
Ealing Primary Care Standard
121
Paper: 4 Date Wednesday, 26 July 2017 Presenter Neha Unadkat, Deputy Managing Director Tessa Sandall, Managing Director Author Neha Unadkat Responsible Director Tessa Sandall, Managing Director Clinical Lead Dr Mohini Parmar, Clinical Lead Confidential Yes ☐ No Items are only confidential if it is in the public interest for them to be so The Governing Body is asked to: The Governing Body is being asked to Ratify the decisions made by the Investment Committee (IC) and the Primary Care Committee (PCC). If the Governing Body does not ratify, then the issues preventing such will be returned to the relevant non-conflicted Committee for (re-)consideration. • Ratify the outcomes of the Primary Care Commissioning Committee (PCC) on the 19 th July • Ratify the outcomes of the Investment Committee (IC) on the 20 th July • Note that if the GB believe the decision of the PCC or the recommendation of the IC require further assurance, the request would be required to go back to the relevant committee for consideration to ensure that conflicts are appropriately managed • Note the additional supporting slides which demonstrate the decision making process for the Standard The Investment Committee were asked to: • Note the outcome of the Primary Care Commissioning Committee’s consideration of the whole case on the 19 th July which will be reported to the committee on the 20 th July • Approve on-going/renewal of funding relating OOH, Paediatric Phlebotomy, LIS, Dementia (£7.2M annually 18/19 – 20/21) Title of paper Ealing Primary Care Standard
Transcript of Ealing Primary Care Standard
Paper: 4
Date Wednesday, 26 July 2017
Presenter Neha Unadkat, Deputy Managing Director
Tessa Sandall, Managing Director
Author Neha Unadkat
Responsible Director
Tessa Sandall, Managing Director
Clinical Lead Dr Mohini Parmar, Clinical Lead
Confidential Yes ☐ No Items are only confidential if it is in the public interest for them to be so
The Governing Body is asked to:
The Governing Body is being asked to Ratify the decisions made by the Investment Committee (IC) and the Primary Care Committee (PCC).
If the Governing Body does not ratify, then the issues preventing such will be returned to the relevant non-conflicted Committee for (re-)consideration.
• Ratify the outcomes of the Primary Care Commissioning Committee (PCC) on the
19th July • Ratify the outcomes of the Investment Committee (IC) on the 20th July • Note that if the GB believe the decision of the PCC or the recommendation of the IC
require further assurance, the request would be required to go back to the relevant committee for consideration to ensure that conflicts are appropriately managed
• Note the additional supporting slides which demonstrate the decision making process for the Standard
The Investment Committee were asked to:
• Note the outcome of the Primary Care Commissioning Committee’s consideration of the whole case on the 19th July which will be reported to the committee on the 20th July
• Approve on-going/renewal of funding relating OOH, Paediatric Phlebotomy, LIS, Dementia (£7.2M annually 18/19 – 20/21)
Title of paper Ealing Primary Care Standard

Paper: 4
• Approve investment of £923k 18/19-20/21 new funding from core funding is
affordable based on conservative savings case • Confirm the approach taken to manage Conflicts of Interest was proper and robust • Note the view of the non-conflicted F&P members; • Inform the Governing Body of the decisions of the Investment Committee for
ratification by the Governing Body
The Primary Care Commissioning Committee were asked to:
• Consider and Approve the Ealing Standard and the supporting business case. • Approve the use of the headroom in the primary care allocation to fund in 2017/2018
the access specification and from 2018/2019 to support the standards relating to access, screening, prevention and patient experience.
• Note that the standards have been developed by clinical leads with a period of co-production with the broader CCG membership.
• Note that the costing of the standards has been developed in line with the OOH costing model or using the Local Improvement Scheme (LIS) as the benchmark, with clinical leads determining the length of the clinical interventions and the staff groups involved, with the officers using this information to cost the standards.
• Agree to a KPI Moratorium in 17/18 to allow practices to mobilise effectively • Note the report provided by Healthwatch on Access to general practice in Ealing.
Summary of purpose and scope of report
The CCGs ambition in commissioning the Ealing Standard is:
1. To have equity of offer and access to patients registered with an Ealing GP through commissioning the Ealing Standard
2. To reduce the unwarranted variation in general practice and improve outcomes for individuals
3. To address the concerns and feedback received from patients regarding access to general practice and drive ongoing improvement over the term of the Ealing Standard.
4. To address the needs of the population as identified in the Joint Strategic Needs Analysis (JSNA) and ensure the primary care standards deliver a full, holistic offer of care for patients
5. To support and improve resilience and sustainability within general practice whilst meeting the strategic requirements as set out in the NWL STP, 5YFV, and the Strategic Commissioning Framework (SCF). It is very clear that general practice is the golden thread that runs through all five of the delivery areas of the STP supporting and enabling the realisation of the triple aims of the STP of Improving Health & Wellbeing, Improving care & quality, Improving productivity and closing the financial gap.
6. To utilise the opportunity that Primary Care Delegation has provided in enabling the

Paper: 4
CCG to direct the use of the headroom within the primary care allocation for Ealing GPs. The headroom recognises the historical underfunding in general practice from a national level and the increasing allocation addresses this up to and including 2020/2021.
7. That the CCG commissions an equitable offer on an equitable financial basis from practices and therefore the Ealing Standard is the commissioning intention for PMS discussions to support the NHS England required renegotiation of PMS premium funding.
The CCG is requesting approval relating to three funding streams as outlined below:
8. To utilise £2.8m of the headroom during 2017/2018 with a focus on access increasing to £3,474k to support access, prevention, screening and patient experience recurrently.
9. As the allocation increases in future years, following managing any growth pressures or increases in core primary care spend, such as funding implications of national contract negotiations, increases in rents, rates and applying any NHS business rules as directed by NHSE, further headroom funding released is allocated to support primary care in Ealing to further stretch the primary care offer through stretched targets or new standards in line with the needs of the population.
10. To seek agreement that the funding already being utilised from the CCG programme budget, £7.2m, should continue to be used to commission the Out of Hospital (OOH) services as part of the Ealing Standard. That this agreement is made based on the understanding that the care will need to be provided from somewhere within the healthcare system and for a proportion of the services this would be at a higher cost, £2.6m, in the acute service.
11. To seek agreement to additional investment from CCG programme budget of £923k into the Ealing Standard noting that the costs have been derived through either the out of hospital costing model or through the LIS incentive scheme approach. The request for an additional £923k annually is made against the most conservative realisation of savings derived directly from the standard of £1,160k in 2018/2019 with a total incremental saving at the end of the 2020/2021 of £4,124k.
12. That the Ealing Standard enables the implementation of primary care led elements of the STP across the five domain areas and underpins some of the financial benefits to be realised e.g. on going investment into primary care to support mental health care enabling the Like Minded business case (DA4), enabling the use of PAMS (DA1) or the system wide programmes on Diabetes, Hypertension and AF (DA2).
13. To seek approval for a moratorium on the KPIs in 17/18 to start to mobilise and prepare for phase 2 in April 2018. This is in line with the process to mobilise the original OOH services contract with primary care
That the committee note the approach to the costing of the standards and the approach to contracting:
14. That the costing of the standards has been developed in line with the OOH costing

Paper: 4
model or using the Local Improvement Scheme (LIS) as the benchmark, with clinical leads determining the length of the clinical interventions and the staff groups involved, with the officers using this information to cost the standards. This was further reviewed by a finance officer outside of Ealing.
15. That the Ealing standard is commissioned as a single wrap around contract from each provider of medical services.
That there is a need to invest in mobilisation through internal and additional resource:
16. That additional resource is agreed as part of the business case to support mobilisation of the standard throughout the rest of 2017/2018 and this is funded from the primary care allocation and the headroom available. That this mobilisation is overseen by a steering group made up of CCG clinical leads and managers with responsibility for primary care. That this group reports into and includes members from the Primary Care Commissioning Committee, F&P and that Healthwatch are included as members.
That the following assurances have been received through:
a) Independent Review Panel has reviewed all the new standards in line with the
original out of hospital services business case and confirmed their view that General Practice is the ‘most capable provider’
b) Finance & Performance and Primary Care Commissioning Committees have approved the core primary care budget delegated to CCGs, subject to a desktop review by the District Valuer on the rent increases pressure on the budget and a review of the rates implication
Feedback will be provided in the committee meeting from the discussion held at F&P.
Quality & Safety/ Patient Engagement/ Impact on patient services:
The Standards are designed to:
1. Provide an equity of offer and access to patients registered with an Ealing GP through commissioning the Ealing Standard
2. Reduce the unwarranted variation in general practice and improve outcomes for individuals
3. Address the concerns and feedback received from patients regarding access to general practice and drive ongoing improvement over the term of the Ealing Standard.
4. Address the needs of the population as identified in the Joint Strategic Needs Analysis (JSNA) and ensure the primary care standards deliver a full, holistic offer of care for patients

Paper: 4
Finance, resources and QIPP
The Business Case sets out the case for:
1. Agreement to invest the increase in allocation (Headroom) of £2.8M during 2017/2018 with a focus on access increasing to £3,474k to support access, prevention, screening and patient experience recurrently.
2. To continue to invest the funding allocated to the Out of Hospital Contract, Dementia Contract, Local Improvement Scheme Budget and the Paediatric Phlebotomy contract of £7.2M, but into the Primary Care Standard.
3. Agreement for a further £923K to be invested from core CCG funds into these standards.
The Net Savings following the reinvestment of the request for core funding based on the most conservative case is as follows:
Financial Period
2018/2019 2019/2020 - Cumulative
2020/2021 Cumulative
Total Core additional funding £923,258 £1,855,749 £2,797,564
Conservative case benefit realisation £1,159,511 £2,543,214 £4,123,130
Net savings £236,253 £687,465 £1,325,566
% savings on additional funding 26% 37% 47%
Conservative case incremental saving year on year
£1,159,511 £1,383,703 £1,579,916
Equality / Human Rights / Privacy impact analysis
An Equality Impact Assessment has been conducted and is available in the Business Case.
Risk Mitigating actions
The complete risk register is available in the business case

Paper: 4
Supporting documents
Ealing Primary Care Standards Business Case Ealing Primary Care Standards
Governance and reporting
Committee name Date discussed Outcome

Document Name Ealing Standard Decision Making Business Case
Version V.15
Status Final
Author Neha Unadkat – Deputy Managing Director Primary Care & Integration
Tessa Sandall – Managing Director
Date created 30 May 2017
Date last amended 12 July 2017
Ealing Standard Decision Making Business Case

Ealing New Primary Care Offer Business Case
July 2017 i
Contents
1 Introduction ................................................................................................................................ 1
1.1 Purpose of this business case ............................................................................................ 1
1.2 Structure and content of this document ............................................................................... 1
2 Strategic case ............................................................................................................................ 2
2.1 Strategic context ................................................................................................................. 2
2.1.1 National context ........................................................................................................... 3
2.1.2 Regional (London-wide) context .................................................................................. 4
2.1.3 North West London context ......................................................................................... 5
2.2 Case for change ............................................................................................................... 18
2.2.1 Patient Perspective .................................................................................................... 18
2.2.2 Population Perspective .............................................................................................. 19
2.2.3 General Practice perspective ..................................................................................... 19
2.2.4 Economic Case ......................................................................................................... 21
2.2.5 Financial sustainability ............................................................................................... 22
2.2.6 Headroom funding opportunity ................................................................................... 22
2.2.7 High administrative burden ........................................................................................ 23
2.2.8 Case for change summary ......................................................................................... 23
2.3 Investment objectives ....................................................................................................... 24
3 Economic Case........................................................................................................................ 25
3.1 Critical success factors ..................................................................................................... 25
3.2 Long list of options ............................................................................................................ 26
3.2.1 OOHS contract .......................................................................................................... 27
3.2.2 LIS contract ............................................................................................................... 28
3.2.3 Winter resilience funding ........................................................................................... 30
3.2.4 Paediatric phlebotomy and dementia ......................................................................... 31
3.2.5 PMS funding .............................................................................................................. 32
3.2.6 Headroom funding ..................................................................................................... 33
3.2.7 Summary of long list analysis .................................................................................... 35
3.3 Short list appraisal ............................................................................................................ 35
3.3.1 Short listed options .................................................................................................... 35
3.3.2 Short list benefit and dis-benefits analysis ................................................................. 35
3.4 The preferred option ......................................................................................................... 37
4 Commercial case ..................................................................................................................... 38
4.1 The Commissioning Strategy ............................................................................................ 38

Ealing New Primary Care Offer Business Case
July 2017 ii
4.2 Payment Mechanisms ...................................................................................................... 39
4.3 Contractual and Other Issues ........................................................................................... 40
4.3.1 Type of contract ......................................................................................................... 40
4.3.2 Contract management ............................................................................................... 40
5 Financial case .......................................................................................................................... 41
5.1 Available funding .............................................................................................................. 41
5.2 Costing of the specifications ............................................................................................. 41
5.3 Affordability assessment ................................................................................................... 44
5.3.1 The Primary Care headroom investment ........................................................................ 44
5.3.2 The renewal of the funding for the services detailed in the above section ...................... 44
5.3.3. The request for additional investment into the standards .............................................. 44
5.3.4 Savings attributable to the Ealing Standard .................................................................... 44
5.3.1 The Primary Care headroom investment ......................................................................... 44
5.5 Impact on PMS practices .................................................................................................. 56
6 Management case ................................................................................................................... 59
6.1 Governance ...................................................................................................................... 59
6.2 Mobilisation plan ............................................................................................................... 60
6.3 Provider development ....................................................................................................... 62
6.4 Resourcing Requirements in the CCG .............................................................................. 65
7 Conclusion and Recommendation ........................................................................................... 66
Appendix 3 Equality impact statement ............................................................................................ 68
Appendix 4 Risk register ................................................................................................................. 82
Appendix 5 OOHS contracts ........................................................................................................... 85
Appendix 6 Outcome of the Independent Review Panel ................................................................. 86
Appendix 7 Annual Self Declaration .............................................................................................. 109
Appendix 8: Primary Care Offer Steering Group TOR ................................................................... 111

Ealing New Primary Care Offer Business Case
July 2017 1
1 Introduction
1.1 Purpose of this business case
- The purpose of this business case is to seek approval to commission the Ealing Primary
Care standard commencing with access in 2017/2018 with the full standard being
commissioned from 2018 through until 2021. The investment will be used to fund the
Ealing Standard, which aims to improve the resilience of general practice, improve
access for patients, reduce unwarranted variation in health outcomes and ensure long
term sustainability in the local health system. The Ealing Standard is a contract for
primary care providers for the delivery of a set of 23 standards that focuses on the
delivery of high quality care in general practice
1.2 Structure and content of this document
This business case sets out to consider the five cases that align to the HMT Green Book
guidance:
The Strategic Case: setting out the strategic context and the case for change, together
with the supporting investment objectives for the scheme
The Economic Case: setting out the available options to meet the investment objectives
and establishing which is the preferred option
The Commercial Case: outlining the commercial strategy for the preferred option?
The Financial Case: confirming the funding arrangements and affordability for the
preferred option?
The Management Case: demonstrating that the preferred option is achievable and can
be delivered successfully to cost, time and quality.
The following sections provide the evidence for each of these five cases in turn.
Ealing New Primary Care Offer Business Case
July 2017 2
2 Strategic case
This section will set out the current situation for primary care in Ealing and the strategic context
in terms of national, regional and local drivers for change. It will also set out the case for change
and the investment objectives of this project.
2.1 Strategic context
Ealing is the largest borough in North West London and works within the collaboration of eight
CCGs in North West London. The STP has been developed by commissioners, providers and
with local authorities across North West London and has a triple aim of Improving Health &
Wellbeing, Improving care & quality and Improving productivity and closing the financial gap.
The golden thread running across and within the STP is general practice; the five delivery areas
within the STP all require general practice to enable the benefits they describe. However,
primary care cannot deliver this on its own, but as part of a system aligned to deliver to the same
outcomes. Therefore, primary care must be commissioned and supported to become resilient
and transformed, so that it is not working in isolation.
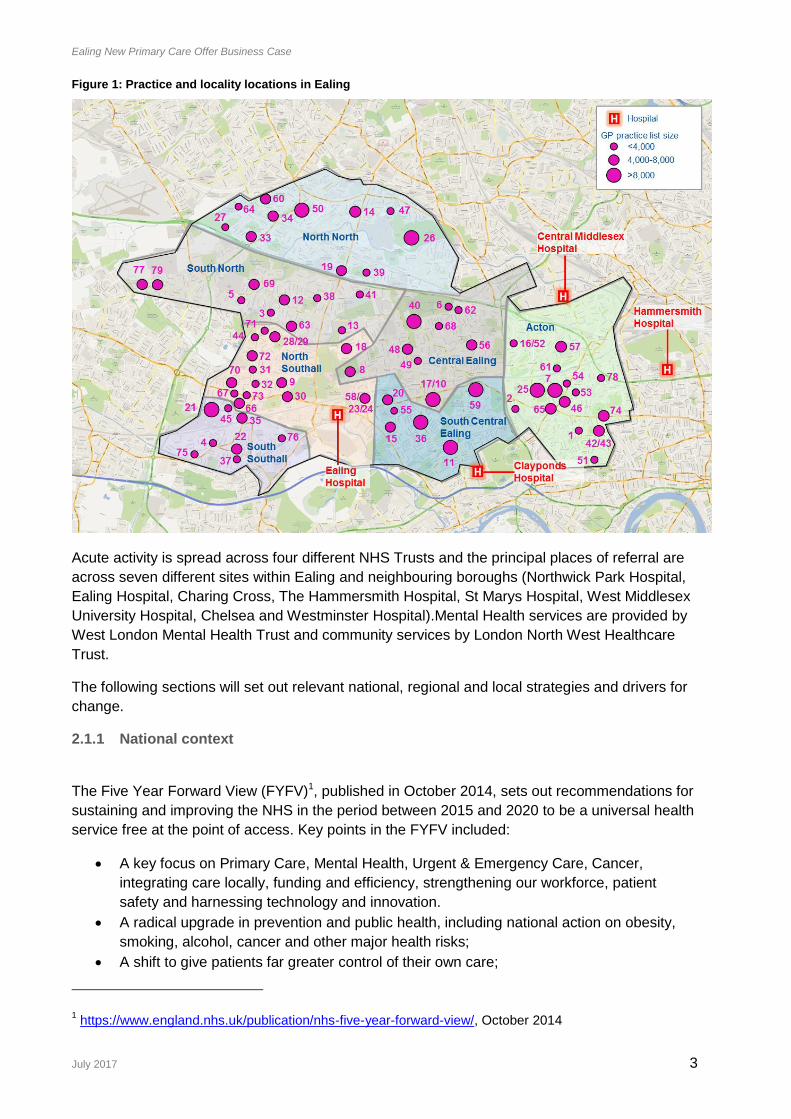
Ealing Clinical Commissioning Group (Ealing CCG) commissions services from 76 GP practices,
meeting the needs of 425,000 registered patients. Practices are arranged into seven locality
networks, as shown in Figure 1. Of the 76 practices, 64 hold GMS contracts, 7 hold PMS
contracts and 5 hold APMS contracts. Ealing GP Federation was formed in October 2014,
representing all 76 practices. The Federation has been commissioned to deliver an Out of
Hospital Services (OOHS) contract through the member practices. In addition to the core and
OOHS contracts, practices in Ealing also deliver an annual Local Improvement Scheme (LIS),
paediatric phlebotomy, winter resilience and dementia contracts and some deliver out of hours
services.
Ealing New Primary Care Offer Business Case
July 2017 3
Figure 1: Practice and locality locations in Ealing
Acute activity is spread across four different NHS Trusts and the principal places of referral are
across seven different sites within Ealing and neighbouring boroughs (Northwick Park Hospital,
Ealing Hospital, Charing Cross, The Hammersmith Hospital, St Marys Hospital, West Middlesex
University Hospital, Chelsea and Westminster Hospital).Mental Health services are provided by
West London Mental Health Trust and community services by London North West Healthcare
Trust.
The following sections will set out relevant national, regional and local strategies and drivers for
change.
2.1.1 National context
The Five Year Forward View (FYFV)1, published in October 2014, sets out recommendations for
sustaining and improving the NHS in the period between 2015 and 2020 to be a universal health
service free at the point of access. Key points in the FYFV included:
A key focus on Primary Care, Mental Health, Urgent & Emergency Care, Cancer,
integrating care locally, funding and efficiency, strengthening our workforce, patient
safety and harnessing technology and innovation.
A radical upgrade in prevention and public health, including national action on obesity,
smoking, alcohol, cancer and other major health risks;
A shift to give patients far greater control of their own care;
1 https://www.england.nhs.uk/publication/nhs-five-year-forward-view/, October 2014

Ealing New Primary Care Offer Business Case
July 2017 4
Decisive steps to break down the barriers in how care is provided between family doctors
and hospitals, between physical and mental health, between health and social care e.g.
through Primary and Acute Care Systems (PACS);
Support from the NHS’ national leadership to develop radical new care delivery options
including permitting groups of GPs to combine with nurses, other community health
services, hospital specialists and perhaps mental health and social care to create
integrated out-of-hospital care e.g. through Multispecialty Community Providers (MCPs);
Urgent and emergency care services redesign to integrate between A&E departments,
GP out-of-hours services, urgent care centres, NHS 111, and ambulance services;
Greater support for frail older people living in care homes;
A ‘new deal’ for GPs, including investing more in primary care, while stabilising core
funding for general practice nationally over the next two years and a shift in investment
from acute to primary and community services.
The GP Forward View (GPFV)2, published in April 2016, reiterated these themes with a ‘triple
reinvention’ for general practice, comprising recommendations for changes to the ‘clinical
model’, ‘career model’ and ‘business model’. The report pledges a 14% real-terms rise in
general practice investment, with an expectation of local CCG investment on top of this rise in
national funding. It sets out recommendations to grow the number of qualified GPs, support
practices to be more resilient and establish new rules to reimburse up to 100% of premises
developments. It also sets out support to establish federations and ‘superpartnerships’, as well
as direct funding for improved in hours and out of hours access, including clinical hubs and
reformed urgent care.
The Primary Care Home (PCH) model3 was launched by the National Association of Primary
Care in October 2015, supported by NHS England and the NCM programme. It expresses ideas
about improving joint working within and beyond general practice, developed over more than a
decade by clinicians around the country. Initially, fifteen rapid test sites were chosen to test the
principles of the primary care home, there are now more than ninety. The model is based on four
defining characteristics:
Provision of care to a defined, registered population of between 30,000 and 50,000;
An integrated workforce, with a strong focus on partnerships spanning primary,
secondary and social care inclusive of patients and the voluntary sector;
A combined focus on personalisation of care with improvements in population health
outcomes; and
Aligned clinical financial drivers through a unified, whole population budget with
appropriate shared risks and rewards.
The PCH embraces some of the characteristics of the MCP model set out in the FYFV.
2.1.2 Regional (London-wide) context
The Strategic Commissioning Framework for Primary Care Transformation in London (SCF)
aims to support primary care transformation across the capital, responding to strategies for
general practice set out in the FYFV and findings of the London Health Commission. The SCF
sets out a new vision for primary care in the capital, and describes what patients should be able
to expect from primary care. There are 17 service specifications in the SCF, grouped into the
2 https://www.england.nhs.uk/gp/gpfv/, April 2016
3 http://www.napc.co.uk/primary-care-home, accessed June 2017

Ealing New Primary Care Offer Business Case
July 2017 5
themes of Accessible, Coordinated and Proactive Care as presented in Figure 2. Importantly
the SCF was worked up in collaboration with many patients and carers, the LMC, clinical
representatives, CCGs and NHS England colleagues.
Figure 2: SCF service specifications
The SCF is clear that investment into primary care is required to be able to deliver the
specifications, as well as improvements to the capacity and diversity of the primary care
workforce in London.
2.1.3 North West London context
The eight CCGs in North West London work together as a collaboration underpinned by the
CWHHE CCG collaboration and the Federation of CCGs in Brent, Harrow and Hillingdon. Each
of the CCGs is currently delivering an ambitious Out of Hospital (OOH) programme intended to
ensure that patients are at the centre of care, with the registered GP providing, managing and
coordinating the care received. A key part of each OOH strategy is the intent in each CCG to
support the continued development of high quality primary care at both a practice level and
network of practices level. Most recently NWL CCGs have worked together with providers and
Local Authority colleagues to develop the STP in response to national requirements. The STP
builds on the work delivered to establish a vision for care delivery in North West London in
Shaping a Healthier Future but considers more broadly its response to the FYFV. The vision for
the STP is set out in the table below and what is clear is the critical importance of general
practice throughout the STP with a delivery area focused on the transformation of this part of the
system as well as an enabler throughout all the delivery areas.

Ealing New Primary Care Offer Business Case
July 2017 6
Figure 3: STP vision for care in North West London
Figure 3 illustrates that the golden thread running across and within the STP is general practice; the
five delivery areas within the STP all require general practice to enable the benefits they describe.
However, primary care cannot deliver this on its own, but as part of a system aligned to deliver to
the same outcomes. Therefore, primary care must be commissioned and supported to become
resilient and transformed, so that it is not working in isolation.
As indicated above the STP builds on the work health partners started with the Shaping a
Healthier Future (SaHF) programme. The SaHF programme is led by clinicians and has been
set up to develop proposals that will improve both hospital and out of hospital care. SaHF is a
reconfiguration that requires a fundamental change in the way both acute and community
services are delivered with a focus on delivering care as close to patients’ homes as is possible.
Following a significant programme of consultation with patients, carers, members of the public
and professionals across North West London, the SaHF Decision Making Business Case
(DMBC) was signed off in February 20134. This set out a vision for the future of care delivery in
North West London which would be localised, centralised and integrated.
4 https://www.healthiernorthwestlondon.nhs.uk/documents/joint-committee-primary-care-trusts-nwl/jcpcts-
meeting-papers-19022013/decision-making, accessed June 2017

Ealing New Primary Care Offer Business Case
July 2017 7
Figure 4: SaHF DMBC vision for care in North West London
The SaHF case focused on both the acute reconfiguration and out of hospital care with Out of
Hospital strategies underpinning the acute changes. Ealing CCG has been working to deliver
the out of hospital strategy over a number of years which had the transformation of general
practice as a critical enabler. Within the delivery of the acute configuration are the changes
which enable Ealing Hospital to transform into a local hospital and hub for the Borough.
Alongside two further hubs in the Borough the transformation requires comprehensive out of
hospital care underpinned by resilient general practice. The case for the Ealing Standard as set
out in this business case and in the support documents providers general practice with clear
requirements in terms of the standards of care expected to support comprehensive out of
hospital care to the registered population in Ealing with the income that practices can expect to
receive if they deliver the standard.
Central London, West London, Hammersmith & Fulham, Hounslow and Ealing CCGs have
elected to work together as a collaboration of CCGs: CWHHE.
2.1.4 Local Ealing context
The GP Forward set out the transformation objective and expectation of local areas to ensure
primary care is a sustained and resilient component of the overall health system recognising the
critical role it plays to coordinate and proactively support patients.
Ealing’s primary care health economy has been significantly underfunded historically, however, it
has survived and provided the population of Ealing with a primary care service in very difficult
financial circumstances. Ealing general practice has faced many challenges including the
historical under investment, workforce challenges and the lack of capacity and compliance in
estate,.
In 2012, a business case was approved for investment in primary care to work in an integrated
care programme (ICP) as networks of practices serving a population of between 40,000 and
70,000 patients, with comprehensive care planning for individuals that need proactive and
Localised
1
Centralised Integrated
3
• Reduced admissions due to
better local management of
care
• Improved support for
patients with LTCs and
mental health problems
• Improved patient experience
and satisfaction
• Improved carer experience
• Better clinical outcomes
including reduced morbidity
and mortality
• Reduced readmission
• Reduced lengths of stay
• Increased staff training,
skills and job satisfaction
• Increased multidisciplinary
working – improved
coordination
• Improved access to
information leading to better
patient care
• Reduction in unnecessary
investigations and duplicate
assessments
• Improved efficiency and
pathways
Qu
alit
y &
exp
erie
nce
im
pro
ve
me
nts
2

Ealing New Primary Care Offer Business Case
July 2017 8
coordinated care, with any complex cases discussed at multi-disciplinary group (MDG) meetings
where social services, generalist consultants, such as care of the elderly consultants and
diabetes consultants, community nursing teams including Diabetes Specialist nurses and
community matrons or district nurses and community pharmacists. These MDG meetings are
still active across the borough, although less frequent. Through the MDG meetings and
significant investment in training and support, practices started to work together as networks of
practices, recognising that the issues each practice faced with complex patients or inefficient
pathways across the rest of the system were shared across all practices. The primary care
networks started to become a source of peer learning, sharing and support.
In 2014, a business case was agreed across CWHHE for significant investment in a range of 19
services specifications – the Out of Hospital Services contract (OOH). The ICP programme was
subsumed within these services, and took the infrastructure and support for practices to a new
level. As a result of the business case a Federation emerged with all practices across Ealing
becoming a member of the Federation. The principle of this investment was to deliver
population based care, so that no matter which practice a patient was registered at they could
get access to all of the 19 service lines. In some cases at the smaller practices, if they were not
able to safely provide a particular service, the patient registered at that practice could access the
service at another local service. The Federation (Ealing GP Ltd) is responsible for ensuring
population coverage and the safety of the service, as well as supporting practices to run the
business management function that sitst behind the services. It is fair to say that the
mobilisation of the OOH contract was very difficult with an overly complex IT system and
payment mechanism. However, in December 2016, following an in depth review of the IT
system templates and payment processes, an improved set of specifications and underpinning
templates were provided.
The OOH contract is now delivering all the services across the borough although take up is
variable and has been achieved at different rates dependent on the service lines.
In August 2016, following the launch of the GPFV, Ealing CCG ran a series of workshops to
understand the risks in primary care, primarily in terms of workforce and estates.
Key Highlights - Estates:
69 Baseline Estates survey conducted
58 of the properties built before 1961 and therefore do not meet the current design
standards for the delivery of primary care
4 properties constructed since 2000
30 of the surveyed premises have 4 clinical rooms or less
5 of the premises have 10 clinical rooms or more
63 of the premises surveyed were found to be fully or over utlilised
45 of the premises had potential to expand clinical service activity
Backlog Maintenance over coming 5 years was estimated to be approximately £1.6M
with £0.4M required immediately Figure 3
Improvement grants (Previously known as Primary Care Infrastructure funds (PCIF) and
Primary Care Transformation Funds (PCTF) supported by CCG for 26 sites, with 7 of the
sites providing additional clinical space. Funding source NHSE and undergoing NHSE
Due diligence.
8 Estates, Technology Transformation Fund (ETTF) bids submitted to NHSE, all on
pipeline with NHSE, but not supported as yet.

