Editorial Case Report Peripheral Nerve Stimulator guided...
3
Editorial Introduction In the recent years, chest wall blocks have gained popularity amongst the anesthesiologists across the globe. These blocks are superficial and provide aneasier approach to the thoracic wall for perioperative analgesia needed for thoracic surgeries. In 2011, Blanco et al.first described the “PECS” block as a novel analgesia technique for breast surgery [1,2]. The very next year, in 2012, he published the ultrasound (US) techniques for PEC I and PEC II blocks [3]. In 2013, he described a further modification to his PEC blocks, the serratus anterior plane (SAP) block, which covered awider areaand provided superior analgesia.He described blocking the anterior chest wall by depositing local anesthetic (LA) aboveand/or below the SA muscle under US guidance and named this technique asSAPblock [4]. Various publications have described the analgesic efficacy of the SAP block for post-thoracotomy, breast surgery, multiple rib fracture, and other chest wall procedures [5,6]. This novel, superficial and easy to approach analgesia technique is limited by the availability of US machines,especially in the developing world. In this article, we describe a novel approach using a peripheral nerve stimulator (PNS), which will expand the usage of this block. Anatomy relevant to the SAP block The SAP contains the chest wall nerves and includesthe lateral branches of the thoracic intercostal nerves and the long thoracic nerve. The thoracic intercostal nerves arising from T2 to T6, and lying between the SA and the external intercostal muscles. These intercostal nerves give lateral and anterior branches. The lateral branches of the intercostal nerves pierce the SA muscle at the midaxillary level to lie on it and provide the anterior and posterior terminal branches. The lateral cutaneous branch of the second intercostal nerve does not divide into anterior and posterior branches and contribute to the intercostobrachial nerve. The anterior branches cross in front of the internal mammary artery, pierce the intercostales interni muscle, the intercostal membranes and pectoralismajor muscle to supply the breast in its medial aspect [7,8]. The long thoracic nerve or SA nerve arises from the brachial plexus (C5-C7) to enter the axilla behind the rest of the brachial plexus and rest on the SA muscle at the midaxillary level (Fig. 1) [8,9]. Description of the technique The SAPblock done by PNS technique needs the patient to be in the lateral position with block side up and with the arm in front of the chest or insupine position with theipsilateral arm abducted. The midaxillary line is identified and marked. The 5th rib is traced to this line and the intersection point marked. This point is the needle insertion point(Fig. 2 and3). A 50 mm insulated nerve stimulator needle with asyringe filled with LA attached to the extension Peripheral Nerve Stimulator guided serratus anterior plane block: A novel approach to the chest wall block Ritesh Roy¹,Shiv Kumar Singh²,Gaurav Agarwal¹, Chandrasekhar Pradhan¹ Introduction: In the recent years, chest wall blocks have gained popularity among theanesthesiologists across the globe. Blanco et al. initially described the ultrasound (US) guided chest wall blocks that used local anesthetic (LA) deposition under pectoralis major (PEC I), then under the pectoralis minor (PEC II) butlater modified these PEC blocksto cover larger areas of the chest wall by depositing LA more proximally under and/or above the serratus anterior (SA) muscle (SA plane block). Technique of block: Please refer the Article Discussion: The long thoracic nerve or SA nerve arises from the brachial plexus (C5-C7) to enter the axilla behind the rest of the brachial plexus and rest on the SA muscle at the midaxillary level. The limitation of this superficial and easy to approach analgesia technique is the availability of US machines. In this article, we describe a novel approach to the SA plane block with the use of a peripheral nerve stimulator (PNS). Keywords:Chest wall blocks, pectoralblocks, serratus anterior plane, serratus anterior plane block, ultrasound, peripheral nerve stimulator, ultrasound-guided, peripheral nerve stimulatorguided. Case Report Abstract Journal of Anaesthesia and Critical Care Case Reports 2017 Sep-Dec;3(3):24-26 1 Consultant Anesthesiologist, CARE Hospitals, Bhubaneswar, Odisha, India, 2 Consultant Anaesthesiologist, Royal Liverpool University Hospitals, Prescot Streets, Liverpool, UK L7 8XP Address of Correspondence Dr. GauravAgarwal, 1510/B, Sector 6, CDA, Cuttack– 753014, Odisha, India. E-mail: [email protected] © 2017 by Journal of Anaesthesia and Critical Care Case Reports| Available on www.jaccr.com | This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. Journal of Anaesthesia and Critical Care Case Reports Volume 3 Issue 3 Sep-Dec 2017 Page 24-26 24 | | | | | Dr. Ritesh Roy Dr.Shiv Kumar Singh Dr. Chandrasekhar Pradhan Dr. Gaurav Agarwal
Transcript of Editorial Case Report Peripheral Nerve Stimulator guided...

