Education - POCUS Journalpocusjournal.com/wp-content/uploads/2017/12/POCUSJ-vol-01-iss-0… · June...
4
FEB 2016 vol. 01 iss. 01 Education Practice Research Editorial Board Emergency Department/ FAST Dr. Joseph Newbigging, MD Dr. Louise Rang, MD Critical Care Dr. Suzanne Bridge, MD Anesthesiology Dr. Rob Tanzola, MD Dr. Rene Allard, MD Internal Medicine Dr. Barry Chan, MD Cardiology Dr. Amer Johri, MD Julia Herr, MSc Inside Welcome to POCUS J Case Files: Use of POCUS for assessment of dyspnea in the Emergency Department Cardiac amyloidosis using on routine hand held ultrasound Shocking out with severe hypoxia ISSN: 23698543
Transcript of Education - POCUS Journalpocusjournal.com/wp-content/uploads/2017/12/POCUSJ-vol-01-iss-0… · June...

FEB 2016 vol. 01 iss. 01
Education PracticeResearch
Editorial Board
Emergency Department/FASTDr. Joseph Newbigging, MDDr. Louise Rang, MD
Critical CareDr. Suzanne Bridge, MD
AnesthesiologyDr. Rob Tanzola, MDDr. Rene Allard, MD
Internal MedicineDr. Barry Chan, MD
CardiologyDr. Amer Johri, MDJulia Herr, MSc
Inside
Welcome to POCUS J
Case Files:
Use of POCUS for assessment of dyspnea in the Emergency Department
Cardiac amyloidosis using on routine handheld ultrasound
Shocking out with severe hypoxia
ISSN: 23698543

2 | POCUS J | FEB 2016 vol. 01 iss. 01
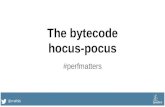
Figure 1. POCUS of right ventricle (subcostal view).
A 65 yearold man presented to the Emergency Department at
Kingston General Hospital with progressive shortness of breath, fatigue, dull chest discomfort that worsened with deep breathing and exertion. The patient was referred to cardiology for congestive heart failure and ordered troponin, chest xray (CXR), and electrocardiogram (ECG). The patient had a previous history of nonST elevation myocardial infarction, stable, mild chronic obstructive pulmonary disease (COPD), and low normal estimated glomerular filtration rate. A physical examination determined that the patient was hemodynamically stable, revealed an oxygen saturation of 89% on room air, and auscultation showed normal heart sounds with no S3 heard. The patient’s jugular venous pressure was difficult to visualize, the chest was
clear, and there was mild lower leg edema. CXR and ECG results returned normal, and troponin was 0.09. The Differential included: acute coronary syndrome (ACS, ischemia), pulmonary embolism (PE), pneumonia/COPD exacerbation.
A transthoracic echo (TTE) was ordered for the morning following admission, and a bedside echocardiogram was conducted with a handheld ultrasound unit (VScan, GE), revealing a dilated hypokinetic right ventricle and grossly normal left ventricular systolic function. The pointofcare cardiac ultrasound (POCUS) led to a new Differential: PE and ACS/right ventricular infarct.
Following the POCUS and confirmatory limited TTE, the patient was sent for an urgent computed tomography (CTPA) to confirm pulmonary embolism, and was admitted to the internal medicine unit. An Urgent full TTE was ordered that evening to document RV dysfunction Respirology was consulted to consider the need for thrombolytics.
Conclusion: In this case the applica
Case FileUse of POCUS for assessment of dyspnea in the Emergency Department
by Jennifer Meloche, MDQueen's University, Cardiology
Visit the online article to view additional content from this case: pocusjournal.com/article/20160101p2b
tion of POCUS significantly altered the initial differential and led to rapid diagnosis of a pulmonary embolism and appropriate management.
Welcome to the first issue of the world’s first journal dedic
ated solely to pointofcare ultrasound. The Pointofcare Ultrasound Journal (POCUS J) is unique in its dedication to showcasing studies performed by any specialty whether it’s the Emergency Department, Critical Care, Anesthesiology, Cardiology, Primary Care or Allied Health. We envision working with and highlighting existing resources whether they are studies published in traditional imaging journals, learning websites, blogs, or social media education tools. In this platform, we offer an opportunity for cases and studies to be peer evaluated
Welcome to POCUS Jby expert educators dedicated to understanding the advantages and limitations of POCUS. The POCUS J will be offered in digital format on a quarterly basis. We are interested in not only publishing cases that demonstrate the value of POCUS to the physical exam and the diagnostic process but also highlight the limitations. This technology has disrupted our traditional approach to patient assessment, but important questions remain: What is the best way to teach POCUS? How do we maintain quality? What are the indications? We hope to explore such questions in each issue of this journal and welcome you to join the adventure!
Dr. Johri is an Associate Professor at Queen’s University, Harvard
trained imaging scientist, and holds a Heart and Stroke Foundation Clinical Scientist Career award. He has published on methods of
teaching POCUS, and the limitations of this technology in the cardiology realm. He can be followed on twitter @amerjohri and has a blog at www.VascNet.com.
by Amer M. Johri, MD Queen's University, Department of Medicine
Read online: pocusjournal.com/article/20160101p2a

