Duality of Interest Declaration - KDIGO · 2019-02-13 · Spironolactone 25 mg added on top of...
27
1 Speaker: Peter Rossing I report the following potential duality/dualities of interest in the field covered by my lecture: Consultancy agreement Bayer AG Other consultancy and/or speaking fees to his institution from:Astra Zeneca, BMS, Boehringer Ingellheim, Eli Lilly, Novo Nordisk, Sanofi Aventis, Astellas, Abbvie Research grants from:Abbvie, Novo Nordisk, Novartis Personal shares in Novo Nordisk A/S All honorary payed to Steno Diabetes Center Duality of Interest Declaration KDIGO
Transcript of Duality of Interest Declaration - KDIGO · 2019-02-13 · Spironolactone 25 mg added on top of...

1
§ Speaker: Peter Rossing § I report the following potential duality/dualities of interest in the
field covered by my lecture: § Consultancy agreement Bayer AG
§ Other consultancy and/or speaking fees to his institution from:Astra Zeneca, BMS, Boehringer Ingellheim, Eli Lilly, Novo Nordisk, Sanofi Aventis, Astellas, Abbvie
§ Research grants from:Abbvie, Novo Nordisk, Novartis § Personal shares in Novo Nordisk A/S
§ All honorary payed to Steno Diabetes Center
Duality of Interest Declaration
KDIGO

J Ingelfinger NEJM 2008
KDIGO

The Renin-Angiotensin-Aldosterone System (RAAS)
Progression of renal- and cardiovascular disease
Angiotensinogen
Angiotensin I
Angiotensin II
Aldosterone
K+-↓ Na+ ↑
Cardiac Hypertrophy Endothelial dysfunction Inflammation
Glomerular sclerosis tubular damage
HR variability ↓ Baroreceptor sensitivity ↓
KDIGO

Incomplete Blockade of Aldosterone by ACE-I & ARB
Angiotensinogen
Ang I
Ang II
Renin
ACE ACE-I Chymase
ARB
Aldosterone Potassium
KDIGO

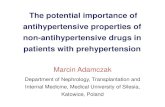
ΔGFR in 63 type 1 diabetic patients with DN
Aldosterone escape vs. non escape group (breakthrough vs non-breakthrough)
-4
0
4
8
12
16
20
Escape group
Non escape group
5.0
2.4
p < 0.05
Dec
line
in G
FR (m
l/min
/yea
r)
Schjoedt et al, Diabetologia 2004
KDIGO

Spironolactone in Chronic Renal Disease - Uncontrolled Studies
Author (year) Study Population Duration
(weeks) Background
therapy Reduction of Proteinuria
Reduction of BP (mm Hg)
Chrysostomou (2001)
DN and non-DN (n=8) 4 ACE 54% -
Sato A. et al (2003)
T2 DM with micro- or macro-albuminuria (n=15)
24 ACE 25% -
Nitta K. et al (2004)
Non-DN (n=22) 26 ARB 15% 9/7
Sato A. et al (2005)
DN and non-DN (n=32) 12 ACE 38% -
Bianci S. et al (2005)
DN and non-DN (n=42) 8 ACE-I or ARB 50% -
Spironolactone 25 mg added on top of previous antihypertensive treatment
DN=Diabetic Nephropathy, Non-DN=Non Diabetic Nephropathy
KDIGO

-10
-8
-6
-4
-2
0
-30
-20
-10
0
Response to spironolactone 25 mg 20 Type 1 Diabetic Patients with Diabetic Nephropathy
- 30 (-41 to -17) %
- 8 (-17 to 1) mm Hg
- 3 (-7 to 0) mm Hg
Rel
ativ
e ch
ange
(%)
Albuminuria 24-hrs Blood Pressure
Baseline: 831 (624, 1106) mg/d 144 (3) 72 (2) mm Hg
Cha
nge
(mm
Hg)
Schjoedt et al., Kid. Int. 2005
SBP DBP
KDIGO

-10
-8
-6
-4
-2
0
-30
-20
-10
0
Response to spironolactone 25 mg in 20 diabetic patients with nephrotic range albuminuria
- 32 (-21 to -42) %
- 6 - (-10 to-2)
mm Hg
- 4 - (-6 to -2) mm Hg
Rel
ativ
e ch
ange
(%)
Albuminuria
Baseline: 3718 (2910 - 4749) mg/d 144 (3) 72 (2) mm Hg
Cha
nge
(mm
Hg)
Schjoedt et al., Kid. Int. 2006
24-hrs Blood Pressure
nephrotic range albuminuria: albuminuria>2500mg/d = total proteinuria>3500 mg/d
SBP DBP
KDIGO

