Drugs for Insomnia beyond Benzodiazepines:...
49
1521-0081/70/2/197–245$35.00 https://doi.org/10.1124/pr.117.014381 PHARMACOLOGICAL REVIEWS Pharmacol Rev 70:197–245, April 2018 Copyright © 2018 by The American Society for Pharmacology and Experimental Therapeutics ASSOCIATE EDITOR: ERIC L. BARKER Drugs for Insomnia beyond Benzodiazepines: Pharmacology, Clinical Applications, and Discovery Tobias Atkin, Stefano Comai, and Gabriella Gobbi Neurobiological Psychiatry Unit, Department of Psychiatry, McGill University Health Center, McGill University, Montreal, Quebec, Canada (T.A., S.C., G.G.); and Division of Neuroscience, San Raffaele Scientific Institute and Vita-Salute University, Milan, Italy (S.C.) Abstract ................................................................................... 199 I. Introduction ............................................................................... 200 A. Insomnia as a Public Health Burden ................................................... 200 B. Changes in the Nosology of Insomnia in Diagnostic and Statistical Manual of Mental Disorders-V ............................................................................ 200 C. Clinical Guidelines for Insomnia Treatment and the Necessity of a Translational Approach .............................................................................. 200 D. The Dark Side of Benzodiazepines and Z-Drugs and the Off-Label Use of Other Drugs . . 201 II. Sleep Architecture ......................................................................... 201 III. The Receptor-Mediated Mechanism of Action of Hypnotics .................................. 202 A. GABA Receptor ........................................................................ 202 B. Serotonin Receptors .................................................................... 202 C. Serotonin 2 Receptors ................................................................... 203 D. Serotonin 1A Receptors ................................................................ 203 E. Noradrenaline Receptors ............................................................... 203 F. Dopamine Receptors ................................................................... 204 G. Orexin Receptors....................................................................... 205 H. Melatonin Receptors ................................................................... 205 I. Histamine Receptors ................................................................... 206 J. Other Receptors ....................................................................... 206 K. From Receptors to Sleep Circuits....................................................... 207 IV. Melatonergic Drugs ........................................................................ 208 A. Agomelatine ........................................................................... 208 1. Mechanism of Action................................................................ 208 2. Pharmacokinetics ................................................................... 208 3. Indications ......................................................................... 209 4. Results in Insomnia Disorder ....................................................... 209 5. Other Results....................................................................... 209 6. Conclusion.......................................................................... 209 B. Prolonged-Release Melatonin ........................................................... 209 1. Indications ......................................................................... 209 2. Pharmacokinetics ................................................................... 209 3. Results in Insomnia Disorder ....................................................... 209 4. Other Results....................................................................... 209 5. Conclusion.......................................................................... 209 Address correspondence to: Gabriella Gobbi, Neurobiological Psychiatry Unit, Department of Psychiatry, Ludmer Research and Training Building, 1033, Avenue des Pins Ouest, Montreal, Quebec, Canada H3A 1A1. E-mail: [email protected] This work was supported by the Quebec Network on Suicide, Mood Disorders, and Related Disorders and the Canadian Depression Research and Intervention Network (CDRIN). G.G. has received grants from the Canadian Institute of Health Research (CIHR), the Canada Foundation for Innovation (CFI), the Fonds de recherche du Québec – Santé (FRQS), and the Quebec Network on Suicide, Mood Disorders and Related Disorders. G.G. is an inventor and assignee in patents regarding the sleep properties of selective melatonin MT 2 agonists. https://doi.org/10.1124/pr.117.014381. 197 by guest on February 10, 2020 Downloaded from
Transcript of Drugs for Insomnia beyond Benzodiazepines:...

1521-0081/70/2/197–245$35.00 https://doi.org/10.1124/pr.117.014381PHARMACOLOGICAL REVIEWS Pharmacol Rev 70:197–245, April 2018Copyright © 2018 by The American Society for Pharmacology and Experimental Therapeutics
ASSOCIATE EDITOR: ERIC L. BARKER
Drugs for Insomnia beyond Benzodiazepines:Pharmacology, Clinical Applications, and Discovery
Tobias Atkin, Stefano Comai, and Gabriella Gobbi
Neurobiological Psychiatry Unit, Department of Psychiatry, McGill University Health Center, McGill University, Montreal, Quebec, Canada(T.A., S.C., G.G.); and Division of Neuroscience, San Raffaele Scientific Institute and Vita-Salute University, Milan, Italy (S.C.)
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 199I. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200
A. Insomnia as a Public Health Burden . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200B. Changes in the Nosology of Insomnia in Diagnostic and Statistical Manual of Mental
Disorders-V . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200C. Clinical Guidelines for Insomnia Treatment and the Necessity of a Translational
Approach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200D. The Dark Side of Benzodiazepines and Z-Drugs and the Off-Label Use of Other Drugs . . 201
II. Sleep Architecture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201III. The Receptor-Mediated Mechanism of Action of Hypnotics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202
A. GABA Receptor . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202B. Serotonin Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 202C. Serotonin 2 Receptors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203D. Serotonin 1A Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203E. Noradrenaline Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 203F. Dopamine Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 204G. Orexin Receptors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205H. Melatonin Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 205I. Histamine Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 206J. Other Receptors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 206K. From Receptors to Sleep Circuits. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 207
IV. Melatonergic Drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 208A. Agomelatine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 208
1. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2082. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2083. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2094. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2095. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2096. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
B. Prolonged-Release Melatonin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2091. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2092. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2093. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2094. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2095. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 209
Address correspondence to: Gabriella Gobbi, Neurobiological Psychiatry Unit, Department of Psychiatry, Ludmer Research andTraining Building, 1033, Avenue des Pins Ouest, Montreal, Quebec, Canada H3A 1A1. E-mail: [email protected]
This work was supported by the Quebec Network on Suicide, Mood Disorders, and Related Disorders and the Canadian DepressionResearch and Intervention Network (CDRIN).
G.G. has received grants from the Canadian Institute of Health Research (CIHR), the Canada Foundation for Innovation (CFI), the Fondsde recherche du Québec – Santé (FRQS), and the Quebec Network on Suicide, Mood Disorders and Related Disorders. G.G. is an inventor andassignee in patents regarding the sleep properties of selective melatonin MT2 agonists.
https://doi.org/10.1124/pr.117.014381.
197
by guest on February 10, 2020
Dow
nloaded from

C. Ramelteon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2091. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2092. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2133. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2134. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2135. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 213
D. Tasimelteon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2131. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2132. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2133. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2134. Results in Healthy Volunteers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2175. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2176. Results in Other Conditions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2177. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217
V. Orexin Receptor Antagonist Drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217A. Suvorexant . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 217
1. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2172. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2173. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2174. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2175. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
VI. Antidepressant Drugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220A. Amitriptyline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 220
1. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2202. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2203. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2204. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2205. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2216. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221
B. Mirtazapine. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2211. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2212. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2213. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2214. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2225. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2226. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 222
C. Trazodone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2221. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2222. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2223. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2224. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2225. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2226. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
D. Low-Dose Doxepin (,6 mg/day) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2271. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2272. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2273. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2274. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2275. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2276. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
ABBREVIATIONS: AUC, area under the curve; BZDs, benzodiazepines; CHMP, Committee for Medicinal Products for Human Use; DSM,Diagnostic and Statistical Manual of Mental Disorders; EEG, electroencephalogram; 5-HT, serotonin; KO, knockout; LC, locus coeruleus; LDT/PPT, lateralpontine tegmentum/pedunculopontine tegmental nuclei; MDD, major depressive disorder; MNPO, median preoptic nucleus;NREM, non-rapid eye movement sleep; OX, orexin; PRM, prolonged-release melatonin; PSQI, Pittsburgh Sleep Quality Index; PTSD,posttraumatic stress disorder; RCT, randomized-controlled trial; REM, rapid eye movement sleep; RT, reticular thalamus; SCN,suprachiasmatic nuclei; SDL, sublaterodorsal nuclei; SSRI, selective serotonin reuptake inhibitor; SWS, slow-wave sleep; vlPO, ventrolateralpreoptic area; WASO, wake after sleep onset; WT, wild type.
198 Atkin et al.

VII. Anticonvulsant Drugs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227A. Gabapentin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 227
1. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2272. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2293. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2294. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2295. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2296. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231
B. Pregabalin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2311. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2312. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2313. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2314. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2315. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2316. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231
VIII. Atypical Antipsychotic Drugs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 231A. Olanzapine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 233
1. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2332. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2333. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2334. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2335. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2336. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 233
B. Quetiapine. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2351. Mechanism of Action. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2352. Indications . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2353. Pharmacokinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2354. Results in Insomnia Disorder . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2355. Other Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2356. Conclusion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235
IX. Discoveries, Novel Pathways, and Pipelines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238A. Discoveries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238
1. Adenosine Receptor Agonist. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2382. Casein Kinase-1d/«. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2383. Selective Melatonin MT2 Receptors. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2384. Selective Orexin-2 Antagonist . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 238
B. Pipelines. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2391. Lumateperone . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2392. Piromelatine. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239
X. Conclusions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 239Acknowledgments. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240
Abstract——Although the GABAergic benzodiaze-pines (BZDs) and Z-drugs (zolpidem, zopiclone, andzaleplon) are FDA-approved for insomnia disorderswith a strong evidence base, they have many side effects,including cognitive impairment, tolerance, reboundinsomnia upon discontinuation, car accidents/falls,abuse, and dependence liability. Consequently, theclinical use of off-label drugs and novel drugs that donot target the GABAergic system is increasing. Thepurpose of this review is to analyze the neurobiologicaland clinical evidence of pharmacological treatments ofinsomnia, excluding the BZDs and Z-drugs. We analyzedthe melatonergic agonist drugs, agomelatine, prolonged-release melatonin, ramelteon, and tasimelteon; the dualorexin receptor antagonist suvorexant; themodulators of
the a2d subunit of voltage-sensitive calcium channels,gabapentin and pregabalin; the H1 antagonist, low-dosedoxepin; and the histamine and serotonin receptorantagonists, amitriptyline, mirtazapine, trazodone,olanzapine, and quetiapine. The pharmacology andmechanism of action of these treatments and theevidence-base for the use of these drugs in clinicalpractice is outlined alongwith novel pipelines. Thereis evidence to recommend suvorexant and low-dosedoxepin for sleep maintenance insomnia; there isalso sufficient evidence to recommend ramelteon forsleep onset insomnia. Although there is limitedevidence for the use of the quetiapine, trazodone,mirtazapine, amitriptyline, pregabalin, gabapentin,agomelatine, and olanzapine as treatments for
Drugs for Insomnia beyond Benzodiazepines 199

insomnia disorder, these drugs may improve sleepwhile successfully treating comorbid disorders, witha different side effect profile than the BZDs and
Z-drugs. The unique mechanism of action of eachdrug allows for a more personalized and targetedmedical management of insomnia.
I. Introduction
A. Insomnia as a Public Health Burden
Insomnia is a significant public health burden,increasing work absenteeism and health care costsin a large proportion of the population. It causesaltered cognition, emotional disturbances, and re-duced quality of life (Zammit et al., 1999; Wickwireet al., 2016). Insomniacs commonly complain of irri-tability, daytime sleepiness, low energy and motiva-tion, physical discomfort, and impaired cognitivefunctioning (Buysse et al., 2007; Fortier-Brochuet al., 2012; Morin and Jarrin, 2013), not to mentiondeficits in working memory, episodic memory, andsome aspects of executive functioning (Fortier-Brochuet al., 2012).The prevalence rate of insomnia in the general
population has been estimated as low as 5% to as highas 50% (Ohayon, 2002; Morin and Jarrin, 2013). Mostepidemiologic studies have found that about one-thirdof adults (30%–36%) report at least one symptom ofinsomnia, like difficulty initiating sleep or maintainingsleep; this rate drops to 10%–15% when daytimeconsequences, like excessive daytime sleepiness, areadded to the definition (Ohayon, 2002; Morin andJarrin, 2013). From 1999 to 2010, the number ofprescriptions for any sleep medication increased by293% (Ford et al., 2014). Strong increases in thepercentage of office visits resulting in a prescrip-tion for second generation benzodiazepines or Z-drugs(zopiclone, zolpidem, or zaleplon) sleep medications(;350%), benzodiazepine receptor agonists (;430%),and any sleep medication (;200%) were noted (Fordet al., 2014).
B. Changes in the Nosology of Insomnia in Diagnosticand Statistical Manual of Mental Disorders-V
The publication of the fifth edition of the Diagnosticand Statistical Manual of Mental Disorders (DSM-5)(American Psychiatric Association, 2013) fundamen-tally changed the landscape of sleep medicine and thediagnosis of insomnia. In DSM-IV, primary insomniawas distinguished from insomnia that is secondary toanother diagnosis, including major depressive disorderand generalized anxiety disorder. DSM-IV understoodsecondary insomnia as a symptom of a primary psychi-atric disease: the secondary insomnia was expected tonormalize with treatment of the primary disorder(American Psychiatric Association, 2013). However,clinical research has established that this “secondary”insomnia is often resistant to treatment of the primarydisorder: in the STAR*D trial, after remission with a
course of citalopram therapy, 54.9% of remitters con-tinued to experience midnocturnal insomnia and 71.7%continued to experience sleep disturbance in some form(Nierenberg et al., 2010). DSM-5 has eliminated pri-mary insomnia as a diagnosis in favor of insomniadisorder, which may occur alongside other diagnoseslike major depressive disorder. This revised definitionobliges the clinician to treat insomnia as a comorbidity,rather than a symptom of a primary illness. In thisreview, we use the term “insomnia disorder,” exceptwhen a published study explicitly states that it analyzespatients with “primary insomnia.”
C. Clinical Guidelines for Insomnia Treatment andthe Necessity of a Translational Approach
New evidence-based clinical practice guidelines forthe treatment of insomnia disorder were recentlypublished in The Journal of Clinical Sleep Medicine(Sateia et al., 2017a), representing the first comprehen-sive, systematic analysis of single agents for the treat-ment of insomnia disorder, developed using the GRADEmethodology (Grading of Recommendations, Assess-ment, Development, and Evaluation) (Sateia et al.,2017b). Unfortunately, the level of evidence for all ofthe authors’ recommendations was “weak.” This evalu-ation means that the strength of the evidence in thepublished data were low. Notably, all of the recom-mended treatments for sleep onset insomnia besidesramelteon are Z-drugs or BZD hypnotics. For sleepmaintenance insomnia, three of five of the treatmentoptions are Z-drugs or BZDs.
The dearth of strong published evidence led us toadopt a translational approach in exploring treatmentsfor insomnia disorder, integrating the neurobiologicalmechanism of action of each drug gleaned from basicscience and integrating it with reported clinical dataand current medical practice. This approach is cur-rently the standard in pharmacological research and isa priority for federal and foundational grants. Althoughclinical research is critical for establishing evidence-based guidelines for treatment, knowledge gleanedfrom basic research can be helpful for the clinicaljudgment of the therapeutic efficacy of hypnotics andthe treatment of psychiatric comorbidities (Comai et al.,2012a,b).
In this review, we will focus on drugs that are notBZDs or Z-drug, because an extensive literature al-ready exists. Our approach will be translation, offeringalternatives to BZDs and Z-drugs. We will also de-scribe novel hypnotic compounds and pharmaceuticalpipelines.
200 Atkin et al.

D. The Dark Side of Benzodiazepines and Z-Drugsand the Off-Label Use of Other Drugs
Although the market for insomnia medications con-tinues to be dominated by BZDs and Z-drugs, bothcategories of drug have numerous problematic effects asshort-term treatment and, in particular, as long-termtherapy. BZDs are associated with hangover effects thenext day, cognitive or memory impairment, the rapiddevelopment of tolerance, rebound insomnia upon discon-tinuation, car accidents or falls, and a substantial risk ofabuse and dependence (Foy et al., 1995; Hemmelgarnet al., 1997; Soldatos et al., 1999; Ashton, 2005). A largeproportion of people prescribedBZDdrugs become chronicusers. Furthermore, BZDs are a factor in approximately5%–10% of car accidents, although the rate in individualstudies varies from 1% to 65% (Thomas, 1998).Z-drugs also cause cognitive impairments: case con-
trol studies find that BZD or Z-drug use approximatelydoubles the risk of being involved in a motor vehicleaccident (Thomas, 1998; Gunja, 2013b). They can pro-duce dependence (Lugoboni et al., 2014) as well asnext-day cognitive, memory, psychomotor and balanceimpairments (Mets et al., 2011).The problems with BZDs have led clinicians to pre-
scribe other medications that are perceived to be lessharmful or to be less liable to addiction. As an example,in the United States in 2002, the antidepressantmedication trazodone was the most commonly pre-scribed medication for insomnia, with 34% moreprescriptions than the most commonly prescribedFDA-approved treatment (Walsh, 2004). The PrescriberNational Summary Report, Calendar Year 2014 poolsdata from all the Medicare recipients in the UnitedStates. In one cross-sectional study of American adults,3% of 32,328 people used a “prescription medicationcommonly used for insomnia” in the previous month:38% of those who received a hypnotic medication re-ceived Z-drugs, 31% trazodone, 17% BZDs, 11% quetia-pine, and only 5% received doxepin (Bertisch et al.,2014). This study confirms that drugs prescribed off-label are very common in the treatment of insomnia,despite the low number of randomized, controlled trials(RCTs).
II. Sleep Architecture
In mammals, physiological sleep is divided into twostrikingly distinct states known as non-rapid eye move-ment (NREM) and rapid eye movement (REM) sleep.Historically, NREM sleep was subdivided into fourstages (stages 1, 2, 3, 4) defined according to differentelectroencephalogram (EEG) patterns (Rechtschaffenand Kales, 1968). According to the manual of theAmerican Academy of Sleep Medicine published in2007 (Iber et al., 2007), NREM sleep is now dividedinto three progressively deeper stages of sleep named
stage N1, stage N2, and stage N3 (formerly stages 3 and4). REM sleep is now officially referred to as stage R.The EEG pattern in NREM sleep is synchronous andpresents characteristic waveforms: sleep spindles,K-complexes, and high-voltage slow waves. Stage N1accounts for 2%–5% of total sleep time and is the phaseof transition between the awake state and sleep. StageN2 accounts for 45%–55% of total sleep time and occursthroughout the entire sleep period. The descent fromstage N1 to stage N2 is characterized by a decrease inthe frequency of the EEG trace paralleled by an increasein its amplitude. The EEG hallmark of N2 are thetawaves. N2 is also characterized by the occasional occur-rence of a series of high-frequencywaves (8–14Hz) knownas sleep spindles, generated by interactions betweenthalamic and cortical neurons (De Gennaro and Ferrara,2003), and fast and high-amplitude wave forms known asK-complexes also occur (Amzica and Steriade, 2002).According to Rechtschaffen and Kales’ (1968) criteria, aK-complex is defined as anegative slowwave immediatelyfollowed by a positive wave exceeding 0.5 seconds induration.
As stage N2 sleep progresses, high-voltage, slow-wave activity appears as the subject enters stage N3.Stage N3, which corresponds to deep or delta-wavesleep and reflects slow-wave sleep (SWS), occurs mostlyin the first third of the night and accounts for 5%–15% oftotal sleep time. During this sleep stage, there is afurther fall in blood pressure, a slowing of breathing,and a reduction in body temperature, with reducedmuscle activity, although muscles maintain their tonusand thus some movements can be observed.
Stage R or REM sleep is defined by low-amplitudedesynchronized theta EEG activity and represents20%–25% of total sleep time. It occurs in four to fiveepisodes throughout the night and is characterized bycomplete disappearance of muscle tone paradoxicallyassociated with a cortical but also hippocampal activa-tion and rapid eye movements. Since REM sleep EEGactivity closely or paradoxically resembled the EEG ofalert-waking subjects, this sleep stage has been alsoreferred as paradoxical sleep, particularly in studiesconducted in animals.
In physiological conditions, the activity of the brainover the course of the night proceeds from wakingthrough the three stages of NREM sleep and thenREM sleep. NREM sleep and REM sleep continue toalternate through the night in a cyclical fashion, usuallywith a total of four to five sleep cycles throughout thenight. Importantly, as sleep progresses, the time spentin stage N3 becomes shorter, whereas the time spent inREMgets longer. The average length of the first NREM-REM sleep cycle is between 70 and 100 minutes andthat of the second and later cycles is about 90–120 minutes. Sleep architecture, including the durationof the different stages as well as the duration of aNREM-REM cycle, is strongly dependent on the
Drugs for Insomnia beyond Benzodiazepines 201

subject’s age. With aging, humans tend to experience anincrease in the latency to fall asleep, more fragmentedsleep, and less time spent in SWS, particularly in theearly cycles of sleep. One of the parameters providinginformation concerning sleep fragmentation is the“sleep efficiency index” that is a measure of thepercentage of total time in bed actually spent sleepingand is calculated by the sum of the time spent in sleepstage N1, N2, N3, and REM, divided by the total timespent in bed. Specific details on the changes in the sleepstructure occurring during aging are outside the scopeof this paper but are analyzed in a comprehensive recentreview written by Mander et al. (2017). Restorativesleep is not only dependent on an adequate duration ofsleep; the physiological architecture of sleep must beconserved. Under certain conditions and with certainpharmacological treatments, the total duration of sleepmay remain unchanged or increased, but deviationsfrom normal sleep architecture generate increasedsleep fragmentation. Disturbances in subjects’ sleeparchitecture results in a sense of having had nonrestor-ative sleep and is associated with next-day impairmentsin conducting daily activities. Unfortunately, most ofthe drugs currently used as hypnotics—in particularbenzodiazepines, but also Z-compounds to a lesserextent—disturb sleep architecture (Bastien et al.,2003; Gunja, 2013a).
III. The Receptor-Mediated Mechanism of Actionof Hypnotics
Drugs currently used to treat insomnia mainly act onspecific ionotropic or G-protein-coupled receptors lo-cated in specific brain areas. Each receptor modulatesdifferent characteristics of sleep. It is thus important forthe clinician to understand the mechanism of action ofeach hypnotic to target better its effect in individualpatients. This translational approach helps to build amore personalized medicine, targeted to the patient,that overcomes the limitations of overarching clinicalguidelines. While guidelines tend to homogenize thepatient population, a translational approach based onthe mechanism of action of each drug may help totarget the individual patient and his or her particularcomorbidities.
A. GABA Receptor
The most studied receptors in the treatment ofinsomnia are the GABAA receptors, GABA being thechief inhibitory neurotransmitter in the mammaliannervous system,where BZDs and Z-drugs act. BZDs andZ-drugs act as positive allosteric modulators at theGABAA binding site, potentiating GABA’s inhibitoryeffect (Stahl, 2008). The combination of GABA at thereceptor’s agonist site and benzodiazepine-receptoragonists at the allosteric site increases the frequencyof the chloride channel opening to an extent that does
not occur with GABA alone (Stahl, 2008). The result isneuronal inhibition. Similar to other ligand-gated ionchannels, the GABAA receptor is composed of fivesubunits belonging to different subunit classes (a1–6,b1–3, g1–3, d, «, u, p) that are distributed throughoutthe brain differentially; there is also some interindivid-ual variability in their localization. For a detailedreview on this topic, please see Olsen and Sieghart(2009). In this way, BZDs and Z-drugs exert their effectsas sedatives, anxiolytics, anticonvulsants, muscle re-laxants, and hypnotics. The main difference betweenBZDs and Z-drugs is in their receptorial affinitiestoward the different GABAA subunits. BDZs showsimilar affinity to the a1, a2, a3, and a5 receptorsubtypes. In contrast, most of the Z-drugs show higheraffinity for a subset of the alpha subunits, mainly the a1receptor subtype, that seems to be specifically impli-cated in sleep but not in anxiety. Zaleplon, zopiclone,and zolpidem have high affinity and potency for the a1subunit and low affinity and potency at a2 and a3
subunits; eszopiclone—the (S)-enantiomer of zopiclone—has high affinity and potency for the a2 and a3subunits (Nutt and Stahl, 2010). Due to their selectiveagonism, Z-drugsmainly produce sedative and hypnoticproperties and likely display improved tolerability overthe BZDs (Wilson and Nutt, 2007).
This review will focus on alternate mechanisms ofaction that are not directly mediated through GABAreceptors, with the exception of the gabapentinoids(pregabalin and gabapentin). Although pregabalin andgabapentin are analogs of GABA, they do not binddirectly to GABAA or benzodiazepine receptors. Instead,they inhibit the a2d-1 subunit voltage-dependent cal-cium channels. They have been found to increase SWSsleep in patients diagnosed with epilepsy and insomnia(Bazil et al., 2012) and healthy adults (Foldvary-Schaefer et al., 2002; Hindmarch et al., 2005). Furtherdevelopment of novel a2d calcium channels like ataga-balin (PD 200390) was pursued for the treatment ofinsomnia but then discontinued following unsatisfac-tory trial results (Springer Adis Insight, 2017).
B. Serotonin Receptors
The 5-HT-containing neurons of the dorsal raphenuclei discharge maximally during waking and de-crease their firing during SWS; they cease firing duringREM sleep, similar to the norepinephrine-containingneurons of the locus coeruleus (Jones, 2005). The5-HT1A agonist OH-DPAT, which decreases 5-HT firingactivity by activating its autoreceptors (Gobbi et al.,2001) increases REM sleep (Portas et al., 1996). Al-though 5-HT1A receptors are autoreceptors located atthe somatodendritic level, 5-HT1B receptors are autore-ceptors localized at postsynaptic sites. 5-HT1B receptorsare also used as heteroceptors in many cells throughoutthe brain to inhibit the release of neurotransmittersother than serotonin (Marek, 2010). Furthermore,
202 Atkin et al.

serotonergic neurons attenuate cortical activationthrough inhibitory influences on other neurons of theactivating systems, including acetylcholine-containingneurons (Jones, 2005).
C. Serotonin 2 Receptors
The 5-HT2 receptor is located in the prefrontal andorbitofrontal cortex, the (subgenual) anterior cingulatecortex, the occipital, and parietal cortex (vanDyck et al.,2000; Adams et al., 2004; Hinz et al., 2007); in thenucleus accumbens, olfactory tubercule, and the hippo-campus (Pompeiano et al., 1994; Barnes and Sharp,1999; López-Giménez et al., 2001); and in the locuscoeruleus, areas that are important for both sleepmodulation and mood regulation (Szabo and Blier,2001).At the cellular level, 5-HT2A receptors are located on
apical dendrites on pyramidal cells and, particularly insubcortical regions, on local (GABAergic) interneurons(Jakab and Goldman-Rakic, 1998; Barnes and Sharp,1999; Aghajanian and Sanders-Bush, 2002). Althoughthe mechanism of action of 5-HT2A/2C receptor antago-nists has yet to be fully elucidated, it is likely that theypromote SWS via a reduction of inhibitory input to thecells of the ventrolateral preoptic nucleus that fireduring sleep. Through postsynaptic 5-HT2A receptorson GABAergic cells of the reticular thalamus, seroto-nergic fibers from the dorsal raphe and supralemniscalnucleus (B9) modulate the reticular thalamus that inturn regulates sleep and wakefulness (Rodrìguez et al.,2011).Recent studies with more subtype-selective 5-HT2A
and 5-HT2C receptor ligands (antagonists and inverseagonists), as well as experiments in knockout (KO)mice,support a role for 5-HT2A receptor subtypes in pro-moting SWS and the 5-HT2C receptor in promotingREM (Popa et al., 2005).Ritanserin, a potent antagonist of the serotonin
receptors 5-HT2A and 5-HT2C, has been found to in-crease SWS in healthy volunteers to a greater degreethan ketanserin (a drug with less potent effects as anantagonist of the 5-HT2C receptor, used clinically as anantihypertensive) (Sharpley et al., 1994). Ritanserinwas never commercialized for safety problems, althoughit did show efficacy at increasing SWS and delta activityin young male poor sleepers (Viola et al., 2002), under-lining the importance of these receptors in the regula-tion of SWS.Interestingly, many hypnotic drugs prescribed off-
label (trazodone, mirtazapine, olanzapine, quetiapine)act through 5-HT2A and 5-HT2C receptors to enhancesleep (Landolt and Wehrle, 2009). Trazodone, the first5-HT2A antagonist, was initially developed as an anti-depressant, but is currently one of the most commonhypnotics prescribed in the clinic (Bertisch et al., 2014).Similarly, the 5- and 10-mg doses of olanzapine com-pared with placebo, significantly increased SWS, sleep
continuity measures, and subjective sleep quality(Sharpley et al., 2000). See Tables 1 and 2 for thereceptorial affinities of each drug and for their effects onsleep architecture, respectively.
D. Serotonin 1A Receptors
The 5-HT1A receptor is the main 5-HT autoreceptor,located at the somatodendritic level of the 5-HT neuronsof the dorsal raphe as well as at synaptic terminals inthe hippocampus and prefrontal cortex. 5-HT1 knockout(KO) mice have increased 5-HT firing activity (Richeret al., 2002) and decreased REM sleep, but not SWS(Boutrel et al., 2002); the 5-HT1A agonist OH-DPATinduces a decrease in REM sleep in the first 2 hoursafter injection followed by an increase in REM after 6–8hours (Boutrel et al., 2002). 8-OH-DPAT (1.0–4.0 mg)injected into the dorsal raphe nucleus increased slow-wave sleep and decreased wakefulness, although itsadministration of subcutaneously induced biphasiceffects such that low doses decreased wakefulness andincreased slow-wave sleep while higher doses inducedopposite effects, perhaps due to the opposing effects ofthe 5-HT1A autoreceptors and heteroreceptors (Montiand Jantos, 1992). Given these opposing and complexeffects, employing 5-HT1A partial agonists is a rationalapproach to insomnia, given their capacity to act asagonists when the levels of endogenous agonist are lowand as antagonists when the levels of endogenousagonist are high.
5-HT1B knockout mice have increased REM sleep andlower SWS during the light phase and lack REM sleeprebound after deprivation, suggesting that the blockageof 5-HT1B receptors increases REM and decreasesNREM sleep (Boutrel et al., 1999). In agreement withthis finding, in wild-type (WT) mice, the 5-HT1B ago-nists CP 94253 andRU24969 induced a dose-dependentreduction of paradoxical sleep during the 2–6 hoursafter injection, whereas the 5-HT1B/1D antagonist GR127935 enhanced paradoxical sleep (Boutrel et al.,1999).
Quetiapine and trazodone both act on 5-HT1A recep-tors as partial agonists (Richelson and Souder, 2000;Odagaki et al., 2005).
E. Noradrenaline Receptors
Similarly to 5-HT neurons, the norepinephrine-containing neurons of the locus coeruleus (LC) nucleidischarge maximally during waking and decreasetheir firing during SWS; they are nearly silent duringparadoxical or REM sleep (Jones, 2005).
The most important adrenergic receptors implicated insleep are a1 and a2 receptors. a2 Receptors are located atpresynaptic terminals, acting as themain norepinephrineneuron autoreceptors, although they are also present atthe postsynaptic terminal. The activation of the a2
autoreceptor decreases LC activity, while, in contrast, a2
receptor blockade using a2 antagonists increases the
Drugs for Insomnia beyond Benzodiazepines 203

firing activity of LC neurons (Gobbi and Blier, 2005). Infact, although the a2 agonist clonidine decreases LCactivity and thus promotes sleep (particularly SWS) whileinhibiting REM (De Sarro et al., 1987; Berridge et al.,2012), there is evidence that the selective a2 antagonistyohimbine increases wakefulness, at least in rats (Mäkeläand Hilakivi, 1986).
However, selective knockdown of a2A-adrenergicreceptors in the LC abolished a2 agonist dexmedetomidine-induced loss-of-righting-reflex, but not sedation (Zhanget al., 2015). These findings implicate other structuresbesides the LC in a2 receptorial regulation of arousal:these structures include the preoptic area, in which a2
receptors are situated on GABAergic interneurons,which influence sleep through reciprocal inhibitoryprojections to the W systems; or the prefrontal cortex,where a2 receptors are likewise situated on GABAer-gic neurons (Manns et al., 2003; Luppi et al., 2017).
Indeed, when GABAergic neurons (“OFF neurons”)containing a2 receptors located in the prefrontal cortexare stimulated during SWS, their firing activity ceases,which likely produces paradoxical or REM sleep (Mannset al., 2003). This complex a2 receptor-mediated mech-anism may account for the manner in which the a2
antagonist mirtazapine promotes sleep, although itincreases LC firing (Gobbi and Blier, 2005).
The a1 and beta adrenergic receptors are also in-volved in the regulation of arousal. While individualadministration of the a1 blocker prazosin producesdecreased behavioral arousal and individual adminis-tration of the beta noradrenergic antagonist timololhas no effect, coadministration of prazosin and timololproduces a substantial, synergistic increase in slow-wave firing activity with a corresponding strongsedative effect behaviorally (Berridge and Espana,2000).
F. Dopamine Receptors
Dopamine neurons are also active during wakeful-ness and decrease during REM sleep and SWS (Montiand Monti, 2007). In particular, the dopamine D2
receptor is one of the main receptors involved in sleepregulation. D2KO mice exhibit a significant decrease inwakefulness, with a concomitant increase in NREMandREM sleep and a drastic decrease in low-frequencyelectroencephalogram delta power (0.75–2 Hz) ofNREM sleep, especially during the first 4 hours follow-ing lights off. In agreement with these findings, the D2
antagonist raclopride mimicked these effects in WTmice (Qu et al., 2010). Similarly, the dopamine D2
receptor antagonists haloperidol and chlorpromazinehave the tendency to induce sleepiness in humansubjects, while blockers of the dopamine transporterlike amphetamine and modafinil increase wakefulnessby increasing extracellular levels of dopamine in thesynapse (Schmitt and Reith, 2010). In contrast, para-doxically, the antiparkinsonian D2 agonist ropinirole
TABLE
1Sum
maryof
mainmolecular
targetsof
hypn
otic
drug
sMecha
nism
-of-action
detailscanbe
foun
din
thetext
ofthis
review
,inreview
articles
(San
ger,20
04;W
ilsonan
dArgyrop
oulos,20
05;S
ills,2
006;
Stahl,20
09),an
d/or
inthesu
mmaryof
prod
uct
characteristicsforea
chindividu
aldr
ug.
Dru
g5-HT1
5-HT2
5-HT3
5-HT7
a1
a2
MT1/M
T2
OX1/O
X2
H1
5-HTT
NET
D1
D2
D4
m1
Voltage
-Gated
Ca2
+Cha
nnels
GABAA
Ram
elteon
XTas
imelteon
XMelaton
inpr
olon
ged-releas
eX
Ago
melatine
XX
Low
-dosedo
xepin
XX
XSuv
orex
ant
XTrazodo
ne
XX
XX
XAmitryptiline
XX
XX
XQuetiapine
X*
X*
X*
X*
X*
X*
XX*
Olanz
apine
XX
XX
XX
XGab
apen
tin
XPrega
balin
XMirtaza
pine
XX
XX
XBen
zodiaz
epines
XZ-com
pounds
X
*Bindingmainly
dueto
itsmetab
olitenorqu
etiapine.
204 Atkin et al.

