
Educating children and young people with FASD · Educating children and young people with FASD ......
72
Educating children and young people with FASD Dr Carolyn Blackburn, Birmingham City University, [email protected]
Transcript of Educating children and young people with FASD · Educating children and young people with FASD ......

Educating children and young people with FASD
Dr Carolyn Blackburn, Birmingham City University, [email protected]

Overview of session
• FASD and developmental risk
• Implications for learning and engagement in learning
• Overlaps with attachment and relational issues
• What do educators need to know?
• Overview of possible pedagogical approaches
Carolyn Blackburn 2016

Part 1
• Why is alcohol a problem in pregnancy?
Carolyn Blackburn 2016
Teratogens • Drugs (prescribed –
inhalents, peniciliin, diet pills vitamin A)
• Illegal drugs (cocaine, heroin)
• Alcohol
• Lead, mercury, solvents and other environmental pollutants
• Maternal diseases (cancer, toxoplasmosis, chicken pox, TB)
• Herbal medications?
• Maternal stress
Carolyn Blackburn 2016

Carolyn Blackburn 2016
Of all the substances of abuse…alcohol produces by far the most serious neurobehavioral effects in the foetus. • US Institute of Medicine (2006)

For the mother…
• Lack of concentration, memory and attention;
• Mental health problems such as anxiety and depression;
• Risk of schizophrenia;
• Damage to liver and other health problems;
• Overall weathering effect related to SES, nutrition, living conditions
Carolyn Blackburn 2016

For the child …
• Miscarriage
• Stillbirth
• Intrauterine growth restriction
• Pre-term birth
• Low birth weight
• Small for gestational age at birth
• Small for age in childhood
• Birth defects
• Microcephaly and small head circumference
• NAS
• FASD
• Neurodevelopmental outcomes
Carolyn Blackburn 2016
Central nervous system damage
Alcohol can cause foetal cell death, and disrupt the way cells specialise, grow and migrate to create different parts of the developing baby, most significantly the neurons in the brain. Furthermore, alcohol can reduce the flow of blood to the foetal brain which means that at birth infants may suffer from low blood oxygen levels (Lebel et al., 2011; Vaux, 2010; Weinberg, 2009).
Carolyn Blackburn 2016

Carolyn Blackburn 2016
• Fetal Alcohol Spectrum Disorders (FASD) is an educational term which recognises the range of effects resulting from prenatal exposure to alcohol. These include physical and intellectual delays and differences leading to the diagnosis of a range of co-existing conditions.
• Alcohol is a teratogen (a substance which interferes with the normal development of the embryo or foetus) that readily crosses the placenta.
• In the absence of a developed blood filtration system, the foetus is totally unprotected from alcohol circulating in the blood system.
What is FASD?

1 in 100?
• ‘...we estimate that the current prevalence of FASD in populations of younger school children may be as high as 2-5% in the US and some Western European countries.’ May, P.A., Gossage, P.J. et al. (2009) Dev. Disabil. Res. Rev. 15:176-192
Carolyn Blackburn 2016

Women’s drinking habits
Carolyn Blackburn 2016
In 2001 a survey of women in Britain revealed that 8% of women aged 18-24 years had consumed at least 35 units of alcohol in the past week (Plant and Plant 2001, Plant et al. 2002).
This is defined as ‘harmful drinking’ by the Department of Health and the Home Office (2007). High levels of heavy drinking by young women have been noted by other investigators (Office for National Statistics 2004, 2006, Williamson et al. 2003, Scottish
Government 2007, 2008)
The scale of the problem
Carolyn Blackburn 2016
Evidence from a number of sources suggests that women will continue to drink at pre-pregnancy levels until the pregnancy is confirmed.
This is particularly true if the pregnancy was unplanned (Tough et al. 2006). It has been noted that approximately 84% of UK mothers under the age of 20 years report their pregnancies were unplanned (Dex and Joshi 2005, Hanson, Joshi and Dex 2010).
Therefore, at the most vulnerable time for the foetus, the mother may still be drinking at pre-pregnancy level.

