DYSPHAGIA Mr Andrew Lale Consultant ENT surgeon.
25
DYSPHAGIA DYSPHAGIA Mr Andrew Lale Consultant ENT surgeon
-
Upload
regina-butler -
Category
Documents
-
view
229 -
download
2
Transcript of DYSPHAGIA Mr Andrew Lale Consultant ENT surgeon.
DYSPHAGIADYSPHAGIA
Mr Andrew Lale
Consultant ENT surgeon
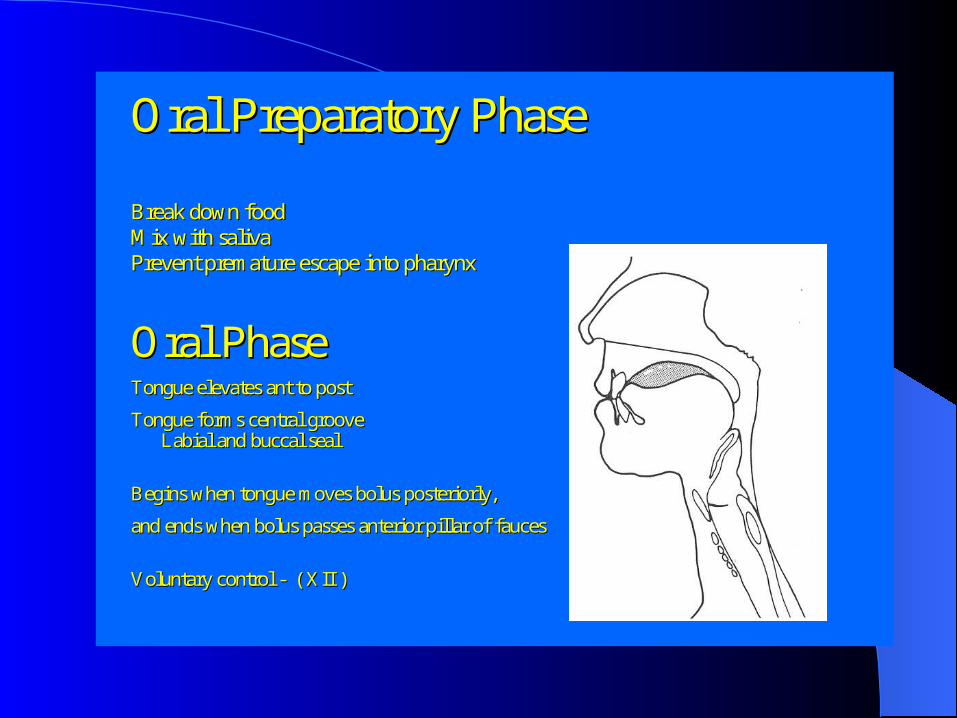
Oral Preparatory PhaseOral Preparatory Phase
Break down foodBreak down foodMix with salivaMix with salivaPrevent premature escape into pharynxPrevent premature escape into pharynx
Oral PhaseOral PhaseTongue elevates ant to postTongue elevates ant to post
Tongue forms central grooveTongue forms central grooveLabial andLabial and buccalbuccal sealseal
Begins when tongue moves bolusBegins when tongue moves bolus posteriorlyposteriorly, ,
and ends when bolus passes anterior pillar ofand ends when bolus passes anterior pillar of faucesfauces
Voluntary control Voluntary control -- ( XII )( XII )

Pharyngeal PhasePharyngeal Phase
Begins when bolus passes anterior pillar or Begins when bolus passes anterior pillar or faucesfaucesEnds when bolus passes through upper oesophageal sphincter into Ends when bolus passes through upper oesophageal sphincter into oesophagusoesophagusVelum elevates and contracts, closing nasal passage, bolus propeVelum elevates and contracts, closing nasal passage, bolus propelled through pharynx, lled through pharynx, larynx closed and elevated, respiration inhibited, upper oesophalarynx closed and elevated, respiration inhibited, upper oesophageal sphincter relaxesgeal sphincter relaxes
Involuntary control Involuntary control –– ( IX, X, XII )( IX, X, XII )

OesophagealOesophageal PhasePhase
Begins when bolus enters Begins when bolus enters oesophagusoesophagusEnds when bolus passes through lower Ends when bolus passes through lower oesophageal oesophageal sphincter into stomach 8sphincter into stomach 8--20 seconds later20 seconds laterSequential peristaltic wave propels bolus Sequential peristaltic wave propels bolus Relaxation of lower Relaxation of lower oesophageal oesophageal sphinctersphincter
Involuntary control Involuntary control –– ( X )( X )

SWALLOWINGSWALLOWING
“5 minute consultation” CAUSES: Acute Neurogenic Globus pharyngeus Laryngopharyngeal reflux Strictures and narrowing Pharyngeal Pouches

CONSULTATIONCONSULTATION
True Dysphagia or feeling of a lump?Dysphagia for what?Regurgitation or Aspiration?Gastro-oesophageal reflux current or past?Change of Diet or weight loss?Odynophagia
ACUTE DYSPHAGIAACUTE DYSPHAGIA
History: FB. Previous problems.Examination: Drooling. Pain. Pyrexia.
OdynophagiaTreatment:Food bolus: Buscopan, fizzy drink, refer at
1 hourFB: Refer

