E-Learning Triple Negative Breast Cancer is Still an Unmet...
67
TRIPLE NEGATIVE BREAST CANCER IS STILL AN UNMET NEED Valentina Guarneri and Maria Vittoria Dieci University of Padova Istituto Oncologico Veneto IRCCS, Padova, Italy
Transcript of E-Learning Triple Negative Breast Cancer is Still an Unmet...

TRIPLE NEGATIVE BREAST CANCER IS STILL AN UNMET NEED
Valentina Guarneri and Maria Vittoria Dieci
University of Padova
Istituto Oncologico Veneto IRCCS, Padova, Italy

Introduction:
Definition, epidemiology, clinical behaviour
State of the art
Neoadjuvant/Adjuvant
Advanced disease
How to improve on CT
Heterogeneity: exploiting TNBC diversity to identify druggable pathways
OUTLINE

Triple negative breast cancer (TNBC) definition:
– lack of expression of estrogen receptor and progesterone receptor
HER2 not overexpressed/amplified
10-20% of all breast cancers
Most BRCAmut carriers develop TNBC
TNBC includes rare histologies
Metaplastic, medullary, adenoid cystic carcinoma
High cell proliferation, poor cellular differentiation, many recurrent copy number
imbalances, and mutations in the TP53
TNBC: INTRODUCTION
Triple negative breast cancer is the most lethal form of breast cancer
TNBC is heterogeneous and harbours several molecular alterations
The prevalence of TNBC is higher in women of Afro–American ethnicity
TNBC is more frequently diagnosed in younger women
Higher risk of earlier relapse
High risk for visceral involvement (CNS included)
Median survival from the time of developing metastases rarely >1 year
Endocrine therapy and anti-HER2 treatments are not effective; high
chemosensitivity
TNBC: INTRODUCTION

HAZARD RATES OF PROGRESSION
AND DEATH: TNBC VS. OTHERS
Liedtke C, et al., J Clin Oncol 2008;26;1275–81. Reprinted with permission. © 2008 American Society of Clinical Oncology. All rights reserved.
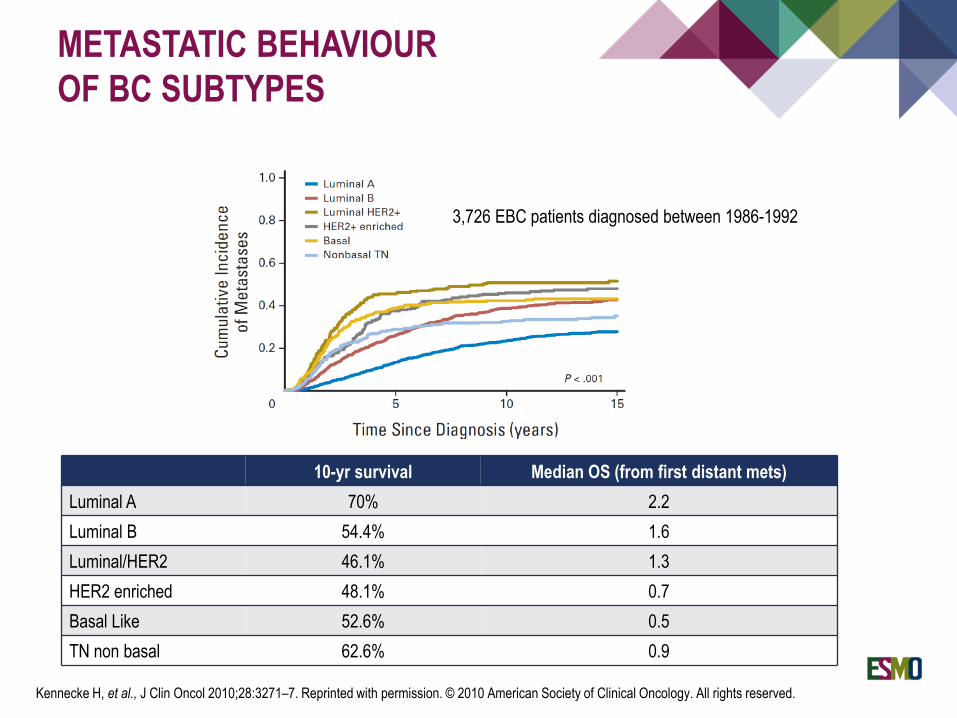
3,726 EBC patients diagnosed between 1986-1992
10-yr survival Median OS (from first distant mets)
Luminal A 70% 2.2
Luminal B 54.4% 1.6
Luminal/HER2 46.1% 1.3
HER2 enriched 48.1% 0.7
Basal Like 52.6% 0.5
TN non basal 62.6% 0.9
METASTATIC BEHAVIOUR
OF BC SUBTYPES
Kennecke H, et al., J Clin Oncol 2010;28:3271–7. Reprinted with permission. © 2010 American Society of Clinical Oncology. All rights reserved.
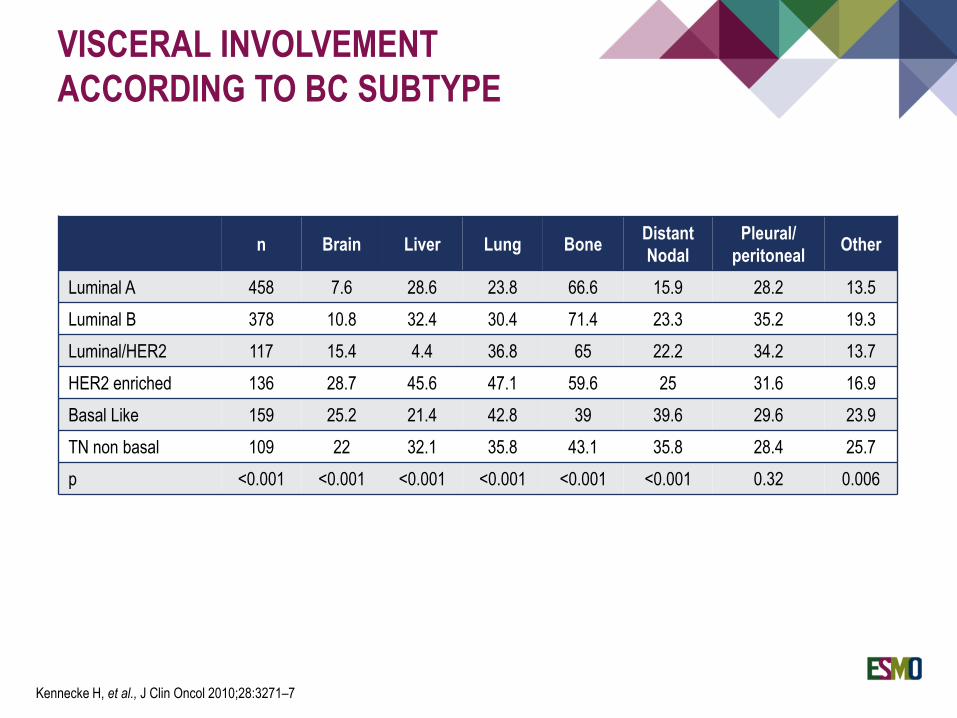
n Brain Liver Lung BoneDistant
Nodal
Pleural/
peritonealOther
Luminal A 458 7.6 28.6 23.8 66.6 15.9 28.2 13.5
Luminal B 378 10.8 32.4 30.4 71.4 23.3 35.2 19.3
Luminal/HER2 117 15.4 4.4 36.8 65 22.2 34.2 13.7
HER2 enriched 136 28.7 45.6 47.1 59.6 25 31.6 16.9
Basal Like 159 25.2 21.4 42.8 39 39.6 29.6 23.9
TN non basal 109 22 32.1 35.8 43.1 35.8 28.4 25.7
p <0.001 <0.001 <0.001 <0.001 <0.001 <0.001 0.32 0.006
VISCERAL INVOLVEMENT
ACCORDING TO BC SUBTYPE
Kennecke H, et al., J Clin Oncol 2010;28:3271–7