also induces sleepiness, but mostly daytime sleepinessand sleep attacks during the day (Paus et al., 2003),likely through activation of D2 autoreceptors that de-crease DA firing activity during the daytime.
G. Orexin Receptors
The orexins (OXs), also known as the hypocretins, area pair of excitatory neuropeptide hormones with ap-proximately 50% sequence homology: orexin-A andorexin-B (hypocretin-1 and -2). They are producedexclusively by a population of neurons in the lateralhypothalamic area (de Lecea et al., 1998; Sakurai et al.,1998). Physiological effects of the OXs in the brainresult from the activation of two G-protein-coupledreceptors, named orexin 1 (OX1) and orexin 2 (OX2)receptors (Sakurai et al., 1998). OX1 has one-orderhigher affinity for OX-A than for OX-B, whereas OX2
binds OX-A and OX-B with similar affinities.The orexinergic system is known to promote behav-
ioral arousal, increase food intake and locomotor activ-ity (Sakurai et al., 1998; Nakamura et al., 2000), andinduce wakefulness (Hagan et al., 1999). In addition,the OXs appear to regulate the stress response byincreasing the activity of the hypothalamic-pituitaryaxis (Al-Barazanji et al., 2001). Furthermore, they areimplicated in the pathophysiology and treatment ofdepressive-like behavior (Nollet et al., 2011).KO animals that lack the prepro-orexin gene, OX2
gene, or orexin neurons have narcolepsy-like behavior,including fragmentation of sleep/wakefulness, directtransitions from wake to REM sleep, and sudden lossof muscle tone while still awake (cataplexy) (Chemelliet al., 1999; Lin et al., 1999; Hara et al., 2001; Willieet al., 2003). However, OX1KOmice havemild or almostno abnormality in the regulation of sleep and wakeful-ness, suggesting that the orexin signal through OX2 hasa more critical role in the regulation of sleep andwakefulness, especially in the maintenance of arousal.
The expression pattern of orexin receptors matches theafferent projections of orexin neurons throughout thebrain. The few studies using selective antagonists ofthe OX1 and OX2 receptors have demonstrated thatselective blockade of OX2, but not OX1, increases REMand NREM. However, coadministration of the selectiveOX1 antagonist and the selective OX2 antagonist in-tensified the effect of OX2 blockade on REM and NREM(Dugovic et al., 2009). Other studies have agreed thatOX1 may play a role in the regulation of sleep andarousal (Mieda et al., 2011).
A novel orexin antagonist (suvorexant) was recentlyput on the market and other selective orexin antago-nists are under development (Winrow and Renger,2014).
H. Melatonin Receptors
The neurohormonemelatonin activates twoG-protein-coupled receptors, MT1 and MT2. Melatonin is impli-cated in circadian rhythms and sleep regulation,but the differential role of its individual receptorsremains undefined.
Melatonin receptors have a specific localization thatimplicates them in physiological functions related tosleep (Lacoste et al., 2015). MT2 receptors are located inthe reticular thalamus, an area involved in modulatingSWS (Steriade et al., 1993), as well as the substantianigra (pars reticulata), supraoptic nucleus, red nucleus,and the CA2, CA3, CA4 areas of the hippocampus andSCN (Ekmekcioglu, 2006; Ochoa-Sanchez et al., 2011),while MT1 is located in the locus coeruleus, the dorsalraphe, and areas CA2 and CA3 of the hippocampus andSCN (Lacoste et al., 2015).
Recently our group has better characterized thedifferential role of each receptor in sleep function usingMT1KO, MT2KO, and double MT1-MT2KO as well asselective MT2 ligands (Comai et al., 2013). MT2KOmicehave a selective disruption of SWS during the inactive
TABLE 2Summary of the effects of the different hypnotic drugs on the sleep architecture and their potential to induce dependence liability
Drug Latency toSleep Onset
Effect on NREM Sleep Effect onREM Sleep
SleepEfficiency
DependenceLiabilityStage N1 Stage N2 Stage N3 also referred as SWS
Benzodiazepines ↓ ↓ ↑ ↓ ↓ ↑ HighZ-drugs ↓ ↔ ↑ ↔ ↔ ↑ ModerateRamelteon ↓ ↔ ↑ ↓ ↔ ↑ LowTasimelteon ↓ n.a. n.a. n.a. ↑ ↑ LowMelatonin prolonged-release ↓ ↔ ↔ ↔ ↔ ↑ LowAgomelatine ↓ ↔ ↔ ↑ ↔ ↑ LowLow-dose doxepin ↓ ↔ ↑ ↔ ↔ ↑ LowSuvorexant ↓ ↔ ↑ ↔ ↑ ↑ LowTrazodone ↔ ↔/↓ ↔/↓ ↔/↑ ↔/↓ ↔ LowAmitryptiline ↓ n.a. n.a ↑ ↓ ↑ LowQuetiapine ↓ ↔ ↑ ↔↓ ↓ ↑ LowOlanzapine ↓ ↔ ↔/↑ ↑ ↓/↔/↑ ↑ LowGabapentin ↔ ↔ ↔ ↑ ↔ ↑/↔ ModeratePregabalin ↓ ↔ ↔ ↑ ↓ ↑ ModerateMirtazapine ↔ ↓ ↔ ↑ ↔ ↑ Low
↑: Increase; ↓: decrease; ↔: no change. n.a.: not assessed.
Drugs for Insomnia beyond Benzodiazepines 205

phase and increased wakefulness, whereas MT1KOmice have a selective disruption of REM during theinactive phase and an increase of NREM. These resultselucidate the opposing and differential effects of the tworeceptors in the neurobiology of sleep.DualMT1-MT2 KOmice only show a small increase in
wakefulness, without a difference in total sleep com-pared with their WT counterparts (Comai et al., 2013),establishing that the MT1 and MT2 receptors may haveopposing roles. This interpretation fits with the factthat melatonin and drugs that bind both MT1 and MT2
only modify the time to induction of sleep, without aglobal effect on total sleep time or sleep architecture(Comai et al., 2015). Thus, the absolute benefit ofmelatonin compared with placebo is smaller than otherpharmacological treatments for insomnia (Ferracioli-Oda et al., 2013). Similarly, ramelteon, a dual agonist ofboth MT1 and MT2, has only been approved by the FDAfor the treatment of insomnia characterized by difficultywith sleep onset; it does not affect total sleep duration orincrease SWS.
I. Histamine Receptors
The sole source of brain histamine is neurons local-ized in the hypothalamic tuberomammillary nuclei(Haas and Panula, 2003). These neurons project axonsto the whole brain, although functionally distincthistaminergic neural circuits differentially influenceindividual brain regions. Four histamine receptors havebeen identified: H1, H2, H3, and H4 (Takahashi et al.,2002). In general, histamine modulates inflammatoryresponses through peripheral H1 receptors and modu-lates gastric acid secretion through peripheral H2
receptors. This led to the discovery and therapeuticuse of potent selective H1 and H2 receptor antagonists.In contrast to the H1, H2, and H4 receptors, the H3
receptor is predominantly expressed in the CNS(Lovenberg et al., 1999; Oda et al., 2000), acting as anautoreceptor on presynaptic neurons and controllinghistamine turnover. H3 receptors have also been shownto act as heteroreceptors in dopamine-, serotonin-,noradrenaline-, GABA-, and acetylcholine-containingneurons (Schlicker et al., 1994).The H1 receptor is probably the most important
physiological histamine target in the maintenance ofwaking. In animal studies, H1 receptor agonists increasewake duration (Passani and Blandina, 2011). H1 receptorKO mice show fewer incidents of brief awakening (,16-second periods), prolonged durations of NREM sleepepisodes, a decreased number of state transitions betweenNREM sleep and wakefulness, and a shorter latency forinitiating NREM sleep. When the H3 receptor antagonistciproxifan was administered intraperitoneally to WTmice, wakefulness increased in the mice in a dose-dependent manner but did not increase at all in H1KOmice, highlighting the interdependent functional relation-ship between H1 and H3 receptors (Huang et al., 2006).
H3KO mice show clear signs of enhanced histamin-ergic neurotransmission and vigilance, with higherEEG u power during spontaneous wakefulness andduring behavioral tasks. During the dark period, theydisplay deficient wakefulness and signs of sleep de-terioration, such as pronounced sleep fragmentationand reduced cortical slow activity during SWS, whichoccurs due to a desensitization of postsynaptic hista-minergic receptors as a result of constant histaminerelease (Gondard et al., 2013).
Prescription drugs like mirtazapine, quetiapine, andhydroxyzine—not tomention nonprescription sleep aidslike diphenhydramine—act on histaminergic neurons.
J. Other Receptors
Other receptors involved in sleep, but which remainto be pharmacologically exploited, include the adeno-sine A1 and A2 receptors (Jacobson and Gao, 2006).Interestingly, the arousal effect of the adenosine antag-onist caffeine is mediated through the adenosine A2A
receptor, but not the A1 receptor (Huang et al., 2005).Adenosine mediates the somnogenic effects of prior
wakefulness and likewise plays an important role in theregulation of the duration and depth of sleep afterwakefulness (reviewed by Greene et al. (2017). Phar-macological data suggest that A1A receptors are in-volved in the regulation of sleep, although a lack of A1A
receptors is not sufficient to prevent homeostatic regu-lation of sleep (Stenberg et al., 2003). It is conceivablethat although the A1A receptor is an important factor forsleep regulation in normal animals, other factors, suchas the A2A receptor, may compensate for the absence ofthe A1A receptor when it is deleted in knockout models.Indeed, it has been shown that the A2A receptor has akey role in adenosine-mediated sleep-promoting effects(Urade et al., 2003).
Melanin-concentrating hormone (MCH) neurons areknown to be active during REM sleep and the stimula-tion of these neurons promotes REM sleep; indeed,electrophysiological recordings of MCH neurons acrossthe natural sleep-wake demonstrates that they do notfire during waking, fire occasionally during NREMsleep, and fire maximally during REM sleep (Hassaniet al., 2009). Importantly, they are colocalized withorexin neurons in the lateral hypothalamic area andadjacent zona incerta but as unique cell populationsspatially intermingled with each other (reviewed byYamashita and Yamanaka (2017).
Importantly, when MCH neurons are active, theyinhibit orexin neurons, and knockout of MCH peptideand the MCHR1 receptor in mice produces less REMand NREM sleep. Optogenetic studies have confirmedthe role of MCH neurons in inducing REM sleep:optogenetic activation of these cells during NREM sleepproduces REM, but activation during wakefulnessproduces no effect. MCH neurons also play a role inNREM sleep, because temporally controlled ablation of
206 Atkin et al.

these cells increases wakefulness and decreases NREMsleep duration without affecting REM sleep (Tsunematsuet al., 2014).
K. From Receptors to Sleep Circuits.
The manner in which unique neurotransmitters andindividual brain areas reciprocally interact is still notunderstood in its entirety. The neural circuits thatgenerate arousal and sleep (both NREM and REM)remain to be completely elucidated.Humans are diurnal mammals, with a circadian clock
that promotes wakefulness during the day, even ashomeostatic sleep drive builds up. Importantly, sleeptiming is phase-linked to intrinsic circadian rhythm-controlled temperature rhythms as well as extrinsiclight and dark signaling (Scammell et al., 2017).In mammals, the circadian rhythm is organized by
the suprachiasmatic nuclei (SCN). The retinohypotha-lamic tract, which contains the intrinsically photosen-sitive retinal ganglion cells and the photopigmentmelanopsin, projects directly and monosynaptically tothe SCN via the optic nerve and the optic chiasm. TheSCN, which is rich in MT1 and MT2 receptors (Lacosteet al., 2015), projects to the paraventricular nucleus,and the “darkness” signal is eventually relayed tosympathetic fibers that innervate the pineal gland,which produces melatonin in response to darkness.Melatonin then stimulates the brain’s MT2 receptorsin the NREM sleep activating regions of the brain: thereticular thalamus and the preoptic areas, includingboth the ventrolateral preoptic area (vlPO) and themedian preoptic nucleus (MNPO) (Ochoa-Sanchezet al., 2011; Lacoste et al., 2015). Specifically, theMNPO appears to regulate the firing activity of thevlPO (Chou et al., 2002). It has been shown that duringthe transition from wakefulness to sleep, the MNPO—
which specifically contains neurons that fire duringslow-wave and paradoxical sleep, with slow dischargingactivity,5 Hz—begin to fire not before, but after, sleeponset, with a gradual increase in discharge rate (Sakai,2011). During NREM sleep, the vlPO sends inputs thatact to reduce the activity of the orexinergic arousalsystem and the monoamine nuclei (including the ven-tral tegmental area containing DA neurons, the dorsalraphe containing 5-HT neurons, and the LC containingNE neurons) by releasing the inhibitory neurotrans-mitters GABA and galanin. As a feedback mecha-nism, vlPO neurons receive reciprocal inputs from thearousal nuclei, including the ventral tegmental area,dorsal raphe, and LC; the vlPO also receives input fromthe histaminergic tuberomammillary nucleus(Adamantidis et al., 2010).The reticular thalamus (RT) is another area essential
for NREM sleep: people suffering from fatal familialinsomnia show thalamic disruption that inactivatestheir ability to sleep, which is paralleled by a dysfunc-tion in melatonin production (Portaluppi et al., 1994).
RT neurons discharge in burst activity exclusivelyduring NREM, and thalamocortical pathways projectthis synchronous burst activity, intermingled withperiods of silence, onto the cortex. This rhythmic firingactivity generates the synchronized EEG pattern typi-cal of SWS, which produces disconnection between thecortex and the outside world (Steriade and Timofeev,2003). The RT is also rich in melatonin MT2 receptors,which are likely activated at the beginning of sleep(Ochoa-Sanchez et al., 2011). Disconnection betweenthe prefrontal cortex and sensory input is greatestduring Stage 4 of NREM sleep, when the frequency ofthe EEG trace is the lowest and its amplitude is thehighest. Conversely, during wakefulness, the RT andthalamocortical neurons are depolarized by inputs fromthe reticular activating system of the brain stem anddischarge instead with a tonic activity (adapted fromSteriade et al., 1993; Purves et al., 2004).
REM sleep, in contrast, is regulated by other brainareas. Many researchers have hypothesized that REMsleep ismediatedmostly through cholinergic neurons locatedin the lateralpontine tegmentum/peduncolopontine teg-mental nuclei (LDT/PPT). These neurons are activeduring REM sleep and generate the cortical activationand atonia typical of this sleep stage and are inactiveduring NREM sleep. Indeed, LDT/PPT neurons sendinputs to the ventromedial medulla, which inhibitsmotor neurons by releasing GABA and glycine into thespinal and brain stemmotor neurons, producing atonia.LDT/PPT neurons are also the main source of acetyl-choline to the thalamus: activation of this acetylcholinepathway depolarizes thalamic neurons, generating thecortical activation associated with REM sleep anddreaming. Other nuclei important for REM sleep regu-lation are 1) the sublaterodorsal nucleus (SDL), whichproduces GABA and glutamate and projects to theglycinergic/GABAergic premotor neurons in the ventro-medial medulla and ventral horn of the spinal cord, andthrough these circuits likely inhibits motor neuronsduring REM sleep, and 2) the MCH-containing neuronsthat fire during REM sleep and decrease their activityduring NREM sleep and wakefulness. The “REM-offversus REM-on” theory of REM sleep hypothesizes thatduring the REM-on period, LDT/PPT, SDL, and MCHneurons are active and inhibit monoamine neurons aswell asmotor neurons, while during the REM-off period,the vlPAG/LPT is inhibited by MCH neurons and otherneurotransmitters (Saper et al., 2001; reviewed inEspaña and Scammell, 2011).
Other cholinergic nuclei that are active during REMsleep and wakefulness include the basal forebrain andthe lateral hypothalamus; these same nuclei areinhibited during NREM sleep.
The manner in which the brain alternates cycles ofNREM and REM remains unknown, although someresearchers have proposed the existence of a mutuallyinhibitory circuit between vlPAG/LPT and the SDL.
Drugs for Insomnia beyond Benzodiazepines 207

Figure 1 is a schematic representation of nuclei impor-tant during sleep, illustrating the circuits that modu-late the sleep/wake cycle and their respective receptors.
IV. Melatonergic Drugs
A. Agomelatine
1. Mechanism of Action. Similar to melatonin,agomelatine inhibits firing activity in the SCN, likelythrough its full agonist activity at MT1; it is also anagonist at the MT2 receptor (McAllister-Williams et al.,2010). Agomelatine has low affinity for the 5-HT1A and5-HT2B receptors, and its effects are thought to bemediated by its antagonism of the 5-HT2C receptor,with a pKi of 6.2 at human receptors (Millan et al.,2003). In animals, chronic administration of agomela-tine produces a dose-dependent increase in dopamineand norepinephrine levels in the frontal cortex, withoutan effect on serotonin (European Medicines Agency,
2008a); like many other antidepressants, agomelatineadministration is associated with increased expressionof brain-derived neurotrophic factormRNA and enhancedneurogenesis in the hippocampus (Banasr et al., 2006). Inone study, agomelatine given at the onset of the late phaseinduced no changes in rat polygraphic recordings. How-ever, when it was administered shortly before dark phase,agomelatine (10 and 40 mg/kg) enhanced the duration ofREM and SWS sleep and decreased the duration of thewake state for 3hours (Descamps et al., 2009). A summaryof the pharmacological targets of agomelatine is reportedin Table 1.
2. Pharmacokinetics. Agomelatine is rapidly andwell-absorbed following oral administration (.80%)(EuropeanMedicines Agency, 2016). However, absolutebioavailability is low and variation between individualsis substantial, with increased bioavailability in womencompared with men. Elderly people likewise experiencegreater exposure to the drug, with AUC and Cmax 4- and
Fig. 1. Brain areas involved in the regulation of sleep and wakefulness with their respective receptors. Top left, green: When the brain enters NREM,neurons of the arousal system decrease their firing activity. This includes the serotonin neurons of the dorsal raphe (DR), the dopaminergic neurons ofthe ventral tegmental area (VTA), and the noradrenergic neurons of the locus coeruleus (LC). These neurons are silent during REM. OX1- and OX2-containing orexinergic neurons of the lateral hypothalamus decrease their firing activity during NREM and REM. The histaminergic H1-containingneurons of the tuberomammillary nucleus (TMN) decrease their firing activity during sleep. During wakefulness, these arousal centers each sendwidespread ascending projections to the cerebral cortex, stimulating cortical desynchronization with high-frequency gamma and low-frequency thetarhythmic activity. Bottom left, black: The receptors likely responsible for the switch from wakefulness to NREM sleep are MT1 and MT2 receptorsexpressed in suprachiasmatic neurons, which receive inputs directly from the retinohypothalamic tract (RHT), influenced by light and external stimuli.The transition from NREM and REM is controlled by the ventrolateral periaqueductal gray area (vlPAG), containing melatonin MT2 receptors, GABA,and glutamate receptors. Top right, red: During NREM sleep, two nuclei are particularly active: the reticular thalamus (RT), containing melatonin MT2and GABA receptors, which is responsible for thalamocortical input to the prefrontal cortex (showing synchronized activity during NREM), and theventrolateral preoptic area (vlPAG), containing GABA and galanin receptors, which inhibits noradrenergic, serotonergic, cholinergic, histaminergic,and hypocretinergic neurons. These nuclei play a role in the “reciprocal inhibitory” model of the sleep-wake switch. Bottom right, blue: The vlPAG is aputative “REM ON” nucleus, switching the brain to the REM sleep mode. During REM, the sublateral nucleus (SLD), the basal forebrain (BF), and thelateral tegmentum/ pedunculopontine tegmentum (LDT/PPT, rich in acetylcholine receptors) and the ventromedial medulla (VM) neurons becomeparticularly active. Note that the basal forebrain is active in REM and wakefulness and inhibited during NREM.
208 Atkin et al.

13-fold higher for patients $75 years old compared withpatients ,75 years old (European Medicines Agency,2016). Smoking, oral contraceptive pills, and the presenceof hepatic impairment likewise significantly affect ago-melatine’s pharmacokinetics. The metabolism of agome-latine occurs mainly via hepatic CYP1A2, and CYP1A2polymorphisms have been shown to significantly affectthe pharmacokinetics the drug (Song et al., 2014).3. Indications. Agomelatine is approved for use in
the European Union and Canada for the treatment ofmajor depressive disorder (MDD) but not approved inthe United States (Sansone and Sansone, 2011). Clin-ical studies examining the hypnotic effects of agomela-tine are detailed in Table 3.4. Results in Insomnia Disorder. No studies of ago-
melatine as a treatment of insomnia disorder were found.5. Other Results. The studies of agomelatine were
conducted in people diagnosed with major depressivedisorder. In a 6-week randomized, double-blinded com-parison study (N = 332) in people diagnosed with majordepressive disorder (Kasper et al., 2010), agomelatinewas significantly superior to sertraline at improvingsleep latency (P , 0.001) and sleep efficiency (P ,0.001); furthermore, symptoms of depression (P, 0.05)and anxiety (P, 0.05) improved significantlymore withagomelatine than with sertraline. Another randomized,double-blinded study comparing agomelatine and esci-talopram (N = 138) found that agomelatine resulted in agreater reduction in sleep latency than escitalopram fromweek 2 onward (Quera-Salva et al., 2011). Moreover,although escitalopram reduced the number of sleep cyclesrelative to baseline, agomelatine preserved the number ofsleep cycles. Finally, a review that pooled the results fromthree randomized studies (N=721) comparingagomelatineto SSRIs or venlafaxine (Quera-Salva et al., 2010) estab-lished that agomelatine increases SWS, improves sleepefficiency, and resynchronizesSWSto the first sleep cycle ofthe night in patients with major depressive disorder whilenot changing the amount or latency of REM sleep.6. Conclusion. A summary of the effects of agomelatine
on sleep architecture is presented in Table 2. There is goodevidence that agomelatine is superior to other antidepres-sants at reducing sleep latency in patients with majordepressive disorder based on one review and two random-ized, double-blind comparison studies (Kasper et al., 2010;Quera-Salva et al., 2010, 2011).Based on these samestudies,the evidence is weak for the use of agomelatine in insomnia.
B. Prolonged-Release Melatonin
1. Indications. Melatonin is FDA-approved as adietary supplement with no dosage restriction. InEurope, prolonged-release melatonin 2 mg/day is ap-proved for the treatment of insomnia in elderly patients.PRM is a new option in the treatment arsenal for
insomnia. It is targeted specifically toward older adults,potentially because endogenous melatonin productiondeclineswith age and PRMmimics the pharmacokinetics
of endogenous melatonin (Lemoine and Zisapel, 2012).However, a 3-week RCT found that the effects of PRM inpatients with low endogenous melatonin among all agesdid not differ fromplacebo (Wade et al., 2010); in contrast,PRM significantly reduced sleep latency compared withthe placebo in elderly patients irrespective of melatoninlevels (219.1 vs.21.7minutes). This finding supports theidea that PRM has targeted efficacy specifically amongthe elderly, the same group of patients for whombenzodiazepine treatment is discouraged due to theincreased risk of falls, accidents, and cognitive impair-ment (“What’s Wrong,” 2004). Clinical studies examiningthe hypnotic effects of PRM are detailed in Table 4.
2. Pharmacokinetics. Absorption of orally ingestedmelatonin is complete in healthy adults, although itmay be decreased by up to 50% in the elderly (EuropeanMedicines Agency, 2017). Melatonin has linear phar-macokinetics over the dosage range of 2–8 mg, althoughbioavailability is only about 15%, and the rate ofprolonged-release melatonin absorption is affected byfood: the presence of food delayed the absorption ofprolonged-release melatonin, resulting in a later andlower peak plasma concentration in the fed state. Themetabolism of melatonin is mainly mediated by CYP1Aenzymes, although exogenous administration of melato-nin does not induce these enzymes, even at suprather-apeutic dosages (European Medicines Agency, 2017).
3. Results in Insomnia Disorder. Four RCTs andone open-label trial found PRM effective in the treat-ment of primary insomnia in the elderly. Only one RCT,the largest one (N = 791), included patients below55 years of age; this study demonstrated that PRMwas only effective in the subgroup of patients over55 years old, validating its specific efficacy among theelderly but not other groups (Wade et al., 2010). Amongthe elderly in this study, PRM reduced subjective sleeplatency compared with baseline by 219.1 versus 21.7 minutes for placebo.
4. Other Results. One RCT (N = 80) in patients withmild to moderate Alzheimer’s disease with and withoutinsomnia comorbidity found that patients treated withPRM had significantly superior cognitive performanceduring the trial; in contrast, PSQI scores did notsignificantly change in the study, although sleep effi-ciency was found significantly to improve in patientswith and without comorbid insomnia (Wade et al., 2014).
5. Conclusion. A summary of the effects of PRM onsleep architecture is presented in Table 2. There is goodevidence that PRM is effective in the treatment ofinsomnia disorder in adults over 55 years of age, basedon four RCTs. There is also evidence that PRM is noteffective in the treatment of primary insomnia inyounger adults, based on one RCT (Wade et al., 2010).
C. Ramelteon
1. Mechanism of Action. Ramelteon is a potent andhighly selective agonist at the MT1 and MT2 receptors
Drugs for Insomnia beyond Benzodiazepines 209

TABLE
3Sum
maryof
stud
iesas
sessingtheeffectsof
agom
elatine(A
GM)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Kas
peret
al.(201
0)18
–60
Major
depr
essive
disord
er6-wkrand
omized
,do
uble-blind
compa
risonstud
yof
AGM
25-50mg/da
yvs.sertraline
50–10
0mg/da
y.N
=33
2.
AGM
was
sign
ifican
tlysu
perior
tosertraline
from
week1to
week
6by
impr
ovem
entin
SOL,
P,
0.00
1,an
dim
prov
emen
tin
SE,P
,0.00
1.Dep
ressivean
dan
xietysymptom
salso
impr
oved
morewithAGM
than
sertraline
.
Incide
nceof
trea
tmen
t-em
erge
ncyad
verseev
ents
(AEs)
was
48.0%
forAGM
and49
.1%
forsertraline
.Mostcommon
repo
rted
AEs
inboth
grou
pswerehe
adache
,drymou
th,a
nddiarrhea.
Fatigue
morecommon
inAGM
grou
pan
dhy
perhyd
rosismore
common
insertralin
egrou
p.
AGM
iseffectiveat
redu
cing
symptom
sof
insomniain
depr
essed
patien
tsan
dsign
ifican
tly
supe
rior
tosertraline
.
Que
ra-Salva
etal.(20
10)
NS
Major
depr
essive
disord
erRev
iew
withpo
oled
analysis
ofthreerand
omized
stud
iesat
end-po
intor
after6or
8wk
oftrea
tmen
twithAGM
25/50mg/da
yvs.SSRIs
orve
nlafax
ine.
N=72
1.
HAM-D
Item
4,ea
rlyinsomnia:
AGM
25/50mg/da
yredu
ced
scorefrom
1.46
0.7to
0.56
0.7
aten
dpoint
vs.placeb
oredu
ced
scorefrom
1.46
0.7to
0.76
0.8,
P,
0.00
1.For
HAM-D
Item
4,middleinsomnia:
compa
rison
betw
eenplaceb
oan
dAGM
yielde
dP
=0.01
5.For
HAM-D
Item
5,late
insomnia:
compa
risonbe
tweenplaceb
oan
dAGM
yielde
dP
=0.00
6.
Not
analyz
ed.
AGM
iseffectiveat
redu
cing
symptom
sof
insomniain
depr
essed
patien
tsan
dsu
perior
toothe
ran
tide
pressa
nts.
Que
ra-Salva
etal.(20
11)
19–60
Major
depr
essive
disord
er6-wkwithop
tion
al18
-wk
extens
ionpe
riod
rando
mized
,do
uble-blind
compa
risonstud
yof
AGM
25–50
mg/da
yvs.escitalop
ram
10–20
mg/da
y.N
=13
8.
AGM
sign
ifican
tlyredu
cedSOL
from
week2on
wards
compa
red
withescitalopr
am:estimated
differen
ce(m
inute)
atweek
2was
219
[ 230
,29],P
,0.00
1;at
week6was
214
[224
,25],
P=0.01
3;at
wee
k24
was
218
[233
,23],P
,0.00
01.T
STwas
increa
sedwithAGM
but
decrea
sedwithescitalopr
amrelative
toba
seline
.SE
was
stab
lewithAGM
butde
crea
sed
withescitalopr
am.Num
berof
sleepcycles
was
stab
lewith
AGM
butde
crea
sedwith
escitalopr
am.
Withd
rawalsdu
eto
AEswere
less
freque
ntwithag
omelatine
(3%)than
escitalopram
(8%).
Proportionof
patie
ntsreporting
atleaston
eAE
was
lower
with
agom
elatinethan
escitalopram
(66%
vs.8
2%,P
=0.03
8).
Hea
dache,
nasoph
aryn
gitis,
andna
usea
werethemost
common
AEsin
both
grou
ps.
AGM
iseffectiveat
redu
cing
symptom
sof
insomniain
depr
essed
patien
tsan
dsu
perior
toescitalopr
am.
210 Atkin et al.

