Ductal Carcinoma In Situ - AHN · Ductal Carcinoma In Situ A.A. Sahin, M.D. ... R Breast Biopsy ....
49
04/04/2016 1 Ductal Carcinoma In Situ A.A. Sahin, M.D. Professor of Pathology and Translation Molecular Pathology Section Chief of Breast Pathology 23 rd Annual Seminar in Pathology Outline • Incidence and natural history of DCIS • Morphologic features and differential diagnosis • Treatment of DCIS based on biologic factors • Ongoing clinical trials Outline • Morphologic features of spindle cells lesions • Differential diagnosis • Case presentations
Transcript of Ductal Carcinoma In Situ - AHN · Ductal Carcinoma In Situ A.A. Sahin, M.D. ... R Breast Biopsy ....

04/04/2016
1
Ductal Carcinoma In Situ
A.A. Sahin, M.D.
Professor of Pathology and Translation Molecular Pathology
Section Chief of Breast Pathology
23rdAnnual Seminar in Pathology
Outline
• Incidence and natural history of DCIS
• Morphologic features and differential
diagnosis
• Treatment of DCIS based on biologic
factors
• Ongoing clinical trials
Outline
• Morphologic features of spindle cells
lesions
• Differential diagnosis
• Case presentations

04/04/2016
2
Ductal Carcinoma In Situ
• Incidence: ≈ 62,000 new cases US
2015 • 25% screen detected carcinomas • 20% of our practice
Diagnosis and Management of Ductal Carcinoma in Situ
Virnig BA, Shamliyan T, Tuttle TM, et al. 2009, 1-549
Diagnosis and Management of Ductal Carcinoma in Situ
Virnig BA, Shamliyan T, Tuttle TM, et al. 2009, 1-549

04/04/2016
3
Diagnosis and Management of Ductal Carcinoma in Situ
Virnig BA, Shamliyan T, Tuttle TM, et al. 2009, 1-549
DCIS is Heterogeneous
Diverse:
–Presentation
–Clinical Features
–Biology (Behavior)
Risk of invasive cancer after biopsy alone
N Ca %
Farrow 1970 (25) 5 20
Haagensen 1971 (11) 8 73
Millis 1975 (8) 2 25
Rosen 1980 (15) 8 53
Eusebi 1994 (80) 11 14
Page 1995 (28) 9 32
Mean = 28%

04/04/2016
4
Natural history of low grade DCIS
• 28 patients with low grade identified
from 1950-1968
• 30 yrs follow up
• 11 (39%) invasive cancer
• 5 (18%) breast cancer deaths
• 4 of the 5 breast cancer deaths occurred within 15 years
M Sanders D Page et al Cancer 2005
Nurses' Health Study DCIS
• Review of 1877 breast bx specimens
• 13 bx specimens with DCIS
• Received no treatment beyond the diagnostic bx
Collins et al Cancer 2005;103:1778-84
Nurses' Health Study DCIS
Result:
compared with nonproliferative lesions
13.5 OR for DCIS for development of invasive breast carcinoma (n=6)
20.1 OR for the development of any subsequent invasive or in situ breast ca event (n = 10)
Collins et al Cancer 2005;103:1778-84
04/04/2016
5
Nurses' Health Study DCIS
4 - low nuclear grade
6 - intermediate nuclear grade
3 - high nuclear grade
0 - comedo-type necrosis
Invasive carcinomas developed among women with DCIS of all nuclear grades
All 10 breast carcinoma events (100%) were in the ipsilateral breast
Collins et al Cancer 2005;103:1778-84
Nurses' Health Study DCIS
Conclusion:
These results provided further evidence that patients with DCIS who received no treatment beyond a diagnostic biopsy were at substantially increased risk for developing ipsilateral invasive breast carcinoma, and that the increased risk in this setting was seen in DCIS of low, intermediate, and high nuclear grades
Collins et al Cancer 2005;103:1778-84
Sequential and Parallel Models of Breast Carcinogenesis
N Inv DCIS P
N
P
Inv
DCIS
Alternative model
Inv DCIS
04/04/2016
6
Differential Diagnosis
• Atypical ductal hyperplasia
• Lobular carcinoma in situ
• Intravascular tumor
• Invasive ductal carcinoma
ATYPICAL DUCTAL HYPERPLASIA
Intraductal epithelial proliferation
with some, but not all features of
low grade intraductal carcinoma
Definition
ATYPICAL DUCTAL HYPERPLASIA
Intraductal epithelial proliferation
with cytologic features identical to
low grade intraductal carcinoma but
lacks architectural features or
quantitatively too small
Revised Definition

