VA DMAS CMHRS, Residential, EPSDT Behavioral Therapy (ABA ...

EPSDTProvider Orientation Packet
Early and Periodic Screening, Diagnosis and Treatment

2
EPSDT Provider Orientation Packet Table of Contents
Frequently Asked Questions and EPSDT Department Responsibilities . . . . . . . . . . . . . . . . . . . . . . . . . . . .3
Important Telephone Numbers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
EPSDT Components . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
EPSDT Periodicity Schedule . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6-7
EPSDT Reporting/Billing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8-9
EPSDT Referral Process . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
EPSDT Eligibility Confirmation Fax Transmittal Sheet . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
EPSDT Medical Record Review Requirements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
EPSDT Expanded Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11-12
EPSDT Screenings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Appendices
A . Recommended Immunizations from the CDC and Department of Health & Human Services . A1-14
B. Body Mass Index Charts from the CDC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . B1-2

3
Frequently Asked QuestionsQ: What is Early and Periodic Screening, Diagnosis and Treatment (EPSDT)?A: • EPSDT is a Federally mandated program for Medicaid-eligible children ages birth to 21 years,
which began in 1967 .
• EPSDT uses a Periodicity Schedule based on the AAP/ Bright Futures Standards of Care and State guidelines .
Q: Who do I contact with billing or other questions/concerns about the EPSDT program? A: Please contact Provider Services or Provider Claims Service Unit at (800) 578-0775 .
Q: What are the timely filing requirements for EPSDT? A: Providers must file within 180 days from the original date of service. This is consistent with
Passport’s policy for all claims .
Q: Am I allowed to file sick and EPSDT visits for the same date of service? A: Yes, providers may file sick and EPSDT visits for the same date of service. Please follow standard
coding guidelines for reporting the sick visit in addition to the EPSDT service .
Q: How can I verify if a member is eligible for EPSDT? A: • To verify EPSDT eligibility for four (4) or fewer members, call the EPSDT team at (877) 903-
0082 ext. 8210 and leave a message. You will receive a response within one hour during regular business hours .
• To confirm EPSDT eligibility for five (5) or more members, please complete the EPSDT Eligibility Confirmation Fax Transmittal Sheet (available on page 10) and fax to the EPSDT team at (800) 492-2854 at least 24 hours in advance. You will receive a faxed response within 24 hours.
Q: How do I determine the interval screenings for EPSDT? A: Please go to Passport’s website and click on EPSDT for the Interval Screening Calculator .
Q: How do I request outreach for non-compliant EPSDT members? A: • Passport asks the provider office to attempt outreach to a member three times (i.e. phone calls,
letters, and/or postcards) prior to contacting Passport for outreach .
• If these efforts have failed, please contact the EPSDT team at (877) 903-0082 ext. 8210 to schedule member outreach. The requesting provider will receive notification regarding the outcome of the home visit within 60 days of the outreach request .
EPSDT Department ResponsibilitiesPassport Health Plan (Passport) is committed to working with our provider partners to improve the health and quality of life of our youngest members by using a comprehensive, integrated approach to care. Passport’s EPSDT staff receive system notifications when outreach is necessary and when mem-bers are non-compliant .
Here are some of the ways we may assist you with continuity and coordination of care for our members:
• Provide telephonic member and parent/guardian outreach and education .
• Remove barriers to care by assisting with transportation, scheduling appointments, and referrals to social services and specialists .
• Confirm EPSDT eligibility for providers.
• Refer members for a home visit, at the PCP’s request .

4
Important Telephone NumbersCare Coordination Program Coordinator - Pediatric Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (502) 242-4941
EPSDT Outreach Care Connector . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (877) 903-0082
Other Passport DepartmentsProvider Services and Provider Claims Service Unit . . . . . . . . . . . . . . . . . . . . . . . . . . . . (800) 578-0775 Member Services . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (800) 578-0603 Utilization Management . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (800) 578-0636
Local Assistance Vaccines for Children Program . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . (502) 564-4478
Transportation Brokers BROKER COUNTIES PHONE
NUMBER
LKLP Community Action Council
Adair, Allen, Barren, Bath, Boyd, Breathitt, Breckinridge, Butler, Carter, Clay, Edmonson, Elliott, Grayson, Green, Greenup, Hardin, Harlan, Hart, Jackson, Knott, Larue, Lawrence, Lee, Leslie, Letcher, Logan, Marion, Meade, Menifee, Metcalfe, Morgan, Nelson, Owsley, Perry, Rowan, Simpson, Taylor, Warren, Wolfe
1-800-245-2826
Pennyrile Allied Community Services
Caldwell, Christian, Crittenden, Hopkins, Livingston, Lyon, Muhlenberg, Todd, Trigg
1-800-467-4601
Audubon Area Community Services (GRITS)
Ballard, Calloway, Carlisle, Daviess, Fulton, Graves, Hancock, Henderson, Hickman McLean, Marshall, McCracken, Ohio, Union, Webster
1-800-816-3511
Rural Transit Enterprises (RTEC)
Bell, Clinton, Cumberland, Knox, Laurel,McCreary, Monroe, Pulaski, Rockcastle, Russell, Wayne, Whitley
1-800-321-7832
Federated Transit Services of the Bluegrass (FTSB)
Boone, Bourbon, Bullitt, Campbell, Carroll, Clark, Estill, Fayette, Gallatin, Grant, Harrison, Henry, Jefferson, Kenton, Madison, Montgomery, Nicholas, Oldham, Owen, Pendleton, Powell, Shelby, Spencer, Trimble
1-888-848-0989
Bluegrass Community Action Partnership (BGCAP)
Anderson, Boyle, Casey, Franklin, Garrard, Jessamine, Lincoln, Mercer, Scott, Washington, Woodford
1-800-456-6588
Licking Valley Community Action Program (LVCAP)
Bracken, Fleming, Lewis, Mason, Robertson 1-800-803-1310
Sandy Valley Transportation Services
Floyd, Johnson, Magoffin, Martin, Pike 1-800-444-7433

5
EPSDT ComponentsMedical History
• Physical Exam
• Height and Weight
• Weight to Height Ratio, BMI
• Hearing Screen
• Vision Screen
• Dental Screen
Growth and Development
• Social and Emotional Skills
• Sexual Development
• Gross Motor Skills
• Fine Motor Skills
• Cognitive, Linguistic, and Communication Skills
• Diet and Nutrition
Labs
• Urinalysis
• Lead
• Hematocrit
• Hemoglobin
• Tuberculosis
• Lipid Profile for Dyslipidemia Screening
Anticipatory Guidance
• Tobacco / Drugs / Alcohol Use
• Sex, STIs and Pregnancy
• Mental Health
• Nutrition and Physical Activity
• Dental/Oral Health
•Family Support, Establishing Routines
•Discipline, Problem Solving, Anger Management, Conflict Resolution
•Peer Relationships and Bullying
•Social and Academic Competency
•Computer and Social Media Use
•Self-Responsibility
•Safety - Home, Sports, Recreational, Car Seat, Poisoning, Infant Choking, Sleep Outines
•Mental Health, Stressors, Mood Changes, Depression
Immunizations
• 2018 Immunization Schedules
(Available on page 6 and 7)
Health and Education
• Parents and Children
• Teens

6
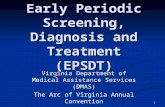
EPSDT Periodicity Schedule
INFA
NCY
EARL
Y CH
ILD
HO
OD
MID
DLE
CH
ILD
HO
OD
AD
OLE
SCEN
CEA
GE1
Pren
atal
2N
ewbo
rn3
3-5
d4By
1 m
o2
mo
4 m
o6
mo
9 m
o12
mo
15 m
o18
mo
24 m
o30
mo
3 y
4 y
5 y
6 y
7 y
8 y
9 y
10 y
11 y
12 y
13 y
14 y
15 y
16 y
17 y
18 y
19 y
20 y
21 y
HIS
TORY
Initi
al/In
terv
all
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
l
MEA
SURE
MEN
TS
Leng
th/H
eigh
t and
Wei
ght
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
l
Hea
d Ci
rcum
fere
nce
ll
ll
ll
ll
ll
l
Wei
ght f
or L
engt
hl
ll
ll
ll
ll
l
Body
Mas
s In
dex5
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
l
Bloo
d Pr
essu
re6
êê
êê
êê
êê
êê
êê
ll
ll
ll
ll
ll
ll
ll
ll
ll
l
SEN
SORY
SCR
EEN
ING
Visi
on7
êê
êê
êê
êê
êê
êê
ll
ll
êl
êl
êl
êê
lê
êê
êê
ê
Hea
ring
l8
l9
êê
êê
êê
êê
êl
ll
êl
êl
l10
ll
DEV
ELO
PMEN
TAL/
BEH
AVIO
RAL
HEA
LTH
Dev
elop
men
tal S
cree
ning
11l
ll
Autis
m S
pect
rum
Dis
orde
r Scr
eeni
ng12
ll
Dev
elop
men
tal S
urve
illan
cel
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
l
Psyc
hoso
cial
/Beh
avio
ral A
sses
smen
t13l
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
Toba
cco,
Alc
ohol
, or D
rug
Use
Ass
essm
ent14
êê
êê
êê
êê
êê
êD
epre
ssio
n Sc
reen
ing15
ll
ll
ll
ll
ll
Mat
erna
l Dep
ress
ion
Scre
enin
g16l
ll
l
PHYS
ICA
L EX
AM
INAT
ION
17l
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
PRO
CED
URE
S18
New
born
Blo
od l
19 l
20
New
born
Bili
rubi
n21l
Criti
cal C
onge
nita
l Hea
rt D
efec
t22l
Imm
uniz
atio
n23l
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
Ane
mia
24ê
lê
êê
êê
êê
êê
êê
êê
êê
êê
êê
êê
êê
Lead
25ê
êl
or ê
26ê
l o
r ê26
êê
êê
Tube
rcul
osis
27ê
êê
êê
êê
êê
êê
êê
êê
êê
êê
êê
êê
Dys
lipid
emia
28ê
êê
êl
êê
êê
êl
Sexu
ally
Tra
nsm
itted
Infe
ctio
ns29
êê
êê
êê
êê
êê
êH
IV30
êê
êê
lê
êê
Cerv
ical
Dys
plas
ia31
l
ORA
L H
EALT
H32
l33
l33
êê
êê
êê
êê
Fluo
ride
Varn
ish34
l
Fluo
ride
Supp
lem
enta
tion35
êê
êê
êê
êê
êê
êê
êê
êê
êê
êê
AN
TICI
PATO
RY G
UID
AN
CEl
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
ll
l
Each
chi
ld a
nd fa
mily
is u
niqu
e; th
eref
ore,
thes
e Re
com
men
datio
ns fo
r Pre
vent
ive
Pedi
atric
Hea
lth
Care
are
des
igne
d fo
r the
car
e of
chi
ldre
n w
ho a
re re
ceiv
ing
com
pete
nt p
aren
ting,
hav
e no
m
anife
stat
ions
of a
ny im
port
ant h
ealth
pro
blem
s, an
d ar
e gr
owin
g an
d de
velo
ping
in a
sat
isfa
ctor
y fa
shio
n. D
evel
opm
enta
l, ps
ycho
soci
al, a
nd c
hron
ic d
isea
se is
sues
for c
hild
ren
and
adol
esce
nts
may
re
quire
freq
uent
cou
nsel
ing
and
trea
tmen
t vis
its s
epar
ate
from
pre
vent
ive
care
vis
its. A
dditi
onal
vi
sits
als
o m
ay b
ecom
e ne
cess
ary
if ci
rcum
stan
ces
sugg
est v
aria
tions
from
nor
mal
.
Thes
e re
com
men
datio
ns re
pres
ent a
con
sens
us b
y th
e A
mer
ican
Aca
dem
y of
Ped
iatr
ics
(AA
P)
and
Brig
ht F
utur
es. T
he A
AP
cont
inue
s to
em
phas
ize
the
grea
t im
port
ance
of c
ontin
uity
of c
are
in
com
preh
ensi
ve h
ealth
sup
ervi
sion
and
the
need
to a
void
frag
men
tatio
n of
car
e.
Refe
r to
the
spec
ific
guid
ance
by
age
as li
sted
in th
e Br
ight
Fut
ures
Gui
delin
es (H
agan
JF, S
haw
JS,
Dun
can
PM, e
ds. B
right
Fut
ures
: Gui
delin
es fo
r Hea
lth S
uper
visi
on o
f Inf
ants
, Chi
ldre
n, a
nd A
dole
scen
ts.
4th
ed. E
lk G
rove
Vill
age,
IL: A
mer
ican
Aca
dem
y of
Ped
iatr
ics;
201
7).
The
reco
mm
enda
tions
in th
is s
tate
men
t do
not i
ndic
ate
an e
xclu
sive
cou
rse
of tr
eatm
ent o
r sta
ndar
d
of m
edic
al c
are.
Var
iatio
ns, t
akin
g in
to a
ccou
nt in
divi
dual
circ
umst
ance
s, m
ay b
e ap
prop
riate
.
Copy
right
© 2
017
by th
e A
mer
ican
Aca
dem
y of
Ped
iatr
ics,
upda
ted
Febr
uary
201
7.
No
part
of t
his
stat
emen
t may
be
repr
oduc
ed in
any
form
or b
y an
y m
eans
with
out p
rior w
ritte
n pe
rmis
sion
from
the
Am
eric
an A
cade
my
of P
edia
tric
s ex
cept
for o
ne c
opy
for p
erso
nal u
se.
Reco
mm
enda
tion
s fo
r Pre
vent
ive
Pedi
atri
c H
ealt
h Ca
reBr
ight
Fut
ures
/Am
eric
an A
cade
my
of P
edia
tric
s
KEY:
l
= to
be
perf
orm
ed
ê =
risk
ass
essm
ent t
o be
per
form
ed w
ith
appr
opri
ate
acti
on to
follo
w, i
f pos
itiv
el
= ra
nge
duri
ng w
hich
a s
ervi
ce m
ay b
e pr
ovid
ed
1.
If a
child
com
es u
nder
car
e fo
r the
firs
t tim
e at
any
poi
nt o
n th
e sc
hedu
le, o
r if a
ny it
ems
are
not a
ccom
plis
hed
at th
e su
gges
ted
age,
the
sche
dule
sho
uld
be b
roug
ht u
p-to
-dat
e at
the
earli
est p
ossi
ble
time.
2.
A p
rena
tal v
isit
is re
com
men
ded
for p
aren
ts w
ho a
re a
t hig
h ris
k, fo
r firs
t-tim
e pa
rent
s, an
d fo
r tho
se w
ho re
ques
t a
conf
eren
ce. T
he p
rena
tal v
isit
shou
ld in
clud
e an
ticip
ator
y gu
idan
ce, p
ertin
ent m
edic
al h
isto
ry, a
nd a
dis
cuss
ion
of
bene
fits
of b
reas
tfee
ding
and
pla
nned
met
hod
of fe
edin
g, p
er “T
he P
rena
tal V
isit”
( htt
p://
pedi
atric
s.aap
publ
icat
ions
.org
/co
nten
t/12
4/4/
1227
.full)
.
3.
New
born
s sh
ould
hav
e an
eva
luat
ion
afte
r birt
h, a
nd b
reas
tfee
ding
sho
uld
be e
ncou
rage
d (a
nd in
stru
ctio
n an
d su
ppor
t sh
ould
be
offer
ed).
4.
New
born
s sh
ould
hav
e an
eva
luat
ion
with
in 3
to 5
day
s of
birt
h an
d w
ithin
48
to 7
2 ho
urs
afte
r dis
char
ge fr
om th
e ho
spita
l to
incl
ude
eval
uatio
n fo
r fee
ding
and
jaun
dice
. Bre
astf
eedi
ng n
ewbo
rns
shou
ld re
ceiv
e fo
rmal
bre
astf
eedi
ng
eval
uatio
n, a
nd th
eir m
othe
rs s
houl
d re
ceiv
e en
cour
agem
ent a
nd in
stru
ctio
n, a
s re
com
men
ded
in “B
reas
tfee
ding
and
th
e U
se o
f Hum
an M
ilk” (
http
://pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
29/3
/e82
7.fu
ll). N
ewbo
rns
disc
harg
ed le
ss th
an
48 h
ours
aft
er d
eliv
ery
mus
t be
exam
ined
with
in 4
8 ho
urs
of d
isch
arge
, per
“Hos
pita
l Sta
y fo
r Hea
lthy
Term
New
born
s”
(htt
p://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/125
/2/4
05.fu
ll ).
5.
Scre
en, p
er “E
xper
t Com
mitt
ee R
ecom
men
datio
ns R
egar
ding
the
Prev
entio
n, A
sses
smen
t, an
d Tr
eatm
ent o
f Chi
ld
and
Adol
esce
nt O
verw
eigh
t and
Obe
sity
: Sum
mar
y Re
port
” (ht
tp://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/120
/Su
pple
men
t_4/
S164
.full)
.
6.
Bloo
d pr
essu
re m
easu
rem
ent i
n in
fant
s an
d ch
ildre
n w
ith s
peci
fic ri
sk c
ondi
tions
sho
uld
be p
erfo
rmed
at v
isits
be
fore
age
3 y
ears
.
7.
A v
isua
l acu
ity s
cree
n is
reco
mm
ende
d at
age
s 4
and
5 ye
ars,
as w
ell a
s in
coo
pera
tive
3-ye
ar-o
lds.
Inst
rum
ent-
base
d sc
reen
ing
may
be
used
to a
sses
s ris
k at
age
s 12
and
24
mon
ths,
in a
dditi
on to
the
wel
l vis
its a
t 3 th
roug
h 5
year
s of
age
. Se
e “V
isua
l Sys
tem
Ass
essm
ent i
n In
fant
s, Ch
ildre
n, a
nd Y
oung
Adu
lts b
y Pe
diat
ricia
ns” (
http
://pe
diat
rics.a
appu
blic
atio
ns.
org/
cont
ent/
137/
1/e2
0153
596)
and
“Pro
cedu
res
for t
he E
valu
atio
n of
the
Visu
al S
yste
m b
y Pe
diat
ricia
ns”
(htt
p://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/137
/1/e
2015
3597
).
8.
Confi
rm in
itial
scr
een
was
com
plet
ed, v
erify
resu
lts, a
nd fo
llow
up,
as
appr
opria
te. N
ewbo
rns
shou
ld b
e sc
reen
ed,
per “
Year
200
7 Po
sitio
n St
atem
ent:
Prin
cipl
es a
nd G
uide
lines
for E
arly
Hea
ring
Det
ectio
n an
d In
terv
entio
n Pr
ogra
ms”
(h
ttp:
//pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
20/4
/898
.full)
.
9.
Verif
y re
sults
as
soon
as
poss
ible
, and
follo
w u
p, a
s ap
prop
riate
.
10.
Scre
en w
ith a
udio
met
ry in
clud
ing
6,00
0 an
d 8,
000
Hz
high
freq
uenc
ies
once
bet
wee
n 11
and
14
year
s, on
ce b
etw
een
15 a
nd 1
7 ye
ars,
and
once
bet
wee
n 18
and
21
year
s. Se
e “T
he S
ensi
tivity
of A
dole
scen
t Hea
ring
Scre
ens
Sign
ifica
ntly
Im
prov
es b
y Ad
ding
Hig
h Fr
eque
ncie
s” (h
ttp:
//w
ww
.jaho
nlin
e.or
g/ar
ticle
/S10
54-1
39X(
16)0
0048
-3/f
ullte
xt).
11.
See
“Iden
tifyi
ng In
fant
s an
d Yo
ung
Child
ren
With
Dev
elop
men
tal D
isor
ders
in th
e M
edic
al H
ome:
An
Alg
orith
m fo
r D
evel
opm
enta
l Sur
veill
ance
and
Scr
eeni
ng” (
http
://pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
18/1
/405
.full)
.
12.
Scre
enin
g sh
ould
occ
ur p
er “I
dent
ifica
tion
and
Eval
uatio
n of
Chi
ldre
n W
ith A
utis
m S
pect
rum
Dis
orde
rs”
(htt
p://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/120
/5/1
183.
full)
.
13.
This
ass
essm
ent s
houl
d be
fam
ily c
ente
red
and
may
incl
ude
an a
sses
smen
t of c
hild
soc
ial-e
mot
iona
l hea
lth, c
areg
iver
depr
essi
on, a
nd s
ocia
l det
erm
inan
ts o
f hea
lth. S
ee “P
rom
otin
g O
ptim
al D
evel
opm
ent:
Scre
enin
g fo
r Beh
avio
ral a
nd
Emot
iona
l Pro
blem
s” (h
ttp:
//pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
35/2
/384
) and
“Pov
erty
and
Chi
ld H
ealth
in th
e U
nite
d St
ates
” (ht
tp://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/137
/4/e
2016
0339
).
14.
A re
com
men
ded
asse
ssm
ent t
ool i
s av
aila
ble
at h
ttp:
//w
ww
.cea
sar-
bost
on.o
rg/C
RAFF
T/in
dex.
php.
15.
Reco
mm
ende
d sc
reen
ing
usin
g th
e Pa
tient
Hea
lth Q
uest
ionn
aire
(PH
Q)-2
or o
ther
tool
s av
aila
ble
in th
e G
LAD
-PC
tool
kit a
nd a
t htt
p://
ww
w.a
ap.o
rg/e
n-us
/adv
ocac
y-an
d-po
licy/
aap-
heal
th-in
itiat
ives
/Men
tal-H
ealth
/Doc
umen
ts/M
H_
Scre
enin
gCha
rt.p
df. )
16.
Scre
enin
g sh
ould
occ
ur p
er “I
ncor
pora
ting
Reco
gniti
on a
nd M
anag
emen
t of P
erin
atal
and
Pos
tpar
tum
Dep
ress
ion
Into
Pe
diat
ric P
ract
ice”
(htt
p://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/126
/5/1
032)
.
17.
At e
ach
visi
t, ag
e-ap
prop
riate
phy
sica
l exa
min
atio
n is
ess
entia
l, w
ith in
fant
tota
lly u
nclo
thed
and
old
er c
hild
ren
undr
esse
d an
d su
itabl
y dr
aped
. See
“Use
of C
hape
rone
s D
urin
g th
e Ph
ysic
al E
xam
inat
ion
of th
e Pe
diat
ric P
atie
nt”
(htt
p://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/127
/5/9
91.fu
ll).
18.
Thes
e m
ay b
e m
odifi
ed, d
epen
ding
on
entr
y po
int i
nto
sche
dule
and
indi
vidu
al n
eed.
(con
tinue
d)

