Early Childhood Caries in Cambodia - Minerva Access
184
i Early Childhood Caries in Cambodia Bathsheba Turton BDS MComDent (Otago) A thesis submitted in total fulfilment of the requirements for the degree of Doctor of Philosophy 21 September 2018 Melbourne Dental School, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne.
Transcript of Early Childhood Caries in Cambodia - Minerva Access

i
Early Childhood Caries in Cambodia
Bathsheba Turton BDS MComDent (Otago)
A thesis submitted in total fulfilment of the requirements for the degree of
Doctor of Philosophy
21 September 2018
Melbourne Dental School,
Faculty of Medicine, Dentistry and Health Sciences,
The University of Melbourne.

ii
Abstract
Children in Cambodia have a severe burden of caries and data from the Cambodian national
oral health survey reflect that four in five 6-year-old children have one or more pulpally
involved teeth. One of the key features of dental caries in Cambodia is that most of the lesions
go untreated and most of the dental services are orientated towards those in an urban setting
and involve management of pain only. Global evidence on prevention of dental caries suggests
that interventions focusing on topical application of fluorides in the form of toothpastes or
varnishes and application of pit and fissure sealants (FS) might be the most effective
interventions for reducing caries experience.
Two groups of investigations were conducted; the first group of investigations were part of the
SEAL Cambodia project and the second group were part of the Cambodia Smile Project. The
aims of the SEAL Cambodia project were to evaluate two different protocols for the placement
of glass ionomer cement-based fissure sealants and the prevention of dental caries in the FPM
of 6 to 8 year old children in three provinces of Cambodia, then to investigate the caries
preventive effect of a refined protocol for GIC fissure protection in FPM of 6 to 8 year-old
children in Cambodia. The Cambodia Smile investigation aimed to describe the
epidemiological aspects of Early Childhood Caries in a Cambodian context, then investigate
the effectiveness of a pilot strategy for the reduction of dental caries experience in Cambodian
preschool children through an integrated primary health care model.
The original SEAL Cambodia project rendered a non-significant 10% preventive fraction for
new carious lesions on first permanent molars after 1-year. The modified protocol rendered a
90% preventive fraction at 1-year and 30% preventive fraction at 2-years.
The Cambodia Smile results affirmed existing evidence that Early Childhood Caries (ECC)
affected a large proportion of young children and that a package of oral health interventions
integrated with the routine vaccination schedule can render a 66% reduction in the severity of
dental caries among 2-year-old children.
This collection of studies represents the first efforts to build evidence around the reorientation
of dental services towards preventive therapies in a Cambodian context. Further investigation
is needed to better understand the social, structural and behavioural aspects of the ECC
phenomenon in Cambodia in order to better inform strategy. The SEAL Cambodia project
provides sufficient evidence for an appropriate clinical protocol for the application of FS in a

iii
Cambodian context. The Cambodia Smile pilot provides sufficient evidence to justify up-scale
and monitoring of a similar project to reduce the disease burden among a larger proportion of
Cambodian children.

iv
Dedication
To My Dad - The Dreamer
I’m not quite convinced that dreams ever come true. I think that dreams only ever come
through.
You might have had your head in the clouds, but when it comes down to it, I think that
you’ve got to be a little out of touch with reality in order to make a dream come through.
Maybe dreaming is about being open.
There was a farm and a motorbike and a factory, then you went to fix aeroplanes. There was a
shoe shop and a wee house with a yard then you went to study and preach. There was a
chapel and village and a bunch of cows and you brought the books of the world into our
house.
We didn’t know anything about Dentistry or Cambodia or PhDs but I think that the fact that
you were a dreamer made my dreams come through.
To My Mother, Kim Turton, who was the first person to introduce me to the concept of a PHD.
It’s true, my gear is ‘Piled High and Deep’ in her garage!

v
Declaration
This is to certify that:
i. The thesis comprises only my original work towards the PhD except where
indicated
ii. Due to acknowledgement has been made in the text to all other material used
iii. The thesis is less than 100,000 words in length, exclusive of tables, maps,
bibliographies and appendices
Bathsheba Jael Turton_____ _________ 21 September 2018

vi
Acknowledgements
First and foremost thank you to my supervisors Prof David Manton and Dr Felicity Crombie
who supported me through out, were always available, were excellent communicators and
without whom I wouldn’t have been able to realise the dream of participating in the world of
preventive dentistry in Cambodia
Assoc Prof Callum Durward – my advisor and the father of modern dentistry in Cambodia and
without whom, this research would not be possible. Yours are the shoulders that I stand on
when I want to gain a better view.
Phillip Sussex – who set up the SEAL protocol training materials. In addition, he inspired
critical thinking and made it possible to consider an at-scale intervention in a Cambodian
context.
The organisations and companies who sponsored the projects: GC Asia, Cam Kids, Ivolcar
Vivadent, and ANZSPD who provided support for projects.
Scholarships
Peter and Barbara Dennison who provided mentorship and support in interpreting my
experiences dealing with the problem of caries in Cambodia.
Dr Karen Sokal Gutierez who provided ongoing mentorship, friendship and support and helped
me to understand the situation better.
The Partnering organisations; International University Phnom Penh, Cambodia Dental
Association, Cambodia World Family, Buddhist Library Project, Australia-New Zealand
society of paediatric dentistry, Global Child Dental Fund and Cam Kids who cooperated to
make these projects possible. A special mention to One-2-One Cambodia who provided
administrative oversight for the projects.
Drs Tepirou Chher, and Sithan Hak from the Oral health Bureau who supported projects,
provided advice and continue to relentlessly advocate for better oral health for Cambodian
people.
Dr Sopharith Soeun who provided training for primary health care providers in the Cambodia
Smile intervention and is providing ongoing mentorship and training in the upscale phase.
Midwives in the health centres in Kampong Speu who made an impact for the Cambodia smile
intervention and were able to provide useful feedback that will shape dental prevention into the
future.
Ms Liong Sao who acted as a research assistant and who had the ability to solve problems
before I knew they were happening.

vii
Dental students of the Univeristiy of Puthisastra, International University, and University of
Health Sciences, Phnom Penh Cambodia. Dental students placed fissure sealants, collected and
entered data and made these projects possible.
For the SEAL Cambodia Project: Chen Pagna, Sok Povrath, Sok SereyPiseth, Sreang Rattanak
For the Cambodia smile cross-sectional study: Dr Yos Chantho, Dr Tak Ranouch, and Dr Soy
Rasy
For the Cambodia Smile intervention: Sieng Tida, Cham Roeun, Heng Chanlay, Sok Phirak,
Loy Sreylan, and Horn Vitou.
Laura Spero who helped with editing, endured my frustrations, and facilitated my problem
solving. You continue to inspire me.

viii
Table of Content
Abstract ..................................................................................................................................... ii
Dedication ................................................................................................................................ iv
Declaration................................................................................................................................ v
Acknowledgements ................................................................................................................. vi
Table of Content ................................................................................................................... viii
List of Tables ........................................................................................................................ xiii
List of figures .......................................................................................................................... xv
List of Appendices ................................................................................................................. xvi
Abbreviations ....................................................................................................................... xvii
Publications and Presentations ............................................................................................ xix
1.0 Chapter 1 – Literature Review .................................................................................... 2
1.1 Dental caries ....................................................................................................................... 2
1.1.1 The caries balance ......................................................................................................... 3
1.1.2 Observing and quantifying the signs of dental caries ................................................... 5
1.2 Early childhood caries ....................................................................................................... 7
1.2.1 Early childhood caries................................................................................................... 7
1.2.2 The maternal-child link to ECC .................................................................................... 9
1.2.3 Nursing habits and ECC.............................................................................................. 10
1.2.3.1 Breast feeding ...................................................................................................... 10
1.2.3.2 Bottle feeding ....................................................................................................... 13
1.2.4 The diet and ECC ........................................................................................................ 13
1.2.5 The bacteria and ECC ................................................................................................. 15
1.2.6 Host factors ................................................................................................................. 16
1.2.7 Socio-behavioural factors and risk modelling ............................................................ 17
1.3 Prevention of ECC ........................................................................................................... 19
ix
1.3.1 Maternal-child interventions ....................................................................................... 20
1.3.2 School based interventions ......................................................................................... 21
1.3.3 Multi-sectorial cooperation ......................................................................................... 21
1.4 Prevention of ECC – managing the diet ........................................................................ 22
1.5 Prevention of ECC – Fluorides and topical agents ....................................................... 22
1.5.1 Fluoridated toothpaste ................................................................................................. 23
1.5.2 Fluoride Varnish ......................................................................................................... 24
1.5.3 Other fluoride delivery systems .................................................................................. 25
1.5.4 Bioavailable calcium and phosphate substrates .......................................................... 26
1.5.5 Antibacterial agents for preventing ECC .................................................................... 27
1.6 Prevention of caries on First Permanent Molars (FPM) .............................................. 28
1.6.1 Pit and Fissure sealants ........................................................................................... 29
1. 7 The situation in Cambodia ............................................................................................. 30
1.7.1 General health experiences in Cambodia .................................................................... 30
1.7.2 Dental caries in Cambodia .......................................................................................... 31
1.7.3 Policies, politics, and practice in Cambodia ............................................................... 33
1.7.3.1 Community health centres in Cambodia .............................................................. 33
1.7.3.2 Dental nurses in Cambodia .................................................................................. 33
1.7.3.3 Traditional Dentists .............................................................................................. 34
1.7.3.4 University Trained Dentists ................................................................................. 34
1.7.3.5 The Oral Health Bureau ....................................................................................... 34
1.8 Summary of literature review ......................................................................................... 35
1.9 References Chapter 1 ....................................................................................................... 36
2.0 Chapter 2 – The SEAL Cambodia pilot studies ............................................................ 50
2.0.1 The ‘birth’ of the SEAL Cambodia Community Project ............................................ 51
2.1 Aim .................................................................................................................................... 53
2.2 Objective ........................................................................................................................... 53

x
2.3 Methods ............................................................................................................................. 54
2.3.1 Selection of teeth for FS ............................................................................................. 54
2.3.2 Pilot A – one year evaluation of the original cohort ................................................... 54
2.3.2.1 Clinical examination at baseline and one year follow-up .................................... 55
2.3.3 Pilot B - pilot study using a revised protocol .............................................................. 55
2.3.2.1 Clinical examination ............................................................................................ 56
2.3.4 Data collection and analysis........................................................................................ 56
2.4 Results ............................................................................................................................... 57
2.4.1 Pilot A ......................................................................................................................... 57
2.4.2 Pilot B ......................................................................................................................... 63
2.5 Discussion.......................................................................................................................... 67
2.5.1 Caries prevention in Pilot A ........................................................................................ 69
2.5.1.1 Alternatives to achieve caries prevention in FPM ............................................... 69
2.5.2 The retention of FS material in Pilot B ....................................................................... 70
2.5.2.1 The pattern of material loss.................................................................................. 71
2.5.2.2 High vs Low viscosity GIC.................................................................................. 73
2.6 Conclusion ........................................................................................................................ 73
2.7 References Chapter 2 ....................................................................................................... 74
3.0 Introduction – SEAL Cambodia evaluation of a modified protocol for placing Fuji
VII Fissure Sealants (FS)....................................................................................................... 78
3.1 Aim .................................................................................................................................... 79
3.2 Objectives.......................................................................................................................... 79
3.3 Methods ............................................................................................................................. 80
3.3.1 Clinical procedures ..................................................................................................... 80
3.3.2 Clinical examination and questionnaire ...................................................................... 81
3.3.3 Part 1 – Methods for One-year investigation .............................................................. 81
3.3.4 Part 2 – Two year analysis .......................................................................................... 81

xi
3.3.5 Data analysis ............................................................................................................... 82
3.4 Results ............................................................................................................................... 83
3.4.1 Part 1 – One year comparison of old and new cohorts. .............................................. 83
3.4.2 Part 2 – Two year evaluation of the modified protocol. ............................................. 89
3.5 Discussion.......................................................................................................................... 95
3.5.1 General findings .......................................................................................................... 95
3.5.2 Preventive benefit of the SEAL Cambodia intervention ............................................ 95
3.5.3 Protocol considerations ............................................................................................... 96
3.5.4 Self-reported oral symptoms ....................................................................................... 98
3.5.5 The theoretical argument for SEAL as a preventive strategy ..................................... 98
3.6 Conclusion ........................................................................................................................ 99
3.7 References Chapter 3 ..................................................................................................... 100
4.0 Chapter 4 – Cambodia Smile cross-sectional study. Introduction ............................ 101
4.1 Aim .................................................................................................................................. 103
4.2 Objective ......................................................................................................................... 103
4.3 Methods ........................................................................................................................... 104
4.3.1 General approach ...................................................................................................... 104
4.3.2 Participants ................................................................................................................ 104
4.3.3 Clinical Measures...................................................................................................... 105
4.3.4 The questionnaire ...................................................................................................... 105
4.3.5 Data analysis ............................................................................................................. 105
4.4 Results ............................................................................................................................. 107
4.5 Discussion........................................................................................................................ 118
4.5.1 Caries experience within the Cambodia Smile cross-sectional survey ..................... 118
4.5.2 ECC and nursing habits ............................................................................................ 119
4.5.3 ECC and oral hygiene practices in Cambodia .......................................................... 122
4.5.4 Other risk indicators for ECC ................................................................................... 122
xii
4.6 Conclusions ..................................................................................................................... 123
4.7 References Chapter 4 ..................................................................................................... 124
5.0 Chapter 5 – The Cambodia Smile intervention .......................................................... 130
5.1 Aims ................................................................................................................................. 131
5.2 Objective ......................................................................................................................... 131
5.3 Methods ........................................................................................................................... 132
5.3.1 Health Centre and Population Selection ................................................................... 132
5.3.3 Clinical Protocol for the intervention ....................................................................... 132
5.3.4 The questionnaire for the two-year follow-up .......................................................... 133
5.3.5 Clinical measures ...................................................................................................... 133
5.3.6 Data collection and analysis...................................................................................... 133
5.4 Results ............................................................................................................................. 135
5.5 Discussion........................................................................................................................ 142
5.5.1 Differences in Oral Health Related Quality of Life .................................................. 142
5.5.2 Differences in caries experience by participation in the intervention ....................... 143
5.6 Conclusions ..................................................................................................................... 145
5.7 References Chapter 5 ..................................................................................................... 146
6.0 Chapter 6 - Overview, limitations, and recommendations of the SEAL Cambodia and
Cambodia Smile projects .................................................................................................... 152
6.1 Summary of findings from the ‘SEAL Cambodia’ project ........................................ 152
6.2 Summary of findings from the Cambodia Smile project ........................................... 155
6.3 Conclusions ..................................................................................................................... 158
6.4 References Chapter 6 ..................................................................................................... 159

xiii
List of Tables
Table 1.1 – Case definitions of Early Childhood Caries (ECC) and Severe Early Childhood
Caries (sECC) ............................................................................................................................ 8
Table 1.2 Dental caries experience in Cambodia between 1990 and 2011 ............................. 32
Table 2.1 – Pilot A – Attrition analysis for the 1-year follow-up by gender and age.............. 57
Table 2.2 – Pilot A - Caries experience at baseline by group membership, gender and age. .. 58
Table 2.3 – Pilot A - Caries incidence and sealant retention by group membership ............... 59
Table 2.4 – Pilot A - Caries incidence in the intervention group by baseline caries experience
and age ..................................................................................................................................... 60
Table 2.5 – Pilot A - Number of retained sealants by caries experience and gender .............. 62
Table 2.6 – Pilot B – Gender and group membership after cases with caries FPM at baseline
were removed ........................................................................................................................... 64
Table 2.7 – Pilot B - Proportion of sealant retention by material type in the intervention group
…………………...................................................................................................................... 65
Table 2.8 – Pilot B - Proportion of Fuji VII® FS retained at one month and one year by group
membership .............................................................................................................................. 66
Table 3.1 – Part 1 – Attrition analysis for the One year follow-up by group membership and
caries experience. ..................................................................................................................... 83
Table 3.2 – Part 1 - Sociodemographic Characteristics of Participants. .................................. 84
Table 3.3 – Part 1 - Clinical Characteristics of participants by group membership. ............... 86
Table 3.4 – Part 1 - Caries preventive increment by group membership at one year. ............. 87
Table 3.5 – Part 1 - Logistic regression model for risk of developing new carious lesions based
on group membership. ............................................................................................................. 88
Table 3.6 – Part 2 - Characteristics of participants by gender, age, and group membership and
school. ...................................................................................................................................... 89
Table 3.7 – Part 2 - Clinical characteristics of participants according to sociodemographic
factors. ...................................................................................................................................... 90
Table 3.8 – Part 2 - Participant attrition analysis for the 2 year follow-up of the second cohort.
………………………………………………………………………………………...91

xiv
Table 3.9 – Part 2 - Proportion of children with new carious lesions on occlusal of FPM at 2-
years by group membership. .................................................................................................... 92
Table 3.10 – Part 2 - Proportion children with new cavitated occlusal and interproximal carious
lesions by group membership. ................................................................................................. 93
Table 3.11 – Part 2 - Logistic regression models showing odds ratio for the chance of
developing one or more occlusal lesions on FPM at two-years............................................... 94
Table 4.2 – Cambodia Smile Cross-sectional study - Socio-demographics characteristics by
caries experience of the child. ................................................................................................ 109
Table 4.3 – Cambodia Smile cross-sectional study - Maternal caries experience by Child caries
experience. ............................................................................................................................. 110
Table 4.4 – Cambodia Smile cross-sectional study - Questions on nursing habits and oral health
behaviours by responses from the primary-caregiver. ........................................................... 112
Table 4.5 – Cambodia Smile cross-sectional survey - Questions on dietary habits by responses
from the primary caregiver. ................................................................................................... 114
Table 4.6 – Cambodia Smile cross-sectional survey - Bivariate analysis of dental behaviours
by child caries experience. ..................................................................................................... 116
Table 4.7 – Cambodia Smile cross-sectional study - Binomial logistic regression model for
Socio-behavioural habits by presence of significant caries. .................................................. 117
Table 5.1 – Attrition analysis of intervention group at 1-year. .............................................. 135
Table 5.2 – Sociodemographic characteristics of participants at follow-up by group. .......... 136
Table 5.3 – Caries severity by number of contacts among the intervention group. .............. 137
Table 5.4 – Caries experience by sociodemographic characteristics. .................................... 138
Table 5.5 – Clinical characteristics by exposure to the intervention. .................................... 140
Table 5.6 – Differences within the Family Impact Scale and subscale impacts and mean scores
by group membership. ........................................................................................................... 141

xv
List of figures
Figure 1.1 - The caries imbalance .............................................................................................. 4
Figure 2.1 – Selection and follow-up of children in Pilot B .................................................... 63

xvi
List of Appendices
Appendix 1 – Consent SEAL Cambodia (Original)
Appendix 2 – Post operative information SEAL Cambodia
Appendix 3 – SEAL Baseline examination form
Appendix 4 – SEAL Follow-up examination form
Appendix 5 – Standard SEAL Form
Appendix 6 – The SEAL Cambodia original protocol
Appendix 7 – The SEAL Cambodia modified protocol
Appendix 8 – Examination forms and questionnaire for the Cambodia smile cross-sectional
survey
Appendix 9 – Clinical documentation and Questionnaires for the Cambodia Smile
Intervention
Appendix 10 – Publications
Appendix 11 – Ethical approval documentation

xvii
Abbreviations
AAPD American Association of Pediatric Dentistry
ANZSPD The Australia and New Zealand Society of Paediatric Dentistry
BPOC Basic Package of Oral Cares
CAST The Caries Assessment Spectrum and Treatment Index
CHC Community Health Centre
CHX Chlorhexadine
CNOHS Cambodia National Oral Health Survey
CPP -ACP Casein Phosophopeptide-Amorphous Calcium Phosphate
CWF Community water fluoridation
DMF/DMFT/dmf Decayed, Missing, and Filled Teeth Index.
ECC Early Childhood Caries
FIS Family Impact Scale
FP Fissure Protection
FPM First Permanent Molars
FS Fissure Sealants
FV Fluoride Varnish
GCDF Global Child Dental Fund
GIC Glass Ionomer Cement
HBM Human Breast Milk
ICC Intra Class Correlation
ICDAS International Caries Detection and Assessment System
LB Lactobacilli
LMIC Low-to Middle-income countries
MMP Matrix Metalloproteanise
MOEYS Ministry of Education Youth and Sport
MOH Ministry of Health
NGOs Non-Governmental Organisations
OHB Oral Health Bureau
OHE Oral Health Education including diet advice, oral hygiene instruction
and delivery of toothbrush with a supply of fluoridated toothpaste
OHRQoL Oral-Health-Related Quality-of-Life
PCG Primary care giver
PUFA Pulpally involved, Ulcerated, Fistula, and Abscess index
SD Standard Deviation
SDF Silver Diammine Fluoride
sECC severe - Early childhood caries
SES Socioeconomic Status
SM Streptococcus mutans

xviii
SPSS Statistical Package for the Social Sciences
UN United Nations
WHO World Health Organization
WSL White spot lesions
y years
χ2 Chi-squared test

xix
Publications and Presentations
This thesis is based partially on the following publications by the author and manuscripts
which are reproduced in Appendix 10.
1. Turton B J, Durward C S, Manton D (2015) Early Childhood Caries and Maternal
Caries Experience in a Convenience Sample of Cambodian Pre-schoolers. Pediatric
Dental Journal 25 (1), pp. 14-18.
2. Turton B J, Durward CS, Manton D, Bach K, Yos C (2015) Socio-behavioural risk
factors for early childhood caries (ECC) in Cambodian preschool Children European
Archives of Paediatric Dentistry. 17(2), pp. 97-105.
3. Tac N, Turton B, Durward C (2016) Retention of Glass Ionomer Cement fissure
sealant using a revised protocol Cambodian Dental Journal 12, 14-18.
4. Turton B and Durward C. Management of Early Childhood Caries – a Comparison of
Different Approaches. Thai Dental Public Health Journal 2017 Jan-Feb;22(suppl.),
pp. 67-77
Presentations
1. Turton, B.*, Durward, C., Bach, K., Manton, D. (2014) Seal Cambodia – 60,000
children over 3 years; IADR SEA 28TH Annual meeting, Kutching, Malaysia.
2. Souen, S., Turton, B., Durward, C. (2015) Integrating oral health and general health in
a Cambodian setting; IADR SEA 29th Annual meeting, Bali, Indonesia.
3. Tak, N., Turton, B., Durward, C. (2015) Seal Cambodia – A comparison of two
protocols; IADR SEA 29th Annual meeting, Bali, Indonesia.
4. Turton, B.*, Durward, C. (2015) Seal Cambodia – Placing fissure protection in a
community setting Successfully; FDI world Congress, Bangkok, Thailand.
5. Turton, B.*, (2015) Cambodia Smile – integrating oral health and general health in a
Cambodian setting. 2015 Global children’s nutrition and oral health symposium,
UCSF, California, USA.
6. Turton, B.*, Durward, C., Crombie, F., Manton D. SEAL Cambodia: Improved Caries
Prenvtion with a modified Protocol. (2016) . IADR General Session. Seoul, Republic
of Korea.

xx
7. Sreng, R., Turton, B., Chen, P., Sok S, Durward C. (2016) SEAL Cambodia – Retention
rates of ART Sealants according to provider type. IADR General Session. Seoul,
Republic of Korea.
8. Sopharith, S., Turton B.*, Durward, C., Crombie, F, Manton, D., (2016) Cambodia
Smile – Preliminary results from an early childhood caries intervention. IADR General
Session. Seoul, Republic of Korea.
9. Turton, B.*, Durward, C., Tac, N., & Manton, D. J. (2016). Seal Cambodia Caries
Prevention Using a Modified Protocol for School-based GIC Sealant Placement. 63rd
Congress of the European Organisation for Caries Research in Athens, Greece.
10. Turton B.*, (2017). Reorientation of Dental Services – Lessons Learnt From Cambodia.
Oral Health Improvement Strategies for Asia (IMUOHS): Online Conference. Kuala
Lumpur, Malaysia.
11. Turton B.,* (2017). Management of ECC, Lessons Learnt from Cambodia. 9th Asian
Conference for Oral Health Promotion in School Children. Siem Reap, Cambodia.
12. Turton, B.*, Durward, C., Soeun, S., Crombie, F., Manton, D., (2017). Cambodia Smile
– 2-year follow-up of a community based Early Childhood Caries (ECC) intervention.
Congress of the International Association of Paediatric Dentistry. Santiago, Chile.
13. Turton, B.*, Crombie, F., Durward, C., Manton D. (2018). Seal Cambodia – a tale of
two protocols. ANZSPD, Brisbane, Australia.
14. Turton, B.*, Durward, C., Soeun S., Crombie, F*., Manton, D. (2018). Cambodia Smile
– Caries Prevention by primary health care providers. ORCA, Copenhagen, Denmark

1
Chapter 1
Literature Review
Published in part as: Turton B and Durward C. Management of Early Childhood Caries
– a Comparison of Different Approaches. Thai Dental Public Health Journal 2017 Jan-
Feb;22(suppl.):67-77
Presented in part at the 9th Asian Conference for Oral Health Promotion in School
Children. (2017) Siem Reap, Cambodia: Turton B. Management of ECC, Lessons Learnt
from Cambodia.

2
1.0 Chapter 1 – Literature Review
Introduction
Dental caries remains the most prevalent disease in the world, accounting for a considerable
health burden in both developed and developing countries (Kassebaum 2015). Dental caries is
a multifactorial disease involving an interplay between the bacteria, the host, and the diet, with
free-sugars recently being given emphasis as the most potent initiator and driver of the caries
process (Sheiham & James 2015). In light of this, the globalisation of food sources and the
nutrition transition towards highly processed and high added-sugar foods has been
contemporaneous with the plateauing of improvements in caries rates in developed countries
and increases in dental caries experience among at-risk populations. Countries in the South
East Asian Region are thought to have the most severe caries experience worldwide and
Cambodia has been reported as having the most severe experience of Early Childhood Caries
(ECC) in that region (Duangthip et al. 2017).
Dental caries is classified by the World Health Organization (WHO) as a non-communicable
disease and has a multidirectional relationship with other common conditions such as under-
nutrition (Hooley et al. 2012a). This literature review aims to describe the process of dental
caries, particularly in the context of the pre-school age-group. In addition, the current best
practices for prevention and management of dental caries in a Cambodian context will be
considered.
1.1 Dental caries
Before examining the risk factors associated with ECC, it is appropriate to consider the caries
process first. Dental caries is a behaviourally driven bacterially-based process that can lead to
the irreversible loss of mineralised tooth structure (Fejerskov 1997) and it is the most prevalent
disease in humans (Allukian 2000; Frencken et al. 2012). Although world-wide estimates may
be somewhat out-dated, dental caries affects 60 - 90% of children and almost all adults
(Petersen et al. 2005; Marcenes et al. 2013). Also of concern is that the prevalence and severity
of dental caries appears to be increasing for those in Low and Middle Income Countries (LMIC)
and that the progressive decline in the dental caries experience amongst individuals from
developed countries appears to have plateaued (Petersen et al. 2005; Kassebaum et al. 2015).
Furthermore, when caries experience is broken down by socio-demographic characteristics
within countries, it is possible to see that individuals in the younger age groups and those in

3
disadvantaged minority groups, such as indigenous peoples, are most at risk (Poon et al. 2015;
Schwendicke et al. 2015). The reason these groups are experiencing a disproportionate level of
disease experience could be that the lifestyle and environment in the respective settings may
modify the balance of variables and interventions that contribute to the caries process. (Tiwari
et al. 2018)
1.1.1 The caries balance
The concept of a caries balance (Figure 1) recognises that a carious lesion exists in a dynamic
state where-by protective factors and pathological factors interact (Featherstone 1999). When
the pathological factors are dominating, net mineral loss occurs. In the situation that the system
fails to correct itself (with protective factors) then cavitation may occur at the tooth surface
once sufficient mineral is lost from the lesion (Kidd & Fejerskov 2004; Featherstone 2004).
The pathological factors relate to the oral microbiome, the diet and the host (individual) in the
context of time. With regards to the microbiome, it is important to recognise that the
microorganisms along with by-products and supporting structures on the surface of the tooth
exist within and make up a biofilm. Furthermore, the presence of specific bacteria and bacterial
by-products within that biofilm will alter the environment at the surface of the tooth. Various
bacteria have been implicated in the caries process such as Streptococcus mutans (SM),
Streptococcus sobrinus, Actinomyces, Bifidobacteria and Lactobacilli (LB) (Takahashi 2015).
Almost all human beings carry these organisms; it is not specific species that are responsible
for the caries process but rather a dysbiotic ecological community of bacteria (Marsh 2004).
When the biofilm has a higher proportion of acid producing (acidogenic) and acid resistant
(aciduric) bacteria, combined with insufficient calcium and phosphate ions in the biofilm
solution at the tooth surface to maintain saturation with respect to tooth mineral, then net
mineral loss will occur. When organic acids are produced by the bacteria the hydrogen ions
will dissociate and diffuse into the dental enamel, and in doing so, dissolve the mineral content
of the tooth to eventually produce the clinically detectable signs of a carious lesion.

4
Figure 1.1 –The caries imbalancea
aFeatherstone (Featherstone 2004).
Some species of bacteria are more acidogenic and aciduric than others. These species thrive in
an environment with a high frequency of exposure to fermentable carbohydrates, specifically
free-sugars (WHO 2015). When fermentable carbohydrates are provided as a substrate to the
biofilm then primarily lactic acid is produced, which can rapidly lower pH and dissolve
mineral. In that situation, bacteria which can withstand (and flourish in) an acidic environment
will become the dominant species in an oral environment rich in fermentable carbohydrates. In
other words; the diet will place selective pressures on the biofilm to favour species with
particular characteristics (Ruby & Goldner 2007).
The ability of a food or drink to promote the caries process is termed ‘cariogenicity’
(Tahmassebi et al. 2006). It is both the quantity and the frequency of exposure to fermentable
carbohydrates that triggers this transformation. Regular snacking has been associated with a
higher caries burden (Feldens et al. 2012). In addition, there is evidence at the population level
of a dose-response effect of sugar ingestion to dental caries (Moynihan 2005; Sheiham & James
2015). One of the key protective mechanisms from the host is saliva, which has an ability to
help food bolus formation and subsequent oral clearance, buffer acid, and to provide a reservoir

5
of protein-stabilised supersaturated (with respect to tooth mineral) concentrations of calcium
and phosphate that facilitates remineralisation among other functions (Featherstone 2006).
In a normal scenario and given enough time, the effect of the bacterially-derived acid at the
time of eating can be balanced by the saliva-based protective mechanisms within the mouth; if
the health of the host (individual) is compromised, decreasing salivary quality and/or quantity,
then these protective mechanisms may not be operating optimally, and the caries balance will
tip towards net mineral loss. The bicarbonate system is the major salivary mechanism for acid
buffering in addition to components such as phosphate, urea and amphoteric proteins and
enzymes. Maintenance of a neutral pH is important for sustaining super-saturation of
bioavailable minerals with respect to tooth mineral at the ionic concentrations present in the
mouth (Humphrey & Williamson 2001).
The ability of saliva to function both as an acid buffer and as a mineral reservoir compensates
for the fluctuations in pH. This means that the pH can decrease without violating the critical
pH, the lowest pH at which the solution is saturated with respect to tooth mineral. The critical
pH fluctuates depending the amount of calcium and phosphate available in the biofilm solution.
At a lower pH then a greater concentration of calcium and phosphate is required in order to
prevent net mineral loss from occurring (Dawes 2003). In the situation that the host has an
underlying systemic health condition, then the saliva may be of poor quality or low quantity
and thereby be unable to prevent mineral loss from dental enamel. That is to say, for a
compromised host the pathological factors are more likely to dominate, and the signs of dental
caries will appear in areas below undisturbed cariogenic biofilm (Featherstone 2004).
1.1.2 Observing and quantifying the signs of dental caries
The signs of dental caries may be observed along a spectrum of changes that are first detected
clinically as a white spot lesions of enamel (WSL) on a desiccated enamel surface, advancing
to enamel surface roughness, cavitation and eventually infection of the dental pulp by bacteria
(Kidd & Fejerskov 2004). It is important that indices used to measure the burden of disease are
able to capture the full spectrum of disease presentation and there have been a number of
attempts to achieve this. The Decayed, Missing and Filled (DMF) index is the most common
and is recommended by the World Health Organisation because of its ease of use (WHO 2013).
The main limitation of the DMF index is that it only captures the presence of a carious lesion
when surface cavitation is present (Broadbent & Thomson, 2005). To address this issue the
International Caries Detection and Assessment System (ICDAS) was developed to detect and

6
record the signs of dental caries from an early WSL (only detectable when the tooth is dry)
through to gross loss of hard tooth structure (Ismail et al. 2007). The disadvantage of this
system it that it requires optimal tooth cleaning and drying and illumination to detect the earliest
lesion which limits its use in a field environment, although some variations of ICDAS have
been created to address this. For example, the Caries Assessment Spectrum and Treatment
(CAST) index was developed which records the signs of caries at the stage in which a carious
lesion is visible on a wet surface. The data generated by CAST can be easily manipulated to
generate DMF data for cross comparison to historical datasets (Frencken et al. 2011). However,
the uptake and use of CAST has been limited.
Although it is important to detect the early consequences of the caries process, in some settings
a large proportion of carious lesions go untreated, leading to a high prevalence of pulpally
involved teeth. The Philippines is one of these settings and it was here that the Pulpally-
involved Ulcerated Fistula and Abscess (PUFA) index was developed (Monse et al. 2010). This
index can be used to effectively quantify the severity of the effect of carious lesions on the pulp
and has been useful in examining the relationship between severe dental caries and malnutrition
(Benzian et al. 2011). The main disadvantage of the PUFA index is that it is best used in
addition to one of the other indices rather than independently, and so it may represent an
additional administrative burden on examiners.
One of the other challenges in classifying carious lesions is to recognise the differences in
disease progression between the primary and the permanent dentitions. Regardless of the index
used, each index requires that the primary and permanent dentitions are to be reported
separately. The reason why this is important is that the two dentitions differ in both anatomy
and by their presence in the mouth during the evolving stages of growth and development
(WHO 2013). This is particularly the case for preschool children who can demonstrate a rapidly
progressing and severe expression of dental caries due to their unique dietary and oral hygiene
habits (Douglas et al. 2001).

7
1.2 Early childhood caries
1.2.1 Early childhood caries
Preschool children represent a unique group in that their dental caries disease experience can
change rapidly (Douglass et al. 2001) and that they are in the process of evolving through many
developmental milestones. Although the caries process is the same for both adults and children,
when a young child suffers from ECC (defined in Table 1) the process can happen more quickly
and the experience of ECC is often considered as a subset of caries within the general caries
disease spectrum. The reasons that the disease might progress rapidly are related to a
combination of the unique behavioural context of a growing child and tooth morphology
(Ismail 2003). The other unique aspect of this disease experience is that the symptoms of the
disease have a profound impact on quality of life for both the child and those around them. The
impacts of the disease are not just isolated to the affected individual (Martins-Júnior et al.
2013).
To complicate matters further, there is a lack of consistency with the language used to describe
the caries experience of young children. This may be because different socio-behavioural
features tend to be implicit in each setting (Dye et al. 2015; Harris et al. 2004). The result has
been terms such as ‘baby bottle tooth decay’ or ‘nursing caries’ (Ismail & Sohn 1999). The
problem with these terms is that they do not capture the degree of severity amongst different
children or groups. Also, from a conceptual point of view, the aetiologically specific terms
(philosophically) could block consideration of other aetiological factors, which are important
when trying to understand the disease in various settings (Milnes 1996).
Quantifying dental caries amongst different populations has often been achieved using
indicator age groups as defined by the WHO, however, these fail to examine the disease
experience in those below six years-of-age; whereas open lesions can develop before the child
is two years-of-age (Douglass et al. 2001). Estimates of world-wide caries experience suggest
that the prevalence and severity of the disease has been reduced considerably over the last 50
to 100-years. However, for those individuals in LMIC and for those in compromised
socioeconomic settings, dental caries experience has increased (Pitts et al. 2011; Schwendicke
et al. 2015; Willems et al. 2005). Global data on the prevalence of dental caries in preschool
children in developed countries is as low as 1% to as high as 50%; and the prevalence of dental
caries in preschool children in developing countries is as high as 70% (Milnes 1996; Petersen
et al. 2005). This contrasts what has been reported in countries such as the Philippines (Monse

8
et al. 2010), Cambodia (Todd et al. 1994; Turton et al. 2015), and Brazil (Chaffee et al. 2013)
where it is estimated that nearly 100% of preschool children have cavitated carious lesions.
The same severe disease burden is often observed for indigenous groups within developed
settings (Hsieh et al. 2014; Peressini et al. 2004; Schroth et al. 2009; Ministry of Health, New
Zealand 2011; Hallett & O’Rourke 2003). Further estimates have suggested that the majority
of dental needs occur in a minority of the most vulnerable groups of children (Mouradian 2001;
Schwendicke et al. 2015; Moffat et al. 2017).
Aside from the differences in dental caries distribution between different populations, the other
issue that is not clear is whether dental caries in preschool children represents one single disease
paradigm or whether there are multiple disease patterns present. For instance, it has been
reported that the most common area for carious lesions to develop in young children is on the
buccal surfaces of the maxillary anterior teeth (Saleem et al. 2015; Sowole et al. 2007). Also,
there is some discussion about whether the second primary molars will develop carious lesions
to a greater extent because they have deeper pits and fissures (Sowole et al. 2007). It is likely
that one influencing factor in the difference in caries experience by tooth type would be because
the diet is different at the differing ages of eruption of specific teeth (Douglass et al. 2001;
Hallett & O’Rourke 2006).
This highlights the need for diagnostic criteria that are age dependant and site specific. The
American Association of Paediatric Dentistry (AAPD) has partly addressed this when it
presented a set of diagnostic criteria for both ECC and Severe-ECC (sECC) (Table 1).
Throughout the remainder of the present review ECC and sECC will be defined by those
criteria laid out in Table 1.
Table 1.1 – Case definitions of Early Childhood Caries (ECC) and Severe Early
Childhood Caries (sECC)a
Age (Months) ECC sECC
<12 1 or more dmf surfacesb 1 or more smooth dmf surfaces
12-23 1 or more dmf surfaces 1 or more smooth dmf surfaces
36-47 1 or more dmf surfaces 1 or more cavitated, filled, or missing (due to
caries) smooth surfaces in the primary
maxillary anterior teeth OR dmfs score > 4
48-59 1 or more dmf surfaces 1 or more cavitated, filled, or missing (due to
caries) smooth surfaces in the primary
maxillary anterior teeth OR dmfs score > 5
60-71 1 or more dmf surfaces 1 or more cavitated, filled, or missing (due to
caries) smooth surfaces in the primary
maxillary anterior teeth OR dmfs score > 6 aadapted from Drury et al. 1999.

9
bAny carious lesion, non-cavitated or cavitated, missing due to caries or filled surface. Includes primary teeth
only.
Another consideration when describing carious lesions is the impacts which are not captured
by counting teeth. Diagnostic criteria and clinical measures are helpful, but they do not capture
the effect of experience of the disease on the individual completely (Locker & Allen, 2007)
(McGrath et al. 2004). Carious lesions in preschool children have implications for further caries
experience (Broadbent et al. 2008), growth and development (including speech), and the ability
of that child to perform their social role in society (Schroth et al. 2009; Alkarimi et al. 2012;
Li et al. 2015; Hooley et al. 2012; Sheiham 2006; Ayhan et al. 1996; Broder 2007).
Dental caries is, in most individuals, preventable (Allukian 2000; Petersen 2003; Watt et al.
2015) and so all potential impacts could be avoided. In light of this, one of the ways in which
the preschool group differs from other age groups is that some of the risk behaviours associated
with dental caries are, to a large extent, dependent on the caregiver (Mouradian 2001). For
more than 25-years there have been active calls to focus on the relationship between mothers
and maternal and child oral health services in order to reduce the burden of dental caries at the
population level (Frazier & Horowitz 1990).
1.2.2 The maternal-child link to ECC
Although there is a strong evidence-base for associations between maternal and child oral
health, the causal relationship is less clear (Abiola et al. 2009). Some authors have gone as far
as to describe both direct and indirect causal relationships (Okada et al. 2002) and it may be
more appropriate to consider a multi-factorial model in which the characteristics of the mother
influence known protective and pathological factors in the child (Featherstone 2004). When
maternal characteristics are considered in the context of the traditional causal triad of dental
caries (host, bacteria and diet) then the complexity of the relationship can be observed (Selwitz
et al. 2007).
From a psycho-social point of view, the resistance of the host (child) to pathological factors is
related to maternal nutritional status (Black et al. 2008) and psychological maternal stress
(Tang et al. 2005). In addition, the child’s diet is also influenced by maternal stress and
maternal oral health literacy independently of socioeconomic status which also has an effect
(Divaris et al. 2011; Vann et al. 2010). The description of these interactions does not take into
account the expression of cariogenic bacteria in a young child’s mouth which has been

10
associated with high maternal salivary counts of S. mutans and Lactobacilli (as indicators of a
cariogenic diet) (Chaffee et al. 2013), preterm low birth weight (Boggess & Edelstein 2006),
and maternal oral hygiene practices (Chaffee et al. 2013). To add to the complexity, the
relationship between maternal characteristics and oral hygiene practices in young children are
further associated with parental stress (Finlayson 2007; Menon et al. 2000), parental attitudes
(Adeniyi et al. 2009; Tang et al. 2005), maternal oral health literacy, maternal age, maternal
education, and maternal location of residence (Abiola Adeniyi et al. 2009).
In the absence of a direct causative pathways (Okada et al. 2002) and standardised collection
of data (Kuthy 1997) it can be challenging to make a clear statement about how maternal
characteristics influence child oral health outcomes. Despite the multifactorial relationship, the
evidence of an association between caries experience in the child and caries experience in the
mother (Hooley et al. 2012b). Furthermore, it has been demonstrated that maternal caries
experience, particularly untreated lesions, at the time of birth can predict the caries experience
of their respective offspring into adulthood (Shearer et al. 2011; Harris et al. 2004; Smith et al.
2002). It is likely that both mother and child are exposed to a majority of the same protective
and pathological factors and so the presentation of carious lesions will depend upon how the
caries balance is managed in both individuals.
1.2.3 Nursing habits and ECC
Balancing protective and pathological factors is pertinent in the debate about optimal nursing
habits. One of the key issues for debate is the contribution of human breast milk (HBM) to the
dental caries process. Nursing and early childhood feeding practices are culturally bound, the
evidence for this is seen in the way that nursing habits vary widely in different settings
(Rasbridge 1995) and the way in which mothers wish to conform to social norms for nursing
in order to avoid being seen as a ‘bad mother’ (Desclaux 2009). Taking into account cultural
variation, the understanding of the relationship between dental caries and nursing habits is
distorted by a lack of investigations into breast-feeding habits and associated dietary
components in a developing world setting, and a lack of consistency with regards to reporting
such habits (Chaffee et al. 2014; Valaitis et al. 1999; Feldens et al. 2012). Despite this deficit,
some aspects of nursing are universally accepted, and this is important to consider because
there are many stakeholders in the debate and health professionals should deliver a consistent
message (Fewtrell et al. 2007; WHO, 2003).
1.2.3.1 Breast feeding

11
The present recommendation from WHO is that children should be exclusively breast-fed for
the first six months-of-life. It is widely accepted that exclusive breast-feeding during the first
six months of life can reduce the risk of gastroenteritis, infections, asthma, atopic disease and
diabetes. All of these benefits are thought to be achieved by the complex and unique
combination of micronutrients, proteins, immune complexes and carbohydrates (Marriott et al.
2012; Ribeiro & Ribeiro 2004). This combination is distinct from other processed milk
substrates such as cow’s milk, (Lönnerdal 2003) which, in comparison, has a higher buffering
capacity and lower carbohydrate content (Bowen & Lawrence 2005). In other words, breast
milk contains substrates which are capable of nourishing a biofilm rich in acidogenic and
acidoduric bacteria. Whether HBM has the right characteristics to initiate that pathological
transformation of the biofilm is in question. It has been argued that the amount of bio-available
calcium and phosphate present in human breast milk can prevent the biofilm from reaching a
critical pH with respect to tooth mineral at which net mineral loss occurs (Erickson & Mazhari
1999). This is the basis for the hypothesis that HBM has no cariogenic potential provided that
it is the only source of carbohydrate (Nunes et al. 2012). A recent study tested the idea by
exposing children with and without ECC to HBM then measuring saliva and biofilm pH; the
study found that the HBM did not lead to a change in pH (Neves et al. 2016).
In the developing world there has been a recent increase in the availability and consumption of
refined sugars (Chaffee & Cheng 2014). In addition, sugar is being added to almost all
processed foods and those processed foods have become more accessible than traditional
(unprocessed) food, this phenomenon limits consumer choice (Ludwig & Nestle, 2008). The
universal availability of refined sugars could modify the relationship between HBM and the
dental caries process. When the context of complimentary feeding is considered, if all of the
foods added to the diet of the young child include refined sugar then the biofilm could become
highly cariogenic. When the transformed cariogenic biofilm is exposed to HBM the metabolic
bi-products will be highly acidic (Chaffee et al. 2014). These differences in the characteristics
of the biofilm across different settings (i.e. settings where complimentary foods are low or high
in sugar) could also explain why some investigations report breastfeeding to be a protective
behaviour (Peterson et al. 2003; Roberts et al. 1994; Silver et al. 1992; Vignaraja et al. 1992)
while others report breastfeeding as a risk indicator (Nunes 2012, Chaffee 2014). It could be
theorised that the role that HBM plays in ECC is inconsistent across different settings (Valaitis
et al. 1999) and that it is often confounded by other socio-behavioural aspects (Erickson &
Mazhari 1999; Harris et al. 2004).