04/04/2016
7
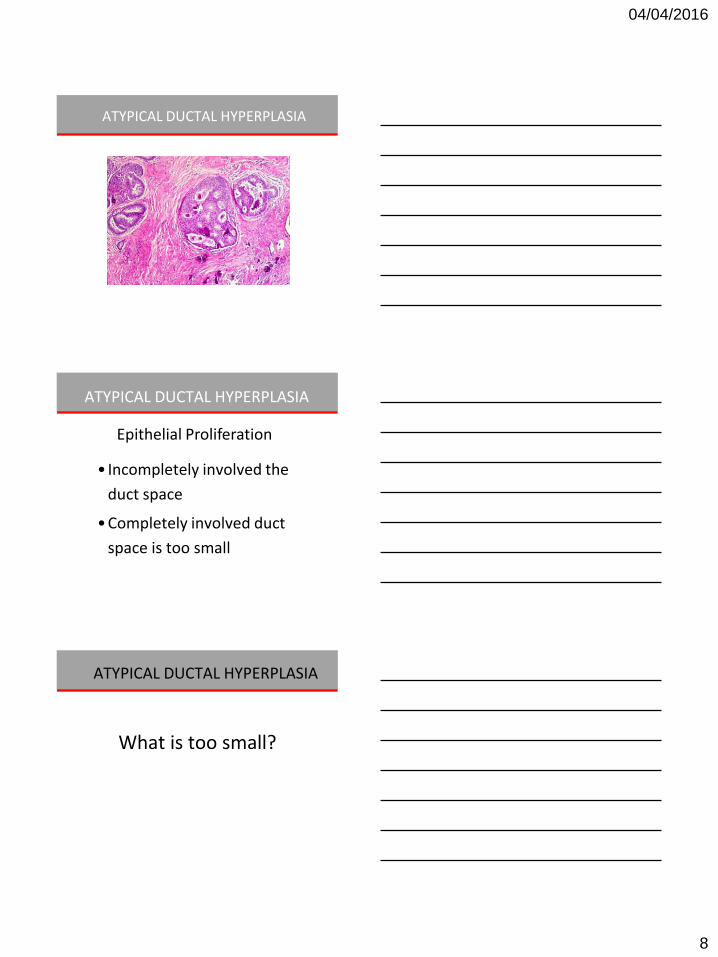
FEATURES OF DCIS
•Uniform population of cells
•Smooth geographic spaces with even cellular placement
•Hyperchromatic nuclei
ATYPICAL DUCTAL HYPERPLASIA
• Monotonous, uniform rounded cell
population
• Organized nuclear distribution
• Subtle increase in N/C ratio
Cytologic Features
ATYPICAL DUCTAL HYPERPLASIA
04/04/2016
8
ATYPICAL DUCTAL HYPERPLASIA
ATYPICAL DUCTAL HYPERPLASIA
• Incompletely involved the
duct space
• Completely involved duct
space is too small
Epithelial Proliferation
ATYPICAL DUCTAL HYPERPLASIA
What is too small?

04/04/2016
9
ATYPICAL DUCTAL HYPERPLASIA
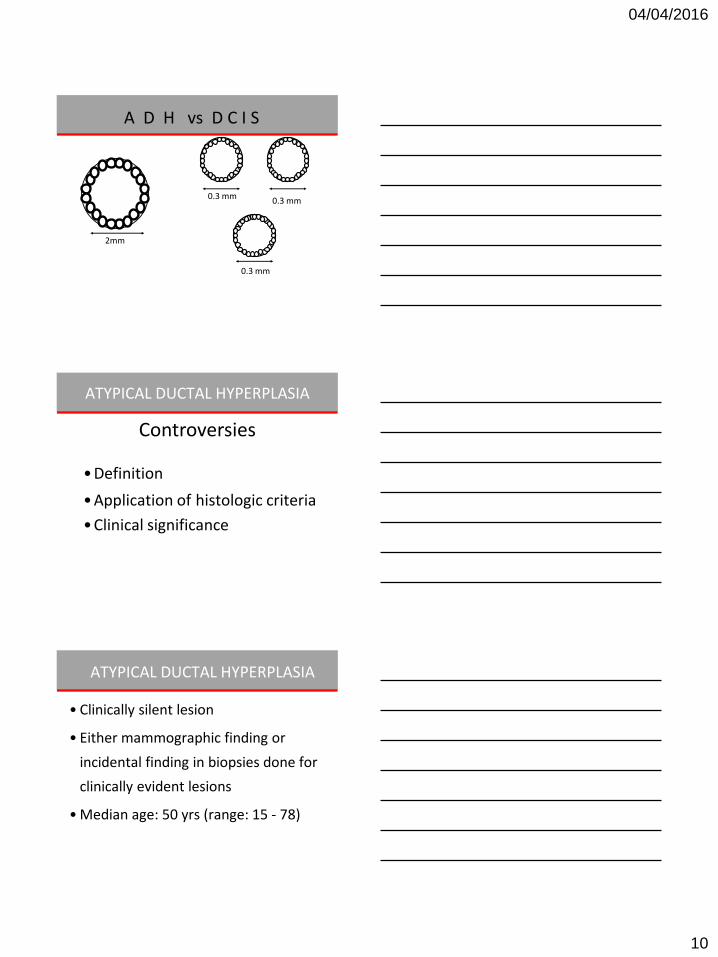
• Two membrane bound spaces
• 2 mm in aggregate cross-sectional
diameter
Quantitative Criteria
A D H
1mm 1mm
1mm 1mm
D C I S
04/04/2016
10
2mm
0.3 mm 0.3 mm
0.3 mm
A D H vs D C I S
ATYPICAL DUCTAL HYPERPLASIA
• Definition
• Application of histologic criteria
• Clinical significance
Controversies
ATYPICAL DUCTAL HYPERPLASIA
• Clinically silent lesion
• Either mammographic finding or
incidental finding in biopsies done for
clinically evident lesions
• Median age: 50 yrs (range: 15 - 78)
04/04/2016
11
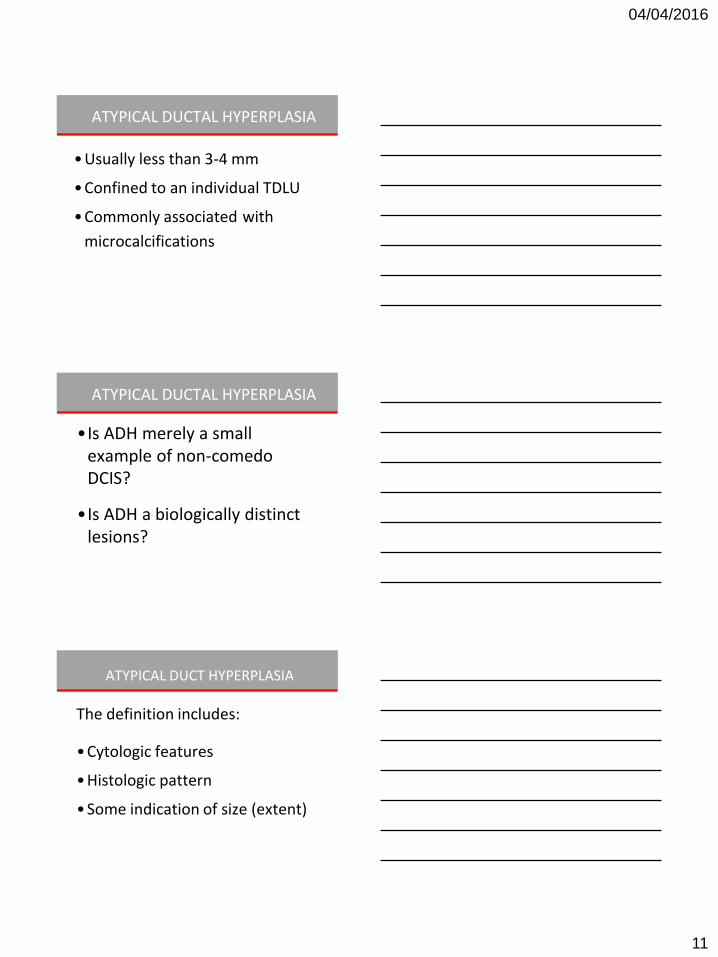
ATYPICAL DUCTAL HYPERPLASIA
• Usually less than 3-4 mm
• Confined to an individual TDLU
• Commonly associated with
microcalcifications
ATYPICAL DUCTAL HYPERPLASIA
•Is ADH merely a small example of non-comedo DCIS?
•Is ADH a biologically distinct
lesions?
ATYPICAL DUCT HYPERPLASIA
The definition includes:
• Cytologic features
• Histologic pattern
• Some indication of size (extent)