Why does binge drinking matter?
Carolyn Blackburn 2016
This pattern of heavy episodic drinking is pertinent as what is now being called now called binge drinking is recognised as the most risky for the unborn child.
(Plant, 2013 in press) in Carpenter, Blackburn and Egerton, FASD and Interdisciplinary Perspectives. London: Routledge

Carolyn Blackburn 2016
Front loading

Carolyn Blackburn 2016

Carolyn Blackburn 2016
Glass letter Volume Alcohol content
(%)
No of units in glass Number of glasses
needed to have a
binge (6 units in
one sitting)
A 125 9 1.1 5.5
B 125 13 1.6 4
C 250 9 2.3 2.5
D 250 13 3.25 1.8

Part 2 • What are the implications for
learning and development?
• What do educators need to know?
Carolyn Blackburn 2016

Carolyn Blackburn 2016
Educational or Diagnostic Term Factors Required for Confirmation/Diagnosis
Fetal Alcohol Syndrome (FAS) Confirmed exposure to maternal alcohol;
Facial dysmorphology;
Growth retardation; and
Central nervous system dysfunction.
Partial FAS (pFAS) Confirmed exposure to maternal alcohol;
Facial dysmorphology; and either
Growth retardation or central nervous system dysfunction.
Alcohol-related Neurodevelopmental Disorder (ARND)
Confirmed exposure to maternal alcohol; and
Central nervous system dysfunction
Alcohol-Related Birth Defects (ARBD) Presence of congenital anomalies e.g. cardiac, skeletal, renal ocular, auditory – known to be associated with prenatal alcohol exposure.

Carolyn Blackburn 2016

Carolyn Blackburn 2016
Neurons are destroyed, deformed and/or displaced
Brain structures are weakened
Brain messages are disrupted Brain activity is no longer adaptive and predictable Brain cannot function properly
Carolyn Blackburn 2016
Characteristics of children with FASD
• 35% are born pre term
• 65% are born with low birth weight
• Only 7% diagnosed at birth, the
average age of diagnosis is 3.3 years
• 53% have microcephaly
• 24% have significant birth defects
• 85% have behavioural problems
• 40% lived with birth parent (which
means that 60% do not)
• 51% have a sibling with FASD
(which means that one child with
FASD in the family should trigger
more support for the family in future
pregnancies). Elliott, E. (2013) Australian Perspectives on FASD. In Carpenter,
Blackburn and Egerton (2013) Interdisciplinary Approaches to FASD.
London: Routledge.

Carolyn Blackburn 2016
The “Social” Synapses

For some children, maternal alcohol consumption represents a risk which is additional to pre-existing biological genetic and/or psychosocial influences, such as psychological trauma, impoverished environment or socio-economic status, rendering them vulnerable to a ‘toxic trio of risk factors.
Blackburn, 2013 , Walking through a moonless night:
FASD and Early Childhood Intervention in Carpenter, Blackburn and Egerton 2013 FASD: Interdisciplinary Perspectives
Carolyn Blackburn 2016
When I was pregnant I couldn’t get up
in the morning without throwing up and
having a drink and I knew that I
shouldn’t, but I couldn’t function
without a it. I did put the drink down
when he was about 6 months, and the
maruianja when he was about year ..
then I had a wake up call. I had to
decide which one am I going to choose
- my son or the drugs ?
Mentally I was unfit, I had suicidal
thoughts, I had thoughts about
harming my son, was seeing things, I
was a mess. Having a baby and trying
to deal with my head was difficult.

