EAACI Guidelines on Allergen Immunotherapy: allergic ... · 2 Allergic rhinoconjunctivitis (AR) is...
66
Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 1 EAACI Guidelines on Allergen Immunotherapy: allergic rhinoconjunctivitis 1 2 Draft 1.0; 12th May 2017 3 4 5 Short title: EAACI Rhinoconjunctivitis Allergen Immunotherapy Guidelines 6 7 Key words: allergen immunotherapy, allergy, allergic conjunctivitis, allergic rhinitis, 8 rhinoconjunctivitis 9 10 Abbreviations: 11 AR, allergic rhinoconjunctivitis; AIT, allergen immunotherapy; AGREE II, Appraisal of 12 Guidelines for Research & Evaluation; ARIA, Allergic Rhinitis and it Impact on Asthma; EPIT, 13 epicutaneous immunotherapy; EAACI, European Academy of Allergy and Clinical 14 Immunology; EMA, European Medicines Agency; HDM, house dust mite; ICER, incremental 15 cost-effectiveness ratio; NARES, non-allergic rhinitis with eosinophilia syndrome; QALY, 16 quality-adjusted life years; RCT, randomized controlled trial; SPT, skin prick test; SMD, 17 standardized mean difference; SCIT, subcutaneous immunotherapy; SLIT, sublingual 18 immunotherapy; SmPC, manufacturer‘s product information (SmPC), summary or product 19 characteristics. 20
Transcript of EAACI Guidelines on Allergen Immunotherapy: allergic ... · 2 Allergic rhinoconjunctivitis (AR) is...

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 1
EAACI Guidelines on Allergen Immunotherapy: allergic rhinoconjunctivitis 1
2
Draft 1.0; 12th May 2017 3
4
5
Short title: EAACI Rhinoconjunctivitis Allergen Immunotherapy Guidelines 6
7
Key words: allergen immunotherapy, allergy, allergic conjunctivitis, allergic rhinitis, 8
rhinoconjunctivitis 9
10
Abbreviations: 11
AR, allergic rhinoconjunctivitis; AIT, allergen immunotherapy; AGREE II, Appraisal of 12
Guidelines for Research & Evaluation; ARIA, Allergic Rhinitis and it Impact on Asthma; EPIT, 13
epicutaneous immunotherapy; EAACI, European Academy of Allergy and Clinical 14
Immunology; EMA, European Medicines Agency; HDM, house dust mite; ICER, incremental 15
cost-effectiveness ratio; NARES, non-allergic rhinitis with eosinophilia syndrome; QALY, 16
quality-adjusted life years; RCT, randomized controlled trial; SPT, skin prick test; SMD, 17
standardized mean difference; SCIT, subcutaneous immunotherapy; SLIT, sublingual 18
immunotherapy; SmPC, manufacturer‘s product information (SmPC), summary or product 19
characteristics. 20

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 2
ABSTRACT 1
Allergic rhinoconjunctivitis (AR) is an allergic disorder affecting the nose and eyes with a 2
prevalence of about 20% of the general population. Symptoms are frequently controlled with 3
avoidance measures and pharmacotherapy. However, many patients continue to have 4
ongoing symptoms and impaired quality of life. Allergen immunotherapy (AIT) represents an 5
important additional therapeutic option. These Guidelines have been prepared by the 6
European Academy of Allergy and Clinical Immunology’s (EAACI) Taskforce on AIT for AR 7
and are part of the EAACI presidential project ‘AIT Guidelines’. They aim to provide evidence-8
based clinical recommendations and have been informed by a formal systematic review and 9
meta-analysis. Their generation has followed the Appraisal of Guidelines for Research and 10
Evaluation (AGREE II) approach. The process included representation of the full range of 11
stakeholders. Key sections cover ‘general considerations before initiating AIT for AR’, ‘allergen 12
immunotherapy for AR: evidence-based, clinical recommendations’, ‘other approaches for 13
AIT’, ‘allergen factors that may affect the efficacy of AIT for AR’, ’patient factors that may affect 14
the efficacy of AIT for AR’, ‘how long should AIT be continued for in AR’, ‘adverse events with 15
ASIT for AR’, ‘preventive effects of AIT for AR’, ‘pharmacoeconomic aspects of AIT versus 16
pharmacotherapy for AR’ and ‘summary, gaps in the evidence and future perspectives’. In 17
general, broad evidence for the clinical efficacy of AIT exists but a product-specific evaluation 18
of evidence is recommended. 19
20

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 3
SECTION A: INTRODUCTION 1
Allergic rhinoconjunctivitis (AR) is an allergic disorder affecting the nose and eyes, resulting 2
in chronic, mostly eosinophilic, inflammation of the nasal mucosa and conjunctiva [Eifan 2016; 3
Greiner 2011]. Allergic rhinitis, with or without conjunctivitis, is one of the most prevalent 4
allergic diseases affecting around a fifth of the general population [Singh 2010; Meltzer 2009; 5
Ait-Khaled 2009]. It is associated with considerable loss of productivity and impaired school 6
performance [Walker 2007]. 7
AR can usually be diagnosed from its typical presentation (Figure A). Symptoms include 8
itching, sneezing, watery nasal discharge often nasal congestion [Roberts 2013]. There is 9
often associated eye symptoms (watery, red and/or itchy eyes). Symptoms may be described 10
as seasonal and/or perennial; as intermittent or persistent; or mild, moderate or severe 11
according to its impact on quality of life (Bousquet 2008). Symptoms are related to exposure 12
to the offending allergen as well as to non-specific triggers such as smoke, dust, viral 13
infections, strong odors and cold air [Roberts 2013]. Evidence of allergen-specific IgE 14
sensitization to one or more aeroallergens suggested by the history supports the diagnosis. 15
AR may co-exist with other forms of rhinitis (Figure A). Additionally, AR may be associated 16
with sinusitis symptoms, auditory dysfunction and asthma [Roberts 2013]. 17
The aims of AR management are to control symptoms and reduce inflammation. Where 18
possible, allergen avoidance can be recommended although effective allergen avoidance is 19
not always feasible [Terreehorst 2003; Sheikh A Cochrane review 2010]. Many patients rely 20
on pharmacotherapy with e.g., oral or topical antihistamines, intranasal corticosteroids, topical 21
cromoglycate or leukotriene receptor antagonists [Roberts 2013]. However, these therapies 22
do not alter the natural history of AR. Additionally, despite medication, a significant number of 23
patients continue to experience symptoms that impair their quality of life. Allergen 24
immunotherapy (AIT) that involves regular subcutaneous (SCIT) or sublingual (SLIT) 25
administration of the culprit allergen(s) may not only desensitize a patient thereby ameliorating 26
symptoms but also modify the underlying natural history of the disease [Pfaar 2014; Jutel 27
2015; Jutel 2016]. 28
These Guidelines have been prepared by the European Academy of Allergy and Clinical 29
Immunology’s (EAACI) Taskforce on Allergen Immunotherapy (AIT) for Rhinoconjunctivitis 30
and are part of the EAACI AIT Guidelines. These Guidelines aim to provide evidence-based 31
recommendations for the use of AIT for patients with allergic rhinitis with or without 32
conjunctivitis. AR will be used to signify either allergic rhinitis or allergic rhinoconjunctivitis. 33
The primary audience are clinical allergists, although the guidelines are of relevance to other 34
healthcare professionals (e.g. primary care workers, other specialist doctors, nurses and 35
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 4
pharmacists working across a range of clinical settings) dealing with AR. The development of 1
the Guidelines has been informed by a formal systematic review and meta-analysis of AIT for 2
AR [Dhami 2017], with systematic review principles being used to identify additional evidence, 3
where necessary. 4
5
6 7
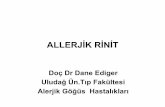
Figure A. Differential diagnosis of allergic rhinoconjunctivitis 8
Adapted from Roberts 2013. Local allergic rhinitis may be seen where there is only evidence 9
of local nasal allergic sensitization [Campo 2015; Carmen 2010]. There are numerous other 10
causes of non-allergic, non-infectious rhinitis, examples are non-allergic rhinitis with 11
eosinophilia syndrome (NARES) and gastro-oesophageal reflux [Roberts 2013]. In individual 12
patients, symptoms may be driven by more than one trigger. Rhinosinusitis is not included in 13
the scope of these Guidelines. 14

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 5
Box 1. Key terms
Rhinitis Inflammation of the nasal epithelium resulting in at least two nasal
symptoms: rhinorrhea, blockage, sneezing or itching.
Conjunctivitis Inflammation of the conjunctiva characterized by watery, itchy, red
eyes.
Sensitization Detectable allergen specific IgE antibodies, either by means of skin
prick test (SPT) or specific IgE antibodies in a blood sample
Allergen
immunotherapy (AIT) Repeated allergen administration at regular intervals to modulate
immune response in order to reduce symptoms and the need of
medication for clinical allergies and to prevent the development of new
allergies and asthma (adapted from European Medicines Agency
(EMA)). This is also sometimes known as allergen specific
immunotherapy, desensitization and hypo-sensitization
Subcutaneous
immunotherapy (SCIT) Form of allergen immunotherapy where the allergen is administered as
a series of subcutaneous injections.
Sublingual
immunotherapy (SLIT) Form of allergen immunotherapy where the allergen is administered
under the tongue.
Short-term efficacy Clinical benefit to the patient while they are receiving AIT
Long-term efficacy Clinical benefit to the patient for at least one year after cessation of the
AIT course. This implies that the AIT has altered the natural history of
the patient’s allergic disease.
1

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 6
SECTION B: METHODOLOGY 1
These Guidelines were produced using the Appraisal of Guidelines for Research & Evaluation 2
(AGREE II) approach [Agree Collaboration 2003; Brouwers 2010], a structured approach to 3
guideline production. This is designed to ensure appropriate representation of the full range 4
of stakeholders, a careful search for and critical appraisal of the relevant literature, a 5
systematic approach to the formulation and presentation of recommendations and steps to 6
ensure that the risk of bias is minimized at each step of the process. The process started in 7
April 2015 beginning with detailed face-to-face discussions agreeing the process and the key 8
clinical areas to address, followed by face-to-face meetings and regular web-conferences in 9
which professional and lay representatives participated. 10
11
Clarifying the scope and purpose of the guidelines 12
The scope of these EAACI Guidelines is multifaceted, providing statements that assist 13
clinicians in the optimal use of AIT in the management of patients with AR and identifying gaps 14
for further research. 15
16
Ensuring appropriate stakeholder involvement 17
Participants in the EAACI Taskforce on AIT for Allergic Rhinoconjunctivitis represented a 18
range of 16 countries and disciplinary and clinical backgrounds, including allergists, 19
paediatricians, primary care doctors, ophthalmology, ENT, pharmacists, immunologists, 20
nurses and patient representatives. Representatives of immunotherapy product manufactures 21
were given the opportunity to review and comment on the draft guidelines as part of the peer 22
review and public comment process. These comments were considered by the Taskforce and, 23
where appropriate, revisions were made. 24
25
Systematic reviews of the evidence 26
The initial full range of clinical questions that were considered important were rationalized 27
through several rounds of iteration to agree on one key question: what is the effectiveness, 28
cost-effectiveness and safety of AIT in patients with allergic rhinoconjunctivitis. This was then 29
pursued through a formal systematic review of the evidence [Dhami 2016; Dhami 2017]. 30
31
Formulating recommendations 32

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 7
We graded the strength and consistency of key findings from these systematic reviews (Dhami 1
2017) to formulate evidence-based recommendations for clinical care [Oxford Centre for 2
Evidence-based Medicine] (Box 2). This involved formulating clear recommendations with the 3
strength of evidence underpinning each recommendation. Where the systematic review did 4
not cover the clinical area, we took a hierarchical approach reviewing other evidence until we 5
could formulate a recommendation, i.e.: (i) other systematic reviews on the subject to see if 6
these provided any clarity on the topic; (ii) randomized controlled trials (RCTs) within these 7
systematic reviews; (iii) other RCTs known to Taskforce members; and (iv) a consensus-8
based approach. Recommendations apply to all ages unless otherwise indicated in the tables. 9
Experts identified the resource implications of implementing the recommendations, barriers, 10
and facilitators to the implementation of each recommendation, advice on approaches to 11
implementing the recommendations and suggested audit criteria that can help with assessing 12
organizational compliance with each recommendation (see Supporting Information Tables SX, 13
….) 14
15
Peer review and public comment 16
A draft of these guidelines was externally peer-reviewed by invited experts from a range of 17
organizations, countries, and professional backgrounds. Additionally, the draft guidelines were 18
made available on the EAACI Website for a 3 week period in May 2017 to allow a broader 19
array of stakeholders to comment. All feedback was considered by the Taskforce and, where 20
appropriate, final revisions were made in the light of the feedback received. We will be pleased 21
to continue to receive feedback on these Guidelines, which should be addressed to the 22
corresponding author. 23
24
Identification of evidence gaps 25
The process of developing these Guidelines has identified a number of evidence gaps which 26
are prioritized (see Online supplement). 27
28
Editorial independence and managing conflict of interests 29
The production of these Guidelines was funded and supported by EAACI. The funder did not 30
have any influence on the guideline production process, on its contents or on the decision to 31
publish. Taskforce members’ conflict of interests were declared at the start of the process and 32
taken into account by the Taskforce Chairs as recommendations were formulated. Final 33

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 8
decisions about strength of evidence for recommendations were checked by the 1
methodologists who had no conflict of interests in this area. 2
Updating the guidelines 3
EAACI plans to update these guidelines in 2022 unless there are important advances before 4
then. 5
6
7 8
9
Box 2: Assigning levels of evidence and recommendations [Oxford Centre for Evidence-based Medicine]
Level of evidence
Level I Systematic reviews, meta-analysis, randomized controlled trials
Level II Two groups, nonrandomized studies (e.g., cohort, case–control)
Level III One group nonrandomized (e.g., before and after, pretest, and post-test)
Level IV Descriptive studies that include analysis of outcomes (single-subject design, case series)
Level V Case reports and expert opinion that include narrative literature, reviews, and consensus statements
Grades of recommendation
Grade A Consistent level I studies
Grade B Consistent level II or III studies or extrapolations from level I studies
Grade C Level IV studies or extrapolations from level II or III studies
Grade D Level V evidence or troublingly inconsistent or inconclusive studies at any level
Strength of recommendations
Strong Evidence from studies at low risk of bias /high quality studies
Moderate Evidence from studies at moderate risk of bias /moderate quality studies
Weak Evidence from studies at high risk of bias /low quality studies
Recommendations are phrased according to the strength of recommendation: strong: “is recommended”; moderate: “can be recommended”; weak: “may be recommended in specific circumstances”; negative: “can not be recommended”.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 9
SECTION C: GENERAL CONSIDERATIONS BEFORE INITIATING AIT FOR AR 1
General indications 2
AIT is only indicated in the presence of symptoms strongly suggestive of allergic rhinitis, with 3
or without conjunctivitis (Table 1) [Dhami 2017]. Many patients will also have co-existing 4
asthma. There should be symptoms on aeroallergen exposure and evidence of IgE-5
sensitization (positive SPT or serum specific-IgE) to one or more clinically relevant allergens 6
[Dhami 2017]. Component resolved diagnostics may have a role in optimizing AIT therapy, 7
but definitive trials to show this approach enhances AIT outcomes are awaited. SPT or 8
specific-IgE results may not identify the important allergens, particularly in polysensitized 9
patients with perennial symptoms. In these circumstances, nasal or conjunctival provocation 10
testing may be helpful, but again there is no definitive evidence that this approach can optimize 11
the selection of the correct allergen for AIT therapy. For AIT to be indicated, a patient should 12
be experiencing moderate-to-severe symptoms (e.g. ARIA categories moderate-to-severe 13
intermittent or persistence [ARIA]), despite avoidance measures and optimal 14
pharmacotherapy, that interfere with their usual daily activities or sleep. AIT may also be 15
considered in less severe AR where a patient wishes to take advantage of its long term effect 16
on rhinitis and potential to prevent asthma [ref prevention guidelines]. Lastly, only AIT products 17
with evidence of efficacy for AR should be used (Pfaar et al. 2014; Bachert et al. 2015). The 18
approach to using AIT for AR across the healthcare system is summarized in Figure B. 19
20
Absolute and relative contraindications 21
Even when AIT is the suitable therapy for a patient with AR, there may be absolute 22
contraindications for its use (Table 2). There are also relative contraindications for 23
conditions/concomitant diseases, where the risks from AIT may outweigh the expected 24
benefits. 25
26 27 28 29
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 10
Table 1. General indications for AIT for AR
General indications Key references
Contextual considerations
AIT should be considered when all of these criteria are met:
has symptoms strongly suggestive of allergic rhinitis, with or without conjunctivitis
there is evidence of IgE-sensitization (positive SPT and / or serum specific-IgE) to one or more clinically relevant allergen
experiencing moderate-to-severe symptoms interfering with their usual daily activities or sleep despite regular and appropriate pharmacotherapy and / or avoidance strategies
Dhami 2017
A diagnosis of allergic rhinitis and evidence of IgE-sensitisation were entry criteria for RCTs in the systematic review.
AIT may also be considered in less severe AR where a patient wishes to take advantage of its long term effect on rhinitis and potential to prevent asthma
[ref prevention AIT guidelines]
AIT has the potential to alter the natural history of disease reducing AR symptoms after cessation of therapy and preventing the development of asthma.
Standardized AIT products with evidence of efficacy in the clinical documentation should preferably be used
Dhami 2017 These products have consistent formulations and so different batches are likely to have similar effects.
However, the systematic review reveals a considerable heterogeneity in effectiveness between products and therefore a product-specific evaluation of efficacy is demanded.
Formatted: English (United Kingdom)
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 11
Table 2. General contraindications for AIT for AR
Key references Contextual considerations
The following are considered to be contraindications:
Uncontrolled asthma Pitsios 2015; Cox 2011; Bousquet 1989; Lockey 2001 Bernstein 2004; CSM 1986; Normansell 2015; Calderon 2012
Weak evidence of risk from case reports or case series of adverse events with AIT. Taskforce considered that these were contraindications to AIT.
Active, systemic, autoimmune disorders
Cabrera 1993; Sánchez-Morillas 2005; Fiorillo 2011
Active malignant neoplasia Wöhrl 2011; Palomares 2010; Larenas-Linnemann 2016
AIT initiation during pregnancy Metzger 1978; Chaudhuri 2008]
With the following, AIT should only be used with caution when benefits outweigh potential risks in an individual patient:
Beta-blocker therapy Hiatt 1985; Matsumura 1976; Cleaveland 1972; Lang 1995
Weak evidence of risk. These may both compromise a patient’s ability to tolerate an episode of anaphylaxis; this must be considered when deciding whether AIT is appropriate.
Severe cardiovascular diseases, e.g. coronary artery disease
Linneberg 2012; Larenas-Linnemann 2016
Systemic autoimmune disorders in remission/organ specific (Eg autoimmune thyroiditis)
Pitsios 2015; Cox 2011; Walker 2011; Linneberg 2012; Larenas-Linnemann 2016
Weak evidence of risk from case reports or case series of adverse events with AIT. Taskforce considered that careful consideration and discussion with patient and the treating physician and a case-by-case decision is required before commencing AIT.
Severe psychiatric disorders Pitsios 2015
Poor adherence Pitsios 2015
Primary and secondary Immunodeficiencies
Pitsios 2015; Larenas-Linnemann 2016
ACE-inhibitors Epstein 2016

