Echocardiography and the neonatologist
4
Echocardiography and the neonatologist Lindsey Hunter Neil Patel Abstract Echocardiographic assessment can be broadly divided into functional and structural assessment. Functional echocardiography in the hands of an appropriately trained neonatologist is an accessible and useful modality in the neonatal intensive care unit. This tool allows the neonatologist to assess various parameters, e.g. ventricular outputs and SVC flow, ventricular function, pulmonary pressures and ductus arteriosus and implement immediate management as result. It is essential that there is support from the paediatric cardiologist to prevent misdiagnosis of congenital heart disease and implement further management. Keywords ductus arteriosus; echocardiography; functional assessment; neonatal intensive care; structural assessment; SVC flows; ventricular function Part 1: overview of practice Over the past decade echocardiography has increasingly become both a useful and accessible modality within neonatal units. Echocardiography (echo) is a powerful tool in the hands of an appropriately trained operator. Echo assessment can be broadly divided into functional and structural assessments. There is a distinct overlap between the two assessment categories, each will inform the other and neither should be considered in isolation. Structural assessment of congenital heart disease is impera- tive to delineate basic and complex cardiac anatomy including identifying significant anomalies. Functional assessment is an evaluation of myocardial function and haemodynamics. Although introduced primarily a research tool, functional echo is increasingly employed at the bedside by neonatologists. Serial measurements are used to answer specific and immediate clinical questions in the context of the rapidly changing haemodynamics of a sick neonate. Functional echo should be performed as an adjunct or in addi- tion to existing clinical parameters; e.g. lactate, CRT, heart rate, blood pressure which are of limited value and are open to observer variability. Functional echocardiography provides a direct measure of myocardial function, pulmonary and systemic blood flows and also intra/extra cardiac shunting. Who should undertake echocardiograms within the neonatal intensive care? Practicalities, location and politics can often delay a cardiology assessment within neonatal units. Traditionally the diagnosis and management of significant and complex congenital heart disease has been the realm of the appropriately skilled and experienced paediatric cardiologist. However, if functional echocardiograms are performed by the attending neonatal team frequent assessment and therapeutic adjustment can be made without the immediate input of paediatric cardiologist. The neonatology team must be aware that functional assess- ment does not exclude structural heart defects. This also high- lights a potential medico-legal debate surrounding neonatologists undertaking echocardiograms routinely; the main concern being the potential to misinterpret or even misdiagnose life threatening congenital heart disease. Neonatologists must be are aware of their limitations when structurally assessing the neonatal heart; in particular there are diagnoses which even an experienced cardiologist may find difficult to make or have the potential to miss including coarctation of the aorta, total anomalous pulmo- nary venous drainage (TAPVD), anomalous left coronary artery (ALCAPA), congenitally corrected transposition of the great arteries and atrial isomerisms. To ensure neonatologists are adequately trained and that echocardiography within the neonatal intensive care is safe, open and easily accessible lines of communication between the paediatric cardiologists and the neonatologists is desirable. We recommend a model of support for neonatologists by paediatric cardiologists at a ward level, continuing medical education (CME), echocardiography courses, training materials and ongoing positive feedback. There should be opportunities for the neonatal trainees to work alongside the cardiologists in the form of an official placement. In the UK and worldwide, including at our centre, formally-accredited echocardiography courses are run which are appropriate for neonatologists and allied professionals. In our hospital there is a close working relationship between the paediatric cardiologists and neonatologists with a specialist interest in cardiology. This allows for prompt and timely assessment of newborns with abnormal clinical examination findings or clinical parameters. Both teams meet weekly to discuss the ongoing care of those neonates with significant heart disease in the NICU. Part 2 The second part of this article focuses on the specific functional echocardiographic measures which are used frequently in the neonatal intensive care unit. It is important to stress that these should always be accompanied by a complete assessment of cardiac structure, as discussed above. Whilst we hope to provide some practical insights into these assessments, it is beyond the scope of this article to teach these techniques. Assessment of the ductus arteriosus (DA) Assessment of the DA is most frequently performed in pre-term infants, in whom consideration may be given to closure by surgical or medical therapies, but is also important in Lindsey Hunter MBChB MRCPCH is a Paediatric Cardiology Specialist Trainee in the Cardiology Department Royal Hospital for Sick Children, Glasgow G3 8SJ, UK. Conflicts of interest: none. Neil Patel BA MBChB MRCPCH MD is a Consultant Neonatologist in Neonatal Intensive Care at the Royal Hospital for Sick Children, Glasgow G3 8SJ, UK. Conflicts of interest: none. SYMPOSIUM: NEONATOLOGY PAEDIATRICS AND CHILD HEALTH 21:6 254 Ó 2010 Elsevier Ltd. All rights reserved.
