Dry Eye Syndrome: An Ocular Surface Inflammatory Disease (OSID)
21
1 Ocular Surface Disease Ben Gaddie, O.D., F.A.A.O. Louisville, KY COPE #13171-AS Dry Eye Syndrome: An Ocular Surface Inflammatory Disease (OSID) • Dry Eye Syndrome is a common and under-recognized ocular surface inflammatory disease (OSID) • Inflammation is a hallmark of dry eye 1,2 • A group of disorders of the tear film due to reduced tear production or excessive tear evaporation 1,3 – Affects tear quantity and quality – Associated with symptoms of ocular discomfort – Associated with significant ocular morbidity Adapted with permission from Torkildsen G et al. Rev Ophthalmol. 2005;11:35-38. 1. McDonald MB. Refract Eyecare. 2005;9(suppl):3-6. 2. Stern ME et al. Exp Eye Res. 2004;78:409-416. 3. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003. Epidemiology of Dry Eye Syndrome • Approximately 25% of eye care visits are due to Dry Eye 1 • Up to 40 million Americans may either have symptoms of Dry Eye or are at risk for it 2 – Incidence of Dry Eye increases with age • Up to 51% of patients older than 65 years 3 • Up to 31% of women between 40 and 59 years of age 3 • Despite these numbers, Dry Eye remains remarkably under-diagnosed 4 1. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319. 2. Sheppard JD. Manag Care. 2003;12(suppl):6-8. 3. National Drug Treatment Information (NDTI) Sample Data. 2004-2005:701-702. 4. Perry HD, Donnenfeld ED. Curr Opin Ophthalmol. 2004;15:299-304. Dry Eye Syndrome: Under-recognition Due to Self-Treatment • Many patients use OTC artificial tears and lubricants, which are mostly palliative 1 – Estimated artificial tears USA sales >$145.4 million in 2005 2 • Self-treatment with OTC agents may delay diagnosis and effective therapy – Untreated inflammation associated with Dry Eye can lead to significant irreversible ocular damage 1. Calonge M. Surv Ophthalmol. 2001;45(suppl 2):S227-S239. 2. IMS Dataview 2005. OTC = over-the-counter. Dry Eye Syndrome: Predisposing Factors 1 • Age • Gender • Environment • Anterior segment disease • Medications • Contact lenses • Surgery • Systemic diseases 1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003. Systemic Diseases Associated With Dry Eye Syndrome 1-3 • Diabetes mellitus • Acne rosacea • Thyroid disease • Lymphoma • Inflammatory diseases – Allergy – Asthma – Vasculitis • Sjögren’s syndrome • Autoimmune diseases – Rheumatoid arthritis – Lupus • Neuromuscular disorders – Parkinson’s disease – Bell’s palsy 1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003. 2. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319. 3. Dalzell MD. Manag Care. 2003;12(suppl): 9-13.
Transcript of Dry Eye Syndrome: An Ocular Surface Inflammatory Disease (OSID)

1
Ocular Surface Disease
Ben Gaddie, O.D., F.A.A.O.Louisville, KY
COPE #13171-AS
Dry Eye Syndrome: An Ocular Surface Inflammatory Disease (OSID)
• Dry Eye Syndrome is a common and under-recognized ocular surface inflammatory disease (OSID)
• Inflammation is a hallmark ofdry eye1,2
• A group of disorders of the tear film due to reduced tear production or excessive tear evaporation1,3
– Affects tear quantity and quality– Associated with symptoms of ocular
discomfort– Associated with significant ocular
morbidityAdapted with permission from Torkildsen G et al. Rev Ophthalmol. 2005;11:35-38.
1. McDonald MB. Refract Eyecare. 2005;9(suppl):3-6.2. Stern ME et al. Exp Eye Res. 2004;78:409-416.
3. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.
Epidemiology of Dry Eye Syndrome
• Approximately 25% of eye care visits are due to Dry Eye1
• Up to 40 million Americans may either have symptoms of Dry Eye or are at risk for it2– Incidence of Dry Eye increases with age
• Up to 51% of patients older than 65 years3
• Up to 31% of women between 40 and 59 years of age3
• Despite these numbers, Dry Eye remains remarkablyunder-diagnosed4
1. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.2. Sheppard JD. Manag Care. 2003;12(suppl):6-8.
3. National Drug Treatment Information (NDTI) Sample Data. 2004-2005:701-702.4. Perry HD, Donnenfeld ED. Curr Opin Ophthalmol. 2004;15:299-304.
Dry Eye Syndrome:Under-recognition Due to Self-Treatment
• Many patients use OTC artificial tears and lubricants, which are mostly palliative1
– Estimated artificial tears USA sales >$145.4 million in 20052
• Self-treatment with OTC agents may delay diagnosis and effective therapy– Untreated inflammation associated with Dry Eye can lead to
significant irreversible ocular damage
1. Calonge M. Surv Ophthalmol. 2001;45(suppl 2):S227-S239.2. IMS Dataview 2005.OTC = over-the-counter.
Dry Eye Syndrome: Predisposing Factors1
• Age• Gender• Environment• Anterior segment disease
• Medications• Contact lenses• Surgery• Systemic diseases
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.
Systemic Diseases Associated WithDry Eye Syndrome1-3
• Diabetes mellitus• Acne rosacea• Thyroid disease• Lymphoma• Inflammatory diseases
– Allergy– Asthma– Vasculitis
• Sjögren’s syndrome• Autoimmune diseases
– Rheumatoid arthritis– Lupus
• Neuromuscular disorders– Parkinson’s disease– Bell’s palsy
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.
3. Dalzell MD. Manag Care. 2003;12(suppl): 9-13.