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 12
Figure B. Approach to using AIT for allergic rhinoconjunctivitis Schematic illustration of the approach to using AIT for AR starting with self-medication and management in primary care moving to assessment by an allergist for consideration and initiation of AIT in suitable patients. Structure of healthcare systems differs between countries.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 13
SECTION D: ALLERGEN IMMUNOTHERAPY FOR AR: EVIDENCE-BASED, 1
CLINICAL RECOMMENDATIONS 2
3
AIT is recommended for the treatment of AR in selected adults and children who respond 4
inadequately to regular treatment with anti-allergic drugs and/or experience 5
unacceptable side-effects with anti-allergic medication. This is based on pooled data 6
from an EAACI commissioned meta-analysis [Dhami 2017] of 58 studies of SCIT and 7
SLIT which found a standardized mean difference (SMD) of -0.53 (95% confidence 8
intervals (CI) -0.63, -0.42) for symptoms of rhinoconjunctivitis in favor of AIT compared 9
to placebo, consistent with a moderate clinical effect. This finding was also supported by 10
reductions in medication use (45 studies, SMD -0.37 [95%CI -0.49, -0.26] and also in 11
combined symptom-medication scores (15 studies, SMD -0.49 [95%CI -0.69, -0.30). The 12
high grade of heterogeneity between the trials evaluated underlines the urgent need of 13
an individual product-based evaluation of the evidence for efficacy (Pfaar et al. 2014; 14
Bachert et al. 2015). 15
However, SCIT immunotherapy is in general recommended for the treatment of AR in 16
adults and children with moderate-to severe disease that is sub-optimally controlled 17
despite optimum pharmacotherapy [Dhami 2017](Table 3). The evidence for short-term 18
benefit is stronger for seasonal rhinitis (Grade A for adults) than for perennial rhinitis 19
(Grade B for adults), where few studies have been performed and results are more 20
heterogeneous (Table 3). SCIT is recommended for seasonal disease whether given 21
continuously or pre- or pre/co-seasonally (Table 3, Grades A or B for adults). Pre/co-22
seasonal therapy benefits from a shorter course of treatment; the two regimens have not 23
been directly compared in terms of efficacy or adverse events. 24
SCIT may be administered in aqueous formulation (rarely in Europe) or as a depot 25
adsorbed on aluminum hydroxide or tyroxine. SCIT using either unmodified or modified 26
allergen extracts is recommended for treatment of allergic rhinitis and provides short-27
term benefit (Table 3, Grade A for adults). This is based on evidence from the systematic 28
review [Dhami 2017] that showed both unmodified allergen extracts (SMD [95%CI]) -29
0.65 (-0.93, -0.36) and allergoids/polymerized extracts (SMD [95%CI] -0.60 [-0.89, -0.31] 30
to be effective in reducing symptoms compared to placebo, with additional support from 31
reduced medication requirements and combined symptom-medication scores. Although 32
clinical trials of modified allergens involved shorter courses of treatment, there have been 33
no head-to-head comparisons with unmodified preparations evaluating efficacy or 34
adverse events. 35

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 14
Grass pollen SCIT is recommended (Grade A in adults) to be given for a minimum of 1
three years in order to achieve long-term clinical efficacy following discontinuation of 2
treatment (Table 7). This is supported by three RCTs of continuous treatment with the 3
same aluminum hydroxide-adsorbed allergen extract, two in adults [Durham 1999, 4
James 2011] and one in children [Jacobsen L Allergy 2007]. 5
In general, SLIT is recommended for the treatment of seasonal allergic rhinitis in adults 6
and children. SLIT has been shown to provide short term benefit during therapy with 7
moderate-to severe disease that is sub-optimally controlled despite optimum 8
pharmacotherapy (Table 3) [Dhami 2017]. SLIT is recommended to be taken either 9
continuously or pre-/co-seasonally commencing a minimum of two months and ideally 10
four months prior to the start of the pollen season (Grade A for adults). 11
SLIT may be taken daily either as drops or as tablets that are retained under the tongue 12
for at least one minute and then swallowed. Both are recommended (Grade A or B for 13
adults) based on short-term reductions in symptoms and rescue medication, 14
respectively, for sublingual drops: SMD (95%CIs) -0.41 (-0.65, -0.18) and -0.35 (-0.55, -15
0.14) and for sublingual tablets: -0.56 (-0.80, - 0.33) and -0.42 (-0.64, -0.19) [Dhami 16
2017]. 17
Grass pollen SLIT is recommended (Grade A) to be taken for a minimum of three years 18
in order to provide long-term benefit for at least two years after discontinuation (Table 7). 19
This recommendation is based on four large RCTs [Durham 2012, Didier Clin Trans 20
Allergy 2015, Ott 2009, Valovirta Clin Ther. 2011] (Table 3). This recommendation is 21
further supported by a recent trial that showed that both subcutaneous and sublingual 22
immunotherapy were effective whereas two years treatment was insufficient for long-23
term clinical efficacy after discontinutaion, reinforcing the need for immunotherapy via 24
both routes to be continued for at least 3 years (Scadding GW 2017). 25
Sublingual house dust mite tablet immunotherapy for at least one year is recommended 26
(Grade A) for the short-term treatment of perennial HDM AR in adults [Didier 2015, 27
Durham 2012, Ott 2009, Bergmann 2014, Mosbech 2015, Demoly 2016](Table 3). In one 28
trial of one year of sublingual HDM tablet treatment [Bergman 2013], short-term benefit 29
was followed by reduced symptoms assessed at one year after discontinuation. 30
Where RCTs involving increasing allergen concentrations have been performed there 31
has been clear evidence of a dose-response relationship for both SCIT and SLIT. While 32
higher doses are more effective, they are associated with more side-effects, such that 33
dose selection has been based on a balance of efficacy and side-effects [Didier 2015, 34
Durham 2012, Valovirta 2006, Frew 2006, Jacobsen L Allergy 2007; Calderon 2011]. 35

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 15
Table 3 Recommendations: AIT for treatment of AR: schedules, products, formulations
Recommendation Adults Children and adolescents
Strength of
recommendation Other considerations Key references
E
vid
en
ce l
evel
Gra
de o
f
reco
mm
en
dati
on
Evid
en
ce l
evel
Gra
de o
f
reco
mm
en
dati
on
SCIT
Continuous SCIT is recommended for seasonal AR for short-term benefit in those with moderate-to severe disease
I A I B Strong recommendations for adults based on high quality studies (eg Varney 1991, Walker 2001, Charpin 2007, Ferrer 2005). Moderate recommendation for children as minimal moderate quality studies reporting solely paediatric data (Roberts 2006).
Consistent, moderate-high effect size and low risk of severe systemic allergic side-effects. Most studies reported pediatric and adult data together.
Dhami 2017 SR, eg Adult: Frew 2006, Varney 1991, Walker 2001, Charpin 2007, Ferrer 2005, Dolz 1996, Scadding GW 2017 Paediatric: Roberts 2006
Continuous SCIT is recommended for perennial AR due to house dust mites for short-term benefit
I B I C Strong recommendation for adults based on high quality studies (Tabar 2005, Varney 2003, Dokic 2005). Weak recommendation for children as no exclusive pediatric data.
Moderate effect size, few small adult studies, considerable heterogeneity and risk of systemic allergic side-effects.
Dhami 2017 SR, eg Adult: Tabar 2005, Varney 2003, Dokic 2005, Ewan 1988
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 16
Pre- and pre-/co-seasonal SCIT is recommended for seasonal AR for short-term benefit
I A I B Strong recommendation for adults based on high quality studies (Balda 1998, Bodtger 2002, Varney 1991, Zenner 1997). Moderate recommendation for children as only combined adult/pediatric data of high (Weyer 1981) and unclear (Bousquet 1990) quality.
Consistent, moderate-high effect size in adult studies; low risk of severe systemic allergic side-effects.
Dhami 2017 SR, eg Adult: Balda 1998, Bodtger 2002, Bousquet 1990, Frew 2006, Jutel 2005, Varney 1991 Zenner 1997 Adult/paed: Bousquet 1990, Weyer 1981, Scadding GW JAMA 2017.
Both modified (allergoids) and unmodified allergen extracts are recommended for AR for short-term benefit
I A I B Strong recommendation for adults based on high quality studies for both modified (Brunet 1992, Zenner 1997, Charpin 2007, Dokic 2005, Klimek, 2005) and non-modified (Balda 1998, Bodtger 2002, Charpin 2007, Ortolani 1994, Tabar 2008, Varney 1991, Varney 2003, Walker 2001, Weyer 1981, Zenner 1997) allergen extracts. Weak recommendation for children as no exclusive pediatric data.
Consistent, moderate-high effect size in adult studies; low risk of severe systemic allergic side effects. No exclusive pediatric data.
Dhami 2017 SR, eg Modified: Bousquet 1990, Brunet 1992, Zenner 1997, Charpin 2007, Corrigan 2005, Dokic 2005, Klimek, 2005 Non-modified: Balda 1998, Bodtger 2002, Charpin 2007, Frew 2006, Jutel 2005, Ortolani 1994, Tabar 2008, Varney 1991, Varney 2003, Walker 2001, Weyer 1981, Zenner 1997,Scadding GW JAMA 2017
Continuous grass pollen SCIT is recommended for AR for short and long-term benefit
I A I B Strong recommendation for adults based on above evidence plus two high quality long-term studies (Durham 1999, James 2011). Weak recommendation for children as only one low quality (open design) paediatric long-term study (Jacobsen 2007).
A few adult studies and one pediatric study (designed to assess whether SCIT prevents asthma) demonstrating long-term effectiveness.
Dhami 2017 SR, eg Adult: Durham 1999, James 2011 Paed: Jacobsen L Allergy 2007 H

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 17
SLIT
Pre-/co-seasonal SLIT is recommended for seasonal ARs for short-term benefit
I A I A Strong recommendation based on high quality adult (Dahl 2006a, Dahl 2006b, Durham 2006 L) and paediatric (Caffarelli, 2000, Pajno, 2003 L, Stelmach, 2012) studies.
Consistent, moderate effect size; low risk of severe systemic allergic side-effects.
Dhami 2017 SR, eg Adult: Creticos 2013, Dahl 2006a, Dahl 2006b, Didier 2007, Durham 2006, Hordijk 1998, Palma-Carlos 2006 Paediatric: Caffarelli, 2000, Halken 2010. Pajno, 2003, Stelmach, 2012
Continuous SLIT can be recommended for seasonal AR for short-term benefit
I A I B Moderate-to-strong recommendation based on high (Amar 2009) and low (Ariano 2001, Panzner 2008) quality adult studies plus moderate (Bufe 2004) and unclear (Valovirta 2006) quality paediatric studies.
Moderate effect size; some heterogeneity between studies particularly paediatric ones, low risk of severe systemic allergic side effects.
Dhami 2017 SR, eg Adult: Amar 2009, Ariano, 2001, Panzner, 2008 Paed: Valovirta 2006, Bufe 2004
SLIT with aqueous solutions can be recommended for AR for short-term benefit.
I B I A Moderate recommendation for adults based on a mixture of high (Feliziani 1995), low (Ariano 2001, Bowen 2004, Tari 1990) and unclear (Guez 2000, Hordijk 1998) quality studies. Strong recommendation for pediatrics based on high quality studies (Pajno 2003, Stelmach, 2012).
Moderate effect size, some heterogeneity between adult studies, low risk of severe systemic allergic side-effects.
Dhami 2017 SR, eg Adult: Ariano 2001, Bowen 2004, Feliziani 1995, Guez 2000, Hordijk 1998, Tari 1990 Paed: Pajno 2003, Wahn 2009, Stelmach, 2012

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 18
SLIT with tablets is recommend for AR for short-term benefit.
I A I A Strong recommendation based on high quality adult (Dahl 2006a, Dahl 2006b, Durham 2006, Nolte 2016) and paediatric (Bufe 2009, Caffarelli 2000, Wahn 2009) studies.
Moderate effect size; little heterogeneity between studies, low risk of severe systemic allergic side effects.
Dhami 2017 SR, eg Adult: Dahl 2006a, Dahl 2006b, Durham 2006, Horak 2009, Passalacqua 2006 Paed: Bufe 2009, Caffarelli 2000 Wahn 2009 Scadding GW JAMA 2017, Nolte 2016
Grass pollen SLIT tablets or solution is recommended for allergic rhinoconjunctivitis for long-term benefit.
I A I B Strong recommendation for adults based on high quality studies (Durham 2012, Didier Clin Trans Allergy 2015, Ott 2009). One high quality paediatric study with results only available online on EudraCT(Valovirta Clin Ther. 2011)
Consistent moderate effect size up to 2 years after cessation in adults. One paediatric study (designed to look at prevention of asthma) indicates the same, but full publication is pending.
Dhami 2017 SR, eg Adult: Durham 2012, Didier Clin Trans Allergy 2015, Ott 2009 Paediatric: Valovirta Clin Ther. 2011
HDM SLIT tablet can be recommended for allergic rhinoconjunctivitis for long-term benefit.
I B - C Moderate recommendation based on one large, high quality (Bergmann 2014). No paediatric data.
One study demonstrates effectiveness for a year post-treatment. No paediatric data.
Bergmann 2013
Continuous: year round therapy. Pre-seasonal: before a pollen season. Co-seasonal: during a pollen season. Not all AIT preparations are
licensed for children and adolescents.
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 19
SECTION E: Other approaches for AIT 1
2 Other approaches aim to improve patient convenience and compliance with shorter 3
courses, whilst improving or maintaining efficacy and reducing the risk of systemic side 4
effects (Table 4). As such, adjuvants to AIT extracts are possible candidates (Pfaar et 5
al. 2012). For example, TLR-4 agonists (monophosphoryly lipid A) in combination with a 6
grass allergoid has demonstrated effectiveness, although in a phase 3 trial, efficacy was 7
modest and there are no head to head comparisons [Drachenberg 2001]. The TLR-9 8
agonist (Bacterial DNA oligonucleotides containing a CpG motif) fused to Amb a 1, the 9
major allergen of ragweed showed efficacy in a phase 2 trial [Creticos 2006] although 10
this was not observed in a subsequent phase 3 trial. The combination of anti-IgE 11
injections with conventional and rush AIT with non-modified extracts has been proved to 12
be effective with a marked reduction in systemic side-effects in studies of children 13
[Rolinck-Werninghaus 2004] and adults [Casale 2006], although it is expensive and there 14
is concern when and how to discontinue the anti-IgE when AIT maintenance therapy is 15
achieved [Larenas Linnemann 2014]. 16
Recombinant AIT is attractive as it allows accurate standardization of allergen products 17
and has potential for personalized therapy based on individual allergen sensitivities, and 18
with a hypothetical lower risk of inducing new sensitizations. Subcutaneous recombinant 19
birch (Bet v 1) [Pauli 2008] and a 5- recombinant grass allergen mix [Jutel 2005] have 20
been shown to be efficacious with no safety concerns. A recombinant B cell epitope-21
based vaccine, comprising a recombinant hybrid grass allergen mix combined with a 22
hepatitis B domain surface Pre-S protein as an immunologic carrier has shown efficacy 23
in a phase 2 trial [Zieglmayer 2016]. T cell peptide immunotherapy for cat allergy using 24
mixtures of short T cell epitopes via the intradermal route, had promising results in 25
environmental chamber phase 2 studies [Patel 2013]; it has been reported that a 26
subsequent phase 3 study did not demonstrate effectiveness. Studies with other allergen 27
peptide approaches are in progress [Ellis 2017; Spertini 2016]. 28
There has been recent interest in the use of alternative modalities of delivery including 29
the epicutaneous, intradermal and intra-lymphatic routes. In RCTs, epicutaneous grass 30
pollen immunotherapy (EPIT) has shown modest benefit [Senti 2012] although 31
accompanied by local eczematous reactions at the patch application site. Intradermal 32
grass pollen immunotherapy inhibited allergen-induced cutaneous late responses 33
although in a subsequent RCT it was ineffective and there was evidence of exacerbation 34
of seasonal outcomes and Th2 inflammation in the skin [Slovick JACI 2017]. The intra-35

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 20
lymphatic route, using a grass pollen extract and a modified cat allergen extract, showed 1
efficacy in some trials [Senti 2012, Patterson, A] but not in others [Witten 2013]. 2
3

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 21
Table 4 Recommendations: other approaches for AIT for treatment of AR
Recommendation Adults Children and adolescents
Strength of recommendation Other considerations Key references
Evid
en
ce l
evel
Gra
de o
f
reco
mm
en
dati
on
Evid
en
ce l
evel
Gra
de o
f
reco
mm
en
dati
on
A combination of the TLR-4 agonist monophosphoryly lipid A with pollen allergoid is recommended for AR
I B III C Strong recommendation for adults based on one high quality study (Drachenberg 2001). Weak recommendation for children (Drachenberg 2003).
Moderate effect size, limited randomised controlled data. Only one uncontrolled before and after study paediatric study.
Drachenberg 2001, Drachenberg 2003
Combining anti-IgE injections with AIT for AR is recommended for reducing side-effects
I A I A Strong recommendation based on one high quality adult (Casale 2006) and one high quality paediatric (Rolinck-Werninghaus 2004) study.
Strong consistent evidence but the required length of co-therapy unclear.
Casale 2006, Rolinck-Werninghaus 2004
Recombinant AIT may be recommended for birch and grass pollen allergy
I A - B Quality of studies unclear (Pauli 2008; Jutel 2005).
Some evidence of benefit for adults, no pediatric data.
Pauli 2008; Jutel 2005