-
Upload
lindsey-hunter -
Category
Documents
-
view
213 -
download
0
Transcript of Echocardiography and the neonatologist

SYMPOSIUM: NEONATOLOGY
Echocardiography and theneonatologistLindsey Hunter
Neil Patel
AbstractEchocardiographic assessment can be broadly divided into functional and
structural assessment. Functional echocardiography in the hands of an
appropriately trained neonatologist is an accessible and useful modality
in the neonatal intensive care unit. This tool allows the neonatologist
to assess various parameters, e.g. ventricular outputs and SVC flow,
ventricular function, pulmonary pressures and ductus arteriosus and
implement immediate management as result. It is essential that there is
support from the paediatric cardiologist to prevent misdiagnosis of
congenital heart disease and implement further management.
Keywords ductus arteriosus; echocardiography; functional assessment;
neonatal intensive care; structural assessment; SVC flows; ventricular
function
Part 1: overview of practice
Over the past decade echocardiography has increasingly become
both a useful and accessible modality within neonatal units.
Echocardiography (echo) is a powerful tool in the hands of an
appropriately trained operator. Echo assessment can be broadly
divided into functional and structural assessments. There is
a distinct overlap between the two assessment categories, each
will inform the other and neither should be considered in
isolation.
Structural assessment of congenital heart disease is impera-
tive to delineate basic and complex cardiac anatomy including
identifying significant anomalies.
Functional assessment is an evaluation of myocardial function
and haemodynamics. Although introduced primarily a research
tool, functional echo is increasingly employed at the bedside by
neonatologists. Serial measurements are used to answer specific
and immediate clinical questions in the context of the rapidly
changing haemodynamics of a sick neonate.
Functional echo should be performed as an adjunct or in addi-
tion to existing clinical parameters; e.g. lactate, CRT, heart rate,
blood pressurewhich are of limited value and are open to observer
variability. Functional echocardiography provides a direct
Lindsey Hunter MBChB MRCPCH is a Paediatric Cardiology Specialist
Trainee in the Cardiology Department Royal Hospital for Sick Children,
Glasgow G3 8SJ, UK. Conflicts of interest: none.
Neil Patel BA MBChB MRCPCH MD is a Consultant Neonatologist in Neonatal
Intensive Care at the Royal Hospital for Sick Children, Glasgow G3 8SJ,
UK. Conflicts of interest: none.
PAEDIATRICS AND CHILD HEALTH 21:6 254
measure of myocardial function, pulmonary and systemic blood
flows and also intra/extra cardiac shunting.
Who should undertake echocardiograms within the neonatal
intensive care? Practicalities, location and politics can often delay
a cardiology assessment within neonatal units. Traditionally the
diagnosis and management of significant and complex congenital
heart disease has been the realm of the appropriately skilled and
experienced paediatric cardiologist. However, if functional
echocardiograms are performed by the attending neonatal team
frequent assessment and therapeutic adjustment can be made
without the immediate input of paediatric cardiologist.
The neonatology team must be aware that functional assess-
ment does not exclude structural heart defects. This also high-
lights a potential medico-legal debate surrounding neonatologists
undertaking echocardiograms routinely; the main concern being
the potential to misinterpret or even misdiagnose life threatening
congenital heart disease. Neonatologists must be are aware of
their limitations when structurally assessing the neonatal heart;
in particular there are diagnoses which even an experienced
cardiologist may find difficult to make or have the potential to
miss including coarctation of the aorta, total anomalous pulmo-
nary venous drainage (TAPVD), anomalous left coronary artery
(ALCAPA), congenitally corrected transposition of the great
arteries and atrial isomerisms.