2
Ocular Diseases Associated WithDry Eye Syndrome
• Dry Eye can exist in association with several other ocular surface inflammatory diseases (OSIDs)– Seasonal allergic conjunctivitis (SAC)1
– Giant papillary conjunctivitis (GPC)1
– Blepharitis2,3
– Meibomitis2,3
1. Howes JF. Pharmazie. 2000;55:178-183. 2. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.
3. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.Adapted with permission from Lemp MA. CLAO J. 1995;21:221-231.
American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.
SjSjöögrengrenSyndromeSyndrome
NonNon--SjSjöögrengrenSyndromeSyndrome
BlepharitisBlepharitisMeibomian GlandMeibomian Gland
DysfunctionDysfunctionExposureExposure
Other FactorsOther Factors1. Contact Lenses1. Contact Lenses2. Blink Abnormality2. Blink Abnormality3. Environmental3. Environmental
Deficient AqueousDeficient AqueousTear ProductionTear Production
IncreasedIncreasedEvaporative LossEvaporative Loss
DRY EYEDRY EYESYNDROMESYNDROME
Dry Eye Syndrome: Classification
Pathophysiology of Dry Eye Syndrome: Ocular Surface Inflammation
• Numerous studies have recognized that inflammation plays a key role in the pathogenesis of Dry Eye1-5
• The role of T-cells along with several other inflammatory mediators have been clearly demonstrated in both humans and animal models3,5-7
• Several animal models are currently in use to better understand the pathophysiology of Dry Eye Syndrome5,8,9
1. Perry HD, Donnenfeld ED. Curr Opin Ophthalmol. 2004;15:299-304. 2. McDonald MB. Refract Eyecare. 2005;9(suppl):3-6.3. Pflugfelder SC et al. Cornea. 2000;19:644-649. 4. Wilson SE. Manag Care. 2003;12(suppl):14-19.
5. Stern ME et al. Exp Eye Res. 2004;78:409-416. 6. Gao J et al. Cornea. 1998;17:654-663.7. Stern ME et al. Invest Ophthalmol Vis Sci. 2002;43:2609-2614. 8. Hoffman RW et al. Arthritis Rheum. 1984;27:157-165.
9. Jabs DA, Prendergast RA. Invest Ophthalmol Vis Sci. 1988;29:1437-1443.
Inflammation Underlies Dry Eye Syndrome
• Inflammation affects the external ocular surface components1
– Eyelids– Bulbar and palpebral conjunctival epithelium– Lacrimal and meibomian glands– Corneal epithelium
• Inflammation affects tear production1,2
– Decreased quantity of “normal” tears– Excessive “dysfunctional” tears/mucus
1. Stern ME et al. Exp Eye Res. 2004;78:409-416.2. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.
Neural Regulation of NormalTear Production
LacrimalLacrimalGlandGland
CentralCentralNervousNervousSystemSystem
Secretomotor NerveSecretomotor NerveImpulsesImpulses
Sensory Sensory NerveNerve
ImpulsesImpulsesOcularOcularSurfaceSurface
InflammationInflammation
Adapted with permission from McDonald MB. Refract Eyecare. 2005;9(suppl):3-6.
Inflammation as an Underlying Factor in the Pathophysiology of Dry Eye Syndrome1-3
1. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.2. Pflugfelder SC et al. Cornea. 2000;19:644-649.
3. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.
Inflammatory Cellular InfiltrationInflammatory Cellular Infiltration
Tissue ScarringTissue Scarring
Meibomian Gland/Meibomian Gland/Goblet Cell DysfunctionGoblet Cell Dysfunction
Lacrimal Gland DysfunctionLacrimal Gland Dysfunction
Defective Tear Lipid Film/LayerDefective Tear Lipid Film/LayerDecreased AqueousDecreased AqueousTear ProductionTear Production
Increased Evaporative LossIncreased Evaporative Loss

3
Dry Eye Syndrome:Tear Film Inflammatory Response
• Tear film has a complex biochemical structure1
– External layer that covers and protects the ocular surface epithelium
• Abnormality in tear film composition leads to inflammation2
• Increased concentration of inflammatory cells and other mediators in tears—“hot” tears2
• Inflammation of the tear film can affect the tear-secreting glands
• Abnormal tear film composition, production, and clearance perpetuates the inflammatory cycle → chronic inflammation3
1. Pflugfelder SC et al. Cornea. 2000;19:644-649. 2. McDonald MB. Refract Eyecare. 2005;9(suppl):3-6.
3. Perry HD, Donnenfeld ED. Curr Opin Ophthalmol. 2004;15:299-304.
Inflammatory Mediators of the Tear Film1-4
• T-cells • Matrix-degrading enzymes
– ↑ MMP-9– ↑ Protease activity
• Inflammatory cytokines– ↑ IL-1β– ↑ TNF-α– ↑ TGF-β– ↓ IL-1RA
• Adhesion molecules– ICAM-1– VCAM-1
• Immunoglobulins– ↑ IgM– ↑ IgG– ↓ IgA
• Proinflammatory neural transmitters– Substance P– CGRP
1. McDonald MB. Refract Eyecare. 2005;9(suppl):3-6.2. Perry HD, Donnenfeld ED. Curr Opin Ophthalmol. 2004;15:299-304.
3. Wilson SE. Manag Care. 2003;12(suppl):14-19.4. Stern ME et al. Exp Eye Res. 2004;78:409-416.
Inflammatory Cycle of Dry Eye Syndrome
Adapted with permission from Wilson SE. Manag Care. 2003;12(suppl):14-19.
Chronic IrritationChronic Irritation
InflammationInflammation
Immune ActivationImmune ActivationDevelopment Development of Signs and of Signs and
SymptomsSymptoms
Signs and Symptoms of Dry Eye Syndrome1,2
Signs• Conjunctival
hyperemia/injection• Chemosis• Epiphora• Mucus discharge• Increased blinking frequency
Symptoms• Red eye• Irritation• Dryness, itching• Foreign body sensation• Burning/stinging• Poor/blurred vision• Contact lens intolerance• Photophobia, epiphora
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. McDonald MB. Refract Eyecare. 2005;9(suppl):3-6.
Misdiagnosis of Dry Eye Syndrome
• Diagnosis is primarily based on clinical signs and symptoms reported by patients1,2
• Poor correlation exists between clinical signs and reported symptoms1
• Several tests are available, but not one specific diagnostic test1-3
• Misdiagnosis leads to under-recognition and under-treatment• Long-standing, untreated inflammation → ocular complications
1. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004,4:314-319.2. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.
3.Perry HD, Donnenfeld ED. Curr Opin Ophthalmol. 2004;15:299-304.
Inflammation Associated with Dry Eye Syndrome Can Lead to Ocular Complications1,2
• Infection• Ocular surface keratinization• Corneal ulceration• Conjunctival squamous metaplasia
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. Sheppard JD. Manag Care. 2003;12(suppl):6-8.
These conditions can result in permanent structural These conditions can result in permanent structural damage with possible loss of visual functiondamage with possible loss of visual function11