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 22
SECTION F: ALLERGEN FACTORS THAT MAY AFFECT THE EFFICACY OF AIT 1
for AR 2
3
Standardization of allergen extracts 4
For the common allergens, many companies now provide characterized, standardized, 5
stable preparation for AIT as recommended by European Medicines Agency (EMA) 6
[EMA 2008, regulatory position paper]. For others, such as molds, there are problems 7
with the complexity, variability and stability of the allergens [Coop 2014]. The lack of 8
standardized extracts may hamper the diagnosis of eligible patients for AIT and may 9
impede the effectiveness of AIT [Coop 2014, Twaroch 2015]. Additionally, non-10
standardized preparations may vary between batches increasing the potential for side 11
effects. Further purification and characterization of such allergens [Twaroch 2015, Lizaso 12
2006, Slater 2014] may result in better extracts for the future. Where possible, 13
standardized allergen products should be used for AIT. Further discussion is available 14
in a position paper on regulatory aspects of AIT [regulatory position paper]. 15
Formulation of SLIT preparations 16
In deciding on the appropriate preparation to use for AIT, the formulation should be taken 17
into account. For example, three large studies have showed efficacy for HDM SLIT 18
tablets [Bergmann 2014, Demoly 2016, Mosbech 2014] whereas three HDM SLIT 19
studies with sublingual drops were negative [Bahçeciler, 2007, Guez, 2000, Hirsch, 20
1997], and another only demonstrated efficacy in the first and not the second year 21
[Passalacqua 2006]. However, many factors such as differences in allergen content, 22
administered volume, number of participants and statistical power of the study may 23
explain the differences between tablets and drops. We recommend that AIT products 24
with evidence of efficacy in the clinical documentation should preferentially be used. 25
Allergen mixtures 26
Both mixtures of grass pollen and mixtures of tree pollen are frequently used in AIT and 27
such an approach is effective [Dhami 2017]. The use of different, non-taxonomically 28
related allergens mixed in one AIT product has been evaluated in a very limited number 29
of studies. One SCIT study showed that a depigmented-polymerized mixed grass/birch 30
pollen extract was effective over placebo [Pfaar 2013]. A small study in children 31
demonstrated efficacy using a mixture of grass pollen and HDM SLIT [Swaney 2012]. 32
One study assessed the efficacy of multi-inhalant allergen subcutaneous AIT (tree, grass 33

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 23
and weed pollen; moulds; cat and dog dander; dust and storage mites), it demonstrated 1
no efficacy over placebo [Radcliffe 2003]. Sublingual immunotherapy that employed a 2
momomeric Phleum pratense grass pollen extract was more effective when given alone 3
compared to when given in an equivalent dose as part of a combination with a 9-pollen 4
multi-allergen sublingual extract [Amar 2009]. 5
There are a number of potential drawbacks of mixing allergens including a dilutional 6
effect, potential allergen degradation due to enzymatic activity of some allergens and the 7
difficulties of adequately demonstrating efficacy of a high number of allergen 8
combinations and/or different products. The European Medicines Agency has 9
recommended that only homologous allergens (usually ones that are taxonomically 10
related, for example a mixture of grass pollen extracts [Didier A JACI 2006]) should be 11
mixed and that allergens with enzymatic activity (e.g. HDM) should be never used in a 12
mixture [EMA-AIT GL 2008]. We therefore recommend only homologous allergens to be 13
mixed in AIT preparations until further evidence is available substantiating the efficacy 14
of other mixtures (see Online supplement). Alternatively, extracts should be given 15
separately. 16
17
Specific allergens 18
In the recent meta-analysis, there were sufficient SCIT and SLIT studies for subgroup 19
analyses by specific allergens (Dhami 2017). Short-term effectiveness was 20
demonstrated for HDM (symptoms score SMD -0.73; 95%CI -1.37, -0.10), grass pollen 21
(-0.45; -0.54,-0.36); tree pollen (-0.57; -0.92, -0.21) and weed pollen (-0.68; -1.06, -0.30). 22
However, there was lots of heterogeneity for all allergens, particularly molds (-0.56; -23
2.29, 1.18), suggesting that different preparations may be more or less effective. 24

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 24
Table 5 Recommendations: allergen factors that affect the efficacy of AIT for AR
Recommendation Adults Children and Adolescents
Strength of recommendation Other considerations Key references
Evid
en
ce l
evel
Gra
de o
f
reco
mm
en
dati
on
Evid
en
ce l
evel
Gra
de o
f
reco
mm
en
dati
on
Either a single allergen or a mixture of well documented homologous allergens from that biological family that covers the major allergens are recommended for patients with AR who are allergic to grass pollens, tree pollens or HDM
I B I B Strong recommendations on basis of high quality grass pollen (single grass, eg Bufe 2009, Dahl 2006a; mixture of grasses, eg Didier 2007, Ott 2009), tree pollen (single tree, eg Bodtger 2002 Charpin 2007; mixture of trees, eg Balda 1998) and house dust mite (single, eg De Bot 2011, Hirsch, 1997; mixture, eg Passalacqua 1998) studies.
Strong RCT evidence that these are effective approaches. Supported by regulators.
Dhami 2017, Demoly 2016, EMA 2008
Mixtures of allergens from non-related biological families are not recommended as AIT preparations except for products with supportive published evidence
I B - B Strong recommendation based on a negative high quality study with multiple allergens (Radcliffe 2003). One positive high quality study combining grass and tree pollens (Pfaar 2013).
No evidence of effectiveness for almost all mixtures.
EMA 2008, regulatory position paper. Radcliffe 2003, Pfaar 2013
Examples of homologous, taxonomically related allergens from the same biological family are the grasses or tree pollens. Also see Table 3.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 25
SECTION G: PATIENT FACTORS THAT EFFECT THE EFFICACY OF AIT FOR AR
Polysensitized patients
Epidemiological data indicate that most patients with AR are polysensitized [Migueres et al.
2014]. Consequently, consideration needs to be given as to whether patients are (i) clinically
mono-allergic (where only one allergen is driving symptoms) and polysensitised or (ii) poly-
allergic (with clear cut symptoms on exposure to multiple different allergens) and
polysensitised. This may be apparent from the history or may need investigation with
component resolved diagnostics or assessment with nasal or conjunctival provocation
challenges [Demoly 2016]. Immunotherapy with a single allergen extract is effective in the
former while immunotherapy has been shown to be ineffective (Adkinson F jr NEJM) or less
effective in the later situation (Amirr/Nelson JACI).
For a poly-sensitized patient who is poly-allergic for homologous (biologically related) allergens
(e.g. two grass pollens), a single allergen preparation or a mixture of two homologous allergens
is recommended [Demoly 2016]. For polysensitized patients where allergens are not
homologous, separate AIT preparations for one or two of the clinically most important allergens
are recommended with doses given 30-60 minutes apart at separate locations when two are
selected [Demoly 2016; Calderon 2012. This represents a trade-off between efficacy and
safety as both are dose-dependent.
Co-existing asthma
Uncontrolled or poorly controlled asthma is considered to be an absolute contraindication to
AIT [Pitsios 2015; Cox 2011; Bousquet 1989; Lockey 2001 Bernstein 2004; CSM 1986;
Normansell 2015]. Studies that have assessed the impact of co-existing asthma on the efficacy
of AIT [Bufe 2004] have reported no effect.. Co-existing asthma is seen in many participants
in the published AR studies [Dhami 2017]. When controlled, mild-to-moderate asthma does
not seem to be a safety issue with AIT [Dhami 2017; Virchow 2016; Asthma AIT guidelines;
Pfaar et al. 2014].
Specific pediatric issues
Similarly to adults, AIT should be considered in pediatric patients with AR with evidence of
IgE-sensitization to clinically relevant allergens (Table 1, 3).

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 26
The evidence for the efficacy of AIT for AR is limited in children younger than five years of
age. Some clinical studies have shown the efficacy and safety of both SCIT and SLIT in
preschool children (Pajno 2012; Shao 2014; Fiocchi 2005; Agostinis 2005; Roberts 2006),
and children were included from four years onward in several of the big SLIT trials (Bufe
2009, Wahn 2009). However, repeated injections of SCIT can be traumatic in small children
[Pajno 2013; Arroabarren 2015]. The decision to start the treatment has to be taken on a
case by case basis together with the patients and their family. It depends on several factors,
such as the severity of the allergic disease, the clear exposure-symptoms pattern supported
by allergic sensitisation testing, the impairment of the health related quality of life and the
expected acceptance and adherence to the AIT.
There are more data to drive recommendations for school age children and adolescents
although major gaps still exist (Table 3). Many of the SCIT trials are now relatively old, many
enrolled a few children or do not present pediatric only analyses. Continuous and pre- and
pre/co-seasonal SCIT can be recommended (Grade B) for children with seasonal AR (Table
3). Continuous SCIT is also recommended for perennial AR, but with a weaker evidence
grade due to the inconsistency in the trial data (Grade C)(Table 3). There are no exclusive
pediatric data for allergoid preparations. One open RCT suggests that SCIT for grass pollen
driven AR does have a long-term benefit [Jacobsen L Allergy 2007]. For SLIT, there are
recent pediatric trial data to support this approach. In general, pre-co-seasonal SLIT is
recommended for seasonal AR (Grade A). For continuous SLIT, the results are more
heterogeneous, probably because of the products used (Grade B) (Table 3). Both tablet
and aqueous formulations are recommended although there is more heterogeneity in
results with the latter (Table 3). There is now one unpublished trial supporting the long-term
effectiveness for the grass pollen tablet and reduction in asthma synmptoms [Valovirta Clin
Ther. 2011](Grade B), there are no similar evidence for the aqueous preparations nor the
HDM tablet.
Elderly
A detailed allergy history is especially important when evaluating older adults suffering with
rhinitis as other types of rhinitis that may mimic AR symptoms. There are very few studies
specifically evaluating the use of AIT in the elderly but SLIT with grass pollen and HDM has
been demonstrated to be effective and safe in two studies [Bozek 2014 and 2016]. AIT elicits
responses comparable to studies with younger patients. Another important considerations in

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 27
this age group, when contemplating treatment with AIT, is the higher prevalence of
comorbidities. Examples are hypertension, coronary artery disease, cerebrovascular disease,
and/or cardiac arrhythmias. Also, treatment with medication such as beta-blockers that may
impair the treatment of anaphylaxis with adrenaline (epinephrine) (see Box 2).
Pregnancy
There is one prospective study investigating the safety of AIT in pregnancy [Shaikh 2012] and
several retrospective studies suggest that there is no greater risk of prematurity, fetal
abnormality, or other adverse pregnancy outcome in women who receive AIT during
pregnancy [Metzger 1978]. Observations about anaphylaxis in pregnant and breastfeeding
women are largely derived from case reports [Chaudhuri 2008] and are generally reassuring
[Oykhman 2015]. However, the balance between benefits and potential risks in pregnant
patients changes, these should be discussed with the patient. AIT takes months to work, but
systemic reactions and their resultant treatment can potentially harm the baby and/or mother.
It is therefore recommended that AIT is not initiated during pregnancy but, if already initiated,
AIT may be continued during pregnancy or breastfeeding in consultation with the patient’s
general practitioner and obstetrician if former AIT treatment has always been tolerated well.
Adherence
There is a great variance between studies (both real life studies and clinical trials) in the criteria
used for evaluating compliance and in the rates of compliance [Incorvaria-- Incorvaia 2010;
Scurati 2010; Egert-Schmidt 2014; Keil JACI 2013, Vaswani 2015; Leader 2016; Savi 2013].
The range of reported compliance varied from 18% to over 90%, higher in clinical studies than
real-life surveys. The main causes for poor adherence are reported to be side effects,
inconvenience, lack of efficacy or forgetting to use [Incorvaria-- Incorvaia 2010; Scurati 2010;
Egert-Schmidt 2014; Vaswani 2015; Leader 2016; Makatsori M 2014]. A few other factors have
been associated with poor adherence, for example age and patient’s educational level.
Potential ways to improve adherence are the use of reminder mechanisms (e.g. alarm on
mobile phone, internet based tools, service (SMS) electronic reminders, social networks,
mobile applications (apps) and monitoring systems – the approach should be tailored to the
patient), approaches to improving patient-doctor communication and patient education [Savi
2013; Demoly 2016]. One randomized study suggests that adherence is much better with 3

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 28
monthly follow up appointments compared to 6 or 12 monthly follow up [Vita 2010].
Recommendations are summarized in Table 6.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 29
Table 6: Recommendations: patient factors that affect the efficacy of AIT for AR
Recommendation Evidence level
Grade of recommendation
Strength of recommendation
Other considerations Key references
Polysensitized patients
Polysensitized patients who are mono-allergic are recommended to receive AIT for the specific allergen that is driving their AR symptoms
I A Based on expert review of RCT and observational data plus clinical experience.
Demoly 2016, Kim 2006
Polysensitized patients who are poly-allergic for taxonomically related homologous allergens can be recommended to receive either a single allergen or a mixture of homologous allergens from that biological family that covers all the major allergens
II B Based on expert review of RCT and observational data plus clinical experience.
Demoly 2016, EMA advice.
Patients who are poly-allergic for non-homologous allergens may be recommended to start AIT with either the allergen responsible for most of their allergic rhinoconjunctivitis symptoms or separate treatment with the two clinically most important allergens
II C Based on expert review of RCT and observational data plus clinical experience.
Demoly 2016, EMA advice; Radcliffe 2003, Kim 2006, Pfaar 2013.
.Co-existing asthma
Controlled asthma is not a contraindication to AIT I A Strong recommendation based on high quality studies (asthma AIT SR)
Evidence described in asthma AIT systematic review.
Dhami 2017; Virchow 2016; Asthma AIT SR and asthma AIT guidelines
Specific pediatric issues

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 30
Consideration of AIT is recommended in pediatric patients with AR with evidence of IgE-sensitization to clinically relevant allergens
I A Strong recommendations from high quality studies (eg Caffarelli 2000, Pajno 2003, Stelmach 2012, Bufe 2009, Caffarelli 2000)
See Table 3 for detailed review.
Caffarelli 2000, Pajno 2003, Stelmach 2012, Bufe 2009, Caffarelli 2000
In children aged less than 5 years of age, it is recommended that consideration should be given to likely benefits and risks associated with AIT for AR
IV D May be more difficult to make a definitive diagnosis of AR in pre-school children. Safety seems to be similar in this age group as per older patients.
Rodriguez-Santos 2008; Rienzo VD 2005
Elderly
AIT can be recommended in otherwise healthy elderly patients with AR whose symptoms cannot be adequately controlled by pharmacotherapy
I A (SCIT), B (SLIT) Moderate to strong recommendation based on one high quality SCIT study (Bozek 2016) and two SLIT studies of unclear quality (Bozek 2014, Bozek 2012).
Consistent RCT data for SLIT, only one SCIT study. Also see Table 2. A detailed clinical assessment is recommended as other types of rhinitis may mimic allergic rhinitis in older patients.
Bozek 2012, 2014, 2016
Pregnancy
If patients have not started AIT and are pregnant, it is recommended to wait until after pregnancy to initiate therapy
V D Based on balance of additional risk versus benefits.
Expert opinion
If have commenced AIT and still in up-dosing phase, it may be recommended that the current dose is continued and up-dosing is resumed when pregnancy is completed
IV C Based on observational data.
Metzger 1978

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 31
If on maintenance AIT, it may be recommended that the current dose is continued
III C Weak recommendation based on propsective cohort study [Shaikh 2012]
Expert opinion
Adherence
It is recommended that patients understands about how AIT works and the need to take regular doses
II B Based on observational data.
Savi 2013
It may be recommended that patients use reminders to maximize adherence with SLIT therapy
V D Based on observational data.
Savi 2013, Demoly 2016
It can be recommended that patients on SLIT are followed up every 3 months to maximize adherence
I B Moderate recommendation based on a pseudo-randomized study (Vita 2010).
Vita 2010
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 32
SECTION H: HOW LONG SHOULD AIT BE CONTINUED FOR IN AR? 1
2
Most clinical studies evaluating the efficacy of AIT follow participants for one or two years 3
on therapy. The EMA currently recommends an experimental, randomized, controlled 4
design involving three years of therapy with a two year follow up period off treatment. 5
These studies demonstrate a sustained benefit for SLIT grass pollen therapy for two 6
years off therapy for one tablet [Durham 2010], for one year off for another tablet [Didier 7
2015] and for one year off drops [Ott 2009]. There are some data to suggest that HDM 8
SLIT drops gives sustained benefit for at least one year after three years of therapy in 9
one RCT [Lin 2016] and another observational one [Stelmach 2012]. There is less 10
evidence on the optimal duration of therapy. In a randomized cessation of therapy study, 11
participants who stopped therapy after 3 or 4 years of grass pollen SCIT did as well three 12
years later as participants who continued therapy [Durham 1999]. Similarly, children 13
randomized to 3 or 5 years HDM SCIT had similar outcomes at five years [Arroabarren 14
2015] as did adults randomized to 3 years of ragweed SCIT [Naclerio 1997]. A recent 15
study of grass pollen allergic patients showed that two years treatment with either SCIT 16
or SLIT tablets were effective compared to placebo whereas two years was insufficient 17
for long-term efficacy that was measured at 3 years, one year off treatment (Scadding 18
GW 2017). So for patients with AR a minimum of three years of immunotherapy is 19
recommended in order to achieve long-term efficacy after treatment discontinuation 20
(Table 7). 21
22