7
Sum
mar
y of
Cha
nges
Mad
e to
the
Brig
ht F
utur
es/A
AP
Reco
mm
enda
tion
s fo
r Pre
vent
ive
Pedi
atri
c H
ealt
h Ca
re(P
erio
dici
ty S
ched
ule)
This
sch
edul
e re
flect
s ch
ange
s ap
prov
ed in
Feb
ruar
y 20
17 a
nd p
ublis
hed
in A
pril
2017
. Fo
r upd
ates
, vis
it w
ww
.aap
.org
/per
iodi
city
sche
dule
. Fo
r fur
ther
info
rmat
ion,
see
the
Brig
ht F
utur
es G
uide
lines
, 4th
Edi
tion,
Evi
denc
e an
d Ra
tiona
le c
hapt
er
(htt
ps://
brig
htfu
ture
s.aap
.org
/Brig
ht%
20Fu
ture
s%20
Doc
umen
ts/B
F4_E
vide
nce_
Ratio
nale
).
CH
AN
GES
MA
DE
IN F
EBR
UA
RY 2
017
HEA
RIN
G
•Ti
min
g an
d fo
llow
-up
of th
e sc
reen
ing
reco
mm
enda
tions
for h
earin
g du
ring
the
infa
ncy
visi
ts h
ave
been
del
inea
ted.
Ado
lesc
ent r
isk
asse
ssm
ent h
as c
hang
ed to
scr
eeni
ng o
nce
durin
g ea
ch ti
me
perio
d.
•Fo
otno
te 8
has
bee
n up
date
d to
read
as
follo
ws:
“Con
firm
initi
al s
cree
n w
as c
ompl
eted
, ver
ify re
sults
, and
follo
w u
p, a
s ap
prop
riate
. N
ewbo
rns
shou
ld b
e sc
reen
ed, p
er ‘Y
ear 2
007
Posi
tion
Stat
emen
t: Pr
inci
ples
and
Gui
delin
es fo
r Ear
ly H
earin
g D
etec
tion
and
Inte
rven
tion
Prog
ram
s’ (h
ttp:
//pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
20/4
/898
.full)
.”
•Fo
otno
te 9
has
bee
n ad
ded
to re
ad a
s fo
llow
s: “V
erify
resu
lts a
s so
on a
s po
ssib
le, a
nd fo
llow
up,
as
appr
opria
te.”
•Fo
otno
te 1
0 ha
s be
en a
dded
to re
ad a
s fo
llow
s: “S
cree
n w
ith a
udio
met
ry in
clud
ing
6,00
0 an
d 8,
000
Hz
high
freq
uenc
ies
once
bet
wee
n 11
and
14
year
s, on
ce b
etw
een
15 a
nd 1
7 ye
ars,
and
once
bet
wee
n 18
and
21
year
s. Se
e ‘T
he S
ensi
tivity
of A
dole
scen
t Hea
ring
Scre
ens
Sign
ifica
ntly
Impr
oves
by
Addi
ng H
igh
Freq
uenc
ies’
(htt
p://
ww
w.ja
honl
ine.
org/
artic
le/S
1054
-139
X(16
)000
48-3
/ful
ltext
).”
PSYC
HO
SOC
IAL/
BEH
AV
IOR
AL
ASS
ESSM
ENT
•Fo
otno
te 1
3 ha
s be
en a
dded
to re
ad a
s fo
llow
s: “T
his
asse
ssm
ent s
houl
d be
fam
ily c
ente
red
and
may
incl
ude
an a
sses
smen
t of c
hild
so
cial
-em
otio
nal h
ealth
, car
egiv
er d
epre
ssio
n, a
nd s
ocia
l det
erm
inan
ts o
f hea
lth. S
ee ‘P
rom
otin
g O
ptim
al D
evel
opm
ent:
Scre
enin
g fo
r Be
havi
oral
and
Em
otio
nal P
robl
ems’
(htt
p://
pedi
atric
s.aap
publ
icat
ions
.org
/con
tent
/135
/2/3
84) a
nd ‘P
over
ty a
nd C
hild
Hea
lth in
the
Uni
ted
Stat
es’ (
http
://pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
37/4
/e20
1603
39).”
TOB
ACC
O, A
LCO
HO
L, O
R D
RU
G U
SE A
SSES
SMEN
T
•Th
e he
ader
was
upd
ated
to b
e co
nsis
tent
with
reco
mm
enda
tions
.
DEP
RES
SIO
N S
CR
EEN
ING
•Ad
oles
cent
dep
ress
ion
scre
enin
g be
gins
rout
inel
y at
12
year
s of
age
(to
be c
onsi
sten
t with
reco
mm
enda
tions
of t
he U
S Pr
even
tive
Serv
ices
Tas
k Fo
rce
[USP
STF]
).
MA
TER
NA
L D
EPR
ESSI
ON
SC
REE
NIN
G
•Sc
reen
ing
for m
ater
nal d
epre
ssio
n at
1-,
2-, 4
-, an
d 6-
mon
th v
isits
has
bee
n ad
ded.
•Fo
otno
te 1
6 w
as a
dded
to re
ad a
s fo
llow
s: “S
cree
ning
sho
uld
occu
r per
‘Inco
rpor
atin
g Re
cogn
ition
and
Man
agem
ent o
f Per
inat
al
and
Post
part
um D
epre
ssio
n In
to P
edia
tric
Pra
ctic
e’ (h
ttp:
//pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
26/5
/103
2).”
NEW
BO
RN
BLO
OD
•Ti
min
g an
d fo
llow
-up
of th
e ne
wbo
rn b
lood
scr
eeni
ng re
com
men
datio
ns h
ave
been
del
inea
ted.
•Fo
otno
te 1
9 ha
s be
en u
pdat
ed to
read
as
follo
ws:
“Con
firm
initi
al s
cree
n w
as a
ccom
plis
hed,
ver
ify re
sults
, and
follo
w u
p, a
s ap
prop
riate
. The
Rec
omm
ende
d U
nifo
rm N
ewbo
rn S
cree
ning
Pan
el (h
ttp:
//w
ww
.hrs
a.go
v/ad
viso
ryco
mm
ittee
s/m
chba
dvis
ory/
herit
able
diso
rder
s/re
com
men
dedp
anel
/uni
form
scre
enin
gpan
el.p
df),
as d
eter
min
ed b
y Th
e Se
cret
ary’
s Ad
viso
ry C
omm
ittee
on
Her
itabl
e D
isor
ders
in N
ewbo
rns
and
Child
ren,
and
sta
te n
ewbo
rn s
cree
ning
law
s/re
gula
tions
(htt
p://
gene
s-r-
us.u
thsc
sa.e
du/s
ites/
gene
s-r-
us/fi
les/
nbsd
isor
ders
) est
ablis
h th
e cr
iteria
for a
nd c
over
age
of n
ewbo
rn s
cree
ning
pro
cedu
res
and
prog
ram
s.”
•Fo
otno
te 2
0 ha
s be
en a
dded
to re
ad a
s fo
llow
s: “V
erify
resu
lts a
s so
on a
s po
ssib
le, a
nd fo
llow
up,
as
appr
opria
te.”
NEW
BO
RN
BIL
IRU
BIN
•Sc
reen
ing
for b
iliru
bin
conc
entr
atio
n at
the
new
born
vis
it ha
s be
en a
dded
.
•Fo
otno
te 2
1 ha
s be
en a
dded
to re
ad a
s fo
llow
s: “C
onfir
m in
itial
scr
eeni
ng w
as a
ccom
plis
hed,
ver
ify re
sults
, and
follo
w u
p,
as a
ppro
pria
te. S
ee ‘H
yper
bilir
ubin
emia
in th
e N
ewbo
rn In
fant
≥35
Wee
ks’ G
esta
tion:
An
Upd
ate
With
Cla
rifica
tions
’ (h
ttp:
//pe
diat
rics.a
appu
blic
atio
ns.o
rg/c
onte
nt/1
24/4
/119
3).”
DYS
LIPI
DEM
IA
•Sc
reen
ing
for d
yslip
idem
ia h
as b
een
upda
ted
to o
ccur
onc
e be
twee
n 9
and
11 y
ears
of a
ge, a
nd o
nce
betw
een
17 a
nd 2
1 ye
ars
of a
ge (t
o be
con
sist
ent w
ith g
uide
lines
of t
he N
atio
nal H
eart
, Lun
g, a
nd B
lood
Inst
itute
).
SEX
UA
LLY
TRA
NSM
ITTE
D IN
FEC
TIO
NS
•Fo
otno
te 2
9 ha
s be
en u
pdat
ed to
read
as
follo
ws:
“Ado
lesc
ents
sho
uld
be s
cree
ned
for s
exua
lly tr
ansm
itted
infe
ctio
ns (S
TIs)
pe
r rec
omm
enda
tions
in th
e cu
rren
t edi
tion
of th
e A
AP
Red
Book
: Rep
ort o
f the
Com
mitt
ee o
n In
fect
ious
Dis
ease
s.”
HIV
•A
sub
head
ing
has
been
add
ed fo
r the
HIV
uni
vers
al re
com
men
datio
n to
avo
id c
onfu
sion
with
STI
s se
lect
ive
scre
enin
g re
com
men
datio
n.
•Sc
reen
ing
for H
IV h
as b
een
upda
ted
to o
ccur
onc
e be
twee
n 15
and
18
year
s of
age
(to
be c
onsi
sten
t with
reco
mm
enda
tions
of
the
USP
STF)
.
•Fo
otno
te 3
0 ha
s be
en a
dded
to re
ad a
s fo
llow
s: “A
dole
scen
ts s
houl
d be
scr
eene
d fo
r HIV
acc
ordi
ng to
the
USP
STF
reco
mm
enda
tions
(h
ttp:
//w
ww
.usp
reve
ntiv
eser
vice
stas
kfor
ce.o
rg/u
spst
f/us
pshi
vi.h
tm) o
nce
betw
een
the
ages
of 1
5 an
d 18
, mak
ing
ever
y eff
ort t
o pr
eser
ve c
onfid
entia
lity
of th
e ad
oles
cent
. Tho
se a
t inc
reas
ed ri
sk o
f HIV
infe
ctio
n, in
clud
ing
thos
e w
ho a
re s
exua
lly a
ctiv
e, p
artic
ipat
e in
inje
ctio
n dr
ug u
se, o
r are
bei
ng te
sted
for o
ther
STI
s, sh
ould
be
test
ed fo
r HIV
and
reas
sess
ed a
nnua
lly.”
OR
AL
HEA
LTH
•A
sses
sing
for a
den
tal h
ome
has
been
upd
ated
to o
ccur
at t
he 1
2-m
onth
and
18-
mon
th th
roug
h 6-
year
vis
its. A
sub
head
ing
has
been
add
ed fo
r fluo
ride
supp
lem
enta
tion,
with
a re
com
men
datio
n fr
om th
e 6-
mon
th th
roug
h 12
-mon
th a
nd 1
8-m
onth
thro
ugh
16-y
ear v
isits
.
•Fo
otno
te 3
2 ha
s be
en u
pdat
ed to
read
as
follo
ws:
“Ass
ess
whe
ther
the
child
has
a d
enta
l hom
e. If
no
dent
al h
ome
is id
entif
ied,
pe
rfor
m a
risk
ass
essm
ent (https://www.aap
.org/RiskA
ssessm
entToo
l) an
d re
fer t
o a
dent
al h
ome.
Rec
omm
end
brus
hing
with
flu
orid
e to
othp
aste
in th
e pr
oper
dos
age
for a
ge. S
ee ‘M
aint
aini
ng a
nd Im
prov
ing
the
Ora
l Hea
lth o
f You
ng C
hild
ren’
(htt
p://
pedi
atric
s.aa
ppub
licat
ions
.org
/con
tent
/134
/6/1
224)
.”
•Fo
otno
te 3
3 ha
s be
en u
pdat
ed to
read
as
follo
ws:
“Per
form
a ri
sk a
sses
smen
t (https://www.aap
.org/RiskA
ssessm
entToo
l). S
ee
‘Mai
ntai
ning
and
Impr
ovin
g th
e O
ral H
ealth
of Y
oung
Chi
ldre
n’ (h
ttp:
//pe
diat
rics.
aapp
ublic
atio
ns.o
rg/
cont
ent/
134/
6/12
24).”
•Fo
otno
te 3
5 ha
s be
en a
dded
to re
ad a
s fo
llow
s: “I
f prim
ary
wat
er s
ourc
e is
defi
cien
t in
fluor
ide,
con
side
r ora
l fluo
ride
supp
lem
enta
tion.
See
‘Flu
orid
e U
se in
Car
ies
Prev
entio
n in
the
Prim
ary
Care
Set
ting’
(htt
p://
pedi
atric
s.aa
ppub
licat
ions
.org
/co
nten
t/13
4/3/
626)
.”
19.
Confi
rm in
itial
scr
een
was
acc
ompl
ishe
d, v
erify
resu
lts, a
nd fo
llow
up,
as
appr
opria
te.
The
Reco
mm
ende
d U
nifo
rm N
ewbo
rn S
cree
ning
Pan
el (h
ttp:
//w
ww
.hrs
a.go
v/ad
viso
ryco
mm
ittee
s/m
chba
dvis
ory/
herit
able
diso
rder
s/re
com
men
dedp
anel
/un
iform
scre
enin
gpan
el.p
df),
as d
eter
min
ed b
y Th
e Se
cret
ary’
s Ad
viso
ry C
omm
ittee
on
Her
itabl
e D
isor
ders
in N
ewbo
rns a
nd C
hild
ren,
and
stat
e ne
wbo
rn sc
reen
ing
law
s/re
gula
tions
(htt
p://
gene
s-r-
us.u
thsc
sa.e
du/s
ites/
gene
s-r-
us/fi
les/
nb
sdis
orde
rs.p
df) e
stab
lish
the
crite
ria fo
r and
cov
erag
e of
new
born
scr
eeni
ng
proc
edur
es a
nd p
rogr
ams.
20.
Verif
y re
sults
as
soon
as
poss
ible
, and
follo
w u
p, a
s ap
prop
riate
.
21.
Confi
rm in
itial
scr
eeni
ng w
as a
ccom
plis
hed,
ver
ify re
sults
, and
follo
w u
p,
as a
ppro
pria
te. S
ee “H
yper
bilir
ubin
emia
in th
e N
ewbo
rn In
fant
≥35
Wee
ks’
Ges
tatio
n: A
n U
pdat
e W
ith C
larifi
catio
ns” (
http
://pe
diat
rics.a
appu
blic
atio
ns.o
rg/
cont
ent/
124/
4/11
93).
22.
Scre
enin
g fo
r crit
ical
con
geni
tal h
eart
dis
ease
usi
ng p
ulse
oxi
met
ry s
houl
d be
pe
rfor
med
in n
ewbo
rns,
afte
r 24
hour
s of
age
, bef
ore
disc
harg
e fr
om th
e ho
spita
l, pe
r “En
dors
emen
t of H
ealth
and
Hum
an S
ervi
ces
Reco
mm
enda
tion
for P
ulse
O
xim
etry
Scr
eeni
ng fo
r Crit
ical
Con
geni
tal H
eart
Dis
ease
” (ht
tp://
pedi
atric
s.aa
ppub
licat
ions
.org
/con
tent
/129
/1/1
90.fu
ll).
23.
Sche
dule
s, pe
r the
AA
P Co
mm
ittee
on
Infe
ctio
us D
isea
ses,
are
avai
labl
e at
ht
tp://
redb
ook.
solu
tions
.aap
.org
/SS/
Imm
uniz
atio
n_Sc
hedu
les.a
spx.
Eve
ry v
isit
shou
ld b
e an
opp
ortu
nity
to u
pdat
e an
d co
mpl
ete
a ch
ild’s
imm
uniz
atio
ns.
24.
See
“Dia
gnos
is a
nd P
reve
ntio
n of
Iron
Defi
cien
cy a
nd Ir
on-D
efici
ency
Ane
mia
in
Infa
nts
and
Youn
g Ch
ildre
n (0
–3 Y
ears
of A
ge)”
(htt
p://
pedi
atric
s.aap
publ
icat
ions
.or
g/co
nten
t/12
6/5/
1040
.full)
.
25.
For c
hild
ren
at ri
sk o
f lea
d ex
posu
re, s
ee “L
ow L
evel
Lea
d Ex
posu
re H
arm
s Ch
ildre
n:
A R
enew
ed C
all f
or P
rimar
y Pr
even
tion”
(htt
p://
ww
w.c
dc.g
ov/n
ceh/
lead
/ACC
LPP/
Fina
l_D
ocum
ent_
0307
12.p
df).
26.
Perf
orm
risk
ass
essm
ents
or s
cree
ning
s as
app
ropr
iate
, bas
ed o
n un
iver
sal s
cree
ning
re
quire
men
ts fo
r pat
ient
s w
ith M
edic
aid
or in
hig
h pr
eval
ence
are
as.
27.
Tube
rcul
osis
test
ing
per r
ecom
men
datio
ns o
f the
AA
P Co
mm
ittee
on
Infe
ctio
us
Dis
ease
s, pu
blis
hed
in th
e cu
rren
t edi
tion
of th
e A
AP
Red
Book
: Rep
ort o
f the
Co
mm
ittee
on
Infe
ctio
us D
isea
ses.
Test
ing
shou
ld b
e pe
rfor
med
on
reco
gniti
on
of h
igh-
risk
fact
ors.
28.
See
“Inte
grat
ed G
uide
lines
for C
ardi
ovas
cula
r Hea
lth a
nd R
isk
Redu
ctio
n in
Chi
ldre
n an
d A
dole
scen
ts” (
http
s://
ww
w.n
hlbi
.nih
.gov
/hea
lth-t
opic
s/in
tegr
ated
-gui
delin
es-
for-
card
iova
scul
ar-h
ealth
-and
-ris
k-re
duct
ion-
in-c
hild
ren-
and-
adol
esce
nts)
.
29.
Ado
lesc
ents
sho
uld
be s
cree
ned
for s
exua
lly tr
ansm
itted
infe
ctio
ns (S
TIs)
per
re
com
men
datio
ns in
the
curr
ent e
ditio
n of
the
AA
P Re
d Bo
ok: R
epor
t of t
he
Com
mitt
ee o
n In
fect
ious
Dis
ease
s.
30.
Ado
lesc
ents
sho
uld
be s
cree
ned
for H
IV a
ccor
ding
to th
e U
SPST
F re
com
men
datio
ns
(htt
p://
ww
w.u
spre
vent
ives
ervi
cest
askf
orce
.org
/usp
stf/
usps
hivi
.htm
) onc
e be
twee
n th
e ag
es o
f 15
and
18, m
akin
g ev
ery
effo
rt to
pre
serv
e co
nfid
entia
lity
of th
e ad
oles
cent
. Tho
se a
t inc
reas
ed ri
sk o
f HIV
infe
ctio
n, in
clud
ing
thos
e w
ho a
re s
exua
lly
activ
e, p
artic
ipat
e in
inje
ctio
n dr
ug u
se, o
r are
bei
ng te
sted
for o
ther
STI
s, s
houl
d be
te
sted
for H
IV a
nd re
asse
ssed
ann
ually
.
31.
See
USP
STF
reco
mm
enda
tions
(htt
p://
ww
w.u
spre
vent
ives
ervi
cest
askf
orce
.org
/us
pstf
/usp
scer
v.ht
m).
Indi
catio
ns fo
r pel
vic
exam
inat
ions
prio
r to
age
21 a
re n
oted
in
“Gyn
ecol
ogic
Exa
min
atio
n fo
r Ado
lesc
ents
in th
e Pe
diat
ric O
ffice
Set
ting”
(h
ttp:
//pe
diat
rics.
aapp
ublic
atio
ns.o
rg/c
onte
nt/1
26/3
/583
.full)
.
32.
Ass
ess
whe
ther
the
child
has
a d
enta
l hom
e. If
no
dent
al h
ome
is id
entif
ied,
per
form
a
risk
asse
ssm
ent (https://www.aap
.org/RiskA
ssessm
entToo
l) an
d re
fer t
o a
dent
al
hom
e. R
ecom
men
d br
ushi
ng w
ith fl
uorid
e to
othp
aste
in th
e pr
oper
dos
age
for a
ge.
See
“Mai
ntai
ning
and
Impr
ovin
g th
e O
ral H
ealth
of Y
oung
Chi
ldre
n” (h
ttp:
//pe
diat
rics.
aapp
ublic
atio
ns.o
rg/c
onte
nt/1
34/6
/122
4).
33.
Perf
orm
a ri
sk a
sses
smen
t (https://www.aap
.org/RiskA
ssessm
entToo
l). S
ee
“Mai
ntai
ning
and
Impr
ovin
g th
e O
ral H
ealth
of Y
oung
Chi
ldre
n” (h
ttp:
//pe
diat
rics.
aapp
ublic
atio
ns.o
rg/c
onte
nt/1
34/6
/122
4).
34.
See
USP
STF
reco
mm
enda
tions
(htt
p://
ww
w.u
spre
vent
ives
ervi
cest
askf
orce
.org
/us
pstf
/usp
sdnc
h.ht
m).
Onc
e te
eth
are
pres
ent,
fluor
ide
varn
ish
may
be
appl
ied
to a
ll ch
ildre
n ev
ery
3–6
mon
ths
in th
e pr
imar
y ca
re o
r den
tal o
ffice
. Ind
icat
ions
fo
r flu
orid
e us
e ar
e no
ted
in “F
luor
ide
Use
in C
arie
s Pr
even
tion
in th
e Pr
imar
y Ca
re
Sett
ing”
(htt
p://
pedi
atric
s.aa
ppub
licat
ions
.org
/con
tent
/134
/3/6
26).
35.
If pr
imar
y w
ater
sour
ce is
def
icie
nt in
fluo
ride,
con
side
r ora
l flu
orid
e su
pple
men
tatio
n.
See
“Flu
orid
e U
se in
Car
ies
Prev
entio
n in
the
Prim
ary
Care
Set
ting”
(htt
p://
pedi
atric
s.
aapp
ublic
atio
ns.o
rg/c
onte
nt/1
34/3
/626
).
(con
tinue
d)

8
EPSDT Reporting/BillingBilling for EPSDT Services
All EPSDT services must be submitted as part of the standard electronic (837) or paper (CMS-1500) claims submission process .
Steps for Billing EPSDT Services
To submit EPSDT services via claims you must:
1. Continue to bill using the same codes for comprehensive history and physical exam you use today . These codes must correspond with the member’s age .
• 99381-99385 – New Patient Series
• 99391-99395 – Established Patient Series
2. Add an “EP” modifier to the physical exam code only when all components of the appropriate EPSDT screening interval have been completed and documented in the member’s medical record . Do not add the EP modifier to other services being billed (i.e. immunizations). As a reminder, do not bill lab or testing components individually if they were conducted as part of an EPSDT screen-ing interval .
3. Acknowledge the following health evaluation services have been completed by submitting the appropriate CPT Category II codes, according to the member’s screening age, as outlined below . CPT II codes must include a nominal charge (i .e . $ .01 or $1 .00 not blank or zero) in order to adjudicate correctly .
Member Age: CPT II Code: Description:Two (2) Years and Above 3008F To confirm the BMI has been performed and documented in the
member’s medical record. (Value and percentile must be recorded.)
Nine (9) Years and Above 2014F To confirm the member’s mental status has been assessed and documented in the member’s medical record.
NOTE: Failure to submit these CPT II codes will result in denial of the EPSDT payment.