Carolyn Blackburn 2016
“We just need help to deal with the guilt … and to gel together as a family”

AHHD/FASD/AUTISM
Carolyn Blackburn 2016
Inattention
Hyperactivity
Impulsivity
Language deficits
Poor social understanding
Poor imagination
Poor planning
Tics
Cognitive flexibility problems
Obsessionality
Working memory deficits

Early Childhood
Carolyn Blackburn 2016
Some or all of the following may apply to preschoolers with FASD:
• feeding and sleep problems
• poor motor coordination, and poor fine and gross motor
• control
• flitting from one activity/area to another, exhibiting butterfly-like movements
• more interest in people than objects
• difficulty with social skills
• overly friendly and indiscriminate with relationships, may
• seek out affection
• expressive language may be delayed or children may be
• overly talkative (but lack richness of speech, thought or
• grammar complexity)
• receptive language often delayed; even if children are talkative, they may not understand much of what is said to them
• inability to understand danger, often fearless
• low tolerance for frustration and prone to temper tantrums
• difficulty following directions or doing as told
• short attention span
• easily distracted or hyperactive
• difficulty with changes and transitions, prefer routines
• difficulty integrating sensory information, such as sound,
• touch, light, smells, movement, etc.)
For example
Carolyn Blackburn 2016
Shauna, age 6 – ‘a bit young for her age; not catching up’Eager and happy, expressive and talkative
• Highly distractible - diverted by even the smallest distraction
• Does not seem able to follow directions. • Things Shauna knows one day seem to be gone from her memory the next. • After 6 weeks, Shauna still has not grasped classroom routines • The teacher has not been successful in helping her catch up.
• Still uses an immature grasp to write • Shauna is making progress in reading • Her math and writing skills are at preschool or kindergarten level
• She has made only one friend because of her immature behavior • She has had several temper tantrums, often when the schedule for the day has
changed unexpectedly. (Department of Health and Human Services, 2007)
In Later Childhood
• Developmental delays – across all domains
• Behaviour (inattention, hyperactivity, impulsivity
distractibility, aggression – sensory seeking)
• Social and emotional vulnerability
• Relationships – peers and
adults
• Medical/health issues
Carolyn Blackburn 2016

Carolyn Blackburn 2016
Difficulties that disrupt learning
• Developmental level of functioning
• Sensory systems
• Language and communication
• Processing pace: How fast the brain works
• Learning and memory
• Abstract thinking
• Executive functioning
Diane Malbin (2012)
‘Neurobehavioral approach to developing effective interventions’ FASDLive September 12-14 Saskatoon, SK A –

Carolyn Blackburn 2016
© FASD Trust / Jodee Kulp, www.betterendings.org

• Resistance to change and opposition
• Extremes of cognitive inflexibility lead to a significant inability to cope with change;
• Learnt patterns of behaviour to avoid these;
• Not seen all the time but mainly times of high arousal;
• Psychological overlay can be significant leading to severely disruptive behaviour;
• High rates of oppositional defiant disorder.
Carolyn Blackburn 2016

Carolyn Blackburn 2016
‘I struggled to make and keep friends. I was the class clown. All I wanted was for the other kids in the class to like me. My mum said the cleverer kids in the class used to use me and set me up. Resulting in me always being in trouble in primary school... I am always pushing the boundaries and do not learn from my mistakes.’
Matthew, FASAware

• Co-morbid diagnosis:
FASD plus …. Reactive Attachment Disorder (RAD), Sensory Integration Disorder (SID), Autistic Spectrum Disorder (ASD), Attention Hyperactivity Disorder (ADHD), Oppositional Defiant Disorder (ODD), Anxiety Disorder, vision and hearing impairments (all in one student)
• Multiple family placements (9 by the age of 5)
• Loneliness of being the only child in a school with FASD
• Lack of knowledge, training and understanding
Compounded by:
Carolyn Blackburn 2016

Carolyn Blackburn 2016
• Aloof
• Over Excited
• Easily Distracted
• Anxious
• Fearful
• Obsessional
• Impulsive
• Noisy
• Boisterous
• Overactive
• High levels of disability in all settings

0 2 4 6 8 10 12
Receptive Language
Expressive Language
Written Language
Personal Living Skills
Domestic Living Skills
Community Living Skills
Interpersonal Skills
Play and Leisure
Coping Skills
Functional Age
Functional Age
Chronological Age: 13
Carolyn Blackburn 2016
Carolyn Blackburn 2016
• ‘Whilst she reads as a 14 year old, I will teach her as a 14 year old.’ (Headteacher)

