
Xie-Xie Dr. Xiaoming Zhang, Professor Dr. Ji-cheng Li, and Professor Dr. Lizhong Du.
Upload
alfred-grayCategory
view
214download
0
EATINGEATING DISORDERSDISORDERS
Review Course in PsychiatryReview Course in PsychiatryUniversity of OttawaUniversity of Ottawa
20122012
Dr. Wendy Spettigue, Associate ProfessorDr. Wendy Spettigue, Associate Professorand Dr. Clare Roscoe, Assistant Professorand Dr. Clare Roscoe, Assistant ProfessorUniversity of OttawaUniversity of [email protected]@cheo.on.ca

Eating Disorders OverviewEating Disorders Overview
• Epidemiology
• Diagnosis
• Understanding Eating Disorders– Etiology, Risk Factors, and Power
• Medical Complications
• Principles of Treatment
• Outcome

Epidemiology:Epidemiology:• Prevalence
A.N. 0.5-1% (for strictly defined) B.N. 1-3% EDNOS 3-10%
• ♀ : ♂ 10 : 1
• Onset– A.N. : 13-20 yrs (peaks at 14 and 18 yrs)
: 5% present after 20 years of age– B.N. : 16.5-19 yrs old

Types of Eating DisordersTypes of Eating Disorders1. Anorexia Nervosa
– Restricting Type– Binge-Eating/Purging Type
2. Bulimia Nervosa − Purging Type− Nonpurging Type
3. Eating Disorder NOS

Definitions: Anorexia NervosaDefinitions: Anorexia NervosaA. Refusal to maintain body
weight Body weight <85% of expected
B. Intense fear of gaining weight
C. Distorted body image - or Undue influence of weight on self-worth, - or Denial of seriousness of the low weight
D. Amenorrhea: the absence of at least 3 consecutive menstrual cycles

Common Symptoms of A.N.:Common Symptoms of A.N.:
• Restricting intake
• Exercising
• Standing, moving, restlessness
• Self-induced vomiting
• Diet pills, laxatives

Anorexia Nervosa cont’dAnorexia Nervosa cont’d
• Specify:– Restricting Type – Binge-Eating / Purging Type
Purging - Vomiting- Laxatives- Diuretics- Enemas

Bulimia NervosaBulimia NervosaA. Recurrent Binge Eating:
1. Eating a very large amount of food in a discrete period of time
2. Lack of control during the episode
B. Recurrent Compensatory behavior
to prevent weight gain (vomiting, laxatives, fasting, over-exercising…)

Bulimia NervosaBulimia Nervosa
C. A. and B. occur at least:• 2x / week for 3 months
D. Self-worth unduly influenced by shape and weight
E. Not A.N.

Bulimia Nervosa Cont..Bulimia Nervosa Cont..
• Specify:– Purging Type – Nonpurging Type

The Bulimic CycleThe Bulimic Cycle
• A binge is almost always the result of dieting and food restriction.
• Purging is the result of:
– Fear of weight gain
– The perception of stomach discomfort
– Shame caused by the loss of control over eating
Restrict
Binge
Purge

Eating Disorder NOS Eating Disorder NOS (EDNOS)(EDNOS)
Patient does not meet all the criteria for an eating disorder. For example:
– A.N. with normal periods– A.N. with the psychological criteria but is
above 85%ile for weight– Frequent purging but no binge-eating and
above 85%ile for weight– Binge Eating Disorder will be a new
diagnostic category in the next DSM

Understanding Eating DisordersUnderstanding Eating Disorders
• Rates of body dissatisfaction are > 85% in females, and up to 90% of teenage girls will go on a diet. What happens to the 5%, (and the boys), that go on to develop Eating Disorders?