12
Widespread confounding has made it difficult to reach a consensus about the relationship
between HBM and the dental caries process. While it is accepted that exclusive breast-feeding
should occur over the first six months of life (WHO, 2003), there is currently no consensus on
what age breast-feeding should stop and how that might influence the ‘caries equation’
(Chaffee et al. 2014). Some from the dental community have suggested that breast-feeding
should stop as soon as the child is able to drink from a cup (Ribeiro & Ribeiro, 2004) while
others from the nursing community have said that there is no right time and that mothers should
be encouraged to breast-feed for as long as they can (Valaitis et al. 1999). The right time to
stop may differ depending on the individual and social contexts (Salone et al. 2013).
This lack of clarity in terms of evidence may be due to the fact that prolonged breast-feeding
is not well defined. For some countries it is uncommon to breast-feed past 6 or 12 months
(Hallett & O’Rourke 2003; Peres et al. 2017) while in other countries it is normal to breast-
feed past the age of two years (Chaffee et al. 2014). In those countries in which breast feeding
commonly stops before the first year-of-age, HBM does not appear to contribute to detectible
signs of carious lesions (Erickson & Mazhari 1999). In contrast, a setting where children sleep
with their parents, where night time ‘on demand’ suckling occurs, and where the child is breast-
fed past the age of two years, then HBM has been implicated as a risk factor for sECC (Chaffee
et al. 2014; Thitasomakul et al. 2009; van Palenstein Helderman et al. 2006; Serwint et al.
1993). Recently, there have been more studies which identify higher risk of ECC associated
with breast-feeding past 24 months (Avila et al. 2015; Wong et al. 2017; Feldens et al. 2012;
Peres et al. 2017).
The challenge in defining nursing habits lies in the fact that not all children are exclusively
breast-fed during the first six months of their life. Non-exclusive breast feeding differs across
different settings, even within the same region. For example, the prevalence of exclusive
breast-feeding up to six months for Vietnam is estimated to be 15.5%, for Timor Leste 30.7%,
for Philippines 33.7%, for Indonesia 38.9% and for Cambodia 60.1% (Khitdee 2017).
Furthermore, exclusive breast-feeding can differ within families and communities. Children
are less likely to be exclusively breast-fed during the first six months if they were the first born,
have a working mother, or have an ‘older’ mother (Senarath et al. 2010). The effect that a
particular nursing habit might have on dental caries is dependent on the day-to-day dietary and
oral hygiene behaviours, as well as the age of the child (Chaffee & Cheng 2014). Furthermore,
social indicators are associated with both caries and variations in food profiles (Gatica et al.
2012).

13
1.2.3.2 Bottle feeding
The bottle is the main viable alternative to breast-feeding for delivery of nutrition to the child
during infancy. The timing, content, and frequency of drinking are key aspects when describing
the risk of bottle-feeding in the ECC process. Children who are allowed to sip on their bottle
(carrying cariogenic contents) for a prolonged period of time, particularly at night time while
they are sleeping, have a high risk of ECC (Gussy et al. 2006; Hallett & O’Rourke 2003;
Hooley 2012b; Peltzer & Mongkolchati 2015). The other aspect to consider is whether there
are long-term health impacts (chronic disease, learning outcomes, growth and development)
associated with bottle-feeding as opposed to breast-feeding. It was recently reported that in a
middle-class context within a developed country, once fixed family effects are taken into
account, there are no adverse health outcomes associated with bottle-feeding (Colen & Ramey
2014). This statement draws the reader back to the idea that the risk of bottle-feeding
contributing to unfavourable oral health outcomes depends upon the way that children are
bottle-fed rather than the modality itself.
1.2.4 The diet and ECC
The transition of the child from a liquid diet towards a solid diet is fraught with challenges, and
one of those is the addition of free sugars to the diet. In many settings, various forms of sugar
are being added to an infant’s food (Thitasomakul et al. 2009), the infant’s bottle or even to the
breast milk (Ribeiro & Ribeiro 2004). This is a significant problem because of the effect that
sugar has in: (1) transforming the biofilm into a cariogenic biofilm, with a low pH and under-
saturation with respect to tooth mineral (Leme et al. 2006); (2) ‘recalibrating’ the child towards
favouring sweet foods; and (3) contributing to obesity and diabetes, which are reaching
epidemic levels in young children across the globe (Ka & Ca, 2012; Lustig et al. 2012; Moodie
et al. 2013). These problems are amplified by the world-wide increase in the gross consumption
of sugar, especially in low income groups, where those in the lowest income quintile residing
in urban areas increased the proportion of caloric sweetener within total carbohydrates from
10.0% to 27.7% between the years 1962 and 2000 (Popkin & Nielsen 2003; Ismail et al. 1997;
Drewnowski, 2000).
In terms of sugar, not all sugars are equal in their ability to contribute to disease processes and
the recent release of the WHO recommendations, free sugars are major contributors to dental
caries and chronic disease. Free sugars are “all monosaccharides and disaccharides added to
foods by the manufacturer, cook or consumer, plus sugars naturally present in honey, syrups

14
and fruit juices” (WHO 2015). Free sugars have been shown to contribute to dental caries in
excess of other sugar groups such as intrinsic sugars, which are those sugars naturally
incorporated within the structure of intact grains, fruits and vegetables. Free sugars easily
diffuse into the biofilm and can be potent initiators of the caries process (Sheiham & James
2015).
One of the most potent vehicles for delivery of free sugars are sugary liquids which include
sugary medicines, beverages with added sugar, fruit juices (in their natural state without
additives), and soft drinks (Hallett & O’Rourke 2003). The reason sugary drinks are such potent
mediators of dental caries is both because of the high quantity of sugar contained within the
drink, and also because it may be consumed from a vessel other than a cup (such as a bottle)
thus continuously delivering sugar to the mouth and biofilm over a prolonged period of time
(Tahmassebi et al. 2006). When a child is able to expose the oral environment to a sugary drink
for many hours during the course of a day (e.g. through prolonged sipping), the ability of saliva
to neutralise acid will be compromised and the biofilm will become more acidogenic (Wan et
al. 2003). The mineral loss that occurs as a result is more rapid for immature enamel such as
that found in an infant’s mouth (Tahmassebi et al. 2006). The evidence for the relationship
between free sugars and more severe caries experiences is seen in the association between
caries and consumption of soft drinks between meals, consumption of table sugars, and
consumption of sugary desserts (Ismail et al. 1997; Sheiham & James 2015).
The presence of sugars in any particular food can be said to increase the potential of that
substrate to cause dental caries; however the actual cariogenicity of one food in comparison to
another can vary. There are a number of characteristics that make a particular food cariogenic,
such as retentiveness and chemical composition which has led to the formulation of a
cariogenicity index (Chaffee & Cheng 2014; Evans et al. 2013). One of the problems with
determining the potential of a food to cause dental caries is that the effect of a food on the
caries balance is moderated by the frequency and mode of delivery. There are a multitude of
different variables that may not always be captured by a simple measure of presence or absence
of a substrate in the diet; furthermore, other socio-behavioural factors may modify the way that
a substrate interacts or is delivered to the oral environment (Gatica et al. 2012). This means
that in certain settings, a food consumed in a particular way may have a higher cariogenic
potential than the same food consumed in a different setting in a different way.

15
1.2.5 The bacteria and ECC
A further aspect contributing to the complexity of the caries process involves the characteristics
of the biofilm and how they will moderate the impact of a cariogenic substrate on the caries
balance. Although SM has been established as an aetiological factor in the caries process, the
presence or absence of SM is not a sufficiently sensitive predictor for the presence of clinical
disease (Harris et al. 2004). To address this, SM data are often presented in two ways; bacterial
counts from saliva, and bacterial counts from the plaque biofilm. Using these techniques, once
cariogenic bacteria reach a certain number within the biofilm, then following exposure to a
fermentable carbohydrate rapid demineralisation can occur (Klock & Krasse 1979; Li &
Caufield 1995). In other words, when a biofilm high in cariogenic bacteria is exposed to a
cariogenic substrate then rapid production of acid will occur, but if a healthy biofilm (where
acidogenic and acidoduric bacteria have not been favoured) is exposed to the same substrate
then the rate of demineralisation will be slower, because not as much acidic by-product will be
produced (Ruby & Goldner 2007).
There is much debate over which specific species within the biofilm are primary agents for
propagating the caries process. In light of this, efforts have been made to characterise the
biofilm by looking at particular strains of bacteria present: common strains have been shown
within races and families, particularly between mothers and their children, and between
siblings and among social groups (Li & Caufield 1995; Mitchell et al. 2009). This commonality
supports the hypothesis that infants receive the bacteria from members of their family and
social community and so the question of mode of transmission has been raised (Berkowitz
2003). Along with the debate around transmission there are questions concerning common
behaviours within a social community leading to selective pressures for certain strains of
bacteria to be prominent. Shared community behaviours can lead to a commonality in the
prominent bacteria as has been observed by some (Yang et al. 2012). This appears to be
consistent with the finding that if members in a child’s community (such as a mother or a
brother) are carrying cariogenic bacteria, then that child is more likely to have detectable levels
of those bacteria at an earlier age (Wan et al. 2003). This could also be a confounder in the
literature that shows that detectable SM has been associated with behaviours such as kissing
the infant on the lips, sharing eating utensils or pre-chewing food (Pattanaporn 2012; Li &
Caufield 1995; Wan et al. 2003). Again, selective pressures shared by a family group (driven
by a shared cariogenic diet) could have also lead to the association between the proportion of

16
SM or LB in the mother’s saliva, and the presence of sECC (Chaffee et al. 2013; Tinanoff et
al. 2002).
The detection of SM in the oral cavity is possible before tooth eruption and some studies show
the age of detection is associated with sECC (Wan et al. 2001). This finding has been used in
the debate between an infective theory versus an ecological theory; the infective theory was
popular before more sophisticated means of detecting microbial species were employed. Now,
with methods such as PCR and m16RNA, it is known that a non-shedding surface (e.g. a tooth)
is not required for the presence of SM (Nyvad et al. 2013). These new analytical methods
helped support the second theory, which proposes that ECC is propagated by the continuous
presence of potentially cariogenic bacteria and that the biofilm can achieve cariogenic potential
at any stage (Wan et al. 2003). Also, taking into account the near universal presence of SM
(Harris et al. 2004; Li & Caufield 1995; Tinanoff et al. 2002), when the biofilm is exposed to
free sugars (fermentable carbohydrates) with high frequency and oral persistence, then it will
transform and net mineral loss can subsequently occur. This process is independent from the
age of the host, or the time of eruption (Harris et al. 2004; Wan et al. 2001). In that scenario,
and in the context of the described process, the clinical signs of disease will be observed on the
teeth. If the biofilm is transformed (because of the cariogenic diet) at the time that newly
erupted teeth with immature enamel are present then it is likely that caries will progress more
rapidly (Berkowitz 2003). If the biofilm is dysbiotic then more cariogenic bacteria will
dominate and SM will be detectable as a risk indicator.
1.2.6 Host factors
The expression of dental caries and its clinical signs will be modified by the characteristics of
the host. Although biochemical changes occur at the surface of the tooth it is important to
consider the caries process in the context of the individual and the interplay of all the related
body systems. Two of the key mechanisms by which host factors modify the caries process are
the excretion of saliva, the thickness and mineral density of the enamel and the shape of the
tooth (tooth morphology) (Fejerskov & Kidd 2009). Although salivary dysfunction is unusual
in young children, when saliva has poor quality or is of insufficient quantity, then the
antibacterial defences are reduced, acid and calcium buffering is decreased and substrate is
cleared less efficiently from the mouth. This places the child at greater risk of caries,
particularly if the diet is high in free-sugars. Medications, medical care (especially

17
radiotherapy) and immuno-suppressive diseases can affect the saliva and subsequently tip the
caries balance away from health (Featherstone 2004; Ribeiro et al. 2013).
In addition to saliva, the status of the ‘host’ can also be compromised if there is a disturbance
in the development of the dental enamel. Such a disturbance can result in dental enamel that is
low in mineral content (hypomineralisation) or decreased in thickness (hypoplasia) with
various clinical presentations (Elfrink et al. 2014). Enamel formation (amelogenesis) happens
during the early stages of growth and development from the second trimester of gestation until
late childhood, and the process can be interrupted or compromised by febrile disease,
medications, environmental pollutants (Ribeiro et al. 2013; and malnutrition (Alvarez 1995;
Fonseca, 2017; Silva et al. 2016). In the situation that amelogenesis is compromised leading to
hypomineralised enamel then the enamel may be more soluble in response to pH changes
within the biofilm (Ghanim et al. 2013). If amelogenesis results in tooth morphology that is
plaque retentive, such as in the case of deep pits and fissures, or in the presence of enamel
hypoplasia, then the biofilm may have a physical niche and not be disturbed on a regular basis
by tooth-brushing, however, a cariogenic state needs to be present (Fejerskov & Kidd, 2009).
While the environmental factors described above can influence the morphology of tooth
structure, there is also evidence that genetics can play a significant role in the expression of
caries patterns. Some genotypes associated with tooth formation have been identified as either
increasing the risk of or protecting from carious lesion formation (Abbasoglu 2015; Olszowski,
2015). Some estimates report that caries expression is up to 40% hereditary (Galton 2012),
while others suggest that the genetic components influence the caries pattern (Shaffer 2009).
Should the genotype play a significant role in moderating caries expression, then this could be
an important target for therapeutic intervention at a molecular or genetic level in the future.
1.2.7 Socio-behavioural factors and risk modelling
Although compromised tooth morphology increases caries risk, the actual clinical presentation
of dental caries is not primarily dependent on the shape of the tooth but rather the interaction
between the tooth surface and the social and behavioural habits of the individual (Harris et al.
2004; Frencken et al. 2012). The socio-behavioural factors represent the interlacing of all of
the different protective and pathological factors, the combination of which is unique to an
individual (and even a tooth surface) but may show trends within communities (Harris et al.
2004). In recognition of this, many efforts have been made to build predictive models to
identify those at a higher risk of developing sECC; however, the models do not appear to be

18
applicable between one population and the next. For example, the USA first started to consume
high quantities of ‘sugar swetened soft drinks in the 1940’s. During this period soda was being
consumed at just one-to-two servings-per-day and only by those of higher socioeconomic
background. A contemporaneous study reported that sugar sweetened beverages, despite their
sugar content, were not a risk indicator for caries experience (Bibby 1955). It could have been
that those who could afford to buy soda were also more likely to use fluoride toothpaste which
helped to maintain the caries balance (Tahmassebi et al. 2006). In contrast, consumption of
sugary drinks appears to be an important predictor for dental caries risk in 2015 in Vietnam,
where there has been a 109% increase in the consumption of sugar sweetened beverages from
2009 to 2014 (Silver, 2015.). In Vietnam oral hygiene practices are not universal, which
probably also increases the caries risk (Do et al. 2009). Although there has not been a national
oral health survey in Vietnam since the year 1999 it is thought that caries experience is
increasing with the increased access to sugar (Do et al. 2009).
This highlights the challenging scenario around preventing and managing ECC and the way in
which protective factors and pathological factors are moderated by an individual’s behaviour
and their environment. That tension has led to some debate as to whether dental caries can be
considered a communicable disease or whether it is a non-communicable disease (Tyas et al.
2000). WHO lists dental caries as a non-communicable disease and there have been recent
efforts to apply the strategies for managing chronic diseases to managing ECC (Edelstein &
Ng 2015). It is clear that dental caries is dependent upon commensal bacteria and dependent
upon exposure to fermentable carbohydrates (free-sugars) but whether the clinical signs of the
disease are observed will depend largely upon the drivers of the caries process and how they
exist in the context of an individual lifestyle (Fejerskov & Kidd 2009; Featherstone 2004;
Harris et al. 2004). Nearly all human beings carry the virulent strains of SM and all humans
consume carbohydrates, but not all humans will develop the clinical signs of dental caries until
the socio-behavioural aspects meet a threshold that tips the caries balance towards pathology
(Petersen et al. 2005; Wan et al. 2003). Whether or not dental caries develops depends upon
the presence of several common risk factors that also determine the presence of other non-
communicable diseases such as diabetes and cardiac disease. For this reason, from the
perspective of population health, dental caries is considered to be a non-communicable disease
(Tyas et al. 2000) and strategies for managing chronic diseases can be applied to the ECC
problem (Edelstein & Ng 2015).

19
Understanding the aetiology of ECC is important for the effective distribution of resources for
prevention and reduction of the burden of disease across a population. To date, the most
universal predictor of future dental caries experience is past dental caries experience; but that
is not useful for an infant who does not yet have teeth in the mouth (Fontana, 2015). In saying
that, once the teeth have erupted then the early signs of dental caries can be observed at a point
in which the damage is reversible. The early signs of ECC are WSL and when observed they
can predict future disease experience and indicate a child who may require further support to
stay cavity free.
1.3 Prevention of ECC
Dental caries (and ECC) is a multifactorial disease and so even with the appropriate application
of preventive dental products, at the most optimal frequency, ECC may still occur if the social
and behavioural determinants of the disease are not addressed. Traditionally, the mantra of oral
health education involved telling patients that they should see their dentists regularly, that they
should brush their teeth two times-per-day and that they should stop eating sugar. These ideas
have created some unrealistic expectations around the power of knowledge to result in
behavioural change and those expectations are thought to have resulted in victim blaming
(Frazier & Horowitz 1990). Oral health education has been shown to be effective in producing
a long-term increase in dental knowledge, but it has not been shown to have a long-term impact
on behaviour change or a reduction in caries risk or changes in diet (Sheiham & Watt 2000).
The nuance in the difference between oral health education and oral health promotion is
important, as the desired outcome of both is a change in behaviour and subsequently a lower
risk of disease. Oral health promotion involves transforming knowledge into action rather than
(just) the transfer of information (Pine 2013). To achieve this, oral health promotion is
something that needs to be interlaced with the social determinants of the disease (Chaffee &
Cheng 2014). The conventions of health promotion describe prevention in terms of primary
prevention which is “action taken prior to the onset of disease”, secondary prevention “as the
application of available measures to detect early departures from health and to introduce
appropriate treatment and interventions” and tertiary prevention as measures to reduce or
eliminate long-term impairments and disabilities, minimising suffering caused by existing
departures from good health and to promote patient’s adjustments to his/her condition”
(Mbawala et al. 2015).

20
Although there has been limited success, primary prevention through health promotion is
essential given the nature of the disease process, which is very hard to reverse once a lesion
has been initiated. Primary prevention should work on controlling the primary drivers of dental
caries, the diet and removing plaque from the teeth (oral hygiene). Secondary prevention,
through products such as topical fluorides, and tertiary prevention, through placement of dental
restorations, might slow the disease process, but ultimately that person will still be at risk of
the disease unless primary prevention has been successful (Litt et al. 1995). For primary
prevention to be successful it needs to be integrated within a variety of different settings and
the intervention must happen as early in the disease process as possible (Steffensen, 1990).
Some authors suggest that intervention should occur in an easily controlled environment such
as a school setting; others suggest that intervention should occur during the first two years of
life (Gussy et al. 2006; Vanobbergen et al. 2001; Schröder & Granath 1983); others advocate
for intervention during the first year of life (Rozier et al. 2003; Schroth et al. 2009); and still
others recommend focusing on the mother during pregnancy (Chaffee et al. 2013; Wigen &
Wang 2012). In any case, the intervention must be co-ordinated across all health disciplines
(Watt 2007) and the two most popular models for doing that are through maternal-child
services or through school institutions.
1.3.1 Maternal-child interventions
There is a need for consistency across health disciplines and given that the infant is largely
dependent on the adults in their life for the food that they consume and hygiene practices, the
mother is often the chosen target for such interventions. A number of interventions including
motivational interviewing for the mother have been reported to be effective in behaviour
change (Harrison et al. 2007; Kowash et al. 2000; Tiwari et al. 2015) as well as reducing the
proportion of children with detectible SM, which implies a less cariogenic biofilm (Jameisonet
al. 2018; Mitchell et al. 2009). Unfortunately, maternal-child interventions are not without
barriers such as lack of funding, the attitudes and behaviours of those mothers who might need
it most, the location and geographical barriers associated with those most at risk, the
knowledge, skills and enthusiasm of health providers in performing motivational interviewing,
and the failure of the health system to be patient-centred, making it acceptable from the ‘health
consumers’ point of view (Steffensen 1990). Despite the challenges, maternal-child
interventions appear to be a promising target in addressing the social determinants of disease
(Medeiros et al. 2015).

21
1.3.2 School based interventions
The key limitation around targeting services at preschool children is that accessing children in
a community setting can be logistically challenging. Focusing an intervention on an institution
where children and families regularly gather has the benefit of being logistically
straightforward and, in addition, an institution such as a school is a contained environment
which can be influenced and altered. There are a number of school-based interventions that
have been shown to reduce caries experience; these include the ‘Irene donut’ in Indonesia
(Adyatmaka et al. 2017) and the ‘Fit For Schools’ program in Cambodia, Vietnam, Laos, and
the Philippines (Duijster et al. 2017). Modifying an environment that a child participates in
alters their perception of what is ‘normal’ and has a higher chance of altering behaviour (Kay
& Locker 1996). Modifying the school environment allows for modification of multiple
determinants of dental caries all in one location. A school represents a place where there is an
intersection of multiple sectors of the community in a single environment.
1.3.3 Multi-sectorial cooperation
Many determinants for dental caries are shared among other non-communicable diseases and
efforts should be directed at common risk factors. In general, the common risk factors are listed
as smoking, alcohol ingestion, diet, exercise, and stress management. By addressing some of
these determinants which are related to oral health, there could also be a reduction in diabetes
and other non-communicable disease and duplication of effort can be avoided (Sheiham &
Watt 2000). To facilitate this, strong multi-sectorial relationships need to be fostered (Frazier
& Horowitz 1990). With respect to dental caries, early risk identification and subsequent early
intervention is important. Typically, the first contact after birth of an infant with the healthcare
system is with a primary health care worker who is administering vaccinations, and therefore
they are well placed to intervene (Schroth et al. 2009; Rozier et al. 2003; Douglass et al. 2001;
Litt et al. 1995; Schröder & Granath 1983).
Dental interventions, such as placement of Fluoride Varnish (FV), for preschool children can
be carried out successfully by non-dental professionals in a number of different settings (Isong
et al. 2011; Mouradian 2001; Slade et al. 2011; Smith & Riedford 2013; Steffensen 1990). This
demonstrates the opportunity to avoid duplication of effort and a possible opportunity for cross-
sector co-operation. In saying that, barriers exist, such as primary health care workers already
being burdened with multiple tasks (Slade et al. 2007). To manage the barriers for such
integration, it may be ideal to adopt a ‘three-pronged’ approach by engaging (first) the

22
community, (second) the health professionals and preschool teachers, and (third) the preschool
children (Cariño et al. 2003).
Reducing the barriers to accessing oral health care can lead to improvements in oral health. A
notable barrier can be whether the service is provided in a way that is accessible and culturally
appropriate (Schluter et al. 2007; Schroth et al. 2009) with services reoriented to meet the
needs of the target group (Albino & Tiwari 2016; Jamieson et al. 2018). In the case of ECC,
preschool children are usually reliant on their caregivers to first perceive the need and then
second to access care. Often there is no perceived need until the clinical manifestations of
dental caries are severe and primary prevention or even secondary prevention is no longer
feasible (Litt et al. 1995; Nowjack-Raymer & Gift 1990). A well-structured service that is
affordable and accessible will be used by preschool children and their caregivers and ultimately
lead to improvements in health outcomes (Gross–Panico & Freeman 2012; Binkley et al. 2005).
1.4 Prevention of ECC – managing the diet
One area that is particularly difficult to influence is that of diet; especially infant diets during
the transition period from a liquid diet to a solid diet. Many different health disciplines have an
interest in this aspect of life; paediatricians know that appropriate food at this age will lead to
better growth and development (Darapheak et al. 2013), dietitians recommend that a good
variety of food at this age will lead to a varied and healthy diet later on (Arimond & Ruel 2004),
and dentists know that if the frequency of exposure to free sugars is unfavourable then sECC
will result (Feldens et al. 2012). There is consensus around the benefits of decreased
consumption of free sugars and around the importance of introducing a variety of nutritious
foods (WHO, 2015).
1.5 Prevention of ECC – Fluorides and topical agents
The premier tool for secondary prevention of dental caries is the use of fluoridated products
and there is good evidence for the use of dental products containing fluoride in reducing the
caries burden (Featherstone 1999; Petersen & Lennon 2004). There are three mechanisms
through which caries prevention with fluoride is achieved (1) enhanced remineralisation
through modification of the ionic saturation within the biofilm fluid with relation to fluorapatite
(2) reduced demineralisation because the fluorapatite that is formed in the enamel of the tooth
after exposure is less soluble than the native impure hydroxyapatite, and (3) the antibacterial

23
activity in which high concentration fluoride inhibits cariogenic bacterial metabolism
(Fejerskov 2004)
The benefits of fluoride were recognised in the US Surgeon General’s report on reducing
caries; (Evans & Kleinman 2000). That report called for supervised tooth-brushing, systemic
fluoride supplementation, use of FV and gels, and intensive patient counselling (Allukian 2000;
Tinanoff & Reisine 2009). The WHO identifies access to fluoride as an important public health
priority for reducing disease burden (Petersen & Ogawa, 2016). Other authors have highlighted
the need for combined approaches using more than one fluoride source (Cariño et al. 2003;
Holve 2008; Schroth et al. 2009) and still others have laid out distinct guidelines for prevention
of ECC (Gussy et al. 2006). It is clear that more than one strategy is needed to reduce the
burden of dental caries and that use of dental products is just one of these options (Frencken et
al. 2012).
1.5.1 Fluoridated toothpaste
The WHO promotes fluoridated toothpaste in its Basic Package of Oral Care (BPOC) in which
it lists, among other things, access to low cost fluoride containing vehicles as being important
(Petersen 2003). In many cases, low cost fluoride has taken the form of fluoridated toothpaste
and so it is important to consider the common arguments around the use of fluoridated
toothpaste. The main risk associated with fluoride toothpastes in young children is that of dental
fluorosis, and so the concentration of fluoride in the toothpaste must balance the risk of dental
caries against the risk of dental fluorosis (Wong et al. 2011). The use of a higher concentration
fluoride toothpaste is well justified in a high-risk patient as there is evidence that a higher
concentration of fluoride in toothpaste will have a greater preventive effect compared with a
lower concentration (Marinho et al. 2003; Wright et al. 2014; dos Santos et al. 2013).
The research investigating the use of toothpaste in the preschool age-group has focused on the
method and the frequency of administration (Hsieh et al. 2014). Ingesting more than a ‘pea
sized’ amount of 1000 ppm toothpaste has been associated with mild fluorosis in some studies
(Wright et al. 2014). Ideally the toothpaste should be administered in a supervised setting
(Macintosh et al. 2010; Hölttä & Alaluusua 1992; Rong, et al. 2003), two times-per-day, and
the toothpaste slurry should be in the mouth for at least two minutes and expectorated without
rinsing or eating anything for two hours after brushing (Kaneilis 2000; Sjögren et al. 1995).
Unfortunately, as mentioned above, oral hygiene behaviours are associated with the socio-
economic characteristics of the child and some groups are unable to undertake these habits.

24
1.5.2 Fluoride Varnish
In the situation that a child or family are unable to undertake effective and regular oral hygiene
practices, or where there is additional caries risk, it may be beneficial to supplement with
professionally applied fluorides. Of the professionally applied fluorides, Fluoride Varnish (FV)
has been the most explored therapy with systematic reviews determining preventive fractions
between 5% and 63% (Mishara 2017). FV is effective for several reasons. Firstly, because it is
carried in a suspension that adheres to the tooth, the tooth surface is exposed to a high
concentration of fluoride ions for an extended period compared to other topical products; that
predictably facilitates the formation of fluorapatite within tooth enamel which is more resistant
to demineralisation than hydroxyapatite (Cochrane & Reynolds 2012). In addition, the fluoride
ions enhance remineralisation and inhibit biofilm production by inhibiting bacterial
metabolism (Fejerskov 2004).
Ideally, FV would be applied three to four times-per-year for optimal preventive effect in
preschool children and a dose response relationship has been demonstrated where by multiple
applications are more effective at reducing dental caries (Carvalho et al. 2010; Weintraub et al.
2006). At population level, the measured impact of FV is that it appears to slow the progression
of the lesion rather than stopping its initiation (Holve 2008) and it has been shown to be able
to reverse early (non-cavitated) enamel lesions in the presence of bioavailable calcium and
phosphate (Bawden 1998). This is achieved by increased mineral density in the outer surface
rather than in the deeper layers of the white spot lesion (Pithon et al. 2015). An antibacterial
effect has been demonstrated (Lippert et al. 2014), although a recent study demonstrated that
the type of microflora present does not change following FV therapy (Anderson et al. 2016).
Despite early promise for the use of FV therapy in the preschool age group, a number of studies
in the last 10-years have produced results which might suggest limited benefits. Of the studies
that report FV to be ineffective, some are underpowered (Memarpour 2015; Oliveira 2014);
other studies are in populations with a prevalence of ECC below 40% at around 2 years-of-age
(Agouropoulos et al. 2014; Anderson et al. 2016; Divaris et al. 2013; Jiang et al. 2014; Oliveira
et al. 2014). Some researchers recruited only participants who had already achieved 2 to 3
years-of-age with no clinical signs of dental caries (Muñoz-Millán et al. 2018; Tickle et al.
2017). Still other researchers have reported issues with FV being applied on a conditional basis
whereby clinicians didn’t always apply FV where it is needed or FV was only applied in
perceived high-risk cases, potentially biasing the measured outcome of the therapy at a

25
population level. If only those children who are very obviously at a high risk of developing
new carious lesions receive FV therapy, then other high and medium risk children who did not
receive FV therapy are still less likely to develop lesions based on the socio-behavioural
differences rather than being based on the benefits (or lack there-of) of the FV therapy,
(Fontana 2018). With this in mind, it seems possible that application of FV to lower caries risk
populations (prevalence <40% at 2-years) without systematic criteria for application is unlikely
to adjust the prevalence of carious lesions in preschool children. Despite this, it is likely that
even when the FV fails to prevent the initiation of a lesion, it will still slow the progression of
an existing lesion (Tickle et al. 2017).
1.5.3 Other fluoride delivery systems
Fluoride Varnish, along with other fluoride products, works in part by inhibiting bacterial
metabolism whilst present, enhancing remineralisation and reducing demineralisation. These
effects are primarily mediated by the presence of fluoride at the surface of the teeth rather than
by incorporation of fluoride into the enamel of developing teeth (Featherstone 1999; Tyas et
al. 2000). There are other ways of applying fluoride topically such as fluoride rinses and
fluoride gels; they both present the risk of ingestion and have not been shown to be as effective
as FV (Wong et al. 2011; Petersen & Lennon 2004).
It is clear that the vast majority of the benefits of fluoride are achieved topically, although there
is well documented success in administration of fluoride systematically. Fluoride drops or
fluoride tablets have been shown to reduce caries in high risk populations (Marya et al. 2012;
Featherstone 1999). In contrast to administration of fluoride tablets, Community Water
Fluoridation (CWF) has the advantage of not requiring any behaviour change for success and
when delivering it across a population, it can reduce inequalities between the rich and the poor
(Sisson, 2007). The economic benefit of CWF has been estimated in the most recent analysis
to realise a nine times cost benefit compared with restorative care (Moore et al. 2017).
While CWF is ingested, most of the benefit is achieved through the topical effect of fluoride at
the tooth surface and there is evidence that water with 0.7-1.0 ppm fluoride reaches therapeutic
levels in the oral cavity (Featherstone 1999). The benefits of systemic ingestion of fluoride on
an erupted tooth are less clear and some studies have demonstrated benefit in that scenario
(Cho et al 2014; Newbrun 2007; Buzalaf et al. 2011). The most recent systematic review found
a 35% reduction in the permanent dentition and a 26% reduction in carious lesions in the
26
primary dentition (Iheozor-Ejiofor et al. 2015). However, this review likely underestimated the
real benefits due to restrictive review criteria (Rugg-Gunn 2016).
That there is a large body of evidence for the benefits of CWF and that the therapy has been
demonstrated to reduce inequalities are two are the considerations that have led to CWF being
considered as one of the 10 great public health achievements of the 20th century (Rugg-Gunn
et al. 2016). In spite of this, CWF has been subject to allegations of harm as a result of ‘mass
medication’. There is evidence that CWF benefits at-risk communities the most; however, even
those in higher socioeconomic groups benefit. There is also evidence that there could be a 12%
increase in enamel defects (Iheozor-Ejiofor et al. 2015): some evidence suggests that the
particular type of enamel defect that increases is a diffuse opacity rather than those defects of
more concerning appearance (MacKay & Thomson 2005). Multiple systematic reviews have
demonstrated that CWF at therapeutic levels is not associated with adverse health outcomes
(Broadbent et al. 2015). Although it is clear that CWF and fluoride tablets benefit the
community, the problem is that high risk populations in a developing world setting do not
always have access to reticulated water systems and they may not be able to access fluoride
tablets which may represent a burden in terms of behaviour change and finances.
1.5.4 Bioavailable calcium and phosphate substrates
Although fluoride has long been the mainstay of preventive dentistry, it has limitations;
namely, the failure of most commercial products to provide bioavailable calcium and phosphate
ions to rebuild the enamel matrix and the failure to replace mineral at a subsurface level
(Cochrane et al. 2010). Although fluoride can enhance remineralisation, if there are no free
calcium and phosphate ions available in solution at the surface of the tooth then
remineralisation cannot progress after the salivary sourced supply is exhausted (Cochrane &
Reynolds 2012). Early attempts to address this deficit involved the delivery of non-soluble
calcium and phosphate and there was little success (Cochrane et al. 2010). The situation
changed when calcium and phosphate ions were delivered along with stabilising peptides that
could ensure that the appropriate substrate was bioavailable for remineralisation. One of the
more effective of such systems include Casein phosophopeptide-amorphous calcium phosphate
(CPP-ACP); this system stabilises the calcium and phosphate ions together in small clusters
(~2 nm diameter) which allows for the ability to create significantly increased concentrations
of calcium and phosphate, more than six times higher than in saliva. The presence of
bioavailable calcium and phosphate enhances remineralisation at the tooth surface (Cochrane

27
& Reynolds 2012). This remineralisation can be further enhanced by the presence of fluoride,
which has been shown to have an additive effect (Cochrane & Reynolds 2012; Nongonierma
& FitzGerald 2012). The in vitro studies for such products are able to demonstrate large
changes in mineral content within dental enamel and in vivo studies are increasing in number
(Nongonierma & FitzGerald 2012). Recent studies in preschool populations show positive
results after the use of products containing CPP-ACP; however, those studies demonstrated
some limitations in terms of cost and compliance which could compromise application at a
larger scale and for more disadvantaged populations (Plonka et al. 2013; Pukallus et al. 2013).
1.5.5 Antibacterial agents for preventing ECC
Aside from high concentration fluoride products, antibacterial treatments have been tested
regarding their efficacy in reducing ECC, including the use of povidone iodine, xylitol,
chlorhexidine (CHX) products and silver compounds. Small pilot samples have shown some
promising indications of a reduced risk of enamel demineralisation associated with application
of povidone iodine every two months (Lopez et al. 2002); however, swabbing the mouth with
povidone iodine at the end of dental treatment under general anaesthetic was not shown to be
effective in reducing future caries increment (Twetman 2008). Recent systematic analysis has
been able to demonstrate a moderate caries reduction after regular exposure to xylitol in the
form of chewing gums or lozenges. The caries reduction is thought to be achieved because the
xylitol, as a sugar substitute, is not able to be metabolised into acid thereby driving a less
acidogenic biofilm and potentially a more diverse biofilm (Marghalani et al. 2017). The results
of this therapy are still inconclusive.
The studies testing CHX have been split between application to the mother and application to
the child; they are also split between CHX varnishes and CHX rinses. One of the limitations of
CHX is that it is highly positively charged which means that it binds to the outer surface of a
biofilm rather than penetrating. It has been demonstrated that CHX does have an effect on SM
and there is mixed evidence about the ability of CHX to inhibit the transmission of SM from
mother to child (Twetman 2008). It is possible that the inconsistencies in terms of when the
mother receives the CHX therapy may have led to inconsistencies in results. In any case,
although CHX has been able to reduce SM levels in mothers, this reduction is transient and not
maintained long-term (Chaffee et al. 2013). In practice, that means that a transient reduction in
SM levels in the mother does not necessarily change the biofilm characteristics of the mother
or of the child (Gussy et al. 2006). There is some evidence that the application of CHX

28
varnishes for the child 2 to 4-times per year may reduce ECC when combined with professional
visits (Gisselsson et al. 2005). However, the evidence for CHX gels and rinses to prevent ECC
is lacking, likely because it does not address the drivers of the caries process (Tyas et al. 2000).
Another possibility for the benefits of CHX is in terms of Matrix Metalloproteinase (MMP)
inhibition leading to preservation of dentine structures (Breschi et al. 2010; Tjäderhane et al.
2013) In light of the current evidence, CHX may be effective as an adjunct therapy in an overall
preventive program, however, products containing fluoride and/or bio-available calcium and
phosphate are still the mainstay of ECC prevention.
The final group of antibacterial agents that have been widely studied, are silver compounds
such as silver nitrate (with sodium fluoride) and silver diammine fluoride (SDF). These agents
are thought to act both through the previously stated actions of fluoride and through MMP
inhibition (Zhao et al. 2018). Although there is some evidence that the biofilm activity is altered
after the tooth surface is treated by SDF, recent evidence suggests that the abundance of caries-
associated bacteria that are present on the surface of SDF treated carious lesions remains
unchanged (Milgrom 2018). While SDF has largely been examined for its ability to arrest the
progression of cavitated carious lesions (Contreras et al. 2017), there is also some evidence that
it will prevent lesion cavitation in First Permanent Molars (FPM) (Zhi et al. 2012). SDF appears
to be most useful in the management of cavitated lesions, rather than earlier (ICDAS 1 & 2)
lesions, where its affect is similar to that of FV (Duangthip et al. 2017).
1.6 Prevention of caries on First Permanent Molars (FPM)
The FPM represents the transition from a complete primary dentition into the mixed and
permanent dentition and a new chance to achieve a healthy and functional dentition over time.
There is some logic to support the targeting of FPM as the most susceptible tooth in the
permanent dentition and as a strategy for producing a higher proportion of adolescent children
with a sound dentition. The key methods for preventing cavitated carious lesions in FPM are
(a) the use of pit and fissure sealants (Ahovuo-Saloranta et al. 2017), (b) the use of the ‘cross
brushing’ technique with fluoride toothpaste (Braga et al. 2009; Frazão 2011), (c) the
application of FV and (d) the placement of SDF (Zhi et al. 2012). The therapy with the most
evidence is the use of pit and fissure sealants; however, some questions remain around the most
effective materials and the preventive benefits among populations with varying caries
experience (Ahovuo-Saloranta et al. 2017).
29
1.6.1 Pit and Fissure sealants
The general consensus suggests that fissure sealing or protection (with resin or GIC-based
products) placed on sound or non-cavitated carious lesions will prevent the progression or
initiation of carious lesions in pits and fissures (Wright et al. 2016). The mechanisms by which
resin-based fissure sealing works are by mechanical blockage of plaque retentive features and
creation of an easily cleansable surface where the bacteria in the base of the lesion is isolated
from the substrate. In the case of GIC fissure protection there is the mechanical protection of
the pits and fissures, as well as the exchange of fluoride ions at the material-tooth interface,
which, in vitro, has been demonstrated to create an enamel surface with increased fluorapatite
which is more resistant to acid dissolution following loss of the GIC material (Chow & Vogel
2001). Some guidelines describe the preferred timing of placement of a fissure sealant to be
within the first year after tooth eruption. After a tooth has been present in the mouth for 2-years
and remained healthy, some then suggest that there is limited benefit to be gained by placing a
sealant in a pit or fissure system provided that there is no change in caries risk behaviours
(Wright et al. 2016). Therefore, pit and fissure sealants do not address the factors that drive the
caries process and they do not change the characteristics associated with caries risk.
While there are some conventions around timing and risk criteria for placement of fissure
sealants, there are ongoing debates around which materials might perform better over time. It
is clear that there are differences in retention according to material type, with resin sealants
being retained longer; however, prevention of carious lesions in pits and fissures appears to be
comparable between resin and GIC sealants at 24 months (Zhang et al. 2013; Yeogepal 2015;
Ahovuo-Saloranta 2017). The evidence demonstrating preventive benefit for time periods
longer than 24 months is sparse, but studies do favour a similar conclusion (Ahovuo-Saloranta
2017) while long term studies strongly favour resin fissure sealant materials (Simonsen 2011).
The limitations in evidence come from the fact that the quality of studies using GIC materials
appears to be lower than for studies using resin-based materials; therefore, it is difficult to draw
strong conclusions (Ahovuo-Saloranta et al. 2017).
One of the key debates around choice of materials is whether retention of the material is needed
in order to achieve caries prevention. It is clear that resin sealants have higher retention rates
and that resin sealants rely on retention as the mechanism for effective prevention. In contrast,
while GIC sealants may be lost, remnants might remain at a microscopic level deep inside the
pit or fissure and that this might provide the preventive effect. Some microscopic imaging has

30
suggested that this might be the case (Hu et al. 2016). GIC forms a calcium bond at the tooth
surface and material is lost due to wear and cohesive failure which can leave remnants of GIC
attached to the tooth surface. The loss of GIC material from a caries-stable tooth surface could
also be a potential advantage for a patient who would then not be required to pay to maintain
that material in place as is the case for resin sealants.
Within the two main types of materials (resin composite or GlC) there are also variations of
the materials such as different generations of resins, high or low viscosity, or chemical and
light cured materials, and also some materials that are a mixture of GIC and resin (e.g.
Compomers and resin modified GICs); at this stage there are no clear additional benefits from
using these hybrid materials, since the body of evidence is still very limited (Ahovuo-Saloranta
et al. 2017).
1. 7 The situation in Cambodia
A number of differences exist between the Cambodian environment and that of countries where
the majority of research on caries prevention has been carried out. Cambodia is a developing
country located in the heart of South East Asia with a coast line to the Gulf of Thailand.
Cambodia has a rich history with its height of prosperity between the ninth and fifteenth
centuries; since then Cambodia has battled border disputes with Vietnam and Thailand,
colonialism by the French, and most recently a civil war and the genocidal Khmer Rouge
regime. In the early 1990’s the United Nations (UN) entered Cambodia in addition to numerous
Non-Governmental Organisations (NGO). In present day Cambodia, the presence of the UN is
much less obvious and there are more NGO’s per capita than any other nation on earth. Despite
this, an estimated 24% of the population remain below the poverty line and the government
continues to allow foreign interests to pillage the natural resources under the eyes of
government leaders who have been in power for nearly 30-years (Brinkley 2011). On the
positive side, Cambodia has been relatively politically stable in recent decades and economic
growth has been consistently strong; and more of the population have joined the growing
middle class, which is mostly located in Phnom Penh (Strangio 2014).
1.7.1 General health experiences in Cambodia
Consistent with economic development comes a transition from a traditional diet towards a diet
high in sugar and ultra-processed foods (Drewnowski, 2000). Along with this is a stark rise in
non-communicable diseases such as diabetes and hypertension (WHO 2017) with little

31
infrastructure to deal with chronic diseases and their consequences (WHO 2012). There have
been some improvements in nutrition as exemplified by the rate of stunting which went from
more than half of 5 year-old children down to two in five over the last 15-years; however,
progress seems to have plateaued in the last five years. There have also been considerable
improvements in the infant mortality rate which has decreased from 95 down to 28 per 1000
live births between the years 2000 and 2014 (National Institute of Statistics 2015).
In light of the consistently high rates of under-nutrition of Cambodian children, recent
interventions have focused on infant feeding practices. Recently the WHO has identified that
there have been some advances made in exclusive breast-feeding during the first six months in
Cambodia; however, complimentary feeding practices are less than optimal (Helen Keller
International 2015). Sugar is being introduced into the diet early, while meat and vegetables
are being introduced relatively late (Marriott et al. 2012; Desclaux & Alfieri 2009), and only
one-in-three Cambodian children are receiving the ‘minimally acceptable diet’ (National
Institute of Statistics 2015). Furthermore, a lack of variety in the diet has been associated with
high rates of stunting in Cambodian children (Darapheak et al. 2013). The effect of these diets
is also seen in the high rate of iron deficiency anaemia (more than half) and vitamin A
deficiency (two in five), which are among the highest rates in the world (Black et al. 2008;
National Institute of Statistics 2015).
1.7.2 Dental caries in Cambodia
Along with high rates of under-nutrition, Cambodia also has a high caries burden with nearly
all (97%) of children who are 6 years-of-age having cavitated, untreated carious lesions. This
is not surprising considering the low rates of tooth-brushing and the early introduction of
dietary sugar (Chher et al. 2016) along with reported on-demand feeding practices (Chher
2016; Turton 2015; Rasbridge & Kulig 1995). Furthermore, it is interesting to note that the
severity of caries for those in the younger age groups is much higher than that in the older age
groups who experienced childhood before the nutrition transition (Table 2). Not only is the
caries experience more severe for the younger age-groups but it can also be observed that there
has been an increase in caries experience between 1990 when the first sample was taken and
2011 when the second sample was taken.