Foreign bodiesForeign bodies

Strictures and narrowingStrictures and narrowing
Malignant/benignCricopharyngeal barC-spine osteophytesKyphosisPost cricoid web

Cricopharyngeal barCricopharyngeal bar

OsteophytesOsteophytes
NeurogenicNeurogenic
CVAMotor neurone diseaseMultiple SclerosisParkinson’s diseaseMyaesthena gravis
GLOBUS PHARYGEUSGLOBUS PHARYGEUS
Previously Globus HystericusWorse when NOT eating or drinkingNo true dysphagia solids/liquidsNo odynophagiaNo reguritation/aspirationVariable history. ?exclude reflux…..

Laryngopharyngeal Reflux Laryngopharyngeal Reflux (LPR)(LPR)
Reflux of gastric acid to larynx/pharynxMay be “silent”Symptoms include feeling of a lump,
odynophagia/chronic sore throat, chronic cough (especially nightime), hoarse voice and “mucous in throat”.

LPR InvestigationsLPR Investigations
Nasopharyngoscopy, red post cricoid region.
? Barium swallow?Oesophageal pH manometry

LPR treatmentLPR treatment
6 weeks PPI + Gaviscon initiallyAt review further 6 weeks treatment if
improvingGeneral laryngeal hygiene measuresIf no better, rigid pharyngo-
oesophagoscopypH manometry ?fundoplication
Pharyngeal pouchesPharyngeal pouches
HISTORYLong Hx dysphagiaRegurgitation esp at night“gurgling” swallowAspiration (recurrent pneumonia)Weight loss and change in Diet.
Pharyngeal PouchesPharyngeal Pouches
EXAMINATIONNasopharyngoscopy might show poolingUnlikely to feel anything in neckBarium swallow

Pharyngeal pouchesPharyngeal pouches
TREATMENTSurgical if fit for GA(External approach)Endoscopic stapling, low morbidity and
high success rate.

PouchesPouches
BARIUM SWALLOW.jpg
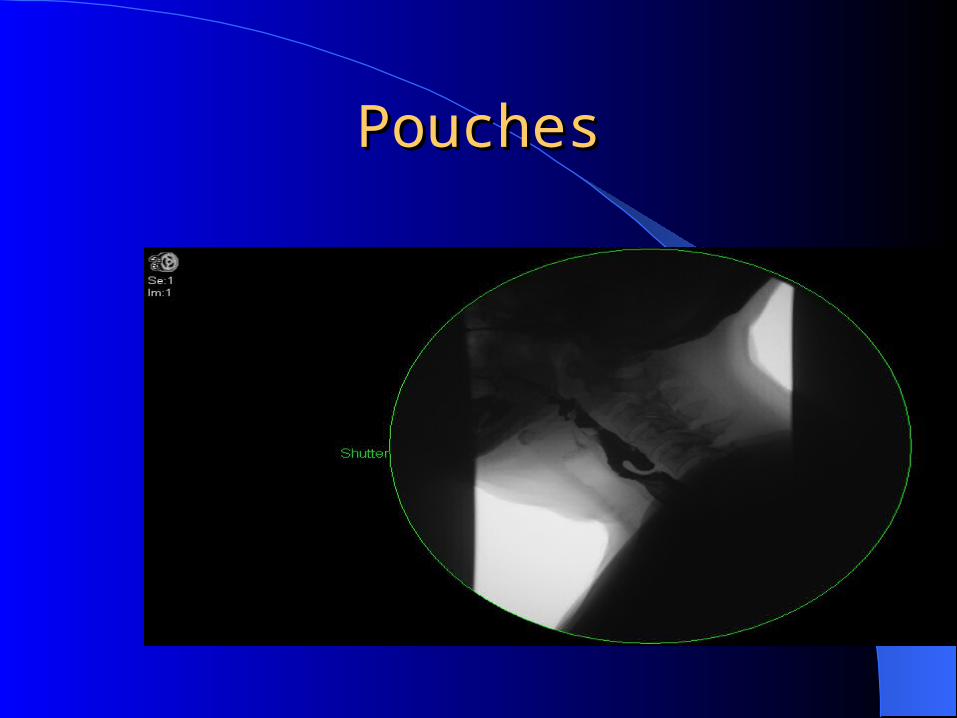
PouchesPouches
BARIUM SWALLOW.jpg
Summary :Fast track patientsSummary :Fast track patients
Young male patient Short historyOdynophagiaSmoking and AlcoholWeight lossAspiration and reguritation
Summary: Globus patientsSummary: Globus patients
Variable historyNo true dysphagiaYoung femaleNo weight lossAssociated anxiety

Summary: Pouch patientsSummary: Pouch patients
Older male/femaleREGURGITATIONGurgling swallowRecurrent chest infectionsWeight loss
ThankyouThankyou