8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Epistaxis Menorrhagia Hematuria GI Joint Muscle CNS Post-partum/ post-
op
Mouth
Hemophilia RBDs

Edward P. Sloan, MD, MPH, FACEP
History
• What is the Bleeding Disorder?• vWD, Hemophilia A/B, other factor deficiency or platelet disorder

Edward P. Sloan, MD, MPH, FACEP
History
• What is the severity of the factor deficiency?
• Severe - < 1% factor present • Bleed spontaneously and often e.g. weekly
• Moderate – 1-5 %• Can have spontaneous bleeding but less frequent e.g. monthly
• Mild - > 5 %• Bleed only when hemostasis is challenged
e.g. trauma and surgery

Edward P. Sloan, MD, MPH, FACEP
History
• Do they have a inhibitor (assoc with congenital factor def)?• What is their HIV/Hepatitis Status?• How is the bleeding disorder being
treated?• When was your most recent treatment or infusion?• Are you taking other medications?

Edward P. Sloan, MD, MPH, FACEP
Hemorrhage HistoryHemorrhage History
• General - Weakness and orthostasis
• Musculoskeletal (joints) - Tingling, cracking, warmth, pain, stiffness, and refusal to use joint (children)
• CNS - Headache, stiff neck, vomiting, lethargy, irritability, and spinal cord syndromes

Edward P. Sloan, MD, MPH, FACEP
Hemorrhage HistoryHemorrhage History
• GI - Hematemesis, melena, frank red blood per rectum, and abdominal pain
• Genitourinary - Hematuria, renal colic, and postcircumcision bleeding

Edward P. Sloan, MD, MPH, FACEP
Hemorrhage HistoryHemorrhage History
• Other - Epistaxis, oral mucosal hemorrhage, hemoptysis, dyspnea (hematoma leading to airway obstruction), compartment syndrome symptoms, and contusions; excessive bleeding with routine dental procedures

Edward P. Sloan, MD, MPH, FACEP
Physical Exam
• General hemorrhage signs
• Organ-specific hemorrhage signs
• Hepatitis signs
• Infections signs
• Medic Alert bracelet
• Wallet

Edward P. Sloan, MD, MPH, FACEP
Physical Exam
• General hemorrhage signs
• Organ-specific hemorrhage signs
• Hepatitis signs
• Infections signs
• Medic Alert bracelet• Wallet (Hemophilia Treatment Center Card)Hemophilia Treatment Center Card)

Edward P. Sloan, MD, MPH, FACEP
Laboratory Testing
• CBC (Hb, platelets, WBC)• PT, aPTT• vWF:Ag (Von Willibrand factor antigen)• Ristocetin Co-Factor
• Measures vWF activity to identify qualitative vWF disorder
• Factor coagulant activity • e.g. VIII:C, IX:C in hemophilias
• Bleeding time?

Edward P. Sloan, MD, MPH, FACEP
Lab Results for Bleeding DisordersLab Results for Bleeding Disorders Prolonged Prolonged PTPT
Prolonged Prolonged aPTTaPTT
Prolonged PT Prolonged PT and aPTTand aPTT
Inherited Inherited DisordersDisorders
• FVII DeficiencyFVII Deficiency • vWF Type 2&3 vWF Type 2&3 • FVIII, FIX, FXI or FVIII, FIX, FXI or FXII deficiencyFXII deficiency
• FII, fibrinogen, FV, X FII, fibrinogen, FV, X or a combined factor or a combined factor deficiencydeficiency
AcquiredAcquired
DisordersDisorders
• FVII InhibitorFVII Inhibitor• Vit K deficiencyVit K deficiency• Liver diseaseLiver disease• Warfarin useWarfarin use
• Inhibitor to FVIII, Inhibitor to FVIII, IX, XI, XII, vWF IX, XI, XII, vWF • Heparin useHeparin use
• Direct thrombin Direct thrombin inhibitor inhibitor • Inhibitor to FII, Inhibitor to FII, fibrinogen or FV or Xfibrinogen or FV or X• Liver disease, DIC, Liver disease, DIC, combined heparin and combined heparin and warfarin usewarfarin use