To ensure neonatologists are adequately trained and that
echocardiography within the neonatal intensive care is safe, open
and easily accessible lines of communication between the
paediatric cardiologists and the neonatologists is desirable. We
recommend a model of support for neonatologists by paediatric
cardiologists at a ward level, continuing medical education
(CME), echocardiography courses, training materials and
ongoing positive feedback. There should be opportunities for the
neonatal trainees to work alongside the cardiologists in the form
of an official placement. In the UK and worldwide, including at
our centre, formally-accredited echocardiography courses are run
which are appropriate for neonatologists and allied professionals.
In our hospital there is a close working relationship between
the paediatric cardiologists and neonatologists with a specialist
interest in cardiology. This allows for prompt and timely
assessment of newborns with abnormal clinical examination
findings or clinical parameters. Both teams meet weekly to
discuss the ongoing care of those neonates with significant heart
disease in the NICU.
Part 2
The second part of this article focuses on the specific functional
echocardiographic measures which are used frequently in the
neonatal intensive care unit. It is important to stress that these
should always be accompanied by a complete assessment of
cardiac structure, as discussed above. Whilst we hope to provide
some practical insights into these assessments, it is beyond the
scope of this article to teach these techniques.
Assessment of the ductus arteriosus (DA)
Assessment of the DA is most frequently performed in pre-term
infants, in whom consideration may be given to closure by
surgical or medical therapies, but is also important in
� 2010 Elsevier Ltd. All rights reserved.
SYMPOSIUM: NEONATOLOGY
duct-dependent congenital cardiac disease and for assessment of
pulmonary artery pressures.
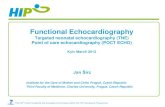
The DA is typically directly visualized from a high left para-
sternal view. From this position the entire length of the DA can
be demonstrated between proximal descending aorta and
pulmonary artery, and a Doppler of flow velocities and directions
may be performed (Figure 1).
The diameter of the DA may be measured at its insertion into
the pulmonary artery from 2-dimensional and colour Doppler
images. Any constriction of the PDA usually occurs at this point.
Ductal diameters, and the presence of constriction, may assist
prediction of spontaneous duct closure.
There is increasing interest in defining a haemodynamically
significant ductus arteriosus (HSDA). This depends on combined
echocardiographic and clinical assessment, and may be assisted
by a scoring system such as that proposed by McNamara et al.
(Ref). Echocardiographic findings in HSDA are of moderate to
large sized ductuswith unrestricted left-to-right flowof reasonably
high velocity. The echo may also demonstrate reversed diastolic
flow in the proximal descending aorta which may accompany
evidence of impaired abdominal end organ perfusion.
The shunt size through a DA may also be assessed indirectly
by measurement of the left atrium:aortic diameter ratio (LA:Ao).
A left-to-right ductal shunt leads to increased pulmonary venous
return, leading to enlargement of the LA and an increase in the
ratio. Both LA and Ao diameters are obtained from a parasternal,
long-axis m-mode image, the aortic valve diameter is measured
at end diastole and the maximal LA diameter at end systole. A
ratio of greater >1.5:1 is associated with a HSDA.
Management of the HSDA remains controversial and variable.
Early targeted treatment using NSAIDs, ibuprofen or indometh-
acin, is advocated by some authors to achieve greater rates of DA
closure and minimize the pathological consequence of an HSDA.
Serial echocardiography allows more selective, targeted and
shorter courses of NSAID to be given, thereby minimizing the
risks of side effects.
RVOT
MPA
LPA
Descending
aorta
Patent
ductus
Pulse wave
Doppler sample
RPA
Figure 1 Schematic diagram of DA demonstrating position for Doppler of
DA flow.
PAEDIATRICS AND CHILD HEALTH 21:6 255
Calculation of ventricular outputs and superior vena cava
(SVC) flows
Measurement of systemic blood flow, combined with blood
pressure allows more informed therapeutic decisions to be made
in the haemodynamically compromised infant. Echocardiography
allows non-invasive measurement of flows in infants where
invasive flow monitoring is too risky or technically challenging.
