Durable remission in pediatric ALL with CAR T-cell therapyDurable remission in pediatric ALL with...
26
Durable remission in pediatric ALL with CAR T-cell therapy David M. Barrett, MD/PhD Center for Childhood Cancer Research Children’s Hospital of Philadelphia Perelman School of Medicine University of Pennsylvania Philadelphia, PA
Transcript of Durable remission in pediatric ALL with CAR T-cell therapyDurable remission in pediatric ALL with...
Durable remission in pediatric ALL with CAR T-cell therapy
David M. Barrett, MD/PhD Center for Childhood Cancer Research
Children’s Hospital of Philadelphia Perelman School of Medicine
University of Pennsylvania Philadelphia, PA
Disclosures for David M. Barrett, MD, PhD
Royalty N/A
Receipt of intellectual property/ Patent holder
N/A
Consulting fee N/A
Speakers bureau N/A
Fees for non-CME services N/A
Contracted research N/A
Ownership interest (stocks, stock options)
N/A
Other N/A
N/A = Not Applicable (no conflicts listed) Presentation includes discussion of off-label or unapproved use of a drug or medical device

Roadblocks to Successful Cellular Immunotherapy for Cancer
PROBLEM
• Targeting
• Expansion ex vivo
• Expansion in the host
• Persistence
• Effector:Target ratio –
create sufficient effector
cells for clinical success
SOLUTION
• CAR or TCR
• GMP cell culture
• ?Young T cells
• ?Memory T cells
• Need evidence for
efficacy, not just safety,
in phase 1
Abbreviations: CAR, chimeric antigen receptor; GMP, good manufacturing practice; TCR, T-cell receptor

CART19: Chimeric Antigen Receptor T cells against CD19

Redirecting the Specificity of T cells–
Proposed Mechanism of Action of
CTL019 cells
• Gene transfer technology is used to
stably express CARs on T cells,
conferring novel antigen specificity1,2
• CTL019 cells can thus be directed
against any tumor cell that expresses
the CD19 surface antigen
• CTL019 therapy takes advantage of
the cytotoxic potential of T cells
thereby killing tumor cells in an
antigen-dependent manner1,3
• Persistent CTL019 cells consist of
both effector (cytotoxic) and central
memory T cells3
1. Milone MC, et al. Mol Ther. 2009;17:1453-1464.
2. Hollyman D, et al. J Immunother. 2009;32:169-180.
3. Kalos M, et al. Sci Transl Med. 2011;3:95ra73.
T cell
CD19
Native TCR
Tumor cell
CTL019 cell
Dead tumor cell
Anti-CD19 CAR construct
High Rates of Remission Induction in ALL with CTL019
Over 110 patients have been treated with CTL019
(CLL, ALL, NHL)
• Pediatric ALL cohort (N=25): – 22/25 CRs (88%), 3 after blinatumomab
– 6 relapses,
including 2 CD19(-) relapses (1 after blinatumomab)
• All ALL (N=30) (pediatric plus adult):
– 27/30 CRs (90%)
– 7 total relapses
– Short follow-up (median 8 months, range 2-30 months)