Edward P. Sloan, MD, MPH, FACEP
Laboratory Testing
• PT: Extrinsic, should be normal unless FVII deficiency or acquired
• aPTT: Intrinsic, elevated in moderate hemophilia disease severity

Edward P. Sloan, MD, MPH, FACEP
Other ED Testing
• Extremity xrays
• Head CT
• Abdominal CT
• Tests for increased compartment pressures
• Nuclear bleeding studies

Edward P. Sloan, MD, MPH, FACEP
Emergency Department Emergency Department ManagementManagement

Edward P. Sloan, MD, MPH, FACEP
Initial Management
• Treat the patient• ABCs• Direct hemorrhage control• Hemodynamic support• Crystalloids• Blood products • Specifically assist hemostasis

Edward P. Sloan, MD, MPH, FACEP
Primary hemostasis:Primary hemostasis:• Vasoconstriction Vasoconstriction • Platelet adhesion Platelet adhesion • Platelet aggregation and contraction Platelet aggregation and contraction
Secondary hemostasis:Secondary hemostasis:• Activation of coagulation factors Activation of coagulation factors • Formation of fibrinFormation of fibrin
Fibrinolysis:Fibrinolysis:• Activation of fibrinolysis Activation of fibrinolysis • Lysis of the plugLysis of the plug
The 3 Phases of Hemostasis The 3 Phases of Hemostasis

Edward P. Sloan, MD, MPH, FACEP
Blood Vessel & EndotheliumBlood Vessel & Endothelium• Hemostasis requires and Hemostasis requires and
involves various physiological involves various physiological components:components:
• The blood vessel wallThe blood vessel wall
• Endothelial cellsEndothelial cells• Subendothelial tissueSubendothelial tissue• Smooth muscle cellsSmooth muscle cells
• The components of bloodThe components of blood
• Platelets (thrombocytes)Platelets (thrombocytes)• Coagulation (clotting) Coagulation (clotting)
factorsfactors• Fibrinolytic/ anticoagulant Fibrinolytic/ anticoagulant
proteinsproteins

Edward P. Sloan, MD, MPH, FACEP
Primary Hemostasis: Primary Hemostasis: VasoconstrictionVasoconstriction
• The first response The first response to endothelial to endothelial injury is the injury is the constriction of the constriction of the damaged vessel damaged vessel which reduces the which reduces the blood flow blood flow at the site of at the site of injuryinjury

Edward P. Sloan, MD, MPH, FACEP
Primary Hemostasis: Primary Hemostasis: Formation of a Platelet PlugFormation of a Platelet Plug
• The exposure of The exposure of subendothelial subendothelial components such as components such as collagen promotes collagen promotes platelet adhesionplatelet adhesion
• The adherence of The adherence of platelets to the sub-platelets to the sub-endothelium leads to endothelium leads to platelet activation and platelet activation and the formation of platelet the formation of platelet aggregates (platelet aggregates (platelet plug)plug)

Edward P. Sloan, MD, MPH, FACEP
• At the site of vascular injury At the site of vascular injury binding of endogenous factor binding of endogenous factor VII/VIIa to tissue factor (TF) VII/VIIa to tissue factor (TF) leads to the generation of small leads to the generation of small amounts of thrombin amounts of thrombin
• Thrombin activates platelets Thrombin activates platelets and additional coagulation and additional coagulation factors which subsequently factors which subsequently generate large amounts of generate large amounts of thrombin thrombin
• This “thrombin burst” induces This “thrombin burst” induces the generationthe generationof a haemostatic plugof a haemostatic plugthat prevents furtherthat prevents furtherblood loss blood loss
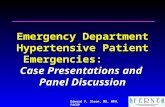
Secondary HemostasisSecondary Hemostasis
Adapted from Hoffman M et al., 2001.1