4
Need for Early Diagnosis and Treatment
• Inflammation is often present long before clinical signs1
• Goal is to arrest inflammation before damage is irreversible2
– Institute immediate therapy that is safe and effective– Ensure adequate dose and duration of therapy
• Early diagnosis and proper treatment lead to better outcomes2
1. O’Brien TP. Refract Eyecare. 2005;9(suppl):7-11. 2. Sheppard JD. Manag Care. 2003;12(suppl):20-25.
Dry Eye International Task Force:Diagnostic Recommendations• A panel of experts achieved consensus on diagnostic parameters for Dry Eye• Dry Eye Syndrome severity classification, based on signs and symptoms
Mild to moderate symptoms No corneal signsMild to moderate conjunctival signsModerate to severe symptomsTear film signs, visual signsMild corneal punctate stainingConjunctival stainingSevere symptomsMarked corneal punctate stainingCentral corneal stainingFilamentary keratitisExtremely severe symptoms/altered lifestyleSevere corneal staining, erosionsConjunctival scarring
Level 1
Level 2
Level 3
Level 4
Adapted with permission from O’Brien TP. Refract Eyecare. 2005;9(suppl):7-11.
Dry Eye Syndrome:Optimal Diagnostic Approach
• Complete patient history and physical examination1
• One or more diagnostic tests2,3
– Completed over a period of time– Best approach to increase sensitivity and specificity in diagnosis
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. Perry HD, Donnenfeld ED. Curr Opin Ophthalmol. 2004;15:299-304.3. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.
Diagnostic Tests for Dry Eye Syndrome
• Standard in-office diagnostic tests1,2
– Schirmer test – Fluorescein tear breakup time– Ocular surface dye staining
• Rose bengal • Lissamine green • Fluorescein
• Other available (out-of-office) diagnostic tests– Tear film osmolarity– Tear lactoferrin– Impression/brush cytology
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.
Diagnostic Tests for Dry Eye Syndrome (cont)
• More sophisticated laboratory tests1,2
– Fluorescein tear clearance/tear function index– Lacrimal gland function test – Meibography– Tear film osmolarity– Tear fluid protein immunoassays– Tear lactoferrin– Impression/brush cytology
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.
Dry Eye International Task Force:Therapeutic Recommendations•A panel of experts achieved consensus on therapeutic parameters for Dry Eye
•Treatment options corresponding to the 4 severity levelsPatient educationEnvironmental modificationsControl systemic medicationsPreserved tearsAllergy control
If no improvement, add level 2 treatmentsUnpreserved tearsGels/nighttime ointmentsNutritional support Topical corticosteroidsCyclosporineSecretagogues
If no improvement, add level 3 treatmentsTetracyclinesPunctal plugs (once inflammation is controlled)
If no improvement, add level 4 treatmentsSystemic antiinflammatory therapyAcetylcysteineMoisture gogglesSurgery (punctal cautery)
Level 1
Level 2
Level 3
Level 4
Adapted with permission from O’Brien TP. Refract Eyecare. 2005;9(suppl):7-11.
5
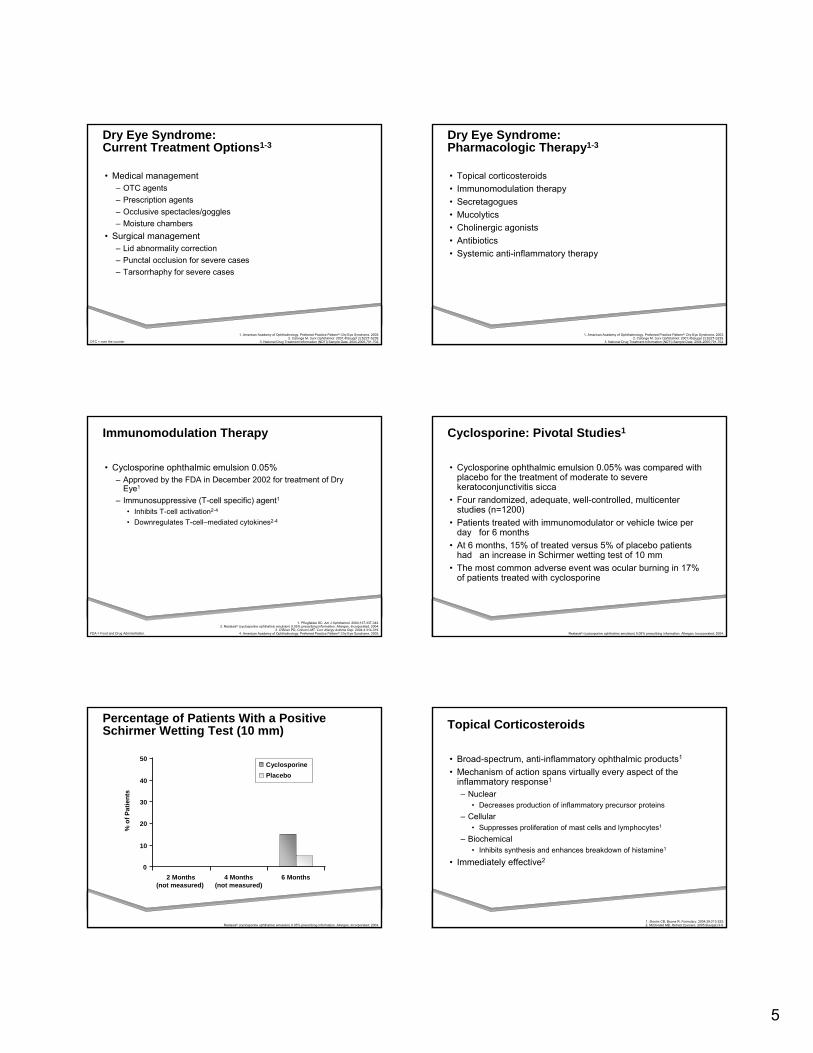
Dry Eye Syndrome: Current Treatment Options1-3
• Medical management– OTC agents– Prescription agents– Occlusive spectacles/goggles– Moisture chambers
• Surgical management– Lid abnormality correction– Punctal occlusion for severe cases– Tarsorrhaphy for severe cases
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. Calonge M. Surv Ophthalmol. 2001;45(suppl 2):S227-S239.
3. National Drug Treatment Information (NDTI) Sample Data. 2004-2005;701-702.OTC = over the counter.
Dry Eye Syndrome:Pharmacologic Therapy1-3
• Topical corticosteroids• Immunomodulation therapy• Secretagogues• Mucolytics• Cholinergic agonists• Antibiotics• Systemic anti-inflammatory therapy
1. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.2. Calonge M. Surv Ophthalmol. 2001;45(suppl 2):S227-S239.
3. National Drug Treatment Information (NDTI) Sample Data. 2004-2005;701-702.
Immunomodulation Therapy
• Cyclosporine ophthalmic emulsion 0.05% – Approved by the FDA in December 2002 for treatment of Dry
Eye1
– Immunosuppressive (T-cell specific) agent1• Inhibits T-cell activation2-4
• Downregulates T-cell–mediated cytokines2-4
1. Pflugfelder SC. Am J Ophthalmol. 2004;137:337-342.2. Restasis® (cyclosporine ophthalmic emulsion) 0.05% prescribing information. Allergan, Incorporated; 2004.
3. O’Brien PD, Collum LMT. Curr Allergy Asthma Rep. 2004;4:314-319.4. American Academy of Ophthalmology. Preferred Practice Pattern®: Dry Eye Syndrome. 2003.FDA = Food and Drug Administration.
Cyclosporine: Pivotal Studies1
• Cyclosporine ophthalmic emulsion 0.05% was compared with placebo for the treatment of moderate to severe keratoconjunctivitis sicca
• Four randomized, adequate, well-controlled, multicenter studies (n=1200)
• Patients treated with immunomodulator or vehicle twice per day for 6 months
• At 6 months, 15% of treated versus 5% of placebo patients had an increase in Schirmer wetting test of 10 mm
• The most common adverse event was ocular burning in 17% of patients treated with cyclosporine
Restasis® (cyclosporine ophthalmic emulsion) 0.05% prescribing information. Allergan, Incorporated; 2004.
Percentage of Patients With a PositiveSchirmer Wetting Test (10 mm)
0
10
20
30
40
50
2 Months(not measured)
4 Months(not measured)
6 Months
Cyclosporine Placebo
% o
f Pat
ient
s
Restasis® (cyclosporine ophthalmic emulsion) 0.05% prescribing information. Allergan, Incorporated; 2004.
Topical Corticosteroids
• Broad-spectrum, anti-inflammatory ophthalmic products1
• Mechanism of action spans virtually every aspect of the inflammatory response1
– Nuclear• Decreases production of inflammatory precursor proteins
– Cellular• Suppresses proliferation of mast cells and lymphocytes1
– Biochemical• Inhibits synthesis and enhances breakdown of histamine1
• Immediately effective2
1. Slonim CB, Boone R. Formulary. 2004;39:213-222.2. McDonald MB. Refract Eyecare. 2005;9(suppl):3-6.