TABLE
4Sum
maryof
studies
assessingtheeffectsof
thepr
olon
ged-releas
emelaton
inform
ulation(PRM)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Arbon
etal.(201
5)55
–64
Hea
lthypa
rticipan
tsDou
ble-blind,
placeb
o-controlle
d,four-w
aycrossovertrial.PRM
2mgvs.tem
azep
am20
mgvs.
zolpidem
(10mg)
vs.p
lacebo
.N
=16
PRM
hasminor
effectson
stag
eN3in
compa
risonwiththose
oftemaz
epam
andzolpidem
.
10ad
verseev
ents
ofmild
intensity
dueto
PRM.The
mostcommon
repo
rted
were
gastrointestinal
disord
ers
(con
stipation,
drymou
th,
flatulence,
andna
usea
),ne
rvou
ssystem
disorders
(balan
cedisorder,som
nolence,
andhe
adache
),an
dgene
ral
disorders(fa
tigu
ean
dfeeling
hot).
PRM
does
notsign
ifican
tly
affect
sleeppa
rameters
inelde
rly.
Dolev
(201
1)See
Mirtaza
pinesection
Lem
oine
etal.(20
07)
55+
Primaryinsomnia
2-wksing
le-blind
placeb
oru
n-in
period
follow
edby
a3-wkRCTtrea
tmen
tpe
riod
.PRM
2mg/da
yvs.placeb
o.N
=17
0.
PRM
impr
oved
QOSmea
sured
byLSEQ
(222
.5vs.216
.5,
P=0.04
7).
Ninepa
tien
tsin
each
trea
tmen
tgrou
prepo
rted
AEs.The
most
common
repo
rted
AEswere
mild
.Diarrhe
aoccurred
inon
epa
tien
treceivingPRM
and
onepa
tien
treceivingplacebo.
PRM
iseffectiveat
redu
cing
symptom
sof
insomniain
theelde
rly.
Lem
oine
etal.(20
11)
20–80
Primaryinsomnia
6–12
moop
en-lab
elcontinua
tion
trial.PRM
2mg/da
y.N
=24
4.
Themea
n(+S.E.M
.)pe
rcen
tage
ofnigh
tspe
rweekscored
bythepa
tien
tsas
“good”
or“very
good
”increa
sedprogressively
withtrea
tmen
tdu
ration
.At
theplatea
ulevel,54
%–56
%of
nigh
tspe
rweekwerescored
as“good”
or“verygood
”(i.e.,
3.8nigh
ts/wk)
compa
redwith
26%
(i.e.,1
.8nigh
ts/wk)
atba
selin
e(P
,0.00
1),w
hich
was
maintaine
dthroug
hout
trial.
PRM
discon
tinu
ationev
enafter12
mowas
not
associated
withAEs,
withd
rawal
symptom
s,or
supp
ressionof
endo
geno
usmelaton
inpr
oduc
tion
.Most
common
repo
rted
even
tswereph
aryn
gitis(12.4%
)an
dba
ckpa
in(11.8%
).
PRM
iseffectiveat
redu
cing
symptom
sof
insomnia
aslong
-term
trea
tmen
t.
Lem
oinean
dZisa
pel(201
2)55
+Primaryinsomnia
Postho
can
alysis
ofpo
oled
antihy
perten
sive
drug
-trea
tedsu
bpop
ulations
from
four
rand
omized
,do
uble-
blindtrials
ofPRM
and
placeb
ofor3wk.
N=58
9.
Bytheen
dof
the6-mo
trea
tmen
tpe
riod
,mea
nssu
bjective
impr
ovem
entin
patien
ts’ev
aluated
SOL
was
sign
ifican
tlyhigh
erwith
PRM
(25.89
minutes)
than
withplaceb
o(7.54minutes)
P=0.02
.
Rateof
AEsnormalized
per
100pa
tien
t-wee
kswas
lower
forPRM
(3.66)
than
for
placeb
o(8.53).
PRM
isefficaciou
san
dsa
fein
prim
aryinsomnia
patien
tstrea
tedwith
antihyp
ertensive
drugs
Luthringe
ret
al.(20
09)
55+
Primaryinsomnia
2-wksing
le-blind
placeb
oru
n-in
follow
edby
3-wkRCT
ofPRM
2mg/da
yfor3wk
follow
edby
a3-wk
withd
rawal
period
.N
=40
PRM
grou
phad
sign
ifican
tly
shorterSOL(9
min;P
=0.02
)compa
redwiththeplaceb
ogrou
pan
dscored
sign
ificantly
better
intheCriticalFlicke
rFusionTest(P=0.00
8)witho
utne
gatively
affectingsleep
structurean
darchitecture.
Halfof
thepa
tien
tsreported
substantialim
provem
entin
QOSat
homewithPRM
compa
redwith15
%with
placebo(P
=0.01
8).N
oreboun
deffectswereobserved
during
withd
rawal
AEswerereported
by11
patien
tsin
each
treatm
entgrou
p.The
mostcom
mon
AEwas
headache,
repo
rted
byfour
patien
tsin
thePRM
grou
pan
dthreein
theplaceb
ogrou
p.No
sign
ificant
diffe
rencein
the
incide
nceof
AEs.
PRM
was
effectivein
redu
cing
symptom
sof
insomnia.
(con
tinued
)
Drugs for Insomnia beyond Benzodiazepines 211

TABLE
4—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Otm
aniet
al.(200
8)55
+Hea
lthy
participan
tsRCT
crossove
rstud
y.PRM
2mg,
zolpidem
10mg,
PRM
+zolpidem
vs.placeb
o.Effects
onps
ycho
motor
func
tion
s,mem
oryrecall,
anddr
ivingsk
ills
were
assessed
at1,
4han
dmorning
follow
ing
administration.
N=16
.
Amain‘‘treatmen
t’’effect
was
foun
dforallva
riab
les(P
,0.05
)Zo
lpidem
sign
ifican
tly
increa
sedseda
tion
compa
red
withplaceb
oat
1hou
r(P
=0.00
11,P,
0.00
01,
resp
ective
ly)an
d4hou
rspo
stdo
sing
(P,
0.00
01for
both)an
dcompa
redwith
PRM
at1hou
r(P
=0.03
,P,
0.00
01,respe
ctively)
and
4hou
r(P
=0.01
5forbo
th).
N/A
PRM
does
not
hav
esign
ifican
tcogn
itive
adve
rseeffectsin
the
elde
rly.
Wad
eet
al.(20
07)
55–80
Primaryinsomnia
2-wksing
le-blind
placeb
oru
n-in
period
follow
edby
a3-wkRCTtrea
tmen
tpe
riod
.PRM
2mg/da
yvs.placeb
o.N
=35
4.
PRM
impr
oved
qualityof
sleep
mea
suredby
LSEQ
(222
.5vs.216
.5,P
=0.04
7).
24%
and21
%of
patien
tsin
the
resp
ective
PRM
andplaceb
ogrou
psrepo
rted
AEs.
Most
common
lyrepo
rted
effects
werenas
opharyn
gitisan
dhe
adache
ormigraine.
PRM
iseffectiveat
redu
cing
symptom
sof
insomniain
theelde
rly.
Wad
eet
al.(20
10)
18–80
Primaryinsomnia
2-wksing
le-blind
placeb
oru
n-in
period
follow
edby
3-wkRCTof
PRM
2mg/da
yvs.placeb
o;26
-wkex
tens
ion
stud
ywith2wkof
sing
le-
blindplaceb
oru
n-ou
t.N
=79
1
PRM
inpa
tien
tswithlow
endo
geno
usmelaton
inrega
rdless
ofag
edidnot
impr
oveSOL
compa
red
withplaceb
o,whe
reas
PRM
sign
ifican
tlyredu
cedSOL
compa
redwithplaceb
oin
elde
rlypa
tien
tsrega
rdless
ofmelaton
inleve
ls(2
19.1
vs.21.7min;P
=0.00
2).
AE
ratesweresimilar
betw
een
PRM
andplaceb
ogrou
ps.
34.5%
and35
.9%
ofresp
ective
PRM-an
dplaceb
o-trea
tedpa
tien
tsrepo
rted
anyAE
duringthe
trea
tmen
tpe
riod
.In
extens
ionpe
riod
,73
.8%
and
76.8%
ofPRM-an
dplaceb
o-trea
tedsu
bjects
repo
rted
any
AE.Mostcommon
even
tswerenas
opharyn
gitis,
arthralgia,diarrh
ea,
resp
iratorytractinfections
,an
dhea
dach
e.
PRM
iseffectiveat
redu
cing
symptom
sof
insomniain
theelde
rly.
The
resu
lts
demon
strate
short-
and
long
-term
efficacy
and
safety
ofPRM
inelde
rly
insomniapa
tien
ts.Low
melaton
inpr
oduc
tion
rega
rdless
ofag
eis
not
useful
inpr
edicting
resp
onsesto
melaton
intherap
yin
insomnia.
Wad
eet
al.(20
14)
52–85
Mildto
mod
erate
Alzheimer’s
diseas
e,withan
dwithou
tinsomnia
comorbidity
2-wksing
le-blin
dplaceb
orun-in
follo
wed
by24
-wkRCTan
d2-wkplaceb
orun-ou
tpe
riod
.PRM
2mg/da
yvs.p
lacebo
.N
=80
.
Patientstrea
tedwithPRM
(24wk)
hadsign
ifican
tly
better
cogn
itivepe
rforman
cethan
thosetrea
tedwith
placeb
o,as
mea
suredby
the
IADL(P
=0.00
4)an
dMMSE
(P=0.04
4).M
eanADAS-C
ogdidnot
differ
betw
eenthe
grou
ps.ThePSQIglob
alscoreim
prov
edin
PRM
(21.62
[2.74],P
=0.00
4)bu
tno
tplaceb
ogrou
p(0.74
[2.52],P
=0.13
9)
AE
ratesweresimilar
betw
een
PRM
andplaceb
ogrou
ps.
82.1%
ofPRM
patien
tsrepo
rted
AEsvs.67
.6%
ofplaceb
o-trea
tedpa
tien
ts.
Add
-onPRM
has
positive
effectson
cogn
itive
func
tion
ingan
dsleep
maintenan
cein
AD
patien
tscompa
redwith
placeb
o,pa
rticularly
inthosewithinsomnia
comorbidity.
212 Atkin et al.

with an affinity 3–16 times higher than that of melato-nin (Kato et al., 2005). Its affinity for MT2 is eight timeslower than its affinity for MT1. This binding profiledistinguishes ramelteon from melatonin and tasimel-teon, which both display more affinity for the MT1
receptor than the MT2 receptor (Lavedan et al., 2015).The hypnotic effect of ramelteon is mediated by itspotent, long-lasting agonism of themelatonin receptors,because it does not exhibit affinity for benzodiazepinereceptors, dopamine receptors, opiate receptors, ionchannels, and does not affect the activity of variousenzymes (Kato et al., 2005) (Table 1). While studies inrats and monkeys confirm that ramelteon reduces timeto sleep onset without affecting total sleep time(Yukuhiro et al., 2004; Fisher et al., 2008), ramelteonincreases total sleep time in cats (Miyamoto et al., 2004).2. Indications. Ramelteon is FDA-approved for the
treatment of insomnia characterized by difficulty withsleep onset (US FDA, 2010a). Notably, the EuropeanMedicines Agency initially rejected Takeda Pharma-ceutical Company’s application (filed inMarch 2007) forlack of efficacy. Later, in September 2008, the companywithdrew their Marketing Authorization Application tothe Committee for Medicinal Products for Human Use(CHMP). The CHMP was concerned that the companyhad not demonstrated the effectiveness of ramelteon,because only one aspect of insomnia, the time to fallasleep, had been assessed in the trials (EuropeanMedicines Agency, 2008b). Furthermore, only one ofthe three studies that had been carried out in thenatural setting found a significant difference in thetime taken to fall asleep between patients takingramelteon and those taking placebo, and this differencewas considered too small to be clinically relevant. Whenother aspects of sleep were considered, ramelteon didnot have any effect (Kuriyama et al., 2014). The CHMPwas also concerned that Takeda had not demonstratedthe long-term effectiveness of ramelteon (EuropeanMedicines Agency, 2008b). Clinical studies examiningthe hypnotic effects of ramelteon are detailed in Table 5.3. Pharmacokinetics. At a dose range of 4–64 mg,
ramelteon undergoes rapid, high first-pass metabolismand exhibits linear pharmacokinetics (US FDA, 2010a).However, the drug shows substantial intersubject var-iability inmaximal serum concentration and area underthe concentration curve. Median peak concentrationoccurs at about 0.75 hours after fasted oral administra-tion. Although total absorption is at least 84%, absolutebioavailability is only 1.8% because of extensive first-pass metabolism (US FDA, 2010a). It has a half-life ofabout 1–2.6 hours. CYP1A2 is the major liver enzymeinvolved in the hepatic metabolism of ramelteon, al-thoughCYP2C andCYP3A4 are also involved to a lesserdegree: the drug is extensively transformed to itshydroxylated M-II metabolite, with serum AUC valuesthat average approximately 30 times those of the parentdrug (Greenblatt et al., 2007). It has been argued that
M-II, with its longer half-life and greater systemicexposure, may contribute significantly to the hypnoticeffect of ramelteon: M-II has been shown to bind tohuman MT1 and MT2 receptors, although with loweraffinity (Ki: 114 and 566 pmol/l for MT1 and MT2,respectively) (Nishiyama et al., 2014). Taking ramelteonwith a high-fat meal changes its pharmacokinetics; thearea under the concentration curve for a single 16mgdoseis 31% higher, whereas maximal concentration is 22%lower than when administered in a fasted state (US FDA,2010b). For this reason, the US FDA does not recommendtaking ramelteon after a high-fat meal. Moreover, clear-ance is significantly reduced in the elderly,
4. Results in Insomnia Disorder. Two meta-analyses found ramelteon effective at reducing sub-jective sleep latency time in primary insomnia (Liu andWang, 2012; Kuriyama et al., 2014). The first studyanalyzed 4055 patients (Liu and Wang, 2012) and thesecond analyzed 5812 patients (Kuriyama et al., 2014).One, a pooled analysis of four trials comparing ramel-teon to placebo, found that active treatment reducedsubjective sleep latency by 24.22 minutes, 95% confi-dence interval 25.66 to 22.77 minutes (P , 0.00001)(Liu and Wang, 2012). The other had similar results forsubjective sleep latency reduction, although it pooledresults from 12 studies:24.30 minutes, 95% confidenceinterval 27.01 to 21.58 minutes (Q = 23.64; df = 11)(Kuriyama et al., 2014). However, it did not find thatramelteon increased total sleep time significantly morethan placebo (Kuriyama et al., 2014).
5. Conclusion. A summary of the effects of ramel-teon on sleep architecture is presented in Table 2. Thereis strong evidence that ramelteon is effective in thetreatment of insomnia disorder characterized by diffi-culty with sleep onset, based on two meta-analyses (Liuand Wang, 2012; Kuriyama et al., 2014).
D. Tasimelteon
1. Mechanism of Action. Tasimelteon displays com-parable potency to melatonin at the MT1 receptor,whereas its affinity for MT2 is 2.1–4.4 times greater thanits affinity for MT1 (Lavedan et al., 2015). Its agonism atthese receptors is selective, as it lacks any other signif-icant interactions with receptors or enzymes (Table 1).
2. Indications. Tasimelteon is the first FDA-approved treatment of non-24-hour sleep-wake disorder(non-24), for which it was granted orphan drug status.Initially, Vanda Pharmaceuticals evaluated the efficacyof tasimelteon in the treatment of insomnia in phase IIand phase III studies (Vanda Pharmaceuticals Inc.,2008; Feeney et al., 2009), but the compound has onlyreceived regulatory approval for the treatment of non-24. Clinical studies examining the hypnotic effects oframelteon are detailed in Table 6.
3. Pharmacokinetics. The pharmacokinetics of tasi-melteon is linear over dose ranges from3 to 300mg,with anabsolute oral bioavailability of 38.3%and amean half-life of
Drugs for Insomnia beyond Benzodiazepines 213

TABLE
5Sum
maryof
stud
iesas
sessingtheeffectsof
ramelteon
(RMT)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Erm
anet
al.
(200
6)18
–64
Chronicpr
imary
insomnia
Five-pe
riod
crossove
rRCT.RMT
4vs.8vs.
16vs.32
mg/da
yvs.
placeb
o.N
=10
7.
PSG
LPS(m
inute)was
37.7
for
placeb
ovs.24
.0forRMT
4mg/
day,
P,
0.00
1,vs.2
4.3forRMT
8mg/da
y,P,
0.00
1,vs.2
4.0for
RMT
16mg/da
y,P
,0.00
1,vs.
22.9
forRMT
32mg/da
y,P
,0.00
1.P
,0.00
1forov
erall
effect.
Nodifferen
cein
numbe
ror
type
ofAEsbe
tweenactive
trea
tmen
tan
dplaceb
ogrou
p.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia.
Goone
ratne
etal.(20
10)
#60
Obs
tructivesleep
apnea
4-wkRCT.RMT
8mg/
dayvs.placeb
o.N
=21
.
Objective
polysomno
grap
hicSOL
(minute)
was
20.4
623
.2at
baselinein
theRMT
grou
pan
d9.76
10.3
aftertrea
tmen
t.In
theplaceb
ogrou
p,ob
jectiveSOL
was
16.6
617
.5at
baseline
and
34.4
630
.7aftertrea
tmen
t.For
betw
eengrou
pscompa
rison:
P=0.00
8.Subjective
SOL
was
notsign
ifican
tlyim
prov
ed.
Fou
rAEsoccu
rred
inRMT
arm
andtw
oin
placeb
oarm;n
onejudg
edrelatedto
trea
tmen
t.
RMTmay
beeffectiveat
redu
cingsymptom
sof
insomniain
olde
rad
ults.
Koh
saka
etal.
(201
1)20
–65
Chr
onic
prim
ary
insomnia
Crossov
erRCT(five
period
sof
2nigh
tsea
ch).RMT4vs.8
vs.
16vs.32
mg/da
yvs.
placeb
o.N
=65
.
LPS(m
inute)was
29.026
28.55
forRMT
4mg/da
y,22
.126
18.16forRMT
8mg/da
y,28
.17
629
.40forRMT
16mg/da
y,24
.376
32.79forRMT
32mg/
day,
and35
.276
40.68for
placeb
o.Differenc
esbe
tween
trea
tmen
tan
dplaceb
owereon
lysign
ifican
tforRMT8an
d32
mg/
day.
How
ever,the
line
arPva
lue
tren
dwas
:P
=0.00
46.
The
numbe
rof
patien
tswith
anAE
was
higher
inthe
16an
d32
mg/da
ythan
withplaceb
oan
dthe4an
d8mg/da
ydo
ses.
The
most
common
AEswere
somno
lenc
e,he
adache
,malaise,an
ddizziness.
RMT
8an
d32
mg/da
yareeffectiveat
redu
cingsymptom
sof
insomnia.
Kur
iyam
aet
al.
(201
4)18
–93
Chr
onic,pr
imary,
orps
ycho
physiological
insomnia;bipo
lar
disord
er;insomnia
associated
with
obstru
ctivesleep
apnea
Systematic
review
and
meta-an
alysis
ofplaceb
o-controlled
RCTs.
N=58
12.
RMT
was
sign
ifican
tlyas
sociated
withredu
cedsu
bjective
SOL
andim
prov
edQOS.It
was
not
associated
withincrea
sed
subjective
totalsleeptime.
Only
sign
ifican
tAE
was
somno
lenc
e.Nodifferen
cein
occu
rren
ceof
othe
rAEs
betw
eenRMTan
dplaceb
o.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia.
Liu
andWan
g(201
2)18
andov
erDSM-IV
prim
ary
chronic
insomnia
Systematic
review
and
meta-an
alysis
ofplaceb
o-controlled
RCTs.
N=40
55
Significant
impr
ovem
ents
inself-
repo
rted
andpo
lysomno
grap
hic
SOL,T
ST,latency
toREM.No
impr
ovem
entin
percen
tage
ofREM.
RMTwas
not
associated
with
ahighrisk
ratioof
any
freq
uent
AEscompa
red
withplaceb
o.How
ever,
thereweresign
ifican
tly
moresu
bjective
repo
rtsof
atleas
ton
eAE
withRMT.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia.
May
eret
al.
(200
9)18
–79
Chr
onic
prim
ary
insomnia
6-moRCT.RMT
8mg/
dayvs.placeb
o.N
=45
1.
RMT
cons
istently
redu
cedLPS
compa
redwithba
seline
and
compa
redwithplaceb
oas
mea
suredby
objective
polysomno
grap
hy.R
MTredu
ced
LPS(m
inute)
from
70.75at
baseline
to32
.02at
week1.
Sim
ilar
effectswereob
served
atea
chfollow
up.
Incide
nceof
AEswas
similar
betw
eenRMT
(51.8%
)an
dplaceb
o(50.7%
)grou
ps.
Eightpa
tien
tsin
RMTan
d10
patien
tsin
placeb
odiscon
tinued
dueto
anAE.
Leu
kope
niaoccu
rred
inon
eRMT-treated
subject
andwas
judg
edas
possibly
trea
tmen
trelated.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia
over
the
cour
seof
6mo. (con
tinued
)
214 Atkin et al.

TABLE
5—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
McE
lroy
etal.
(201
1)18
–65
Bipolar
Idisord
er8-wkRCT.8mg/da
yRMT
vs.placeb
o.N
=21
.
RMTan
dplaceb
oan
dsimilar
rates
ofredu
ctionin
symptom
sof
insomnia,
man
ia,an
dglob
alseve
rity
ofillness.
RMT
was
associated
withim
prov
edde
pressive
symptom
s.Pittsbu
rghIn
somniaRating
Scale
totalscoredifferen
cefrom
baseline
tofina
lvisit:placeb
o,269
.3vs.R
MT,2
54.2,P
=0.46
.
Onepa
tien
tof
21whowere
rando
mized
withdr
ewdu
eto
seda
tion
(RMT
grou
p).
Nopa
rticipan
tex
perien
ced
aseriou
sAE.S
malls
ample
size
limitsab
ilityto
detect
mea
ning
fuldifferen
cesin
theoccu
rren
ceof
AEs.
RMT
may
not
beeffectiveat
redu
cing
symptom
sof
insomniain
bipo
larI
disord
er.
NCT#0
0755
495
18–80
Primaryinsomnia
byDSM-IV-TR
5-wkRCT.RMT
8mg/
day+do
xepin3mg/
dayvs.R
MT8mg/da
yvs.do
xepin3mg/da
yvs.placeb
o.N
=47
2.
RMT8mg/da
y+do
xepin3mg/da
ywas
sign
ifican
tlysu
perior
toplaceb
oat
redu
cingLPSat
wee
k1,
P,
0.00
1.How
ever,at
week
3,P
=0.40
0,an
dat
wee
k5,
P=
0.12
2.RMT
8mg/da
y+do
xepin
3mg/dwas
sign
ifican
tly
supe
rior
toplaceb
oat
increa
sing
TSTat
alltim
epo
ints:P
,0.00
1at
week1,
P=0.01
7at
week3,
and0.03
6an
dweek5.
The
ratesof
AEsweresimilar
amon
galltrea
tmen
tgrou
ps:28
.1%
ofRMT
+do
xepin,3
0.8%
fordo
xepin,
35.9%
forRMT,36
.6%
for
placeb
o.Mostrepo
rted
AEs
weresomnolen
ce(4.9%)
andhe
adache
(4.5%),with
somno
lenc
eoccu
rringwith
thegrea
test
incide
ncein
theRMT
+do
xepingrou
p(8.8%).
RMT
+do
xepinis
effectiveat
redu
cing
symptom
sof
insomnia.
Sub
jective
sleepqu
ality
impr
oved
morewith
RMT
+do
xepinthan
withRMT
alon
eov
er5wkof
trea
tmen
t.
Rothet
al.
(200
6)64
–93
Primaryinsomnia
35-nightRCT.RMT
4mg/da
yvs.8
mg/da
yvs.placeb
o.N
=82
9.
LPS(m
inute)at
wee
k1was
70.2
forRMT
4mg/da
yvs.78
.5min
forplaceb
o,P=0.00
8;it
was
70.2
forRMT
8mg/da
yvs.78
.5forplaceb
o,P=0.00
8.RMTalso
sign
ifican
tlyincrea
sedTST
and
rebo
undinsomnia
orwithdr
awal
effectswereno
tob
served
follow
ingdiscon
tinu
ation.
Incide
nceof
AEswas
similar
amon
galltrea
tmen
tgrou
ps.In
cide
nce
ofan
yAE:51
.5%
ofplaceb
ogrou
p,54
.8%
ofRMT4mg/
day,
58.0%
ofRMT
8mg/
day.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia.
Rothet
al.
(200
7)65
–83
Chr
onic
prim
ary
insomnia
9-wk,
three-pe
riod
crossove
rRCT
trial
withtrea
tmen
tad
ministeredfor
2nightspe
rtrea
tmen
t.RMT
4vs.
8mg/da
yvs.placeb
o.N
=10
0.
SOL
(minute)was
28.7
forRMT
4mg/da
yvs.38
.4forplaceb
o,P,
0.00
1;30
.8forRMT
8mg/
dayvs.38
.4forplaceb
o,P
=0.00
5.TST
andSE
werealso
sign
ifican
tlyim
prov
ed.
Incide
nceof
AEscons
idered
trea
tmen
t-relatedwas
placeb
o7%
,RMT4mg/da
y11
%,a
ndRMT
8mg/da
y5%
.Noev
iden
ceof
nex
t-da
yps
ycho
motor
orcogn
itiveeffects.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia.
Uch
imur
aet
al.
(201
1)Mea
n:4
8.8;
S.D
.:17
.2Chronic
insomnia
RCT.RMT
4vs.8mg/
dayvs.placeb
ofor
2wkfollow
edby
dose
escalation
to8vs.
16vs.4mg/da
y,resp
ective
ly,for
2wk.
N=11
43.
LSmea
nweeklysu
bjective
SOL
(minute)
atweek1:
RMT
4mg/
daywas
notsign
ifican
tly
supe
rior
toplaceb
o,P
=0.93
15.
RMT
8mg/da
ywas
not
sign
ifican
tlysu
perior
toplaceb
o,P=0.09
05.
42.1%
intheplaceb
o/4mg/
daygrou
p,42
.5%
inthe4/
8mg/da
ygrou
pan
d41
.8%
inthe8/16
mg/da
ygrou
prepo
rted
atleas
ton
etrea
tmen
t-em
erge
ntAE
Theincide
ncesof
AEs
amon
gthetrea
tmen
tgrou
pswerecompa
rable,
andnodo
se–resp
onse
relation
shipswere
observed
.
RMT
may
not
beeffectiveat
redu
cing
symptom
sof
insomnia.
(con
tinued
)
Drugs for Insomnia beyond Benzodiazepines 215

TABLE
5—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Uch
iyam
aet
al.
(201
1)20
–85
Chronic
insomnia
4-wkRCT.RMT
8mg/
dayvs.placeb
ofor
2wkfollow
edby
2-wk
placeb
oru
n-ou
tpe
riod
tomon
itor
rebo
undinsomnia.
N=98
7.
RMT
was
sign
ifican
tlysu
perior
toplaceb
oat
redu
cing
SOLat
week
1bu
tinsign
ifican
tlysu
perior
toplaceb
oat
week2.
LSmea
n(in
minute)
forRMT
was
61.156
0.97
atweek1vs.65
.696
0.97
forplaceb
o.
Noev
iden
ceof
rebo
und
insomnia.2.7%
ofRMT
grou
pan
d2.3%
ofplaceb
ogrou
pdiscon
tinued
dueto
AEs.
Themostcommon
reas
onin
both
grou
pswas
nas
opharyn
gitis.
One
seriou
sad
verseeffect
occu
rred
inRMT
grou
p,a
road
accide
nt.15
hafter
taking
drug
.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia
after1wkof
trea
tmen
t.
Wan
g-Weiga
nd
etal.(20
11)
18–64
Chronic
insomnia
3-wkRCT.RMT
8mg/
dayvs.placeb
o.N
=55
6.
For
mea
nsu
bjective
SOL
relative
toplaceb
o:week1-redu
ctionof
4.1min,P
=0.08
8.Week2:
redu
ctionof
2.8min,P
=0.25
8.Week3:
redu
ctionof
4.9min,P
=0.06
0.Nosign
ifican
tdifferen
cefrom
placeb
o.
Som
nolenc
eoccu
rred
in1.8%
ofplaceb
ogrou
pan
d4.4%
ofRMT
grou
p.The
prop
ortion
ofsu
bjects
with
anytrea
tmen
t-relatedAEs
was
similar
betw
een
grou
ps(placebo
15.4%,
ramelteon
16.5%).
RMT
8mg/da
ymay
not
beeffectiveat
redu
cingsymptom
sof
insomnia.
Zammit
etal.
(200
7)18
–64
Primaryinsomnia
5-wkRCT.RMT
8vs.
16mg/da
yvs.p
lacebo
.N
=40
5.
LPS(m
inute)at
wee
k1was
32.2
forRMT
8mg/da
yvs.28
.9for
RMT
16mg/da
yvs.47
.9for
placeb
o,P
,0.00
1;sign
ifican
tim
prov
emen
tsweremaintaine
dat
weeks
3an
d5.
Noev
iden
ceof
next-day
pharmacolog
icresidu
aleffects.
Noev
iden
ceof
rebo
undinsomnia
follow
ingdiscon
tinu
ation
ofRMT.Mostcommon
AE
inallg
roups
was
hea
dach
e.
RMT
iseffectiveat
redu
cingsymptom
sof
insomnia.
Zammit
etal.
(200
9)$65
Insomnia
Thr
ee-w
aycrossove
rRCT.RMT
8mg/da
yvs.zolpidem
10mg/
dayvs.placeb
o.N
=33
.
While
zolpidem
sign
ifican
tly
impa
ired
performan
ceon
the
sens
oryorga
niza
tion
test,turn
time,
andturn
sway
(P,
0.00
1forall),R
MT
didno
tpr
oduc
ean
ydifferen
cesfrom
placeb
o.Im
med
iate
recallde
clined
sign
ifican
tlywithzolpidem
(P=
0.00
2)while
itwas
similar
toplaceb
oforRMT.
N/A
RMT
didnot
impa
irmiddle-of-the
-night
balanc
e,mob
ility,
ormem
oryin
olde
rad
ults
relative
toplaceb
o
216 Atkin et al.