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 33
Table 7. Recommendations: How long should AIT for allergic rhinoconjunctivitis be continued?
Recommendation Evidence
level Grade of recommendation
Strength of recommendation Contextual comments
Key references
AIT is recommended as efficacy is seen from the first year of therapy
I A Strong recommendation based on high quality studies (eg Balda 1998, Bergmann 2013, Bousquet 1990, Didier Clin Trans Allergy 2015, Zenner 1997)
Generally consistent data.
Dhami 2017, Bergmann 2013, Didier Clin Trans Allergy 2015
To achieve long-term efficacy, it is recommended that a minimum of 3 years of therapy is used
I A Strong recommendation based on high quality longterm adult studies (Durham 1999, James 2011, Durham 2012, Didier Clin Trans Allergy 2015, Ott 2009, Bergmann 2014), one low quality pediatric study (Jacobsen 2007) plus one pediatric study with data only on EudraCT (Valovirta Clin Ther. 2011).
Consistent data. Durham 2012, Dider 2015, Ott 2009, Lin 2016, Stelmach 2012, Arroabarren 2015, Naclerio, Durham 1999 Scadding JAMA 2017
Formatted: English (United Kingdom)
Formatted: English (United Kingdom)
Formatted: English (United Kingdom)
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 34
SECTION I: ADVERSE EVENTS WITH AIT FOR AR 1
2
SCIT 3
SCIT is a safe and well-tolerated treatment in selected patients when the injections are 4
given in a medical setting experienced with this kind of treatment [Alvarez-Cuesta 2006; 5
Cox 2012; Malling 2000; EAACI SR; Pfaar 2014]. 6
Systemic allergic adverse reactions to SCIT can range between mild to severe adverse 7
reactions of the skin, upper and lower airways, gastrointestinal tract, or the 8
cardiovascular system (Table SB in online supplement). In a three year survey that 9
included over 20 million injection visits, systemic reactions were reported in 0.1% of 10
injections; there were no fatalities [Epstein 2011] although 4 were reported in the follow 11
up survey [Epstein 2016]. Fatal, allergic, adverse reactions have though been reported 12
in earlier surveys [Lockey 2001; Bernstein 2004]. Over 80% of reactions occurred within 13
30 minutes after injection; very few of the delayed ones were severe. It is therefore 14
recommended that patients stay in clinic for at least 30 minutes after an injection. There 15
are a number of possible risk factors for systemic adverse reactions (Table 9). 16
Interestingly, rush [Brehler 2010] and ultra-rush [Cardona 2012 and Casanovas 2006] 17
build up schedules with modified allergens are not associated with more adverse events 18
than conventional ones. When one or more severe adverse reactions occur, the allergist 19
should re-discuss the benefits and risks of SCIT therapy with the patient and decide 20
whether or not treatment should be continued. 21
Redness, itching or swelling represent local reactions at the injection site. These occur 22
frequently after around half of injections [Dhami 2017]. Local measures (e.g., cooling or 23
topical glucocorticoids) or oral antihistamines may be helpful for these reactions. 24
Increased local adverse reactions do not predict an increased individual risk of a 25
systemic adverse reaction [Kelso 2004]. In case of enlarged local adverse reactions 26
(redness and/or swelling >10 cm in diameter) occur at the injection site, the 27
manufacturer‘s product information (SmPC) leaflet provides adaptions of the dosing-28
schemes for the next injection. When local adverse effects occur, pre-medication with 29
an H1-antihistamine can be used to reduce the frequency and severity of adverse 30
reactions but this prophylactic treatment does not prevent the onset of systemic adverse 31
reactions [Nielsen 1996; Reimers 2000]. Alternatively, case series indicate that modified 32
allergen extracts are associated with less adverse effects [Brehler 2010, Cardona 2012, 33
Casanovas 2006 & 2007]. For aluminum hydroxide containing SCIT products, rarely 34
granulomas have been described from a foreign body reaction mainly caused by 35

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 35
incorrect intradermal administration as well as contact allergic reactions, new onset of 1
protein contact dermatitis or a vasculitic inflammatory reactions have been reported 2
[Vogelbruch 2000, Netterlid 2009, Frost et al., Allergy 1985]. If these reactions to SCIT 3
occur, treatment with another aluminum hydroxide-free product is preferred [Pfaar 2014]. 4
5
SLIT 6
SLIT is regarded to be a safe and well-tolerated treatment [Radulovic 2010; Canonica 7
2014; Dhami 2017; Pfaar 2014]. 8
Severe systemic reactions with SLIT are much less likely than with SCIT although the 9
overall rate of any adverse reactions is similar in both SCIT and SLIT [Dhami 2017]. In a 10
review of 66 SLIT studies (over 4000 patients who received over a million doses), there 11
was one systematic reaction for approximately every four years of treatment and only 12
one severe systematic reaction per 384 treatment years [Cox 2006]. There are no new 13
safety concerns in more recent studies [Dhami 2017]. Several severe reactions - in some 14
cases with severe anaphylaxis - are described in the literature occurring within 30 15
minutes of sublingual administration of allergens in droplet or tablet form [Calderon 16
2012]. In these cases, SLIT was not administered according to the standards (non-17
standardized extracts, rush protocols, excessive allergen dose, patients in whom SCIT 18
had previously been interrupted due to severe reactions). As in SCIT, concomitant, 19
poorly controlled asthma has been reported to be associated with severe systemic 20
reactions after SLIT [Calderon 2012]. The majority of adverse events in SLIT develop at 21
home without any medical observations (as after SCIT). Patients should therefore be 22
informed about how to recognize and manage reactions, particularly severe ones. 23
Patients also need education on what to do if a dose is forgotten and when SLIT should 24
be temporarily interrupted (e.g. oropharyngeal lesions) [Pfaar 2014]. When one or more 25
severe adverse reactions occur, the allergist should re-discuss the benefits and risks of 26
SLIT with the patient and decide whether or not treatment should be continued. 27
The frequency of local adverse events during SLIT correlates with the dosage and has 28
been reported to be 40% to 75%, for example temporary local mucosal reactions (oral 29
pruritus or dysesthesia, swelling of the oral mucosa, throat irritation) or abdominal pain 30
[Canonica 2014, Cox 2006; Calderon 2012; Passalacqua 2013]. Most of these reactions 31
occur during the initial phase of the treatment course (commonly in the first three weeks). 32
They are commonly considered to be of mild intensity mild and generally [Canonica 33
2014]. Nethertheless, these reactions may occasionally lead to cessation of treatment, 34
as observed in 4-8% of cases reported in recent trials of SLIT tablets (Blaiss 2011, 35

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 36
Mosbech 2014, Didier 2007, Dahl 2006).(see section “adherence”). As in SCIT, local 1
adverse reactions may be diminished by the intake of (oral) antihistamines. 2
3
4
Box 3. Risk factors for systemic reactions during AIT
Current allergy symptoms and potential allergen exposure
Current infections
Mast cell disease
Previous systemic reaction to SCIT or SLIT
Hyperthyroidism
Unstable or uncontrolled or severe asthma
A high degree of sensitization
Excess dose escalation during initiation
Beta-blockers use
Poor injection technique
Overdose of allergen extract
Failure to follow manufacturer's recommendation for dose reduction when change to new production batch
High-intensity physical exercise
Sauna
5 From Pfaar et al., Allergo J Int., 2014 6
7
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 37
Table 8. Recommendations: adverse events with AIT for AR
Recommendation Evidence level
Grade of recommendation
Strength of recommendation
Contextual comments Key references
SCIT or SLIT
For correctly selected patients, SCIT or SLIT is recommended as, appropriately administered, it is safe and well tolerated
I A Strong recommendation based on high quality RCT studies and observational studies (Dhami 2017)
Consistent evidence. Dhami 2017
It is recommended that asthma should be controlled before commencing AIT as insufficiently controlled asthma is a risk factor for both SCIT and SLIT
III C Expert opinion from observational studies
Bernstein 2004; Amin 2006; Calderon 2012
Premedication with an antihistamine is recommended as it reduces the frequency and severity of local and systemic cutaneous reactions but does not eliminate the risk of other systemic adverse reactions
I A Strong recommendation based on high quality studies (Nielsen 1996, Reimers 2000).
Consistent strong evidence from RCT studies
Nielsen 1996; Reimers 2000
When one or more severe adverse reactions occur, it may be recommended that the allergist should re-discuss the benefits and risks of AIT therapy with the patient and decide whether or not treatment should be continued
V D Expert opinion from clinical experience
Expert opinion
SCIT

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 38
It is recommended that patients should wait in the clinic for at least 30 minutes after a SCIT injection
III C Consistent observational data
Epstein 2011
If granulomas develop with aluminum hydroxide containing SCIT products, it may be recommended that treatment should be continued with an allergen extract that does not contain aluminum hydroxide
V D Expert opinion
It is recommended that SCIT should be administered by competent staff with immediate access to resuscitation equipment and a doctor trained in managing anaphylaxis.
I C Consistent observational data
Dhami 2017
SLIT
Where there is concern about the possibility that AIT may cause systemic adverse reactions, SLIT can be recommended as the preferred approach as it is associated with a lower risk of such reactions than SCIT.
II B Expert opinion based on consistent observational data
Epstein 2011; Cox 2006
It is recommended that patients should wait in clinic for at least 30 minutes after an initial SLIT dosage
III C Expert opinion based on consistent observational data
Calderon 2012
It is recommended that patients receiving SLIT should be informed about how to recognized and manage reactions, particularly severe ones. Patients also need to know what to do if a SLIT preparation is forgotten and when SLIT should be temporarily interrupted (e.g. oropharyngeal lesions).
V D Expert opinion from clinical experience
Expert opinion

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 39
SECTION J: PREVENTIVE EFFECTS OF AIT FOR AR 1
2
A three years course of AIT reduces the likelihood that children and adolescents with 3
allergic rhinitis and pollen allergy go on to develop asthma until at least 2 years 4
posttreatment [EAACI Prevention SR]. There is no documentation for a preventive effect 5
of HDM AIT or for prevention of new sensitivities. It is important to be aware that patients 6
included in these studies had less severe AR than those included in studies on AIT for 7
treatment. This is further discussed in the EAACI AIT Prevention Guidelines [prevention 8
AIT guideline]. 9
10
SECTION K: PHARMACOECONOMIC ASPECTS OF AIT VERSUS 11
PHARMACOTHERAPY FOR AR 12
13
Pharmacoeconomic studies that only analyze costs in monetary units have reported 14
beneficial health care expenditure of AIT in the long-run although savings in the first year 15
are not expected to be economic over symptomatic anti-allergic medications. The 16
majority of pharmacoeconomics studies support the viewpoint that AIT gives value for 17
money, with cost-effectiveness within 6 years of treatment initiation (Meadows 2013). 18
Retrospective and prospective observational studies have shown that SCIT and SLIT 19
positively affects health care expenditure in pharmacotherapy with a reduction between 20
12% and 80% (Ariano 2006, Berto 2005, Hankin et al. 2008; Hankin et al. 2010; Hankin 21
et al. 2013). A reduction in medical costs in the AIT versus placebo groups have been 22
repeatedly reported, but these savings did not compensate the costs of AIT (Creticos et 23
al. 1996; Berto et al. 2008; Ariano et al. 2006). 24
In contrast to cost-only studies, cost-effectiveness and cost-utility analysis evaluates the 25
effects of treatment in terms of clinical benefits or health-related quality of life (i.e., 26
quality-adjusted life years [QALYs]). An incremental cost-effectiveness ratio (ICER), 27
which is defined as costs divided by benefits, can be calculated to estimate the costs of 28
a certain gain. Several health economics studies that include cost-effectiveness and cost 29
utility calculations have demonstrated that SCIT and SLIT are economically 30
advantageous (Schadlich et al. 2000; Petersen et al. 2005; Berto et al. 2006; Bachert et 31
al. 2007). 32
Seven studies based on RCT data conducted from a health system perspective and 33
using QALYS as their outcome measure suggest that SLIT and SCIT would be 34

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 40
considered cost-effective in this patient population in England at the standard National 1
Institute for Health and Care Excellence (NICE) cost-effectiveness threshold of £20,000 2
(€24616) per QALY (Nasser 2008, Poulsen 2008, Keidig 2007, Ronaldson 2014, 3
Westerhout 2012, Verheggen 2015, Reinhold 2016). ICERs for AIT seemed to vary 4
substantially between different health systems suggesting that straightforward 5
conclusions may not be generalizable even across seemingly similar countries.(Keidig 6
2007). Finally, the quality of the studies and the general lack of attention to characterizing 7
uncertainty and handling missing data should be taken into account when interpreting 8
these results. 9
SECTION L: SUMMARY, GAPS IN THE EVIDENCE AND FUTURE 10
PERSPECTIVES 11
12
The EAACI Taskforce on AIT for Rhinoconjunctivitis has developed these guidelines as 13
part of the EAACI AIT Guidelines project. The guidelines has been informed by a formal 14
systematic review and meta-analysis of AIT for AR [Dhami 2017], The guidelines provide 15
evidence-based recommendations for the use of AIT for patients with allergic rhinitis with 16
or without allergic conjunctivitis. A summary of the guidelines is provided in Box 3. The 17
recommendations should be of value to all healthcare professionals involved in the 18
management of patients with AR. 19
There are many areas in these guidelines where there is no high quality evidence, these 20
signify the gaps in the current evidence base. The key ones are highlighted here and in 21
Table 9. There is a major gap in the evidence base for the clinical effectiveness of AIT 22
in children and adolescents with recommendations at least one grade lower than for 23
adults in most areas. As AR usually starts in childhood and AIT changes the natural 24
history of the disease and prevents the development of asthma, this age group has most 25
to benefit. Once safety is established in adult studies, pediatric studies need to be 26
commenced using common outcome measures (Pfaar 2014). There is also little data in 27
the elderly particularly for patients with multi-morbidity. Additionally, more randomized 28
controlled trials need to follow participants post cessation of therapy to establish long-29
term clinically effectiveness. Agreement about the clinically meaningful effect size of AIT 30
treatment would assist in the interpretation of clinical trial data. Additionally we need data 31
from randomized cost-effectiveness and cost utility studies to use in discussions with 32
healthcare funders. We need biomarkers to predict and quantify the effectiveness of AIT 33
to assist in patient selection (Shamji 2017). The poor adherence associated with SLIT is 34
likely to be impacting on its effectiveness; we need to develop novel approaches to 35
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 41
improve effectiveness in partnership with patients. Finally, to allow better comparison of 1
safety between approaches, a unified approach to classifying side effects is required. 2
Despite all these gaps we have clear evidence for the clinical effectiveness of AIT for 3
moderate-to-severe AR that is otherwise uncontrolled despite optimal pharmacotherapy 4
with evidence-based recommendations for specific patient groups and specific 5
approaches. There is now a need to ensure that primary care healthcare professionals 6
know which patients might benefit from AIT, that national healthcare providers 7
understand that AIT is cost-effective and that patients and patient support groups are 8
aware of this approach. 9

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 42
Table 9. Gaps in the evidence
Gaps Plan to address Priority
Value of provocation tests in identifying the most appropriate allergen to use in AIT
Prospective controlled studies to assess benefit of provocation testing
Moderate
Good evidence base for contraindications to AIT Registries recording patient details, AIT, outcome and adverse effects
Low
Lack of biomarkers to predict and quantify the effectiveness of AIT Prospective observational studies to validate potential predictive biomarkers
High
Agreement about the clinically meaningful effect size of AIT treatment (active versus placebo treated patients)
Consensus discussion High
High quality randomized controlled data for children and adolescents More prospective controlled trials High
For some AIT productions there is poor data for clinical effectiveness Additional prospective controlled trials; use of products with proven effectiveness
Moderate
Evidence for clinical effectiveness post treatment cessation More prospective controlled trials with follow up post treatment cessation
High
Effectiveness of mixtures of homologous allergens from the same, related or different biological families
More prospective controlled trials Moderate
Management of AIT in patients who become pregnant on therapy More prospective observational studies Moderate
Standardization of grading of adverse effects of AIT Future clinical trials should use the WAO systemic reaction grading system
High
Approaches to minimize adverse effects More prospective observation and controlled trials Moderate
Approaches to improve adherence with SLIT Working patients to develop to develop novel approaches that can be tested in prospective controlled trials
High
Lack of standardized AIT preparations for orphan allergens Multi-centre studies Low
Randomized cost-effectiveness and cost utility studies adjusted to socioeconomic differences within and between countries
Additional studies with a health economics focus High

