Emergency cholecystectomy for benign gallbladder diseases ...

Formosan Journal of Surgery (2013) 46, 208e210
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: www.e-f js .com
CASE REPORT
Duplication of gallbladder with a commonneck: A rare anatomical malformation
Tariq Ahmed Mala a,*, Shahid Amin Malla b, Rahul Gupta c,Niharika Ved a, Ved Bushan Gupta a, Imtiaz Shah d
aDepartment of Surgery, ASCOMS and Hospital, Sidhra Jammu (J and K) 180017, Indiab Shyam Shah Medical College, Rewa (M.P.), Indiac SPMCHI, SMS Hospital, Jaipur, Rajasthan, IndiadDepartment of Urology, ASCOMS and Hospital, Sidhra Jammu (J and K) 180017, India
Received 21 June 2013; received in revised form 18 July 2013; accepted 24 September 2013Available online 19 November 2013
KEYWORDSbiliary anomalies;double gallbladder
Conflicts of interest: All authorsfinancial or non-financial conflicts of inmatter or materials discussed in the m* Corresponding author. Departmen
Hospital, Sidhra Jammu (J and K) 180E-mail address: drtariq_6481mala@
1682-606X/$ - see front matter Copyrhttp://dx.doi.org/10.1016/j.fjs.2013.
Summary Gallbladder duplication is a rare congenital anomaly. We report a rare case of dou-ble gallbladder in a young female, which was missed on ultrasonography, but was successfullytreated by open cholecystectomy. It is paramount for an operating surgeon to be familiar withthe anatomical details of the biliary system to prevent any inadvertent injury to the commonbile duct and hepatic artery.Copyright ª 2013, Taiwan Surgical Association. Published by Elsevier Taiwan LLC. All rightsreserved.
1. Introduction
Gallbladder duplication is a rare anatomical malformationoccurring in about 1/4000 births.1 Anatomical variations inthe biliary system are associated with higher chances ofcommon bile duct injury, especially during laparoscopiccholecystectomy.2e5 Preoperative imaging is helpful for
declare that they have noterest related to the subjectanuscript.t of Surgery, ASCOMS and017, India.rediffmail.com (T.A. Mala).
ight ª 2013, Taiwan Surgical Asso09.001
diagnosis. Surgical removal of both gallbladders withintraoperative cholangiography seems to be the appro-priate treatment.
2. Case report
A 35-year-old female presented with fatty dyspepsia asso-ciated with recurrent postprandial abdominal distentionwithout any pain, nausea, vomiting, jaundice, or fever.Physical examination showed no abdominal tenderness.Laboratory values, serum biochemistry, C-reactive proteinand liver functions were normal. Ultrasound examination ofthe abdomen showed a distended gallbladder and choleli-thiasis, without any anatomical variation (Fig. 1). The
ciation. Published by Elsevier Taiwan LLC. All rights reserved.