Carolyn Blackburn 2016
‘Most of her difficulties stem from her impulsive
behaviours. She finds it very difficult to regulate her behaviours, especially in an environment where there is a lot of stimulation going on. A lot of noise, a lot of people around or tactile objects that might be fun to touch or to look at – that can really affect her focus.’
Jade’s teacher Http://www.nofas-uk.org/ http://www.youtube.com/watch?v=lgY9jSUkOhc 1:04-2:20

“I like science but there’s a lot of information
to process … sometimes I’ll just sit and look out of the window or doodle… sometimes I have to leave the room … it would be good to have a TA to write things down, then I can just listen.”
FAS-eD Project, 2010 www.nofas-uk.org
Carolyn Blackburn 2016

Complex Health Needs:
• Visual and hearing impairments
• Heart problems
(a leak on one of the valves)
• Feeding problems, food choices
• Skeletal problem
(bones are not formed properly)
• Mobility difficulties which impact ability to walk distances and
run/small stature
• Doubly incontinent
Carolyn Blackburn 2016

Challenges – medical/health issues
“His successes are … learning to read, learning
to write, learning to talk and his ability to mimick and understand, everything really that we didn’t think he would be able to do when we first adopted him. We were told he would never do anything. But he’s just excelled in everything. I think he has some problems, but everything he does is magic really and an achievement in itself.”
FAS-eD Project, 2010 www.nofas-uk.org
Carolyn Blackburn 2016
“I’ve always wanted somebody to come along and say I’m going to look this child with FAS as a child with severe medical problems. We’ve had so many medical professionals involved …. not many of them have known enough about FAS to say this is standard procedure with a child with this condition.”
FAS-eD Project, www.nofas-uk.org
Carolyn Blackburn 2016

“I’m going
to be a
superhero” Carolyn Blackburn 2016

Challenges - fantasy and reality
“That’s where children like x fall down, he seems like he’s doing well and he’s got it sussed, he sounds like a capable student, but he can’t separate fact from fantasy. He’s 11 and he lives in a world of Disney and make believe, he really believes he can be a Superhero and his understanding of fantasy is comparable with that of a 4 year old.”
FAS-eD project, 2010 www.nofas-uk.org
Carolyn Blackburn 2016
Carolyn Blackburn 2016
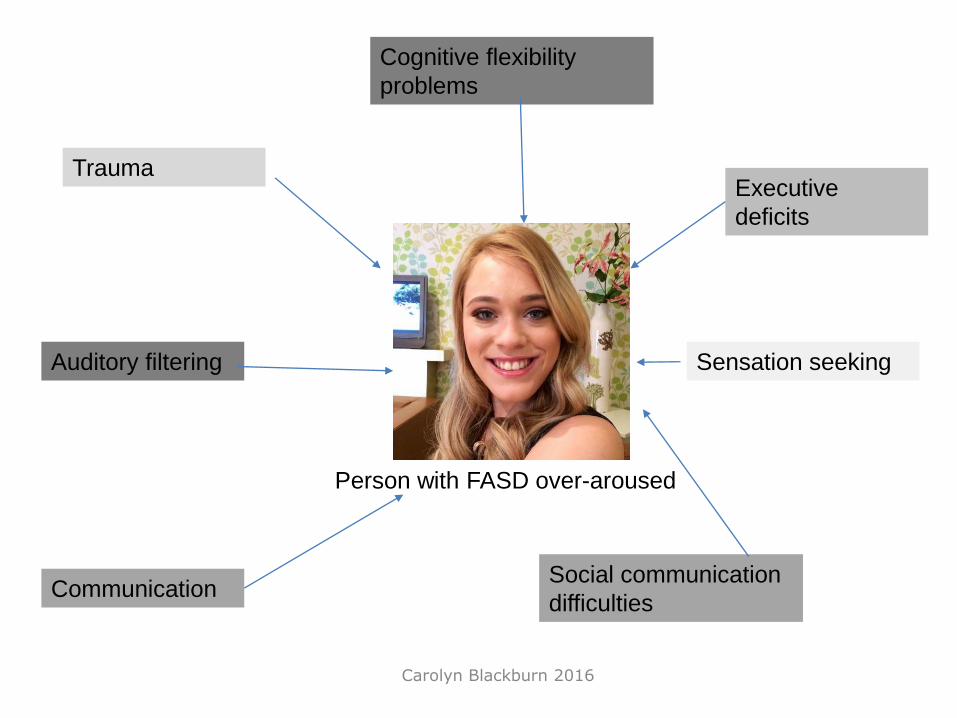
Person with FASD over-aroused
Trauma
Social communication
difficulties
Cognitive flexibility
problems
Sensation seeking
Communication
Executive
deficits
Auditory filtering

