
Early Mobilization in the ICU - NYSPFP · Ralph Carumba, MS, RN, CCRN Jodi Herbsman, MS, PT, DPT ....
29
EARLY MOBILIZATION IN THE ICU Ralph Carumba, MS, RN, CCRN Jodi Herbsman, MS, PT, DPT
Transcript of Early Mobilization in the ICU - NYSPFP · Ralph Carumba, MS, RN, CCRN Jodi Herbsman, MS, PT, DPT ....

EARLY MOBILIZATION IN THE ICURalph Carumba, MS, RN, CCRNJodi Herbsman, MS, PT, DPT

About NYU Langone Hospital (Tisch)• Academic Medical Center• 705-Bed Acute-Care Tertiary Facility
• 18 Medical ICU Beds
• 9 Surgical ICU Beds• Magnet® Recognized (3 times consecutively)
• Rusk Rehabilitation ranked #8 in US News and World Report (#1 in New York State)
2

Objectives• Define the ABCDEF Bundle and how it was implemented and NYULHC• Describe how to initiate an early mobilization program
• Share the results of effective early mobilization programs in the adult and pediatric ICUs at NYULHC
• Review strategies for sustainability of a program• Discuss challenges and successes with implementing an early mobility program
3

What is Early Mobilization?• The proactive provision of physical therapy to
critically ill patients on ICUs. Includes:– sitting on edge of the bed
– sitting on chair
– Ambulating(Fraser, Spiva, Forman, & Hallen, 2015)
• “Early” defined as “the interval starting with initial physiologic stabilization and continuing through the ICU stay” (Fraser, Spiva, Forman, & Hallen, 2015)
• In practice, early mobility programs can be difficult to implement given the complexity of safely mobilizing a patient while still on a ventilator. (Klompas, 2015)
4

Early Mobilization and Ventilator Associated Events• Immobility is associated with atelectasis and pneumonia• Early physical and/or occupational therapy
– Can decrease time on the ventilator
– Reduce risk of acute delirium
– Has been associated with lower rates of complications and Ventilator Associated Pneumonia(Cocoros & Klompas, 2016)
5

The “ABCDEF(+G)” Bundle
6

ICU Checklist • Helps to ensure standard
ICU needs are addressed for each patient
• Designed to promote discussion on different matters of care
• Utilized with morning and evening rounds
7

Safe Patient Handling • Each room in MICU & SICU equipped with
ceiling lift devices
• Utilized to assist patients with repositioning, transferring between chair/bed, and mobilization
• Used by RN, PT/OT
8

Starting an Early Mobilization Program• Leadership support • Business plan
• Forming a team
9

10

Interventions Summary• Increased staffing and intensity of service based on business proposal (Adult)
• Interdisciplinary team mobilized (Adult and Peds)
• PICU admission order set updated (Adult and Peds)
• Algorithm created (Peds)
• Patient scheduling (Adult and Peds)
• Therapy/Nursing education and training provided (Adult and Peds)
• Family advisor interviews conducted with patients and caregivers (Peds)
• Family advisor/nursing discussions conducted (Peds)
11

Early Mobilization:Contraindications, Precautions, and Signs of Intolerance
12

Start/End Points
Process
Decision Point Sub-process
Legend
13
14

PICU Patients Mobilized Within Established Time Frame
Scheduling of patients for therapies initiated 4/11/16
Family advisor discussions with families initiated 6/2/16
Mobilization training initiatedfor nursing staff 6/6/16
PICU Admission Order Set Updated to include activity
orders 11/19/15
Algorithm Finalized 2/25/16
Initiated late shift for PT/OT 3 days a week to increase POD#0 coverage 11/1/16
0
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%%
of P
atie
nts
Mob
ilize
d w
ithin
Est
ablis
hed
Tim
e Fr
ame
Week Ending Date% of Patients Who Met the Desired Clinical Outcome Median Goal
Des
ired
Dire
ctio
n
15

Time From PICU Admission to First Mobilization
0
5
10
15
20
25
30
35
40
45
50
55
60
Wee
kly
Aver
age
(in H
ours
)
Date
Daily Average Hours Centerline Control Limits
Desired
Direction
16

Outcomes (PICU)
20%
82%76%
12%
60%
89% 91% 91%
52%
85%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Activity Orders PT Orders OT Orders SLP Orders % Patients Mobilizedwithin recommended time
frame
Perc
ent o
f Pat
ient
s
PRE (N=51) POST (N=46)
17