TN
HR+/HER2- HER2+
Reprinted from Cortazar P, et al., Lancet 2014;384164–72. Copyright 2014, with permission from Elsevier.
CHEMOSENSITIVITY OF TNBC:
pCR AND LONG-TERM OUTCOME

Introduction:
Definition, epidemiology, clinical behaviour
State of the art
Neoadjuvant/Adjuvant setting
Advanced disease
How to improve on CT
Heterogeneity: exploiting TNBC diversity to identify druggable pathways
OUTLINE
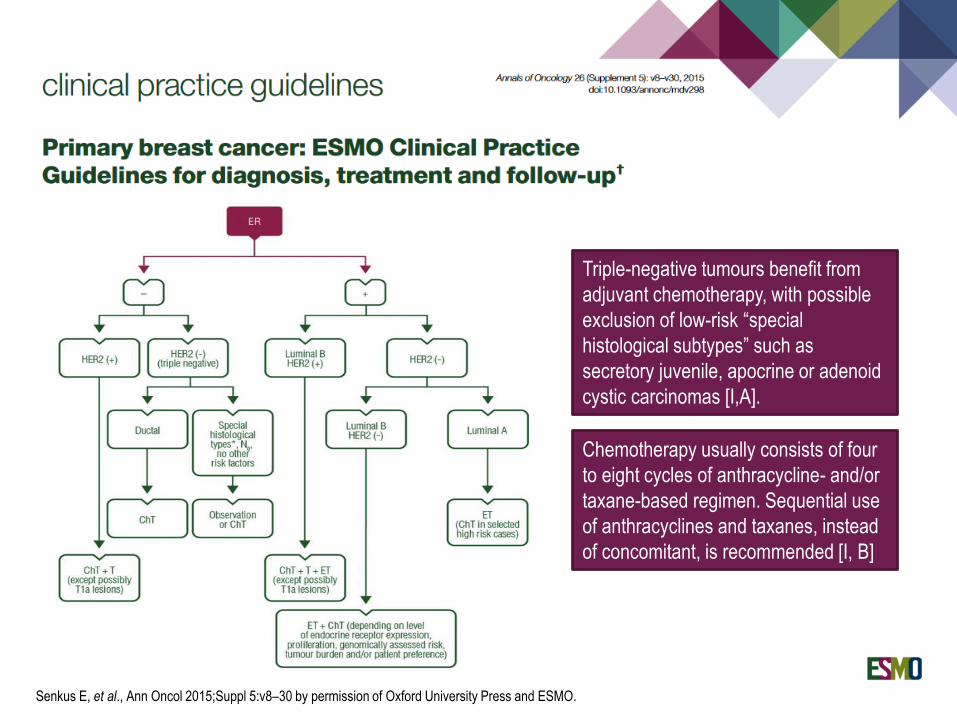
Triple-negative tumours benefit from
adjuvant chemotherapy, with possible
exclusion of low-risk “special
histological subtypes” such as
secretory juvenile, apocrine or adenoid
cystic carcinomas [I,A].
Chemotherapy usually consists of four
to eight cycles of anthracycline- and/or
taxane-based regimen. Sequential use
of anthracyclines and taxanes, instead
of concomitant, is recommended [I, B]
Senkus E, et al., Ann Oncol 2015;Suppl 5:v8–30 by permission of Oxford University Press and ESMO.

Anthracycline vs. no CT Anthra+Tax vs. no Tax
PROGRESS IN ADJUVANT CT
Reprinted from EBCTCG. The Lancet 2012;379(9814):432–44 + Supplement. Copyright 2012, with permission from Elsevier.

British Columbia Cancer Agency stage I-III BC (7,178 patients)
1,132 (15.8%) patients with ER neg and HER2 neg BC
Cohort 1: 1986 - 1992 Cohort 2: 2004 - 2008
PROGRESS IN ADJUVANT CT:
EFFECT FOR TNBC
Cossetti RJD, et al., J Clin Oncol 2015;33:65–73. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.

ADJUVANT CHEMOTHERAPY FOR
PATIENTS WITH SMALL TNBC
No chemotherapy Chemotherapy
5yrs DFS
T1a: 96%
T1b: 93%
5yrs DFS
T1a: 100%
T1b: 96%
Vaz-Luis I, et al., J Clin Oncol 2014;32:2142–50. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.

Guideline statements LoE Consensus
Sequential monotherapy is the preferred choice for MBC. Combination CT
should be reserved for patients with rapid clinical progression, life-
threatening visceral metastases, or need for rapid symptom and/or disease
control.
IA 96% (25) yes
4% (1) abstain
(26 voters)
In patients pre-treated (in the adjuvant or metastatic setting) with an
anthracycline and a taxane, and who do not need combination
chemotherapy, single-agent capecitabine, vinorelbine, or eribulin are the
preferred choices.
Additional choices include gemcitabine, platinum agents, taxanes, and
liposomal anthracyclines.
The decision should be individualised and take into account different
toxicity profiles, previous exposure, patient references, and country
availability.
IB 77.1% (27) yes
20.0% (7) abstain
(35 voters)
UPDATE ON HER2neg ABC

HER2+ HER2+HER2– HER2–
HR –HR +
MBC
(Poly)chemoRx
Paclitaxel+Beva
BRCA mutated
DNA damaging CT
PARPi
Trastuzumab +
Pertuzumab + taxane
Trastuzumab
+ Chemo
Lapatinib +
capecitabine
TDM-1
Lapatinib +
trastuzumab
AI + trastuzumab
AI + lapatinib
SERMs
SERD
AI
OFS
AI+ everolimus
AI + CDK4/6 inh.
Trastuzumab +
taxane
Chemotherapy
HOW TUMOUR BIOLOGY DRIVES
OUR THERAPEUTIC CHOICES
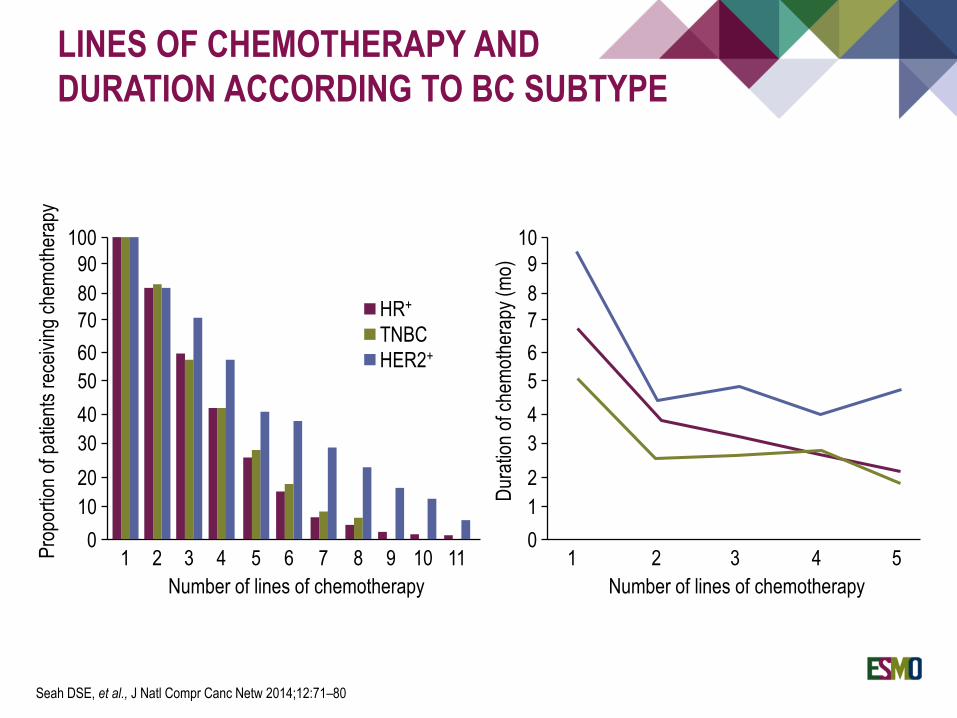
LINES OF CHEMOTHERAPY AND
DURATION ACCORDING TO BC SUBTYPE
Seah DSE, et al., J Natl Compr Canc Netw 2014;12:71–80
Number of lines of chemotherapy
Pro
port
ion
of p
atie
nts
rece
ivin
g ch
emot
hera
py
1 2 3 4 5 6 7 8 9 10 110
10
20
30
40
50
60
70
80
90
100
HR+
TNBC
HER2+
Number of lines of chemotherapy
Dur
atio
n of
che
mot
hera
py (
mo)
1 2 3 4 50
1
2
3
4
5
6
7
8
9
10