Calculation of flows requires measurement of a valve diam-
eter, or vessel, to calculate its cross sectional area (CSA). A pulse
wave Doppler flow of velocity against time is then obtained
across the valve, or within the vessel, and the area under this
traced for one cardiac cycle to generate the velocity time integer
(VTI). The flow (in volume/time) is equal to the product of CSA,
VTI and heart rate and is often divided by weight for expression
as ml/kg/min.
Cardiac output¼ Velocity time integer
� valve cross sectional area� heart rate
Right and left ventricular outputs may be measured this way and
have been shown to change in RDS, PDA and high output states.
In the absence of any shunts right (RVO) and left ventricular
outputs (LVO) are equal to each other and systemic blood flow
(SBF), and are normally between 220 and 250 ml/kg/min.
However, atrial and ductal shunts are common in pre-term
infants (refs) and will lead to differences between RVO and LVO,
such that ventricular outputs cannot be considered equal to SBF.
It has therefore been suggested that measurement of SVC
flow, i.e. blood flow returning to the heart, may provide a better
proportional measure of SBF, independent of shunts. A subcostal
Doppler of SVC flow entering the RA is obtained and combined
with SVC diameter measurements from long-axis views to
calculate SVC flows, which are normally around 80 ml/kg/min.
SVC Flow¼ Velocity time integer� SVC cross sectional area
� heart rate
SVC flows appear to be low in a proportion of pre-term infants
(newborn low output state) who may be at risk of hypotension,
IVH and neurodevelopmental abnormality (HUNT).
Although not in widespread clinical use, appropriately trained
and equipped neonatal units may routinely measure ventricular
outputs and SVC flows.
It should be appreciated that the error in any flow measure-
ment may be as high as 25%, due to the numerous measure-
ments involved.
Ventricular function
Ventricular function assessment is complicated by the complex
nature of the cardiac cycle and 3-dimensional geometry of the
ventricles.
Rapid clinical assessment of ventricular function is often
based on subjective opinion from 2-dimensional images obtained
in the long and short parasternal axes and apical 4-chamber
views. This technique has the significant limitations of being
subjective, observer dependent and non-quantitative.
Quantitative volumetric measures of LV function include
ejection fraction and fractional shortening, calculated from
� 2010 Elsevier Ltd. All rights reserved.
LARA
LVRV
Doppler beam
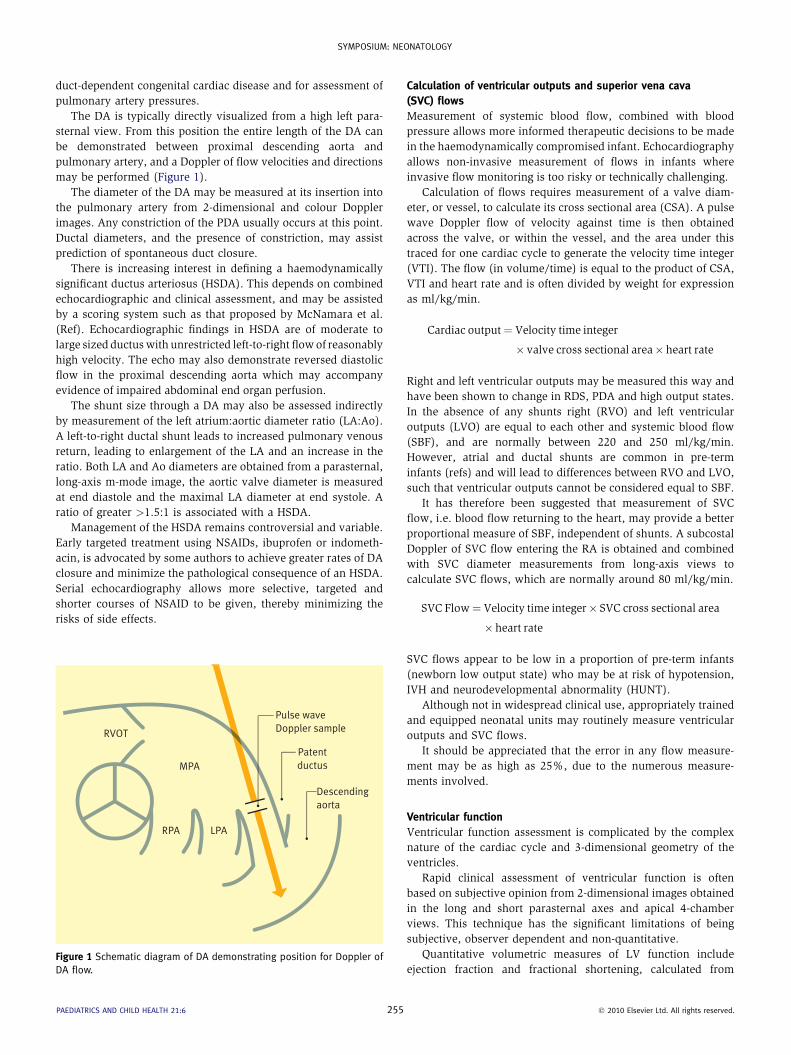
Figure 2 Apical 4-chamber view demonstrating position of Doppler sample
for measurement of tricuspid regurgitation velocity.