Eating Disorders:Eating Disorders:
• Eating disorders are not a fad or phase, and not the same as dieting
• Eating disorders are severe mental illnesses with significant medical risks
• Eating disorders are not the fault of the parents or the child

The Development of an EDThe Development of an ED
Vulnerable Youth
-Risk factors-Comorbidities-Low self-esteem
Stressors
Need to Gain Control / Feel Better
Dieting
Sense of Achievement
Increased Dieting
Snowballing of behaviours
Eating Disorder

Risk Factors for ANRisk Factors for ANIndividual Family CulturalFemale Gender Family History of ED /
Anxiety / Mood disorder / OCPD
Idealization of thinness, “normative discontent” for female body image
Perfectionism / Obsessionality/ “harm avoidance”
Early life: “high concern parenting”
Gay males
Low self-esteem / Sense of ineffectiveness
Lack of family meals Activity where thinness = success e.g. modeling / acting
Eagerness to please / High sensitivity/ self-consciousness
Competitive sports with emphasis on thinness: e.g.. gymnastics / ballet
Puberty Peer group that over-values appearances

Risk Factors for BNRisk Factors for BN
Individual Family CulturalFemale Family Hx of obesity Idealization of
thinness
Low self-esteem / Sense of ineffectiveness
Family Hx of Mood /Anxiety / ED / or Substance Abuse / Cluster B PD
Specific sports / activities as AN
Critical comments re. weight / shape / eating
Hx of sexual abuse
Volatile / conflicted family environments

Co-Morbidity of A.N.:Co-Morbidity of A.N.:
• 50-65% Depression (i.e. #1 comorbidity)
• >50% Anxiety Disorders (esp. GAD, Social Phobia and OCD)
• Perfectionism
• “Cluster ‘C’ P.D. traits, e.g.. OCPD (rigidity, restraint, obsessiveness)

Comorbidity of B.N.:Comorbidity of B.N.:
• Depression 50-65%%, #1 comorbidity • Anxiety in >50% (esp. GAD and Social Phobia)• Substance Abuse• Impulsivity/risk-taking behaviors• Borderline Personality Disorder traits• PTSD• Bipolar Spectrum disorders

E.D. SpectrumE.D. Spectrum
• A.N.-------------A.N./B-P--------------B.N.
• Perfectionistic Chaotic
• Compliant Unstable moods
• Anxious Substance abuse
• Sensitive Impulsive
• Possible OCPD Possible BPD

Understanding Eating Understanding Eating Disorders:Disorders:

Eating Disorders come from: Eating Disorders come from: • Feeling “not good enough”
• Feeling worried or stressed
• Feeling “out of control”
• Feeling you don’t deserve good things
• Feeling like you should keep your problems to yourself / not burden others
• Wanting to be accepted and liked
• Not wanting to give others something to criticize or tease you about

The Development of an EDThe Development of an ED
Vulnerable Youth
-Risk factors-Comorbidities-Low self-esteem
Stressors
Need to Gain Control / Feel Better
Dieting
Sense of Achievement
Increased Dieting
Snowballing of behaviours
Powerful Eating Disorder

i.e. What makes
an Eating
Disorder so
Strong?

What an Eating Disorder What an Eating Disorder does….does….
• Complete preoccupation with food and weight
• Isolation
• Give up or dramatically alter relationships with family and friends
• Effects on school / work
• Effects on sports / hobbies

Why so powerful? Why so powerful? Understanding the Eating Understanding the Eating
DisorderDisorder
• Effects of starvation
• The Meaning of the Eating Disorder
• An illness by nature that creates denial / poor insight

Effects of StarvationEffects of Starvation
• Ancel Keys, University of Minnesota, during WWII
• Psychologically “Normal” men, with superior “psychobiological stamina”
Semi-starvation
(lost 25% body weight)

Effects of StarvationEffects of Starvation• Change of Eating Habits
– Started to eat in silence, prolonged time, unusual mixing of food
• Social Changes– Men became withdrawn, decrease wish to socialize,
lack of interest in sex or intimacy – Less humour
• Cognitive Changes– Impaired concentration– Impaired comprehension and judgment

Effects of StarvationEffects of Starvation
• Emotional Changes– Depression– Irritability– Frequent outbursts of anger– Extreme mood swings– Social withdrawal– High levels of anxiety (including nail biting) – Almost 20% experienced extreme emotional
deterioration, even psychosis (some hospitalized) – Most changes persisted through refeeding, became
worse for some

