East London Foundation Trust Our WRES story · ELFT Workforce profile •BME representation by...
40
East London Foundation Trust Our WRES story Sandi Drewett Director of Human Resources and Organisation Development
Transcript of East London Foundation Trust Our WRES story · ELFT Workforce profile •BME representation by...

East London Foundation Trust
Our WRES story
Sandi Drewett
Director of Human Resources and
Organisation Development
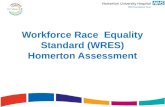
Mental health services Newham, Tower Hamlets, City & Hackney, Luton &
Bedford
Forensic services All above & Waltham Forest, Redbridge, Barking &
Dagenham, Havering
Child & Adolescent services, including tier 4
inpatient service
Regional Mother & Baby unit
Community health services Newham
IAPT Newham, Richmond and Luton
Speech & Language Barnet
Why it’s important
• Diverse teams, inclusively led, produce better
outcomes than homogenous teams (or
diverse teams not inclusively led)
• Particularly relevant to healthcare, where
team performance depends significantly on
sharing of information

Our Journey
6
• It is typical of an NHS Trust to
collate Data but not do anything
strategic with it.
Use data to
drive
Organizational
and
cultural
change
Improving
data
Collection
and
data
quality
Historically
basic
data
collection
Understand
and
triangulate
data