32
Table 1.2 Dental caries experience in Cambodia between 1990 and 2011a
Age
group Year n Prevalence
Mean number of DMFT
DT MT FT DMFT
12
1990 288 79.5 1.5 0.1 0.0 1.6
2011 272 78.3 3.4 0.1 0.1 3.5
15
1990 265 69.1 1.6 0.1 0.0 1.7
2011 230 80.4 3.9 0.1 0.3 4.2
35-44
1990 270 89.5 3.4 2.5 0.5 6.4
2011 408 80.4 3.8 1.3 0.5 5.6
65-74 1990 253 93.3 3.3 13.0 0.1 16.4
60-84 2011 397 75.8 3.8 4.1 0.1 8.1
ataken from Chher et al. 2016.
In Cambodia, dental caries experience is almost ubiquitous, and lesions largely go untreated,
subsequently contributing to large impacts on Oral-Health-Related Quality-of-Life (OHRQoL)
(Turton et al. 2015) that cannot be improved with transient access to dental care (Turton et al.
2015). A recent study that investigated dental caries experience in an NGO-supported
community demonstrated that one in three children manifested the signs of dental caries at one
year-of-age, and that three in four manifested signs at two years-of-age (Bach 2014).
Furthermore, the research demonstrated that one of the major issues was inappropriate feeding
practices during the transitional feeding stage when new (highly fermentable) solid foods were
added to the diet (Bach 2014). This demonstrates that the caries experience in Cambodia is
severe, that it largely goes untreated and that the signs of the disease are detectable early in life.

33
1.7.3 Policies, politics, and practice in Cambodia
Untreated carious lesions are just one of the challenges associated with living or working in
Cambodia. In response to this, multiple local Cambodian NGO’s have attempted to meet the
dental needs of the population by providing dental care, often in a mobile dental setting. In the
scenario of transient mobile dental visits by foreign and local dentists and dental students, there
are a number of issues that could undermine the sustained management of the disease. Some
authors have identified the following mechanisms: lack of coverage and sustainability;
inappropriate volunteer actions; lack of evidence-based volunteer actions; lack of
accountability of volunteer and NGO actions; and lack of integration with and devaluation of
existing local healthcare systems and it’s workers (Holmgren 2011). There is a place for foreign
and local volunteers to assist in disease management; however, this must be with careful
consideration of the local health care systems, local health professionals and local cultural
characteristics.
1.7.3.1 Community health centres in Cambodia
In theory, all Cambodians have access to a Community Health Centre (CHC) at which they can
receive maternal care as well as vaccinations and vitamin supplementation for preschool
children. However, the rates of access to care vary from 58% for children of mothers with no
education, and 70% for children of educated mothers. It is interesting to note that the staff at
these CHCs may be on a wage less than US$100.00 per month depending on the region and
that their wage is supplemented by incentive payments to conduct particular interventions such
as vaccinations (Matsuoka et al. 2013). Anecdotal evidence also suggests that payment is
sometimes sought from the patients by the health care workers, and that patients may be
encouraged to seek treatment at the home of the primary health care provider where they can
charge a fee-for-service.
1.7.3.2 Dental nurses in Cambodia
Despite the challenges, Cambodia has produced one innovative response to the oral health care
situation through the creation of the ‘dental nurse’ scope of practice. Dental nurses undertake
a three-year associate degree program with education divided between primary health care
nursing and basic dental interventions (Glass Ionomer Cement (GIC) sealants, fluoride
applications, oral health education, local anaesthesia, scaling, Atraumatic Restorative
Technique (ART) restorations and extractions). Dental nurses are mostly employed at CHCs

34
in rural areas and can provide the BPOC as advocated by the WHO. Since dental nurses were
permitted to open their own private practices in 2016, and since most graduates are now not
employed by the Ministry of Health, their role in providing oral health promotion services in
the community is limited. There are now four dental nurse schools and most students come
from Phnom Penh or provincial capitals. One of the issues for those working for the provincial
health departments has been that the dental nurses are poorly resourced and supported, and
without the necessary materials or instruments they have been unable to fulfil this role (Chher
et al. 2009). Also, the evidence from the Cambodian National Oral Health Survey (CNOHS)
suggests that this is not a service that is frequented by the wider population.
1.7.3.3 Traditional Dentists
Perhaps, the most common practitioner that a mother and her child might seek dental treatment
from is the traditional dentist (Oral Health Bureau 2014), who practice dentistry usually out of
their homes, based on training received in an apprentice-like system where skills are passed
down, usually within families. In July 2015 there was a report that 200 such practices had been
closed down because they were not registered; however, it is likely that they later re-opened by
paying a registered university-trained dentist to use their name to register the clinic (Jackson et
al. 2015). This is worrying because one study showed that less than one in four of these
practices had appropriate sterilising procedures (Thim & Durward, 2016). Recently there has
been a shift at the Ministry of Health level that is looking to support the existing dental council
to regulate the practice of dentistry along with the other medical professions (USAID ASSIST
Project, 2014) and that might provide a pathway for these traditional dentists to either
demonstrate their competence or to stop any new traditional dental practices from opening.
1.7.3.4 University Trained Dentists
Part of the reason why traditional dentists are still thriving in Cambodia may relate to the very
low number of university trained dentists working in rural Cambodia, and the higher fees
charged by university-trained dentists. Following the fall of the Khmer Rouge, there were only
34 university-trained dentists left. Although the profession has been rebuilt over the last three
decades, generally, new graduate dentists prefer to practice in the larger urban centres
(Durward et al. 2016). The lure of the city is potent, and there is a growing dental tourism
industry (Nguon & Kay 2008). Consequently, conventional dental services are largely
unobtainable by the rural preschool child who is suffering from a severe disease burden.
1.7.3.5 The Oral Health Bureau

35
The Oral Health Bureau (OHB) sits within the Department of Preventive Medicine of the
Ministry of Health. The role of the OHB is to advise the Ministry of Health on policy and
practice for maintaining oral health at population level. The OHB has explicitly recognised that
that dental services are generally not accessible to those in need (Chher et al. 2016). There is
an acceptance that it is not possible to build an extensive network of dental services and even
if there could be, it would not address the underlying determinants of the disease and that
children would continue to manifest the signs of dental caries. Recommendations issued by the
OHB included working towards better access to low cost fluoride, focusing on preventing
dental caries from birth by targeting mothers and children, and setting up demonstration
programs to assess the cost-effectiveness of alternative preventive programs (Oral Health
Bureau 2014).
1.8 Summary of literature review
Addressing the issue of dental caries among young children at population level can be
challenging due to the social and structural barriers that exist in Cambodia. Despite this,
addressing ECC is a key public health issue since the disease is almost universal and has wide
ranging impacts for the individual children and for those around them. Children in Cambodia
have a severe experience of dental caries along with a number of other chronic health
conditions. The socio-political landscape for providing oral health care in Cambodia is
challenging and there is a need for better support and integration with the existing health
infrastructure. Although, a number of effective preventive modalities are available to address
the problem of ECC, the Oral Health Bureau recognises that more research is required to
demonstrate the feasibility and the effectiveness of such prevention-oriented programs in a
Cambodian setting (Chher et al. 2016).

36
1.9 References Chapter 1
Abiola Adeniyi, A., Eyitope Ogunbodede, O., Sonny Jeboda, O., & Morenike Folayan, O.
(2009). Do maternal factors influence the dental health status of Nigerian pre-school children?
International Journal of Paediatric Dentistry, 19(6), 448–454.
Adyatmaka, I, Adyatmaka, A, & Bachtiar, A. (2017). Dental Immunisation - Urgency to build
empowerment in community. Pennsylvania, USA: AEGIS Publications, LLC.
Agouropoulos, A., Twetman, S., Pandis, N., Kavvadia, K., & Papagiannoulis, L. (2014).
Caries-preventive effectiveness of fluoride varnish as adjunct to oral health promotion and
supervised tooth-brushing in preschool children: A double-blind randomized controlled trial.
Journal of Dentistry; Oxford, 42(10), 1277–1283.
https://doi.org/http://dx.doi.org.ezp.lib.unimelb.edu.au/10.1016/j.jdent.2014.07.020
Ahovuo-Saloranta, A., Forss, H., Walsh, T., Nordblad, A., Mäkelä, M., & Worthington, H. V.
(2017). Pit and fissure sealants for preventing dental decay in permanent teeth. In Cochrane
Database of Systematic Reviews. John Wiley & Sons, Ltd. Retrieved from
http://onlinelibrary.wiley.com.ezp.lib.unimelb.edu.au/doi/10.1002/14651858.CD001830.pub5
/abstract
Albino, J., & Tiwari, T. (2015). Preventing Childhood Caries: A Review of Recent Behavioral
Research. Journal of Dental Research. https://doi.org/10.1177/0022034515609034
Allukian Jr, M. (2000). The neglected epidemic and the surgeon general’s report: a call to
action for better oral health. American Journal of Public Health, 90(6), 843.
Alvarez, J. O. (1995). Nutrition, tooth development, and dental caries. The American Journal
of Clinical Nutrition, 61(2), 410S – 416S.
Anderson, M., Dahllöf, G., Twetman, S., Jansson, L., Bergenlid, A.-C., & Grindefjord, M.
(2016). Effectiveness of Early Preventive Intervention with Semiannual Fluoride Varnish
Application in Toddlers Living in High-Risk Areas: A Stratified Cluster-Randomized
Controlled Trial. Caries Research, 50(1), 17–23. https://doi.org/10.1159/000442675
Anderson, M., Grindefjord, M., Dahllöf, G., Dahlén, G., & Twetman, S. (2016). Oral
microflora in preschool children attending a fluoride varnish program: a cross-sectional study.
BMC Oral Health, 16(1), 130. https://doi.org/10.1186/s12903-016-0325-6
Arimond, M., & Ruel, M. T. (2004). Dietary diversity is associated with child nutritional status:
evidence from 11 demographic and health surveys. The Journal of Nutrition, 134(10), 2579–
2585.
Avila, W. M., Pordeus, I. A., Paiva, S. M., & Martins, C. C. (2015). Breast and Bottle Feeding
as Risk Factors for Dental Caries: A Systematic Review and Meta-Analysis. PLoS One; San
Francisco, 10(11), e0142922.
https://doi.org/http://dx.doi.org.ezp.lib.unimelb.edu.au/10.1371/journal.pone.0142922
Bach K. (2014) The Oral Health of Cambodian Pre-School-Aged Children. DCD Thesis.
Faculty of Medicine, Dentistry and Health Science, The University of Melbourne.

37
Bawden, J. W. (1998). Fluoride varnish: a useful new tool for public health dentistry. Journal
of Public Health Dentistry, 58(4), 266–269.
Benzian, H., Monse, B., Heinrich-Weltzien, R., Hobdell, M., Mulder, J., & van Palenstein
Helderman, W. (2011). Untreated severe dental decay: a neglected determinant of low Body
Mass Index in 12-year-old Filipino children. BMC Public Health, 11(1), 558.
Berkowitz, R. J. (2003). Causes, treatment and prevention of early childhood caries: a
microbiologic perspective. Journal of the Canadian Dental Association, 69(5), 304–307.
Bibby, B. G. (1955). Effect of sugar content of foodstuffs on their caries-producing
potentialities. The Journal of the American Dental Association, 51(3), 293–306.
https://doi.org/10.14219/jada.archive.1955.0186
Black, R. E., Allen, L. H., Bhutta, Z. A., Caulfield, L. E., De Onis, M., Ezzati, M. (2008).
Maternal and child undernutrition: global and regional exposures and health consequences. The
Lancet, 371(9608), 243–260.
Boggess, K. A., & Edelstein, B. L. (2006). Oral health in women during preconception and
pregnancy: implications for birth outcomes and infant oral health. Maternal and Child Health
Journal, 10(1), 169–174.
Bowen, W. H., & Lawrence, R. A. (2005). Comparison of the cariogenicity of cola, honey,
cow milk, human milk, and sucrose. Pediatrics, 116(4), 921–926.
Braga, M. M., Mendes, F. M., De Benedetto, M. S., & Imparato, J. C. P. (2009). Effect of silver
diammine fluoride on incipient caries lesions in erupting permanent first molars: a pilot study.
Journal of Dentistry for Children, 76(1), 28–33.
Breschi, L., Mazzoni, A., Nato, F., Carrilho, M., Visintini, E., Tjäderhane, L., Pashley, D. H.
(2010). Chlorhexidine stabilizes the adhesive interface: A 2-year in vitro study. Dental
Materials, 26(4), 320–325. https://doi.org/10.1016/j.dental.2009.11.153
Brinkley, J. (2011). Cambodia’s curse. Foreign Affairs, 88. Retrieved from
https://www.foreignaffairs.org/articles/cambodia/2009-03-01/cambodias-curse
Broadbent, J. M., & Thomson, W. M. (2005). For debate: problems with the DMF index
pertinent to dental caries data analysis. Community Dentistry and Oral Epidemiology, 33(6),
400–409.
Buzalaf, M.A.R., Pessan, J.P., Honório, H.M. and Ten Cate, J.M., 2011. Mechanisms of action
of fluoride for caries control. In Fluoride and the oral environment (Vol. 22, pp. 97-114).
Karger Publishers.
Cariño, K. M. G., Shinada, K., & Kawaguchi, Y. (2003). Early childhood caries in northern
Philippines. Community Dentistry and Oral Epidemiology, 31(2), 81–89.
Carvalho, D. M., Salazar, M., Oliveira, B. H. de, & Coutinho, E. S. F. (2010). Fluoride
varnishes and decrease in caries incidence in preschool children: a systematic review. Revista
Brasileira de Epidemiologia, 13(1), 139–149.

38
Chaffee, B. W., & Cheng, A. (2014). Global Research Trends on Early-Life Feeding Practices
and Early Childhood Caries: A Systematic Review. Journal of Oral Diseases, 2014. Retrieved
from http://www.hindawi.com/journals/jod/2014/675658/abs/
Chaffee, B. W., Feldens, C. A., & Vítolo, M. R. (2014). Association of long-duration
breastfeeding and dental caries estimated with marginal structural models. Annals of
Epidemiology, 24(6), 448–454.
Chaffee, B. W., Gansky, S. A., Weintraub, J. A., Featherstone, J. D. B., & Ramos-Gomez, F.
J. (2013). Maternal oral bacterial levels predict early childhood caries development. Journal of
Dental Research, 93(3), 238-244.
Chher, T., Hak, S., Courtel, F., & Durward, C. (2009). Improving the provision of the Basic
Package of Oral Care (BPOC) in Cambodia. International Dental Journal, 59(1), 47–52.
Chher T, Turton B, Hak S, Beltran E, Courtel F, Durward C, & Hobdell M. (2016). Dental
caries experience in Cambodia: Findings from the 2011 Cambodia National Oral Health
Survey. Journal of International Oral Health 1(1), 1-16.
Cho, H.J., Jin, B.H., Park, D.Y., Jung, S.H., Lee, H.S., Paik, D.I. and Bae, K.H., 2014. Systemic
effect of water fluoridation on dental caries prevalence. Community Dentistry and Oral
Epidemiology, 42(4), pp.341-348.
Chow, L. C., & Vogel, G. L. (2001). Enhancing remineralization. Operative Dentistry, pp 27–
38.
Cochrane, N. J., Cai, F., Huq, N. L., Burrow, M. F., & Reynolds, E. C. (2010). New approaches
to enhanced remineralization of tooth enamel. Journal of Dental Research, 89(11), 1187–1197.
Cochrane, N. J., & Reynolds, E. C. (2012). Calcium phosphopeptides—mechanisms of action
and evidence for clinical efficacy. Advances in Dental Research, 24(2), 41–47.
Colen, C. G., & Ramey, D. M. (2014). Is breast truly best? Estimating the effects of
breastfeeding on long-term child health and wellbeing in the United States using sibling
comparisons. Social Science & Medicine, 109, 55–65.
Contreras, V., Toro, M. J., Elías-Boneta, A. R., & Encarnación-Burgos, A. (2017).
Effectiveness of silver diamine fluoride in caries prevention and arrest: a systematic literature
review. General Dentistry. Retrieved from
http://www.agd.org/media/391570/GenDent_MJ17_Contreras.pdf
Darapheak, C., Takano, T., Kizuki, M., Nakamura, K., & Seino, K. (2013). Consumption of
animal source foods and dietary diversity reduce stunting in children in Cambodia.
International Archives of Medicine, 6(1), 29.
Desclaux, A., & Alfieri, C. (2009). Counseling and choosing between infant-feeding options:
overall limits and local interpretations by health care providers and women living with HIV in
resource-poor countries (Burkina Faso, Cambodia, Cameroon). Social Science & Medicine,
69(6), 821–829.

39
Divaris, K., Lee, J. Y., Baker, A. D., & Vann Jr, W. F. (2011). The relationship of oral health
literacy with oral health-related quality of life in a multi-racial sample of low-income female
caregivers. Health Qual Life Outcomes, 9(108), 1172–1186.
Divaris, K., Preisser, J. S., & Slade, G. D. (2013). Surface-Specific Efficacy of Fluoride
Varnish in Caries Prevention in the Primary Dentition: Results of a Community Randomized
Clinical Trial. Caries Research, 47(1), 78–87. https://doi.org/10.1159/000344015
Do, L. G., Spencer, A. J., Roberts-Thomson, K., Trinh, H. D., & Nguyen, T. T. (2009). Oral
health status of Vietnamese children: findings from the National Oral Health Survey of
Vietnam 1999. Asia-Pacific Journal of Public Health. Retrieved from
http://aph.sagepub.com/content/early/2009/07/02/1010539509340047.abstract
dos Santos, A. P. P., Nadanovsky, P., & de Oliveira, B. H. (2013). A systematic review and
meta-analysis of the effects of fluoride toothpastes on the prevention of dental caries in the
primary dentition of preschool children. Community Dentistry and Oral Epidemiology, 41(1),
1–12. https://doi.org/10.1111/j.1600-0528.2012.00708.x
Drewnowski, A. (2000). Nutrition transition and global dietary trends. Nutrition, 16(7–8), 486–
487. https://doi.org/10.1016/S0899-9007(00)00295-1
Duangthip, D., Gao, S. S., Lo, E. C. M., & Chu, C. H. (2017). Early childhood caries among
5-to 6-year-old children in Southeast Asia. International Dental Journal, 67(2), 98–106.
Duangthip, D., Wong, M. C. M., Chu, C. H., & Lo, E. C. M. (2017). Caries arrest by topical
fluorides in preschool children: 30-month results. Journal of Dentistry 1(70), 74-79.
Duijster, D., Monse, B., Dimaisip-Nabuab, J., Djuharnoko, P., Heinrich-Weltzien, R., Hobdell,
M., … Benzian, H. (2017). “Fit for school” – a school-based water, sanitation and hygiene
programme to improve child health: Results from a longitudinal study in Cambodia, Indonesia
and Lao PDR. BMC Public Health, 17, 302. https://doi.org/10.1186/s12889-017-4203-1
Thim S, Durward C. (2016). Traditional dentists practices in Siem Reap Cambodia Dental
Journal 6, 6-12.
Edelstein, B. L., & Ng, M. W. (2015). Chronic Disease Management Strategies of Early
Childhood Caries: Support from the Medical and Dental Literature. Pediatric Dentistry, 37(3),
281–287.
Elfrink, M. E., Moll, H. A., Kiefte-de Jong, J. C., Jaddoe, V. W., Hofman, A., Jacob, M., &
Veerkamp, J. S. (2014). Pre-and postnatal determinants of deciduous molar hypomineralisation
in 6-year-old children. The generation R study. Retrieved from
http://dx.plos.org/10.1371/journal.pone.0091057
Erickson, P. R., & Mazhari, E. (1999). Investigation of the role of human breast milk in caries
development. Pediatric Dentistry, 21, 86–90.
Evans, E. W., Hayes, C., Palmer, C. A., Bermudez, O. I., Naumova, E. N., Cohen, S. A., &
Must, A. (2013). Development of a pediatric cariogenicity index. Journal of Public Health
Dentistry, 73(3), 179–186. https://doi.org/10.1111/jphd.12009

40
Evans, C.A. and Kleinman, D.V., 2000. The Surgeon General's report on America's oral health:
opportunities for the dental profession. The Journal of the American Dental Association,
131(12), pp.1721-1728.
Featherstone, J. D. (1999). Prevention and reversal of dental caries: role of low level fluoride.
Community Dentistry and Oral Epidemiology, 27(1), 31–40.
Featherstone, J. D. B. (2004). The continuum of dental caries—evidence for a dynamic disease
process. Journal of Dental Research, 83(suppl 1), C39–C42.
Fejerskov, O. (2004). Changing Paradigms in Concepts on Dental Caries: Consequences for
Oral Health Care. Caries Research, 38(3), 182–191.
Fejerskov, O., & Kidd, E. (2009). Dental caries: the disease and its clinical management. John
Wiley & Sons. Retrieved from
https://books.google.com.au/books?hl=en&lr=&id=fZfXWhSmG1UC&oi=fnd&pg=PR1&dq
=kidd+caries+cause&ots=OwH7O70sEI&sig=fjXX1b3C8PDUf8WgPAZOmEH0Fx0
Feldens, C. A., Rodrigues, P. H., de Anastácio, G., Vítolo, M. R., & Chaffee, B. W. (n.d.).
Feeding frequency in infancy and dental caries in childhood: a prospective cohort study.
International Dental Journal. 68(2), 113-121.
Feldens, C. A., Rodrigues, P. H., Rauber, F., Chaffee, B. W., & Vitolo, M. R. (2012). Food
expenditures, cariogenic dietary practices and childhood dental caries in southern Brazil.
Caries Research, 47(5), 373–381.
Fewtrell, M. S., Morgan, J. B., Duggan, C., Gunnlaugsson, G., Hibberd, P. L., Lucas, A., &
Kleinman, R. E. (2007). Optimal duration of exclusive breastfeeding: what is the evidence to
support current recommendations? The American Journal of Clinical Nutrition, 85(2), 635S –
638S.
Finlayson, T. L., Siefert, K., Ismail, A. I., & Sohn, W. (2007). Psychosocial factors and early
childhood caries among low-income African–American children in Detroit. Community
Dentistry and Oral Epidemiology, 35(6), 439–448.
Fonseca, M. A. da. (2017). Malnutrition and Oral Health in Children. Current Oral Health
Reports, 4(2), 92–96. https://doi.org/10.1007/s40496-017-0130-6
Fontana, M. (2015). The Clinical, Environmental, and Behavioral Factors That Foster Early
Childhood Caries: Evidence for Caries Risk Assessment. Pediatric Dentistry, 37(3), 217–225.
Fontana, M., Eckert, G.J., Keels, M.A., Jackson, R., Katz, B., Levy, B.T. and Levy, S.M., 2018.
Fluoride Use in Health Care Settings: Association with Children’s Caries Risk. Advances in
Dental Research, 29(1), pp.24-34.
Frazão, P. (2011). Effectiveness of the bucco-lingual technique within a school-based
supervised tooth-brushing program on preventing caries: a randomized controlled trial. BMC
Oral Health, 11(1), 11.
Frencken, J. E., de Amorim, R. G., Faber, J., & Leal, S. C. (2011). The Caries Assessment
Spectrum and Treatment (CAST) index: rational and development. International Dental
Journal, 61(3), 117–123.

41
Frencken, J. E., Peters, M. C., Manton, D. J., Leal, S. C., Gordan, V. V., & Eden, E. (2012).
Minimal intervention dentistry for managing dental caries–a review. International Dental
Journal, 62(5), 223–243.
Gatica, G., Barros, A.J., Madruga, S., Matijasevich, A. and Santos, I.S., 2012. Food intake
profiles of children aged 12, 24 and 48 months from the 2004 Pelotas (Brazil) birth cohort: an
exploratory analysis using principal components. International Journal of Behavioral Nutrition
and Physical Activity, 9(1), p.43.
Ghanim, A., Manton, D., Marino, R., Morgan, M., & Bailey, D. (2013). Prevalence of
demarcated hypomineralisation defects in second primary molars in Iraqi children.
International Journal of Paediatric Dentistry, 23(1), 48–55.
Gisselsson, H., Emilson, C.-G., Birkhed, D., & Björn, A.-L. (2005). Approximal caries
increment in two cohorts of schoolchildren after discontinuation of a professional flossing
program with chlorhexidine gel. Caries Research, 39(5), 350–356.
Gussy, M. G., Waters, E. G., Walsh, O., & Kilpatrick, N. M. (2006). Early childhood caries:
current evidence for aetiology and prevention. Journal of Paediatrics and Child Health, 42(1-
2), 37–43.
Hallett, K. B., & O’Rourke, P. K. (2003). Social and behavioural determinants of early
childhood caries. Australian Dental Journal, 48(1), 27–33.
Harrison, R., Benton, T., Everson-Stewart, S., & Weinstein, P. (2007). Effect of Motivational
Interviewing on Rates of Early Childhood Caries: A Randomized Trial. Pediatric Dentistry,
29(1), 16–22.
Harris, R., Nicoll, A. D., Adair, P. M., & Pine, C. M. (2004). Risk factors for dental caries in
young children: a systematic review of the literature. Community Dental Health, 21(1), 71–85.
Helen Keller International. (2015). Assessment of Promotion of Foods Consumed by Infants
and Young Children in Phnom Penh: Assessment and Research on Child Feeding (ARCH) –
Cambodia Country Report. Retrieved September 30, 2016, from http://archnutrition.org/wp-
content/uploads/2016/07/Assessment-of-Promotion-of-Foods-Consumed-by-Infants-and-
Young-Children-in-Phnom-Penh-2.pdf
Hölttä, P., & Alaluusua, S. (1992). Effect of supervised use of a fluoride toothpaste on caries
incidence in pre-school children. International Journal of Paediatric Dentistry, 2(3), 145–149.
Holve, S. (2008). An observational study of the association of fluoride varnish applied during
well child visits and the prevention of early childhood caries in American Indian children.
Maternal and Child Health Journal, 12(1), 64–67.
Hooley, M., Skouteris, H., Boganin, C., Satur, J., & Kilpatrick, N. (2012a). Body mass index
and dental caries in children and adolescents: a systematic review of literature published 2004
to 2011. Syst Rev, 1(1), 57.
Hooley, M., Skouteris, H., Boganin, C., Satur, J., & Kilpatrick, N. (2012b). Parental influence
and the development of dental caries in children aged 0–6 years: a systematic review of the
literature. Journal of Dentistry, 40(11), 873–885.

42
Hsieh, H.-J., Huang, S.-T., Tsai, C.-C., & Hsiao, S.-Y. (2014). Tooth-brushing habits and risk
indicators of severe early childhood caries among aboriginal Taiwanese. Asia-Pacific Journal
of Public Health, 26(3), 238–247.
Hu, X., Zhang, W., Fan, M., Mulder, J., & Frencken, J. E. (2016). Frequency of remnants of
sealants left behind in pits and fissures of occlusal surfaces after 2 and 3 years. Clinical Oral
Investigations, 1–7. https://doi.org/10.1007/s00784-016-1766-7
Iheozor-Ejiofor, Z., Worthington, H.V., Walsh, T., O'Malley, L., Clarkson, J.E., Macey, R.,
Alam, R., Tugwell, P., Welch, V. and Glenny, A.M., 2015. Cochrane Review of Water
Fluoridation. Fluoride, 48(3), p.269.
Ismail, A. I. (2003). Determinants of health in children and the problem of early childhood
caries. Pediatric Dentistry, 25(4), 328–333.
Ismail, A. I., Sohn, W., Tellez, M., Amaya, A., Sen, A., Hasson, H., & Pitts, N. B. (2007). The
International Caries Detection and Assessment System (ICDAS): an integrated system for
measuring dental caries. Community Dentistry and Oral Epidemiology, 35(3), 170–178.
Ismail, A. I., Tanzer, J. M., & Dingle, J. L. (1997). Current trends of sugar consumption in
developing societies. Community Dentistry and Oral Epidemiology, 25(6), 438–443.
Jackson Will, Kaliyann Thia, Moung Vandy, Putting the bite on ‘traditional dentists’, 27 March
2015, Phnom Penh Post: https://www.phnompenhpost.com/post-weekend/putting-bite-
traditional-dentists
Jamieson, L., Smithers, L., Hedges, J., Parker, E., Mills, H., Kapellas, K., Lawrence, H.P.,
Broughton, J.R. and Ju, X., 2018. Dental Disease Outcomes Following a 2-Year Oral Health
Promotion Program for Australian Aboriginal Children and Their Families: A 2-Arm Parallel,
Single-blind, Randomised Controlled Trial. EClinicalMedicine, 1, 43-50.
Jiang, E. M., Lo, E. C. M., Chu, C. H., & Wong, M. C. M. (2014). Prevention of early childhood
caries (ECC) through parental tooth-brushing training and fluoride varnish application: A 24-
month randomized controlled trial. Journal of Dentistry; Oxford, 42(12), 1543–1550.
https://doi.org/http://dx.doi.org.ezp.lib.unimelb.edu.au/10.1016/j.jdent.2014.10.002
Kaneilis, M. J. (2000). Caries risk assessment and prevention: strategies for Head Start, Early
Head Start, and WIC. Journal of Public Health Dentistry, 60(3), 210–217.
Ka, S., & Ca, P. (2012). Childhood dental caries and childhood obesity. Different problems
with overlapping causes. American Journal of Dentistry, 25(1), 59–64.
Kassebaum, N. J., Bernabé, E., Dahiya, M., Bhandari, B., Murray, C. J. L., & Marcenes, W.
(2015). Global Burden of Untreated Caries A Systematic Review and Metaregression. Journal
of Dental Research, 0022034515573272.
Kay, E. J., & Locker, D. (1996). Is dental health education effective? A systematic review of
current evidence. Community Dentistry and Oral Epidemiology, 24(4), 231–235.
https://doi.org/10.1111/j.1600-0528.1996.tb00850.x
Khitdee, C. (2017). The Epidemiology of Early Childhood Caries. Thai Dental Public Health
Journal, 22(supp 1).

43
Kidd, E. A. M., & Fejerskov, O. (2004). What constitutes dental caries? Histopathology of
carious enamel and dentin related to the action of cariogenic biofilms. Journal of Dental
Research, 83(suppl 1), C35–C38.
Klock, B., & Krasse, B. (1979). A comparison between different methods for prediction of
caries activity. European Journal of Oral Sciences, 87(2), 129–139.
https://doi.org/10.1111/j.1600-0722.1979.tb00664.x
Kowash, M. B., Pinfield, A., Smith, J., & Curzon, M. E. J. (2000). Dental health education:
effectiveness on oral health of a long-term health education programme for mothers with young
children. British Dental Journal, 188(4), 201–205.
K Pattanaporn, P. S. (2012). Mode of delivery, mutans streptococci colonization, and early
childhood caries in three- to five-year-old Thai children. Community Dentistry and Oral
Epidemiology, 41(3). https://doi.org/10.1111/cdoe.12013
Kuthy, R. A., Siegal, M. D., & Wulf, C. A. (1997). Establishing maternal and child health data
collection priorities for state and local oral health programs. Journal of Public Health Dentistry,
57(4), 197–205.
Leme, A. P., Koo, H., Bellato, C. M., Bedi, G., & Cury, J. A. (2006). The role of sucrose in
cariogenic dental biofilm formation—new insight. Journal of Dental Research, 85(10), 878–
887.
Lippert, F., Hara, A. T., Martinez-Mier, E. A., & Zero, D. T. (2014). Laboratory Investigations
Into the Potential Anticaries Efficacy of Fluoride Varnishes. Pediatric Dentistry, 36(4), 291–
295.
Li, Y., & Caufield, P. W. (1995). The fidelity of initial acquisition of mutans streptococci by
infants from their mothers. Journal of Dental Research, 74(2), 681–685.
Lönnerdal, B. (2003). Nutritional and physiologic significance of human milk proteins. The
American Journal of Clinical Nutrition, 77(6), 1537S – 1543S.
Lopez, L., Berkowitz, R., Spiekerman, C., & Weinstein, P. (2002). Topical antimicrobial
therapy in the prevention of early childhood caries: a follow-up report. Pediatric Dentistry,
24(3), 204–206.
Ludwig, D. S., & Nestle, M. (2008). Can the food industry play a constructive role in the
obesity epidemic? Journal of American Medical Association, 300(15), 1808–1811.
Lustig, R. H., Schmidt, L. A., & Brindis, C. D. (2012). Public health: The toxic truth about
sugar. Nature, 482(7383), 27–29.
Macintosh, A. C., Schroth, R. J., Edwards, J., Harms, L., Mellon, B., & Moffatt, M. (2010).
The impact of community workshops on improving early childhood oral health knowledge.
Pediatric Dentistry, 32(2), 110–117.
Mackay, T.D. and Thomson, W., 2005. Enamel defects and dental caries among Southland
children. New Zealand Dental Journal, 101(2), pp.35-43.