SYMPOSIUM: NEONATOLOGY
long-axis parasternal m-mode images. Though widely employed
this technique measures systolic function only, is prone to
measurement error and is not independent of changes in loading
conditions. An alternative measure of LV systolic function is the
relationship between LV mean velocity of circumferential fibre
shortening (LV MVCF). This technique is said to have the
advantages of being pre-load independent and takes after-load
into account. However, LV MVCF requires measurements of LV
volume, LV wall thickness, ejection time and arterial pressure
and is arguably too cumbersome for routine clinical use.
An alternative global measure of ventricular function is the
Myocardial Performance Index (MPI), or Tei index. This is
derived from time intervals during the cardiac cycle. Though
easily performed in neonates MPI gives no indication of systolic
and diastolic functions, and is also load-dependent i.e. changes
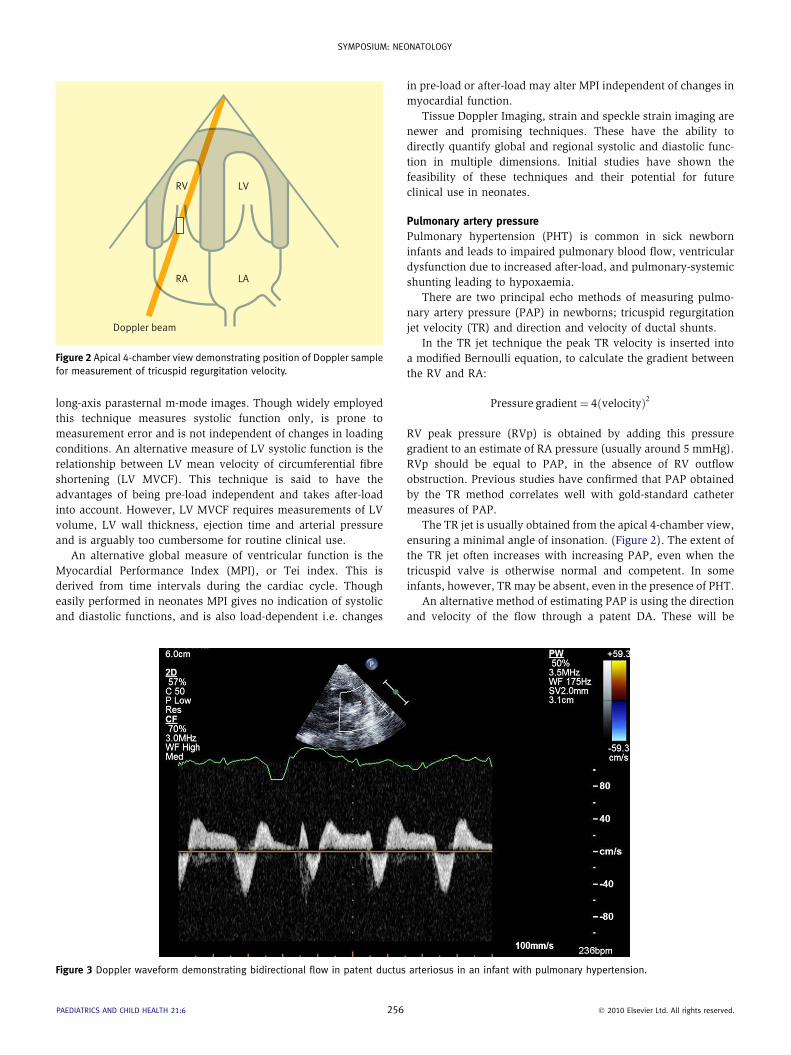
Figure 3 Doppler waveform demonstrating bidirectional flow in patent ductus
PAEDIATRICS AND CHILD HEALTH 21:6 256
in pre-load or after-load may alter MPI independent of changes in
myocardial function.