04/04/2016
12
Atypical Ductal Hyperplasia
vs
Intraductal Carcinoma
Benign
vs
Malignant
ADH vs low grade DCIS
Are they distinct entities?
Intraductal Epithelial Proliferations of Breast

04/04/2016
13
Yes • Magnitude of risk
varies
• Laterality of risk different
• Type of subsequent ca. histology different
No
• Histologic criteria poorly defined difficult to have standard criteria
• Molecular/geneticfeatures are similar
• ADH appears to be a neoplastic, clonal proliferation of cells identical to those of low grade DCIS
• Less completely developed
ADH vs DCIS
• AH are “markers” of generalized increase in risk and not precursor lesions
• Family history more than doubles breast cancer risk among women with AH
• Among women with AH, risk highest in first 10 years after bx.
Changing Views of AH

04/04/2016
14
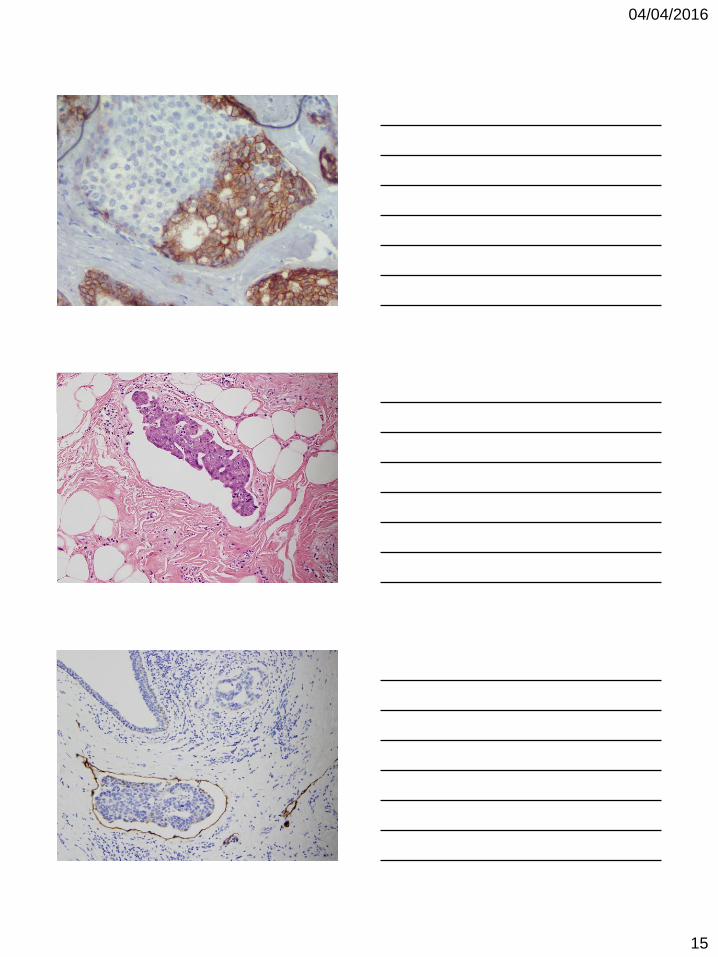
A D H / D C I S
A D H / D C I S
04/04/2016
15

04/04/2016
16
Challenges:
- Understanding molecular genetic pathogenesis
- Identification of clinical relevance
- Effective strategies for management
- Development of reproducible criteria for
classification
Classification of In situ Epithelial Proliferations the Breast
Classification of In situ Epithelial Proliferations the Breast
Usual hyperplasia
Hyperplastic Neoplastic
“Malignant” “Benign”
“Well-informed” DCIS ? Some forms
of LCIS
ADH / low grade DCIS ? Lob Neoplasia ? Columnar alteration
carcinoma in situ adenoma /
neoplasia /low grade
DCIS
Allelic imbalance analysis suggests
that low grade & high grade
carcinomas follow different genetic
pathways
Roylance et al. J Pathol 2002; 196:32-36
Classification of In situ Epithelial Proliferations the Breast

04/04/2016
17
Genetic alterations
LOH Studies
UDH Approx 10% (0-30%) usually one locus only
ADH Approx 50% Similar loci to low grade DCIS and similar Alterations found in subsequent inv ca of same breast
50 – 80% numerous sites (similar to inv ca)
DCIS
Bocker et al Virchow Arch A Pathol Anat 421 315 & 323, 1992 Shoker et al J Pathol 188; 237, 1999 put on an excel spreadsheet
Hyperplasia Neoplasia
CK 5, 6, 14 + -
ER Heterogeneous Homogeneous

