DELIRIUM PREVENTION.. A NON - PHARMACOLOGICAL …...•Pre-delirium care bundle
Upload
sylvia-robertsonCategory
view
213download
0
Duke GEC
www.interprofessionalgeriatrics.duke.edu
Delirium Teaching Rounds: Insult to Injury
October 7, 2011

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Objectives
• Identify risk factors and key presenting features of delirium
• Appreciate the role of different professions in recognition and management
• Find opportunities to improve communication about delirium
Duke GEC
www.interprofessionalgeriatrics.duke.edu
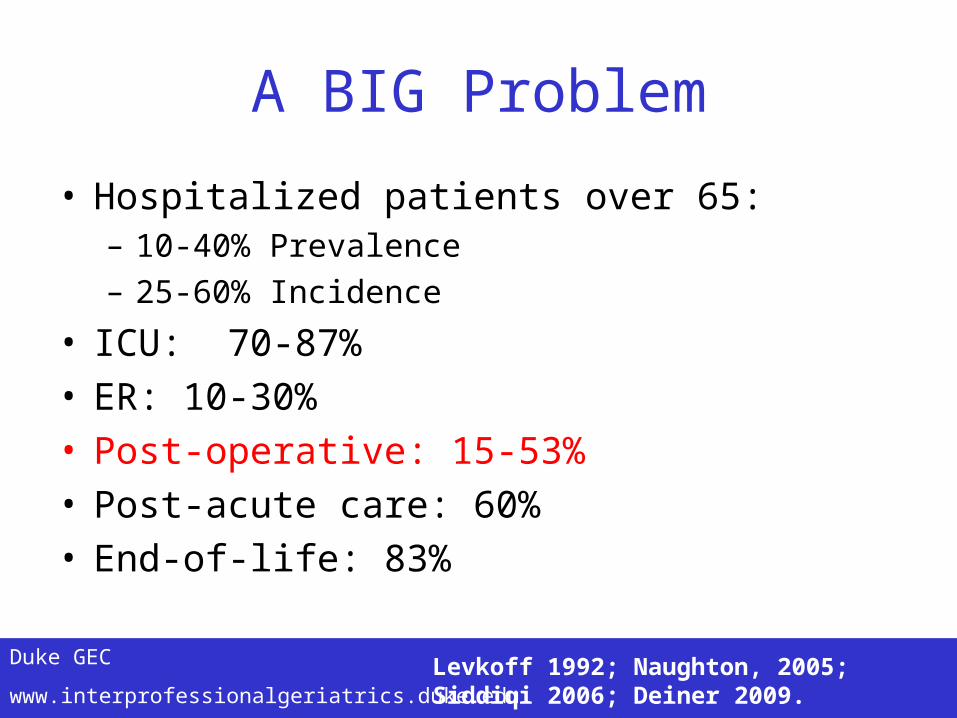
A BIG Problem
• Hospitalized patients over 65: – 10-40% Prevalence– 25-60% Incidence
• ICU: 70-87%• ER: 10-30%• Post-operative: 15-53%• Post-acute care: 60%• End-of-life: 83%
Levkoff 1992; Naughton, 2005; Siddiqi 2006; Deiner 2009.
Duke GEC
www.interprofessionalgeriatrics.duke.edu
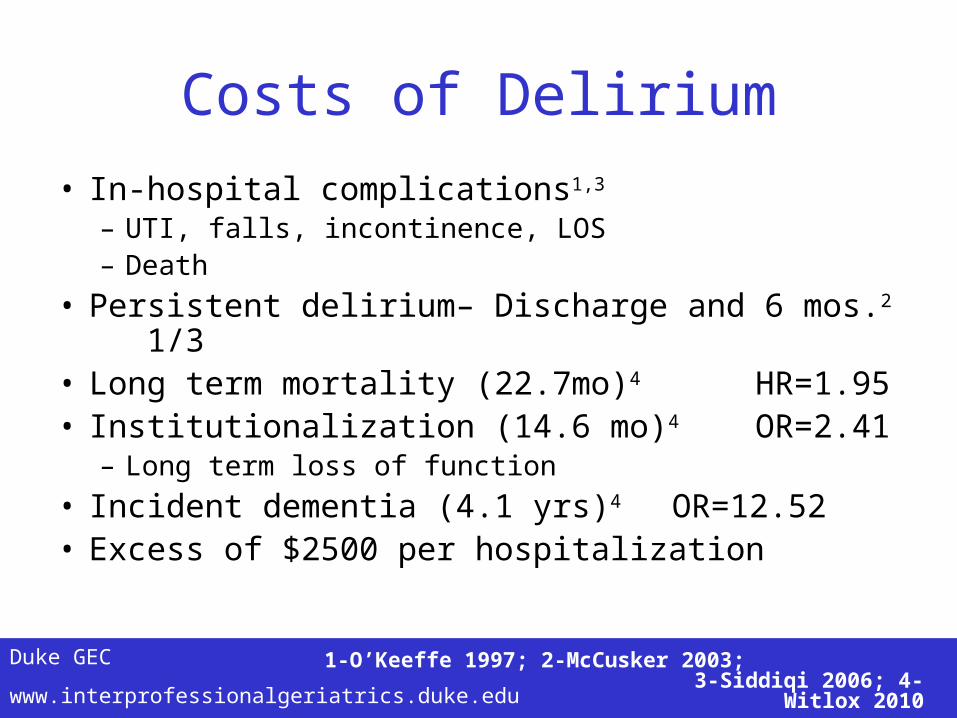
Costs of Delirium• In-hospital complications1,3
– UTI, falls, incontinence, LOS– Death
• Persistent delirium– Discharge and 6 mos.2 1/3• Long term mortality (22.7mo)4 HR=1.95• Institutionalization (14.6 mo)4 OR=2.41
– Long term loss of function• Incident dementia (4.1 yrs)4
OR=12.52• Excess of $2500 per hospitalization
1-O’Keeffe 1997; 2-McCusker 2003; 3-Siddiqi 2006; 4-Witlox 2010