Introduction:
Definition, epidemiology, clinical behaviour
State of the art
Neoadjuvant/Adjuvant
Advanced disease
How to improve on CT
Heterogeneity: exploiting TNBC diversity to identify druggable pathways
OUTLINE
Chemotherapy is the mainstay of treatment in both early and advanced settings.
Treatment options have mostly remained unchanged over years
Recent attempts to further exploit TN chemosensitivity:
1. NEO/ADJUVANT setting:
Schedule
Maintenance
New cytotoxics/new formulations
2. ADVANCED setting:
New cytotoxics/new formulations
3. THE PLATINUM SALTS STORY
4. THE BEVACIZUMAB STORY
SYSTEMIC TREATMENT FOR TNBC:
CURRENT STATUS
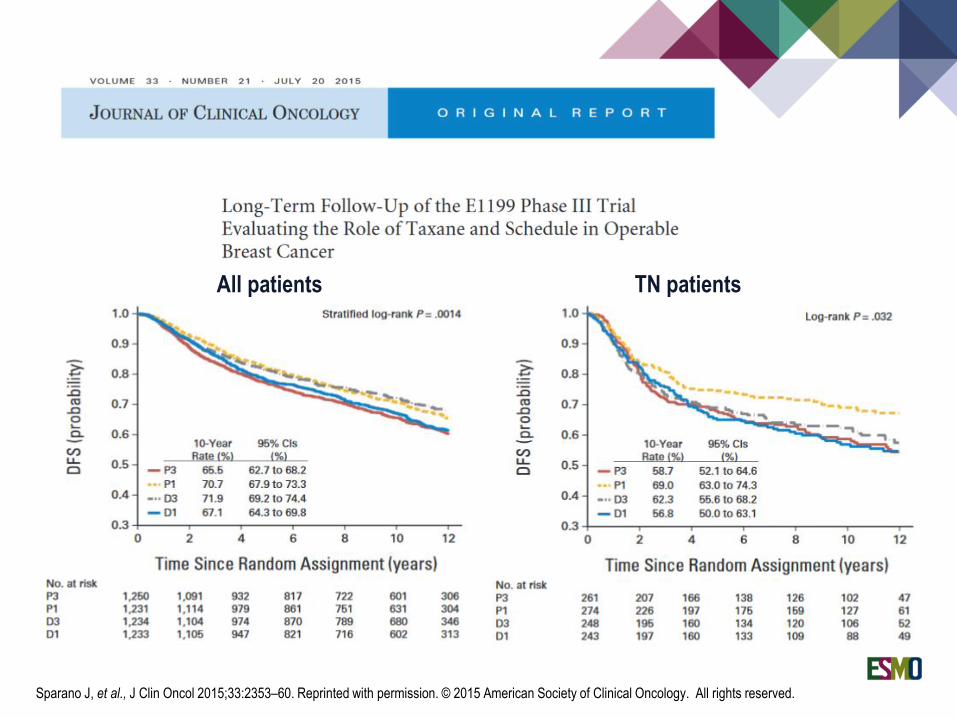
All patients TN patients
Sparano J, et al., J Clin Oncol 2015;33:2353–60. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
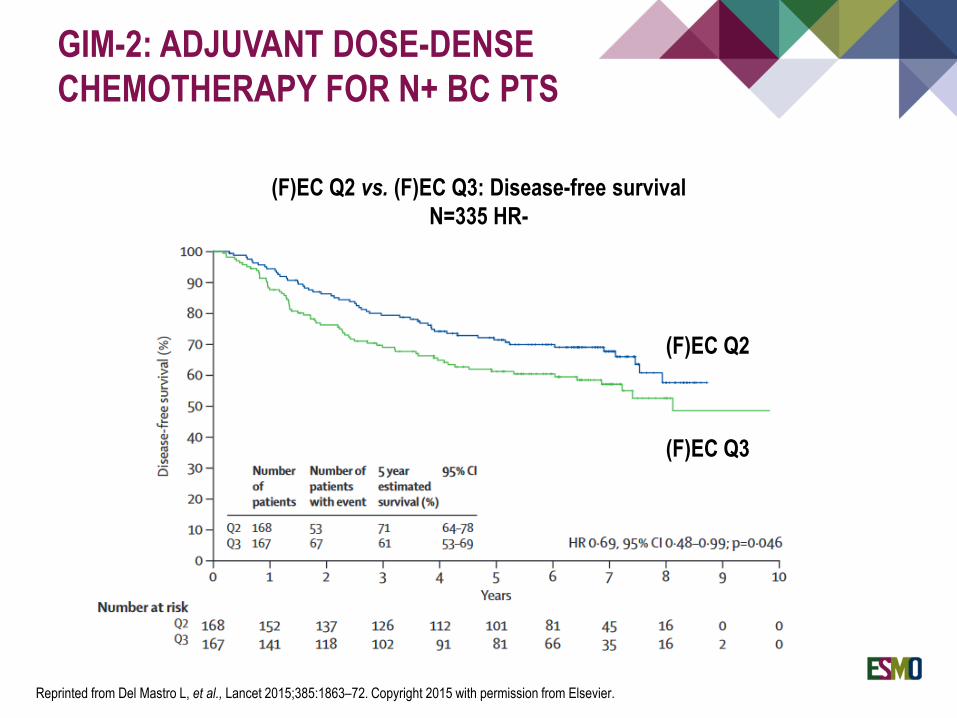
(F)EC Q2 vs. (F)EC Q3: Disease-free survival
N=335 HR-
(F)EC Q2
(F)EC Q3
GIM-2: ADJUVANT DOSE-DENSE
CHEMOTHERAPY FOR N+ BC PTS
Reprinted from Del Mastro L, et al., Lancet 2015;385:1863–72. Copyright 2015 with permission from Elsevier.

