Ectopic pregnancy
27
-
Upload
arya-anish -
Category
Health & Medicine
-
view
379 -
download
0
Transcript of Ectopic pregnancy
History
Lawson Tait – first successful
salpingectomy;1884
Stromme – first conservative
surgery(salpingostomy); 1953
Medical Management
Surgical Management
Surgically administered medical
management
Expectant Management
In case of unruptured pregnancies.
Methotrexate
Antineoplastic drug
Acts as a Folic acid antagonist
ADVANTAGES:
Avoids surgery and anaesthesia
Less expense
Less tubal damage
More chance of future fertlity
CRITERIA FOR SELECTION
Haemodynamically stable
No intrauterine pregnancy on ultrasound
No tubal rupture
Size of ectopic < 4cm
If there is fetal cardiac activity use with caution
βhCG level preferably < 3000 IU/L
Investigations : Full blood count, LFT and
RFT
Exposure to sun should be avoided
Folic acid tablets should not be given
‘Seperation pain’
If medical management fails surgery is
indicated and it becomes necessary in
about 10% women
After methotrexate administration, βhCG is
better for monitoring and ultrasound is not
used
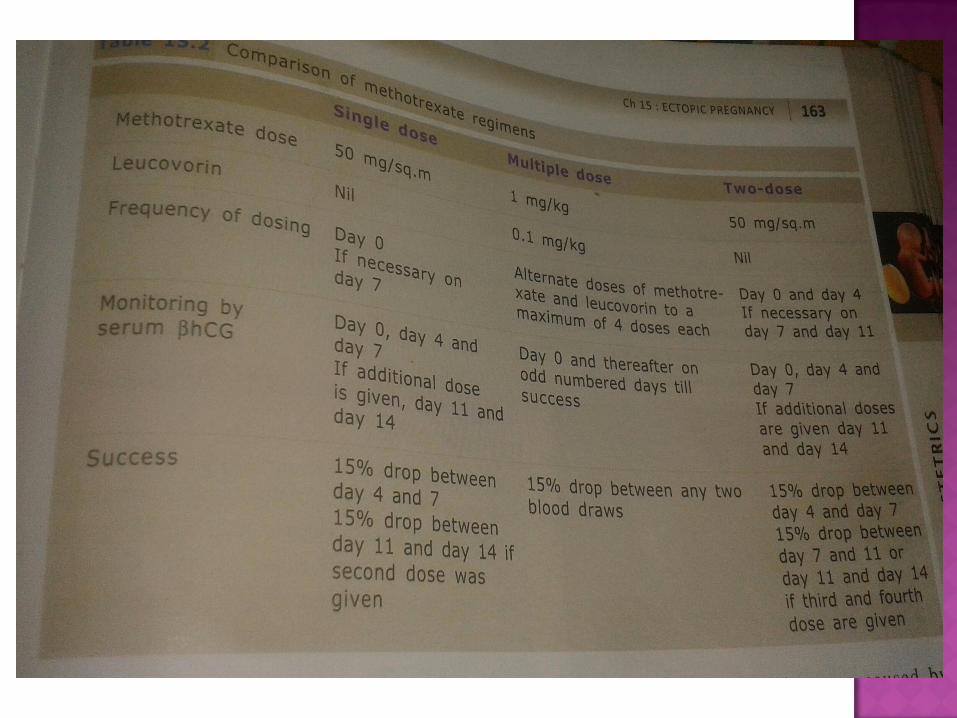
SINGLE DOSE REGIMEN
Single dose of methotrexate
MULTIPLE DOSE REGIMEN
Methotrexate & Leucovorin on alternate days to a
maximum of 4 doses
TWO DOSE REGIMEN
Second dose of methotrexate on day 4
Both conservative surgery & salpingectomy can
be performed at laparoscopy and laparotomy.
Laparoscopy is preferable.
But the laparoscopic experience of the surgeon
and the haemodynamic stability of the patient
matters.
Conservative measures are indicated when the
woman has not completed her family.But in 5%
cases, persistent ectopic has been noted and
hence serial serum βhCG is indicated.
LINEAR SALPINGOSTOMY
In ampullary ectopic
A linear incision is made on the antimesenteric border of the tube immediately over the ectopic and the products will extrude out.
SEGMENTAL RESECTION
When the ectopic is at the isthmus
Segmental resection is followed by isthmoampullaryanastomosis, if necessary.
SALPINGECTOMY
The safest and complete method ,provided the other tube is normal. Ipsilateral ovary should be conserved.