SadnessShameGuiltFearEmptiness
Powerless
FAT
Weight control
Powerful
The Power of an Eating The Power of an Eating Disorder:Disorder:

The Meaning of the Eating DisorderThe Meaning of the Eating Disorder
• The Eating Disorder is one thing I am good at
• Not eating pushes my other worries away
• The Eating Disorder makes me feel powerful, special and in control
• The Eating Disorder means I don’t have to grow up
• Eating means I am weak and a failure
• The Eating disorder is who I am

Medical Complications Medical Complications of Eating Disordersof Eating Disorders
Eating Disorders affect the whole bodyEating Disorders affect the whole body
• Brain, thinking, cognitions• Hair• Dental Disease• Heart• Fluids/ electrolytes• Muscles, bones• Kidneys• GI system• Hormones• Skin
Eating Disorders can..…Eating Disorders can..…
• Result in heart arrhythmias which, in severe cases can be fatal.
• Result in structural brain changes
• Cause osteoporosis (poor bone health)
• Delay puberty
• Stop/ Stunt Growth
• Interfere with pregnancy

Medical Complications of Medical Complications of Eating DisordersEating Disorders
System Starvation Purge
CV Low BP, low HR, small heart, QTc prolongation, cardiac arrest
Arrhythmias (K), cardiac arrest
Metabolic / Heme Hypothermia, Anemia, Leukopenia, poor immunity
Metabolic alkalosis, hypokalemia

