Duplication of the common bile duct A case report€¦ · Duplication of the common bile duct –A...
1
Duplication of the common bile duct – A case report 1 Department of Surgery, Spital Linth, Uznach, Switzerland, 2 Department of Medicine, Gastroentrology, Spital Linth, Uznach, Switzerland, 3 Department of Radiology, Cantonal Hospital of St. Gallen, St. Gallen, Switzerland Anatomical variants of the extrahepatic bile duct system occur in approximately 42% of the population. On the other hand, duplication of the common bile duct is a very rare congenital abnormality, which is often associated with recurrent cholangitis or pancreatitis, as well as an increased risk of malignant degeneration. Therefore diagnostics using MRI and ERCP as well as the therapeutic strategy are a challenge. Classification and division according to Choi et al. describe 5 different types of anatomical variants of the common bile duct. Our case presents a patient with a duplication of the DHC type Vb (Fig. 1). Introduction We have treated a 50-year-old woman, who presented herself with severe coliform epigastric pain and febrile temperature. The gall bladder has been removed several years ago due to severe cholecystitis with cholecystolithiasis. A cholestatic hepatopathy was found as well. However the duplication of the common bile duct was not detected. At present the patient showed increasing inflammation values under antibiotic therapy and the suspicion of cholangitis. Case Report The performed MRCP showed a duplication anomaly (Fig. 2a) and a choledocholithiasis (Fig. 2b) of the right common bile duct. The following ERCP procedure for stone removing was only partially successful. After recurring of inflammatory and cholestasis parameters, the choledochus duplicate was resected (Fig. 3) by means of biliodigestive anastomosis. Intraoperatively, a massive dilated ductus hepatocholedochus is shown, as well as a slender left main bile duct (Fig.4a,b). After resection of the right bile duct on the pancreatic upper edge, the latter measures 2 cm in diameter (Fig.4a,b). The intraoperative preparation follows the two bile ducts up to cranial, which is continued into the normal intrahepatic bile duct system (Fig.1). Immediately proximal to the communicating connection between the two ducts, the resection occurs at the border to the intrahepatical normal bile duct system and attachment of a biliodigestive anastomosis by means of a retrocolitical pulled Roux-Y jejunal loop. There was an uncomplicated postoperative course with an antibiotic therapy administered over 10 days, because of the existing cholangitis. Histology showed no signs of malignancy. The final control 14 days postoperatively was inconspicuous with a decrease of transaminases. One month after operation the patient was already 20% more workable, after another month the patient worked at full capacity. Results In patients with recurrent cholangitis an anatomical variant must be considered, especially after removing the gall bladder and the lack of complete recovery. In the rare cases of types Va (5) and Vb (1) is a risk of malignancy up to 25%, as well as frequently occurring complicated choledocholithiasis. Therefore according to recommended literature the preoperative diagnosis is essential for the planning of the therapeutic strategy by means of biliodigestive anastomosis. Conclusion A. Schulz 1 , F. Boxberger 2 , A. Heinle 3 , S. Schär 3 , C. von der Lippe 1 , F. Hetzer 1 Fig.1 Duplication of the common bile duct system type Vb, schematic presentation 1. Arora A. et al. Common bile duct duplication: The more the murkier. Saudi J Gastroenterology 2015;2:51-4 2. Hammad T. et al, Two cases of Type Va extrahepatic bile duct duplication with distal Klatskin Tumor surgically treated with Whipple procedere and Hepaticojejunostomy,ACG Case Rep J 2015 ;3 (1) : 49-52 3. Kim S.W. et al. Duplication of the extrahepatic bile duct in association with choledocholithiasis as depicted by MDCT, Korean J Radiol 2008; 9 : 550 – 554 4. Gupta V., Chandra A., Duplication of the extrahepatic bile duct, Congenital Anomalies 2012; 52, 176 - 178 References Fig.2b MRCP coronal slice, on the left side Ductus hepatocholedochus dexter with a Choledocholithiasis, on the right side Ductus hepatocholedochus sinister without stones Fig.2a MRCP axial slice, showed the duplication of the common bile duct Fig.3 Intraoperative situs Fig.4 Resection of the duplication with the blue marked dilated right common bile duct; a closed, b open a b
Transcript of Duplication of the common bile duct A case report€¦ · Duplication of the common bile duct –A...