Carolyn Blackburn 2016
• Secondary behavioral symptoms • Easily tired, fatigued • Anxious • Lonely, isolated • Shut down; flat affect • Fearful, withdrawn • Depressed • Frustrated, short fuse, angry
FASDLive 2012 September 12-14 Saskatoon, SK A Neurobehavioral Approach to Developing
Effective Interventions – Diane V Malbin
Emotional wellbeing, mental health and resilience

Part 3
• Possible pedagogical interventions
Carolyn Blackburn 2016

School leaders
Carolyn Blackburn 2016
‘Headteachers need the type of information that gives them a sound, solid appreciation of how fetal alcohol spectrum disorder is going to impact on the effectiveness of the child as a learner.’ http://www.youtube.com/watch?v=v1jphhbS9rg (2.02-2.29)

Assessment first?
• SDQ – measures emotional, hyperactivity, conduct, peer relationships and pro-social behaviour;
• Sensory profile – some conduct/hyperactivity is actually sensory seeking behaviour – needs to be assessed;
• Engagement in learning.
Carolyn Blackburn 2016

Educational Intervention
Carolyn Blackburn 2016
• Special or mainstream education?
• Which area of learning/development is the main problem?
• Which professionals need to be involved?

Interventions based on:
• Environment rather than within child characteristics
• Routine
• Structure
• Communication
• Observation/triggers
• Short tasks - exercise
• Don’t try harder, try differently!
Carolyn Blackburn 2016

Carolyn Blackburn 2016
• Reframing our understanding
• Redefining behaviours as symptoms
• Achieving change through accommodations
• Standard interventions don’t work!
Diane Malbin (2012)
‘Neurobehavioral approach to developing effective interventions’ FASDLive September 12-14 Saskatoon, SK A –
We need appropriate responses…

Shifting paradigms
Carolyn Blackburn 2016
Alberta Learning (2004) Teaching Students with Fetal Alcohol Spectrum Disorder: Building Strengths, Creating Hope. Edmonton: Alberta Learning. https://education.alberta.ca/media/377037/fasd.pdf