1.360.4hours (USFDA,2014b). Like for ramelteon, takingtasimelteon with a high-fat meal lowers Cmax (by 44%) anddelaysTmax (by 1.75 hours) compared with the fasted state.For this reason, the FDA recommends that the drug not betaken with food. CYP1A2 and CYP3A4 are the majorisoenzymes associated with its hepatic metabolism, andmajor metabolites have 13-fold or less activity at melatoninreceptors (US FDA, 2014b). Exposure to tasimelteonincreases approximately twofold in the elderly comparedwith nonelderly adults and in women approximately 20%–
30% compared withmen. Smokers had approximately 40%lower exposure to tasimelteon than nonsmokers.4. Results in Healthy Volunteers. Two short RCTs of
tasimelteon in healthy volunteers have been published: aphase II RCT and a phase III RCT (again in healthyvolunteers) of the drug as a treatment of transient in-somnia induced by shifted sleep (Rajaratnam et al., 2009).In the phase II trial, the individuals were monitored forseven nights: three at baseline, three after a 5-houradvance of the sleep-wake schedule, and one night aftertreatment. In the phase II RCT, tasimelteon reduced sleeplatency and increased sleep efficiency relative to placeboand shifted the plasma melatonin rhythm to an earlierhour. The phase III study had similar positive results.5. Results in Insomnia Disorder. There were no
published studies of tasimelteon in patients diagnosedwith insomnia disorder. However, one clinical trial inpatients with primary insomnia (NCT#00548340), whichwas published only as an abstract, found a significantmean change in latency to persistent sleep [standarderror]: 45.0 [2.965] for tasimelteon 20 mg/day versus 46.4[2.954] for tasimelteon 50 mg/day versus 28.3 [3.020] forplacebo (Vanda Pharmaceuticals Inc., 2014).6. Results in Other Conditions. Other trials were
conducted in patients diagnosed with non-24 sleep-wake disorder (Lockley et al., 2015), for which tasimel-teon has gained FDA approval as an orphan drug(Dhillon and Clarke, 2014). The investigators foundthat tasimelteon significantly improved entrainment.7. Conclusion. A summary of the effects of tasimel-
teon on sleep architecture is presented in Table 2. Thereis poor-quality evidence for the use of tasimelteon in thetreatment of insomnia disorder, based on two studies inhealthy volunteers (Rajaratnam et al., 2009).
V. Orexin Receptor Antagonist Drugs
A. Suvorexant
1. Mechanism of Action. Suvorexant’s effect as ahypnotic is attributable to its selective antagonism ofthe orexin receptors OX1R and OX2R (Winrow et al.,2011; Yin et al., 2016) (Table 1). In vitro assay panelsdemonstrate suvorexant’s selectivity for the orexinreceptors over 170 known receptors and enzymes (Coxet al., 2010). In mice, suvorexant has been shown toselectively increase REM sleep in the first 4 hours afterdosing (Hoyer et al., 2013).
2. Indications. Suvorexant is FDA approved for thetreatment of insomnia characterized by difficulty withsleep onset and/or sleep maintenance at the doses of 5,10, 15, and 20 mg/day but not the higher doses studiedin the clinical trials (US FDA, 2014a). The FDA chosenot to approve suvorexant at the 30 or 40 mg/day dosesstudied in the phase III trials because of safety concerns,particularly next-day driving impairment at doses of 20mg/d and higher (US FDA, 2014a). There were also a fewreports of sleep paralysis and hallucinations, unconsciousnighttime behaviors, and narcolepsy-like events amongdrug-treated subjects. Clinical studies examining thehypnotic effects of suvorexant are detailed in Table 7.
3. Pharmacokinetics. Exposure to suvorexantdoesnotincrease linearly over the dosage range 10–80 mg becausethe drug is absorbed less at higher doses (US FDA, 2014a).The mean bioavailability of suvorexant 10 mg is 82% andingestion of the drug with food does not meaningfully affectAUC or Cmax but does delay Tmax by approximately 1.5hours. Steady-state pharmacokinetics are achieved in3 days, and the mean half-life of the drug is 12 hours(95% confidence interval: 12–13). Exposure to suvorexant ishigher inwomen than inmen,withAUCincreased17%andCmax increased 9%, for suvorexant 40 mg.
4. Results in Insomnia Disorder. There are twosystematic reviews of suvorexant as a treatment ofprimary insomnia (Citrome, 2014; Kishi et al., 2015).Although both reviews analyze the same four phase IIand phase III trials in insomnia patients, one of themdiffers from the other by following PRISMA reportingguidelines (Kishi et al., 2015). Both systematic reviewsanalyzed the same four phase II and phase III RCTs andcame to similar conclusions: that suvorexant was safeand effective for the treatment of insomnia. Suvorexantimproved subjective total sleep time (weighted meandifference = 220.16, 95% confidence interval = 225.01to 215.30, 1889 patients, three trials) and subjectivetime to sleep onset (weighted mean difference = 27.62,95% confidence interval = 211.03 to 24.21, 1889 pa-tients, three trials) (Kishi et al., 2015).
Subgroup analysis of approved (15 and 20 mg/day)versus unapproved (30 or 40 mg/day) found that forefficacy, the number needed to treat values versusplacebo of suvorexant 40 and 30 mg/day and that ofthe 20 and 15 mg/day doses were the same: 8 (Citrome,2014). However, for adverse effects, there were numberneeded to harm values versus placebo of 13 for thehigher doses and 28 for the lower doses, indicating thatthe lower doses are better tolerated. Although the othersystematic review did not specifically analyze approvedversus unapproved doses, the authors performed ananalysis in which they excluded the higher doses fromthe primary outcomes and found that suvorexantremained superior to placebo in subjective total sleeptime and subjective time to sleep onset at 1 month(Kishi et al., 2015). Suvorexant was found to have anefficacy similar to the benzodiazepines, ramelteon, and
Drugs for Insomnia beyond Benzodiazepines 217

TABLE
6Sum
maryof
stud
iesas
sessingtheeffectsof
tasimelteon
(TMT)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Johnsa
and
Nev
ille
(201
4)Heterog
eneous
Heterog
eneous
Rev
iew
offour
RCTs.
Inon
eph
aseII
trial,sign
ifican
tsh
ifts
incircad
ianrh
ythm
wereob
served
only
forTMT
100mg/da
y.In
aph
aseIII
trial,LPSwas
sign
ifican
tly
impr
oved
intheTMTgrou
prelative
toplaceb
o.The
SET
andRESETtrials
both
found
TMTto
sign
ifican
tlyim
prov
een
trainm
entin
non-24
-hou
rsleep-wak
edisord
erpa
tien
ts.
Frequ
ency
andseve
rity
ofAEsweresimilar
across
trea
tmen
tgrou
ps.Most
common
AEswere
somnolen
cean
dhe
adache
.
TMT
iseffectiveat
redu
cing
symptom
sof
non-24
-hou
rsleep-wak
edisord
er.
Lockley
etal.
(201
5)18
–75
Total
blindn
esswith
non-24-hou
rsleep-
wak
edisord
er
TwoRCTs,
SET
(26wk,
N=84
)an
dRESET
(19wk,
N=20
).TMT
20mg/da
yvs.p
lacebo
.
TMT
sign
ifican
tlyim
prov
eden
trainm
ent,althou
ghthe
effect
didnot
last
after
discon
tinu
ation.
Nosign
ifican
tdifferen
cein
thediscon
tinu
ationrate
dueto
AEsbe
twee
nthe
TMT
(6%)an
dplaceb
o(4%)grou
ps.Hea
dach
ean
dincrea
sedalan
ine
aminotrans
ferase
occu
rred
inmorepa
tien
tsreceivingTMTthan
placeb
o.
TMT
iseffectiveat
redu
cing
symptom
sof
non-24
-hou
rsleep-wak
edisord
er.
NCT#0
0548
340
18–65
Primaryinsomnia
5-wkRCT.TMT
20vs.
50mg/da
yvs.p
lacebo
.N
=32
1.
Statisticswereno
tcond
ucted.
Mea
nch
ange
inLPS[S.E.]
was
45.0
[2.965
]forTMT
20mg/da
y,46
.4[2.954
]for
TMT50
mg/da
y,an
d28
.3[3.020
]forplaceb
o.Mea
nch
ange
inTST
was
51.4
[4.794
],52
.0[4.775
],an
d39
.9[4.882
]forthesa
me
resp
ective
grou
ps.
Mostcommon
AEswere
nasoph
aryn
gitisan
dhe
adache
.
Statisticswereno
tcond
ucted.
Rajaratna
met
al.(20
09)
Phas
eII
RCT:
18–50
.Phas
eIII
RCT:21
–50
.
Phas
eII
RCT:hea
lthy
volunteers.Pha
seIII
RCT:hea
lthy
volunteers
with
indu
cedtran
sien
tinsomnia
TwoRCTs.
Pha
seII
RCT:T
MT10
vs.2
0vs.
50vs.1
00mg/da
yvs.
placebo.
N=39
.Pha
seIIIRCT:T
MT20
vs.
50vs.1
00mg/da
yvs.
placebo.
N=41
1.
Intheph
aseII
RCT,TMT
redu
cedSOL
andincrea
sed
SE
compa
redwithplaceb
o.In
theph
aseIIIstud
y,TMT
impr
oved
SOL,SE,an
dWASO.L
PSwas
sign
ifican
tlyredu
cedrelative
toplaceb
o:in
phas
eII
stud
y,TMT10
mg/da
y,P
=0.00
3;50
mg/da
y,P
=0.01
9;10
0mg/da
y,P=0.02
1.In
the
phas
eIIIstud
y,alldo
sesof
TMT,P
,0.00
1forredu
cing
LPS.
Rates
ofAEsweresimilar
betw
eenTMT
and
placeb
o.
TMT
iseffectiveat
redu
cing
symptom
sof
insomnia
inamod
elof
circad
ianrh
ythm
disord
ers.
218 Atkin et al.

TABLE
7Sum
maryof
stud
iesas
sessingtheeffectsof
suvo
rexa
nt(SVX)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Citrome(201
4)18
–87
Primaryinsomnia
Systematic
review
offour
phas
eII
andph
aseIII
RCTs.
LSmea
ndifferen
cefrom
placeb
oin
subjective
TST
atmon
th1(m
inute):18
.4,P
,0.00
1for
SVX15
or20
mg;
22.7,P
,0.00
1forSVX
30or
40mg.
LSmea
ndifferen
cefrom
placeb
oin
SOL
bypo
lysomno
grap
hyat
mon
th1(m
inute):29.1,
P,
0.00
1for
SVX
15or
20mg;
211
.4,
P,
0.00
1forSVX
30or
40mg.
Reb
oundinsomnia
and
withdr
awal
effectsnot
observed
aftertrea
tmen
tdiscon
tinu
ation.
Som
nolenc
eis
themost
common
AE.
SVX
iseffectiveat
redu
cing
symptom
sof
insomnia.
Highe
rdo
sesaremore
effectivebu
tmay
hav
ea
high
errisk
ofAEs.
Herringet
al.(201
2)18
–64
Primaryinsomnia
byDSM-IV
4-wkcrossove
rRCT.SVX
10vs.2
0vs.4
0vs.8
0mg/
day.
N=25
4.
Objective
ly-m
easu
redLPS
(minute)at
EOSwas
chan
ged
relative
toplaceb
o22.3[2
12.2,
7.5]
for10
mg/da
y,222
.3[232
.3,2
12.3]for
20mg/da
y,23.8
[213
.8,6
.3]for40
mg/da
y,29.5
[219
.7,0.7]for
80mg/da
y.How
ever,
ingene
ral,morerobu
steffectswere
observed
forSV
X40
and80
mg/da
yon
subjectiv
eSO
L,o
bjectiv
eTST
,an
dsubjectiv
eQOS.
10an
d20
mg/da
ysh
owed
similar
leve
lsof
adve
rse
effectsto
placeb
o,while
40an
d80
mg/da
yha
dincrea
sedad
verseeffects.
One
patien
treceiving
SVX
80mg/da
yhad
amildvisu
alha
lluc
ination
anddiscon
tinu
ed.Most
common
AEswere
somno
lenc
e,he
adache
,an
ddizziness.
SVX
iseffectiveat
redu
cing
symptom
sof
insomnia.
SVX
10an
d20
mg/da
yarebe
tter
toleratedthen
40an
d80
mg/da
y.
Herringet
al.(201
6)non
elde
rly
(18–
64)an
delde
rly($
65)
Primaryinsomnia
byDSM-IV-TR
Two3-moRCTsin
elde
rly
andno
n-elde
rlypa
tien
ts.
SVX
40/30mg/da
yvs.
SVX
20/15mg/da
yvs.
placeb
o.N
=10
21in
first
RCTan
dN
=10
19in
secondRCT.
Sub
jectiveSOL(m
inute)
differen
cebe
tweenSVX
40/30mg/da
yan
dplaceb
oat
mon
th3:
28.4
[212
.8,24.0]
intrial1,
213
.2[2
19.4,27.0]
intrial2.
Themostcommon
AE
that
was
increa
sedforSVXvs.
placeb
owas
nex
t-da
ysomno
lenc
e.
SVX
iseffectiveat
redu
cing
symptom
sof
insomnia.
SVX
40/30mg/da
ywas
supe
rior
toplaceb
oon
almostallsu
bjective
and
polysomnog
raph
yen
dpo
ints
inbo
thtrials;S
VX
20/15mg/da
ywas
supe
rior
toplaceb
oon
man
ysu
bjective
mea
sures.
Kishi
etal.(201
5)NS
Primaryinsomnia
byDSM-IV
Systematic
review
and
meta-an
alysis
offour
placeb
o-controlled
RCTs.
N=30
76.
Mea
npo
oled
(15an
d40
mg/da
y)differen
cebe
tweenSVX
and
placeb
oin
subjective
TST
atmon
th1(m
inute):220
.16
[225
.01,
215
.30].Mea
npo
oled
(15an
d40
mg/da
y)diffe
rence
betw
eenSV
Xan
dplaceboin
subjectiv
eTST
atmon
th1(m
inute):2
7.62
[211
.03,
24.21
].
Discontinua
tion
dueto
all-
cause,
inefficacy,
and
intolerabilitydidno
tdiffe
rbetw
eengrou
ps.S
VX
grou
pha
dhigh
erincidence
ofab
norm
aldreams,
somno
lence,
excessive
daytim
esleepine
ss,fatigue
,an
ddrymou
th.
SVX
iseffectiveat
redu
cing
symptom
sof
insomnia.
(con
tinued
)
Drugs for Insomnia beyond Benzodiazepines 219

sedating antidepressants at reducing symptoms of in-somnia (Kishi et al., 2015).
5. Conclusion. Asummary of the effects of suvorexanton sleep architecture is presented in Table 2. There isstrong evidence that suvorexant is effective at reducingsymptoms of insomnia disorder at doses 15–40 mg/day,based on two systematic reviews (Citrome, 2014; Kishiet al., 2015). Suvorexant exerts strong effects on increas-ing total sleep time. Lower doses may be preferred, perFDA guidelines, to minimize the risk of adverse effects.
VI. Antidepressant Drugs
Sedating antidepressants are commonly prescribed forinsomnia: one analysis found that they were prescribedmore often than the FDA-approved treatments for in-somnia in 2002 (Walsh, 2004; McCall, 2016). Trazodonewas the most commonly prescribed medication for in-somnia in 2002, with 34% more prescriptions than themost commonly prescribed FDA-approved treatment(Walsh, 2004). In fact, there were 5.28 million prescrip-tions for antidepressants for insomnia and only 3.4millionprescriptions for FDA-approved hypnotics (Walsh, 2004).
A. Amitriptyline
1. Mechanism of Action. Amitriptyline is a tricyclicantidepressant with strong effects as a serotonergicreuptake inhibitor [SERT Ki (nM) = 3.13] (Vaishnaviet al., 2004) and moderate effects as a norepinephrinereuptake inhibitor [NET Ki (nM) = 22.4] (Tatsumi et al.,1997). Indeed, serotonergic-norepinephrine reuptakeinhibitors lack hypnotic properties, and as thus, ami-triptyline’s hypnotic effects are attributable to its pro-file as an H1 and H2 receptor antagonist as well as a5-HT2A and 5-HT2C antagonist. Main molecular targetsof amitriptyline are summarized in Table 1.
2. Indications. Amitriptyline is FDA approved forthe treatment of major depressive disorder (Alphapharm,2012). Clinical studies examining the hypnotic effects ofamitriptyline are detailed in Table 8.
3. Pharmacokinetics. Amitriptyline is well-absorbedwith peakplasma concentrations occurringwithin 6 hoursof oral administration (Alphapharm, 2012). The meanhalf-life of amitriptyline is 22.4 hours, whereas the meanhalf-life of its active metabolite nortriptyline is 26 hours.Amitriptyline is 96% bound to plasma proteins, andundergoes extensive first-pass metabolism in the liver tonortriptyline viaN-demethylation mediated by CYP2C19(Rudorfer and Potter, 1999). Other liver enzymes involvedin its metabolism are CYP2D6 and CYP3A4 (RudorferandPotter, 1999).Genetic heterogeneity betweenpatientsaffects the concentration of the drug in the body, partic-ularly the ratio between amitriptyline and nortriptyline(Rudorfer and Potter, 1999).
4. Results in Insomnia Disorder. No studies ofamitriptyline as a treatment of insomnia disorder wereidentified.
TABLE
7—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Michelsonet
al.(20
14)
18+
Primaryinsomnia
byDSM-IV-TR
Yea
rlon
gRCTwitha
subs
eque
nt2-mo
rand
omized
discon
tinu
ationph
asein
which
participan
tsgive
nplaceb
oweresw
itch
edto
SVX
andvice
versa.
SVX
40mg/da
yforpa
tien
tsyo
unge
rthan
65,3
0mg/
dayforpa
tien
tsolde
rthan
65,o
rplaceb
o.N
=78
1.
Cha
ngein
subjective
SOL(m
inute)
atmon
th12
forSVX
was
226
.6[2
30.5,222
.7]vs.217
.0[2
22.6,211
.4]forplaceb
o,P=0.00
55.C
hang
ein
subjective
TST
(minute)at
mon
th12
was
60.5
[54.0,
66.9]forSVXvs.3
3.0
[23.7,
42.2]for
placebo,P,
0.0001.
Mostcommon
AE,
somno
lenc
e,repo
rted
for
13%
ofpa
tien
tsreceiving
SVX
vs.3%
ofthose
receivingplaceb
o.Fatiguean
ddr
ymou
thwerealso
increa
sedfor
SVX
vs.placeb
ogrou
ps.
SVX
iseffectiveat
redu
cing
symptom
sof
insomnia.
SVX
ispr
obab
lynot
associated
withrebo
und
insomnia
during
discon
tinu
ationafter1yr
oftrea
tmen
t.
Sunet
al.(201
3)18
–45
Hea
lthy
young
men
Fou
r-pe
riod
crossove
rRCT
follow
edby
afifthpe
riod
toas
sess
pharmacok
inetics.
SVX
10vs.50
vs.10
0mg/da
yN
=22
(com
pleted
19).
SVX50
and10
0mgde
crea
sedLPS
andWASO
andincrea
sedSE
andTST.
Allrepo
rted
adve
rseev
ents
weremild.
Themost
freq
uently
repo
rted
adve
rseev
ents
were
somno
lenc
e(20%
inthose
receivingSVX
100mg)
andhea
dach
e.
SVX
iseffectiveat
prom
otingsleepin
healthysu
bjects
witho
utkn
ownsleep
impa
irmen
ts
220 Atkin et al.

5. Other Results. Two studies of amitriptyline as atreatment of secondary insomnia were identified. Onestudy examined amitriptyline’s effect on sleep in healthyvolunteers when administered chronically (Hartmannand Cravens, 1973) and one study analyzed patients withopiate withdrawal insomnia (Srisurapanont and Jarusur-aisin, 1998). The study in healthy volunteers foundaltered sleep patterns in the group given amitriptylinecompared with placebo, with those given the drug dis-playing increased total sleep time, increasedSWS, and lessREM (“desynchronized” sleep) (Hartmann and Cravens,1973). The other study compared amitriptyline 50 mg/dayto lorazepam 1–4 mg/day in patients with opiate with-drawal insomnia, finding that although amitriptyline waslikely as effective as lorazepam at relieving insomniasymptoms, it may have been associated with a hangovereffect thenext day (Srisurapanont andJarusuraisin, 1998).
6. Conclusion. A summary of the effects of amitrip-tyline on sleep architecture is presented in Table 2.Based on amitriptyline’s effect in a study of healthyvolunteers (Hartmann and Cravens, 1973) of increasingtotal sleep time and its efficacy in opiate withdrawalinsomnia, there is weak evidence of its efficacy in thetreatment of insomnia disorder.
B. Mirtazapine
1. Mechanism of Action. Mirtazapine is classified asa noradrenergic and specific serotonergic antidepres-sant, because it enhances adrenergic and serotonergicneurotransmission in a manner distinct from otherclasses of drugs. Its effects as a sedative and as ahypnotic are attributable to its blockade of the hista-mine H1 receptor. By antagonizing a2-autoreceptors itincreases norepinephrine release; by antagonizing a2-het-eroreceptors it increases serotonin release, although itseffect on serotonergic systems is specific to 5-HT1A-medi-ated neurotransmission, because it also blocks the 5-HT2
and 5-HT3 receptors (Anttila and Leinonen, 2001) (SeeTable 1 for the list ofmirtazapine’smainmolecular targets).In mice, thermal hyperalgesia and sleep disturbance in amodel of neuropathic pain were nearly completely normal-ized by mirtazapine administration (Enomoto et al., 2012).
2. Indications. Mirtazapine is FDA approved for thetreatment of major depressive disorder in adults (USFDA, 2007b). Clinical studies examining the hypnoticeffects of mirtazapine are detailed in Table 9.
3. Pharmacokinetics. Mirtazapine is rapidly andcompletely absorbed and has a half-life of between20 and 40 hours, with women exhibiting significantlylonger elimination half-lives thanmen (mean half of life37 hours for women vs. 26 hours for men) (US FDA,2007b). Peak plasma concentration is reached within2 hours of administration, and the presence or absenceof food does not significantly affect its pharmacoki-netics. Plasma levels are linear to dose over a dose rangeof 15–80 mg. The drug is 85% bound to plasma proteins.The drug’s absolute bioavailability is about 50%, and
TABLE
8Summaryof
stud
iesas
sessingtheeffectsof
amitryptiline(A
MT)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Hartm
annan
dCrave
ns(197
3)21
–35
Hea
lthyvo
lunteers
1125
-night
crossove
rstud
y.AMT
50mg/da
yvs.placeb
ovs.
reserp
ine0.50
mg/da
yvs.
chlorp
romaz
ine50
mg/da
yvs.
chloralhyd
rate
500mg/da
yvs.
chlord
iazepo
xide
50mg/da
y.N
=14
.
TST
increa
sedforAMT
relative
toplaceb
othroug
hout
trial.SWS
increa
sedan
dSOL
decrea
sed
earlydu
ring
administration.
REMS(“de
sync
hron
ized
sleep”)
was
redu
cedthrough
outthe
trial,mostpr
ofou
ndly
inthe
firstfew
days
ofad
ministration.
Sub
jectsthem
selves
asfeeling
worse
inthemorning
during
AMT
trea
tmen
t.Rep
orts
offeelingsick
increa
sedforweeks
3an
d4on
andwee
ks1an
d2off
med
ication.
Rep
orts
ofun
usua
lps
ycho
logicfeelings
increa
sedin
week4on
med
ication.
AMTis
prob
ably
effectiveat
redu
cing
symptom
sof
insomnia.
Men
dlew
iczet
al.
(199
1)25
–68
Depressed
inpa
tients
Retrosp
ective
stud
ybe
fore
trea
tmen
twithAMT
andat
5-7
wkfollow
up.
AMT
(165
635
mg/da
y).N
=18
.
Marke
dsu
ppressionof
REM
sleep.
Increa
sein
stag
e1an
dstag
e2NREM
slee
pan
dnoch
ange
sin
SWSan
dlatenc
yto
sleep
onset.
Not
assessed
.AMT
indu
cesalargeREM
sleepsu
ppressionin
depr
essedinpa
tien
ts.
Srisu
rapa
non
tan
dJa
rusu
raisin
(199
8)
18–65
Opiatewithdr
awal
insomnia
6-da
yrand
omized
,do
uble-blind
trial.AMT
25–10
0mg/da
yvs.
lorazepa
m1–
4mg/da
y.N
=27
.
Eas
eof
gettingto
sleep
question
nairescores
ontheSEQ
were17
7.46
53.9
forAMT
and
184.56
85.4
forlorazepa
m,P
=0.80
.Eas
eof
awak
eningfrom
sleepon
theSEQ
was
132.86
47.9
forAMT
and16
7.66
38.4
forlorazepa
m,P
=0.04
7.
Non
eof
thepa
tien
tsrepo
rted
any
seriou
sAEsdu
ringthestudy
.Awak
eningfrom
sleepafter
AMT
was
moredifficult
than
afterlorazepa
m.
AMT
isas
effectiveas
lorazepa
mat
redu
cing
symptom
sof
insomnia
associated
withop
iate
withdr
awal
syndr
ome,
thou
ghit
may
beas
sociated
witha
hang
over
effect.
Drugs for Insomnia beyond Benzodiazepines 221

in vitro data indicate that cytochromes 2D6, 1A2, and3A are responsible for the formation of its metabolites(US FDA, 2007b).4. Results in Insomnia Disorder. No studies of
mirtazapine as a treatment of primary insomnia wereidentified, except for a case series (Dolev, 2011) con-ducted in perimenopausal women who suffered frominsomnia (N = 11) and who were not depressed by theHAM-D scale (Hamilton, 1960). In this study, thesubjects were given mirtazapine 15 mg/day for 2–4 weeks followed by treatment with prolonged-releasemelatonin 2 mg/day concurrent with the tapering ofmirtazapine over 1–3 months. Combination treatmentwith mirtazapine and melatonin during the taperingperiod reduced PSQI global scores from 14.45 6 1 atbaseline to 6.00 6 0.7 at endpoint. Sleep latency asmeasured by PSQI question 2 decreased from 52.73 614.04 minutes at baseline to 18.64 6 2.87 minutes atendpoint.5. Other Results. Five studies of mirtazapine as a
treatment of secondary insomnia were identified. Therewas one open-label study (N = 36) in patients withadvanced cancer and pain or other distressing symp-toms, including insomnia (Theobald et al., 2002); oneopen-label trial (N = 6) in patients diagnosed withmajordepressive disorder and poor sleep quality (Winokuret al., 2000); one randomized trial (N = 19) comparingmirtazapine to fluoxetine in patients diagnosed withmajor depressive disorder and insomnia (Winokuret al., 2003); one open-label study (N = 53) in patientswith cancer and comorbid MDD, anxiety disorders, oradjustment disorder (Cankurtaran et al., 2008); and oneopen-label study (N = 42) in patients with cancer andMDD (Kim et al., 2008). In these studies, mirtazapinewas generally effective at reducing symptoms of in-somnia; in the randomized trial, it was more effectivethan fluoxetine (Winokur et al., 2003).6. Conclusion. A summary of the effects of mirtaza-
pine on sleep architecture is presented in Table 2. Thereis weak evidence that mirtazapine is effective at re-ducing symptoms of insomnia disorder, based on onecase series (Dolev, 2011) and the available open-labelevidence of mirtazapine’s effectiveness in secondaryinsomnia.
C. Trazodone
1. Mechanism of Action. Trazodone’s effect as ahypnotic is attributable to its moderate antihistaminer-gic activity at the H1 receptor, its partial agonism at the5HT1A receptor (Odagaki et al., 2005), its antagonism ofthe 5HT1C and 5HT2 receptors, and its antagonism ofthe postsynaptic a1-adrenergic receptor (Schatzbergand Nemeroff, 2009; McCall, 2016). It also exerts rela-tively weak, although specific, reuptake inhibitioneffects at the 5-HT transporter (see Table 1 for asummary of trazodone’s main targets). Thus, trazodonehas amixed profile as both an agonist and an antagonist
of serotonin receptors. In rats, trazodone has beenshown to increase NREMS without affecting REMS(Lelkes et al., 1994).
2. Indications. Trazodone is FDA approved for thetreatment of depression. A survey revealed that trazodonewas the first-line choice of 78% or psychiatrists whenprescribing medications to treat SSRI-induced insomnia(Dording et al., 2002). As mentioned previously, in 2002,trazodone was the most commonly prescribed medicationfor insomnia, with 34% more prescriptions than the mostcommonly prescribed FDA-approved treatment (Walsh,2004). Clinical studies examining the hypnotic effects oftrazodone are detailed in Table 10.
3. Pharmacokinetics. Trazodone’s half-life is 7.0 61.2 after multiple oral administration and shows linearpharmacokinetics within the dosage range of 50–150 mg/day (Nilsen et al., 1993). Its absorption isirregular in fasting subjects, but it is improved if thedrug is taken after food. However, no differences areobserved in the total amount of trazodone absorbedwithand without food: its bioavailability values are 65 6 6%and 63.4%, respectively (Nilsen and Dale, 1992). Thedrug is primarily metabolized by the liver enzymeCYP3A4, and inhibition of this enzyme by other drugsleads to high blood levels of trazodone (Rotzinger et al.,1998). CYP3A4 mediates the metabolism of trazodone toits main active metabolite, m-chlorophenylpiperazine,which has 5-HT2C agonist and 5-HT2A antagonisticproperties (Rotzinger et al., 1998).
4. Results in Insomnia Disorder. One 2-week paral-lel group RCT (N = 306) in patients with primaryinsomnia was identified (Walsh et al., 1998). The studycompared treatment with trazodone 50 mg/day totreatment with zolpidem 10 mg/day and placebo aftera 1-week placebo lead-in period. During the first week,both drugs produced significantly shorter self-reportedsleep latency and longer self-reported sleep durationthan placebo. Sleep latency was significantly shorterwith zolpidem thanwith trazodone. Duringweek 2, onlythe zolpidem group maintained a significantly shortersleep latency than the placebo group, and sleep durationdid not vary significantly among groups.
5. Other Results. Two reviews on the use of trazo-done as a treatment of insomnia were identified (Jamesand Mendelson, 2004; Mendelson, 2005). Both reviewspredominantly analyzed studies of trazodone in pa-tients diagnosed with major depressive disorder. Al-though trazodone was shown to increase total sleeptime in patients with MDD (James and Mendelson,2004), there was limited evidence of its efficacy(Mendelson, 2005). The high rate of discontinuationdue to adverse events, which included sedation, dizzi-ness, and psychomotor impairment, make the risk-benefit ratio of trazodone therapy for insomnia un-certain (Mendelson, 2005). Furthermore, there is a riskof priapism in 1 out of 6000 patients treated withtrazodone (James and Mendelson, 2004).
222 Atkin et al.

TABLE
9Sum
maryof
stud
iesas
sessingtheeffectsof
mirtaza
pine
(MRT)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clus
ion
Aslan
etal.
(200
2)18
–30
You
nghea
lthyvo
lunteers
RCT
withacuteinjectionof
MRT(30mg)
vs.p
lacebo
.N
=20
.
MRT
increa
sedstag
eN3,
sleep
efficien
cy,didnot
alterREM
sleep
andde
crea
sedthenumbe
rof
awak
enings
andtheirdu
ration
during
sleep.
Not
analyz
ed.
MRTis
effectivein
indu
cing
NREM
slee
pwithou
taffectingREM
sleepin
healthysu
bjects.
Can
kurtaran
etal.(20
08)
18–65
Can
cerwithmajor
depr
essive
disord
er,
anxietydisord
ers,
orad
justmen
tdisord
er
6-wkop
en-lab
eltrial.MRT
5–30
mg/da
yvs.
imipramine5–
100mg/
dayvs.un
trea
tedcontrol
grou
pthat
refuseddr
ugtherap
y.N
=53
.
Percent
ofpa
tien
tsrepo
rtingnightly
difficulty
fallingas
leep
inMRT
grou
pde
crea
sedfrom
65at
baseline
to15
aten
dpoint
vs.ade
crea
sefrom
53.8
atba
seline
inim
ipramine
grou
pto
30.8
aten
dpoint
vs.a
decrea
sefrom
50at
baseline
incontrolgrou
pto
30at
endp
oint.
Not
analyz
ed.
MRTis
effectiveat
redu
cing
symptom
sof
insomniain
canc
erpa
tien
ts,an
dmoreeffectivethan
imipramine.
Dolev
(201
1)45
–52
Perim
enop
ausa
lwom
enwithinsomnia
whodid
not
suffer
from
depr
ession
byHAM-D
Cas
eseries.MRT
15mg/
dayfor2-4wkfollow
edby
trea
tmen
twith2mg
prolon
ged-releas
emelaton
inwithtape
ring
ofMRT
for1–
3mo.
N=
11.
Com
bina
tion
trea
tmen
twithMRT
andmelaton
indu
ringMRT
tape
ring
period
redu
cedPSQI
glob
alscores
from
14.456
1at
baseline
to6.00
60.7at
endp
oint.
SOLas
mea
suredby
PSQIqu
estion
2(m
inute)
decrea
sedfrom
52.736
14.04at
baseline
to18
.646
2.87
aten
dpoint.
NoAEswererepo
rted
.MRTfollow
edby
prolon
ged-
releas
emelaton
inad
d-on
trea
tmen
tfollow
edby
melaton
inmon
othe
rapy
iseffectiveat
redu
cing
symptom
sof
insomniain
perimen
opau
salwom
en.
Kim
etal.(200
8)22
–79
Can
cerpa
tien
tswith
depr
ession
4-wkop
en-lab
eltrial.MRT
15–45
mg/da
y.N
=42
.Amou
ntof
sleep(hou
rs)increa
sed
from
3.66
1.9at
baseline
to6.86
2.5at
endp
oint,P
,0.00
1.Eas
eof
gettingto
sleepsu
bscale
ofthe
Cho
nnam
Nationa
lUnive
rsity
Hospital-Leeds
Sleep
Eva
luation
Que
stionn
aire
decrea
sedfrom
4.26
1.0at
baseline
to2.46
1.0at
endp
oint,P
,0.00
1.
Fou
rpa
tien
tsdiscon
tinued
MRT
dueto
side
effects
(Twodu
eto
seda
tion
andon
eea
chfor
general
wea
knessor
cons
tipa
tion
).
MRTis
effectiveat
redu
cing
symptom
sof
insomniain
canc
erpa
tien
ts.
Theoba
ldet
al.
(200
2)40
–83
Adv
ancedcancerpa
tien
tswithpa
inan
dothe
rdistressingsymptom
s
Ope
n-labe
lcrossove
rstud
yof
MRT
15/30mg/da
y.N
=36
.
The
rewereno
sign
ifican
tdifferen
ces
onNRSscales
mea
suring
insomnia.
How
ever,therewas
atren
dtoward
impr
oved
sleep.
Only
onepa
tien
twithdr
ewdu
eto
MRT
side
effects.
MRT
may
beeffectiveat
redu
cing
symptom
sof
insomnia
incancer
patien
ts.
Winok
uret
al.
(200
0)18
–65
Major
depr
essive
disord
erwithpo
orsleepqu
ality
2-wkop
en-lab
elstud
y.MRT
15–30
mg/da
y.N
=6.
SOL
impr
oved
,P
=0.00
9.TST
impr
oved
,P=0.00
4.SE
impr
oved
,P=0.00
03.M
RTdidno
tsign
ificantly
affect
REM
sleeppa
rameters.
Fourof
sixsubjects
reported
daytim
esomnolencedu
ring
week
1,though
thecomplaints
resolved
byweek2.
MRTis
effectiveat
redu
cing
symptom
sof
insomnia.
Winok
uret
al.
(200
3)18
–45
Major
depr
essive
disord
erwithinsomnia
8-wkrand
omized
trial.
MRT
15–45
mg/da
yvs.
fluo
xetine
20–40
mg/da
y.N
=19
.
MeanSO
L(m
inute)
bypolysomno
grap
hydecreasedfrom
34.3
624
.0at
baselin
eto
10.9
69.6at
Week9in
MRTgrou
p,P,
0.05
vs.3
8.66
32.2
atba
selin
eto
43.3
628
.4at
Week8in
fluoxetine
grou
p.Total
sleeptime(m
inute)
increasedfrom
327.96
81.8
atba
selin
eto
428.16
73.6
atWeek8in
MRTgrou
p,P,
0.05
vs.3
17.4
668
.8at
baselin
eto
325.16
116.4in
fluoxetinegrou
p.
Not
analyz
ed.
MRTis
effectiveat
redu
cing
symptom
sof
insomnia,
andsu
perior
tofluo
xetine
.
Drugs for Insomnia beyond Benzodiazepines 223

TABLE
10Sum
maryof
stud
iesas
sessingtheeffectsof
traz
odon
e(TRZ)
onsleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Cam
argo
set
al.
(201
4)60
+Alzhe
imer’sdiseas
e2-wkRCT.TRZ50
mg/da
yvs.placeb
o.N
=30
.Actigraph
y:TRZsu
bjects
slep
t42
.5min
morethan
placeb
osu
bjects
andpe
rcen
tsleepincrea
sed8.5%
.Noeffect
oncogn
itionor
WASO
ornu
mbe
rof
awak
enings
AEstran
sien
tan
dmild.
Trazodo
nemay
beeffectiveat
redu
cing
symptom
sof
insomniain
olde
rad
ults
withAlzheimer’sdiseas
e.
Cunningh
amet
al.(19
94)
18+
Major
depr
ession
6-wkRCTof
traz
odon
evs.
venlafax
inevs.placeb
o.96
resp
onde
rscontinue
din
a1-yr
doub
le-blind
continua
tion
phas
e.Ave
rage
doses:
156–
160mg/da
yve
nlafax
ine
and29
4–30
0mg/da
yTRZ.N
=22
5.
TRZpr
oduc
edmoreim
prov
emen
ton
thesleepdistur
banc
efactor
ofthe
HAM-D
,bu
tve
nlafax
inemore
effectivein
cogn
itivedistur
banc
ean
dretard
ationfactorsof
theHAM-
D.
Significantly
morepa
tien
tsdiscon
tinued
TRZdu
eto
dizzinessthan
patien
tstaking
placeb
oor
venlafax
ine.
Significantly
morepa
tien
tsdiscon
tinu
edve
nlafaxinedu
eto
nau
sea.
TRZis
effectiveat
redu
cing
symptom
sof
insomnia
inpa
tien
tswithMDD.
Fried
man
net
al.
(200
8)16
–65
DSM-IV
curren
talcoho
lde
pend
ence
andsleep
disturban
ce
12-w
kRCT.TRZ50
–
150mg/da
yvs.placeb
o.N
=17
3.
TRZgrou
pexperien
cedless
improvem
ent
inproportion
ofda
ysab
stinen
tdu
ring
administrationof
medication,
andan
increase
inthenu
mberof
drinks
per
drinking
dayon
cessationofstud
y.TRZ
improved
sleepqu
ality(PSQ
Imean
chan
ge23.02
[23.38
,22.67
]),bu
tafter
cessationsleepqu
alityequa
lized
with
placebo.
TRZgrou
prepo
rted
moredr
ymou
th.
Althou
ghTRZredu
ced
symptom
sof
insomnia,
itmay
impe
deim
prov
emen
tsin
alcoho
lism
during
detoxification
andlead
toincrea
seddr
inkingwhen
stop
ped.
Haffm
ansan
dVos
(199
9)mea
n:44
Previou
sseve
remajor
depr
ession
;cu
rren
tinsomniasecond
ary
tobrofarom
ine
trea
tmen
t
Crossov
erRCT.T
RZ50
mg/
dayas
adjunct
tobrofarom
ine15
0–25
0mg/
day.
N=7.
TRZdidno
tim
prov
eSOL,total
sleep
time,
ortimeaw
ake.
TRZredu
ced
thenumbe
rof
awak
enings
(P=
0.01
9)an
dincrea
sedstag
eIV
sleep
(P=0.08
8).
WhiletakingTRZ,on
epa
tien
trepo
rted
cons
tipa
tion
and
naus
ea,o
nepa
tien
trepo
rted
vertigo,
drymou
th,a
nd
palpitations,
andon
epa
tien
tha
dting
ling
feelings
inch
inan
dmod
eratehe
artbur
n.
TRZmay
not
beeffectiveat
redu
cing
symptom
sof
insomniasecond
aryto
trea
tmen
twithstim
ulating
antide
pressa
nts,
butmay
increa
seslow
-wav
esleep.
James
and
Men
delson
(200
4)
Varied.
Varied.
Rev
iew.
TRZincrea
sestotalsleeptimein
patien
tswithMDD,tho
ughthere
arefew
data
tosu
pportitsus
ein
non-de
pressedpa
tien
ts.
The
reis
ano
tablerisk
ofpriapism
in1ou
tof
6000
patien
tstrea
tedwith
TRZ.
The
reis
also
arisk
oforthostatichy
potens
ionan
dtheindu
ctionof
cardiac
arrhythm
iasin
patien
tswith
preexistingcardiacdisease.
TRZha
smoreside
effectsthan
conv
ention
alhy
pnotics,
mak
ingitsrisk
-ben
efit
ratio
uncertain.
Karam
-Hag
ean
dBrower
(200
3)seeGab
apen
tinsection
Kay
nak
etal.
(200
4)20
–50
Insomnia
seconda
ryto
trea
tmen
tw/SSRI,
DSM-IV
depr
ession
2-wkcrossove
rRCTw/
1-wkwas
hou
t.TRZ
100mg/da
y+SSRIs
vs.
placeb
o+SSRIs.N
=12
.
TRZsign
ificantly
increasedtotals
leep
time,percen
tage
ofstage3an
d4sleep,
SE,sleep
continuity
anddecreased
numberof
awak
enings.A
tweek3,
completingboth
TRZan
dplacebo
treatm
ents
w/w
asho
ut,m
eanglobal
PSQ
Iscores
inboth
grou
psredu
ced
from
156
2.5to
56
1.6.
Total
polysomno
grap
hicsleeptime(m
inute)
increasedfrom
382.17
658
to42
86
39on
last
TRZnigh
t,P,
0.05
.SOL
notsign
ificantly
improved.
TRZpe
riod
associated
w/o
nesu
bjectrepo
rtingmild
acid
indigestionan
dtw
orepo
rting
mild
daytim
eseda
tion
.
TRZmay
beeffectiveat
redu
cingsymptom
sof
SSRI-
indu
cedinsomnia.
(con
tinued
)
224 Atkin et al.