04/04/2016
18
Breast Carcinogenesis Model
Moulis & Sgroi, 2008
LOH 16q
Her-2 and p53
Lobular Carcinoma
High Grade Carcinoma
Low Grade Carcinoma
16q
High Grade Pathway
E Cadherin
17q
?Common Precursor
Low Grade Pathway
04/04/2016
19
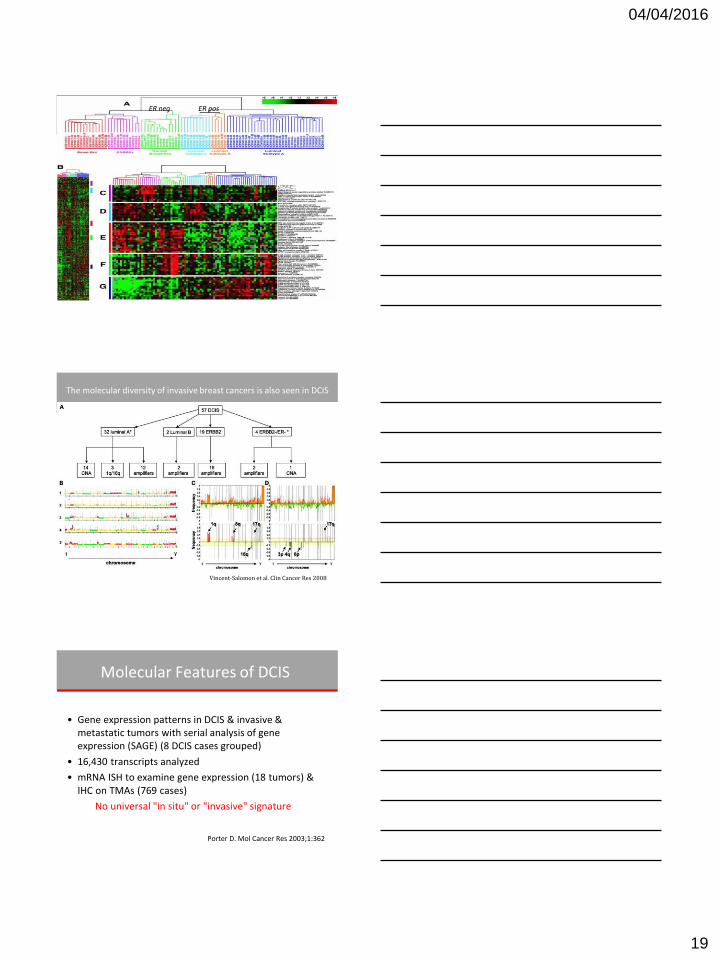
Sorlie, et al.
PNAS 2001
ER neg ER pos
The molecular diversity of invasive breast cancers is also seen in DCIS
Vincent-Salomon et al. Clin Cancer Res 2008
Molecular Features of DCIS
• Gene expression patterns in DCIS & invasive & metastatic tumors with serial analysis of gene expression (SAGE) (8 DCIS cases grouped)
• 16,430 transcripts analyzed
• mRNA ISH to examine gene expression (18 tumors) & IHC on TMAs (769 cases)
No universal "in situ" or "invasive" signature
Porter D. Mol Cancer Res 2003;1:362
04/04/2016
20
DCIS Heterogeneity
• Morphologic and biologic diversity has important implications with regard to mammographic evaluation, distribution in the breast and patient management
Clinical Behavior
Clinical Factors
Young age
Genetic background
Treatment Factors Extent of excision Use of XRT
Use of hormonal therapy
Tumor Factors
Size/extent of lesion
Nuclear grade/necrosis
Volume of DCIS at margin
D C I S
Determination of Size
• Frequently underestimated
• Accurate assessment requires
careful evaluation of specimens
by multidisciplinary approach

04/04/2016
21
D C I S
• 50 yr old presented with
suspicious microcalcifications on
a screening mammogram
• She underwent a core biopsy
showing DCIS and had segmental
mastectomy
D C I S Pathology Report
Gross: 5 X 4 X 3 cm specimen is cross
sectioned and representative sections
are submitted in 20 cassettes
Final: DCIS measuring 0.8 cm
Margins free, closest margin 1.0 cm
Previous biopsy changes
D C I S

04/04/2016
22
XX XX
DCIS measures 0.8 cm and is 1.0 cm from the nearest margin
. . . . . . . . . .
. . . . . . .
. . . .
. . . .
.
. .
. . . . . . .
. . . . . . . . .
.