9
EPSDT Services Requiring Resubmission
The EPSDT Screening Form will no longer be accepted by Passport for resubmission, regardless of the date of service . All EPSDT services requiring resubmission must be submitted to Passport via the billing process described above .
Other Codes for Capturing Health Status Information
The Plan encourages all providers to submit additional CPT Category II codes to describe and report other important health status information. Examples include:
• 1035F – Current Smokeless Tobacco User• 1039F – Intermittent Asthma• 1000F – Tobacco Use Assessed (CAD, CAP, COPD, PV, DM)• 4004F – Patient Screened for Tobacco Use and Received Tobacco Cessation Counseling (if
identified as a tobacco user)
Passport accepts all valid CPT Category II codes . These codes are for informational purposes only and do not qualify for reimbursement . However, these codes must be submitted with a nominal charge (i .e . $ .01 or $1 .00 not blank or zero) in order to adjudicate correctly . Codes will display as de-nied on the remittance advice with a description stating “non-covered services .”
EPSDT Referral ProcessThe Department for Medicaid Services (DMS) has requested that Passport provide new statistics related to the EPSDT program that we aid in administering for the region. Specifically, Passport must conduct and demonstrate follow-up to members, and refer providers and consultants to ensure that members receive medically necessary evaluation, diagnostics, and/or treatment as a result of referrals related to EPSDT screenings .
Please be sure to file claims appropriately and keep medical records up to date.

10
Pass
port
Hea
lth P
lan
5100
Com
mer
ce C
ross
ings
Driv
eLo
uisv
ille,
KY
4022
9Ph
one:
502
-585
-821
0 Fa
x: 1
-800
-492
-285
4
To c
onfir
m E
PSD
T el
igib
ility
on
five
(5) o
r mor
e m
embe
rs, p
leas
e fa
x yo
ur re
ques
t to
the
EPSD
T Te
am a
t 1-8
00-4
92-2
854,
at l
east
24
hour
s in
adv
ance
. Oth
erw
ise,
pl
ease
leav
e a
mes
sage
on
the
EPSD
T Te
am V
oice
mai
l at 5
02-5
85-8
210.
FAX
TRA
NSM
ITTA
L C
onfir
mat
ion
of e
ligib
ility
is n
ot a
gua
rant
ee o
f pay
men
t.
Confi
dent
ialit
y no
tice:
Thi
s fa
x is
inte
nded
for t
he s
ole
use
of th
e in
divi
dual
and
ent
ity to
who
m it
is a
ddre
ssed
and
may
con
tain
info
rmat
ion
that
is c
onfid
entia
l and
exe
mpt
from
dis
clos
ure
unde
r ap
plic
able
law
. If y
ou a
re n
ot th
e in
tend
ed a
ddre
ssee
nor
aut
horiz
ed to
rece
ive
this
fax
for t
he in
tend
ed a
ddre
ssee
, you
are
her
eby
notifi
ed th
at y
ou m
ay n
ot u
se, c
opy,
dis
clos
e or
dis
trib
ute
to a
nyon
e th
e m
essa
ge o
r any
info
rmat
ion
cont
aine
d in
the
mes
sage
to a
nyon
e. If
you
hav
e re
ceiv
ed th
is fa
x in
err
or, p
leas
e im
med
iate
ly a
dvis
e th
e se
nder
at t
he p
hone
num
ber l
iste
d at
the
top
of th
e pa
ge a
nd
shre
d th
e fa
x. T
hank
you
ver
y m
uch.
©
2012
Pas
spor
t Hea
lth P
lan
RR-1
2118
To:
EPSD
T Te
amFr
om:
Fax:
1-80
0-49
2-28
54Pa
ge(s
):
Phon
e:50
2-58
5-82
10D
ate:
Re:
EPSD
T El
igib
ility
Con
firm
atio
nCC
:
Pass
port
Hea
lth P
lan
Mem
ber I
.D. #
Nam
eD
.O.B
.D
.O.S
.
1. 2. 3. 4. 5. 6. 7. 8. 9. 10.
Pass
port
Use
Onl
yEl
igib
ility
Day
s fo
r thi
s Sc
reen
Yes
No
Reas
on

11
EPSDT Medical Record Review RequirementsTo ensure all EPSDT components are being performed, services must be documented in the members’ chart .
Key areas of focus are:• History & physical exam
- Height & weight - Weight to length percentile up to 24 months, then the BMI percentile is calculated on the growth chart .
• BMI (Value & percentile must be plotted for members under the age of 20)
• Hearing Screening ages 4yrs-6yrs/8yrs/10yrs/ once between 11-14 years, once between 15-17 years, once between18-21 years
• Vision screening 3yr-6yr/ 8yr/10yr/12 yr/ 15yr
• Labs including lead screen at 12 and 24 months of age
• Behavioral/psychosocial assessment ages newborn to 21 years .
• Depression screen ages 12 years to 21 years .
• Anticipatory guidance
• Dental referral / dental home established
• Up-to-date immunization record and/or current immunization certification
These items are based on Passport’s/AAP’s periodicity schedule EPSDT Expanded Services
EPSDT Expanded ServicesEPSDT Expanded Services are those services required to treat conditions detected during an encounter with a health care professional and eligible for payment under the Federal Medicaid program but not currently recognized under the State plan . All Passport members under age 21 are also eligible for EPSDT Expanded Services when such services are determined to be medically necessary . Authorization is required through the Utilization Management Department to determine medical necessity and length of approval . Approval may be granted as long as the conditions for medical necessity continue to be met and the member remains eligible for Passport benefits.
Prior Authorization Process for EPSDT Expanded Services
Providers must forward all requests for EPSDT Expanded Services to the Passport Utilization Manage-ment (UM) department for medical necessity review .
Providers must also attach a letter of medical necessity outlining the rationale for the request and the benefit that requested service(s) will yield for the member. Although Utilization Management will accept letters of medical necessity from either a member’s PCP, a participating specialist or ancillary provider, the PCP will be asked to approve the treatment plan if he/she was not involved in the initial request to ensure continuity of care .
EPSDT Expanded / Special Services:1. EPSDT Expanded / Special Services are available only to individuals under age 21. Services may be provided through the last day of the month in which the individual turns 21. For example, if some-one is receiving services through the EPSDT Special Services Program, and their 21st birthday is March 16, they may continue to receive services through EPSDT Special Services through March 31 (if they are still eligible for Medicaid .)

12
EPSDT ScreeningsEPSDT Screenings include these areas of health in which the PCP must check for members ages birth to 21 years:
• Medical history and physical exams • Dental screens• Vision screens • Lab tests including blood lead level • Hearing screens • Immunizations (shots)• Nutrition • Growth and development check: (social, personal, • Mental health / depression screening, language and motor skills) tobacco / alcohol / substance use and abuse • Body Mass Index (BMI) assessments, and other age appropriate counseling
Members should have an EPSDT Screening at the following ages:
Infancy Early Childhood Middle Childhood AdolescenceBirth to 1 month 15 months 5 years 11 years
2 months 18 months 6 years 12 years4 months 24 months 7 years 13 years6 months 30 months 8 years 14 years9 months 3 years 9 years 15 years12 months 4 years 10 years 16 years
17 years18 years19 years20 years
2 . EPSDT Special Services does not cover:
a. Respite care, environmental, educational, vocational, cosmetic, convenience, experimental, or over the counter items .
3. Examples of a service covered under EPSDT:
a. Additional pairs of eyeglasses after the Medicaid Vision Program has paid for the first two pair in a year .
b . Additional dental cleanings after the Medicaid Dental Program has paid for two cleanings .
c . Nutritional products when they are used as a supplement rather than as the child’s total nutrition .
d . Speech therapy, occupational therapy or physical therapy when the therapy does not meet the criteria for the Medicaid Home Health Program .
e . Private Duty Nursing beyond the 2,000 hour per year limit .
4 . All EPSDT Special Services require a review for medical necessity by the appropriate entity (i .e ., Superior for vision services) .
5 . If a service is covered under the State Plan the service would not be considered EPSDT special ser-vices, but would fall under the member’s regular Passport coverage .

A-1
Rec
omm
end
ed Im
mun
izat
ion
Sch
edul
e fo
r C
hild
ren
an
d A
dol
esce
nts
Ag
ed 1
8 Ye
ars
or Y
oun
ger
, UN
ITED
STA
TES,
201
8
Ap
pro
ved
by
the
Ad
vis
ory
Co
mm
itte
e o
n Im
mu
niz
atio
n P
ract
ice
s (w
ww
.cd
c.g
ov
/va
ccin
es/
aci
p)
Am
eri
can
Aca
de
my
of
Pe
dia
tric
s (w
ww
.aa
p.o
rg)
Am
eri
can
Aca
de
my
of
Fam
ily
Ph
ysic
ian
s (w
ww
.aa
fp.o
rg)
Am
eri
can
Co
lle
ge
of
Ob
ste
tric
ian
s a
nd
Gy
ne
colo
gis
ts(w
ww
.aco
g.o
rg)
• Co
nsul
t rel
evan
t AC
IP s
tate
men
ts fo
r det
aile
d re
com
men
datio
ns
(ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/in
dex.
htm
l).•
Whe
n a
vacc
ine
is n
ot a
dmin
iste
red
at th
e re
com
men
ded
age,
ad
min
iste
r at a
sub
sequ
ent v
isit.
• U
se c
ombi
natio
n va
ccin
es in
stea
d of
sep
arat
e in
ject
ions
whe
n ap
prop
riate
.•
Repo
rt c
linic
ally
sig
nific
ant a
dver
se e
vent
s to
the
Vacc
ine
Adv
erse
Ev
ent R
epor
ting
Syst
em (V
AER
S) o
nlin
e (w
ww
.vae
rs.h
hs.g
ov) o
r by
tele
phon
e (8
00-8
22-7
967)
. •
Repo
rt s
uspe
cted
cas
es o
f rep
orta
ble
vacc
ine-
prev
enta
ble
dise
ases
to
you
r sta
te o
r loc
al h
ealth
dep
artm
ent.
• Fo
r inf
orm
atio
n ab
out p
reca
utio
ns a
nd c
ontr
aind
icat
ions
, see
ww
w.
cdc.
gov/
vacc
ines
/hcp
/aci
p-r
ecs/
gene
ral-r
ecs/
cont
rain
dica
tions
.htm
l.
U.S
. Dep
artm
ent o
f Hea
lth
and
Hum
an S
ervi
ces
Cen
ters
for D
isea
se C
ontr
ol a
nd P
reve
ntio
n
Vac
cin
e ty
pe
Ab
bre
viat
ion
Bra
nd
(s)
Dip
hthe
ria, t
etan
us, a
nd a
cellu
lar p
ertu
ssis
vac
cine
DTa
PD
apta
cel
Infa
nrix
Dip
hthe
ria, t
etan
us v
acci
neD
TN
o Tr
ade
Nam
e
Hae
mop
hilu
s infl
uenz
ae ty
pe
B va
ccin
eH
ib (P
RP-T
)
Hib
(PRP
-OM
P)
Act
HIB
Hib
erix
Pedv
axH
IB
Hep
atiti
s A
vac
cine
Hep
AH
avrix
Vaqt
a
Hep
atiti
s B
vacc
ine
Hep
BEn
gerix
-BRe
com
biv
ax H
B
Hum
an p
apill
omav
irus
vacc
ine
HPV
Gar
dasi
l 9
Influ
enza
vac
cine
(ina
ctiv
ated
)IIV
Mul
tiple
Mea
sles
, mum
ps,
and
rub
ella
vac
cine
MM
RM
-M-R
II
Men
ingo
cocc
al s
erog
roup
s A
, C, W
, Y v
acci
neM
enA
CW
Y-D
Men
AC
WY-
CRM
Men
actr
aM
enve
o
Men
ingo
cocc
al s
erog
roup
B v
acci
neM
enB-
4CM
enB-
FHb
pBe
xser
oTr
umen
ba
Pneu
moc
occa
l 13-
vale
nt c
onju
gate
vac
cine
PCV1
3Pr
evna
r 13
Pneu
moc
occa
l 23-
vale
nt p
olys
acch
arid
e va
ccin
ePP
SV23
Pneu
mov
ax
Polio
viru
s va
ccin
e (in
activ
ated
)IP
VIP
OL
Rota
viru
s va
ccin
esRV
1RV
5Ro
tarix
Rota
Teq
Teta
nus,
dip
hthe
ria, a
nd a
cellu
lar p
ertu
ssis
vac
cine
Tdap
Ada
cel
Boos
trix
Teta
nus
and
dip
hthe
ria v
acci
neTd
Teni
vac
No
Trad
e N
ame
Varic
ella
vac
cine
VAR
Variv
ax
Co
mb
inat
ion
Vac
cin
es
DTa
P, h
epat
itis
B an
d in
activ
ated
pol
iovi
rus
vacc
ine
DTa
P-H
epB-
IPV
Pedi
arix
DTa
P, in
activ
ated
pol
iovi
rus
and
Hae
mop
hilu
s infl
uenz
ae
typ
e B
vacc
ine
DTa
P-IP
V/H
ibPe
ntac
el
DTa
P an
d in
activ
ated
pol
iovi
rus
vacc
ine
DTa
P-IP
VKi
nrix
Qua
drac
el
Mea
sles
, mum
ps,
rub
ella
, and
var
icel
la v
acci
nes
MM
RVPr
oQua
d
This
sch
edul
e in
clud
es re
com
men
datio
ns in
eff
ect a
s of
Jan
uary
1, 2
018.
The
tab
le b
elow
sho
ws
vacc
ine
acro
nym
s, a
nd b
rand
nam
es fo
r vac
cine
s ro
utin
ely
reco
mm
end-
ed fo
r chi
ldre
n an
d ad
oles
cent
s. T
he u
se o
f tra
de n
ames
in th
is im
mun
izat
ion
sche
dule
is fo
r id
entifi
catio
n p
urp
oses
onl
y an
d do
es n
ot im
ply
end
orse
men
t by
the
AC
IP o
r CD
C.

A-2
Figu
re 1
. Rec
omm
end
ed Im
mun
izat
ion
Sche
dul
e fo
r Chi
ldre
n an
d A
dol
esce
nts
Age
d 1
8 Ye
ars
or Y
oung
er—
Uni
ted
Sta
tes,
201
8.
(FO
R T
HO
SE W
HO
FA
LL B
EHIN
D O
R S
TAR
T LA
TE, S
EE T
HE
CAT
CH
-UP
SCH
EDU
LE [F
IGU
RE
2]).
Thes
e re
com
men
datio
ns m
ust b
e re
ad w
ith th
e fo
otno
tes
that
follo
w. F
or th
ose
who
fall
behi
nd o
r sta
rt la
te, p
rovi
de c
atch
-up
vacc
inat
ion
at th
e ea
rlies
t opp
ortu
nity
as
indi
cate
d by
the
gree
n ba
rs in
Fig
ure
1.
To d
eter
min
e m
inim
um in
terv
als
betw
een
dose
s, s
ee th
e ca
tch-
up s
ched
ule
(Fig
ure
2). S
choo
l ent
ry a
nd a
dole
scen
t vac
cine
age
gro
ups
are
shad
ed in
gra
y.
NO
TE: T
he a
bov
e re
com
men
dat
ions
mus
t be
read
alo
ng w
ith
the
foot
note
s of
this
sch
edul
e.
Vacc
ine
Birt
h1
mo
2 m
os4
mos
6 m
os9
mos
12 m
os15
mos
18 m
os19
-23
mos
2-3
yrs
4-6
yrs
7-10
yrs
11-1
2 yr
s13
-15
yrs
16 y
rs17
-18
yrs
Hep
atiti
s B1 (
Hep
B)
Rota
viru
s2 (RV
) RV1
(2-d
ose
serie
s); R
V5 (3
-dos
e se
ries)
Dip
hthe
ria, t
etan
us, &
ace
llula
r pe
rtus
sis3 (
DTa
P: <
7 yr
s)
Hae
mop
hilu
s infl
uenz
ae ty
pe b
4
(Hib
)
Pneu
moc
occa
l con
juga
te5
(PC
V13)
Inac
tivat
ed p
olio
viru
s6 (IP
V: <
18 y
rs)
Influ
enza
7 (IIV
)
Mea
sles
, mum
ps, r
ubel
la8 (
MM
R)
Varic
ella
9 (V
AR)
Hep
atiti
s A
10 (H
epA
)
Men
ingo
cocc
al11
(Men
AC
WY-
D
>9
mos
; Men
AC
WY-
CRM
≥2
mos
)
Teta
nus,
diph
ther
ia, &
ace
llula
r pe
rtus
sis13
(Tda
p: >
7 yr
s)
Hum
an p
apill
omav
irus14
(HPV
)
Men
ingo
cocc
al B
12
Pneu
moc
occa
l pol
ysac
char
ide5
(PPS
V23)
2nd d
ose
1st do
seSe
e fo
otno
te 1
1
See
foot
note
14
Ann
ual v
acci
natio
n (II
V) 1
or 2
dos
es
See
foot
note
5
Tdap
See
foot
note
22nd
dos
e1st
dose
4th d
ose
3rd d
ose
2nd d
ose
1st do
se
2-do
se s
erie
s, S
ee fo
otno
te 1
0
4th d
ose
3rd d
ose
2nd do
se1st
dose
2nd do
se1st
dose
3rd o
r 4th
dos
e,
See
foot
note
4Se
e fo
otno
te 4
2nd do
se1st
dose
2nd do
se1st
dose
5th d
ose
4th d
ose
3rd d
ose
2nd d
ose
1st do
se
3rd d
ose
2nd d
ose
1st do
se
Ann
ual v
acci
natio
n (II
V)
1 do
se o
nly
See
foot
note
8
See
foot
note
12
No
reco
mm
enda
tion
Rang
e of
reco
mm
ende
d ag
es
for c
erta
in h
igh-
risk
gro
ups
Rang
e of
reco
mm
ende
d ag
es fo
r all
child
ren
Rang
e of
reco
mm
ende
d ag
es
for c
atch
-up
imm
uniz
atio
nRa
nge
of re
com
men
ded
ages
for n
on-h
igh-
risk
grou
ps
that
may
rece
ive
vacc
ine,
sub
ject
to
indi
vidu
al c
linic
al d
ecis
ion
mak
ing

A-3
FIG
UR
E 2.
Cat
ch-u
p im
mun
izat
ion
sche
dul
e fo
r per
sons
age
d 4
mon
ths–
18 y
ears
who
sta
rt la
te o
r who
are
mor
e th
an 1
mon
th b
ehin
d—
Uni
ted
Sta
tes,
201
8.Th
e fig
ure
belo
w p
rovi
des
catc
h-up
sch
edul
es a
nd m
inim
um in
terv
als
betw
een
dose
s fo
r chi
ldre
n w
hose
vac
cina
tions
hav
e be
en d
elay
ed. A
vac
cine
ser
ies
does
not
nee
d to
be
rest
arte
d, re
gard
less
of t
he ti
me
that
has
ela
psed
bet
wee
n do
ses.
Use
the
sect
ion
appr
opria
te fo
r the
chi
ld’s
age.
Alw
ays
use
this
tabl
e in
con
junc
tion
with
Fig
ure
1 an
d th
e fo
otno
tes
that
follo
w.
Ch
ildre
n a
ge
4 m
on
ths
thro
ug
h 6
yea
rs
Vacc
ine
Min
imum
A
ge fo
r D
ose
1
Min
imum
Inte
rval
Bet
wee
n D
oses
Dos
e 1
to D
ose
2D
ose
2 to
Dos
e 3
Dos
e 3
to D
ose
4D
ose
4 to
Dos
e 5
Hep
atiti
s B1
Birt
h4
wee
ks8
wee
ks a
nd a
t lea
st 1
6 w
eeks
aft
er fi
rst d
ose.
M
inim
um a
ge fo
r the
fina
l dos
e is
24
wee
ks.
Rota
viru
s2
6 w
eeks
Max
imum
age
fo
r firs
t dos
e is
14
wee
ks, 6
day
s
4 w
eeks
4 w
eeks
2
Max
imum
age
for fi
nal d
ose
is 8
mon
ths,
0 da
ys.
Dip
hthe
ria, t
etan
us, a
nd
acel
lula
r per
tuss
is3
6 w
eeks
4 w
eeks
4 w
eeks
6 m
onth
s6
mon
ths3
Hae
mop
hilu
s infl
uenz
ae
typ
e b
46
wee
ks
4 w
eeks
if
first
dos
e w
as a
dmin
iste
red
bef
ore
the
1st b
irth
day.
8 w
eeks
(as
final
dos
e)
if fir
st d
ose
was
adm
inis
tere
d at
age
12
thro
ugh
14 m
onth
s.
No
furt
her d
oses
nee
ded
if fir
st
dose
was
adm
inis
tere
d at
age
15
mon
ths
or o
lder
.
4 w
eeks
4 if
curr
ent a
ge is
you
nger
than
12
mon
ths
and
firs
t dos
e w
as a
dmin
iste
red
at y
oung
er th
an a
ge 7
mon
ths,
an
d a
t lea
st 1
pre
viou
s do
se w
as P
RP-T
(Act
Hib
, Pen
tace
l, H
iber
ix) o
r unk
now
n.
8 w
eeks
and
age
12
thro
ugh
59 m
onth
s (a
s fin
al d
ose)
4
• if
curr
ent a
ge is
you
nger
than
12
mon
ths
and
firs
t dos
e w
as a
dmin
iste
red
at a
ge 7
thro
ugh
11
mon
ths;
O
R•
if cu
rren
t age
is 1
2 th
roug
h 59
mon
ths
and
firs
t dos
e w
as a
dmin
iste
red
bef
ore
the
1st b
irth
day,
an
d
seco
nd d
ose
adm
inis
tere
d at
you
nger
than
15
mon
ths;
O
R•
if b
oth
dose
s w
ere
PRP-
OM
P (P
edva
xHIB
; Com
vax)
an
d w
ere
adm
inis
tere
d b
efor
e th
e 1st
bir
thda
y.
No
furt
her d
oses
nee
ded
if p
revi
ous
dose
was
adm
inis
tere
d at
age
15
mon
ths
or o
lder
.
8 w
eeks
(as
final
dos
e)
This
dos
e on
ly n
eces
sary
for c
hil-
dren
age
12
thro
ugh
59 m
onth
s w
ho re
ceiv
ed 3
dos
es b
efor
e th
e 1st
b
irth
day.
Pneu
moc
occa
l co
njug
ate5
6 w
eeks
4 w
eeks
if
first
dos
e ad
min
iste
red
bef
ore
the
1st b
irth
day.
8 w
eeks
(as
final
dos
e fo
r hea
lthy
ch
ildre
n)if
first
dos
e w
as a
dmin
iste
red
at th
e 1st
bir
thda
y or
aft
er.
No
furt
her d
oses
nee
ded
for h
ealt
hy c
hild
ren
if fir
st d
ose
was
ad
min
iste
red
at a
ge 2
4 m
onth
s or
ol
der.
4 w
eeks
if
curr
ent a
ge is
you
nger
than
12
mon
ths
and
prev
ious
dos
e gi
ven
at <
7 m
onth
s ol
d.
8 w
eeks
(as
final
dos
e fo
r hea
lthy
chi
ldre
n)
if p
revi
ous
dose
giv
en b
etw
een
7-11
mon
ths
(wai
t unt
il at
leas
t 12
mon
ths
old)
; O
Rif
curr
ent a
ge is
12
mon
ths
or o
lder
and
at l
east
1 d
ose
was
giv
en b
efor
e ag
e 12
mon
ths.
No
furt
her d
oses
nee
ded
for h
ealt
hy c
hild
ren
if p
revi
ous
dose
adm
inis
tere
d at
age
24
mon
ths
or o
lder
.
8 w
eeks
(as
final
dos
e)
This
dos
e on
ly n
eces
sary
for c
hil-
dren
age
d 12
thro
ugh
59 m
onth
s w
ho re
ceiv
ed 3
dos
es b
efor
e ag
e 12
m
onth
s or
for c
hild
ren
at h
igh
risk
who
rece
ived
3 d
oses
at a
ny a
ge.
Inac
tivat
ed p
olio
viru
s66
wee
ks4
wee
ks6
4 w
eeks
6 if cu
rren
t age
is <
4 y
ears
6 m
onth
s (a
s fin
al d
ose)
if c
urre
nt a
ge is
4 y
ears
or o
lder
6 m
onth
s6 (min
imum
age
4 y
ears
for
final
dos
e).
Mea
sles
, mum
ps,
rub
ella
812
mon
ths
4 w
eeks
Varic
ella
912
mon
ths
3 m
onth
sH
epat
itis
A10
12 m
onth
s6
mon
ths
Men
ingo
cocc
al11
(Men
AC
WY-
D ≥
9 m
os;
Men
AC
WY-
CRM
≥2
mos
)6
wee
ks8
wee
ks11
See
foot
note
11
See
foot
note
11
Ch
ildre
n a
nd
ad
ole
scen
ts a
ge
7 th
rou
gh
18
year
sM
enin
goco
ccal
11
(Men
AC
WY-
D ≥
9 m
os;
Men
AC
WY-
CRM
≥2
mos
)
Not
Ap
plic
able
(N
/A)
8 w
eeks
11
Teta
nus,
dip
hthe
ria;
teta
nus,
dip
hthe
ria, a
nd
acel
lula
r per
tuss
is13
7 ye
ars13
4 w
eeks
4 w
eeks
if
first
dos
e of
DTa
P/D
T w
as a
dmin
iste
red
befo
re th
e 1st
birt
hday
. 6
mon
ths
(as
final
dos
e)
if fir
st d
ose
of D
TaP/
DT
or T
dap
/Td
was
adm
inis
tere
d at
or a
fter
the
1st b
irth
day.
6 m
onth
s if
first
dos
e of
DTa
P/D
T
was
adm
inis
tere
d b
efor
e th
e 1st
b
irth
day.
Hum
an p
apill
omav
irus14
9 ye
ars
Rout
ine
dosi
ng in
terv
als
are
reco
mm
ende
d.14
Hep
atiti
s A
10N
/A6
mon
ths
Hep
atiti
s B1
N/A
4 w
eeks
8 w
eeks
an
d a
t lea
st 1
6 w
eeks
aft
er fi
rst d
ose.
Inac
tivat
ed p
olio
viru
s6N
/A4
wee
ks6
mon
ths6
A fo
urth
dos
e is
not
nec
essa
ry if
the
third
dos
e w
as a
dmin
iste
red
at a
ge 4
yea
rs o
r old
er a
nd a
t lea
st 6
mon
ths
afte
r the
pre
viou
s do
se.
A fo
urth
dos
e of
IPV
is in
dica
ted
if al
l pr
evio
us d
oses
wer
e ad
min
iste
red
at <
4 ye
ars
or if
the
third
dos
e w
as
adm
inis
tere
d <
6 m
onth
s af
ter t
he
seco
nd d
ose.
Mea
sles
, mum
ps,
rub
ella
8N
/A4
wee
ks
Varic
ella
9N
/A3
mon
ths
if yo
unge
r tha
n ag
e 13
ye
ars.
4
wee
ks if
age
13
year
s or
old
er.
NO
TE: T
he a
bov
e re
com
men
dat
ions
mus
t be
read
alo
ng w
ith
the
foot
note
s of
this
sch
edul
e.