44
Marcenes, W., Kassebaum, N. J., Bernabé, E., Flaxman, A., Naghavi, M., Lopez, A., &
Murray, C. J. L. (2013). Global Burden of Oral Conditions in 1990-2010 A Systematic
Analysis. Journal of Dental Research, 0022034513490168.
Marghalani, A. A., Guinto, E., Phan, M., Dhar, V., & Tinanoff, N. (2017). Effectiveness of
Xylitol in Reducing Dental Caries in Children. Pediatric Dentistry, 39(2), 103–110.
Marinho, V. C., Higgins, J., Logan, S., & Sheiham, A. (2003). Fluoride toothpastes for
preventing dental caries in children and adolescents. The Cochrane Library. Retrieved from
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD002278/full
Marriott, B. P., White, A., Hadden, L., Davies, J. C., & Wallingford, J. C. (2012). World Health
Organization (WHO) infant and young child feeding indicators: associations with growth
measures in 14 low-income countries. Maternal & Child Nutrition, 8(3), 354–370.
https://doi.org/10.1111/j.1740-8709.2011.00380.x
Martins-Júnior, P. A., Vieira-Andrade, R. G., Corrêa-Faria, P., Oliveira-Ferreira, F., Marques,
L. S., & Ramos-Jorge, M. L. (2013). Impact of early childhood caries on the oral health-related
quality of life of preschool children and their parents. Caries Research, 47(3), 211–218.
Marya, C. M., Ashokkumar, B. R., Dhingra, S., Dahiya, V., & Gupta, A. (2012). Exposure to
High-Fluoride Drinking Water and Risk of Dental Caries and Dental Fluorosis in Haryana,
India. Asia-Pacific Journal of Public Health, 1010539512460270.
Matsuoka, S., Obara, H., Nagai, M., Murakami, H., & Lon, R. C. (2013). Performance-based
financing with GAVI health system strengthening funding in rural Cambodia: a brief
assessment of the impact. Health Policy and Planning, czt030.
https://doi.org/10.1093/heapol/czt030
Medeiros, P. B., Otero, S. A., Frencken, J. E., Bronkhorst, E. M., & Leal, S. C. (2015).
Effectiveness of an oral health program for mothers and their infants. International Journal of
Paediatric Dentistry, 25(1), 29–34.
Memarpour M, Fakhraei E, Dadaein S, Vossoughi M. Efficacy of Fluoride Varnish and Casein
Phosphopeptide-Amorphous Calcium Phosphate for Remineralization of Primary Teeth: A
Randomized Clinical Trial. Med Princ Pract. 2015 May;24(3):231–7. Menon. (n.d.). Parental
stress as a predictor of early childhood caries among preschool children in India. International
Journal of Paediatric Dentistry, 23(3), 160–165. https://doi.org/10.1111/j.1365-
263X.2012.01238.x
Ministry of Health. 2010. Our Oral Health: Key findings of the 2009 New Zealand Oral Health
Survey. Wellington: Ministry of Health
Mitchell, S. C., Ruby, J. D., Moser, S., Momeni, S., Smith, A., Osgood, R., Childers, N. (2009).
Maternal transmission of mutans streptococci in severe-early childhood caries. Pediatric
Dentistry, 31(3), 193.
Moffat, S. M., Foster Page, L. A., & Thomson, W. M. (2017). New Zealand’s School Dental
Service over the Decades: Its Response to Social, Political, and Economic Influences, and the
Effect on Oral Health Inequalities. Frontiers in Public Health, 5, 177.
https://doi.org/10.3389/fpubh.2017.00177

45
Monse, B., Heinrich-Weltzien, R., Benzian, H., Holmgren, C., & van Palenstein Helderman,
W. (2010). PUFA–An index of clinical consequences of untreated dental caries. Community
Dentistry and Oral Epidemiology, 38(1), 77–82.
Moodie, R., Stuckler, D., Monteiro, C., Sheron, N., Neal, B., Thamarangsi, T., (2013). Profits
and pandemics: prevention of harmful effects of tobacco, alcohol, and ultra-processed food and
drink industries. The Lancet, 381(9867), 670–679.
Moore, D., Poynton, M., Broadbent, J. M., & Thomson, W. M. (2017). The costs and benefits
of water fluoridation in NZ. BMC Oral Health, 17(1), 134. https://doi.org/10.1186/s12903-
017-0433-y
Muñoz-Millán, P., Zaror, C., Espinoza-Espinoza, G., Vergara-Gonzalez, C., Muñoz, S., Atala-
Acevedo, C., & Martínez-Zapata, M. J. (2018). Effectiveness of fluoride varnish in preventing
early childhood caries in rural areas without access to fluoridated drinking water: A randomized
control trial. Community Dentistry and Oral Epidemiology, 46(1), 63–69.
https://doi.org/10.1111/cdoe.12330
National Institute of Statistics, Directorate General for Health, and ICF International (2015).
Cambodia Demographic and Health Survey 2014. Phnom Penh, Cambodia, and Rockville,
Maryland, USA: National Institute of Statistics, Directorate General for Health, and ICF
International.
Neves, P. A. M., Ribeiro, C. C. C., Tenuta, L. M. A., Leitão, T. J., Monteiro-Neto, V., Nunes,
A. M. M., & Cury, J. A. (2016). Breastfeeding, Dental Biofilm Acidogenicity, and Early
Childhood Caries. Caries Research, 50(3), 319–324. https://doi.org/10.1159/000445910
Newbrun, E., 2004. Systemic benefits of fluoride and fluoridation. Journal of Public Health
Dentistry, 64, pp.35-39.
Nguon S and Kay K (2008); Cambodia Opens Wide for Dental Tourism Phnom Penh Post
(http://www.phnompenhpost.com/national/cambodia-opens-wide-dental-tourism accessed on
15 October 2015)
Nongonierma, A. B., & FitzGerald, R. J. (2012). Biofunctional properties of
caseinophosphopeptides in the oral cavity. Caries Research, 46(3), 234–267.
Nunes, A. M. M., Alves, C. M. C., Borba de Araújo, F., Ortiz, T. M. L., Ribeiro, M. R. C.,
Silva, A. A. M. da, & Ribeiro, C. C. C. (2012). Association between prolonged breast-feeding
and early childhood caries: a hierarchical approach. Community Dentistry and Oral
Epidemiology, 40(6), 542–549. https://doi.org/10.1111/j.1600-0528.2012.00703.x
Nyvad, B., Crielaard, W., Mira, A., Takahashi, N., & Beighton, D. (2013). Dental Caries from
a Molecular Microbiological Perspective. Caries Research, 47(2), 89–102.
https://doi.org/http://dx.doi.org.ezp.lib.unimelb.edu.au/10.1159/000345367
Okada, M., Kawamura, M., Kaihara, Y., Matsuzaki, Y., Kuwahara, S., Ishidori, H., & Miura,
K. (2002). Influence of parents’ oral health behaviour on oral health status of their school
children: an exploratory study employing a causal modelling technique. International Journal
of Paediatric Dentistry, 12(2), 101–108. https://doi.org/10.1046/j.1365-263X.2002.00338.x
46
Oliveira, B. H., Salazar, M., Carvalho, D. M., Falcão, A., Campos, K., & Nadanovsky, P.
(2014). Biannual Fluoride Varnish Applications and Caries Incidence in Preschoolers: A 24-
month Follow-Up Randomized Placebo-Controlled Clinical Trial. Caries Research, 48(3),
228–236. https://doi.org/10.1159/000356863
Oral health Bureau, Department of Preventive Medicine, Ministry of Health Cambodia (2014)
Final report of the 2011 Cambodia National Oral Health Survey
Peltzer, K., & Mongkolchati, A. (2015). Severe early childhood caries and social determinants
in three-year-old children from Northern Thailand: a birth cohort study. BMC Oral Health,
15(1), 108.
Peres, K. G., Nascimento, G. G., Peres, M. A., Mittinty, M. N., Demarco, F. F., Santos, I. S.,
Barros, A. J. D. (2017). Impact of Prolonged Breastfeeding on Dental Caries: A Population-
Based Birth Cohort Study. Pediatrics, 140(1), e20162943. https://doi.org/10.1542/peds.2016-
2943
Petersen, P. E. (2003). The World Oral Health Report 2003: continuous improvement of oral
health in the 21st century–the approach of the WHO Global Oral Health Programme.
Community Dentistry and Oral Epidemiology, 31(s1), 3–24.
Petersen, P. E., Bourgeois, D., Ogawa, H., Estupinan-Day, S., & Ndiaye, C. (2005). The global
burden of oral diseases and risks to oral health. Bulletin Of The World Health Organization,
83(9), 661–669.
Petersen, P. E., & Lennon, M. A. (2004). Effective use of fluorides for the prevention of dental
caries in the 21st century: the WHO approach. Community Dentistry and Oral Epidemiology,
32(5), 319–321.
Petersen, P. E., & Ogawa, H. (2016). Prevention of dental caries through the use of fluoride–
the WHO approach. Community Dental Health, 33(2), 66–68.
Pithon, M. M., dos Santos, M. J., Andrade, C. S., Leão Filho, J. C. B., Braz, A. K. S., de Araujo,
R. E., Maia, L. C. (2015). Effectiveness of varnish with CPP–ACP in prevention of caries
lesions around orthodontic brackets: an OCT evaluation. The European Journal of
Orthodontics, 37(2), 177–182.
Plonka, K. A., Pukallus, M. L., Holcombe, T. F., Barnett, A. G., Walsh, L. J., & Seow, W. K.
(2013). A randomized controlled clinical trial comparing a remineralizing paste with an
antibacterial gel to prevent early childhood caries. Pediatric Dentistry, 35(1), e8–e12.
Popkin, B. M., & Nielsen, S. J. (2003). The Sweetening of the World’s Diet. Obesity Research,
11(11), 1325–1332. https://doi.org/10.1038/oby.2003.179
Pukallus, M. L., Plonka, K. A., Holcombe, T. F., Barnett, A. G., Walsh, L. J., & Seow, W. K.
(2013). A Randomized Controlled Trial of a 10 Percent CPP-ACP Cream to Reduce Mutans
Streptococci Colonization. Pediatric Dentistry, 35(7), 550–555.
Quinonez, R. B., Keels, M. A., Vann Jr, W. F., McIver, F. T., Heller, K., & Whitt, J. K. (2000).
Early childhood caries: analysis of psychosocial and biological factors in a high-risk
population. Caries Research, 35(5), 376–383.

47
Rasbridge, L. A., & Kulig, J. C. (1995). Infant feeding among Cambodian refugees. MCN: The
American Journal of Maternal/Child Nursing, 20(4), 213–218.
Ribeiro, N. M., & Ribeiro, M. A. (2004). Breastfeeding and early childhood caries: a critical
review. Jornal de Pediatria, 80(5), s199–s210.
Ribeiro, T. R., Dria, K. J., de Carvalho, C. B. M., Monteiro, A. J., Fonteles, M. C., de Moraes
Carvalho, K., & Fonteles, C. S. R. (2013). Salivary peptide profile and its association with
early childhood caries. International Journal of Paediatric Dentistry, 23(3), 225–234.
https://doi.org/10.1111/j.1365-263X.2012.01258.x
Rong, W. S., Bian, J. Y., Wang, W. J., & De Wang, J. (2003). Effectiveness of an oral health
education and caries prevention program in kindergartens in China. Community Dentistry and
Oral Epidemiology, 31(6), 412–416.
Ruby, J., & Goldner, M. (2007). Nature of symbiosis in oral disease. Journal of Dental
Research, 86(1), 8–11.
Rugg-Gunn, A. J., Spencer, A. J., Whelton, H. P., Jones, C., Beal, J. F., Castle, P., Lennon, M.
A. (2016). Critique of the review of’Water fluoridation for the prevention of dental caries’
published by the Cochrane Collaboration in 2015. British Dental Journal, 220(7), 335–340.
Salone, L. R., Vann, W. F., & Dee, D. L. (2013). Breastfeeding: an overview of oral and general
health benefits. The Journal of the American Dental Association, 144(2), 143–151.
Schluter, P. J., Durward, C., Cartwright, S., & Paterson, J. (2007). Maternal Self-Report of Oral
Health in 4-Year-Old Pacific Children from South Auckland, New Zealand: Findings from the
Pacific Islands Families Study. Journal of Public Health Dentistry, 67(2), 69–77.
Schroth, R. J., Harrison, R. L., & Moffatt, M. E. (2009). Oral health of indigenous children and
the influence of early childhood caries on childhood health and well-being. Pediatric Clinics
of North America, 56(6), 1481–1499.
Selwitz, R. H., Ismail, A. I., & Pitts, N. B. (2007). Dental caries. The Lancet, 369(9555), 51–
59.
Senarath, U., Dibley, M. J., & Agho, K. E. (2010). Factors associated with nonexclusive
breastfeeding in five East and Southeast Asian countries: a multilevel analysis. Journal of
Human Lactation. Retrieved from
http://jhl.sagepub.com/content/early/2010/01/28/0890334409357562.abstract
Serwint, J. R., Mungo, R., Negrete, V. F., Duggan, A. K., & Korsch, B. M. (1993). Child-
rearing practices and nursing caries. Pediatrics, 92(2), 233–237.
Shearer, D. M., Thomson, W. M., Broadbent, J. M., & Poulton, R. (2011). Maternal oral health
predicts their children’s caries experience in adulthood. Journal of Dental Research, 90(5),
672–677.
Sheiham, A., & James, W. P. T. (2015). Diet and Dental Caries The Pivotal Role of Free Sugars
Reemphasized. Journal of Dental Research, 0022034515590377.
https://doi.org/10.1177/0022034515590377

48
Silva, M.J., Scurrah, K.J., Craig, J.M., Manton, D.J. and Kilpatrick, N., 2016. Etiology of molar
incisor hypomineralization–A systematic review. Community Dentistry and Oral
Epidemiology, 44(4), pp.342-353.
Silver, M. (2015). Guess Which Country Has The Biggest Increase In Soda Drinking. Retrieved
June 25, 2015, from http://www.npr.org/sections/goatsandsoda/2015/06/19/415223346/guess-
which-country-has-the-biggest-increase-in-soda-drinking
Simonsen, R.J. and Neal, R.C., 2011. A review of the clinical application and performance of
pit and fissure sealants. Australian Dental Journal, 56, pp.45-58.
Sisson, K. L. (2007). Theoretical explanations for social inequalities in oral health. Community
Dentistry and Oral Epidemiology, 35(2), 81–88. https://doi.org/10.1111/j.1600-
0528.2007.00354.x
Sjögren, K., Birkhed, D., & Rangmar, B. (1995). Effect of a modified toothpaste technique on
approximal caries in preschool children. Caries Research, 29(6), 435–441.
Smith, R. E., Badner, V. M., Morse, D. E., & Freeman, K. (2002). Maternal risk indicators for
childhood caries in an inner city population. Community Dentistry and Oral Epidemiology,
30(3), 176–181. https://doi.org/10.1034/j.1600-0528.2002.300303.x
Steffensen, J. E. (1990). Literature and concept review: issues in maternal and child oral health.
Journal of Public Health Dentistry, 50(6), 358–369.
Strangio, S. (2014). Hun Sen’s Cambodia. Yale University Press. Retrieved from
https://books.google.com.au/books?hl=en&lr=&id=xRY2BQAAQBAJ&oi=fnd&pg=PR1&d
q=Hun+sens+cambodia&ots=ecRAws6gtg&sig=jEMPiy2aHhZ-DjDc3hcKFF-LZkw
Tac N, Turton B, Durward C (2016) Retention of Glass Ionomer Cement tissure sealant using
a revised protocol Cambodian Dental Journal 12, 14-18.
Tahmassebi, J. F., Duggal, M. S., Malik-Kotru, G., & Curzon, M. E. J. (2006). Soft drinks and
dental health: a review of the current literature. Journal of Dentistry, 34(1), 2–11.
Tang, C., Quinonez, R. B., Hallett, K., Lee, J. Y., & Kenneth Whitt, J. (2005). Examining the
association between parenting stress and the development of early childhood caries.
Community Dentistry and Oral Epidemiology, 33(6), 454–460.
Thitasomakul, S., Piwat, S., Thearmontree, A., Chankanka, O., Pithpornchaiyakul, W., &
Madyusoh, S. (2009). Risks for early childhood caries analyzed by negative binomial models.
Journal of Dental Research, 88(2), 137–141.
Tickle, M., O’Neill, C., Donaldson, M., Birch, S., Noble, S., Killough, S. Verghis, R. (2017).
A randomized controlled trial of caries prevention in dental practice. Journal of Dental
Research, 0022034517702330.
Tinanoff, N., Kanellis, M. J., & Vargas, C. M. (2002). Current understanding of the
epidemiology, mechanisms, and prevention of dental caries in preschool children. Pediatric
Dentistry, 24(6), 543–551.

49
Tinanoff, N. and Reisine, S., 2009. Update on early childhood caries since the Surgeon
General's Report. Academic pediatrics, 9(6), pp.396-403.
Tjäderhane, L., Nascimento, F. D., Breschi, L., Mazzoni, A., Tersariol, I. L. S., Geraldeli, S.,
Pashley, D. H. (2013). Optimizing dentin bond durability: Control of collagen degradation by
matrix metalloproteinases and cysteine cathepsins. Dental Materials, 29(1), 116–135.
https://doi.org/10.1016/j.dental.2012.08.004
Turton, B. J., Thomson, W. M., Foster Page, L. A., Saub, R., & Ishak, A. R. (2015).
Responsiveness of the Child Perceptions Questionnaire 11–14 for Cambodian children
undergoing basic dental care. International Journal of Paediatric Dentistry, 25(1), 2–8.
Turton, B. J., Thomson, W. M., Page, L. A. F., Saub, R. B., & Razak, I. A. (2015). Validation
of an Oral Health–Related Quality of Life Measure for Cambodian Children. Asia-Pacific
Journal of Public Health, 27(2), NP2339–NP2349.
Twetman, S. (2008). Prevention of Early Childhood Caries (ECC) Review of literature
published 1998–2007. European Archives of Paediatric Dentistry, 9(1), 12–18.
Tyas, M. J., Anusavice, K. J., Frencken, J. E., & Mount, G. J. (2000). Minimal intervention
dentistry—a review*. International Dental Journal, 50(1), 1–12.
USAID Assist Project. (2014) Strengthening health professionals regulation in Cambodia.
[ONLINE] Available from: https://www.usaidassist.org/sites/assist/files
/strengthening_health_professions_regulation_in_cambodia_-_fact_sheet_30_sept_2014_
english_0.pdf [accessed on 15 October 2015]
Valaitis, R., Hesch, R., Passarelli, C., Sheehan, D., & Sinton, J. (1999). A systematic review
of the relationship between breastfeeding and early childhood caries. Canadian Journal of
Public Health= Revue Canadienne de Sante Publique, 91(6), 411–417.
Vann, W. F., Lee, J. Y., Baker, D., & Divaris, K. (2010). Oral Health Literacy among Female
Caregivers Impact on Oral Health Outcomes in Early Childhood. Journal of Dental Research,
89(12), 1395–1400.
van Palenstein Helderman, W. H., Soe, W., & Van’t Hof, M. A. (2006). Risk factors of early
childhood caries in a Southeast Asian population. Journal of Dental Research, 85(1), 85–88.
Wan, A. K. L., Seow, W. K., Purdie, D. M., Bird, P. S., Walsh, L. J., & Tudehope, D. I. (2001).
Oral colonization of Streptococcus mutans in six-month-old predentate infants. Journal of
Dental Research, 80(12), 2060–2065.
Wan, A. K. L., Seow, W. K., Purdie, D. M., Bird, P. S., Walsh, L. J., & Tudehope, D. I. (2003).
A longitudinal study of Streptococcus mutans colonization in infants after tooth eruption.
Journal of Dental Research, 82(7), 504–508.
Weintraub, J. A., Ramos-Gomez, F., Jue, B., Shain, S., Hoover, C. I., Featherstone, J. D. B., &
Gansky, S. A. (2006). Fluoride Varnish Efficacy in Preventing Early Childhood Caries. Journal
of Dental Research, 85(2), 172–176. https://doi.org/10.1177/154405910608500211
World Health Organization (2013) Oral health surveys: basic methods - 5th edition. Sao Paulo,
Brazil, University of Sao Paulo.

50
World Health Organisation. (2004) International immunisation framework. [Online] Available
from: www.who.int/immunization/.../NUVI_Impact_on_IS_H_FrameworkRefs. [Accessed 5
Sept 2015]
World Health Organization. (2012) Health service delivery profile Cambodia. [Online]
Available from: http://www.wpro.who.int/health_services/
service_delivery_profile_cambodia.pdf. [Accessed 12 March 2018]
World Health Organization (2015) Guideline: Sugars intake for adults and children. [Online]
Available from: http://apps.who.int/iris/handle/10665/149782 [Accessed 17 May 2016]
World Health Organization (2003) Global strategy for infant and young child feeding. [Online]
Available from:
https://books.google.com/books?hl=en&lr=&id=biABXOXrajYC&oi=fnd&pg=PR4&dq=wh
o+reccomendation+infant+nutrition%5C&ots=1lC0e8b_RI&sig=JIuxNFypdzeuYUvC03q-
sJ-4now [Accessed 7 May 2018]
World Health Organization (2017) Noncommunicable diseases: progress monitor 2017.
Geneva: World Health Organization.
Wong, M., Glenny, A.-M., Tsang, B. W., Lo, E., Worthington, H. V., & Marinho, V. C. (2011).
Cochrane review: Topical fluoride as a cause of dental fluorosis in children. Evidence-Based
Child Health: A Cochrane Review Journal, 6(2), 388–439.
Wong, P. D., Birken, C. S., Parkin, P. C., Venu, I., Chen, Y., Schroth, R. J., & Maguire, J. L.
(2017). Total Breast-Feeding Duration and Dental Caries in Healthy Urban Children. Academic
Pediatrics, 17(3), 310–315. https://doi.org/10.1016/j.acap.2016.10.021
Wright, J. T., Hanson, N., Ristic, H., Whall, C. W., Estrich, C. G., & Zentz, R. R. (2014).
Fluoride toothpaste efficacy and safety in children younger than 6 years: a systematic review.
The Journal of the American Dental Association, 145(2), 182–189.
Wright, J. T., Tampi, M. P., Graham, L., Estrich, C., Crall, J. J., Fontana, M., (2016). Sealants
for preventing and arresting pit-and-fissure occlusal caries in primary and permanent molars:
a systematic review of randomized controlled trials—a report of the American Dental
Association and the American Academy of Pediatric Dentistry. The Journal of the American
Dental Association, 147(8), 631–645.
Yang, F., Zeng, X., Ning, K., Liu, K.-L., Lo, C.-C., Wang, W., Chang, X. (2012). Saliva
microbiomes distinguish caries-active from healthy human populations. The ISME Journal,
6(1), 1.
Zhao, I.S., Gao, S.S., Hiraishi, N., Burrow, M.F., Duangthip, D., Mei, M.L., Lo, E.C.M. and
Chu, C.H., 2018. Mechanisms of silver diamine fluoride on arresting caries: a literature review.
International Dental Journal, 68(2), pp.67-76.
Zhi, Q. H., Lo, E. C. M., & Lin, H. C. (2012). Randomized clinical trial on effectiveness of
silver diamine fluoride and glass ionomer in arresting dentine caries in preschool children.
Journal of Dentistry, 40(11), 962–967.
48
Chapter 2
A GIC Fissure Protection intervention in Cambodia – 12 month
results and Pilot Study
Published in part as: Tac N, Turton B, Durward C (2016) Retention of Glass Ionomer
Cement tissue sealant using a revised protocol Cambodian Dental Journal 12, 14-18.
Presented in part as:
Turton B, Durward C, Bach K, Manton D. (2014) Seal Cambodia – 60,000 children over 3
years; IADR SEA 28TH Annual meeting, Kutching, Malaysia.
Tak N, Turton B, Durward C. (2015) Seal Cambodia – A comparison of two protocols; IADR
SEA 29th Annual meeting, Bali, Indonesia.
Turton B, Durward C. (2015) Seal Cambodia – Placing fissure protection in a community
setting successfully; FDI World Congress, Bangkok, Thailand.

49
Abstract
Objective: To compare two different protocols for the placement of hand-mixed GIC Fissure
Protection (FP) placed on FPM of 6 to 8 year-old Cambodian children as part of the SEAL
Cambodia Project.
Methods: The study had two pilots: Pilot A, a one-year evaluation of the original cohort and
protocol; and Pilot B a one-year evaluation of a new protocol. Pilot A included a cohort of
children who received FP using the original protocol (Group A), along with a matched control
group (Group B) who did not receive FP. Pilot B involved two convenience samples of children
who were recruited based on the routine schedule of schools to be sealed as part of the wider
Seal Cambodia Project. One group received FP using the modified protocol (Group C) while
the other received FP using the original protocol (Group D). The modified protocol involved
control of the temperature of the material, the timing of mixing, and placement.
Results: Pilot A achieved a 61% follow-up rate with 26.8% retention and 10% preventive
increment at 1-year. Pilot B achieved an 86% follow-up rate, with 67.1% retention rate at 6-
months.
Conclusion: The protocol associated with Pilot B achieved a higher sealant retention rate and
should be adopted at scale across the SEAL Cambodia project.
50
2.0 Chapter 2 – The SEAL Cambodia pilot studies
Dental caries experience in Cambodia is severe and the services available to manage the burden
of disease are limited. The very low ‘filled’ (<1%) component of the dmft/DMFT reported in
the 2011 CNOHS reported that most Cambodian children had not received prior dental
treatment (Chher et al. 2016). Therefore, if a carious lesion develops, it is likely that no
operative treatment would be received, and eventually the tooth (often associated with pain and
infection) could require extraction. It is clear that the drivers of the severe caries experience in
Cambodia are behavioural and mediated through late oral hygiene practices and unfavourable,
high added sugar diets (Chher et al. 2016). Although the aetiological factors of the caries
process might be shared among other high caries groups, few interventional studies in settings
similar to Cambodia have been published. Therefore, it is important to establish evidence for
the most effective and efficient preventive techniques in a Cambodian environment (Chher et
al. 2009). This involves selection of the best techniques as well as the most appropriate
logistical models for delivery. These concepts are influenced by the limited resources and the
ubiquitous distribution of disease across the population.
In the case of Cambodia, dental caries affects the majority of young children, with 97% of 6
year-old children having one or more cavitated lesions, and 86% having one or more pulpally
involved teeth. The disease is more severe in urban areas, especially the Phnom Penh and
Kampot provinces (Chher et al. 2016). When considering a population-wide intervention, the
general options are to consider either a targeted approach or a whole population approach.
Targeted approaches are most appropriate when the burden of disease sits within limited
subsections of the community, such is the case in more developed settings, and documented in
New Zealand and Australia with the lift-the-lip campaign, Scotland with the Child Smile
project, and the USA with the well child program (Chia et al. 2015; Lam et al. 2012;
Macpherson et al. Anopa et al. 2013; Holve, 2008).
In Cambodia, the near universal caries experience justifies a ‘whole population’ approach. In
terms of the methods available to prevent dental caries, the best evidence supports tooth-
brushing with fluoride toothpaste, placement of fissure sealants, and professional topical
fluoride placement. Daily tooth-brushing with fluoride toothpaste can reduce dental caries
incidence by between 20-40% (Marinho et al. 2003). Fissure protection with both glass
ionomer cement and resin-based sealants has been reported to prevent new carious lesions on
FPM by up to 80% over 3 y (Ahovuo-Saloranta et al. 2016). Studies on fluoride varnish are
51
extensive and systematic analysis suggests that applications 2 to 3 times-per-year can reduce
caries experience by up to 40% (Agouropoulos et al. 2014). Each of these approaches have
implications for the structure of how services are delivered.
2.0.1 The ‘birth’ of the SEAL Cambodia Community Project
In 2011 the Global Child Dental Fund (GCDF), an international charity focused on oral health,
initiated a meeting of local and international dental specialists to consider which technologies
and which organisational structures might be appropriate for addressing the high rate of dental
caries in Cambodian children. There was consensus to move away from extraction-based
‘bottom of the cliff’ interventions, and towards “upstream” interventions to prevent carious
lesions developing. The GCDF Taskforce was formed in Cambodia, which included oral health
stakeholders from the Ministry of Health, The Cambodian Dental Association, Non-
Governmental Organisations (NGOs), and local and international universities, and gave its
strong support to this innovative child oral health project. Out of that taskforce the ‘SEAL
Cambodia’ Community Project was born. The rationale of SEAL Cambodia was that if most
of the new lesions in the permanent dentition occurring between 6 to 8 years-of-age were
occurring on FPM, then targeting those teeth would reduce the overall burden of caries during
the primary school years and into adolescence. The delivery of services in a school setting
rather than a community setting was deemed to be more cost-effective and targeted. And along
with the logistical benefit, it also offered a way to reorientate local and visiting volunteers to
participate in a dental intervention which was focused on upstream intervention such as
prevention.
The GCDF Task force set out a plan to engage local and international partners in providing a
proven preventive intervention for young children, which could serve as a demonstration model
of care in a developing world setting. A target was set for placing FP on the FPM of 60,000 6
to 8 year-old children with GIC over a three year period. Sponsorship for the project was
obtained from GCDF, CamKids (the Cambodian Children’s Charity) and GC Asia (which also
donated the GIC sealant material Fuji VII). The project was accepted and approved by the
Ministry of Health (MOH), and the Ministry of Education, Youth and Sport (MOEYS). The
Australia and New Zealand Society of Paediatric Dentistry (ANZSPD) also made a donation
in the first year enabling the purchase of a tuk tuk (motorcycle pulled passenger trailer) to
transport local and overseas volunteers to the schools around Phnom Penh to provide FP.

52
Although there is a lot of evidence to support the use of GIC fissure sealants, no research is
available for the efficacy of FS in a population with such extreme caries experience as
Cambodia. The ART technique was chosen for placement of FS and most studies that
investigated the use of that technique used high viscosity GIC such as Fuji IX® (GC Corp,
Tokyo, Japan) or Ketac Fil® (3MTM ESPETM) as recommended in the original paper (de
Amorim et al. 2012). In contrast, SEAL Cambodia planned a low viscosity GIC (Fuji VII®, GC
Corp, Tokyo, Japan) which was designed specifically for fissure protection. Fuji VII® releases
more fluoride than higher viscosity GIC materials, is said to flow more readily into fissure
systems and is more moisture tolerant, making it more suitable for placement on partially
erupted teeth (Ganesh & Tandon 2007). The disadvantage is that Fuji VII® has a lower
compressive strength, although, this is less important in a sealant scenario. Another concern
around using a low viscosity GIC was that the Fuji III® precursor to Fuji VII® showed very
limited retention with just one in six sealants being retained over two years in previous studies
(Fross et al. 1994; Poulsen et al. 2001). Given that individuals targeted by the SEAL Cambodia
project were a distinctive population with an extreme caries experience and almost no access
to dental care, and that there were some special considerations around material choice, it was
prudent to closely monitor clinical outcomes including both caries prevention and retention of
sealant material order to ensure that the most reasonable outcomes were being achieved.

53
2.1 Aim
To evaluate two different protocols for the placement of FS and the prevention of dental caries
in the FPM of 6 to 8 year-old children in three provinces of Cambodia.
2.2 Objective
To evaluate the caries preventive effect and retention, respectively, of FS placed using different
protocols in two pilot samples taken from within the SEAL Cambodia Project.

54
2.3 Methods
The study reports on two pilot studies that are quasi-randomised control trials: Pilot A, a one
year evaluation of the original cohort and protocol; and Pilot B, a one year evaluation of a new
protocol. Each pilot examined a different clinical protocol to assess: caries prevention in the
case of Pilot A; and improvement in the retention in the case of Pilot B. All clinical
examinations and clinical procedures were conducted in a school yard setting with battery
powered lights and children in a supine position. Consent was gained by sending the consent
forms to the school the week prior to the examination, and parents were given an opportunity
to withdraw their child’s participation should they wish (Appendix 1). Children were free to
refuse assent at the time of examination with no consequences. Participants were given oral
hygiene education with a ratio of one instructor to five children and they were given a
toothbrush prior to the placement of the sealants, or following the examination for those in the
control group. This ensured that the teeth were clean prior to examination and placement of
GIC sealants. Children were also sent home with an information sheet (Appendix 2) after
participating to inform the parents of the need for additional dental treatment where
appropriate. Ethics approval was provided by the National Committee for Health Research,
Ministry of Health, Cambodia.
2.3.1 Selection of teeth for FS
The occlusal surfaces of FPM were checked visually to detect the presence of cavitated carious
lesions. Sealants were only applied to partially or fully erupted, non-cavitated FPM including
those with staining or early carious lesions (but no underlying enamel shadow). Sealants were
placed by a mix of Cambodian Dental students, foreign dental students and dental therapy
students, as well as Cambodian and Foreign dentists.
2.3.2 Pilot A – one year evaluation of the original cohort
The first pilot involved a representative sample of 433 children selected using randomised
cluster selection at class level from the population eligible to participate in the SEAL Cambodia
project who made up the ‘intervention’ group (Group A). The control group consisted of 249
children from schools that were not included in the project (Group B). The clinical procedure
for placement of FS was as follows, with up to two teeth (opposing arches) treated
simultaneously (1) the dentine conditioner was applied to a clean tooth and then removed with
a wet cotton pellet; (2) the tooth was dried using cotton pellets; (3) hand-mixed Fuji VII® was

55
placed onto the occlusal surface of the tooth and pressed into the fissures using the operators’
finger (no defined duration) which was lubricated with cocoa butter or Vaseline (Unilever,
USA) and no subsequent occlusal adjustment.
2.3.2.1 Clinical examination at baseline and one year follow-up
Six examiners were calibrated prior to undertaking examinations (ICC >0.85). Teeth were
scored using the methods described in the ‘WHO basic survey methods’ book. Two indices
were used: the DMF index at surface level (WHO 2013); in addition, each tooth was given a
score using the PUFA Index (Monse et al. 2010). The clinical documentation used is included
in Appendix 3 and 4. Participants were divided into terciles based on caries experience as
consistent with the significant caries index (Bratthall 2000) to define those in ‘high’, ‘very
high’, and ‘extreme’ caries groups.
Evaluation of FS was based on the proportion of material that was remaining. FS that covered
more than 2/3 of the fissure system was recorded as ‘fully retained’. If FS material was present
but covered less than 2/3 it was recorded as ‘partially retained’. If the FS was not detectable
visually it was recorded as ‘lost’.
2.3.3 Pilot B - pilot study using a revised protocol
The second part involved two convenience samples recruited based on the routine schedule of
schools to be part of the sealant program as dictated by the school health department, MOEYS.
Group D involved 101 children from a school which received fissure sealants the week after
Group C according to the original protocol used for Group A; Group C involved a cluster of
115 children who attended the schools that were scheduled for routine sealant placement the
following week.
The original protocol was modified for participants in Group C. There were four changes; the
first change was to cool the GIC liquid material by placing it in a container of ice between uses.
The second change was placing one sealant at a time. The next change was the exact timing of
mix and finger press: a timer was placed next to each operator and set for 20 seconds for the
mix and one minute for the finger press. The last change was the occlusal check and adjustment
after placement. Articulating paper was used to detect any ‘high spots’ of sealants after
placement and a large spoon excavator used to reduce any ‘high spots’.

56
Two materials were trialled in Group C using a split-mouth design alternating the side the
sealants were placed based on the day that the children presented. There were four days when
sealants were placed; for day 1 and day 2 Fuji VII® was placed on the left side while Fuji IX®
was placed on the right side. For days 3 and 4, Fuji VII® was placed on the right side and Fuji
IX® on the left. Those in Group D had FS placed using the original protocol as described in
Section 2.3.2.
2.3.2.1 Clinical examination
At baseline, the standard SEAL Cambodia form was used to record data on the type of material
placed (Appendix 5). A different form was used at follow-up at one week, one month, six
months and one year and the FS retention was rated based on presence of the GIC material as
described in Section 2.3.2.1 (Appendix 4). No measure for carious lesions was used for Pilot
B follow-up.
2.3.4 Data collection and analysis
Data were entered into SPSS Ver. 20 (IBM, NY, USA) and analysed to produce descriptive
statistics on baseline caries experience and caries incidence (Pilot A) as well as sealant
retention (Pilot A and Pilot B). Descriptive analyses were performed as well as bivariate
analyses to examine differences in caries experience and sealant retention by group
membership. Baseline caries groups were defined using the Significant Caries Index (Bratthall,
2000) where by the group was divided by terciles based on dmft. Differences in means among
groups were compared using the Kruskal-Wallis test and differences in proportions among
groups were compared using the chi-squared test. Differences in means among related samples
were examined using the Wilcoxon signed-rank test.

57
2.4 Results
2.4.1 Pilot A
Data on the sociodemographic characteristics of participants by attrition at 1-year are presented
in Table 2.1. The mean age of participants was 8.1 (SD 1.1) years-of-age and there was no
significant difference in gender or age by loss to follow-up.
Table 2.1 – Pilot A – Attrition analysis for the 1-year follow-up by gender and age
(brackets contain row percentages unless otherwise indicated).
Baseline
N (column %)
One year follow-up
N (row %)
Lost to follow-up
N (row %)
Group membership
Control 251 (36.7) 163 (64.9) 88 (35.1)
Intervention 433 (63.3) 262 (60.5) 171 (39.5)
Age group
<6 years 18 (2.6) 12 (66.7) 6 (33.3)
7 years 149 (21.8) 92 (61.7) 57 (38.3)
8 years 282 (41.2) 183 (64.9) 99 (35.1)
>9 years 235 (34.4) 138 (58.7) 97 (41.3)
Gender
Male 358 (52.3) 215 (60.1) 143 (39.9)
Female 326 (47.7) 210 (64.4) 116 (35.6)
Total 684 (100.0) 425 (62.1) 259 (37.9)
Data on caries experience by membership to the control group or intervention group is
presented in Table 2.2. There was a statistically significant difference in caries experience by
gender whereby males had a more severe dmft than females. There was also a statistically
significant difference in caries experience by membership of the control or intervention group
with those in the intervention group having a higher caries experience. There was no difference
in caries experience by loss to follow-up.

58
Table 2.2 – Pilot A - Caries experience at baseline by group membership, gender and age.
dmft
Mean (SD)
DMFT
Mean (SD)
Any caries
N (Row %)
Any PUFA
N (Row %)
Treatment group
Control 7.5 (4.1)a 2.2 (2.1) 232 (93.2) 169 (67.9)a
Intervention 8.3 (3.8) 2.3 (2.2) 412 (94.2) 336 (77.6)
Follow-up
Lost 7.9 (4.0) 2.4 (2.4) 247 (93.6) 198 (75.0)
Followed-up 8.1 (3.9) 2.1 (2.0) 397 (94.7) 307 (73.3)
Sex
Male 8.4 (4.0)a 2.2 (2.1) 334 (94.6) 269 (76.2)
Female 7.6 (3.9) 2.2 (2.1) 306 (94.2) 233 (71.7)
Age group <6 y 8.2 (4.9)a 1.9 (2.7)a 16 (94.1)a 10 (58.8)a
7 y 8.9 (3.7) 2.1 (2.1) 143 (96.0) 114 (76.5) 8 y 8.7 (3.7) 2.1 (1.9) 268 (97.1) 220 (79.7) >9 y 6.6 (3.9) 2.6 (2.4) 212 (90.2) 156 (66.4)
Overall 8.0 (3.9) 2.2 (2.2) 640 (94.4) 502 (74.0)
aP-value <0.01; Kruskal-Wallis for comparison of means among groups or χ2 test for comparison of proportions
among groups within the same column.
Data on caries incidence and sealant retention by group membership are presented in Table
2.3; participants who were lost due to follow-up were not included in this analysis. There were
no statistically significant differences in the proportion or number of teeth eligible to be sealed
by group membership. Also, there was no statistically significant difference in caries incidence
by group membership. Despite this it does appear that there may have been a 10% preventive
benefit for those in the intervention group. The retention rate for sealants was low with only
approximately one in four sealants retained (including partially retained).
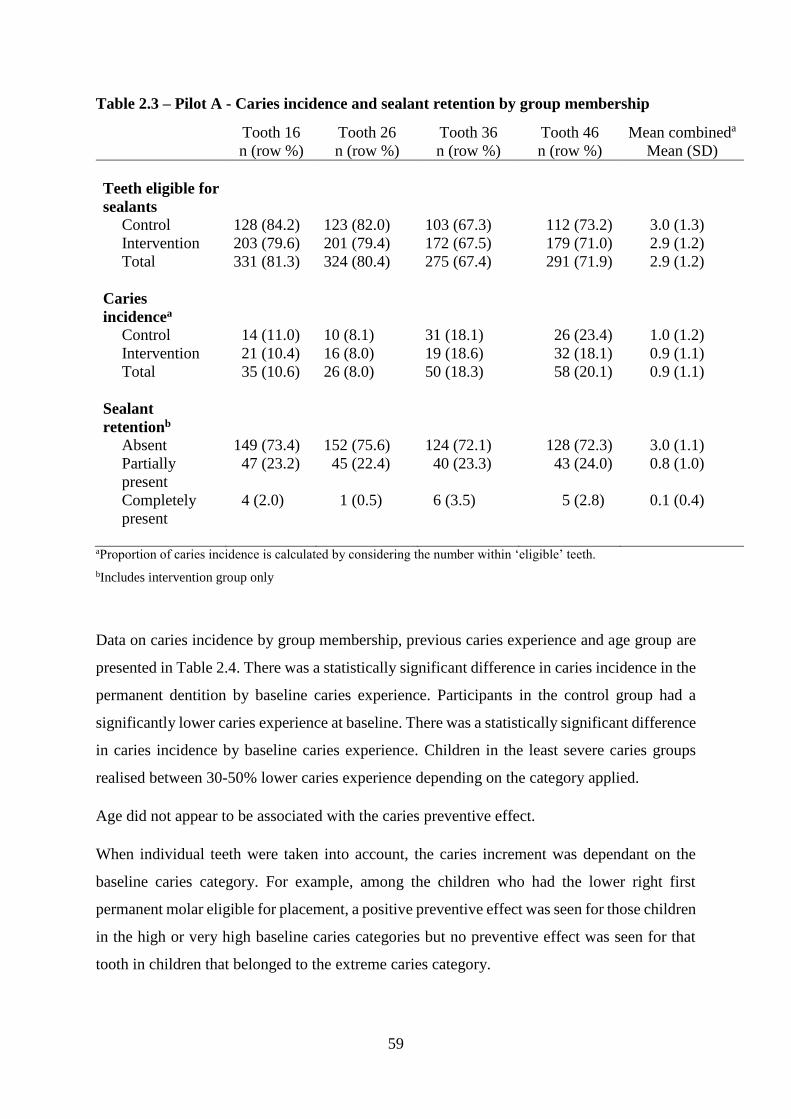
59
Table 2.3 – Pilot A - Caries incidence and sealant retention by group membership
Tooth 16
n (row %)
Tooth 26
n (row %)
Tooth 36
n (row %)
Tooth 46
n (row %)
Mean combineda
Mean (SD)
Teeth eligible for
sealants
Control 128 (84.2) 123 (82.0) 103 (67.3) 112 (73.2) 3.0 (1.3)
Intervention 203 (79.6) 201 (79.4) 172 (67.5) 179 (71.0) 2.9 (1.2)
Total 331 (81.3) 324 (80.4) 275 (67.4) 291 (71.9) 2.9 (1.2)
Caries
incidencea
Control 14 (11.0) 10 (8.1) 31 (18.1) 26 (23.4) 1.0 (1.2)
Intervention 21 (10.4) 16 (8.0) 19 (18.6) 32 (18.1) 0.9 (1.1)
Total 35 (10.6) 26 (8.0) 50 (18.3) 58 (20.1) 0.9 (1.1)
Sealant
retentionb
Absent 149 (73.4) 152 (75.6) 124 (72.1) 128 (72.3) 3.0 (1.1)
Partially
present
47 (23.2) 45 (22.4) 40 (23.3) 43 (24.0) 0.8 (1.0)
Completely
present
4 (2.0) 1 (0.5) 6 (3.5) 5 (2.8) 0.1 (0.4)
aProportion of caries incidence is calculated by considering the number within ‘eligible’ teeth.
bIncludes intervention group only
Data on caries incidence by group membership, previous caries experience and age group are
presented in Table 2.4. There was a statistically significant difference in caries incidence in the
permanent dentition by baseline caries experience. Participants in the control group had a
significantly lower caries experience at baseline. There was a statistically significant difference
in caries incidence by baseline caries experience. Children in the least severe caries groups
realised between 30-50% lower caries experience depending on the category applied.
Age did not appear to be associated with the caries preventive effect.
When individual teeth were taken into account, the caries increment was dependant on the
baseline caries category. For example, among the children who had the lower right first
permanent molar eligible for placement, a positive preventive effect was seen for those children
in the high or very high baseline caries categories but no preventive effect was seen for that
tooth in children that belonged to the extreme caries category.

60
Table 2.4 – Pilot A - Caries incidence in the intervention group by baseline caries experience and agea
Tooth 16
n = 41
Tooth 26
n = 30
Tooth 36
n = 109
Tooth 46
n = 93 Mean number
INT
n (row %) CON
n (row %)
INT n (row %)
CON n (row %)
INT n (row %)
CON n (row %)
INT n (row %)
CON n (row %)
INT Mean (SD)
CON Mean (SD)
Caries group
(deciduous)
High dmft
dmft <6
7 (53.8) 6 (46.2) 5 (55.6) 4 (44.4) 18 (48.6) 19 (51.4) 11 (44.0) 14 (56.0) 0.7 (0.9) 1.0 (1.2)c
Very high dmft
dmft 6-to 9
2 (28.6) 5 (7.4) 2 (28.6) 5 (71.4) 5 (27.8) 13 (72.2) 5 (26.3) 14 (73.7) 1.1 (1.2) 1.2 (1.3)
Extreme dmft
dmft >9
8 (38.1) 13 (61.9) 5 (35.7) 9 (64.3) 18 (33.3) 36 (66.7) 18 (36.7) 31 (63.3) 0.9 (1.1) 0.9 (1.0)
Caries group
(permanent)a
High DMFT
DMFT <1
2 (50.0) 2 (50.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0 (0.0) 0.3 (0.7) 0.6 (1.1)
Very high DMFT
DMFT = 1
15 (40.5) 22 (59.5) 0 (0.0) 2 (100.0) 4 (30.8) 9 (69.2) 2 (20.0) 8 (80.0) 0.7 (0.9) 0.4 (0.8)
Extreme DMFT
DMFT >2
15 (40.5) 22 (59.5) 12 (42.9) 16 (57.1) 37 (38.5) 59 (61.5) 32 (38.6) 51 (61.4) 1.2 (1.2) 1.4 (1.2)
Pulpally involved
No pufa 14 (38.9) 22 (61.1) 0 (0.0) 1 (100.0)b 9 (52.9) 8 (47.1) 5 (41.7) 7 (58.3)b 1.0 (1.1)c 1.1 (1.2)
Any pufa 3 (60.0) 2 (40.0) 12 (41.4) 17 (58.6) 32 (34.8) 60 (65.2) 29 (35.8) 52 (64.2) 0.5 (0.8) 0.9 (1.1)
Age
<6 y 0 (0.0) 1 (100.0) 0 (0.0) 1 (100.0) 0 (0.0) 2 (100.0) 0 (0.0) 1 (100.0) 0.6 (1.1) 0.0 (0..0)
7 y 3 (33.3) 6 (66.7) 2 (33.3) 4 (66.7) 7 (35.0) 13 (65.0) 9 (50.0) 9 (50.0) 1.0 (0.7) 1.0 (1.3)
8 y 6 (42.9) 8 (57.1) 2 (20.0) 8 (80.0) 14 (35.0) 26 (65.0) 11 (32.4) 23 (67.6) 0.9 (1.3) 1.0 (1.3)
>9 y 8 (47.1) 9 (52.9) 8 (61.5) 5 (38.5) 20 (42.6) 27 (57.4) 14 (35.0) 26 (65.0) 1.3 (1.1) 1.1 (1.3)
aINT stands for “intervention group” and CON stands for “control group”; percentages are calculated based on the number of eligible teeth bP-value <0.001; χ2 test or Kruskal-Wallis test for
differences among groups within the same column cP-value <0.01; χ2 and Kruskal-Wallis test as appropriate for differences among groups within the same column

61
Data on sealant retention by caries experience and age are presented in Table 2.5. Children
with one or more pulpally involved teeth at baseline had a statistically significant greater
chance of losing the fissure protection on tooth 46. Children in the lower age groups had a
statistically significant greater chance of retaining the FS on teeth 36 and 46. Sealant retention
was statistically different among age-groups and those in the younger age group were more
likely to retain the FS material. There is some evidence that sealant retention is related to
baseline caries experience and age.