Analyze and
feedback
data
• Collection of qualitative data by
different means. Improved use
of ESR and other systems.
• Data cleansing exercises and
better use of systems.
• Staff Survey, FFT surveys and
focus groups. Monitoring in
terms of consistency between
localities.
• Frequent reports to SDB,
Board, Workforce Committee
etc.
• Triangulate between data
collection methods i.e. Staff
Survey, FFT surveys,
Disciplinarys, Grievances, Exit
interviews and performance
dashboards.
• To improve, recruitment and
selection, reduce the number of
formal process to cascade data
to decision makers. Thinking
Space Training (Unconscious
Bias)
• Lessons learned following ET
cases
• Service users involved in every
part
• Learning is the focus and not
blame.

It’s important to create a culture in
which staff are more valued. The
staff that feel most undervalued and
least rewarded section of the NHS
workforce – its BME staff – not least
since the evidence is that their
treatment is a good predictor of the
quality of patient care.
At a time when there appears to be
a consensus on the 5
benefits of diversity for all those
receiving health services there can
be no better time to change, once
and for all, the “snowy peaks” of the
NHS.
‘Employee engagement
emerges as the best
predictor of NHS trust
outcomes. No combination
of key scores or single
scale is as effective in
predicting trust performance
on a range of outcomes
measures as is the scale
measure of employee
engagement’
Professor Michael West
Staff Engagement We don’t have the
head start that others
do. It’s not a level
playing field. But we’re
just as talented. All we
need is a bit of help to
unleash our potential.
Sadiq Khan, Mayor
London

The quality culture we want to nurture
A listening and learning organisation
Empowering staff to drive improvement
Increasing transparency and
openness
Re-balancing quality control, assurance and improvement
Patients, carers and families at the heart of all
we do

Staff feedback
Our practice
• Clinically led organisation
• Invested focus on learning and development
programmes for every level and group of staff
– Reflective practice the norm for clinicians
• Focus on learning from what’s going well
• Long term approach to workforce planning with
universities
• QI projects – targeting underlying issues in a
sustained way
• Networks and mentoring
r
Our approach to Quality
Improvement (QI)
• Improvement action to focus on
issues most relevant to staff
satisfaction
• Link with existing work
streams/quality improvement
project where appropriate
• Further work to identify causes of
issues/success identified; in-year
surveys to be launched