Editorial
IntroductionIn the recent years, chest wall blocks have gained popularity amongst the anesthesiologists across the globe. These blocks are superficial and provide aneasier approach to the thoracic wall for perioperative analgesia needed for thoracic surgeries. In 2011, Blanco et al.first described the “PECS” block as a novel analgesia technique for breast surgery [1,2]. The very next year, in 2012, he published the ultrasound (US) techniques for PEC I and PEC II blocks [3]. In 2013, he described a further modification to his PEC blocks, the serratus anterior plane (SAP) block, which covered awider areaand provided superior analgesia.He described blocking the anterior chest wall by depositing local anesthetic (LA) aboveand/or below the SA muscle under US guidance and named this technique asSAPblock [4]. Various publications have
described the analgesic efficacy of the SAP block for post-thoracotomy, breast surgery, multiple rib fracture, and other chest wall procedures [5,6]. This novel, superficial and easy to approach analgesia technique is limited by the availability of US machines,especially in the developing world. In this article, we describe a novel approach using a peripheral nerve stimulator (PNS), which will expand the usage of this block.
Anatomy relevant to the SAP blockThe SAP contains the chest wall nerves and includesthe lateral branches of the thoracic intercostal nerves and the long thoracic nerve. The thoracic intercostal nerves arising from T2 to T6, and lying between the SA and the external intercostal muscles. These intercostal nerves give lateral and anterior branches. The lateral branches of the intercostal nerves pierce the SA muscle
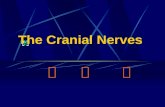
at the midaxillary level to lie on it and provide the anterior and posterior terminal branches. The lateral cutaneous branch of the second intercostal nerve does not divide into anterior and posterior branches and contribute to the intercostobrachial nerve. The anterior branches cross in front of the internal mammary artery, pierce the intercostales interni muscle, the intercostal membranes and pectoralismajor muscle to supply the breast in its medial aspect [7,8]. The long thoracic nerve or SA nerve arises from the brachial plexus (C5-C7) to enter the axilla behind the rest of the brachial plexus and rest on the SA muscle at the midaxillary level (Fig. 1) [8,9].
Description of the techniqueThe SAPblock done by PNS technique needs the patient to be in the lateral position with block side up and with the arm in front of the chest or insupine
position with theipsilateral arm abducted. The midaxillary line is identified and marked. The 5th rib is traced to this line and the intersection point marked. This point is the needle insertion point(Fig. 2 and3).
A 50 mm insulated nerve stimulator needle with asyringe filled with LA attached to the extension
Peripheral Nerve Stimulator guided serratus anterior plane block: A novel approach to the chest wall block
Ritesh Roy¹,Shiv Kumar Singh²,Gaurav Agarwal¹, Chandrasekhar Pradhan¹
Introduction: In the recent years, chest wall blocks have gained popularity among theanesthesiologists across the globe. Blanco et al. initially described the ultrasound (US) guided chest wall blocks that used local anesthetic (LA) deposition under pectoralis major (PEC I), then under the pectoralis minor (PEC II) butlater modified these PEC blocksto cover larger areas of the chest wall by depositing LA more proximally under and/or above the serratus anterior (SA) muscle (SA plane block). Technique of block: Please refer the ArticleDiscussion: The long thoracic nerve or SA nerve arises from the brachial plexus (C5-C7) to enter the axilla behind the rest of the brachial plexus and rest on the SA muscle at the midaxillary level. The limitation of this superficial and easy to approach analgesia technique is the availability of US machines. In this article, we describe a novel approach to the SA plane block with the use of a peripheral nerve stimulator (PNS).Keywords:Chest wall blocks, pectoralblocks, serratus anterior plane, serratus anterior plane block, ultrasound, peripheral nerve stimulator, ultrasound-guided, peripheral nerve stimulatorguided.