Ealing New Primary Care Offer Business Case
July 2017 9
Figure 5: Quality of Estates following baseline estates survey
Figure 6: Improvement Grant across the borough

Ealing New Primary Care Offer Business Case
July 2017 10
Key Highlights – Quality of Service Provision:
18 single-handed practices (figure 5)
At the time of creating this (July 2016), not all practices had been rated by CQC, At the
time in Ealing there were: 1 Outstanding practice, 26 Good, 5 Requires Improvement, 1
Inadequate, 45 not yet published
Data source for performance against General Practice High Level Indicators (GPHLI)
found at www. Priamrycare.nhs.uk:
Indicators include those relating to long term condition management, prescribing, hospital
admissions, public health screening and immunisation targets, and patient experience
Practice data for each indicator is compared nationally and if a data point falls outside 2
standard errors from the national average it is considered an outlier.
A practice is considered an outlier overall of they have 6 or more outlying data points,
and this may warrant further investigation to assess whether the variation is warranted.
Using 2014/15 data:
o 5 practices with 9-10 Outlying Points
o 5 with 6-8 Outlying points,
o All other practices with 0-5 Outlying points
Figure 7: Practice list size and single handed practices
Key Highlights – Workforce:
Data Collated from Workforce Minimum data set via Primary Care Tool and publically
available reported as at 30th September 2015 – 9 practices did not report

Ealing New Primary Care Offer Business Case
July 2017 11
NOTE: This data does not include locum GPs and 9 practices did not report their data
GPs
172.29 Full time equivalent (FTE) GPs in Ealing (excluding Locums) – based on
reporting practices
In Ealing 2,110 Patients per FTE GP, ranging from 1686 (Acton) to 2994 (North Southall)
London Average is 1929 patients per FTE GP, England average is 1826 patients per
FTE GP.
GP Age profile by Network Figure 6
Nurses
69.7 FTE Nurses in Ealing Primary Care
In Ealing 5395 patients per FTE Nurse, ranging from 3669 (Central Ealing) to 6838
(North Southall)
London Average is 5572 patients per FTE Nurse, England average is 3802 patients per
FTE Nurse.
Nurse Age profile by Network Figure 7
Figure 8: GP Age Profile by Locality

Ealing New Primary Care Offer Business Case
July 2017 12
Figure 9: Nurse age profile by network
Delegated commissioning
In February 2017, the CCG membership made a decision to vote in the responsibility for delegated Primary Care Commissioning to move from NHS England to the CCG. All 8 CCGs in NWL submitted an application to NHS England on 05 December 2016, with agreed caveats. The vote took place in February, with a formal announcement on 24 February 2017 regarding the decision taken by our membership.
This move to full delegation of Primary Care (General Practice) commissioning, assuming full responsibility for commissioning General Practice services in response to the needs and circumstance of their registered populations took effect from 1st April 2017 and supports:
o The delivery of the NW London STP, and in particular, the Local Services strategy that it proposed across our sector of London;
o The CCG to drive efficiency, best value, and consistency in our locally-driven commissioning approach and processes, and in the outcomes derived across NW London; and
o Secures the most efficient and effective governance processes for Primary Care commissioning.

Ealing New Primary Care Offer Business Case
July 2017 13
PMS Review
In February 2014 NHS England’s area teams received national guidance setting out a
requirement to review and renegotiate all PMS contracts, originally by the end of March 2016,
then with a 3 month extension and now extended further to be completed by October 2017. The
purpose of the review is to secure best value from future investment of the ‘premium’ element of
Primary Medical Services (PMS) funding. There is a NWL steering group providing a forum to
agree a single NWL approach where desirable. Otherwise under delegated commissioning
arrangements, Ealing CCG is required to take the lead role in arrangements related to PMS
funding. It is intended that as a result of the PMS review, any additional investment in general
practice services that go beyond core national requirements (whether this is deployed through
PMS or through other routes) should:
Reflect joint NHS England and CCG strategic plans for primary care;
Secure services or outcomes that go beyond what is expected of core general practice or
improve primary care premises;
Help reduce health inequalities;
Give equality of opportunity to all GP practices, i.e. PMS, General Medical Services
(GMS) and Alternative Providers Medical Services (AMPS) (provided they are able to
satisfy locally determined requirements); and
Support fairer distribution of funding at a locality level. All funding released by the review
will be reinvested into general practice.
In Ealing there are 7 practices with a PMS contract. The total value of the premium for the PMS
practices is circa £650k.
Guidance from NHS England confirms that all practices where income reduces by 5% or more
should be offered a minimum of 2 years of transition support. However, in NWL the PMS
Steering group agreed phasing of transition support up to 4 years if a practice is due to lose
more than 15%. Any funds released following the any reinvestment of transition support would
be reinvested back into general practices in the local borough. Figure 10 and 11 show the
principles agreed by the PMS steering group which Ealing CCG has agreed to adopt following
consideration at the Primary Care Commissioning Committee.

Ealing New Primary Care Offer Business Case
July 2017 14
Figure 10: Transition phasing based on loss at a practice.
Figure 11: illustrative example of transition support for practices
Ealing New Primary Care Offer Business Case
July 2017 15
Feedback from patients on Access to Primary Care
Although Ealing CCG has been collating a lot of feedback from patients when conducting
various engagement events across the borough, the overriding feedback we receive is about
access to General Practice..
As a result, Ealing CCG asked Healthwatch to conduct a targeted survey across the borough to
establish the feedback more formally in order to understand in more detail what specific aspects
of access to general practice need improving. The actual report from Healthwatch can be found
in Appendix 2.
A total of 2,000 surveys were conducted across the whole borough with surveys undertaken at:
Local community events and festivals
Shopping areas
Buses, tubes and transport hubs
GP surgeries and Health Centres
Ealing Hospital outpatients department
Primary and Secondary schools
The main findings of the surveys conducted were:
1. While respondents’ experiences of obtaining routine GP appointments varied there were
nuances within this position and many respondents did state they faced difficulties in
getting routine appointments.
While some made statements indicating that it was a struggle to get through busy
telephone lines to book their appointments in the mornings, others complained that
receptionists in GP surgeries were rude; that it cost them money to call for appointments
and some said they were frustrated with the process and it felt like a futile struggle. A
notable number of patients indicated they did not book routine appointments at all whilst
others would have to wait a month in order to see their preferred doctor – and many
reported this preference over perceived changing locums.
On the other hand, however, patients praised their GPs for their services and empathy,
understood the pressures and therefore were satisfied with the service despite any
issues in getting a routine appointment – this understanding was borne through in other
areas of the survey also. One patient in particular mentioned that they had been provided
the extraordinary facility of a home visit for a blood test by their GP.
Specifically reviewing routine appointment times the largest number of our respondents
said they got their routine appointment within 1-2 weeks. This was followed by a slightly
smaller number of respondents who said it took 2 weeks or more to be given an
appointment. A significantly smaller number of respondents said they got their
appointment in 4-6 days, followed by those who said they got it in 2-3days, the very
same day or on the next day. Interestingly, the number of those who said they got it the
same day was higher than those who said they got it the next day.
The most conspicuous complaint from patients was regarding the GP phone being
consistently engaged, or the inconvenience of their being kept waiting between

Ealing New Primary Care Offer Business Case
July 2017 16
approximately 20-30 minutes in a queue. Some people also stated that by the time they
got through to the Practice, there were no longer any appointments available for them.
2. Most of our respondents reported that they did not find it difficult to obtain urgent
appointments.
3. Regarding Urgent Appointments, the majority (over 60%) of our respondents said they
got their appointment on the same day. Next, were those who said they got their
appointment the next day (over 20%). About 7% said they were given an appointment in
2-3 days; next were those who said they got it in 2-3 days, 1-2 weeks or in 4-6 days in
that order.
A number of respondents spoken to had gone to the urgent care centre when they
couldn’t get a urgent GP appointment – mostly this did apply to out of hours but there
were occurrences of attendance at UCC when they simply couldn’t get a appointment at
the GP surgery within an acceptable timeframe.
4. When contacting the surgery by phone early indications suggest the majority of our
respondents rated their experience as “Fair”. This was followed by “Good” and “Very
good”. Next were those who described it as “Poor” or “Very Poor”. Patient experiences
regarding their ability to contact local surgeries via telephone seems to be more positive
than negative though there is room for improvement as suggested by those who rated
their experience as “Very Poor” and “Poor”. As indicated in a previous question above, in
this instance there were also a large number of patients who remained satisfied with the
phone system, despite its difficulties, due to their appreciation of the population
pressures facing GP surgeries.
5. Our patient responses to their experience of obtaining advice from GPs via the telephone
reveals that the majority rated it negatively, describing it as “Very Poor” / “Poor”. Among
the problems they mentioned were the huge difficulty to get through to the practice on the
phone or that they were not able to speak to doctors on the phone at all. Instead, they
spoke to nurses or the receptionist, however a number also reported a system whereby
the doctor would phone back later in the day
The next highest total consisted of respondents who said they were not sure about their
experience of getting advice from a GP. The large number of those “Not Sure”, seems to
indicate that many patients were unable to say anything clearly because they did not
expect to be able to speak to a GP for advice. Some patients who clearly said that they
were not aware of this service and so did not have this expectation nor had they tried to
speak to a GP on the phone for medical advice also corroborate this. GP Telephone
consultations could therefore be a possible area of opportunity in terms of easing access
pressures.
This was followed by those who rated it positively as “Good”/ “Very Good”/
“Excellent”/”Very Good”. Among them were some who said the doctor called back quite
soon.
6. Regarding currently booking appointments online, the majority of our respondents said
they were booking online. A large number of patients said they were “Not Sure” about
booking online. A slightly smaller number than those who said they were “Not Sure”,

Ealing New Primary Care Offer Business Case
July 2017 17
responded by reporting that they were not going on line for their bookings. Those who did
not reply formed the smallest group within our sample. The cross section of respondents
in this sample clearly demonstrates a discrepancy between commuters and non-
commuters. Commuters were predominantly on-line and if not would consider registering
to enable online access to their GP. Whereas a significant number of respondents who
were not commuters but locality patients were not online and were either unsure as to
whether they could register online or didn’t want to.
7. Regarding willingness or agreeing to start booking appointments online, the majority of
our respondents said they were agreeable to do so. However there were two further
significant groups consisting of respondents who did not wish to reply to this question
and those who said they would not like to go online to book their appointments. It is our
assertion that the majority numbers are very likely commuters and those respondents
who were less willing to try on-line booking are Ealing based non-commuters. It will be
interesting to identify in the full report the further demographic of these groups.
In general, our survey makes it evident that although there is public awareness about
online services, which many patients use there are also significant numbers who do not
wish to book appointments online. This is assignable to a variety of reasons that include
the following: people not being computer literate (especially older people), illiteracy, not
having a computer, not having internet access, problems with their Password, not liking
the impersonal nature of online services, and inability to book appointments well into the
future (1 or 2 weeks) via using online services.
8. From responses to the choice of extended opening hours for local surgeries, it is evident
that our respondents considered Monday to Friday evenings the most popular. This was
very closely followed by a preference for Saturday extended hours.
Monday to Friday mornings was voted 3rd in order of preference and Sunday received the
least support from our respondents. A small number of patients said they were happy
with the opening times at present and did not want any change. An almost equal number
did not give any response.
9. Responses to our questionnaire revealed that nearly all respondents were aware about
Nurses being present in GP surgeries. There were a small number who said they did not
know about Nurses or were “Not Sure” about them/their services.
A much smaller sample identified an awareness of Healthcare Assistants (HCAs).
However, a significantly high number of respondents in our sample, reported being
unsure about HCAs.
Awareness of Clinical Pharmacists received the highest number of “No” responses from
our respondents. Patients also responded in good numbers saying that they were “Not
Sure” about services offered by Clinical Pharmacists at their GP practice. In this case,
most respondents were aware of and utilised chemists nearby, but not within the surgery.
10. From patient responses it is clear that there is low awareness of the Urgent Care
Centre (UCC) as well as the NHS111 service. A number of those who said they knew of
the UCC were older people or those with young children who knew about it because they
had already used its services. Similarly, it can be said that most of those who said they
knew about NHS 111 were those who had used the service.

Ealing New Primary Care Offer Business Case
July 2017 18
Comparing awareness of both, it is clear that more people mentioned being aware of the
UCC than that of NHS111. Very few respondents were in the Did Not Answer (or DNA)
category as regards both UCC and NHS 111 services.
Some other observations from Healthwatch
1. It appears that those patients who made online appointments also tended to have fewer
problems in booking GP appointments.
2. Those who booked online also tended to be aware of NHS 111 services.
3. Though some older people in their 50s and 60s reported to be online service users, there
were also many among that particular group who said that they were not going online.
They also tended to be prominent among those who clearly said they did not want to go
online for making appointments, were unsure about it or were reluctant to go online
because they preferred phoning their Surgery or had other practical reasons (already
mentioned above) for not making use of Online GP services.
4. Many disabled people seemed to be unaware of various NHS services such as UCC,
NHS 111 or HCA.
2.2 Case for change
From data and conversations with patients, clinicians and other stakeholders, it is recognised
that general practice in Ealing is facing a range of urgent challenges. These are set out in the
sections below.
2.2.1 Patient Perspective
The GP Patient Survey consistently reports a poorer experience of making an appointment and
lower levels of satisfaction with practice opening times among patients in Ealing CCG’s
catchment area than among patients in other CCGs in London. Latest available data from July
2017 indicates that 67% of patients in Ealing report a positive experience of making an
appointment with their practice, compared to 69% average across London and 74% average
nationally. In terms of opening hours, 72% of patients in Ealing reported they were happy with
opening hours, compared to 76% nationally5. This is also in line with feedback from local Ealing
Healthwatch surveys. A patient’s ease of access to their Practice, and preferred GP, can affect
their experience and quality of care and health outcomes.6
The SCF confirms that good access to primary care should consist of rapid access for patients
who want to speak to someone as soon as possible, continuity of care for patients with on-going
health needs or vulnerable groups who need to be understood by everyone they see and
convenient access for patients who work during core hours and who may want to access primary
care through multiple channels.
5 GP Patient Survey results, July 201. Fieldwork January to March 2017: https://gp-
patient.co.uk/SurveysAndReports 6 The King’s Fund, (2012) Exploring the association between quality of care and the experience
of patients London

Ealing New Primary Care Offer Business Case
July 2017 19
Good access to general practice has an impact on the health system overall. Inadequate
capacity in General Practice can lead to an increase in demand for Accident & Emergency
(A&E), and other hospital services.7 The National Audit Office reported in 2015 that nationally
practices that were open for 45 hours or less per week had, on average, an 8% higher A&E
attendance rate, after adjusting for differences in patients’ age and gender.8
Overall it is important that Ealing CCG focus on improving patient access to primary care, both
to improve patient experience and to reduce potentially increased costs in the acute sector.
2.2.2 Population Perspective
The STP commits to providing care for the population of Ealing. Historically, primary care
provision and a number of services commissioned from primary care were commissioned based
on whether a practice had the expertise or interest in delivering a service. When the OOH
contract was commissioned the clear principle was that all services could be accessed by all
patients, even though their own practice may not deliver all the services. The IT system
(SystmOne) enabled referrals to be sent between practices, so that patients did not have to
travel very far to receive a slightly more enhanced or specialised service. This principle must be
carried forward and all patients no matter which practice they are registered with should be able
to access all services.
The STP also describes clearly the intention to move to a more proactive approach to care,
focussing on not only diagnosis and treatment but prevention and screening. Primary care has a
significant role to play in delivering the much needed proactive and prevention strategy.
However, with the increasing demands on practices, and an elderly population who require more
support and continuity, primary care is in danger of side lining the important prevention
discussions. If primary care are not effectively commissioned and targeted to deliver their part of
the prevention pathway, as has been described in a number of national programmes, the NHS
will soon become unaffordable.
2.2.3 General Practice perspective
Primary care in Ealing is under unprecedented strain, with a rise in the number of appointments and increasing numbers of practices who report that their current workload is unmanageable or unsustainable. This is supported by Figure 12, which shows that the number of registered patients per FTE GP in Ealing is significantly higher than the London and England averages, and the number of registered patients per FTE Nurse in Ealing is comparable to the London average, but significantly higher than the England average.
Figure 12: Number of patients per FTE GP and Nurse in Ealing
7 Rosen R., (2014) Meeting need or fuelling demand? London: Nuffield Trust & NHS England
8 National Audit Office (2015) A Stocktake of Access to General Practice and (2017), improving
access to general practice

Ealing New Primary Care Offer Business Case
July 2017 20
NOTE: This data does not include locum GPs and 9 practices did not report their data
The current GP workforce in Ealing is ageing and facing a ‘retirement bubble’ which has the potential to put the system under greater strain. This is set out in 13, which shows that some localities in Ealing (such as Central Ealing and South Central Ealing) have a much higher proportion of workforce over 55 than the London and England averages. In addition, 21% of practices in Ealing are single handed, which is the third highest proportion of single handed practices in London, after Barking and Dagenham and Havering. If GPs in single handed practices retire or are otherwise unable to work then this can pose significant business continuity issues and impact negatively on patient care.
Figure 13: Percentage of workforce over 55 in Ealing

Ealing New Primary Care Offer Business Case
July 2017 21
Currently there is little support for struggling GP practices, with an increased number of practices
facing closure or serious viability issues. Ealing CCG urgently needs to address these issues to
ensure long term sustainability within the health economy and positive outcomes for patients.
In addition to the workforce concerns, the OOH Contract, Dementia and Paediatric Phlebotomy
contracts issued by Ealing CCG are due to end in April 2018 and agreement needs to be
reached to commit to this funding on going. Having a registered GP providing, managing and
coordinating the care included in the standard will ensure patients can receive appropriate care
closer to home and the cost of delivering care is reduced. To ensure these benefits continue to
accrue, a new contract and business case for the delivery of enhanced primary care in general
practice is required.
The continued investment of the funds for the OOH contracts will ensure the good work that has
been undertaken in primary care to deliver an enhanced range of services across the borough,
as well as supporting practices to develop its core service offering and improving access, will
help practices to plan longer term, and feel confident to commit to recruiting staff, improving
resilience, sustainability and continuity of care for patients.
2.2.4 Economic Case
General practice has a critical role to play in all 5 of the Delivery Areas articulated in the STP
and is the golden thread running through the STP:

Ealing New Primary Care Offer Business Case
July 2017 22
Figure 14: Role of Primary Care in delivering the STP
Without primary care, many of the system benefits would not be realised, This ranges from
complementing and delivering components of the prevention strategy led by Public Health, to
ensuring people with Mental Health needs are identified early and sign posted to the right
support services, and from ensuring the role as the navigator to the rest of the health system is
being delivered optimally, supported by the rest of the system and ensuring individuals with
complex needs have continuity of care and get the right support at the right time to reduce the
risk of deterioration.
It is essential to note that primary care cannot deliver this on its own, but as part of a system
aligned to deliver to the same outcomes.
In order for primary care to deliver its part of the pathway, it is essential to commission and
support primary care to become resilient and transformed in a way that ensures sustainability, so
that it is not working in isolation from each other or from the rest of the system.
2.2.5 Financial sustainability
In Ealing over the next 15 years we expect to see larger rises in the segments of the population
that have increased health needs than in the wider population. This means that activity, and the
cost of delivering services, will increase faster than our overall headline population growth would
imply. NHS budgets, while increasing more than other public sector budgets, are constrained
and significantly below both historical funding growth levels and the expected increase in
demand, while social care budgets face cuts of around 40%. If we do nothing, the NHS in Ealing
will have a significant funding gap by 20/21.
Ealing CCG faces the continued financial challenge to deliver more with constrained resources.
The gap between the expected growth in demand and the expected growth in the financial
allocations (the amount of money available to Ealing CCG) requires the CCG to identify
approximately £67m of savings between 2017/18 and 2020/21. These savings are targeted to be
achieved by reducing spend in the acute setting and shifting it into the out of hospital setting. In
order to implement this strategy, Ealing CCG will need to revise and invest in its primary care
offer to patients and practices as well as considering the investment and offer in the broader out
of hospital landscape.
2.2.6 Headroom funding opportunity
Ealing CCG’s NHS England funding allocation is being increased on a yearly and recurrent basis
up to 2020/21 such that the 2020/21 allocation is 25% greater than the 2016/17 allocation. The
increase in allocation (known as ‘headroom funding’) is in recognition of the comparatively low
levels of primary care funding received by Ealing primary care. Figure 15 shows the average
payment per weighted patient made to practices across London, England and the CWHHE
CCGs for core services, and shows that Ealing practices currently receive significantly less than
the London and England averages and the lowest of the CWHHE CCGs.

Ealing New Primary Care Offer Business Case
July 2017 23
Figure 15: Average pounds per weighted patient payment made to CCGs
Ealing CCG has committed to investing the headroom funding into primary care, and therefore
has the opportunity to improve funding to general practice – positively impacting on practice
resilience, skill mix, long term sustainability and taking the opportunity to reduce unwarranted
variation in outcomes.
2.2.7 High administrative burden
At present primary care deliver a number of isolated contracts, with a high administrative burden
and costs. In developing any future commissioning options an aim must be to reduce the
unnecessary administrative burden and complexity. The OOH contract is a real example in how
not to make the monitoring of any contract so complex that it has unexpected consequences on
practice administrative burden. With Ealing CCG now with delegated responsibility, there is a
real opportunity to reduce the number of contracts, payment mechanisms and reconciliation
processes without reducing the value from rigorously monitoring the mobilisation and delivery of
future contracts.
2.2.8 Case for change summary
It is now clear that the pressures on general practice in Ealing are so significant – and increasing
- that doing nothing is not an option. Taking no action will result in a deterioration of the current
position in terms of:
Increased financial unsustainability;
Poorer access and longer waiting times for patients;
Reduced services available to patients in the primary care setting
A disenfranchised and demoralised workforce which cannot manage demand, or
innovate to improve services.
Ealing CCG now has the opportunity to address these pressures by revising its offer to patients
and practices for the delivery of enhanced primary care.

Ealing New Primary Care Offer Business Case
July 2017 24
2.3 Investment objectives
To address the case for change, Ealing CCG has developed the some investment objectives
which were agreed by the Primary Care Specification Steering Group for the new primary care
offer:
Standardise what patients can expect from primary care in Ealing, reducing unwarranted
variation in access and improving outcomes;
Improve sustainability and resilience of primary care in Ealing;
Achieve value for money and equity of funding across primary care;
Reduce pressure on acute sector; and,
Move towards a goals based commissioning approach.
Ealing New Primary Care Offer Business Case
July 2017 25
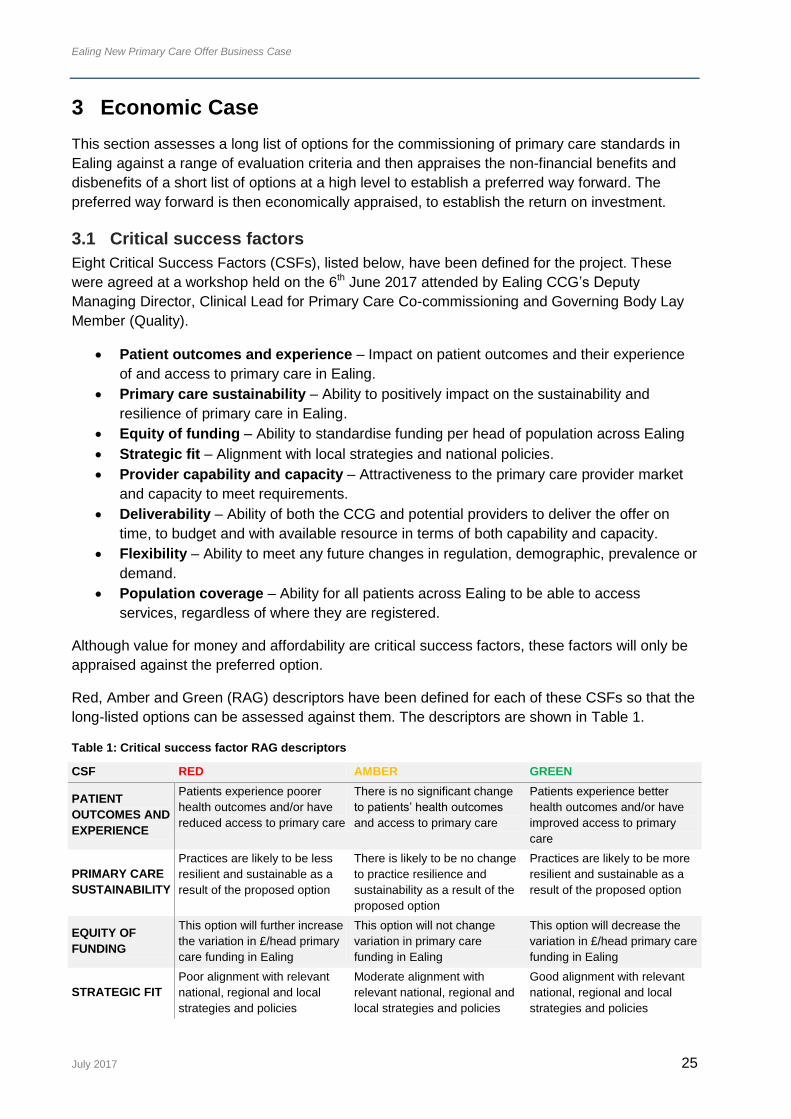
3 Economic Case
This section assesses a long list of options for the commissioning of primary care standards in
Ealing against a range of evaluation criteria and then appraises the non-financial benefits and
disbenefits of a short list of options at a high level to establish a preferred way forward. The
preferred way forward is then economically appraised, to establish the return on investment.
3.1 Critical success factors
Eight Critical Success Factors (CSFs), listed below, have been defined for the project. These
were agreed at a workshop held on the 6th June 2017 attended by Ealing CCG’s Deputy
Managing Director, Clinical Lead for Primary Care Co-commissioning and Governing Body Lay
Member (Quality).
Patient outcomes and experience – Impact on patient outcomes and their experience
of and access to primary care in Ealing.
Primary care sustainability – Ability to positively impact on the sustainability and
resilience of primary care in Ealing.
Equity of funding – Ability to standardise funding per head of population across Ealing
Strategic fit – Alignment with local strategies and national policies.
Provider capability and capacity – Attractiveness to the primary care provider market
and capacity to meet requirements.
Deliverability – Ability of both the CCG and potential providers to deliver the offer on
time, to budget and with available resource in terms of both capability and capacity.
Flexibility – Ability to meet any future changes in regulation, demographic, prevalence or
demand.
Population coverage – Ability for all patients across Ealing to be able to access
services, regardless of where they are registered.
Although value for money and affordability are critical success factors, these factors will only be
appraised against the preferred option.
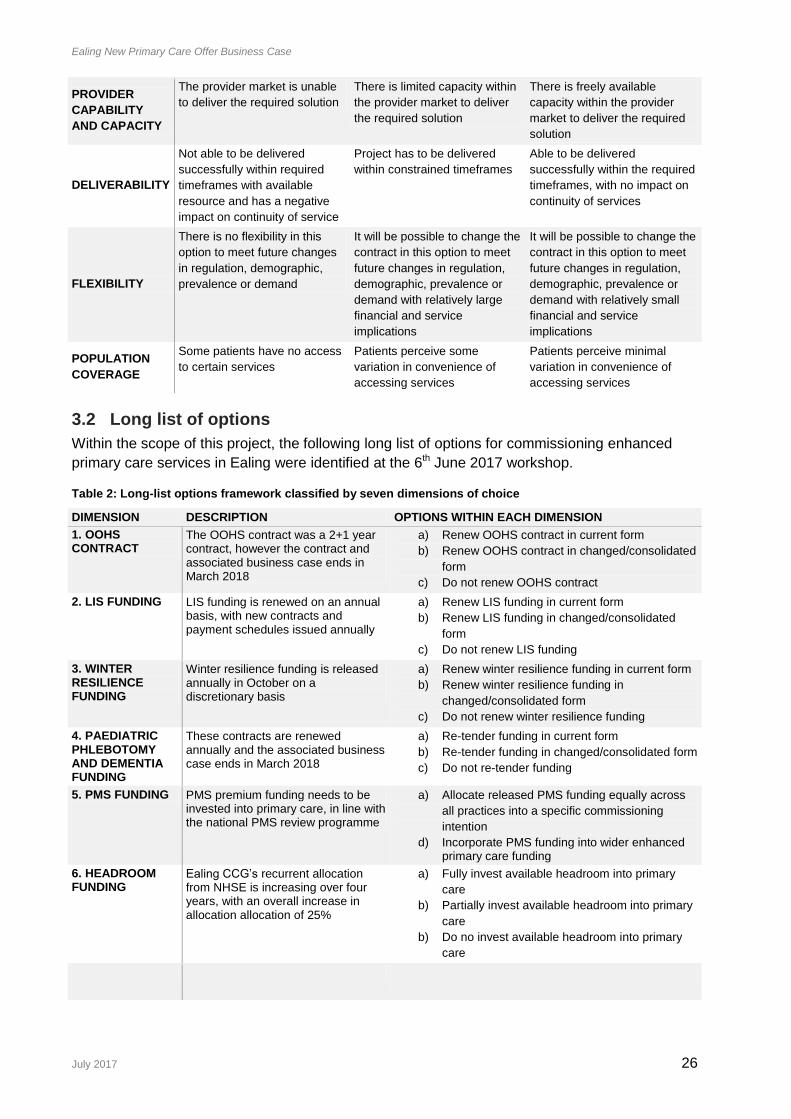
Red, Amber and Green (RAG) descriptors have been defined for each of these CSFs so that the
long-listed options can be assessed against them. The descriptors are shown in Table 1.
Table 1: Critical success factor RAG descriptors
CSF RED AMBER GREEN
PATIENT
OUTCOMES AND
EXPERIENCE
Patients experience poorer
health outcomes and/or have
reduced access to primary care
There is no significant change
to patients’ health outcomes
and access to primary care
Patients experience better
health outcomes and/or have
improved access to primary
care
PRIMARY CARE
SUSTAINABILITY
Practices are likely to be less
resilient and sustainable as a
result of the proposed option
There is likely to be no change
to practice resilience and
sustainability as a result of the
proposed option
Practices are likely to be more
resilient and sustainable as a
result of the proposed option
EQUITY OF
FUNDING
This option will further increase
the variation in £/head primary
care funding in Ealing
This option will not change
variation in primary care
funding in Ealing
This option will decrease the
variation in £/head primary care
funding in Ealing
STRATEGIC FIT
Poor alignment with relevant
national, regional and local
strategies and policies
Moderate alignment with
relevant national, regional and
local strategies and policies
Good alignment with relevant
national, regional and local
strategies and policies
Ealing New Primary Care Offer Business Case
July 2017 26
PROVIDER
CAPABILITY
AND CAPACITY
The provider market is unable
to deliver the required solution
There is limited capacity within
the provider market to deliver
the required solution
There is freely available
capacity within the provider
market to deliver the required
solution
DELIVERABILITY
Not able to be delivered
successfully within required
timeframes with available
resource and has a negative
impact on continuity of service
Project has to be delivered
within constrained timeframes
Able to be delivered
successfully within the required
timeframes, with no impact on
continuity of services
FLEXIBILITY
There is no flexibility in this
option to meet future changes
in regulation, demographic,
prevalence or demand
It will be possible to change the
contract in this option to meet
future changes in regulation,
demographic, prevalence or
demand with relatively large
financial and service
implications
It will be possible to change the
contract in this option to meet
future changes in regulation,
demographic, prevalence or
demand with relatively small
financial and service
implications
POPULATION
COVERAGE
Some patients have no access
to certain services
Patients perceive some
variation in convenience of
accessing services
Patients perceive minimal
variation in convenience of
accessing services
3.2 Long list of options
Within the scope of this project, the following long list of options for commissioning enhanced
primary care services in Ealing were identified at the 6th June 2017 workshop.
Table 2: Long-list options framework classified by seven dimensions of choice
DIMENSION DESCRIPTION OPTIONS WITHIN EACH DIMENSION
1. OOHS CONTRACT
The OOHS contract was a 2+1 year contract, however the contract and associated business case ends in March 2018
a) Renew OOHS contract in current form
b) Renew OOHS contract in changed/consolidated
form
c) Do not renew OOHS contract
2. LIS FUNDING LIS funding is renewed on an annual basis, with new contracts and payment schedules issued annually
a) Renew LIS funding in current form
b) Renew LIS funding in changed/consolidated
form
c) Do not renew LIS funding
3. WINTER RESILIENCE FUNDING
Winter resilience funding is released annually in October on a discretionary basis
a) Renew winter resilience funding in current form
b) Renew winter resilience funding in
changed/consolidated form
c) Do not renew winter resilience funding
4. PAEDIATRIC PHLEBOTOMY AND DEMENTIA FUNDING
These contracts are renewed annually and the associated business case ends in March 2018
a) Re-tender funding in current form
b) Re-tender funding in changed/consolidated form
c) Do not re-tender funding
5. PMS FUNDING PMS premium funding needs to be invested into primary care, in line with the national PMS review programme
a) Allocate released PMS funding equally across
all practices into a specific commissioning
intention
d) Incorporate PMS funding into wider enhanced primary care funding
6. HEADROOM FUNDING
Ealing CCG’s recurrent allocation from NHSE is increasing over four years, with an overall increase in allocation allocation of 25%
a) Fully invest available headroom into primary
care
b) Partially invest available headroom into primary
care
b) Do no invest available headroom into primary
care