TABLE
10—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
LeBon
etal.
(200
3)18
–65
Alcoh
olde
pende
nce
withph
ysiologic
depe
nde
nce
byDSM-
IV;alcoho
l-indu
ced
sleepdisord
ers,
insomnia
type
(DSM-
IV)
4-wkRCT.TRZ50
mg/da
yvs.placeb
o.N
=16
.SE
was
increa
sedin
TRZgrou
p.No
bene
fitin
placeb
ogrou
p.HAM-D
andCGIwerealso
better
inTRZ
grou
p.
Mostfreq
uen
tAEsin
theTRZ
grou
pwerehan
gove
rsan
ddizziness.
Doseredu
ction
from
200to
150mg/da
yredu
cedtheseAEs.
Inplaceb
ogrou
p:AEsinclude
dhe
adache
s,ha
ngov
er,an
dsk
inirritation
.
TRZmay
beeffectiveat
redu
cing
symptom
sof
insomnia.
Men
delson
(200
5)Varied.
Varied.
Rev
iew
of18
stud
ies.
Lim
ited
eviden
ceof
efficacy
ofTRZ,
man
ytrials
weresm
allan
dwere
cond
uctedin
depr
essedpa
tien
ts.
Highrate
ofdiscon
tinu
ation
dueto
side
effectsinclud
ing
seda
tion
,dizziness,
and
psycho
motor
impa
irmen
t.Thisraises
conc
erns
abou
ttheuse
ofTRZin
theelde
rly.
TRZrisk
-ben
efit
ratioin
insomniaremains
uncertain.
Mou
retet
al.
(198
8)35
–60
depr
essedin-patients
withaMADRS
score.20
Ope
n-labe
lstud
ywithTRZ
(400
–60
0mg/da
y)for
5wk.
N=10
.
TRZde
crea
sedlatenc
yto
sleepon
set
andintras
leep
awak
enings,
increa
sedTST
anddidnot
affect
REM
sleeptime.
Anincrea
sein
REM
sleeplatenc
ywas
foun
don
lyat
theen
dof
the5-wktrial.
Nau
sea,
dizziness.
TRZis
effectiveat
redu
cing
symptom
sof
insomnia
inde
pressedpa
tien
ts.
Nierenbe
rget
al.
(199
4)mea
n:41.9
S.D
.:10
Antidep
ressan
t-as
sociated
insomnia
inpa
tien
tstrea
ted
withfluo
xetine
orbu
prop
ion
Crossov
erRCT.T
RZ50
mg/
dayvs.placeb
o.Mea
nleng
thof
trea
tmen
t:6.5da
ysforTRZvs.
4.6da
ysforplaceb
o.N
=17
.
67%
repo
rted
impr
ovem
entwithTRZ
vs.13
%withplaceb
o.Im
prov
emen
twithTRZan
dnot
placeb
oon
PSQI
andYale-New
Hav
enscores.
Day
timeseda
tion
occu
rred
inon
epa
tien
t.Priap
ism
didnot
occu
r,bu
ton
epa
tien
tde
velope
dapr
olon
ged
erection
,pr
omptingado
sede
crea
se.
TRZmay
beeffectiveat
redu
cing
symptom
sof
insomnia.
Sch
arfan
dSachais(199
0)Dep
ressed
patien
tswith
sleepdisturban
ces
8-wksing
le-blind
stud
ywithTRZ15
0–40
0mg/
day.
N=6.
After
5wk,
TRD
impr
oved
sleep
efficien
cy(from
80.6
612
.3%
to91
.96
4.9%
),increa
sedTST
(from
387.16
59.2
to44
1.36
23.7
min),
prolon
gedREM
sleeplatenc
ybu
tdidnot
affect
theam
ount
ofREM
sleep.
TRZen
hanc
edsleep-related
penile
tumescenc
e.
Not
analyz
ed.
TRZaffectsREM
sleepin
youngmen
andredu
ced
awak
enings
andmov
emen
t/arou
sals
prob
ably
dueto
its
seda
ting
prop
erties.
Stein
etal.
(201
2)mea
n:38
.2S.D
.:8.6
Methad
one
maintenan
cetrea
tmen
tof
opioid
depe
nde
nce
6-moRCT.T
RZ50
–15
0mg/
dayvs.placeb
o.N
=13
7.Placebo
subjects
repo
rted
sign
ifican
tly
high
ersleepqu
alityrating
sthan
TRZsu
bjects,P
=0.04
.Polysom
nograp
hy:totalsleeptime
was
notsign
ifican
tlyim
prov
edin
TRZsu
bjects,P
=0.18
.
Betweenba
seline
and1mo,
TRZgrou
psign
ifican
tly
morelike
lyto
repo
rtincrea
sedthirst
ordr
ymou
th,P=0.00
1,an
dde
crea
sedap
petite,P
=0.04
.
Trazodo
neis
not
effectiveat
redu
cing
symptom
sof
insomniain
patien
tson
methad
onemaintenan
cetrea
tmen
twithsleep
distur
banc
e.
Walsh
etal.
(199
8)21
–65
Primaryinsomnia
byDSM-IIIR
2-wkpa
rallel-group
compa
risonRCT.TRZ
50mg/da
yvs.zolpidem
10mg/da
yvs.placeb
owith1-wkplaceb
olead
-in.N
=30
6.
Dur
ingfirstweek,
both
drug
spr
oduc
edsign
ifican
tlysh
orterself-
repo
rted
SOL(SSL)an
dlong
erself-
repo
rted
sleepdu
ration
(SSD)than
placeb
o.SSLwas
sign
ifican
tly
shorterwithzolpidem
than
with
TRZ.
Dur
ingWeek2,
only
the
zolpidem
grou
pmaintaine
da
sign
ifican
tlysh
orterSOL
than
the
placeb
ogrou
p,an
dSSD
didnot
vary
sign
ifican
tlyam
onggrou
ps.
Treatmen
t-em
ergent
AEs
reported
by65
.4%
ofplacebo
patien
ts,7
6.5%
ofzolpidem
patien
ts,a
nd75
%of
TRZ
patien
ts.H
eada
cheoccurred,
respectively,in19
%,2
4%,a
nd30
%of
participan
ts.
Somno
lenceoccurred,
respectively,in8%
,16%
,and
23%
ofpa
rticipan
ts.T
reatmen
tgene
rally
well-tolerated.
TRZmay
beless
effectivethan
zolpidem
atdo
sesstud
iedat
redu
cing
symptom
sof
insomnia.
(con
tinued
)
Drugs for Insomnia beyond Benzodiazepines 225
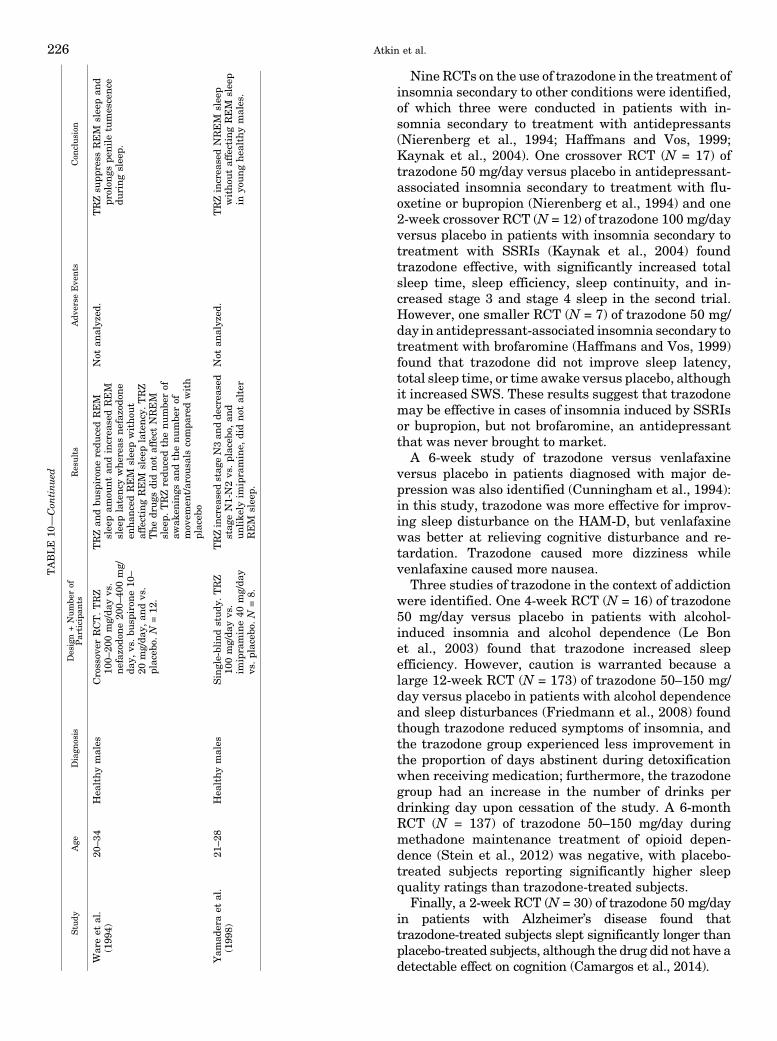
Nine RCTs on the use of trazodone in the treatment ofinsomnia secondary to other conditions were identified,of which three were conducted in patients with in-somnia secondary to treatment with antidepressants(Nierenberg et al., 1994; Haffmans and Vos, 1999;Kaynak et al., 2004). One crossover RCT (N = 17) oftrazodone 50 mg/day versus placebo in antidepressant-associated insomnia secondary to treatment with flu-oxetine or bupropion (Nierenberg et al., 1994) and one2-week crossover RCT (N = 12) of trazodone 100 mg/dayversus placebo in patients with insomnia secondary totreatment with SSRIs (Kaynak et al., 2004) foundtrazodone effective, with significantly increased totalsleep time, sleep efficiency, sleep continuity, and in-creased stage 3 and stage 4 sleep in the second trial.However, one smaller RCT (N = 7) of trazodone 50 mg/day in antidepressant-associated insomnia secondary totreatment with brofaromine (Haffmans and Vos, 1999)found that trazodone did not improve sleep latency,total sleep time, or time awake versus placebo, althoughit increased SWS. These results suggest that trazodonemay be effective in cases of insomnia induced by SSRIsor bupropion, but not brofaromine, an antidepressantthat was never brought to market.
A 6-week study of trazodone versus venlafaxineversus placebo in patients diagnosed with major de-pression was also identified (Cunningham et al., 1994):in this study, trazodone was more effective for improv-ing sleep disturbance on the HAM-D, but venlafaxinewas better at relieving cognitive disturbance and re-tardation. Trazodone caused more dizziness whilevenlafaxine caused more nausea.
Three studies of trazodone in the context of addictionwere identified. One 4-week RCT (N = 16) of trazodone50 mg/day versus placebo in patients with alcohol-induced insomnia and alcohol dependence (Le Bonet al., 2003) found that trazodone increased sleepefficiency. However, caution is warranted because alarge 12-week RCT (N = 173) of trazodone 50–150 mg/day versus placebo in patients with alcohol dependenceand sleep disturbances (Friedmann et al., 2008) foundthough trazodone reduced symptoms of insomnia, andthe trazodone group experienced less improvement inthe proportion of days abstinent during detoxificationwhen receiving medication; furthermore, the trazodonegroup had an increase in the number of drinks perdrinking day upon cessation of the study. A 6-monthRCT (N = 137) of trazodone 50–150 mg/day duringmethadone maintenance treatment of opioid depen-dence (Stein et al., 2012) was negative, with placebo-treated subjects reporting significantly higher sleepquality ratings than trazodone-treated subjects.
Finally, a 2-week RCT (N = 30) of trazodone 50 mg/dayin patients with Alzheimer’s disease found thattrazodone-treated subjects slept significantly longer thanplacebo-treated subjects, although the drug did not have adetectable effect on cognition (Camargos et al., 2014).
TABLE
10—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Wareet
al.
(199
4)20
–34
Hea
lthymales
Crossov
erRCT.TRZ
100–
200mg/da
yvs.
nefaz
odon
e20
0–40
0mg/
day,
vs.bu
spiron
e10
–20
mg/da
y,an
dvs.
placeb
o.N
=12
.
TRZan
dbu
spiron
eredu
cedREM
sleepam
ount
andincrea
sedREM
sleeplatenc
ywhe
reas
nefaz
odon
een
hanc
edREM
sleepwitho
utaffectingREM
sleeplatenc
y.TRZ
The
drug
sdidno
taffect
NREM
sleep.
TRZredu
cedthenu
mbe
rof
awak
enings
andthenu
mbe
rof
mov
emen
t/arou
sals
compa
redwith
placeb
o
Not
analyz
ed.
TRZsu
ppress
REM
slee
pan
dpr
olon
gspe
nile
tumescenc
edu
ringslee
p.
Yam
aderaet
al.
(199
8)21
–28
Hea
lthymales
Single-blindstudy
.TRZ
100mg/da
yvs.
imipramine40
mg/da
yvs.placeb
o.N
=8.
TRZincrea
sedstag
eN3an
dde
crea
sed
stag
eN1-N2vs.placeb
o,an
dun
like
lyim
ipramine,
didnot
alter
REM
slee
p.
Not
analyz
ed.
TRZincrea
sedNREM
slee
pwitho
utaffectingREM
sleep
inyo
unghea
lthymales.
226 Atkin et al.

6. Conclusion. A summary of the effects of trazodoneon sleep architecture is presented in Table 2. There isgood evidence that trazodone is effective at reducingsymptoms of insomnia in patients with SSRI-inducedinsomnia based on two RCTs (Nierenberg et al., 1994;Kaynak et al., 2004). Trazodone use is discouraged ininsomnia associated with opioid dependence or alcohol-ism based on one negative RCT in patients on metha-donemaintenance treatment (Stein et al., 2012) and thesafety concerns in one RCT conducted in patients withalcoholism (Friedmann et al., 2008).
D. Low-Dose Doxepin (,6 mg/day)
1. Mechanism of Action. Doxepin is a tricyclicantidepressant with significant antihistaminic effects.Doxepin is themost potent antihistamine of the tricyclicantidepressants, with four times the potency of ami-triptyline and 800 times the potency of diphenhydra-mine at the H1 receptor (Richelson, 1979; Gillman,2007). At standard antidepressant doses, .75 mg/day,doxepin inhibits the reuptake of serotonin and norepi-nephrine and antagonizes cholinergic, histaminergic,and a-adrenergic activity. As a hypnotic, doxepin isused at low doses; at doses ,10 mg/day, it theoreticallyaffects only the histamine receptor, with no meaningfuleffects on the noradrenergic and serotonergic systems(McCall, 2016) (see Table 1).2. Indications. Low-dose doxepin , under the brand
name Silenor (Pernix Therapeutics, Morristown, NJ),is FDA approved for the treatment of insomniacharacterized by difficulties with sleep maintenanceto a maximum dose of 6 mg/day (US FDA, 2010b).Doxepin is also approved as an antidepressant inthe treatment of “psychoneurotic patients with de-pression and/or anxiety.” Clinical studies examiningthe hypnotic effects of low-dose doxepin are detailed inTable 11.3. Pharmacokinetics. Low-dose doxepin has a ter-
minal half-life of 15.3 hours, whereas the half-life ofnordoxepin, Median to peak concentration (Tmax) ofdoxepin 6 mg occurs 3.5 hours after oral administrationto healthy fasted subjects; Tmax is delayed by approxi-mately 3 hours if the drug is taken with a high-fat meal,whereas AUC is increased by 41% and Cmax by 15% (USFDA, 2010b). For this reason, it is recommended thatdoxepin be taken without food, to minimize the risk ofnext day effects. The major liver enzymes responsiblefor the metabolism of doxepin are CYP2C19 andCYP2D6, whereas CYP1A2 and CYP2C9 are involvedto a lesser extent. The drug is 80% bound to plasmaproteins. Notably, doxepin interacts with cimetidine(causes a twofold increase in doxepin Cmax and AUC)and sertraline (causes AUC to be increased 21% andCmax to be increased 32%) (US FDA, 2010b).4. Results in Insomnia Disorder. One systematic
review (Yeung et al., 2015), five published RCTs (Rothet al., 2007; Scharf et al., 2008a; Krystal et al., 2011,
2010; Lankford et al., 2012), and one unpublished RCT(Takeda Global Research & Development Center Inc.,2008) of low-dose doxepin as a treatment of primaryinsomnia were identified. The systematic review in-cluded two studies of doxepin at antidepressant doses(25–300 mg/day) that are excluded in this review. Theauthors did not perform meta-analysis of pooled resultsdue to heterogeneity but confirmed that low-dosedoxepin had a small to medium effect size versusplacebo for sleep maintenance and sleep duration, butwas ineffective at improving the time to sleep onset. Thefindings in the individual RCTs cited above generallycame to similar conclusions as the recent systematicreview, although some RCTs used subjective measure-ments and others used polysomnographic measurements.
The unpublished clinical trial is a double-dummystudy of ramelteon + low-dose doxepin versus each drugas monotherapy versus placebo (Takeda Global Re-search & Development Center Inc., 2008). It found thatramelteon + low-dose doxepin was significantly moreeffective than ramelteon + placebo by polysomnography-measured wake time after sleep onset and total sleeptime, as well as subjective wake time after sleep onset.
5. Other Results. A single night RCT of low-dosedoxepin in healthy volunteers was also identified (Rothet al., 2010). In this trial, the investigators attempted toinduce transient insomnia using the first-night effect aswell as a 3-hour phase advance. Low-dose doxepin waseffective at reducing latency to sleep and increasingtotal sleep time.
6. Conclusion. A summary of the effects of low-dosedoxepin on sleep architecture is presented in Table 2.There is strong evidence that low-dose doxepin iseffective at reducing symptoms of primary insomniabased on one systematic review (Yeung et al., 2015), fivepublished RCTs (Roth et al., 2007; Scharf et al., 2008a;Krystal et al., 2011, 2010; Lankford et al., 2012), andone unpublished RCT (Takeda Global Research & De-velopment Center Inc., 2008). Low-dose doxepin exertsa strong on improving sleep maintenance.
VII. Anticonvulsant Drugs
A. Gabapentin
1. Mechanism of Action. Gabapentin is an anticon-vulsant drug that binds to the a2d subunit of voltage-sensitive calcium channels (Gee et al., 1996) (Table 1). Itcrosses several lipid membrane barriers; in vitro, it hasbeen shown to modulate the activity of the GABAsynthesizing enzyme, glutamic acid decarboxylase,and the glutamate synthesizing enzyme, branched-chain amino acid transaminase (Taylor, 1997). Itsmodulation of the GABAergic and glutamatergic sys-tems probably underlies its effect as a hypnotic andanxiolytic. Gabapentin is known to increase SWSwithout affecting other polygraphic variables and with-out causing increased drowsiness during the day
Drugs for Insomnia beyond Benzodiazepines 227

TABLE
11Sum
maryof
stud
iesas
sessingtheeffectsof
low-dosedo
xepine
(DXP)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Krystal
etal.
(201
0)65
+Primaryinsomnia
byDSM-IV
12-w
kRCT.DXP
1mg/da
yvs.
3mg/da
yvs.placeb
o.N
=24
0.
LPSwas
not
sign
ifican
tlydifferen
tfrom
placeb
oforan
ydo
seof
DXP.
How
ever,WASO
was
sign
ifican
tly
redu
cedat
alltimepo
ints
inthe
DXP
3mg/da
ygrou
p(P
,0.00
1)an
don
night1(P
,0.01
)an
dnight
85(P
,0.05
),bu
tnot
nigh
t29
intheDXP1mg/da
ygrou
p.TST
was
increa
sedsign
ifican
tlyin
theDXP
3mg/da
ygrou
pat
alltimepo
ints
andin
theDXP1mg/da
ygrou
pat
night1(P
,0.05
)an
dnight85
(P,
0.05
)bu
tnot
night29
.
Rates
oftrea
tmen
t-em
erge
ntAEs
werelower
intheDXP
grou
psthan
theplaceb
ogrou
p:52
%of
placeb
osu
bjects
repo
rted
anAE
compa
red
withDXP1mg/da
y(40%
)an
dDXP
3mg/da
y(38%
).Less
discon
tinu
ationwithDXP
aswell:
placeb
odiscon
tinu
ationwas
14%,
DXP
1mg/da
ywas
9%,DXP3mg/
daywas
10%.Noev
iden
ceof
nex
t-da
yseda
tion
.
Low
-doseDXP
iseffective
atredu
cingsymptom
sof
insomnia.
Krystal
etal.
(201
1)18
–64
Primaryinsomniaby
DSM-IV-TR
35-day
RCT
follow
edby
two
nightsof
sing
le-blind
placeb
otrea
tmen
tto
assess
discon
tinu
ationeffects.
DXP
3mg/da
yvs.6mg/da
yvs.
placeb
o.N
=22
1.
Bypo
lysomnog
raph
y:LPSwas
only
impr
oved
relative
toplaceb
oin
both
DXP3an
d6mg/da
yon
night1,
P,
0.00
01,an
dno
tim
prov
edon
nigh
t15
or29
.TST
was
sign
ifican
tly
impr
oved
forbo
thdo
sesan
dforall
timepo
ints
except
night
15in
the
3mg/da
ygrou
p.WASO
was
sign
ifican
tlyim
prov
edat
alltime
points
andin
both
dosa
gegrou
ps.
Rates
ofdiscon
tinu
ationweresimila
rbe
tweentrea
tmen
tarms:
placeb
o=
12%,D
XP3mg/da
y=12
%,D
XP
6mg/da
y=11
%.N
oclinically
meaning
fulchan
gesin
mea
nlaboratory
values,E
CGs,
body
weigh
t,or
vitalsign
s.
Low
-doseDXP
iseffective
atredu
cingsymptom
sof
insomnia.
DXP
seem
spa
rticularly
effectiveat
maintaining
sleep.
Lan
kfordet
al.
(201
2)65
+Primaryinsomniaby
DSM-IV-TR
4-wkRCT.DXP6mg/da
yvs.
placeb
o.N
=25
5.Sub
jectiveTST
(minute)
increa
sed
from
283.16
50.0
to34
6.16
66.4
atwee
k4in
theDXP
grou
pvs.an
increa
sefrom
293.56
49.1
to33
6.4
664
.7at
week4in
theplaceb
ogrou
p,P
,0.01
(DXP
sepa
rated
from
placeb
oon
this
mea
sure
byweek1).Sub
jectiveWASO
was
redu
cedrelative
toplaceb
oat
week
1(P
,0.00
01)an
dwee
k4
(P,
0.01
).
Rates
ofAEsweresimila
rbetw
een
grou
ps:2
7%forplaceboan
d31
%for
DXP6mg/da
y.Rates
ofdiscon
tinu
ationwerelower
forDXP:
placebo=10
%vs.D
XP6mg/da
y=5%
.Nochan
gesin
laboratory
values,
ECGs,body
weigh
t,ne
urologic
exam
inations,o
rvitalsign
s.
Low
-doseDXP
iseffective
atredu
cingsymptom
sof
insomnia.
NCT#0
0755
495
seeRam
elteon
section
Rothet
al.(20
07)
18–64
Chronicpr
imary
insomniaby
DSM-IV
Fou
r-grou
pcrossove
rRCTwith
2po
lysomno
grap
hic
assessmen
tnightspe
rtrea
tmen
t.DXP1mg/da
yvs.
3mg/da
yvs.6mg/da
yvs.
placeb
o.N
=67
.
For
themeasuremen
tof
LPS
(polysom
nograp
hy),no
neof
the
treatm
ents
werestatistically
better
than
placeboby
onean
alysis;a
statisticalre-an
alysispo
stho
cfoun
dP
=0.01
39forDXP6mg.Allthreedo
ses
improved
totalsleeptimerelative
toplacebo:P=0.00
05forDXP1mg/da
y,P,
0.00
01forDXP3mg/da
y,P,
0.00
01forDXP6mg/da
y.
AEsin
theDXP
grou
psoccu
rred
ata
similar
rate
ofthosein
theplaceb
ogrou
pan
ddidnot
appe
arto
bedo
se-
related.
Hea
dach
ean
dsomno
lenc
ewerethemostcommon
AEs.
Low
-doseDXP
iseffective
inthetrea
tmen
tof
insomnia.
Alldo
sesof
DXP
sign
ifican
tly
impr
oved
SE
duringthe
entire
nigh
t,ea
chon
eP,
0.05
.Only
DXP3mg/
dayan
dDXP
6mg/da
ysign
ifican
tlyim
prov
edwak
etimedu
ring
sleep.
Rothet
al.(20
10)
25–55
Hea
lthypa
rticipan
tsrequ
ired
tohav
eno
history
ofinsomnia
andnormal
slee
ppa
tterns
during
last
3mo.
Transien
tinsomnia
was
indu
ced
inpa
rticipan
ts.
OnenightRCT.DXP
6mg/da
yvs.placeb
o.N
=56
5.Bypo
lysomnog
raph
y:LPSwas
47.7
659
.5min
intheplaceb
ogrou
pan
d31
.86
44.0
min
intheDXP
grou
p,P
,0.00
01.TST
was
increa
sed
51.1
min
intheDXP
grou
prelative
totheplaceb
ogrou
p,P
,0.00
01.
Incide
nceof
AEswas
similar
toplaceb
o.Onon
emea
sure
ofne
xt-
dayresidu
aleffects(the
Digit
Sym
bolSub
stitutionTest)
there
was
nodifferen
cebe
tweenDXPan
dplaceb
o.How
ever,DXPresu
lted
instatisticallysign
ifican
tworsening
ontw
oothe
rscales,theSym
bol
Cop
yingTestan
dtheVisual
Analog
Scale
forsleepine
ss.
DXPis
effectiveat
redu
cing
symptom
sof
insomnia.
(con
tinued
)
228 Atkin et al.