Electrocardiograms (EKGs)Electrocardiograms (EKGs)
QTc
• Normal Malnourishment

Medical Complications Medical Complications
System Starvation Purge
Reprod. Amenorrhea, Infertility, complications in pregnancy
Amenorrhea (or oligomenorrhea), infertility
Derm Dry skin and hair, lanugo hair
Russell’s sign, enlarged parotid glands, perioral skin irritation, periocular petechiae
GI Constipation Hematemesis, esophagitis, reflux, poor muscle tone in colon (laxative abuse)
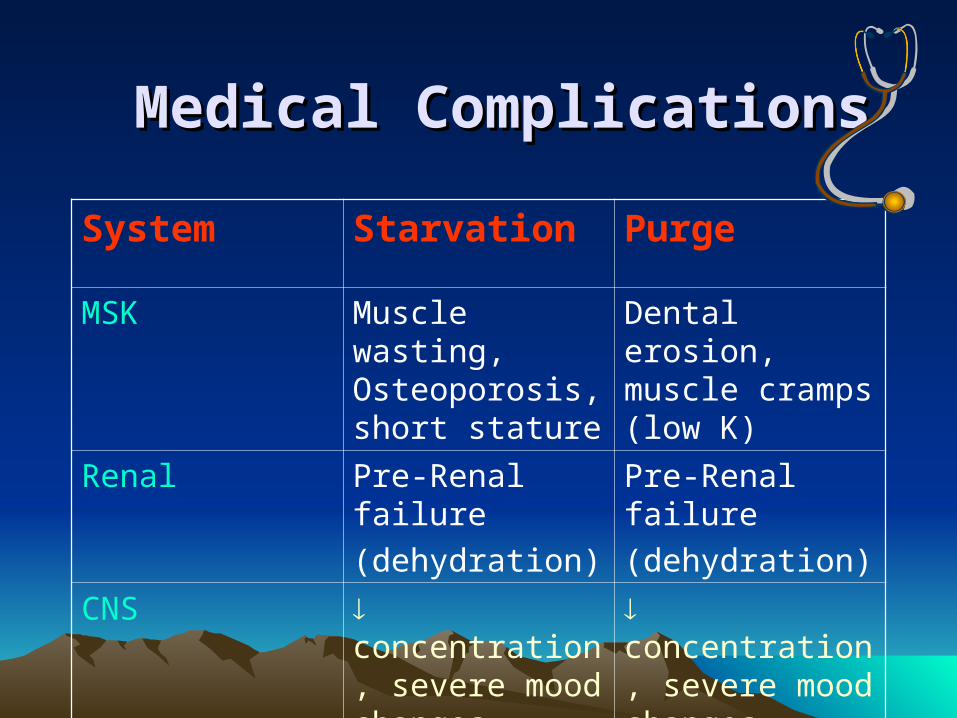
Medical ComplicationsMedical Complications
System Starvation Purge
MSK Muscle wasting, Osteoporosis, short stature
Dental erosion, muscle cramps (low K)
Renal Pre-Renal failure
(dehydration)
Pre-Renal failure
(dehydration)
CNS concentration, severe mood changes, white & gray matter
concentration, severe mood changes
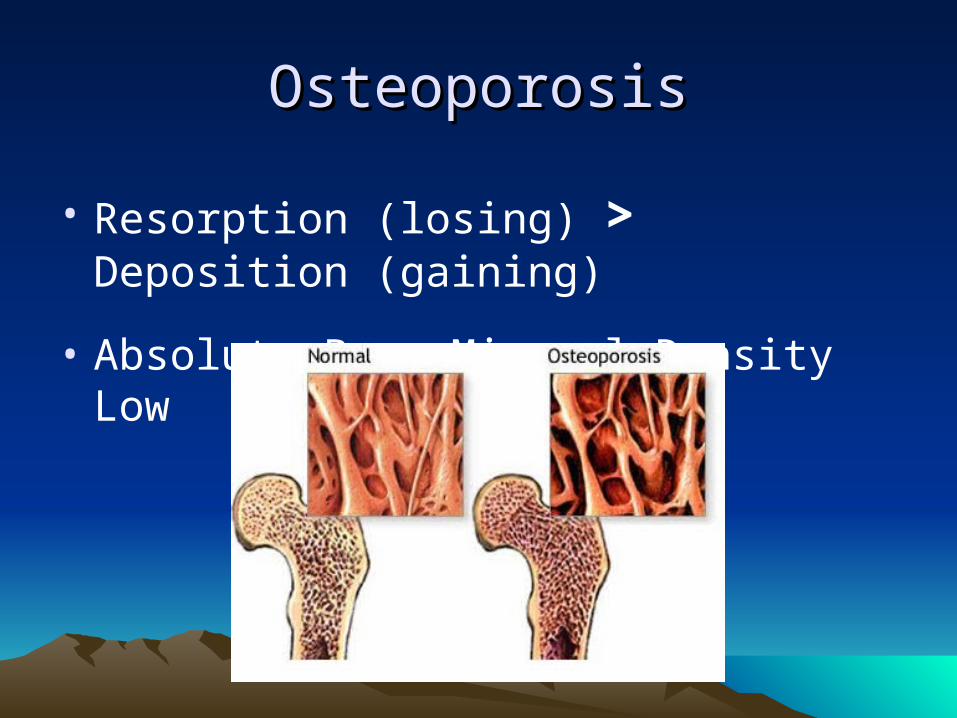
OsteoporosisOsteoporosis
• Resorption (losing) > Deposition (gaining)
• Absolute Bone Mineral Density Low

Structural brain changes MRI FindingsStructural brain changes MRI Findings - - Katzman et al, Katzman et al,
19961996
Adolescent Females ControlsAdolescent Females Controls
14 years14 years 15 years15 years 16 years16 years
Adolescent Females With ANAdolescent Females With AN

Labs in Eating Disorders:Labs in Eating Disorders:
• BUN (dehydration)
• Amylase (vomiting)
• Cholesterol
(starvation)
• Na, K, CL (vomiting/laxatives)
• LH, FSH, estrogen
(starvation)
• RBCs (starvation)
• WBCs (starvation)
• T3

Refeeding SyndromeRefeeding Syndrome
• May occur within 4 days, in severely malnourished pts (<70% IBW)
• During starvation: There is a an intracellular loss of electrolytes, in particular phosphate.
• With feeding, insulin is secreted• This stimulates cellular uptake of
phosphate (and other electrolytes), which can lead to profound hypophosphataemia.