Ealing New Primary Care Offer Business Case
July 2017 27
Six dimensions of choice were identified, with options listed out within each dimension. The
following sections score the options available within each dimension against the CSFs and sets
out the preferred option within each dimension. It should be noted that not all CSFs are
applicable to all option categories and so no score is given where this is the case. It was agreed
at the 6th June workshop that any options scoring red against any CSF would not be considered
further, and if one option scored green against many more CSFs than other options within the
dimension then that would be taken forward for further consideration. If multiple options within a
dimension scored well against the CSFs then they would both be taken forward for further
consideration,
3.2.1 OOHS contract
The Out of Hospital Services (OOHS) contract is commissioned across the CWHHE CCGs and
consists of 18 separate services (please see Appendix 5 OOHS contracts for the full list of
specifications). For OOHS, Ealing CCG contracts with the Ealing GP Federation and separately
with the 76 member practices. In addition, there is a separate tripartite agreement setting out the
responsibilities of all three parties to the agreement. The contract was first commissioned in
Ealing in July 2015 for a period of two years, and subsequently extended to March 2018 as per
the contract terms. There is no option to further extend the contract after March 2018 and
agreement is required for the services to be commissioned on-going.
The options considered within this business case that are available to Ealing CCG to continue to
commission and fund the enhanced primary care services currently sitting within the OOHS
contract are:
Renew OOHS contract in the current form: new business case to be written for the
current funding protocol and service specifications so that the current conditions of the
OOHS contract are replicated exactly.
Renew OOHS contract in a changed or consolidated form within the primary care
standard: OOHS services and funding to be incorporated into a single wraparound
contract, together with other enhanced primary care services, to ensure a single
consistent offer across the borough that takes a population based approach and has
equal funding for each practice.
Do not renew OOHS contract: OOHS services and associated funding to terminate at the
end of March 2018 with no replacement in place.
Table 3 summarises how the three options for commissioning services currently within the
OOHS contract score against the CSFs. It demonstrates that renewing the OOHS contract in a
changed form scores highest against the CSFs and therefore is the preferred way forward for
the OOHS contract dimension.

Ealing New Primary Care Offer Business Case
July 2017 28
Table 3: CSF scoring for the OOHS contract options
CSF RENEW IN CURRENT FORM RENEW IN CHANGED
FORM
DO NOT RENEW
PATIENT
OUTCOMES AND
EXPERIENCE
No change is expected in patient experience with this option
Patient experience expected to improve as the service specifications will be improved in response to patient feedback
No OOHS services therefore patient experiences and outcomes will be poorer
PRIMARY CARE
SUSTAINABILITY
No change is expected in primary care sustainability with this option
Primary care sustainability expected to improve as the service specifications will be improved in response to practice feedback
No OOHS funding therefore primary care sustainability will be reduced as there is a lower level of funding
EQUITY OF
FUNDING
No change is expected in equity of funding with this option
Wraparound contract to ensure equity of funding
Equal withdrawal of funding across the 76 practices therefore no impact
STRATEGIC FIT This option does not align with national accountable care organisation themed programmes/strategies
Population based approach aligns with national accountable care organisation themed programmes/strategies
Not offering OOHS is not in line with national primary care policies
PROVIDER
CAPABILITY AND
CAPACITY
The provider market already delivers this option well
It may be difficult to find sufficient capacity and the correct skill mix in the local workforce
n/a if contract not offered
DELIVERABILITY The provider market already delivers this option well
Project has to be delivered within constrained timeframes with several different services incorporated into the wraparound
Not offering the contract will have a negative impact on continuity of service
FLEXIBILITY This contract offers moderate flexibility as it is CWHHE wide
The local nature will enable the contract to be written flexibility
Not offering the contract means there is no flexibility in the future to react to changes in OOHS needs
POPULATION
COVERAGE
This option offers moderate population coverage, however patients have reported limited access to some services
Unclear if population coverage will improve until all 76 providers have signed up
Not offering the contract will mean there is no population coverage
SUMMARY Option not taken forward Option taken forward Option not taken forward
3.2.2 LIS contract
The Ealing CCG Local Improvement Scheme (LIS) is an annually renewed contract with the
following objectives:
Network Development and Unplanned Care
Planned Care
Achievement of Local Priorities
Improve the Quality of Prescribing
The services and actions required of the practices by the scheme are updated on an annual
basis. In 2017/18, the Local Improvement Scheme (LIS) commissioned care planning,
hypertension, atrial fibrillation, Improved Access to Psychological Therapies (IAPT), asthma,
cancer and Chronic Kidney Disease (CKD) services, together with a prescribing incentive
scheme. The LIS also has certain pre-qualifying business management criteria and a quality and
clinical component. The total funding associated with the LIS in 2017/18 was £5/registered
patient.

Ealing New Primary Care Offer Business Case
July 2017 29
The options considered within this business case that are available to Ealing CCG to continue to
commission and fund the enhanced primary care services currently sitting within the LIS contract
are:
Renew the LIS contract in the current form: renew the LIS contract through to 2018/19,
updating or changing any specific services required in the contract as in previous years.
Renew the LIS contract in a changed or consolidated form: LIS services and funding to
be incorporated into a single wraparound contract, together with other enhanced primary
care services, to ensure a single consistent offer across the borough that takes a
population based approach and has equal funding for each practice.
Do not renew the LIS contract: LIS services and associated funding to terminate at the
end of March 2018 with no replacement in place.
Table 4 summarises how the three options for commissioning services currently within the LIS
contract score against the CSFs. It demonstrates that renewing the LIS contract in a changed
form scores highest against the CSFs and therefore is the preferred way forward for the LIS
contract dimension.
Table 4: CSF scoring for the LIS contract options
CSF RENEW IN CURRENT FORM RENEW IN CHANGED
FORM
DO NOT RENEW
PATIENT
OUTCOMES AND
EXPERIENCE
No change is expected in patient experience with this option
Patient experience expected to improve as the service specifications will be improved in response to patient feedback
No LIS contract therefore patient experiences and outcomes will be poorer
PRIMARY CARE
SUSTAINABILITY
No change is expected in primary care sustainability with this option
Primary care sustainability expected to improve as the service specifications will be improved in response to practice feedback
No LIS contract therefore primary care sustainability will be reduced as there is a lower level of funding
EQUITY OF
FUNDING
No change is expected in equity of funding with this option
Wraparound contract to ensure equity of funding
Equal withdrawal of funding across the 76 practices therefore no impact
STRATEGIC FIT The LIS contract already has moderate alignment with national accountable care organisation themed programmes/strategies
Population based approach aligns with national accountable care organisation themed programmes/strategies
Not offering the funding and requirements of the LIS at all is not in line with national primary care policies
PROVIDER
CAPABILITY AND
CAPACITY
The provider market already delivers this option well
It may be difficult to find sufficient capacity and the correct skill mix in the local workforce
n/a if contract not offered
DELIVERABILITY The provider market already delivers this option well
Project has to be delivered within constrained timeframes with several different services incorporated into the wraparound
Not offering the contract will have a negative impact on continuity of service
FLEXIBILITY The contract is renewed locally every year and therefore already offers flexibility.
The local nature will enable the contract to be written flexibility
Not offering the contract means there is no flexibility in the future to react to changes in CCG/population needs
POPULATION
COVERAGE
This option offers moderate population coverage, however patients have reported limited access to some services
Unclear if population coverage will improve until all 76 providers have signed up
Not offering the contract will mean there is no population coverage
SUMMARY Option not taken forward Option taken forward Option not taken forward
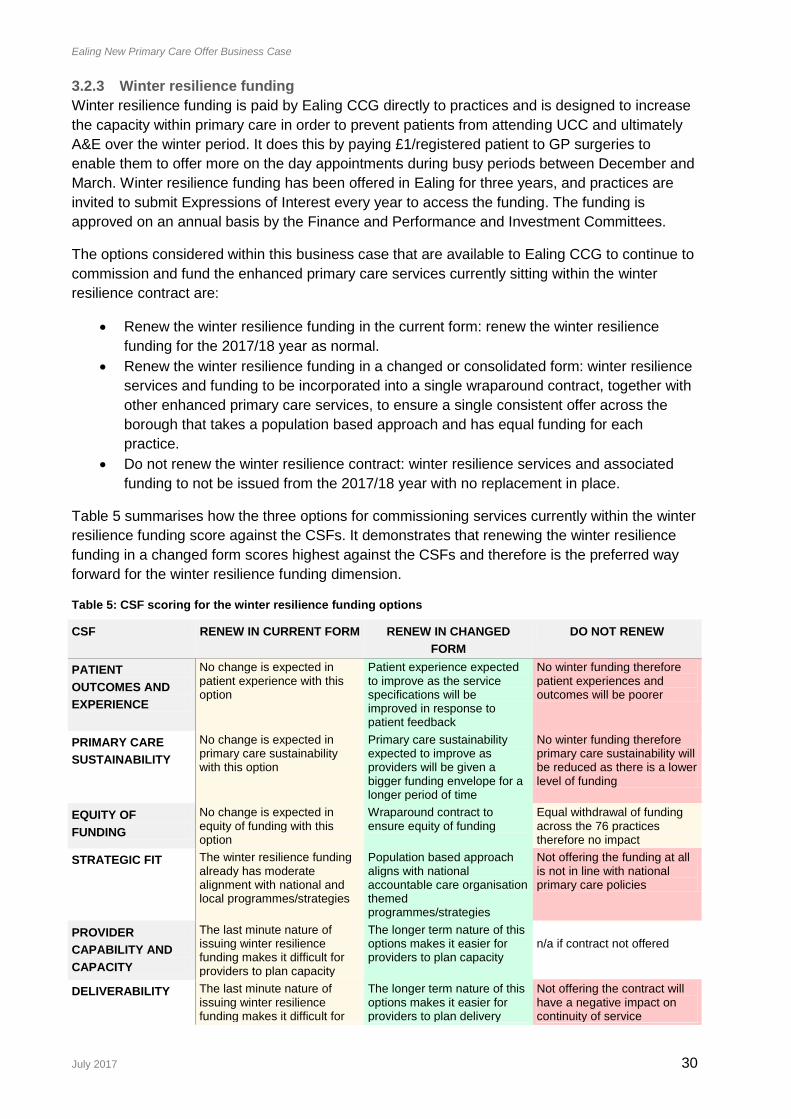
Ealing New Primary Care Offer Business Case
July 2017 30
3.2.3 Winter resilience funding
Winter resilience funding is paid by Ealing CCG directly to practices and is designed to increase
the capacity within primary care in order to prevent patients from attending UCC and ultimately
A&E over the winter period. It does this by paying £1/registered patient to GP surgeries to
enable them to offer more on the day appointments during busy periods between December and
March. Winter resilience funding has been offered in Ealing for three years, and practices are
invited to submit Expressions of Interest every year to access the funding. The funding is
approved on an annual basis by the Finance and Performance and Investment Committees.
The options considered within this business case that are available to Ealing CCG to continue to
commission and fund the enhanced primary care services currently sitting within the winter
resilience contract are:
Renew the winter resilience funding in the current form: renew the winter resilience
funding for the 2017/18 year as normal.
Renew the winter resilience funding in a changed or consolidated form: winter resilience
services and funding to be incorporated into a single wraparound contract, together with
other enhanced primary care services, to ensure a single consistent offer across the
borough that takes a population based approach and has equal funding for each
practice.
Do not renew the winter resilience contract: winter resilience services and associated
funding to not be issued from the 2017/18 year with no replacement in place.
Table 5 summarises how the three options for commissioning services currently within the winter
resilience funding score against the CSFs. It demonstrates that renewing the winter resilience
funding in a changed form scores highest against the CSFs and therefore is the preferred way
forward for the winter resilience funding dimension.
Table 5: CSF scoring for the winter resilience funding options
CSF RENEW IN CURRENT FORM RENEW IN CHANGED
FORM
DO NOT RENEW
PATIENT
OUTCOMES AND
EXPERIENCE
No change is expected in patient experience with this option
Patient experience expected to improve as the service specifications will be improved in response to patient feedback
No winter funding therefore patient experiences and outcomes will be poorer
PRIMARY CARE
SUSTAINABILITY
No change is expected in primary care sustainability with this option
Primary care sustainability expected to improve as providers will be given a bigger funding envelope for a longer period of time
No winter funding therefore primary care sustainability will be reduced as there is a lower level of funding
EQUITY OF
FUNDING
No change is expected in equity of funding with this option
Wraparound contract to ensure equity of funding
Equal withdrawal of funding across the 76 practices therefore no impact
STRATEGIC FIT The winter resilience funding already has moderate alignment with national and local programmes/strategies
Population based approach aligns with national accountable care organisation themed programmes/strategies
Not offering the funding at all is not in line with national primary care policies
PROVIDER
CAPABILITY AND
CAPACITY
The last minute nature of issuing winter resilience funding makes it difficult for providers to plan capacity
The longer term nature of this options makes it easier for providers to plan capacity
n/a if contract not offered
DELIVERABILITY The last minute nature of issuing winter resilience funding makes it difficult for
The longer term nature of this options makes it easier for providers to plan delivery
Not offering the contract will have a negative impact on continuity of service

Ealing New Primary Care Offer Business Case
July 2017 31
providers to plan delivery
FLEXIBILITY The last minute nature of issuing winter resilience funding makes it difficult for providers to plan
The longer term nature of this options makes it easier for providers to plan around other priorities
Not offering the contract means there is no flexibility in the future to react to changes in CCG/population needs
POPULATION
COVERAGE
This option offers moderate population coverage
Unclear if population coverage will improve until all 76 providers have signed up
Not offering the contract will mean there is no population coverage
SUMMARY Option not taken forward Option taken forward Option not taken forward
3.2.4 Paediatric phlebotomy and dementia
The standalone paediatric phlebotomy contract has historically been issued to ensure parents
can access phlebotomy services for their children close to home and to avoid unnecessary
activity in the acute sector. The CCG currently holds multiple contracts with multiple GP
providers, each at a different price and age range. In addition the waiting time to access
paediatric phlebotomy service is increasing and there is limited capacity to deliver the service
within the workforce. The current contract for paediatric phlebotomy ends in March 2018,.
The standalone dementia contract is designed to support discharge of patients with dementia
from secondary to primary care. The contract is designed to encourage joined up working
between practices involved and West London Mental Health trust. The contract was first issued
in 2016 and was aligned to end at the same time of OOHS, at which point a more holistic view
could be taken about the future of the service.
The options considered within this business case that are available to Ealing CCG to continue to
commission and fund the enhanced primary care services currently sitting within the paediatric
phlebotomy and dementia contracts are:
Re-tender the paediatric phlebotomy and dementia contracts in the current form: new
business case to be written for the current service specifications so that the current
conditions of the paediatric phlebotomy and dementia contracts are replicated exactly.
Commitment to renewing the paediatric phlebotomy and dementia contracts in a
changed or consolidated form: the relevant services and funding to be incorporated into
a single wraparound contract, together with other enhanced primary care services, to
ensure a single consistent offer across the borough that takes a population based
approach and has equal funding for each practice.
Do not re-tender the paediatric phlebotomy and dementia contracts: relevant services
and associated funding to terminate at the end of March 2018 with no replacement in
place.
Table 6 summarises how the three options for commissioning services currently within the
paediatric phlebotomy and dementia contracts score against the CSFs. It demonstrates that
renewing the paediatric phlebotomy and dementia contracts in a changed form scores highest
against the CSFs and therefore is the preferred way forward for the paediatric phlebotomy and
dementia contracts dimension.

Ealing New Primary Care Offer Business Case
July 2017 32
Table 6: CSF scoring for the paediatric phlebotomy and dementia contract options
CSF RE-TENDER IN CURRENT
FORM
RENEW IN CHANGED
FORM
DO NOT RE-TENDER
PATIENT
OUTCOMES AND
EXPERIENCE
No change is expected in patient experience with this option
Patient experience expected to improve as the service specifications will be improved in response to patient feedback
No paediatric phlebotomy and dementia services therefore patient experiences and outcomes will be poorer
PRIMARY CARE
SUSTAINABILITY
No change is expected in primary care sustainability with this option
Primary care sustainability expected to improve as providers will be given a bigger funding envelope for a longer period of time
No additional funding therefore primary care sustainability will be reduced
EQUITY OF
FUNDING
No change is expected in equity of funding with this option
Wraparound contract to ensure equity of funding
Equal withdrawal of funding across the 76 practices therefore no impact
STRATEGIC FIT This funding already has moderate alignment with national and local programmes/strategies
Population based approach aligns with national accountable care organisation themed programmes/strategies
Not offering the services at all is not in line with national primary care policies
PROVIDER
CAPABILITY AND
CAPACITY
There is limited provider capacity for paediatric phlebotomy and good capacity for dementia
It may be difficult to find sufficient capacity and the correct skill mix in the local workforce
n/a if contract not offered
DELIVERABILITY The contract must be retendered at the end of 2017/18
Project has to be delivered within constrained timeframes with several different services incorporated into the wraparound
Not offering the contract will have a negative impact on continuity of service
FLEXIBILITY Retendering the contract at the end of this FY offers the opportunity to address and new priorities
The local nature will enable the contract to be written flexibility
Not offering the contract means there is no flexibility in the future to react to changes in CCG/population needs
POPULATION
COVERAGE
There is moderate population coverage for paediatric phlebotomy and poor coverage for dementia services
Unclear if population coverage will improve until all 76 providers have signed up
Not offering the contract will mean there is no population coverage
SUMMARY Option not taken forward Option taken forward Option not taken forward
3.2.5 PMS funding
Of the 76 practices in Ealing CCG, 7 practices have locally negotiated Personal Medical
Services (PMS) contracts that have a different level of core funding to providers with nationally
negotiated General Medical Services (GMS) contracts. Ealing CCG is required to review and
renegotiate all PMS contracts with the aim of securing best value from future investment of the
‘premium’ element of PMS funding. Under delegated commissioning arrangements, Ealing CCG
is responsible for the commissioning arrangements related to PMS funding.
The level of “PMS premium” funding currently invested in contracts with Ealing CCG practices is
circa £650k based on the NHSE-derived methodology and understanding at this time. This will
need to be confirmed with the PMS practices themselves. A transition period to equalisation of
contracts may apply for some practices depending on the scale of the financial impact.

Ealing New Primary Care Offer Business Case
July 2017 33
It is intended that as a result of the PMS review any additional investment in general practice
services that go beyond core national requirements should reflect CCG strategic plans for
primary care, help reduce health inequalities and give equality of opportunity to all GP practices
(provided they are able to satisfy locally determined requirements) and support fairer distribution
of funding at a locality level.
The options considered within this business case that are available to Ealing CCG to invest PMS
funding are:
Allocate released PMS funding equally across all practices into a specific commissioning
intention i.e equally split funding across all 76 Ealing CCG practices and invest funding
into a specific commissioning intention.
Incorporate PMS funding into wider enhanced primary care funding: incorporate PMS
funding into a single wraparound contract, together with other enhanced primary care
services, to ensure a single consistent offer across the borough that takes a population
based approach and has equal funding for each practice.
Table 7 summarises how the two options for investing PMS funding score against the CSFs. It
demonstrates incorporating PMS funding into wider enhanced primary care funding scores
highest against the CSFs and therefore is the preferred way forward for the PMS funding
dimension.
Table 7: CSF scoring for PMS funding options
CSF ALLOCATE PMS FUNDING INTO A
SPECIFIC COMMISSIONING INTENTION
INCORPORATE PMS FUNDING INTO
WIDER ENHANCED PRIMARY CARE
FUNDING
PATIENT OUTCOMES
AND EXPERIENCE
Relatively small amount of funding there difficult to make a meaningful change to patient experience
Improved patient outcomes as small funding amount gets incorporated into wider wraparound pot giving a multiplier effect
PRIMARY CARE
SUSTAINABILITY
Relatively small amount of funding there difficult to make a meaningful change to sustainability
Improved sustainability as small funding amount gets incorporated into wider wraparound pot giving a multiplier effect
EQUITY OF FUNDING Relatively small amount of funding there difficult to make a meaningful change to equity of funding
Improved equity of funding as small funding amount gets incorporated into wider wraparound pot giving a multiplier effect
STRATEGIC FIT Completing the PMS review is strategically in line with national policy
Completing the PMS review is strategically in line with national policy
PROVIDER CAPABILITY
AND CAPACITY
Provider market likely to have capacity to deliver a relatively small contract
It may be difficult to find sufficient capacity and the correct skill mix in the local workforce
DELIVERABILITY Any standalone PMS review investment contract would be small and independent of other contracts and therefore easy to deliver
Project has to be delivered within constrained timeframes with several different services incorporated into the wraparound
FLEXIBILITY The small funding amount would require a very targeted and therefore inflexible contract to invest the funding into
Improved flexibility as small funding amount gets incorporated into wider wraparound pot giving a multiplier effect
POPULATION
COVERAGE
Unclear if population coverage will improve until all 76 providers have signed up
Improved population coverage as small funding amount gets incorporated into wider wraparound pot giving a multiplier effect
SUMMARY Option not taken forward Option taken forward
3.2.6 Headroom funding
Ealing CCG’s NHS England funding allocation is being increased on a yearly and recurrent basis
up to 2020/21 such that the 2020/21 allocation is 25% greater than the 2016/17 allocation. The

Ealing New Primary Care Offer Business Case
July 2017 34
increase in allocation (known as ‘headroom funding’) is in recognition of the comparatively low
levels of primary care funding received by Ealing primary care. A portion of this increase has
been committed to premises rent and rate reviews, funding as per standing financial instructions
and regulations and other specific, pre-committed areas of spend including contingency.
However, the majority of the increase in allocation presents an opportunity to invest in Primary
Care. The options considered within this business case that are available to Ealing CCG to
invest available headroom into primary care are:
Fully invest available headroom into primary care: incorporate headroom funding into a
single wraparound contract, together with other enhanced primary care services, to
ensure a single consistent offer across the borough that takes a population based
approach and has equal funding for each practice.
Do no invest available headroom into primary care: treat the additional funding as a cost
saving against existing targets.
Table 8 summarises how the two options for investing headroom funding score against the
CSFs. It demonstrates that wholly investing the headroom funding into primary care scores
highest against the CSFs and therefore is the preferred way forward for the headroom funding
dimension.
Table 8: CSF scoring for headroom investment options
CSF INVEST WHOLLY IN
PRIMARY CARE
DO NOT INVEST IN
PRIMARY CARE
PATIENT OUTCOMES AND EXPERIENCE Patient experience expected to improve as the service specifications will be improved in response to patient feedback
No improvement to patient outcome will be delivered without any investment
PRIMARY CARE SUSTAINABILITY Primary care sustainability expected to improve as providers will be given a bigger funding envelope for a longer period of time
No improvement to primary care sustainability will be delivered without any investment
EQUITY OF FUNDING Wraparound contract to ensure equity of funding
No impact to funding
STRATEGIC FIT Population based approach aligns with national accountable care organisation themed programmes/strategies
Not investing the headroom at all is not in line with national primary care policies
PROVIDER CAPABILITY AND CAPACITY It may be difficult to find sufficient capacity and the correct skill mix in the local workforce
n/a if contract not offered
DELIVERABILITY Project has to be delivered within constrained timeframes with several different services incorporated into the wraparound
n/a if contract not offered
FLEXIBILITY The local nature will enable the contract to be written flexibility
Not offering the contract means there is no flexibility in the future to react to changes in CCG/population needs
POPULATION COVERAGE Improved population coverage as practices take up and deliver on behalf of each other as per current OOH contract
Not offering the contract will mean there is no population coverage

Ealing New Primary Care Offer Business Case
July 2017 35
SUMMARY Option taken forward Option not taken forward
3.2.7 Summary of long list analysis
The assessment of long-listed options against the agreed CSFs has confirmed the following
elements of the preferred way forward:
Renew the OOHS, Paediatric Phlebotomy and Dementia contracts in a changed form –
incorporating them within a single wraparound enhanced primary care contract
Renew the LIS and Winter Resilience contracts in a changed form – incorporating them
within a single wraparound enhanced primary care contract
Incorporate PMS funding and headroom funding into wider enhanced primary care
funding
3.3 Short list appraisal
The long list process reviewed all the options available to ECGG, set out in Table 2, and by the
process of scoring the options against the CSFs arrived at the preferred way forward, set out in
Section 3.2.7. In accordance with HM Treasury Green Book guidance, the preferred option must
also be benchmarked against the do nothing and do minimum (in this case the status-quo)
options. This process is usually undertaken to confirm the Value for Money (VfM) of the
preferred option, however in this case a qualitative appraisal of the benefits and dis-benefits of
the preferred option and two benchmarked options will be undertaken, to confirm the relative
benefit of implementing the preferred option. This is because the qualitative appraisal confirms
that the do nothing and do minimum options are not well aligned with the CCG’s publicly stated
aims and commitments of delivering care close to home and investing headroom into primary
care.
3.3.1 Short listed options
The three shortlisted options are described in Table 9.
Table 9: Short listed options
OPTION TITLE DESCRIPTION
1 Do nothing Allow OOHS, paediatric phlebotomy and dementia contracts to end with no replacement, renew LIS and winter resilience funding, make no change to Out of Hours premium funding, invest PMS funding into a specific commissioning intention and treat headroom funding as a cost saving
2 Do minimum (status quo)
Write a business case for renewing OOHS, paediatric phlebotomy and dementia contracts in their current state, renew LIS and winter resilience funding, invest PMS funding into a specific commissioning intention and treat headroom funding as a cost saving
3 Preferred Option
Incorporate OOHS, LIS, Winter Resilience, Paediatric Phlebotomy, Dementia, PMS Review and Headroom funding into a single wraparound contract delivering enhanced primary care using a population based approach against a set of standards forming an Ealing Standard.
These options were agreed with the Deputy Managing Director at Ealing CCG as the most likely
scenarios in the do nothing and do minimum cases. In particular it was felt that renewing LIS and
winter resilience funding has become a part of business as usual within Ealing CCG and
therefore offering that funding is likely in the do nothing scenario.
3.3.2 Short list benefit and dis-benefits analysis
The benefits and dis-benefits of the three shortlisted options were considered by Ealing CCG’s
Clinical Lead for Primary Care Co-Commissioning. This analysis is set out in