How I learn best...
Carolyn Blackburn 2016
Some people find it impossible to believe my problems…
Following verbal instructions sometimes confuses me. When I’m asked to do something like take out the garbage, I won’t understand or the words get all mixed up in my mind. For example, my stepfather gives me a command to do
something, and it’s like I don’t hear him clearly, even if he is in the same room. It’s like I block out words and phrases.
Visual contact is a very important way of learning for me. When a teacher shows a topic, I can understand it. I am not able to focus on reality if disaster strikes. I am acting on excitement.
http://fasdcenter.samhsa.gov/documents/reach_to_teach_final_011107.pdf
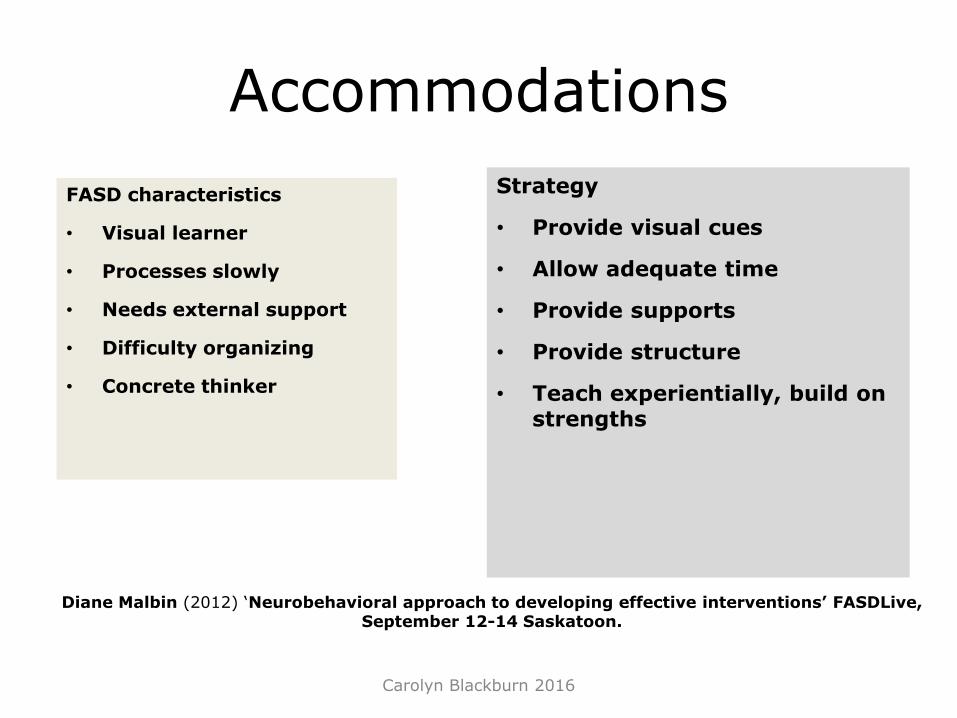
Accommodations
Carolyn Blackburn 2016
FASD characteristics
• Visual learner
• Processes slowly
• Needs external support
• Difficulty organizing
• Concrete thinker
Strategy
• Provide visual cues
• Allow adequate time
• Provide supports
• Provide structure
• Teach experientially, build on strengths
Diane Malbin (2012) ‘Neurobehavioral approach to developing effective interventions’ FASDLive, September 12-14 Saskatoon.

Carolyn Blackburn 2016
FASD characteristics
• One thing at a time
• Memory problems
• Impulsive
• Easily overstimulated
• Difficulty predicting
• Difficulty problem solving
Strategy
• Provide step-by-step cues and guidance
• Provide visual support; Repeat, repeat
• Structure and rehearse
• Provide calming opportunities
• Provide visual cues, role
play situation, Social Stories, etc.
Accommodations

Students like me
• https://www.youtube.com/watch?v=_t5TuEDeKCs
Carolyn Blackburn 2016

Carolyn Blackburn 2016
Maths
Carolyn Blackburn 2016
http://www.youtube.com/watch?v=H5O0O
EPKfxE 1:25-3:05

Transitions
Carolyn Blackburn 2016
• Bridging tasks (e.g. collecting resources)
• Hour glass as visual countdown
• Songs signalling end of the activity
• Transition buddy

Build on strengths
Carolyn Blackburn 2016
• Often gregarious, fun loving, caring and affectionate.
• Can be sensitive, loyal, kind and trusting in relationships
• Can succeed in structured situations.
• Often enjoy repetitive work
• Strong sense of fairness
• Strong visual memories,
• Good verbal fluency
• Positive use of visual language techniques. They can often
• Learn effectively using a hands-on approach.
• A rich imagination which enhances storytelling
• Creativity in visual arts and music
• Athletic skills in individual sports.
• High energy level
Alberta Learning (2004) Teaching Students with Fetal Alcohol Spectrum Disorder: Building Strengths, Creating Hope. Edmonton: Alberta Learning. https://education.alberta.ca/media/377037/fasd.pdf