A-4
VACC
INE
INDI
CATI
ON
Preg
nanc
y
Imm
unoc
ompr
omise
d st
atus
(exc
ludi
ng H
IV
infe
ctio
n)
HIV
infe
ctio
nCD
4+ co
unt†
Kidn
ey fa
ilure
, end
-st
age
rena
l dise
ase,
on
hem
odia
lysis
Hear
t dise
ase,
chro
nic l
ung
dise
ase
CSF
leak
s/
coch
lear
im
plan
ts
Aspl
enia
and
per
siste
nt
com
plem
ent c
ompo
nent
defic
ienc
ies
Chro
nic
liver
di
seas
eDi
abet
es
<15%
or
tota
l CD4
ce
ll cou
nt of
<2
00/m
m3
≥15%
or
tota
l CD4
ce
ll cou
nt of
≥2
00/m
m3
Hep
atit
is B
1
Rota
viru
s2
Dip
hthe
ria, t
etan
us, &
ace
llula
r per
tuss
is3
(DTa
P)
Hae
mop
hilu
s infl
uenz
ae ty
pe b
4
Pneu
moc
occa
l con
juga
te5
Inac
tivat
ed p
olio
viru
s6
Influ
enza
7
Mea
sles
, mum
ps, r
ubel
la8
Varic
ella
9
Hep
atiti
s A
10
Men
ingo
cocc
al A
CW
Y11
Teta
nus,
diph
ther
ia, &
ace
llula
r per
tuss
is13
(Tda
p)
Hum
an p
apill
omav
irus14
Men
ingo
cocc
al B
12
Pneu
moc
occa
l pol
ysac
char
ide5
Fig
ure
3. V
acci
nes
that
mig
ht b
e in
dic
ated
for
child
ren
an
d a
do
lesc
ents
ag
ed 1
8 ye
ars
or
you
ng
er b
ased
on
med
ical
ind
icat
ion
s
SCID
*
*Sev
ere
Com
bin
ed Im
mun
odefi
cien
cy† Fo
r add
ition
al in
form
atio
n re
gard
ing
HIV
lab
orat
ory
par
amet
ers
and
use
of li
ve v
acci
nes;
see
the
Gen
eral
Bes
t Pra
ctic
e G
uide
lines
for I
mm
uniz
atio
n “A
ltere
d Im
mun
ocom
pet
ence
” at:
ww
w.c
dc.g
ov/v
acci
nes/
hcp
/aci
p-r
ecs/
gene
r-al
-rec
s/im
mun
ocom
pet
ence
.htm
l; an
d Ta
ble
4-1
(foo
tnot
e D
) at:
ww
w.c
dc.g
ov/v
acci
nes/
hcp
/aci
p-r
ecs/
gene
ral-r
ecs/
cont
rain
dica
tions
.htm
l.
Vacc
inat
ion
acco
rdin
g to
the
rout
ine
sche
dule
reco
mm
ende
d
Reco
mm
ende
d fo
r per
sons
with
an
add
ition
al ri
sk fa
ctor
for w
hich
th
e va
ccin
e w
ould
be
indi
cate
d
Vacc
inat
ion
is re
com
men
ded,
an
d ad
ditio
nal d
oses
may
be
nece
ssar
y b
ased
on
med
ical
co
nditi
on. S
ee fo
otno
tes.
No
reco
mm
enda
tion
Con
trai
ndic
ated
Prec
autio
n fo
r vac
cina
tion
NO
TE: T
he a
bov
e re
com
men
dat
ions
mus
t be
read
alo
ng w
ith
the
foot
note
s of
this
sch
edul
e.

A-5
Foot
note
s — R
ecom
men
ded
Imm
uniz
atio
n Sc
hedu
le fo
r Chi
ldre
n an
d A
dole
scen
ts A
ged
18 Y
ears
or Y
oung
er, U
NIT
ED S
TATE
S, 2
018
For f
urth
er g
uida
nce
on th
e us
e of
the
vacc
ines
men
tione
d b
elow
, see
: ww
w.c
dc.g
ov/v
acci
nes/
hcp
/aci
p-r
ecs/
inde
x.ht
ml.
Fo
r vac
cine
reco
mm
enda
tions
for p
erso
ns 1
9 ye
ars
of a
ge a
nd o
lder
, see
the
Adu
lt Im
mun
izat
ion
Sche
dule
.
Ad
dit
ion
al in
form
atio
n•
For i
nfor
mat
ion
on c
ontr
aind
icat
ions
and
pre
caut
ions
for t
he u
se o
f a v
acci
ne, c
onsu
lt th
e G
ener
al B
est P
ract
ice
Gui
delin
es fo
r Im
mun
izat
ion
and
rele
vant
AC
IP
stat
emen
ts, a
t ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/in
dex.
htm
l. •
For c
alcu
latin
g in
terv
als
betw
een
dose
s, 4
wee
ks =
28
days
. Int
erva
ls o
f >4
mon
ths
are
dete
rmin
ed b
y ca
lend
ar m
onth
s.•
With
in a
num
ber r
ange
(e.g
., 12
–18)
, a d
ash
(–) s
houl
d be
read
as “
thro
ugh.
”•
Vacc
ine
dose
s ad
min
iste
red
≤4
days
bef
ore
the
min
imum
age
or i
nter
val a
re c
onsi
dere
d va
lid. D
oses
of a
ny v
acci
ne a
dmin
iste
red
≥5
days
ear
lier t
han
the
min
imum
in
terv
al o
r min
imum
age
sho
uld
not b
e co
unte
d as
val
id a
nd s
houl
d be
repe
ated
as
age-
appr
opria
te. T
he re
peat
dos
e sh
ould
be
spac
ed a
fter
the
inva
lid d
ose
by
the
reco
mm
ende
d m
inim
um in
terv
al. F
or fu
rthe
r det
ails
, see
Tab
le 3
-1, R
ecom
men
ded
and
min
imum
age
s and
inte
rval
s bet
wee
n va
ccin
e do
ses,
in G
ener
al B
est P
ract
ice
Gui
delin
es fo
r Im
mun
izat
ion
at w
ww
.cdc
.gov
/vac
cine
s/hc
p/ac
ip-r
ecs/
gene
ral-r
ecs/
timin
g.ht
ml.
• In
form
atio
n on
trav
el v
acci
ne re
quire
men
ts a
nd re
com
men
datio
ns is
ava
ilabl
e at
ww
wnc
.cdc
.gov
/tra
vel/.
• Fo
r vac
cina
tion
of p
erso
ns w
ith im
mun
odefi
cien
cies
, see
Tab
le 8
-1, V
acci
natio
n of
per
sons
with
prim
ary
and
seco
ndar
y im
mun
odefi
cien
cies
, in
Gen
eral
Bes
t Pra
ctic
e G
uide
lines
for I
mm
uniz
atio
n, a
t ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/ge
nera
l-rec
s/im
mun
ocom
pete
nce.
htm
l; an
d Im
mun
izat
ion
in S
peci
al C
linic
al C
ircum
stan
ces.
(In:
Ki
mbe
rlin
DW
, Bra
dy M
T, Ja
ckso
n M
A, L
ong
SS, e
ds. R
ed B
ook:
201
5 re
port
of t
he C
omm
ittee
on
Infe
ctio
us D
isea
ses.
30th
ed.
Elk
Gro
ve V
illag
e, IL
: Am
eric
an A
cade
my
of
Pedi
atric
s, 2
015:
68-1
07).
• Th
e N
atio
nal V
acci
ne In
jury
Com
pens
atio
n Pr
ogra
m (V
ICP)
is a
no-
faul
t alte
rnat
ive
to th
e tr
aditi
onal
lega
l sys
tem
for r
esol
ving
vac
cine
inju
ry c
laim
s. A
ll ro
utin
e ch
ild a
nd
adol
esce
nt v
acci
nes
are
cove
red
by V
ICP
exce
pt fo
r pne
umoc
occa
l pol
ysac
char
ide
vacc
ine
(PPS
V23)
. For
mor
e in
form
atio
n; s
ee w
ww
.hrs
a.go
v/va
ccin
ecom
pens
atio
n/in
dex.
htm
l.
1.
Hep
atit
is B
(Hep
B) v
acci
ne.
(min
imu
m a
ge:
bir
th)
Bir
th D
ose
(Mo
nov
alen
t Hep
B v
acci
ne
on
ly):
• M
oth
er is
HB
sAg
-Neg
ativ
e: 1
dos
e w
ithin
24
hour
s of
bir
th fo
r med
ical
ly s
tab
le in
fant
s >
2,00
0 gr
ams.
Infa
nts
<2,
000
gram
s ad
min
iste
r 1 d
ose
at
chro
nolo
gica
l age
1 m
onth
or h
osp
ital d
isch
arge
.•
Mo
ther
is H
BsA
g-P
osi
tive
: ɱG
ive
Hep
B v
acci
ne
and
0.5
mL
of H
BIG
(at
sep
arat
e an
atom
ic s
ites)
with
in 1
2 ho
urs
of
bir
th, r
egar
dles
s of
bir
th w
eigh
t. ɱTe
st fo
r HBs
Ag
and
anti-
HBs
at a
ge 9
–12
mon
ths.
If H
epB
serie
s is
del
ayed
, tes
t 1–2
m
onth
s af
ter fi
nal d
ose.
• M
oth
er’s
HB
sAg
sta
tus
is u
nkn
own
: ɱG
ive
Hep
B v
acci
ne
with
in 1
2 ho
urs
of b
irth
, re
gard
less
of b
irth
wei
ght.
ɱFo
r inf
ants
<2,
000
gram
s, g
ive
0.5
mL
of H
BIG
in
add
ition
to H
epB
vacc
ine
with
in 1
2 ho
urs
of
bir
th.
ɱD
eter
min
e m
othe
r’s H
BsA
g st
atus
as
soon
as
pos
sib
le. I
f mot
her i
s H
BsA
g-p
ositi
ve, g
ive
0.5
mL
of H
BIG
to in
fant
s >
2,00
0 gr
ams
as s
oon
as
pos
sib
le, b
ut n
o la
ter t
han
7 da
ys o
f age
.
Ro
uti
ne
Seri
es:
• A
com
ple
te s
erie
s is
3 d
oses
at 0
, 1–2
, and
6–1
8 m
onth
s. (M
onov
alen
t Hep
B va
ccin
e sh
ould
be
used
for d
oses
giv
en b
efor
e ag
e 6
wee
ks.)
• In
fant
s w
ho d
id n
ot re
ceiv
e a
bir
th d
ose
shou
ld
beg
in th
e se
ries
as s
oon
as fe
asib
le (s
ee F
igur
e 2)
.•
Adm
inis
trat
ion
of 4
do
ses
is p
erm
itted
whe
n a
com
bin
atio
n va
ccin
e co
ntai
ning
Hep
B is
use
d af
ter
the
bir
th d
ose.
• M
inim
um
ag
e fo
r the
fina
l (3r
d or
4th
) dos
e: 2
4 w
eeks
. •
Min
imu
m In
terv
als:
Dos
e 1
to D
ose
2: 4
wee
ks /
Dos
e 2
to D
ose
3: 8
wee
ks /
Dos
e 1
to D
ose
3: 1
6 w
eeks
. (W
hen
4 do
ses
are
give
n, s
ubst
itute
“Dos
e 4”
for “
Dos
e 3”
in th
ese
calc
ulat
ions
.)C
atch
-up
vac
cin
atio
n:
• U
nvac
cina
ted
per
sons
sho
uld
com
ple
te a
3-d
ose
serie
s at
0, 1
–2, a
nd 6
mon
ths.
• A
dole
scen
ts 1
1–15
yea
rs o
f age
may
use
an
alte
rnat
ive
2-do
se s
ched
ule,
with
at l
east
4 m
onth
s b
etw
een
dose
s (a
dult
form
ulat
ion
Rec
om
biv
ax
HB
onl
y).
• Fo
r oth
er c
atch
-up
gui
danc
e, s
ee F
igur
e 2.
2.
Ro
tavi
rus
vacc
ines
. (m
inim
um
ag
e: 6
wee
ks)
Ro
uti
ne
vacc
inat
ion
:
Ro
tari
x: 2
-dos
e se
ries
at 2
and
4 m
onth
s.
Ro
taTe
q: 3
-dos
e se
ries
at 2
, 4, a
nd 6
mon
ths.
If an
y do
se in
the
serie
s is
eith
er R
otaT
eq o
r un
know
n, d
efau
lt to
3-d
ose
serie
s.
Cat
ch-u
p v
acci
nat
ion
:•
Do
not s
tart
the
serie
s on
or a
fter
age
15
wee
ks, 0
da
ys.
• Th
e m
axim
um a
ge fo
r the
fina
l dos
e is
8 m
onth
s, 0
da
ys.
• Fo
r oth
er c
atch
-up
gui
danc
e, s
ee F
igur
e 2.
3.
Dip
hth
eria
, tet
anu
s, a
nd
ace
llula
r per
tuss
is (D
TaP)
va
ccin
e. (m
inim
um
ag
e: 6
wee
ks [4
yea
rs fo
r K
inri
x o
r Q
uad
race
l])
Ro
uti
ne
vacc
inat
ion
:•
5-do
se s
erie
s at
2, 4
, 6, a
nd 1
5–18
mon
ths,
and
4–6
ye
ars.
ɱPr
osp
ecti
vely
: A 4
th d
ose
may
be
give
n as
ea
rly
as a
ge 1
2 m
onth
s if
at le
ast 6
mon
ths
have
ela
pse
d si
nce
the
3rd
dose
. ɱR
etro
spec
tive
ly: A
4th
dos
e th
at w
as
inad
vert
entl
y gi
ven
as e
arly
as
12 m
onth
s m
ay
be
coun
ted
if at
leas
t 4 m
onth
s ha
ve e
lap
sed
sinc
e th
e 3r
d do
se.
Cat
ch-u
p v
acci
nat
ion
:•
The
5th
dose
is n
ot n
eces
sary
if th
e 4t
h do
se w
as
adm
inis
tere
d at
4 y
ears
or o
lder
.•
For o
ther
cat
ch-u
p g
uida
nce,
see
Fig
ure
2.

A-6
4.
Hae
mop
hilu
s in
fluen
zae
typ
e b
(Hib
) vac
cin
e.
(min
imum
ag
e: 6
wee
ks)
Rou
tin
e va
ccin
atio
n:
• A
ctH
IB, H
iber
ix, o
r Pen
tace
l: 4-
dose
ser
ies
at 2
, 4,
6, a
nd 1
2–15
mon
ths.
• Pe
dva
xHIB
: 3-d
ose
serie
s at
2, 4
, and
12–
15 m
onth
s.C
atch
-up
vac
cin
atio
n:
• 1s
t dos
e at
7–1
1 m
onth
s: G
ive
2nd
dose
at l
east
4
wee
ks la
ter a
nd 3
rd (fi
nal)
dose
at 1
2–15
mon
ths
or
8 w
eeks
aft
er 2
nd d
ose
(whi
chev
er is
late
r).
• 1s
t dos
e at
12–
14 m
onth
s: G
ive
2nd
(fina
l) do
se a
t le
ast 8
wee
ks a
fter
1st
dos
e.•
1st d
ose
bef
ore
12 m
onth
s an
d 2
nd
dos
e b
efor
e 15
mon
ths:
Giv
e 3r
d (fi
nal)
dose
8 w
eeks
aft
er 2
nd
dose
.•
2 d
oses
of P
edva
xHIB
bef
ore
12 m
onth
s: G
ive
3rd
(fina
l) do
se a
t 12–
59 m
onth
s an
d at
leas
t 8 w
eeks
af
ter 2
nd d
ose.
• U
nvac
cin
ated
at 1
5–59
mon
ths:
1 d
ose.
• Fo
r oth
er c
atch
-up
guid
ance
, see
Fig
ure
2.
Spec
ial S
itua
tion
s:•
Ch
emot
her
apy
or ra
dia
tion
trea
tmen
t 12
–59
mon
ths
ɱU
nvac
cina
ted
or o
nly
1 do
se b
efor
e 12
mon
ths:
G
ive
2 do
ses,
8 w
eeks
apa
rt ɱ2
or m
ore
dose
s be
fore
12
mon
ths:
Giv
e 1
dose
, at
leas
t 8 w
eeks
aft
er p
revi
ous
dose
.D
oses
giv
en w
ithin
14
days
of s
tart
ing
ther
apy
or
durin
g th
erap
y sh
ould
be
repe
ated
at l
east
3 m
onth
s af
ter t
hera
py c
ompl
etio
n.•
Hem
atop
oiet
ic s
tem
cel
l tra
nsp
lant
(HSC
T)•
3-do
se s
erie
s w
ith d
oses
4 w
eeks
apa
rt s
tart
ing
6 to
12
mon
ths
afte
r suc
cess
ful t
rans
plan
t (re
gard
less
of
Hib
vac
cina
tion
hist
ory)
.•
An
atom
ic o
r fun
ctio
nal
asp
len
ia (i
ncl
udin
g s
ickl
e ce
ll d
isea
se)
12–5
9 m
onth
s ɱU
nvac
cina
ted
or o
nly
1 do
se b
efor
e 12
mon
ths:
G
ive
2 do
ses,
8 w
eeks
apa
rt.
ɱ2
or m
ore
dose
s be
fore
12
mon
ths:
Giv
e 1
dose
, at
leas
t 8 w
eeks
aft
er p
revi
ous
dose
.U
nim
mun
ized
* pe
rson
s 5 y
ears
or o
lder
ɱG
ive
1 do
se•
Elec
tive
sp
len
ecto
my
Uni
mm
uniz
ed*
pers
ons
15 m
onth
s or
old
er ɱG
ive
1 do
se (p
refe
rabl
y at
leas
t 14
days
bef
ore
proc
edur
e).
• H
IV in
fect
ion
12–5
9 m
onth
s ɱU
nvac
cina
ted
or o
nly
1 do
se b
efor
e 12
m
onth
s: G
ive
2 do
ses
8 w
eeks
ap
art.
ɱ2
or m
ore
dose
s b
efor
e 12
mon
ths:
Giv
e 1
dose
, at l
east
8 w
eeks
aft
er p
revi
ous
dose
.U
nim
mun
ized
* pe
rson
s 5–1
8 ye
ars
ɱG
ive
1 do
se•
Imm
un
og
lob
ulin
defi
cien
cy, e
arly
co
mp
on
ent
com
ple
men
t defi
cien
cy12
–59
mon
ths
ɱU
nvac
cina
ted
or o
nly
1 do
se b
efor
e 12
m
onth
s: G
ive
2 do
ses,
8 w
eeks
ap
art.
ɱ2
or m
ore
dose
s b
efor
e 12
mon
ths:
Giv
e 1
dose
, at l
east
8 w
eeks
aft
er p
revi
ous
dose
.
*Uni
mm
uniz
ed =
Les
s th
an ro
utin
e se
ries
(thr
ough
14
mon
ths)
OR
no d
oses
(14
mon
ths
or o
lder
)
5.
Pneu
moc
occa
l vac
cin
es. (
min
imum
ag
e: 6
wee
ks
[PC
V13
], 2
year
s [P
PSV
23])
Ro
uti
ne
vacc
inat
ion
wit
h P
CV
13:
• 4-
dose
ser
ies
at 2
, 4, 6
, and
12–
15 m
onth
s.C
atch
-up
vac
cin
atio
n w
ith
PC
V13
:•
1 do
se fo
r hea
lthy
chi
ldre
n ag
ed 2
4–59
mon
ths
with
any
inco
mp
lete
* PC
V13
sche
dule
• Fo
r oth
er c
atch
-up
gui
danc
e, s
ee F
igur
e 2.
Spec
ial s
itu
atio
ns:
Hig
h-r
isk
con
dit
ion
s:
Ad
min
iste
r P
CV
13 d
ose
s b
efo
re P
PSV
23 if
p
oss
ible
.C
hro
nic
hea
rt d
isea
se (p
arti
cula
rly
cyan
oti
c co
ng
enit
al h
eart
dis
ease
an
d c
ard
iac
failu
re);
ch
ron
ic lu
ng
dis
ease
(in
clu
din
g a
sth
ma
trea
ted
w
ith
hig
h-d
ose
, ora
l, co
rtic
ost
ero
ids)
; dia
bet
es
mel
litu
s:A
ge
2–5
year
s:•
Any
inco
mp
lete
* sc
hedu
les
with
: ɱ3
PCV1
3 do
ses:
1 d
ose
of P
CV1
3 (a
t lea
st 8
w
eeks
aft
er a
ny p
rior P
CV1
3 do
se).
ɱ<
3 PC
V13
dose
s: 2
dos
es o
f PC
V13,
8 w
eeks
af
ter t
he m
ost r
ecen
t dos
e an
d gi
ven
8 w
eeks
ap
art.
• N
o hi
stor
y of
PPS
V23:
1 d
ose
of P
PSV2
3 (a
t lea
st 8
w
eeks
aft
er a
ny p
rior P
CV1
3 do
se).
Ag
e 6-
18 y
ears
:•
No
hist
ory
of P
PSV2
3: 1
dos
e of
PPS
V23
(at l
east
8
wee
ks a
fter
any
prio
r PC
V13
dose
).
For f
urth
er g
uida
nce
on th
e us
e of
the
vacc
ines
men
tione
d b
elow
, see
: ww
w.c
dc.g
ov/v
acci
nes/
hcp
/aci
p-r
ecs/
inde
x.ht
ml.
Cer
ebro
spin
al fl
uid
leak
; co
chle
ar im
pla
nt:
Ag
e 2–
5 ye
ars:
• A
ny in
com
ple
te*
sche
dule
s w
ith:
ɱ3
PCV1
3 do
ses:
1 d
ose
of P
CV1
3 (a
t lea
st 8
w
eeks
aft
er a
ny p
rior P
CV1
3 do
se).
ɱ<
3 PC
V13
dose
s: 2
dos
es o
f PC
V13,
8 w
eeks
af
ter t
he m
ost r
ecen
t dos
e an
d gi
ven
8 w
eeks
ap
art.
• N
o hi
stor
y of
PPS
V23:
1 d
ose
of P
PSV2
3 (a
t lea
st 8
w
eeks
aft
er a
ny p
rior P
CV1
3 do
se).
Ag
e 6–
18 y
ears
:•
No
hist
ory
of e
ither
PC
V13
or P
PSV2
3: 1
dos
e of
PC
V13,
1 d
ose
of P
PSV2
3 at
leas
t 8 w
eeks
late
r.•
Any
PC
V13
but
no
PPSV
23: 1
dos
e of
PPS
V23
at
leas
t 8 w
eeks
aft
er th
e m
ost r
ecen
t dos
e of
PC
V13
• PP
SV23
but
no
PCV1
3: 1
dos
e of
PC
V13
at le
ast 8
w
eeks
aft
er th
e m
ost r
ecen
t dos
e of
PPS
V23.
Sick
le c
ell d
isea
se a
nd
oth
er h
emo
glo
bin
op
ath
ies;
an
ato
mic
or
fun
ctio
nal
asp
len
ia; c
on
gen
ital
o
r ac
qu
ired
imm
un
od
efici
ency
; HIV
infe
ctio
n;
chro
nic
ren
al fa
ilure
; nep
hro
tic
syn
dro
me;
m
alig
nan
t neo
pla
sms,
leu
kem
ias,
lym
ph
om
as,
Ho
dg
kin
dis
ease
, an
d o
ther
dis
ease
s as
soci
ated
w
ith
trea
tmen
t wit
h im
mu
no
sup
pre
ssiv
e d
rug
s o
r ra
dia
tio
n th
erap
y; s
olid
org
an tr
ansp
lan
tati
on
; m
ult
iple
mye
lom
a:A
ge
2–5
year
s:•
Any
inco
mp
lete
* sc
hedu
les
with
: ɱ3
PCV1
3 do
ses:
1 d
ose
of P
CV1
3 (a
t lea
st 8
w
eeks
aft
er a
ny p
rior P
CV1
3 do
se).
ɱ<
3 PC
V13
dose
s: 2
dos
es o
f PC
V13,
8 w
eeks
af
ter t
he m
ost r
ecen
t dos
e an
d gi
ven
8 w
eeks
ap
art.
• N
o hi
stor
y of
PPS
V23:
1 d
ose
of P
PSV2
3 (a
t lea
st 8
w
eeks
aft
er a
ny p
rior P
CV1
3 do
se) a
nd a
2nd
dos
e of
PPS
V23
5 ye
ars
late
r.A
ge
6–18
yea
rs:
• N
o hi
stor
y of
eith
er P
CV1
3 or
PPS
V23:
1 d
ose
of
PCV1
3, 2
dos
es o
f PPS
V23
(1st
dos
e of
PPS
V23
adm
inis
tere
d 8
wee
ks a
fter
PC
V13
and
2nd
dose
of
PPSV
23 a
dmin
iste
red
at le
ast 5
yea
rs a
fter
the
1st
dose
of P
PSV2
3).
• A
ny P
CV1
3 b
ut n
o PP
SV23
: 2 d
oses
of P
PSV2
3 (1
st
dose
of P
PSV2
3 to
be
give
n 8
wee
ks a
fter
the
mos
t re
cent
dos
e of
PC
V13
and
2nd
dose
of P
PSV2
3 ad
min
iste
red
at le
ast 5
yea
rs a
fter
the
1st d
ose
of
PPSV
23).