Ealing New Primary Care Offer Business Case
July 2017 36
Table 10.
Table 10: Short list benefit and dis-benefit analysis
BENEFITS DIS-BENEFITS
OPTION 1: DO NOTHING
Increased cost savings achieved through not investing headroom and OOHS monies
Reduced overall demand for service delivery at practices – which may benefit practices that are currently understaffed
Gives the opportunity to wait for a national programme to be implemented, which would reduce the costs of implementing any enhanced primary scheme and give national alignment
Short term cost savings contributed towards
The services available to patients in the community would significantly decrease – reducing patient satisfaction and potentially outcomes
The costs of delivering the services currently under OOH would be significantly more expensive elsewhere in the system
Other providers (such as secondary care and mental health providers) would experience a significant increase in demand – destabilising the rest of the system
Reduced integration between health providers within the system
Potentially be forced to adopt a national programme which would not be tailored to local needs and requirements
OPTION 2: DO MINIMUM
Fewer change processes required to transition to this option as CCG and providers are already familiar with the process
Issuing multiple short term contracts allows for greater flexibility from the CCG’s perspective as changes can easily be made to individual contracts
Short term cost savings contributed towards
Activity based contracts makes it difficult for providers to implement long term strategies
Not changing enhanced primary care contracting would not address ongoing concerns within the local system
Some contracts are currently issued annually which makes long term planning difficult for the both CCG and providers
OPTION 3: PREFERRED OPTION
Reduced costs in the acute sector
A four year wraparound contract provides greater security and assurances to the provider landscape about their future stability
Potentially reduced on-costs for the administration of the contract at both commissioner and provider level resulting in a higher percentage of contract value spent on patient care
Reduced risk of overlapping contracts and duplication across multiple contracts
A wraparound contract would result in a more seamless care delivery to patients, with fewer interface issues or contractual gaps
One quality contract would enable simplified communications between the commissioner, provider and patient
Would support delivery of STP
This approach has been implemented in other areas successfully from where the learning has been taken.
Potentially reduced capacity to respond agilely to external factors due to the large size of the contract
The requirement to take a single contracting approach across all specifications reduces flexibility (i.e some specifications can’t be paid by service with others paid on a capitated basis)
Short term cost savings not contributed towards
Overall it was felt that the benefit and dis-benefit analysis reinforced the suitability of the
preferred option. The do nothing option would entirely remove a large section of service delivery
from the primary care setting, making delivery of those services more likely to take place in the
acute setting which is likely to be more expensive and more inconvenient for the patient. The do
minimum option would continue the status quo but not improve the sustainability and resilience
of primary care or address patient concerns over access. The Preferred Option provides the

Ealing New Primary Care Offer Business Case
July 2017 37
opportunity to invest the PMS review and headroom funding into primary care in the long term in
order to deliver meaningful improvements to patient experience and outcomes and also to
reduce cost in the acute sector. The full Return on Investment (RoI) delivered by the preferred
option is further explored in Section 5.
3.4 The preferred option
As set out above, the preferred option for commissioning enhanced primary care within Ealing
CCG is to:
Renew the OOHS, Paediatric Phlebotomy and Dementia contracts in a changed form –
incorporating them within a single wraparound enhanced primary care contract
Renew the LIS and Winter Resilience contracts in a changed form – incorporating them
within a single wraparound enhanced primary care contract
Incorporate PMS funding and headroom funding into wider enhanced primary care
funding
In order to deliver this option, Ealing CCG collaboratively developed a set of standards for the
single wraparound contract, collectively known as the ‘Ealing Primary Care Standard.’ The
development of the standards was overseen by the Ealing CCG ‘Primary Care Steering Group’ –
a group with clinical representation from the Ealing CCG Clinical Leads and local and London-
wide LMC, an Ealing CCG lay governing body member and Ealing CCG senior management.
The development of the standards was led by Clinical Leads and developed in a series of four
Council of Members meetings with Ealing CCG member practices, and additional drop in
sessions. A key learning from the process of commissioning the out of hospital services was the
need for local clinical leadership and this design process has enabled this.
In total there are 23 service specifications included within the Ealing Primary Care Standard, as
set out in Table 11. All of the standards are included in Appendix 1. It should be noted that these
23 include and build on the 18 Out of Hospital specifications.
Table 11: 23 service specifications in the Ealing Primary Care Standard
HEALTHCARE AND LONG TERM CONDITION MANAGEMENT
HEALTHCARE IMPROVEMENT ACCESS, SAFETY AND EXPERIENCE
Mental Health Cancer screening Access Diabetes Prevention Homelessness
Respiratory Self-care & use of patient Activation Measures
Medicines optimisation and medicines safety
Cardiovascular Learning disability Drug monitoring Musculoskeletal Carers Patient experience Ring Pessary Demand management
Care Planning And Coordination Business management (Pre-Qualifier)
End Of Life Care Wound Care Phlebotomy Dementia

Ealing New Primary Care Offer Business Case
July 2017 38
4 Commercial case
4.1 The Commissioning Strategy
Ealing CCG set out in its Annual Commissioning Intention document for 2014/2015 both the
approach they intended to take to commissioning a range of ‘Out of Hospital’ services and their
view that in the majority of instances GPs were the most capable providers of these services.
The CCGs published the intention to let the OOH contract to primary care in Ealing and received
no challenge to either the approach or the commissioning route.
The process incorporates the Out of Hospital framework that the CCGs across CWHHE
developed to support the procurement of out of hospital services. The framework balances the
requirements of complying with the law and reducing legal challenge with the need to make
effective and integrated commissioning decisions that are right for the local population.
The services that the original process covered when the OOH services contract was let are:
Ambulatory blood pressure monitoring (ABPM)
Anticoagulation
Care planning
Chronic Obstructive Pulmonary Disease (COPD)
Diabetes
Electrocardiogram (ECG)
Homeless care
Management of common mental health issues
Mental health – transfer of care
Near patient testing
Phlebotomy
Ring pessary
Vasectomy
Wound care
The second stage of the process includes:
Additional Respiratory Components
Musculoskeletal Services (MSK)
End of Life
Dementia
Cancer Screening
Self Care and Patient Activation Measures
Learning Disability
Carers
Access
Prevention
Medicines Safety and Optimisation
Demand Management
Ankle-Brachial Pressure Index (ABPI)
The process includes setting up an Independent Review Panel to review the recommended
procurement approach for each of the services.
Ealing New Primary Care Offer Business Case
July 2017 39
The panel was asked to review the recommendations for each service in the context of both
national direction and importantly the STP and the CCGs Out of Hospital Strategies.
The panel was made up of:
Lay Member
Non-Conflicted GP (Out of Area)
Quality Lead for CWHHE
Primary Care Manager from NHSE for NWL (2)
The panel considered each service in turn and the outcome was recorded on each of the sheets
for the services. The outputs of the Independent Review can be found in Appendix 6.
The commissioning of the Standard is therefore proposed at an individual practice level on a
direct award basis.
4.2 Payment Mechanisms
Services are split between
capitation-based services 75% for delivery and 25% based on achievement against KPIs
(KPIs are paid on sliding scale of achievement)
activity-based on achievement of agreed Minimum data-set
prevalence-based services based on current Out of Hospital Services. Diabetes is paid
on 40% against prevalence and 60% against achievement at a CCG level. Mental
Health may be paid on a prevalence based mechanism but if not would revert to the
capitation based approach. As the contract is developed over time, the CCG will assess
which of the activity based work, if any, can move to a capitation based model.
The KPIs for the capitation component are weighted based on a range of factors. These are:
• Effective care
• Difficulty to implement
• Patient experience
• Clinical impact elsewhere
• Financial impact elsewhere
• Collaborative working
Practices will be paid on a sliding scale of achievement.
A further 1 % in 18/19 will be allocated (based on affordability) for delivery based on a Goals
Framework Target. In 18/19, the Goals Framework will be aligned to delivery of a reduction in
unwarranted variation in Non-Elective Admissions and unwarranted variation in planned care.
It is not proposed to use the CQUIN function within the NHS Standard contract for this due to the
approach being taken with the payment related to the Goals Framework.

Ealing New Primary Care Offer Business Case
July 2017 40
It is proposed that the KPIs relating to access in the first six month of the contract (October to
March 2017) are not enforced to support mobilisation. It is proposed KPIs are live and
monitored from April 2018.
4.3 Contractual and Other Issues
4.3.1 Type of contract
Practices will be offered a contract for services with a 3.5 year term with the ability to sub
contract to other primary care list based providers.
The quality standards / key performance indicators and specific reporting requirements for
measuring practice performance are set out in each of the standards.
Variations to contract will be in writing and signed by both parties. Variations involving an
increase in price must only be made within the limit of the financial delegated authority.
Practices will be required to make a self-declaration once a year, similar to the process under
the contract management of the Out of Hospital Services – Appendix 7.
Practices are also expected to fulfil all contractual requirements for their core contract, including
all annual declarations to NHSE and CQC as required.
The contract will be held with each individual practice, however, there will be provision in the
contract to allow sub-contracting to other practices to deliver services on their behalf with the
agreement of the CCG.
4.3.2 Contract management
The responsibility for managing delivery under the contract as well as relationship management
will be with the CCG primary care team on the signing of the contract. The CCG will support and
work with practices to ensure that they provide safe care in line with the standard and that all
patients across the borough have access to all the services.
The critical part of the contract is the mobilisation phase – further information in section 6.2.
Ealing New Primary Care Offer Business Case
July 2017 41
5 Financial case
5.1 Available funding
This business case requires funding from both the primary care allocation and the CCG
programme budget as follows:
1. £3.5m worth of headroom funding from the Primary Care allocation from 2018/2019 with
£2.8m being requested in 2017/2018.
2. £7.2m worth of funding from the CCG core budget broken down as:
Renewal of out of hospital services £5.4mRenewal of Paediatric phlebotomy £0.2m,Dementia £0.1m,
LIS £1.1m Winter Resilience funds £0.4m.
3. Additional core funding to support the additional requirements and new standards £923k
This section will set out the approach to costing the standards and the affordability for the CCG
in commissioning the standards.
5.2 Costing of the specifications
A costing model was developed to support the commissioning of the out of hospital services in
2014 across the five CCGs in CWHHE. The Investment Committee has previously reviewed the
approach to the costing model when considering the OOH contract and had the opportunity to
discuss and agree the model. CCGs in CWHHE agreed that when costing services to be
commissioned from primary care this would be the approach used to enable an equitable
approach to the pricing of services. The approach is shown below:
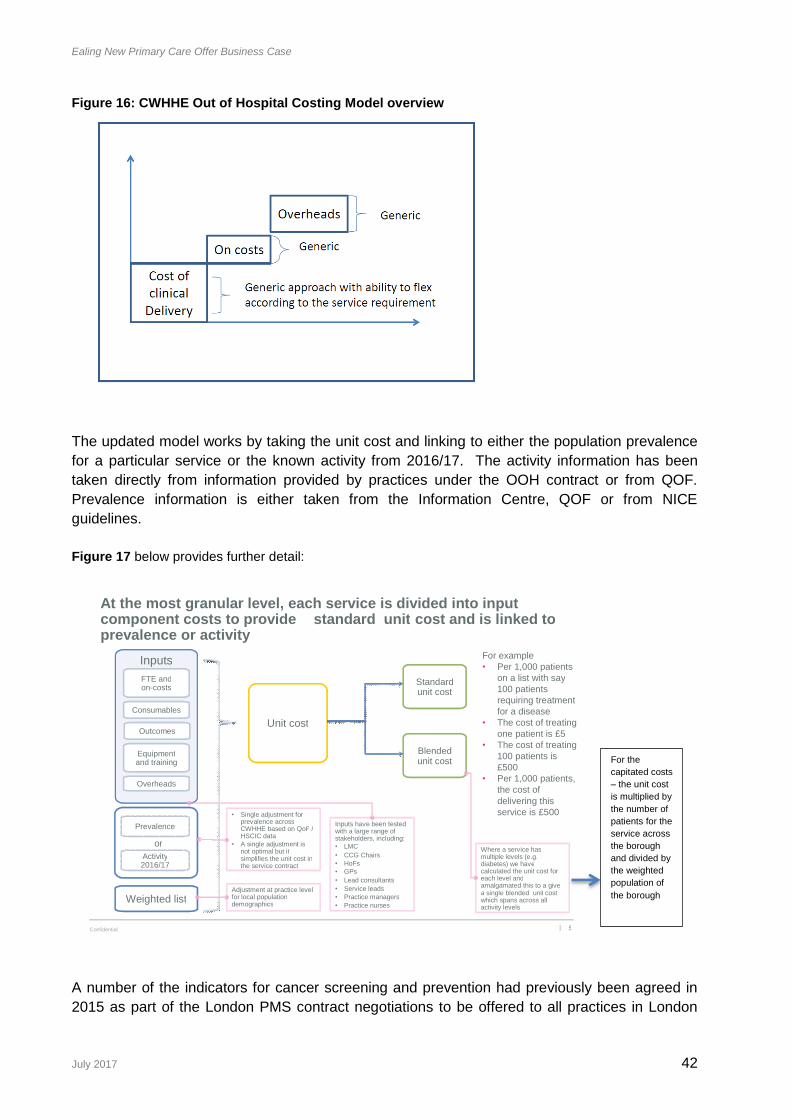
Ealing New Primary Care Offer Business Case
July 2017 42
Figure 16: CWHHE Out of Hospital Costing Model overview
The updated model works by taking the unit cost and linking to either the population prevalence
for a particular service or the known activity from 2016/17. The activity information has been
taken directly from information provided by practices under the OOH contract or from QOF.
Prevalence information is either taken from the Information Centre, QOF or from NICE
guidelines.
Figure 17 below provides further detail:
A number of the indicators for cancer screening and prevention had previously been agreed in
2015 as part of the London PMS contract negotiations to be offered to all practices in London
5 Confidential |
At the most granular level, each service is divided into input component costs to provide standard unit cost and is linked to prevalence or activity
Inputs
FTE and on - costs
Consumables
Equipment and training
Overheads
Standard unit cost
Outcomes U nit cost
Blended unit cost
Where a service has multiple levels (e.g. diabetes) we have calculated the unit cost for each level and amalgamated this to a give a single blended unit cost which spans across all activity levels
I nputs have been tested with a large range of stakeholders, including: • LMC • CCG Chairs • HoFs • GPs • Lead consultants • Service leads • Practice managers • Practice nurses
For example • P er 1,000 patients
on a list with say 100 patients requiring treatment for a disease
• The cost of treating one patient is £5
• The cost of treating 100 patients is £500
• Per 1,000 patients, the cost of delivering this service is £500
Prevalence
Activity 2016/17
Weighted list
• Single adjustment for prevalence across CWHHE based on QoF / HSCIC data
• A single adjustment is not optimal but it simplifies the unit cost in the service contract
A djustment at practice level for local population demographics
or
For the
capitated costs
– the unit cost
is multiplied by
the number of
patients for the
service across
the borough
and divided by
the weighted
population of
the borough

Ealing New Primary Care Offer Business Case
July 2017 43
following the PMS review. The value of the indicator for achievement has been used as a
benchmark for these services.
Using this methodology, the services have been priced as set out in table 13.
Table 12: Pricing of the services within Ealing standard (full year)
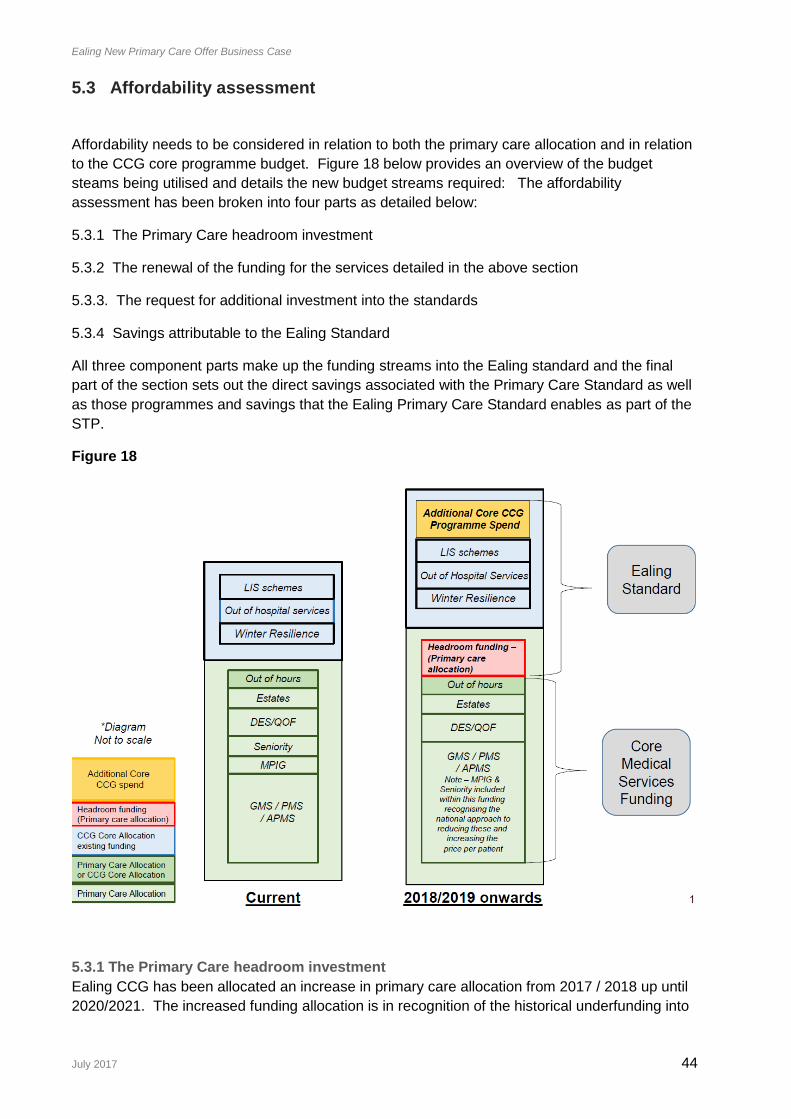
Ealing New Primary Care Offer Business Case
July 2017 44
5.3 Affordability assessment
Affordability needs to be considered in relation to both the primary care allocation and in relation
to the CCG core programme budget. Figure 18 below provides an overview of the budget
steams being utilised and details the new budget streams required: The affordability
assessment has been broken into four parts as detailed below:
5.3.1 The Primary Care headroom investment
5.3.2 The renewal of the funding for the services detailed in the above section
5.3.3. The request for additional investment into the standards
5.3.4 Savings attributable to the Ealing Standard
All three component parts make up the funding streams into the Ealing standard and the final
part of the section sets out the direct savings associated with the Primary Care Standard as well
as those programmes and savings that the Ealing Primary Care Standard enables as part of the
STP.
Figure 18
5.3.1 The Primary Care headroom investment
Ealing CCG has been allocated an increase in primary care allocation from 2017 / 2018 up until
2020/2021. The increased funding allocation is in recognition of the historical underfunding into

Ealing New Primary Care Offer Business Case
July 2017 45
primary care within Ealing based on the national funding steams. Figure 19 below shows the
increases to funding that have been published by NHS England for Ealing CCG:
Figure 19
Table 14 below provides the actual funding increases over the four years:
Year of increase in allocation Sum
2017/2018 £4,825,000
2018/2019 £2,244,000
2019/2020 £1,991,000
2020/2021 £2,706,000
Since becoming delegated on the 1st April 2017 the CCG has been going through the process of
determining the primary care budget that is needed for the 76 practice from within the overall
allocation. The CCG has had to work through a number of risks in order to determine a draft
budget and determine the headroom that is available to invest into practices to address the
historical underfunding to meet the needs of the Ealing population. This draft budget has been
recommended for approval by both the Primary Care Committee and the Finance &
Performance committee subject to the work of district valuer to better understand the risks on
premises.
The summary of the draft primary care budget is shown below in Table 15:
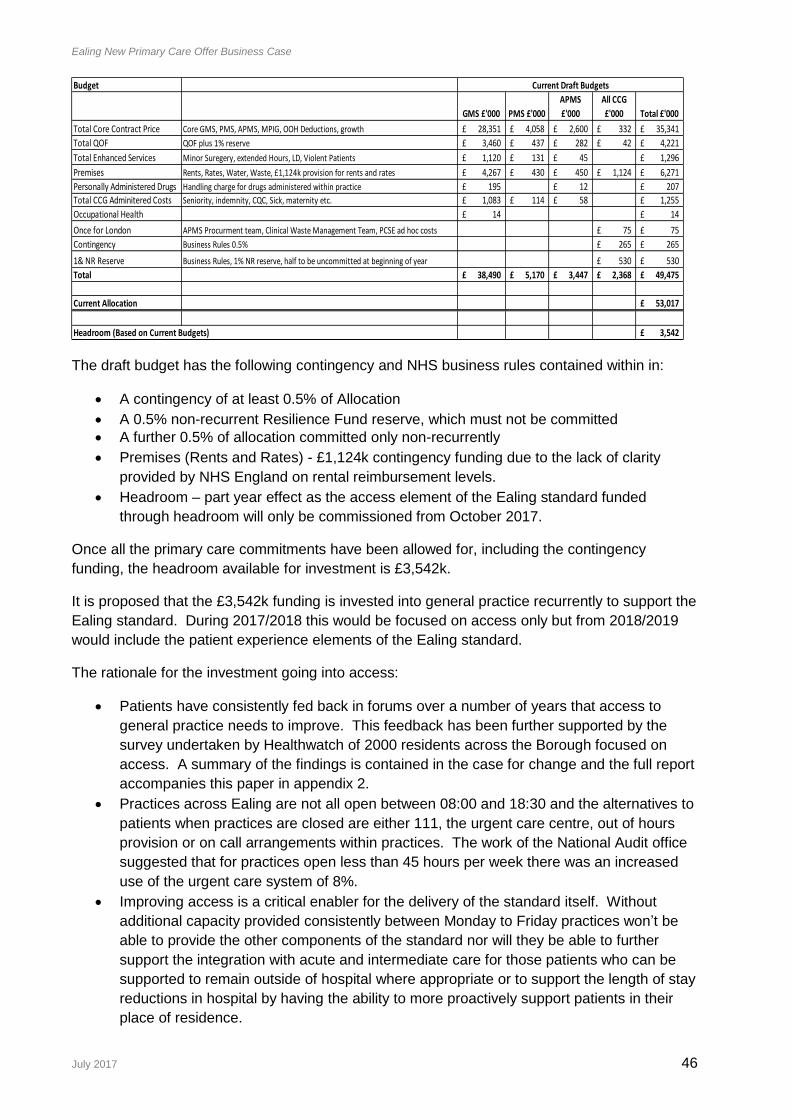
Ealing New Primary Care Offer Business Case
July 2017 46
The draft budget has the following contingency and NHS business rules contained within in:
A contingency of at least 0.5% of Allocation
A 0.5% non-recurrent Resilience Fund reserve, which must not be committed
A further 0.5% of allocation committed only non-recurrently
Premises (Rents and Rates) - £1,124k contingency funding due to the lack of clarity
provided by NHS England on rental reimbursement levels.
Headroom – part year effect as the access element of the Ealing standard funded
through headroom will only be commissioned from October 2017.
Once all the primary care commitments have been allowed for, including the contingency
funding, the headroom available for investment is £3,542k.
It is proposed that the £3,542k funding is invested into general practice recurrently to support the
Ealing standard. During 2017/2018 this would be focused on access only but from 2018/2019
would include the patient experience elements of the Ealing standard.
The rationale for the investment going into access:
Patients have consistently fed back in forums over a number of years that access to
general practice needs to improve. This feedback has been further supported by the
survey undertaken by Healthwatch of 2000 residents across the Borough focused on
access. A summary of the findings is contained in the case for change and the full report
accompanies this paper in appendix 2.
Practices across Ealing are not all open between 08:00 and 18:30 and the alternatives to
patients when practices are closed are either 111, the urgent care centre, out of hours
provision or on call arrangements within practices. The work of the National Audit office
suggested that for practices open less than 45 hours per week there was an increased
use of the urgent care system of 8%.
Improving access is a critical enabler for the delivery of the standard itself. Without
additional capacity provided consistently between Monday to Friday practices won’t be
able to provide the other components of the standard nor will they be able to further
support the integration with acute and intermediate care for those patients who can be
supported to remain outside of hospital where appropriate or to support the length of stay
reductions in hospital by having the ability to more proactively support patients in their
place of residence.
Budget
GMS £'000 PMS £'000
APMS
£'000
All CCG
£'000 Total £'000
Total Core Contract Price Core GMS, PMS, APMS, MPIG, OOH Deductions, growth 28,351£ 4,058£ 2,600£ 332£ 35,341£
Total QOF QOF plus 1% reserve 3,460£ 437£ 282£ 42£ 4,221£
Total Enhanced Services Minor Suregery, extended Hours, LD, Violent Patients 1,120£ 131£ 45£ 1,296£
Premises Rents, Rates, Water, Waste, £1,124k provision for rents and rates 4,267£ 430£ 450£ 1,124£ 6,271£
Personally Administered Drugs Handling charge for drugs administered within practice 195£ 12£ 207£
Total CCG Adminitered Costs Seniority, indemnity, CQC, Sick, maternity etc. 1,083£ 114£ 58£ 1,255£
Occupational Health 14£ 14£
Once for London APMS Procurment team, Clinical Waste Management Team, PCSE ad hoc costs 75£ 75£
Contingency Business Rules 0.5% 265£ 265£
1& NR Reserve Business Rules, 1% NR reserve, half to be uncommitted at beginning of year 530£ 530£
Total 38,490£ 5,170£ 3,447£ 2,368£ 49,475£
Current Allocation 53,017£
Headroom (Based on Current Budgets) 3,542£
Current Draft Budgets

Ealing New Primary Care Offer Business Case
July 2017 47
The historical underfunding in practices in Ealing has made it more difficult to invest in
the staff required to provide access and therefore targeting the funding in this way
enables practices to open between 08:00 and 18:30 and provide further services
throughout this period.
Investing in access has provided the CCG with the opportunity to specify requirements
within the standard that support timely home visiting, different modes of access,
increased opening hours, a minimum of 100 appointments per week per 1000 patients
(105/1000 per week in winter months) requirement ,and the requirement to undertake
demand and capacity audits with an improvement trajectory agreed.
That value for money is being achieved through this approach as the CCG is using the
Out of Hospital services costing model to determine the price which has been agreed as
the approach to take by the Investment Committee.
Figure 20 below shows how the headroom will be invested in from 2017 onwards.
As indicated in table 15 above the allocation increases annually over the next three years. The
CCG will review the budget requirements annually and proposes the following in terms of
balancing further investment into the Ealing with meeting the funding agreements reached
nationally that need to be paid for through the primary care allocation at a CCG level as well as
managing the know risks such as premises:
The funding priorities from the allocation over subsequent years are:
Growth in population
• Increase in national contract negotiations
• Rent increases

Ealing New Primary Care Offer Business Case
July 2017 48
• Rates increases
• Other unknown primary care risks which materialise and require a call on funding
• Increase in access provision (appointments / 000 / week)
• Incentives for achievement against Goals Framework
• More Standards
In summary the business case is setting out the case that the headroom in the primary care
budget should be invested into general practice in Ealing to address the historical underfunding
that is set out in figure 19. Without this investment it becomes very difficult to practices to
sustain current delivery and improve capacity and the breadth of service provision at the levels
that have been articulated within the Ealing Standard.
The CCG will focus this additional investment of £3.5m to support the access specification in
2017/2018 with the addition in 2018/2019 of the patient experience, screening & prevention and
patient experience.
5.3.2 The renewal of the funding for the services detailed in the above sections
In addition to the primary care allocation Ealing CCG received a core programme allocation of
£492m in 2017/18 and of this Ealing CCG spends approximately 3% on services from general
practice. The CCG committed £5.4m into Out of Hospital services, £0.4m to primary care winter
resilience, £1.9m to local incentive schemes and £0.1m to Dementia and £0.2m Paediatric
Phlebotomy in 2017/2018. This section of the business case sets out the case that this funding
should be renewed and committed to the Ealing Primary Care standard between 2018 and 2021.
Figure 21 below provides a view of the elements of funding that is being requested; the
additional shown in yellow and the renewal request shown in blue:

Ealing New Primary Care Offer Business Case
July 2017 49
The list of services that falls into the category of renewal is:
Ambulatory blood pressure monitoring (ABPM)
Anticoagulation
Care planning
Chronic Obstructive Pulmonary Disease (COPD)
Diabetes
Electrocardiogram (ECG)
Homeless care
Management of common mental health issues
Mental health – transfer of care
Near patient testing
Phlebotomy
Ring pessary
Wound care
Paediatric Phlebotomy
LIS
Dementia
Respiratory (diagnostic spirometry)
End of life care
Demand Management
Drug Monitoring
Carers
Learning Disability
Medicine Optimisation and safety
Winter Resilience. The total of the request to renew/ fund these services into the Ealing standard from April 18 to March 2021 is at an annual cost of core funding of £7.2m. As indicated in previous sections the services have been costed using the out of hospital services approach. The Ealing Standard is intended to be commissioned as a single wrap around contract to support general practice meet the needs of the Ealing population as identified within the JSNA. This also supports the move that the CCG wishes to make in terms of paying on a capitated model which the standard sets out to do for the majority of the services. For two of the services the payment will be linked to prevalence and for the remaining services it has not been possible to move them from an activity based payment. Despite the different payment mechanisms the standard is being offered as a single wrap around over a 3.5 year contract term to enable general practice to consider the workforce it needs to deliver the services and then make the appropriate investments. Should the renewal of these services not be agreed it would risk the approach being taken and slow down the transformation journey that the CCG recognises is critical for both general practice but also for the wider healthcare system. An assessment has been undertaken of what the financial impact would be of withdrawing the
funding and therefore service provision from general practice. The service provision is likely to
fall back into the acute sector and where this is quantifiable through the availability of an acute
tariff this has been calculated below as shown in table 16:
Cost of OOH activity Cost of OOH activity if
delivered within a Acute
setting (based on 16/17
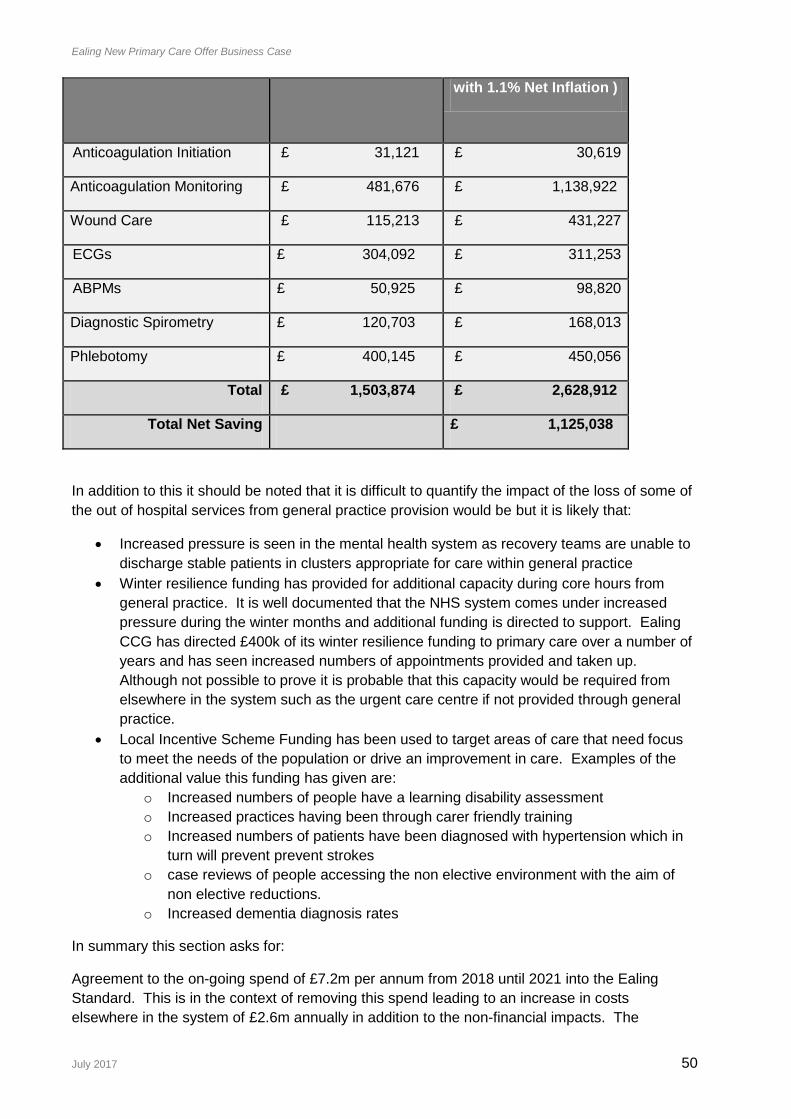
Ealing New Primary Care Offer Business Case
July 2017 50
with 1.1% Net Inflation )
Anticoagulation Initiation £ 31,121 £ 30,619
Anticoagulation Monitoring £ 481,676 £ 1,138,922
Wound Care £ 115,213 £ 431,227
ECGs £ 304,092 £ 311,253
ABPMs £ 50,925 £ 98,820
Diagnostic Spirometry £ 120,703 £ 168,013
Phlebotomy £ 400,145 £ 450,056
Total £ 1,503,874 £ 2,628,912
Total Net Saving £ 1,125,038
In addition to this it should be noted that it is difficult to quantify the impact of the loss of some of
the out of hospital services from general practice provision would be but it is likely that:
Increased pressure is seen in the mental health system as recovery teams are unable to
discharge stable patients in clusters appropriate for care within general practice
Winter resilience funding has provided for additional capacity during core hours from
general practice. It is well documented that the NHS system comes under increased
pressure during the winter months and additional funding is directed to support. Ealing
CCG has directed £400k of its winter resilience funding to primary care over a number of
years and has seen increased numbers of appointments provided and taken up.
Although not possible to prove it is probable that this capacity would be required from
elsewhere in the system such as the urgent care centre if not provided through general
practice.
Local Incentive Scheme Funding has been used to target areas of care that need focus
to meet the needs of the population or drive an improvement in care. Examples of the
additional value this funding has given are:
o Increased numbers of people have a learning disability assessment
o Increased practices having been through carer friendly training
o Increased numbers of patients have been diagnosed with hypertension which in
turn will prevent prevent strokes
o case reviews of people accessing the non elective environment with the aim of
non elective reductions.
o Increased dementia diagnosis rates
In summary this section asks for:
Agreement to the on-going spend of £7.2m per annum from 2018 until 2021 into the Ealing
Standard. This is in the context of removing this spend leading to an increase in costs
elsewhere in the system of £2.6m annually in addition to the non-financial impacts. The
Ealing New Primary Care Offer Business Case
July 2017 51
agreement to the renewal of funding also supports the CCGs intention to commission a single
wrap around contract over multiple years enabling practices to consider the workforce
requirements and transformation required to improve resilience.
5.3.3 The request for additional investment into the standards
In developing the Ealing standard the review work highlighted a number of areas where further
commissioning is required to meet the needs of the Ealing population as identified within the
JSNA as well as in some areas set appropriate standards of care for general practice to meet.
Within this there have been some standards developed which are entirely new and some Out of
Hospital services that have been reviewed with additional requirements added to which have
then driven an additional cost. This additional cost needs to be considered in the context of then
need to invest in general practice to improve resilience and to support the transformation
journey. The agreement to make this funding available from the core programme budget will
support the intention to commission a single wrap around contract over multiple years enabling
practices to consider the workforce requirements and make necessary investments to support
the delivery of the standard across Ealing.
The list of these services are:
Additional Respiratory Components
Musculoskeletal Services (MSK)
End of Life
Cancer Screening
Self Care and Patient Activation Measures
Prevention
Learning Disability
Carers
Access
Prevention
Medicines Safety and Optimisation
Ankle-Brachial Pressure Index (ABPI)
As detailed in the earlier part of this section these costs have been derived by using the out of
hospital costing model or using LIS schemes as the benchmark. The costs are set out in detail
in table 13 earlier in this section but the total request for additional funding is £923k.
5.3.4 Savings attributable to the Ealing Standard
Work has been undertaken to determine what financial impact there would be on secondary care
as a consequence of investing in the Ealing Standard.
Within the aim of the Ealing Standard is to set a range of standards and fund a level of care that
enables general practice to move to a more proactive and planned model of care, Clinical leads
modelled the impact that the standards would have on both non elective and planned care
systems. Activity and financial changes are attributed to specific standards where it was
possible to make clear modelling assumptions. As established earlier in the business case, this
methodology supports the STP in moving towards a more proactive and planned care system
that includes preventative services which help reduce unwarranted variation and decreased
unplanned admissions into secondary care.

Ealing New Primary Care Offer Business Case
July 2017 52
Activity assumptions have been shown against the IMBC target which was agreed by the
Governing Body to support the Strategic Outline Case for the capital that supports the delivery of
SaHF. This profile is important as it sets out the expected shape change in the NWL healthcare
system and therefore it is important that Ealing’s planning tracks back to these underlining
business assumptions. The activity profiling has therefore also utilised activity growth
assumptions detailed within the IMBC planning.
Table 17 below shows the estimated Non Elective activity reductions derived from modelling the
Ealing Standards:
Financial Period
QIPP Drivers 2018/19 2019/20 2020/21
ImBC QIPP Target 3021 3594 1801
Diabetes Primary Care QIPP 198 186 177
Asthma Primary Care QIPP 336 315 299
COPD Primary Care QIPP 164 154 146
EOL Primary Care QIPP 197 185 175
Total Primary Care QIPP 895 840 797
QIPP Other 2126 2754 1004
Total QIPP 3021 3594 1801
NEL Admission Rate per 1000 82.77 77.76 77.01
The assumptions that underpin the activity change are set out below in table 18:
The activity profile converted into cost is shown in table 19 below:
QIPP Drivers Financial Period
2018/19 2019/20 2020/21
Diabetes Primary Care QIPP £ 344,759 £ 323,524 £ 309,738
Asthma Primary Care QIPP £ 369,756 £ 346,981 £ 329,233
COPD Primary Care QIPP £ 381,572 £ 358,069 £ 339,754
EOL Primary Care QIPP £ 675,185 £ 633,597 £ 601,188
Total Primary Care QIPP £ 1,771,274 £ 1,662,172 £ 1,579,915
Note: All savings are based on unit costs for the QIPP drivers during 2016/17 adjusted by the
annual inflators/deflators in the Ealing CCG Financial Plan
In summary the total NEL admissions that could be saved over the four years alongside the cost
is shown below in table 20:
DiabetesAssumed improved management of patients will prevent emergency admissions for diabetes as a primary diagnosis and that this will recur as patients
might be frequent users of emergency services and new patients are diagnosed.
Asthma There is evidence that increasing the number of patients on preventative asthma medicine can lead to a 75% reduction in secondary care events.
Assumption that the opportunity will recur as patients would be likely to be admitted annually otherwise and new cases will be diagnosed.
COPD Emergency readmissions within 90 days are avoidable if patients referred to pulmonary rehabilitation and prescribed rescue packs. Assumption that
exacerbations requiring emergency admission are inevitable so the opportunity is recurrent.
EOL
Assumption that 1% of the registered population is at an end of life stage. Deaths in hospital where the reason for admission is cancers and tumours),
problems of circulation or problems of the respiratory system. Recurrent due to the assumption about prevalence. There is a probably a further
opportunity based on all emergency admissions during a reference period prior to death.

Ealing New Primary Care Offer Business Case
July 2017 53
Financial Period
2018/2019 2019/2020 2020/2021
NEL Reduction 895 840 797
Cost Saving £1,771,274 £1,662,172 £1,579,916
In addition to the non-elective savings that are anticipated; the standard will also support
planned care savings.
The planned care savings are set out in table 21 below with the underpinning assumptions set
out underneath this in table 22. It should be noted that the activity changes are only profiled for
two of the years that it is intended to commission the standard as the opportunity available will
be saved in that period.
QIPP Drivers
Financial Period
2018/19 2019/20 2020/21
ECGs 1,613 538 -
MSK 785 262 -
Anticoagulation 3,908 1,303 -
Total Primary Care Planned Care QIPP 6306 2103 0
The assumptions that underpin this change profile are:
Table 22:
The activity change shown in cost terms is detailed in the table 23 below:
QIPP Drivers
Financial Period
2018/19 2019/20 2020/21
ECGs £ 318,243 £ 106,187 -
MSK £ 92,469 £ 30,854 -
Planned Care QIPP
ECGs Assumed shift of 100% of ECGs performed at the first out patient appointment.
MSK Avoidable first out patient appointments due to inappropriate referrals for PPwT and estimated follow up attendances.
Anticoagulation Assumes that initiation and maintenance of anticoagulation should be delivered by Out Of Hospital Services.

Ealing New Primary Care Offer Business Case
July 2017 54
Anticoagulation £ 137,036 £ 45,724 -
Total Primary Care Planned Care QIPP £ 547,748 £ 182,765 0
The total gross savings that can be directly attributed to the Ealing standard are shown below in
table 24:
Financial Period
2018/2019 2019/2020 2020/2021
NEL Gross Cost Saving £1,771,274 £1,662,172 £1,579,916
Planned Care Gross Cost Saving £547,748 £182,765 0
Total Gross saving £2,319,022 £1,844,937 £1,579,916
The activity and cost savings shown in the tables above are the total opportunities identified as
available. Evaluation of mobilisations of other large programmes that have been undertaken
demonstrate that it is unlikely that the maximum savings will be derived in year one. Three
options have been determined based on learning from previous mobilisations and are set out
below in table 25:
The recommended case is the conservative case delivering by 2021 a total incremental gross
saving of £4,123,130.
It should also be noted that this means that we are not
Overall Summary
The section sets out the case that:
1. Investment should be made from the headroom within the primary care allocation of
£2.8m in 2017/2018 and budgeted for £3.5m in 2018/2019 to invest into access,
screening & prevention services and patient experience standards. The funding has
been made available nationally and reflects the historic distance from target levels of
funding for practices within Ealing CCG.
2. That agreement to the renewal/ongoing spend for the out of hospital services, LIS and
winter resilience is made. The annual cost of this is £7.2m. This spend is already
committed within CCG core programme budgets and if the funding is ceased will see an
Gross Savings in Finanical Years
2018/19 2019/20 2020/21 TOTAL
A. Best Case 2,319,022 1,844,938 1,579,916 5,743,875
Service delivery as per initial modelling
assumptions
B. Mid Range 1,855,218 1,844,938 1,579,916 5,280,071
Service delivery ramp up: Year 1 = 80%
and Year 2 & 3 = 100%
C.Conservative Case 1,159,511 1,383,703 1,579,916 4,123,130
Service delivery ramp up: Year 1 = 50%,
Year 2 = 75%, Year 3 = 100%

Ealing New Primary Care Offer Business Case
July 2017 55
estimated cost increase in the acute system of £2.6m in addition to a number of non-
quantifiable impacts.
3. That the additional investment of £923k from the core programme spend is agreed on the
basis of the savings that can be attributed to the standard as a whole and summarised in
table 26 below:
Financial Period
2018/2019 2019/2020 2020/2021
Total Core Additional Funding £923K £923K plus inflation,
growth (demographic
and non demographic)
£923K plus inflation,
growth (demographic
and non demographic)
Conservative benefit realisation £1,159,511 £1,383,703 £1,579,916
Net saving £235,511 £459,703 £655,916
It should be noted that all three funding streams are required to enable the commissioning the
Ealing Standard and without any one of the funding streams it would prevent the CCG from
commissioning a single wrap around contract across the 3.5 year contract term that is proposed.
5.4 Enabling STP Delivery
As indicated in earlier sections the Ealing Standard is a critical driver in enabling the delivery of
the NWL STP for Ealing. In addition to the case that has been set out work has been
undertaken to demonstrate where the Ealing Standard will be supporting the five delivery areas
all of which have been determined to have financial benefits to the NWL system and is set out in
figure 21 below:

Ealing New Primary Care Offer Business Case
July 2017 56
5.5 Impact on PMS practices
The increase in allocation provides the opportunity to approach the sustainability of primary care
in a different way.
In Ealing there are 7 PMS practices and the amount of premium released in Year is minimal as
the overall value of PMS premium in Ealing is approximately £650k. Spread across all practices
in Ealing, the premium would not add much value and therefore the primary care standard would
incorporate the PMS review.
One of the principles for the PMS review is to ensure any premium released from PMS practices
is released into general practice and commissioned for 1st October 2017 in line with our primary
care commissioning approach to the increased allocation.
Ealing is committed to commissioning primary care in a way that ensures any funding:
1. Released from the PMS review is reinvested into General Practice
2. Is equitably invested into General Practice
3. Supporting PMS practices with transition funding to ensure there is no destabilisation of any
practice
The access targets have been developed using information and benchmarking from areas that
have commissioned such targets such as Bolton and Salford. Feedback has also been collated
from the Patient and Public Engagement work that has been conducted over the last year,
where access to GP's has been a raised concern and supported by the Survey carried out by
Healthwatch.

Ealing New Primary Care Offer Business Case
July 2017 57
In order to ensure we meet the timeframes for the PMS Review our Governing Body has
previously agreed to include the review of PMS practices with the overall Primary Care
Standard.
There are only 7 practices with a PMS contract in Ealing and therefore the time required to meet
and negotiate with the practices will be faster than in some of the other CCGs, but will also be
staggered and support the Central teams to stagger their work.
Offer letters will be sent out soon after the GB and in the letters, the PMS practices will be
offered a visit to discuss their practices position and options week commencing 24th July 2017.
This will not be the first time the practice would have seen their information as the letter which
breakdowns how the PMS will be calculated will was sent in April using the 16/17 contract
values. In addition all practices have had the opportunity to be involved in the development of
the Commissioning Intentions during May and June 2017. The final offer will be sent using
17/18 figures with the full impact of the Commissioning Intentions for their practice.
The approach to transition has been considered at the Commissioning Committee on the 10th
May. Ealing has already been clear that any funds released are reinvested back into general
practice, equitably, while supporting PMS practices transition aware from PMS premium. In
2015 and 2016, during the initial approach to the PMS review before the ‘pause’, a mapping
exercise was conducted to understand what the impact of the review would be on the individual
practices. At this time, there was no major change expected as a result of the review, apart from
one practice, where they had employed staff that spoke Tamil.
However, during this review, it is our intention to ask each practice again, how they would
transition, in order to understand what the impact would on services to patients. The Impact
assessment would be undertaken in 2 steps.
1. Financial impact on the practice and staffing implications. These will be explored in
detail at the individual practice meeting. Ealing CCG has commissioned NELCSU to
support the financial modelling for each practice to understand the impact on the
practice while they transition to the new offer. This will be used to talk the practices
through the implications as part of the contract negotiation.
2. Equality Impact on services to patients. Once it is clear what the financial impact and
therefore what the potential staffing impact would be on the practice, working closely
with the practice the Equality Impact Assessment will be refreshed.
Transition funding aims to support PMS practices to remain stable as they move to new income
and service arrangements as part of the PMS Review. It is calculated by considering the
difference between the current 16/17 PMS contract values and the GSE (global sum equivalent),
as well as the income offered through newly commissioning services.
Potential income loss (e.g. the difference between current income and GSE + Commissioning
intentions) for year 1 determines each practice’s ‘transition pathway’, allowing transitional offers
to be calculated for the full PMS review period. There are 3 transition pathways, with each
offering different lengths of funding based on magnitude of income lost.
Final Practice offers will be based on updated 17/18 figures when available, with initial ‘baseline
letters’ using 16/17 figures as an interim measure, however this will not alter the transition
pathway of any Practices within the CCG.

Ealing New Primary Care Offer Business Case
July 2017 58
This recommended transition methodology, calculating transition by taking account of income
from newly commissioned services, was recommended for all CCGs at the 2nd February 2017
NWL PMS Review Steering Group, which has an advisory function to each CCG’s Primary Care
Commissioning Committee. The impact on the 7 PMS practices is considered commercially
sensitive and will therefore be considered in private Primary Care Commissioning Committee if
the Governing Body agrees this Business Case. This will be followed by detailed conversations
with individual practices.

Ealing New Primary Care Offer Business Case
July 2017 59
6 Management case
6.1 Governance
As the development of this Ealing Primary Care Standard is clinically led, it is essential that all
actual or perceived conflicts of interest are managed proactively.
Member Engagement
To ensure we get the right answer for our population, the clinical standards have been initially
developed by the Clinical leads and then tested through a co-production phase with the CCGs
clinical membership.
To manage any perceived conflicts, no clinicians were involved in developing the actual financial
case or costing, which was led by officers of the CCG.
Council of Members Co-production workshops 10th May 2017
24th May 2017
14th June 2017
5th July 2017
Member Drop-in sessions 31st May 2017
7th June 2017
LMC at Primary Care Steering Groups
LMC (Local and Londonwide) 18th July 2017
LMC (Local and Londonwide) 25th July 2017
Primary Care Steering Group
The primary care steering group was established to oversee the development of the Standards.
The Terms of Reference (TOR) for the Primary Care Steering Group can be found in Appendix
8. This Steering group consisted of Lay Partners, LMC (Local and Londonwide), CCG Clinical
Leads, Managing Director, Managerial leads within CCG, Communications team and
Healthwatch in attendance once although invited on going.
Independent Review Panel
In addition, each new standard which was developed was tested at an Independent Review
Panel, made up of a Lay Member, a non-conflicted GP from outside of the borough, 2 members
from the NHSE team based working across North West London and the Acting Director of
Quality for CWHHE. This was held on the 5th July 2017. The independent review panel was put
in place to test the recommendation that general practice was the most capable provider of the
standard. This aligns to the procurement process that the Governing Body currently has in place
and also mirrors the process followed for the commissioning of the initial set of out of hospital
services.

Ealing New Primary Care Offer Business Case
July 2017 60
Sign off process
As the potential for conflicts (both actual and perceived) are great with this programme as CCGs
are membership organisations and the contract would be let to members, the following sign off
process for the offer has been agreed.
Extraordinary F&P – All conflicted members will abstain 12th July 2017
Primary Care Commissioning Committee (Public) - All conflicted members will abstain 19th July 2017
Investment Committee 20th July 2017
Governing Body in Public – All Conflicted members will abstain 26th July 2017
Due to the tight timelines the following process has been agreed with the Local LMC:
Initial comments 14th July 2017
Review meeting 1 18th July 2017
Review meeting 2 25th July 2017
It was agreed that any issues still outstanding after review meeting 2 will be shared with the Governing
Body on the 26th July.
6.2 Mobilisation plan
Figure 22 below provides an overview of the programme of work from commencement through
to full mobilisation on April 2018.
The mobilisation will be overseen by a steering group made up of CCG clinical leads and managers with responsibility for primary care. This group reports into and includes members from the Primary Care Commissioning Committee, F&P and that Healthwatch are included as members.
Figure 22 Summary of activities
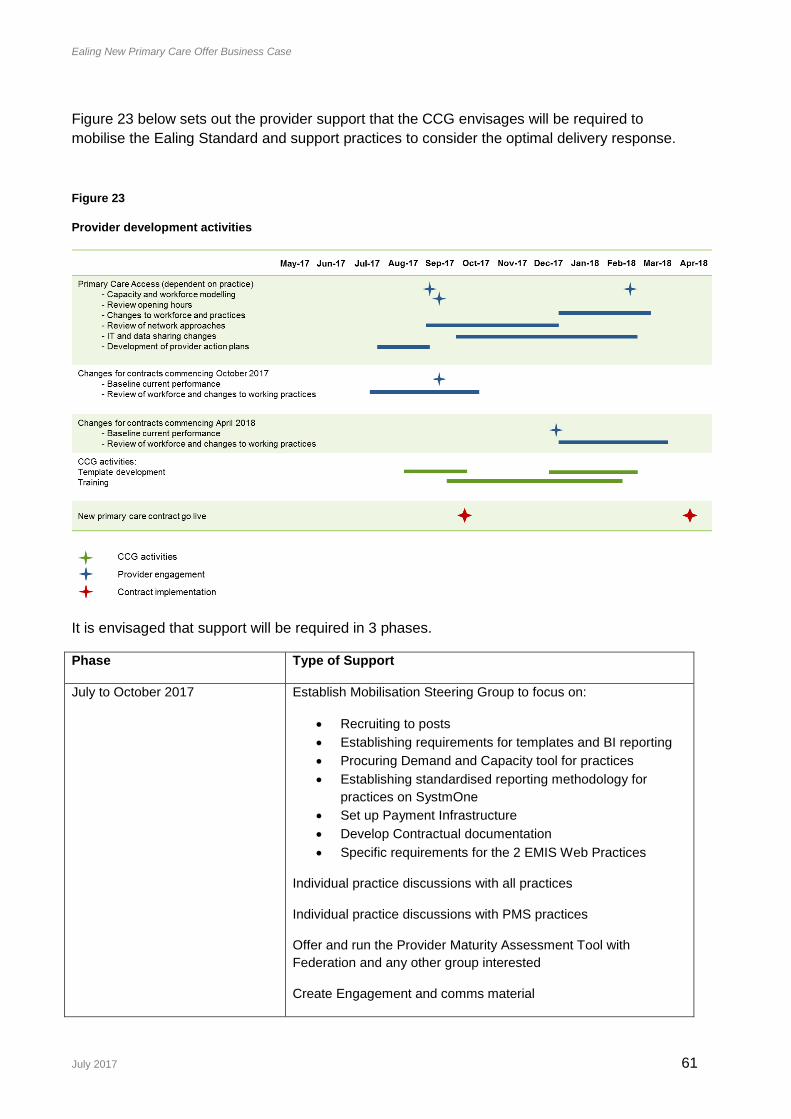
Ealing New Primary Care Offer Business Case
July 2017 61
Figure 23 below sets out the provider support that the CCG envisages will be required to
mobilise the Ealing Standard and support practices to consider the optimal delivery response.
Figure 23
Provider development activities
It is envisaged that support will be required in 3 phases.
Phase Type of Support
July to October 2017 Establish Mobilisation Steering Group to focus on:
Recruiting to posts
Establishing requirements for templates and BI reporting
Procuring Demand and Capacity tool for practices
Establishing standardised reporting methodology for
practices on SystmOne
Set up Payment Infrastructure
Develop Contractual documentation
Specific requirements for the 2 EMIS Web Practices
Individual practice discussions with all practices
Individual practice discussions with PMS practices
Offer and run the Provider Maturity Assessment Tool with
Federation and any other group interested
Create Engagement and comms material

Ealing New Primary Care Offer Business Case
July 2017 62
Issue contracts
October 2017- March 2018 Support practices to run the Demand and Capacity tools
Support practices to standardise the recording of appointments on
SystmOne
Develop dashboards with the WSIC team to support the delivery of
the contract
Establish thresholds for services commencing in April, where they
have not already been set e.g. Diabetes and Access
April 2018 onwards Mobilise full contract with dashboards
Ensure population coverage
Provide regular data to practices
Monitor KPIs and provide practices with regular data on
performance against KPIs
Quarterly activity based services reconciliation
Close of OOH services contract and reconciliation of 17/18 data
Close of LIS and reconciliation of 17/18 data
6.3 Provider development
In order to deliver the Ealing Standard to the timeline set out in 6.2 above, the CCG
acknowledges that Providers will need targeted support to develop their capacity and capabilities
individually but in particular, collectively at network level.
It is proposed that following the agreement of this business case, and prior to the
commencement of services, the CCG and providers work together to understand the
development support that might be needed. It is currently envisaged that providers may need
support in the areas:
Information technology to facilitate new care models and ways of working
Clinical skills across the primary care workforce
Business operations and administration at scale
Business intelligence and analytics (including population health analysis)
Demand and capacity management
This support will be underpinned by allowing providers the capacity to implement changes to the
service to ensure that they are set up for success.