04/04/2016
23
. . . . . . . . . .
. . . . . . .
. . . .
. . . .
.
. . . . . . . . .
. . . . . . . . . .
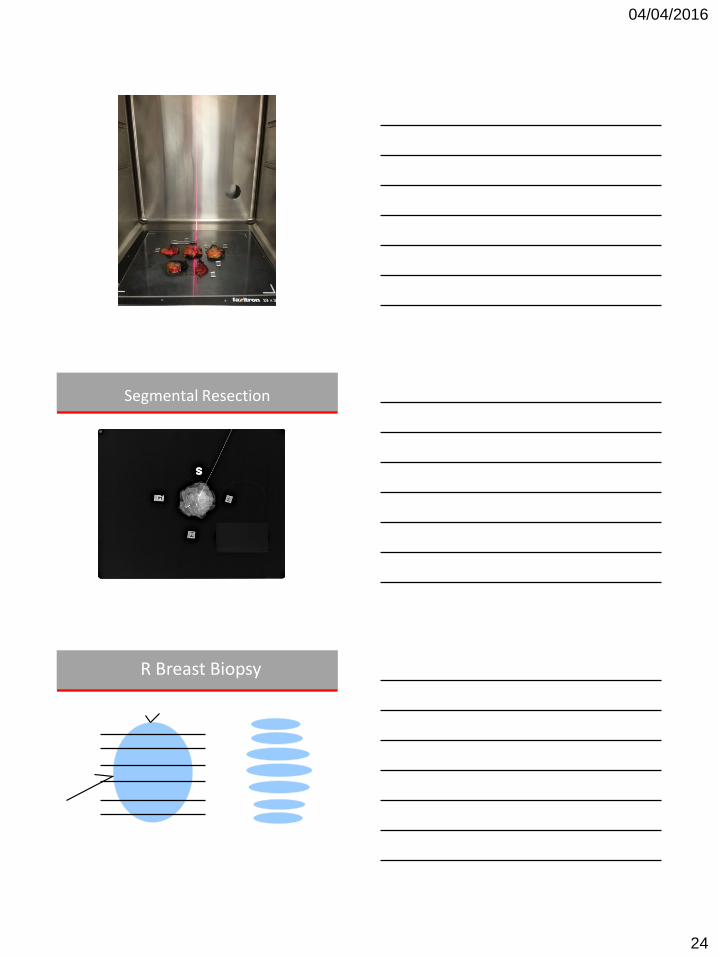
DCIS measures 5 cm and extends to multiple surgical margins
superior
lateral
R Breast Biopsy
04/04/2016
24
Segmental Resection
R Breast Biopsy

04/04/2016
25
Segmental Resection
1 3 2
4 5 6
7 8 9
10 11
12 13 14

04/04/2016
26
B18
B19 B20 B21
B22
B23
1 8
2 9
3 10
4 11
5 12
6 13
7 14
X
X
X
X
X
X
X
1 3 2
4 5 6
7 8 9
10 11
12 13 14
5 12
04/04/2016
27
S
M L X
X X X
X
X
X
I
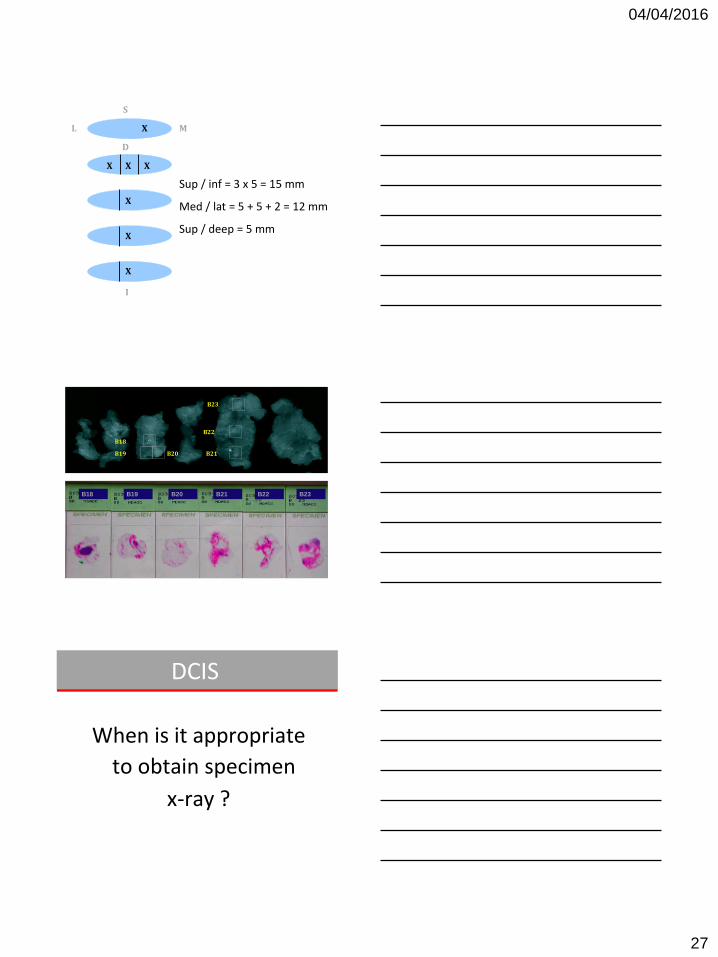
Sup / inf = 3 x 5 = 15 mm
Med / lat = 5 + 5 + 2 = 12 mm
Sup / deep = 5 mm
D
B18 B19 B20 B21 B22 B23
B18
B19 B20 B21
B22
B23
DCIS
When is it appropriate
to obtain specimen
x-ray ?

04/04/2016
28
DCIS Whenever preoperative
mammographic findings suggest
that extent of the disease may not
be appreciated by gross
evaluation
DCIS
DCIS

04/04/2016
29
DCIS
DCIS
•Clinically relevant
•Reproducibly applicable by different observers
DCIS
• Histologic grading should include:
• nuclear grade
• architectural pattern
• presence of necrosis
2012 Consensus Conference of the Classification of DCIS