CMM MAINTENANCE AFTER
ADJUVANT CHEMOTHERAPY
75% TNBC
Presented By Colleoni M, at 2015 ASCO Annual Meeting. Reproduced courtesy of Marco Colleoni.

CMM MAINTENANCE AFTER
ADJUVANT CHEMOTHERAPY
All patients TN patients
Presented By Colleoni M, at 2015 ASCO Annual Meeting. Reproduced courtesy of Marco Colleoni.

Sur
gery
12 weeks 12 weeks
N=1200
R*
*Centrally confirmed:- Subtypes HER 2/ HR- Ki67- SPARC
Paclitaxel80 mg/ m2
weekly
nab-Paclitaxel
125 mg/ m2
weekly
Epirubicin 90 mg/m2
Cyclophosphamide 600 mg/m2
If HER2 positive:
Trastuzumab 8 mg/kg (loading dose) followed
by 6 mg/kg
Pertuzumab (absolute dose per application) 840
mg (loading dose) followed by 420 mg
If H
ER
2 po
sitiv
e: tr
astu
zum
ab
acc.
to A
GO
Gui
delin
es
Core biopsy
Cor
e bi
opsy
* (a
fter
ant
i-HE
R2
trea
tmen
t / b
efor
e st
udy
entr
y)
Arm A
Arm B
Core biopsy
optional
Core biopsy
optional
R*
Cor
e bi
opsy
* (b
efor
est
udy
entr
y)
N=60(HER2 positive)
6 weeks
FINAL STUDY DESIGN
(AFTER 400 PATIENTS RECRUITED)
*Randomizations carried out simultaneouslyPresented by Untch M. San Antonio Breast Cancer Symposium, December 9-13, 2014. Reproduced courtesy of Michael Untch.

GEPAR7: SUBGROUP ANALYSIS
Reprinted from Untch M, Lancet 2016;17(3):345-56. Copyright 2015, with permission from Elsevier.
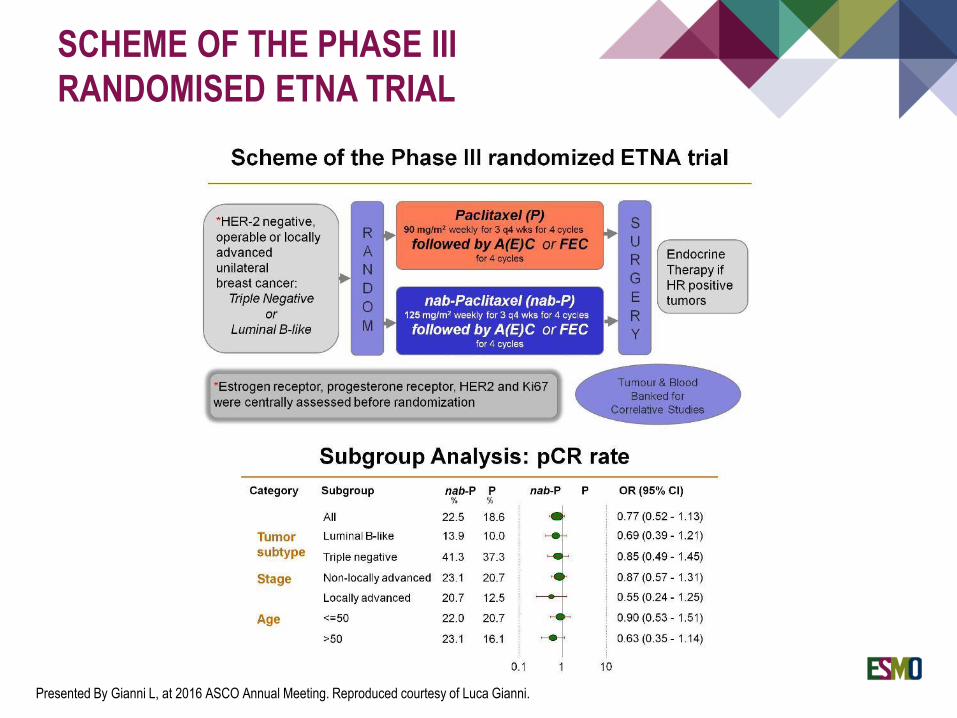
SCHEME OF THE PHASE III
RANDOMISED ETNA TRIAL
Presented By Gianni L, at 2016 ASCO Annual Meeting. Reproduced courtesy of Luca Gianni.

Chemotherapy is the mainstay of treatment in both early and advanced settings.
Treatment options have mostly remained unchanged over years.
Recent attempts to further exploit TN chemosensitivity:
1. NEO/ADJUVANT setting:
Schedule
Maintenance
New cytotoxics/new formulations
2. ADVANCED setting:
New cytotoxics/new formulations
3. THE PLATINUM SALTS STORY
4. THE BEVACIZUMAB STORY
SYSTEMIC TREATMENT FOR TNBC:
CURRENT STATUS

In advanced breast cancer patients already treated with anthracyclines and taxanes
(301 study)
ERIBULIN VS. CAPECITABINE
Kaufman PA, et al., J Clin Oncol 2015;33:594–601