6
Topical SteroidsTopical SteroidsWork HereWork Here
Topical Corticosteroids Work Early to Block Multiple Pathways of Inflammatory Cascade
Membrane PhospholipidsMembrane Phospholipids
Phospholipase APhospholipase A22
Arachidonic AcidArachidonic Acid
LipoxygenaseLipoxygenase
HydroperoxidesHydroperoxides
LeukotrienesLeukotrienes(LTC(LTC44, LTD, LTD44, LTE, LTE44, LTB, LTB44))
ProstaglandinsProstaglandins(PGF(PGF22, PGD, PGD22, PGE, PGE22))
CycloCyclo--OxygenaseOxygenase
Cyclic EndoperoxidesCyclic Endoperoxides
ProstacyclinProstacyclin(PCI(PCI22))
Thromboxane AThromboxane A22(TXA(TXA22))
HeparinHeparin HistamineHistamine
TT--CellsCellsMembraneMembrane
StabilizationStabilization
Mast CellMast Cell
PAFPAFTryptaseTryptaseChymaseChymase
Adapted with permission from Donnenfeld ED. Refract Eyecare. 2005;9(suppl):12-16.
Progenitor Cell ProliferationProgenitor Cell Proliferation
Cyclosporine Cyclosporine Works HereWorks Here
Topical SteroidsTopical SteroidsWork HereWork Here
PAF = platelet-activating factor.
Topical Corticosteroids: Limitations
• With most topical corticosteroids, complications are a concern with long-term use1
– Increased IOP– Cataract formation– Exacerbation of viral and/or fungal infections
1. Donnenfeld ED. Refract Eyecare. 2005;9(suppl):12-16.
Need for an optimal corticosteroidNeed for an optimal corticosteroidthat allows for that allows for safesafe longlong--term useterm use
IOP = intraocular pressure.
The Ideal Ophthalmic Corticosteroid Therapy for Dry Eye Syndrome• Broad-spectrum anti-inflammatory properties• Rapid onset of action • Targeted, site-specific activity• Complete symptom control
– eg, burning, stinging• Potent, but safe for prolonged use• Minimal adverse events• Works synergistically with immunomodulators
The Role of LOTEMAX®
in Dry Eye Inflammation
Loteprednol Etabonate:The Only Ester Corticosteroid• Unique topical steroid
– Retrometabolic drug design1-4
• Modification of an existing molecule to reduce or eliminate unwanted adverse events• Prednisolone derivative• Position 20 ester group replaces the ketone group
1. Bodor N. Pharmazie. 2001;56(suppl 1):S67-S74.2. Novack GD et al. J Glaucoma. 1998;7:266-269.
3. Howes J, Novack GD. J Ocul Pharmacol Ther. 1998;14:153-158.4. Holland EJ. Refract Eyecare. 2005;9(suppl):17-19.
HOHO
CHCH33
OO
OHOHCHCH33
CHCH33
CHCH33
HOHO
OO
OCHOCH22CICI
OCOOCO22CC22HH55
C = OC = O
Position 20 EsterPosition 20 Ester
Position 20 Position 20 KetoneKetone
C = OC = O
CHCH22OHOH
LoteprednolEtabonate
Prednisolone
Loteprednol Etabonate: Clinical Benefits of the Only Ester Corticosteroid
• Benefits of the ester group– Efficacy
• High lipophilicity leads to better penetration1,2
• Lipophilic index 10 times higher than dexamethasone1,2
• Rapid/targeted receptor binding leads to enhanced therapeutic effect3,4
• 4.3 times greater binding affinity to steroid receptors than dexamethasone5
– Safety• Unlike any other corticosteroid, loteprednol etabonate only becomes
activated when bound to receptor5
• Rapid inactivation of unbound drug by circulating esterases leads to an inactive metabolite and minimal adverse events3,4
– Significantly reduced incidence of IOP increase5
– Decreased risk of cataract61. Alberth M et al. J Biopharm Sci. 1991;2:115-125.
2. Howes JF. Pharmazie. 2000;55:178-183. 3. Novack GD et al. J Glaucoma. 1998;7:266-269.
4. Howes J, Novack GD. J Ocul Pharmacol Ther. 1998;14:153-158.5. Holland EJ. Refract Eyecare. 2005;9(suppl):17-19.6. Manabe S et al. J Clin Invest. 1984;74:1803-1810.