A-7
For f
urth
er g
uida
nce
on th
e us
e of
the
vacc
ines
men
tione
d b
elow
, see
: ww
w.c
dc.g
ov/v
acci
nes/
hcp
/aci
p-r
ecs/
inde
x.ht
ml.
• PP
SV23
but
no
PCV1
3: 1
dos
e of
PC
V13
at le
ast
8 w
eeks
aft
er th
e m
ost r
ecen
t PPS
V23
dose
and
a 2
nd
dose
of P
PSV2
3 to
be
give
n 5
year
s aft
er th
e 1s
t dos
e of
PPS
V23
and
at le
ast 8
wee
ks a
fter
a d
ose
of P
CV1
3.C
hro
nic
live
r d
isea
se, a
lco
ho
lism
:A
ge
6–18
yea
rs:
• N
o hi
stor
y of
PPS
V23:
1 d
ose
of P
PSV2
3 (a
t le
ast
8 w
eeks
aft
er a
ny p
rior P
CV1
3 do
se).
*Inc
omp
lete
sch
edul
es a
re a
ny s
ched
ules
whe
re
PCV1
3 do
ses
have
not
bee
n co
mp
lete
d ac
cord
ing
to
AC
IP re
com
men
ded
catc
h-up
sch
edul
es. T
he to
tal
num
ber
and
tim
ing
of d
oses
for c
omp
lete
PC
V13
serie
s ar
e di
ctat
ed b
y th
e ag
e at
firs
t vac
cina
tion.
See
Ta
ble
s 8
and
9 in
the
AC
IP p
neum
ococ
cal v
acci
ne
reco
mm
enda
tions
(ww
w.c
dc.g
ov/m
mw
r/p
df/r
r/rr
5911
) for
com
ple
te s
ched
ule
deta
ils.
6.
Inac
tiva
ted
po
liovi
rus
vacc
ine
(IP
V).
(m
inim
um
ag
e: 6
wee
ks)
Ro
uti
ne
vacc
inat
ion
:•
4-do
se se
ries a
t age
s 2, 4
, 6–1
8 m
onth
s, an
d 4–
6 ye
ars.
A
dmin
iste
r the
fina
l dos
e on
or a
fter
the
4th
birt
hday
an
d at
leas
t 6 m
onth
s af
ter t
he p
revi
ous
dose
.C
atch
-up
vac
cin
atio
n:
• In
the
first
6 m
onth
s of
life
, use
min
imum
age
s an
d in
terv
als o
nly
for t
rave
l to
a p
olio
-end
emic
regi
on o
r du
ring
an o
utb
reak
.•
If 4
or m
ore
dose
s wer
e gi
ven
befo
re th
e 4t
h bi
rthd
ay,
give
1 m
ore
dos
e at
age
4–6
yea
rs a
nd a
t le
ast
6 m
onth
s af
ter t
he p
revi
ous
dose
.•
A 4
th d
ose
is n
ot n
eces
sary
if th
e 3r
d do
se w
as g
iven
on
or
afte
r th
e 4t
h b
irth
day
and
at le
ast
6 m
onth
s af
ter t
he p
revi
ous
dose
.•
IPV
is n
ot ro
utin
ely
reco
mm
ende
d fo
r U.S
. res
iden
ts
18 y
ears
and
old
er.
Seri
es C
on
tain
ing
Ora
l Po
lio V
acci
ne
(OP
V),
eith
er
mix
ed O
PV-IP
V or
OPV
-onl
y se
ries:
• To
tal n
umbe
r of d
oses
nee
ded
to c
ompl
ete
the
serie
s is
the
sam
e as
tha
t re
com
men
ded
for
the
U.S
. IPV
sc
hedu
le. S
ee w
ww
.cdc
.gov
/mm
wr/
volu
mes
/66/
wr/
mm
6601
a6.h
tm?s
_cid
=m
m66
01a6
_w.
• O
nly
triv
alen
t OPV
(tO
PV) c
ount
s to
war
d th
e U
.S. v
acci
natio
n re
quire
men
ts. F
or g
uida
nce
to
asse
ss d
oses
doc
umen
ted
as “O
PV” s
ee w
ww
.cd
c.go
v/m
mw
r/vo
lum
es/6
6/w
r/m
m66
06a7
.ht
m?s
_cid
=m
m66
06a7
_w.
• Fo
r oth
er c
atch
-up
gui
danc
e, s
ee F
igur
e 2.
7.
Infl
uen
za v
acci
nes
. (m
inim
um a
ge:
6 m
onth
s)R
outi
ne
vacc
inat
ion
:•
Adm
inis
ter a
n ag
e-ap
prop
riate
form
ulat
ion
and
dose
of i
nflue
nza
vacc
ine
annu
ally
. ɱC
hild
ren
6 m
onth
s–8
year
s w
ho d
id n
ot
rece
ive
at le
ast 2
dos
es o
f infl
uenz
a va
ccin
e be
fore
July
1, 2
017
shou
ld re
ceiv
e 2
dose
s se
para
ted
by a
t lea
st 4
wee
ks.
ɱPe
rson
s 9
year
s an
d o
lder
1 d
ose
• Li
ve a
tten
uate
d in
fluen
za v
acci
ne (L
AIV
) not
re
com
men
ded
for t
he 2
017–
18 s
easo
n.
• Fo
r add
ition
al g
uida
nce,
see
the
2017
–18
AC
IP
influ
enza
vac
cine
reco
mm
enda
tions
(MM
WR
Aug
ust 2
5, 2
017;
66(2
):1-2
0: w
ww
.cdc
.gov
/mm
wr/
volu
mes
/66/
rr/p
dfs/
rr66
02.p
df).
(For
the
2018
–19
seas
on, s
ee th
e 20
18–1
9 A
CIP
in
fluen
za v
acci
ne re
com
men
datio
ns.)
8.
Mea
sles
, mum
ps,
and
rub
ella
(MM
R) v
acci
ne.
(min
imum
age
: 12
mon
ths
for r
outi
ne v
acci
nati
on)
Rou
tin
e va
ccin
atio
n:
• 2-
dose
ser
ies
at 1
2–15
mon
ths
and
4–6
year
s.•
The
2nd
dose
may
be
give
n as
ear
ly a
s 4
wee
ks a
fter
th
e 1s
t dos
e.C
atch
-up
vac
cin
atio
n:
• U
nvac
cina
ted
child
ren
and
adol
esce
nts:
2 d
oses
at
leas
t 4 w
eeks
apa
rt.
Inte
rnat
ion
al tr
avel
:•
Infa
nts
6–11
mon
ths:
1 d
ose
befo
re d
epar
ture
. Re
vacc
inat
e w
ith 2
dos
es a
t 12–
15 m
onth
s (1
2 m
onth
s fo
r chi
ldre
n in
hig
h-ris
k ar
eas)
and
2nd
dos
e as
ear
ly a
s 4
wee
ks la
ter.
• U
nvac
cin
ated
ch
ildre
n 1
2 m
onth
s an
d o
lder
: 2
dose
s at
leas
t 4 w
eeks
apa
rt b
efor
e de
part
ure.
Mum
ps
outb
reak
:•
Pers
ons
≥12
mon
ths
who
pre
viou
sly
rece
ived
≤
2 do
ses
of m
umps
-con
tain
ing
vacc
ine
and
are
iden
tified
by
publ
ic h
ealth
aut
horit
ies
to b
e at
in
crea
sed
risk
durin
g a
mum
ps o
utbr
eak
shou
ld
rece
ive
a do
se o
f mum
ps-v
irus
cont
aini
ng v
acci
ne.
9.
Vari
cella
(VA
R) v
acci
ne.
(min
imum
age
: 12
mon
ths)
Rou
tin
e va
ccin
atio
n:
• 2-
dose
ser
ies:
12–
15 m
onth
s an
d 4–
6 ye
ars.
• Th
e 2n
d do
se m
ay b
e gi
ven
as e
arly
as
3 m
onth
s af
ter t
he 1
st d
ose
(a d
ose
give
n af
ter a
4-w
eek
inte
rval
may
be
coun
ted)
.
Cat
ch-u
p v
acci
nat
ion
:•
Ensu
re p
erso
ns 7
–18
year
s w
ithou
t evi
denc
e of
im
mun
ity (s
ee M
MW
R 20
07;5
6[N
o. R
R-4]
, at
ww
w.c
dc.g
ov/m
mw
r/pd
f/rr
/rr5
604.
pdf)
hav
e 2
dose
s of
var
icel
la v
acci
ne:
ɱA
ges
7–1
2: ro
utin
e in
terv
al 3
mon
ths
(m
inim
um in
terv
al: 4
wee
ks).
ɱA
ges
13
and
old
er: m
inim
um in
terv
al 4
wee
ks.
10.
Hep
atit
is A
(Hep
A) v
acci
ne.
(min
imum
ag
e: 1
2 m
onth
s)R
outi
ne
vacc
inat
ion
:•
2 do
ses,
sep
arat
ed b
y 6-
18 m
onth
s, b
etw
een
the
1st a
nd 2
nd b
irthd
ays.
(A s
erie
s be
gun
befo
re th
e 2n
d bi
rthd
ay s
houl
d be
com
plet
ed e
ven
if th
e ch
ild
turn
s 2
befo
re th
e se
cond
dos
e is
giv
en.)
Cat
ch-u
p v
acci
nat
ion
:•
Any
one
2 ye
ars
of a
ge o
r old
er m
ay re
ceiv
e H
epA
va
ccin
e if
desi
red.
Min
imum
inte
rval
bet
wee
n do
ses
is 6
mon
ths.
Spec
ial p
opul
atio
ns:
Pr
evio
usly
unv
acci
nate
d pe
rson
s w
ho s
houl
d be
va
ccin
ated
: •
Pers
ons
trav
elin
g to
or w
orki
ng in
cou
ntrie
s w
ith
high
or i
nter
med
iate
end
emic
ity
• M
en w
ho h
ave
sex
with
men
•
Use
rs o
f inj
ectio
n an
d no
n-in
ject
ion
drug
s
• Pe
rson
s w
ho w
ork
with
hep
atiti
s A
viru
s in
a
rese
arch
labo
rato
ry o
r with
non
-hum
an p
rimat
es
• Pe
rson
s w
ith c
lott
ing-
fact
or d
isor
ders
•
Pers
ons
with
chr
onic
live
r dis
ease
• Pe
rson
s w
ho a
ntic
ipat
e cl
ose,
per
sona
l con
tact
(e
.g.,
hous
ehol
d or
regu
lar b
abys
ittin
g) w
ith a
n in
tern
atio
nal a
dopt
ee d
urin
g th
e fir
st 6
0 da
ys a
fter
ar
rival
in th
e U
nite
d St
ates
from
a c
ount
ry w
ith h
igh
or in
term
edia
te e
ndem
icity
(adm
inis
ter t
he 1
st d
ose
as s
oon
as th
e ad
optio
n is
pla
nned
—id
eally
at l
east
2
wee
ks b
efor
e th
e ad
opte
e’s
arriv
al).
11.
Sero
gro
up A
, C, W
, Y m
enin
goc
occa
l vac
cin
es.
(Min
imum
ag
e: 2
mon
ths
[Men
veo]
, 9 m
onth
s [M
enac
tra]
.R
outi
ne:
• 2-
dose
ser
ies:
11-
12 y
ears
and
16
year
s.C
atch
-Up
:•
Age
13-
15 y
ears
: 1 d
ose
now
and
boo
ster
at a
ge
16-1
8 ye
ars.
Min
imum
inte
rval
8 w
eeks
.•
Age
16-
18 y
ears
: 1 d
ose.

A-8
For f
urth
er g
uida
nce
on th
e us
e of
the
vacc
ines
men
tione
d b
elow
, see
: ww
w.c
dc.g
ov/v
acci
nes/
hcp
/aci
p-r
ecs/
inde
x.ht
ml.
CS2
7045
7-M
Spec
ial p
opul
atio
ns
and
sit
uati
ons:
A
nat
omic
or f
unct
ion
al a
sple
nia
, sic
kle
cell
dis
ease
, H
IV in
fect
ion
, per
sist
ent c
omp
lem
ent c
omp
onen
t d
efici
ency
(in
clud
ing
ecu
lizum
ab u
se):
• M
enve
o ɱ1s
t dos
e at
8 w
eeks
: 4-d
ose
serie
s at 2
, 4, 6
, and
12
mon
ths.
ɱ1s
t dos
e at
7–2
3 m
onth
s: 2
dose
s (2n
d do
se a
t le
ast 1
2 w
eeks
aft
er th
e 1s
t dos
e an
d af
ter t
he 1
st
birt
hday
). ɱ1s
t dos
e at
24
mon
ths o
r old
er: 2
dos
es a
t lea
st 8
w
eeks
apa
rt.
• M
enac
tra
ɱPe
rsis
tent
com
plem
ent c
ompo
nent
defi
cien
cy:
ʲ
9–23
mon
ths:
2 do
ses a
t lea
st 1
2 w
eeks
apa
rt
ʲ24
mon
ths o
r old
er: 2
dos
es a
t lea
st 8
wee
ks
apar
t ɱA
nato
mic
or f
unct
iona
l asp
leni
a, si
ckle
cel
l di
seas
e, o
r HIV
infe
ctio
n:
ʲ
24 m
onth
s or o
lder
: 2 d
oses
at l
east
8 w
eeks
ap
art.
ʲ
Men
actr
a m
ust b
e ad
min
iste
red
at le
ast 4
w
eeks
aft
er c
ompl
etio
n of
PC
V13
serie
s.Ch
ildre
n w
ho tr
avel
to o
r liv
e in
cou
ntri
es w
here
m
enin
goco
ccal
dis
ease
is h
yper
ende
mic
or
epid
emic
, inc
ludi
ng c
ount
ries
in th
e A
fric
an
men
ingi
tis
belt
or d
urin
g th
e H
ajj,
or e
xpos
ure
to a
n
outb
reak
att
ribu
tabl
e to
a v
acci
ne s
erog
roup
:•
Child
ren
<24
mon
ths o
f age
: ɱM
enve
o (2
-23
mon
ths)
:
ʲ1s
t dos
e at
8 w
eeks
: 4-d
ose
serie
s at 2
, 4, 6
, and
12
mon
ths.
ʲ
1st d
ose
at 7
-23
mon
ths:
2 do
ses (
2nd
dose
at
leas
t 12
wee
ks a
fter
the
1st d
ose
and
afte
r the
1s
t birt
hday
). ɱM
enac
tra
(9-2
3 m
onth
s):
ʲ
2 do
ses (
2nd
dose
at l
east
12
wee
ks a
fter
the
1st d
ose.
2nd
dos
e m
ay b
e ad
min
iste
red
as
early
as 8
wee
ks a
fter
the
1st d
ose
in tr
avel
ers)
.•
Child
ren
2 ye
ars o
r old
er: 1
dos
e of
Men
veo
or
Men
actr
a.N
ote:
Men
actr
a sh
ould
be
give
n ei
ther
bef
ore
or a
t th
e sa
me
time
as D
TaP.
For M
enA
CW
Y bo
oste
r dos
e re
com
men
datio
ns fo
r gro
ups l
iste
d un
der “
Spec
ial
popu
latio
ns a
nd si
tuat
ions
” abo
ve, a
nd a
dditi
onal
m
enin
goco
ccal
vac
cina
tion
info
rmat
ion,
see
men
ingo
cocc
al M
MW
R pu
blic
atio
ns a
t: w
ww
.cdc
.gov
/va
ccin
es/h
cp/a
cip-
recs
/vac
c-sp
ecifi
c/m
enin
g.ht
ml.
12.
Sero
gro
up B
men
ing
ococ
cal v
acci
nes
(min
imum
ag
e: 1
0 ye
ars
[Bex
sero
, Tru
men
ba]
.C
linic
al d
iscr
etio
n: A
do
lesc
ents
no
t at i
ncr
ease
d
risk
for
men
ing
oco
ccal
B in
fect
ion
wh
o w
ant
Men
B v
acci
ne.
Men
B va
ccin
es m
ay b
e gi
ven
at c
linic
al d
iscr
etio
n to
ad
oles
cent
s 16
–23
year
s (p
refe
rred
age
16–
18 y
ears
) w
ho a
re n
ot a
t inc
reas
ed ri
sk.
• B
exse
ro: 2
dos
es a
t lea
st 1
mon
th a
par
t.•
Tru
men
ba:
2 d
oses
at l
east
6 m
onth
s ap
art.
If th
e 2n
d do
se is
giv
en e
arlie
r tha
n 6
mon
ths,
giv
e a
3rd
dose
at l
east
4 m
onth
s af
ter t
he 2
nd.
Spec
ial p
op
ula
tio
ns
and
sit
uat
ion
s:A
nat
om
ic o
r fu
nct
ion
al a
sple
nia
, sic
kle
cell
dis
ease
, per
sist
ent c
om
ple
men
t co
mp
on
ent
defi
cien
cy (i
ncl
ud
ing
ecu
lizu
mab
use
), s
ero
gro
up
B
men
ing
oco
ccal
dis
ease
ou
tbre
ak•
Bex
sero
: 2-d
ose
serie
s at
leas
t 1 m
onth
ap
art.
• Tr
um
enb
a: 3
-dos
e se
ries
at 0
, 1-2
, and
6 m
onth
s.
No
te: B
exse
ro a
nd T
rum
enb
a ar
e no
t in
terc
hang
eab
le.
For a
dditi
onal
men
ingo
cocc
al v
acci
natio
n in
form
atio
n, s
ee m
enin
goco
ccal
MM
WR
pub
licat
ions
at
: ww
w.c
dc.g
ov/v
acci
nes/
hcp
/aci
p-r
ecs/
vacc
-sp
ecifi
c/m
enin
g.ht
ml.
13.
Teta
nus
, dip
hth
eria
, an
d a
cellu
lar p
ertu
ssis
(T
dap
) vac
cin
e. (m
inim
um a
ge:
11
year
s fo
r ro
utin
e va
ccin
atio
ns,
7 y
ears
for c
atch
-up
va
ccin
atio
n)
Ro
uti
ne
vacc
inat
ion
: •
Ad
ole
scen
ts 1
1–12
yea
rs o
f ag
e: 1
dos
e.•
Preg
nan
t ad
ole
scen
ts: 1
dos
e du
ring
each
p
regn
ancy
(pre
fera
bly
dur
ing
the
earl
y p
art o
f ge
stat
iona
l wee
ks 2
7–36
). •
Tdap
may
be
adm
inis
tere
d re
gard
less
of t
he
inte
rval
sin
ce th
e la
st te
tanu
s- a
nd d
ipht
heria
-to
xoid
-con
tain
ing
vacc
ine.
Cat
ch-u
p v
acci
nat
ion
:•
Ad
ole
scen
ts 1
3–18
wh
o h
ave
no
t rec
eive
d T
dap
: 1
dose
, fol
low
ed b
y a
Td b
oost
er e
very
10
year
s.•
Pers
on
s ag
ed 7
–18
year
s n
ot f
ully
imm
un
ized
w
ith
DTa
P:
1 do
se o
f Tda
p a
s p
art o
f the
cat
ch-u
p
serie
s (p
refe
rab
ly th
e fir
st d
ose)
. If a
dditi
onal
dos
es
are
need
ed, u
se T
d.
• C
hild
ren
7–1
0 ye
ars
who
rece
ive
Tdap
in
adve
rten
tly o
r as
part
of t
he c
atch
-up
serie
s m
ay
rece
ive
the
rout
ine
Tdap
dos
e at
11–
12 y
ears
.•
DTa
P in
adve
rten
tly
giv
en a
fter
the
7th
bir
thd
ay:
ɱC
hild
7–1
0: D
TaP
may
cou
nt a
s pa
rt o
f ca
tch-
up s
erie
s. R
outin
e Td
ap d
ose
at 1
1-12
m
ay b
e gi
ven.
ɱA
dol
esce
nt 1
1–18
: Cou
nt d
ose
of D
TaP
as th
e ad
oles
cent
Tda
p bo
oste
r. •
For o
ther
cat
ch-u
p gu
idan
ce, s
ee F
igur
e 2.
14.
Hum
an p
apill
omav
irus
(HPV
) vac
cin
e (m
inim
um
age:
9 y
ears
)R
outi
ne
and
cat
ch-u
p v
acci
nat
ion
:•
Rout
ine
vacc
inat
ion
for a
ll ad
oles
cent
s at
11–
12
year
s (c
an s
tart
at a
ge 9
) and
thro
ugh
age
18 if
no
t pre
viou
sly
adeq
uate
ly v
acci
nate
d. N
umbe
r of
dose
s de
pend
ent o
n ag
e at
initi
al v
acci
natio
n:
ɱA
ge
9–14
yea
rs a
t in
itia
tion
: 2-d
ose
serie
s at
0 a
nd 6
–12
mon
ths.
Min
imum
inte
rval
: 5
mon
ths
(rep
eat a
dos
e gi
ven
too
soon
at l
east
12
wee
ks a
fter
the
inva
lid d
ose
and
at le
ast 5
m
onth
s af
ter t
he 1
st d
ose)
. ɱA
ge
15 y
ears
or o
lder
at i
nit
iati
on: 3
-dos
e se
ries
at 0
, 1–2
mon
ths,
and
6 m
onth
s.
Min
imum
inte
rval
s: 4
wee
ks b
etw
een
1st
and
2nd
dose
; 12
wee
ks b
etw
een
2nd
and
3rd
do
se; 5
mon
ths
betw
een
1st a
nd 3
rd d
ose
(rep
eat d
ose(
s) g
iven
too
soon
at o
r aft
er th
e m
inim
um in
terv
al s
ince
the
mos
t rec
ent d
ose)
.•
Pers
ons
who
hav
e co
mpl
eted
a v
alid
ser
ies
with
an
y H
PV v
acci
ne d
o no
t nee
d an
y ad
ditio
nal d
oses
. Sp
ecia
l sit
uat
ion
s:•
His
tory
of s
exu
al a
bu
se o
r ass
ault
: Beg
in s
erie
s at
ag
e 9
year
s.•
Imm
un
ocom
pro
mis
ed*
(incl
ud
ing
HIV
) age
d 9–
26 y
ears
: 3-d
ose
serie
s at
0, 1
–2 m
onth
s, a
nd 6
m
onth
s.•
Preg
nan
cy: V
acci
natio
n no
t rec
omm
ende
d,
but t
here
is n
o ev
iden
ce th
e va
ccin
e is
har
mfu
l. N
o in
terv
entio
n is
nee
ded
for w
omen
who
in
adve
rten
tly re
ceiv
ed a
dos
e of
HPV
vac
cine
w
hile
pre
gnan
t. D
elay
rem
aini
ng d
oses
unt
il af
ter
preg
nanc
y. P
regn
ancy
test
ing
not n
eede
d be
fore
va
ccin
atio
n.*S
ee M
MW
R, D
ecem
ber 1
6, 2
016;
65(4
9):1
405–
1408
, at
ww
w.c
dc.g
ov/m
mw
r/vo
lum
es/6
5/w
r/pd
fs/
mm
6549
a5.p
df.