E301: OVERALL SURVIVAL
Kaufman PA, et al., J Clin Oncol 2015;33:594–601. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
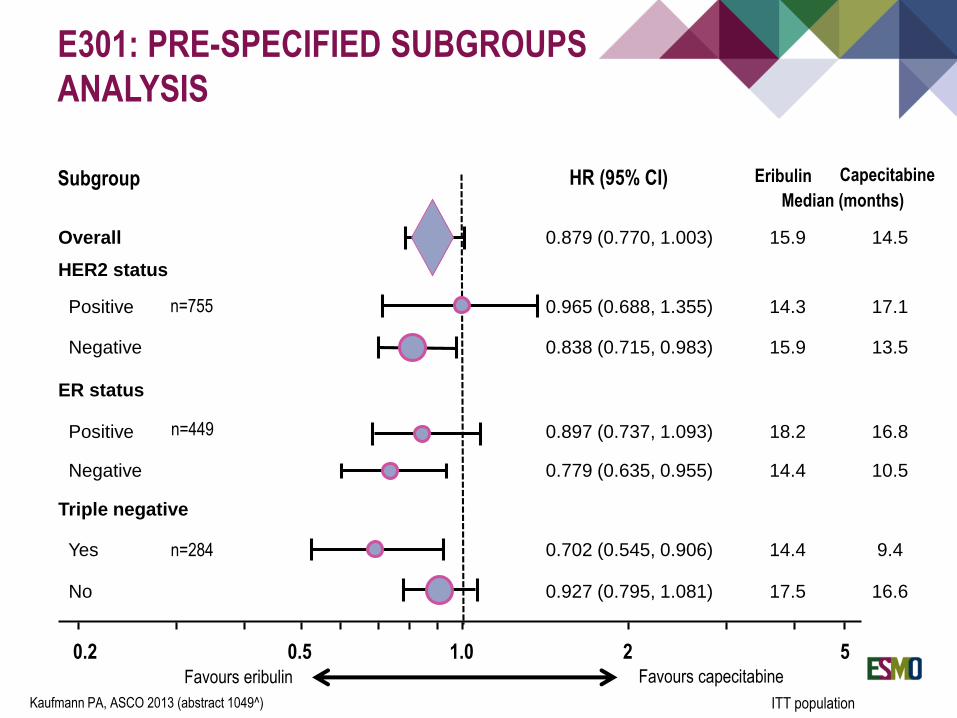
Overall 0.879 (0.770, 1.003) 15.9 14.5
HER2 status
Positive 0.965 (0.688, 1.355) 14.3 17.1
Negative 0.838 (0.715, 0.983) 15.9 13.5
ER status
Positive 0.897 (0.737, 1.093) 18.2 16.8
Negative 0.779 (0.635, 0.955) 14.4 10.5
Triple negative
Yes 0.702 (0.545, 0.906) 14.4 9.4
No 0.927 (0.795, 1.081) 17.5 16.6
Subgroup HR (95% CI) Eribulin Capecitabine
Median (months)
0.2 0.5 1.0 2 5
n=755
n=449
n=284
Favours eribulin Favours capecitabine
E301: PRE-SPECIFIED SUBGROUPS
ANALYSIS
ITT populationKaufmann PA, ASCO 2013 (abstract 1049^)
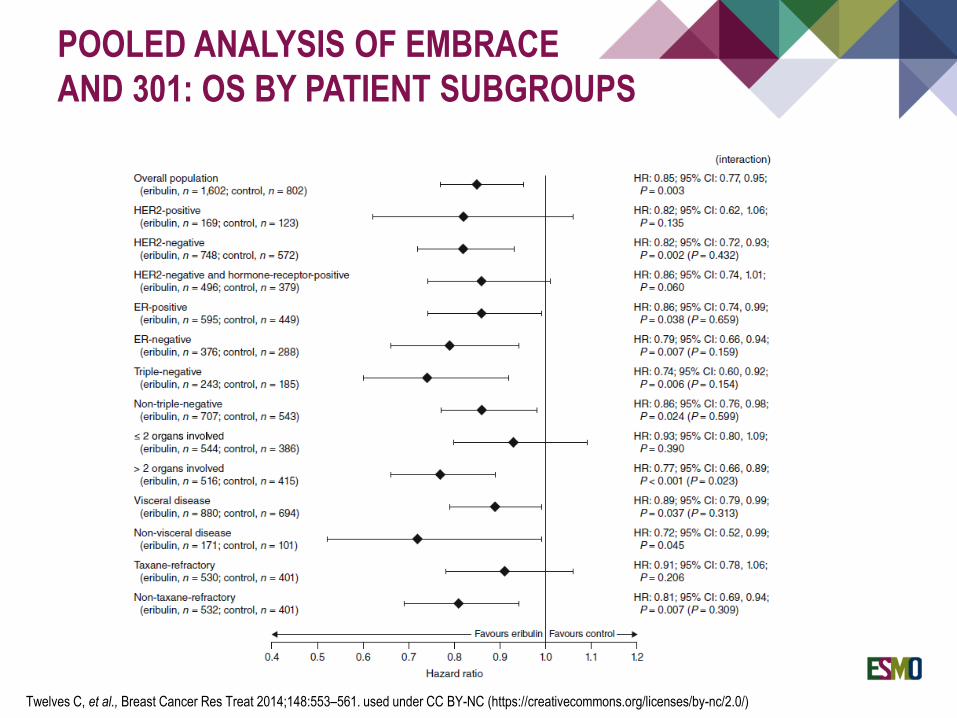
POOLED ANALYSIS OF EMBRACE
AND 301: OS BY PATIENT SUBGROUPS
Twelves C, et al., Breast Cancer Res Treat 2014;148:553–561. used under CC BY-NC (https://creativecommons.org/licenses/by-nc/2.0/)

Chemotherapy is the mainstay of treatment in both early and advanced settings.
Treatment options have mostly remained unchanged over years.
Recent attempts to further exploit TN chemosensitivity:
1. NEO/ADJUVANT setting:
Schedule
Maintenance
New cytotoxics/new formulations
2. ADVANCED setting:
New cytotoxics/new formulations
3. THE PLATINUM SALTS STORY
4. THE BEVACIZUMAB STORY
SYSTEMIC TREATMENT FOR TNBC:
CURRENT STATUS

DRUG-SPECIFIC CHEMOTHERAPY
FOR TNBC?

0
10
20
30
40
50
60
TAC
Gepar31
EC-D EC-D+Bev
Gepar53
PM PM+carbo
(+ Bev)
Gepar64
P-AC P+carbo-AC
(+/- Bev)
CALGB406035
P+carbo+bev
Ca.Pa.Be6nabP-EC
Gepar78
EC-P
(+/-gem)
NeoTango2
nabP-carbo
ADAPT7
pCR RATES (BREAST/AXILLA)
IN TNBC
1. Huober J, BCRT 2010; 2. Earl HM, Lancet Oncol 2014; 3. von Minckwitz G, NEJM 2012; 4. von Minckwitz G, Lancet Oncol 2014; 5. Sikov WM, J Clin
Oncol 2015; 6. Guarneri V, Ann Surg Oncol 2015; 7. Gluz O, SABCS 2015; 8. Untch M, Lancet Oncol 2016
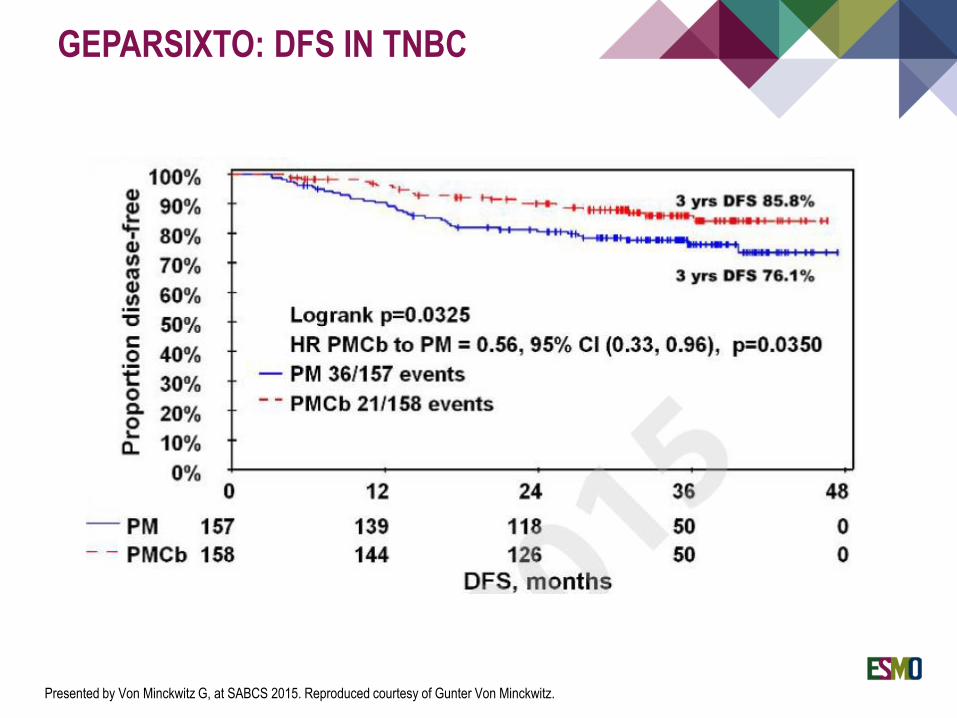
GEPARSIXTO: DFS IN TNBC
Presented by Von Minckwitz G, at SABCS 2015. Reproduced courtesy of Gunter Von Minckwitz.