FEB 2016 vol. 01 iss. 01 | POCUS J | 3
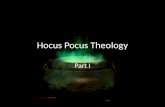
Figure 1. Parasternal long axis view. Severe thickening of the left ventricular walls, as well as thickening of both the mitral and the aortic valves.
Figure 1. Parasternal short axis view.
Case FileCardiac amyloidosis using on routine handheld ultrasound
A 64 yearold man presented to the Kingston General Hospital
with cardiac arrest. At the time of EMS arrival, the ECG showed ventricular tachycardia. The patient was intubated and ventilated. Multiple defibrillations were required to convert the patient back to normal sinus rhythm. At the bedside, a physical examination revealed a blood pressure of 82/46, a heart rate of 110 beats per minute which was regular, and oxygen saturations of 99%. The patient’s JVP was elevated at 7 cm above the sternal angle. Heart tones were normal, but a systolic murmur which was holosystolic and radiated to the apex
was appreciated. Lung fields were clear.
A bedside echocardiogram (VScan, GE) showed evidence of severe left ventricular and right ventricular thickening. Both atria were severely dilated. The mitral, tricuspid, and aortic valves appeared thickened. Myocardial speckling was not appreciated. Both the left and right ventricular function appeared to be moderately impaired.
During the hospital admission, the patient was treated with supportive care and was extubated. A fat pad biopsy was completed which made a definitive diagnosis of amyloidosis and the hematology service was consulted. However, the patient experienced an asystolic cardiac arrest, failed resuscitation, and died in hospital.
by Jeffrey Wilkinson, MDQueen's University, Department of Medicine
Visit the online article to view additional content from this case: pocusjournal.com/article/20160101p3a
Case FileShocking out with severe hypoxia
Clinical Vignette: 36 year old presented in acute respiratory
distress, hypotension (BP 70/40 with HR 120), and severe hypoxia (SpO2 80s with partial rebreather). Thoracic auscultation was normal though the heart sounds were masked by her breath sounds. The jugular venous pulse (JVP) was grossly distended with no leg edema.
PoCUS Indication: Clinically, the high JVP and clear lungs suggested an obstructive mechanism for which both pulmonary embolism (PE) and pericardial tamponade could yield such findings.
Image Acquisition: Basic Focused Assessed Transthroacic ECHO (FATE) was performed (See Figures, and online supplemental videos).
Image Interpretation: Pericardial effusion was absent yet the right ventricle (RV) was dilated acutely as the RV wall thickness was normal (subcostal). The systolic Dseptum (parasternal) suggested an elevated RV afterload. Along with the hyperdynamic left ventricle (LV) and normal left atrium (LA), there was likely a flow obstruction between the RV to LA which maybe related to the “lesion” in the RV.
Clinical Synthesis: Given clinical features and PoCUS findings, the most likely etiology was PE.
Vignette Resolution: Standard echocardiogram revealed a large ovoid mass attached to the RV septum with systolic dynamic right ventricular outflow tract obstruction, and CTPA revealed bilateral PE. Thrombolysis improved oxygenation though the mass persisted requiring surgical excision. Pathology verified that it was a thrombus.
by Barry Chan, MDQueen's University, Internal Medicine
Visit the online article to view aditional content and extended analysis of this case: pocusjournal.com/article/20160101p3b

4 | POCUS J | FEB 2016 vol. 01 iss. 01
About Us
Winfocus Mexico 2016May 1114, 2016 – Cozumel, Mexico
27th Annual Scientific Sessions, American Society of Echocardiographywww.asescientificsessions.orgJune 1014, 2016 – Seattle, WA, USA
12th Winfocus World Congress on Ultrasound in Emergency & Critical Care www.winfocus.orgSeptember 710, 2016 – Ljubljana, Slovenia
Announcements
POCUS Journal is dedicated to the advancement of research and the promotion of education in the field of vascular medicine.
POCUS journal is a publication of VascNet, and can be found online at pocusjournal.com
As a publication of VascNet, you can receive email updates when a new issues is available by subscribing to the VascNet email newsletter.
Visit: pocusjournal.com/subscribe/ POCUS Journal is a publication of VascNet
VascNet is a research network researchers, clinicians, and experts in the field of cardiovascular medicine.
Visit us at vascnet.com to learn more.
VascNet94 Stuart St., Kingston, ON Canada, K7L 3N6
ISSN: 23698543
Fourth Annual World Congress Ultrasound in Medical Educationwww.wcume.orgSeptember 2325, 2016 – Lubbock, TX, USA
EuroEchoImaging 2016, European Society of Cardiologywww.escardio.org/ESC2016December 710, 2016 – Leipzig, Germany
The online version of the FEB 2016 issue of POCUS Journal is available at pocusjournal.com/issue/vol01iss012016 and includes additional media and images from the case studies.