A-9
Rec
omm
end
ed Im
mu
niz
atio
n S
ched
ule
for A
du
lts
Ag
ed 1
9 Ye
ars
or O
lder
, Un
ited
Sta
tes,
201
8
U.S
. Dep
artm
ent o
f Hea
lth a
nd H
uman
Ser
vice
sCe
nter
s fo
r Dis
ease
Con
trol
and
Pre
vent
ion
In F
ebru
ary
2018
, the
Rec
omm
ende
d Im
mun
izat
ion
Sche
dule
for A
dults
Age
d 19
Yea
rs o
r Old
er, U
nite
d St
ates
, 201
8 be
cam
e eff
ectiv
e, a
s re
com
men
ded
by th
e A
dvis
ory
Com
mitt
ee o
n Im
mun
izat
ion
Prac
tices
(A
CIP)
and
app
rove
d by
the
Cent
ers
for D
isea
se C
ontr
ol a
nd P
reve
ntio
n (C
DC
). Th
e ad
ult i
mm
uniz
atio
n sc
hedu
le w
as a
lso
appr
oved
by
the
Am
eric
an C
olle
ge o
f Phy
sici
ans,
the
Am
eric
an A
cade
my
of F
amily
Ph
ysic
ians
, the
Am
eric
an C
olle
ge o
f Obs
tetr
icia
ns a
nd G
ynec
olog
ists
, and
the
Am
eric
an C
olle
ge o
f N
urse
-Mid
wiv
es.
CDC
anno
unce
d th
e av
aila
bilit
y of
the
2018
adu
lt im
mun
izat
ion
sche
dule
in th
e M
orbi
dity
and
Mor
talit
y W
eekl
y Re
port
(MM
WR)
.1 The
sch
edul
e is
pub
lishe
d in
its
entir
ety
in th
e An
nals
of I
nter
nal M
edic
ine.
2
The
adul
t im
mun
izat
ion
sche
dule
con
sist
s of
figu
res
that
sum
mar
ize
rout
inel
y re
com
men
ded
vacc
ines
fo
r adu
lts b
y ag
e gr
oups
and
med
ical
con
ditio
ns a
nd o
ther
indi
catio
ns, f
ootn
otes
for t
he fi
gure
s, an
d a
tabl
e of
vac
cine
con
trai
ndic
atio
ns a
nd p
reca
utio
ns. N
ote
the
follo
win
g w
hen
revi
ewin
g th
e ad
ult
imm
uniz
atio
n sc
hedu
le:
• Th
e fig
ures
in th
e ad
ult i
mm
uniz
atio
n sc
hedu
le s
houl
d be
revi
ewed
with
the
acco
mpa
nyin
g fo
otno
tes.
• Th
e fig
ures
and
foot
note
s di
spla
y in
dica
tions
for w
hich
vac
cine
s, if
not p
revi
ousl
y ad
min
iste
red,
sh
ould
be
adm
inis
tere
d un
less
not
ed o
ther
wis
e.•
The
tabl
e of
con
trai
ndic
atio
ns a
nd p
reca
utio
ns id
entifi
es p
opul
atio
ns a
nd s
ituat
ions
for w
hich
va
ccin
es s
houl
d no
t be
used
or s
houl
d be
use
d w
ith c
autio
n.•
Whe
n in
dica
ted,
adm
inis
ter r
ecom
men
ded
vacc
ines
to a
dults
who
se v
acci
natio
n hi
stor
y is
in
com
plet
e or
unk
now
n.•
Incr
ease
d in
terv
al b
etw
een
dose
s of
a m
ultid
ose
vacc
ine
serie
s do
es n
ot d
imin
ish
vacc
ine
effec
tiven
ess;
it is
not
nec
essa
ry to
rest
art t
he v
acci
ne s
erie
s or
add
dos
es to
the
serie
s be
caus
e of
an
ext
ende
d in
terv
al b
etw
een
dose
s.•
Com
bina
tion
vacc
ines
may
be
used
whe
n an
y co
mpo
nent
of t
he c
ombi
natio
n is
indi
cate
d an
d w
hen
the
othe
r com
pone
nts
of th
e co
mbi
natio
n ar
e no
t con
trai
ndic
ated
.•
The
use
of tr
ade
nam
es in
the
adul
t im
mun
izat
ion
sche
dule
is fo
r ide
ntifi
catio
n pu
rpos
es o
nly
and
does
not
impl
y en
dors
emen
t by
the
ACI
P or
CD
C.
Spec
ial p
opul
atio
ns th
at n
eed
addi
tiona
l con
side
ratio
ns in
clud
e:
• Pr
egna
nt w
omen
. Pre
gnan
t wom
en s
houl
d re
ceiv
e th
e te
tanu
s, di
phth
eria
, and
ace
llula
r per
tuss
is
vacc
ine
(Tda
p) d
urin
g pr
egna
ncy
and
the
influ
enza
vac
cine
dur
ing
or b
efor
e pr
egna
ncy.
Liv
e va
ccin
es (e
.g.,
mea
sles
, mum
ps, a
nd ru
bella
vac
cine
[MM
R]) a
re c
ontr
aind
icat
ed.
• A
sple
nia.
Adu
lts w
ith a
sple
nia
have
spe
cific
vac
cina
tion
reco
mm
enda
tions
bec
ause
of t
heir
incr
ease
d ris
k fo
r inf
ectio
n by
enc
apsu
late
d ba
cter
ia. A
nato
mic
al o
r fun
ctio
nal a
sple
nia
incl
udes
con
geni
tal o
r acq
uire
d as
plen
ia, s
plen
ic d
ysfu
nctio
n, s
ickl
e ce
ll di
seas
e an
d ot
her
hem
oglo
bino
path
ies,
and
sple
nect
omy.
• Im
mun
ocom
prom
isin
g co
nditi
ons.
Adu
lts w
ith im
mun
osup
pres
sion
sho
uld
gene
rally
avo
id
live
vacc
ines
. Ina
ctiv
ated
vac
cine
s (e
.g.,
pneu
moc
occa
l vac
cine
s) a
re g
ener
ally
acc
epta
ble.
H
igh-
leve
l im
mun
osup
pres
sion
incl
udes
HIV
infe
ctio
n w
ith a
CD
4 ce
ll co
unt <
200
cells
/μL,
re
ceip
t of d
aily
cor
ticos
tero
id th
erap
y w
ith ≥
20 m
g of
pre
dnis
one
or e
quiv
alen
t for
≥14
day
s,
prim
ary
imm
unod
efici
ency
dis
orde
r (e.
g., s
ever
e co
mbi
ned
imm
unod
efici
ency
or c
ompl
emen
t co
mpo
nent
defi
cien
cy),
and
rece
ipt o
f can
cer c
hem
othe
rapy
. Oth
er im
mun
ocom
prom
isin
g co
nditi
ons
and
imm
unos
uppr
essi
ve m
edic
atio
ns to
con
side
r whe
n va
ccin
atin
g ad
ults
can
be
foun
d in
IDSA
Clin
ical
Pra
ctic
e G
uide
line
for V
acci
natio
n of
the
Imm
unoc
ompr
omis
ed H
ost.3
Add
ition
al in
form
atio
n on
vac
cina
ting
imm
unoc
ompr
omis
ed a
dults
is in
Gen
eral
Bes
t Pra
ctic
e G
uide
lines
for I
mm
uniz
atio
n.4
Add
ition
al re
sour
ces
for h
ealth
car
e pr
ovid
ers
incl
ude:
• D
etai
ls o
n va
ccin
es re
com
men
ded
for a
dults
and
com
plet
e A
CIP
stat
emen
ts a
t ww
w.c
dc.g
ov/
vacc
ines
/hcp
/aci
p-r
ecs/
inde
x.ht
ml
• Va
ccin
e In
form
atio
n St
atem
ents
that
exp
lain
ben
efits
and
risk
s of
vac
cine
s at
ww
w.c
dc.g
ov/
vacc
ines
/hcp
/vis
/inde
x.ht
ml
• In
form
atio
n an
d re
sour
ces
on v
acci
natin
g pr
egna
nt w
omen
at w
ww
.cdc
.gov
/vac
cine
s/ad
ults
/rec
-va
c/pr
egna
nt.h
tml
• In
form
atio
n on
trav
el v
acci
ne re
quire
men
ts a
nd re
com
men
datio
ns a
t ww
w.c
dc.g
ov/t
rave
l/de
stin
atio
ns/li
st•
CDC
Vacc
ine
Sche
dule
s A
pp fo
r im
mun
izat
ion
serv
ice
prov
ider
s to
dow
nloa
d at
ww
w.c
dc.g
ov/
vacc
ines
/sch
edul
es/h
cp/s
ched
ule-
app.
htm
l•
Adu
lt Va
ccin
atio
n Q
uiz
for s
elf-
asse
ssm
ent o
f vac
cina
tion
need
s ba
sed
on a
ge, h
ealth
con
ditio
ns,
and
othe
r ind
icat
ions
at w
ww
2.cd
c.go
v/ni
p/ad
ultim
msc
hed/
defa
ult.a
sp
• Re
com
men
ded
Imm
uniz
atio
n Sc
hedu
le fo
r Chi
ldre
n an
d Ad
oles
cent
s Age
d 18
Yea
rs o
r You
nger
at
ww
w.c
dc.g
ov/v
acci
nes/
sche
dule
s/hc
p/ch
ild-a
dole
scen
t.htm
l
Repo
rt s
uspe
cted
cas
es o
f rep
orta
ble
vacc
ine-
prev
enta
ble
dise
ases
to th
e lo
cal o
r sta
te h
ealth
de
part
men
t, an
d re
port
all
clin
ical
ly s
igni
fican
t pos
tvac
cina
tion
even
ts to
the
Vacc
ine
Adv
erse
Eve
nt
Repo
rtin
g Sy
stem
at w
ww
.vae
rs.h
hs.g
ov o
r by
tele
phon
e, 8
00-8
22-7
967.
All
vacc
ines
incl
uded
in th
e ad
ult i
mm
uniz
atio
n sc
hedu
le e
xcep
t 23-
vale
nt p
neum
ococ
cal p
olys
acch
arid
e an
d zo
ster
vac
cine
s ar
e co
vere
d by
the
Vacc
ine
Inju
ry C
ompe
nsat
ion
Prog
ram
. Inf
orm
atio
n on
how
to fi
le a
vac
cine
inju
ry c
laim
is
ava
ilabl
e at
ww
w.h
rsa.
gov/
vacc
inec
ompe
nsat
ion
or b
y te
leph
one,
800
-338
-238
2. S
ubm
it qu
estio
ns
and
com
men
ts to
CD
C th
roug
h w
ww
.cdc
.gov
/cdc
-info
or b
y te
leph
one,
800
-CD
C-IN
FO (8
00-2
32-
4636
), in
Eng
lish
and
Span
ish,
8:0
0am
–8:0
0pm
ET,
Mon
day–
Frid
ay, e
xclu
ding
hol
iday
s.
The
follo
win
g ab
brev
iatio
ns a
re u
sed
for v
acci
nes
in th
e ad
ult i
mm
uniz
atio
n sc
hedu
le (i
n th
e or
der o
f th
eir a
ppea
ranc
e):
IIVin
activ
ated
influ
enza
vac
cine
RIV
reco
mbi
nant
influ
enza
vac
cine
Tdap
teta
nus
toxo
id, r
educ
ed d
ipht
heria
toxo
id, a
nd a
cellu
lar p
ertu
ssis
vac
cine
Tdte
tanu
s an
d di
phth
eria
toxo
ids
MM
Rm
easl
es, m
umps
, and
rube
lla v
acci
neVA
Rva
ricel
la v
acci
ne
RZV
reco
mbi
nant
zos
ter v
acci
neZV
Lzo
ster
vac
cine
live
HPV
vac
cine
hum
an p
apill
omav
irus
vacc
ine
PCV1
313
-val
ent p
neum
ococ
cal c
onju
gate
vac
cine
PPSV
2323
-val
ent p
neum
ococ
cal p
olys
acch
arid
e va
ccin
eH
epA
hepa
titis
A v
acci
neH
epA
-Hep
Bhe
patit
is A
vac
cine
and
hep
atiti
s B
vacc
ine
Hep
Bhe
patit
is B
vac
cine
Men
AC
WY
sero
grou
ps A
, C, W
, and
Y m
enin
goco
ccal
vac
cine
Men
Bse
rogr
oup
B m
enin
goco
ccal
vac
cine
Hib
Hae
mop
hilu
s infl
uenz
ae ty
pe b
vac
cine
1. M
MW
R M
orb
Mor
tal W
kly
Rep.
201
8;66
(5):x
x–xx
. Ava
ilabl
e at
ww
w.c
dc.g
ov/m
mw
r/vo
lum
es/6
7/xx
xxxx
xxxx
.2.
Ann
Inte
rn M
ed. 2
018;
168:
xxx–
xxx.
Ava
ilabl
e at
ann
als.
org/
aim
/art
icle
/doi
/10.
7326
/M17
-343
9.3.
Clin
Infe
ct D
is. 2
014;
58:e
44-1
00. A
vaila
ble
at w
ww
.idso
ciet
y.or
g/Te
mpl
ates
/Con
tent
.asp
x?id
=32
2122
5601
1.4.
Kro
ger e
t al.
Ava
ilabl
e at
ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/ge
nera
l-rec
s/in
dex.
htm
l.

A-10
Figu
re 1
. Rec
omm
end
ed im
mun
izat
ion
sche
dul
e fo
r ad
ults
age
d 1
9 ye
ars
or o
lder
by
age
grou
p, U
nite
d S
tate
s, 2
018
This
figu
re s
houl
d be
revi
ewed
with
the
acco
mpa
nyin
g fo
otno
tes.
This
figu
re a
nd th
e fo
otno
tes
desc
ribe
indi
catio
ns fo
r whi
ch v
acci
nes,
if no
t pre
viou
sly
adm
inis
tere
d, s
houl
d be
adm
inis
tere
d un
less
not
ed o
ther
wis
e.
Vac
cin
e19
–21
year
s22
–26
year
s27
–49
year
s50
–64
year
s≥
65 y
ears
Infl
uen
za1
Tdap
2 or T
d2
MM
R3
VA
R4
RZ
V5
(pre
ferr
ed)
ZV
L5
HP
V–F
emal
e6
HP
V–M
ale6
PCV
137
PP
SV23
7
Hep
A8
Hep
B9
Men
AC
WY
10
Men
B10
Hib
11
1 d
ose
annu
ally
1 d
ose
ZVL
2 d
oses
RZV
(pre
ferr
ed)
1 d
ose
1 d
ose
2 or
3 d
oses
dep
end
ing
on a
ge a
t ser
ies
init
iati
on
2 or
3 d
oses
dep
end
ing
on a
ge a
t ser
ies
init
iati
on
1 or
2 d
oses
dep
end
ing
on in
dic
atio
n (if
bor
n in
195
7 or
late
r)
1 d
ose
Tdap
, the
n Td
boo
ster
eve
ry 1
0 yr
s
1 or
2 d
oses
dep
end
ing
on in
dic
atio
n
2 or
3 d
oses
dep
end
ing
on v
acci
ne
3 d
oses
2 d
oses
1 or
2 d
oses
dep
end
ing
on in
dic
atio
n, th
en b
oost
er e
very
5 y
rs if
risk
rem
ains
2 or
3 d
oses
dep
end
ing
on v
acci
ne
1 or
3 d
oses
dep
end
ing
on in
dic
atio
n
Reco
mm
ende
d fo
r adu
lts
who
mee
t the
ag
e re
quire
men
t, la
ck d
ocum
enta
tion
of
vacc
inat
ion,
or l
ack
evid
ence
of p
ast i
nfec
tion
Reco
mm
ende
d fo
r adu
lts
with
oth
er
indi
catio
nsN
o re
com
men
datio
n
oror

A-11
Figu
re 2
. Rec
omm
end
ed im
mun
izat
ion
sche
dul
e fo
r ad
ults
age
d 1
9 ye
ars
or o
lder
by
med
ical
con
dit
ion
and
oth
er in
dic
atio
ns, U
nite
d S
tate
s, 2
018
This
figu
re s
houl
d be
revi
ewed
with
the
acco
mpa
nyin
g fo
otno
tes.
This
figu
re a
nd th
e fo
otno
tes
desc
ribe
indi
catio
ns fo
r whi
ch v
acci
nes,
if no
t pre
viou
sly
adm
inis
tere
d, s
houl
d be
adm
inis
tere
d un
less
not
ed o
ther
wis
e.
Vac
cin
ePr
egna
ncy1-
6
Imm
uno
-co
mp
rom
ised
(e
xclu
din
g H
IV
infe
ctio
n)3-
7,11
HIV
infe
ctio
nC
D4+
cou
nt
(cel
ls/μ
L)3-
7,9-
10A
sple
nia,
co
mp
lem
ent
defi
cien
cies
7,10
,11
End
-sta
ge re
nal
dis
ease
, on
he
mod
ialy
sis7,
9
Hea
rt o
rlu
ng d
isea
se,
alco
holis
m7
Chr
onic
live
r d
isea
se7-
9D
iab
etes
7,9
Hea
lth
care
per
sonn
el3,
4,9
Men
who
ha
ve s
ex
wit
h m
en6,
8,9
<20
0≥
200
Infl
uen
za1
Tdap
2 or T
d2
1 d
ose
Td
ap e
ach
p
reg
nan
cy
MM
R3
VA
R4
RZ
V5
(pre
ferr
ed)
ZV
L5
HP
V–F
emal
e63
do
ses
thro
ug
h a
ge
26 y
rs
HP
V–M
ale6
2 o
r 3 d
ose
s
thro
ug
h a
ge
26 y
rs
PCV
137
PP
SV23
7
Hep
A8
Hep
B9
Men
AC
WY
10
Men
B10
Hib
113
do
ses
HSC
T
reci
pie
nts
on
ly
Reco
mm
ende
d fo
r adu
lts
who
mee
t the
ag
e re
quire
men
t, la
ck d
ocum
enta
tion
of
vacc
inat
ion,
or l
ack
evid
ence
of p
ast i
nfec
tion
Reco
mm
ende
d fo
r adu
lts
with
oth
er
indi
catio
nsC
ontr
aind
icat
edN
o re
com
men
datio
n
3 d
ose
s
2 o
r 3 d
ose
s d
epen
din
g o
n v
acci
ne
1 d
ose
1 d
ose
1, 2
, or 3
do
ses
dep
end
ing
on
ind
icat
ion
2 o
r 3 d
ose
s d
epen
din
g o
n v
acci
ne
1 o
r 2 d
ose
s d
epen
din
g o
n in
dic
atio
n ,
then
bo
ost
er e
very
5 y
rs if
risk
rem
ain
s
2 d
ose
s R
ZV
at a
ge
>50
yrs
(pre
ferr
ed)
con
trai
nd
icat
ed
con
trai
nd
icat
ed
1 o
r 2 d
ose
s d
epen
din
g o
n in
dic
atio
n
2 o
r 3 d
ose
s th
rou
gh
ag
e 26
yrs
2 d
ose
s
3 d
ose
s th
rou
gh
ag
e 26
yrs
1 d
ose
annu
ally
1 d
ose
Tdap
, the
n Td
boo
ster
eve
ry 1
0 yr
s
2 o
r 3 d
ose
s th
rou
gh
ag
e 21
yrs
1 d
ose
ZV
L at
ag
e >
60 y
rsco
ntr
ain
dic
ated
oror