CALGB 40603 (ALLIANCE)
EVENT FREE SURVIVAL
Presented by Sikov WM, SABCS 2015. Reproduced courtesy of Willian Sikov.

pCR RATES BY gBRCA STATUS
AND CARBOPLATIN IN TNBC
Presented by Von Minckwitz G, at SABCS 2014. Reproduced courtesy of Gunter Von Minckwitz.

pCR RATES BY TREATMENT AND
ACCORDING TO HR DEFICIENCY
STATUS (ypT0 ypN0)
Presented By Von Minckwitz G, at 2015 ASCO Annual Meeting. Reproduced courtesy of Gunter Von Minckwitz.

TNT PHASE III TRIAL FOR TN
METASTATIC BC
Tutt A, et al., SABCS 2014

TNT PHASE III TRIAL FOR TN
METASTATIC BC
Tutt A, et al., SABCS 2014

Tutt A, et al., SABCS 2014
TNT PHASE III TRIAL FOR TN
METASTATIC BC

TNT PHASE III TRIAL FOR TN
METASTATIC BC
Tutt A, et al., SABCS 2014

Chemotherapy is the mainstay of treatment in both early and advanced settings.
Treatment options have mostly remained unchanged over years.
Recent attempts to further exploit TN chemosensitivity:
1. NEO/ADJUVANT setting:
Schedule
Maintenance
New cytotoxics/new formulations
2. ADVANCED setting:
New cytotoxics/new formulations
3. THE PLATINUM SALTS STORY
4. THE BEVACIZUMAB STORY
SYSTEMIC TREATMENT FOR TNBC:
CURRENT STATUS

HYPOXIA-RELATED FEATURES
AND BASAL-LIKE TUMOURS
VEGF 13-gene VEGF-signature
Exp
ress
ion
Perou CM, The Oncologist 2010; 15(5):39-48. By permission by Alphamed Press ©2010
Antiangiogenic approaches work in TNBC at least as well as other subtype,
possibly more

POOLED ANALYSIS OF FIRST-LINE
BEVACIZUMAB: PFS
Miles DW, et al., Ann Oncol 2013;24:2773–80. By permission of Oxford University Press and ESMO.
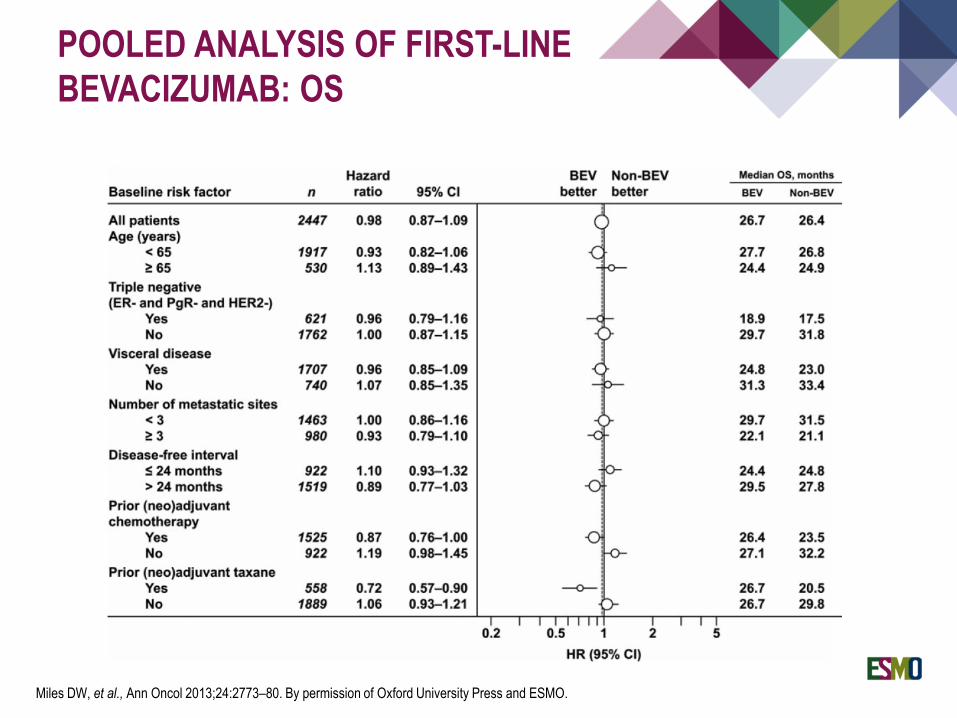
POOLED ANALYSIS OF FIRST-LINE
BEVACIZUMAB: OS
Miles DW, et al., Ann Oncol 2013;24:2773–80. By permission of Oxford University Press and ESMO.

NSABP-B402GEPAR51
NEOADJUVANT CHEMOTHERAPY
AND BEVACIZUMAB FOR HER2– NEGATIVE BC
Adapted from 1. von Minckwitz G, et al., N Engl J Med 2012;366(4):299-309; and 2. Miklos GL. N Engl J Med 2012;366(17):1638
Subgroup1 No. of pts
Odds Ratio (95% CI)
Test for interaction
All patients 1925 1.29 (1.02-1.65)
Age 0.26
<40 yr 304 1.71 (0.99-2.95)
≥40 yr 1621 1.20 (0.92-1.58)
Tumour stage 0.92
cT1-cT3 1690 1.30 (1.01-1.67)
cT4a-cT4d 235 1.23 (0.49-3.10)
Lymph-node stage 0.63
cN0 767 1.20 (0.84-1.74)
cN1-cN3 1096 1.36 (0.98-1.89)
Disease stage 0.16
Operable 1702 1.23 (0.96-1.59)
Locally advanced 223 2.43 (0.96-6.15)
Histologic type 0.91
Ductal or other 1713 1.31 (1.02-1.68)
Lobular 208 1.23 (0.40-3.79)
Tumour grade 0.15
1 or 2 1085 1.01 (0.66-1.53)
3 829 1.48 (1.09-2.02)
Hormone-receptor status 0.07
Negative 663 1.67 (1.21-2.31)
Positive 1262 0.99 (0.66-1.50)
Subgroup Odds Ratio (95% CI) Day test
All patients 1.29 (0.98, 1.92)
Clinical tumour size 0.76
2-4 cm 1.24 (0.85, 1.83)
>4 cm 1.35 (0.93, 1.96)
Clinical nodal status 0.44
Positive 1.15 (0.77, 1.75)
Negative 1.42 (0.98, 2.05)
Hormone receptor status 0.24
Positive 1.67 (1.07, 2.58)
Negative 1.18 (0.82, 1.72)
Age at entry 0.94
<50 yr 1.29 (0.9, 1.83)
≥50 yr 1.30 (0.89, 1.93)
Tumour grade 0.73
Low 0.78 (<0.25, 3.65)
Intermediate 1.21 (0.67, 2.2)
High 1.4 (1.00, 1.91)
BEVACIZUMAB ADDED TO NEOADJUVANT
CHEMOTHERAPY FOR BREAST CANCER

CALGB 40603:
RESULTS BEV/NO BEV
Sikov WM, et al., J Clin Oncol 2014;33:13–21. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.

GEPARQUINTO: NEOADJUVANT
BEVACIZUMAB AND SURVIVAL
von Minckwitz G, et al., Ann Oncol 2014;25:2363-72. By permission of Oxford University Press and ESMO.

BEATRICE PHASE III
ADJUVANT TRIAL
Reprinted from Cameron D, Lancet 2013;14:933–42. Copyright 2013, with permission from Elsevier.