Tissue Doppler Imaging, strain and speckle strain imaging are
newer and promising techniques. These have the ability to
directly quantify global and regional systolic and diastolic func-
tion in multiple dimensions. Initial studies have shown the
feasibility of these techniques and their potential for future
clinical use in neonates.
Pulmonary artery pressure
Pulmonary hypertension (PHT) is common in sick newborn
infants and leads to impaired pulmonary blood flow, ventricular
dysfunction due to increased after-load, and pulmonary-systemic
shunting leading to hypoxaemia.
There are two principal echo methods of measuring pulmo-
nary artery pressure (PAP) in newborns; tricuspid regurgitation
jet velocity (TR) and direction and velocity of ductal shunts.
In the TR jet technique the peak TR velocity is inserted into
a modified Bernoulli equation, to calculate the gradient between
the RV and RA:
Pressure gradient¼ 4ðvelocityÞ2
RV peak pressure (RVp) is obtained by adding this pressure
gradient to an estimate of RA pressure (usually around 5 mmHg).
RVp should be equal to PAP, in the absence of RV outflow
obstruction. Previous studies have confirmed that PAP obtained
by the TR method correlates well with gold-standard catheter
measures of PAP.
The TR jet is usually obtained from the apical 4-chamber view,
ensuring a minimal angle of insonation. (Figure 2). The extent of
the TR jet often increases with increasing PAP, even when the
tricuspid valve is otherwise normal and competent. In some
infants, however, TR may be absent, even in the presence of PHT.
An alternative method of estimating PAP is using the direction
and velocity of the flow through a patent DA. These will be
arteriosus in an infant with pulmonary hypertension.
� 2010 Elsevier Ltd. All rights reserved.
Practice points
C Echocardiography is a convenient and increasingly important
tool in the assessment and management of newborn infants in
the intensive care unit.
C Neonatologists performing echocardiography must be
appropriately trained, and should work collaboratively with
a supportive local Paediatric Cardiology team.
C Neonatal echocardiography includes structural and functional
assessments.
C Complete structural assessment is imperative to detect
complex cardiac anatomy, which should be managed in
conjunction with the Paediatric Cardiology Team.
C Functional assessment allows improved understanding of the
mechanisms of cardiovascular compromise infants with and
without structural anomalies.
C Functional assessment includes measures of ventricular
function, pressures (including pulmonary arterial pressures),
and blood flows in the heart and major vessels.
SYMPOSIUM: NEONATOLOGY
dependent on the pressure gradient between the pulmonary
artery and aorta at any point in the cardiac cycle. Ductal flow will
be left-to-right if aortic pressure (Aop) exceeds PAP. As PAP
increases flow in the DA may reverse, becoming bidirectional
(Figure 3). If PAP is above aortic pressure throughout the cardiac
cycle, as in severe pulmonary hypertension, then DA flow will be
exclusively right-to-left flow.
The velocity of the DA flow can be inserted into the Bernoulli
equation to calculate the peak pressure gradient between PA and
Aop. However, this peak gradient does not equal the true
difference between peak PA and peak Aop. This is because RV
and LV ejections do not necessarily coincide, and therefore peak
PAP and peak Aop are not simultaneous either.
PAP is not linearly related to RV function, and therefore any
assessment of pulmonary pressures should include an assess-
ment of ventricular function.