INDICATIONS:
When the tube is not salvageable
Uncontrolled bleeding from the tube
Recurrent ectopic occurs in the same tube
Childbearing is complete
Previous sterilisation
PERSISTENT ECTOPIC
Diagnosed by plateauing or rising serum βhCG values following salpingostomy.
Under ultrasound guidance, direct injection of
a drug is given into the ectopic.
Methotrexate, patassium chloride,
hyperosmolar glucose and PGF2α can be used.
Direct injection of KCl into the sac can be
combined with medical management , in case
of a live ectopic otherwise suited for medical
management.
This is not much employed today.
Option for clinically stable asymptomatic women with an ultrasound diagnosis of ectopic pregnancy and initial serum βhCG below the discriminatory zone (preferably <1000 IU/L) and subsequent falling levels.
These women should be counselled properly and should be within easy reach of the hospital.
Monitoring should be with serial serum βhCG twice weekly.
Infertility (fertility rate around 65%)
Repeat Ectopic (risk of a future ectopic is about
12%)
Heterotopic Pregnancy
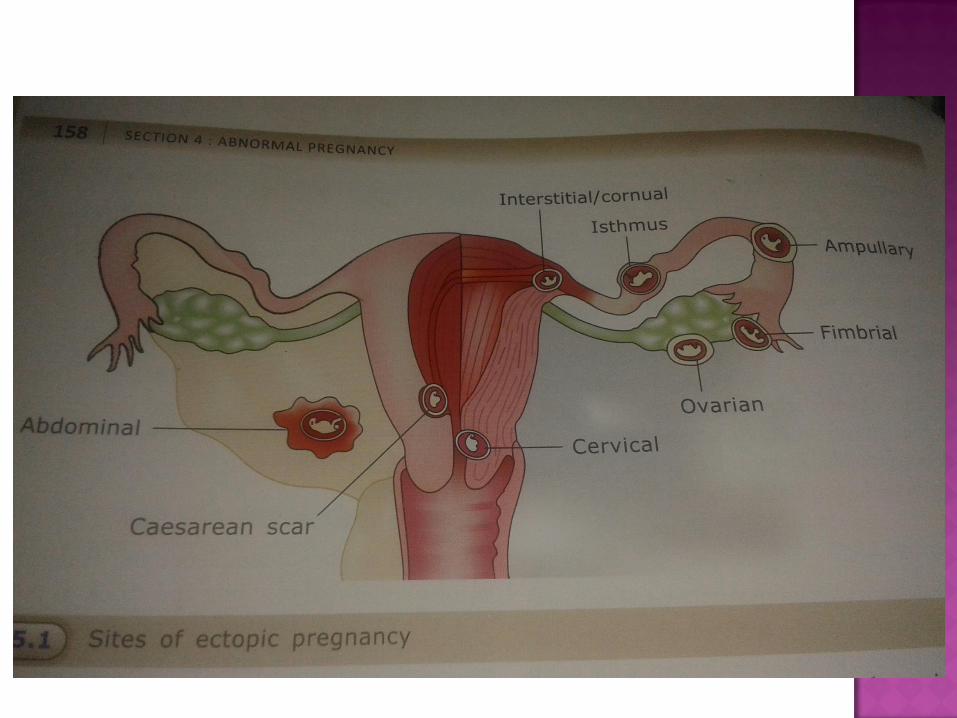
Interstitial and Cornual Pregnancy
Intraligamentous Pregnancy
Abdominal Pregnancy
Cervical Pregnancy
Ovarian Pregnancy
An ectopic pregnancy coexists with an
intraabdominal pregnancy.
Incidence has increased from 1 in
30,000 pregnancies in the past to 1 in
100 pregnancies.
Serial monitoring of serum βhCG is not
helpful.
Management : Surgical
Interstitial : In the proximal intramural part of the tube
Cornual : In the upper and lateral uterine cavity
Involves myometrium and advance to a later
stage (even upto 16 weeks).
USG shows a bulge in the cornual area, with an extremely thin myometrial mantle surrounding gestational sac. The sac should be located more than 1cm from the endometrial echo.
The pregnancy can also be in a rudimentary horn of a bicornuate uterus, usually the horn is non communicating. If diagnosed earlier, excision of the rudimentary horn and the tube of the affected side can be done.
Within the broad ligament
Rare; due to penetration of the tubal wall
by the trophoblast and its advancement
between the two layers of the broad
ligament.
Usually secondary; after early tubal
rupture or abortion. The fertilised ovum
implants on the peritoneum and continues
to grow.
A primary abdominal pregnancy is
extremely rare.
STUDIFORD CRITERIA
Both tubes and ovaries should be normal
Uteroperitoneal fistula should not be seen
The pregnancy is related exclusively to the peritoneal
surface.