Figure 1 Distended gallbladder with multiple calculi.
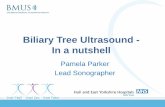
Figure 3 Duplication of gallbladder with tip of arterial for-ceps in common neck (black arrow).
A rare anatomical malformation 209
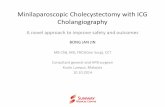
patient underwent open cholecystectomy. At exploration,duplication of the gallbladder was confirmed as a Y-shapedtype (vesica fellea divisa). Both the gallbladders, with theduct showing common cystic figures, were removed in thesame procedure (Figs. 2 and 3). The bile duct was tracedand was found to be normal (Fig. 4), and so there was noneed for intraoperative cholangiography. On follow-up, thepatient was doing well without any complaints.
3. Discussion
In the 5th or early 6th week of gestation, the gallbladderprimordium may become bifurcated and lead to duplica-tion. A split in the primordium leads to formation ofduplication, while a true accessory gallbladder results froman extra primordium. It has been found in 1/4000 births.1,6
The first reported human case was noted in a sacrificialvictim of Emperor Augustus in 31 BC.5 The following isBoyden’s classification1,7: (1) vesica fellea divisa (bilobedor bifid gallbladder, double gallbladder with a commonneck); (2) vesica fellea duplex (double gallbladder with twocystic ducts), (i) Y-shaped type (the two cystic ducts unitingbefore entering the common bile duct) and (ii) H-shaped
Figure 2 Duplication of gallbladder with two stones in eachfundus (arrows).
type (ductular type, the two cystic ducts entering sepa-rately into the biliary tree). In our case, it was a bilobedgallbladder with a common neck. Clinically it may beasymptomatic as in our case, or the symptoms may be inthe form of acute or chronic cholecystitis, cholelithiasis,empyema, torsion, cholecystocolic fistula, lump in theabdomen, and carcinoma.2e8 Several publications havereported successful laparoscopic surgery for bilobed oreven trilobed gallbladders.2,4,8,9 In asymptomatic patientswith duplication of the gallbladder, cholecystectomy isusually not advised.2 Ultrasonography, magnetic resonance
Figure 4 Single cystic duct stump held by artery forceps withnormal common bile duct.

210 T.A. Mala et al.
cholangiopancreatography (MRCP), computed tomographyscanning, scintigraphy, and oral cholecystography are not100% sensitive in identifying biliary ductal anomalies. Theultrasonography can help diagnose duplication of the gall-bladder sometimes on the basis of certain points,10 how-ever, ultrasonographic appearance may be confused withthat of choledochal cysts, gallbladder diverticulum, Phry-gian cap, extrinsic fibrous bands across the gallbladder, anda folded gallbladder of Horattas. In our case, preoperativeultrasonography was performed, which showed normalbiliary anatomy except for multiple cholelithiasis, andtherefore intraoperative cholangiography was not neededbecause the rest of the anatomy was clear.
Congenital anomalies of the gallbladder are rare andmay cause diagnostic or surgical problems which can beprevented by giving special attention to the biliary ductaland arterial anatomy. Laparoscopic cholecystectomy withintraoperative cholangiography seems to be the appro-priate treatment.
References
1. Boyden EA. The accessory gallbladder: an embryological andcomparative study of aberrant biliary vesicles occurring in manand the domestic mammals. Am J Anat. 1926;38:199e231.
2. Gigot J, Van Beers B, Goncette L, et al. Laparoscopic treat-ment of gallbladder duplication: a plea for removal of bothgallbladders. Surg Endosc. 1997;11:479e482.
3. de Leeuw TG, Verbeek PC, Rauws EA, Gouma DJ. A double orbilobar gallbladder as a cause of severe complications after(laparoscopic) cholecystectomy. Surg Endosc. 1995;9:998e1000.
4. Borghi F, Giraudo G, Geretto P, Ghezzo L. Perforation of misseddouble gallbladder after primary laparoscopic cholecystec-tomy: endoscopic and laparoscopic management. J Lapa-roendosc Advan Surg Tech. 2007;18:429e431.
5. Udelsman R, Sugarbaker PH. Congenital duplication of thegallbladder associated with an anomalous right hepatic artery.Am J Surg. 1985;149:812e815.
6. Custo Garcia J, Weber A, Seerano Berry F, Tanur Tatz B. Doublegallbladder treated successfully by laparoscopy. J Lapa-roendosc Surg. 1993;3:153e155.
7. Lamah M, Karanjia ND, Dickson GH. Anatomical variations ofthe extrahepatic biliary tree: review of the world literature.Clin Anat. 2001;14:167e172.
8. Horattas MC. Gallbladder duplication and laparoscopic man-agement. J Laparoendosc Adv Surg Tech A. 1998;8:231e235.
9. Schroeder C, Draper KR. Laparoscopic cholecystectomy fortriple gallbladder. Surg Endosc. 2003;9:1322.
10. McDonald KL, Lwin T. Sonographic and scintigraphic evaluationof gallbladder duplication. Clin Nucl Med. 1986;11:692e693.