62
Table 2.5 – Pilot A - Number of retained sealants by caries experience and gender (brackets contain row percentages unless otherwise indicated)
Tooth 16
(N = 206)
Tooth 26
(N = 206)
Tooth 36
(N=178)
Tooth 46
(N=185)
Lost
N (%)
Retained
N (%)
Lost
N (%)
Retained
N (%)
Lost
N (%)
Retained
N (%)
Lost
N (%)
Retained
N (%)
All FPM Mean (SD)
Baseline caries
group (primary)
High dmft
dmft <6
47 (71.2) 19 (28.8) 50 (73.5) 18 (26.5) 43 (72.9)
16 (27.1) 43 (71.7) 17 (28.3) 0.6 (1.0)
Very High dmft
dmft 6-to 9
24 (68.6) 11 (31.4) 27 (79.4) 7 (20.6) 21 (70.0) 9 (30.0) 17 (60.7) 11 (39.3) 0.6 (0.9)
Extreme dmft
dmft >9
83 (79.0) 22 (21.0) 82 (78.8) 22 (21.2) 67 (75.3) 22 (24.7) 76 (78.4) 21 (21.6) 0.7 (1.1)
Baseline caries
group (permanent)
High
DMFT <1
41 (82.0) 9 (18.0) 41 (83.7) 8 (16.3) 40 (72.7) 15 (27.3) 40 (74.1) 14 (25.9) 0.6 (1.0)
V. High
DMFT = 1
39 (73.6) 14 (26.4) 45 (83.3) 9 (16.7) 41 (77.4) 12 (22.6) 38 (69.1) 17 (30.9) 0.6 (1.0)
Extreme
DMFT >2
74 (71.8) 29 (28.2) 73 (70.9) 30 (29.1) 50 (71.4) 20 (28.6) 58 (76.3) 18 (23.7) 0.7 (1.0)
Pulpally involved
No pufa 36 (75.0) 12 (25.0) 33 (73.3) 12 (26.7) 29 (67.4) 14 (32.6) 28 (65.1) 15 (34.9) 0.7 (1.0)
Any pufa 118 (74.7) 40 (25.3) 126 (78.3) 35 (21.7) 102 (75.6) 33 (24.4) 108 (76.1) 34 (23.9) 0.6 (1.0)
Age
<6 y 2 (66.7) 3 (33.3) 2 (66.7) 1 (33.3) 2 (50.0) 2 (50.0) 1 (25.0) 3 (75.0) 0.9 (1.5)a
7 y 33 (75.0) 11 (25.0) 33 (71.7) 13 (28.3) 28 (68.3) 13 (31.7) 31 (66.0) 16 (34.0) 0.9 (1.2)
8 y 68 (74.7) 23 (25.3) 65 (74.7) 22 (25.3) 56 (70.0) 24 (30.0) 61 (75.3) 20 (24.7) 0.7 (0.9)
>9 y 51 (75.0) 17 (25.0) 59 (84.3) 11 (15.7) 45 (84.9) 8 (15.1) 43 (71.1) 10 (18.9) 0.4 (0.9)
aP-value <0.05; χ2 test or Kruskal-Wallis test as appropriate for examining differences among groups within the same column

63
2.4.2 Pilot B
The attrition data is presented in Figure 2.1 and 58 children were excluded from the analysis
as at least one cavitated first permanent molar was present. During the one month follow-up,
there was no dropout in the control group, but there was an 8% dropout rate (N=9) in the
intervention group. This rate increased so that the incremental drop out at the the six month
follow-up for the intervention group was 36.5% (N=32). At one year follow-up, there was a
14% (N=6) dropout rate in the control group, while there was 19.1% (N=22) in the intervention
group.
Figure 2.1 – Selection and follow-up of children in Pilot B

64
Data on the sociodemographic characteristics of those in Pilot B are presented in Table 2.6.
After excluding children who did not meet the inclusion criteria, there were differences in
gender by group membership. There was a lower number of female children (37.2%) compared
to male children (62.8%) in the control group. The mean age of children in the control group
was 9.0y while the mean age in the intervention group was 9.2y, which was not considered
significant.
Table 2.6 – Pilot B – Gender and group membership after cases with caries FPM at
baseline were removed
Male
N (row %)
Female
N (row %)
Total
N (column %)
Control 27 (62.8) 16 (37.2) 43 (28.9)
Intervention 54 (50.9) 52 (49.1) 106 (71.1)
Total 81 (54.4) 68 (45.6) 149 (100.0)
At the one week and one-year follow up, there was no significant difference in the number of
sound sealants that were completely retained by material type (data presented in Table 2.7). At
the one month and six-month follow-up Fuji VII® material had a statistically significant greater
chance of being fully retained. At one month Fuji IX® material was three times more likely to
be completely lost.

65
Table 2.7 – Pilot B - Proportion of sealant retention by material type in the intervention
group (numbers are percentages)a
One week One month Six months One year
VII IX P-value VII IX P-value VII IX P-value VII IX P-value
Sound 84.0 79.7 0.317 76.5 64.2 0.005 8.9 16.1 0.041 3.7 2.7 1.000
High 5.2 0.5 0.013 0.0 0.0 n/a - - - - - -
Partially
lost
9.0 9.4 0.858 16.0 13.7 0.587 48.2 24.4 <0.001 33.0 31.4 0.014
Completely
lost
1.9 10.3 0.003 7.6 22.2 <0.001 42.9 59.5 0.006 63.3 77.1 0.016
aP-value calculated using Wilcoxon Signed Rank Test; ‘VII’ refers to Fuji VII material and ‘IX’ refers to Fuji IX
material.
At one month, there was a statistically significant difference in sealant retention by group
membership, but at one year that difference was no longer significant (data presented in Table
2.8). Within the intervention group a more than 10% increase in the rate of retention at one
month was observed, but the differences at one year were not significant.

66
Table 2.8 – Pilot B - Proportion of Fuji VII® FS retained at one month and one year by
group membershipa
One month One year
Group D
(%)
Group C
(%) P-valueb
Group D
(%)
Group C
(%) P-valueb
Sound 63.9 76.5 0.019 4.7 3.7 0.331
Partially lost 23.9 16.0 <0.001 31.8 33.0 0.892
Completely lost 9.9 7.6 0.072 63.5 63.3 0.845
aGroup D were those in Pilot B that had FS placed using the original protocol and Group C were those in Pilot B
who had FS placed using a modified protocol. bP-value calculated using Kruskal-Wallis statistic for differences among groups within the same row.

67
2.5 Discussion
The SEAL Cambodia project represents the first time that Fuji VII® FS has been applied to
prevent dental caries at large scale in Cambodia and the first time that it has been evaluated
among a population with such a severe caries experience. The present study examined two pilot
protocols, each looking at a different clinical procedure to: achieve caries prevention in the
case of Pilot A; and improve retention in the case of Pilot B. The later pilot (Pilot B) was put
in place as a response to the unfavourable findings in the first pilot and changes were based on
a critical review of the initial findings. Pilot A demonstrated that there was poor FS retention,
a smaller than expected caries preventive effect, and that statistically significant clinical
benefits were only realised in the less severe caries groups. Pilot B of the study demonstrated
that modifications in the original protocol could improve retention; it could be postulated that
this is likely associated with a better preventive increment but would need to be the subject of
future research to establish evidence.
Before considering the findings in more detail, it is appropriate to first consider the strengths
and limitations of the study. Regarding Pilot B, there were significant vulnerabilities due to the
small sample size and limited follow-up at 1-year. In addition, requiring four non-cavitated
FPM for the split mouth design meant that the sample was biased towards the less severe
spectrum of caries in a potentially eligible population where one in four children that are 6
years-of-age have at least one cavitated first permanent molar. Those factors also meant that
the children in Pilot B were not comparable to the children in Pilot A who had a more severe
caries experience.
Regarding Pilot A, the strengths were that the study was sufficiently powered to examine
clinically significant caries preventive effect; however, the sample did not reach the ideal target
and older children were included into the sampling frame. This is because in Cambodia it is
common for children to repeat grades or start school late. Therefore, it is normal to have a wide
variety of ages at each grade level. The follow-up rate for Pilot A did not reach the desired 70%
and so the sample could be vulnerable to follow-up bias; however, no differences were seen at
1-year follow-up by gender, age, or baseline caries experience. In addition, the age profile of
the children in this cohort was similar to that reported among the wider population of children
participating in the SEAL Cambodia project (One-2-One Cambodia 2016). Although the cohort
was representative of the wider SEAL project, those in the control group had a significantly

68
lower caries experience at baseline and this could have masked some of the preventive benefits
of the intervention.

69
2.5.1 Caries prevention in Pilot A
The caries experience in this group was so severe that even in the lower tercile of caries
experience there was a mean dmft > 5, which matches the caries profile of most other groups
that are considered to be ‘high caries’ experience. It has been reported that caries experience
among groups is likely to moderate the caries preventive effect achieved by a FS intervention
(Ahovuo-Saloranta et al. 2017). Within Pilot A, there was potentially a benefit that was not
statistically significant and that combined with the existing body of evidence around FS as a
caries preventive strategy meant that further investigation was warranted. This is the first time
that the material has been assessed among a group with such severe caries experience and it
could be that the indices used to examine caries progression were not sensitive enough to detect
the benefits rendered. This was also a first in terms of an upstream dental intervention,
implemented at large scale in Cambodia.
2.5.1.1 Alternatives to achieve caries prevention in FPM
As this was ‘new territory’ it was appropriate to examine alternative ways to achieve prevention
of carious lesions on FPM. That included consideration for the present protocol in terms of
understanding of the material science and consideration of other materials. The alternative
materials that could be considered for pit and fissure caries prevention could be Fluoride
Varnish (FV) or Silver Diammine Fluoride (SDF) which have been able to demonstrate a
preventive increment of around 40% on FPM (Liu et al. 2012). Alternatively, supervised ‘cross
brushing’ in schools was able to achieve significant reductions in plaque and a reduction in
caries experience (Frazão, 2011; Nourallah & Splieth, 2004). Finally, the other material for
consideration would have been resin materials for the placement of FS. Resin fissure protection
is often considered the gold standard, but it would involve considerable and unfeasible
additional infrastructure and support in terms of clinic set up and transport to clinics. While
SDF or FV require less investment, these interventions do not yet have a broad body of
evidence to support effectiveness for caries prevention on FPM; and cannot yet be
recommended for large scale interventions at population level. In contrast, the benefit of the
SEAL Cambodia protocol from an organisational and logistical perspective is that it is a
discrete, one-off intervention, with very little need for investment in infrastructure and with a
good evidence of potential benefit. For that reason, it was favourable and justified to consider
continuation of the SEAL Cambodia Community Project using the modified protocol.

70
2.5.2 The retention of FS material in Pilot B
Given that the community-based project was still ongoing during the testing of a modified
protocol, an indicator of success other than 1-year caries increment was desired and therefore
retention of FS material at 3 and 6-months was the outcome used to inform the decision making
of the SEAL Cambodia project. Although retention is not the primary outcome of interest, if
the fissure protection was lost early then it could help to explain why the caries prevention was
not as beneficial as expected in Pilot A. The theory behind FS is that the material will protect
the pit and fissure system during the most vulnerable period so of development; when the tooth
has newly erupted and enamel maturation is occurring and the tooth is more difficult to reach
with a toothbrush. Therefore, it could be argued that FS are not needed after that initial
protection period and this is the rationale behind the fact that both resin and GIC fissure
protection is thought to render the same preventive effect despite the fact that resin sealants are
better retained (Mickenautsch & Yengopal, 2013). In saying that, it could be that resin FS has
been easier to detect because it stays in bulk while GIC materials are thought to be ‘micro-
retained’ (Hu et al, 2016).
In the case of the cohort in Pilot A, new carious lesions were forming on teeth that lost clinically
detectable traces of Fuji VII® FS. The major question raised was whether or not sufficient
retention (micro or macro) had been achieved. Therefore, being able to increase the presence
of clinically detectable Fuji VII® material was thought to be a desirable indictor in the pathway
to caries prevention. Achieving better retention, therefore required a careful consideration of
the material properties and setting reaction. Subsequently this informed the modification to the
clinical protocol.
A key consideration for avoiding failure was to consider ways in which the setting reaction
could be controlled. The GIC setting reaction involves three phases (1) the decomposition of
glass in an acid-base reaction during the initial mixing (2) the second phase involves the
migration of ions that occurs during the working time and (3) the gelatinous phase as the
material gradual reconstructs in the inorganic fragments to becomes more rigid by creating a
matrix that increases in strength over the following 24-hours (Berg & Croll, 2015; Croll &
Nicholson, 2002). According to the manufacturer’s instructions the mixing should take 20
seconds and the initial set should take 1-minute; however, clinical observation suggested that
the setting reaction was happening much faster in the hotter, more humid weather (GC
Corporation, 2018). In addition, FS were placed for children in Group A (Pilot A) during April

71
which has an average temperature of 35 degrees Celsius in Phnom Penh. The limited working
time also meant that the time taken to place the material on more than one tooth could also
compromise the bonding to the tooth surface and so there should be only one tooth per mix. If
the material reaches the tooth during the second phase, then fewer free ions will be available
in the mix to allow for ionic exchange and adhesion to the tooth surface. The first phase and
bonding were further exploited by delivering the material to the tooth at the optimal time after
mixing and timing the mixing so that only 20 seconds was spent.
Timing was also important during the second phase of the setting. It is during the first and
second phase that the material is most vulnerable to moisture contamination (Berg & Croll
2015). During this time, contact with saliva can result in leaching of the ions from the material
and the result is a lower compressive strength. Therefore, meticulous moisture control was
achieved by holding the finger over the sealant for a full minute as counted by a timer. During
the original protocol anecdotal evidence suggested that operators were waiting until the second
phase of setting when the material was in the gelatinous phase before placing the finger because
they were worried that the material would stick to the glove when they removed the finger. For
an experienced operator, timing might not be such an issue because the work flow is more
efficient; however, SEAL Cambodia involved a multitude (over 100) of different operators
with varying level of experience and there is evidence that the dental students applied the
protocol with differing success to that of experienced Cambodian dental nurses (Sreang 2016).
The final measure to optimise FS retention was the adjustment of the occlusion. Given that Fuji
VII has a lower compressive strength to high viscosity (Fuji IX) GIC material then protection
of the material from the occlusion may have been important. Those protocol considerations
and the presence of multiple operators with varying levels of experience highlight the
importance of having a robust protocol, with strict timing and control measures in order to
ensure consistent results in turn better quality of care.
2.5.2.1 The pattern of material loss
Even with the control measures described in the previous paragraph, the retention of sealants
was lower than that reported in other studies (Chen & Liu 2013). There were four studies that
could be found which examined retention of Fuji VII material over multiple time points during
the first year of placement. One study reported retention rates around 80% at 1-year (Chen &
Liu, 2013), while another found retention rates around 40% (Kamala & Hegde, 2008). The key
differences among the protocols was that those studies with high retention rates only sealed
72
teeth which were fully erupted and clinically judged to be deep or susceptible to caries. In
contrast, those studies with the lower retention rates and the SEAL Cambodia project sealed
all FPM that were present or partially present in the mouth.
Another assumption had been made around the loss of FS was that there might have been a
primary loss of sealants during the first week due to unfavourable occlusal force. This may
have been possible for one in twenty Fuji VII® FS that were lost using the modified protocol
even after occlusal adjustment; however, it appears that the material is being lost gradually
over time in a more linear fashion. This linear pattern of loss was present in other retention
studies of Fuji VII GIC material (Chen & Liu 2013; Kamala & Hegde 2008). Such a pattern
could suggest a wear process rather than a gross fracture or a gross failure of adhesive bonding.
In saying that, the pattern of loss in Pilot A is not known and so, after taking into account the
properties of the material and application conditions, primary failure to bond cannot be ruled
out in that protocol.
What was not reported in the previous literature was differences in retention by tooth position
and sociodemographic characteristics. Among those in Group A, children who were in the 6-
year age-group, those who were in the less severe caries category and mandibular molars
appeared to have higher retention rates. Perhaps those younger children were more likely to
have non-cavitated deep pits and fissures whereas deep pits and fissures in older age groups
were already cavitated and hence not sealed/included in the study. This suggests some benefit
could be gained by shifting the target grade range from the second grade down to the first grade.
That mandibular teeth were more likely to have retained the sealant could be because the
material was systematically placed on the lower teeth before the maxillary teeth meaning that
the mandibular teeth received material at an early phase of the setting process. The other
possibility is that the lower teeth may have been more likely to have the finger press applied
because placing a finger in the mandibular arch is more ergonomically comfortable. This logic
supports the protocol for only placing only one sealant at a time and for holding the finger in
place for a full minute.
That those with higher caries rates were more likely to lose the FS could suggest something
about the level of acid in the oral environment is relevant for retention. The acid could be
coming from the sugary diet which drives the caries process, or due to the presence of
acidogenic plaque at the interface of the FS material and the tooth. Alternatively, it is more
likely that it could be due to acidic foods, and there are previous reports of high rates of erosion

73
among Cambodian children (Kubota et al. 2016). The presence of plaque or acid could
potentially create an erosive process on the GIC material. Unfortunately, the SEAL Cambodia
project did not collect data on those variables which drive the caries process (such as sugar
consumption) or record erosion and so it is not possible to estimate these influences or make
adaptions to the protocol which would counteract that.
2.5.2.2 High vs Low viscosity GIC
It was interesting that in Pilot B of the present study, Fuji IX® material was significantly more
likely to be lost at 1-week in a primary failure scenario. Despite this, at one-year the differences
were not significant. It is therefore possible to say that Fuji VII® low viscosity material
performed better in the early stages; however, it is not known whether the better performance
and one month and six months will render a better caries preventive effect. Also of note, the
modified protocol was designed to optimise the properties of Fuji VII®. It might be that Fuji
IX® would have performed better in the original protocol due to the longer working time which
may have given sufficient placement time despite the heat and humidity of the Cambodian
school-yard environment.
2.6 Conclusion
The original protocol used for the SEAL Cambodia project did not render the retention rates or
the caries preventive effects that were anticipated (Pilot A) therefore modifications to that
protocol were tested (Pilot B). The caries prevention achieved differed depending on the
severity of the baseline caries experience, whereby those with more extreme caries experience
realised a lower preventive increment. Pilot B applied a modified protocol and achieved better
retention rates at one month and six months compared to the original protocol. This informed
the practice of the SEAL Cambodia community project and further investigation is needed to
examine whether the higher retention rates using the modified protocol in the early stages of
Pilot B will render a greater caries preventive effect when implemented at scale.

74
2.7 References Chapter 2
Agouropoulos, A., Twetman, S., Pandis, N., Kavvadia, K. & Papagiannoulis, L. (2014) Caries-
preventive effectiveness of fluoride varnish as adjunct to oral health promotion and supervised
tooth-brushing in preschool children: A double-blind randomized controlled trial. Journal of
Dentistry, 42 (10), 1277–1283.
Ahovuo-Saloranta, A., Forss, H., Walsh, T., Nordblad, A., Mäkelä, M. & Worthington, H. V.
(2017) Pit and fissure sealants for preventing dental decay in permanent teeth. In Cochrane
Database of Systematic Reviews 2017(7):1-67.
Croll, T (2015). Glass Ionomer Restorative Cement Systems: An Update. Pediatric Dentistry,
37(2), 116–124
Bratthall, D. (2000) Introducing the Significant Caries Index together with a proposal for a new
global oral health goal for 12-year-olds. International Dental Journal, 50 (6), 378–384.
Chen, X. X. & Liu, X. G. (2013) Clinical comparison of Fuji VII and a resin sealant in children
at high and low risk of caries. Dental Materials Journal, 32 (3), 512–518.
Chher, T., Hak, S., Courtel, F. & Durward, C. (2009) Improving the provision of the Basic
Package of Oral Care (BPOC) in Cambodia. International Dental Journal, 59 (1), 47–52.
Chher T., Turton B., Hak S., Beltran E., Courtel F., Durward C. & Hobdell M. (2016) Dental
caries experience in Cambodia: Findings from the 2011 Cambodia National Oral Health
Survey. Journal of International Oral Health, 8 (1), 1.
Chia, L., Densie, I. & Morgan, C. (2015) An exploratory study of parental knowledge of early
childhood oral health care in Southland, New Zealand. NZ Dent J, 111 (1), 18–24.
Croll, T. P. & Nicholson, J. W. (2002) Glass ionomer cements in pediatric dentistry: review of
the literature. Pediatric Dentistry, 24 (5), 423–429.
de Amorim, R. G., Leal, S. C. & Frencken, J. E. (2012) Survival of atraumatic restorative
treatment (ART) sealants and restorations: a meta-analysis. Clinical Oral Investigations, 16
(2), 429–441.
Forss, H., Saarni, U.-M. & Seppä, L. (1994) Comparison of glass-ionomer and resin-based
fissure sealants: a 2-year clinical trial. Community Dentistry and Oral Epidemiology, 22 (1),
21–24.
Frazão, P. (2011) Effectiveness of the bucco-lingual technique within a school-based
supervised tooth-brushing program on preventing caries: a randomized controlled trial. BMC
Oral Health, 11 (1), 11.
Ganesh, M. & Tandon, S. (2007) Clinical evaluation of FUJI VII sealant material. Journal of
Clinical Pediatric Dentistry, 31 (1), 52–57.
GC Corporation (2018) Manufacturers instructions for GC Fuji VII radiopaque Glass Ionomer
Cement and Stabilisation Material [Online]
http://www.gcaustralasia.com/Upload/product/pdf/5/GC-Fuji-VII-CAPSULE_IFU-EN.pdf
[Accessed 30 August 2018].

75
Holve, S. (2008) An observational study of the association of fluoride varnish applied during
well child visits and the prevention of early childhood caries in American Indian children.
Maternal and Child Health Journal, 12 (1), 64–67.
Hu, X., Zhang, W., Fan, M., Mulder, J. & Frencken, J. E. (2016) Frequency of remnants of
sealants left behind in pits and fissures of occlusal surfaces after 2 and 3 years. Clinical Oral
Investigations, 21 (1), 1–7.
Kamala, B. & Hegde, A. (2008) Fuji III vs. Fuji VII glass ionomer sealants–a clinical study.
Journal of Clinical Pediatric Dentistry, 33(1), 29–33.
Kubota, Y., Ly, S., Turton, B., Gonzalez, M., Abu Kasim, N., Chew, H., Durward, C., (2014)
The Relationship between Tooth Erosion and Lifestyle in Cambodian Adolescents. Presented
at the South East Asian Division Meeting, Kuching, Malaysia.
Lam, S. P. L., Baros, H., O’Grady, M. J., Kendall, G. E., Messer, L. B. & Slack-Smith, L. M.
(2012) Patterns of attendance of children under 12 years at school dental service in Western
Australia. The Open Dentistry Journal, 6, 69.
Liu, B. Y., Lo, E. C. M., Chu, C. H. & Lin, H. C. (2012) Randomized trial on fluorides and
sealants for fissure caries prevention. Journal of Dental Research, 91 (8), 753 – 758.
Macpherson, L. M. D., Anopa, Y., Conway, D. I. & McMahon, A. D. (2013) National
supervised tooth-brushing program and dental decay in Scotland. Journal of Dental Research,
92 (2), 109–113.
Marinho, V. C., Higgins, J., Logan, S. & Sheiham, A. (2003) Fluoride toothpastes for
preventing dental caries in children and adolescents. The Cochrane Library (1), 1-103.
Mickenautsch, S. & Yengopal, V. (2013) Validity of sealant retention as surrogate for caries
prevention – a systematic review. PLoS ONE, 8 (10), e77103.
Monse, B., Heinrich-Weltzien, R., Benzian, H., Holmgren, C. & van Palenstein Helderman,
W. (2010) PUFA–An index of clinical consequences of untreated dental caries. Community
Dentistry and Oral Epidemiology, 38 (1), 77–82.
Nourallah, A. W. & Splieth, C. H. (2004) Efficacy of Occlusal Plaque Removal in Erupting
Molars: A Comparison of an Electric Toothbrush and the Cross-Tooth-brushing Technique.
Caries Research, 38 (2), 91–94.
One-2-One Cambodia (2016) SEAL Cambodia Final Report. Phnom Penh, Cambodia.
Poulsen, S., Beiruti, N. & Sadat, N. (2001) A comparison of retention and the effect on caries
of fissure sealing with a glass-ionomer and a resin-based sealant. Community Dentistry and
Oral Epidemiology, 29 (4), 298–301.
Sreng R, Turton B, Chen P, Serey P, Durward C. (2016) SEAL Cambodia – Retention rates of
ART Sealants according to provider type. IADR General Session. Seoul, Republic of Korea.
Turton B, Durward C, Bach K, Manton D. (2014) Seal Cambodia – 60,000 children over 3
years. IADR SEA 28TH Annual meeting, Kutching, Malaysia.

76
Chapter 3
SEAL Cambodia – Evaluation of a modified protocol for
placement of Fuji VII Fissure Sealants
Presented in part as:
Turton B, Crombie F, Durward C, Manton D (2018) Seal Cambodia – a tale of two
protocols. ANZSPD, Brisbane, Australia.
Turton, B., Durward, C., Crombie, F., Manton D. (2016) SEAL Cambodia: Improved
Caries Prevention with a modified Protocol. IADR General Session. Seoul, Republic of
Korea

77
Abstract
Objective: To evaluate the caries preventive effect of hand-mixed GIC Fissure Protection (FS)
placed on FPM of 6-8 year-old children in Cambodia using two different protocols.
Methods: A school-based randomised controlled trial involved two cohorts. The first included
an intervention group (Group A) who received FS using the original protocol and a control
group (Group B) who did not receive FS. The second cohort involved an intervention group
(Group C) who received FS using a modified protocol and a matched control group (Group D)
who received FS using the original protocol. The modified protocol involved control of the
temperature of the material, the timing of mixing and placement, and adjustment of the
occlusion. Groups A, B, and C were followed-up at 1 y and Groups C and D were followed-up
at 2 y. Data analysis examined differences in caries incidence by Group.
Results: At 1 y and 2 y, 62.8%, and 68.0% follow-up rates were achieved, respectively. The
mean age was 8.1 y (SD 1.2) for the first cohort, and 6.6 y (SD 0.6) for the second cohort. The
baseline mean dmft for the first and second cohorts was 8.0 (SD 3.9) and 9.9 (SD 4.3)
respectively. There was no statistically significant difference in caries increment between
Groups in the first cohort at1 y. A preventive fraction of 89.1% at 1 y and 32.3% at 2 y was
achieved using the modified protocol in the second cohort (P < 0.05). Children with extreme
caries experience (dmft > 8) realised half the preventive fraction at 2 y compared to those with
dmft < 8 (22.3% and 45.8% respectively).
Conclusions: Children suffered from an extreme burden of dental caries. The modified FS
protocol had a significant impact on the caries preventive effect, although it was lower than
that reported in other studies. A more holistic approach is needed to reduce the burden of dental
caries in Cambodia.

78
3.0 Introduction – SEAL Cambodia evaluation of a modified
protocol for placing Fuji VII Fissure Sealants (FS)
The burden of dental caries in Cambodia is severe and the SEAL Cambodia project was
designed as a first step in reorientating dental services towards a more upstream approach. A
strong body of evidence supports FS as an intervention next in efficacy to tooth-brushing with
fluoridated toothpaste in terms of caries prevention. The rationale for the SEAL Cambodia
project was that by sealing the most susceptible permanent teeth, the First Permanent Molar
(FPM), soon after eruption, the proportion of permanent teeth affected by carious lesions could
be dramatically reduced.
Initially a protocol for GIC Fuji VII FS was developed and field-tested (Protocol found in
Appendix 6) and results presented in Chapter 2. The first FS protocol did not render the one
year caries preventive effect that was expected and a new application protocol was developed
aiming to increase retention (Tac et al. 2016). It was thought that the limited preventive effect
of the original protocol was due to lack of control of the temperature of the GIC material before
application, the moisture control in the mouth, the timing of mixing and placement, and the
lack of occlusal adjustment. Following discussions within the research team, several steps in
the protocol were revised and the new protocol was subsequently implemented for the
remainder of the SEAL Cambodia program. (Appendix 7)
While the pilot of the revised protocol appeared to be promising, further investigation was
required to validate the rationale of the study around reducing the burden of carious lesions and
their subsequent consequences in the permanent dentition. Over the course of the investigation
updated meta-analysis became available which suggested that there was insufficient evidence
for the use of GIC FS in achieving caries prevention and estimated preventive fractions
between 39% and -3% over two years (Ahovuo-Saloranta et al. 2017). Few high-quality studies
have examined the success of these interventions in a developing world context and among a
population which has such a severe caries experience as children in Cambodia. Furthermore,
none of the existing studies have child-reported measures (such as quality of life instruments)
as an outcome measure.
The aim of this study was to evaluate the caries prevention achieved among 6 to 8 year-old
Cambodian children using a modified GIC FS protocol shown to improve early retention rates.

79
Such a study will add to the quality of evidence around the benefits of GIC FS to reduce the
burden of caries among vulnerable populations.
3.1 Aim
To investigate the caries preventive effect of GIC FS in FPM of 6 to 8 year-old children in
Cambodia using a modified protocol that had previously improved retention rates.
3.2 Objectives
i. to evaluate the caries preventive effect of a modified FS placement protocol at one year
compared with the original protocol and a control group,
ii. to evaluate the caries preventive effect of FS placed using the modified protocol at two years
compared to a control group.

80
3.3 Methods
The present study had two parts; Part 1 was a comparison of the caries preventive effect of GIC
fissure sealants among the modified and original cohorts at one year, and Part 2 examined the
caries preventive effect of the modified cohort at two years against a contemporaneous control
group. Within the two parts there were four clinical groups: Group A was the original
intervention group, Group B was the original (negative) control group, Group C was the
modified protocol (intervention group) of the new cohort, and Group D was the positive control
group of the new cohort. All clinical examinations and clinical procedures were conducted in
a school-yard setting with battery-powered head-lights and children in a supine position.
Consent was gained by sending the consent forms to the school the week prior to the
examination and parents were given an opportunity to withdraw their child’s participation
should they wish (Appendix 1). Children were free to refuse assent at the time of examination
with no consequences. Participants were given oral hygiene education with a ratio of one
instructor to five children and they were given a toothbrush prior to the placement of the
sealants or following the examination for those in the control group. This ensured that the teeth
were clean prior to examination and placement of GIC sealants. Ethics approval was provided
by the National Committee for Health Research, Ministry of Health, Cambodia.
3.3.1 Clinical procedures
Participants in Group A (intervention group) and Group D (positive control) received FS using
the original protocol. It was not intended that Group D would receive FS; however, an
organisation which had previously partnered with the SEAL Cambodia project provided FS
independently for the schools in Group D. That organisation did not receive training on the
modified protocol. The original protocol involved up to two teeth (opposing arches) being
treated simultaneously (1) the dentine conditioner was applied to a clean tooth and then
removed with a wet cotton pellet; (2) the tooth was dried using cotton pellets; (3) hand-mixed
Fuji VII® was placed onto the occlusal surface of the tooth and pressed into the fissures using
the operators’ finger (no defined duration) which was lubricated with cocoa butter or Vaseline
and no subsequent occlusal adjustment.
The modified protocol which was applied to Group C involved the same work flow but with
some modifications: (a) cooling of the GIC liquid (Fuji VII® Liquid) in a cup of ice prior to
mixing; (b) timing the mixing (20 seconds) and placement of the material (60 seconds) using
a digital timer according to the manufacturer’s instructions; (c) placing one sealant at a time;

81
(d) placing the finger over the sealant for one minute using a timer; and (e) testing and adjusting
the occlusion if needed. Appendix 6 and 7 provides further detail on the two protocols.
3.3.2 Clinical examination and questionnaire
The DMF index was recorded at surface level according to the WHO Basic Survey Methods
(WHO, 2013). Each tooth was also given a score using the PUFA Index (Monse et al. 2009).
The degree of retention of FS material and the presence of any cavitated carious lesions on the
occlusal surfaces of FPM were recorded. Evaluation of FS was based on the proportion of
remaining material. Sealants that covered more than 2/3 of the fissure system were recorded as
‘fully retained’. If FS material was present but covered less than 2/3 of the fissure system, it
was recorded as ‘partially retained’. If the FS was not detectable visually it was recorded as
‘lost’.
Participants in Group C and Group D were asked a set of questions at each examination
including questions on oral hygiene, and four questions from the Oral Symptoms Domain of
the Child Perceptions Questionnaire which had been previously validated for use in a
Cambodian Setting (Turton et al. 2015). The questions were about mouth pain, sores (ulcers),
bad breath and food impaction in the context of the previous three months. The response
options for each item were “Never” (score 0), “Once or twice” (score 1), “Sometimes” (score
2), “Often” (score 3), and “Every day or almost every day” (score 4).
3.3.3 Part 1 – Methods for One-year investigation
The first part of the study involved three groups; Group A was the original intervention group
(N = 433), Group B was the original control group (N =262) and Group C was the modified
protocol intervention group (N = 364). Although the control group of the modified protocol
(Group D the positive control) was recruited contemporaneously to the intervention group, they
were not examined at 1 y due to logistical limitations. All groups were selected based on
randomised cluster sampling using the list of eligible schools provided by the School Health
Department. The inclusion criteria for the modified intervention group involved targeting for
age (not older than 7 y) in contrast to the original cohort which targeted based on the school
grade level of the child. Examiners were calibrated against an experienced dental
epidemiologist (BT) and achieved a kappa score higher than 0.85.
3.3.4 Part 2 – Two year analysis

82
The second part of the study involved two groups: Group C as described in Part 1 as the
modified protocol, the comparative group was a positive control group who had sealants placed
using the original protocol (Group D). Follow-up was maximised by working with school
administrators, having more than one ‘wave’ of data collection, and working with teachers to
identify children who were part of the cohort. Examiners went through with school
administrators the original hand-written hard copy of the school roll based on the first day of
school enrolment as well as electronic versions to account for those children who might have
modified their names between base-line and follow-up visits. There were two waves of data-
collection with examiners returning to schools two weeks later to capture any additional
children who might have been absent during the first wave of data collection. In addition,
teachers and classmates who may have taught the child at baseline were asked to identify
children who were not able to be found using the previously described means.
3.3.5 Data analysis
Data were entered into SPSS Ver. 20 (IBM, NY, USA) and data were analysed to produce
descriptive statistics on baseline caries experience and caries incidence as well as FS retention.
Data was collected on oral symptoms based on the prevalence of impacts, a child was said to
have an impact in oral symptoms if they responded with score 3 or higher to any of the items
in the domain. Descriptive analyses were performed as well as bivariate analysis to examine
differences in caries experience and FS retention by group membership. Caries groups were
defined using the Significant Caries Index (Bratthall 2000) whereby the group was divided by
terciles based on caries experience in the primary dentition (dmft). Differences in means among
groups were compared using the Kruskal-Wallis test and differences in proportions among
groups were compared using chi-squared test. Differences in means among related samples
were examined using the Wilcoxon signed rank test.

83
3.4 Results
3.4.1 Part 1 – One year comparison of old and new cohorts.
Data on attrition for Part 1 are presented in Table 3.1. There was no significant difference in
follow-up by gender or baseline caries experience.
Table 3.1 – Part 1 – Attrition analysis for the One year follow-up by group membership
and caries experience.
Total
N (Column %)
Lost
N (Row %)
One year Follow-up
N (Row %)
Group A (Original
intervention)
Male 237 (54.7) 98 (41.4) 139 (58.6)
Female 196 (45.3) 73 (37.2) 123 (62.8)
Total 433 (41.3) 171 (39.5) 262 (60.5)
Group B (Original Control)
Male 116 (46.2) 42 (36.2) 74 (63.8)
Female 135 (53.8) 46 (34.1) 89 (65.9)
Total 251 (24.0) 88 (35.0) 163 (64.9)
Group C (Modified protocol)
Male 181 (49.7) 68 (37.6) 113 (62.4)
Female 183 (50.3) 63 (34.4) 120 (64.6)
Total 364 (34.7) 131 (36.0) 233 (64.0)
Baseline caries group
High (dmft 0-5) 318 (30.3) 108 (34.0) 210 (66.0)
Very High (dmft 6-9) 356 (34.0) 136 (38.2) 220 (61.8)
Extreme (dmft >10)) 374 (35.7) 146 (39.0) 228 (61.0)
Total 1048 (100.0) 390 (37.2) 658 (62.8)

84
Data on sociodemographic characteristics of participants in Part 1 are presented in Table 3.2.
Children were spread evenly across schools although there was one large school (School XXI
from Phnom Penh) which had twice as many participants than other schools. Half of the
children in the sample were 8 years-of-age or older.
Table 3.2 – Part 1 - Sociodemographic Characteristics of Participants.
Male
N (Row %)
Female
N (Row %)
Total
N (Column %)
Age group (years)a
6-7 266 (50.6) 260 (49.4) 526 (50.7)
>8 263 (51.5) 248 (48.5) 511 (49.3)
School code
School I 12 (41.4) 17 (58.6) 29 (2.8)
School II 10 (41.7) 14 (58.3) 24 (2.3)
School III 18 (42.9) 24 (57.1) 42 (4.0)
School IV 26 (54.2) 22 (45.8) 48 (4.6)
School V 32 (64.0) 18 (36.0) 50 (4.8)
School VI 11 (44.0) 14 (56.0) 25 (2.4)
School VII 20 (55.6) 16 (44.4) 36 (3.4)
School VIII 11 (55.0) 9 (45.0) 20 (1.9)
School IX 33 (42.3) 45 (57.7) 78 (7.4)
School X 30 (62.5) 18 (37.5) 48 (4.6)
School XI 11 (73.3) 4 (26.7) 15 (1.4)
School XII 17 (51.5) 16 (48.5) 33 (3.1)
School XIII 2 (33.3) 4 (66.7) 6 (0.6)
School XIV 9 (47.7) 10 (52.6) 19 (1.8)
School XV 25 (47.2) 28 (52.8) 53 (5.1)
School XVI 24 (57.1) 18 (42.9) 42 (4.0)
School XVII 27 (50.9) 26 (49.1) 53 (5.1)
School XVIII 35 (55.6) 28 (54.5) 63 (6.0)
School XIX 15 (45.5) 18 (54.5) 33 (3.1)
School XX 36 (52.9) 32 (47.1) 68 (6.5)
School XXI 72 (53.7) 62 (46.3) 134 (12.8)
School XXII 32 (41.6) 45 (58.4) 77 (7.3)
School XXIII 26 (50.0) 26 (50.0) 52 (5.0)
TOTAL 534 (51.0) 514 (49.0) 1048 (100.0)
aDate of birth information missing from 9 participants

85
There was a statistically significant difference in the severity of caries by age-group, group
membership and school attendance (data are presented in Table 3.3). Children in Group C were
younger than those in Groups A and B. Those in Group C had a lower DMFT and a higher
dmft. There was a statistically significant amount of variation in caries experience among
schools.