Carolyn Blackburn 2016
• Anxiety – Routines – Schedules
• Memory issues – Provide one direction or rule at a time – Review rules regularly. – Use a lot of repetition, repetition, repetition and if I forget
repetition, repetition, repetition!
• Over stimulation – Simplify my environment – Provide one-to-one physical presence. – Know what situations over stimulate me
• Sensory differences
– Learn my sensory triggers and help me learn to avoid them – I may not like to be tickled or touched – Provide "chill down zones" for comfort and safety
Advice from Liz Kulp, a young woman with FASD
http://www.braidedcord.net/ideas-family.html

Social support
Carolyn Blackburn 2016
• Role play
• Social stories
• Friendship circles
• Friendship with older children of the same sex
• Friendship with the little girl next door needs to be along on adult appropriate lines
• Appropriate social distance, friendships,
Mental health
Carolyn Blackburn 2016
• At all times in their life, up to 90% of people with FASD are likely to have mental health problems, including when they are children. They need loving support to gain a healthy and positive self-image, and to accept their unique differences.

Carolyn Blackburn 2016
• Secondary behavioral symptoms • Easily tired, fatigued • Anxious • Lonely, isolated • Shut down; flat affect • Fearful, withdrawn • Depressed • Frustrated, short fuse, angry
FASDLive 2012 September 12-14 Saskatoon, SK A Neurobehavioral Approach to Developing
Effective Interventions – Diane V Malbin
Carolyn Blackburn 2016
• Tertiary symptoms Are the net
result of a chronic poor fit, failure, isolation and alienation:
• Trouble in school • Social services involvement • Involvement with justice • Homelessness • Addictions/ mental health issues,
suicide
FASDLive 2012 September 12-14 Saskatoon, SK A Neurobehavioral Approach to Developing
Effective Interventions – Diane V Malbin
Protective factors
Carolyn Blackburn 2016
• A stable and caring home - the greatest protective factor to outcome is supported
• Early identification and a good stable environment can improve the odds of avoiding adverse life events by 2- to 4- fold.8 K

Why diagnose?
Carolyn Blackburn 2016
• Interventions are counter-intuitive
• Mental health
– Child in control
– Something they know more about than peers
– Something people want to know/hear about
• Families can change their behaviour
• Educators and families can plan ahead
• No services specific to FASD
• Lack of professional confidence around diagnosis
• Lack of professional awareness
• Political will
• Not recognised
• In denial
• Stigmatising families
Why people don’t diagnose?

Families
Carolyn Blackburn 2016
We both now care full time for our three children. Working would not be an option: every day we have a meeting or medical appointment for the children.
Sleep deprivation is the hardest to overcome ...
Eva went for respite after her carers were trained for four months and it broke down after one night... there are not enough carers who could cope with our children
http://www.bemyparent.org.uk/features/hurdles-and-happiness,294,AR.html

Classroom Management Strategies
Carolyn Blackburn 2016
• Keep teaching and instruction simple and specific.
• Employ adaptive teaching techniques which focus upon the child’s interests, strengths and developmental stage.
• Use consistent and predictable language to support understanding.
• Use visual cues and aids to accompany verbal instructions. (e.g. visual timetables).
• Provide concrete learning resources and opportunities to support learning.
• Use pre-learning, rehearsing and practising of desirable skills and behaviours.
• Engineer repetition.
• Note strategies used by the student and build on these and/or teach more effective alternatives.
• Give instructions and tasks in small steps to support understanding and executive function and provide opportunities for oral or alternative methods of testing progress and competence.
• Give warning and instructions well ahead of transitions, and give support.
• Provide a structured learning environment (e.g. classroom spaces, time, work, etc.).
• Have consistent and predictable routines (e.g. providing visual schedules of activities) .
• Make cause and effect explicit (e.g. outcomes of decisions).
• Identify triggers for increased hyperactivity and inattention such as noise and smells and reduce them;
• Reward effort rather than achievement and allow extra time for tasks and tests.
• Provide consistent language and behaviour management strategies between home and school.
Resources
Carolyn Blackburn 2016