Introduction:
Definition, epidemiology, clinical behaviour
State of the art
Neoadjuvant/Adjuvant
Advanced disease
How to improve on CT
Heterogeneity: exploiting TNBC diversity to identify druggable pathways
OUTLINE

THE GENOMIC COMPLEXITY
OF TNBC
1. Reprinted by permission from Macmillan Publishers Ltd: Nature Stephens PJ, et al., 2009;462(7276):1005-10. Copyright 2009.
2. Reprinted by permission from Macmillan Publishers Ltd: Nature. Shah SP, et al., 2012;486(7403):395-9. Copyright 2012.

Basal-like 1 and Basal-like 2 Cell proliferation, DNA damage response
Immunomodulatory Immune signalling
Mesenchymal-like and Mesenchymal stem-like EMT, motility and growth-factor pathways
Luminal AR Androgen receptor signaling
TNBCTYPE
Lehmann BD, et al., J Clin Invest 2011;121:2750–67. Reproduced with permission of American Society for Clinical Investigation in the format use in an
ecoursepack via Copyright Clearance Center.

DSB, double-strand break; HR, homologous recombination
SSB, single-strand break
PARP
DNA damage (SSBs)
DNA replication
(accumulation of DNA DSBs)
Normal cell
with functional HR pathwayHR-deficient tumour cell
Cell survival Cell death
HR-mediated
DNA repair
Impaired HR-mediated
DNA repair
Tumour-selective cytotoxicity
PARP inhibition
PARP INHIBITION AND TUMOUR-
SELECTIVE SYNTHETIC LETHALITY
Farmer H, et al., Nature 2005;434:917–921; Bryant HE, et al., Nature 2005;434:913–917; McCabe N, et al., Cancer Res 2006;66:8109–8115

Reprinted from Tutt A, et al., Lancet 2010;37:235-44. Copyright 2013, with permission from Elsevier.

PHASE III TRIALS OF PARP
INHIBITORS IN HER2NEG
BRCA1/2MUT BC PATIENTS
Potent PARP inhibitor at
MTD as continuous
exposure
Physician Choice within
SOC options
Capecitabine
or
Vinorelbine
or
Eribulin
or
Gemcitabine
gBRCA1 / BRCA2 Carriers
Advanced anthracycline
taxane resistant breast
cancer
Primary
endpoint
PFS
Olaparib – OLYMPIAD - NCT02000622
Talazoparib (BMN 673)
– EMBRACA - NCT01945775
Niraparib – EORTC / BIG BRAVO Trial
R
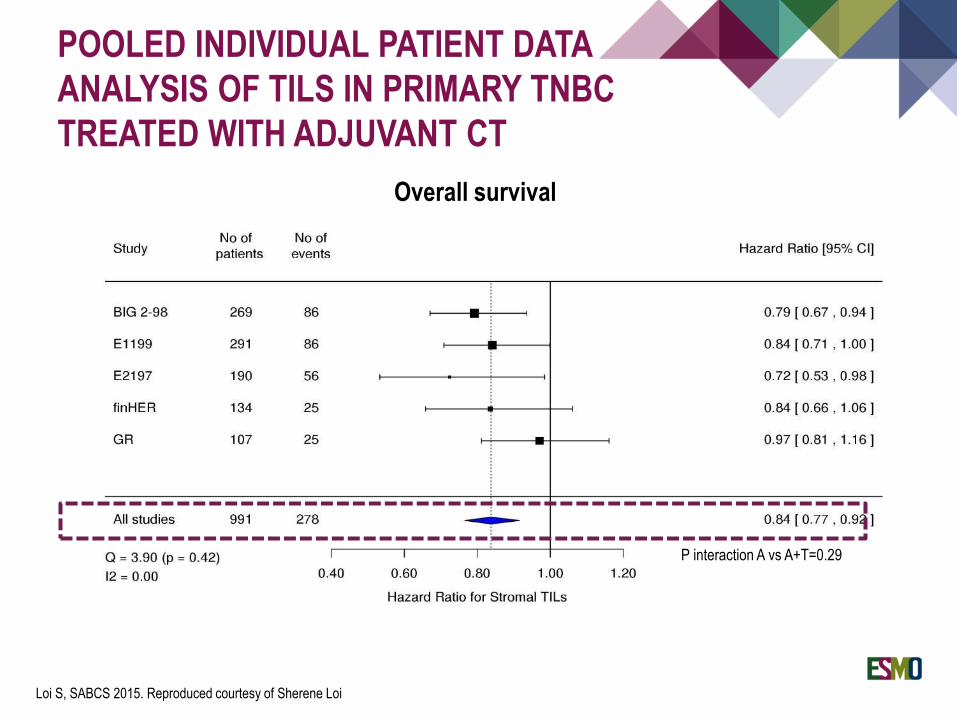
POOLED INDIVIDUAL PATIENT DATA
ANALYSIS OF TILS IN PRIMARY TNBC
TREATED WITH ADJUVANT CT
P interaction A vs A+T=0.29
Overall survival
Loi S, SABCS 2015. Reproduced courtesy of Sherene Loi

p=0.0019 p=0.0017
5yr-MFS: 81.5% vs. 46%
HR 0.24, 95%CI 0.09-0.645yr-OS: 91% vs. 55%
HR 0.19, 95%CI 0.06-0.61
Dieci MV, et al., Ann Oncol. 2014;25:611–8. © The Author 2014. Published by Oxford University Press on behalf of the European Society for Medical
Oncology. All rights reserved.
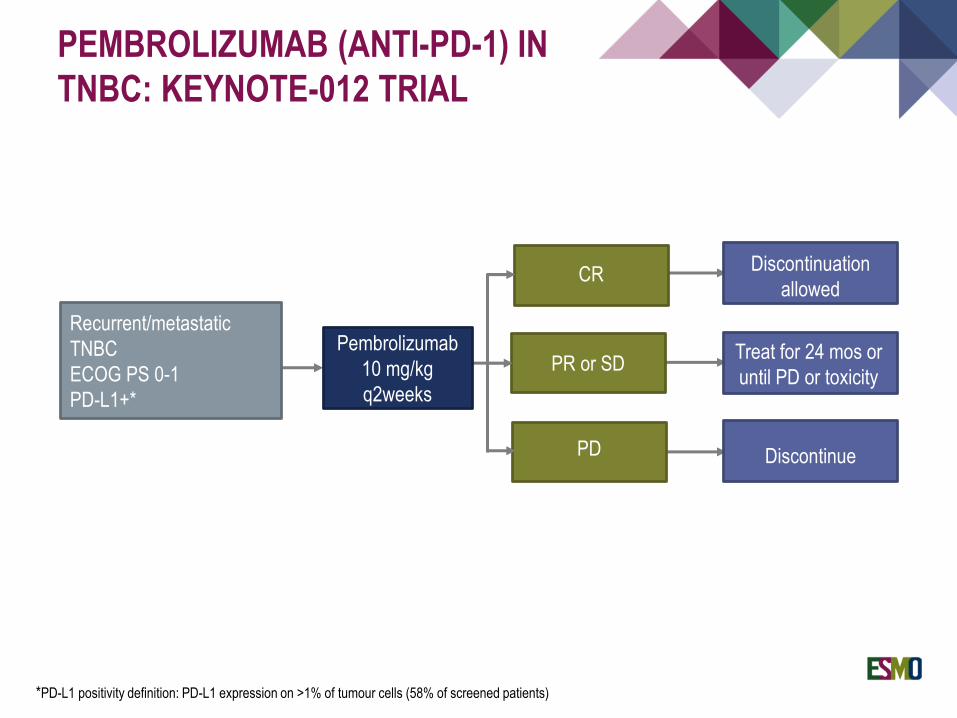
Recurrent/metastatic
TNBC
ECOG PS 0-1
PD-L1+*
CR
PR or SD
PD
Discontinuation
allowed
Treat for 24 mos or
until PD or toxicity
Discontinue
PEMBROLIZUMAB (ANTI-PD-1) IN
TNBC: KEYNOTE-012 TRIAL
Pembrolizumab
10 mg/kg
q2weeks
*PD-L1 positivity definition: PD-L1 expression on >1% of tumour cells (58% of screened patients)