86
Table 3.3 – Part 1 - Clinical Characteristics of participants by group membership.
DMFT
Mean (SD) P-value
dmft
Mean (SD) P-value
Any caries
N (Row %) P-value
Sex
Male 1.8 (2.1) 0.397 9.1 (4.2) 0.010 520 (97.4) 0.318
Female 1.9 (2.0) 8.4 (4.2) 497 (96.7)
Age group
6-7 y 1.5 (1.8) < 0.001 9.7 (4.2) < 0.001 514 (97.7) 0.120
>8 y 2.3 (2.1) 7.8 (3.9) 492 (96.3)
Group membership
Group A 2.2 (2.1) < 0.001 7.5 (4.1) < 0.001 240 (95.6) 0.209
Group B 2.3 (2.2) 8.3 (3.8) 420 (97.0)
Group C 1.2 (1.6) 10.2 (4.3) 357 (98.1)
School
School I 3.0 (2.6) < 0.001 8.3 (4.0) < 0.001 28 (96.6) 0.031
School II 2.3 (1.9) 8.8 (3.6) 24 (100.0)
School III 2.3 (25) 5.7 (4.0) 38 (90.5)
School IV 3.1 (2.7) 8.8 (3.6) 48 (100.0)
School V 2.4 (2.4) 8.2 (3.8) 50 (100.0)
School VI 2.5 (2.2) 8.0 (4.1) 25 (100.0)
School VII 2.3 (2.0) 8.7 (3.2) 36 (100.0)
School VIII 3.1 (2.5) 8.7 (3.5) 20 (100.0)
School IX 2.1 (1.8) 7.2 (4.3) 73 (93.6)
School X 2.9 (2.7) 8.1 (3.4) 48 (100.0)
School XI 2.4 (2.8) 8.1 (4.3) 15 (100.0)
School XII 2.1 (1.5) 8.6 (4.3) 33 (100.0)
School XIII 5.2 (1.8) 6.2 (3.2) 5 (83.3)
School XIV 1.5 (1.4) 6.8 (4.1) 17 (89.5)
School XV 2.2 (1.80 7.8 (3.8) 49 (92.5)
School XVI 1.4 (1.6) 8.4 (3.7) 40 (95.2)
School XVII 1.4 (1.4) 8.3 (4.3) 52 (98.1)
School XVIII 1.7 (1.8) 8.5 (4.1) 59 (93.7)
School XIX 1.2 (1.6) 10.2 (4.4) 32 (97.0)
School XX 1.7 (1.6) 10.3 (4.3) 67 (98.5)
School XXI 1.2 (1.6) 10.4 (4.3) 131 (97.8)
School XXII 0.9 (1.5) 9.5 (4.2) 75 (97.4)
School XXIII 1.0 (1.3) 10.8 (4.4) 52 (100.0)
TOTAL 1.9 (2.0) 8.8 (4.2) 1017 (97.0)
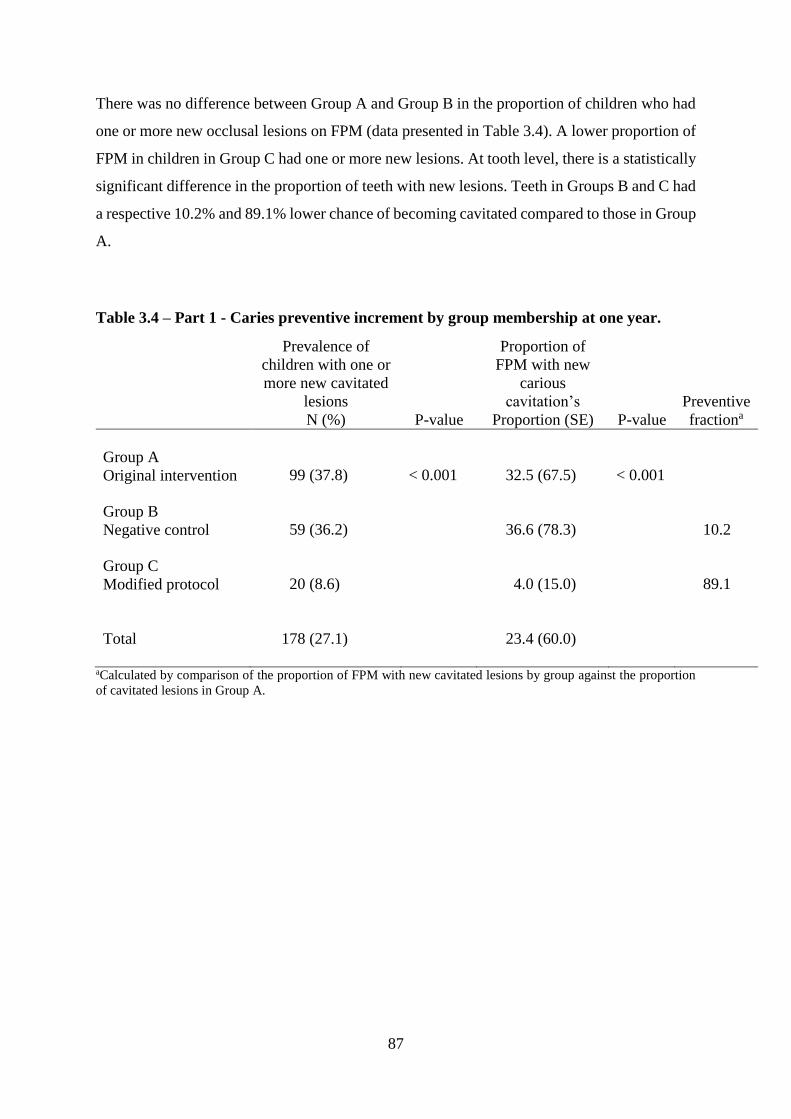
87
There was no difference between Group A and Group B in the proportion of children who had
one or more new occlusal lesions on FPM (data presented in Table 3.4). A lower proportion of
FPM in children in Group C had one or more new lesions. At tooth level, there is a statistically
significant difference in the proportion of teeth with new lesions. Teeth in Groups B and C had
a respective 10.2% and 89.1% lower chance of becoming cavitated compared to those in Group
A.
Table 3.4 – Part 1 - Caries preventive increment by group membership at one year.
Prevalence of
children with one or
more new cavitated
lesions
N (%) P-value
Proportion of
FPM with new
carious
cavitation’s
Proportion (SE) P-value
Preventive
fractiona
Group A
Original intervention 99 (37.8) < 0.001 32.5 (67.5) < 0.001
Group B
Negative control 59 (36.2) 36.6 (78.3) 10.2
Group C
Modified protocol 20 (8.6) 4.0 (15.0) 89.1
Total 178 (27.1) 23.4 (60.0)
aCalculated by comparison of the proportion of FPM with new cavitated lesions by group against the proportion
of cavitated lesions in Group A.

88
Children in Group A and Group B had more than six times the possibility for developing new
lesions on FPM (Table 3.5) when compared with Group C once baseline caries experience,
school, and gender were adjusted for.
Table 3.5 – Part 1 - Logistic regression model for risk of developing new carious lesions
based on group membership.a
B(SE) Odds Ratio (95% CI) P-value
Constant
-2.37 (0.23) - < 0.001
Group A
Original intervention 1.80 (0.29) 6.04 (3.46, 10.56) < 0.001
Group B
Negative control 1.87 (0.27) 6.47 (3.84, 10.90) < 0.001
Group C
Modified Protocol 0.0b
aCox and Snell – 0.102; Nagelkerke – 0.148; McFadden – 0.092 bThis parameter is set to zero because it is redundant

89
3.4.2 Part 2 – Two year evaluation of the modified protocol.
There was no significant difference in the distribution of the sociodemographic participants by
gender or age (Table 3.6); children in the control group had a statistically significant greater
proportion of female participants, although some schools (Schools II, IV, and V) had
statistically significant greater proportion of males. The mean age overall was 6.6 (SD 0.6)
years with no significant difference by group membership; Group C, 8.9 years (SD 0.6); Group
D, 6.5 years-of age (SD 0.6).
Table 3.6 – Part 2 - Characteristics of participants by gender, age, and group membership
and school.
Male
N (Row %)
Female
N (Row %)
Total
N (Column %) P-valuea
Age group (years)
Six 123 (48.0) 133 (52.0) 256 (41.7) 0.678
Seven 156 (47.3) 174 (52.7) 330 (53.7)
Eight 11 (39.3) 17 (60.7) 28 (4.6)
Group membership
Group C
Modified protocol 181 (50.8) 175 (19.2) 356 (57.5)
0.031
Group D
Positive control 113 (43.0) 150 (57.0) 263 (42.5)
School
School I 21 (20.0) 84 (80.0) 105 (17.0) < 0.001
School II 24 (60.0) 16 (40.0) 40 (6.5)
School III 24 (44.4) 30 (55.6) 54 (8.7)
School IV 21 (65.6) 11 (34.4) 32 (5.2)
School V 15 (65.2) 8 (34.8) 23 (3.7)
School VI 4 (100) 0 (0.0) 4 (0.6)
School VII 4 (80.0) 1 (20.0) 5 (0.8)
School VIII 15 (46.9) 17 (53.1) 32 (5.2)
School IX 36 (53.7) 31 (46.3) 67 (10.8)
School X 72 (55.8) 57 (44.2) 129 (20.8)
School XI 32 (42.1) 44 (57.9) 76 (12.3)
School XII 26 (50.0) 26 (50.0) 52 (8.4)
Total 294 (47.5) 325 (52.5) 619 (100.0)
aP-value calculated using χ2 statistics for differences among groups within the same column

90
There were some differences in dmft by gender, and school attendance. Males and some schools
had greater caries experience reaching statistical significance (Data are presented in Table 3.7).
Table 3.7 – Part 2 - Clinical characteristics of participants according to sociodemographic factors.
dmft
Mean (SD) P-valuea
DMFT
Mean (SD) P-valuea
Any caries
N (%) P-valuea
Sex
Male 10.4 (4.4) 0.013 1.2 (1.6) 0.001 290 (98.6) 0.562
Female 9.4 (4.1) 1.2 (1.6) 320 (98.5)
Age group (years)
Six 10.2 (4.6) 0.326 0.8 (1.4) < 0.001 251 (98.0) 0.611
Seven 9.8 (4.1) 1.6 (1.7) 326 (98.8)
Eight 9.0 (3.6) 1.7 (2.1) 28 (100.0)
Group membership
Group C 10.2 (4.3) 0.052 1.2 (1.6) 0.344 349 (98.0) 0.186
Group D 9.5 (4.2) 1.3 (1.7) 261 (99.2)
School
School I 9.8 (4.2) 0.013 1.3 (1.7) 0.064 104 (99.0) 0.955
School II 10.4 (4.0) 1.4 (1.6) 40 (100.0)
School III 7.6 (3.8) 1.3 (1.5) 53 (98.1)
School IV 10.6 (4.9) 1.4 (1.5) 32 (100.0)
School V 9.5 (3.5) 1.9 (2.8) 23 (100.0)
School VI 8.0 (5.8) 0.8 (1.0) 4 (100.0)
School VII 11.8 (3.8) 1.8 (1.8) 5 (100.0)
School VIII 10.2 (4.7) 1.2 (1.6) 31 (96.9)
School IX 10.3 (4.4) 1.7 (1.6) 66 (98.5)
School X 10.4 (4.3) 1.1 (1.6) 126 (97.7)
School XI 9.5 (4.1) 0.9 (1.6) 74 (97.4)
School XII 10.8 (4.4) 1.0 (1.3) 52 (100.0)
Total 9.9 (4.3) 1.3 (1.6) 610 (98.5)
aThe P-values presented are for differences among groups within the same column.

91
Data on attrition for Part 2 are presented in Table 3.8. There was a statistically significant
difference in follow-up by gender within the Group D where by a greater proportion of females
were followed-up at two years. There were no gender differences in follow-up within Group C
and there were no differences in follow-up by baseline caries experience.
Table 3.8 – Part 2 - Participant attrition analysis for the 2 year follow-up of the second
cohort.
Lost
N (%)
2-year follow up
N (%)
Total
N (Column %) P-valuea
Group C - Modified Protocol
Male 62 (34.3) 119 (65.7) 181 (49.7) 0.284
Female 59 (32.2) 124 (67.8) 183 (50.3)
Total 121 (33.2) 243 (66.8) 364 (57.5)
Group D – Positive Control
Male 45 (39.8) 68 (60.2) 113 (43.0) 0.017
Female 40 (26.7) 110 (73.3) 150 (57.0)
Total 85 (32.3) 178 (67.7) 263 (42.5)
Baseline Caries group
High (dmft <8) 61 (35.3) 112 (64.7) 173 (27.6) 0.576
Very High (dmft 8-10) 70 (30.4) 160 (69.6) 230 (36.7)
Extreme(dmft >10) 75 (33.5) 149 (66.5) 224 (35.7)
Total 206 (32.9) 421 (67.1) 627 (100.0)
aP-value for examining differences among groups within the same column

92
The children in Group C had a statistically significant greater FS retention rate at two years.
Those in Group D who had FS placed using the old protocol had a 7.5% (SE 21.6) retention
rate while those in the Group C who had sealants placed using the new protocol had a 17.1%
(SE 29.4) retention rate (P < 0.001). Children in Group C had a statistically significant one
third lower chance of developing a new carious lesion on FPM (Table 3.9). Differences were
further amplified after participants were stratified by baseline caries experience. Those children
in the High caries group had twice the caries preventive fraction compared with the two more
extreme risk groups. There was no significant difference in the prevalence of new pulpally
involved lesions; however, those in Group C had a statistically significantly lower chance of
experiencing oral symptoms.
Table 3.9 – Part 2 - Proportion of children with new carious lesions on occlusal of FPM
at 2-years by group membership.
Group C
Modified protocol
N (%)
Group D
Positive control
N (%)
Preventive
fraction (%) P-valuea
>1 new lesions FPM 72 (29.6) 70 (39.3) 32.3 0.024
>1 new pulpally
involved FPM 64 (26.3) 57 (32.0) 17.8 0.122
>1 impacts in oral
symptoms 117 (48.1) 122 (68.5) 29.8 < 0.001
Caries group
High 10 (16.7) 16 (30.8) 45.8 0.062
Very High 27 (30.3) 28 (39.4) 23.1 0.150
Extreme 35 (37.2) 26 (47.3) 21.4 0.152
aP-value for differences among groups within the same rows

93
The mean number of new interproximal lesions on FPM was 0.3 (SD 0.6) with a statically
significant greater mean number of interproximal lesions (P = 0.037; Kruskal-Wallis) in the
Modified Protocol group (0.3; SD 0.7) compared with the positive control group (0.2; SD 0.5).
One in five children (N = 83) within this cohort developed new interproximal lesions over the
observation period. Overall, the mean number of new lesions in FPMs was 0.5 (SD 0.8) for
both groups; therefore, interproximal lesions account for over half of the FPM increment in the
intervention group C and a lower proportion in the Positive Control group D (Table 3.10). Once
participants were divided by baseline caries experience, the preventive fraction was larger for
those with a less extreme caries experience.
Table 3.10 – Part 2 - Proportion children with new cavitated occlusal and interproximal
carious lesions by group membership.
Group C
Modified
Protocol
N (%)
Group D
Positive Control
N (%)
Preventive
fraction
(%)a P-valueb
>1 new occlusal
cavitated lesions on FPM 53 (21.8) 63 (35.4) 38.4 0.002
>1 new interproximal
cavitated lesions on FPM 56 (23.0) 24 (15.2) - 0.029
Baseline Caries group
High (dmft <8) 6 (10.0) 15 (28.8) 65.3 0.015
Very High (dmft 8-10) 23 (25.8) 24 (33.8) 23.7 0.298
Extreme(dmft >10) 24 (25.5) 24 (43.6) 41.5 0.029
aPreventive fraction calculated by dividing the proportion of that in the positive control group by that in the
modified protocol group bP-value relates to differences in groups within the same row

94
Data on odds ratios for developing new cavitated lesions on FPM by group membership are
presented in Table 3.11. Two models were created using logistic regression, when all lesions
involving the occlusal surface were considered then those in the control group had a 1.54x
greater chance of developing a new lesion over two years. After the occlusal lesions that
involved interproximal surfaces were excluded; children in the positive control group had twice
the chance of developing new lesions that were situated on the occlusal surface.
Table 3.11 – Part 2 - Logistic regression models showing odds ratio for the chance of
developing one or more occlusal lesions on FPM at two-years.a
Model 2 – All new lesions involving the occlusal and approximal lesions.b
B(SE) Odds Ratio (95% CI) P-value
Constant 0.86 (0.14) - < 0.001
Group D
Positive Control -0.431 (0.208) 1.54 (1.02, 2.314) 0.038
Group C
Modified Protocol 0
Model 3 – new lesions involving only occlusal surface.c
B(SE) Odds Ratio (95% CI) P-value
Constant -1.227 - < 0.001
Group D
Positive Control 0.675 (0.221) 1.96 (1.27, 3.03)
0.002
Group C
Modified Protocol 0
aAdjusted for school of attendance and baseline caries experience bCox and Snell – 0.010; Nagelkerke – 0.014; McFadden – 0.008 cCox and Snell – 0.022; Nagelkerke – 0.032; McFadden – 0.019

95
3.5 Discussion
3.5.1 General findings
The present study examined the effectiveness of the original SEAL Cambodia protocol against
a modified protocol at one and two years. It represents an important contribution to the limited
body of evidence around the prevention of caries using GIC FS applied outside the dental
surgery given that the most recent meta-analysis reported insufficient evidence for this
technology (Ahovuo‐Saloranta et al. 2017). The modified protocol produced a large preventive
increment at one year and a moderate preventive increment at two years. Child participants had
an extreme experience of dental caries which resulted in a high incidence of open approximal
lesions on FPM that extended onto the occlusal surface. Before detailed examination of the
findings of the study, it is appropriate to examine the study strengths and limitations.
The strengths were associated with the robust randomised cluster sampling procedure;
however, the follow-up rates fell short of the ideal. Further measures were put in place at the
two year follow-up which resulted in a 5% increase in follow-up. The children in the study
were representative of the wider SEAL project and representative of those in their respective
province based on data from the Cambodia National Oral Health Survey (CNOHS) (Chher et
al. 2016). Despite this, it appears that the rate of approximal lesions on FPM was higher in
Phnom Penh compared with Kampot and this may have limited some of the comparability
among the second cohort (Groups C and D).
This is the first study to report caries preventive fractions of GIC sealants among a group of
children with a disproportionately severe caries experience. It has been reported in other studies
that higher caries risk was associated with lower preventive increments, as observed in the
present study (Ahovuo-Saloranta et al. 2017). Children in the lower tercile of caries experience
had a comparable caries experience to those considered to be in the ‘high risk’ group of
previously published investigations.
3.5.2 Preventive benefit of the SEAL Cambodia intervention
The caries experience at baseline played an important role in explaining the overall caries
preventive effect at two years. Those in the extreme caries groups did not realise a statistically
significant reduction in the incidence of new carious lesions on FPM. The 38% preventive
fraction achieved was at the higher end of the confidence interval reported in the most recent

96
Cochrane review (Ahovuo‐Saloranta et al. 2017). It is clear that this preventive increment
would not have been possible without the use of the revised protocol that featured additional
control measures. It is also worth commenting that 20% of the children in the intervention
group developed new carious lesions on approximal surfaces during the course of observation.
Although caries prevention/control was observed among this group, this intervention did not
address the drivers of dental caries such as dietary or oral hygiene practices. That meant that
the same teeth which may have realised some benefit on the occlusal surface could have been
compromised by the cavitated approximal lesions. As such, the value of the SEAL Cambodia
intervention lies in its place as an appropriate first step of the dental community in Cambodia
to re-orientate services from ‘bottom of the cliff’ and towards services based on a foundation
of interventions to maintain oral health. That an untold number of dental students, dentists,
therapists and hygienists from Cambodia and abroad participated in delivering this intervention
was a valuable demonstration of the possibilities in terms of the role of dental professionals to
move ‘up stream’. Seal Cambodia formed a foundation upon which the dental community
could better understand the target population and form the basis upon which more
comprehensive strategy could be built; One-2-One Cambodia 2016.
3.5.3 Protocol considerations
One of the important findings of the project was the difference in preventive increment across
two different protocols, both of which were consistent with the manufacturer’s instructions and
based on the assumption of a temperate working environment. The key difference between the
protocols was the use of control measures to regulate the operators work flow and material
temperature. While GIC materials are claimed to be moisture tolerant, it appears that there is
wide variation in setting reaction depending on the temperature of the liquid. The original
protocol used material at ‘room temperature’ that is likely to be higher than 30 °C which could
have resulted in a faster setting time and the FS material being delivered to the tooth in the
‘gelatinous’ phase rather than during the initial working phase (Berg & Croll 2015). This would
have resulted in the material failing to flow into the deep pits and fissures and failing to form
an adhesive bond on the surface of the tooth. The gelatinous phase of setting is the time at
which the material is most sensitive to leaching valuable ions on contact with moisture (Berg
& Croll 2015). Therefore, the additional moisture control provided by the one-minute finger
press was essential for protecting the material as it transitions through the setting phases. This
ensured the maximum compressive strength of the material could be achieved. Finally, the

97
temperature of the material affects the volume dispensed by one drop from the GIC liquid
bottle. At 25-30 °C approximately 115-120 drops can be dispensed. In contrast, only 100-105
drops were dispensed from a bottle that is cooler than 20 °C. The temperature of the liquid had
a major impact on all steps of the SEAL protocol.
It is possible that the choice of Fuji VII® rather than Fuji IX® could have created a scenario in
which the protocol is more technique sensitive. Fuji IX® has a two minute working time
compared to a working time for Fuji VII® of one minute. Although a pilot study demonstrated
better retention of Fuji VII® at 6 months, it is possible that there could be some benefit in using
Fuji IX® in order to allow for a more forgiving protocol. In any case, the SEAL Cambodia
project shows that an adjustment and strict monitoring of a protocol, taking into account local
conditions, can make the difference between whether an intervention benefits participants or
not.
While the preventive fraction at one year was comparable to that in other studies, the two year
preventive fraction was lower than expected (40%) and the finding that sealants were being
lost gradually over time leads to the question of whether GIC was the optimal choice of
material. It could be possible that a resin sealant with a higher retention rate could have
achieved higher two year preventive results. Unfortunately, placing resin sealants would
require significant equipment investment and it is unlikely that this would have been achievable
at scale or in the school environment in Cambodia. The alternative to a school environment
would be to transport children to an equipped clinic but that would have been more problematic
in terms of consent, transport costs, supervision, safety and time lost from class. In addition,
many of the teeth that were targeted for sealants were not yet fully erupted and therefore, resin
sealants, requiring meticulous moisture control, were contraindicated.
The next question to consider is why the retention rates were lower than those reported in other
studies (Chen & Liu, 2013). The Pilot studies (Chapter 2) demonstrated that the loss of material
is gradual, rather than because of early failure, therefore, it is proposed that the material is lost
due to wear or an erosive process. Other researchers have reported the presence of retained
GIC fragments held microscopically in the base of the fissure system (Kamala & Hegde, 2008;
Chen & Liu, 2013). It is not clear if this might be the case for the present study due to the fact
that those studies were on ART Sealants placed using high viscosity Fuji IX GIC rather than
Fuji VII. In light of the early loss of GIC, one should consider whether re-examining children
and replacing or repairing lost or deficient GIC sealants after one year should be recommended.

98
This conundrum further highlights the inadequacy of GIC fissure sealants as a stand-alone and
one-off preventive strategy.
3.5.4 Self-reported oral symptoms
One unique aspect of this study is the inclusion of a self-reported oral health measure as an
outcome. Although there was no statistically significant difference in the prevalence of new
pulpally involved lesions, and a higher rate of approximal carious lesions among Group C (the
modified protocol group) there was a significant difference in oral symptoms as reported by
the oral symptoms subdomain of the Child Perceptions Questionnaire. The proportion of
children in the original validation sample with impacts in oral symptoms was similar to those
in the control group of the second cohort (Turton et al. 2015) and the intervention appeared to
realise a one third reduction in the proportion of children experiencing oral symptoms. A
reduction in oral symptoms among a population with such a severe caries experience is
valuable and warrants further investigation into the role of dental interventions in improving
the quality-of-life for young children in Cambodia.
3.5.5 The theoretical argument for SEAL as a preventive strategy
The theory behind targeting FPM in 6 to 8 year-old children was that (a) the majority of new
lesions that occur in the early permanent dentition occur on occlusal surfaces of FPMs, (b) that
there is a window of around two years when enamel is less mature and more soluble, and (c)
that diet and oral hygiene may improve across the primary school years due to a fixed school
routine and lower consumption of sugary food (Chher et al. 2016). Unfortunately, the natural
history of caries among Cambodian children did not follow the pattern described in other
sealant studies among mostly western populations which have better access to fluoride and
lower exposure to non-nutritious foods.
In Cambodian children a large number of lesions develop in permanent teeth other than FPM
and analysis of the CNOHS data shows that two in five 12-year-old children have cavitated
carious lesions on maxillary anterior teeth. In addition, improvements in oral hygiene routines
and dietary practices don’t appear to occur until the children are older and reach secondary or
high school (Oral Health Bureau, 2014). Part of this is because primary school in Cambodia is
only four hours-per-day and 180 days-per-year. Although there is a ‘healthy food’ policy from
the school health department (Ministry of Education Youth and Sport, 2015), anecdotal
evidence would suggest that most schools make further income by allowing vendors onto the

99
school grounds to sell (often non-nutritious) foods and drinks to children. This demonstrates
that the underlying theory, based on ‘at risk’ populations in a western setting do not apply well
in a Cambodian setting.
In addition to the socio-behavioural factors compromising the success of a sealant program in
6 to 8 year-old children, the present project was confounded by the uncontrolled caries process
that was underway by the time the children arrived in the school environment. One in four
participants already had cavitated lesions in FPM at baseline. This suggests the need to address
the caries process for children before they enter the school system. At the time that the SEAL
Cambodia strategy was conceived in 2010 there had only been one published report of ECC in
a small Cambodian community of garment workers’ children (Todd et al. 1994). A more
comprehensive understanding of the natural history of dental caries, particularly among the
youngest age groups, would have been helpful in informing strategy for larger scale oral health
interventions in Cambodia.
3.6 Conclusion
The modified FS protocol rendered an improved preventive fraction compared to the original
protocol at one year. However, the two year preventive increment was not as beneficial as
expected due to a large proportion of approximal lesions on FPM. Further investigation is
needed to examine how benefit could be gained by addressing the caries burden prior to the
arrival of children in the school environment.

100
3.7 References Chapter 3
Ahovuo‐Saloranta, A., Forss, H., Walsh, T., Nordblad, A., Mäkelä, M. & Worthington, H.V.
(2017) Pit and fissure sealants for preventing dental decay in permanent teeth. The Cochrane
Library.7, CD001830.
Berg, Joel H. & Theodore P. Croll (2015) Glass Ionomer Restorative Cement Systems: An
Update. Pediatric Dentistry, 37 (2), 116–124.
Bratthall, D. (2000) Introducing the Significant Caries Index Together with a Proposal for a
New Global Oral Health Goal for 12-Year-Olds. International Dental Journal 50, (6), 378–
384.
Chen, X. X. & Liu, X.G. (2013) Clinical Comparison of Fuji VII and a Resin Sealant in
Children at High and Low Risk of Caries. Dental Materials Journal, 32 (3), 512–518.
Chher, T., Turton, B.J., Hak, S., Beltran, E., Courtel, F., Durward, C. & Hobdell, M. (2016)
Dental caries experience in Cambodia: Findings from the 2011 Cambodia National Oral Health
Survey. Journal of International Oral Health, 8 (1), 1.
Kamala, B. & Hegde, A. (2008) Fuji III vs. Fuji VII glass ionomer sealants–a clinical study.
Journal of Clinical Pediatric Dentistry, 33 (1), 29-33.
Ministry of Education Youth and Sport, Cambodia (2015) Policy for food in schools.
One-2-One Cambodia (2016) SEAL Cambodia final report. Phnom Penh, Cambodia.
Oral Health Bureau, Ministry of Health Cambodia (2014) Cambodia National Oral Health
Survey Final Report. Phnom Penh, Cambodia.
Tak N, Turton B, Durward C (2015) Seal Cambodia – A comparison of two protocols; IADR
SEA 29th Annual meeting, Bali, Indonesia.Presentation ID: 071
Todd, R.V., Durward, C.S., Chot, C., So, P.K. & Im, P. (1994) The dental caries experience,
oral hygiene and dietary practices of preschool children of factory workers in Phnom Penh,
Cambodia. International Journal of Paediatric Dentistry, 4(3), pp.173-178.
Turton, B.J., Thomson, W.M., Foster Page, L.A., Saub, R.B. & Razak, I.A. (2015) Validation
of an oral health–related quality of life measure for Cambodian children. Asia Pacific Journal
of Public Health, 27 (2), NP2339-NP2349.

99
Chapter 4
Socio-behavioural risk factors for Early Childhood Caries
(ECC) in Cambodian preschool children.
Published in part as:
Turton B J, Durward C S, Manton D (2015) Early Childhood Caries and Maternal
Caries Experience in a Convenience Sample of Cambodian Pre-schoolers. Pediatric
Dental Journal 25 (1), pp. 14-18.
Turton B J, Durward CS, Manton D, Bach K, Yos C (2015) Socio-behavioural risk
factors for early childhood caries (ECC) in Cambodian preschool Children
European Archives of Paediatric Dentistry. 17(2), pp. 97-105

100
Abstract
Objective: The aim of the present study was to explore the socio-behavioural risk factors
for ECC in Cambodia.
Methods: A convenience sample of 362 Primary Caregiver (PCG)-child dyads with
children ranging from birth through to six years-of-age participated in a structured
interview and intra-oral examination.
Results: 244 of 362 (65.6%) participants had Early Childhood Caries (ECC) and 50.6%
had Severe Early Childhood Caries (sECC). There were significant associations between
caries experience and tooth-brushing, dietary and nursing habits. The Odds Ratio (OR)
for sECC in children who started brushing before the age of 18 months was 0.41 (CI 0.18,
0.93), whilst for children who continued to breast-feed after the age of two years the OR
was 5.31 (CI 1.50, 18.79).
Conclusions: The most prominent risk factors for ECC in the present study were lack of
tooth-brushing and continued breast-feeding past the age of two years.

101
4.0 Chapter 4 – Cambodia Smile cross-sectional study.
Introduction
Children in Cambodia have a high burden of dental caries and the CNOHS reported that
the mean dmft for 6 year-old children was 9.0 (SD 4.9) and the prevalence of pulpally
involved primary teeth was 64.8% (Chher et al. 2016). This burden of dental caries
suggests that school age is too late for successful preventive intervention and prior to the
present study, little was understood about the natural history of ECC in the Cambodian
context. The only published report on ECC in Cambodian preschool children prior to this
body of work was from a convenience sample of the children of factory workers in Phnom
Penh in 1994. The authors reported a mean dmft of 5.7 (SD 5.2) for children with a mean
age of 4 (SD 1.4) years (Todd et al. 1994). Aside from this study, there is very little
information available about the pattern, severity and risk factors involved with the caries
experience of Cambodian pre-schoolers. Although the cause and drivers of dental caries
are well known and well documented (Sheiham & James 2015), specific investigation in
each setting is beneficial in order to better understand how known socio-behavioural
factors influence ECC in a Cambodian environment.
Dental caries in preschool children has been given a variety of labels including ‘baby-
bottle decay’, ‘nursing caries’ and most commonly ECC and severe-ECC (sECC) (Ismail
& Sohn 1999). The American Academy of Paediatric Dentistry defines sECC as ‘any
sign of smooth-surface caries in children below the age of 3 years; from ages 3 through
5, 1 or more cavitated, missing (due to caries), or filled smooth surfaces in primary
maxillary anterior teeth or a decayed, missing, or filled score of ≥ 4 (age 3), ≥ 5 (age 4),
or ≥ 6 (age 5)’(Drury et al. 1999). All definitions involve the use of the DMF/dmf index
which has some limitations in capturing the true extent of dental caries in the Cambodian
population as the carious lesion is often extensive and this is not fully captured by the
DMF/dmf index, in addition the carious lesions are largely untreated (Chu et al. 2008;
Todd et al. 1994). To address this issue the PUFA index is used to record the severity of
untreated carious lesions by recording the extent of pulpal involvement and augments the
information provided by the DMF index, and as such more accurately describes untreated
carious lesions in high caries populations (Monse et al. 2010).
The impact of ECC on the lives of children includes pain and infection, failure to thrive,
low weight, difficulty studying and absenteeism from school, and social problems

102
(Abanto et al. 2011; Gift et al. 1992). These justify an investigation of ECC in the
Cambodian environment. Such an investigation also provides some context for the
possibility that addressing and reducing caries experience in this age group may lead to
improved life-long oral health among the wider Cambodian population.
That Cambodian children have severe caries experience that is not well described
highlights the need to understand the underlying determinants of dental caries in the
Cambodian context better. Previous authors studying young children in other countries
have proposed risk models for ECC and implicated, as contributing/associated factors,
some common variables such as bottle-feeding, prolonged night-time breast-feeding, the
consumption of sugary drinks, lack of oral hygiene habits, low socioeconomic status
(SES), and high maternal caries experience (Çolak et al. 2013). Studies relating to
Cambodia report unfavourable oral hygiene practices and weaning practices (Chu et al.
2008; Bach 2015).
Two of the most common predictors of a child’s dental caries experience are untreated
caries experience of the primary caregiver (PCG) (Abiola et al. 2009; Li & Caufield 1995;
Nowjack-Raymer & Gift 1990; Steffensen 1990) and SES (Willems et al. 2005; Desai &
Alva 1998). The typical family unit in Cambodia may be different from that in other
societies and anecdotal evidence suggests that the grand-parents often play an important
role in raising children. Previous studies have not investigated the relationship between
caries experience of the PCG and preschool children they care for in Cambodia.
The ‘Cambodia Smile’ cross-sectional study was conducted to investigate the risk
indicators for ECC in the Cambodian context to inform strategies for reducing the burden
of dental caries among young children in Cambodia.

103
4.1 Aim
To describe the epidemiological aspects of ECC in a Cambodian context in order to
identify modifiable risk factors for future intervention.
4.2 Objective
To examine the natural history of caries disease patterns and to identify the socio-
behavioural factors of ECC that are risk indicators of severe caries experience among a
convenience sample of Cambodian preschool children and their Primary Care Givers.

104
4.3 Methods
4.3.1 General approach
The present study was a cross-sectional survey of a convenience sample of 362 Primary
Caregiver-child dyads. Each PCG took part in a structured interview and both the PCG
and the child had a standardized intra-oral examination. This survey was part of the
‘Cambodia Smile’ project, an initiative by a locally-based NGO One-2-One Cambodia.
This chapter reports some of the findings from the ‘Cambodia Smile’ survey.
Data collected by the NGO was collected under the jurisdiction of an organisation
conducting a needs assessment for a health program. The de-identified data set was then
analysed for the present study and ethical approval for re-analysis of the existing data set
was provided by University of Melbourne, Health Sciences Human Ethics Sub-
Committee (Ethics ID: 1545412). The investigators followed ethical principles by
obtaining informed consent (from the individuals and from community leaders) and
ensuring that participants benefited from taking part in the survey; each participant
received a toothbrush and fluoridated (1000 ppm F) toothpaste as well as oral health
education.
4.3.2 Participants
A convenience sample of PCGs and their preschool children (younger than 6 years-of-
age) was obtained through mobile dental clinics. The local village chiefs gave consent
for the survey and invited members of the village to participate. Children from three
provinces of Cambodia took part: Kampong Speu (two different sites with 95 pairs from
Kampong Speu 1, and 92 pairs from Kampong Speu 2); Preveng (77 pairs); and Phnom
Penh (98 pairs). Interviewers and examiners consisted of senior dental students and
dentists (all native Khmer speakers) who volunteered to work in a mobile dental clinic
(operated by the NGO One-2-One Cambodia). The team comprised six examiners and
interviewers at each survey site. All were trained and underwent standardization exercises
before the study began.
All PCGs with a preschool child were invited to take part and the interviewers obtained
informed consent by explaining the study verbally and then obtaining written consent.
All interviews were conducted in Khmer.

105
4.3.3 Clinical Measures
Teeth were not cleaned and were examined wet, consistent with WHO guidelines (WHO
2013). The lead investigator trained four other examiners by examining five participants
and comparing and discussing the findings. Each tooth was given two codes, one for
DMFT status and another for PUFA status (Monse et al. 2013). The data were recorded
on paper records (Appendix 8) then entered into an Excel® spread sheet (Microsoft Corp.,
WA, USA). ECC and sECC were determined according to definitions given by the
American Academy of Pediatric Dentistry (AAPD). Caries severity was further
categorised by using the Significant Caries Index (Bratthall, 2000), which identified the
most severely affected 30% of participants. For this variable all PCGs were grouped
together and children were grouped according to age.
4.3.4 The questionnaire
Parents or Caregivers were asked a range of questions relating to oral health and general
health behaviours. Each interviewer spoke Khmer as their first language and received
training on how to conduct the interviews. The interviews were structured and conducted
in Khmer and followed a written set of questions. The items that were used along with
the response options are presented in Table 4.4 & 4.5. If the PCG responded that breast-
feeding had continued past the age of 24 months (even if the feeding had ceased at the
time of the examination), they were categorised as breast-feeding over the age of two-
years.
4.3.5 Data analysis
Data were analysed using SPSS Ver. 20 (IBM, NY, USA). Descriptive statistics were
generated prior to undertaking bivariate and multivariate analysis. Differences among
proportions were compared using the chi-squared (χ2) test. Differences between means
were compared using the Mann-Whitney U-test or the Kruskal-Wallis H-test as
appropriate. Multivariate analysis was conducted by using binary logistic regression to
examine the predictors of sECC and a multinomial stepwise regression model to predict
membership to the groups of ‘ECC’, ‘sECC’, and ‘Significant Caries’. The version of
SPSS did not have an option for producing collinearity statistics for logistic models and
therefore the same variables were entered into a linear regression model to test for multi-
collinearity. All variables identified with a statistically significant association with caries

106
experience during bivariate analysis were entered into the binary logistic regression
model.

107
4.4 Results
Data on the sociodemographic characteristics of participants by sex are presented in
Table 4.1. The children were aged from 1 month to 6 years-of-age. Mean age was 42
months (SD 19). Greater than two thirds of participants had their mother as the primary
caregiver. There was an even distribution by sex and location, however, the mean age of
participants differed significantly (P < 0.005; χ2 test) by their relationship to the PCG and
by location. Children who did not have their mother as their PCG were, on average, eight
months older and those from the Phnom Penh sample were five months younger than the
mean age (P < 0.005; t-test).
Table 4.1 – Cambodia Smile cross-sectional study - Sociodemographic characteristics of
participants.a
Male
N (%)
Female
N (%)
Mean Age in
months (SD)
Total
N (column %)
Location
Kampong Speu 1 50 (28.2) 44 (24.0) 44 (18)b 95 (26.2)
Prey Veng 37 (20.9) 39 (21.3) 42 (23) 77 (21.3)
Phnom Penh 51 (28.8) 47 (25.7) 36 (17) 98 (27.1)
Kampong Speu 2 39 (22.0) 53 (29.0) 46 (18) 92 (25.4)
Primary caregiver
Mother 124 (70.1) 135 (73.8) 40 (19)b 261 (72.1)
Other primary
caregiver
53 (29.9) 48 (26.2) 48 (17)b 101 (27.9)
Education of
primary caregiver
Illiterate 40 (22.6) 35 (19.1) 42 (19) 75 (20.7)
Preschool 48 (27.1) 58 (29.0) 42 (18) 101 (27.9)
Primary school 64 (36.2) 74 (40.4) 42 (20) 139 (38.4)
Secondary school 11 (6.2) 5 (2.7) 44 (19) 17 (4.7)
University 14 (7.9) 16 (8.7) 38 (21) 30 (8.3)
Total c 177 (48.9) 183 (50.6) 42 (19) 362 (100.0)
a Sex data missing from two participants; brackets contain row percentages unless otherwise indicated. b Significantly difference among groups within the same column; P < 0.05; χ2 test or Kruskal-Wallis test
as appropriate.

108
Some differences existed in caries experience of the children based on sociodemographic
indicators (Table 4.2). There was a statistically significant difference in caries experience
of the children by location and relationship to the PCG. Children who had someone other
than their mother as their PCG had a higher dmft score and approximately 5% greater
prevalence of ‘any caries’ experience and sECC when compared with the overall group.
The children from Prey Veng had a higher dmft (7.0 SD 6.4); however, the children from
Kampong Speu 1 had a higher prevalence of caries (+ 10%) and a higher prevalence of
sECC, cavitated carious lesions in anterior and posterior teeth (+ 5%). Two thirds of
children had cavitated carious lesions present and one half had sECC. Approximately half
of the children had cavitated carious lesions involving the posterior teeth and nearly two
thirds of children had cavitated carious lesions involving the anterior teeth.
The bivariate analysis of PCG caries experience by caries experience of the children is
presented in Table 4.3. A significant positive association existed between child and
mother caries experience. Children of mothers with pulpally involved teeth or ‘significant
caries’ had more greater caries experience (P < 0.05). There was no statistically
significant association between the caries experience of the PCG who were not the
mothers of the children in their care.

109
Table 4.2 – Cambodia Smile Cross-sectional study - Socio-demographics characteristics by caries experience of the child.
dmft
Mean (SD)
Any caries
N (row %)
Any PUFA
N (row %)
SECC
N (row %)
Significant caries
N (Row %)
Anterior Caries
N (row %)
Posterior caries
N (row %)
Sex
Male 5.4 (5.5) 117 (66.1) 45 (25.4) 90 (52.9) 60 (33.9) 107 (60.5) 97 (54.8)
Female 5.3 (5.5) 123 (67.2) 59 (32.2) 85 (49.7) 60 (32.8) 107 (58.5) 98 (53.6)
Location (Community)
Kampong Speu 1 5.6 (5.5)a 74 (77.1)a 27 (28.1)a 61 (63.5)a 33 (34.4)a 67 (69.8)a 62 (64.6)a
Prey Veng 7.0 (6.4) 54 (67.5) 35 (43.8) 40 (59.7) 40 (50.0) 51 (63.8) 49 (31.2)
Phnom Penh 3.4 (4.8) 50 (50.5) 26 (26.3) 33 (33.7) 26 (26.3) 43 (43.4) 38 (38.4)
Kampong Speu 2 4.4 (4.4) 66 (68.0) 17 (17.5) 44 (48.4) 23 (23.7) 56 (57.7) 50 (51.5)
Primary Caregiver education
Illiterate 5.6 (5.4) 56 (72.7) 23 (29.9) 41 (56.9) 26 (33.8) 49 (63.6) 44 (57.1)
Preschool 4.2 (4.6) 62 (59.6) 27 (26.0) 44 (44.4) 26 (25.0) 53 (51.0 52 (50.0)
Primary school 5.8 (5.9) 95 (66.4) 42 (29.4) 70 (51.9) 51 (35.7) 89 (62.2) 76 (53.1)
Secondary school 6.0 (5.0) 13 (76.5) 3 (17.6) 10 (58.8) 7 (41.2) 10 (58.8) 16 (51.6)
University 5.3 (6.2) 18 (58.1) 10 (32.3) 13 (44.8) 51 (35.7) 16 (51.6) 11 (64.7)
PCG relationship to child
Mother 6.1 (5.2)b 165 (61.3)a 76 (28.3) 121 (47.5)b 90 (32.8) 151 (56.1) 132 (49.1)a
Other relationship 5.0 (5.6) 79 (76.7) 29 (28.2) 57 (58.8) 32 (31.1) 66 (64.1) 67 (65.0)
Total 5.3 (5.4) 244 (65.6) 105 (28.2) 178 (50.6) 122 (32.8) 217 (58.3) 199 (53.5)
a P < 0.01; χ2 test or Kruskal-Wallis test as appropriate for comparison of groups within the same column b P < 0.05; χ2 test or Kruskal-Wallis test as appropriate for comparison of groups within the same column

110
Table 4.3 – Cambodia Smile cross-sectional study - Maternal caries experience by Child caries experience.
dmft
Mean (SD)
Any caries
N (row %)
Any PUFA
N (row %)
SECC
N (row %)
Significant caries
N (row %)
Anterior caries
N (row %)
Posterior Caries
N (row %)
Mother
Any caries 5.1 (5.6)a 152 (63.3)b 70 (29.2) 111 (48.9) 82 (34.2) 138 (57.5) 123 (51.2)b
Any PUFA 5.8 (5.8) 108 (67.5)b 55 (34.4)a 81 (54.4)b 62 (38.8)b 98 (61.2)b 89 (55.6)b
Significant Caries 6.9 (6.1)a 63 (70.8)b 31 (34.8) 52 (65.0)a 42 (47.2)a 61 (68.5)b 54 (60.7)b
Other Caregiver
Any caries 6.3 (5.2) 70 (79.5) 24 (27.3) 50 (61.0) 28 (31.8) 58 (65.9) 58 (65.9)
Any PUFA 6.5 (5.5) 55 (79.7) 19 (27.5) 39 (60.0) 23 (33.3) 48 (69.6) 45 (65.2)
Significant Caries 6.7 (5.8) 30 (81.1) 10 (27.0) 20 (60.6) 13 (35.1) 27 (73.0) 21 (56.8)
a P< 0.01; χ2 test or Kruskal-Wallis test as appropriate for differences among groups within the same column b P<0.05; χ2 test or Kruskal-Wallis test as appropriate for differences among groups within the same column

111
The responses to the questionnaire are presented in Table 4.4 and 4.5. Nearly two thirds of
children did not have their teeth cleaned and of those who did, three in five did not have any
help with brushing. Most of the mothers (95.4%) had breast-fed the child at some stage and
more than half of the mothers with children 4 to 5 years-of-age were still breast feeding. In
addition, the great majority of children (94.4%) slept with their mother at some stage, and more
than two thirds of the children aged over three years still slept with their mother at night.