Ealing New Primary Care Offer Business Case
July 2017 63
Practice level development
The CCG has already been providing support to practices as described under the GPFV. The
support can be summarised under the 10 High Impact Actions in table 25 below:
10 High
Impact
Actions
Examples of types of
activities
Examples of
Outputs/Outcom
es
Comments / work already in
progress
1. Active Signposting
Online portal;
Reception based
navigators
Release of
clinical capacity
within practice
In collaboration with Ealing
CEPN we have already
commissioned and committed
funding for bespoke training to be
delivered to all practices over the
next 2 years. The aim of this
training is to improve GP
receptionists’ knowledge of the
range of in-practice, social and
voluntary care options available
to patients and helping them to
develop the people/telephone
skills to find the most appropriate
care options for each patient.
We are also investing in Numed
Screens in all practices across
Ealing which provide tailored
support and advice to the
practice population by
signposting patients to the most
appropriate services as well as
offering self-care advice.
2. New consultation types (telephone, on-line, video)
Telephone consultations; E-consultations; Text messages/phone notifications; Group[ consultations
Improvement in appointments per 1000 Improved patient survey outcomes
The ETTF Digital programmes are being implemented and will support practices directly to progress various new consultation types.
3. Reduce DNAs Easy cancellation; reminders; patient recording; read-back; report attendances; recue ‘just in case’
Improved patient survey outcomes
SMS Texting is available through the practice systems.
4. Develop the Team (developing the practice team to support all members of the team to operate at the top of their license)
Advanced nurse practitioner; physician associates; Pharmacists; medical assistant; paramedics; Therapists
Increase in clinical capacity Improved patient survey outcomes
Ealing CEPN has been running a range of training for practice staff over the last 2 years. This training will continue to support individuals (clinical and non-clinical) to continually develop their skills with a range of training programmes offered.
5. Productive Matching capacity and Increase in We are building on our practice
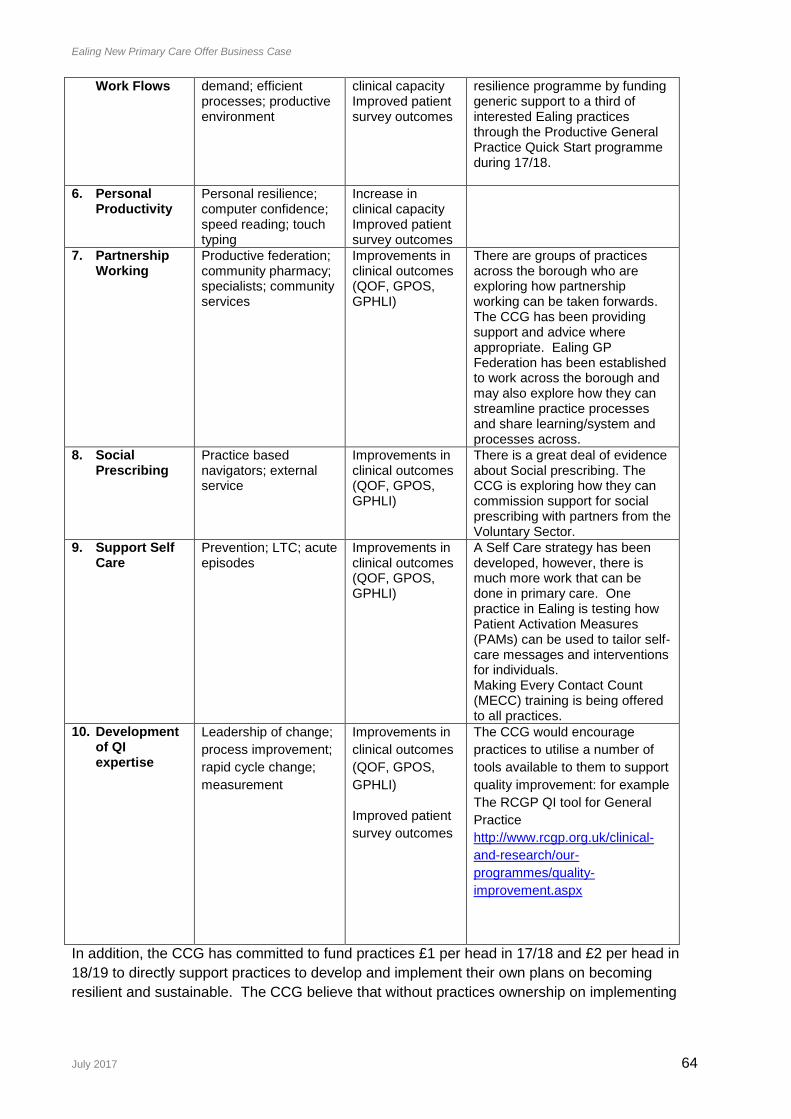
Ealing New Primary Care Offer Business Case
July 2017 64
Work Flows
demand; efficient processes; productive environment
clinical capacity Improved patient survey outcomes
resilience programme by funding generic support to a third of interested Ealing practices through the Productive General Practice Quick Start programme during 17/18.
6. Personal Productivity
Personal resilience; computer confidence; speed reading; touch typing
Increase in clinical capacity Improved patient survey outcomes
7. Partnership Working
Productive federation; community pharmacy; specialists; community services
Improvements in clinical outcomes (QOF, GPOS, GPHLI)
There are groups of practices across the borough who are exploring how partnership working can be taken forwards. The CCG has been providing support and advice where appropriate. Ealing GP Federation has been established to work across the borough and may also explore how they can streamline practice processes and share learning/system and processes across.
8. Social Prescribing
Practice based navigators; external service
Improvements in clinical outcomes (QOF, GPOS, GPHLI)
There is a great deal of evidence about Social prescribing. The CCG is exploring how they can commission support for social prescribing with partners from the Voluntary Sector.
9. Support Self Care
Prevention; LTC; acute episodes
Improvements in clinical outcomes (QOF, GPOS, GPHLI)
A Self Care strategy has been developed, however, there is much more work that can be done in primary care. One practice in Ealing is testing how Patient Activation Measures (PAMs) can be used to tailor self-care messages and interventions for individuals. Making Every Contact Count (MECC) training is being offered to all practices.
10. Development of QI expertise
Leadership of change;
process improvement;
rapid cycle change;
measurement
Improvements in
clinical outcomes
(QOF, GPOS,
GPHLI)
Improved patient
survey outcomes
The CCG would encourage
practices to utilise a number of
tools available to them to support
quality improvement: for example
The RCGP QI tool for General
Practice
http://www.rcgp.org.uk/clinical-
and-research/our-
programmes/quality-
improvement.aspx
In addition, the CCG has committed to fund practices £1 per head in 17/18 and £2 per head in
18/19 to directly support practices to develop and implement their own plans on becoming
resilient and sustainable. The CCG believe that without practices ownership on implementing

Ealing New Primary Care Offer Business Case
July 2017 65
changes on the ground, any transformation support the CCG provides will not have the desired
impact, hence the investment.
Providers at Scale development
Through the development of the OOH services contract, Ealing GP Ltd (Federation of all
practices in Ealing) emerged. It is unclear what the ambition of the Federation is as of April
2018 when the OOH services come to an end. The Federation may envisage itself as a
management function on behalf of the practices, but may have wider ambitions in delivering
services itself as an entity in itself practices which practices could sub-contract to as allowed in
the contract. Ultimately the role of the Federation will need to be agreed between itself and its
shareholders; however the CCG recognises there it has a role in enabling the dialogue and
facilitating it.
In order to understand the ambition and ability of the Federation to take this role in Ealing, the
CCG will facilitate a Maturity Assessment with the Federation in a number of stages. This
approach requires further discussion with the Federation Board and there is an initial discussion
set up to do so and therefore it may be that this process is iterated through discussions.
Stage 1: Maturity Assessment of Federation carried out with independent Facilitation team
during September
Stage2: Practices/ groups of practces invited to participate in their own maturity assessment if
interested in a workshop setting during September
Stage 3: Workshop with practices and Federation presented with results of the Maturity
Assessment by the Facilitation team followed by Network based discussions on options for
providers at scale during October
6.4 Resourcing Requirements in the CCG For the mobilisation phase to be effective, significant resource will be required at the CCG to
support practices totalling £510,000 in the context of investing just under £12m through the
standard. The following resources have been identified as being required:
£50k for the Demand and Capacity Analysis Tool for practices to use
£12k to run the series of Provider Development workshops
£279k for 7 additional mobilisation team members (Band 7) to directly support each
Network to mobilise the contract for a period of 12 months between October 2017 –
September 2018
£75k for 1 Band 8d to oversee the mobilisation of the contract for a period of 9 months
between October 2017- June 2018
£31k for 1 Band 8a for System One specialist support to develop the templates on
System One and enable the BI team to extract the data required to monitor the
contract for 6 months between October 2017 – March 2018
£63k (recurrently) for 1 band 8a for BI support to establish the dashboards on a
regular basis for the contract, working closely with the WSIC dashboard team and
supporting reconciliation

Ealing New Primary Care Offer Business Case
July 2017 66
The CCG is supporting and resourcing the CEPN which will support education and
training across the standard
The CCG will through the mobilisation steering group consider the clinical resourcing
requirements to support a QI methodology to support delivering the standard
7 Conclusion and Recommendation
The CCGs ambition in commissioning the Ealing Standard is:
1. To have equity of offer and access to patients registered with an Ealing GP through commissioning the Ealing Standard
2. To reduce the unwarranted variation in general practice and improve outcomes for individuals
3. To address the concerns and feedback received from patients regarding access to general practice and drive ongoing improvement over the term of the Ealing Standard.
4. To address the needs of the population as identified in the Joint Strategic Needs Analysis (JSNA) and ensure the primary care standards deliver a full, holistic offer of care for patients
5. To support and improve resilience and sustainability within general practice whilst meeting the strategic requirements as set out in the NWL STP, 5YFV, and the Strategic Commissioning Framework (SCF). It is very clear that general practice is the golden thread that runs through all the delivery areas of the STP supporting and enabling the realisation of the triple aims of the STP of Improving Health & Wellbeing, Improving care & quality, Improving productivity and closing the financial gap.
6. To utilise the opportunity that Primary Care Delegation has provided in enabling the CCG to direct the use of the headroom within the primary care allocation for Ealing GPs. The headroom recognises the historical underfunding in general practice from a national level and the increasing allocation addresses this up to and including 2020/2021.
7. That the CCG commissions an equitable offer on an equitable financial basis from practices and therefore the Ealing Standard is the commissioning intention for PMS discussions to support the NHS England required renegotiation of PMS premium funding.
The CCG is requesting approval relating to three funding streams as outlined below:
8. To utilise £2.8m of the headroom during 2017/2018 with a focus on access increasing to £3,474k to support access, prevention, screening and patient experience recurrently.
9. As the allocation increases in future years, following managing any growth pressures or increases in core primary care spend, such as funding implications of national contract negotiations, increases in rents, rates and applying any NHS business rules as directed by NHSE, further headroom funding released is allocated to support primary care in Ealing to further stretch the primary care offer through stretched targets or new standards in line with the needs of the population.
10. To seek agreement that the funding already being utilised from the CCG programme budget, £7.2m, should continue to be used to commission the Out of Hospital (OOH) services as part of the Ealing Standard. That this agreement is made based on the understanding that the care will need to be provided from somewhere within the healthcare system and for a proportion of the services this would be at a higher cost, £2.6m, in the acute service.

Ealing New Primary Care Offer Business Case
July 2017 67
11. To seek agreement to additional investment from CCG programme budget of £923k into the Ealing Standard noting that the costs have been derived through either the out of hospital costing model or through the LIS incentive scheme approach. The request for an additional £923k annually is made against the most conservative realisation of savings derived directly from the standard of £1,160k in 2018/2019 with a total incremental saving at the end of the 2020/2021 of £4,124k.
12. That the Ealing Standard enables the implementation of primary care led elements of the STP across the five domain areas and underpins some of the financial benefits to be realised e.g ongoing investment into primary care to support mental health care enabling the Like Minded business case (DA4), enabling the use of PAMS (DA1) or the system wide programmes on Diabetes, Hypertension and AF (DA2).
13. To seek approval for a moratorium on the KPIs in 17/18 to start to mobilise and prepare for phase 2 in April 2018. This is in line with the process to mobilise the original OOH services contract with primary care
That the committee note the approach to the costing of the standards and the approach to
contracting:
14. That the costing of the standards has been developed in line with the OOH costing model or using the Local Improvement Scheme (LIS) as the benchmark, with clinical leads determining the length of the clinical interventions and the staff groups involved, with the officers using this information to cost the standards. This was further reviewed by a finance officer outside of Ealing.
15. That the Ealing standard is commissioned as a single wrap around contract from each provider of medical services.
That there is a need to invest in mobilisation through internal and additional resource:
16. That additional resource is agreed as part of the business case to support mobilisation of the standard throughout the rest of 2017/2018 and this is funded from the primary care allocation and the headroom available. That this mobilisation is overseen by a steering group made up of CCG clinical leads and managers with responsibility for primary care. That this group reports into and includes members from the Primary Care Commissioning Committee, F&P and that Healthwatch are included as members.

Ealing New Primary Care Offer Business Case
July 2017 68
Appendix 3 Equality impact statement
Equality and Health Inequalities Analysis
1 Title: The Ealing Standard – Quality Framework for Primary Care 2017/18 – 2020/21
Ealing CCG - July 2017
What are the intended outcomes of this work? Include outline of objectives and function aims Ealing CCG serves a GP registered population of more than 430,000 patients, with 76 GMS/PMS/APMS Contracts. NHS England is increasing the funding allocation on a yearly basis from 2017/18 up to 2020/21, which will allow the CCG to substantially increase the total investment in primary care across Ealing between 2017 and 2021. Ealing CCG intend to use this investment to change from commissioning multiple services from practices to taking a single commissioning approach, with a single wraparound contract for all non-core CCG commissioned services. The ‘Ealing Standard’ will be holistic, improve outcomes and provide better value for money, providing vital investment to ensure primary care in Ealing is both sustained and transformed. It will also help to address equity of funding across practices and public and patient concerns regarding equality of access across the patch. The new Ealing Standard will incorporate:
Available NHS England investment that has not been otherwise allocated to fund
changes in the core contract, changes in rents and rates reimbursements and
demographic changes.
All existing discretionary CCG funding for services, including winter resilience, LIS
schemes and the Out of Hospital services
Reinvestment of the PMS premium
The contract will be offered across general practice in Ealing, with phase one due to commence from 1 October 2017, and full implementation from 1 April 2018. It contains 23 standards covering healthcare and long term condition management, health improvement and access, safety and experience. The majority of standards described are not new and an Equality Assessment has been conducted previously; rather they are being brought together in a single document for the first time. While the impact of the Ealing Standard as a whole will be considered, standards that are new, and therefore the focus of this Equality Analysis are:
Access
Musculoskeletal health
Prevention
Respiratory disease
Carers
Self-care and use of Patient Activation Measures
End of Life care

Ealing New Primary Care Offer Business Case
July 2017 69
Please outline which Equality Delivery System (EDS2) Goals/Outcomes this work relates to? See Annex B for EDS2 Goals and Outcomes
Goal Number Description of outcome
Better health outcomes
1.1 Services are commissioned, procured, designed and delivered to meet the health needs of local communities
1.2 Individual people’s health needs are assessed and met in appropriate and effective ways
1.3 Transitions from one service to another, for people on care pathways, are made smoothly with everyone well-informed
1.4 When people use NHS services their safety is prioritised and they are free from mistakes, mistreatment and abuse
1.5 Screening, vaccination and other health promotion services reach and benefit all local communities
Improved patient access and experience
2.1 People, carers and communities can readily access hospital, community health or primary care services and should not be denied access on unreasonable grounds
2.2 People are informed and supported to be as involved as they wish to be in decisions about their care
2.3 People report positive experiences of the NHS
2.4 People’s complaints about services are handled respectfully and efficiently
Who will be affected by this work? e.g. staff, patients, service users, partner organisations etc.
Registered Patients of Ealing GPs
Families and carers of patients
Staff working in General Practice
Evidence
What evidence have you considered? List the main sources of data, research and other sources of evidence (including full references) reviewed to determine impact on each equality group (protected characteristic). This can include national research, surveys, reports, research interviews, focus groups, pilot activity evaluations or other Equality Analyses. If there are gaps in evidence, state what you will do to mitigate them in the Evidence based decision making section on page 9 of this template. While the impact of the whole Ealing Standard has been considered, the new elements have been considered in more detail, with references listed below.
General:
Ealing JSNA
Public Health England Health Profiles for London –
Ealing New Primary Care Offer Business Case
July 2017 70
Ealing CCG PPE reports to Governing Body
Standard Alternative Provider Medical Services Contract 2016/17 available at https://www.england.nhs.uk/gp/gpfv/investment/gp-contract/
http://www.kingsfund.org.uk/press/press-releases/our-response-don-berwicks-report-patient-safety
Francis, R. (QC) (2013) Report of the Mid Staffordshire NHS Foundation Trust Public Inquiry London:TSO Available at: www.midstaffspublicinquiry.com/report
HM Government, (2014) The Care Act 2014 Available at:www.legislation.gov.uk/ukpga/2014/23/contents/enacted
National Association for Patient Participation (NAPP), (2014) Available at: www.napp.org.uk/overview.html
NHS England (NHSE), (2014) National GP Survey Results Available at: www.england.nhs.uk/statistics/category/statistics/gp-patient-survey/
Access
GP Patient Survey, Ipsos MORI
UCC Data
The King’s Fund, (2012) exploring the association between quality of care and the experience of patients London.
Kontopantelis, E., Roland, M., Reeves, D., (2010 Patient experience of access to Primary Care: identification of predictors in a national patient survey BMC Family Practice Vol: 11 p.61
Bottle, A; Tsang, C; Parsons, C; Majeed, A; Soljak, M; Aylin, P (2012), Association between patient and general practice characteristics and unplanned first time admissions for cancer, observational study. British Journal of cancer, 107 (8),
Rosen R., (2014) Meeting need or fuelling demand? London: Nuffield Trust & NHS England The King’s Fund, (2011) Improving the quality of care in general practice London.
National Audit Office (2015) A Stocktake of Access to General Practice and (2017), improving access to general practice
Imison C, Curry N, Holder H, Castle-Clarke S, Nimmons D, Appleby J, Thorlby R, Lombardo S (2017) Shifting the balance of care, Great expectations, Nuffield Trust
NHSE (2014) Emergency Admissions Technical Paper Carers
Carers UK, (2014) The State of Caring 2014 Available at www.carersuk.org/for-professionals/policy/policy-library/state-of-caring-2014
Ealing JSNA 2016 Carers https://www.ealing.gov.uk/download/downloads/id/11340/carers_chapter_2016.pdf
Ealing Council and Ealing Clinical Commissioning Group (CCG) Joint Carers' Strategy 2012-18
Schonegevel, L. (2013) Macmillan briefing on carers issues Available at: www.macmillan.org.uk/Documents/GetInvolved/Campaigns/MPsCommons2ndReadingBriefing.pdf
NHS England (NHSE), (2014) Commitment to Carers Available at: www.england.nhs.uk/wp-content/uploads/2014/05/commitment-to-carers-may14.pdf
Self-care
Supporting people to manage their health, Kings Fund, 2014, available at: https://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/supporting-people-manage-health-patient-activation-may14.pdf
NHS England PAMs guidance, available at: https://www.england.nhs.uk/ourwork/patient-participation/self-care/patient-activation/pa-faqs/
Prevention
British Society of Gastroenterology (BSG), (2010) Alcohol related disease: Meeting the challenge of improved quality of care and better use of resources London.
Connor, JP, Haber, PS, Hall, WD: Alcohol use disorders. The Lancet, Vol.386, No. 9997, Sep 5, 2015.
Department of Health DH, (2013) CVD Outcomes Strategy: Improving outcomes for people with
or at risk of cardiovascular disease London.
Murray C.J. et al., (2013) UK Health Performance: findings of the Global Burden of Disease Study 2010 The Lancet Vol: 381 pp. 997-1020.
NICE (2006) PH Intervention Guidance 1: Brief interventions and referral for smoking cessation

Ealing New Primary Care Offer Business Case
July 2017 71
in primary care and other settings.
Public Health England (PHE), (2013) NHS Health Check implementation review and action plan
London.
Public Health England (PHE), (2015a) Local Alcohol Profiles Available at: www.lape.org.uk/
Public Health England (PHE), (2015b) Local Tobacco Control Profiles
Available at: www.tobaccoprofiles.info
Public Health England (PHE), (2015c) Tackling high blood pressure From evidence into action. Available at: www.gov.uk/government/publications/high-blood-pressure-action-plan
Stroke Association, (2014) About Stroke Available at: www.stroke.org.uk/about-stroke
Department of Health (DH), (2014) [Online] Available at: www.gov.uk/government/uploads/system/uploads/attachment_data/file/316007/FluImmunisationLetter2014_accessible.pdf
Public Health England (PHE), (2014) Public Health Outcomes Framework for England 2013-2016 Available at: www.phoutcomes.info/
Ealing Health and Wellbeing Strategy 2016-2021 available at https://www.ealing.gov.uk/downloads/download/3755/health_and_wellbeing_strategy
Respiratory
Ealing JSNA
BTS / SIGN Asthma guidelines 2016
Improving the quality of diagnostic spirometry in adults: the National Register of certified professionals and operators
Salford quality standards for primary care
NICE COPD Quality Standards
London Asthma Standards for Children and Young People End of Life
NICE Quality Standard 13 – End of Life care for adults
www.nice.org.uk/guidance/qs13
www.dyingmatters.org
www.goldstandardsframework.org.uk
Ealing JSNA
NWL STP MSK
Preventing musculoskeletal disorders, Fenton, Public Health England 2016.
https://publichealthmatters.blog.gov.uk/2016/01/11/preventing-musculoskeletal-disorders-has-wider-impacts-for-public-health/
Public Health Outcomes Framework
Health and Work: Spotlight on musculoskeletal conditions (MSK), Public Health England and The Work Foundation 2016 https://app.box.com/s/1qm34sx148rx6nyywnjow131xaplp3zl
Arthritis Research UK. Musculoskeletal Health. A Public Approach. Chesterfield: ARUK; 2014. http://www.arthritisresearchuk.org/~/media/Files/Policy%20files/2014/public-health-guide.ashx
National Clinical Guideline Centre. Osteoarthritis Care and management in adults. London: Royal College of Physicians, 2014. https://www.nice.org.uk/Guidance/cg177
National Institute for Health and Care Excellence. Low back pain and sciatica in over 16s: assessment and management (NICE guideline NG59). 2016. www.nice.org.uk/guidance/ng59
Musculoskeletal Health in Ealing. Chapter for Ealing Joint Strategic Needs Assessment 2014, Bernstein, NHS Ealing CCG and London Borough Ealing, 2014
http://www.ealingccg.nhs.uk/media/1859/Ealing_JSNA_MSk_Health_pre-pub_2014-09-06.pdf
Age Consider and detail age related evidence. This can include safeguarding, consent and welfare issues. The Ealing Standard will improve care for people of all ages, but particularly: Children: through the provision of delivery standards for childhood asthma, immunisations and

Ealing New Primary Care Offer Business Case
July 2017 72
proactive health improvement work on childhood tooth decay and obesity. In Ealing, 23.9% of year 6 children are classified as obese, worse than the average for England, so the standard will help protect the health of children. Older adults: through the provision of delivery standards for a wide range of health conditions which particularly impact upon older adults, including cardiovascular, musculoskeletal, dementia, end of life, proactive health checks and cancer screening. In 2013, the top three underlying causes of death people aged 65+ in Ealing were circulatory disorders, cancer and respiratory disorders. (JSNA, 2014) so the new standards will help protect the health of older people. The MSK standard, with provisions for falls assessments, will also support the wellbeing of older adults. Pulse Checks, one of the provisions of the new prevention standard, could help identify AF earlier and could prevent 4,500 strokes and 3,000 deaths per year in the UK (Stroke Association, 2014). Most people affected by strokes are over 65. Safeguarding of both children and vulnerable adults is included in the Ealing Standard to ensure the protection of these groups from harm and abuse. Access will be improved for all age groups, with various forms of access being supported such as online booking of appointments, e-prescribing, online-consultations and generally more appointments offered.
Disability Consider and detail disability related evidence. This can include attitudinal, physical and social barriers as well as mental health/ learning disabilities. The Ealing Standard contains specific measures on both mental health and learning disabilities, which already form part of existing services. In the recent ‘Big Health Check’ engagement event for people with learning disabilities, for the first time LD patients reported positive experiences while attending their GP appointments, with some excellent examples of good practice. These examples have been built upon in the new standards. The KPIs help protect disabled people’s wellbeing by ensuring care is proactive, coordinated and looks after not just their mental health or learning disability, but also their physical health (with a requirement to provide an annual health assessment a KPI for both the mental health and learning disability standards) and vice versa. There are clear requirements for adherence to Accessible Information Standards, including communication support. Disabled people will also benefit from improved access to their GP surgery, including online methods, which for some people may be very helpful. The carers standard will help improve the wellbeing of those who support disabled people (some of whom may also be disabled themselves) with proactive health assessments, flu jabs, and referral to support services.
Gender reassignment (including transgender) Consider and detail evidence on transgender people. This can include issues such as privacy of data and harassment. There is limited specific reference to gender reassignment in the Ealing Standard, however, as many of the measures are about empowering proactive and personalised contact by GP practices, this will benefit all patients, and even more so for patients who are perhaps less likely to attend their GP surgery due to fear of discrimination.
Ealing New Primary Care Offer Business Case
July 2017 73
Marriage and civil partnership Consider and detail evidence on marriage and civil partnership. This can include working arrangements, part-time working, caring responsibilities. There is limited specific reference to marriage and civil partnership in the Ealing Standard; however the Carers Standard may provide some protection for married people and people in a civil partnership, who care for their loved ones. This ensures carers are identified – even those who do not identify as such and feel they are doing what any husband / wife / civil partner would do. It will help protect their health and wellbeing with annual health checks, flu jabs and referral to support services, including talking therapies.
Pregnancy and maternity Consider and detail evidence on pregnancy and maternity. This can include working arrangements, part-time working, caring responsibilities. The Ealing Standard will help improve the health of pregnant patients by improving access to appointments, and through health improvement measures such as providing all pregnant patients with a flu jab. When they have the baby, the access standard will ensure practices will provide a same day assessment for all children under 12 with urgent needs. If the pregnant patient is also a carer, the carer standard will help support them. The Ealing JSNA (2016) identified a higher proportion of females providing unpaid care compared with males.
Race Consider and detail race related evidence. This can include information on difference ethnic groups, Roma gypsies, Irish travellers, nationalities, cultures, and language barriers. The Ealing JSNA (2014) highlights that race is one of the risk factors for Type 2 diabetes – people of Black African, Caribbean or South Asian origin are more at risk. According to the last Census (2011), there were 41% Ealing residents of Asian or Black ethnic origin, so the Ealing Standard may help protect their health by improving diabetes care in general practice, as well as implementing preventative measures through NHS Health Checks. The Health Checks will also identify risk factors for cardiovascular disease, which is also known to have a higher incidence in the BME population. Evidence suggests that people from certain ethnic groups are less likely to participate in bowel and breast cancer screening. However positive endorsement from a healthcare professional can increase screening uptake. The cancer screening standard will ensure that patients receive personal contact from their practice if they do not respond to invitations for bowel and breast screening. This may help ensure that additional people from black and minority ethnic groups are screened and do not develop cancer. There are a wide range of languages spoken in Ealing and there is a clear expectation in the Ealing Standard that patients should have access to accessible information and communication support.

Ealing New Primary Care Offer Business Case
July 2017 74
Religion or belief Consider and detail evidence on people with different religions, beliefs or no belief. This can include consent and end of life issues. According to the 2011 Census 44% of the residents of Ealing regard themselves as Christian, down from 51% in 2001. The proportion of Muslims has increased from 10% to 16%, with the proportions of other major religions remaining more or less the same as during the last census. The new standards mean patients will benefit from improved access to appointments within general practice. If there are cultural or religious regions why people don’t access health care – for example cancer screening – the new standard will ensure practices make personal contact with the individual and so may be able to arrange for special provisions to be made. The self-care standard will enable patients to self-define what is important to them in improving their health, which will enable them to take account of their religion and belief. People at the end of life sometimes experience spiritual difficulties, in addition to a range of physical health issues. The new KPIs ensuring regular reviews with the patient, and an after death analysis at network level to consider lessons learnt.
Sex Consider and detail evidence on men and women. This could include access to services and employment. The Ealing Standard will improve the health of both men and women who in some cases have similar needs – for example, the MSK standard. Low back and neck pain is now the leading cause of disability in England for both men and women combined. Women are more likely to be unpaid carers, with a higher proportion of females than males in Ealing taking on this role (9.5% females v 7.6% males) so they will benefit from the carers specification. Women who may be less likely to attend for breast screening (such as those from BME groups and Muslim women) may be more likely to attend following personal following up healthcare professional. Some standards, such as ring pessary, are targeted at females specifically and will provide additional services closer to home, making them easier to access. Both men and women will benefit from the self-care standard as they will be able to self-define what is important to them in improving their health, which will enable them to take account of their gendered needs.
Sexual orientation Consider and detail evidence on heterosexual people as well as lesbian, gay and bisexual people. This could include access to services and employment, attitudinal and social barriers.
There is limited specific reference to sexual orientation in the Ealing Standard; however, as many of the measures are about improving access, proactive care and empowering self-care, this will benefit all patients.

Ealing New Primary Care Offer Business Case
July 2017 75
Carers Consider and detail evidence on part-time working, shift-patterns, general caring responsibilities. Carers will benefit from their loved ones being able to access primary care more easily, with a case management approach when appropriate, and regular reviews for those at the end of life. Their loved ones will be proactively identified if they are at risk of a wide range of health conditions. Carers themselves will be more readily identified – even those who do not identify as such and feel they are doing what any family member would do. It will help protect their health and wellbeing with annual health checks, flu jabs and referral to support services, including talking therapies.
Other identified groups Consider and detail evidence on groups experiencing disadvantage and barriers to access and outcomes. This can include different socio-economic groups, geographical area inequality, income, resident status (migrants, asylum seekers). The Ealing Standard includes measures to improve the health and wellbeing of other identified groups with vulnerabilities, included people who are homeless. People who are homeless may experience difficulties in accessing primary care, due to inappropriate registration policies, perceived discrimination and staff attitudes, lack of flexibility in services provided and communication barriers. They may have a number of complex health problems, and may also require proactive support to manage their health needs, for example, targeted support, regular and/or longer appointments. The Ealing Standard sets clear delivery standards designed to address this and improve their experience and health outcomes.
Ealing New Primary Care Offer Business Case
July 2017 76
Engagement and involvement
How have you engaged stakeholders with an interest in protected characteristics in gathering evidence or testing the evidence available?
See below.
How have you engaged stakeholders in testing the policy or programme proposals?
A Steering Group was set up to oversee the creation of the Ealing Standard, which includes lay members, Clinical Leads and the LMC. This met fortnightly throughout the development of the proposal. At various stages of development, right from the beginning, the Council of Members were engaged in shaping the work. The majority of services described in the Ealing Standard are not new, so have been widely engaged on previously, and feedback gathered during the duration of the contracts, which have informed this analysis. In particular, lay members have been active members of the Contract Management Group, which has overseen the management of the existing out of hospital services contract, along with the provider’s patient reference group. A wide variety of feedback has been gathered from specific groups (some listed below) and patient feedback on primary care compiled by Ealing Healthwatch. Access has been identified as patient’s biggest concern, which has been addressed in the new standard. The Ealing Standard supports the local delivery of the pan-London Strategic Commissioning Framework for Primary Care, which was contributed to by over 1,500 key stakeholders, including large numbers of patients.
For each engagement activity, please state who was involved, how and when they were engaged, and the key outputs:
This includes:
Council of Members meetings on 10 May, 24 May, 14 June & 5th July 2017 to discuss the rationale, delivery and metrics of each specification taking detailed feedback;
Additional ‘drop in’ sessions for GPs to attend and give their views;
The collection of patient feedback on general practice, over the course of a year;
The implementation of a specific patient survey on primary care access, led by Ealing Healthwatch;
Patient engagement events held in 2016 to explore appropriate KPIs for patient experience measures;
Annual ‘Healthcheck’ event with people with learning disabilities – taking the opportunity in these Standards to build upon what people with learning disabilities have told us improved their care
Engagement with Practice PPG and Network PPG members on specific clinical services on 10 May 2017

Ealing New Primary Care Offer Business Case
July 2017 77
Summary of Analysis Considering the evidence and engagement activity you listed above, please summarise the impact of your work. Consider whether the evidence shows potential for differential impacts, if so state whether adverse or positive and for which groups and/or individuals. How you will mitigate any negative impacts? How you will include certain protected groups in services or expand their participation in public life? Now consider and detail below how the proposals impact on elimination of discrimination, harassment and victimisation, advance the equality of opportunity and promote good relations between groups. As the aim of the Ealing Standard is to be a ‘wraparound’ contract, ensuring that patients across Ealing have access to the same level of high quality of care wherever they access primary care, which should have a positive impact on people with protected characteristics. In addition to commitment to improving access and standardising high quality clinical care, the Ealing Standard has a definite focus on proactive screening and identification of health needs, of care planning and management for those who would benefit from it, and of addressing the wider determinants of wellbeing and self-care. These should have a positive impact on people with protected characteristics. In addition to this, the Ealing Standard makes explicit the need to make reasonable adjustments for people with protected characteristics.
Eliminate discrimination, harassment and victimisation
Where there is evidence, address each protected characteristic (age, disability, gender, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sexual orientation). Much of the Ealing Standard supports people with multiple needs and vulnerabilities, who may experience discrimination, harassment and victimisation. This investment in primary care will ensure there is additional access in primary care where these individuals can experience ongoing support. Where certain populations may experience real or perceived discrimination in their access to primary care, measures to address this are outlined in the standard. For example, ensuring that homeless people do not experience discrimination in their ability to register with a GP practice.
Advance equality of opportunity
Where there is evidence, address each protected characteristic (age, disability, gender, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sexual orientation). The Ealing Standard may help advance equality of opportunity between people who share a protected characteristic and those who do not by ensuring that all patients in Ealing have access to a consistent set of high quality primary care services, closer to home, regardless

Ealing New Primary Care Offer Business Case
July 2017 78
of who they are or where they live. In particular, the self-care standard will advance equality of opportunity by helping patients move away from being passive recipients of care to being active partners in their own health. The use of Patient Activation Measures will help them develop their knowledge, skills and confidence to make informed decisions and adapt their health related behaviours.
Ealing New Primary Care Offer Business Case
July 2017 79
Promote good relations between groups
Where there is evidence, address each protected characteristic (age, disability, gender, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sexual orientation). The Ealing Standard may help promote good relations between groups by ensuring that all patients in Ealing have access to a consistent set of high quality primary care services, closer to home, regardless of who they are or where they live.
Evidence based decision-making
Please give an outline of what you are going to do, based on the gaps, challenges and opportunities you have identified in the summary of analysis section. This might include action(s) to eliminate discrimination issues, partnership working with stakeholders and data gaps that need to be addressed through further consultation or research.
Ensure that the Steering Group takes account of the feedback in the Healthwatch report when it is published;
Ensure that the need to pay due regard to the specific needs of people with protected characteristics is highlighted in communication about the contract and that practices include this in their mobilisation plan;
Amend the Patient Experience standard to make explicit the need to consider how to improve the experiences of people of different race/religion/sexual orientation/gender identity and how they can feel comfortable and welcome in primary care settings;
Ensure that practice Patient Participation Groups are actively involved in overseeing the mobilisation of the Ealing Standard and helping their practices as a ‘critical friend’, with particular regard for the patients in the practice with protected characteristics. This should also be the case for the local Healthwatch and the lay members on the CCG Steering Group.
How will you share the findings of the Equality analysis? This can include corporate governance, other directorates, partner organisations and the public.
The Equality analysis will accompany the business case and draft Ealing Standard document when it is reviewed by the Governing Body for decision.