Case Report
Abstract
Journal of Anaesthesia and Critical Care Case Reports 2017 Sep-Dec;3(3):24-26
1Consultant Anesthesiologist, CARE Hospitals, Bhubaneswar, Odisha, India,2Consultant Anaesthesiologist, Royal Liverpool University Hospitals, Prescot Streets, Liverpool, UK L7 8XP
Address of CorrespondenceDr. GauravAgarwal, 1510/B, Sector 6, CDA , Cuttack– 753014, Odisha, India.E-mail: [email protected]
© 2017 by Journal of Anaesthesia and Critical Care Case Reports| Available on www.jaccr.com | This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License
(http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Anaesthesia and Critical Care Case Reports Volume 3 Issue 3 Sep-Dec 2017 Page 24-2624 | | || |
Dr. Ritesh Roy Dr.Shiv Kumar Singh
Dr. Chandrasekhar Pradhan
Dr. Gaurav Agarwal

tubing is used for performing the block. Following preparing the area with antiseptic solution, sterile drapes are applied,and the area around the landmark is infiltrated with LA solution. The nerve stimulator is set to an initial current of 1mA of 0.1ms duration and 1Hz frequency. Once the LA has taken effect, the block needle is inserted at the above point and slowly advanced till the SA muscle contraction is noted, stimulation of long thoracic nerve that supplies the muscle. The needle is kept at this depth and current is reduced to 0.3mA. Persistence of contraction of SA at this level confirms the needle placement at target site, i.e.above the SA muscle plane. The LA drug (20mls of 0.2% ropivacaine) is slowly injected in increments with frequent negative aspirations at 5.0mls aliquots.Our target is to block the lateral and posterior cutaneous branches of the intercostal nerves that lie in the same plane as the long thoracic nerve. (Fig 4)
DiscussionIn 2013, Blanco et al. first described a new block of the thoracic wall, the serratus plane block under US guidance. LA was deposited in the SA Plane. The lateral cutaneous branches of the intercostal nerves, before dividing into anterior and posterior branches are blocked as they pass through this plane to supply sensation to most of the
chest wall. The authors observed that an injection superficial to the SA muscle spreads wider and lasts longer than an injection deep to it [3]. Varghese et al. have done anatomical studies to describe widespread of LA in SAP block using US guidance techniques as described by Blanco et al.[10]. The risk of LA toxicity remains low in this technique as lower volume of anesthetic, as compared to other fascial plane blocks, is required for a higher spread and the absorption is lower as the plane is avascular [11].This can be considered an advantage over alternative technique such as intercostal nerve block. Dermatomal block after a single thoracic paravertebral injection is unpredictable and varies widely[12,13]. Wide dermatomal spread with paravertebral block and intercostal blocks need multiple injections, which are time-consuming, and associated with increased incidence of pneumothorax[14,15,16,17]. If the specialist is skilled with US and has a good understanding of the sonoanatomy of the lateral thoracic wall, serratus plane block is a superficial and easy to perform, with a high success rate and minimal incidence of complications. In situations where US machine is not available, it will not be possible for the block to be administeredand, if the specialist is not skilled in the use of US, failure and/or pneumothorax could easily result [11]. SAP
block has been studied by various researchers as a consistent and reliable block for hemithorax analgesia, particularly for breast surgeries [18], post-thoracotomy pain[6], multiple rib fractures, and other chest wall procedures [5]. The limitation of the novel technique being, availability of US machine. This limitation can be offset by the PNS guided technique as described above. It is comparatively reliable technique for the SAP block.
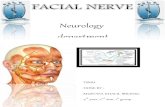
Our experienceThe authors have used this technique in more than 100 cases until now and documented the drug spread using US of the blocked area in patients after PNS guided injection of the drug and noticed good spread of the LA in the plane above SA muscle described as SA plane block as well as good post-operative pain relief (Fig.5a and b). Most of the patients were managed with simple oral analgesics in the post-operative period, and of the cases receiving this block, only 5 patients needed analgesia supplementation with opioids.
Limitations SAP block is a relatively safe and superficial block that can be done by even those who are new to regional anesthesia, but concerns relating to deep puncture and pneumothorax remains. This area is a
Roy R et al www.jaccr.com
Journal of Anaesthesia and Critical Care Case Reports Volume 3 Issue 3 Sep-Dec 2017 Page 24-2625 | | || |
�
Figure 2: Landmarks of serratus anterior plane block.Figure 3:Schematic description of the landmarks and the injection point.Figure 1: Anatomy relevant to the serratus anteriorplane
block.
�
Figure 4:Anatomical depiction of the drug spread. Figure 5: (a, b) Drug spread in serratus anterior plane with aperipheral nerve stimulator (PNS)
A B

www.jaccr.com
Journal of Anaesthesia and Critical Care Case Reports Volume 3 Issue 3 Sep-Dec 2017 Page 24-2626 | | || |
relatively avascular and block needs to be done with caution to remain superficial, to avoid crossing ribs in any circumstances. Althoughour experience in the number of cases done is limited; we have not encountered any complications yet. Larger studies need to be done to establish the safety of the technique compared to other modalities.We have observed the spread of LA under US, contrast study using
fluoroscopy or evenmagnetic resonance imaging (MRI) would define the spread much better.