112
Table 4.4 – Cambodia Smile cross-sectional study - Questions on nursing habits and oral
health behaviours by responses from the primary-caregiver.
Oral Hygiene N
(column %)
Does your child have his/her teeth
cleaned?
Yes
No
142 (38.2)
230 (61.8)
If yes how? Toothbrush
Other
125 (88.0)
17 (12.0)
Who brushes your child’s teeth?
Child by themselves
Child with help from parent
or someone else
81 (57.0)a
61 (43.0)
How often does your child usually have
his/her teeth brushed?
Less than once a day
> Once a day
34 (23.9)a
108 (76.1)
What age did tooth-brushing start?
Given in months < 18 months
>18 months
31 (8.3)a
341 (91.7)
Does your child use toothpaste?
Yes
No
106 (74.6)a
36 (25.4)
If your child doesn’t use toothpaste, why
not?
Don’t think it’s necessary
Cost too much money
Other reason
Data missing
20 (27.8)a
27 (37.5)
25 (34.7)
70
Nursing Habits
Did (or does) your child sleep with you at
night
Yes
No
351 (94.4)
21 (5.6)
If yes, age of stopping sleeping with child
Age given in
months and
grouped into
years.
>1 year
> 2 years
> 3 years
> 4 years
351 (100.0)
331 (94.3)
291 (82.9)
244 (69.5)
Did you ever breast-feed your child?
Yes
No
355 (95.4)
17 (4.6)
Still breast feeding?
Yes
No
76 (20.4)b
296 (79.6)
If no, when did breast-feeding stop
Age in months
then grouped
into years
>1 year
> 2 years
> 3 years
> 4 years
355
(100.0)b
338 (95.2)
276 (77.7)
208 (58.6)
After age 1 did your child breast-feed at
night?
Yes
No
Don’t Know
253 (71.3)b
91 (25.6)
11 (3.1)
a Proportion within those who brush their teeth b Proportion within those who breastfeed

113
The mean age for introducing solids into the infants’ diet was just older than one year
(Table 4.5). Half of the caregivers reported adding sugar to weaning foods. Most of the
children consumed sweet drinks and sweet foods more than two times-per-day.
Only one in three PCG reported that their child had ever used a baby bottle. Among those
who had used a bottle, the mean age for stopping bottle-feeding was two years. Within
the bottle-feeding group, two thirds were bottle-fed at night beyond the age of one year,
and one third added sugar to the contents of the bottle.

114
Table 4.5 – Cambodia Smile cross-sectional survey - Questions on dietary habits by responses from the
primary caregiver.a
Dietary Habits
What age did you introduce solid foods to your child?
Given in months (Mean and standard
deviation)
13 (SD 13)
What weaning foods did you give to your baby?
Asked to list and if
sugar was added.
Sugar added
No sugar added
195 (51.6)
180 (48.4)
How many times during the day does your child have:
sweet drinks, sweets, sweet snacks, fruit, vegetables,
plain (unsweetened) milk
Frequency given as
> two times per day.
select >1
Sweet drinks
Sweets
Sweet snacks
Fruit
Vegetables
Plain milk
332 (89.2)
294 (79.0)
212 (57.0)
304 (81.7)
129 (34.7)
328 (88.2)
What does your child usually drink?
Asked to list.
Select >1.
Water
Milk
Juice
Coffee
327 (87.9)
55 (14.8)
49 (13.2)
12 (3.2)
What snacks does your child usually eat?
Asked to list. Could
select >1
Packaged snacks
Rice porridge
Rice
Fruit
Sweet fried cake
Sweet bread
Ice cream
Meat
Other
185 (49.7)
143 (38.4)
177 (47.6)
20 (5.4)
26 (7.0)
24 (6.5)
3 (0.8)
7 (1.9)
5 (1.3)
Bottle-feeding Habits
Did you ever bottle-feed your child?
Yes
No
111 (29.8)
261 (70.2)
When did bottle-feeding start? Mean age given in months
8 (SD 8)
When did bottle-feeding stop (unless still bottle
feeding)?
Give age that bottle feeding stopped
(mean age given in months)
24 (SD 23)
After Age 1, did your child bottle-feed at night?
Yes
No
Missing
72 (66.1)b
37 (33.9)
2
What did you put in the bottle?
Asked to list and
whether sugar was
added
Sugar added
No Sugar added
29 (26.1)b
82 (73.9)
After age 1, how often did you child have a bottle
during the day?
Answer given in
times per day
< 3 times per day
> 3 times per day
Don’t know
33 (29.7)b
66 (59.5)
12 (10.8)
What age do you think bottle-feeding should stop? Give age that bottle feeding stopped
(mean age given in months) 24 (SD 16)
a Data are presented as Number of participants and percentage among response options of the question unless otherwise indicated. b Proportion within those that
bottle feed.

115
There was a statistically significant difference in caries experience by certain socio-behavioural
variables (Table 4.6). Higher caries experience was found in infants who did not brush, did not
have help brushing, used toothpaste, ate more than one sweet snack as their usual snack, drank
juice as their usual drink, slept with their mother at night, or breast-fed beyond the age of two.
Children who were bottle-fed or who started tooth-brushing before 18 months-of-age had a
significantly lower caries experience. There was no significant difference in caries experience
by frequency of tooth-brushing, age of introducing solids, type of weaning food, frequency of
snacking, having sugar added to the bottle, age of stopping bottle-feeding, having a bottle at
night, or frequency of bottle-feeding during the day.
Children who used toothpaste had statistically significant differences in eating behaviours
compared with those who did not; including a higher exposure to sweet snacks. The use of
toothpaste was not included in the regression analysis because of the possibility that it was
confounded by other variables; in particular, consumption of non-nutritious foods.

116
Table 4.6 – Cambodia Smile cross-sectional survey - Bivariate analysis of dental
behaviours by child caries experience.
a P <0.05; Kruskal Wallis or χ2 test as appropriate to examine differences among groups within the same column b P <0.001; Kruskal-Wallis or χ2 test as appropriate examine differences among groups within the same column
Mean dmft
(SD)
Any caries
N (%)
sECC
N (%)
Significant
caries
N (%)
Oral Hygiene
Tooth-brushing
Yes 5.1 (5.0) a 94 (66.2) 70 (51.5) 43 (30.3)
No 5.4 (5.8) 150 (65.2) 108 (50.0) 79 (34.3)
Help with brushing
Yes 3.6 (4.8)b 31 (50.8)b 23 (39.0)a 26 (32.1)
No 6.2 (4.9) 63 (77.8) 47 (61.0) 17 (27.9)
Started brushing
Before 18m 3.8 (5.6) 11 (45.8)a 9 (37.5) 6 (25.0)
After 18m 5.3 (4.9) 83 (70.3) 61 (54.5) 37 (31.4)
Use toothpaste
Yes 5.6 (4.9)a 78 (73.6)a 58 (56.9)a 31 (30.2)
No 3.6 (5.1) 16 (44.4) 12 (35.3) 11 (30.6)
Dietary habits
>1 Usual snack is
sweet
Yes 5.6 (5.5) 38 (70.4) 31 (60.8) 24 (44.4)a
No 5.2 (5.5) 206 (64.8) 147 (48.8) 98 (30.8)
Juice as usual drink
Yes 7.0 (5.6)a 38 (77.6) 31 (66.0)a 21 (42.9)
No 5.0 (5.4) 206 (63.8) 147 (48.2) 101 (31.3)
Nursing habits
Still breast-feeding
with after 2y
No 1.4 (3.1)b 16 (25.8)b 16 (24.8)b 16 (25.8)
Yes 6.1 (5.5) 228 (73.5) 162 (55.9) 106 (34.2)
Still sleeping with
mother after age 2y
No 0.5 (1.3)b 3 (15.8)b 3 (15.8)b 3 (15.8)
Yes 5.5 (5.5) 241 (68.3) 175 (52.6) 119 (33.7)
Bottle-feeding
Ever bottle-fed
Yes 4.7 (5.1) 45 (60.8) 36 (49.3) 22 (29.7)a
No 6.6 (6.5) 49 (69.0) 33 (53.2) 33 (46.5)

117
The presence of Significant Caries was influenced both positively and negatively in the binary
logistic regression model (Table 4.7); children who started tooth-brushing before the age of 18
months (compared to those who started brushing after 18 months of age) had a 41% less chance
of presenting with sECC; children who did not have help with tooth-brushing had twice the
chance of developing sECC; and children who were still breast-feeding after the age of two
years were more than five times more likely to have sECC. There was no evidence of multi-
collinearity in the tolerance values or the variance inflation factor (VIF), and the pseudo R2
statistics indicated that the model was a good fit.
Table 4.7 – Cambodia Smile cross-sectional study - Binomial logistic regression model for
Socio-behavioural habits by presence of significant caries.a
B(SE) Odds Ratio (95% CI) P-Value
Constant -1.7 (0.64) - -
Does not have help with brushing 0.75 (0.26) 2.11 (1.28, 3.50) 0.003
Started brushing before 18m -0.89 (0.42) 0.41 (0.18, 0.93) 0.033
Breast-feeding after the age of
two years 1.67 (0.65) 5.31 (1.50, 18.79) 0.010
aR2 = 0.93 (Homer & Lemenshow), 0.06 (Cox & Snell), 0.08 (Nagelkerke). Model χ2 = 465.96

118
4.5 Discussion
In the present study the socio-behavioural risk factors associated with ECC in a
convenience sample of Cambodian children were investigated. Oral hygiene habits,
breast-feeding habits, bottle-feeding habits and dietary habits were directly associated
with caries experience. Breast-feeding beyond the age of two years and the lack of early
oral hygiene habits were strong predictors of caries experience.
Before discussing the findings further, it is appropriate to consider the strengths and
weaknesses of the present study. The strengths of the study lie in the geographically
diverse sample, the high consent rate, the relatively large number of subjects, and the
broad range of topics explored in the questionnaire. The participants came from three
rural areas as well as Phnom Penh. This increased the chance of diversity within the
sample; however, since convenience sampling was used, the findings of this study may
not be generalizable to the entire Cambodian pre-school population.
Another weakness is related to the relatively large number of interviewers and examiners
involved in data collection, which could have resulted in a lack of consistency in the data.
In addition, data collection was conducted over a period of 18 months and inter-examiner
and intra-examiner reliability were not determined. In spite of this, the survey was a good
first step at quantifying caries experience of preschool children in Cambodia.
4.5.1 Caries experience within the Cambodia Smile cross-sectional
survey
This sample had a high burden of dental caries and the pattern was more severe than that
reported for other settings (Duangthip et al 2017; Khitdee 2016). The dmft of the 6 year-
old children in the present study is consistent with that reported by the CNOHS and so it
is conceivable that the caries experience of this sample could be similar to that
experienced elsewhere in Cambodia (Chher et al. 2016). The pattern of caries suggests
that there were more children with carious lesions in the anterior segment than in the
molars. This indicated that the caries process was starting on anterior teeth and then
developing on the molars in a pattern that is typical for ECC, as the primary incisors erupt
first.

119
One of the aspects of the present study that highlights the severe nature of caries
experienced by this group is the prevalence of pulpally involved teeth. Nearly one third
of children had one or more pulpally involved teeth, compared to a Brazilian study in
which only 5% of preschool children had one or more pulpally involved teeth. And yet
the prevalence of caries in the Brazil sample is similar to the present study (approximately
two thirds of children dmft > 1) (Gradella et al. 2011). This emphasises the more severe
pattern of dental caries experienced by Cambodian preschool children.
The PCG in this sample also had a high burden of dental caries. The prevalence of caries
and the number of pulpally involved teeth is consistent with the findings of the CNOHS
(Chher et al. 2016). The presence of frank open carious lesions in the mouths of the
mothers has often been suggested to indicate a more cariogenic microflora in the mother’s
mouth that is subsequently passed on to the child (Berkowitz 2003); alternatively, and
more likely, it may be that the mothers who have unrestored cavitated lesions have higher
risk behaviours for poor oral health and that these behaviours are moderating the
expression of dental caries in their children as described in other settings (Rai & Tiwari
2018; Tiwari et al. 2018; Philip et al. 2018) .
The present study supports the general consensus of the literature that maternal caries
experience is associated with, and is a good predictor of, dental caries experience in
preschool children (Rai & Tiwari 2018; Abiola et al. 2009; Li & Caufield 1995; Nowjack-
Raymer & Gift 1990; Steffensen 1990). Of note in the present study is that that the caries
experience of non-maternal caregivers was not associated with the child’s caries
experience. It could be that the reason for this lack of association is because the children
may not be left in the care of ‘other’ caregivers until after caries risk behaviours have
been established. This theory is supported by the finding that children who were left with
non-maternal caregivers were significantly older than those children were cared for by
their mothers. The severe dental caries experience in this study supports the view that
ECC is a pressing and urgent problem in Cambodia.
4.5.2 ECC and nursing habits
One of the findings that sets the results of present study apart from others is the
considerable risk ratio for dental caries associated with breast-feeding past the age of two
years. Before this finding is discussed further, it is important to observe that beliefs and
practices around infant feeding are culturally bound and some of these may be unique to

120
the Cambodian population (Desai & Alva 1998). Some of the infant feeding practices in
this population that may differ from other countries included the finding that almost all
the mothers slept with their child at night, often for several years. All these findings are
supported by previous studies of infant feeding practices in Cambodia (Desai & Alva
1998; Ismail & Sohn 1999; Willems et al. 2005).
The literature about whether there is an association between prolonged on-demand breast-
feeding at night and dental caries experience in early childhood is divided. In many
countries such practices are very uncommon, whereas in Cambodia they are almost
universal. The literature is also confusing in that breast- and bottle-feeding practices and
ECC itself are not reported in a consistent manner (Peres et al. 2017; Chaffee et al. 2014;
Thomson et al. 1996).
Reference to ‘prolonged breast-feeding’ as being ‘more than one year’ by authors is
common and few mothers in the West continue breast-feeding longer than this (Chaffee
& Cheng, 2014). In contrast, most of the children in the present study were breast-fed for
more than two years, almost all mothers slept with their infants, and nocturnal breast-
feeding was very prevalent, even amongst many older preschool children. A recent study
from Brazil was the first to examine the relationship between ECC and breast-feeding
beyond the age of two years, and their findings are consistent with the results of the
present study; in that they also reported a significantly higher prevalence of sECC in the
children who had been breast-fed past 2 years-of-age (Chaffee et al. 2014).
Although it is important to acknowledge the potential for confounding risk factors, it is
also useful to consider how breast-milk could interact with the caries process. The
mechanisms by which the mother’s breast-milk could be promoting the caries process
include both the composition of the milk and the temporal relationship (frequency of
exposure, duration of exposure, and timing of exposure) of the substrate on the teeth. The
cariogenic capacity of HBM, in particular, its limited acid buffering capacity and
relatively high lactose content has been investigated (Bowen & Lawrence 2005; Thomson
et al. 1996). The fact that HBM does not buffer acid as effectively as other milks may not
always be a problem because human breast-milk is usually coupled with saliva which has
a good buffering capacity. This leads on to one possible explanation for the relationship
between breast-feeding over the age of two years and sECC; that is, those children who
are being breast-fed at night (whilst they are sleeping with their mothers) have a

121
prolonged exposure to the carbohydrate (namely fermentable lactose) when saliva flow
is at its lowest and when there is little or no buffering capacity in the mouth. This is often
coupled with poor oral hygiene, leading to a thick, highly cariogenic biofilm.
Another mechanism by which the caries process may be potentiated by breast milk relates
to the frequency of snacking. The fact that breast-milk requires no preparation means that
children are able to breast-feed on-demand, as compared with the time required and extra
expense to prepare a bottle. Also, previous investigators have observed that feeding
practices in Cambodia tend to be directed towards ‘appeasing the child’s desires’. That is
to say, the common understanding of parents for a child crying is that they are hungry; if
they do not cry then reportedly there is no feeding initiated. Likewise, the child is not
encouraged to complete a full meal serving (whether from breast or bottle) and so they
become hungry sooner (Rasbridge & Kulig, 1995). These factors contribute to the
increasing frequency of carbohydrate exposures in the mouth.
In addition, weaning practices and time of solids introduction to the diet may also play a
role. The most common weaning food is rice porridge (“bor bor”), which often has sugar
added. White rice has a very high starch content (approximately 82%) (Snow & O’Dea,
1981), and evidence from in vitro animal and human studies show that dietary starches
are potential cariogenic substances (Scannapieco et al. 1993). Hydrolysis of cooked
starches produces significantly greater concentrations of maltose than raw starches and
subsequently a higher demineralisation potential (Brudevold et al. 1985). With
inadequate brushing and removal of food debris, the clearance time of these starches may
be extended along with the cariogenic potential.
There are likely to be strong cultural and traditional influences at play in relation to infant
feeding practices in Cambodia and it is recognized that changing health-related
behaviours can be difficult, especially where habits may be regarded as “normal” and
“healthy”. However, it is encouraging to note that there has been some recent success in
modifying infant feeding habits by engaging Buddhist nuns in Banteay Meanchey
province (Cambodia). The nuns in this study met with expectant mothers in a range of
settings and provided breast-feeding advice. The results showed a measurable change in
feeding habits whereby those in the intervention group had a higher rate of exclusive
breast-feeding when compared to a control group (Crookston et al. 2007).

122
It is clear that a coordinated approach would be required to bring about changes in such
long-established and culturally ingrained early childhood feeding behaviours;
furthermore, it is important to make sure that breast-feeding recommendations are clear
and consistent with WHO and the MOH recommendations in order to avoid providing
conflicting messages (Desclaux & Alfieri 2009; Marriott et al. 2010). An open cross-
discipline discussion around this issue would be helpful. This is especially important as
changes in infant feeding practices are becoming apparent with an improvement in the
economic status of the country and the use of the baby bottle with either milk formula or
improvised (often sweetened) milk replacements is becoming more popular within many
families in Cambodia (Helen Keller International 2015).
4.5.3 ECC and oral hygiene practices in Cambodia
Although modifying infant feeding habits is an attractive target for intervention, it is
important that a multifaceted coordinated approach is adopted. Another major area of
concern highlighted in the present study was the lack of good oral hygiene practices. Most
of the preschool children did not brush their teeth, and the majority of those who did,
brushed unassisted.
The effect of tooth-brushing, and the effect of the child having assistance while tooth-
brushing was seen most markedly in the binary regression model where the odds ratio for
sECC was more than halved by the early introduction of tooth-brushing. It is of note that
the study did not determine whether the brushing was associated with the use of fluoride
toothpaste, which is known to have an important effect on reducing caries increment
(Marinho 2009). It is known that many toothpastes in Cambodia either contain no fluoride
or contain low concentrations (Chher & Hak 2005). There are significant access issues to
affordable and appropriate toothpastes in Cambodia. The findings of the present study
suggest that the lack of tooth-brushing with fluoride toothpaste in this age group could
be a significant contributor to the severity of dental caries experienced.
4.5.4 Other risk indicators for ECC
It was surprising that although snacking on sweet foods and drinks was found to be
positively associated with ECC, it did not feature in the predictive model. One possible
explanation is that these variables were masked as predictors because the snacking on
sweet foods is happening concurrently with breast-feeding from a very early age or it is

123
so ubiquitous. In two previous Cambodian studies, the estimates for the prevalence of
exclusive breast-feeding at six months-of-age ranged from 15% (National Institute of
Statistics 2015)) to 60% (Senarath et al. 2010). The finding that the diets of many young
children are not optimal may not only be contributing to poor oral health but also to poor
nutritional outcomes (National Institute of Statistics 2010).
4.6 Conclusions
The results of the present study confirmed that preschool children in Cambodia are likely
to have a severe experience of dental caries which is associated with maternal caries
experience, late initiation of oral hygiene practices, and prolonged breastfeeding. In the
present study, breast-feeding continuing past the age of two years and lack of tooth-
brushing were significant predictors of dental caries experience in preschool children.
The unique socio-behavioural habits around nursing present in these children highlight
the need for a coordinated and multifaceted approach to improving the dental caries
outcomes of Cambodian pre-schoolers. Information from the present survey may help to
inform strategies to reduce the burden of dental caries in Cambodia.

124
4.7 References Chapter 4
Abanto, J., Carvalho, T. S., Mendes, F. M., Wanderley, M. T., Bönecker, M. & Raggio,
D. P. (2011) Impact of oral diseases and disorders on oral health-related quality of life of
preschool children. Community Dentistry and Oral Epidemiology, 39 (2), 105–114.
Abiola Adeniyi, A., Eyitope Ogunbodede, O., Sonny Jeboda, O. & Morenike Folayan, O.
(2009) Do maternal factors influence the dental health status of Nigerian pre-school
children? International Journal of Paediatric Dentistry, 19 (6), 448–454.
Bach K. (2014) The Oral Health of Cambodian Pre-School-Aged Children. DCD Thesis
submitted to the Faculty of Medicine, Dentistry and Health Science of The University of
Melbourne.
Berkowitz, R. J. (2003) Causes, treatment and prevention of early childhood caries: a
microbiologic perspective. Journal of the Canadian Dental Association, 69 (5), 304–307.
Bowen, W. H. & Lawrence, R. A. (2005) Comparison of the cariogenicity of cola, honey,
cow milk, human milk, and sucrose. Pediatrics, 116 (4), 921–926.
Bratthall, D. (2000) Introducing the Significant Caries Index together with a proposal for
a new global oral health goal for 12-year-olds. International Dental Journal, 50 (6), 378–
384.
Brudevold, F., Goulet, D., Tehrani, A., Attarzadeh, F., & Van Houte, J. (1985) Intraoral
demineralization and maltose clearance from wheat starch. Caries Research, 19 (2), 136–
144.
Chaffee, B. W. & Cheng, A. (2014) Global Research Trends on Early-Life Feeding
Practices and Early Childhood Caries: A Systematic Review. Journal of Oral Diseases,
2014.
Chaffee, B. W., Feldens, C. A. & Vítolo, M. R. (2014) Association of long-duration
breastfeeding and dental caries estimated with marginal structural models. Annals of
Epidemiology, 24 (6), 448–454.
Chher T. & Hak S. (2005) Fluoride content of toothpastes sold in Cambodia 2001 and
2004. Ministry of Health, Cambodia.
Chher, T., Turton, B.J., Hak, S., Beltran, E., Courtel, F., Durward, C. & Hobdell, M.,
(2016) Dental caries experience in Cambodia: Findings from the 2011 Cambodia
National Oral Health Survey. Journal of International Oral Health, 8 (1), 1.
Chu, C. H., Wong, A. W. Y., Lo, E. C. M. & Courtel, F. (2008) Oral health status and
behaviours of children in rural districts of Cambodia. International Dental Journal, 58
(1), 15–22.
Çolak, H., Dülgergil, Ç. T., Dalli, M., & Hamidi, M. M. (2013) Early childhood caries
update: A review of causes, diagnoses, and treatments. Journal of Natural Science,
Biology, and Medicine, 4 (1), 29.
Crookston, B. T., Dearden, K. A., Chan, K., Chan, T. & Stoker, D. D. (2007) Buddhist
nuns on the move: An innovative approach to improving breastfeeding practices in
Cambodia. Maternal & Child Nutrition, 3 (1), 10–24.

125
Desai, S. & Alva, S. (1998) Maternal education and child health: Is there a strong causal
relationship? Demography, 35 (1), 71–81.
Desclaux, A. & Alfieri, C. (2009) Counseling and choosing between infant-feeding
options: overall limits and local interpretations by health care providers and women living
with HIV in resource-poor countries (Burkina Faso, Cambodia, Cameroon). Social
Science & Medicine, 69 (6), 821–829.
Drury, T. F., Horowitz, A. M., Ismail, A. I., Maertens, M. P., Rozier, R. G. & Selwitz, R.
H. (1999). Diagnosing and reporting early childhood caries for research purposes: a
report of a workshop sponsored by the National Institute of Dental and Craniofacial
Research, the Health Resources and Services Administration, and the Health Care
Financing Administration. Journal of Public Health Dentistry, 59 (3), 192–197.
Duangthip, D., Gao, S.S., Lo, E.C.M. & Chu, C.H. (2017) Early childhood caries among
5- to 6-year old children in Southeast Asia. International Dental Journal, 67 (2), 98-106.
Gift, H. C., Reisine, S. T. & Larach, D. C. (1992) The social impact of dental problems
and visits. American Journal of Public Health, 82 (12), 1663–1668.
Gradella, C. M., Bernabé, E., Bönecker, M. & Oliveira, L. B. (2011) Caries prevalence
and severity, and quality of life in Brazilian 2- to 4-year-old children. Community
Dentistry and Oral Epidemiology, 39 (6), 498–504.
Helen Keller International (2014) Assessment of Promotion of Foods Consumed by
Infants and Young Children in Phnom Penh: Assessement and Research on Child Feeding
(ARCH) – Cambodia Country Report.
Ismail, A. I. & Sohn, W. (1999) A systematic review of clinical diagnostic criteria of
early childhood caries. Journal of Public Health Dentistry, 59 (3), 171–191.
Khitdee, C. (2017) The epidemiology of Early Childhood Caries. Thai Dental Public
Health Journal, 22(sup), 4-10
Li, Y. & Caufield, P. W. (1995) The fidelity of initial acquisition of mutans streptococci
by infants from their mothers. Journal of Dental Research, 74 (2), 681–685.
Marinho, V. C. C. (2009) Cochrane reviews of randomized trials of fluoride therapies for
preventing dental caries. European Archives of Paediatric Dentistry, 10 (3), 183–191.
Marriott, B. P., White, A. J., Hadden, L., Davies, J. C. & Wallingford, J. C. (2010) How
well are infant and young child World Health Organization (WHO) feeding indicators
associated with growth outcomes? An example from Cambodia. Maternal & Child
Nutrition, 6 (4), 358–373.
Ministry of Health, Cambodia (2015) Cambodia Demographic and Health Survey
Monse, B., Heinrich-Weltzien, R., Benzian, H., Holmgren, C. & van Palenstein
Helderman, W. (2010) PUFA–An index of clinical consequences of untreated dental
caries. Community Dentistry and Oral Epidemiology, 38 (1), 77–82.
Nowjack-Raymer, R. & Gift, H. C. (1990) Contributing factors to maternal and child oral
health. Journal of Public Health Dentistry, 50 (6), 370–378.

126
Peres, K. G., Nascimento, G. G., Peres, M. A., Mittinty, M. N., Demarco, F. F., Santos,
I. S., Matijasevich, A. & Barros, A. J. D. (2017) Impact of Prolonged Breastfeeding on
Dental Caries: A Population-Based Birth Cohort Study. Pediatrics, 140 (1), e20162943.
Philip, N., Suneja, B. & Walsh, L.J. (2018) Ecological approaches to dental caries
prevention: paradigm shift or shibboleth? Caries Research, 52 (1-2),153-165.
Rai, N.K. & Tiwari, T. (2018) Parental Factors influencing the Development of early
childhood caries in Developing Nations: a Systematic Review. Frontiers in public health,
6, 64.
Rasbridge, L. A. & Kulig, J. C. (1995) Infant feeding among Cambodian refugees. MCN:
The American Journal of Maternal/Child Nursing, 20 (4), 213–218.
Scannapieco, F. A., Torres, G. & Levine, M. J. (1993) Salivary α-amylase: role in dental
plaque and caries formation. Critical Reviews in Oral Biology & Medicine, 4 (3), 301–
307.
Senarath, U., Dibley, M.J. and Agho, K.E., 2010. Factors associated with nonexclusive
breastfeeding in 5 east and southeast Asian countries: a multilevel analysis. Journal of
Human Lactation, 26(3), pp.248-257.
Sheiham, A. & James, W.P.T. (2015) Diet and dental caries: the pivotal role of free sugars
reemphasized. Journal of Dental Research, 94 (10), 1341-1347.
Snow, P. & O’Dea, K. (1981) Factors affecting the rate of hydrolysis of starch in food.
The American Journal of Clinical Nutrition, 34 (12), 2721–2727.
Steffensen, J. E. (1990) Literature and concept review: issues in maternal and child oral
health. Journal of Public Health Dentistry, 50 (6), 358–369.
Thomson, M. E., Thomson, C. W. & Chandler, N. P. (1996) In vitro and intra-oral
investigations into the cariogenic potential of human milk. Caries Research, 30 (6), 434–
438.
Tiwari, T., Wilson, A.R., Mulvahill, M., Rai, N. & Albino, J. (2018) Maternal factors
associated with early childhood caries in urban Latino children. JDR Clinical &
Translational Research, 3 (1), 83-90.
Todd, R. V., Durward, C. S., Chot, C., So, P. K. & Im, P. (1994) The dental caries
experience, oral hygiene and dietary practices of preschool children of factory workers
in Phnom Penh, Cambodia. International Journal of Paediatric Dentistry, 4 (3), 173–
178.
Willems, S., Vanobbergen, J., Martens, L. & De Maeseneer, J. (2005) The Independent
Impact of Household-and Neighborhood-based Social Determinants on Early Childhood
Caries: A Cross-sectional Study of Inner-city Children. Family & Community Health, 28
(2), 168–175.
World Health Organization (2013) Oral health surveys: basic methods. World Health
Organization.

128
Chapter 5
Evaluation of a primary care based ECC intervention -
Cambodia Smile
Souen S, Turton B, Durward C. (2015) Integrating oral health and general health in a
Cambodian setting; IADR SEA 29th Annual meeting, Bali, Indonesia.
Turton B (2015) Cambodia Smile – integrating oral health and general health in a
Cambodian setting. 2015 Global childrens nutrition and oral health symposium, UCSF,
California, USA.
Sopharith S, Turton B, Durward C, Crombie F, Manton D. (2016) Cambodia Smile –
Preliminary results from an early childhood caries intervention. IADR General Session.
Seoul, Republic of Korea.
Turton B, Durward C, Soeun S, Crombie F, Manton D (2017). Cambodia Smile – 2-year
follow-up of a community based Early Childhood Caries (ECC) intervention. Congress
of the International Association of Paediatric Dentistry. Santiago, Chile.
Turton, B., Durward, C., Soeun S., Crombie, F., Manton, D. (2018) Cambodia Smile –
Caries Prevention by primary health care providers. ORCA, Copenhagen, Denmark.

129
Objectives: To test a primary care-based intervention to prevent ECC using primary
healthcare-workers in public health centres.
Methods: A Total of 262 Mother-child dyads were recruited at birth and followed for two
years (intervention group) and a contemporaneous sample of 184 participants from ages 18 to
30 months were recruited from surrounding districts (control group). Intervention group
participants received oral health information, toothbrushes with fluoride toothpaste, fluoride
varnish (NFlor protect; Ivoclar Vivadent, Schaan, Liechtenstein), and dietary advice integrated
with existing vaccinations, de-worming, and vitamin A schedule. At follow-up, intraoral
examinations were conducted to detect carious lesions including white spot lesions using the
South East Asian recommendations for epidemiological surveys of ECC.
Results: Of the intervention group 185/262 were followed-up (70.2%) and there was no
statistically significant difference in age in months between the control group (22.2; SD 2.4)
and the intervention group (21.9; SD 2.6). There was no statistically significant difference in
caries experience by sex. A significant (p < 0.001) difference existed in the number and
prevalence of carious lesions between the intervention group (2.9; SD 3.0 and 68.1%) and
control group (8.7; SD 4.9 and 94.0%). There was a significant difference in preventive
increment depending on the components of the intervention; children who had Oral Hygiene
Education (OHE) and dietary advice only during the first 6 months of life had a 25.0%
preventive increment while those who had OHE during the first 6 months of life as well as FV
application had a 62.5% preventive increment when compared to the control group.
Conclusions: The Cambodia Smile primary care-based intervention significantly reduced
caries experience. Further advocacy is required in order to upscale this intervention across
Cambodia.

130
5.0 Chapter 5 – The Cambodia Smile intervention
The oral health of Cambodian children is amongst the poorest in the world. At age 6 y, 98% of
children have carious lesions, with a mean dmft of 9.0, and a mean of 2.7 pulpally-involved
teeth (Chher et al. 2016). This severe burden of disease has previously been reported to have
severe impacts on the Oral health Related Quality of Life of Cambodian Children (Khoun et
al. 2018; Turton 2018; Turton et al. 2015). Perhaps part of the reason for those severe impacts
are that most of the carious lesions go untreated. That is to say, the ‘D’ or ‘decayed’ component
of the dmft/DMFT index accounts for most (99%) of the disease experience. The result is that
most children enter school in a state of uncontrolled caries risk with numerous untreated carious
lesions.
Dental caries is a behaviourally moderated disease initiated by the metabolism of fermentable
carbohydrates by bacteria on the surface of the tooth, the acidic by-products of which
demineralise the enamel, subsequently leading to cavitation of the tooth surface (Sheiham &
James, 2015). The key driver in the presence of those untreated carious lesions is a diet with
large amounts of sugar. The average preschool child in Phnom Penh consumes three sugary
sweetened beverages per-day (Turton et al. 2018). While specific quantification of sugar
content was not performed in that study, it is more than likely that the consumption of sugar
by young children in Cambodia exceeds that recommended by the World Health Organization
(WHO) (Moynihan and Kelly, 2014). Unfortunately, the evidence around strategies to reduce
sugar intake by preschool children are still limited though motivational interviewing appears
to be the most promising method in other settings; however, there is not yet any evidence for
the use of such techniques for improvement in oral health in countries similar to Cambodia
(Jameson 2018; Albino and Tiwari, 2015).
Acknowledging that the diet is difficult to influence, it is important to employ another? key
mediator in reducing the impact of sugar on caries progression which is the use of fluoride
(Bernabé et al. 2016). Fluoride varnish (FV) together with tooth-brushing with fluoride
toothpaste is an attractive method for delivering fluoride in communities where reticulated
water systems for the delivery of community water fluoridation are not available. All of those
interventions have been shown to be cost-effective, safe to use and effective (Marinho et al.
2003).
A recent cross-sectional survey identified the late oral hygiene practices and unfavourable
nursing habits as risk indicators for ECC in Cambodia suggesting that the high consumption of

131
sugar by Cambodian pre-schoolers is not being moderated by the use of fluoride toothpaste
(Turton et al. 2015). Furthermore, exposure to fluoride toothpaste is occurring at an older age
than desirable. Recent evidence has supported the implementation of caries preventive efforts
before one year-of-age and even before the child is born by targeting pregnant mothers
(Phantumvanit et al. 2018; Sokal-Gutierrez et al. 2016; Leong et al. 2013; Wigen & Wang
2012).
The health professionals who have the most contact with Cambodian children and mothers
during the early years of life are the midwives and nurses (primary care providers) based in
community health centres. Nine out of ten mothers receive post-natal care and three out of four
children receive their full complement of basic vaccinations (MOH, Cambodia, 2015). There
is a growing body of evidence to support dental interventions carried out by primary health
care providers who have many opportunities to integrate oral health promotion with general
health and nutrition interventions. However, at this stage, there are no models for mobilising
primary health care providers for oral health interventions in a Cambodian setting. An
affordable, accessible and appropriate intervention to address ECC in Cambodia could involve
providing oral health education to mothers and babies, together with the application of fluoride
varnish to children, delivered alongside existing health interventions by primary health care
providers. The present study seeks to examine the outcome of a pilot intervention to deliver an
oral health intervention through the primary health care structure in Cambodia.
5.1 Aims
To investigate the effectiveness of a pilot strategy for the reduction of dental caries experience
in Cambodian preschool children through an integrated primary health care model.
5.2 Objective
To investigate the effects on dental caries experience among a sample of young children in
Kampong Speu district through packaging the delivery of oral health education and topical
fluoride applications with the existing programs for de-worming, vitamin A supplementation
and vaccinations.

132
5.3 Methods
A two year interventional study based in CHC was undertaken. Mothers were invited to
participate with their new-born babies and consent was gained both verbally (explained by
primary health care provider) and in writing (Appendix 9). Participants were matched with a
control group who were recruited after two years to make a comparative evaluation of the
outcome of the program. Therefore, individuals in the control group still benefitted from
participating in the study. Ethical review was provided by the National Ethics Committee for
Health Research in Cambodia and by the University of Melbourne, Health Sciences Human
Ethics Sub-Committee (Ethics ID: 1545412). Copies of the ethical review documents are
included in Appendix 11.
5.3.1 Health Centre and Population Selection
The study sample size was calculated based on the assumption that children in the intervention
group would have a mean d1mft at least one tooth less than those in the control group. Using
the data from the previously conducted cross-sectional survey where the mean dmft of 2 year-
olds was 3 (SD 3), 95% power, and a significance level 0.05, it was determined that a sample
size of 392 (196 in the control and 196 in the intervention) would be required. However follow-
up can be difficult in a Cambodian environment and so an arbitrary 30% was added to each
group, therefore a sample of 520 mother-child dyads was required.
Participants for the intervention group were recruited from four health centres in the province
of Kampong Speu between February and July of 2015 with mother-child dyads invited into the
study until the sample size was filled. Recruitment of the control group was conducted during
October 2016 from four different health centres in the same province. None of the children had
access to fluoridated water.
5.3.3 Clinical Protocol for the intervention
The clinical protocol involved the delivery of dietary advice, oral hygiene instruction with flip
charts, and provision of toothbrush and fluoride toothpaste for both mother and baby at baseline
and for baby at subsequent visits. The package of dietary advice, oral hygiene instruction and
delivery of fluoride toothpaste with toothbrush is what is referred to in this chapter as Oral
Health Education (OHE). In addition up to 0.4 mL of 7000 ppm fluoride varnish (NFlor Protect
FV, Ivoclar-Vivadent, Schaan, Liechtenstein) was placed on tooth surfaces once teeth erupted
into the mouth. These interventions were delivered concurrently with routine visits for

133
vaccinations, vitamin A supplementation and de-worming tablets. Two additional
opportunities were provided at 15 and 21 months-of-age to supplement the routine contacts
representing six opportunities for intervention over the first two years-of-life.
5.3.4 The questionnaire for the two-year follow-up
The questionnaire included questions on oral knowledge and behaviours and diet; however,
analyses of these aspects are beyond the present scope. All data collection forms are presented
in Appendix 9. Data analyses for the present study included data on the Family Impact Scale
(FIS), maternal education and household income level. The FIS is an OHRQoL instrument
which has been validated for use in a Cambodian population previously. The FIS includes eight
questions across three domains; family activities, family emotions, and family conflict. The
response options for each item were “Never” (score 0), “Once or twice” (score 1), “Sometimes”
(score 2), “Often” (score 3), or “Every day or almost every day (score 4). A participant was
said to have an ‘impact’ in a particular item if they responded with a score 3 or above in any
item.
5.3.5 Clinical measures
Teeth were not cleaned and were examined wet according to the guidelines described for the
South East Asian Index for Early Childhood Caries (SEA-ECC). Each tooth was given two
codes, one for SEA-ECC and another for PUFA status (Monse et al. 2010). Data from the SEA-
ECC are presented as d1mft for carious lesions limited to enamel and d2mft for carious lesions
extending to dentine and cavitated. The term ‘severity of caries’ in this study refers to the
number of lesions in an individual rather than the depth of the lesions. The Greens Simplified
Plaque index was used to assess the amount of plaque accumulation observed on the primary
right central incisor. Children were examined in the supine position using hand held torches
and mouth mirrors with appropriate universal infection control measures in place.
5.3.6 Data collection and analysis
Data were collected on stage-appropriate forms and participants were identified by a unique
identification (ID) number (Appendix 9). Midwives were given a list of children to follow-up
and one phone call a month was made between the research co-ordinator to the health centre
to encourage follow-up. Data were entered into IBM SPSS version 23 and both descriptive and
bivariate analyses were performed. No multivariate analysis was performed because no

134
differences in caries experience by sociodemographic indicators were found and sampling
procedures controlled for variations between the groups.

135
5.4 Results
There was no significant difference in age in months between the control group (22.2; SD 2.4)
and the intervention group (21.9; SD 2.6); There was no significant difference in group
membership by gender, or sociodemographic indictors such as the mother’s education or the
household income by loss to follow-up (Table 5.1).
Table 5.1 – Attrition analysis of intervention group at 1-year.
Baseline
N (row %)
Lost
N (row %)
Followed-up
N (column %) P-value
Sexa
Male 123 (47.1) 40 (32.5) 83 (67.5) 0.157
Female 138 (52.9) 36 (26.1) 102 (73.9)
Household income
<50 22 (8.4) 6 (27.3) 16 (72.7) 0.689
51-150 160 (61.1) 44 (27.5) 116 (72.5)
151-250 74 (28.2) 25 (33.8) 49 (66.2)
>250 6 (2.3) 1 (16.7) 5 (83.3)
Total 262 (100.0) 76 (29.0) 186 (71.0)
aGender data missing from one participant.

136
There were statistically significant differences between control and intervention groups in
terms of maternal education and household income. Participants in the intervention group had
a broader spread of participants across education levels and household income levels (Table
5.2).
Table 5.2 – Sociodemographic characteristics of participants at follow-up by group.
Intervention
N (row %)
Control
N (row %)
Total
N (column %) P-value
Sexa
Male 83 (48.8) 87 (51.2) 170 (46.1) 0.359
Female 102 (51.3) 97 (48.7) 199 (53.9)
Maternal Education
Illiterate 17 (100.0) 0 (0.0) 17 (4.6) <0.001
Primary 108 (37.0) 184 (63.0) 292 (78.9)
Secondary or High-
school
58 (100.0) 0 (0.0) 58 (15.7)
Tertiary 3 (100.0) 0 (0.0) 3 (0.8)
Household income
<50 16 (100.0) 0 (0.0) 16 (4.3) <0.001
51-150 116 (38.7) 184 (61.3) 300 (81.1)
151-250 49 (100.0) 0 (0.0) 49 (13.2)
>250 5 (100.0) 0 (0.0) 5 (1.4)
Total 186 (50.3) 184 (49.7) 370 (100.0)
aGender data missing from one participant.

137
Most participants received three or fewer contacts across the intervention period and those who
had four contacts had the lowest caries experience (Table 5.3). Children who had six contacts
had the most severe caries experience.
Table 5.3 – Caries severity by number of contacts among the intervention group.
Number of contacts
d3mfta
Mean (SD) P-valueb
One (N = 63) 2.9 (2.8) 0.359
Two (N = 58) 3.5 (3.6)
Three (N = 28) 2.5 (3.1)
Four (N = 16) 1.8 (2.9)
Five (N=19) 2.9 (2.3)
Six (N=2) 4.5 (0.7)
ad3mft denotes cavitated lesions in the primary dentition. bKruskal-Wallis test for examining the difference in mean d3mft by number of contacts received.
Data on caries experience are presented in Table 5.4. There were no significant differences in
caries experience according to sociodemographic characteristics.