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Clinical Features of Delirium
• Acute or subacute onset• Fluctuating intensity of symptoms • Inattention • Disorganized thinking• Altered level of consciousness
– Hypoactive v. Hyperactive• Sleep disturbance• Emotional and behavioral problems

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Insult to Injury
• Mrs. F is a 78 year old resident of Durham admitted after a fall in her home…..
• Gather with others in your profession• Read the case and discuss the questions• Designate a spokesperson• Have fun!

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Improving The Odds of Recognition
• Prediction by risk– Predisposing and precipitating factors
• Team observations– Nursing notes
• Clinical examination– CAM
Duke GEC
www.interprofessionalgeriatrics.duke.edu
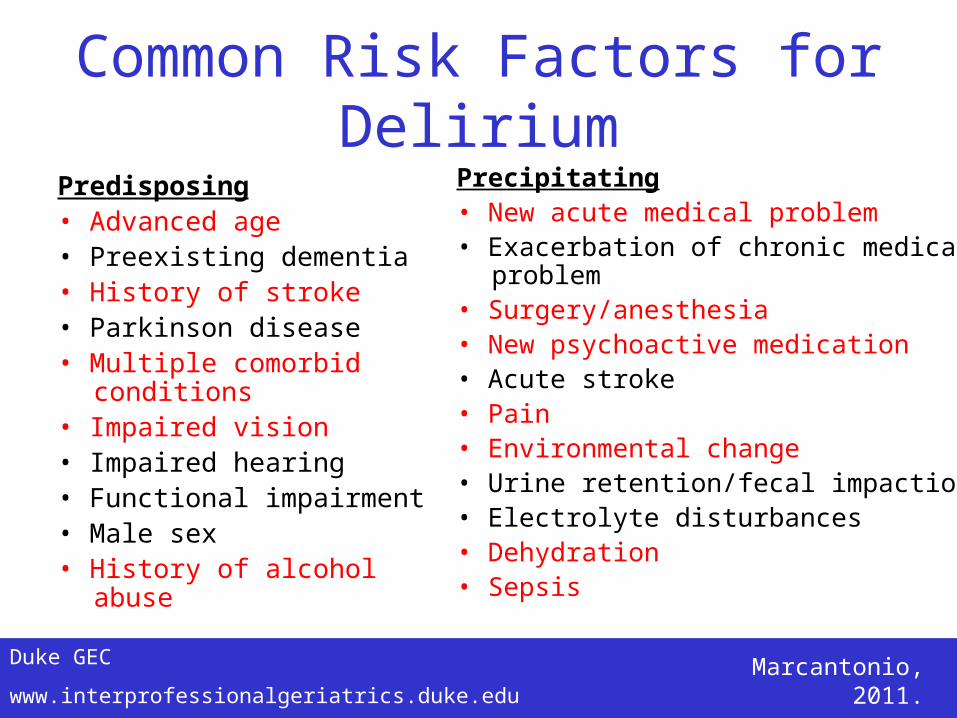