7
Lotemax® for the Treatment of Dry Eye Inflammation• Lotemax was compared with placebo for the treatment of the
inflammatory component of Dry Eye in patients with delayed tear clearance
• Randomized, double-masked, placebo-controlled, multicenter comparison
• Patients with Dry Eye (n=66)– 32 patients treated with Lotemax– 34 patients treated with placebo
• Subjects received either Lotemax or placebo QID in both eyes for 4 weeks
1. Pflugfelder SC et al. Am J Ophthalmol. 2004;138:444-457.QID = 4 times per day.
Efficacy of Lotemax® in Patients With Moderate Symptoms of Dry Eye Inflammation*
Subjects With Corneal Staining Score ≥10 andConjunctival Hyperemia Score ≥2 at Baseline
4040
2020
00
--2020
--4040
--6060
PrimaryPrimarySubjectiveSubjectiveOutcomeOutcome††
PrimaryPrimaryObjectiveObjectiveOutcomeOutcome‡‡
CentralCentralCornealCornealStainingStaining
InferiorInferiorTarsalTarsal
InferiorInferiorBulbarBulbar
NasalNasalBulbarBulbar
RednessRedness
--50.150.1
--22.222.2--10.110.1
3.83.8 0.00.0
--11.111.1
--35.735.7--21.121.1 --25.025.0 --28.628.6
--47.147.1
4.44.412.512.5
33.333.3LotemaxLotemax PlaceboPlacebo
Impr
ovem
ent
Perc
enta
ge C
hang
eFr
om B
aseli
ne
HyperemiaHyperemia
Adapted with permission from Pflugfelder SC et al. Am J Opthalmol. 2004;138:444-457.
*Seen at 2 weeks and maintained after 4 weeks.†Worst symptom.‡Composite corneal staining score for worst eye.
Efficacy of Lotemax® in Patients With Moderate Symptoms of Dry Eye Inflammation (cont)
• The Lotemax-treated group showed greater improvement than the vehicle group in both primary subjective and primary objective outcomes
• Lotemax resulted in greater improvement than the vehicle group in multiple indices of conjunctival hyperemia
• Lotemax showed much greater improvement than the vehicle group in central corneal staining score
• Improvements achieved in the Lotemax-treated group at 2 weeks were maintained after 4 weeks of treatment when compared with the vehicle group
1. Pflugfelder SC et al. Am J Opthalmol. 2004;138:444-457.
• Improvement in central corneal staining was associated with a significant improvement in the surface regularity index at2 weeks (P=.05)1
– Videokeratoscopy performed in a subset of patients• Clinically relevant improvement: central corneal staining is
positively correlated with a potential improvement in visual acuity1,2
1. Pflugfelder SC et al. Am J Ophthalmol. 2004;138:444-457.2. de Paiva CS, Pflugfelder SC. Ophthalmology. 2003;110:1102-1109.
Efficacy of Lotemax® in Patients With Moderate Symptoms of Dry Eye Inflammation (cont)
Safety of Lotemax® in Patients With Moderate Symptoms of Dry Eye Inflammation
• Reported adverse events were similar for both the Lotemax and the placebo groups1
• There were no clinically significant IOP changes in either group1
• There were no signs of cataract formation1
• Safety of loteprednol etabonate has been further supported by several long-term follow-up studies1,2
1. Pflugfelder SC et al. Am J Ophthalmol. 2004;138:444-457. 2. Novack GD et al. J Glaucoma. 1998;7:266-269.IOP = intraocular pressure.
Efficacy and Safety of Lotemax® in Patients With Moderate Symptoms of Dry Eye Inflammation1
• When used as monotherapy, Lotemax resulted in greater improvement in objective signs and symptoms of Dry Eye than placebo at both 2 and 4 weeks
• Lotemax also improved the surface regularity index and corneal staining, which are correlated with visual acuity
• Lotemax demonstrated no clinically significant IOP elevation following 1 month of therapy for Dry Eye
• Treatment of Dry Eye patients with Lotemax beyond 2 weeks carries an excellent benefit-to-risk ratio
1. Pflugfelder SC et al. Am J Ophthalmol. 2004;138:444-457.IOP = intraocular pressure.

8
Lotemax®: Potential Use of Concomitant Therapy in Dry Eye Inflammation• Topical corticosteroids have a rapid onset of action for faster relief and
can be used concomitantly with cyclosporine1
– Cyclosporine may require up to 6 months to produce a clinicallytherapeutic effect
• In clinical practice, concomitant therapy of Lotemax and cyclosporine for Dry Eye has been reported to be far more effective than either therapy used alone2,3
– Clinical trials have yet to be completed• Lotemax may help minimize adverse events such as burning and
stinging associated with cyclosporine2,3
• Lotemax may help improve patient compliance and satisfaction with topical cyclosporine therapy2,3
• Lotemax is the #1 corticosteroid used in combination with cyclosporine for the treatment of Dry Eye Inflammation4
1. Pflugfelder SC. Am J Ophthalmol. 2004;137:337-342. 2. O’Brien TP. Refract Eyecare. 2005;9(suppl):7-11.
3. Donnenfeld ED. Refract Eyecare. 2005;9(suppl):12-16. 4. National Drug Treatment Information (NDTI) Sample Data. 2004-2005:701-702.
Zylet®: Site-Active Corticosteroid Plus Broad-Spectrum Aminoglycoside
Loteprednol Etabonate 0.5%1
• Site-active corticosteroid• Inhibits inflammatory response
to a variety of inciting agents– May act by inducing
phospholipase A2 inhibitory proteins, collectively known as lipocortins
Tobramycin 0.3%1
• Broad-spectrum aminoglycoside
• Inhibits bacterial protein synthesis– Binds to bacterial ribosomes
1. Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension) [package insert]. Tampa, Fla: Bausch & Lomb Incorporated; 2005.
Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
Loteprednol Etabonate 0.5%:First and Only Ester Corticosteroid
Ester1-3
• LoteprednolKetone1-3
• Prednisolone• Fluorometholone• Dexamethasone• Medrysone• Rimexolone
1. Lotemax [package insert]. Tampa, Fla: Bausch & Lomb Incorporated; 2002.2. Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension) [package insert].
Tampa, Fla: Bausch & Lomb Incorporated; 2005.3. Howes J et al. J Ocul Pharmacol Ther. 1998;14:153-158.
Ester vs. Ketone Corticosteroids
Loteprednol Etabonate 0.5%:Single-Step Metabolism1
1. Druzgala P et al. Curr Eye Res. 1991;10:933-937.
Common TobramycinSusceptible Bacterial Pathogens1,2
• Staphylococci• Streptococci• Pseudomonas aeruginosa• Escherichia coli• Klebsiella pneumoniae• Enterobacter aerogenes• Proteus mirabilis
• Morganella morganii• Proteus vulgaris (most strains)• Haemophilus influenzae• Haemophilus aegyptius• Moraxella lacunata• Acinetobacter calcoaceticus• Neisseria (some species)
1. Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension) [package insert]. Tampa, Fla: Bausch & Lomb Incorporated; 2005. 2. Tobrex [package insert]. Forth Worth, Tex: Alcon Laboratories, Inc; 1980.
Key Zylet® Clinical Studies: Efficacy and SafetyTobramycin: No impact on Loteprednol Etabonate0.5% Bioavailability Analysis of intent-to-treat population1
1. Data on file, Bausch & Lomb Incorporated, 2004...
Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
9
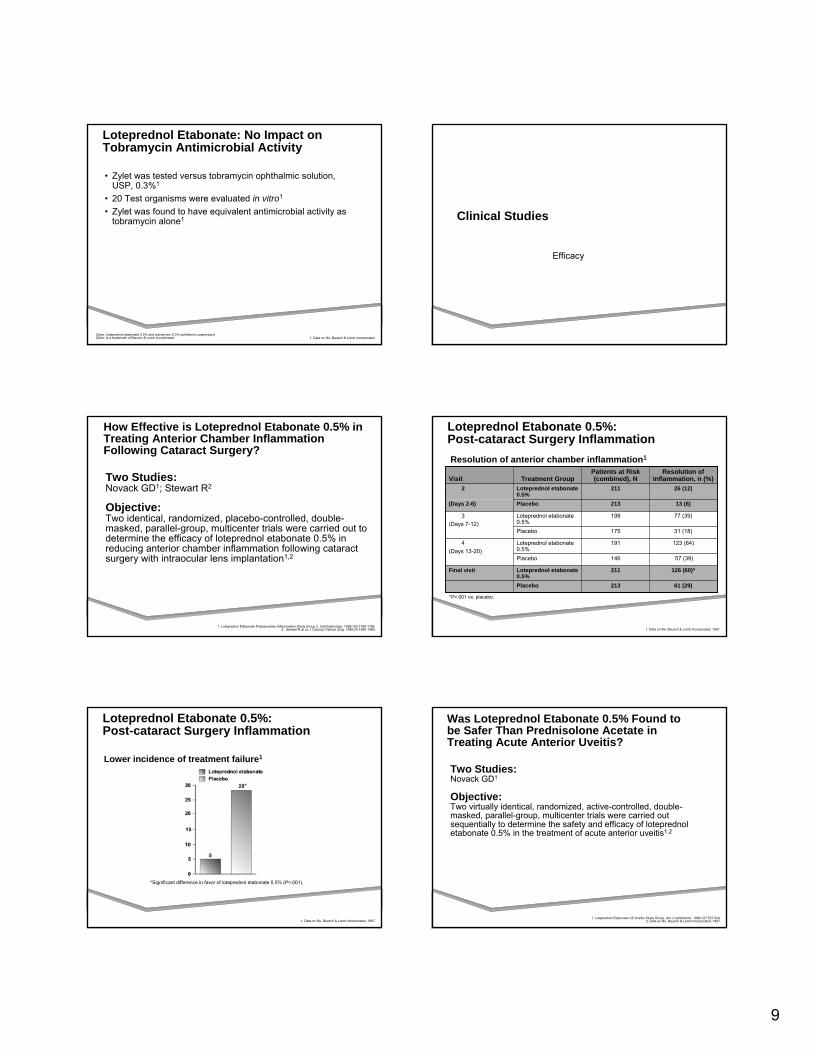
Loteprednol Etabonate: No Impact on Tobramycin Antimicrobial Activity
• Zylet was tested versus tobramycin ophthalmic solution, USP, 0.3%1
• 20 Test organisms were evaluated in vitro1
• Zylet was found to have equivalent antimicrobial activity as tobramycin alone1
1. Data on file, Bausch & Lomb Incorporated.Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
Clinical Studies
Efficacy
Two Studies:Novack GD1; Stewart R2
Objective:Two identical, randomized, placebo-controlled, double-masked, parallel-group, multicenter trials were carried out to determine the efficacy of loteprednol etabonate 0.5% in reducing anterior chamber inflammation following cataract surgery with intraocular lens implantation1,2
1. Loteprednol Etabonate Postoperative Inflammation Study Group 2. Ophthalmology. 1998;105:1780-1786.2. Stewart R et al. J Cataract Refract Surg. 1998;24:1480-1489.
How Effective is Loteprednol Etabonate 0.5% in Treating Anterior Chamber Inflammation Following Cataract Surgery?
Loteprednol Etabonate 0.5%: Post-cataract Surgery InflammationResolution of anterior chamber inflammation1
1. Data on file, Bausch & Lomb Incorporated, 1997.
13 (6)213Placebo(Days 2-6)
26 (12)211Loteprednol etabonate 0.5%
2
126 (60)*211Loteprednol etabonate 0.5%
Final visit
61 (29)213Placebo
123 (64)191Loteprednol etabonate 0.5%
4(Days 13-20)
57 (39)146Placebo
77 (39)198Loteprednol etabonate 0.5%
3(Days 7-12)
31 (18)175Placebo
Resolution of Inflammation, n (%)
Patients at Risk (combined), NTreatment GroupVisit
*P<.001 vs. placebo.
Loteprednol Etabonate 0.5%: Post-cataract Surgery Inflammation
Lower incidence of treatment failure1
*Significant difference in favor of loteprednol etabonate 0.5% (P<.001).
1. Data on file, Bausch & Lomb Incorporated, 1997.
Two Studies: Novack GD1
Objective:Two virtually identical, randomized, active-controlled, double-masked, parallel-group, multicenter trials were carried out sequentially to determine the safety and efficacy of loteprednoletabonate 0.5% in the treatment of acute anterior uveitis1,2
Was Loteprednol Etabonate 0.5% Found to be Safer Than Prednisolone Acetate in Treating Acute Anterior Uveitis?
1. Loteprednol Etabonate US Uveitis Study Group. Am J Ophthalmol. 1999;127:537-544.2. Data on file, Bausch & Lomb Incorporated, 1997.