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 43
Box 3. Summary of the EAACI Rhinoconjunctivitis AIT Guidelines
The EAACI Guidelines on Allergen Immunotherapy (AIT) for allergic rhinitis (AR) aim to provide evidence-based recommendations for the use of AIT for patients with AR.
Development of the guidelines has been based on a formal systematic review and meta-analysis of AIT for AR.
AIT should be considered with symptoms strongly suggestive of allergic rhinitis, with
or without conjunctivitis; evidence of IgE-sensitization to one or more clinically
relevant allergen; and moderate-to-severe symptoms despite regular and
appropriate pharmacotherapy and / or avoidance strategies.
AIT may also be considered in less severe AR where a patient wishes to take
advantage of its long term effect on rhinitis and potential to prevent asthma.
A product based evaluation of evidence is recommended.
Standardized AIT products with evidence of efficacy in the clinical documentation
should preferably be used.
Key contraindications are uncontrolled asthma; active, systemic autoimmune
disorders; active malignant neoplasia. Careful review of benefits and risks are
required with beta-blocker or ACE-inhibitor therapy, severe cardiovascular disease,
other autoimmune disorders, severe psychiatric disease, poor adherence and
immunodeficiency.
Continuous SCIT is recommended for seasonal (Grade A, B for children) or
perennial (Grade B, C for children) AR for short-term benefit in those with moderate-
to severe disease
Pre- and pre-/co-seasonal SCIT is recommended for seasonal AR for short-term benefit
(Grade A, B for children)
Both modified (allergoids) and unmodified allergen extracts are recommended for AR
for short-term benefit (Grade A, B for children)
Continuous grass pollen SCIT is recommended for AR for short and long-term
benefit (Grade A, B for children)
Pre-/co-seasonal or continuous SLIT is recommended for seasonal ARs for short-
term benefit (Grade A, B for continuous in children)
SLIT with tablets (Grade A) or aqueous solutions (Grade B, A in children) can be
recommended for AR for short-term benefit.
Grass pollen SLIT tablets or solution is recommended for allergic rhinoconjunctivitis
for long-term benefit (Grade A, B for children).
HDM SLIT tablet can be recommended for allergic rhinoconjunctivitis for long-term
benefit (Grade B, C for children).
Polysensitized patients who are poly-allergic for taxonomically related homologous allergens
can be recommended to receive either a single allergen or a mixture of homologous allergens
from that biological family that covers all the major allergens (Grade B)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 44
Patients who are poly-allergic for non-homologous allergens may be recommended
to start AIT with either the allergen responsible for most of their allergic
rhinoconjunctivitis symptoms or separate treatment with the two clinically most
important allergens (Grade C).
In children aged less than 5 years of age, it is recommended that consideration
should be given to likely benefits and risks associated with AIT for AR (Grade D).
AIT can be recommended in otherwise healthy elderly patients with AR whose
symptoms cannot be adequately controlled by pharmacotherapy (Grade A for SCIT,
B for SLIT)
If patients have not started AIT and are pregnant, it is recommended to wait until
after pregnancy to initiate therapy (Grade D).
It can be recommended that patients on SLIT are followed up every 3 months to
maximize adherence (Grade B).
To achieve long-term efficacy, it is recommended that a minimum of 3 years of
therapy is used (Grade A).
Premedication with an antihistamine is recommended as it reduces the frequency
and severity of local and systemic cutaneous reactions but does not eliminate the
risk of other systemic adverse reactions (Grade A).
It is recommended that patients should wait in the clinic for at least 30 minutes after
a SCIT injection (Grade C).
It is recommended that SCIT should be administered by competent staff with
immediate access to resuscitation equipment and a doctor trained in managing
anaphylaxis. (Grade C).
It is recommended that patients should wait in clinic for at least 30 minutes after an initial
SLIT dosage (Grade C).
It is recommended that patients receiving SLIT should be informed about how to
recognized and manage reactions, particularly severe ones (Grade D).
Many gaps in the underpinning evidence have been identified and prioritized.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 45
REFERENCES
Introduction
Ait-Khaled N, Pearce N, Anderson HR, Ellwood P, Montefort S, Shah J. Global map of the prevalence of symptoms of rhinoconjunctivitis in children: The International Study of Asthma and Allergies in Childhood (ISAAC) Phase Three. Allergy 2009; 64(1): 123-48.
Bauchau V, Durham SR. Prevalence and rate of diagnosis of allergic rhinitis in Europe. The European respiratory journal: official journal of the European Society for Clinical Respiratory Physiology 2004; 24(5): 758-64.
Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A et al. Allergic rhinitis and its impact on asthma ARIA 2008 update in collaboration with the World Health Organization, GA2LEN and Aller Gen. Allergy 2008;63:8–160.
Bousquet et al, ARIA Update 2008, http://www.whiar.org/docs/ARIA-Report-2008.pdf
Brozek et al. Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 revision. J Allergy Clin Immunol. 2010 Sep;126(3):466-76. Doi: 10.1016/j.jaci.2010.06.047.
Calderon MA, Alves B, Jacobson M, Hurwitz B, Sheikh A, Durham S. Allergen injection immunotherapy for seasonal allergic rhinitis. Cochrane Database Syst Rev 2007; (1): CD001936.
P. Campo, C. Rondón, H. J. Gould, E. Barrionuevo, P. Gevaert, M. Blanca. Local IgE in non-allergic rhinitis. Clinical & Experimental Allergy, 2015 (45) 872–881.
Canonica GW, Cox L, Pawankar R, et al. Sublingual immunotherapy: World Allergy Organization position paper 2013 update. The World Allergy Organization journal 2014; 7(1): 6.
Dahl R, Andersen PS, Chivato T, Valovirta E, de Monchy J. National prevalence of respiratory allergic disorders. Respiratory medicine 2004; 98(5): 398-403.
W. O. Eifan and S. R. Durham. Pathogenesis of rhinitis. Clinical & Experimental Allergy, 2016
(46) 1139–1151.
Greiner AN, Hellings PW, Rotiroti G, Scadding GK. Allergic rhinitis. Lancet 2011; 378(9809): 2112-22.
Jutel et al. International Consensus on Allergen Immunotherapy II: Mechanisms, standardization, and pharmacoeconomics. J Allergy Clin Immunol 2016;137:358-68
Jutel M, Agache I, Bonini S, Burks AW, Calderon M, Canonica W, Cox L, Demoly P, Frew AJ, O’Hehir R, Kleine-Tebbe J, Muraro A, Lack G, Larenas D, Levin M, Nelson H, Pawankar R, Pfaar O, van Ree R, Sampson H, Santos AF, Du Toit G, Werfel T, Gerth van Wijk R, Zhang L, Akdis CA. International consensus on allergy immunotherapy. J Allergy Clin Immunol. 2015 Sep;136(3):556-68. Doi: 10.1016/j.jaci.2015.04.047. Epub 2015 Jul 7.
Kopp MV, Niggemann B, Forster J. House dust mite allergy: complete removal of the provoking allergen is a primary therapeutic approach. Allergy 2009;64:1402–3.
Larenas-Linnemann D, Pfaar O. Patient-reported outcomes and quality-of-life questionnaires in the assessment of rhinoconjunctivitis in childhood. Current opinion in allergy and clinical immunology 2014; 14(3): 192-9.
Meltzer EO, Blaiss MS, Derebery MJ, Mahr TA, Gordon BR, Sheth KK, Simmons AL, Meltzer EO, Wallace D, Dykewicz M, Shneyer L. Minimal Clinically Important Difference (MCID) in
Field Code Changed
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 46
Allergic Rhinitis: Agency for Healthcare Research and Quality or Anchor-Based Thresholds? The journal of allergy and clinical immunology In practice 2016; 4(4): 682-8 e6.
Muche-Borowski C, Kopp M, Reese I et al. [Evidencebased and consented guideline on allergy prevention – update 2009]. Allergo J 2009;18:332–41.
Pfaar O, Bachert C, Bufe A, Buhl R, Ebner C, Eng P, et al. Guideline on allergen-specific immunotherapy in IgE-mediated allergic diseases: S2k Guideline of the German Society for Allergology and Clinical Immunology (DGAKI), the Society for Pediatric Allergy and Environmental Medicine (GPA), the Medical Association of German Allergologists (AeDA), the Austrian Society for Allergy and Immunology (ÖGAI), the Swiss Society for Allergy and Immunology (SGAI), the German Society of Dermatology (DDG), the German Society of Oto- Rhino-Laryngology, Head and Neck Surgery (DGHNO-KHC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Pneumology (GPP), the German Respiratory Society (DGP), the German Association of ENT Surgeons (BV-HNO), the Professional Federation of Paediatricians and Youth Doctors (BVKJ), the Federal Association of Pulmonologists (BDP) and the German Dermatologists Association (BVDD). Allergo J Int. 2014;23(8):282-319.
Radulovic S, Wilson D, Calderon M, Durham S. Systematic reviews of sublingual immunotherapy (SLIT). Allergy 2011; 66(6): 740-52.
Roberts G, Xatzipsalti M, Borrego LM, Custovic A, Halken S, Hellings PW, Papadopoulos NG, Rotiroti G, Scadding G, Timmermans F, Valovirta E. Paediatric rhinitis: position paper of the European Academy of Allergy and Clinical Immunology. Allergy 2013; 68: 1102-16.
Rondon C, Campo P, Herrera R, et al. Nasal allergen provocation test with multiple aeroallergens detects polysensitization in local allergic rhinitis. J Allergy Clin Immunol 2011; 128(6): 1192-7.
Silva CHM, Silva T, Morales N, Fernandes K, Pinto R. Quality of life in children and adolescents with allergic rhinitis. Braz J Otorhinolaryngol 2009;75:642–649.
Singh K, Axelrod S, Bielory L. The epidemiology of ocular and nasal allergy in the United States, 1988-1994. J Allergy Clin Immunol. 2010;126(4):778.
Terrehorst 2003. N Engl J Med. 2003 Jul 17;349(3):237-46. Evaluation of impermeable covers for bedding in patients with allergic rhinitis. http://www.nejm.org/doi/full/10.1056/NEJMoa023171
Walker S, Khan W, Fletcher M, Cullinan P, Harris J, Sheikh A. Seasonal allergic rhinitis is associated with a detrimental effect on examination performance in United Kingdom teenagers: case-control study. J Allergy Clin Immunol 2007;120:381–387.
Wingertzahn MA, Boyle JM. Burden of allergic rhinitis: results from the Pediatric Allergies in America survey. J Allergy Clin Immunol. 2009;124(3 Suppl):S43.
Rondón C1, Romero JJ, López S, Antúnez C, Martín-Casañez E, Torres MJ, Mayorga C, R-Pena R, Blanca M. Local IgE production and positive nasal provocation test in patients with persistent nonallergic rhinitis. J Allergy Clin Immunol. 2007; 119(4): 899-905.
Methodology
Agree Collaboration 2003
Brouwers 2010
Oxford Centre for Evidence-based Medicine
Field Code Changed

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 47
General considerations
Agostinis F, Tellarini L, Canonica GW, Falagiani P, Passalacqua G. Safety of sublingual immunotherapy with a monomeric allergoid in very young children. Allergy 2005;60:133-134.
Álvarez-Cuesta E, Bousquet J, Canonica GW, Durham SR, Malling HJ, Valovirta E; EAACI, Immunotherapy Task Force. Standards for practical allergen-specific immunotherapy. Allergy 2006;61(Suppl 82):1-20.18.
Bachert C, Larche M, Bonini S, Canonica GW, Kundig T, et al. (2015) Allergen immunotherapy on the way to product-based evaluation-a WAO statement. World Allergy Organ J 8: 29
Bernstein DI, Wanner M, Borish L, Liss GM. Twelve-year survey of fatal reactions to allergen injections and skin testing: 1990-2001. J Allergy Clin Immunol 2004;113:1129-1136.
Bousquet J, Hejjaoui A, Dhivert H, Clauzel AM, Michel FB. Systemic reactions during the rush protocol in patients suffering from asthma. J Allergy Clin Immunol 1989;83:797-780.
Bousquet J, Mantzouranis E, Cruz AA, Aït-Khaled N, Baena-Cagnani CE, Bleecker ER et al. Uniform definition of asthma severity, control, and exacerbations: document presented for the World Health Organization Consultation on Severe Asthma. J Allergy Clin Immunol 2010;126:926-938.
Cabrera GE, Citera G, Gutiérrez M, Scopelitis E, Espinoza LR. Digital vasculitis following allergic desensitization treatment. J Rheumatol 1993;20:1970-1972.
Cadavid AP, Bannenberg GL, Arck PC, Fitzgerald JS, Markert UR. Prevention and treatment of allergic asthma in pregnancy: from conventional drugs to new therapeutical approaches. Curr Pharm Biotechnol 2011;12:758-764.
Calderon MA, Simons FER, Malling H-J, Lockey RF, Moingeon P, Demoly P. Sublingual allergen immunotherapy: mode of action and its relationship with the safety profile. Allergy 2012; 67: 302–311.
Cleaveland CR, Rangno RE, Shand DG. A standardized isoproterenol sensitivity test. The effects of sinus arrhythmia, atropine, and propranolol. Arch Intern Med 1972;130:47-52.
Cox L, Nelson H, Lockey R, Calabria C, Chacko T, Finegold I et al. Allergen immunotherapy: a practice parameter third update. J Allergy Clin Immunol 2011;127:S1-55.
CSM Update: Desensitising vaccines. Br Med J 1986;293:948.
Demoly P, Piette V, Daures JP. Treatment of allergic rhinitis during pregnancy. Drugs 2003;16:1813-1820.
Di Rienzo V, Pagani A, Parmiani S, Passalacqua G, Canonica GW. Post-marketing surveillance study on the safety of sublingual immunotherapy in pediatric patients. Allergy 1999;54:1110-1113.
Fenwick MJ, Muwanga CL. Anaphylaxis and monoamine oxidase inhibitors—the use of adrenaline. J Accid Emerg Med 2000;17:143-144.
Fiocchi A, Pajno G, La Grutta S, Pezzuto F, Incorvaia C, Sensi L et al. Safety of sublingual-swallow immunotherapy in children aged 3 to 7 years. Ann All Asthma Immunol 2005;95:254-258.
Fodeman J, Jariwala S, Hudes G, Jerschow E, Rosenstreich D. Subcutaneous allergen immunotherapy in 3 patients with HIV. Ann Allergy Asthma Immunol 2010;105:320-321.
Fiorillo A, Fonacier L, Diola C. Safety of Allergenic Immunotherapy in Systemic Lupus Erythematosus J Allergy Clin Immunol 2006;117(2 Suppl);S264.
Gani F, Braida A, Lombardi C, Del Guidice A, Senna G, Passalaqua G. Rhinitis in Pregnancy. Eur Ann Allergy Clin Immunol 2003;35:306-313.
Formatted: English (United Kingdom)
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 48
Garcia-Robaina JC, Sanchez I, de la Torre F, Fernandez-Caldas E, Casanovas M. Successful management of mite-allergic asthma with modified extracts of Dermatophagoides pteronyssinus and Dermatophagoides 48tanda in a double-blind, placebo-controlled study. J Allergy Clin Immunol 2006;118:1026-1032.
Hiatt WR, Wolfel EE, Stoll S, Nies AS, Zerbe GO, Brammell HL, et al. beta-2 Adrenergic blockade evaluated with epinephrine after placebo, atenolol, and nadolol. Clin Pharmacol Ther 1985;37:2-6.
Larenas-Linnemann DES, Hauswirth DW, Calabria CW, Sher LD, Rank MA. American Academy of Allergy, Asthma & Immunology membership experience with allergen immunotherapy safety in patients with specific medical conditions. Allergy Asthma Proc 2016; 37:e112–e122; doi: 10.2500/aap.2016.37.3981
Lang DM. Anaphylactoid and anaphylactic reactions. Hazards of beta-blockers. Drug Saf 1995;12:299-304.
Linneberg A, Jacobsen RK, Jespersen L, Abildstrom SJ. Association of subcutaneous allergen-specific immunotherapy with incidence of autoimmune disease, ischemic heart disease, and mortality. J Allergy Clin Immunol 2012;129(2);413-419.
Livingston MG, Livingston HM. Monoamine oxidase inhibitors. An update on drug interactions. Drug Saf 1996;14:219-227Matsumura Y, Tan EM, Vaughan JH. Hypersensitivity to histamine and systemic anaphylaxis in mice with pharmacologic beta adrenergic blockade: protection by nucleotides. J Allergy Clin Immunol 1976;58:387-394.
Lockey RF, Nicoara-Kasti GL, Theodoropoulos DS, Bukantz SC. Systemic reactions and fatalities associated with allergen immunotherapy. Ann Allergy Asthma Immunol 2001;87:47-55.
Marcoval J, Moreno A, Maña Titel J. Subcutaneous sarcoidosis localized to sites of previous desensitizing injections. Clin Exp Dermatology 2007;33:132-134.
Normansell R, Kew KM, Bridgman AL. Sublingual immunotherapy for asthma. Cochrane Database of Systematic Reviews 2015, Issue 8. Art. No.: CD011293. DOI: 10.1002/14651858.CD011293.pub2.
Palomares O, Yaman G, Azkur AK, Akkoc T, Akdis M, Akdis CA. Role of T regulatory cells in immune regulation of allergic diseases. Eur J Immunol 2010;40:1-9.
Paniagua MJ, Bosque M, Asensio O, Larramona H, Marco MT. Immunoterapia con un extracto de ácaros en niños menores de cinco años. Allergol Immunopathol 2002;30:20-24.
Penagos M, Compalati E, Tarantini F, Baena-Cagnani R, Huerta J, Passalacqua G et al. Efficacy of sublingual immunotherapy in the treatment of allergic rhinitis in pediatric patients 3 to 18 years of age: a meta-analysis of randomized, placebo-controlled, double-blind trials. Ann Allergy Asthma Immunol 2006;97:141-148.
Pitsios C, Demoly P, Bilò MB, Gerth van Wijk R, Pfaar O, et al. Clinical Contraindications to Allergen Immunotherapy: an EAACI Position Paper. Allergy, 2015; 70:897-909
Randhawa IS, Junaid I, Klaustermeyer WB. Allergen immunotherapy in a patient with human immunodeficiency virus: effect on T-cell activation and viral replication. Ann Allergy Asthma Immunol 2007;98:495-497
Rienzo VD, Minelli M, Musarra A, Sambugaro R, Pecora S, Canonica WG et al. Post-marketing survey on the safety of sublingual immunotherapy in children below the age of 5 years. Clin Exp Allergy 2005;35:560-564.
Rodriguez-Santos O. Sublingual immunotherapy in allergic rhinitis and asthma in 2-5-year-old children sensitized to mites. Rev Alerg Mex 2008;55:71-75.
Formatted: English (United Kingdom)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 49
Rodríguez Pérez N, Ambriz Moreno MJ. Inocuidad de la immunotherapia y pruebas cutáneas con alergenos en niños menores de cinco años de edad. Rev Al Méx 2006;53:47-51.
Rienzo VD, Minelli M, Musarra A, Sambugaro R, Pecora S, CanonicaWG et al. Post-marketing survey on the safety of sublingual immunotherapy in children below the age of 5 years. Clin Exp Allergy
Rodriguez-Santos O. Sublingual immunotherapy in allergic rhinitis and asthma in 2–5-year-old children sensitized to mites. RevAlerg Mex 2008;55:71–75.
Sánchez-Morillas L, Reaño Martos M, Iglesias Cadarso A, Pérez Pimiento A, Rodríguez Mosquera M, Domínguez Lázaro AR. Vasculitis during immunotherapy treatment in a patient with allergy to Cupressus arizonica. Allergol Immunopathol 2005;33:333-334.
Schiappoli M, Ridolo E, Senna G, Alesina R, Antonicelli L, Asero R, et al. A prospective Italian survey on the safety of subcutaneous immunotherapy for respiratory allergy. Clin Exp Allergy 2009;39:1569-74.
Shaikh WA, Shaikh SW.
Steiner UC, Furrer H, Helbling A. Specific immunotherapy in a pollen-allergic patient with Human Immunodeficiency Virus infection. WAO Journal 2009;2:57-58.
Walker SM, Durham SR, Till SJ, Roberts G, Corrigan CJ, Leech SC et al. BSACI GUIDELINES Immunotherapy for allergic rhinitis. Clin Exp Allergy 2011;41:1177-1200Webster WS, Freeman JAD. Prescription drugs and pregnancy. Exp Opin Pharmacother 2003;4:949-961.
Wöhrl S, Kinaciyan T, Jalili A, Stingl G, Moritz KB. Malignancy and Specific Allergen Immunotherapy: The results of a Case Series. Int Arch Allergy Immunol 2011;156:313-319.
ALLERGEN IMMUNOTHERAPY FOR ALLERGIC RHINOCONJUNCTIVITIS: EVIDENCE AND CLINICAL RECOMMENDATIONS
Arvidsson MB, Löwhagen O, Rak S. Effect of 2-year placebo-controlled immunotherapy on airway symptoms and medication in patients with birch pollen allergy. J Allergy Clin Immunol. 2002 May;109(5):777-83
B. R. Balda, H. Wolf, C. Baumgarten, L. Klimek, G. Rasp, G. Kunkel, et al. Tree-pollen allergy is efficiently treated by short-term immunotherapy (STI) with seven preseasonal injections of molecular standardized allergens. Allergy. Aug;53(8):740–8.
U. Bodtger, L. K. Poulsen, H. H. Jacobi, H. J. Malling. The safety and efficacy of subcutaneous birch pollen immunotherapy - a one-year, randomised, double-blind, placebo-controlled study. Allergy. Apr;57(4):297–305.
J. Bousquet, A. Hejjaoui, W. Skassa-Brociek, B. Guerin, H. J. Maasch, H. Dhivert, et al. Double-blind, placebo-controlled immunotherapy with mixed grass-pollen allergoids. I. Rush immunotherapy with allergoids and standardized orchard grass-pollen extract. J Allergy Clin Immunol. Oct;80(4):591–8.
Brunet C, Pierre-Michel 6dard, Aubert Lavoie, et al. Allergic rhinitis to ragweed pollen I. Reassessment of the effects of imrnunotherapy cellular and hurnoral responses.
D. Charpin, M. Gouitaa, M. Dron-Gonzalvez, M. F. Fardeau, Y. P. Massabie-Bouchat, B. Hugues, et al. Immunotherapy with an aluminum hydroxide-adsorbed Juniperus ashei foreign pollen extract in seasonal indigenous cypress pollen rhinoconjunctivitis. A double-blind, placebo-controlled study. Int Arch Allergy Immunol. 2007;143(2):83–91.
Clavel R, Bousquet J, Andre C. Clinical efficacy of sublingual-swallow immunotherapy: a double-blind, placebo-controlled trial of a standardized five-grass-pollen extract in rhinitis.
Formatted: English (United Kingdom)
Formatted: English (United Kingdom)
Formatted: German (Switzerland)
Formatted: German (Switzerland)