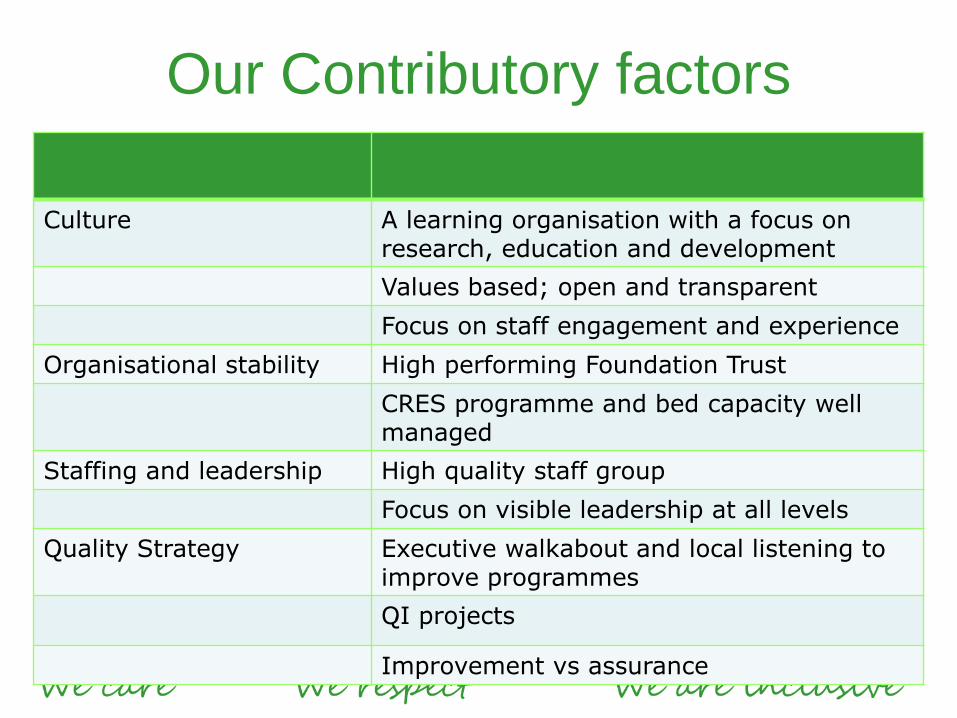
Our Contributory factors
Culture
A learning organisation with a focus on research, education and development
Values based; open and transparent
Focus on staff engagement and experience
Organisational stability High performing Foundation Trust
CRES programme and bed capacity well managed
Staffing and leadership High quality staff group
Focus on visible leadership at all levels
Quality Strategy Executive walkabout and local listening to improve programmes
QI projects
Improvement vs assurance
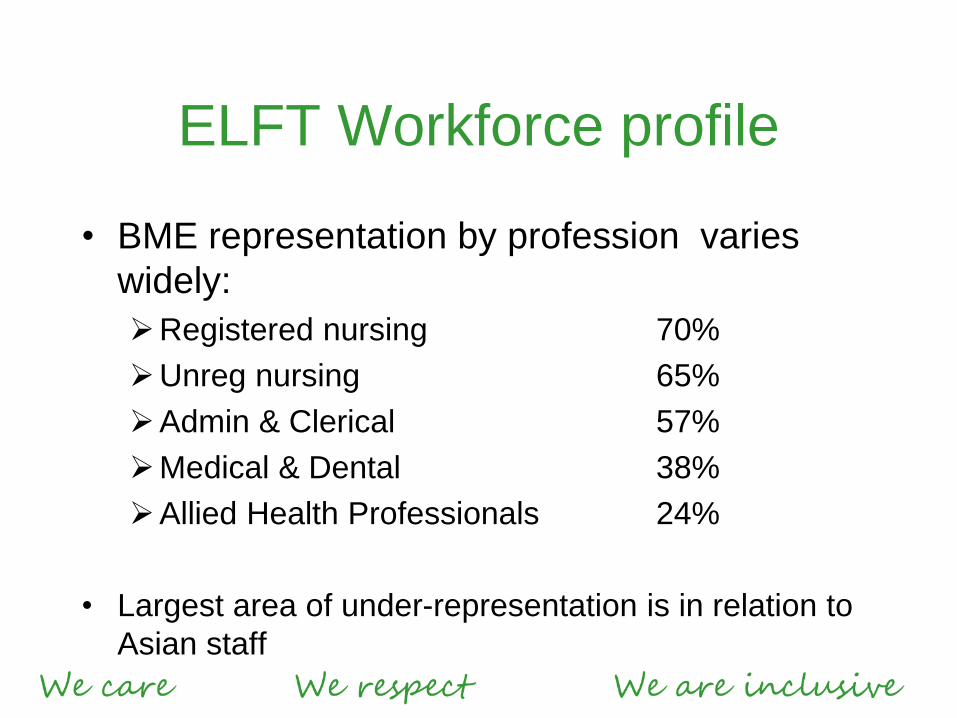
ELFT Workforce profile
• BME representation by profession varies
widely:
Registered nursing 70%
Unreg nursing 65%
Admin & Clerical 57%
Medical & Dental 38%
Allied Health Professionals 24%
• Largest area of under-representation is in relation to
Asian staff
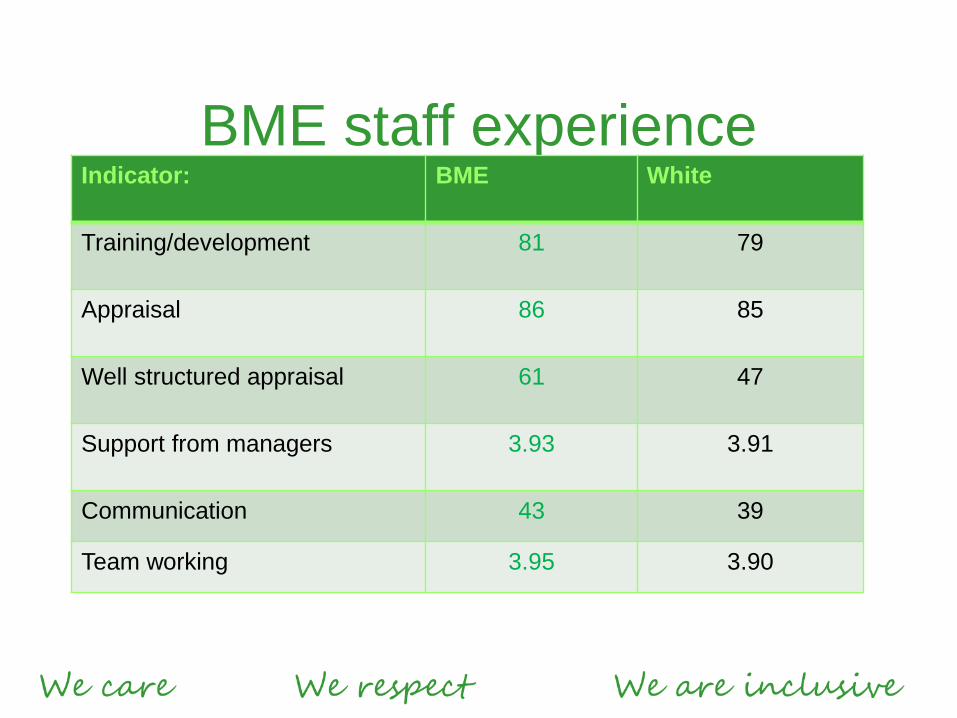
BME staff experience Indicator: BME White
Training/development 81 79
Appraisal 86 85
Well structured appraisal 61 47
Support from managers 3.93 3.91
Communication 43 39
Team working 3.95 3.90
9 November 2016 East London NHS Foundation Trust Page 24
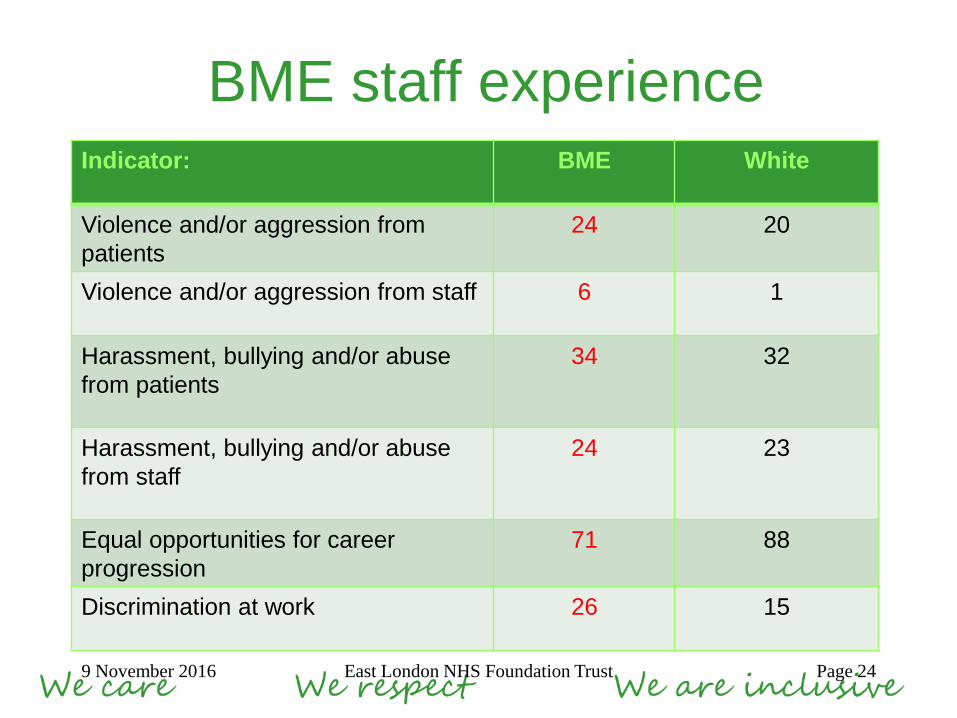
BME staff experience Indicator: BME White
Violence and/or aggression from
patients
24 20
Violence and/or aggression from staff 6 1
Harassment, bullying and/or abuse
from patients
34 32