10
ParameterLoteprednol Etabonate
0.5%Prednisolone Acetate
1.0%
Cell 72% (58/81) 87%* (77/89)
Flare 66% (52/79) 82%* (72/88)
Pain 90% (69/77) 85% (75/88)
Photophobia 79% (58/73) 78% (64/82)
1. Data on file, Bausch & Lomb Incorporated, 1997.2. Loteprednol Etabonate US Uveitis Study Group. Am J Ophthalmol. 1999;127:537-544.
Loteprednol Etabonate 0.5%: Acute Anterior Uveitis
Anti-inflammatory efficacy1,2
*P=.015
Loteprednol Etabonate 0.5%: Acute Anterior Uveitis
Resolution of anterior chamber cell reaction1
Intent-to-treat N=170*P=.015†36 to 72 hours after end of treatment
1. Data on file, Bausch & Lomb Incorporated, 1997.
Loteprednol Etabonate 0.5%: Acute Anterior Uveitis
Resolution of anterior chamber flare reaction1
Intent-to-treat N=170*P=0.017†36 to 72 hours after end of treatment
1. Data on file, Bausch & Lomb Incorporated, 1997.
Two Studies: Asbell P1; Friedlaender MH2
Objective:Two randomized, double-masked, placebo-controlled, parallel-group, prospective, multicenter trials with identical designs were carried out to determine the efficacy of loteprednol etabonate 0.5% in the treatment of contact lens-associated giant papillary conjunctivitis1,2
How Effective is Loteprednol Etabonate 0.5%in the Treatment of Contact Lens-associated Giant Papillary Conjunctivitis?
1. Asbell P et al. CLAO J. 1997;23:31-36.2. Friedlaender MH et al. Am J Ophthalmol. 1997;123:455-464.
Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
1. Asbell P et al. CLAO J. 1997:23:31-36.2. Friedlaender MH et al. Am J Ophthalmol. 1997;123:455-464.
3. Data on file, Bausch & Lomb Incorporated, 1994.
Loteprednol Etabonate 0.5%: Giant Papillary Conjunctivitis
Significant improvement in primary efficacy parameters1-3
Response
<.001<.001<.001P value
78%79%51%222Placebo
91%94%76%221Loteprednol etabonate 0.5%
Lens IntoleranceItchingPapillae
Number of Patients
Loteprednol Etabonate 0.5%: Giant Papillary Conjunctivitis
Significant improvement in secondary efficacy parameters1-3
Response
<.001<.001<.001P value
43%48%58%222Placebo
79%68%85%221Loteprednol etabonate 0.5%
Bulbar Injection
Palpebral Injection
Investigator Global
AssessmentNumber of Patients
1. Asbell P et al. CLAO J. 1997:23:31-36.2. Friedlaender MH et al. Am J Ophthalmol. 1997;123:455-464.
3. Data on file, Bausch & Lomb Incorporated, 1994.