On treatment
Discontinued treatment
Objective response rate: 18.5%
Stable disease: 25.9%
n=32
PEMBROLIZUMAB IN TNBC:
KEYNOTE-012 TRIAL
Nanda R, et al., SABCS 2014. Reproduced courtesy of Rita Nanda

MPDL3280 in n=21 TNBC (PD-L1 IC scores 2/3 )
MPDL3280A (ATEZOLIZUMAB)
IN TNBC
Emens LA, et al., AACR 2015
IC2/3 patients, na ORR
(95% CI)
24-Week PFS
(95% CI)
21 19% (5-42) 27% (7-47)
CR/Pr (n=4)
SD (n=3)
PD (n=9)
Discontinued
New lesion
0 42 84 126
Time on study (days)
168 210 252 294 336 378 420 462 504 546 588
-100
-80
-60
-40
-20
0
20
40
60
80
100
Cha
nge
in s
um o
f lar
gest
dia
met
ers
from
bas
elin
e (%
)

RESULTS<BR />DORA
Presented by Adams SA, et al., ASCO 2016. Reproduced courtesy of Sylvia Adams

Unique subclass of ER-PgR- human tumours characterised by a hormonally regulated
transcriptional programme and response to androgen
ANDROGEN RECEPTOR IN TNBC
Reprinted by permission from Macmillan Publishers Ltd: Doane AS, et al., Oncogene 2006;25:3994–4008, copyright 2006.
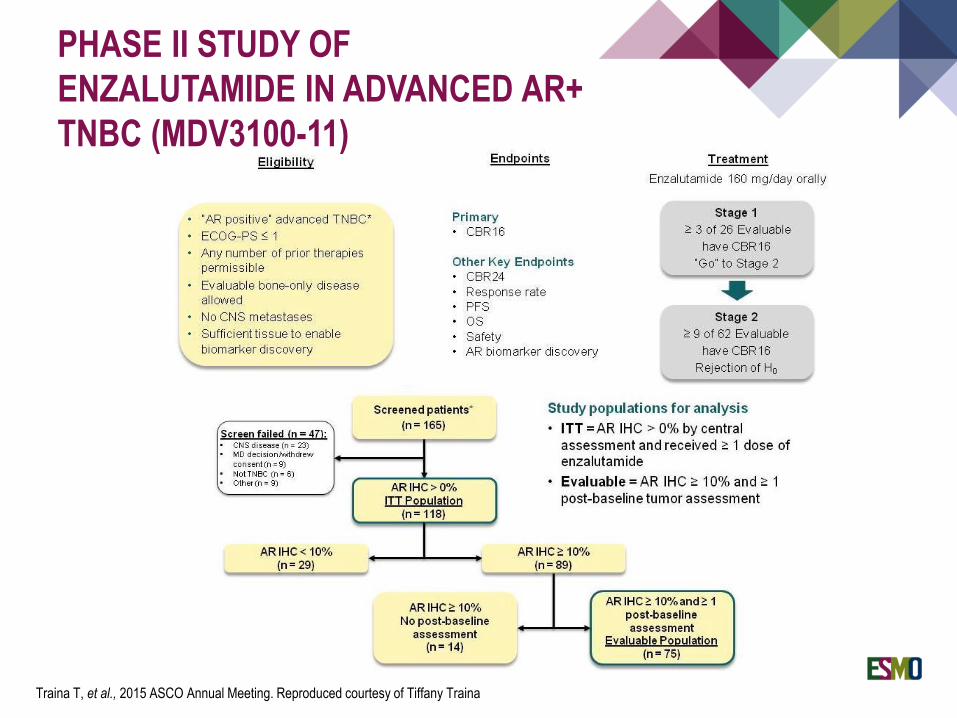
PHASE II STUDY OF
ENZALUTAMIDE IN ADVANCED AR+
TNBC (MDV3100-11)
Traina T, et al., 2015 ASCO Annual Meeting. Reproduced courtesy of Tiffany Traina

PHASE II STUDY OF
ENZALUTAMIDE IN ADVANCED AR+
TNBC (MDV3100-11)
Traina T, et al., 2015 ASCO Annual Meeting. Reproduced courtesy of Tiffany Traina
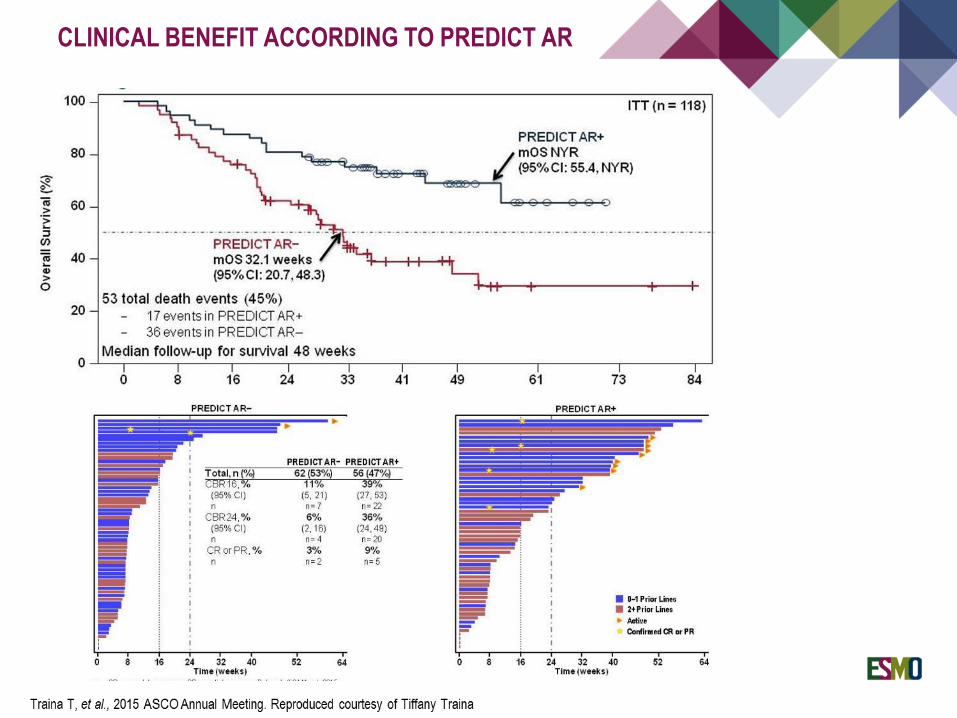
CLINICAL BENEFIT ACCORDING TO PREDICT AR

Chemotherapy remains the mainstay of treatment:
Anthracycline+taxanes: first choice in the neo-/adjuvant setting (the schedule
matters!)
BRCA-mut (or BRCAwt with BRCAness features?): chance for tailored-
chemotherapy with platinum salts
Novel targets and approaches:
Dissecting the diversity of TNBC helps identifying druggable pathways
PARP inhibitors hold great promises for BRCA-mut patients
Immunotherapy on the horizon: what about predictive markers?
CONCLUSIONS

THANK YOU!