Edward P. Sloan, MD, MPH, FACEP
XIIXI
IXVIIIa
XVa
IIa (thrombin)
II (prothrombin)
fibrinogen FibrinClot
FibrinClot
TF
VIIVIIa/TF
X
HMWK,PK
(factor I)
PTPT
PTTPTT How a Blood Clot Forms: Step 2

Edward P. Sloan, MD, MPH, FACEP
What is Broken?
• Platelets
• Clotting factors
• Coagulation cascade

Edward P. Sloan, MD, MPH, FACEP
What Can Be Provided?
• Vitamin K
• FFP (Fresh frozen plasma)• PCC (prothrombin complex concentrate)
• Platelets, packed RBCs, whole blood
• Specific clotting factors
• Anti-fibrinolytics, anti-hemophilics

Edward P. Sloan, MD, MPH, FACEP
Hemophilia A: Factor VIII
• Recombinant factor VIII concentrate is the preferred source of factor VIII. The factor VIII activity level should be corrected to 100% of normal for potentially serious hemorrhage.
• Units factor VIII=(weight in kg)(50 mL plasma/kg)(1 U factor VIII/mL plasma)(desired factor VIII level minus the native factor VIII level)

Edward P. Sloan, MD, MPH, FACEP
Hemophilia A: Factor VIII
• As an example, an 80-kg individual diagnosed with hemophilia with known 1% factor VIII activity level presents to the ED with a severe upper GI bleed.
• Units factor VIII = (80 kg)(50 mL/kg)(1 U factor VIII/mL)(.99) = 3960

Edward P. Sloan, MD, MPH, FACEP
Hemophilia A: Factor VIII
• Next dose: 12 hours later, 1/2 initial dose.
• Minor hemorrhage: 1-3 doses factor VIII.
• Major hemorrhage: many doses, continued factor VIII activity monitoring.
• Goal: trough activity level at least 50%.

Edward P. Sloan, MD, MPH, FACEP
Hemophilia A: Other Rx
• FFP: administer 1 mL IV FFP/U factor VIII.
• Anti-fibrinolytics: • Epsilon aminocaproic acid (Amicar)
• Oral mucosal bleeds, rich fibrinolytic activity
• 200 mg/kg PO/IV initial dose, 100 mg/kg q6h; not to exceed 5 g
• Alternatively, 10 g slow IV (over 2 h), followed by 1 g/h continuous infusion

Edward P. Sloan, MD, MPH, FACEP
Hemophilia A: Other Rx
• Anti-hemophilic agent:• 1-deamino-8-D-arginine vasopressin 1-deamino-8-D-arginine vasopressin (desmopressin acetate, DDAVP)(desmopressin acetate, DDAVP)
• Increase (up to 4-fold) in FVIII plasma levelsIncrease (up to 4-fold) in FVIII plasma levels
• 0.3 mcg/kg in 30-50 mL 0.9% isotonic saline 0.3 mcg/kg in 30-50 mL 0.9% isotonic saline IV over 15-20 minIV over 15-20 min
• Not indicated in platelet type vWBNot indicated in platelet type vWB

Edward P. Sloan, MD, MPH, FACEP
Hemophilia B: Factor IX
• Synthetic recombinant Factor IX
• Units factor IX =(weight in kg)(100 mL/kg)(1 U factor IX/mL)(desired factor IX level minus the native factor IX level)

Edward P. Sloan, MD, MPH, FACEP
Hemophilia B: Factor IX
• As an example, an 80-kg individual diagnosed with hemophilia with known 1% factor IX activity level presents to the ED with a severe CNS bleed.
• Units factor IX = (80 kg)(100 mL/kg) (1 U factor IX/mL)(.99) = 7920

Edward P. Sloan, MD, MPH, FACEP
Hemophilia B: Factor IX
• Next dose: 12 hours later, 1/2 initial dose.
• Minor hemorrhage: 1-3 doses factor IX.
• Major hemorrhage: many doses, continued factor IX activity monitoring.
• Goal: trough activity level at least 50%.