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 50
Bergmann KC, Demoly P, Worm M, Fokkens WJ, Carrillo T, Tabar AI, et al. Efficacy and safety of sublingual tablets of house dust mite allergen extracts in adults with allergic rhinitis. J Allergy Clin Immunol 2014;133:1608-14.
Demoly P, Emminger W, Rehm D, Backer V, Tommerup L, Kleine-Tebbe J. Effective treatment of house dust mite-induced allergic rhinitis with 2 doses of the SQ HDM SLIT-tablet: results from a randomized double-blind, placebo-controlled phase III trial. J Allergy Clin Immunol 2016;137:444-51
C. J. Corrigan1 for the Study Group*, J. Kettner2, C. Doemer2, O. Cromwell2, A. Narkus2. Efficacy and safety of preseasonal-specific immunotherapy with an aluminium-adsorbed six-grass pollen allergoid. Allergy. 2005 Jun;60(6):801-7.Frew AJ, DuBuske L, Frew A, Horak F, Keith P, Corrigan C, Aberer W. Ultrashort-specific immunotherapy successfully treats seasonal allergic rhinoconjunctivitis to grass pollen. Allergy Asthma Proc. 2011;32(3):239–47.
Calderon MA, Alves B, Jacobson M, Hurwitz B, Sheikh A, Durham S. Allergen injection immunotherapy for seasonal allergic rhinitis. The Cochrane database of systematic reviews. 2007(1):Cd001936.
L. S. Cox, T. B. Casale, A. S. Nayak, D. I. Bernstein, P. S. Creticos, L. Ambroisine, et al. Clinical efficacy of 300IR 5-grass pollen sublingual tablet in a US study: the importance of allergen-specific serum IgE. J Allergy Clin Immunol. Dec;130(6):1327–34.
P. S. Creticos, J. Maloney, D. I. Bernstein, T. Casale, A. Kaur, R. Fisher, et al. randomized controlled trial of a ragweed allergy immunotherapy tablet in North American and European adults. J Allergy Clin Immunol. May;131(5):1342–9.
P. S. Creticos, R. E. Esch, P. Couroux, D. Gentile, P. D’Angelo, B. Whitlow, et al. Randomized, double-blind, placebo-controlled trial of standardized ragweed sublingual-liquid immunotherapy for allergic rhinoconjunctivitis.[Erratum appears in J Allergy Clin Immunol. 2014 May;133(5):1502]. J Allergy Clin Immunol. Mar;133(3):751–8.
R. Dahl, A. Stender, S. Rak. Specific immunotherapy with SQ standardized grass allergen tablets in asthmatics with rhinoconjunctivitis. Allergy. Feb;61(2):185–90
A. Didier, H.J. Malling, M. Worm, F. Horak, S. Jäger, A. Montagut, et al.Optimal dose, efficacy, and safety of once-daily sublingual immunotherapy with a 5-grass pollen tablet for seasonal allergic rhinitis. J Allergy Clin Immunol, 120 (2007), pp. 1338–1345.
Alain Didier Hans-Jørgen Malling, Margitta Worm, Friedrich Horak and Gordon L Sussman. Prolonged efficacy of the 300IR 5-grass pollen tablet up to 2 years after treatment cessation, as measured by a recommended daily combined score.Clinical and Translational Allergy 20155:12. DOI: 10.1186/s13601-015-0057-8.
Durham SR, Emminger W, Kapp A, et al. SQ-standardized sublingual grass immunotherapy: confirmation of disease modification 2 years after 3 years of treatment in a randomized trial. J Allergy Clin Immunol. 2012;129(3):717-725.e715.
Durham SR, Walker SM, Varga EM, et al. Long-term clinical efficacy of grass-pollen immunotherapy. N Engl J Med. 1999;341(7):468-475.
Dhami S,Nurmatov U, Roberts G, Pfaar O,Muraro A, Ansotegui I et al.Allergen immunotherapy for allergic rhinoconjunctivitis: protocol for a systematic review Clinical and Translational Allergy20166:12 DOI: 10.1186/s13601-016-0099-6© Dhami et al. 2016.Received: 25 November 2015Accepted: 31 January 2016Published: 22 March 2016.
D. Dokic, J. Schnitker, A. Narkus, O. Cromwell, E. Frank. Clinical effects of specific immunotherapy: a two-year double-blind, placebo-controlled study with a one year follow-up. Makedon Akad Na Nauk Umet Oddelenie Za Bioloshki Meditsinski Nauki Pril. 2005 Dec;26(2):113–29.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 51
P. W. Ewan, M. M. Alexander, C. Snape, P. W. Ind, B. Agrell, S. Dreborg. Effective hyposensitization in allergic rhinitis using a potent partially purified extract of house dust mite. Clin Allergy1988 Sep;18(5):501–8.
M. Ferrer, E. Burches, A. Peláez, A. Muñoz, D. Hernández, A. Basomba, et al. Double-blind, placebo-controlled study of immunotherapy with Parietaria judaica: Clinical efficacy and tolerance. J Investig Allergol Clin Immunol. 2005;15(4):283-92.
Jacobsen L, Niggemann B, Dreborg S, Ferdousi HA, Halken S, Høst A, Koivikko A, Norberg LA, Valovirta E, Wahn U, Möller C; (The PAT investigator group). Specific immunotherapy has long-term preventive effect of seasonal and perennial asthma: 10-year follow-up on the PAT study. Allergy. 2007 Aug;62(8):943-8..
Jutel M, A. L. Jaeger, R. Suck, H. Meyer, H. Fiebig, O. Cromwell. Allergen-specific immunotherapy with recombinant grass pollen allergens. J Allergy Clin Immunol. Sep;116(3):608–13.
L. Klimek, J. Uhlig, R. Mosges, K. Rettig, O. Pfaar. A high polymerized grass pollen extract is efficacious and safe in a randomized double-blind, placebo-controlled study using a novel up-dosing cluster-protocol. Allergy. 2014;Dec;69(12):1629–38.
Mosbech H, Canonica GW, Backer V, de Blay F, Klimek L, Broge L, et al. SQ house dust mite sublingually administered immunotherapy tablet (ALK) improves allergic rhinitis in patients with house dust mite allergic asthma and rhinitis symptoms. Ann Allergy Asthma Immunol 2015;114:134-40.
Maloney J, Bernstein D, Nelson H, et al. Efficacy and safety of grass sublingual immunotherapy tablet, MK-7243: a large randomized controlled trial. Ann Allergy Asthma Immunol. 2014;112:146e153.
Maloney J, Prenner BM, Bernstein DI, Lu S1, Gawchik S, Berman G, Kaur A, Li Z, Nolte H. Safety of house dust mite sublingual immunotherapy standardized quality tablet in children allergic to house dust mites. Ann Allergy Asthma Immunol. 2016 Jan;116(1):59-65. doi: 10.1016/j.anai.2015.10.024. Epub 2015 Nov 6.
Nolte, Hendrik et al. Efficacy of house dust mite sublingual immunotherapy tablet in North American adolescents and adults in a randomized, placebo-controlled trial. Journal of Allergy and Clinical Immunology , Volume 138 , Issue 6 , 1631 – 1638
Nolte H, Maloney J, Nelson HS, Bernstein DI, Lu S, Li Z, Kaur A’ Zieglmayer P, Zieglmayer R, Lemell P, Horak F Onset and dose-related efficacy of house dust mite sublingual immunotherapy tablets in an environmental exposure chamber. J Allergy Clin Immunol. 2015 Jun;135(6):1494-501.
Ott H, Sieber J, Brehler R, F€olster-Holst R, Kapp A, Klimek L, et al. Efficacy of grass pollen sublingual immunotherapy for three consecutive seasons and after cessation of treatment: the ECRIT study. Allergy 2009;64:1394-401.
Powell RJ, Corrigan CJ, Durham SR, U. K. Immunotherapy Study Group. Efficacy and safety of specific immunotherapy with SQ allergen extract in treatment-resistant seasonal allergic rhinoconjunctivitis. J Allergy Clin Immunol. 2006 Feb;117(2):319–25.
Radulovic S, Calderon MA, Wilson D, Durham S. Sublingual immunotherapy for allergic rhinitis. Cochrane Database Syst Rev 2010;(12):CD002893.
Roberts G, Hurley C, Turcanu V, Lack G. Grass pollen immunotherapy as an effective therapy for childhood seasonal allergic asthma.. J Allergy Clin Immunol. 2006 Feb;117(2):263-8.
Scadding GW, Calderon MA, Shamji MH, Eifan AO, Penagos M, Dumitru F, Sever ML, Bahnson HT, Lawson K, Harris KM, Plough AG, Panza JL, Qin T, Lim N, Tchao NK, Togias A, Durham SR; Immune Tolerance Network GRASS Study Team. Effect of 2 Years of