Ealing New Primary Care Offer Business Case
July 2017 80
Health Inequalities Analysis
Evidence 1. What evidence have you considered to determine what health inequalities exist in relation to your work? List the main sources of data, research and other sources of evidence (including full references) reviewed to determine impact on each equality group (protected characteristic). This can include local and national research, surveys, reports, research interviews, focus groups, pilot activity evaluations or other Equality Analyses. If there are gaps in evidence, state what you will do to mitigate them in the Evidence based decision making section on the last page of this template. See evidence section above.
Impact 2. What is the potential impact of your work on health inequalities? Can you demonstrate through evidenced based consideration how the health outcomes, experience and access to health care services differ across the population group and in different geographical locations that your work applies to? Results from the GP Patient Survey consistently report a poorer experience of making an appointment and lower levels of satisfaction with practice opening time than other CCGs in London. This is also in line with feedback from Healthwatch surveys. A patient’s ease of access to their Practice, and preferred GP, can affect their quality of care and health outcomes (The King’s Fund, 2012).
Looking at the evidence, there is great variability across Ealing practices both in the number of appointments they offer (from less than 70 per 1000 patients to more than 100 per 1000 patients) and their opening times (some closing for lunch and/or half days). This would inevitably lead to inequality of access for patients across Ealing. The aim of the Access standard is to provide very clear expectations for improved access, in every practice, for the benefit of every patient. It provides costed evidence and appropriate investment so that this is achievable by 2020. While the aim of the Ealing Standard is to provide consistent, high quality primary care to all registered patients, the standards identify when population groups should be targeted to ensure this succeeds. Many of the standards integrate across healthcare needs, to ensure health inequalities are targeted and mitigated – for example, referring people with severe and enduring mental health needs to physical health checks, and referring people with long term conditions, and those who are carers, to talking therapies and other forms of support. Groups that have previously experienced health inequalities will benefit from additional focus on screening for a range of health issues, and personal follow up if they do not attend. This will particularly benefit BME groups who experience a higher risk factor in some of these conditions (e.g. diabetes or CVD) but may be less likely to attend screening. Groups that may experience disadvantage due to their circumstances, such as carers or those who are homeless, will be targeted for additional support. Emphasis on self-care and the use of patient activation measures will help clinicians and

Ealing New Primary Care Offer Business Case
July 2017 81
patients have conversations that take in to account the unique needs of individuals.
3. How can you make sure that your work has the best chance of reducing health inequalities? The KPIs in the Ealing Standard all have metrics which can be tracked through the duration of the contract. It will be possible to review the impact of different metrics and make changes if required to better improve the health of disadvantaged groups and tackle health inequalities. There will be substantial ongoing patient engagement on the Ealing Standard, and lay members in the Steering Group will oversee this and pay particular attention to the impact on health inequalities. The impact might take some time to be clearly demonstrated – for some practices this will be a journey of improvement throughout the duration of the contract, to 2020. However, practices will receive support from the CCG to ensure they are on an improvement trajectory and that health inequalities will be addressed. Over the years, the proportion of the contract paid on the basis of population health will be increased, which will increase the emphasis practices’ place on addressing health
inequalities locally.
Monitor and Evaluation 4. How will you monitor and evaluate the effect of your work on health inequalities? See above.
For your records
Name of person(s) who carried out these analyses:
Claire Wilson
Name of Sponsor Director:
Neha Unadkat, Deputy Managing Director – Primary and Integrated Care
Date analyses were completed:
10th July 2017
Review date: 10th July 2018

Ealing New Primary Care Offer Business Case
July 2017 82
Appendix 4 Risk register
ID Type Risk
Pre mitigation rating
Mitigation
Post mitigation rating
Likelihood (1-5)
Impact (1-5)
Score (RAG)
Likelihood (1-5)
Impact (1-5)
score / RAG
1 Operations
There is a risk that transferring services from several existing contracts to a new single wraparound contract may impact on the continuity of service offered to Ealing patients
4 4 16
Go-live of the new access component of the contract will be in September 2017, with a six month lead time until full contract go-live, giving sufficient time to engage with all the practices so that they understand any changes in service requirements and are ready for the go-live date
3 3 9
2 Finance
There is a risk that the cost to deliver the service specification for the wraparound contract is greater or significantly lower than the existing service financial envelope
4 4 16
Engagement with providers through Council of Members meetings, feasibility discussions with clinical leads and developing a robust costing approach
2 3 6
3 PMO
There is a risk of that external expertise required to support the development of the business case will not be secured in time which may impact on the ability to meet the July deadline
4 4 16
Experience suggests the market responds quickly and positively to working in NWL. Employ approach similar to successfully tendered projects of similar type
2 2 4
4 Finance
There is the risk that negotiations with 76 practices, the Local Medical Committee and the local Federation may be protracted, causing delays in implementation
4 4 16 Engage with the LMC, Federation and practices early in the process and test the Contract Specification with the CoM
3 4 12
5 Procurement
There is a risk that the market for extended primary care services in Ealing will not be willing or able to deliver outcomes based care
3 5 15
Engage with providers cross Ealing and invest the provisional provider development fund in readying providers to deliver outcomes based care
2 5 10

Ealing New Primary Care Offer Business Case
July 2017 83
ID Type Risk Pre mitigation rating Mitigation Post mitigation rating
6 Procurement
There is a risk that other providers may challenge the most capable provider procurement route, requiring a full market testing and consequential delays in implementation
3 5 15
Seek legal and procurement advice at an early stage and seek Governing Body approval of the procurement process (within the business case )with the legal and procurement advice in hand
3 2 6
7 Procurement
There may be an actual or perceived conflict of interest for primary care staff in CCG roles working to develop this contract
3 5 15
Robust management of the contract development and approval process, making decisions at CCG committees and involving lay members in decision making
3 4 12
8 Clinical
The intended benefits of outcomes based care may be difficult to realise if they are deprioritised by providers facing significant demand pressures coupled with workforce gaps
3 4 12 Invest the provisional provider development fund in readying providers to deliver outcomes based care
2 5 10
9 Comms
There is a risk that purdah may limit engagement with the public, resulting in a less than optimal engaged public audience prior to business case decision making in July
3 3 9 Draw on existing engagement already undertaken on Access. Plan engagement event post-election (and pre GB meeting).
2 2 4
10 Clinical
There is the risk that the workforce is unavailable locally to deliver the services in the way specified within any future contract
4 4 16
Invest the provisional provider development fund in readying existing workforce to deliver outcomes based care and encourage providers to begin developing workforce plans well before contract go-live
3 4 12

Ealing New Primary Care Offer Business Case
July 2017 84
ID Type Risk Pre mitigation rating Mitigation Post mitigation rating
11 Finance
There is a risk that in order to balance the CCG position, funds that are not committed (including the headroom monies) are held to ensure that the control total is met
3 5 15
The headroom within the allocation has been provided centrally as it is recognised that Ealing practices are further from the target level of funding and therefore can only be invested into general practice. The request to invest the headroom monies will be supported by a business case that demonstrates a return on invest for committing these funds (and any others that would be within the offer).
2 5 10
12 Finance
There is a risk that the precise value of the available headroom funding cannot be determined until premises reviews and other contingencies are accounted for.
3 4 12
A desktop review of premise rent evaluations will be conducted during June to provide better certainty of the value of the available headroom funding.
2 4 8
13 Contractual/Clinical
There is a risk that the national GP contract will change in the future due to wider political changes or that clinical practice will change in the future causing portions of the Ealing Standard to become incorrect or duplicate what is in other contracts.
2 4 8 Include variation or termination clauses in the contract allowing the CCG to flexibly respond to changes in the environment.
2 2 4
14 Finance/Contractual
There is a risk that the PMS contract negotiations are delayed resulting from the wider primary care offer negotiations.
3 3 9
Conduct separate meetings with the PMS practices to keep them informed of timelines and engage with them individually to understand specific issues.
1 3 3
Ealing New Primary Care Offer Business Case
85
Appendix 5 OOHS contracts
The 18 OOHS service specifications are:
1. Ambulatory Blood Pressure Monitoring (ABPM) 2. Warfarin Monitoring 3. Warfarin Advanced Monitoring 4. Case Finding, Care Planning, Care Management 5. Wound Care 6. Coordinate My Care 7. Diabetes Level 1 8. Diabetes Level 2 9. ECG 10. High Risk Diabetes 11. Homeless 12. Serious & Long Term Mental Health Needs (Enhanced Case Management) 13. Complex Common Mental Health Needs (Enhanced Case Management) 14. Near Patient Monitoring 15. Phlebotomy 16. Ring Pessary 17. Spirometry 18. Extended Hours

Ealing New Primary Care Offer Business Case
86
Appendix 6 Outcome of the Independent Review Panel
Outcome of Independent
Review Panel Ealing Primary Care Standards
5th July 2017
Version 1, 24th
March
2014
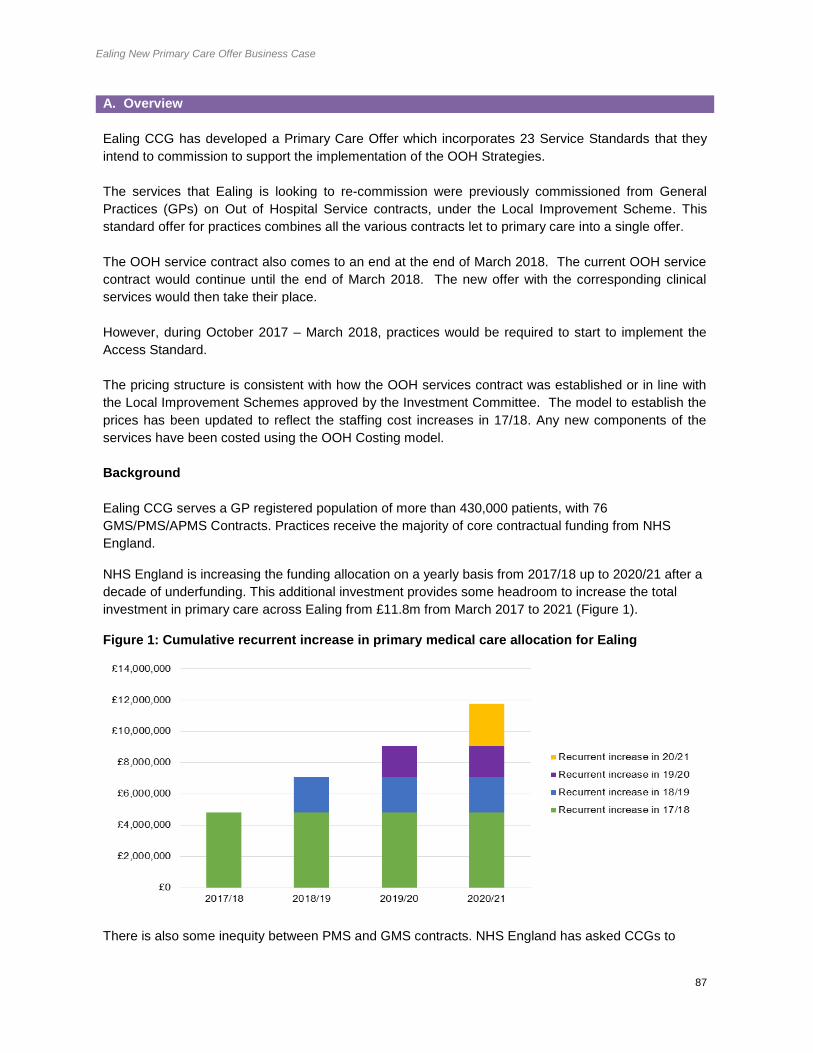
Ealing New Primary Care Offer Business Case
87
A. Overview
Ealing CCG has developed a Primary Care Offer which incorporates 23 Service Standards that they
intend to commission to support the implementation of the OOH Strategies.
The services that Ealing is looking to re-commission were previously commissioned from General
Practices (GPs) on Out of Hospital Service contracts, under the Local Improvement Scheme. This
standard offer for practices combines all the various contracts let to primary care into a single offer.
The OOH service contract also comes to an end at the end of March 2018. The current OOH service
contract would continue until the end of March 2018. The new offer with the corresponding clinical
services would then take their place.
However, during October 2017 – March 2018, practices would be required to start to implement the
Access Standard.
The pricing structure is consistent with how the OOH services contract was established or in line with
the Local Improvement Schemes approved by the Investment Committee. The model to establish the
prices has been updated to reflect the staffing cost increases in 17/18. Any new components of the
services have been costed using the OOH Costing model.
Background
Ealing CCG serves a GP registered population of more than 430,000 patients, with 76
GMS/PMS/APMS Contracts. Practices receive the majority of core contractual funding from NHS
England.
NHS England is increasing the funding allocation on a yearly basis from 2017/18 up to 2020/21 after a
decade of underfunding. This additional investment provides some headroom to increase the total
investment in primary care across Ealing from £11.8m from March 2017 to 2021 (Figure 1).
Figure 1: Cumulative recurrent increase in primary medical care allocation for Ealing
There is also some inequity between PMS and GMS contracts. NHS England has asked CCGs to

Ealing New Primary Care Offer Business Case
88
review all contracts to give equality of opportunity to all GP practices to support fairer distribution of
funding at a locality level and provide equality of opportunity to all practices to provide the same range
of services. The level of “PMS premium” funding currently invested in contracts with Ealing practices is
£640,000 which will be invested fairly across all practices over a 4 year timeframe.
The CCG also commissions a number of services from practices directly for services outside the core
contract that are best delivered from primary care for a registered population. With effect from the 1st
April 2017, Ealing CCG took on responsibility for the commissioning of general practice contracts and
the overall management of the primary care allocation. This enables us to accelerate and localize
primary care transformation, with increased autonomy to shape future primary care services and a
stronger voice for General Practice to influence decision making.
Ealing CCG intend to use this investment to change from commissioning multiple services from
practices to taking a single commissioning approach, with a single wraparound contract for all non-
core CCG commissioned services. The ‘Ealing Standard’ will be holistic, improve outcomes and kpi
provide better value for money, providing vital investment to ensure primary care in Ealing is both
sustained and transformed. It will also help to address equity of funding across practices and public
and patient concerns regarding equality of access across the patch.
The new Ealing Standard will incorporate:
Available NHS England investment that has not been otherwise allocated to fund changes in
the core contract, changes in rents and rates reimbursements and demographic changes.
All existing discretionary CCG funding for services, including winter resilience, LIS schemes
and the Out of Hospital services
Reinvestment of the PMS premium
Funding made available from practices opting out of out of hours services, which will be
separately procured for all patients.
NHS England funding for essential and additional services, estates, Directed Enhanced Services
(DES) and Quality and Outcomes Framework (QOF) will remain outside the Ealing Standard.
The majority of services transferring to the Ealing standard will be paid on a capitation basis; some will
continue to be paid on an activity or prevalence basis. This may change over time (Figure 2).
Capitation-based Activity-based
Respiratory (except diagnostic spirometry)
Cardiovascular (AF, HTN/ABPM, HF)
Musculoskeletal health
Care Planning and co-ordination
End of Life care
Wound Care
Dementia
Cancer screening
Prevention
Self care
Learning Disabilities
Carers
Cardiovascular (Warfarin Monitoring,
Warfarin Initiation, ECG)*
Diabetes (initiation)*
Respiratory (Diagnostic Spirometry)*
Phlebotomy*
Ring Pessary*
Homeless*
ABPI*

Ealing New Primary Care Offer Business Case
89
Access
Medicines optimisation and medicines safety
Drug Monitoring (NPT)
Patient Experience
Business Management (Pre-Qualifier)
Demand Management
Prevalence-based
Diabetes (High Risk and care for patients with
diabetes)
Mental Health
Figure 2: Summary of payment mechanism for each standard of contract
Independent Review Panel Process
Ealing CCG set out in its Annual Commissioning Intention document for 2014/2015 both the approach
they intended to take to commissioning a range of ‘Out of Hospital’ services and their view that in the
majority of instances GPs were the most capable providers of these services. The CCGs published
the intention to let the OOH contract to primary care in Ealing and received no challenge to either the
approach or the commissioning route.
The same process will be applied for this contract.
The process incorporates the Out of Hospital framework that the CCGs across North West London
developed to support the procurement of out of hospital services. The framework balances the
requirements of complying with the law and reducing legal challenge with the need to make effective
and integrated commissioning decisions that are right for the local population.
The services that the original process covered when the OOH services contract was let are:
Ambulatory blood pressure monitoring (ABPM)
Anticoagulation
Care planning
Chronic Obstructive Pulmonary Disease (COPD)
Diabetes
Electrocardiogram (ECG)
Homeless care
Management of common mental health issues
Mental health – transfer of care
Near patient testing
Phlebotomy
Ring pessary
Vasectomy
Wound care
The second stage of the process includes:
Additional Respiratory Components
Musculoskeletal Services (MSK)
End of Life
Dementia
Cancer Screening
Self Care and Patient Activation Measures
Learning Disability
Carers
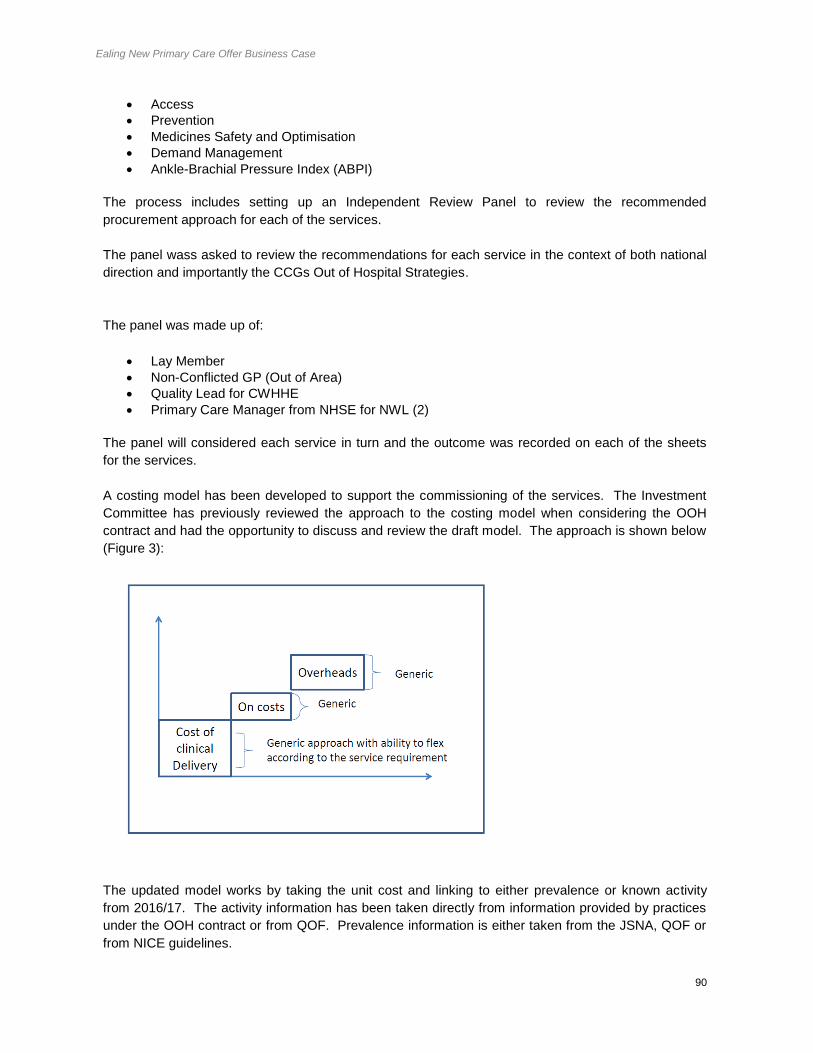
Ealing New Primary Care Offer Business Case
90
Access
Prevention
Medicines Safety and Optimisation
Demand Management
Ankle-Brachial Pressure Index (ABPI)
The process includes setting up an Independent Review Panel to review the recommended
procurement approach for each of the services.
The panel wass asked to review the recommendations for each service in the context of both national
direction and importantly the CCGs Out of Hospital Strategies.
The panel was made up of:
Lay Member
Non-Conflicted GP (Out of Area)
Quality Lead for CWHHE
Primary Care Manager from NHSE for NWL (2)
The panel will considered each service in turn and the outcome was recorded on each of the sheets
for the services.
A costing model has been developed to support the commissioning of the services. The Investment
Committee has previously reviewed the approach to the costing model when considering the OOH
contract and had the opportunity to discuss and review the draft model. The approach is shown below
(Figure 3):
The updated model works by taking the unit cost and linking to either prevalence or known activity
from 2016/17. The activity information has been taken directly from information provided by practices
under the OOH contract or from QOF. Prevalence information is either taken from the JSNA, QOF or
from NICE guidelines.

Ealing New Primary Care Offer Business Case
91
The diagram below provides further detail (Figure 4):
B. Financial Summary
This paper is followed by a series of summary sheets for each service. The financial section shows
the total expected cost at Ealing CCG level.
Overall Recommendations:
The Independent Review panel was asked to review the proposed procurement approach for each service and make a recommendation to the governing body.
5 Confidential |
At the most granular level, each service is divided into input component costs to provide standard unit cost and is linked to prevalence or activity
Inputs
FTE and on - costs
Consumables
Equipment and training
Overheads
Standard unit cost
Outcomes U nit cost
Blended unit cost
Where a service has multiple levels (e.g. diabetes) we have calculated the unit cost for each level and amalgamated this to a give a single blended unit cost which spans across all activity levels
I nputs have been tested with a large range of stakeholders, including: • LMC • CCG Chairs • HoFs • GPs • Lead consultants • Service leads • Practice managers • Practice nurses
For example • P er 1,000 patients
on a list with say 100 patients requiring treatment for a disease
• The cost of treating one patient is £5
• The cost of treating 100 patients is £500
• Per 1,000 patients, the cost of delivering this service is £500
Prevalence
Activity 2016/17
Weighted list
• Single adjustment for prevalence across CWHHE based on QoF / HSCIC data
• A single adjustment is not optimal but it simplifies the unit cost in the service contract
A djustment at practice level for local population demographics
or
For the
capitated costs
– the unit cost
is multiplied by
the number of
patients for the
service across
the borough
and divided by
the weighted
population of
the borough

Ealing New Primary Care Offer Business Case
92
Overall Recommendation Table:
Service Line Recommendation from
IRP
Cost
1 Respiratory (new components) Most capable provider £214,329
2 Musculoskeletal Services (MSK) Most capable provider £316,369
3 End of Life (new components) Most capable provider £270,052
4 Dementia Most capable provider £66,245
5 Cancer Screening Most capable provider £195,108
6 Self Care and Patient Activation
Measures
Most capable provider £25,396
7 Learning Disability Most capable provider £117,065
8 Carers Most capable provider £180,927
9 Access Only capable provider £2,838,824
10 Prevention Most capable provider £147,393
11 Medicines Safety and Optimisation Most capable provider £390,217
12 Demand Management Most capable provider £18,532
13 Wound Care (ABPI) Most capable provider £24,230
Total £4,804,777
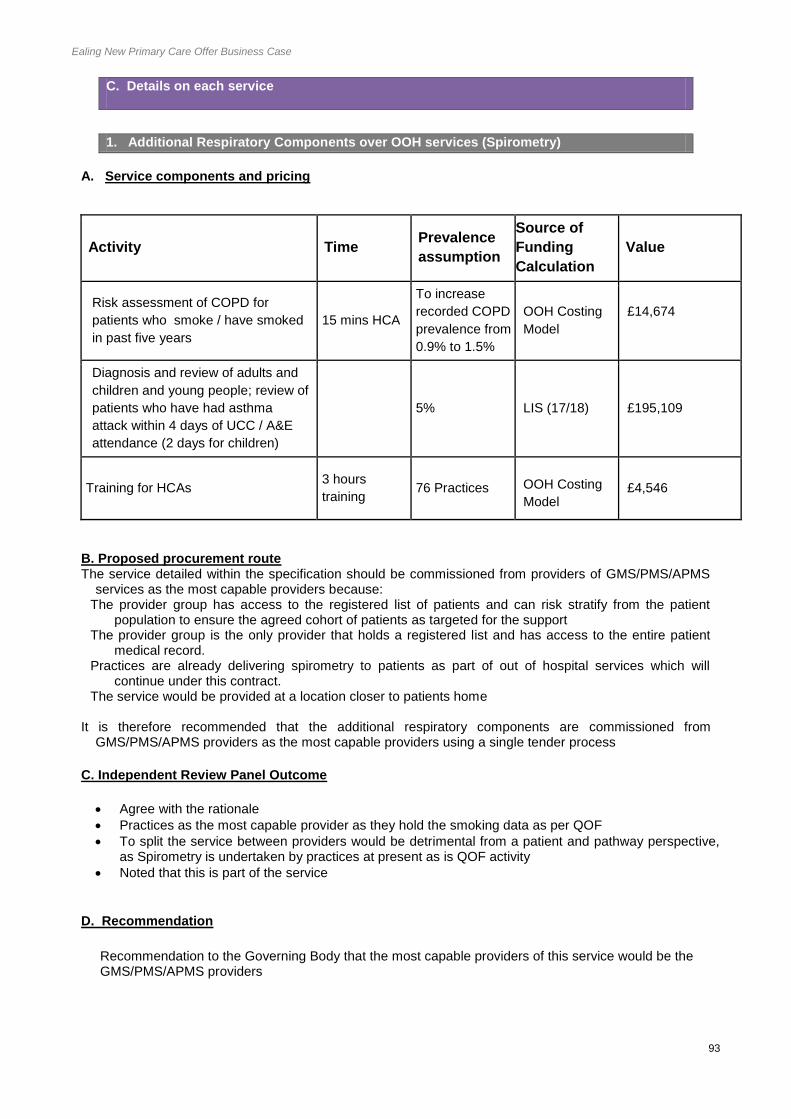
Ealing New Primary Care Offer Business Case
93
C. Details on each service
1. Additional Respiratory Components over OOH services (Spirometry)
A. Service components and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Risk assessment of COPD for
patients who smoke / have smoked
in past five years
15 mins HCA
To increase
recorded COPD
prevalence from
0.9% to 1.5%
OOH Costing
Model
£14,674
Diagnosis and review of adults and
children and young people; review of
patients who have had asthma
attack within 4 days of UCC / A&E
attendance (2 days for children)
5%
LIS (17/18) £195,109
Training for HCAs 3 hours
training 76 Practices
OOH Costing
Model £4,546
B. Proposed procurement route The service detailed within the specification should be commissioned from providers of GMS/PMS/APMS
services as the most capable providers because: The provider group has access to the registered list of patients and can risk stratify from the patient
population to ensure the agreed cohort of patients as targeted for the support The provider group is the only provider that holds a registered list and has access to the entire patient
medical record. Practices are already delivering spirometry to patients as part of out of hospital services which will
continue under this contract. The service would be provided at a location closer to patients home
It is therefore recommended that the additional respiratory components are commissioned from
GMS/PMS/APMS providers as the most capable providers using a single tender process
C. Independent Review Panel Outcome
Agree with the rationale
Practices as the most capable provider as they hold the smoking data as per QOF
To split the service between providers would be detrimental from a patient and pathway perspective, as Spirometry is undertaken by practices at present as is QOF activity
Noted that this is part of the service
D. Recommendation
Recommendation to the Governing Body that the most capable providers of this service would be the GMS/PMS/APMS providers