Common Risk Factors for DeliriumPredisposing• Advanced age• Preexisting dementia• History of stroke• Parkinson disease• Multiple comorbid conditions• Impaired vision• Impaired hearing• Functional impairment• Male sex• History of alcohol abuse
Precipitating• New acute medical problem• Exacerbation of chronic medical problem• Surgery/anesthesia• New psychoactive medication• Acute stroke• Pain• Environmental change• Urine retention/fecal impaction• Electrolyte disturbances• Dehydration• Sepsis
Marcantonio, 2011.
Duke GEC
www.interprofessionalgeriatrics.duke.edu
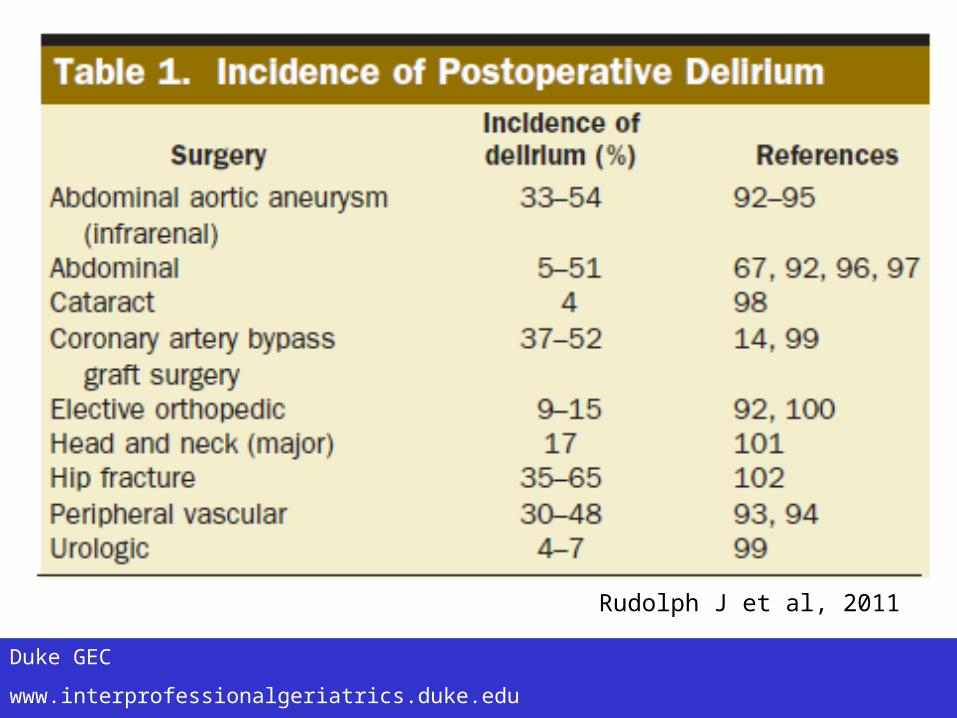
Rudolph J et al, 2011

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Rudolph J et al, 2011

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Team Input• Chart Screening Checklist• Nurses’ commonly charted behavioral signs
(Sensitivity= 93.33%, Specificity =90.82% vs CAM)• Pulling at tubes, verbal abuse, odd behavior,
“confusion”, etc• 97.3% of diagnoses of delirium can be made by
nurses’ notes alone using CSC• 42.1% of diagnoses made by physicians’ notes alone
using CSC
Kamholz, AAGP 1999