Barriers to Mobilizing Non-Vented Patients (PICU)
18

Barriers to Mobilizing Vented Patients (PICU)
19

Greatest Concerns About Mobilizing Patients (PICU)
20

Key Components of Sustainability• Supportive management structure• Change structure (to prevent “slip back”)
• Robust, transparent feedback system
• Shared sense of the system to be improved• Culture of improvement
• Engaged staff
• Formal capacity to build programs
(Institute for Healthcare Improvement, n.d.)
21

Implementation/Sustain Plan
Activity Status
Identify process owner/create transition plan
PT Supervisor with assistance from project manager.
Monitor performance/data collection
Currently on paper, collected daily. Long-term goal to transition to using reports from EHR.
Standards and procedures Still in process of being hardwired. Education to continue.
Training On-going
Transition Plan Goal is unit/therapy leadership to integrate early mobility into daily care treatment. Transition near completion.
22

Challenges• Coordination of the mobilization team in real-time
• Coordination of training
• Changing culture is gradual
• Time and resources
• Documentation consistency
• Sustainability
23

Successes/Wins• Strong team collaboration (including family advisors)
• Positive feedback from patients and families
• Improved clinical care
• Cost saving
• No adverse events
24

25
Questions?

References• Bailey, P., Thomsen, G.E., Spuhler, V.J., et al, Early activity is feasible and safe in respiratory failure patients. Crit Care Med
2007; 35:139-145.
• Balas M.C., Vasilevskis E.E., Olsen K.M., Schmid K.K., Shostrom V., Cohen M.Z., … Burke W.J. Effectiveness and safety of the awakening and breathing coordination, delirium monitoring/management, and early exercise/mobility bundle. Crit Care Med. 2014 May;42(5):1024-36.
• Brahmbhatt, N., Murugan, R., Milbrandt, E.B. Early mobilization improves functional outcomes in critically ill patients. Crit Care2010; 14:321.
• Choong K, Chanci F, Clark H, et al. Practice recommendations for early mobilization in critically ill children. J Pediatr Intensive Care 2017; Efirst.
• Cocoros, N., Klompas, M. Infect Dis Clin N Am 30 (2016) 887–908.
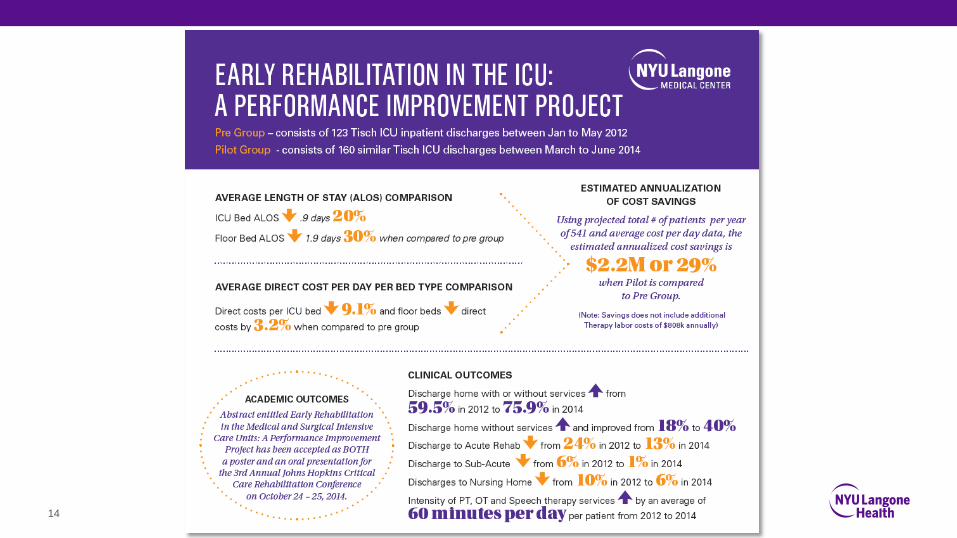
• Corcoran JR, Herbsman JM, Bushnik T, et al. Early rehabilitation in the medical and surgical intensive care units for patients with and without mechanical ventilation: An interprofessional performance improvement project. PM R 2016; 1-7.
• Dowdy, D.W., Eid, M.P., Sedrakyan, A. et al, Quality of life in adult survivors of critical illness: a systematic review of the literature. Intensive Care Med 2005; 31:611-620.
• Fraser, D., Spiva, L., Forman, W., Hallen, C. Original research: Implementation of an early mobility program in an ICU. AJN. 2015; 115(12)
26