Organisations • NOFAS-UK (National Organisation on Fetal Alcohol Syndrome) www.nofas-uk.org NOFAS-UK promotes public
awareness about the risks of alcohol consumption during pregnancy with the goal to reduce the number of babies being born with FASD. It further acts as a source of information to the general public, press and to medical professionals.
• NOFAS-USA (National Organisation on Fetal Alcohol Syndrome) www.nofas.org NOFAS seeks to create a global community free of alcohol-exposed pregnancies and a society supportive of individuals already living with FASD.
• NOFAS Circle of Hope www.nofas.org/circleofhope/ The NOFAS Circle of Hope peer-mentoring program works to reduce the stigma birth mothers face by connecting them with other women who have the same experience.
• FASD Trust www.fasdtrust.co.uk The FASD Trust provides support for those affected by FASD and training / information for the professionals seeking to support them. It runs support groups for those affected by FASD across the UK, hosts various professional forums and has a variety of training and other resources for those affected by or interested in FASD.
• FASD Scotland www.fasdscotland.com/ FASD Scotland offers information, support and advice on FASD.
• FASD clinic, Surrey and Borders NHS Foundation Trust www.fasdclinic.com/resources this clinic has developed a resource page for families and professionals including a series of video blogs explaining aspects of FASD.
• EU FASD Alliance www.eufasd.org/ The European FASD Alliance was founded in 2011 to meet the need for European professionals and NGOs concerned with FASD to share ideas and work together.
• FASD Network UK www.fasdnetwork.org/ FASD Network UK is a social enterprise providing support to caregivers of children and adults with FASD. It also provides training for professionals and practitioners and advocates for services for people with FASD.
• EU Birth Mothers Support Network www.eurobmsn.org/default.html The European Birth Mother Network - FASD is a network of women who consumed alcohol during pregnancy and may have a child or children with FASD. The network offers a place where mothers can share their experience and support each other.
Carolyn Blackburn 2016

References
Carolyn Blackburn 2016
• Blackburn, C. (2017) Developing inclusive practice for young children with FASD London: Routledge
• Blackburn, C. (2015) Just one won’t hurt Special World http://www.specialworld.net/2015/09/01/just-one-wont-hurt/
• Carpenter, B., Blackburn. C. and Egerton, J. (Eds) (2013) FASD: Interdisciplinary Perspectives London: Routledge
• Blackburn, Carpenter and Egerton (2012) Educating Children and Young People with Fetal Alcohol Spectrum Disorders. London: Routledge
• Blackburn, C. (2012) Drinking it in. SEN Magazine September/October 2012 SEN60 pp 80-83
• Blackburn, C. (2010) Facing the challenge and shaping the future for primary and secondary aged students with Foetal Alcohol Spectrum Disorders (FAS-eD Project) Project Report. London: NOFAS
• Blackburn, C., (2010) Facing the Challenge and Shaping the Future for Primary and Secondary aged Students with Fetal Alcohol Spectrum Disorders (FAS-eD Project, Project Toolkit including project report, literature review, case studies, podcasts and primary and secondary learning and teaching frameworks)
• Blackburn, C. (2009) Building Bridges with Understanding: FASD Practitioner Resource: Pack Focus on Strategies, 2009, Sunfield Publications/Worcestershire County Council, Winner of Editor's Choice Award, Nursery World Awards, 2009
• Carpenter, B. (2013) Evolving Pedagogy for children and young people with fetal alcohol spectrum disorders in B. Carpenter, C. Blackburn and J. Egerton (Eds) Fetal Alcohol Spectrum Disorders: Interdisciplinary perspectives. London: Routledge pp 123-140
• Elliott, E. (2013) Foetal Alcohol Spectrum Disorders: Australian Perspectives in B. Carpenter, C. Blackburn and J. Egerton (Eds) Fetal Alcohol Spectrum Disorders: Interdisciplinary perspectives. London: Routledge pp294-305


