Duke GEC
www.interprofessionalgeriatrics.duke.edu
1 month before adm PCP Note Episode of confusion following her knee surgery. She does not feel confused presently.
Presents to ED 20:20 ED Verbally converses and oriented 5
Day Admitted 01:25 Adm Data She can’t tell me how many stairs she fell down. She is a little disoriented…reports ~2 beers per day which puts her at risk for withdrawal...monitor closely for signs/symptoms of withdrawal.
Day Admitted 03:05 PRM 10:40 AM BSN Findings: Independent prior to admission: Newly dependent
Hospital Day 1 03:10 Nursing Patient is very drowsy.
Hospital Day 1 10:14 OT Cognition: Alert, changed to lethargic once medication had taken affect.
Hospital Day 1 11:40 PT Cognition: Impaired…Oriented to self, place, time, situation, with significant prompting.
Hospital Day 1 17:25 Post Anesthesia Reports mild post-operative confusion, but per husband significantly better anesthesia recovery than the previous surgery 1 year prior.
Hospital Day 1 18:55 Nursing Pt a/o x 3, unaware of correct date/time…pulling at soft cast on left hand but reorients well.
Hospital Day 1 22:22 Nursing Pt is alert and orientedx4, with mild anxiety present…pulling wrap to arm…told numerous times to leave it alone…order for a hand mitt restraint…is aware if tugging again will be restrained.
Hospital Day 2 03:03 Nursing alert and orientedx2-3, with mild anxiety and occasional hallucinations… pulled out foley catheter...pulled at cast… Bilat hand mitts and wrist restraints were applied.
Hospital Day 2 14:04 Nursing Pt. AOx1-2, very agitated and restless at times... Pt. resting quietly at this time. Family at bedside.
Hospital Day 4 15:00 PT The patient reports "Take this off of me (referring to restraints and mits) so I can run an errand."
Hospital Day 4 18:52 Nursing Pt s/p right radial fracture, right hip fracture, now with delirium r/t possible alcohol w/d.
Hospital Day 5 05:08 Nursing Has been agitated…Sitter at bedside. Restraints. Pt not agitated at the time the BP taken.
Hospital Day 5 18:32 Nursing A&ox4 today with some stm deficits noted.
Hospital Day 5 15:01 Nursing PATIENT CAN BE IMPULSIVE AT TIMES…EMOTINOAL SUPPORT GIVEN

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Substance Abuse and Older AdultsAlcohol can trigger/exacerbate serious
problems including:
• High blood pressure, arrhythmias and heart attacks
• Stroke • Impaired immunity • Cirrhosis / liver diseases • Osteoporosis • GI bleeding • Depression, anxiety, and other
mental health problems • Malnutrition • Sleep disturbances
• Alcohol is the major substance abuse/misuse problem among older adults.
• Approx. 2.5 million older adults in the US have alcohol related problems.
• Physiological changes affecting alcohol metabolism with aging:– Decrease in body water – Increased sensitivity/
decreased tolerance – Decrease in the metabolism in
GI tract

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Substance Abuse and Older AdultsEarly Onset – “hardy survivor”
• Majority are early onset drinkers – Drink for the same reasons younger
people do - to cope with psychosocial or medical problems
• Comorbidities include depression, bipolar disease, and thought disorders
• More health problems
• Continue established drinking patterns as age
Late Onset• 1/3 of older adults with drinking problems
• Psychologically and physically healthier – too “normal," to raise suspicions
• More likely to have increased drinking due to recent losses: death of a spouse divorce, change in health status, life changes
• Milder and more amenable to treatment than early onset drinking problems sometimes resolves spontaneously.
Both appear to use alcohol almost daily; in social settings and at home alone.
Both more likely to use alcohol as palliative/self-medicating measure in response to hurts, losses, and affective changes.

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Duke GEC
www.interprofessionalgeriatrics.duke.edu
Management• Benzodiazepines
– Diazepam or lorazepam– Older adults may require lower doses
• Symptom triggered therapy– Clinical Institute Withdrawal Assessment Scale for Alcohol
(CIWA-A)
• Supportive therapy– Comorbidities– Hydration and nutrition
• Team care

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Mrs. F
History:•Delirium with knee replacement in 2010•4 beers a day and 2mg Clonazepam twice dailyOn presentation:•BAL=80•Na=128

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Mrs. F
Hospital Course and beyond:•Pain management•Sitters and family•Activity•Clonazepam•Geriatrics consultation

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Summary
• Maintain a high level of suspicion– Screen for alcohol use
• Document findings in the chart• Discuss with other members of the team• Inform/educate patients and families

Duke GEC
www.interprofessionalgeriatrics.duke.edu
A better way….
PsychosocialPsychosocial
PharmacologicPharmacologic
PhysiologicPhysiologic
EnvironmentalEnvironmental
Medicine
Nursing
PT/OT
Pharmacy
Social work
Nutrition
PA’s
Patients and
Caregivers
Administrators
NP’s

Duke GEC
www.interprofessionalgeriatrics.duke.edu
Delirium Teaching Rounds “Itching for a Fight!”
November 4, 2011