References (cont.)
• Herridge, M.S., Tansey, C.M., Matte, A., et al, Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med 2011; 364:1293-1304.
• Hodgson, C.L., Stiller, K., Needham, D.M., et al, Expert consensus and recommendations on safety criteria for active mobilization of mechanically ventilated critically ill adults. Crit Care 2014; 18:658.
• Hopkins RO, Choong K, Zebuhr CA, et al. Transforming PICU culture to facilitate early rehabilitation. J Pediatr Intensive Care.2015;4: 204-211.
• Institute for Healthcare Improvement. How-to guide: Sustainability and spread. http://www.ihi.org/resources/Pages/Tools/HowtoGuideSustainabilitySpread.aspx. Accessed August 20, 2017.
• Kahn, J.M., Rubenfeld, G.D., Rohrbach, J., et al, Cost savings attributable to reductions in intensive care unit length of stay for mechanically ventilated patients. Med Care 2008; 46:1226-1233.
• Kayambu, G., Boots, R., Paratz, J. Physical Therapy for the Critically Ill in the ICU: A Systematic Review and Meta-Analysis. CritCare Med 2013; 41:1543-1554.
• Korupolu, R., Zanni, J.M., et al, Early physical medicine and rehabilitation for patients with acute respiratory failure: a quality improvement project. Arch Phys Med Rehabil 2010; 91:536-542.
• Kress, J.P., Hall, J.B. ICU-acquired weakness and recovery from critical illness. N Engl J Med 2014; 370:1626-1635.
27

References (cont.)
• Lord, R.K., Mayhew, C.R., Korupolu, R., et al, ICU early physical rehabilitation programs: financial modeling of cost savings. CritCare Med 2013; 41:717-724.
• Morandi, A., Brummel, N.E., Ely, E.W. Sedation, delirium and mechanical ventilation: the 'ABCDE' approach. Curr Opin Crit Care2011; 17:43-49.
• Morris, P.E., Goad, A., Thompson, C., et al, Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med 2008; 36:2238-2243.
• Needham, DKayambu, G., Boots, R., Paratz, J. Physical Therapy for the Critically Ill in the ICU: A Systematic Review and Meta-Analysis. Crit Care Med 2013; 41:1543-1554.
• Oeyen, S.G., Vandijck, D.M., Benoit, D.D., et al, Quality of life after intensive care: a systematic review of the literature. Crit Care Med 2010; 38:2386-2400.
• Schweickert, W.D., Pohlman, M.C., Pohlman, A.S., et al, Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. Lancet 2009; 373;1874-1882Sukantarat, K., Greer, S., Brett, S., et al, Physical and psychological sequelae of critical illness. Br J Health Psychol 2007; 12:65-74.
• Thomsen, G.E., Snow, G.L., Rodriguez, L., et al, Patients with respiratory failure increase ambulation after transfer to an intensive care unit where early activity is a priority. Crit Care Med 2008; 36:1119-1124.
• Truong, A.D., Fan, E., Brower, R.G., et al, Bench-to-bedside review: mobilizing patients in the intensive care unit--from pathophysiology to clinical trials. Crit Care 2009; 13:216.
28

THANK YOU








![Implementing Hospital Policies & Protocols - NYSPFP Hospital Policies & Protocols Jane Jeffrie Seley DNP MPH GNP BC-ADM CDE CDTC FAADE FAAN. ... • * Use D5NS if corrected [Na+] 140](https://static.fdocuments.net/doc/165x107/5ae105957f8b9ac0428e2dd4/implementing-hospital-policies-protocols-nyspfp-hospital-policies-protocols-jane.jpg)








![DIVISION OF NURSING - NYSPFP · 2016-12-16 · Division of Nursing response to “Access”: • The right patient [the patient is appropriately admitted for necessary care needs]](https://static.fdocuments.net/doc/165x107/5f0dd5fc7e708231d43c5378/division-of-nursing-nyspfp-2016-12-16-division-of-nursing-response-to-aoeaccessa.jpg)