A-12
Foo
tno
tes.
Rec
omm
ende
d im
mun
izat
ion
sche
dule
for a
dult
s ag
ed 1
9 ye
ars
or o
lder
, Uni
ted
Stat
es, 2
018
1.
Infl
uen
za v
acci
nat
ion
ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/va
cc-s
peci
fic/fl
u.ht
ml
Gen
eral
info
rmat
ion
• A
dmin
iste
r 1 d
ose
of a
ge-a
pp
rop
riate
inac
tivat
ed in
fluen
za
vacc
ine
(IIV
) or r
ecom
bin
ant i
nflue
nza
vacc
ine
(RIV
) ann
ually
• Li
ve a
tten
uate
d in
fluen
za v
acci
ne (L
AIV
) is
not r
ecom
men
ded
for t
he 2
017–
2018
influ
enza
sea
son
• A
list
of c
urre
ntly
ava
ilab
le in
fluen
za v
acci
nes
is a
vaila
ble
at
ww
w.c
dc.g
ov/fl
u/p
rote
ct/v
acci
ne/v
acci
nes.
htm
Spec
ial p
opul
atio
ns•
Adm
inis
ter a
ge-a
pp
rop
riate
IIV
or R
IV to
: ʱPr
egn
ant w
om
en ʱA
dult
s w
ith h
ives
-on
ly e
gg
alle
rgy
ʱA
dult
s w
ith e
gg
alle
rgy
oth
er th
an h
ives
(e.g
., an
gioe
dem
a or
resp
irato
ry d
istr
ess)
: Adm
inis
ter I
IV o
r RIV
in
a m
edic
al s
ettin
g un
der s
uper
visi
on o
f a h
ealt
h ca
re
pro
vide
r who
can
reco
gniz
e an
d m
anag
e se
vere
alle
rgic
co
nditi
ons
2.
Teta
nus,
dip
hthe
ria,
and
per
tuss
is v
acci
nati
onw
ww
.cdc
.gov
/vac
cine
s/hc
p/ac
ip-r
ecs/
vacc
-spe
cific
/tda
p-t
d.ht
ml
Gen
eral
info
rmat
ion
• A
dmin
iste
r to
adul
ts w
ho p
revi
ousl
y di
d no
t rec
eive
a d
ose
of te
tanu
s to
xoid
, red
uced
dip
hthe
ria to
xoid
, and
ace
llula
r p
ertu
ssis
vac
cine
(Tda
p) a
s an
adu
lt o
r chi
ld (r
outin
ely
reco
mm
ende
d at
age
11–
12 y
ears
) 1 d
ose
of T
dap,
follo
wed
by
a d
ose
of te
tanu
s an
d di
pht
heria
toxo
ids
(Td)
boo
ster
ev
ery
10 y
ears
• In
form
atio
n on
the
use
of T
dap
or T
d as
teta
nus
pro
phy
laxi
s in
wou
nd m
anag
emen
t is
avai
lab
le a
t ww
w.c
dc.g
ov/m
mw
r/p
revi
ew/m
mw
rhtm
l/rr
5517
a1.h
tm
Spec
ial p
opul
atio
ns•
Preg
nan
t wo
men
: Adm
inis
ter 1
dos
e of
Tda
p d
urin
g ea
ch
pre
gnan
cy, p
refe
rab
ly in
the
earl
y p
art o
f ges
tatio
nal w
eeks
27
–36
3.
Mea
sles
, mu
mp
s, a
nd
rub
ella
vac
cin
atio
nw
ww
.cdc
.gov
/vac
cine
s/hc
p/ac
ip-r
ecs/
vacc
-spe
cific
/mm
r.htm
l
Gen
eral
info
rmat
ion
• A
dmin
iste
r 1 d
ose
of m
easl
es, m
ump
s, a
nd ru
bel
la v
acci
ne
(MM
R) to
adu
lts
with
no
evid
ence
of i
mm
unit
y to
mea
sles
, m
ump
s, o
r rub
ella
• Ev
iden
ce o
f im
mun
ity
is:
ʱBo
rn b
efor
e 19
57 (e
xcep
t for
hea
lth
care
per
sonn
el, s
ee
bel
ow)
ʱD
ocum
enta
tion
of re
ceip
t of M
MR
ʱLa
bor
ator
y ev
iden
ce o
f im
mun
ity
or d
isea
se•
Doc
umen
tatio
n of
a h
ealt
h ca
re p
rovi
der-
diag
nose
d di
seas
e w
ithou
t lab
orat
ory
confi
rmat
ion
is n
ot c
onsi
dere
d ev
iden
ce
of im
mun
ity
Spec
ial p
opul
atio
ns•
Preg
nan
t wo
men
an
d n
on
pre
gn
ant w
om
en o
f ch
ildb
eari
ng
ag
e w
ith n
o ev
iden
ce o
f im
mun
ity
to ru
bel
la:
Adm
inis
ter 1
dos
e of
MM
R (if
pre
gnan
t, ad
min
iste
r MM
R af
ter
pre
gnan
cy a
nd b
efor
e di
scha
rge
from
hea
lth
care
faci
lity)
• H
IV in
fect
ion
an
d C
D4
cell
cou
nt ≥
200
cells
/μL
for
at le
ast
6 m
on
ths
and
no e
vide
nce
of im
mun
ity
to m
easl
es, m
ump
s,
or ru
bel
la: A
dmin
iste
r 2 d
oses
of M
MR
at le
ast 2
8 da
ys a
par
t •
Stu
den
ts in
po
stse
con
dar
y ed
uca
tio
nal
inst
itu
tio
ns,
in
tern
atio
nal
trav
eler
s, a
nd h
ou
seh
old
co
nta
cts
of
imm
un
oco
mp
rom
ised
per
son
s: A
dmin
iste
r 2 d
oses
of
MM
R at
leas
t 28
days
ap
art (
or 1
dos
e of
MM
R if
pre
viou
sly
adm
inis
tere
d 1
dose
of M
MR)
• H
ealt
h c
are
per
son
nel
bo
rn in
195
7 o
r la
ter
with
no
evid
ence
of i
mm
unit
y: A
dmin
iste
r 2 d
oses
of M
MR
at le
ast
28 d
ays
apar
t for
mea
sles
or m
ump
s, o
r 1 d
ose
of M
MR
for
rub
ella
(if b
orn
bef
ore
1957
, con
side
r MM
R va
ccin
atio
n)•
Adu
lts
who
pre
vio
usl
y re
ceiv
ed ≤
2 d
ose
s o
f mu
mp
s-co
nta
inin
g v
acci
ne
and
are
iden
tifi
ed b
y p
ub
lic h
ealt
h
auth
ori
ty to
be
at in
crea
sed
ris
k fo
r m
um
ps
in a
n
ou
tbre
ak: A
dmin
iste
r 1 d
ose
of M
MR
• M
MR
is c
ontr
aind
icat
ed fo
r pre
gnan
t wom
en a
nd a
dult
s w
ith
seve
re im
mun
odefi
cien
cy
4.
Var
icel
la v
acci
nat
ion
ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/va
cc-s
peci
fic/v
aric
ella
.htm
l
Gen
eral
info
rmat
ion
• A
dmin
iste
r to
adul
ts w
ithou
t evi
denc
e of
imm
unit
y to
va
ricel
la 2
dos
es o
f var
icel
la v
acci
ne (V
AR)
4–8
wee
ks a
par
t if
pre
viou
sly
rece
ived
no
varic
ella
-con
tain
ing
vacc
ine
(if
pre
viou
sly
rece
ived
1 d
ose
of v
aric
ella
-con
tain
ing
vacc
ine,
ad
min
iste
r 1 d
ose
of V
AR
at le
ast 4
wee
ks a
fter
the
first
dos
e)
• Ev
iden
ce o
f im
mun
ity
to v
aric
ella
is:
ʱU
.S.-b
orn
bef
ore
1980
(exc
ept f
or p
regn
ant w
omen
and
he
alth
car
e p
erso
nnel
, see
bel
ow)
ʱD
ocum
enta
tion
of re
ceip
t of 2
dos
es o
f var
icel
la o
r va
ricel
la-c
onta
inin
g va
ccin
e at
leas
t 4 w
eeks
ap
art
ʱD
iagn
osis
or v
erifi
catio
n of
his
tory
of v
aric
ella
or h
erp
es
zost
er b
y a
heal
th c
are
pro
vide
r ʱLa
bor
ator
y ev
iden
ce o
f im
mun
ity
or d
isea
se
Spec
ial p
opul
atio
ns•
Adm
inis
ter 2
dos
es o
f VA
R 4–
8 w
eeks
ap
art i
f pre
viou
sly
rece
ived
no
varic
ella
-con
tain
ing
vacc
ine
(if p
revi
ousl
y re
ceiv
ed 1
dos
e of
var
icel
la-c
onta
inin
g va
ccin
e, a
dmin
iste
r 1
dose
of V
AR
at le
ast 4
wee
ks a
fter
the
first
dos
e) to
: ʱPr
egn
ant w
om
en w
ith
ou
t evi
den
ce o
f im
mu
nit
y:
Adm
inis
ter t
he fi
rst o
f the
2 d
oses
or t
he s
econ
d do
se a
fter
p
regn
ancy
and
bef
ore
disc
harg
e fr
om h
ealt
h ca
re fa
cilit
y ʱH
ealt
h c
are
per
son
nel
wit
ho
ut e
vid
ence
of i
mm
un
ity
• A
dult
s w
ith H
IV in
fect
ion
an
d C
D4
cell
cou
nt ≥
200
cells
/μL:
M
ay a
dmin
iste
r, b
ased
on
indi
vidu
al c
linic
al d
ecis
ion,
2 d
oses
of
VA
R 3
mon
ths
apar
t•
VAR
is c
ontr
aind
icat
ed fo
r pre
gnan
t wom
en a
nd a
dult
s w
ith
seve
re im
mun
odefi
cien
cy
5.
Zost
er v
acci
nat
ion
ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/va
cc-s
peci
fic/s
hing
les.
htm
l
Gen
eral
info
rmat
ion
• A
dmin
iste
r 2 d
oses
of r
ecom
bina
nt z
oste
r vac
cine
(RZV
) 2–6
m
onth
s ap
art t
o ad
ults
age
d 50
yea
rs o
r old
er re
gard
less
of
past
epi
sode
of h
erpe
s zo
ster
or r
ecei
pt o
f zos
ter v
acci
ne li
ve
(ZVL
)
• A
dmin
iste
r 2 d
oses
of R
ZV 2
–6 m
onth
s ap
art t
o ad
ults
who
p
revi
ousl
y re
ceiv
ed Z
VL a
t lea
st 2
mon
ths
afte
r ZVL
• Fo
r adu
lts
aged
60
year
s or
old
er, a
dmin
iste
r eith
er R
ZV o
r ZV
L (R
ZV is
pre
ferr
ed)
Spec
ial p
opul
atio
ns•
ZVL
is c
ontr
aind
icat
ed fo
r pre
gnan
t wom
en a
nd a
dult
s w
ith
seve
re im
mun
odefi
cien
cy
6.
Hu
man
pap
illom
avir
us
vacc
inat
ion
ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/va
cc-s
peci
fic/h
pv.h
tml
Gen
eral
info
rmat
ion
• A
dmin
iste
r hum
an p
apill
omav
irus
(HPV
) vac
cine
to fe
mal
es
thro
ug
h a
ge
26 y
ears
and
mal
es th
rou
gh
ag
e 21
yea
rs
(mal
es a
ged
22 th
roug
h 26
yea
rs m
ay b
e va
ccin
ated
bas
ed
on in
divi
dual
clin
ical
dec
isio
n)
• Th
e nu
mb
er o
f dos
es o
f HPV
vac
cine
to b
e ad
min
iste
red
dep
ends
on
age
at in
itial
HPV
vac
cina
tion
ʱN
o p
revi
ou
s d
ose
of H
PV
vac
cin
e: A
dmin
iste
r 3-d
ose
serie
s at
0, 1
–2, a
nd 6
mon
ths
(min
imum
inte
rval
s: 4
wee
ks
bet
wee
n do
ses
1 an
d 2,
12
wee
ks b
etw
een
dose
s 2
and
3,
and
5 m
onth
s b
etw
een
dose
s 1
and
3; re
pea
t dos
es if
giv
en
too
soon
) ʱA
ged
9–1
4 ye
ars
at H
PV
vac
cin
e se
ries
init
iati
on
an
d
rece
ived
1 d
ose
or
2 d
ose
s le
ss th
an 5
mo
nth
s ap
art:
A
dmin
iste
r 1 d
ose
ʱA
ged
9–1
4 ye
ars
at H
PV
vac
cin
e se
ries
init
iati
on
an
d
rece
ived
2 d
ose
s at
leas
t 5 m
on
ths
apar
t: N
o ad
ditio
nal
dose
is n
eede
d
Spec
ial p
opul
atio
ns•
Adu
lts
with
imm
un
oco
mp
rom
isin
g c
on
dit
ion
s (i
ncl
ud
ing
H
IV in
fect
ion
) thr
ough
age
26
year
s: A
dmin
iste
r 3-d
ose
serie
s at
0, 1
–2, a
nd 6
mon
ths
• M
en w
ho
hav
e se
x w
ith
men
thro
ugh
age
26 y
ears
: A
dmin
iste
r 2- o
r 3-d
ose
serie
s de
pen
ding
on
age
at in
itial
va
ccin
atio
n (s
ee a
bov
e); i
f no
hist
ory
of H
PV v
acci
ne,
adm
inis
ter 3
-dos
e se
ries
at 0
, 1–2
, and
6 m
onth
s•
Preg
nan
t wo
men
thro
ugh
age
26 y
ears
: HPV
vac
cina
tion
is n
ot re
com
men
ded
durin
g p
regn
ancy
, but
ther
e is
no
evid
ence
that
the
vacc
ine
is h
arm
ful a
nd n
o in
terv
entio
n ne
eded
for w
omen
who
inad
vert
entl
y re
ceiv
e H
PV v
acci
ne
whi
le p
regn
ant;
dela
y re
mai
ning
dos
es u
ntil
afte
r pre
gnan
cy;
pre
gnan
cy te
stin
g is
not
nee
ded
bef
ore
vacc
inat
ion
7.
Pneu
moc
occa
l vac
cin
atio
nw
ww
.cdc
.gov
/vac
cine
s/hc
p/ac
ip-r
ecs/
vacc
-spe
cific
/pne
umo.
htm
l
Gen
eral
info
rmat
ion
• A
dmin
iste
r to
imm
unoc
omp
eten
t adu
lts
aged
65
year
s or
ol
der 1
dos
e of
13-
vale
nt p
neum
ococ
cal c
onju
gate
vac
cine
(P
CV1
3), i
f not
pre
viou
sly
adm
inis
tere
d, fo
llow
ed b
y 1
dose
of 2
3-va
lent
pne
umoc
occa
l pol
ysac
char
ide
vacc
ine
(PPS
V23)
at l
east
1 y
ear a
fter
PC
V13;
if P
PSV2
3 w
as p
revi
ousl
y ad
min
iste
red
but
not
PC
V13,
adm
inis
ter P
CV1
3 at
leas
t 1 y
ear
afte
r PPS
V23
• W
hen
bot
h PC
V13
and
PPSV
23 a
re in
dica
ted,
adm
inis
ter
PCV1
3 fir
st (P
CV1
3 an
d PP
SV23
sho
uld
not b
e ad
min
iste
red
durin
g th
e sa
me
visi
t); a
dditi
onal
info
rmat
ion
on v
acci
ne
timin
g is
ava
ilab
le a
t ww
w.c
dc.g
ov/v
acci
nes/
vpd/
pne
umo/
dow
nloa
ds/p
neum
o-va
ccin
e-tim
ing.