Duplication of the common bile duct – A case report
1 Department of Surgery, Spital Linth, Uznach, Switzerland, 2 Department of Medicine, Gastroentrology, Spital Linth, Uznach, Switzerland,3 Department of Radiology, Cantonal Hospital of St. Gallen, St. Gallen, Switzerland
Anatomical variants of the extrahepatic bile duct system occur in
approximately 42% of the population. On the other hand, duplication of
the common bile duct is a very rare congenital abnormality, which is
often associated with recurrent cholangitis or pancreatitis, as well as
an increased risk of malignant degeneration. Therefore diagnostics
using MRI and ERCP as well as the therapeutic strategy are a
challenge. Classification and division according to Choi et al. describe
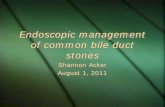
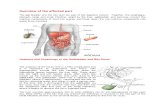
5 different types of anatomical variants of the common bile duct. Ourcase presents a patient with a duplication of the DHC type Vb (Fig. 1).
Introduction
We have treated a 50-year-old woman, who presented herself with
severe coliform epigastric pain and febrile temperature. The gall
bladder has been removed several years ago due to severe
cholecystitis with cholecystolithiasis. A cholestatic hepatopathy was
found as well. However the duplication of the common bile duct was
not detected. At present the patient showed increasing inflammation
values under antibiotic therapy and the suspicion of cholangitis.
Case Report
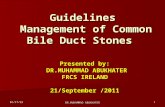
The performed MRCP showed a duplication anomaly (Fig. 2a) and a
choledocholithiasis (Fig. 2b) of the right common bile duct.
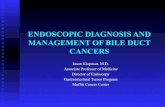
The following ERCP procedure for stone removing was only partially
successful. After recurring of inflammatory and cholestasis parameters, the
choledochus duplicate was resected (Fig. 3) by means of biliodigestive
anastomosis. Intraoperatively, a massive dilated ductus hepatocholedochus
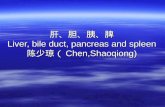
is shown, as well as a slender left main bile duct (Fig.4a,b). After resection of
the right bile duct on the pancreatic upper edge, the latter measures 2 cm in
diameter (Fig.4a,b). The intraoperative preparation follows the two bile ducts
up to cranial, which is continued into the normal intrahepatic bile duct system
(Fig.1). Immediately proximal to the communicating connection between the
two ducts, the resection occurs at the border to the intrahepatical normal bile
duct system and attachment of a biliodigestive anastomosis by means of a
retrocolitical pulled Roux-Y jejunal loop.
There was an uncomplicated postoperative course with an antibiotic therapy
administered over 10 days, because of the existing cholangitis. Histology
showed no signs of malignancy.
The final control 14 days postoperatively was inconspicuous with a decrease
of transaminases. One month after operation the patient was already 20%
more workable, after another month the patient worked at full capacity.
Results
In patients with recurrent cholangitis an anatomical variant must be considered, especially after removing the gall bladder and the lack of complete recovery. In the
rare cases of types Va (5) and Vb (1) is a risk of malignancy up to 25%, as well as frequently occurring complicated choledocholithiasis. Therefore according torecommended literature the preoperative diagnosis is essential for the planning of the therapeutic strategy by means of biliodigestive anastomosis.
Conclusion
A. Schulz1, F. Boxberger2, A. Heinle3, S. Schär3, C. von der Lippe1, F. Hetzer1
Fig.1
Duplication of the common bile duct system
type Vb, schematic presentation
1. Arora A. et al. Common bile duct duplication: The more the murkier. Saudi J Gastroenterology 2015;2:51-4
2. Hammad T. et al, Two cases of Type Va extrahepatic bile duct duplication with distal Klatskin Tumor surgically treated with Whipple procedere and Hepaticojejunostomy, ACG Case Rep J 2015 ;3 (1) : 49-52
3. Kim S.W. et al. Duplication of the extrahepatic bile duct in association with choledocholithiasis as depicted by MDCT, Korean J Radiol 2008; 9 : 550 – 554
4. Gupta V., Chandra A., Duplication of the extrahepatic bile duct, Congenital Anomalies 2012; 52, 176 - 178
References
Fig.2b MRCP coronal slice,
on the left side Ductus hepatocholedochus dexter with a Choledocholithiasis,
on the right side Ductus hepatocholedochus sinister without stones
Fig.2a
MRCP axial slice, showed
the duplication of the
common bile duct
Fig.3 Intraoperative situs
Fig.4 Resection of the duplication with the blue marked dilated right common bile duct;
a closed, b open
a b