Harassment, bullying and/or abuse
from staff
24 23
Equal opportunities for career
progression
71 88
Discrimination at work 26 15
WRES Indicators


WRES Indicators 2015
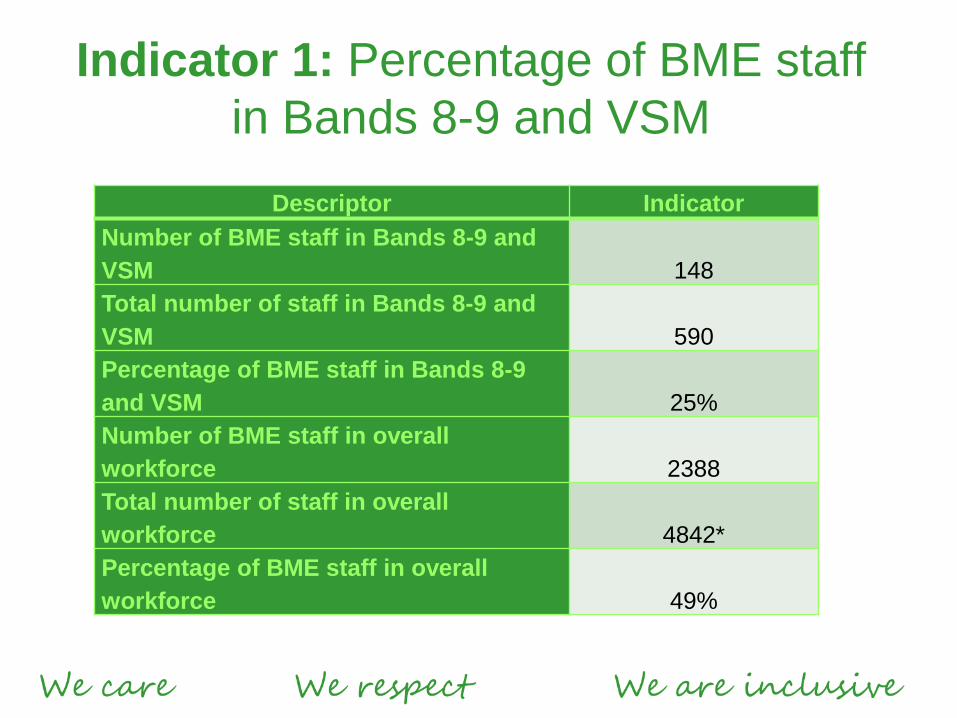
Indicator 1: Percentage of BME staff
in Bands 8-9 and VSM
Descriptor Indicator
Number of BME staff in Bands 8-9 and
VSM 148
Total number of staff in Bands 8-9 and
VSM 590
Percentage of BME staff in Bands 8-9
and VSM 25%
Number of BME staff in overall
workforce 2388
Total number of staff in overall
workforce 4842*
Percentage of BME staff in overall
workforce 49%
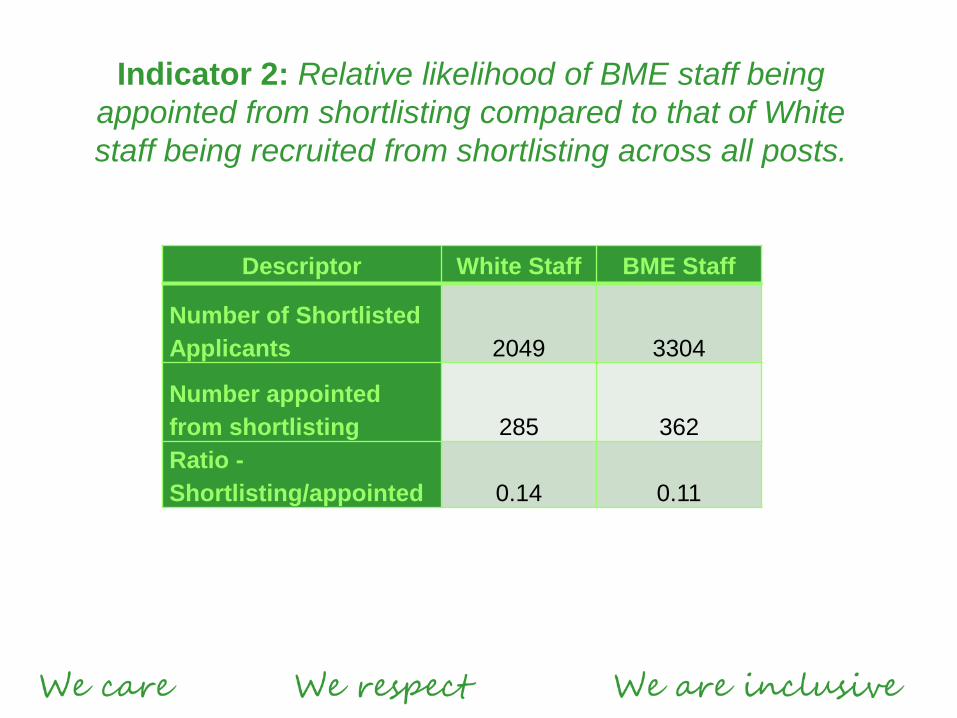
Descriptor White Staff BME Staff
Number of Shortlisted
Applicants 2049 3304
Number appointed
from shortlisting 285 362
Ratio -
Shortlisting/appointed 0.14 0.11
Indicator 2: Relative likelihood of BME staff being
appointed from shortlisting compared to that of White
staff being recruited from shortlisting across all posts.
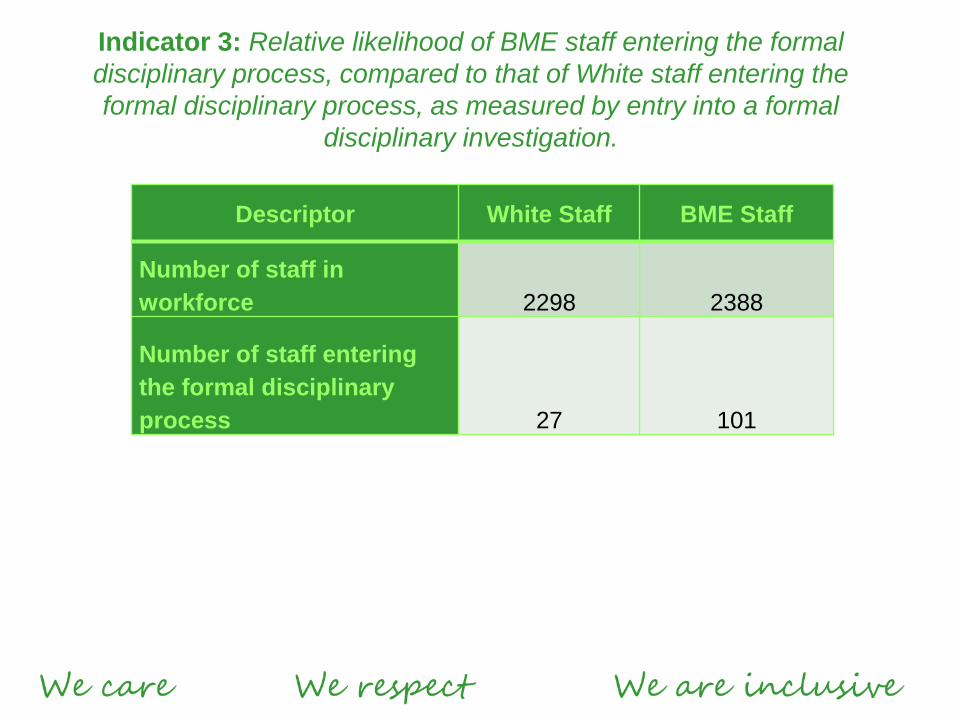
Descriptor White Staff BME Staff
Number of staff in
workforce 2298 2388
Number of staff entering
the formal disciplinary
process 27 101
Indicator 3: Relative likelihood of BME staff entering the formal
disciplinary process, compared to that of White staff entering the
formal disciplinary process, as measured by entry into a formal
disciplinary investigation.