A-13
Spec
ial p
opul
atio
ns•
Adm
inis
ter t
o ad
ults
age
d 1
9 th
roug
h 64
yea
rs w
ith th
e fo
llow
ing
chro
nic
cond
ition
s 1
dose
of P
PSV2
3 (a
t age
65
year
s or
old
er, a
dmin
iste
r 1 d
ose
of P
CV1
3, if
not
pre
viou
sly
rece
ived
, and
ano
ther
dos
e of
PPS
V23
at le
ast 1
yea
r aft
er
PCV1
3 an
d at
leas
t 5 y
ears
aft
er P
PSV2
3):
ʱC
hro
nic
hea
rt d
isea
se (e
xclu
ding
hyp
erte
nsio
n) ʱC
hro
nic
lun
g d
isea
se ʱC
hro
nic
live
r d
isea
se ʱA
lco
ho
lism
ʱD
iab
etes
mel
litu
s ʱC
igar
ette
sm
oki
ng
• A
dmin
iste
r to
adul
ts a
ged
19 y
ears
or o
lder
with
the
follo
win
g in
dica
tions
1 d
ose
of P
CV1
3 fo
llow
ed b
y 1
dose
of
PPSV
23 a
t lea
st 8
wee
ks a
fter
PC
V13,
and
a s
econ
d do
se o
f PP
SV23
at l
east
5 y
ears
aft
er th
e fir
st d
ose
of P
PSV2
3 (if
the
mos
t rec
ent d
ose
of P
PSV2
3 w
as a
dmin
iste
red
bef
ore
age
65
year
s, a
t age
65
year
s or
old
er, a
dmin
iste
r ano
ther
dos
e of
PP
SV23
at l
east
5 y
ears
aft
er th
e la
st d
ose
of P
PSV2
3):
ʱIm
mu
no
defi
cien
cy d
iso
rder
s (in
clud
ing
B- a
nd
T-ly
mp
hocy
te d
efici
ency
, com
ple
men
t defi
cien
cies
, and
p
hago
cytic
dis
orde
rs)
ʱH
IV in
fect
ion
ʱA
nat
om
ical
or
fun
ctio
nal
asp
len
ia (i
nclu
ding
sic
kle
cell
dise
ase
and
othe
r hem
oglo
bin
opat
hies
) ʱC
hro
nic
ren
al fa
ilure
an
d n
eph
roti
c sy
nd
rom
e•
Adm
inis
ter t
o ad
ults
age
d 19
yea
rs o
r old
er w
ith th
e fo
llow
ing
indi
catio
ns 1
dos
e of
PC
V13
follo
wed
by
1 do
se o
f PP
SV23
at l
east
8 w
eeks
aft
er P
CV1
3 (if
the
dose
of P
PSV2
3 w
as a
dmin
iste
red
bef
ore
age
65 y
ears
, at a
ge 6
5 ye
ars
or
olde
r, ad
min
iste
r ano
ther
dos
e of
PPS
V23
at le
ast 5
yea
rs
afte
r the
last
dos
e of
PPS
V23)
: ʱC
ereb
rosp
inal
flu
id le
ak ʱC
och
lear
imp
lan
t
8.
Hep
atit
is A
vac
cin
atio
nw
ww
.cdc
.gov
/vac
cine
s/hc
p/ac
ip-r
ecs/
vacc
-spe
cific
/hep
a.ht
ml
Gen
eral
info
rmat
ion
• A
dmin
iste
r to
adul
ts w
ho h
ave
a sp
ecifi
c ris
k (s
ee b
elow
), or
lack
a ri
sk fa
ctor
but
wan
t pro
tect
ion,
2-d
ose
serie
s of
si
ngle
ant
igen
hep
atiti
s A
vac
cine
(Hep
A; H
avrix
at 0
and
6–
12 m
onth
s or
Vaq
ta a
t 0 a
nd 6
–18
mon
ths;
min
imum
in
terv
al: 6
mon
ths)
or a
3-d
ose
serie
s of
com
bin
ed h
epat
itis
A a
nd h
epat
itis
B va
ccin
e (H
epA
-Hep
B) a
t 0, 1
, and
6 m
onth
s;
min
imum
inte
rval
s: 4
wee
ks b
etw
een
first
and
sec
ond
dose
s,
5 m
onth
s b
etw
een
seco
nd a
nd th
ird d
oses
Spec
ial p
opul
atio
ns•
Adm
inis
ter H
epA
or H
epA
-Hep
B to
adu
lts
with
the
follo
win
g in
dica
tions
: ʱTr
avel
to o
r wor
k in
cou
ntrie
s w
ith h
igh
or in
term
edia
te
hep
atiti
s A
end
emic
ity
ʱM
en w
ho
hav
e se
x w
ith
men
ʱIn
ject
ion
or
no
nin
ject
ion
dru
g u
se ʱW
ork
wit
h h
epat
itis
A v
iru
s in
a r
esea
rch
lab
ora
tory
o
r w
ith
no
nh
um
an p
rim
ates
infe
cted
wit
h h
epat
itis
A
viru
s ʱC
lott
ing
fact
or
dis
ord
ers
ʱC
hro
nic
live
r d
isea
se
ʱC
lose
, per
sona
l co
nta
ct w
ith
an
inte
rnat
ion
al a
do
pte
e (e
.g.,
hous
ehol
d or
regu
lar b
abys
ittin
g) d
urin
g th
e fir
st 6
0 da
ys a
fter
arr
ival
in th
e U
nite
d St
ates
from
a c
ount
ry w
ith
high
or i
nter
med
iate
end
emic
ity
(adm
inis
ter t
he fi
rst d
ose
as s
oon
as th
e ad
optio
n is
pla
nned
) ʱH
ealt
hy a
dult
s th
rou
gh
ag
e 40
yea
rs w
ho
hav
e re
cen
tly
bee
n e
xpo
sed
to h
epat
itis
A v
iru
s; a
dult
s ol
der t
han
age
40 y
ears
may
rece
ive
Hep
A o
r Hep
A-H
epB
if he
pat
itis
A
imm
unog
lob
ulin
can
not b
e ob
tain
ed
9.
Hep
atit
is B
vac
cin
atio
nw
ww
.cdc
.gov
/vac
cine
s/hc
p/ac
ip-r
ecs/
vacc
-spe
cific
/hep
b.ht
ml
Gen
eral
info
rmat
ion
• A
dmin
iste
r to
adul
ts w
ho h
ave
a sp
ecifi
c ris
k (s
ee b
elow
), or
la
ck a
risk
fact
or b
ut w
ant p
rote
ctio
n, 3
-dos
e se
ries
of s
ingl
e an
tigen
hep
atiti
s B
vacc
ine
(Hep
B) o
r com
bin
ed h
epat
itis
A
and
hep
atiti
s B
vacc
ine
(Hep
A-H
epB)
at 0
, 1, a
nd 6
mon
ths
(min
imum
inte
rval
s: 4
wee
ks b
etw
een
dose
s 1
and
2 fo
r H
epB
and
Hep
A-H
epB;
bet
wee
n do
ses
2 an
d 3,
8 w
eeks
for
Hep
B an
d 5
mon
ths
for H
epA
-Hep
B)
Spec
ial p
opul
atio
ns•
Adm
inis
ter H
epB
or H
epA
-Hep
B to
adu
lts
with
the
follo
win
g in
dica
tions
: ʱC
hro
nic
live
r d
isea
se (e
.g.,
hep
atiti
s C
infe
ctio
n, c
irrho
sis,
fa
tty
liver
dis
ease
, alc
ohol
ic li
ver d
isea
se, a
utoi
mm
une
hep
atiti
s, a
lani
ne a
min
otra
nsfe
rase
[ALT
] or a
spar
tate
am
inot
rans
fera
se [A
ST] l
evel
gre
ater
than
twic
e th
e up
per
lim
it of
nor
mal
) ʱH
IV in
fect
ion
ʱPe
rcu
tan
eou
s o
r m
uco
sal r
isk
of e
xpo
sure
to b
loo
d
(e.g
., h
ou
seh
old
co
nta
cts
of h
epat
itis
B su
rfac
e an
tigen
[H
BsA
g]-p
ositi
ve p
erso
ns; a
dult
s yo
unge
r tha
n ag
e 60
ye
ars
with
dia
bet
es m
ellit
us
or a
ged
60 y
ears
or o
lder
w
ith d
iab
etes
mel
litus
bas
ed o
n in
divi
dual
clin
ical
dec
isio
n;
adul
ts in
pre
dial
ysis
car
e or
rece
ivin
g h
emo
dia
lysi
s o
r p
erit
on
eal d
ialy
sis;
rece
nt o
r cur
rent
inje
ctio
n d
rug
u
sers
; hea
lth
car
e an
d p
ub
lic s
afet
y w
ork
ers
at ri
sk fo
r ex
pos
ure
to b
lood
or b
lood
-con
tam
inat
ed b
ody
fluid
s) ʱSe
xual
exp
osu
re r
isk
(e.g
., se
x p
artn
ers
of H
BsA
g-p
ositi
ve p
erso
ns; s
exua
lly a
ctiv
e p
erso
ns n
ot in
a m
utua
lly
mon
ogam
ous
rela
tions
hip
; per
sons
see
king
eva
luat
ion
or
trea
tmen
t for
a s
exua
lly tr
ansm
itted
infe
ctio
n; a
nd m
en
wh
o h
ave
sex
wit
h m
en [M
SM])
ʱRe
ceiv
e ca
re in
set
tin
gs
wh
ere
a h
igh
pro
po
rtio
n o
f ad
ult
s h
ave
risk
s fo
r h
epat
itis
B in
fect
ion
(e.g
., fa
cilit
ies
pro
vidi
ng s
exua
lly tr
ansm
itted
dis
ease
trea
tmen
t, dr
ug-
abus
e tr
eatm
ent a
nd p
reve
ntio
n se
rvic
es, h
emod
ialy
sis
and
end-
stag
e re
nal d
isea
se p
rogr
ams,
inst
itutio
ns fo
r de
velo
pm
enta
lly d
isab
led
per
sons
, hea
lth
care
set
tings
ta
rget
ing
serv
ices
to in
ject
ion
drug
use
rs o
r MSM
, HIV
te
stin
g an
d tr
eatm
ent f
acili
ties,
and
cor
rect
iona
l fac
ilitie
s) ʱTr
avel
to c
ount
ries
with
hig
h or
inte
rmed
iate
hep
atiti
s B
ende
mic
ity
10. M
enin
goc
occa
l vac
cin
atio
nw
ww
.cdc
.gov
/vac
cine
s/hc
p/ac
ip-r
ecs/
vacc
-spe
cific
/men
ing.
htm
l
Spec
ial p
opul
atio
ns: S
erog
roup
s A
, C, W
, and
Y
men
ingo
cocc
al v
acci
ne (M
enA
CW
Y)
• A
dmin
iste
r 2 d
oses
of M
enA
CW
Y at
leas
t 8 w
eeks
ap
art a
nd
reva
ccin
ate
with
1 d
ose
of M
enA
CW
Y ev
ery
5 ye
ars,
if th
e ris
k re
mai
ns, t
o ad
ults
with
the
follo
win
g in
dica
tions
: ʱA
nat
om
ical
or
fun
ctio
nal
asp
len
ia (i
nclu
ding
sic
kle
cell
dise
ase
and
othe
r hem
oglo
bin
opat
hies
) ʱH
IV in
fect
ion
ʱPe
rsis
ten
t co
mp
lem
ent c
om
po
nen
t defi
cien
cy ʱEc
uliz
um
ab u
se•
Adm
inis
ter 1
dos
e of
Men
AC
WY
and
reva
ccin
ate
with
1 d
ose
of M
enA
CW
Y ev
ery
5 ye
ars,
if th
e ris
k re
mai
ns, t
o ad
ults
with
th
e fo
llow
ing
indi
catio
ns:
ʱTr
avel
to o
r liv
e in
co
un
trie
s w
her
e m
enin
go
cocc
al
dis
ease
is h
yper
end
emic
or
epid
emic
, inc
ludi
ng
coun
trie
s in
the
Afr
ican
men
ingi
tis b
elt o
r dur
ing
the
Haj
j ʱA
t ris
k fr
om a
men
ing
oco
ccal
dis
ease
ou
tbre
ak
attr
ibu
ted
to s
ero
gro
up
A, C
, W, o
r Y ʱM
icro
bio
log
ists
rout
inel
y ex
pos
ed to
Nei
sser
ia
men
ingi
tidis
ʱM
ilita
ry r
ecru
its
ʱFi
rst-
year
co
lleg
e st
ud
ents
wh
o li
ve in
res
iden
tial
h
ou
sin
g (i
f the
y di
d no
t rec
eive
Men
AC
WY
at a
ge 1
6 ye
ars
or o
lder
)G
ener
al In
form
atio
n: S
erog
roup
B m
enin
goco
ccal
vac
cine
(M
enB
) ʱM
ay a
dmin
iste
r, b
ased
on
indi
vidu
al c
linic
al d
ecis
ion,
to
youn
g ad
ults
and
ado
lesc
ents
age
d 16
–23
year
s (p
refe
rred
ag
e is
16–
18 y
ears
) who
are
not
at i
ncre
ased
risk
2-d
ose
serie
s of
Men
B-4C
(Bex
sero
) at l
east
1 m
onth
ap
art o
r 2-
dose
ser
ies
of M
enB-
FHb
p (T
rum
enb
a) a
t lea
st 6
mon
ths
apar
t ʱM
enB-
4C a
nd M
enB-
FHb
p a
re n
ot in
terc
hang
eab
le
Spec
ial p
opul
atio
ns: M
enB
• A
dmin
iste
r 2-d
ose
serie
s of
Men
B-4C
at l
east
1 m
onth
ap
art
or 3
-dos
e se
ries
of M
enB-
FHb
p a
t 0, 1
–2, a
nd 6
mon
ths
to
adul
ts w
ith th
e fo
llow
ing
indi
catio
ns:
ʱA
nat
om
ical
or
fun
ctio
nal
asp
len
ia (i
nclu
ding
sic
kle
cell
dise
ase)
ʱPe
rsis
ten
t co
mp
lem
ent c
om
po
nen
t defi
cien
cy ʱEc
uliz
um
ab u
se ʱA
t ris
k fr
om a
men
ing
oco
ccal
dis
ease
ou
tbre
ak
attr
ibu
ted
to s
ero
gro
up
B ʱM
icro
bio
log
ists
rout
inel
y ex
pos
ed to
Nei
sser
ia
men
ingi
tidis
11. H
aem
ophi
lus
influ
enza
e ty
pe
b v
acci
nat
ion
ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/va
cc-s
peci
fic/h
ib.h
tml
Spec
ial p
opul
atio
ns•
Adm
inis
ter H
aem
ophi
lus i
nflue
nzae
typ
e b
vac
cine
(Hib
) to
adul
ts w
ith th
e fo
llow
ing
indi
catio
ns:
ʱA
nat
om
ical
or
fun
ctio
nal
asp
len
ia (i
nclu
ding
sic
kle
cell
dise
ase)
or u
nder
goin
g el
ectiv
e sp
lene
ctom
y: A
dmin
iste
r 1
dose
if n
ot p
revi
ousl
y va
ccin
ated
(pre
fera
bly
at l
east
14
days
bef
ore
elec
tive
sple
nect
omy)
ʱH
emat
op
oie
tic
stem
cel
l tra
nsp
lan
t (H
SCT)
: Adm
inis
ter
3-do
se s
erie
s w
ith d
oses
4 w
eeks
ap
art s
tart
ing
6 to
12
mon
ths
afte
r suc
cess
ful t
rans
pla
nt re
gard
less
of H
ib
vacc
inat
ion
hist
ory

A-14
Vac
cin
e(s)
Ad
dit
ion
al C
ontr
ain
dic
atio
ns
Ad
dit
ion
al P
reca
uti
ons
IIV1
• H
isto
ry o
f Gui
llain
-Bar
ré s
yndr
ome
with
in 6
wee
ks a
fter
pre
viou
s in
fluen
za v
acci
natio
n•
Egg
alle
rgy
othe
r tha
n hi
ves,
e.g
., an
gioe
dem
a, re
spira
tory
dis
tres
s, li
ghth
eade
dnes
s, o
r rec
urre
nt
emes
is; o
r req
uire
d ep
inep
hrin
e or
ano
ther
em
erge
ncy
med
ical
inte
rven
tion
(IIV
may
be
adm
inis
tere
d in
an
inpa
tient
or o
utpa
tient
med
ical
set
ting
and
unde
r the
sup
ervi
sion
of a
hea
lth
care
pro
vide
r who
is a
ble
to re
cogn
ize
and
man
age
seve
re a
llerg
ic c
ondi
tions
)RI
V1•
His
tory
of G
uilla
in-B
arré
syn
drom
e w
ithin
6 w
eeks
aft
er p
revi
ous
influ
enza
vac
cina
tion
Tdap
, Td
• Fo
r per
tuss
is-c
onta
inin
g va
ccin
es: e
ncep
halo
path
y, e
.g.,
com
a, d
ecre
ased
leve
l of c
onsc
ious
ness
, or
pro
long
ed s
eizu
res,
not
att
ribut
able
to a
noth
er id
entifi
able
cau
se w
ithin
7 d
ays
of
adm
inis
trat
ion
of a
pre
viou
s do
se o
f a v
acci
ne c
onta
inin
g te
tanu
s or
dip
hthe
ria to
xoid
or a
cellu
lar
pert
ussi
s
• G
uilla
in-B
arré
syn
drom
e w
ithin
6 w
eeks
aft
er a
pre
viou
s do
se o
f tet
anus
toxo
id-c
onta
inin
g va
ccin
e•
His
tory
of A
rthu
s-ty
pe h
yper
sens
itivi
ty re
actio
ns a
fter
a p
revi
ous
dose
of t
etan
us o
r dip
hthe
ria
toxo
id-c
onta
inin
g va
ccin
e. D
efer
vac
cina
tion
until
at l
east
10
year
s ha
ve e
laps
ed s
ince
the
last
te
tanu
s to
xoid
-con
tain
ing
vacc
ine
• Fo
r per
tuss
is-c
onta
inin
g va
ccin
e, p
rogr
essi
ve o
r uns
tabl
e ne
urol
ogic
dis
orde
r, un
cont
rolle
d se
izur
es, o
r pro
gres
sive
enc
epha
lopa
thy
(unt
il a
trea
tmen
t reg
imen
has
bee
n es
tabl
ishe
d an
d th
e co
nditi
on h
as s
tabi
lized
)M
MR2
• Se
vere
imm
unod
efici
ency
, e.g
., he
mat
olog
ic a
nd s
olid
tum
ors,
che
mot
hera
py, c
onge
nita
l im
mun
odefi
cien
cy o
r lon
g-te
rm im
mun
osup
pres
sive
ther
apy3 , h
uman
imm
unod
efici
ency
viru
s (H
IV) i
nfec
tion
with
sev
ere
imm
unoc
ompr
omis
e•
Preg
nanc
y
• Re
cent
(with
in 1
1 m
onth
s) re
ceip
t of a
ntib
ody-
cont
aini
ng b
lood
pro
duct
(spe
cific
inte
rval
de
pend
s on
pro
duct
)4
• H
isto
ry o
f thr
ombo
cyto
peni
a or
thro
mbo
cyto
peni
c pu
rpur
a•
Nee
d fo
r tub
ercu
lin s
kin
test
ing5
VAR2
• Se
vere
imm
unod
efici
ency
, e.g
., he
mat
olog
ic a
nd s
olid
tum
ors,
che
mot
hera
py, c
onge
nita
l im
mun
odefi
cien
cy o
r lon
g-te
rm im
mun
osup
pres
sive
ther
apy3 , H
IV in
fect
ion
with
sev
ere
imm
unoc
ompr
omis
e•
Preg
nanc
y
• Re
cent
(with
in 1
1 m
onth
s) re
ceip
t of a
ntib
ody-
cont
aini
ng b
lood
pro
duct
(spe
cific
inte
rval
de
pend
s on
pro
duct
)4
• Re
ceip
t of s
peci
fic a
ntiv
iral d
rugs
(acy
clov
ir, fa
mci
clov
ir, o
r val
acyc
lovi
r) 2
4 ho
urs
befo
re
vacc
inat
ion
(avo
id u
se o
f the
se a
ntiv
iral d
rugs
for 1
4 da
ys a
fter
vac
cina
tion)
ZVL2
• Se
vere
imm
unod
efici
ency
, e.g
., he
mat
olog
ic a
nd s
olid
tum
ors,
che
mot
hera
py, c
onge
nita
l im
mun
odefi
cien
cy o
r lon
g-te
rm im
mun
osup
pres
sive
ther
apy3 , H
IV in
fect
ion
with
sev
ere
imm
unoc
ompr
omis
e•
Preg
nanc
y
• Re
ceip
t of s
peci
fic a
ntiv
iral d
rugs
(acy
clov
ir, fa
mci
clov
ir, o
r val
acyc
lovi
r) 2
4 ho
urs
befo
re
vacc
inat
ion
(avo
id u
se o
f the
se a
ntiv
iral d
rugs
for 1
4 da
ys a
fter
vac
cina
tion)
HPV
vac
cine
• Pr
egna
ncy
PCV1
3•
Seve
re a
llerg
ic re
actio
n to
any
vac
cine
con
tain
ing
diph
ther
ia to
xoid
1. F
or a
dditi
onal
info
rmat
ion
on u
se o
f infl
uenz
a va
ccin
es a
mon
g pe
rson
s w
ith e
gg a
llerg
y, s
ee: C
DC
. Pre
vent
ion
and
cont
rol o
f sea
sona
l infl
uenz
a w
ith v
acci
nes:
reco
mm
enda
tions
of t
he A
dvis
ory
Com
mitt
ee o
n Im
mun
izat
ion
Prac
tices
—U
nite
d St
ates
, 201
6–17
influ
enza
sea
son.
MM
WR.
201
6;65
(RR-
5):1
–54.
Ava
ilabl
e at
ww
w.c
dc.g
ov/m
mw
r/vo
lum
es/6
5/rr
/rr6
505a
1.ht
m.
2. M
MR
may
be
adm
inis
tere
d to
geth
er w
ith V
AR
or Z
VL o
n th
e sa
me
day.
If n
ot a
dmin
iste
red
on th
e sa
me
day,
sep
arat
e liv
e va
ccin
es b
y at
leas
t 28
days
. 3.
Im
mun
osup
pres
sive
ste
roid
dos
e is
con
side
red
to b
e da
ily re
ceip
t of 2
0 m
g or
mor
e pr
edni
sone
or e
quiv
alen
t for
2 o
r mor
e w
eeks
. Vac
cina
tion
shou
ld b
e de
ferr
ed fo
r at l
east
1 m
onth
aft
er d
isco
ntin
uatio
n of
im
mun
osup
pres
sive
ste
roid
ther
apy.
Pro
vide
rs s
houl
d co
nsul
t AC
IP re
com
men
datio
ns fo
r com
plet
e in
form
atio
n on
the
use
of s
peci
fic li
ve v
acci
nes
amon
g pe
rson
s on
imm
une-
supp
ress
ing
med
icat
ions
or w
ith im
mun
e su
ppre
ssio
n be
caus
e of
oth
er re
ason
s.4.
Vac
cine
sho
uld
be d
efer
red
for t
he a
ppro
pria
te in
terv
al if
repl
acem
ent i
mm
une
glob
ulin
pro
duct
s ar
e be
ing
adm
inis
tere
d. S
ee: B
est p
ract
ices
gui
danc
e of
the
Adv
isor
y Co
mm
ittee
on
Imm
uniz
atio
n Pr
actic
es (A
CIP
). A
vaila
ble
at
ww
w.c
dc.g
ov/v
acci
nes/
hcp/
acip
-rec
s/ge
nera
l-rec
s/in
dex.
htm
l. 5.
Mea
sles
vac
cina
tion
may
tem
pora
rily
supp
ress
tube
rcul
in re
activ
ity. M
easl
es-c
onta
inin
g va
ccin
e m
ay b
e ad
min
iste
red
on th
e sa
me
day
as tu
berc
ulin
ski
n te
stin
g, o
r sho
uld
be p
ostp
oned
for a
t lea
st 4
wee
ks a
fter
vac
cina
tion.
Tab
le. C
ontr
aind
icat
ions
and
pre
caut
ions
for v
acci
nes
reco
mm
end
ed fo
r ad
ults
age
d 1
9 ye
ars
or o
lder
*Th
e A
dvis
ory
Com
mitt
ee o
n Im
mun
izat
ion
Prac
tices
(AC
IP) r
ecom
men
datio
ns a
nd p
acka
ge in
sert
s fo
r vac
cine
s pr
ovid
e in
form
atio
n on
con
trai
ndic
atio
ns a
nd p
reca
utio
ns re
late
d to
vac
cine
s. C
ontr
aind
icat
ions
are
con
ditio
ns
that
incr
ease
cha
nces
of a
ser
ious
adv
erse
reac
tion
in v
acci
ne re
cipi
ents
and
the
vacc
ine
shou
ld n
ot b
e ad
min
iste
red
whe
n a
cont
rain
dica
tion
is p
rese
nt. P
reca
utio
ns s
houl
d be
revi
ewed
for p
oten
tial r
isks
and
ben
efits
for v
acci
ne
reci
pien
ts. Vac
cin
e(s)
Con
trai
nd
icat
ion
sPr
ecau
tion
s
All
vacc
ines
rout
inel
y re
com
men
ded
for a
dults
• Se
vere
reac
tion,
e.g
., an
aphy
laxi
s, a
fter
a p
revi
ous
dose
or t
o a
vacc
ine
com
pone
nt•
Mod
erat
e or
sev
ere
acut
e ill
ness
with
or w
ithou
t fev
er
Ad
dit
iona
l con
trai
ndic
atio
ns a
nd p
reca
utio
ns fo
r vac
cine
s ro
utin
ely
reco
mm
end
ed fo
r ad
ults
Cont
rain
dic
atio
ns a
nd p
reca
utio
ns fo
r vac
cine
s ro
utin
ely
reco
mm
end
ed fo
r ad
ults
* A
dapt
ed fr
om: C
DC
. Tab
le 6
. Con
trai
ndic
atio
ns a
nd p
reca
utio
ns to
com
mon
ly u
sed
vacc
ines
. Gen
eral
reco
mm
enda
tions
on
imm
uniz
atio
n: re
com
men
datio
ns o
f the
Adv
isor
y Co
mm
ittee
on
Imm
uniz
atio
n Pr
actic
es. M
MW
R.
2011
;60(
No.
RR-
2):4
0–1
and
from
: Ham
bors
ky J,
Kro
ger A
, Wol
fe S
, eds
. App
endi
x A
. Epi
dem
iolo
gy a
nd p
reve
ntio
n of
vac
cine
pre
vent
able
dis
ease
s. 1
3th
ed. W
ashi
ngto
n, D
C: P
ublic
Hea
lth F
ound
atio
n, 2
015.
Ava
ilabl
e at
ww
w.c
dc.
gov/
vacc
ines
/pub
s/pi
nkbo
ok/i
ndex
.htm
l.
Ab
bre
viat
ion
s of
vac
cin
esIIV
in
activ
ated
influ
enza
vac
cine
RIV
reco
mbi
nant
influ
enza
vac
cine
Tdap
te
tanu
s to
xoid
, red
uced
dip
hthe
ria to
xoid
, and
ac
ellu
lar p
ertu
ssis
vac
cine
Td
teta
nus
and
diph
ther
ia to
xoid
sM
MR
m
easl
es, m
umps
, and
rube
lla v
acci
ne
VAR
varic
ella
vac
cine
RZV
reco
mbi
nant
zos
ter v
acci
neZV
L zo
ster
vac
cine
live
HPV
vac
cine
hu
man
pap
illom
aviru
s va
ccin
ePC
V13
13
-val
ent p
neum
ococ
cal c
onju
gate
vac
cine
PP
SV23
23
-val
ent p
neum
ococ
cal p
olys
acch
arid
e va
ccin
e
Hep
A
hepa
titis
A v
acci
neH
epA
-Hep
B he
patit
is A
and
hep
atiti
s B
vacc
ines
Hep
B he
patit
is B
vac
cine
Men
AC
WY
sero
grou
ps A
, C, W
, and
Y m
enin
goco
ccal
vac
cine
Men
B
sero
grou
p B
men
ingo
cocc
al v
acci
neH
ib
Hae
mop
hilu
s infl
uenz
ae ty
pe b
vac
cine
CS27
0457
-A

B-1
2 to 20 years: Girls
Body mass index-for-age percentilesNAME
RECORD #
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
2 543 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
26
24
22
20
18
16
14
12
kg/m2
28
26
24
22
20
18
16
14
12
kg/m2
30
32
34
BMI
BMI
AGE (YEARS)
13
15
17
19
21
23
25
27
13
15
17
19
21
23
25
27
29
31
33
35
Date Age Weight Stature BMI* Comments
95
90
85
75
50
10
25
5
Published May 30, 2000 (modified 10/16/00).

B-2
2 543 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
26
24
22
20
18
16
14
12
kg/m2
28
26
24
22
20
18
16
14
12
kg/m2
30
32
34
BMI
BMI
AGE (YEARS)
13
15
17
19
21
23
25
27
13
15
17
19
21
23
25
27
29
31
33
35
95
90
75
50
25
10
5
85
2 to 20 years: Boys
Body mass index-for-age percentilesNAME
RECORD #
SOURCE: Developed b
(2000).
y the National Center for Health Statistics in collaboration with
the National Center for Chronic Disease Prevention and Health Promotion
http://www.cdc.gov/growthcharts
Date Age Weight Stature BMI* Comments
Published May 30, 2000 (modified 10/16/00).


©2018 PASSPORT HEALTH PLAN (HLTH02480) APP_10/29/2018