Refeeding SyndromeRefeeding Syndrome
Phosphate < 0.50 mmol/l (normal range 0.85-1.40 mmol/l)– rhabdomyolysis, leukocyte dysfunction,
respiratory failure, cardiac failure, hypotension, arrhythmias, seizures, coma, and sudden death
• Therefore initial feeding must be slow and gradual, with careful medical monitoring, and possible phosphate supplementation

Clinical features of a Patient Clinical features of a Patient at Higher Risk of Deathat Higher Risk of Death
1. Very low weight at admission
2. Bradycardia
3. No medical follow-up
4. Longer duration of illness
5. Multiple purging methods
6. Chronic self-harm or suicide attempts
7. Amphetamine or cocaine use
8. Severe alcohol abuse

Eating Disorders OverviewEating Disorders Overview
• Epidemiology
• Diagnosis
• Understanding Eating Disorders– Etiology, Risk Factors, and Power
• Medical Complications
• Principles of Treatment
• Outcome

Principles of Treatment for Principles of Treatment for Eating DisordersEating Disorders

Key Treatment Principles:Key Treatment Principles:• Specialized, multi-disciplinary team• Meet the medical, nutritional and psychological
needs of the patient • Medical stabilization and renourishment is
necessary but not sufficient• Match severity of illness to intensity of treatment• Structured meals, with goal of normalized eating• Combine psychoeducation with therapy• For adults or adolescent BN: group therapy or
individual therapy• For adolescent AN: Family-based Therapy
AN – Initial AssessmentAN – Initial Assessment
Start with a thorough assessment [I]a. Therapeutic alliance & positive regardb. Biopsychosocial formulation using a non-
blaming modelc. May take several hoursd. Essential involvement of family for children
and adolescentse. Involvement of multidisciplinary team
(dietician, other physicians, social work etc)

AN- Initial assessmentAN- Initial assessment
Choosing a treatment setting Inpatients Day Program (5 days / week, 8 hours day) Outpatients

Treatment of Anorexia Treatment of Anorexia Nervosa:Nervosa:
• Medical and Nutritional:– reversal of the effects of starvation;
re-feeding– “food is the medicine”– meal plan, “mechanical eating” – medical management and weighing– No medication found to be effective;
(recent use of atypical antipsychotics); SSRI’s not effective at low weight

Treatment of A.N. Treatment of A.N. cont’d:cont’d:
• Psychological• Therapeutic Alliance• Supportive, compassionate, empathic• Understanding the illness, education• Externalize the illness, lift blame and
shame, challenging ED• Motivational techniques; exploring pros
and cons, comparing to OCD• Exploring and treating co-morbidities

Treatment of A.N. Treatment of A.N. cont’d:cont’d:
– Family Therapy for Children and Adolescents (evidence based)
– CBT; IPT; motivational therapy; groups

AN - MedicationAN - Medication• SSRI’s / antidepressants
– do not seem to work in context of malnourishment [I]– With weight restoration – treating underlying
comorbidities [I]
• Atypical antipsychotics– Limited evidence (help with obsessionality) [II] – Need to monitor for side effects
• Benzos– May help with anxiety prior to a meal [III]

Treatment of BN - GoalsTreatment of BN - Goals
1. Reduce and if possible eliminate binge
eating and purging
2. Treat physical complications
3. Enhance motivation for Rx
4. Provide education (nutrition & normalized eating)
5. Help pts to reassess & change core dysfunctional thoughts, attitudes, motives, conflicts and feelings related to the ED

Treatment of BN - GoalsTreatment of BN - Goals
6. Treat co-morbid psychiatric conditions, including deficits in mood and impulse regulation, self-esteem and behaviour.
7. Enlist family support and provide counseling & therapy where appropriate.
8. Prevent relapse

NutritionalNutritional
• Structured meal plan [I]– Prevents binges and purges
• Assess nutritional intake for pts with all BMI’s (even “normal”), normal weight does not ensure appropriate intake or body composition [I]
• Nutritional education [I]