04/04/2016
30
+
-
-
Low
low
near diploid
1q+, 16q-
No; 8p11.2-p12 (rare)
Luminal A > B
ER/PR
Her2/neu
p53
Proliferation
Number of changes
Ploidy
Recurrent changes
Amplifications
Molecular subtype
+/-
-/+
-/+
Variable
intermediate
aneuploid (50%)
1q+, 8p-, 11q-, 16q-,
8p11.2-p12, 11q13
Luminal A, B
-/+
+/-
+/-
High
High
frequently aneuploid
1q+, 3q+, 17q+, 8q+, 5q-, 11q-,
14q-, 8p-, 13q-
17q12, 6q22, 8q22,11q13, 20q13
Luminal B, Her2, Basal
DCIS Heterogeneity
LG IG HG
DCIS
Most important factor in
successful treatment
Margin Status
DCIS
• Negative
• Positive
?
04/04/2016
31
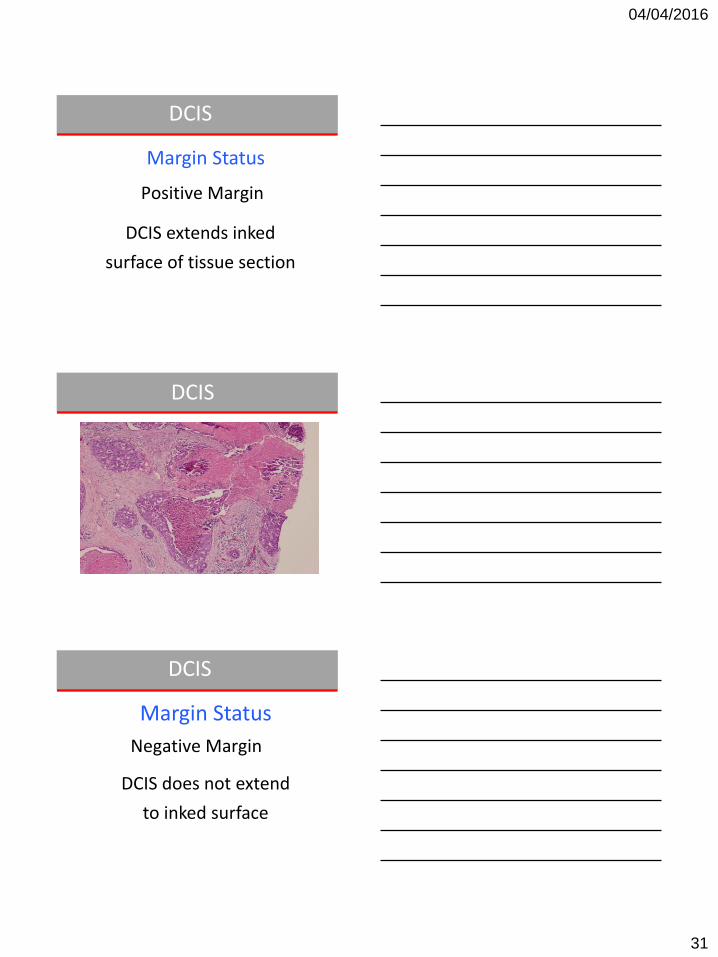
DCIS
Positive Margin
DCIS extends inked
surface of tissue section
Margin Status
DCIS
DCIS
Negative Margin
DCIS does not extend
to inked surface
Margin Status

04/04/2016
32
DCIS
DCIS
DCIS

04/04/2016
33
DCIS
DCIS
DCIS

04/04/2016
34
Margin Evaluation
• For DCIS 50 %
• For inv. ca 5-20 %
Residual disease with < 1 mm clearance
Mathias Worni et al. JNCI J Natl Cancer Inst 2015;107:djv263
Time trends of treatment and survival among Ductal Carcinoma in Situ
Total Mastectomy for DCIS
N Recurrence
Follow-up (yrs)
Farrow et al’70 181 1 5-20
Sunshine et al’85 68 3 >10
Schuh et al’86 52 1 5.5
Fisher et al ’86 28 1 3.2
Arneson et al’89 28 0 6.4
Silverstein et al’95
167 2 6.5

04/04/2016
35
Grade of Invasive Ca Developing within DCIS
Histological grade of invasive ca DCIS grade I II III Total
Low 13
81%
3
19%
0 16
Intermediate 22
24%
63
70%
5
6%
90
High 3
1%
90
42%
119
56%
212
318 Cadman et al. The Breast (1997) 6, 132-137; Olubunmi et al (1994) Seminar in Diag Path 11, 215-222
% Local Recurrence after WLE alone
N All Invasive
NSABP 403 4.7 2.4
EORTC 500 4.2 2.0
Milan 74 4.4 2.7
Florence 106 1.9 1.0
Manchester 127 4.5 1.0
Edinburgh 67 3.5 1.2
Nottingham 97 1.9 1.0
Philadelphia 233 4.4 1.3
Mean = 3.9 1.7
Van Nuys Prognostic Index
Score 1 2 3
Size <16mm 16-40mm >40mm
Margin width >9mm 1-9mm <1mm
Pathology Not high Not high High
No necrosis +/- Necrosis Necrosis
Age >60yr 40-60yr <40yr
Van Nuys Score
4- 6 7 – 9 10 – 12
10-yr LR free 96% 73% 37%

04/04/2016
36
DCIS
• 1804 women randomized
Tamoxifen vs. Placebo
• Ipsilateral cancer events
were evaluated
NSABP B - 24
Lumpectomy/XRT +/- Tamoxifen
DCIS
• Tamoxifen reduced the risk of developing subsequent events (invasive carcinoma or DCIS)
• 37% reduction in the event incidence
NSABP B – 24
DCIS
• ER status was determined
retrospectively in 628 patients
• 77% (428 tumors) were
ER positive

04/04/2016
37
DCIS
DCIS
IBCR ER+ ER-
7% 17%
P = <001
DCIS
04/04/2016
38
DCIS
Breast Cancer Develops Over Time
Breast cancer cells progress through changes over a period of years
Normal Duct
Ductal Hyperplasia
Ductal Hyperplasia with Atypia
Ductal Carcinoma In situ
Invasive Ductal Carcinoma
Reversible with Tamoxifen Reversible ?
Endocrine Therapy for DCIS
• All patients: Lumpectomy + XRT
• 1804 women randomized: Tamoxifen vs.
Placebo
• Breast cancer events (Ipsilateral,
Contralateral, DCIS, invasive)
NSABP B-24