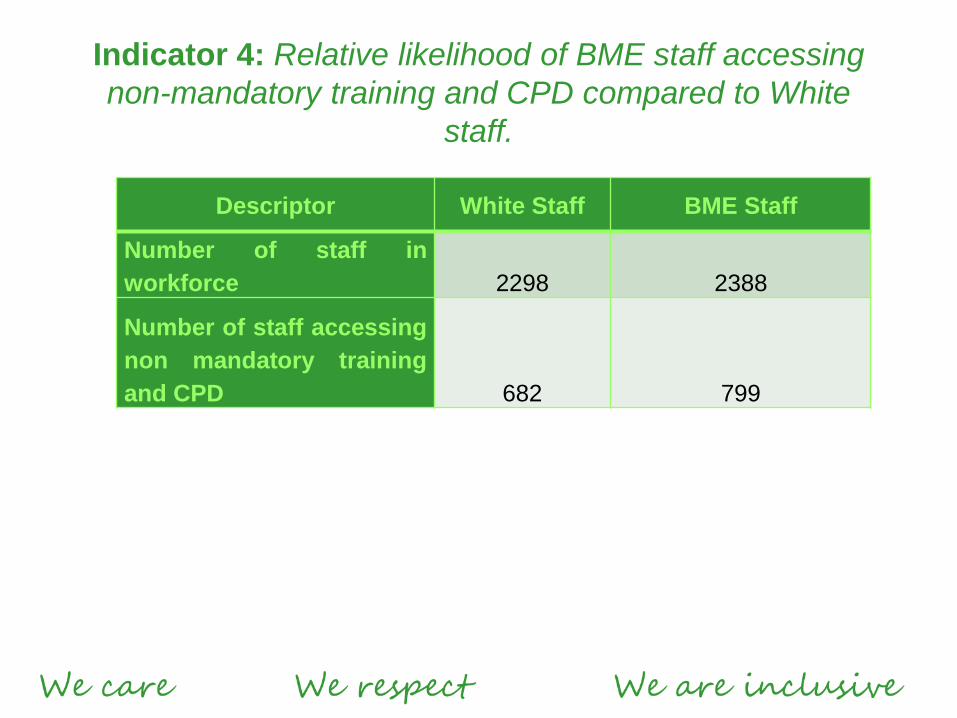
Indicator 4: Relative likelihood of BME staff accessing
non-mandatory training and CPD compared to White
staff.
Descriptor White Staff BME Staff
Number of staff in
workforce 2298 2388
Number of staff accessing
non mandatory training
and CPD 682 799
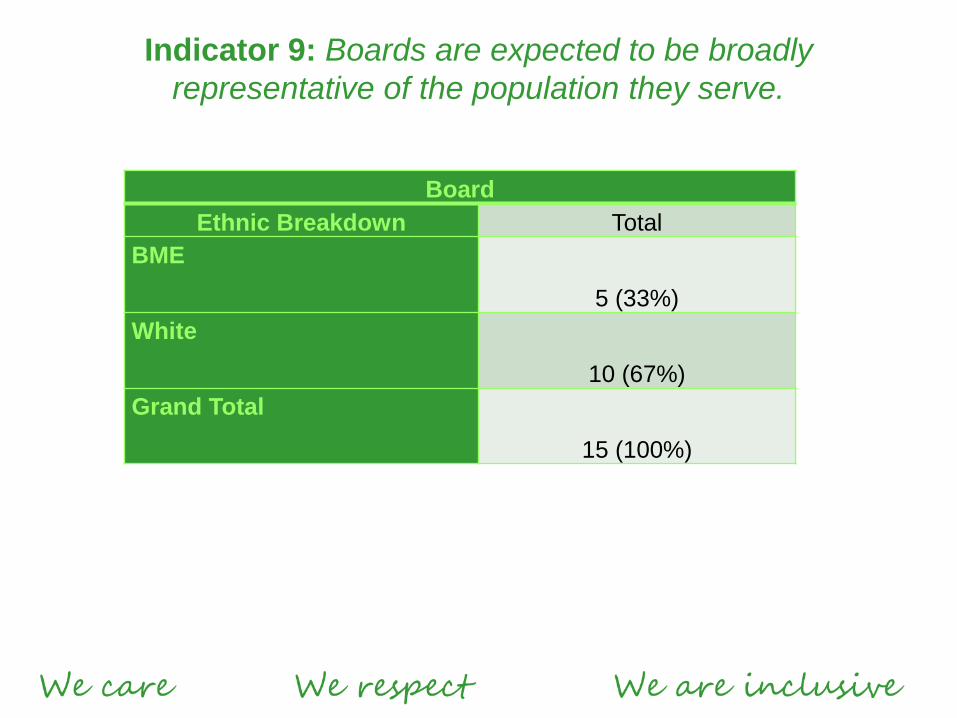
Indicator 9: Boards are expected to be broadly
representative of the population they serve.