ConclusionSerratus plane block is superficial and easy to perform, with a high success rate and minimal incidence of complications. As studied by various researchers, it is a consistent and reliable block for hemithorax
analgesia particularly for breast surgeries, post-thoracotomy pains, multiple rib fractures, and other chest wall procedures. By describing a PNS guided technique; we conclude that we can overcome the limitation of having US machine and proficiency in US-guided blocks. The results of this novel PNS guided technique are comparable to US-guided approach to SAP block.
Roy R et al
1. Blanco R. The ‘pecs block’: A novel technique for providing analgesia after breast surgery. Anaesthesia 2011;66:847-8.
2. Blanco R. Bloqueopectoral (pecs block). Manual de Anestesia Regional EconoanatomıaAvanzada. Spain: EneEdiciones; 2011. p. 92-5.
3. Blanco R, Fajardo M, Maldonado TP. Ultrasound description of Pecs II (mod i f i ed Pecs I ) : A nove l app roach to b reas t su rge ry. RevEspAnestesiolReanim 2012;59:470-5.
4. Blanco R, Parras T, McDonnell JG,Prats-Galino A. Serratus plane block: A novel ultrasound-guided thoracic wall nerve block. Anaesthesia 2013;68:1107-13.
5. Kunhabdulla NP, Agarwal A, Gaur A, Gautam SK, Gupta R, Agarwal A. Serratus anterior plane block for multiple rib fractures. Pain Phys 2014;17:E651-3.
6. Madabushi R, Tewari S, Gautam SK, Agarwal A, Agarwal A. Serratus anterior plane block: A new analgesic technique for post-thoracotomy pain. Pain Physician 2015;18:E421-4.
7. Porzionato A, Macchi V, Stecco C, Loukas M, Tubbs RS, De Caro R, et al. Surgical anatomy of the pectoral nerves and the pectoral musculature. ClinAnat 2012;25:559-75.
8 . F i s c h e r J . A n a t o m y o f t h e A x i l l a . F i s c h e r ’ s M a s t e r y o f S u r g e r y . 2 0 1 2 ; 2 . A v a i l a b l e f r o m : http://www.r2library.com/Resource/Title/1608317404/ch0046s1193 [Last retrieved on 2017 Oct 20].
9. BertelliJA.Longthoracic nerve: Anatomy and functional assessment. J Bone Joint Surg (American)2005;87:993.
10. Varghese L, Johnson M, Barbeau M, Rakesh SV, Magsaysay P, Ganapathy
S. The serratus anterior plane (SAP) block: An anatomical investigation of the regional spread of anesthetic using ultrasound-guided injection. FASEB J 2016;30:560.
11. Tighe SQ, Karmakar MK. Serratus plane block: Do we need to learn another technique for thoracic wall blockade? Anaesthesia 2013;68:1103-6.
12. Cheema S, Richardson J, McGurgan P. Factors affecting the spread of bupivacaine in the adult thoracic paravertebral space. Anaesthesia 2003;58:684-7.
13. Cheema SP, Ilsley D, Richardson J, Sabanathan S. A thermographic study of paravertebral analgesia. Anaesthesia 1995;50:118-21.
14. Naja ZM, El-Rajab M, Al-Tannir MA, Ziade FM, Tayara K, Younes F, et al. Thoracic paravertebral block: Influence of the number of injections. RegAnesth Pain Med 2006;31:196-201.
15. Moore DC. Intercostal nerve block: Spread of India ink injected to the rib’s costal groove. Br J Anaesth 1981;53:325-9.
16. Tobias MD, Ferrante FM. Complications of paravertebral, intercostal, and interpleural nerve blocks. In: Finucane BT, editor. Complications of Regional Anesthesia. Philadelphia, PA: Churchill Livingstone; 1999. p. 77-93.
17. Shanti CM, Carlin AM, Tyburski JG. Incidence of pneumothorax from intercostal nerve block for analgesia in rib fractures. J Trauma 2001;51:536-9.
18. Bhoi D, Pushparajan HK, Talawar P, Kumar A, Baidya DK. Serratus anterior plane block for breast surgery in a morbidly obese patient. J ClinAnesth 2016;33:500-1.
References
Roy R, Singh S. K, Agarwal G, Pradhan C. Peripheral Nerve Stimulator guided serratus anterior plane block: A novel approach to the chest wall block. Journal of Anaesthesia and Critical Care Case Reports Sep-Dec 2017; 3(3):24-26.
How to Cite this Article
Conflict of Interest: Nil Source of Support: None