(Foldvary-Schaefer et al., 2002). In mice, gabapentinalleviates sleep disturbances induced by a neuropathicpain-like condition (Takemura et al., 2011).
2. Indications. Gabapentin is FDA-approved for themanagement of postherpetic neuralgia in adults (USFDA, 2014c). It is FDA approved as adjunctive treat-ment of partial seizures with and without secondarygeneralization in patients over 12 years old withepilepsy and as adjunctive treatment of partial seizuresin patients aged 3–12. Clinical studies examining thehypnotic effects of gabapentin are detailed in Table 12.
3. Pharmacokinetics. The bioavailability of gaba-pentin is inversely proportional to its daily dose: asdosage increases, bioavailability decreases. The bio-availability of gabapentin is 60%, 47%, 34%, 33%, and27% following oral administration of 900, 1200, 2400,3600, and 4800 mg/day of the drug given in threedivided doses (US FDA, 2014c). Less than 3% ofgabapentin is bound to plasma protein, and the drugis not appreciably metabolized in humans. Its elimina-tion half-life is 5–7 hours and is unaltered by dose orfollowing multiple dosing. Taking the drug with foodhas a small effect on its pharmacokinetics, increasingAUC and Cmax by 14% each.
4. Results in Insomnia Disorder. One open-labeltrial conducted in patients with primary insomnia wasidentified (Lo et al., 2010). This study (N = 18; meandose of gabapentin 540 mg/day, range 200–900 mg/day)found polysomnographic evidence of increased sleepefficiency (80.00%–87.17%, P , 0.05) and SWS(10.47%–17.68%, P , 0.005) and decreased wake timeafter sleep onset (16.45%–7.84%, P , 0.05) (Lo et al.,2010). However, gabapentin did not significantly im-prove sleep onset latency (17.58–14.58 minutes, notsignificant).
5. Other Results. Five other studies of gabapentinwere identified. Two of the four studies were RCTs: onewas conducted in patients diagnosed with alcohol de-pendence and comorbid insomnia (Brower et al., 2008)and the other was a single-dose study conducted inpatients with “occasional disturbed sleep” (Rosenberget al., 2014). One open-label comparison study ofgabapentin versus trazodone conducted in patientswithalcohol dependence and “persistent insomnia” (Karam-Hage and Brower, 2003) and an open-label studyconducted in children suffering from refractory in-somnia comorbid to neurodevelopmental or neuro-psychiatric disorders (Robinson and Malow, 2013)were also identified. Finally, one study in healthysubjects was identified (Foldvary-Schaefer et al.,2002).
In the RCT conducted in patients with alcohol de-pendence and comorbid insomnia (N = 21; gabapentin1500 mg/day), treatment group did not predict changesin the Sleep Problems Questionnaire score (Broweret al., 2008). However, gabapentin treatment signifi-cantly reduced the risk of relapse to heavy drinking: at
TABLE
11—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Sch
arfet
al.
(200
8b)
65+
Primaryinsomnia
byDSM-IV
Fou
r-pe
riod
crossove
rRCT.
DXP
1vs.3vs.6mg/da
yvs.
placeb
o.N
=76
.
LPSwas
not
sign
ifican
tlydifferen
tfrom
placeb
oforan
ydo
seof
DXP.
How
ever,TST
andSE
were
sign
ifican
tlyincrea
sedrelative
toplaceb
oforalldo
ses,
P,
0.00
01.
Wak
etimedu
ring
sleepwere
sign
ifican
tlyredu
cedat
alldo
ses,
P,
0.00
01.
Num
berof
AEswas
similar
betw
een
placeb
oan
dDXP
andweresimilar
betw
eenDXP
doses.
Low
-doseDXP
iseffective
atredu
cingsymptom
sof
insomnia.
Italso
increa
sesSE.D
XPseem
spa
rticularly
effectiveat
maintaining
sleep.
Yeu
nget
al.
(201
5).18
Varied
Systematic
review
andmeta-
analysis
ofnine
placeb
o-controlled
RCTs.
Pooledresu
ltswerelargelyno
trepo
rted
dueto
heteroge
neity;
howev
er,theau
thorswereab
leto
conc
lude
thesign
ifican
tefficacy
and
safety
ofDXP3–
6mgforon
eto
two
nigh
ts.
Inyo
ungan
dmiddle-ag
edad
ults,the
incide
nce
ofan
yAEswere27
%,
35%,a
nd32
%in
placeb
o,DXP3mg/
day(R
R=1,27
,95
%CI=0.8,
2.1,
P=0.29
),an
dDXP
6mg/da
y(R
R=1.30
,95
%CI0.8,
2.1,
P=0.29
).Com
mon
AEswere
head
ache
,somno
lenc
e,an
dna
usea
.Results
inolde
rad
ults
weresimilar.
Low
-doseDXP
iseffective
atredu
cingsymptom
sof
insomnia.
Drugs for Insomnia beyond Benzodiazepines 229

TABLE
12Sum
maryof
stud
iesas
sessingtheeffectsof
gaba
pentin
(GBP)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Brower
etal.(200
8)18
+Alcoh
olde
pende
nce
withcomorbid
insomnia
6-wkRCT
plus2-wkplaceb
olead
-inan
dfollow
upvisit
after6wk.
GBP
1500
mg/
dayvs.placeb
o.N
=21
.
60%
ofGBP
grou
prelaps
edto
hea
vydr
inkingby
12wkvs.
100%
oftheplaceb
ogrou
p,P=
0.04
.Treatmen
tgrou
pdidno
tpr
edictch
ange
sin
Sleep
Problem
sQue
stionn
aire
(SPQ)
score.
The
rewereno
sign
ifican
tpo
lysomno
grap
hicdifferen
ces
betw
eengrou
ps.
The
mostcommon
side
effects
attributed
toga
bape
ntin
vs.
placeb
o,resp
ective
ly,were
somno
lenc
e(thr
eesu
bjects
vs.
onesu
bject),he
adache
(thr
eesu
bjects
inea
chgrou
p),
dizziness(twosu
bjects
vs.on
esu
bject),indige
stion(twovs.
four
subjects),ne
rveor
mus
cle
pain
(twosu
bjects
vs.non
e).
GBP
isno
teffectiveat
redu
cing
symptom
sof
insomnia,
thou
ghit
delaye
dtheon
setto
hea
vydr
inking.
Foldv
ary-Sch
aefer
etal.(20
02)
20–46
Hea
lthypa
rticipan
tsRan
domized
stud
y.GBP
titrated
to18
00mg/da
yvs.
untrea
tedgrou
p.N
=19
.
GBP-treated
subjects
hadan
increa
sein
SWScompa
redwith
baseline
.Nodifferen
cein
othe
rpo
lygrap
hicva
riab
les.
GBP
subjects
hadminor
redu
ctions
inarou
sals,a
wak
enings,a
ndstag
esh
ifts
was
observed
intrea
ted
subjects.
One
patien
tex
perien
ced
dizzinessat
high
estdo
sean
dwas
trea
tedwith15
00mg/da
y.
GBP
may
beeffectiveat
increa
singSWSwithou
taffectingothe
ras
pectsof
sleep.
Karam
-Hag
ean
dBrower
(200
3)mea
n:44
S.D.:
14DSM-IV
alcoho
lde
pende
ncewith
persistent
insomnia
4–6-wkop
en-lab
elstudy
.GBP
300–
1800
mg/da
yvs.
traz
odon
e25
–30
0mg/da
y.N
=55
.
Bothgrou
pssh
owed
sign
ifican
tim
prov
emen
tin
sleepfrom
baseline
tofollow
up,P
,0.00
1forea
chgrou
pas
mea
suredby
theSPQ.Total
chan
gein
SPQ
scores
betw
eenthegrou
ps:G
BP
grou
pim
prov
edby
8.86
4.0
while
traz
adon
egrou
pim
prov
ed6.16
3.4,
P=0.02
3.
Bothmed
ications
werewell-
tolerated.
GBPis
effectiveat
redu
cing
symptom
sof
insomnia
inalcoho
lism
and
sign
ifican
tlymore
effectivethan
traz
odon
e.
Loet
al.(201
0)mea
n:43
.2S.D
.:15
.4Primaryinsomnia
4-wkop
en-lab
elstudy
.GBP
200–
900mg/da
y.N
=18
.Bypo
lysomnog
raph
y:GBPdidnot
sign
ifican
tlyim
prov
eSOL,
which
decrea
sedfrom
17.58to
14.58min.GBP
impr
oved
SE
from
80.00%
to87
.17%
,P
,0.05
.WASO
was
sign
ifican
tly
redu
cedfrom
16.45%
to7.84
%,
P,
0.05
.Sleep
stag
eN3
increa
sedfrom
10.47%
to17
.68%
,P
,0.00
5.
Prolactin
leve
lswere
sign
ifican
tlyredu
cedafter
GBP
trea
tmen
t;whether
the
effect
occu
rred
asaresu
ltof
GBP
was
uncertain.
GBPis
effectiveat
redu
cing
symptom
sof
insomnia
andincrea
sesslow
-wav
esleep.
Rob
insonan
dMalow
(201
3)Ped
iatric:
mea
n7.2
Refractoryinsomniain
childr
enwith
neu
rode
velopm
ental
orneu
rops
ychiatric
disord
ers
Ope
n-lab
elstudy
.GBP
6–15
mg/kg
perda
y.N
=23
.
Impr
oved
sleepwas
notedin
78%
ofch
ildr
en.
AEsno
tedin
sixch
ildr
en,m
ostly
agitationan
dworsene
dab
ility
tosleep.
GBPis
effectiveat
redu
cing
symptom
sof
insomnia
inch
ildr
enwith
neu
rode
velopm
entalan
dne
urop
sych
iatric
disord
ers.
Rosen
berg
etal.
(201
4)18
andolde
rOccas
ional
distur
bed
sleep
RCT
usinga5-hph
ase
adva
nceinsomniamod
el.
GBP
250mgvs.GBP
500mgvs.placeb
o.N
=37
7.
LPSwas
notsign
ifican
tlydifferen
tam
onggrou
ps.Mea
ntotalsleep
timewas
sign
ifican
tlygrea
ter
forthega
bape
ntin
grou
ps:3
11.4
68.4min
inplaceb
ogrou
p,35
6.56
7.5min
inGBP25
0mg,
and37
8.8min
inGBP
500mg
grou
p.Percent
slow
-wav
esleep
was
sign
ifican
tlygrea
terin
GBP
grou
ps,12
.6%,15
.4%,an
d17
.0%,resp
ective
ly.
4.2%
ofpa
rticipan
tsrepo
rted
atleas
ton
eAE,with1.6%
ofplaceb
opa
rticipan
ts,4.0%
ofGBP
250mg/da
ypa
rticipan
ts,
and7.2%
GBP
500mg/da
y.Themostcommon
AE
was
hea
dach
e.
GBPis
effectiveat
redu
cing
symptom
sof
insomnia
andincrea
sesslow
-wav
esleep.
230 Atkin et al.
12 weeks, 60% of the gabapentin group had relapsedcompared with 100% of the placebo group. Similarly, inthe single-dose study using a 5-hour phase advancemodel in patients with “occasional disturbed sleep,”gabapentin 250 mg/day and gabapentin 500 mg/daywere not significantly superior to placebo at reducinglatency to persistent sleep. However, the mean totalsleep time was significantly greater for the gabapentingroups: 311.4 [8.4] min in the placebo group versus356.5 [7.5]min in the gabapentin 250mg/day group (P#0.001 compared with placebo) and 378.7 [7.3] min in thegabapentin 500mg/day group (P# 0.001 comparedwithplacebo, P # 0.01 compared with gabapentin 250 mg/day). Wake after sleep onset was significantly improvedin the gabapentin groups, as was the proportion of timespent in SWS (stages 3 and 4) (Rosenberg et al., 2014).Finally, in the open-label comparison study of gabapen-tin and trazodone in alcoholism, gabapentin was signif-icantly more effective.6. Conclusion. A summary of the effects of gabapen-
tin on sleep architecture is presented in Table 2. Thereis some evidence that gabapentin is effective in thetreatment of insomnia disorder according to one open-label trial, although it did not significantly improvesleep onset latency (Lo et al., 2010).
B. Pregabalin
1. Mechanism of Action. Similar to gabapentin,pregabalin binds to a2d subunit-containing voltage-gated calcium channels (Taylor et al., 2007). Pregabalinalso modulates the influx of calcium at nerve terminals,which may accounts for its therapeutic benefit inneuropathic pain, seizures, and anxiety. The mecha-nism of action of pregabalin (Table 1) in improving sleephas not been completely elucidated, but it is known to bedifferent from benzodiazepines as pregabalin is notactive at GABA-A or benzodiazepine receptors (Tayloret al., 2007). Furthermore, although benzodiazepinestypically reduce SWS, pregabalin has been found toincrease it (Hindmarch et al., 2005). In rats, pregabalinhas been found to increase NREMS and REMS, whilemarkedly increasing the duration of NREMS episodesand reducing their number (Kubota et al., 2001). In onestudy, pregabalin increased NREMS in mice with aneuropathic pain-like condition, but not normal mice(Wang et al., 2015).2. Indications. Pregabalin is FDA approved for the
management of neuropathic pain associated with di-abetic peripheral neuropathy, the management of post-herpetic neuralgia, adjunctive therapy for adultpatients with partial onset seizures, the managementof fibromyalgia, and the management of neuropathicpain associated with spinal cord injury (US FDA, 2016).Clinical studies examining the hypnotic effects ofgabapentin are detailed in Table 13.3. Pharmacokinetics. Following oral administra-
tion, peak plasma concentrations of pregabalin occur
within 1.5 hours; its bioavailability is greater than orequal to 90% and is independent of dose (US FDA,2016). The half-life of pregabalin is about 6 hours.Taking pregabalin with food increases Tmax to approx-imately 3 hours and reduces Cmax by 25%–30%, al-though pregabalin can be taken with or without food. Itdoes not bind to plasma proteins and undergoes negli-gible metabolism in humans (US FDA, 2016). Oralclearance tends to decrease with increasing age.
4. Results in Insomnia Disorder. No studies ofpregabalin as a treatment of insomnia disorder wereidentified.
5. Other Results. Three reviews were found analyz-ing the use of pregabalin in patients with insomnia: intwo, patients were primarily diagnosed with general-ized anxiety disorder (Montgomery et al., 2009;Holsboer-Trachsler and Prieto, 2013), and in one,patients were primarily diagnosed with fibromyalgia(Russell et al., 2009). In the most recent review, pooleddata from four RCTs (N = 1354) established that amongpatients with severe difficulty in falling asleep, re-mission was observed in 54.0% of the pregabalin groupversus 29.8% of placebo group (Holsboer-Trachsler andPrieto, 2013). In those with severe difficulty in stayingasleep, remission was observed in 54.2% of pregabalingroup versus 26.7% of placebo group. Finally, in thosewith severe difficulty associated with waking up tooearly, remission was observed in 59.4% of pregabalingroup versus 34.6% of placebo group. The fibromyalgiastudy (N = 1493, two RCTs) likewise found thatpregabalin was significantly superior to placebo inreducing the burden of insomnia symptoms as mea-sured using the Sleep Quality Diary and MedicalOutcomes Study Subscales of Sleep Disturbance, Quan-tity of Sleep, and Sleep Problems Index (Russell et al.,2009). For more information about these psychometricscales, see Smith and Wegener (2003).
6. Conclusion. A summary of the effects of pregaba-lin on sleep architecture is presented in Table 2. Thereis good evidence based on two reviews (Montgomeryet al., 2009; Holsboer-Trachsler and Prieto, 2013) thatpregabalin is effective at reducing symptoms of in-somnia in generalized anxiety disorder. There is alsogood evidence based on one review (Russell et al., 2009)that pregabalin is effective at reducing symptoms ofinsomnia in fibromyalgia. Based on these same reviews,there is weak evidence that pregabalin is effective in thetreatment of insomnia disorder.
VIII. Atypical Antipsychotic Drugs
Sedating atypical antipsychotics, particularly quetia-pine, are often used in the clinic for the management ofinsomnia disorder and insomnia symptoms that occurcomorbid to psychiatric illness (Pringsheim and Gard-ner, 2014). Although they are effective in the manage-ment of bipolar and psychotic disorders, systematic
Drugs for Insomnia beyond Benzodiazepines 231

TABLE
13Sum
maryof
stud
iesas
sessingtheeffectsof
preg
abalin
(PGB)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
DeHaa
set
al.(20
07)
19–67
Epileps
yan
dsu
bjective
sleep
distur
banc
es
4-wkRCTpa
rallel-group
stud
y.PGB
300mg/da
ytw
iceada
yvs.placeb
otw
iceada
y.N
=17
.
PGB
hadpo
sitive
effect
ondistur
bedsleepba
sedon
subjective
assessmen
ts(que
stionn
aires)
butnot
onpo
lysomno
grap
hicmea
sures.
PSG
redu
cedon
lythenu
mbe
rof
awak
enings
(P=0.04
vs.
placeb
o).
Mildto
mod
erate.
Hea
dach
ewas
themostfreq
uen
tAE.Other
AEsweredizzinessan
dsomno
lenc
e.
PGB
impr
oves
sleepcontinuity
andsu
bjective
sleepqu
ality
inep
ilep
ticpa
tien
tswith
sleepcomplaints.
Hindm
arch
etal.
(200
5)18
–50
Hea
lthyad
ult
volunteers
Ran
domized
,do
uble-blind
,placeb
o-an
dactive
-controlled
,three-way
crossove
r.PGB
150mgthree
times
ada
yvs.alpr
azolam
1mgthreetimes
ada
yvs.
placeb
othreetimes
ada
yfor
3da
ys.N
=24
.
PGB
increa
sedTST,stag
eN3,
andsleepefficien
cy,an
dde
crea
sedSOL
andREM
sleep.
NS
PGB
hassign
ifican
teffectson
thesleepof
healthyhu
man
sthat
aredifferen
tfrom
those
ofBZD
;pa
rticularly,it
increa
sesSWSan
dsleep
continuity.
Holsb
oer-Trach
sler
etal.(20
13)
NS
Gen
eralized
anxiety
disord
erRev
iew
ofseve
nRCTs.
PGB
150–
600mg/da
yvs.placeb
o.Pooledremission
data
ininsomniasymptom
sfrom
four
4–6wkRCTs(N
=13
54):
“Sev
ere”
difficulty
offalling
asleep
,remission
observed
in54
.0%
ofPGB
grou
pvs.29
.8%
ofplaceb
ogrou
p;“sev
ere”
difficulty
instay
ingas
leep
,remission
observed
in54
.2%
ofPGB
grou
pvs.26
.7%
ofplaceb
ogrou
p;“sev
ere”
difficulty
withwak
inguptoo
early,
remission
observed
in59
.4%
ofPGB
grou
pvs.34
.6%
ofplaceb
ogrou
p.
Mostfreq
uent
adve
rseeffects,
like
somno
lenc
ean
ddizziness,
are
mostcommon
infirst2wkof
therap
y.The
incide
nceof
somno
lenc
eas
anAEin
patien
tswithmod
erateto
seve
reinsomniawas
lower
than
for
benz
odiazepine
s:PGB
150mg/
day:
24.4%,PGB
300-45
0mg/
day:
26.2%,PGB
600mg/da
y:31
.5%,alpr
azolam
/lorazepa
m:
54.2%,placeb
o:7.8%
.
PGB
iseffectiveat
redu
cing
symptom
sof
insomnia
inge
neralizedan
xietydisord
er.
Mon
tgom
eryet
al.
(200
9)Gen
eralized
anxiety
disord
erRev
iew
ofsixRCTs.
N=18
54.
Inpa
tien
tspr
esen
ting
withhigh
insomnia,
PGB
prod
uced
sign
ifican
tlygrea
ter
impr
ovem
enton
HAM-A
total
scores:PGB
300–
450mg/da
y(2
13.1
60.6);PGB
600mg/
day(2
11.2
60.5)
dose
grou
pscompa
redwithplaceb
o(2
8.36
0.5;
P,
0.00
01for
both
compa
risons
).PGB
150mg/da
ywas
not
sign
ifican
t(2
9.96
0.7;
P=0.05
1).
Total
discon
tinu
ations
werelower
than
placeb
o(25.9%
)for
preg
abalin
150mg/da
y(16.4%
)an
d30
0–45
0mg/da
y(16.4%
),no
nsignificantly
high
erfor
preg
abalin
600mg(27.6%
),an
dsign
ifican
tlyhigh
erfor
alpr
azolam
/lorazepa
m(38.0%
,resp
ective
ly;P
,0.05
.
PGB
300–
600mg/da
yis
effectiveat
redu
cing
symptom
sof
anxietyin
patien
tspr
esen
ting
with
gene
ralizedan
xietydisord
erwithhigh
leve
lsof
insomnia.
Russellet
al.(200
9)18
+Fibromya
lgia
Rev
iew
oftw
oRCTs.
PGB
300,
450,
or60
0mg/da
yvs.
placeb
o.N
=14
93.
Bothstud
iesfoun
dsign
ifican
tim
prov
emen
tin
PGB
grou
prelative
toplaceb
ogrou
pon
:Sleep
Qua
lity
Diary
andMOS
Sub
scales
ofSleep
Disturban
ce,Qua
ntityof
Sleep
,an
dSleep
Problem
sIn
dex.
Pooledresu
ltsno
tlisted
.
Not
analyz
ed.
PGB
iseffectiveat
redu
cing
symptom
sof
insomnia
infibrom
yalgia.
232 Atkin et al.

reviews have found a lack of evidence for the use ofsedating atypical antipsychotics and explicitly recom-mend against prescribing them for insomnia disorder(Thompson et al., 2016). The 2016meta-analysis acknowl-edges that the use of atypical antipsychotics may beappropriate in patients who have failed other treatmentmodalities and who have a comorbid condition that couldbenefit from the primary action of the drug (based onconsensus of experts in sleep medicine). Similarly, guide-lines for the treatment of chronic insomnia report in-sufficient evidence for atypical antipsychotics as first-linetherapy (Schutte-Rodin et al., 2008), but state that themedications may be suitable for patients with comorbidinsomnia who may benefit from the primary action ofthese drugs as well as from the sedating effect.
A. Olanzapine
1. Mechanism of Action. Olanzapine is an atypicalantipsychotic with affinity for the dopamine D1, D2, andD4 receptors; the serotonin 5-HT2A, 5-HT2C, and 5-HT3
receptors; the a1-adrenergic receptor; the histamine H1
receptor; and five muscarinic receptor subtypes(Bymaster et al., 1996). Its hypnotic effects are probablyattributable to its strong antagonism of the H1 antag-onism as well as its antagonism of serotonin receptors.In an assay of compounds tested at the histamine H1
receptor, olanzapine was the most potent compoundRichelsen and Souder (2000) had tested of any class ofcompounds. Olanzapine seems to specifically increaseSWS (Salin-Pascual et al., 1999; Giménez et al., 2007;Kluge et al., 2014). Main molecular targets of olanza-pine are summarized in Table 1.2. Indications. Olanzapine is FDA approved for the
treatment of schizophrenia in adults and adolescents;for the acute treatment of manic or mixed episodesassociated with bipolar I disorder and the maintenancetreatment of bipolar I disorder in adults and adoles-cents; and, as an intramuscular injection, for thetreatment of acute agitation associated with schizo-phrenia and bipolar I mania (US FDA, 2009). Clinicalstudies examining the hypnotic effects of olanzapine aredetailed in Table 14.3. Pharmacokinetics. Olanzapine reaches peak con-
centrations about 6 hours following oral administration,and its elimination half-life ranges from 21 to 54 hours,with a mean of 30 hours (US FDA, 2009). It is eliminatedextensively by first-passmetabolism: about 40% of an oraldose is metabolized before it reaches the systemic circu-lation. Olanzapine is extensivelymetabolized byCYP1A2,CYP2D6, and the flavinmonooxygenase system, althoughits metabolites do not display pharmacological activity atnormal concentrations (US FDA, 2009). Its pharmacoki-netics are not affected by food. The drug is 93% bound toplasma protein. Clearance of olanzapine is approximately30% lower in women than in men, and the eliminationhalf-life of olanzapine is about 1.5 times higher in subjectsgreater than 65 years old.
4. Results in Insomnia Disorder. No studies ofolanzapine as a treatment of insomnia disorder wereidentified.
5. Other Results. Two studies that examined olan-zapine’s effect on sleep (Salin-Pascual et al., 1999;Sharpley et al., 2000) and three studies on olanzapineas a treatment of secondary insomnia were identified(Jakovljevi�c et al., 2003; Khazaie et al., 2010, 2013). Ofthe studies analyzing olanzapine’s effect on sleep, bothwere small: one was an open-label study conducted in20 patients with schizophrenia, during which polysom-nographic recordings were taken for 5 days, withpatients only receiving olanzapine on two nights(Salin-Pascual et al., 1999) and one was a one-dosecrossover RCT conducted in nine healthy male partic-ipants, with 7–14 days washout between doses(Sharpley et al., 2000). The crossover RCT examinedolanzapine 5, 10 mg/day or placebo, whereas the studyin patients with schizophrenia examined olanzapine10 mg/day. Both studies found that olanzapine pro-foundly increased slow-wave sleep and increased totalsleep time as acute treatment.
Of the studies in secondary insomnia, one was con-ducted in patients suffering from treatment-resistantposttraumatic stress disorder (PTSD) (Jakovljevi�c et al.,2003), whereas the other two were in patients withparadoxical insomnia, also known as sleep state mis-perception (Khazaie et al., 2010, 2013). The first studywas in patients suffering from intractable PTSD inwhich open-label olanzapine was added to their currentmedications (Jakovljevi�c et al., 2003). The patients hadrecurrent nightmares and insomnia resistant to numer-ousmedications. In all five cases, olanzapine resulted ina significant improvement in their symptoms. Onerandomized, open-label studywas conducted in patientsdiagnosed with paradoxical insomnia, or sleep-statemisperception (Khazaie et al., 2013). Patients sufferingfrom this disorder complain of difficulties with initiat-ing and maintaining sleep; however, the hallmark ofparadoxical insomnia is that objective polysomno-graphic measures find that the patients are gettingsufficient sleep. In this study, the investigators followedup on a case report study they had published in 2010 -(Khazaie et al., 2010), in which they reported successfultreatment of recalcitrant, paradoxical insomnia witholanzapine in a single patient. The group’s larger studycompared treatment with two different atypical anti-psychotics: olanzapine and risperidone. They foundthat, although both treatments were associated withsignificant improvements in subjective sleep quality,olanzapine was significantly superior to risperidone, asmeasured using the Pittsburgh Sleep Quality Index(PSQI) (Buysse et al., 1989).
6. Conclusion. A summary of the effects of olanza-pine on sleep architecture is presented in Table 2. Thereis weak evidence that olanzapine acutely increasesslow-wave sleep and total sleep time (Salin-Pascual
Drugs for Insomnia beyond Benzodiazepines 233

TABLE
14Sum
maryof
stud
iesas
sessingtheeffectsof
olan
zapine
(OLA)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Jako
vljevi� cet
al.
(200
3)28
–50
Treatmen
t-resistan
tPTSD
withnigh
tmares
andinsomnia
Cas
eseries.OLA
adde
dto
curren
ttrea
tmen
tregimen
.N
=5.
Allfive
patien
tsim
prov
edrapidly
aftertrea
tmen
tinitiation
with
olan
zapine.
NoAEswererepo
rted
.OLA
may
beeffectiveat
redu
cing
sleep
distur
banc
esin
PTSD.
Kha
zaie
etal.(20
13)
60Parad
oxical
insomnia
Cas
erepo
rt.OLA
5mg/da
yad
dedto
trea
tmen
tregimen
.N
=1.
After
6wk,
OLA
trea
tmen
tresu
lted
incompleteremission
ofsymptom
s.
Non
elisted
.OLA
may
beeffectiveat
redu
cingsymptom
sof
parado
xicalinsomnia.
Kha
zaie
etal.(20
13)
Mea
n:53
.4;
S.D
.:14
.4Parad
oxical
insomnia
8-wkrand
omized
,op
en-lab
eltrial.OLA
10mg/da
yvs.
risp
eridon
e4mg/da
y.N
=29
.
Sleep
qualitymea
suredwiththe
Pittsbu
rghSleep
Qua
lity
Inve
ntorysh
owed
sign
ifican
tim
prov
emen
tin
both
trea
tmen
tgrou
ps,thou
ghim
prov
emen
tin
OLA
grou
pwas
supe
rior
torisp
eridon
egrou
p.In
OLA
grou
p,ba
selinemea
nwas
11.8
62.3an
dtrea
tmen
tmea
nwas
2.66
1.6,
P,
0.00
1.In
risp
eridon
egrou
p,ba
seline
mea
nwas
11.1
62.4an
dtrea
tmen
tmea
nwas
56
3.8,
P,
0.00
1.Betweengrou
pscompa
risonyielde
dP
,0.04
.
NoAEswererepo
rted
.OLA
iseffectiveat
redu
cingsymptom
sof
parado
xicalinsomnia.
Kluge
etal.(20
14)
18–65
Sch
izop
hrenia
andreview
oftheliterature
6-wkRCTsing
lecenter.O
LA
5-25
mg/da
yvs.clozap
ine
100–
400mg/da
y.During
thefirst2wk,
thedo
serang
ewas
restricted
(OLA
10–15
mg/da
y,clozap
ine
25–20
0mg/da
y).N
=30
.
OLA
andclozap
ineincrea
sedTST
andsleepefficien
cy,an
dde
crea
sedSOL.Con
cern
ing
sleepstag
es,OLA
increa
sed
SWSan
dde
crea
sedREM
slee
p.
Noclinically
releva
ntsymptom
sof
restless
legs
synd
romewere
observed
.Noothe
rAEswerean
alyz
ed.
OLA
iseffectivein
impr
ovingsleepin
patien
tswith
schizop
hrenia.
Salin-Pas
qual
etal.
(199
9)Mea
n:33
.6;
S.D
.:10
.7Sch
izop
hren
iaFive-nigh
top
en-lab
elpo
lysomno
grap
hicstud
ywithOLA
10mg/da
yad
ministeredfortw
onigh
ts.N
=20
.
OLA
enha
nced
slow
wav
esleep
andincrea
sedtotalsleeptime.
REM
dens
ityincrea
sedan
dstag
e1de
crea
sedwithOLA.
Non
elisted
.OLA
may
increa
seslow
wav
eslee
pan
dtotal
sleeptimein
schizop
hrenia.
Sharpley
etal.
(200
0)33
–60
Hea
lthysu
bjects
One
-dosecrossove
rRCT.
OLA
5mg/da
yvs.OLA
10mg/da
yvs.placeb
o.N
=9.
OLA
subs
tantiallyincrea
sedslow
wav
esleep,
by59
.1%
and83
.3%
forthe5an
d10
mg/da
ydo
ses,
resp
ective
ly.OLA
increa
sed
totalsleeptime.
Non
elisted
.OLA
increa
sesslow
wav
eslee
pan
dtotal
sleeptimein
healthy
subjects.
234 Atkin et al.

et al., 1999; Sharpley et al., 2000), although this effecthas not been confirmed in patients with insomnia.There is also evidence that olanzapine may be usefulin 1) the treatment of insomnia associated with PTSD(Jakovljevi�c et al., 2003) based on a case series and 2)paradoxical insomnia, based on a case report (Khazaieet al., 2010) and a randomized, open-label trial (Khazaieet al., 2013).
B. Quetiapine
1. Mechanism of Action. Quetiapine, a dibenzothia-zepine derivative, is the atypical antipsychotic thatdisplays the lowest D2 affinities (Richelson and Souder,2000; Comai et al., 2012b). It shows antagonism atmultiple neurotransmitter receptors, mainly 5-HT2A,5-HT2c, H1, and D2 (Table 1). Its sedative and hypnoticproperties are attributable to its antagonism of thehistamine H1 receptor and various serotonin receptors.Inmonkeys, neither acute nor chronic administration ofquetiapine improved sleep efficiency, whereas the firstnight after discontinuation, subjects had significantlydecreased sleep efficiency and increases in nighttimeactivity (Brutcher and Nader, 2015).2. Indications. Quetiapine is FDA approved for the
treatment of schizophrenia in adults and adolescents,the treatment of bipolar mania in children and adoles-cents, and the treatment of bipolar depression in adults.Clinical studies examining the hypnotic effects ofquetiapine are detailed in Table 15.3. Pharmacokinetics. Quetiapine fumarate is rap-
idly absorbed after oral administration, reaching peakplasma concentrations within 1.5 hours (US FDA,2017). The drug is 83% bound to serum proteins(DeVane and Nemeroff, 2001). Administration withfood increases Cmax and AUC by 25% and 15%, re-spectively. The drug is mainly eliminated throughhepatic metabolism, specifically CYP3A4, and itsmean terminal elimination half-life is 6 hours. Oralclearance is reduced by 40% in subjects greater than65 years of age, although sex does not affect itspharmacokinetics.4. Results in Insomnia Disorder. One RCT was
identified in patients diagnosed with primary insomnia(Tassniyom et al., 2010). Surprisingly, although obser-vational evidence suggests that atypical antipsychoticslike quetiapine are increasingly prescribed for insom-nia, the 2010 study was the only RCT that was found inthe literature of an atypical antipsychotic in primaryinsomnia, and it had a small sample size of only13 patients who completed the study (Tassniyomet al., 2010). In the RCT, quetiapine 25 mg/day treat-ment was not significantly superior to placebo at in-creasing sleep time and reducing latency to sleep,although there was a trend toward the superiority ofquetiapine (Tassniyom et al., 2010).In contrast, an open-label trial of quetiapine 25–
75 mg/day found that the drug was effective at reducing
symptoms of insomnia, increasing total sleep time andreducing PSQI (Wiegand et al., 2008).
5. Other Results. Eleven other studies of quetiapinethat included sleep parameters were identified: fivewere open label (Juri et al., 2005; Todder et al., 2006;Baune et al., 2007; Pasquini et al., 2009), three wererandomized, placebo-controlled trials (Cohrs et al.,2004; Garakani et al., 2008; McElroy et al., 2010), onewas a review (Anderson and Vande Griend, 2014)pooling many of the studies cited here, one was anaturalistic study (�Sagud et al., 2006), one was a posthoc analysis of two RCTs (Endicott et al., 2008), and onewas a retrospective study (Terán et al., 2008).
One RCT in 14 healthy male subjects found thatquetiapine 25 and 100 mg/day significantly improvedsleep induction and sleep continuity under standardand acoustic stress conditions (Cohrs et al., 2004).Active treatment with quetiapine also increased totalsleep time, sleep efficiency, and subjective sleepquality.
In contrast to the results of the RCT in primaryinsomnia, the open-label studies in other conditionswere generally positive, although they were conductedin a wide range of patient populations. The includedstudies analyzed patients diagnosed with Parkinson’sdisease, treatment-resistant depression, bipolar disor-der, breast cancer with tamoxifen-induced insomnia,and insomnia induced by detoxification from substanceabuse. Unfortunately, a retrospective chart review (N =43) found that quetiapine prescribed for insomnia at amean dose of 120.3 6 58.6 mg/day had adverse meta-bolic side effects (Cates et al., 2009). However, neitherthe RCT of quetiapine 25 mg/day study (Tassniyomet al., 2010) nor the open-label trial of quetiapine 25–75 mg/day (Wiegand et al., 2008) reported the rate ofmetabolic side effects, and the retrospective review didnot perform subgroup analysis of the patients taking25 mg/day (N = 4 at baseline).
6. Conclusion. A summary of the effects of quetia-pine on sleep architecture is presented in Table 2.There is moderate evidence that quetiapine is notsignificantly effective for the treatment of primaryinsomnia, based on one small RCT (Tassniyom et al.,2010). Randomized studies support the usefulness ofquetiapine in insomnia that is secondary to conditionsfor which quetiapine has an FDA-approved indication,like bipolar depression or unipolar depression (asaugmentation). There is Level 1b evidence based ontwo RCTs (Calabrese et al., 2005; McElroy et al., 2010)that quetiapine is effective in the treatment of in-somnia secondary to bipolar depression. There is Level1b evidence based on one RCT (Garakani et al., 2008)and three open-label trials (�Sagud et al., 2006; Todderet al., 2006; Baune et al., 2007) that quetiapine asaugmentation of antidepressants is effective in re-ducing symptoms of insomnia in treatment-resistantdepression.
Drugs for Insomnia beyond Benzodiazepines 235