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 52
Treatment with Sublingual Grass Pollen Immunotherapy on Nasal Response to Allergen Challenge at 3 Years Among Patients with Moderate to Severe Seasonal Allergic Rhinitis: The GRASS Randomized Clinical Trial. JAMA. Feb.2017;14;317:615-625
A. I. Tabar, S. Echechipia, B. E. Garcia, J. M. Olaguibel, M. T. Lizaso, B. Gomez, et al. Double-blind comparative study of cluster and conventional immunotherapy schedules with Dermatophagoides pteronyssinus. J Allergy Clin Immunol. 2005, Jul;116(1):109–18.
Ulugbek N, Dhami S, Arasi S, Roberts G, Pfaar O, Muraro A et al. Allergen Immunotherapy for allergic rhinoconjunctivitis: a systematic overview. Allergy 2017 (in preparation).
V. A. Varney, K. Tabbah, G. Mavroleon, A. J. Frew. 2003 Usefulness of specific immunotherapy in patients with severe perennial allergic rhinitis induced by house dust mite: a double-blind, randomized, placebo-controlled trial. Clin Exp Allergy 2005. Aug;33(8):1076–82.
V. A. Varney, M. Gaga, A. J. Frew, V. R. Aber, A. B. Kay, S. R. Durham. Usefulness of immunotherapy in patients with severe summer hay fever uncontrolled by antiallergic drugs. BMJ. 1991;302(6771):265–9.
Weyer, N. Donat, C. L’Heritier, F. Juilliard, G. Pauli, B. Soufflet, et al. Grass pollen hyposensitization versus placebo therapy. I. Clinical effectiveness and methodological aspects of a pre-seasonal course of desensitization with a four-grass pollen extract. Allergy. Jul;36(5):309–17.
H. P. Zenner, C. Baumgarten, G. Rasp, T. Fuchs, G. Kunkel, B. Hauswald, et al. Short-term immunotherapy: a prospective, randomized, double-blind, placebo-controlled multicenter study of molecular standardized grass and rye allergens in patients with grass pollen-induced allergic rhinitis. J Allergy Clin Immunol. Jul;100(1):23–9.
Alternative novel approaches for immunotherapy
Casale TB, Busse WW, Kline JN, Ballas ZK, Moss MH, Townley RG, Mokhtarani M, Seyfert-Margolis V, Asare A, Bateman K, Deniz Y; Immune Tolerance Network Group Omalizumab pretreatment decreases acute reactions after rush immunotherapy for ragweed-induced seasonal allergic rhinitis. J Allergy Clin Immunol. 2006;117:134-40.
Creticos PS1, Schroeder JT, Hamilton RG, Balcer-Whaley SL, Khattignavong AP, Lindblad R, Li H, Coffman R, Seyfert V, Eiden JJ, Broide D; Immune Tolerance Network Group. Immunotherapy with a ragweed-toll-like receptor 9 agonist vaccine for allergic rhinitis. N Engl J Med. 2006 Oct 5;355(14):1445-55.
Drachenberg KJ, Wheeler AW, Stuebner P, Horak F. A well-tolerated grass pollenspecific allergy vaccine containing a novel adjuvant, monophosphoryl lipid A, reduces allergic symptoms after only four preseasonal injections. Allergy 2001;56:498–505.
Drachenberg KJ, Heinzkill M, Urban E, Woroniecki SR. Efficacy and tolerability of short-term specific immunotherapy with pollen allergoids adjuvanted by monophosphoryl lipid A (MPL) for children and adolescents. Allergol Immunopathol (Madr). 2003;31(5):270-7.
Ellis AK, Frankish CW, O'Hehir RE, Armstrong K, Steacy L, Larché M, Hafner RP.Treatment with grass allergen peptides improves symptoms of grass pollen-induced allergic rhinoconjunctivitis. J Allergy Clin Immunol. 2017 Feb 15. pii: S0091-6749(17)30037-4. doi: 10.1016/j.jaci.2016.11.043.
Jutel M, Jaeger L, Suck R, Meyer H, Fiebig H, Cromwell O. Allergen-specific immunotherapy with recombinant grass pollen allergens. J Allergy Clin Immunol 2005 ;116:608-13.
Larenas-Linnemann D, Wahn U, Kopp M. Use of omalizumab to improve desensitization safety in allergen immunotherapy. J Allergy Clin Immunol 2014; 133(3): 937-937.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 53
Patel D, Couroux P, Hickey P, Salapatek AM, Laidler P, Larché M, Hafner RP. Fel d 1-derived peptide antigen desensitization shows a persistent treatment effect 1 year after the start of dosing: a randomized, placebo-controlled study. J Allergy Clin Immunol 2013; 131:103-9.
Pauli G, Larsen TH, Rak S, Horak F, Pastorello E, Valenta R, Purohit A, Arvidsson M, Kavina A, Schroeder JW, Mothes N, Spitzauer S, Montagut A, Galvain S, Melac M, André C, Poulsen LK, Malling HJ. Efficacy of recombinant birch pollen vaccine for the treatment of birch-allergic rhinoconjunctivitis.J Allergy Clin Immunol. 2008;122:951-60.
Pfaar O, Cazan D, Klimek L, Larenas-Linnemann D, Calderon MA (2012) Adjuvants for immunotherapy. Curr Opin Allergy Clin Immunol 12: 648-657
Rolinck-Werninghaus C, Hamelmann E, Keil T, Kulig M, Koetz K, Gerstner B, Kuehr J, Zielen S, Schauer U, Kamin W, Von Berg A, Hammermann J, Weinkauf B, Weidinger G, Stenglein S, Wahn U; The co-seasonal application of anti-IgE after preseasonal specific immunotherapy decreases ocular and nasal symptom scores and rescue medication use in grass pollen allergic children. Omalizumab Rhinitis Study Group. Allergy;2004;59:973-9.
Senti G, von Moos S, Tay F, Graf N, Sonderegger T, Johansen P, Kündig TM. Epicutaneous allergen-specific immunotherapy ameliorates grass pollen-induced rhinoconjunctivitis: A double-blind, placebo-controlled dose escalation study. J Allergy Clin Immunol. 2012;129:128-35.
Slovick A1, Douiri A2, Muir R3, Guerra A4, Tsioulos K4, Hay E4, Lam EP4, Kelly J5, Peacock JL2, Ying S4, Shamji MH6, Cousins DJ7, Durham SR6, Till SJ8 Intradermal grass pollen immunotherapy increases TH2 and IgE responses and worsens respiratory allergic symptoms. J Allergy Clin Immunol. 2016 Oct 20. pii: S0091-6749(16)31186-1. doi: 10.1016/j.jaci.2016.09.024.
Senti G, Crameri R, Kuster D, Johansen P, Martinez-Gomez JM, Graf N, Steiner M, Hothorn LA, Grönlund H, Tivig C, Zaleska A, Soyer O, van Hage M, Akdis CA, Akdis M, Rose H, Kündig TM. Intralymphatic immunotherapy for cat allergy induces tolerance after only 3 injections. J Allergy Clin Immunol. 2012;129:1290-6.
Spertini F, DellaCorte G, Kettner A, de Blay F, Jacobsen L, Jutel M, Worm M, Charlon V, Reymond C.Efficacy of 2 months of allergen-specific immunotherapy with Bet v 1-derived contiguous overlapping peptides in patients with allergic rhinoconjunctivitis: Results of a phase IIb study. J Allergy Clin Immunol. 2016 Jul;138(1):162-8. doi: 10.1016/j.jaci.2016.02.044. Epub 2016 May 6.
Witten M, Malling HJ, Blom L, Poulsen BC, Poulsen LK. Is intralymphatic immunotherapy ready for clinical use in patients with grass pollen allergy?J Allergy Clin Immunol. 2013;132:1248-1252.Intralymphatic immunotherapy for cat allergy induces tolerance after only 3 injections.
Zieglmayer P, Focke-Tejkl M, Schmutz R, Lemell P, Zieglmayer R, Weber M, Kiss R, Blatt K, Valent P, Stolz F, Huber H, Neubauer A, Knoll A, Horak F, Henning R, Valenta R. Mechanisms, safety and efficacy of a B cell epitope-based vaccine for immunotherapy of grass pollen allergy.EBioMedicine. 2016 Sep;11:43-57. doi: 10.1016/j.ebiom.2016.08.022.
Allergen factors that affect the efficacy of AIT
Amar SM, Harbeck RJ, Sills M, Silveira LJ, O'Brien H, Nelson HS Response to sublingual immunotherapy with grass pollen extract: monotherapy versus combination in a multiallergen extract.J Allergy Clin Immunol. 2009 Jul;124(1):150-156.e1-5. doi: 10.1016/j.jaci.2009.04.037. Epub 2009 Jun 11.
Bergmann KC, Demoly P, Worm M, Fokkens WJ, Carrillo T, Tabar AI, et al. Efficacy and safety of sublingual tablets of house dust mite allergen extracts in adults with allergic rhinitis. J Allergy Clin Immunol. 2014;133(6):1608-14 e6.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 54
Coop CA. Immunotherapy for Mold Allergy. Clin Rev Allergy Immunol. 2014;47(3):289-98.
Cortellini G, Spadolini I, Patella V, Fabbri E, Santucci A, Severino M, et al. Sublingual immunotherapy for Alternaria-induced allergic rhinitis: A randomized placebo-controlled trial. Ann Allergy Asthma Immunol. 2010;105(5):382-6.
Davies JM. Grass pollen allergens globally: The contribution of subtropical grasses to burden of allergic respiratory diseases. Clin Exp Allergy. 2014;44(6):790-801.
Davies JM, Li H, Green M, Towers M, Upham JW. Subtropical grass pollen allergens are important for allergic respiratory diseases in subtropical regions. Clin Transl Allergy. 2012;2(1).
Demoly P, Emminger W, Rehm D, Backer V, Tommerup L, Kleine-Tebbe J. Effective treatment of house dust mite-induced allergic rhinitis with 2 doses of the SQ HDM SLIT-tablet: Results from a randomized, double-blind, placebo-controlled phase III trial. J Allergy Clin Immunol. 2016;137(2):444-51 e8.
Didier A, Worm M, Horak F, Sussman G, de Beaumont O, Le Gall M, Melac M, Malling HJ.Sustained 3-year efficacy of pre- and coseasonal 5-grass-pollen sublingual immunotherapy tablets in patients with grass pollen-induced rhinoconjunctivitis. J Allergy Clin Immunol. 2011 Sep;128(3):559-66. doi: 10.1016/j.jaci.2011.06.022
Didier A, Worm M, Horak F, Sussman G, de Beaumont O, Le Gall M, Melac M, Malling HJ.Sustained 3-year efficacy of pre- and coseasonal 5-grass-pollen sublingual immunotherapy tablets in patients with grass pollen-induced rhinoconjunctivitis. J Allergy Clin Immunol. 2011 Sep;128(3):559-66. doi: 10.1016/j.jaci.2011.06.022
Dreborg S, Agrell B, Foucard T, Kjellman NI, Koivikko A, Nilsson S. A double-blind, multicenter immunotherapy trial in children, using a purified and standardized cladosporium herbarum preparation. Clinical results. Allergy. 1986;41(2):131European Medicines Agency. Guideline on allergen products: production and quality issues. London; 2008 EMEA/CHMP/BWP/304831/2007. http:// www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003333.pdf.
Grendelmeier P. Pollen as the cause of allergies. Ther Umsch. 2001;58(5):285-91.
Guerra F, Galan Carmen C, Daza JC, Miguel R, Moreno C, Gonzalez J, et al. Study of sensitivity to the pollen of Fraxinus spp. (Oleaceae) in Cordoba, Spain. J INVEST ALLERGOL CLIN IMMUNOL. 1995;5(3):166-70.
Hordijk GJ, Antvelink JB, Luwema RA. Sublingual immunotherapy with a 54tandardized grass pollen extract; a double-blind placebo-controlled study. Allergol Immunopathol (Madr). 1998;26(5):234-40.
Horst M, Hejjaoui A, Horst V, Michel FB, Bousquet J. Double-blind, placebo-controlled rush immunotherapy with a standardized Alternaria extract. J ALLERGY CLIN IMMUNOL. 1990;85(2):460-72.
Kuna P, Kaczmarek J, Kupczyk M. Efficacy and safety of immunotherapy for allergies to Alternaria 54tandardi in children. J Allergy Clin Immunol. 2011;127(2):502-8.e6.
Laurent J, Guinnepain MT, Sauvaget J, Lafay M. Allergy to ash (Fraxinus excelsior L.) pollen in Paris. Rev Fr Allergol Immunol Clin. 1998;38(2):89-93.
Lizaso MT, Martínez A, Asturias JA, Algorta J, Madariaga B, Labarta N, et al. Biological standardization and maximum tolerated dose estimation of an Alternaria 54tandardi allergenic extract. J Invest Allergol Clin Immunol. 2006;16(2):94-103.
Markmann S, Groeger M, Becker S, Kramer M. Relevance of Ash pollen allergy in the Munich area. Allergy Eur J Allergy Clin Immunol. 2012;67:628.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 55
Mosbech H, Deckelmann R, de Blay F, Pastorello EA, Trebas-Pietras E, Andres LP, et al. Standardized quality (SQ) house dust mite sublingual immunotherapy tablet (ALK) reduces inhaled corticosteroid use while maintaining asthma control: a randomized, double-blind, placebo-controlled trial. J Allergy Clin Immunol. 2014;134(3):568-75 e7.
Pfaar O e.a. Allergy 2013;68:1306-13
Radcliffe MJ, Lewith GT, Turner RG, Prescott P, Church MK, Holgate ST. Enzyme potentiated 55tandardized55on in treatment of seasonal allergic rhinitis: double blind 55tandardiz controlled study. BMJ. 2003;327(7409):251-4.
Ravi S. Swamy, MDb, ∗ , Neha Reshamwala, MDc, ∗ , Tessa Hunter, BSca, Soujanya Vissamsetti, MDa, Carah B. Santos, MDa, Fuad M. Baroody, MDd, Peter H. Hwang, MDb, Elisabeth G. Hoyte, NPa, Marco A. Garcia, BSca, Kari C. Nadeau, MD, PhDa, Epigenetic modifications and improved regulatory T-cell function in subjects undergoing dual sublingual immunotherapy. Journal of Allergy and Clinical Immunology Volume 130, Issue 1, July 2012, Pages 215–224.e7
Slater JE, Zoch A, Newman-Gerhardt S, Khurana T. Comparison of total protein profile of alternaria 55tandardi extract obtained from various U.S. Allergenic extract manufacturers. J Allergy Clin Immunol. 2014;133(2):AB100.
Tabar AI, Lizaso MT, García BE, Gómez B, Echechipía S, Aldunate MT, et al. Double-blind, placebo-controlled study of Alternaria 55tandardi immunotherapy: Clinical efficacy and safety. Pediatr Allergy Immunol. 2008;19(1):67-75.
Twaroch TE, Curin M, Valenta R, Swoboda I. Mold allergens in respiratory allergy: From structure to therapy. Allergy Asthma Immunol Res. 2015;7(3):205-20.
-40.
Van Niekerk CH, De Wet JI. Efficacy of grass-maize pollen oral immunotherapy in patients with seasonal hay-fever: a double-blind study. Clin Allergy. 1987;17(6):507-13.
Wüthrich B. Ash is not ash. Allergologie. 2006;29(6):231-5.
Patient factors
Agostinis F, Tellarini L, Canonica GW, Falagiani P, Passalacqua G. Safety of sublingual immunotherapy with a monomeric allergoid in very young children. Allergy 2005;60:133.
Arroabarren E, Tabar AI, Echechipía S, Cambra K, García BE, Alvarez-Puebla MJ Optimal duration of allergen immunotherapy in children with dust mite respiratory allergy. Pediatr Allergy Immunol 2015;26:34-41.
Amar, Sheila M et al. 2009. “Response to Sublingual Immunotherapy with Grass Pollen Extract: Monotherapy versus Combination in a Multiallergen Extract.” The Journal of allergy and clinical immunology 124(1): 150–56.e1–5.
Bousquet, J et al. 1991. “Differences in Clinical and Immunologic Reactivity of Patients Allergic to Grass Pollens and to Multiple-Pollen Species. II. Efficacy of a Double-Blind, Placebo-Controlled, Specific Immunotherapy with Standardized Extracts.” The Journal of allergy and clinical immunology 88(1): 43–53.
Bousquet, Philippe Jean et al. 2010. “Assessment of Allergen Sensitization in a General Population-Based Survey (European Community Respiratory Health Survey I).” Annals of Epidemiology 20: 797–803.
Calderón, Moisés A. et al. 2012. “Multiple-Allergen and Single-Allergen Immunotherapy Strategies in Polysensitized Patients: Looking at the Published Evidence.” The Journal of allergy and clinical immunology 129(4): 929–34.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 56
K. Chaudhuri, , J. Gonzales, C.A. Jesurun, M.T. Ambat, S. Mandal-Chaudhuri. Anaphylactic shock in pregnancy: a case study and review of the literature. International Journal of Obstetric Anesthesia Volume 17, Issue 4, October 2008, Pages 350–357
Cox L, Nelson H, Lockey R, Calabria C, Chacko T, Finegold I, et al. Allergen immunotherapy: a practice parameter third update. J Allergy Clin Immunol. 2011;127(1 Suppl):S1-55.
Craig, Timothy J et al. 2008. “Aeroallergen Sensitization Correlates with PC(20) and Exhaled Nitric Oxide in Subjects with Mild-to-Moderate Asthma.” The Journal of allergy and clinical immunology 121(3): 671–77.
Des Roches A, Paradis L, Menardo JL, Bouges S, Daures JP, Bousquet J. Immunotherapy with a standardized dermatophagoides pteronyssinus extract. VI. Specific immunotherapy prevents the onset of new sensitizations in children. J Allergy Clin Immunol 1997, 99:450–453.
Drachenberg, K. J., P. Pfeiffer, and E. Urban. “Sublingual immunotherapy-Results from a multi-centre, 56tandardiz, double-blind, placebo-controlled, study with a 56tandardized birch and grass/rye pollen extract.” Allergologie 24.11 (2001): 525-534.
European Medicines Agency. Guideline on allergen products: production and quality issues. London; 2008 EMEA/CHMP/BWP/304831/2007. http:// www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2009/09/WC500003333.pdf.
Fiocchi A, Pajno G, La Grutta S, Pezzuto F, Incorvaia C, Sensi L, et al. Safety of sublingual –swallow immunotherapy in children aged 3- to 7 years. Ann Allergy Asthma Immunol 2005;95:254-58.
Jacobsen L, Niggemann B, Dreborg S, Ferdousi HA, Halken S, Høst A et al. Specific immunotherapy has long-term preventive effect of seasonal and perennial asthma: 10- year follow-up on the PAT study. Allergy 2007;62:943–948.
W.James Metzger, M.D., Elaine Turner, M.D., Roy Patterson, M.D, J All Clin Immunol 1978; 61(4):268-272
Jutel M, Agache I, Bonini S, Burks AW, Calderon M, Canonica W et al. International consensus on allergy immunotherapy. J Allergy Clin Immunol 2015;136:556-68.
Kim, Kyung Won et al. 2006. “Comparison of Allergic Indices in Monosensitized and Polysensitized Patients with Childhood Asthma.” Journal of Korean medical science 21(6): 1012–16.
Lorenz AR, Lüttkopf D, May S, Scheurer S, Vieths S. The principle of homologous groups in regulatory affairs of allergen products—a proposal. Int Arch Allergy Immunol. 2009;148:1–17.
Migueres, Michel et al. 2014. “Types of Sensitization to Aeroallergens: Definitions, Prevalences and Impact on the Diagnosis and Treatment of Allergic Respiratory Disease.” Clinical and translational allergy 4: 16.
Moller C, Dreborg S, Ferdousi HA, Halken S, Høst A, Jacobsen L et al. Pollen immunotherapy reduces the development of asthma in children with seasonal rhinoconjunctivitis (the PAT-study). J Allergy Clin Immunol 2002;109:251–256. 61.
Nelson, Harold S. 2009. “Multiallergen Immunotherapy for Allergic Rhinitis and Asthma.” The Journal of allergy and clinical immunology 123(4): 763–69.
Oykhman P, Kim HL, Ellis AK. Allergy Asthma Clin Immunol. 2015 Nov 10;11:31. doi: 10.1186/s13223-015-0096-7
Pajno GB, Caminiti L, Crisafulli G, Barberi S, Landi M, Aversa T, Valenzise M, Passalacqua G. Adherence to sublingual immunotherapy in preschool children. Pediatr Allergy Immunol 2012; 23: 688-689.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 57
Pajno GB, Caminiti L, Passalacqua G. Changing the route of immunotherapy administration: an 18-year survey in pediatric patients with allergic rhinitis and asthma. Allergy Asthma Proc 2013;34:523-6.
Passalacqua G, Compalati E, Canonica GW. Sublingual Immunotherapy: Clinical Indications in the WAO-SLIT Position Paper. World Allergy Organ J. 2010 ;3:216-9.
Pfaar, O. et al. 2013. “Depigmented-Polymerized Mixed Grass/birch Pollen Extract Immunotherapy Is Effective in Polysensitized Patients.” Allergy: European Journal of Allergy and Clinical Immunology 68(10): 1306–13.
Roberts G, Hurley C, Turcanu V, Lack G. Grass pollen immunotherapy as an effective therapy for childhood seasonal allergic asthma. J Allergy Clin Immunol. 2006;117:263-8.
IV. Shao J, Cui YX, Zheng YF, Peng HF, Zheng ZL, Chen JY, Li Q, Cao LF. Efficacy and safety of sublingual immunotherapy in children aged 3-13 years with allergic rhinitis. Am J Rhinol Allergy 2014; 28: 131-9.
Shaikh WA, Shaikh SW. A prospective study on the safety of sublingual immunotherapy in pregnancy. Allergy. 2012 Jun;67(6):741-3. doi: 10.1111/j.1398-9995.2012.02815.x. Epub 2012 Apr 5.
Slavin RG. Special considerations in treatment of allergic rhinitis in the elderly: role of intranasal corticosteroids. Allergy Asthma Proc. 2010;31(3):179–84.
How long
Ali I, Goksal K, Ozan B, Gulsen D. Long-term allergen-specific immunotherapy correlates with long-term allergen-specific immunological tolerance. Adv Ther. 2008 Jan;25(1):29-36.
Arroabarren E, Tabar AI, Echechipía S, Cambra K, García BE, Alvarez-Puebla MJ. Optimal duration of allergen immunotherapy in children with dust mite respiratory allergy. Pediatr Allergy Immunol. 2015 Feb;26(1):34-41.
Ariano R, Kroon AM, Augeri G, Canonica GW, Passalacqua G. Long-term treatment with allergoid immunotherapy with Parietaria. Clinical and immunologic effects in a randomized, controlled trial. Allergy. 1999 Apr;54(4):313-9.
Cools M, Van Bever HP, Weyler JJ, Stevens WJ. Long-term effects of specific immunotherapy, administered during childhood, in asthmatic patients allergic to either house-dust mite or to both house-dust mite and grass pollen. Allergy. 2000 Jan;55(1):69-73.
Cox L, Cohn JR. Duration of allergen immunotherapy in respiratory allergy: when is enough, enough? Ann Allergy Asthma Immunol. 2007 May;98(5):416-26.
Durham SR, Yang WH, Pedersen MR, Johansen N, Rak S. Sublingual immunotherapy with once-daily grass allergen tablets: a randomized controlled trial in seasonal allergic rhinoconjunctivitis. J Allergy Clin Immunol. 2006 Apr;117(4):802-9.
Ebner C, Kraft D, Ebner H. Booster immunotherapy (BIT). Allergy 1994; 49(1): 38-42.
Frati F , Dell’Albani I, Incorvaia C. Long-term efficacy of allergen immunotherapy: what do we expect? Immunotherapy. 2013 Feb;5(2):131-3.
Hedlin G, Heilborn H, Lilja G, Norrlind K, Pegelow KO, Schou C, Løwenstein H. Long-term follow-up of patients treated with a three-year course of cat or dog immunotherapy. J Allergy Clin Immunol. 1995 Dec;96(6 Pt 1):879-85.
Lin Z, Liu Q, Li T, Chen D, Chen D, Xu R. The effects of house dust mite sublingual immunotherapy in patients with allergic rhinitis according to duration. Int Forum Allergy Rhinol. 2016 Jan;6(1):82-7.
https://www.ncbi.nlm.nih.gov/pubmed/?term=Li%2520T%255BAuthor%255D&cauthor=true&cauthor_uid=26575696