04/04/2016
39
NSABP B-24 (UPDATED 12 year follow up)
Placebo Tamoxifen p
DCIS 7.6% 6.7% NS
Invasive Cancer
9% 6.6% <0.05
Placebo Tamoxifen p
8.1% 4.9% <0.05
Ipsilateral Breast Events
Contralateral Breast Events
↓ 2.4%
↓ 3.2%
JNCI Monograph, 2010
NSABP B-24 Stratification Based on ER Status
• ER determined in 732 cases – Median f/u 14.5 years
• No benefit in ER negative • HR 0.49 for all breast cancer events among ER+
DCIS • 10-year IBTR
– ER negative = 20% – ER+ placebo= 16% – ER+ tam= 10%
Allred et al, JCO, 2012
UCSF Preoperative Endocrine Treatment for ER-positive DCIS
3-month
MMG MRI
core bx
MMG MRI
Surgery
Letrozole 2.5 mg PO QD Tamoxifen 20 mg PO QD
Exclusion criteria: • palpable disease • microinvasion • not visible on MRI
N= 62
Chen et al, BMC Cancer, 2009

04/04/2016
40
Alteration of biomarker expression is associated with endocrine treatment for DCIS
Ki67 CD68
baseline
treated
Chen et al, BMC Cancer, 2009
Biomarker changes associated with endocrine treatment
0
10
20
30
40
50
60
Baseline Treated0
10
20
30
40
50
60
Baseline Treated
Ki67, premenopausal Ki67, postmenopausal
0
50
100
150
200
250
Baseline Treated
0
50
100
150
200
250
Baseline Treated
CD68, premenopausal CD68, postmenopausal
p=0.04
p=0.001 p=0.002
p=0.0.01
Chen et al, BMC Cancer, 2009
Three-Month Pre-op Endocrine Therapy in DCIS
• Preoperative endocrine therapy of ER-positive DCIS – Safe – Histologic and radiologic changes are evident
• No long term data on efficacy and the question remains in what proportion of women might this therapy actually prevent the occurrence of invasive breast cancer

04/04/2016
41
HER-2/Neu Gene Amplification in DCIS
• High grade- 56% • Low grade- 19% • This also parallels
IDC with DCIS
Hoque et al, Cancer Epi & Prev 2002
Trastuzumab for Treatment of DCIS?
HER2 3+
Kuerer et al. CANCER, 2011
Can we selectively eradicate or prevent HER-2 + invasive breast cancer ?
ER Neg HER2 +
DCIS
ER Neg HER2 + Invasive
Trastuzumab

04/04/2016
42
MDACC Preoperative Trastuzumab Schema for DCIS
DCIS
by Core Biopsy Her 2 +
C O N S E N T
Trastuzumab 8 mg/kg
X One-dose
SURGERY at 3 weeks
Segmental or
Mastectomy
•Blood •Ki67 •cCaspase-3
•Ki67
•cCaspase-3
•Pathologic & Immune Response
Trastuzumab for DCIS Trial
Clinical Pathologic Factors
• Median age: 53 yrs
• Mean Mammographic Size: 5.1 cm
• Overall ER+: 80%
• Overall HER2+: 35%
• Total eligible: 24 patients HER2 Pos
– 12 patient samples not receiving drug used as control experiments
Trastuzumab for DCIS Trial
HER2 Correlated With Grade Grade Total Percent Percent HER2+
I 6% 0%
II 38% 27%
III 56% 44%
04/04/2016
43
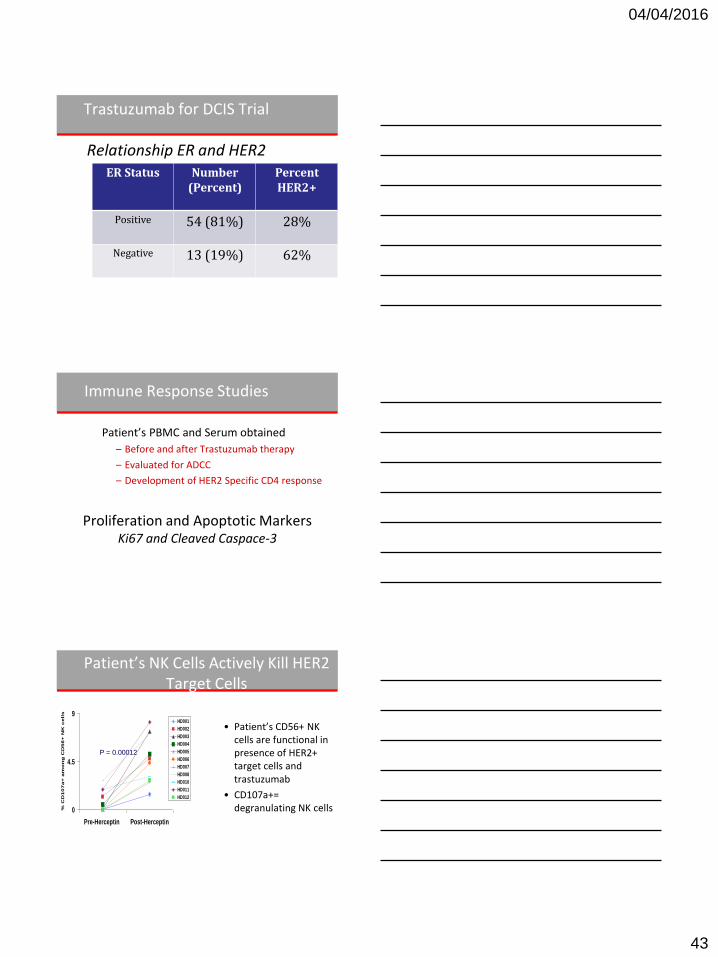
Trastuzumab for DCIS Trial
Relationship ER and HER2 ER Status Number
(Percent) Percent HER2+
Positive 54 (81%) 28%
Negative 13 (19%) 62%
Immune Response Studies
Patient’s PBMC and Serum obtained
– Before and after Trastuzumab therapy
– Evaluated for ADCC
– Development of HER2 Specific CD4 response
Proliferation and Apoptotic Markers Ki67 and Cleaved Caspace-3
Patient’s NK Cells Actively Kill HER2 Target Cells
• Patient’s CD56+ NK cells are functional in presence of HER2+ target cells and trastuzumab
• CD107a+= degranulating NK cells
CD107a Assay with autologous serum
0
4.5
9
Pre-Herceptin Post-Herceptin
% C
D1
07
a+
am
on
g C
D5
6+
NK
ce
lls
HD001
HD002
HD003
HD004
HD005
HD006
HD007
HD008
HD010
HD011
HD012
P = 0.00012
04/04/2016
44
Trastuzumab for DCIS
• Trastuzumab can induce specific immunity in pts w HER2+ DCIS after 3 weeks of treatment
• Future studies-
– PRE-surgical
– What kind of histologic response should we be looking for?
– Which biomarkers to measure?
DCIS ‘Pre-Cancer’ But Treated Like Cancer
• DCIS is a marker for development of invasive breast cancer
• Diagnosis and treatment critical
– Rule out concurrent presence of invasive carcinoma (11-25%)
– Prevent development of invasive ca
– Much like LCIS or ADH
NIH Recommendations
• Develop risk-stratification models to identify subsets of women who have DCIS who are candidates for:
– active surveillance only
– local excision only
– local excision with radiotherapy
– Mastectomy
04/04/2016
45
Treatment of DCIS =
Prevention of Invasive Cancer
Which patients will go on to develop invasive disease?
Addressing overtreatment of Screen detected DCIS; the LORIS Trial
Francis, A. et al European Journal of Cancer 51 (2015) 2296-2303
LORIS Trial in UK 2014 Watch and Wait: Active Surveillance
• Screen detected low/intermediate grade DCIS, > 46 years
• Randomize surgery versus no surgery
– Non-inferiority trial 932 patients
– Primary endpoint: invasive disease at 5 year
– Secondary: Mastectomy rate, quality of life, biomarkers