TABLE
15Sum
maryof
stud
iesas
sessingtheeffectsof
quetiapine
(QTP)on
sleep
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Ande
rson
and
Van
deGrien
d(201
4)
Varied
Varied
Rev
iew
oftheliterature
ofqu
etiapine
inthetrea
tmen
tof
insomnia.
Varied
Given
QTP’sad
verseeffects
profile(see
RCTsab
ove),
QTP’sbe
nefits
have
not
been
prov
ento
outw
eigh
therisk
.
Rob
uststud
iesev
alua
ting
quetiapineforinsomnia
arelack
ing.
Bau
neet
al.(20
07)
Males:mea
n48
.6,S
.D.1
2.9;
Fem
ales:m
ean
50.5,S.D
.13.2
Treatmen
t-resistan
tun
ipolar
orbipo
lar
IIde
pression
4-wkop
en-lab
elin-patient
trial
ofQTP
augm
entation
ofve
nlafax
ineor
escitalopr
am.
Mea
nQTPdo
se34
0mg/da
y,max
800mg/da
y.N
=27
.
PSQItotalscorewas
8.86
2.8at
baseline
and5.26
1.8at
week4,
P=0.00
.PSQIda
ytim
esleepine
sswas
1.96
0.8at
baseline
and0.8
60.7at
week4,
P=0.00
.
Duringthe4-wkstudy
,ne
ithe
rad
verse
metab
olic
orclinical
even
tsno
rsign
ifican
tweigh
tga
inwere
record
ed.
QTPis
effectiveat
redu
cing
symptom
sof
insomniain
patien
tswithde
pression
.
Calab
rese
etal.
(200
5)18
–65
Typ
eIor
Typ
eII
bipo
larde
pression
8-wkRCT.QTP
300vs.
600mg/da
yvs.placeb
o.N
=54
2.
Sleep
difficulties
weremod
erateto
seve
reat
baseline
.PSQItotal
scoreat
last
assessmen
tim
prov
edby
5.16
points
withQTP30
0mg/
dayan
d5.46
points
withQTP
600mg/da
y,compa
redwith2.94
points
forplaceb
o,P
,0.00
1for
both
dosa
gesrelative
toplaceb
o.
QTP60
0mg/da
yex
perien
ced1.6kg
ofweigh
tga
invs.1.0kg
inthe30
0mg/da
ygrou
pan
d0.2kg
intheplaceb
ogrou
p.Mea
nch
ange
infastinggluc
osewas
66
17mg/dl
inQTP
600mg/
day,
36
13mg/dl
inQTP
300mg/da
y,an
d46
26mg/dl
intheplaceb
ogrou
p.
QTPis
effectiveat
redu
cing
symptom
sof
insomniain
bipo
larde
pression
.
Coh
rset
al.(20
04)
19–33
Hea
lthysu
bjects
Nine-nightRCT.Threestudy
period
slasting3da
ys,w
itha
4da
ywas
hout.QTP25
mg/
dayvs.QTP
100mg/da
yvs.
placeb
o.N
=14
.
Bothdo
sesQTPsign
ifican
tly
impr
oved
LOSan
dsleep
continuityunde
rstan
dard
and
acou
stic
stress
cond
itions
.Total
sleeptimean
dSE
increa
sed.
Significant
increa
sein
period
iclegmov
emen
tswas
observed
withQTP
100mg/da
y.
QTPincrea
sessleepin
healthyvo
lunteers.
Garak
aniet
al.
(200
8)18
–65
Major
depr
essive
disord
er8-wkRCT.Q
TP25
–10
0mg/da
y+fluo
xetine
20–40
mg/da
yvs.placeb
o+fluo
xetine
.N
=11
4.
Mixed
-effectregression
mod
elssh
owthat
QTP+fluox
etinegrou
pim
prov
edsign
ifican
tlymore
rapidlyon
insomniascores.From
baseline
tofirstfollow
upvisit,P=
0.00
055;
tosecond
follow
upvisit,
P=0.00
04;tothirdfollow
upvisit,
P=0.01
.
Sed
ationwas
more
prev
alen
tin
theQTP
+fluox
etinegrou
p,P
=0.00
6.
QTPis
effectivein
redu
cing
symptom
sof
insomniain
patien
tswithde
pression
.
Keshav
anet
al.
(200
7)QTP
grou
p:mea
n36
.1,
S.D
.9.8
Sch
izop
hren
iaCross-section
al,QTP31
3.33
622
8.71
mg,
vs.risp
eridon
e3.25
62.12
vs.ne
urolep
tic-
naïvepa
tien
ts.N
=39
(patientsalread
ystab
ilized
onQTPor
risp
eridon
e),N
=31
(neu
roleptic-naïve
patien
ts)
REM
coun
tswereelev
ated
inthe
QTPthan
inne
urolep
tic-na
ïve
patien
ts.QTPan
drisp
eridon
etrea
tedpa
tien
tsha
dmore
prom
inen
tSWSan
d%
ofstag
eN2,
andredu
cedREM
slee
pthan
neve
r-trea
tedschizoph
renia
subjects.
Not
analyz
ed.
QTPsu
ppresses
REM
slee
pin
patien
tswith
schizoph
renia.
Its
therap
euticsign
ifican
cerequ
ires
furthe
rinve
stigation.
Juri
etal.(20
05)
Mea
n:67
.6,
S.D
.:8.4
Parkins
on’sdiseas
ewitho
utps
ycho
sis
withinsomnia
12-w
kop
en-lab
eltrial.Mea
nQTPdo
se31
.9mg/da
y,range
12.5–50
mg/da
y.N
=14
.
PSQIredu
cedby
mea
n6
S.D
.3.8
63.9,
P,
0.01
.SOL
redu
cedfrom
826
65.4
minutes
to28
.66
22.7
onlast
visit,P
,0.05
.
Twodiscon
tinuationsdu
eto
restless
legs
synd
rome
that
worsened
since
the
beginn
ingof
trea
tmen
t.Twosu
bjects
also
repo
rted
worsene
dsleepine
ssdu
ring
the
day.
Noworseningof
motor
symptom
sor
orthostaticsymptom
s.
QTPis
effectiveat
redu
cing
symptom
sof
insomniain
Parkinson’sdiseas
epa
tien
tswithinsomnia.
(con
tinued
)
236 Atkin et al.
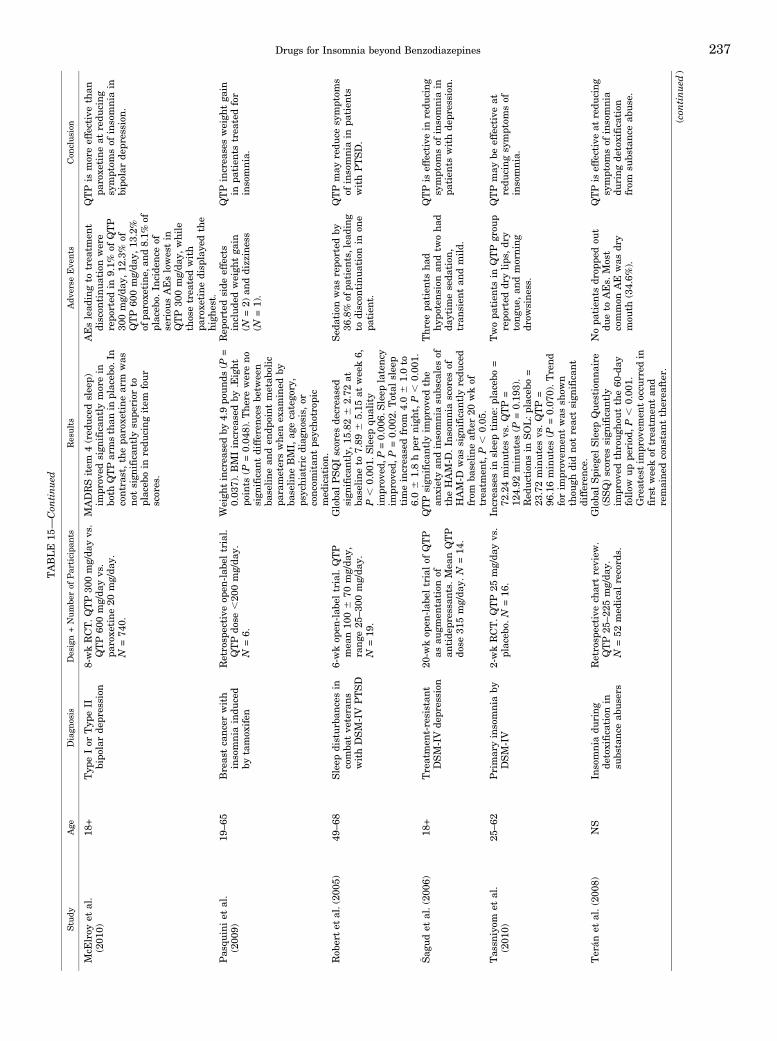
TABLE
15—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
McE
lroy
etal.
(201
0)18
+Typ
eIor
Typ
eII
bipo
larde
pression
8-wkRCT.Q
TP30
0mg/da
yvs.
QTP60
0mg/da
yvs.
paroxe
tine20
mg/da
y.N
=74
0.
MADRSitem
4(red
uced
sleep)
impr
oved
sign
ifican
tlymorein
both
QTParmsthan
inplaceb
o.In
contrast,thepa
roxe
tine
arm
was
notsign
ifican
tlysu
perior
toplaceb
oin
redu
cing
item
four
scores.
AEslead
ingto
trea
tmen
tdiscon
tinu
ationwere
repo
rted
in9.1%
ofQTP
300mg/da
y,12
.3%
ofQTP
600mg/da
y,13
.2%
ofpa
roxe
tine
,and
8.1%
ofplaceb
o.In
cide
nceof
seriou
sAEslowestin
QTP
300mg/da
y,while
thosetrea
tedwith
paroxe
tine
disp
laye
dthe
high
est.
QTPis
moreeffectivethan
paroxe
tine
atredu
cing
symptom
sof
insomniain
bipo
larde
pression
.
Pas
quiniet
al.
(200
9)19
–65
Breas
tcanc
erwith
insomnia
indu
ced
bytamox
ifen
Retrosp
ective
open
-lab
eltrial.
QTPdo
se,20
0mg/da
y.N
=6.
Weigh
tincrea
sedby
4.9po
unds
(P=
0.03
7).BMIincrea
sedby
.Eight
points
(P=0.04
8).The
rewereno
sign
ifican
tdifferen
cesbe
tween
baseline
anden
dpoint
metab
olic
parameterswhen
exam
ined
byba
seline
BMI,
agecatego
ry,
psychiatricdiag
nosis,
orconc
omitan
tps
ycho
trop
icmed
ication.
Rep
ortedside
effects
includ
edweigh
tga
in(N
=2)
anddizziness
(N=1).
QTPincrea
sesweigh
tga
inin
patien
tstrea
tedfor
insomnia.
Rob
ertet
al.(20
05)
49–68
Sleep
disturban
cesin
comba
tve
terans
withDSM-IV
PTSD
6-wkop
en-lab
eltrial.QTP
mea
n10
06
70mg/da
y,rang
e25
–30
0mg/da
y.N
=19
.
Globa
lPSQIscores
decrea
sed
sign
ifican
tly,
15.826
2.72
atba
seline
to7.89
65.15
atweek6,
P,
0.00
1.Sleep
quality
impr
oved
,P=0.00
6.Sleep
latenc
yim
prov
ed,P
=0.00
2.Total
sleep
timeincrea
sedfrom
4.06
1.0to
6.06
1.8hpe
rnigh
t,P
,0.00
1.
Sed
ationwas
repo
rted
by36
.8%
ofpa
tien
ts,lea
ding
todiscon
tinu
ationin
one
patien
t.
QTPmay
redu
cesymptom
sof
insomniain
patien
tswithPTSD.
� Sag
udet
al.(20
06)
18+
Treatmen
t-resistan
tDSM-IV
depr
ession
20-w
kop
en-lab
eltrialof
QTP
asau
gmen
tation
ofan
tide
pressa
nts.
Mea
nQTP
dose
315mg/da
y.N
=14
.
QTP
sign
ifican
tlyim
prov
edthe
anxietyan
dinsomniasu
bscalesof
theHAM-D
.In
somniascores
ofHAM-D
was
sign
ifican
tlyredu
ced
from
baseline
after20
wkof
trea
tmen
t,P
,0.05
.
Thr
eepa
tien
tsha
dhyp
oten
sion
andtw
ohad
daytim
eseda
tion
,tran
sien
tan
dmild.
QTPis
effectivein
redu
cing
symptom
sof
insomniain
patien
tswithde
pression
.
Tas
sniyom
etal.
(201
0)25
–62
Primaryinsomniaby
DSM-IV
2-wkRCT.QTP
25mg/da
yvs.
placeb
o.N
=16
.In
crea
sesin
sleeptime:
placeb
o=
72.24minutes
vs.QTP=
124.92
minutes
(P=0.19
3).
Red
uctionsin
SOL:p
lacebo
=23
.72minutes
vs.QTP=
96.16minutes
(P=0.07
0).Trend
forim
prov
emen
twas
show
nthou
ghdidnot
reactsign
ifican
tdifferen
ce.
Twopa
tien
tsin
QTP
grou
prepo
rted
drylips
,dr
ytongu
e,an
dmorning
drow
sine
ss.
QTPmay
beeffectiveat
redu
cing
symptom
sof
insomnia.
Terán
etal.(200
8)NS
Insomnia
during
detoxification
insu
bstanc
eab
users
Retrosp
ective
chartreview
.QTP25
–22
5mg/da
y.N
=52
med
ical
record
s.
Globa
lSpieg
elSleep
Que
stionn
aire
(SSQ)scores
sign
ifican
tly
impr
oved
throug
hout
the60
-day
follow
uppe
riod
,P
,0.00
1.Greatestim
prov
emen
toccu
rred
infirstweekof
trea
tmen
tan
dremaine
dcons
tant
therea
fter.
Nopa
tien
tsdr
oppe
dou
tdu
eto
AEs.
Most
common
AE
was
dry
mou
th(34.6%
).
QTPis
effectiveat
redu
cing
symptom
sof
insomnia
during
detoxification
from
subs
tanc
eab
use.
(con
tinued
)
Drugs for Insomnia beyond Benzodiazepines 237

IX. Discoveries, Novel Pathways, and Pipelines
The discoveries and pipelines in this section, con-structed using data from a custom search of theCortellis database, are an up-to-date (as of February2017) snapshot of the current state of the research anddevelopment of insomnia medications.
A. Discoveries
1. Adenosine Receptor Agonist. YZG-331 is a prom-ising sedative hypnotic and adenosine analog thatexerts its effects by binding to the adenosine receptor.(See the Other Receptors section for a review of thepharmacology of A1A and A2A.)
2. Casein Kinase-1d/«. The casein kinase-1d andcasein kinase-1« proteins are essential elements of themolecular oscillators known as circadian clocks (Leeet al., 2009). Their importance to the functioning of themammalian circadian rhythm has spurred interest incasein kinase-1d/« inhibitors as potential clinical treat-ments of sleep disorders and other central nervoussystem disorders including neurodegenerative condi-tions (Perez et al., 2011).
3. Selective Melatonin MT2 Receptors. Studies onmelatonin MT1 knockout, MT2 knockout, and doubleMT1-MT2 knockout mice have demonstrated that thesetwo receptors have opposing or complementary func-tions. Whereas MT2 receptor activation promotes SWS,MT1 decreases SWS and increases REMS (Ochoa-Sanchez et al., 2011; Ochoa-Sanchez et al., 2014). Thisevidence prompted the development of novel selectiveMT2 agonists as hypnotics. The compound UCM765 hasgreater MT2 receptor affinity (pKi = 10.18) than mela-tonin (pKi = 9.59) and has about 100-fold higher affinityfor the MT2 receptor than for the MT1 receptor (pKi =8.28). UCM924 also displays MT2 affinity (pKi = 10.2)that is 300-fold higher than forMT1 (pKi = 6.75), with anintrinsic activity for MT1: IAr-hMT1 = 0.1; and for MT2:IAr-hMT2 = 0.4 (Rivara et al., 2009).
Both UCM765 (Ochoa-Sanchez et al., 2011) andUCM924 (Ochoa-Sanchez et al., 2014) increase SWSduring the inactive phase of the day, without significantchange in REMS or sleep architecture. The congenernonselective MT1-MT2 receptor UCM971 did not alterthe 24-hour duration of wakefulness, NREMS, orREMS, but modified the number of episodes. MLTdecreased (237%) the latency to the first episode ofNREMS and enhanced the power of NREMS delta band(+33%), but did not alter the duration of any of the threevigilance states or modify the duration of SWS (Ochoa-Sanchez et al., 2014). These data confirm the impor-tance of targeting the MT2 receptor for hypnotic effects.UCM765 and UCM924 show a good safety profile andare currently under development for clinical studies.
4. Selective Orexin-2 Antagonist. Although dualorexin receptor antagonists like suvorexant are effec-tive at promoting sleep, selective orexin-2 receptor
TABLE
15—
Con
tinued
Study
Age
Diagn
osis
Design+Numbe
rof
Participa
nts
Results
Adv
erse
Eve
nts
Con
clusion
Tod
deret
al.
(200
6)21
–76
Treatmen
t-resistan
tunipo
laror
bipo
lar
depr
ession
compa
redwith
hea
lthy
controls
4-wkop
en-lab
elfollow
upstud
yof
QTP
augm
entation
ofan
tide
pressa
nts.
QTP
50–
800mg/da
y.N
=54
.
Objective
actigrap
hicsleepan
alysis:
nosign
ifican
tdifferen
cewas
foundbe
twee
nWee
ks1an
d4.
SE
didnot
chan
ge.Actua
lsleeptime
was
high
erat
alltimepo
ints
inpa
tien
tscompa
redwithcontrols,
howev
er,S
OL
was
sign
ifican
tly
high
erin
controls
compa
redto
patien
ts.S
ubjectivesleepan
alysis
withPSQI:
statistically
sign
ifican
tim
prov
emen
tsof
total
sleepscore,
qualityof
sleep,
daytim
esleepine
ss,be
tweenthe
weekbe
fore
admission
,Week1,
andWee
k2.
SOL
impr
oved
betw
eenWee
ks1an
d4.
Not
analyz
ed.
QTPmay
beeffectiveat
redu
cing
symptom
sof
insomniain
patien
tswith
depr
ession
.
Wiega
ndet
al.
(200
8)NS
Primaryinsomnia
6-wkop
en-lab
elstudy
.QTP
25–75
mg/da
y.N
=18
.Total
sleeptime(m
inute)
increa
sed
from
358.06
61.4
atba
seline
to39
5.66
62.3
at6w,P
=0.03
.SOL
(minute)
was
22.1
617
.0at
baseline
and24
.26
19.0
at6wk
(P=0.83
).PSQItotalscorewas
redu
cedfrom
13.1
62.3at
baseline
to6.86
3.3at
6wk,
P=
0.00
.
Dry
mou
than
dtran
sien
tha
ngov
ersymptom
swere
record
edmostfreq
uen
tly.
QTPis
effectiveat
redu
cing
symptom
sof
insomnia.
238 Atkin et al.

blockers may preserve sleep architecture to a greaterextent than dual antagonists (Bonaventure et al., 2015).Indeed, only orexin-2 but not orexin-1 is involved in theregulation of sleep (Dugovic et al., 2009). JNJ-42847922is a novel orexin-2 antagonist shown to reduce thelatency to NREM sleep and increase NREM sleep in thefirst 2 hours after administration, without affectingREM sleep in rats (Bonaventure et al., 2015). Impor-tantly, the compound has been shown to reduce time tosleep onset and increase total sleep time after 7 days ofchronic dosing (30 mg/kg). The compound did not pro-duce conditioned-place preference or increase dopaminerelease in the nucleus accumbens, indicating that itlacks intrinsic motivational properties, in contrast tozolpidem. In a Phase I study in healthy human subjects,JNJ-42847922 (10–80 mg/day) significantly increasedsomnolence: 22 of 26 subjects (85%) receiving JNJ-42847922 reported somnolence as an adverse event,whereas only 3 of 13 subjects (23%) receiving placebodid (Bonaventure et al., 2015). The compound’s phar-macokinetic profile in humans was favorable, with ahalf-life of 2 hours. One subject reported experiencingsleep paralysis after receiving the 80 mg/day dose.
B. Pipelines
1. Lumateperone. Lumateperone is a mechanisti-cally novel investigational antipsychotic drug with aunique pharmacological profile, showing very high5-HT2A blocking activity (Ki = 0.54 nM) relative to itsD2 modulating activity. The drug has a 60-fold differ-ence between its affinity for 5HT2A and D2 receptorscompared with a 12-fold difference for risperidone, a12.4-fold difference for olanzapine, and a 0.18-folddifference for aripiprazole (Davis et al., 2015; Snyderet al., 2015). Lumateroperone functions as a modulatorof the D2 receptor by partially agonizing presynaptic D2
receptors and antagonizing postsynaptic D2 receptors(Ki = 32 nM) (Snyder et al., 2015). Furthermore, thedrug blocks the serotonin transporter with strongaffinity (Ki = 62 nM) while having no affinity for theH1 histaminergic or muscarinic receptors (Snyder et al.,2015). Importantly, the drug’s D2 and SERT occupancyincrease with dose (Davis et al., 2015); at low doses, thedrug theoretically functions as a selective 5-HT2A
blocker.The company, Intra-Cellular Therapies (New York,
NY), suggests on their website that lower doses oflumateperone could be useful in the treatment of sleepdisorders, whereas higher doses are targeted to neuro-psychiatric disease. A Phase 2 study (N = 18) oflumateperone as a treatment of insomnia characterizedby sleep maintenance difficulties was discontinuedearly when the investigators found robust evidence ofefficacy, with increased SWS and decreased wake aftersleep time by polysomnography (Intra-Cellular Thera-pies, 2009). Furthermore, lumateperone did not impairnext-day cognition as measured by Leeds Psychomotor
Battery, Digit Symbol Substitution Test, or Word PairAssociates Test.
2. Piromelatine. Piromelatine is a unique drug thatcombines agonist activity atMT1 andMT2with agonismat 5-HT1A/1D receptors (Laudon et al., 2012). Piromela-tine was shown to have both hypnotic and antinocicep-tive effects by electroencephalogram (EEG) recordingsand an animal model of neuropathic pain, partial sciaticnerve ligation (Liu et al., 2014). The drug was found toincrease NREM sleep and decrease wakefulness inpartial sciatic nerve ligation mice. Finally, the investi-gators demonstrated that the effect could be blocked bypreadministration of a melatonin receptor antagonist, a5-HT1A receptor antagonist, or an opiate receptorantagonist (Liu et al., 2014), implicating these receptorsin the mechanism of action of the drug.
In 2013, Neurim Pharmaceuticals (Tel-Aviv, Israel)announced positive results from a phase II randomizedclinical trial (N = 120) of piromelatine in primaryinsomnia (Neurim Pharmaceuticals, 2013). Activetreatment with piromelatine 20 or 50 mg/day over4 weeks resulted in significantly improved wake aftersleep onset, sleep efficiency, and total sleep time. TheClinicaltrials.gov database lists a study currentlyrecruiting patients entitled Safety and Efficacy ofPiromelatine in Mild Alzheimer’s Disease Patients(ReCOGNITION); it also lists a completed study enti-tled The Effect of Neu-P11 on Symptoms in Patientswith D-IBS. These studies indicate that Neurim Phar-maceuticals is exploring piromelatine’s potential effi-cacy in myriad conditions, including irritable bowelsyndrome and Alzheimer’s disease.
X. Conclusions
In the last 20 years, preclinical and clinical researchon sleep has expanded tremendously. The study ofknockoutmice for specific receptors has generated novelscientific knowledge of the unique role of each receptorin the regulation of sleep, the application of optogeneticsto the study of sleep has elucidated new circuits, and thediscovery of clock genes has generated insight into thecellular and molecular mechanisms that regulate sleephomeostasis.
In parallel, clinical studies have investigated howsleep architecture is differentially impaired in variousneuropsychiatric diseases (including major depressivedisorder, posttraumatic stress disorder, and Alzheimerdisease) and the manner in which selective receptors’ligands can improve sleep quality and quantity.
Despite these advancements, BZDs continue to bewidely prescribed, although their use, particularly inthe elderly, is associated with an increased risk of falls,fractures, and emergency hospitalizations. Most or allBZDs and Z-drugs are available as generic drugs; assuch, they are available to providers (private insur-ance companies, universal governmental health care
Drugs for Insomnia beyond Benzodiazepines 239

systems) for a very low cost compared with innovativehypnotics (Tannenbaum et al., 2015; Goreveski et al.,2012). Innovative drugs cannot compete with the priceof BZDs, discouraging academia and pharmaceuticalresearch companies from investing in sleep medicine.Clinicians resort to prescribing drugs off-label, althoughthese compounds often lack a strong evidence base fortheir use.Substantial opportunity remains for pipelines that
target the unmet needs in the insomnia market. Medi-cines with comparable efficacy and improved long-termsafety would hold a competitive advantage over currentfirst-line therapies, especially hypnotic without cognitiveside-effects or not causing motor impairments the nextday. Similarly, drugs that improve sleep quality byaugmenting SWS would be viewed favorably by physi-cians. Moreover, drugs that selectively improve sleep inspecific diseases would be also a new avenue for apersonalized medicine.Advancing drug discovery for insomnia and sleep
disorders requires that the industry, in collaborationwith regulatory authorities, clinical experts, and pa-tient communities, engage in promoting and requiringbetter treatment of this condition. Moreover, there is aneed to better define and agree on the nosology of sleep-related illnesses: the classifications of patient popula-tions and the types of outcomes, other than sleepparameters, to be monitored among clients. Researchinto novel hypnotics may bolster the growing concep-tion that sleep disorders are an integral part of, ratherthan secondary to, diseases such as depression andAlzheimer’s (Wafford and Ebert, 2008). Since theburden of insomnia and sleep disorders will likelyincrease in coming decades due to the aging of thepopulation and the growing use of computer technol-ogies (Fossum et al., 2014), research on novel hypnoticsshould be considered a priority.
Acknowledgments
We acknowledge Martina Dick for technical help in Fig. 1.
Authorship Contributions
Wrote or contributed to the writing of the manuscript: Atkin, Comai,Gobbi.
ReferencesAdamantidis A, Carter MC, and de Lecea L (2010) Optogenetic deconstruction ofsleep-wake circuitry in the brain. Front Mol Neurosci 2:31.
Adams KH, Pinborg LH, Svarer C, Hasselbalch SG, Holm S, Haugbøl S, Madsen K,Frøkjaer V, Martiny L, Paulson OB, et al. (2004) A database of [(18)F]-altanserinbinding to 5-HT(2A) receptors in normal volunteers: normative data and re-lationship to physiological and demographic variables. Neuroimage 21:1105–1113.
Aghajanian GK and Sanders-Bush E (2002) Serotonin, in Neuropsychopharmacology –
The Fifth Generation of Progress (Davis KL, Charney D, Coyle JT, and Nemeroff C,eds) pp 15–25, Lippincott Williams & Wilkins, New York.
Al-Barazanji KA, Wilson S, Baker J, Jessop DS, and Harbuz MS (2001) Centralorexin-A activates hypothalamic-pituitary-adrenal axis and stimulates hypotha-lamic corticotropin releasing factor and arginine vasopressin neurones in consciousrats. J Neuroendocrinol 13:421–424.
Alphapharm (2012) Prescribing information for Endep Amitriptyline Hydrochloride.Alphapharm Pty Limited. Millers Point, Australia.
American Psychiatric Association (2013) Diagnostic and Statistical Manual of MentalDisorders, 5th ed, American Psychiatric Pub., Arlington, VA.
Amzica F and Steriade M (2002) The functional significance of K-complexes. SleepMed Rev 6:139–149.
Anderson SL and Vande Griend JP (2014) Quetiapine for insomnia: a review of theliterature. Am J Health Syst Pharm 71:394–402.
Anttila SA and Leinonen EV (2001) A review of the pharmacological and clinicalprofile of mirtazapine. CNS Drug Rev 7:249–264.
Arbon EL, Knurowska M, and Dijk DJ (2015) Randomised clinical trial of theeffects of prolonged-release melatonin, temazepam and zolpidem on slow-waveactivity during sleep in healthy people. J Psychopharmacol 29:764–776.
Ashton H (2005) The diagnosis and management of benzodiazepine dependence. CurrOpin Psychiatry 18:249–255.
Aslan S, Isik E, and Cosar B (2002) The effects of mirtazapine on sleep: a placebocontrolled, double-blind study in young healthy volunteers. Sleep 25:677–679.
Banasr M, Soumier A, Hery M, Mocaër E, and Daszuta A (2006) Agomelatine, a newantidepressant, induces regional changes in hippocampal neurogenesis. Biol Psy-chiatry 59:1087–1096.
Barnes NM and Sharp T (1999) A review of central 5-HT receptors and their function.Neuropharmacology 38:1083–1152.
Bastien CH, LeBlanc M, Carrier J, and Morin CM (2003) Sleep EEG power spectra,insomnia, and chronic use of benzodiazepines. Sleep 26:313–317.
Baune BT, Caliskan S, and Todder D (2007) Effects of adjunctive antidepressanttherapy with quetiapine on clinical outcome, quality of sleep and daytime motor activityin patients with treatment-resistant depression. Hum Psychopharmacol 22:1–9.
Bazil CW, Dave J, Cole J, Stalvey J, and Drake E (2012) Pregabalin increases slow-wave sleep and may improve attention in patients with partial epilepsy and in-somnia. Epilepsy Behav 23:422–425.
Berridge CW and España RA (2000) Synergistic sedative effects of noradrenergica(1)- and b-receptor blockade on forebrain electroencephalographic and behavioralindices. Neuroscience 99:495–505.
Berridge CW, Schmeichel BE, and España RA (2012) Noradrenergic modulation ofwakefulness/arousal. Sleep Med Rev 16:187–197.
Bertisch SM, Herzig SJ, Winkelman JW, and Buettner C (2014) National use ofprescription medications for insomnia: NHANES 1999-2010. Sleep 37:343–349.
Bonaventure P, Shelton J, Yun S, Nepomuceno D, Sutton S, Aluisio L, Fraser I, LordB, Shoblock J, Welty N, et al. (2015) Characterization of JNJ-42847922, a selectiveorexin-2 receptor antagonist, as a clinical candidate for the treatment of insomnia.J Pharmacol Exp Ther 354:471–482.
Boutrel B, Franc B, Hen R, Hamon M, and Adrien J (1999) Key role of 5-HT1Breceptors in the regulation of paradoxical sleep as evidenced in 5-HT1B knock-outmice. J Neurosci 19:3204–3212.
Boutrel B, Monaca C, Hen R, Hamon M, and Adrien J (2002) Involvement of 5-HT1Areceptors in homeostatic and stress-induced adaptive regulations of paradoxicalsleep: studies in 5-HT1A knock-out mice. J Neurosci 22:4686–4692.
Brower KJ, Myra Kim H, Strobbe S, Karam-Hage MA, Consens F, and Zucker RA(2008) A randomized double-blind pilot trial of gabapentin versus placebo to treatalcohol dependence and comorbid insomnia. Alcohol Clin Exp Res 32:1429–1438.
Brutcher RE and Nader MA (2015) Effects of quetiapine treatment on cocaine self-administration and behavioral indices of sleep in adult rhesus monkeys. Psycho-pharmacology (Berl) 232:411–420.
Buysse DJ, Reynolds CF III, Monk TH, Berman SR, and Kupfer DJ (1989) ThePittsburgh sleep quality index: a new instrument for psychiatric practice and re-search. Psychiatry Res 28:193–213.
Buysse DJ, Thompson W, Scott J, Franzen PL, Germain A, Hall M, Moul DE, Nof-zinger EA, and Kupfer DJ (2007) Daytime symptoms in primary insomnia: a pro-spective analysis using ecological momentary assessment. Sleep Med 8:198–208.
Bymaster FP, Calligaro DO, Falcone JF, Marsh RD, Moore NA, Tye NC, Seeman P,and Wong DT (1996) Radioreceptor binding profile of the atypical antipsychoticolanzapine. Neuropsychopharmacology 14:87–96.
Calabrese JR, Keck PE Jr, Macfadden W, Minkwitz M, Ketter TA, Weisler RH,Cutler AJ, McCoy R, Wilson E, and Mullen J (2005) A randomized, double-blind,placebo-controlled trial of quetiapine in the treatment of bipolar I or II depression.Am J Psychiatry 162:1351–1360.
Camargos EF, Louzada LL, Quintas JL, Naves JO, Louzada FM, and Nóbrega OT(2014) Trazodone improves sleep parameters in Alzheimer disease patients: arandomized, double-blind, and placebo-controlled study. Am J Geriatr Psychiatry22:1565–1574.
Cankurtaran ES, Ozalp E, Soygur H, Akbiyik DI, Turhan L, and Alkis N (2008)Mirtazapine improves sleep and lowers anxiety and depression in cancer patients:superiority over imipramine. Support Care Cancer 16:1291–1298.
Cates ME, Jackson CW, Feldman JM, Stimmel AE, and Woolley TW (2009) Metabolicconsequences of using low-dose quetiapine for insomnia in psychiatric patients.Community Ment Health J 45:251–254.
Chemelli RM, Willie JT, Sinton CM, Elmquist JK, Scammell T, Lee C, RichardsonJA, Williams SC, Xiong Y, Kisanuki Y, et al. (1999) Narcolepsy in orexin knockoutmice: molecular genetics of sleep regulation. Cell 98:437–451.
Chou TC, Bjorkum AA, Gaus SE, Lu J, Scammell TE, and Saper CB (2002) Afferentsto the ventrolateral preoptic nucleus. J Neurosci 22:977–990.
Citrome L (2014) Suvorexant for insomnia: a systematic review of the efficacy and safetyprofile for this newly approved hypnotic - what is the number needed to treat, numberneeded to harm and likelihood to be helped or harmed? Int J Clin Pract 68:1429–1441.
Cohrs S, Rodenbeck A, Guan Z, Pohlmann K, Jordan W, Meier A, and Rüther E(2004) Sleep-promoting properties of quetiapine in healthy subjects. Psychophar-macology (Berl) 174:421–429.
Comai S, Ochoa-Sanchez R, Dominguez-Lopez S, Bambico FR, and Gobbi G (2015)Melancholic-like behaviors and circadian neurobiological abnormalities in mela-tonin MT1 receptor knockout mice. Int J Neuropsychopharmacol 18:pyu075.
Comai S, Ochoa-Sanchez R, and Gobbi G (2013) Sleep-wake characterization ofdouble MT1/MT2 receptor knockout mice and comparison with MT1 and MT2 re-ceptor knockout mice. Behav Brain Res 243:231–238.
Comai S, Tau M, Pavlovic Z, and Gobbi G (2012a) The psychopharmacology of ag-gressive behavior: a translational approach: part 1: neurobiology. J Clin Psycho-pharmacol 32:83–94.
240 Atkin et al.