Patient Characteristics
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material
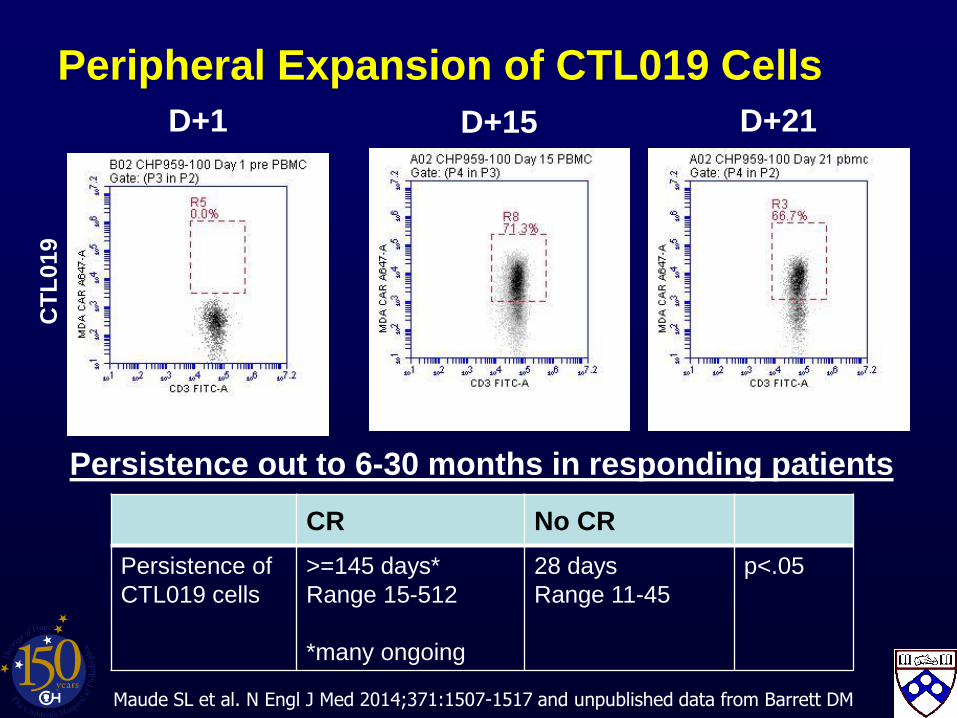
CT
L019
D+1 D+15 D+21
CR No CR
Persistence of
CTL019 cells
>=145 days*
Range 15-512
*many ongoing
28 days
Range 11-45
p<.05
Persistence out to 6-30 months in responding patients
Peripheral Expansion of CTL019 Cells
Maude SL et al. N Engl J Med 2014;371:1507-1517 and unpublished data from Barrett DM
Proliferation and Persistence of CTL019 by QPCR
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material
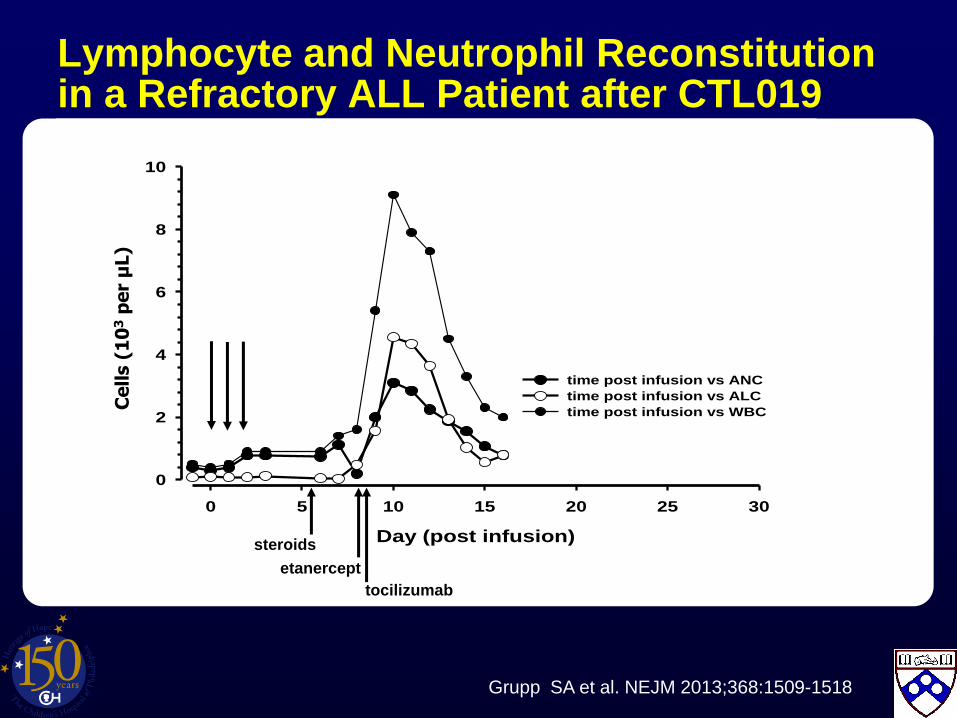
Day (post infusion)
0 5 10 15 20 25 30
Cel
ls (
10^3
per
uL
)
0
2
4
6
8
10
time post infusion vs ANC
time post infusion vs ALC
time post infusion vs WBC
steroids
etanercept
tocilizumab
Lymphocyte and Neutrophil Reconstitution in a Refractory ALL Patient after CTL019
Ce
lls (
10
3 p
er
µL)
Grupp SA et al. NEJM 2013;368:1509-1518
Efficient Trafficking of CTL-019 T Cells to CNS in ALL
CSF
Day 23
Blood
Day 10
Grupp SA et al. NEJM 2013;368:1509-1518
Morphology of CARs In Vivo
Copyrighted material

Persistence of CTL019 by Flow Cytometry
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material
B Cell Aplasia in Peripheral Blood
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material