In abdominal pregnancy,
Nausea and abdominal pain
Malpresentations and superficial fetal parts
Braxton-Hicks contractions not felt
USG : Absence of uterine outline over the fetus
Management : Laparotomy and removal of fetus
Complications : Torrential haemorrhage due to lack of constriction of open vessels after placental seperation
Unless placenta is implanted over vital structures or major blood vessels it should be removed. Or else left in situ and autolysis awaited.
Monitored by serial ultrasound and serum βhCGlevels.
Methotrexate can be given.
Implantation in the endocervical canal below the internal os.
Predisposing factorsPrevious dilatation and curettage
Previous caesarean section
Most common symptom – Painless vaginal bleeding
Usually diagnosed incidentally during a routine scan or during evacuation of a suspected abortion.
Blood flow around the sac is more suggestive of a true cervical pregnancy.
Colour doppler can be used to differentiate between a true cervical pregnancy and an intact gestational sac passing through cervix.
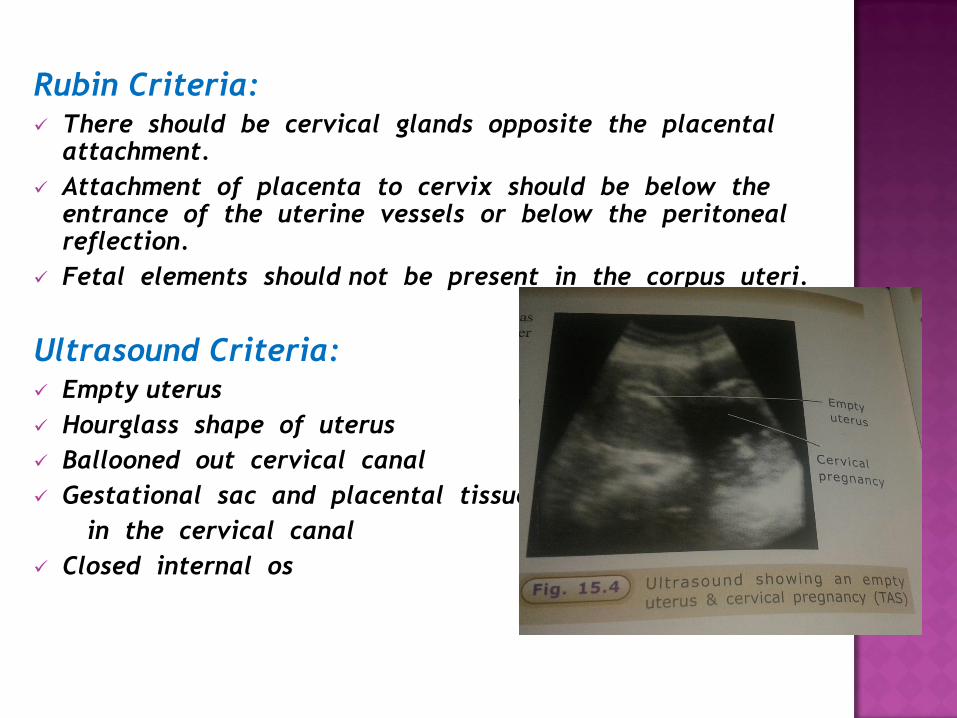
Rubin Criteria: There should be cervical glands opposite the placental
attachment.
Attachment of placenta to cervix should be below the entrance of the uterine vessels or below the peritoneal reflection.
Fetal elements should not be present in the corpus uteri.
Ultrasound Criteria: Empty uterus
Hourglass shape of uterus
Ballooned out cervical canal
Gestational sac and placental tissue
in the cervical canal
Closed internal os
First choice : Medical treatment with
multiple dose methotrexate.
Radiological uterine artery embolisation
followed by evacuation. Bilateral internal
iliac artery ligature has also been tried.
Hysterectomy
Implantation in the ovary
Very rare
Usual consequence : Rupture at an early stage
Management : Surgery; ovariotomy
Methotrexate if diagnosed earlier
Spiegelberg Criteria: The tube on the affected side should be intact.
Fetal sac should occupy the position of the ovary.
Ovary should be connected to the uterus by the ovarian ligament.
Definite ovarian tissue should be found in the sac wall.
In women with a previous caesarean section.
Diagnostic criteria:
An empty uterine cavity
A gestational sac located anteriorly at the level of
the internal os covering the visible or presumed
site of the previous lower uterine segment
caesarean section scar
Evidence of functional trophoblastic /placental
circulation on Doppler examination
An absent “sliding sign” (inability to displace the
gestational sac from its position at the level of
internal os using gentle pressure applied by the
transvaginal probe)