04/04/2016
46
NEW Trial Alliance-CALGB 40903: Phase II Single-Arm Study of Neoadjuvant letrozole for
ER(+) postmenopausal DCIS
3 months Letrozole
MMG MRI
core bx
MMG MRI
Surgery MRI
Clinical exam
stable or responding
progression
3 months Letrozole
regi
stra
tio
n
Measure change Ki67, Imaging-
path correlation PI: Shelley Hwang
N=96
8/1/14: 54
Women with DCIS on BX
Endpoints Primary: 1. Proliferation (Ki67 IHC) in DCIS 2. Toxicity Secondary: 1. DCIS Incidence on excision 2. Modulation of tissue markers
Pre- or post Menopausal EGFR+ or Her2+ DCIS
RANDOMIZE
SURGERY
2-6 weeks
Lapatinib (1000mg) (N=30)
Tissue used for marker analysis (“Pre-treatment”)
Tissue used for marker analysis (“Post-treatment”)
LAPIS Trial (LAPatinib for In Situ Breast Cancer) PI: Powel Brown
Being conducted at BCM, DFCI, WRAMC, Georgetown University, M.D. Anderson, Mayo Clinic Supported by the SPORE Grant and a grant from the Breast Cancer Research Foundation
Placebo (N=30)
Rationale for using Trastuzumab in combination w/ RT in DCIS
• Trastuzumab is a radiosensitizer in HER2
overexpressing cancer cells
• Trastuzumab does not radiosensitize cells which do not overexpress HER2

04/04/2016
47
Summary & Conclusions
• Preoperative therapy paradigm has moved into DCIS
• May allow for more rapid identification of useful alternative pharmacologic interventions
• Sets stage for potential for observation in select patients without further local therapy
The Oncotype DX® Breast Cancer Assay for DCIS Report: A Tool for Shared
Treatment Decisions
PR Ki-67 STK15
Survivin Cyclin B1
MYBL2
GSTM1
Beta-actin GAPDH RPLPO
GUS TFRC
Hormone Receptor Group Proliferation Reference
The DCIS Score result: • Is a continuous variable • Is a quantitative risk assessment (number between 0 – 100) • Reflects each individual patient’s tumor biology
Solin et al. J Natl. Cancer Inst. 2013.
DCIS Score™ Result: Gene Selection

04/04/2016
48
Solin et al. J Natl Cancer Inst. 2013.
The ECOG 5194 study validated the DCIS Score result as a predictor of any LR or an invasive LR
• The DCIS Score result provides greater visibility into the risk of LR based on the underlying tumor biology and separates patients with a lower risk from patients with a higher risk of LR
DCIS Score™ Result: 10-Year Local Recurrence by Risk Group in E5194
Any Local Recurrence Invasive Local Recurrence
Solin et al. J Natl Cancer Inst. 2013.
The ECOG E5194 study validated the DCIS Score result as a predictor of LR (increasing DCIS Score corresponds to increasing risk) • Any DCIS or invasive LR • An invasive LR
DCIS Score™ Result: 10-Year Local Recurrence in E5194
Any Local Recurrence Invasive Local Recurrence
DCIS Score™ Result: 10-Year Invasive or DCIS Local Recurrence by Risk Group in the Ontario
Provincial DCIS Cohort
Rakovitch et al. SABCS 2014.
• As in the E5194 study, this study showed that the DCIS Score result stratifies patients for risk of an invasive LR
• Further, the DCIS Score result was able to stratify patients for risk of a DCIS LR
Invasive Local Recurrence DCIS Local Recurrence
04/04/2016
49
Summary: DCIS
• Novel clinical trial designs
– New emerging targets for DCIS
– Multigene RTPCR Biologic Assays
• DCIS may be ideal opportunity to study promising agents for prevention
• VISION:
– Selective approach for surgery and radiation









![World Journal of Surgical Oncology · 2017. 8. 29. · Lalak (1997) [13] F 68 No At surgery Follicular cell carcinoma JV Thrombectomy segmental resection JV Alive 9 months Patel (1997)](https://static.fdocuments.net/doc/165x107/6100cbc846ff9b68ec3e3045/world-journal-of-surgical-oncology-2017-8-29-lalak-1997-13-f-68-no-at-surgery.jpg)