CTL019 Toxicities
• B cell aplasia
observed in all responding patients to date
managed with IVIg replacement therapy
• Tumor lysis syndrome (TLS)
may be delayed for 20 to 50 days post infusion in CLL
• Cytokine release syndrome (CRS)
reversible, on-target toxicity
Severity related to tumor burden: Treat MRD as outpatient?
• Macrophage activation syndrome (HLH / MAS)
• Neurotoxicity
Significant confusion, aphasia
Occurs in a small number of patients and after CRS
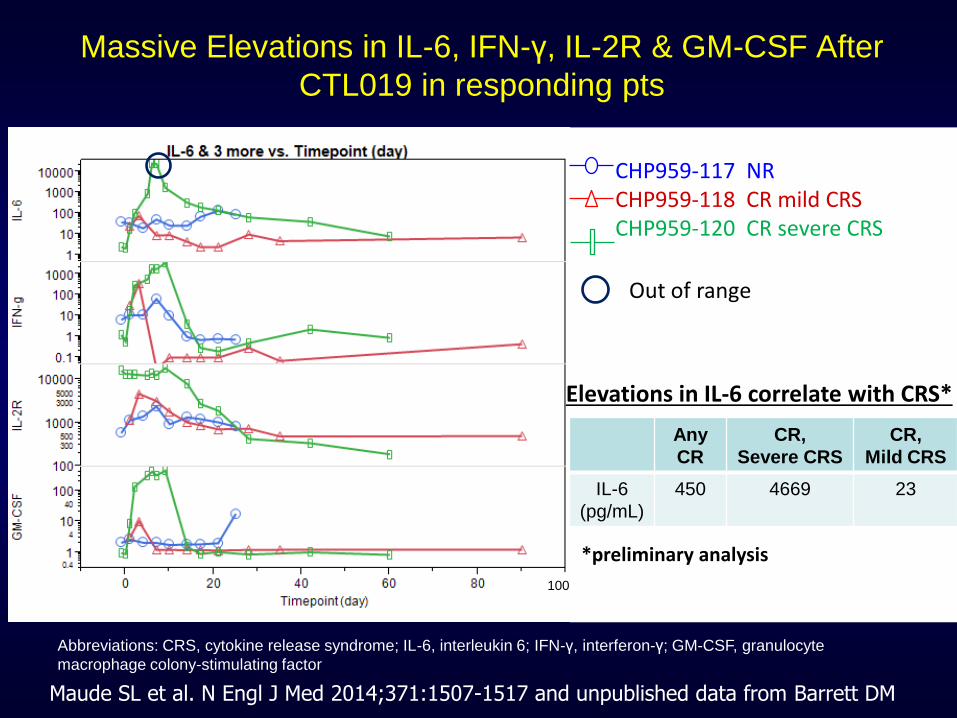
Massive Elevations in IL-6, IFN-γ, IL-2R & GM-CSF After
CTL019 in responding pts
CHP959-117 NR CHP959-118 CR mild CRS CHP959-120 CR severe CRS
Out of range
100
Elevations in IL-6 correlate with CRS*
Any
CR
CR,
Severe CRS
CR,
Mild CRS
IL-6
(pg/mL)
450 4669 23
Abbreviations: CRS, cytokine release syndrome; IL-6, interleukin 6; IFN-γ, interferon-γ; GM-CSF, granulocyte
macrophage colony-stimulating factor
*preliminary analysis
Maude SL et al. N Engl J Med 2014;371:1507-1517 and unpublished data from Barrett DM

Tocilizumab
• IL-6 receptor antagonist
• Blocks IL-6 mediated effects
• Indicated in:
– juvenile idiopathic arthritis (JIA)
– Rheumatoid arthritis (RA)
– In Japan, indication for Castleman’s Disease
• Typically given monthly
• Rare side effects of transaminitis and neutropenia
• We have used 8 mg/kg (4mg/kg possible in <30 kg)

Teachey DT . . . Grupp SA. Blood 2013;121:5154-5157
Blinatumomab Causes HLH/MAS as Well, Reversible With Tocilizumab
Elevated cytokines
• IL-10 (5338 pg/mL)
• IL-6 (681 pg/mL)
• INF-γ (192 pg/mL)
• IL-2R (4872 pg/mL)
Copyrighted material

Correlates with severe CRS: serum markers
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material

Correlates with severe CRS: cytokines
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material
Correlates with severe CRS: disease burden highly predictive
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material
Overall Survival after CTL019 infusion
Maude SL et al. N Engl J Med 2014;371:1507-1517
Copyrighted material
CHP101– BM MRD Testing
Grupp SA et al. NEJM 2013;368:1509-1518
Copyrighted material
CHP101 – CD19 (-) Recurrence
Grupp SA et al. NEJM 2013;368:1509-1518
Copyrighted material

What Is the Potential for Immunotherapy?
• Consolidate patients with MRD
• Reinduce remission
• Produce MRD (-) state prior to allo SCT
• Bridge to SCT
• Multicenter trial/s in pediatric ALL

CTL019 Development Plan
• Pediatrics leads the way
• Breakthrough Therapy designation
• First multisite trial now open
and enrolling
• Global ALL trial 2015
• Target for registration
submission: 2016
TCSL
Simon Lacey Jos Melenhorst Yolanda Mahnake Tatiana Mikheeva Kathleen Haines Akhil Kotian Erica Suppa Irina Kulikovskaya Jennifer Wright
CVPF
Bruce Levine Anne Chew Julio Cotto Zoe Zheng Alexey Bersenev
Patients and Families
CHOP Nursing
CTO Lisa Speicher
CHOP StemCell Lab Giuliana Pierson Yongping Wang CHOP Vector Core PA Dept. of Health
ACC Translational Research
Carl June Carmine Carpenito Michael Milone Yangbing Zhao
HUP Noelle Frey David Porter CHOP Study Staff
Christine Strait Margie Tartaglione Trish Hankins Colleen Callahan Center for Childhood Cancer Research John Maris
Stephan Grupp David Teachey Alix Seif Shannon Maude
Acknowledgements