Board
Ethnic Breakdown Total
BME
5 (33%)
White
10 (67%)
Grand Total
15 (100%)

Process of cultural change
OUTPUTS
• Staff who drive improvement
and change
• Staff feel comfortable to raise
concerns and challenge poor
practice
• Staff are empowered and
have a voice
• Effective partnership working
with Trade Unions
• Staff see the impact of Senior
involvement
• An ability to discuss issues
• Increased engagement
scores
• Proportionate and consistent
outcomes in terms of ER
cases
• Positive messaging about raising concerns
• Cultural change
• Staff Engagement
• Acknowledgement of organisational issues
• Communicating organisational Issues
• Mechanism for managing issues (QI)
• Value staff
INPUTS
Key messaging from the top of the
organisation
Equality forums lead by Exec
Directors
QI initiatives more widely
Key input from front line staff
through QI initiatives
Openness and willingness to
discuss difficult subjects such as
race and race inequality
Commitment to address these
issues at senior levels in the
organisation
What we are doing
• Governance:
– Equalities strategy agreed by Trust Board
– Implementation group meeting monthly
– Internal audit and CQC review
• Listening and learning:
– Staff networks and forums
– Staff surveys
• Culture:
– Senior leadership of staff networks, conferences etc.
– Leadership culture programme - with Kings Fund/NHSI
– Quality culture -10 Quality Improvement projects focusing on reducing
levels of violence & aggression
What we are doing
• Initiatives:
– Recruitment – branding, values based, service user on panel
– Developing a performance framework
– Increased range of development courses and opportunities
(i.e. bands 5-7 management development)
– Mentoring – reverse and BME
– Team reflective practice
– Unconscious bias training
– QI projects: BME career progression, Disciplinary Process
Achievements
• Most diverse workforce in the NHS
• Most diverse Board; only BME chair in London and
only BME Chair/CEO team in the NHS
• BME staff more positive than white staff in majority of
staff survey indicators
• Progress in reducing levels of violence, aggression,
bullying/harassment and discrimination
• One of a few Trusts to have positive Workforce Race
Equality Standards indicators
• Most improved NHS trust – Stonewall rankings
• Increasingly recognised as a leader in this area
Areas for improvement
• The numbers of BME staff disciplined is
disproportionately higher than White staff
• Women, BME and disabled staff are significantly less
positive about the fairness of career progression in
the Trust
• The percentage of staff in BME groups in Bands 8a
to VSM is disproportionately lower than the number
of white staff
• High levels of reported bullying, harassment and
abuse (25% of staff)
• LGBT - stigma, lack of data
Disciplinaries
• Evaluation of three years of cases carried out
• Main findings:
– Some (but not all) disparity driven by the role - i.e.
band 3 and band 5 inpatient nursing staff most
likely to be subject to disciplinaries
– Most disparity relates to Black staff
– Large proportion of cases (25%) not upheld at
hearing
– Significant proportion of cases initiated by
allegations by patients. Staff often suspended for
long periods
Disciplinaries
• Actions: – Increased use of informal resolution; performance framework
being developed
– Nursing staff have developed better local induction
programmes for staff
– Fair Treatment Panel to review all disciplinary cases to
check that they are appropriate for formal hearing, or
whether alternative methods should be used
– Full-time investigator to investigate all cases where staff
subject to suspension
Career progression
• Low scores prevalent in following occupational groups:
– Administration
– Healthcare assistants
– Age 51+
– Women, disabled and BME staff
• Some correlation with quality of line management (women,
disabled staff)
• Directorate scores suggest that organisational change has an
impact
• Generally good access to formal development opportunities
• Increased range of development courses and opportunities (i.e.