11
1. Asbell P et al. CLAO J. 1997:23:31-36. 2. Friedlander MH, et al. Am J Ophthalmol. 1997;123:455-464.
3. Data on file, Bausch & Lomb Incorporated; 1994. 4. Laibovitz RA et al. Invest Ophthal Vis Sci, 1991;32:734. Abstract 344–50.
5. Bartlett JD et al. Curr Eye Res. 1993;12:313-321.Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
How Effective is Loteprednol Etabonate 0.5%in the Treatment of Contact Lens-Associated Giant Papillary Conjunctivitis?
Key results:• Patients on loteprednol etabonate 0.5% experienced significantly
greater improvement in all 3 primary efficacy variables (papillae, itching, lens intolerance) compared with those on placebo– Intergroup differences favored loteprednol etabonate 0.5% by
25% for reduction in size and severity of papillae, 15% for reduction in itching, and 13% for improved contact lens tolerance (P<.001 for each)1-3
– Two additional studies found that loteprednol etabonate 0.5% was both well tolerated and clinically effective in the treatment of giant papillary conjunctivitis4,5
One Study:Dell SJ1
Objective:A randomized, double-masked, placebo-controlled, parallel-group, multicenter trial was carried out to determine the efficacy of loteprednol etabonate 0.5% as prophylaxis against seasonal allergic conjunctivitis1
1. Dell SJ et al. Am J Ophthalmol. 1997;123:791-797.
How Effective is Loteprednol Etabonate 0.5%—the Anti-inflammatory Component of Zylet®—in Preventing Seasonal Allergic Conjunctivitis?
Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
1. Data on file, Bausch & Lomb Incorporated, 1994.
Loteprednol Etabonate 0.5%: Seasonal Allergic Conjunctivitis
Significant improvement in primary efficacy variables1
*P<.001†P<.001Primary composite end point = itching + bulbar injectionItching was evaluated on a scale of 0 to 4Bulbar injection was evaluated on a scale of 0 to 3
1. Dell SJ et al. Am J Ophthalmol. 1997;123:791-797.Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
How Effective is Loteprednol Etabonate 0.5%in Preventing Seasonal Allergic Conjunctivitis?
Key result:• Patients in the loteprednol etabonate 0.5% group never
developed moderate or severe ocular signs and symptoms of allergy during the peak pollen season vs. patients in the placebo group– Loteprednol etabonate 0.5% was effective in the prophylaxis of
seasonal allergic conjunctivitis1
Clinical Studies
Adverse Events
Loteprednol Etabonate 0.5%: Low Incidence of Adverse Events
• Adverse events occurring in 5% to 15% of patients1,2:
• Only 0.2% of patients exhibited a serious adverse event considered possibly or probably related to study medication²
• All of these patients experienced complete resolution upon discontinuation of treatment2
1. Lotemax[package insert]. Tampa, Fla: Bausch & Lomb Incorporated; 2002.2. Data on file, Bausch & Lomb Incorporated; 1997.
3. Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension) [package insert]. Tampa, Fla: Bausch & Lomb Incorporated; 2005.
– Photophobia– Dry eyes– Injection– Discharge– Itching– Chemosis– Foreign body sensation– Burning on instillation– Epiphora– Abnormal vision/blurring

12
Two Studies:Bartlett JD1; Novack GD2
Objective:Both were randomized, double-masked, crossover studies of populations of known steroid responders and an analysis of controlled, randomized trials in subjects treated for ≥28 days were carried out to determine the safety of loteprednol etabonate 0.5% vs. prednisolone acetate 1.0% with regard to elevation in intraocular pressure1,2
1. Bartlett JD et al. J Ocul Pharmacol. 1993;9:157-165.2. Novack GD et al. J Glaucoma. 1998;7:266-269.
What Impact Does Loteprednol Etabonate 0.5% Have on Intraocular Pressure?
Loteprednol Etabonate 0.5%: Intraocular Pressure
No significant elevation in known steroid responders1
1. Adapted from Bartlett JD et al. J Ocul Pharmacol. 1993;9:157-165.
Loteprednol Etabonate 0.5%: Intraocular Pressure
Low incidence of elevation with long-term treatment1
1. Adapted from Novack GD et al. J Glaucoma. 1998;7:266-269.1. Bartlett JD et al. J Ocul Pharmacol. 1993;9:157-165.
2. Novack GD et al. J Glaucoma. 1998;7:266-269.
What Impact Does Loteprednol Etabonate 0.5% Have on Intraocular Pressure?
Key results:• The mean intraocular pressure elevations induced in known steroid responders
were neither statistically nor clinically significant after 6 weeks with loteprednol etabonate 0.5%
• Significant elevations in prednisolone acetate group [18.1 mm Hg at baseline vs. 27.1 mm Hg on day 42 (P<.05)]1
• An analysis of controlled, randomized trials demonstrated a significant elevation in intraocular pressure in only 1.7% of patients on loteprednol etabonate 0.5% compared with 6.7% of patients on prednisolone acetate 1.0%2
Loteprednol Etabonate 0.5%: Clinical Safety
• Studied in >2000 patients in 20 clinical studies1-3
• Ocular Adverse Events:– Very low incidence of IOP rise that was generally transient
in nature1-3
– Only 15 (1.7%) of 901 patients treated 28 days or longer had an IOP rise >10 mm Hg1
– 11 of 15 patients with a clinically significant (>10 mm Hg) IOP response were in GPC studies1
• Patients were allowed to wear lenses indicating possible reservoir effect of lenses
1. Novack GD et al. J Glaucoma. 1998;7:266-269.2. Bartlett JD et al. J Ocul Pharmacol. 1993;9:157-165.
3. Friedlaender MH et al. Am J Ophthalmol. 1997;123:455-464.
Tobramycin 0.3%: Low Incidence of Adverse Events
• Adverse events occurring in <3% of patients1,2:– Hypersensitivity reactions– Local ocular toxicity– Swelling and/or itching of eyelids– Conjunctival erythema
1. Tobrex [package insert]. Forth Worth, Tex: Alcon Laboratories, Inc; 1980.2. Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension) [package insert]. Tampa, Fla: Bausch & Lomb Incorporated; 2005.