138
Table 5.4 – Caries experience by sociodemographic characteristics.
D1mft
(SD) P-value
D2mft
(SD) P-value
Any white spot
N (row %) P-value
Any cavity
N (row %) P-value
Any pufa
N (row %) P-value
Sex
Male 6.3 (5.1) 0.111 1.4 (2.1) 0.311 139 (81.8) 0.422 69 (40.6) 0.195 14 (8.2) 0.105
Female 5.4 (4.8) 1.2 (2.0) 160 (80.4) 71 (35.7) 9 (4.5)
Maternal
Education
Illiterate 5.6 (4.8) 0.494 1.4 (1.9) 0.662 40 (80.0) 0.098 19 (38.0) 0.519 3 (6.0) 0.225
Primary 5.8 (4.7) 1.3 (2.2) 146 (85.9) 71 (41.8) 7 (4.1)
Secondary or
High-school
6.0 (5.2) 1.2 (1.9) 107 (77.0) 48 (34.5) 13 (9.4)
Tertiary 4.2 (5.8) 0.8 (1.6) 7 (63.6) 3 (27.3) 0 (0.0)
Household
income
<50 5.4 (5.1) 0.956 1.4 (2.1) 0.112 23 (85.2) 0.488 10 (37.0) 0.981 0 (0.0) 0.563
51-150 5.9 (5.1) 1.3 (2.2) 80 (79.2) 37 (36.6) 7 (6.9)
151-250 5.8 (4.6) 1.2 (1.8) 110 (84.6) 50 (38.5) 8 (6.2)
>250 5.8 (5.2) 1.3 (2.1) 87 (77.7) 44 (38.5) 8 (7.1)
Total 5.8 (5.0) 1.3 (2.0) 229 (62.1) 140 (37.9) 23 (6.2)
aP-values denote differences among groups within the same column.

139
The mean plaque scores for the control and intervention groups were statistically significantly
different, being 2.1 (SD 1.0) in the control group and 0.9 (SD 0.4) in the intervention group (p
< 0.05). There was no significant difference in frequency of ‘non-nutritious food’ (packaged
snacks, candies and sweet drinks) ingestion by group membership.
There was a statistically significant difference in caries experience by group membership and
exposure to the intervention (Table 5.5). Overall, there was a two thirds reduction in caries
severity (based on d1mft) and a two fifths reduction in prevalence for those who were in the
intervention group. Children who received OHE (with the provision of toothbrush and
toothpaste) had half the severity (d1mft) of those in the control group and those who had one
or more FV exposures had a further one-third reduction (p < 0.05). Exposure to FV was
associated with a small reduction in the prevalence of white spot lesions and there was a one
third reduction in d1mft compared to those who only received OHE. In contrast, children who
received FV had half the d2mft compared to those who received OHE only. Children who
received OHE realised a 25% reduction in the number of cavitated lesions. There was no
significant difference in the prevalence or severity of pulpally involved lesions by group
membership or level of exposure to the intervention but sample sizes were small for this
variable.

140
Table 5.5 – Clinical characteristics by exposure to the intervention.a
d1mft
(SD)
d3mft
(SD)
Any white spot
N (%)
Any cavity
N (%)
Any pufa
N (%)
Control 8.7 (4.9)a 1.6 (2.2)a 173 (94.0)a 88 (47.8)a 17 (7.6)
Intervention
Overall 2.9 (3.0) 1.0 (1.8) 127 (68.3) 53 (28.5) 9 (4.8)
OHE Only 3.3 (3.3)b 1.2 (2.1)b 78 (69.6)b 35 (31.3)b 4 (3.6)
FV & OHE 2.3 (2.5) 0.6 (1.2) 49 (66.2) 18 (24.3) 5 (6.8)
aP-value<0.001 for comparison of means or proportions between the control and intervention groups; χ2 statistic
or Kruskal-Wallis as appropriate. bP-value<0.001 for comparison of means or proportions between the OHE and FV&OHE group; χ2 statistic or
Kruskal-Wallis as appropriate.

141
There were statistically significant differences in the prevalence of impacts and mean scores
across the FIS and all FIS subscales (Table 5.6). Participants in the control group had a 2.5
times greater prevalence of impacts across the FIS; with the FIS subscale of family activities
showing the biggest differences. Families in the control group had a three times greater chance
of having their family activities interrupted by problems with their child’s teeth or mouth.
Differences in mean scores revealed a large effect size across the FIS and small to moderate
differences across the three subscales.
Table 5.6 – Differences within the Family Impact Scale and subscale impacts and mean
scores by group membership.
Intervention Control Overall
Relative
differencea
Impacts - N (%)
Family Impact Scale 29 (15.6) 93 (50.5) 122 (33.0) 69.1
Activities subscale 16 (8.6) 70 (38.0) 86 (23.2) 77.4
Emotions subscale 21 (11.3) 70 (38.0) 91 (24.6) 70.3
Conflict subscale 9 (4.8) 36 (19.6) 45 (12.2) 75.5
Mean Scores - (SD) Effect sizec
Family Impact Scale 3.7 (4.3) 8.0 (7.9) 5.8 (6.7) 0.6
Activities subscale 1.5 (1.9) 3.8 (3.9) 2.6 (3.3) 0.2
Emotions subscale 1.5 (1.6) 2.7 (2.5) 2.1 (2.2) 0.5
Conflict subscale 0.7 (1.6) 1.6 (2.2) 1.1 (2.0) 0.4
Floor and Ceiling effects
Proportion with
minimum score (0)
56 (30.1) 41 (22.5) 97 (26.4) -
Proportion with
maximum score (24)
1 (0.5) 9 (4.9) 10 (2.7) -
aP < 0.001; Kruskal-Wallis or chi squared test as appropriate. b Calculated by dividing the change in prevalence by the baseline prevalence and expressing it as a percentage. c Calculated by dividing the differences in mean scores by the standard deviation of the intervention group.

142
5.5 Discussion
The present study demonstrated that OHI and FV delivered by primary health care providers
in a rural Cambodian setting reduced the prevalence and severity of dental caries at 2 years-of-
age. Children in the intervention group had a two fifths reduction in prevalence and a two thirds
reduction in the severity of dental caries. There was evidence that the FV provided additional
benefit to the OHE alone. This is the first ECC intervention that used an OHRQoL instrument
as an outcome measure for a preventive intervention and the reduction in caries experience led
to a corresponding reduction of the impacts as measured by the FIS. Before considering the
findings of the intervention in detail, it is appropriate to consider the strengths and limitations
of the present study.
The main ethical consideration for this project was that those in the control group did not
receive interventions known to have beneficial effects. This disadvantage was partly mitigated
by the children in the control group receiving oral health interventions at the time of recruitment
and examination at two years-of-age. This compromise in recruitment meant that there were
differences in the sociodemographic characteristics between the control and intervention
groups. This may have been due to the different processes for recruiting participants in the
group. While health centres were selected randomly by the provincial health department staff
and based on the births registered by health centre, the process of finding the children was
based on the child being present within the village at the time of examination. This process was
continued until a sample with sufficient power was recruited and that lead to a bias towards the
middle spectrum of the household income scale. Despite this, no significant differences were
found in caries experience by sociodemographic characteristics.
The study was powered to examine differences in the severity of cavitated carious lesions at
group level and so there are limitations in performing sub-group analysis by number of
exposures to the intervention or the number of pulpally involved teeth. The therapies employed
had sufficient evidence to support their use and so the key focus was to examine a package of
care rather than to establish the viability of individual therapies.
5.5.1 Differences in Oral Health Related Quality of Life
In addition to the benefits at tooth-level, it appears that the Cambodia Smile intervention also
had benefits for the family unit. This study was unique in that it offered an OHRQoL measure;
the choice to use the FIS rather than the Parental-Child Perceptions Questionnaire was based

143
on data from the validation study of those instruments which suggested that for children in the
2 year age-group the FIS would be most sensitive. Any OHRQoL measure that attempts to
assess outcomes for participants who are not yet able to articulate their own opinion comes
with limitations (Varni et al. 2007). Despite this, the differences in mean scores and impacts
across the FIS scale and subscale suggests that the intervention created some benefit in terms
of OHRQoL.
5.5.2 Differences in caries experience by participation in the intervention
The differences in caries experience by exposure to the intervention were consistent with those
observed in other studies (Marinho et al. 2003). In addition, an intuitive pattern was confirmed
whereby those who received both OHE and FV realised a greater preventive fraction. In
addition, the OHE appeared to achieve the largest preventive fraction in the reduction in the
prevalence in white spot lesions. The placement of FV appeared to slow the progression of
white spot lesions to cavitation rather than greatly reduce the presence of white spot lesions.
This is consistent with the current understanding of the role of fluoride in moderating the
progression of caries (Philip et al. 2018, Bernabe et al. 2014, Fejerskov et al. 2004). Perhaps
the tooth-brushing was effective at slowing the progression of carious lesions from the pre-
clinical to clinically detectable white spot lesions, and perhaps the FV helped to slow the
progression from white spot lesion to cavitation? The limitations in sample size means that we
cannot be confident about which therapy rendered the greater preventive effect.
The results of the present study are more favourable than other FV studies reported in recent
literature and it is worth noting that the teeth were examined wet and without cleaning,
therefore the prevalence of white spot lesions may have been underestimated. Of the studies
that report FV to be ineffective, some were underpowered (Memarpour, 2015; Oliveira, 2014)
while other studies were conducted in populations with a prevalence of ECC below 40% at
around 2 years-of-age (Agouropoulos et al. 2014; Anderson et al. 2016; Divaris et al. 2013;
Jiang et al. 2014; Oliveira et al. 2014). Some researchers recruited only participants who had
already reached 2 to 3 years-of-age with no clinical signs of dental caries (Muñoz-Millán et al.
2018; Tickle et al. 2017). Other researchers have reported limited measurable benefits for FV
being applied on a conditional basis whereby clinicians did not adhere to a strict protocol for
identifying those at risk of lesion development (Fontana et al. 2018). This highlights the need
for clinicians to be clear about the selection of candidates for FV application and in the case of
the Cambodia Smile intervention, all children in the cohort were targeted at a stage of

144
development where, after taking into account the socio-behavioural aspects of the caries
disease in a Cambodian environment, maximum benefit could be gained. In addition, children
in the present context had a much higher caries risk and much lower exposure to fluoride in
other forms when compared to other research cohorts.
Despite the gross reductions in dental experience, there were still nine children in the
intervention group who developed one or more pulpally involved carious lesions. While this is
a lower proportion of children than that in the control group, the difference was not statistically
significant, and the study was underpowered in this instance. However, the presence of nine
children among the intervention group with pulpally involved teeth suggests that the Cambodia
Smile package either didn’t reach the children in the present delivery model or that the caries
imbalance present in those children exceeded that which can be moderated by the present
intervention alone. It is interesting that children with the most severe caries experience among
the intervention group were more likely to present for FV treatments. This suggests that there
might be opportunity to augment the benefits of FV by applying silver diammine fluoride to
children who present with cavitated lesions as this has been shown to be effective in other
settings (Duangthip et al. 2016).
When examining the benefits of fluoride therapies for moderating the disease experience it is
important to point out that caries is a socio-behavioural disease and if the drivers of the process
are not controlled, then caries will continue to be a burden at population level. In the present
study, there appears to be an improvement in oral hygiene as indicated by the differences in
plaque scores. However, no significant difference in the frequency of consumption of non-
nutritious foods between the two groups was noted. This suggests that the intervention did not
lead to change in dietary behaviours. There is evidence that other techniques such as
motivational interviewing might be effective in achieving behaviour change in ‘westernised’
settings (Borrelli et al. 2015; Jamieson et al, 2018). However, it is not clear if the same methods
would be effective in a Cambodian setting and more, context specific, research is needed to
examine how those risk behaviours are moderated (Rai and Tiwari, 2018). At this stage the
Cambodia Smile intervention is focused on targeting the most easily modifiable risk factors.
The previous cross-sectional study (Ch. 4) demonstrated that children who initiated oral
hygiene practices before 18 months-of-age had half the caries experience compared with those
who did not. The present study reproduces and validates those findings and suggests that an
improvement in oral hygiene is an achievable modifiable risk factor in the Cambodian setting.

145
Furthermore, risk factors were modified using the primary health care system, non-dental
professionals, and in a way that did not create additional attendance or access burdens for the
household. The main limitation in terms of the intervention was that not all chances for access
were realised and more work is needed to increase the proportion of opportunities that are
realised.
Even though this intervention does not offer a holistic approach to managing the caries process,
it does represent a tangible, population-wide approach, and it appears to be the most practical
first step at reducing the burden of ECC in Cambodia. It was evident that although six
opportunities were provided for intervention, very few of those opportunities were realised and
this highlights the need for multiple safety nets or back-ups in terms of intervention to increase
access. Although fewer than three opportunities on average were realised, that was still enough
to render a preventive effect. Given that that the caries experience is so severe and more than
99% of lesions go untreated, a population-wide role out of the Cambodia Smile intervention to
address the most easily modified risk factors would be appropriate.
5.6 Conclusions
The Cambodia Smile intervention put into practice the WHO recommendations for ECC
interventions (Phantumvanit et al. 2018) and the result was a caries reduction greater than other
previous preventive interventions in Cambodia. This study translates existing evidence around
the benefits of tooth-brushing with fluoride toothpaste and application of fluoride varnish into
a feasible intervention that was successful in a Cambodian environment. The prevalence and
severity of ECC was reduced for those children in the intervention group, however, there was
still a notable burden of caries experience following the intervention. Therefore, additional
administrative mechanisms improving access to the Cambodia Smile protocol and providing a
more holistic intervention might be able to further reduce the caries burden and the subsequent
impacts on OHRQoL. The success of this pilot study is a valuable first step in demonstrating
to key stake holders that it is possible to reduce the impacts that children and families
experience as a result of dental caries in a Cambodian setting.

146
5.7 References Chapter 5
Agouropoulos, A., Twetman, S., Pandis, N., Kavvadia, K. & Papagiannoulis, L. (2014) Caries-
preventive effectiveness of fluoride varnish as adjunct to oral health promotion and supervised
tooth-brushing in preschool children: A double-blind randomized controlled trial. Journal of
Dentistry, 42 (10), 1277–1283.
Anderson, M., Dahllöf, G., Twetman, S., Jansson, L., Bergenlid, A.-C. & Grindefjord, M.
(2016) Effectiveness of Early Preventive Intervention with Semiannual Fluoride Varnish
Application in Toddlers Living in High-Risk Areas: A Stratified Cluster-Randomized
Controlled Trial. Caries Research, 50 (1), 17–23.
Baker, S.R., Foster Page, L., Thomson, W.M., Broomhead, T., Bekes, K., Benson, P.E.,
Aguilar-Diaz, F., Do, L., Hirsch, C., Marshman, Z. & McGrath, C. (2018) Structural
Determinants and Children’s Oral Health: A Cross-National Study. Journal of Dental
Research, 0022034518767401.
Borrelli, B., Tooley, E. M. & Scott-Sheldon, L. A. J. (2015) Motivational Interviewing for
Parent-child Health Interventions: A Systematic Review and Meta-Analysis. Pediatric
Dentistry, 37 (3), 254–265.
Bernabé, E., Vehkalahti, M.M., Sheiham, A., Aromaa, A. & Suominen, A.L., (2014) Sugar-
sweetened beverages and dental caries in adults: a 4-year prospective study. Journal of
Dentistry, 42 (8), 952-958.
Bernabé, E., Vehkalahti, M.M., Sheiham, A., Lundqvist, A. and Suominen, A.L., 2016. The
shape of the dose-response relationship between sugars and caries in adults. Journal of Dental
Research, 95 (2), 167-172.
Chher T., Turton B., Hak S., Beltran E., Courtel F., Durward C. & Hobdell M. (2016) Dental
caries experience in Cambodia: Findings from the 2011 Cambodia National Oral Health
Survey. Journal of International Oral Health, 8 (1), 1.
Chia, L., Densie, I. & Morgan, C. (2015) An exploratory study of parental knowledge of early
childhood oral health care in Southland, New Zealand. New Zealand Dental Journal, 111 (1),
18–24.
Divaris, K., Preisser, J. S. & Slade, G. D. (2013) Surface-Specific Efficacy of Fluoride Varnish
in Caries Prevention in the Primary Dentition: Results of a Community Randomized Clinical
Trial. Caries Research, 47 (1), 78–87.
Dooley, D., Moultrie, N. M., Heckman, B., Gansky, S. A., Potter, M. B. & Walsh, M. M. (2016)
Oral health prevention and toddler well-child care: routine integration in a safety net system.
Pediatrics, 137 (1), e20143532.
Fejerskov, O. (2004) Changing paradigms in concepts on dental caries: consequences for oral
health care. Caries Research, 38 (3), 182-191.
Gussy, M. G., Waters, E. G., Walsh, O. & Kilpatrick, N. M. (2006) Early childhood caries:
current evidence for aetiology and prevention. Journal of Paediatrics and Child Health, 42 (1-
2), 37–43.

147
Hooley, M., Skouteris, H., Boganin, C., Satur, J. & Kilpatrick, N. (2012) Body mass index and
dental caries in children and adolescents: a systematic review of literature published 2004 to
2011. Systematic Reviews, 1 (1), 57.
Jiang, E. M., Lo, E. C. M., Chu, C. H. & Wong, M. C. M. (2014) Prevention of early childhood
caries (ECC) through parental tooth-brushing training and fluoride varnish application: A 24-
month randomized controlled trial. Journal of Dentistry, 42 (12), 1543–1550.
Jamieson, L., Smithers, L., Hedges, J., Parker, E., Mills, H., Kapellas, K., Lawrence, H.P.,
Broughton, J.R. and Ju, X., 2018. Dental Disease Outcomes Following a 2-Year Oral Health
Promotion Program for Australian Aboriginal Children and Their Families: A 2-Arm Parallel,
Single-blind, Randomised Controlled Trial. EClinicalMedicine, (1), 43-50.
Khoun, T., Malden, P. E. & Turton, B. J. (2018) Oral health-related quality of life in young
Cambodian children: a validation study with a focus on children with cleft lip and/or palate.
International Journal of Paediatric Dentistry. 28 (3), 326-334.
Fontana, M., Eckert, G.J., Keels, M.A., Jackson, R., Katz, B., Levy, B.T. & Levy, S.M. (2018)
Fluoride Use in Health Care Settings: Association with Children’s Caries Risk. Advances in
Dental Research, 29 (1), 24-34.
Leong, P. M., Gussy, M. G., Barrow, S.-Y. L., Silva-Sanigorski, A. & Waters, E. (2013) A
systematic review of risk factors during first year of life for early childhood caries.
International Journal of Paediatric Dentistry, 23 (4), 235–250.
Macpherson, L.M.D., Ball, G.E., Brewster, L., Duane, B., Hodges, C.L., Wright, W., Gnich,
W., Rodgers, J., McCall, D.R., Turner, S. & Conway, D.I. (2010) Childsmile: the national child
oral health improvement programme in Scotland. Part 1: establishment and
development. British Dental Journal, 209 (2), 73.
Marinho, V. C., Higgins, J., Logan, S. & Sheiham, A. (2003) Fluoride toothpastes for
preventing dental caries in children and adolescents. The Cochrane Library, CD0002278.
Memarpour, M., Fakhraei, E., Dadaein, S. & Vossoughi, M., (2015) Efficacy of fluoride
varnish and casein phosphopeptide-amorphous calcium phosphate for remineralization of
primary teeth: a randomized clinical trial. Medical Principles and Practice, 24 (3), 231-237.
Monse, B., Heinrich-Weltzien, R., Benzian, H., Holmgren, C. & van Palenstein Helderman,
W. (2010) PUFA–An index of clinical consequences of untreated dental caries. Community
Dentistry and Oral Epidemiology, 38 (1), 77–82.
Muñoz-Millán, P., Zaror, C., Espinoza-Espinoza, G., Vergara-Gonzalez, C., Muñoz, S., Atala-
Acevedo, C. & Martínez-Zapata, M. J. (2018) Effectiveness of fluoride varnish in preventing
early childhood caries in rural areas without access to fluoridated drinking water: A randomized
control trial. Community Dentistry and Oral Epidemiology, 46 (1), 63–69.
Oliveira, B. H., Salazar, M., Carvalho, D. M., Falcão, A., Campos, K. & Nadanovsky, P. (2014)
Biannual Fluoride Varnish Applications and Caries Incidence in Preschoolers: A 24-month
Follow-Up Randomized Placebo-Controlled Clinical Trial. Caries Research, 48 (3), 228–236.

148
Phantumvanit, P., Makino, Y., Ogawa, H., Rugg‐Gunn, A., Moynihan, P., Petersen, P.E.,
Evans, W., Feldens, C.A., Lo, E., Khoshnevisan, M.H. & Baez, R., 2018. WHO global
consultation on public health intervention against early childhood caries. Community Dentistry
and Oral Epidemiology, 46 (3), 280-287.
Philip, N., Suneja, B. & Walsh, L.J. (2018) Ecological approaches to dental caries prevention:
paradigm shift or shibboleth? Caries Research, 52 (1-2), 153-165.
Rai, N.K. & Tiwari, T. (2018) Parental Factors influencing the Development of early childhood
caries in Developing Nations: a Systematic Review. Frontiers in Public Health, 6, 64.
Shearer, D. M., Thomson, W. M., Broadbent, J. M. & Poulton, R. (2011) Maternal oral health
predicts their children’s caries experience in adulthood. Journal of Dental Research, 90 (5),
672–677.
Sheiham, A. & James, W.P.T. (2015). Diet and dental caries: the pivotal role of free sugars
reemphasized. Journal of Dental Research, 94 (10), 1341-1347.
Sokal-Gutierrez, K., Turton, B., Husby, H. & Paz, C.L. (2016). Early childhood caries and
malnutrition: Baseline and two-year follow-up results of a community-based prevention
intervention in rural Ecuador. BMC Nutrition, 2 (1), p.73.
Tickle, M., O’Neill, C., Donaldson, M., Birch, S., Noble, S., Killough, S., Murphy, L., Greer,
M., Brodison, J., Verghis, R. & Worthington, H.V. (2017) A randomized controlled trial of
caries prevention in dental practice. Journal of Dental Research, 96 (7), 741-746.
Turton, B., Durward, C., Manton, D., Bach, K. & Yos, C. (2016) Socio-behavioural risk factors
for early childhood caries (ECC) in Cambodian preschool children: a pilot study. European
Archives of Paediatric Dentistry, 17 (2), 97-105.
Turton, B. J., Thomson, W. M., Page, L. A. F., Saub, R. B. & Razak, I. A. (2015) Validation
of an Oral Health–Related Quality of Life Measure for Cambodian Children. Asia-Pacific
Journal of Public Health, 27 (2), NP2339–NP2349.
Varni, J.W., Limbers, C.A. & Burwinkle, T.M. (2007) How young can children reliably and
validly self-report their health-related quality of life?: An analysis of 8,591 children across age
subgroups with the PedsQL™ 4.0 Generic Core Scales. Health and Quality of Life Outcomes,
5 (1), 1.
Weintraub, J. A., Ramos-Gomez, F., Jue, B., Shain, S., Hoover, C. I., Featherstone, J. D. B. &
Gansky, S. A. (2006) Fluoride Varnish Efficacy in Preventing Early Childhood Caries. Journal
of Dental Research, 85 (2), 172–176.
Wigen, T. I. & Wang, N. J. (2012) Parental influences on dental caries development in
preschool children. An overview with emphasis on recent Norwegian research. Norsk
Epidemiologi, 22 (1), 13-19.
Wong, M., Glenny, A.-M., Tsang, B. W., Lo, E., Worthington, H. V., & Marinho, V. C. (2011)
Cochrane review: Topical fluoride as a cause of dental fluorosis in children. Evidence-Based
Child Health: A Cochrane Review Journal, 6 (2), 388–439.

151
Chapter 6
Overview, limitations and recommendations of the SEAL
Cambodia and Cambodia Smile projects

152
6.0 Chapter 6 - Overview, limitations, and recommendations of the
SEAL Cambodia and Cambodia Smile projects
It is important that therapies for controlling dental caries are critically evaluated in each context
in which they are applied. There is evidence from other settings that FS and fluoride toothpaste,
and FV can render some benefit in the control of the caries process (Peterson et al. 2004;
Yengopal et al. 2009); however, adaptation of those therapies to the Cambodian context had
not yet been explored. The situation in Cambodia is challenging due to the severe burden of
dental caries, an unfavourably positioned work force, and the limited availability of affordable
fluoride toothpaste or fluoridated water. Furthermore, the dental caries disease as a complex
problem amplified by the rising social inequality, and the limited political accountability
(Baker et al. 2018) which reinforces the need for robust multidisciplinary and multisectorial
approaches. This might only be possible when there is evidence around the most appropriate
strategies for control of the caries process.
The present thesis explores the adaptation of preventive therapies for the Cambodian context.
The SEAL Cambodia intervention was successful for preventing dental caries on first
permanent molars using a modified protocol; however, the preventive increment was not as
great as was hoped. The Cambodia Smile intervention was successful at greatly reducing the
burden of dental caries for 2 year-old children among a pilot sample. Both of these interventions
had some significant limitations which present opportunities for further investigation.
6.1 Summary of findings from the ‘SEAL Cambodia’ project
The SEAL Cambodia project was the result of a collaboration among local and international
partners and the stated aim was to provide FS for 60,000 children between the ages of 6 and 8-
years as a way of reducing the caries burden in the permanent dentition. The present study was
aimed at monitoring and evaluating the efficiency of the treatment and the major strength of
the study was that problems in the pilot protocol were identified and remedied with a modified
protocol. The major limitation of the study and the intervention as a package is that it did not
address holistic causes of the caries process. If the project was aimed at managing the caries
process, then outcomes such as improved tooth-brushing habits and altered dietary patterns
would have been outcomes of interest. In contrast, the study focused on a single therapy that
was refined to prevent cavitated lesions on a single tooth surface and as such the failure to
control the wider caries process limited the benefit that the FS therapy in question was able to

153
achieve. The caries process that started, in many cases, on approximal surfaces extended to
occlusal surfaces and compromised the preventive benefit observed on FPM.
As well as limitations in protocol, there were also limitations in the sampling procedures. In
the original cohort (those in Pilot A of Chapter 2), the sampling procedure, while randomised,
produced a control group who had significantly lower caries experience at baseline and this
could have masked some of the benefits rendered within the original pilot study. In the second
cohort (those in Group C and Group D of Chapter 3), the positive control group had a similar
baseline caries experience to that of the modified protocol group but a significantly lower
subsequent incidence of proximal caries. Again, these differences could have masked some of
the benefit of the FS procedure. Despite this, the modified protocol did achieve 2-year
preventive increments which are consistent with the higher end of the confidence interval
around expected benefits from GIC FS procedures (Ahovuo-Saloranta et al. 2016).
One of the benefits that wasn’t captured in the present investigation was the organisational and
structural changes that occurred as a result of the dental community in Cambodia rallying
around an upstream intervention. That meant that 60,000 children experienced dentistry that
was not focused on surgical intervention but on prevention and that the networks dedicated to
paediatric oral heath in Cambodia became more proficient at providing logistical support for
interventions at large scale (One-2-One Cambodia 2016). That the SEAL Cambodia project
represented a first effort to deploy preventive interventions at scale in a Cambodian context is
itself a potentially significant outcome of interest and value that is not captured in the
presentation of caries preventive fractions.
The rationale for the intervention followed conventional knowledge that the most effective
setting to address oral health is in a school where it is logistically easier to deliver an
intervention and the target group is captive in a well-controlled environment (Monse et al.
2010). It also followed the evidence that, next to tooth-brushing with fluoride toothpaste, FS is
the second most effective way to prevent dental caries in children. Although the rationale
behind selecting FS as a key intervention was justified, critical analysis of the data from the
participants of the SEAL Cambodia project led to a better understanding of the natural history
of caries among the Cambodian school population. In particular, the populations amongst
whom other sealant studies have been conducted, experience the majority of their new carious
lesions on permanent teeth on the occlusal surfaces of their FPM. In contrast, one in five
participants in the SEAL Cambodia group developed frank cavitation on an approximal surface

154
that extended to the occlusal surface over the two-year observation period. In this situation FS
is not effective in protecting that tooth from the progression of caries or managing the majority
of lesions among a population. Therefore, although the Fuji VII® FS did render benefit,
managing the majority of carious lesions amongst Cambodian primary school children would
potentially require a combination of approaches. These might include supervised tooth-
brushing and complimentary secondary preventive techniques (Goldman et al. 2017; Ruff &
Niederman, 2018).
SEAL Cambodia is not the only large-scale preventive oral health intervention in Cambodia.
The two other prominent interventions are the Fit For School (FFS) intervention which
rendered a 20% preventive increment (Duijster et al. 2017) and the Bright Smiles Bright
Futures (BSBF) project which has not been evaluated in terms of caries prevention or behaviour
change. The FFS intervention features daily tooth-brushing with 1450 ppm fluoride toothpaste
and it focuses on creating a healthy environment first and foremost (Monse et al. 2010). The
overall caries preventive increment was somewhat higher than that achieved in the SEAL
Cambodia project and it had a larger impact over a wider target group within the primary school
environment. In addition, it is probable that the tooth-brushing slowed the progression of both
approximal and occlusal lesions. In contrast, the SEAL Cambodia strategy had a very specific
function in the prevention of dental caries on the occlusal surfaces of FPM. The FFS project
did not collect any self-reported data on oral symptoms and so it is not possible to say whether
the tooth-brushing resulted in an improvement in OHRQoL, although other similar studies have
reported such improvements (Clark, 2017). The mantra still stands that tooth-brushing with
fluoride toothpaste is the single most effective way to prevent dental caries. In the Cambodian
setting the preventive fraction achieved through the FFS program was lower than that achieved
in other settings, however, that a reduction was achieved reinforces the evidence that tooth-
brushing with fluoride toothpaste should be the first step in implementing any preventive
program. Further investigation could examine how FS could supplement other primary
preventive interventions such as a school-based tooth-brushing program or secondary
interventions such as simple ART restorations in a school setting. It is clear that FS are not a
stand-alone intervention; however, in this case they were a good first step in reorienting dental
services towards a more-upstream approach and an entry point for reorientation of services.

155
6.2 Summary of findings from the Cambodia Smile project
The data from the SEAL Cambodia cohort combined with the cross-sectional data on ECC
from Chapter 4 highlighted that school-age was too late to address the caries problem for
Cambodian children. That most children were exhibiting the signs of dental caries in the early
years of life, and those with an extreme caries burden (dmft > 9) did not respond favourably to
preventive therapies led to the conclusion that dental caries should be managed before children
reach school-age. The risk modelling among a convenience sample of Cambodian pre-
schoolers helped to inform the strategy for the Cambodia Smile pilot even in the presence of
clear shortcomings in the sampling frame of the cross-sectional study (Chapter 4). As a
convenience sample was involved, the findings of the study could not be extrapolated to
represent the wider population. Also, the sample size was not large enough to allow for
meaningful sub-group analysis which limited the investigation in terms of better understanding
of dietary habits across various age groups. Subsequently, the value of the dietary indicators
included in the survey were limited and failed to inform the risk profile. Holistic investigation
of caries in any setting requires understanding of the drivers of the caries process. Therefore,
further investigations are warranted to better understand the dietary patterns, particularly
around nursing habits and complimentary feeding that contribute to the caries process among
preschool children in Cambodia. In addition, investigation is needed to understand the
mediators of those behaviours and the context specific mechanisms for change (Rai and Tiwari,
2018). Despite the limitations of the cross-sectional survey undertaken, the data was a valuable
first attempt at assessing need and modelling the risk indicators among a group of preschool
Cambodian children in the absence of other information.
Although the Cambodia Smile intervention was successful in reducing caries increment among
those in the intervention, there were some limitations that would argue caution around the
interpretation of the results. In particular, the control and intervention groups were recruited
using different sampling procedures and that led to less diversity among the control group in
terms of sociodemographic characteristics. This could have played a role in either amplifying
or masking benefits of the intervention although there were no significant differences in caries
experience by sociodemographic characteristics among the sample. The second limitation is
that although the final follow-up rate was acceptable at around 70%, follow-up or attendance
at each opportunity for the preventive intervention was much lower. That meant that not all
children received FV and the sample was not powered to accurately examine differences based

156
on varying levels of the intervention. Further investigation, at a greater scale, is needed to
understand how those who realized those opportunities for intervention differed from those
who did not. Also, that some children in the intervention group still experienced a severe caries
burden, and one in twenty five children in the intervention group experienced dental abscesses,
suggests that the intervention benefited some participants more than others and the
characteristics of those participants who did not realize the benefits should be further explored.
The identification of late introduction of tooth-brushing habits in the cross-sectional survey
was consistent with the findings of the CNOHS (Chher et al. 2016) and indicated that the
preschool population in Cambodia experienced almost no exposure to fluoride. As such, the
benefits of the Cambodia Smile pilot intervention could largely be attributed to the introduction
of fluoride in a previously non-fluoridated community. The Cambodia Smile intervention was
successful at using fluoride to moderate the relationship between an unfavourable diet and
caries severity. The study replicates the well documented ability of fluoride to reduce disease
burden (Bernabé et al. 2016; Kumar & Moss 2008). The intervention was not successful at
adjusting behaviour around the key driver of the disease, the diet, as evidenced by the absence
of any significant differences in the consumption of non-nutritious foods among the control
and intervention group. The application of fluoride in the form of FV and fluoride toothpaste
is the best effort of a health profession at moderating the symptoms of a behavioural disease.
That the benefits were seen both at tooth level and in the household group, as measured by the
FIS, is sufficient justification for upscaling the Cambodia smile pilot as a first step at reducing
the caries burden at a population level.
It is worth noting that the benefits of FV observed in the present study are greater than those
reported in some more recent studies. This could be explained by the fact that the FV was
applied at a pivotal time, as informed by the cross-sectional data demonstrating that carious
lesions are forming in the first year of life. In contrast, those studies that did not observe the
benefits of FV may have been limited by the fact that the population already had a prevalence
of ECC lower than 40% (Agouropoulos et al. 2014; Anderson et al. 2016; Divaris et al. 2013;
Jiang et al. 2014; Oliveira et al. 2014); the participants were not at optimal age or caries risk to
realize benefit (Muñoz-Millán et al. 2018; Tickle et al. 2017) or the protocol for selection of
cases by the working health professional did not ensure that all those at risk received the FV
(Fontana et al. 2018). Further investigations at a larger scale would be worthwhile to build
evidence for ideal timing, target groups, and policy mechanisms that would inform those health
professionals in practice about the best protocol for selecting cases for application. The

157
protocol for FV application in Cambodia Smile in which every child receives FV application
at each opportunity appears to be suitable for rendering preventive benefits in a Cambodian
setting at dose that is appropriate. This could be confirmed by close monitoring during the
upscale phase to observe both differences in caries and presence of enamel defects.
Furthermore, given the attendance patterns among the target community, applying FV at scale
would not be possible outside of the demonstrated model in a primary health care setting and
by primary health care providers.
Although the fluoride applications were successful, even if the same preventive increments are
realized at population level, there will still be a proportion of children in Cambodia who still
develop carious lesions and for whom the intervention would not work. Therefore, further
research from a mixed-methods approach is needed to better understand the social, structural,
and behavioural aspects of the caries experience in the Cambodian context so that a more
definitive strategy can be implemented. In the meantime, it is clear that the Cambodia Smile
intervention was successful for a large proportion of the group and that is sufficient justification
for upscaling along with close monitoring.

158
6.3 Conclusions
The present series of investigations are an example of the adaptation of strategies to achieve
optimal results in a specific setting. The SEAL Cambodia project adds to the body of evidence
around the use of GIC FS for the prevention of carious lesions on FPM. Further investigation
could focus on the role of FS within a more holistic caries preventive approach in Cambodian
school children. The SEAL Cambodia project was adapted to achieve a favourable preventive
fraction of 90% at 1 year. When the 2-year preventive fraction (30%) was less favourable due
to the presence of approximal lesions, the Cambodia Smile project was a response to the
realization that school-age was too late to address the caries disease among Cambodian
children. The Cambodia Smile intervention builds evidence for the introduction of topical
fluorides at a young age and in this case, such an application (in combination with provision of
fluoride toothpaste) rendered a 66% reduction in caries severity. It is unique in that it is the
first study to demonstrate benefits of such of an intervention in terms of OHRQoL.
Further investigation is needed to better understand the social, structural and behavioural
aspects of the ECC phenomenon in Cambodia in order to better inform strategy for behaviour
change to address the diet. The Cambodia Smile pilot provides sufficient evidence to justify
up-scale and monitoring in order to reduce the disease burden among a larger proportion of
Cambodian children.

159
6.4 References Chapter 6
Agouropoulos, A., Twetman, S., Pandis, N., Kavvadia, K. & Papagiannoulis, L. (2014) Caries-
preventive effectiveness of fluoride varnish as adjunct to oral health promotion and supervised
tooth-brushing in preschool children: A double-blind randomized controlled trial. Journal of
Dentistry, 42 (10), 1277–1283
Anderson, M., Dahllöf, G., Twetman, S., Jansson, L., Bergenlid, A.-C. & Grindefjord, M.
(2016) Effectiveness of Early Preventive Intervention with Semiannual Fluoride Varnish
Application in Toddlers Living in High-Risk Areas: A Stratified Cluster-Randomized
Controlled Trial. Caries Research, 50 (1), 17–23.
Ahovuo-Saloranta, A., Forss, H., Hiiri, A., Nordblad, A. & Mäkelä, M. (2016) Pit and fissure
sealants versus fluoride varnishes for preventing dental decay in the permanent teeth of children
and adolescents. The Cochrane Library, CD003067.
Baker, S.R., Foster Page, L., Thomson, W.M., Broomhead, T., Bekes, K., Benson, P.E.,
Aguilar-Diaz, F., Do, L., Hirsch, C., Marshman, Z. & McGrath, C. (2018) Structural
Determinants and Children’s Oral Health: A Cross-National Study. Journal of Dental
Research, In Print:0022034518767401
Bernabé, E., Vehkalahti, M. M., Sheiham, A., Lundqvist, A. & Suominen, A.L. (2016) The
shape of the dose-response relationship between sugars and caries in adults. Journal of Dental
Research, 95 (2), 167-172.
Chher T., Turton B., Hak S., Beltran E., Courtel F., Durward C. & Hobdell M. (2016) Dental
caries experience in Cambodia: Findings from the 2011 Cambodia National Oral Health
Survey. Journal of International Oral Health, 8 (1), 1.
Clark, E. (2017) Supervised tooth-brushing in Northland. (Doctoral dissertation, University of
Otago).
Duangthip, D., Chu, C.H. & Lo, E.C.M. (2016) A randomized clinical trial on arresting dentine
caries in preschool children by topical fluorides—18 month results. Journal of Dentistry, 44,
57-63.
Divaris, K., Preisser, J. S. & Slade, G. D. (2013) Surface-Specific Efficacy of Fluoride Varnish
in Caries Prevention in the Primary Dentition: Results of a Community Randomized Clinical
Trial. Caries Research, 47 (1), 78–87.
Duijster, D., Monse, B., Dimaisip-Nabuab, J., Djuharnoko, P., Heinrich-Weltzien, R., Hobdell,
M., Kromeyer-Hauschild, K., Kunthearith, Y., Mijares-Majini, M.C., Siegmund, N. &
Soukhanouvong, P. (2017) ‘Fit for school’–a school-based water, sanitation and hygiene
programme to improve child health: Results from a longitudinal study in Cambodia, Indonesia
and Lao PDR. BMC Public Health, 17 (1), 302.
Fontana, M., Eckert, G.J., Keels, M.A., Jackson, R., Katz, B., Levy, B.T. & Levy, S.M. (2018)
Fluoride Use in Health Care Settings: Association with Children’s Caries Risk. Advances in
Dental Research, 29 (1), 24-34.
Goldman, A., Leal, S. C., Amorim, R. G. de & Frencken, J. E. (2017) Treating High-Caries
Risk Occlusal Surfaces in FPM through Sealants and Supervised Tooth-brushing: A 3-Year
Cost-Effective Analysis. Caries Research, 51 (5), 489–499.

160
Jiang, E. M., Lo, E. C. M., Chu, C. H. & Wong, M. C. M. (2014) Prevention of early childhood
caries (ECC) through parental tooth-brushing training and fluoride varnish application: A 24-
month randomized controlled trial. Journal of Dentistry, 42 (12), 1543–1550.
Kumar, J. V. & Moss, M. E. (2008) Fluorides in dental public health programs. Dental Clinics
of North America, 52 (2), 387–401.
Monse, B., Naliponguit, E., Belizario, V., Benzian, H. & Helderman, W. van P. (2010)
Essential health care package for children-the “Fit for School”program in the Philippines.
International Dental Journal, 60 (2), 85–93.
Muñoz-Millán, P., Zaror, C., Espinoza-Espinoza, G., Vergara-Gonzalez, C., Muñoz, S., Atala-
Acevedo, C., & Martínez-Zapata, M. J. (2018) Effectiveness of fluoride varnish in preventing
early childhood caries in rural areas without access to fluoridated drinking water: A randomized
control trial. Community Dentistry and Oral Epidemiology, 46 (1), 63–69.
Oliveira, B. H., Salazar, M., Carvalho, D. M., Falcão, A., Campos, K. & Nadanovsky, P. (2014)
Biannual Fluoride Varnish Applications and Caries Incidence in Preschoolers: A 24-month
Follow-Up Randomized Placebo-Controlled Clinical Trial. Caries Research, 48 (3), 228–236.
One-2-One Cambodia (2016) Final report for SEAL Cambodia. Phnom Penh, Cambodia.
Petersson, L., Twetman, S., Dahlgren, H., Norlund, A., Holm, A.K., Nordenram, G., Lagerlöf,
F., Söder, B., Källestål, C., Mejàre, I. & Axelsson, S., (2004) Professional fluoride varnish
treatment for caries control: a systematic review of clinical trials. Acta Odontologica
Scandinavica, 62 (3),170-176.
Rai, N.K. & Tiwari, T. (2018) Parental Factors influencing the Development of early childhood
caries in Developing Nations: a Systematic Review. Frontiers in Public Health, 16 (6) 64.
Ruff, R. R. & Niederman, R. (2018) Comparative effectiveness of school-based caries
prevention: a prospective cohort study. BMC Oral Health, 18 (1), 53.
Tickle, M., O’Neill, C., Donaldson, M., Birch, S., Noble, S., Killough, S., Murphy, L., Greer,
M., Brodison, J., Verghis, R. & Worthington, H.V. (2017) A randomized controlled trial of
caries prevention in dental practice. Journal of Dental Research, 96 (7), 741-746.
Yengopal, V., Mickenautsch, S., Bezerra, A. C. & Leal, S. C. (2009) Caries-preventive effect
of glass ionomer and resin-based fissure sealants on permanent teeth: a meta analysis. Journal
of Oral Science, 51 (3), 373–382.

161

Minerva Access is the Institutional Repository of The University of Melbourne
Author/s:
Turton, Bathsheba
Title:
Early childhood caries in Cambodia
Date:
2018
Persistent Link:
http://hdl.handle.net/11343/220788
File Description:
Early childhood caries in Cambodia
Terms and Conditions:
Terms and Conditions: Copyright in works deposited in Minerva Access is retained by the
copyright owner. The work may not be altered without permission from the copyright owner.
Readers may only download, print and save electronic copies of whole works for their own
personal non-commercial use. Any use that exceeds these limits requires permission from
the copyright owner. Attribution is essential when quoting or paraphrasing from these works.