PsychologicalPsychological
• CBT: Strong support [I]• IPT: Additional support [II]
(Both individual and group)
• DBT: growing evidence
• Practically, in clinical practice, therapists combine CBT, IPT and other psychodynamic techniques. This combination may better outcomes [II]

PsychologicalPsychological
• Self-help (& professionally guided self-help) programs [I]
• Family therapy for children and youth [II]
• Treatment of co-morbidities, eg. Substance abuse, PTSD…

BN - MedicationBN - Medication
• SSRI: fluoxetine best evidence [I]– Reduces binge eating, purging and psychological
features of ED– Higher doses than needed for MDE (e.g. 60) [I]– Recommend continuing for 9months – 1 year after
symptom-free [II]
• Bupropion: Contraindicated because of seizure risk
Eating Disorders OverviewEating Disorders Overview
• Epidemiology
• Diagnosis
• Understanding Eating Disorders– Etiology, Risk Factors, and Power
• Medical Complications
• Principles of Treatment
• Outcome
Outcome for ANOutcome for AN
• High morbidity and mortality (among highest of all psychiatric illnesses)
• Mortality: 5-20% – 50% suicide– 50% medical complications

Outcome for ANOutcome for AN
• Prognosis in Adolescents:– 50-70% full recovery in 5 years– 10-20% develop chronic AN
• Prognosis in Adults:– 50% “recover”– 25% intermediate outcome– 25% poor outcome

Outcome for B.N.Outcome for B.N.
• Better treatment outcomes compared to A.N.
• Up to 70% recover with treatment
• 15-20% intermediate outcome
• 10-15% continue to do poorly

A.N. A.N. B.N. B.N.
• 50% of AN-R develop bulimic symptoms
within 5 years of weight recovery
• (Crossover from B.N. A.N. is rare)

Outcome cont’d (A.N. and Outcome cont’d (A.N. and B.N.)B.N.)
• Higher rates of Major Depression
• Higher rates of Anxiety (esp. OCD and GAD)
• Higher rates of Substance Abuse for those with history of B.N.

Outcome cont’d:Outcome cont’d:
• Better prognosis associated with:– onset (and treatment) before age 15 yrs– treatment within 3 years of onset of illness– weight recovery within 2 years of treatment
• Worse Prognosis associated with:– later age of onset, longer duration of illness,
previous hospitalizations, greater individual and family disturbance

www. nedic.ca

ReferencesReferences• APA Guidelines, Practice Guideline for the
Treatment of Patients with Eating Disorders, Third Edition, 2006
http://www.psychiatryonline.com/pracGuide/pracGuideTopic_12.aspx
• NICE Guidelines, Eating Disorders, Core interventions in the treatment and management of anorexia nervosa, bulimia nervosa and related eating disorders, January 2004
http://guidance.nice.org.uk/CG9

ReferencesReferences
• Review of Outcome Research in Eating Disorders, International Journal of Eating Disorders, 40:4, May 2007. (Entire journal)
• Klump K et al, Academy for Eating Disorders Position Paper: Eating Disorders are Serious Mental Illnesses, International Journal of Eating Disorders, 42:2, p97-103, 2009.
• Le Grange D et al, Academy for Eating Disorders Position Paper: The Role of the Family in Eating Disorders, International Journal of Eating Disorders, 43:1, p1-5, 2010.
• Rosen, David, Identification and Management of Eating Disorders in Children and Adolescents, Pediatrics, Vol. 126 No. 6 December 2010, pp. 1240-1253

1. What is the prevalence of Anorexia Nervosa in women?
a. 0.1 – 0.2%b. 0.5-1%c. 5%
2. To have a diagnosis of Bulimia Nervosa, the compensatory behaviour must include vomiting.
a. Trueb. False

3. First line treatment for Anorexia Nervosa in the weight restoration phase is:
a. an SSRIb. an appetite stimulant
c. none of the above
4. First line treatment for Bulimia Nervosa includes:
a. an SSRIb. CBTc. all of the above


