13
Zylet®: Adverse Reactions
42-Day Safety Study1
—<4%All Other
4%9%Sting/Burn
18%13%SPK
(1.1 mm Hg)(1.6 mm Hg)Average IOP Increase
4%10%IOP
29%21%Injection
Placebon=56
Zyletn=112
Ocular Events
1. Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)[package insert]. Tampa, Fla: Bausch & Lomb Incorporated; 2005.
Zylet® (loteprednol etabonate 0.5% and tobramycin 0.3% ophthalmic suspension)Zylet® is a trademark of Bausch & Lomb Incorporated.
Patients at Risk for Elevated IOP Associated with Steroid Use
• 14 to 22 million people who are steroid responders1,2
• 3 to 6 million people with ocular hypertension3
• 3 million people with glaucoma3,4
1. EyeMDLink.com. Steroid induced glaucoma. Available at: http://www.eyemedlink.com/Condition.asp?ConditionID=419. Accessed November 16, 2004.2. U.S. Census Bureau. U.S. POPClock projection. Available at: http://www.census.gov/cgi-bin/ popclock. Accessed November 16, 2004.
3. E-medicine Consumer Health. Ocular Hypertension. Available at:www.emdicinehealth.com/articles/37513-1.asp. Accessed November 16, 2004.4. Lee J, Bailey G. Glaucoma: The second-leading cause of blindness in the US. Available at: http://www.allaboutvision.com/conditions/glaucoma.htm. Accessed November 16, 2004.
Proven Clinical Experience with Tobramycin
• Broad-spectrum aminoglycoside antibiotic with over 20 years of real world experience1,2
• Active against both Gram-positive and Gram-negative ocular pathogens1,2
• Binds to bacterial ribosomes, inhibiting protein synthesis1,2
• Generally bacteriostatic, but may be bactericidal in high doses1,2
• Corneal penetration enhanced by lipid solubility1
• Low serum concentrations with ocular administration2
1. de Aguiar Moeller CT et al. Arq Bras Oftalmol. 1999;62. Available at: http://www.abonet.com.br/abo/abo62611.htm. Accessed September 13, 2004. 2. Robert P-Y et al. Drugs. 2001;61:175-185.
Case Study #1
• 49 y/o myopic female seen in refractive consultation. History of contact lens intolerance over past 5 years with giant papillary conjunctivitis (GPC)
• Medical history: Asthma; recent onset of menopause
• Mild GPC• Normal tear meniscus• BCVA 20/25 OU• 3+ lissamine green conjunctival staining • 1+ fluorescein corneal staining• Schirmer with anesthesia 5 OD/4 OS• Ocular Surface Disease Index (OSDI) = 0.39
– Corresponds to severe dry eye• Scale 0-1; normal subjects score 0.05-0.10
3+ Conjunctival Staining3+ Conjunctival Staining

14
• Started on Systane qid• One month later:
– 2+ lissamine green conjunctival staining – 1+ fluorescein corneal staining– Schirmer 5 OD/5 OS
• Patient started on topical lotenpredenol (Lotemax) BID and cyclosporine BID
• Two months later:– BCVA 20/20 OU– 1+ lissamine green conjunctival staining – No fluorescein corneal staining– Schirmer 11 OD/10 OS– GPC resolves
• Patient undergoes uneventful LASIK– Lotemax/cyclosporine treatment made this patient into
a LASIK candidate

15
Case Study #2
• 42 y.o. Caucasian Male• CC: FB Sensation, Dry burning eyes• Eyes constantly red• Can’t go outside - eyes hurt!
Predisposing factors
• Age• Gender• Environment• Anterior Segment
Disease
• Medications• CL Wear• Refractive surgery• Systemic Disease
Systemic Disease
• Diabetes• Arthritis
–Sjogren’s• Thyroid Eye Disease
• Most missed systemic caused?• Rosacea
Rosacea
• Erythema• Telangiectasia• Pustules• Prominent sebaceous glands• Rhinophyma

16
Rosacea
• Presentation• Women: cheeks• Men: nose
Rosacea
• Meibomian gland dysfunction• Dry eye• Blepharitis

17
Ocular Rosacea
• 58% of all rosacea patients• Presenting sign in :• 20%!

18
Rosacea: Treatments
• Tetracyclines: Doxycycline 50mg bid x 1-2 months then qd
• Metrocream• Education• Periostat long term (20mg doxycycline)
Tetracycline MOA
• Accumulation in Oil Glands• Anti-inflammatory component• Regulate enzymatic activity of staph
Cautions
• Photosensitivity• Chelates with dairy products, antacids
etc.• Minocycline may cause vestibular toxicity• Number one drop-out reason? - 25%
Which of the following patients could be given Doxycycline
A. Pregnant woman
C. 8 y.o. child
B. 23 y.o. female with Chlamydia
D. 52 y.o. male with acne rosacea
Tetracycline
• Pregnancy ratings:• A, B, C, D, X
• Rating on tetracycline: D
Which of the following medications should someone on doxycycline avoid
A. Antidepressants
C. Tagamet
B. Antacids
D. Birth control pills

19
Which of the following complications may be related to doxycycline?
A. Dry eye
C. Pseudotumor Cerebri
B. Blepharitis
D. Iritis
Nutritional Supplements: Essential fatty acids
• Flaxseed oil (1000 mg bid if tablet form)• Castor oil• Fish oils • Omega-3 fatty acids - linoleic acid
• Recommendation: Combination flax/fish oil (500mg) begin qd then move to bid/tid
Case 3
• So why does her left eye hurt more than OD even though OD looks worse• How do you counsel this patient?• What is your topical course of therapy?
– NPAT– Restasis/Steroids– BSCL/Moisture goggle
• Do you use for systemic therapy?– Hormone work-up– Nutritional Support– DCN
• What do you do about the filaments• Do you plug immediately?
Case #
• 56 YOWF presents with red eye and moderate pain• VA 20/25 bcc• History of “burned-out” arthritis• Slex as shown

20
Case #
• Differential diagnosis– Allergic conjunctivitis– Viral conjunctivitis– Episcleritis– Scleretis
• Phenylephrine testing– Treatment and diagnostic managment
Lab Workup
• ACE• ANA• CBC w diff• Serum Lysozyme• RF• HLA-B27• ESR• VDRL/FTA-ABS
Case #
• 36 yowf 30-day extended wear FND 8.4 -6.50 OU normal VA• Patient reports increased ocular comfort with contact lenses
on.• Microcystic formation anterior cornea• Stain with nafl• Differential Dx
– SiHi immune reaction or other unknown mechanism– Thygesson’s corneal dystrophy

21
Case #
• 38yowm• FND -5.00 OU• 30 day EW x 2 years• Presents with red, light sensitive eye• 2 days duration• No lens x 24 hours• Photos, management
Case #
• Infectious or inflammatory?• SiHi modulus• Treatment-
– 3d vs 4th generation FQ– Steroids and when?
Case Study #?
• 42 y.o. male 1 month post LASIK• Transient Blur – worse in the evening• Throughout the day• No burning, stinging, dryness etc.



![OSID Diagnostic tool for V4 -(3) [tryb zgodności]...Installing the OSID Diagnostic Tool. •First uninstall all previous versions of OSID Diagnostic. Use the Add or Remove Programs](https://static.fdocuments.net/doc/165x107/612667e2288ab26def3b8230/osid-diagnostic-tool-for-v4-3-tryb-zgodnoci-installing-the-osid-diagnostic.jpg)