bands 5-7 management development)
• Impact of secondment and acting-up processes
Career progression
• Actions:
– Admin and nursing development programmes
– Secondments now advertised in line with permanent roles
– BME mentoring and reverse mentoring programmes
– Admin conference to focus on career progression
– Celebration of BME leadership stories
– QI project – BME rep on recruitment panels
– Review of career paths for each profession
Bullying, harassment and
abuse • Context:
– 73% of reported BH&A occurred 1-2 times in the last year
– Workforce composition – 70% female, 19% disability, 18%
BME
– Hierarchy/Targets/regulation - The Chief Executives Tale,
864 lines of reporting
– Safety critical environment
– Conflict - 33% of staff in the last year report bullying,
harassment or abuse from patients/public
– Constant organisational change
– Wellbeing – 38% suffered work related stress in the past
year
What contributes to bullying
at work? • Bullying is not primarily a problem of interpersonal differences
• Even though bullying plays out during interactions between
individuals, features of jobs and factors in the work environment
are the primary determinants
• Stressful working conditions (role stressors, low control) are
associated with greater exposure to bullying
• Overall, workplace bullying reflects the functioning of the
organisational system
• Current actions focus on an individual level, but we also need to
work on the organisational risk conditions (supervision,
performance management, organisational change etc.), and the
wider system prevention (role and goal clarity, reduce amount of
change, reduce conflict, increase support etc.)
Headlines 18th October 2016
• Hospitals to be named and shamed on agency spending
• The NHS is to publish the names of hospitals that spend too much on agency staff, as well as the incomes of the
highest-earning temporary staff, writes the Times £. The decision to name and shame has been made as the NHS
still spends £250m a month on locums and stand-in staff, despite a cap on hourly rates being imposed almost a year
ago. Jim Mackey, chief executive of NHS Improvement, said: “The NHS simply doesn’t have the money to keep
forking out for hugely expensive agency staff. With hospitals across England struggling with patient demand, trusts
need all the support they can get and trying to cash in on the NHS just isn’t on.” Anthea Mowat, of the British Medical
Association, said: “The measures are nothing but a sticking plaster – naming and shaming trusts or individuals will
not address the underlying issues causing and overreliance on agency workers.”
• Regulators place more trusts in financial special measures
• HSJ £ reports that regulators have placed three more NHS trusts in financial special measures. East Sussex
Healthcare NHS Trust, Gloucestershire Hospitals NHS Foundation Trust, and Brighton and Sussex University
Hospitals NHS Trust have been placed in the regime by NHS Improvement. Chief executive of the regulator, Jim
Mackey, said the three providers going into financial special measures are “causing significant concern”. He added:
“They’ve agreed savings targets locally but are a long way from meeting them…The financial performance of these
three trusts has simply not been good enough and so we’re sending in some targeted support to identify what the
problem is, and help them fix it.” Mackey said £100m of potential extra savings have been identified at the five trusts
already in financial special measures from when it was introduced in July.
• Mental health trust criticised over killings by patients
• The BBC reports that a review has found a mental health trust underestimated the risk posed by its patients and
sometimes did not act on threats to kill. The review examined 10 deaths linked to Sussex Partnership NHS
Foundation Trust patients between 2007 and 2015. It found killings by two of the patients had been “preventable” and
“predictable”. The independent review was commissioned by the trust and NHS England in 2015, and looked at nine
killings committed by patients of the trust and the case of one patient who was killed while under the care of the
trust.
•
Evidenced based strategic
framework for success • Core leadership support that articulates
diversity as a high organisational priority
• Multiple strategies at organisational,
workplace, interpersonal and intrapersonal
levels used simultaneously over a long period
• Mandated targets or actions
Closing remarks • Start where you are
• Look at borough population
• Triangulate your data
• Don’t look at discrimination in isolation
• Where are the bright spots in your community?
• Have the conversation – name the issue
• Senior engagement is key
• Not just about a diverse workforce
• Focus on drivers of experience
• Feedback
• Set yourself some clear actions and measure them
Questions
Your turn
• What’s working well in your trust?
• What have you learned and would want
to share?
Thank you