Ealing New Primary Care Offer Business Case
94
2. Musculoskeletal services
A. Service components and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Refer to weight loss and healthy
lifestyle programmes for people at risk
of lower limb osteoarthritis and back
pain. 5 mins nurse 6.10%
OOH Costing
Model £63,459
Refer patients with a history of falls, or
at medium and high risk of falls, for a
falls assessment, according to local
referral pathway (under development). 5 mins nurse 3.50%
OOH Costing
Model £36,411
Refer people off work for a
musculoskeletal condition for more than
four weeks, when clinically appropriate,
to the ‘Fit for Work’ scheme or an
equivalent occupation health review.
30 mins GP 0.30%
OOH Costing
Model £79,602
Manage patients with chronic
musculoskeletal pain in primary care if
a treatable musculoskeletal condition
has been excluded, particularly those
previously assessed by
musculoskeletal, orthopaedic or pain
services.
5 mins GP 3.70%
OOH Costing
Model
£129,253
Training for clinical and non-clinical
staff.
Drs: 60
minutes/yr
Nurses, HCA:
30 minutes/yr
Reception: 20
minutes/yr
76 Practices
OOH Costing
Model £7,644
B. Proposed procurement route Musculoskeletal services detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because: The provider group has access to the registered list of patients and can proactively case find from the
patient population, refer patients and prescribe. The provider group is the only provider that holds a registered list and has access to the entire patient
medical record. The provider group would be able to manage this vulnerable and complex cohort of patients care in the
context of their complete medical record The service would be provided at a location convenient to the patients’ home.
It is therefore recommended that the musculoskeletal service is commissioned from GMS/PMS/APMS
providers as the most capable providers using a single tender process.
C. Independent Review Panel – outcome
Primary care is the Coordinator/Navigator to the rest of the system and this service would ensure the rest of the pathway is successful

Ealing New Primary Care Offer Business Case
95
This is clarifying the pathway with primary care in the role of the Coorinator/Navigator for the patient and the rest of the system
Additional time reflects the work being asked for by the offer D. Recommendation
Recommendation to the Governing Body that the most capable providers of this service would be the GMS/PMS/APMS providers
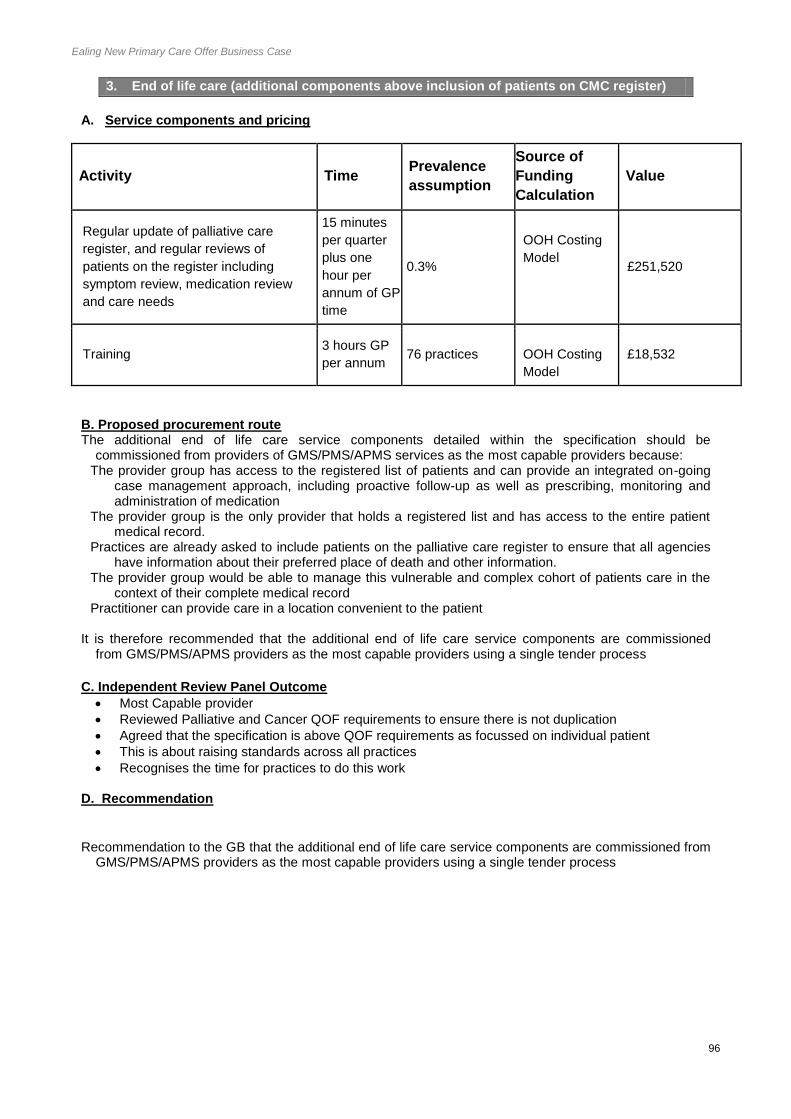
Ealing New Primary Care Offer Business Case
96
3. End of life care (additional components above inclusion of patients on CMC register)
A. Service components and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Regular update of palliative care
register, and regular reviews of
patients on the register including
symptom review, medication review
and care needs
15 minutes
per quarter
plus one
hour per
annum of GP
time
0.3%
OOH Costing
Model £251,520
Training 3 hours GP
per annum 76 practices
OOH Costing
Model
£18,532
B. Proposed procurement route The additional end of life care service components detailed within the specification should be
commissioned from providers of GMS/PMS/APMS services as the most capable providers because: The provider group has access to the registered list of patients and can provide an integrated on-going
case management approach, including proactive follow-up as well as prescribing, monitoring and administration of medication
The provider group is the only provider that holds a registered list and has access to the entire patient medical record.
Practices are already asked to include patients on the palliative care register to ensure that all agencies have information about their preferred place of death and other information.
The provider group would be able to manage this vulnerable and complex cohort of patients care in the context of their complete medical record
Practitioner can provide care in a location convenient to the patient
It is therefore recommended that the additional end of life care service components are commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process
C. Independent Review Panel Outcome
Most Capable provider
Reviewed Palliative and Cancer QOF requirements to ensure there is not duplication
Agreed that the specification is above QOF requirements as focussed on individual patient
This is about raising standards across all practices
Recognises the time for practices to do this work
D. Recommendation
Recommendation to the GB that the additional end of life care service components are commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process

Ealing New Primary Care Offer Business Case
97
4. Dementia
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Maintain >80% in diagnosis
rates
Review of patients with
dementia, including medication
and care plans
Accept referrals form the
Cognitive Impairment and
Dementia Service with support
of link workers and monitor
progression of dementia
>80% for all
patients
diagnosed
OOH Costing
Model
£66,245
B. Proposed procurement route The service for dementia patients detailed within the specification should be commissioned from providers
of GMS/PMS/APMS services as the most capable providers because: The provider group has access to the registered list of patients and can provide an integrated on-going
case management approach, including proactive follow-up as well as prescribing, monitoring and administration of medication
The provider group is the only provider that holds a registered list and has access to the entire patient medical record.
The provider group would be able to manage this vulnerable and complex cohort of patients care in the context of their complete medical record
The service would be provided at a location convenient to the patient
It is therefore recommended that dementia is commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process
C. Independent Review Panel Outcome
Delivery is explicit
KPI is higher than QOF requirement
Money needs to follow the patient as they are transferred from a secondary care setting to primary care and recompense to maintain high level of support for this patient group
Standard recognises that by increasing diagnoses rates, means managing patients to ensure no deterioration and provide proactive support takes more time
D. Recommendation
Recommendation that dementia is commissioned from GMS/PMS/APMS providers as the most capable
providers using a single tender process

Ealing New Primary Care Offer Business Case
98
5. Cancer screening
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Letter / phone call to patients from the practice GP who have not responded to the bowel cancer screening invitation
Increase from 44%
LIS (17/18)
£78,043
Letter / phone call to patients from the practice GP who have not responded or declined to attend a breast cancer screening invitation.
Increase from 67%
PMS London Offer baseline
£117,065
B. Proposed procurement route The cancer screening service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because: The provider group has access to the registered list of patients and is therefore best placed to provide
proactive follow-up The CCGs believe that the costs of competitively procuring the service are high for a service that has a
low value per item and low clinical risk. Enabling providers of GMS/PMS/APMS services to deliver a phlebotomy service supports convenient and
accessible care for patients.
It is therefore recommended that cancer screening is commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process
C. Independent Review Panel Outcome
- The Good Practice Guide for Cancer Screening in London recommends interventions to increase screening uptake through endorsement by a patient’s own GP.
D. Recommendation
Recommendation to GB that cancer screening standard is commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process

Ealing New Primary Care Offer Business Case
99
6. Self care and patient activation measures
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Review Patient Activation Status when reviewing patients care plan and input PAM data. Training on how to use the Patient Activation Status to support self-management of long term conditions.
5 mins
2% of practice population
OOH Costing Model
£16,304
Training for HCAs/Administrative team
3 hours 76 practices OOH Costing Model
£9,092
A. Proposed procurement route The self-care service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because: The provider group has access to the registered list of patients and can provide this service as part of
their an integrated on-going case management approach The service would be provided at a location closer to patients home
It is therefore recommended that self-care and patient activation is commissioned from GMS/PMS/APMS
providers as the most capable providers using a single tender process
B. Independent Review Panel Outcome Supporting patients to take more proactive role in self-care is a key national strategy as well as STP strategy
D. Recommendation
Recommendation to the GB that self-care and patient activation is commissioned from GMS/PMS/APMS
providers as the most capable providers using a single tender process
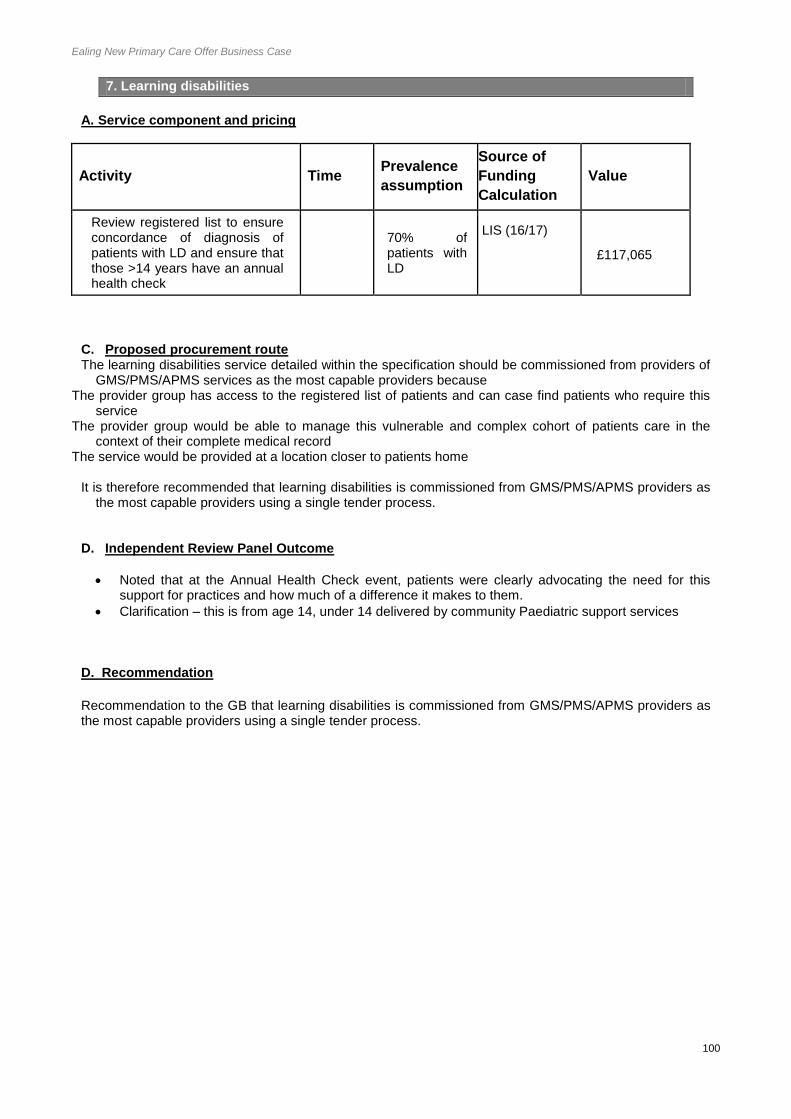
Ealing New Primary Care Offer Business Case
100
7. Learning disabilities
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Review registered list to ensure concordance of diagnosis of patients with LD and ensure that those >14 years have an annual health check
70% of patients with LD
LIS (16/17)
£117,065
C. Proposed procurement route The learning disabilities service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because The provider group has access to the registered list of patients and can case find patients who require this
service The provider group would be able to manage this vulnerable and complex cohort of patients care in the
context of their complete medical record The service would be provided at a location closer to patients home
It is therefore recommended that learning disabilities is commissioned from GMS/PMS/APMS providers as
the most capable providers using a single tender process. D. Independent Review Panel Outcome
Noted that at the Annual Health Check event, patients were clearly advocating the need for this support for practices and how much of a difference it makes to them.
Clarification – this is from age 14, under 14 delivered by community Paediatric support services D. Recommendation
Recommendation to the GB that learning disabilities is commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process.
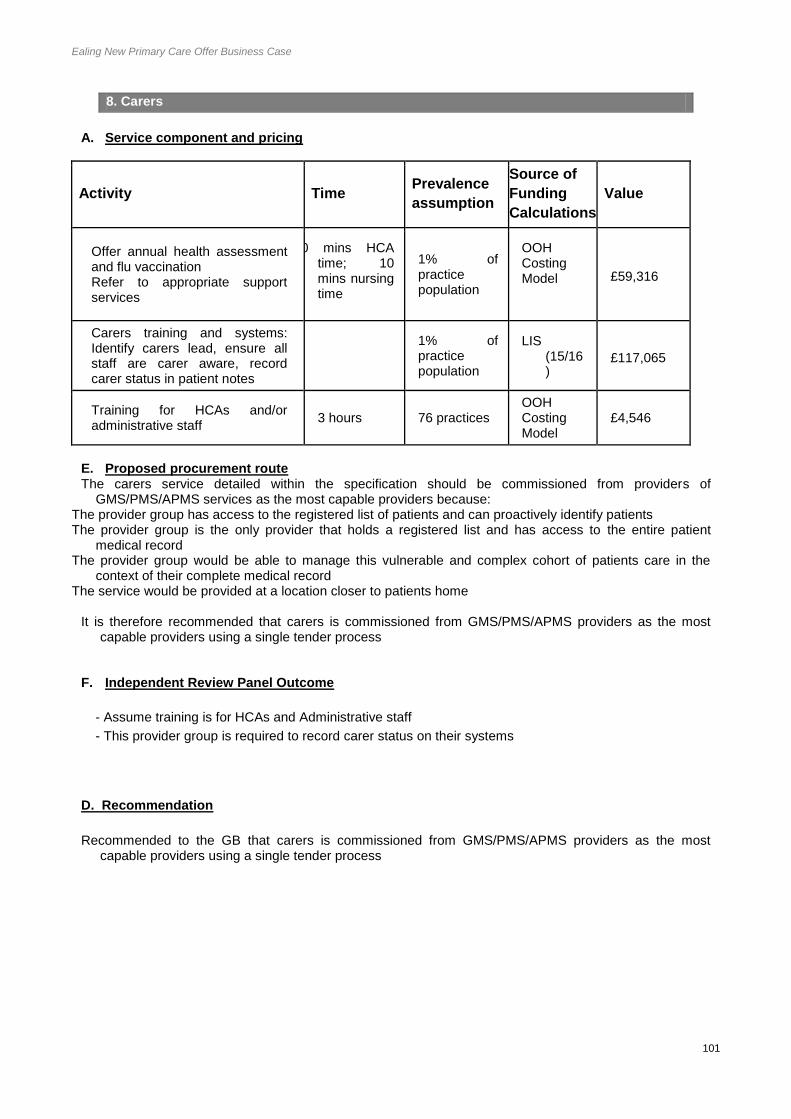
Ealing New Primary Care Offer Business Case
101
8. Carers
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculations
Value
Offer annual health assessment and flu vaccination Refer to appropriate support services
30 mins HCA time; 10 mins nursing time
1% of practice population
OOH Costing Model £59,316
Carers training and systems: Identify carers lead, ensure all staff are carer aware, record carer status in patient notes
1% of practice population
LIS (15/16)
£117,065
Training for HCAs and/or administrative staff
3 hours 76 practices OOH Costing Model
£4,546
E. Proposed procurement route The carers service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because: The provider group has access to the registered list of patients and can proactively identify patients The provider group is the only provider that holds a registered list and has access to the entire patient
medical record The provider group would be able to manage this vulnerable and complex cohort of patients care in the
context of their complete medical record The service would be provided at a location closer to patients home
It is therefore recommended that carers is commissioned from GMS/PMS/APMS providers as the most
capable providers using a single tender process F. Independent Review Panel Outcome
- Assume training is for HCAs and Administrative staff
- This provider group is required to record carer status on their systems
D. Recommendation
Recommended to the GB that carers is commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process

Ealing New Primary Care Offer Business Case
102
9. Access
G. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculations
Value
By 2020, patient access to primary medical care from 8-6.30 Monday to Friday as set out in the strategic commissioning framework; At least 100 appointments per 000 population, 105 during winter period During Opening hours: Staffed reception Under 12 or for any patient with urgent needs seen same day Flexible appointment System Telephone consultations and online booking (4 weeks in advance) Ability to book appointment with clinician of patients choosing through any route Home visits triaged within 1 hour and visit time agreed Accept UCC re-directions
1 GP, 2 x band 4 (HCA / admin) per hour per 1,100 registered list size
100% patient population
OOH Costing Model
£2,838,824
H. Proposed procurement route The access service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the only capable providers because: The terms of the strategic commissioning framework can only be met by general practice. The provider group is the only provider that holds a registered list and has access to the entire patient
medical record. The service would be provided at a location closer to patients home
It is therefore recommended that access is commissioned from GMS/PMS/APMS providers as the only
capable providers using a single tender process
I. Independent Review Panel Outcome
Provided context of development of this standard
And feedback from Patients and Public over the last few years on access to primary care
Explained that Healthwatch is running a survey across the borough – early feedback from the survey has fed into the development of the standard – Report to be added to the Business Case
Primary care funding in Ealing is significantly distant from target funding levels
Add Healthwatch report to Business Case
Clear that these areas of access are not defined in the core contract for PMS/GMS, and 1 APMS contract, however, 4 APMS contracts are aligned to this specification and therefore would not be eligible for this component of the offer.
D. Recommendation

Ealing New Primary Care Offer Business Case
103
Recommendation that access is commissioned from GMS/PMS/APMS providers as the only capable
providers using a single tender process

Ealing New Primary Care Offer Business Case
104
10. Prevention
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculations
Value
Imms call and recall 240 mins admin OOH Costing Model
£82,993
Training 8 hours admin OOH Costing Model
£12,123
Proactive identification of patients with CKD
10 min nurse patient population 4,679
OOH Costing Model £22,640
Blood pressure monitoring
10 min HCA patient population 4,300
OOH Costing Model
£16,304
Management of GFR
10 min HCA patient population 430
OOH Costing Model
£1,630
Pulse Checks 1 min nurse patient population 24,186
OOH Costing Model £11,703
B. Proposed procurement route The prevention service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because: The provider group has access to the registered list of patients and is therefore best placed to risk stratify,
screen and provide proactive follow-up The service would be provided at a location closer to patients home
It is therefore recommended that the prevention service is commissioned from GMS/PMS/APMS providers
as the most capable providers using a single tender process.
C. Independent Review Panel Outcome
Explained that the call/recall for Childhood Imms is not done by the CHIS is Ealing which led to a Serious Incident in 2015/16
D. Recommendation
Recommendation to GB that the prevention service is commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process.

Ealing New Primary Care Offer Business Case
105
11. Medicines safety and optimisation
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculations
Value
Patient safety audit as part of the Medicines Optimisation and Safety Scheme
Identify and review patients with unsafe prescriptions in line with MHRA alerts
Abide by the North West London Integrated Formulary, NICE guidance and other nationally agreed guidance.
n/a
LIS (17/18)
£390,217
B. Proposed procurement route The medicines safety service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because: This service is about managing prescribing for patients from a practices own list safely and to national and
local guidelines
It is therefore recommended that the medicines safety and optimisation service is commissioned from GMS/PMS/APMS providers as the most capable providers using a single tender process.
C. Independent Review Panel Outcome
No additional comments, but clarified that areas for focus for audits, will be agreed annually
D. Recommendation
Recommendation to the GB that the medicines safety and optimisation service is commissioned from
GMS/PMS/APMS providers as the most capable providers using a single tender process

Ealing New Primary Care Offer Business Case
106
12. Demand management
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculations
Value
Refer all referrals through RFS unless the referral is on the specific RFS exclusion list.
Comply with the PPwT Policies; review referral data and engage in practice referral discussions for a range of specialties
Conduct internal practice peer reviews and/or establish processes to review referrals and participate in peer reviews in network based sessions as arranged by the CCG (1 per annum)
3 hours GP time
n/a
Out of Hospital Costing Model
£18,532
B. Proposed procurement route The demand management service detailed within the specification should be commissioned from providers
of GMS/PMS/APMS services as the most capable providers because: This standard requires practices to reflect and peer review their referring practices
It is therefore recommended that demand management is commissioned from GMS/PMS/APMS providers
as the most capable providers using a single tender process. C. Independent Review Panel Outcome Clarification that there would be 1 peer review per annum
D. Recommendation
Recommendation to the GB that the medicines safety and optimisation service is commissioned from
GMS/PMS/APMS providers as the most capable providers using a single tender process

Ealing New Primary Care Offer Business Case
107
13. Wound Care (ABPI)
A. Service component and pricing
Activity Time Prevalence
assumption
Source of
Funding
Calculation
Value
Carry out ABPI 30 minutes
of a nurse
time 1000 patients
OOH Costing
Model
£17,230
Equipment and Training
OOH Costing
Model
£7,000
B. Proposed procurement route The ABPI service detailed within the specification should be commissioned from providers of
GMS/PMS/APMS services as the most capable providers because: – The provider group has skilled staff capable of delivering the service – The provider group would be able to manage this cohort of patients in the context of their
complete medical record – The service would be provided at a location closer to patients home
It is therefore recommended that ABPI is commissioned from GMS/PMS/APMS providers as the most
capable providers using a single tender process
C. Independent Review Panel Outcome
Recognised that the overall standards brings the role of primary care together in supporting the system D. Recommendation
Recommendation that ABPI is commissioned from GMS/PMS/APMS providers as the most capable providers
using a single tender process

Ealing New Primary Care Offer Business Case
108
Notes from IRP 05.07.17:
Introduction and Context provided by Tessa Sandall
Purpose of the meeting is to review specifications to determine whether GMS/PMS/APMS contract holders
were the most capable provider and the services should be commissioned using a single tender waiver
process.
Governing Body signed off the procurement approach which remains in place which sets out the decision
making tree, described in the paper.
The Independent Review Panel (IRP) is a part of that process.
The Panel fed back on each specification as described on the cover sheets.
Overall feedback from IRP
The offer is patient orientated and link to the ‘I’ Statements developed when Whole Systems Integrated Care
was being developed. This will go quite some way to implementing this.
Supports the GPFV on providing resilience and sustainability in general practice, providing continuity and
coordination of care for individuals
This offer will support the agenda of raising standards and reducing variation across primary care thereby
delivering Quality Improvements. It recognizes the need to pay for the work that primary care is having to do
as the population changes and not doing more for the same.
Primary Care is the most capable provider of the overall standards as they are the registered holders of the
list, can provide continuity of care, working with a multi-disciplinary team and provide a
coordination/navigation function for the rest of the system

Ealing New Primary Care Offer Business Case
109
Appendix 7 Annual Self Declaration
Issue Please
Tick
Maintaining and achieving all regulatory requirements including CQC, HTA, HFEA, MHRA, and
medicines regulation
Ensuring delivery of primary medical services contractual and statutory requirements. No unlifted,
uncontested, related breaches in the last 12 months.
Confirming that the practice is registered with the CQC with no conditions, except in circumstances
beyond the control of practices, such as the void position resulting from GP retirements
Having due regard to NHS policy, clinical guidelines, best practice and local CWHHE policies and
procedures
Ensuring that all staff are appropriately credentialed, including:
DBS check
Work permits
Maintenance of professional accreditation and statutory registration
Revalidation for doctors
Confirming that all doctors meet all requirements to practice, do not have any restrictions on their
registration, and are also not under investigation for any clinical matters
Ensuring that appropriate insurance arrangements are in place:
Employers liability
Public liability
Medical negligence cover (doctors only)
Professional liability insurance (nurses and therapists not employed within the NHS)
Ensuring that staff receive regular mandatory training:
General health & safety
Fire
Manual handling
Basic life support
Safeguarding
Infection prevention and control – hand hygiene (basic)

Ealing New Primary Care Offer Business Case
110
Ensuring that appropriate clinical governance arrangements are in place, including but not limited to:
Evidence of having undertaken appropriate checks of staff employed(as above)
Policies and procedures to ensure a safe working environment and safe care for patients
Signed Information Sharing Agreement as part of the Federation or Cluster
Information governance and security – Completion of Information Governance Toolkit
Continuing professional education and other training
Clinical audit and other quality review mechanisms
Review of patient feedback and complaints, action taken and any trends identified
Incident reporting mechanism
Review of incidents with corrective action taken
Maintenance of a clinical risk log
Checking staff vaccinations and incidence of communicable diseases(e.g.Hep B)
Notifying Ealing GPF of any material incident or issue and providing evidence of root cause analysis and corrective action taken
Process for logging and taking action against Clinical Alerts
Evidence of collection of Equality and Diversity data to support delivery of appropriate services for the population served
Ensuring the practice participates in clinical audit cycles and peer review external to their practice
Ensuring the practice has an open list
Ensuring same day appointments are available for patients clinically assessed as requiring them
Ensuring individuals have access to relevant and comprehensive information, in the right formats, to
inform choice and decision-making about their care
Ensuring information and services are available for individuals who are able to self-manage their
conditions or who need care plan support
Ealing New Primary Care Offer Business Case
111
Appendix 8: Primary Care Offer Steering Group TOR
__________________________________________________________________________
Ealing Primary Care Offer steering group Terms of Reference
___________________________________________________________________
1. Purpose
Ealing CCG are developing a primary care offer within the borough, to be commissioned from April
2018. This new offer is distinct from the core GMS and PMS contracts. The aim is also for the
Access component to go live from October 2017. The ‘Ealing Primary Care Offer steering group’ will
oversee and drive this process. It will:
• Oversee the development of a business case for decision making by the Ealing CCG Governing
Body;
• Drive the development of the new contract specification;
• Ensure an appropriate procurement approach is employed, compliant with procurement rules
and providing assurance to the CCG;
• Ensure clinical safety and quality is maintained during and post-contract transition, and risks and
issues managed; and
• Oversee the mobilisation of the new primary care offer.
This is a discussion-only body to oversee the development of the specification. All
recommendations will be made by committees and decisions made by the Governing Body.
2. Responsibilities
To identify and agree services to be commissioning within the new primary care offer, ensuring
all contract interdependencies (GMS, PMS etc.) are realised and managed;
To identify the high level priority outcomes, ensuring service users have been engaged and their
views are reflected in the approach;
To design an outcomes-based framework with linked financial incentives for in scope services;
To identify contract budget, commercial risk and reward arrangements;
To identify KPIs linked to the desired outcomes against which the contract will be monitored;
To oversee the development of the contract service specification and overarching business case
for Ealing CCG Governing Body decision making;
To oversee the development of appropriate procurement documentation ensuring alignment with
procurement legislation;
To manage the commissioning and mobilisation process;
To develop a detailed programme plan (incorporating phases: Plan, Engage, monitoring
progress against plan and escalating any major risks and issues to Ealing CCG Governing
Body for resolution;
To ensure appropriate engagement with protected and disadvantaged groups, and that an
equalities impact assessment has been undertaken;
To ensure all stakeholder groups are identified and appropriately engaged, and the impact on
their services realised;

Ealing New Primary Care Offer Business Case
112
To ensure patient safety and service quality is maintained throughout the process;
To identify and address any risks and issues that may be realised throughout the procurement
process; and
Report progress to the Ealing CCG Governing Body in line with reporting requirements.
3. Reporting and accountability
The Ealing Primary Care offer steering group will be accountable to the Ealing CCG Governing Body and will report to this Body as required.
4. Membership
Dr Mohini Parmar – Chair, Ealing CCG Tessa Sandall – MD, Ealing CCG Dr Vijay Tailor – Governing body member, Ealing CCG Dr Raj Chandok – Governing body member, Ealing CCG Dr Shanker Vijayadeva – Governing body member, Ealing CCG Dr Maria Waters – Governing body member, Ealing CCG Fionnuala O’Donnell - Governing body member, Ealing CCG Sally Armstrong - Governing body member, Ealing CCG Carmel Cahill – Lay governing body member, Ealing CCG Adam Jenkins – Chair of Ealing, Hammersmith and Hounslow LMC Jane Betts – London Wide LMC representative Neha Unadkat – Deputy MD, Ealing CCG Catherine Williams – Interim Head of Primary Care, Ealing CCG Andrew Pike – Assistant Director of Comms & Engagement, Ealing CCG
Additional commissioning, local authority colleagues and service users may be co-opted as necessary to support the Steering Group in specific task and finish groups to complete individual outcomes. The Ealing PMS practices have been offered a position on this steering group but a representative has not yet been nominated. The wider Council of Members will also be offered a position on this steering group.
5. Meetings
The group will meet on a fortnightly basis. Frequency of these meetings may be varied on the direction of the chair.
Papers will be circulated one working day in advance of, and updated action logs one working days after, the meeting.
A meeting quorum is achieved with 50% of members in attendance.
Management and administrative support for the group will be provided by the Primary Care Project Manager.


