Summary
There is an expanding role for functional echocardiographywithin
the NICU, and for neonatologists performing echocardiograms.
However, neonatologistsmust beappropriately trainedand should
work in conjunction with, and supported by, their Paediatric
Cardiology colleagues. Neonatal functional cardiology remains an
area of evolving research and discovery with the aim of improving
outcomes for all infants with haemodynamic compromise. A
FURTHER READING
Carmo K, Evans N, Paradisis M. Duration of indomethacin treatment of the
preterm patent ductus arteriosus as directed by echocardiography.
J Pediatr 2009; 155: 819e22.
Evans N. Diagnosis of patent ductus arteriosus in the preterm newborn.
Arch Dis Child 1993; 68: 58e61.
Evans N. Echocardiography on neonatal intensive care units in Australia
and New Zealand. J Paediatr Child Health 2000; 36(2): 169e71.
Evans N, Kluckow M. Early determinants of right and left ventricular
output in ventilated preterm infants. Arch Dis Child Fetal Neonatal Ed
1996; 74: F88e94.
Hiraishi S, Horiguchi Y, Misawa H, et al. Noninvasive Doppler echocar-
diographic evaluation of shunt flow dynamics of the ductus arteriosus.
Circulation 1987; 75: 1146e53.
Iyer P, Evans N. Re-evaluation of the left atrial to aortic root ratio as
a marker of patent ductus arterious. Arch Dis Child Fetal Neonatal Ed
1994; 70: F112e7.
Kluckow M, Evans N. Superior vena cava flow in newborn infants: a novel
marker of systemic blood flow. Arch Dis Child Fetal Neonatal Ed 2000;
82: F182e7.
Kluckow M, Seri I, Evans N. Functional echocardiography an emerging tool
for the neonatologist. J Pediatr 2007; 150: 125e30.
McNamara PJ, Sehgal A. Towards rational management of the patent
ductus arteriosus: the need for disease staging. Arch Dis Child Fetal
Neonatal Ed 2007; 93(6): F424e7.
PAEDIATRICS AND CHILD HEALTH 21:6 257
Mori K, Nakagawa R, Nii M, et al. Pulsed wave Doppler tissue echocar-
diography assessment of the long axis function of the right and left
ventricles during the early neonatal period. Heart 2004; 90: 175e80.
Osborn DA, Evans N, Kluckow M. Left ventricular contractility in extremely
premature infants in the first day and response to inotropes. Pediatr
Res 2007; 61: 335e40.
Patel N, Mills JF, Cheung MM. Assessment of right ventricular function
using tissue Doppler imaging in infants with pulmonary hypertension.
Neonatology 2009; 96: 193e9.
Patel N, Mills JF, Cheung MM. Use of the myocardial performance index to
assess right ventricular function in infants with pulmonary hyperten-
sion. Pediatr Cardiol 2009; 30: 133e7.
Sehgal A, McNamara PJ. Does point of care functional echocardiography
enhance cardiovascular care in the NICU? J Perinatol 2008; 28:
729e35.
Skinner J, Alverson D, Hunter S. Echocardiography for the neonatologist,
vol. 6. London: Churchill Livingstone, 2000: 133e150.
Skinner JR, Stuart AG, O’Sullivan J, Heads A, Boys RJ, Hunter S. Right
heart pressure determination by Doppler in infants with tricuspid
regurgitation. Arch Dis Child 1993; 69: 216e20.
Skinner JR, Hunter S, Hey EN. Haemodynamic features at presentation in
persistent pulmonary hypertension of the newborn and outcome. Arch
Dis Child Fetal Neonatal Ed 1996; 74: F26e32.
Tsutsumi T, Ishii M, Eto G, Hota M, Kato H. Serial evaluation for myocardial
performance in fetuses and neonates using a new Doppler index.
Pediatr Int 1999; 41: 722e7.
Ward CJ, Purdie J. Diagnostic accuracy of paediatric echocardiograms
interpreted by individuals other than paediatric cardiologists. J Pae-
diatr Child Health 2001; 37: 3316.
� 2010 Elsevier Ltd. All rights reserved.