Edward P. Sloan, MD, MPH, FACEP
Hemophilia B: Factor IX
• Factor IX complex concentrates
• Coagulation factor IX concentrates, pooled plasma product (high purity)

Edward P. Sloan, MD, MPH, FACEP
Hemophilia B: Other Rx
• FFP: administer 1 mL IV FFP/U factor IX.
• Anti-fibrinolytics: • Epsilon aminocaproic acid (Amicar)
• Oral mucosal bleeds, rich fibrinolytic activity
• 200 mg/kg PO/IV initial dose, 100 mg/kg q6h; not to exceed 5 g
• Alternatively, 10 g slow IV (over 2 h), followed by 1 g/h continuous infusion

Edward P. Sloan, MD, MPH, FACEP
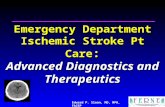
vWDx: Platelet ActivationvWDx: Platelet Activation
- GPIb IX, V : internalized- GPIIbIIIa : 1) membrane expression increased
2) complex occupied by fibrinogen, vonWillebrand Factor ...- P-selectin : translocated to the membrane
RESTING ACTIVATED
ACTIVATION
granules
P-selectin
GPIV
GPIIb-IIIa
GPIb/IX/V
P-selectinGPIIb-IIIa
GPIV GPIb/IX/V
Fibrinogen
50,000
25,000
> 500

Edward P. Sloan, MD, MPH, FACEP
von Willebrand’s Disease Rxvon Willebrand’s Disease Rx
• Anti-hemophilic agent:• Type 1 vWDx • 1-deamino-8-D-arginine vasopressin 1-deamino-8-D-arginine vasopressin (desmopressin acetate, DDAVP)(desmopressin acetate, DDAVP)• Up to 3-6 fold increase in FVIII and 2-4 fold Up to 3-6 fold increase in FVIII and 2-4 fold
increase in vWF plasma levelsincrease in vWF plasma levels• 300 mcg intranasally produces levels 300 mcg intranasally produces levels comparable to IV infusioncomparable to IV infusion • Useful for menorrhagia and epistaxisUseful for menorrhagia and epistaxis

Edward P. Sloan, MD, MPH, FACEP
von Willebrand’s Disease Rxvon Willebrand’s Disease Rx
• Platelet transfusions if other Rx not effective
• Cryoprecipitate, FFP contain functional vWF, not used widely, not used widely

Edward P. Sloan, MD, MPH, FACEP
Rare Bleeding DisordersRare Bleeding Disorders• Congenital factor deficiency of any of the following:
• VII• XI• X• II• V• Combined V and VIII• Fibrinogen• XIII• PAI-1
•Congenital Platelet Disorders•Glanzmann’s Thrombasthenia•Bernard Soulier
•von Willibrands Disease – Types 2 & 3

Edward P. Sloan, MD, MPH, FACEP
Rare Bleeding Disorders: RxRare Bleeding Disorders: Rx
• Stabilize the patient. • Call the hematology/oncology consultant.

Edward P. Sloan, MD, MPH, FACEP
What Can Be Provided?
• Specific clotting factors
• PCC, other concentrates
• Anti-fibrinolytics, anti-hemophilics
• FFP (1 mL per Unit of clotting factor)
• Platelets

Edward P. Sloan, MD, MPH, FACEP
Patient Outcome
• Low Hb, ruptured spleen • IVF, cross-matched blood• 10% Factor VIII levels prior• Units factor VIII = (70 kg)(50 mL/kg)
(1 U factor VIII/mL)(.90) = 3500• Stable to ICU with expectant management

Edward P. Sloan, MD, MPH, FACEP
ConclusionsConclusions
• Complex medical problems
• Lumpers and splitters
• Treat the patient’s hemorrhage
• Identify the disease
• Treat the disease, as able
• Consult liberally
• Admit as indicated

Edward P. Sloan, MD, MPH, FACEP
Questions?Questions?
[email protected] 413 7490
sloan_ema_2007_hemophilia_rbd_092307_final04/10/23 22:55