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 58
Marogna M, Spadolini I, Massolo A, Canonica GW, Passalacqua G. Long-lasting effects of sublingual immunotherapy according to its duration: a 15-year prospective study. J Allergy Clin Immunol 2010; 126(5): 969-75.
Meadows A, Kaambwa B, Novielli N, Huissoon A, Fry-Smith A, Meads C, Barton P, Dretzke J. A systematic review and economic evaluation of subcutaneous and sublingual allergen immunotherapy in adults and children with seasonal allergic rhinitis. Health Technol Assess. 2013 Jul;17(27):vi, xi-xiv, 1-322.
Naclerio RM, Proud D, Moylan B, et al. A double-blind study of the discontinuation of ragweed immunotherapy. J Allergy Clin Immunol 1997; 100:293-300.
Ott H, Sieber J, Brehler R, Fölster-Holst R, Kapp A, Klimek L, Pfaar O, Merk H. Efficacy of grass pollen sublingual immunotherapy for three consecutive seasons and after cessation of treatment: the ECRIT study. Allergy. 2009 Sep;64(9):1394-401.
Stelmach I, Sobocińska A, Majak P, Smejda K, Jerzyńska J, Stelmach W. Comparison of the long-term efficacy of 3- and 5-year house dust mite allergen immunotherapy. Ann Allergy Asthma Immunol. 2012 Oct;109(4):274-8.
Adverse events with AIT for allergic rhinoconjunctivitis
SCIT
Alvarez-Cuesta E, Bousquet J, Canonica GW, Durham SR, Malling HJ, Valovirta E. Standards for practical allergen-specific immunotherapy. Allergy 2006;61 Suppl 82:1–20.
Amin HS, Liss GM, Bernstein DI: Evaluation of near-fatal reactions to allergen immunotherapy injections. J Allergy Clin Immunol. 2006, 117: 169-175. 10.1016/j.jaci.2005.10.010.
Bernstein DI, Wanner M, Borish L, Liss GM: Twelve-year survey of fatal reactions to allergen injections and skin testing: 1990-2001. J Allergy Clin Immunol. 2004, 113: 1129-1136. 10.1016/j.jaci.2004.02.006.
Bernstein DI, JACI 2004; 113: 1129-36Cox L, Larenas-Linnemann D, Lockey RF, Passalacqua G. Speaking the same language: The World Allergy Organization Subcutaneous Immunotherapy Systemic Reaction Grading System. J Allergy Clin Immunol. 2010 Mar;125(3):569-74, 574.e1-574
Bernstein DI, Wanner M, Borish L, Liss GM, Immunotherapy Committee AaoAA, and Immunology: Twelve-year survey of fatal reactions to allergen injections and skin testing: 1990-2001. J Allergy Clin Immunol 2004; 113, 1129Burks AW, Calderon MA, Casale T et al. Update on allergy immunotherapy: American Academy of Allergy, Asthma & Immunology/European Academy of Allergy and Clinical Immunology/PRACTALL consensus report. J Allergy Clin Immunol 2013;131:1288–96.e3.
Calabria CW. Accelerated immunotherapy schedules. Curr Allergy Asthma Rep 2013;13:389–98.
Calabria CW, Cox L. Accelerated immunotherapy schedules and premedication. Immunol Allergy Clin North Am 2011;31:251–63, ix.
Cox L, Calderon M, Pfaar O. Subcutaneous allergen immunotherapy for allergic disease: examining efficacy, safety and cost-effectiveness of current and novel formulations. Immunotherapy 2012;4:601–16.
Cox L, Larenas-Linnemann D, Lockey RF, Passalacqua G. Speaking the same language: The World Allergy Organization subcutaneous immunotherapy systemic reaction grading system. J Allergy Clin Immunol 2010;125:569–74,574.e1–574.e7.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 59
Epstein TG, Liss GM, Murphy-Berendts K, Bernstein DI. Risk factors for fatal and nonfatal reactions to subcutaneous immunotherapy: National surveillance study on allergen immunotherapy (2008-2013). Ann Allergy Asthma Immunol 2016; 116: 354-359.e2.
T.G. Epstein, G.M. Liss, K. Murphy-Berendts, D.I. Bernstein. Immediate and delayed-onset systemic reactions after subcutaneous immunotherapy injections: ACAAI/AAAAI surveillance study of subcutaneous immunotherapy: year 2. Ann Allergy Asthma Immunol, 107 (2011), pp. 426–431.e1
Epstein TG, Liss GM, Murphy-Berendts K, Bernstein DI. AAAAI and ACAAI surveillance study of subcutaneous immunotherapy, year 3: what practices modify the risk of systemic reactions? Ann Allergy Asthma Immunol 2013;110:274–8, 278.e1.
-36.
Frost L, Johansen P, Pedersen S, Veien N, Ostergaard PA, Nielsen MH. Persistent subcutaneous nodules in children hyposensitized with aluminium-containing allergen extracts. Allergy 1985;40:368–72.
Kelso JM. The rate of systemic reactions to immunotherapy injections is the same whether or not the dose is reduced after a local reaction. Ann Allergy Asthma Immunol 2004;92:225–7.
Lockey RF et. Al, Ann Allergy Asthma Immunol 2001; 87: 47-77
Malling HJ. Minimising the risks of allergen-specific injection immunotherapy. Drug Saf 2000;23:323–32.
Netterlid E, Hindsén M, Björk J et al. There is an association between contact allergy to aluminium and persistent subcutaneous nodules in children undergoing hyposensitization therapy. Contact Dermatitis 2009;60:41–9.
Nielsen L, Johnsen CR, Mosbech H, Poulsen LK, Malling HJ. Antihistamine premedication in specific cluster immunotherapy: a double-blind, placebo-controlled study. J Allergy Clin Immunol 1996;97:1207–13.
Passalacqua G, Baena-Cagnani CE, Bousquet J, Canonica GW, Casale TB, Cox L, Durham SR, Larenas-Linnemann D, Ledford D, Pawankar R, Potter P, Rosario N, Wallace D, Lockey RF.Grading local side effects of sublingual immunotherapy for respiratory allergy: speaking the same language. J Allergy Clin Immunol. 2013 Jul;132(1):93-8
Pfaar O, Bachert C, Bufe A, Buhl R, Ebner C, Eng P, et al. Guideline on allergen-specific immunotherapy in IgE-mediated allergic diseases: S2k Guideline of the German Society for Allergology and Clinical Immunology (DGAKI), the Society for Pediatric Allergy and Environmental Medicine (GPA), the Medical Association of German Allergologists (AeDA), the Austrian Society for Allergy and Immunology (ÖGAI), the Swiss Society for Allergy and Immunology (SGAI), the German Society of Dermatology (DDG), the German Society of Oto- Rhino-Laryngology, Head and Neck Surgery (DGHNO-KHC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Pneumology (GPP), the German Respiratory Society (DGP), the German Association of ENT Surgeons (BV-HNO), the Professional Federation of Paediatricians and Youth Doctors (BVKJ), the Federal Association of Pulmonologists (BDP) and the German Dermatologists Association (BVDD). Allergo J Int. 2014;23(8):282-319.
Ragusa FV, Passalacqua G, Gambardella R et al. Nonfatal systemic reactions to subcutaneous immunotherapy: a 10-year experience. J Investig Allergol Clin Immunol 1997;7:151–4.
Reimers A, Hari Y, Müller U. Reduction of side-effects from ultrarush immunotherapy with honeybee venom by pretreatment with fexofenadine: a double-blind, placebo-controlled trial. Allergy 2000;55:484–8.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 60
Vogelbruch M, Nuss B, Körner M, Kapp A, Kiehl P, Bohm W. Aluminium-induced granulomas after inaccurate intradermal hyposensitization injections of aluminium-adsorbed depot preparations. Allergy 2000;55:883–7.
Wedi B, Rueff F. [Pharmacoprophylaxis and co-medications in allergen-specific immunotherapy]. Hautarzt 2011; 62:663–70.
SLIT
Alvarez-Cuesta E, Bousquet J, Canonica GW, Durham SR, Malling HJ, Valovirta E. Standards for practical allergen- specific immunotherapy. Allergy 2006;61 Suppl 82:1–20.
Blaiss M1, Maloney J, Nolte H, Gawchik S, Yao R, Skoner DP.Efficacy and safety of timothy grass allergy immunotherapy tablets in North American children and adolescents. J Allergy Clin Immunol. 2011 Jan;127(1):64-71, 71.e1-4. doi: 10.1016/j.jaci.2010.11.034.
Canonica GW, Cox L, Pawankar R et al. Sublingual immunotherapy: World Allergy Organization position paper 2013 update. The World Allergy Organization journal 2014;7:6.
Cox LS, Larenas Linnemann D, Nolte H, Weldon D, Finegold I, Nelson HS. Sublingual immunotherapy: a comprehensive review. J Allergy Clin Immunol 2006;117:1021–35.
Calderon MA, Simons FE, Malling HJ, Lockey RF, Moingeon P, Demoly P. Sublingual allergen immunotherapy: mode of action and its relationship with the safety profile. Allergy 2012;67:302–11.
M.A. Calderón, F.E.R. Simons, H.-J. Malling, R.F. Lockey, P. Moingeon, P. Demoly. Sublingual allergen immunotherapy: mode of action and its relationship with the safety profile. Allergy, 67 (2012), pp. 302–311
Calderón MA, Larenas D, Kleine-Tebbe J, Jacobsen L, Passalacqua G, Eng PA, Varga EM, Valovirta E, Moreno C, Malling HJ, Alvarez-Cuesta E, Durham S, Demoly P. Allergy. 2011 Oct;66(10):1345-59. doi: 10.1111/j.1398-9995.2011.02669.x. Epub 2011 Jun 28.
Cox LS, Larenas Linnemann D, Nolte H, Weldon D, Finegold I, Nelson HS: Sublingual immunotherapy: a comprehensive review. J Allergy Clin Immunol. 2006, 117: 1021-1035. 10.1016/j.jaci.2006.02.040.
Dahl R1, Kapp A, Colombo G, de Monchy JG, Rak S, Emminger W, Rivas MF, Ribel M, Durham SR Efficacy and safety of sublingual immunotherapy with grass allergen tablets for seasonal allergic rhinoconjunctivitis.J Allergy Clin Immunol. 2006 Aug;118(2):434-40.
Didier A1, Malling HJ, Worm M, Horak F, Jäger S, Montagut A, André C, de Beaumont O, Melac M. Optimal dose, efficacy, and safety of once-daily sublingual immunotherapy with a 5-grass pollen tablet for seasonal allergic rhinitis. J Allergy Clin Immunol. 2007 Dec;120(6):1338-45. Epub 2007 Nov 1.
Epstein TG1, Liss GM2, Murphy-Berendts K3, Bernstein DI4. Risk factors for fatal and nonfatal reactions to subcutaneous immunotherapy: National surveillance study on allergen immunotherapy (2008-2013). Ann Allergy Asthma Immunol. 2016 Apr;116(4):354-359.e2. doi: 10.1016/j.anai.2016.02.001. Epub 2016 Mar 3.
European Academy of Allergy and Clinical Immunology task force report on 'dose-response relationship in allergen-specific immunotherapy'.
Lüderitz-Püchel U, Keller-Stanislawski B, Haustein D. [Risk reevaluation of diagnostic and therapeutic allergen extracts. An analysis of adverse drug reactions from 1991 to 2000]. Bundesgesundheitsbl Gesundheitsforsch Gesundheitsschutz 2001;44:709–18.
Mosbech H1, Deckelmann R2, de Blay F3, Pastorello EA4, Trebas-Pietras E5, Andres LP6, Malcus I7, Ljørring C8, Canonica GW9Standardized quality (SQ) house dust mite sublingual immunotherapy tablet (ALK) reduces inhaled corticosteroid use while maintaining asthma

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 61
control: a randomized, double-blind, placebo-controlled trial. J Allergy Clin Immunol. 2014 Sep;134(3):568-575.e7. doi: 10.1016/j.jaci.2014.03.019. Epub 2014 May 3.
Passalacqua G, Garelli V, Sclifo F, Canonica GW. Sublingual immunotherapy for allergic rhinitis and conjunctivitis. Immunotherapy 2013;5:257–64Radulovic S, Calderon MA, Wilson D, Durham S. Sublingual immunotherapy for allergic rhinitis. Cochrane Database Syst Rev 2010;(12):CD002893.
Passalacqua G, Baena-Cagnani CE, Bousquet J et al. Grading local side effects of sublingual immunotherapy for respiratory allergy: speaking the same language. J Allergy Clin Immunol 2013;132:93–8.
Wahn U1, Tabar A, Kuna P, Halken S, Montagut A, de Beaumont O, Le Gall M; SLIT Study Group. Efficacy and safety of 5-grass-pollen sublingual immunotherapy tablets in pediatric allergic rhinoconjunctivitis. J Allergy Clin Immunol. 2009 Jan;123(1):160-166.e3. doi: 10.1016/j.jaci.2008.10.009. Epub 2008 Nov 29.
Adherence
Egert-Schmidt AM, Kolbe JM, Mussler S, Thum-Oltmer S. Patients' compliance with different administration routes for allergen immunotherapy in Germany. Patient Prefer Adherence. 2014 Oct 24;8:1475-81.
Incorvaria—Incorvaia C, Masieri S, Berto P, Scurati S, Frati F. Specific immunotherapy by the sublingual route for respiratory allergy. Allergy Asthma Clin Immunol. 2010 Nov 9;6(1):29.
Leader BA, Rotella M, Stillman L, DelGaudio JM, Patel ZM, Wise SK. Immunotherapy compliance: comparison of subcutaneous versus sublingual immunotherapy. Int Forum Allergy Rhinol. 2016 May; 6(5):460-4.
Makatsori M, Scadding GW, Lombardo C, Bisoffi G, Ridolo E, Durham SR, Senna G. Dropouts in sublingual allergen immunotherapy trials – a systematic review. Allergy 2014; 69: 571–580.
Pascal Demoly, Giovanni Passalacqua, Oliver Pfaar, Joaquin Sastre, Ulrich Wahn. Patient engagement and patient support programs in allergy immunotherapy: a call to action for improving long-term adherence. Allergy Asthma Clin Immunol 2016; 12: 34.
Savi E, Peveri S, Senna G, Passalacqua G. Causes of SLIT discontinuation and strategies to improve the adherence: a pragmatic approach. Allergy. 2013 Sep;68(9):1193-5.
Scurati S, Frati F, Passalacqua G, Puccinelli P, Hilaire C, Incorvaia C; Italian Study Group on SLIT Compliance.. Adherence issues related to sublingual immunotherapy as perceived by allergists. Patient Prefer Adherence. 2010 Jun 24;4:141-5.-
Sondermann N, Shah-Hosseini K, Henkel K, Schwalfenberg A, Mösges R. [Factors of success for adherence in hyposensitization]. Allergologie 2011;34:441–6
Vaswani R, Garg A, Parikh L, Vaswani S. Non-adherence to subcutaneous allergen immunotherapy: inadequate health insurance coverage is the leading cause. Ann Allergy Asthma Immunol. 2015 Sep;115(3):241-3.
Pharmacoeconomic advantage of AIT versus pharmacotherapy
Ariano R, Berto P, Tracci D, et al. Pharmacoeconomics of allergen immunotherapy compared with symptomatic drug treatment in patients with allergic rhinitis and asthma. Allergy Asthma Proc 2006; 27:159–163
Ariano R, Berto P, Tracci D, Incorvaia C, Frati F. Pharmacoeconomics of allergen immunotherapy compared with symptomatic drug treatment in patients with allergic rhinitis and asthma. Allergy Asthma Proc 2006;27:159-63.

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 62
Bachert C, Vestenbaek U, Christensen J, Griffiths UK, Poulsen PB. Cost-effectiveness of grass allergen tablet (GRAZAX) for the prevention of seasonal grass pollen induced rhinoconjunctivitis—a Northern European perspective. Clin Exp Allergy 2007;37:772-9.
Berto P, Bassi M, Incorvaia C, et al. Cost effectiveness of sublingual immunotherapy in children with allergic rhinitis and asthma. Allerg Immunol (Paris) 2005; 37:303–308.
Berto P, Bassi M, Incorvaia C, et al. Cost effectiveness of sublingual immunotherapy in children with allergic rhinitis and asthma. Allerg Immunol (Paris) 2005; 37:303–308
Berto P, Frati F, Incorvaia C, Cadario G, Contiguglia R, Di Gioacchino M, et al. Comparison of costs of sublingual immunotherapy and drug treatment in grasspollen induced allergy: results from the SIMAP database study. Curr Med Res Opin 2008;24:261-6.
Berto P, Passalacqua G, Crimi N, Frati F, Ortolani C, Senna G, et al. Economic evaluation of sublingual immunotherapy vs symptomatic treatment in adults with pollen-induced respiratory allergy: the Sublingual Immunotherapy Pollen Allergy Italy (SPAI) study. Ann Allergy Asthma Immunol 2006;97: 615-21.
Creticos PS, Reed CE, Norman PS, Khoury J, Adkinson NF Jr, Buncher CR, et al. Ragweed immunotherapy in adult asthma. N Engl J Med 1996;334:501-6.
Hahn-Pedersen J, Worm M, Green W, Andreasen JN, Taylor M. Clin Transl Allergy. 2016 Sep 7;6(1):35. doi: 10.1186/s13601-016-0127-6. eCollection 2016. PMID: 27610217Hankin CS, Cox L, Lang D, Levin A, Gross G, Eavy G, et al. Allergy immuno- therapy among Medicaid-enrolled children with allergic rhinitis: patterns of care, resource use, and costs. J Allergy Clin Immunol 2008;121:227-32.
Hankin CS, Cox L, Lang D, Bronstone A, Fass P, Leatherman B, et al. Allergen immunotherapy and health care cost benefits for children with allergic rhinitis: a large-scale, retrospective, matched cohort study. Ann Allergy Asthma Immunol 2010;104:79-85.
Hankin CS, Cox L, Bronstone A, Wang Z. Allergy immunotherapy: reduced health care costs in adults and children with allergic rhinitis. J Allergy Clin Im- munol 2013;131:1084-91.
Keiding H, Jorgensen KP. A cost-effectiveness analysis of immunotherapy with SQ allergen extract for patients with seasonal allergic rhinoconjunctivitis in selected European countries. Curr Med Res Opin. May 2007;23(5):1113–20.
Petersen KD, Gyrd-Hansen D, Dahl R. Health-economic analyses of subcutaneous specific immunotherapy for grass pollen and mite allergy. Allergol Immunopathol (Madr) 2005;33:296-302.
Poulsen PB, Pedersen KM, Christensen J, Vestenbaek U. [Economic evaluation of a tablet-based vaccination against hay fever in Denmark]. Ugeskr Laeger. Jan 2008: 14;170(3):138–42.
Reinhold T, Brüggenjürgen B. Cost-effectiveness of grass pollen SCIT compared with SLIT and symptomatic treatment. Allergo J Int. 2017;26(1):7-15.
Ronaldson S, Taylor M, Bech PG, Shenton R, Bufe A. Economic evaluation of SQ-standardized grass allergy immunotherapy tablet (Grazax) in children. Clin Outcomes Res. Apr 2014;6(1):187–96.
Schadlich PK, Brecht JG. Economic evaluation of specific immunotherapy versus symptomatic treatment of allergic rhinitis in Germany. Pharmacoeconomics 2000;17:37-52.
Verheggen B, Westerhout K, Schreder C, Augustin M. Health economic comparison of SLIT allergen and SCIT allergoid immunotherapy in patients with seasonal grass-allergic rhinoconjunctivitis in Germany. Clin Transl Allergy. 2015;5(1).

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 63
Westerhout KY, Verheggen BG, Schreder CH, Augustin M. Cost effectiveness analysis of immunotherapy in patients with grass pollen allergic rhinoconjunctivitis in Germany. J Med Econ. 2012;15(5):906–917 12p.
Gaps
Pfaar O, Demoly P, Gerth van Wijk R, Bonini S, Bousquet J, et al. (2014) Recommendations for the
standardization of clinical outcomes used in allergen immunotherapy trials for allergic
rhinoconjunctivitis: an EAACI Position Paper. Allergy 69: 854-867.
Shamji MH, Kappen JH, Akdis M, Jensen-Jarolim E, Knol EF, et al. (2017) Biomarkers for monitoring
clinical efficacy of allergen immunotherapy for allergic rhinoconjunctivitis and allergic asthma: an EAACI
Position Paper. Allergy (Pfaar

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 64
Online supplement
Homologous allergen groups Reproduced from Table SA. From Demoly P 2016

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 65
Grading systems for adverse reactions We intended to use the WAO approach to grading adverse reactions. This proved impossible
as different authors have used different approaches to classifying these. This means that it is
difficult to synthesis the safety data and represents a gap.
Table SB

Rhinoconjunctivitis AIT guideline – draft Draft 1.0; 12th May 2017 66
Pfaar et al., Allergo J Int., 2014
Table SC
Pfaar et al., Allergo J Int., 2014