-10
-8
-6
-4
-2
0
-60
-40
-20
0
-60% (-21 to -80) %
-3 (-8 to 3) mm Hg
0 (-3 to 3) mm Hg
Rel
ativ
e ch
ange
(%)
Albuminuria 24hour Blood Pressure
Baseline: 90 (61-121)mg/d 135 (3) 65 (2) mm Hg
Cha
nge
(mm
Hg)
SBP DBP
S Nielsen Diabetic Medicine 2011
EARLY INTERVENTION Response to spironolactone 25 mg
21 type 1 diabetic patients with microalbuminuria
KDIGO

Spironolactone in diabetic nephropathy
van den Meiracker et al. Journal of Hypertension 2006;24:2285-2292
n=30
n=29
Months
KDIGO

Spironolactone in diabetic nephropathy
van den Meiracker et al. Journal of Hypertension 2006;24:2285-2292
KDIGO

Aldosterone Blockade with Eplerenone in pts with Type 2 DM and albuminuria
Epstein et al. Clin J Am Soc Nephrol 2006;1:940-951
KDIGO

-100
-80
-60
-40
-20
0
-62
-45
-74
Eplerenone Enalapril Epl./Enalapril 200 mg 40 mg 200/10 mg
(n=74) (n=74) (n=67)
UA
E c
hang
e (%
) Eplerenone Efficacy in Diabetic Hypertensive
Patients with Proteinuria
p=0.015
p=0.018
p<0.001
Epstein M et al. Am J Hypertens. 2002; 15(4) part 2:24A
KDIGO

-25
-20
-15
-10
-5
0
-19.5
Mea
n ch
ange
in
bloo
d pr
essu
re
(mm
Hg)
13.2* -15
-21.8
Eplerenone Enalapril Epl./Enal.
-16.2
Eplerenone Efficacy in Diabetic Hypertensive Patients with Proteinuria
Epstein M et al. Am J Hypertens. 2002; 15(4) part 2:24A
SBP DBP SBP DBP SBP DBP
-20.4
*p=0.015 vs Epl/Enal
KDIGO

KDIGO

§ Withdraw potassium supplements
§ Use low doses – spironolactone 25 mg /eplerenone 50 mg
§ Monitor potassium regularly
§ Pause RAAS blocking agents during dehydration
§ Particular caution when GFR is severely reduced
Reducing the Risk of Hyperkalemia During Aldosterone Blockade
KDIGO

17
Presentation title
Date
KDIGO

Type 2 DM resistant hypertension (3drugs BP>130/80) placebo (n=55) or 25 mg spironolactone(n=57)
C Oxlund et al, J Hyp 2013
KDIGO

Spironolactone for resistant hypertension in type 2 DM
C Oxlund et al, J Hyp 2013
KDIGO

§ Reduction of urine albumin/creatinine excretion on 50 mg Spironolactone by 56% (95% Cl 24-88%; p= 0.002)
§ Range of urine albumin response was though massive from 66 mg/g increase to 560 mg/g reduction.
§ Urinary peptide pattern (CKD273) at Baseline predict responders
Responder Prediction
Oxlund, J Hypertension 2013, Lindhardt, ASN 2014
KDIGO

n ~ 3280
Proteomic test
Randomised Double-blinded Placebo controlled
High-risk n ~ 656
Observational
Low-risk n ~ 2624
Three years follow-up
Placebo Spironolactone
Early prevention of DN in T2DM
KDIGO

22
Fine
reno
ne
Finerenone: Why a new Aldo blocker?
Based on preliminary experimental and clinicalearly studies, it is assumed that finerenone protects the heart, and perhaps the kidney, with less adverse effects In particular it is hoped that potassium problems are smaller compared to spironolactone/eplerenone
KDIGO

23
Fine
reno
ne
KDIGO

24
Fine
reno
ne
Baseline Data
KDIGO

25
Fine
reno
ne
Results
? To be presented at
WCN in March 2015 Phase 3 study in planning phase
KDIGO

Conclusions
§ Short-term clinical studies have shown renoprotective effects of aldosterone blockade in patients with chronic renal diseases
§ Aldosterone blockade is generally well tolerated but potassium should be monitored regularly
§ Long-term clinical studies are needed to confirm the beneficial effects on principal renal end-points
KDIGO

Thank you for listening !
KDIGO