Comai S, Tau M, Pavlovic Z, and Gobbi G (2012b) The psychopharmacology of ag-gressive behavior: a translational approach: part 2: clinical studies using atypicalantipsychotics, anticonvulsants, and lithium. J Clin Psychopharmacol 32:237–260.
Cox CD, Breslin MJ, Whitman DB, Schreier JD, McGaughey GB, Bogusky MJ,Roecker AJ, Mercer SP, Bednar RA, Lemaire W, et al. (2010) Discovery of the dualorexin receptor antagonist [(7R)-4-(5-chloro-1,3-benzoxazol-2-yl)-7-methyl-1,4-dia-zepan-1-yl][5-methyl-2-(2H-1,2,3-triazol-2-yl)phenyl]methanone (MK-4305) for thetreatment of insomnia. J Med Chem 53:5320–5332.
Cunningham LA, Borison RL, Carman JS, Chouinard G, Crowder JE, Diamond BI,Fischer DE, and Hearst E (1994) A comparison of venlafaxine, trazodone, andplacebo in major depression. J Clin Psychopharmacol 14:99–106.
Davis RE, Vanover KE, Zhou Y, Bra�si�c JR, Guevara M, Bisuna B, Ye W, Raymont V,Willis W, Kumar A, et al. (2015) ITI-007 demonstrates brain occupancy at sero-tonin 5-HT2A and dopamine D2 receptors and serotonin transporters using posi-tron emission tomography in healthy volunteers. Psychopharmacology (Berl) 232:2863–2872.
De Gennaro L and Ferrara M (2003) Sleep spindles: an overview. Sleep Med Rev 7:423–440.
de Haas S, Otte A, de Weerd A, van Erp G, Cohen A, and van Gerven J (2007)Exploratory polysomnographic evaluation of pregabalin on sleep disturbance inpatients with epilepsy. J Clin Sleep Med 3:473–478.
de Lecea L, Kilduff TS, Peyron C, Gao X, Foye PE, Danielson PE, Fukuhara C,Battenberg EL, Gautvik VT, Bartlett FS II, et al. (1998) The hypocretins:hypothalamus-specific peptides with neuroexcitatory activity. Proc Natl Acad SciUSA 95:322–327.
De Sarro GB, Ascioti C, Froio F, Libri V, and Nisticò G (1987) Evidence that locuscoeruleus is the site where clonidine and drugs acting at a 1- and a 2-adrenoceptorsaffect sleep and arousal mechanisms. Br J Pharmacol 90:675–685.
Descamps A, Rousset C, Millan MJ, Spedding M, Delagrange P, and Cespuglio R(2009) Influence of the novel antidepressant and melatonin agonist/serotonin2Creceptor antagonist, agomelatine, on the rat sleep-wake cycle architecture. Psy-chopharmacology (Berl) 205:93–106.
DeVane CL and Nemeroff CB (2001) Clinical pharmacokinetics of quetiapine: anatypical antipsychotic. Clin Pharmacokinet 40:509–522.
Dhillon S and Clarke M (2014) Tasimelteon: first global approval. Drugs 74:505–511.Dolev Z (2011) Case series of perimenopausal women with insomnia treated withmirtazapine followed by prolonged-release melatonin add-on and monotherapy.Arch Women Ment Health 14:269–273.
Dording CM, Mischoulon D, Petersen TJ, Kornbluh R, Gordon J, Nierenberg AA,Rosenbaum JE, and Fava M (2002) The pharmacologic management of SSRI-induced side effects: a survey of psychiatrists. Ann Clin Psychiatry 14:143–147.
Dugovic C, Shelton JE, Aluisio LE, Fraser IC, Jiang X, Sutton SW, Bonaventure P,Yun S, Li X, Lord B, et al. (2009) Blockade of orexin-1 receptors attenuates orexin-2receptor antagonism-induced sleep promotion in the rat. J Pharmacol Exp Ther330:142–151.
Ekmekcioglu C (2006) Melatonin receptors in humans: biological role and clinicalrelevance. Biomed Pharmacother 60:97–108.
Endicott J, Paulsson B, Gustafsson U, Schiöler H, and Hassan M (2008) Quetiapinemonotherapy in the treatment of depressive episodes of bipolar I and II disorder:improvements in quality of life and quality of sleep. J Affect Disord 111:306–319.
Enomoto T, Yamashita A, Torigoe K, Horiuchi H, Hirayama S, Nakahara K, YanaseM, Sakai H, Ikegami D, Nagase H, et al. (2012) Effects of mirtazapine on sleepdisturbance under neuropathic pain-like state. Synapse 66:483–488.
Erman M, Seiden D, Zammit G, Sainati S, and Zhang J (2006) An efficacy, safety, and dose-response study of Ramelteon in patients with chronic primary insomnia.SleepMed 7:17–24.
España RA and Scammell TE (2011) Sleep neurobiology from a clinical perspective.Sleep 34:845–858.
European Medicines Agency (2008a) CHMP assessment for valdoxan, EuropeanMedicines Agency, London.
European Medicines Agency (2008b) Questions and answers on the withdrawal of themarketing application for ramelteon, European Medicines Agency, London.
European Medicines Agency (2016) Annex I: summary of product characteristics forvaldoxan, European Medicines Agency, London.
European Medicines Agency (2017) Annex I: summary of product characteristics forcircadin, European Medicines Agency, London.
Feeney J, Birznieks G, Scott C, Torres R, Welsch C, Baroldi P, Polymeropoulos M,and Walsh J (2009) Melatonin agonist tasimelteon improves sleep in primary in-somnia characterized by difficulty falling asleep. Sleep 32:A43.
Ferracioli-Oda E, Qawasmi A, and Bloch MH (2013) Meta-analysis: melatonin for thetreatment of primary sleep disorders. PLoS One 8:e63773.
Fisher SP, Davidson K, Kulla A, and Sugden D (2008) Acute sleep-promoting actionof the melatonin agonist, ramelteon, in the rat. J Pineal Res 45:125–132.
Foldvary-Schaefer N, De Leon Sanchez I, Karafa M, Mascha E, Dinner D, and Morris HH(2002) Gabapentin increases slow-wave sleep in normal adults. Epilepsia 43:1493–1497.
Ford ES, Wheaton AG, Cunningham TJ, Giles WH, Chapman DP, and Croft JB(2014) Trends in outpatient visits for insomnia, sleep apnea, and prescriptions forsleep medications among US adults: findings from the National AmbulatoryMedical Care survey 1999-2010. Sleep 37:1283–1293.
Fortier-Brochu E, Beaulieu-Bonneau S, Ivers H, and Morin CM (2012) Insomnia anddaytime cognitive performance: a meta-analysis. Sleep Med Rev 16:83–94.
Fossum IN, Nordnes LT, Storemark SS, Bjorvatn B, and Pallesen S (2014) Theassociation between use of electronic media in bed before going to sleep and in-somnia symptoms, daytime sleepiness, morningness, and chronotype. Behav SleepMed 12:343–357.
Foy A, O’Connell D, Henry D, Kelly J, Cocking S, and Halliday J (1995) Benzodiaz-epine use as a cause of cognitive impairment in elderly hospital inpatients. JGerontol A Biol Sci Med Sci 50:M99–M106.
Friedmann PD, Rose JS, Swift R, Stout RL, Millman RP, and Stein MD (2008)Trazodone for sleep disturbance after alcohol detoxification: a double-blind,placebo-controlled trial. Alcohol Clin Exp Res 32:1652–1660.
Garakani A, Martinez JM, Marcus S, Weaver J, Rickels K, Fava M, and HirschowitzJ (2008) A randomized, double-blind, and placebo-controlled trial of quetiapineaugmentation of fluoxetine in major depressive disorder. Int Clin Psychopharmacol23:269–275.
Gee NS, Brown JP, Dissanayake VU, Offord J, Thurlow R, and Woodruff GN (1996)The novel anticonvulsant drug, gabapentin (Neurontin), binds to the alpha2deltasubunit of a calcium channel. J Biol Chem 271:5768–5776.
Gillman PK (2007) Tricyclic antidepressant pharmacology and therapeutic drug in-teractions updated. Br J Pharmacol 151:737–748.
Giménez S, Clos S, Romero S, Grasa E, Morte A, and Barbanoj MJ (2007) Effects ofolanzapine, risperidone and haloperidol on sleep after a single oral morning dose inhealthy volunteers. Psychopharmacology (Berl) 190:507–516.
Gobbi G and Blier P (2005) Effect of neurokinin-1 receptor antagonists on seroto-ninergic, noradrenergic and hippocampal neurons: comparison with antidepres-sant drugs. Peptides 26:1383–1393.
Gobbi G, Murphy DL, Lesch K, and Blier P (2001) Modifications of the serotonergicsystem in mice lacking serotonin transporters: an in vivo electrophysiologicalstudy. J Pharmacol Exp Ther 296:987–995.
Gondard E, Anaclet C, Akaoka H, Guo R-X, Zhang M, Buda C, Franco P, Kotani H,and Lin J-S (2013) Enhanced histaminergic neurotransmission and sleep-wakealterations, a study in histamine H3-receptor knock-out mice. Neuro-psychopharmacology 38:1015–1031.
Gooneratne NS, Gehrman P, Gurubhagavatula I, Al-Shehabi E, Marie E, and SchwabR (2010) Effectiveness of ramelteon for insomnia symptoms in older adults withobstructive sleep apnea: a randomized placebo-controlled pilot study. J Clin SleepMed 6:572–580.
Gorevski E, Bian B, Kelton CM, Martin Boone JE, and Guo JJ (2012) Utilization,spending, and price trends for benzodiazepines in the US Medicaid program: 1991-2009. Ann Pharmacother 46:503–12.
Greenblatt DJ, Harmatz JS, and Karim A (2007) Age and gender effects on thepharmacokinetics and pharmacodynamics of ramelteon, a hypnotic agent actingvia melatonin receptors MT1 and MT2. J Clin Pharmacol 47:485–496.
Greene RW, Bjorness TE, and Suzuki A (2017) The adenosine-mediated, neuronal-glial, homeostatic sleep response. Curr Opin Neurobiol 44:236–242.
Gunja N (2013a) The clinical and forensic toxicology of Z-drugs. J Med Toxicol 9:155–162.
Gunja N (2013b) In the Zzz zone: the effects of Z-drugs on human performance anddriving. J Med Toxicol 9:163–171.
Haas H and Panula P (2003) The role of histamine and the tuberomamillary nucleusin the nervous system. Nat Rev Neurosci 4:121–130.
Haffmans PM and Vos MS (1999) The effects of trazodone on sleep disturbancesinduced by brofaromine. Eur Psychiatry 14:167–171.
Hagan JJ, Leslie RA, Patel S, Evans ML, Wattam TA, Holmes S, Benham CD, TaylorSG, Routledge C, Hemmati P, et al. (1999) Orexin A activates locus coeruleus cellfiring and increases arousal in the rat. Proc Natl Acad Sci USA 96:10911–10916.
HamiltonM (1960) A rating scale for depression. JNeurol Neurosurg Psychiatry 23:56–62.Hara J, Beuckmann CT, Nambu T, Willie JT, Chemelli RM, Sinton CM, Sugiyama F,Yagami K, Goto K, Yanagisawa M, et al. (2001) Genetic ablation of orexin neuronsin mice results in narcolepsy, hypophagia, and obesity. Neuron 30:345–354.
Hartmann E and Cravens J (1973) The effects of long term administration of psy-chotropic drugs on human sleep. 3. The effects of amitriptyline. Psychopharma-cology (Berl) 33:185–202.
Hassani OK, Lee MG, and Jones BE (2009) Melanin-concentrating hormone neuronsdischarge in a reciprocal manner to orexin neurons across the sleep-wake cycle.Proc Natl Acad Sci USA 106:2418–2422.
Hemmelgarn B, Suissa S, Huang A, Boivin JF, and Pinard G (1997) Benzodiazepineuse and the risk of motor vehicle crash in the elderly. JAMA 278:27–31.
Herring WJ, Connor KM, Ivgy-May N, Snyder E, Liu K, Snavely DB, Krystal AD,Walsh JK, Benca RM, Rosenberg R, et al. (2016) Suvorexant in patients withinsomnia: results from two 3-month randomized controlled clinical trials. BiolPsychiatry 79:136–148.
Herring WJ, Snyder E, Budd K, Hutzelmann J, Snavely D, Liu K, Lines C, Roth T,and Michelson D (2012) Orexin receptor antagonism for treatment of insomnia: arandomized clinical trial of suvorexant. Neurology 79:2265–2274.
Hindmarch I, Dawson J, and Stanley N (2005) A double-blind study in healthy vol-unteers to assess the effects on sleep of pregabalin compared with alprazolam andplacebo. Sleep 28:187–193.
Hinz R, Bhagwagar Z, Cowen PJ, Cunningham VJ, and Grasby PM (2007) Validationof a tracer kinetic model for the quantification of 5-HT(2A) receptors in humanbrain with [(11)C]MDL 100,907. J Cereb Blood Flow Metab 27:161–172.
Holsboer-Trachsler E and Prieto R (2013) Effects of pregabalin on sleep in general-ized anxiety disorder. Int J Neuropsychopharmacol 16:925–936.
Hoyer D, Dürst T, Fendt M, Jacobson LH, Betschart C, Hintermann S, Behnke D,Cotesta S, Laue G, Ofner S, et al. (2013) Distinct effects of IPSU and suvorexant onmouse sleep architecture. Front Neurosci 7:235.
Huang Z-L, Mochizuki T, Qu W-M, Hong Z-Y, Watanabe T, Urade Y, and Hayaishi O(2006) Altered sleep-wake characteristics and lack of arousal response to H3 re-ceptor antagonist in histamine H1 receptor knockout mice. Proc Natl Acad Sci USA103:4687–4692.
Huang Z-L, Qu W-M, Eguchi N, Chen J-F, Schwarzschild MA, Fredholm BB, UradeY, and Hayaishi O (2005) Adenosine A2A, but not A1, receptors mediate thearousal effect of caffeine. Nat Neurosci 8:858–859.
Iber C, Ancoli-Israel S, Chesson A, and Quan SF (2007) The AASM Manual for theScoring of Sleep and Associated Events: Rules, Terminology and Technical Speci-fications. American Academy of Sleep Medicine, Westchester, IL.
Intra-Cellular Therapies (Press release, Jan 13, 2009) Intra-Cellular Therapies An-nounces Successful Outcome of a Phase II Clinical Trial with ITI-007 in PatientsWith Sleep Maintenance Insomnia, Intra-Cellular Therapies, New York.
Jacobson KA and Gao Z-G (2006) Adenosine receptors as therapeutic targets.Nat RevDrug Discov 5:247–264.
Drugs for Insomnia beyond Benzodiazepines 241

Jakab RL and Goldman-Rakic PS (1998) 5-Hydroxytryptamine2A serotonin receptorsin the primate cerebral cortex: possible site of action of hallucinogenic and anti-psychotic drugs in pyramidal cell apical dendrites. Proc Natl Acad Sci USA 95:735–740.
Jakovljevi�c M, �Sagud M, and Mihaljevi�c-Peles A (2003) Olanzapine in the treatment-resistant, combat-related PTSD–a series of case reports. Acta Psychiatr Scand 107:394–396, discussion 396.
James SP and Mendelson WB (2004) The use of trazodone as a hypnotic: a criticalreview. J Clin Psychiatry 65:752–755.
Johnsa JD and Neville MW (2014) Tasimelteon: a melatonin receptor agonist for non-24-hour sleep-wake disorder. Ann Pharmacother 48:1636–1641.
Jones BE (2005) From waking to sleeping: neuronal and chemical substrates. TrendsPharmacol Sci 26:578–586.
Juri C, Chaná P, Tapia J, Kunstmann C, and Parrao T (2005) Quetiapine for in-somnia in Parkinson disease: results from an open-label trial. Clin Neuro-pharmacol 28:185–187.
Karam-Hage M and Brower KJ (2003) Open pilot study of gabapentin versus trazodone totreat insomnia in alcoholic outpatients. Psychiatry Clin Neurosci 57:542–544.
Kasper S, Hajak G, Wulff K, Hoogendijk WJ, Montejo AL, Smeraldi E, RybakowskiJK, Quera-Salva M-A, Wirz-Justice AM, Picarel-Blanchot F, et al. (2010) Efficacy ofthe novel antidepressant agomelatine on the circadian rest-activity cycle and de-pressive and anxiety symptoms in patients with major depressive disorder: arandomized, double-blind comparison with sertraline. J Clin Psychiatry 71:109–120.
Kato K, Hirai K, Nishiyama K, Uchikawa O, Fukatsu K, Ohkawa S, Kawamata Y,Hinuma S, and Miyamoto M (2005) Neurochemical properties of ramelteon (TAK-375), a selective MT1/MT2 receptor agonist. Neuropharmacology 48:301–310.
Kaynak H, Kaynak D, Gözükirmizi E, and Guilleminault C (2004) The effects oftrazodone on sleep in patients treated with stimulant antidepressants. Sleep Med5:15–20.
Keshavan MS, Prasad KM, Montrose DM, Miewald JM, and Kupfer DJ (2007) Sleepquality and architecture in quetiapine, risperidone, or never-treated schizophreniapatients. J Clin Psychopharmacol 27:703–705.
Khazaie H, Rezaie L, Darvishi F, Najafi F, and Avis K (2013) Treatment of para-doxical insomnia with atypical antipsychotic drugs. A comparison of olanzapineand risperidone. Neurosciences 18:64–69.
Khazaie H, Rezaie L, Tahmasian M, and Schwebel DC (2010) Insomnia treatment byolanzapine. Is sleep state misperception a psychotic disorder? Neurosciences 15:110–112.
Kim SW, Shin IS, Kim JM, Kim YC, Kim KS, Kim KM, Yang SJ, and Yoon JS (2008)Effectiveness of mirtazapine for nausea and insomnia in cancer patients with de-pression. Psychiatry Clin Neurosci 62:75–83.
Kishi T, Matsunaga S, and Iwata N (2015) Suvorexant for primary insomnia: asystematic review and meta-analysis of randomized placebo-controlled trials. PLoSOne 10:e0136910.
Kluge M, Schacht A, Himmerich H, Rummel-Kluge C, Wehmeier PM, Dalal M, Hinze-Selch D, Kraus T, Dittmann RW, Pollmächer T, et al. (2014) Olanzapine and clozapinedifferently affect sleep in patients with schizophrenia: results from a double-blind,polysomnographic study and review of the literature. Schizophr Res 152:255–260.
Kohsaka M, Kanemura T, Taniguchi M, Kuwahara H, Mikami A, Kamikawa K, UnoH, Ogawa A, Murasaki M, and Sugita Y (2011) Efficacy and tolerability of ramel-teon in a double-blind, placebo-controlled, crossover study in Japanese patientswith chronic primary insomnia. Expert Rev Neurother 11:1389–1397.
Krystal AD, Durrence HH, Scharf M, Jochelson P, Rogowski R, Ludington E,and Roth T (2010) Efficacy and safety of doxepin 1 mg and 3 mg in a 12-week sleeplaboratory and outpatient trial of elderly subjects with chronic primary insomnia.Sleep 33:1553–1561.
Krystal AD, Lankford A, Durrence HH, Ludington E, Jochelson P, Rogowski R,and Roth T (2011) Efficacy and safety of doxepin 3 and 6 mg in a 35-day sleeplaboratory trial in adults with chronic primary insomnia. Sleep 34:1433–1442.Kubota T, Fang J, Meltzer LT, and Krueger JM (2001) Pregabalin enhances non-rapid eye movement sleep. J Pharmacol Exp Ther 299:1095–1105.
Kuriyama A, Honda M, and Hayashino Y (2014) Ramelteon for the treatment ofinsomnia in adults: a systematic review and meta-analysis. Sleep Med 15:385–392.
Lacoste B, Angeloni D, Dominguez-Lopez S, Calderoni S, Mauro A, Fraschini F,Descarries L, and Gobbi G (2015) Anatomical and cellular localization of melatoninMT1 and MT2 receptors in the adult rat brain. J Pineal Res 58:397–417.
Landolt HP and Wehrle R (2009) Antagonism of serotonergic 5-HT2A/2C receptors:mutual improvement of sleep, cognition and mood? Eur J Neurosci 29:1795–1809.
Lankford A, Rogowski R, Essink B, Ludington E, Heith Durrence H, and Roth T(2012) Efficacy and safety of doxepin 6 mg in a four-week outpatient trial of elderlyadults with chronic primary insomnia. Sleep Med 13:133–138.
Laudon M, Katz A, Metzger D, Staner L, Pross N, Cornette F, Guichard N, Nir T,and Zisapel N (2012) Tolerability, pharmacokinetic and pharmacodynamic evalu-ation of multiple ascending doses of Neu-P11 in insomnia patients. Sleep 35:A221.
Lavedan C, Forsberg M, and Gentile AJ (2015) Tasimelteon: a selective and uniquereceptor binding profile. Neuropharmacology 91:142–147.
Le Bon O, Murphy JR, Staner L, Hoffmann G, Kormoss N, Kentos M, Dupont P, LionK, Pelc I, and Verbanck P (2003) Double-blind, placebo-controlled study of theefficacy of trazodone in alcohol post-withdrawal syndrome: polysomnographic andclinical evaluations. J Clin Psychopharmacol 23:377–383.
Lee H, Chen R, Lee Y, Yoo S, and Lee C (2009) Essential roles of CKIdelta andCKIepsilon in the mammalian circadian clock. Proc Natl Acad Sci USA 106:21359–21364.
Lelkes Z, Obál F Jr, Alföldi P, Erdös A, Rubicsek G, and Benedek G (1994) Effects ofacute and chronic treatment with trazodone, an antidepressant, on the sleep-wakeactivity in rats. Pharmacol Res 30:105–115.
Lemoine P, Garfinkel D, Laudon M, Nir T, and Zisapel N (2011) Prolonged-releasemelatonin for insomnia - an open-label long-term study of efficacy, safety, andwithdrawal. Ther Clin Risk Manag 7:301–311.
Lemoine P, Nir T, Laudon M, and Zisapel N (2007) Prolonged-release melatoninimproves sleep quality and morning alertness in insomnia patients aged 55 yearsand older and has no withdrawal effects. J Sleep Res 16:372–380.
Lemoine P and Zisapel N (2012) Prolonged-release formulation of melatonin (Cir-cadin) for the treatment of insomnia. Expert Opin Pharmacother 13:895–905.
Lin L, Faraco J, Li R, Kadotani H, Rogers W, Lin X, Qiu X, de Jong PJ, Nishino S,and Mignot E (1999) The sleep disorder canine narcolepsy is caused by a mutationin the hypocretin (orexin) receptor 2 gene. Cell 98:365–376.
Liu J and Wang LN (2012) Ramelteon in the treatment of chronic insomnia: sys-tematic review and meta-analysis. Int J Clin Pract 66:867–873.
Liu Y-Y, Yin D, Chen L, Qu W-M, Chen C-R, Laudon M, Cheng N-N, Urade Y,and Huang Z-L (2014) Piromelatine exerts antinociceptive effect via melatonin,opioid, and 5HT1A receptors and hypnotic effect via melatonin receptors in amouse model of neuropathic pain. Psychopharmacology (Berl) 231:3973–3985.
Lo H-S, Yang C-M, Lo HG, Lee C-Y, Ting H, and Tzang B-S (2010) Treatment effectsof gabapentin for primary insomnia. Clin Neuropharmacol 33:84–90.
Lockley SW, Dressman MA, Licamele L, Xiao C, Fisher DM, Flynn-Evans EE, HullJT, Torres R, Lavedan C, and Polymeropoulos MH (2015) Tasimelteon for non-24-hour sleep-wake disorder in totally blind people (SET and RESET): two multi-centre, randomised, double-masked, placebo-controlled phase 3 trials. Lancet 386:1754–1764.
López-Giménez JF, Mengod G, Palacios JM, and Vilaró MT (2001) Regional distri-bution and cellular localization of 5-HT2C receptor mRNA in monkey brain:comparison with [3H]mesulergine binding sites and choline acetyltransferasemRNA. Synapse 42:12–26.
Lovenberg TW, Roland BL, Wilson SJ, Jiang X, Pyati J, Huvar A, Jackson MR,and Erlander MG (1999) Cloning and functional expression of the human hista-mine H3 receptor. Mol Pharmacol 55:1101–1107.
Lugoboni F, Mirijello A, Faccini M, Casari R, Cossari A, Musi G, Bissoli G, Quaglio G,and Addolorato G (2014) Quality of life in a cohort of high-dose benzodiazepinedependent patients. Drug Alcohol Depend 142:105–109.
Luppi P-H, Peyron C, and Fort P (2017) Not a single but multiple populations ofGABAergic neurons control sleep. Sleep Med Rev 32:85–94.
Luthringer R, Muzet M, Zisapel N, and Staner L (2009) The effect of prolonged-release melatonin on sleep measures and psychomotor performance in elderlypatients with insomnia. Int Clin Psychopharmacol 24:239–249.
Mäkelä JP and Hilakivi IT (1986) Effect of alpha-adrenoceptor blockade on sleep andwakefulness in the rat. Pharmacol Biochem Behav 24:613–616.
Mander BA, Winer JR, and Walker MP (2017) Sleep and human aging.Neuron 94:19–36.Manns ID, Lee MG, Modirrousta M, Hou YP, and Jones BE (2003) Alpha 2 adrenergicreceptors on GABAergic, putative sleep-promoting basal forebrain neurons. Eur JNeurosci 18:723–727.
Marek GJ (2010) Electrophysiology of serotonin receptors, inHandbook of BehavioralNeurobiology of Serotonin (C. Müller and B. Jacobs eds) vol. 21, pp 163–182,Elsevier, London.
Mayer G, Wang-Weigand S, Roth-Schechter B, Lehmann R, Staner C, and PartinenM (2009) Efficacy and safety of 6-month nightly ramelteon administration in adultswith chronic primary insomnia. Sleep 32:351–360.
McAllister-Williams RH, Baldwin DS, Haddad PM, and Bazire S (2010) The use ofantidepressants in clinical practice: focus on agomelatine. Hum Psychopharmacol25:95–102.
McCall WV (2010) Off-label use of prescription medications for insomnia: sedatingantidepressants, antipsychotics, anxiolytics, and anticonvulsants, in Insomnia:Diagnosis and Treatment (Sateia MJ and Buysse DJ, eds) p 397, Informa UK Ltd.
McElroy SL, Weisler RH, Chang W, Olausson B, Paulsson B, Brecher M, AgambaramV, Merideth C, Nordenhem A, and Young AH; EMBOLDEN II (TrialD1447C00134) Investigators (2010) A double-blind, placebo-controlled study ofquetiapine and paroxetine as monotherapy in adults with bipolar depression(EMBOLDEN II). J Clin Psychiatry 71:163–174.
McElroy SL, Winstanley EL, Martens B, Patel NC, Mori N, Moeller D, McCoy J,and Keck PE Jr (2011) A randomized, placebo-controlled study of adjunctiveramelteon in ambulatory bipolar I disorder with manic symptoms and sleep dis-turbance. Int Clin Psychopharmacol 26:48–53.
Mendelson WB (2005) A review of the evidence for the efficacy and safety of trazo-done in insomnia. J Clin Psychiatry 66:469–476.
Mendlewicz J, Kempenaers C, and de Maertelaer V (1991) Sleep EEG and ami-tryptiline treatment in depressed inpatients. Biol Psychiatry 30:691–702.
Mets MA, de Vries JM, de Senerpont Domis LM, Volkerts ER, Olivier B, and VersterJC (2011) Next-day effects of ramelteon (8 mg), zopiclone (7.5 mg), and placebo onhighway driving performance, memory functioning, psychomotor performance, andmood in healthy adult subjects. Sleep 34:1327–1334.
Michelson D, Snyder E, Paradis E, Chengan-Liu M, Snavely DB, Hutzelmann J,Walsh JK, Krystal AD, Benca RM, Cohn M, et al. (2014) Safety and efficacy ofsuvorexant during 1-year treatment of insomnia with subsequent abrupt treat-ment discontinuation: a phase 3 randomised, double-blind, placebo-controlled trial.Lancet Neurol 13:461–471.
Mieda M, Hasegawa E, Kisanuki YY, Sinton CM, Yanagisawa M, and Sakurai T(2011) Differential roles of orexin receptor-1 and -2 in the regulation of non-REMand REM sleep. J Neurosci 31:6518–6526.
Millan MJ, Gobert A, Lejeune F, Dekeyne A, Newman-Tancredi A, Pasteau V, RivetJ-M, and Cussac D (2003) The novel melatonin agonist agomelatine (S20098) is anantagonist at 5-hydroxytryptamine2C receptors, blockade of which enhances theactivity of frontocortical dopaminergic and adrenergic pathways. J Pharmacol ExpTher 306:954–964.
Miyamoto M, Nishikawa H, Doken Y, Hirai K, Uchikawa O, and Ohkawa S (2004)The sleep-promoting action of ramelteon (TAK-375) in freely moving cats. Sleep 27:1319–1325.
Montgomery SA, Herman BK, Schweizer E, and Mandel FS (2009) The efficacy ofpregabalin and benzodiazepines in generalized anxiety disorder presenting withhigh levels of insomnia. Int Clin Psychopharmacol 24:214–222.
242 Atkin et al.

Monti JM and Jantos H (1992) Dose-dependent effects of the 5-HT1A receptor agonist8-OH-DPAT on sleep and wakefulness in the rat. J Sleep Res 1:169–175.
Monti JM and Monti D (2007) The involvement of dopamine in the modulation ofsleep and waking. Sleep Med Rev 11:113–133.
Morin CM and Jarrin DC (2013) Epidemiology of insomnia : prevalence, course, riskfactors, and public health burden. Sleep Med Clin 8:281–297.
Mouret J, Lemoine P, Minuit MP, Benkelfat C, and Renardet M (1988) Effects oftrazodone on the sleep of depressed subjects–a polygraphic study. Psychophar-macology (Berl) 95 (Suppl):S37–S43.
Nakamura T, Uramura K, Nambu T, Yada T, Goto K, Yanagisawa M, and Sakurai T(2000) Orexin-induced hyperlocomotion and stereotypy are mediated by the do-paminergic system. Brain Res 873:181–187.
Neurim Pharmaceuticals (Tel-Aviv, Israel) (Press release Feb 18 2013) NeurimPharmaceuticals announces positive Phase 2 clinical trial results of Piromelatinefor the treatment of insomnia, Neurim Pharmaceuticals, Tel-Aviv, Israel.
Nierenberg AA, Adler LA, Peselow E, Zornberg G, and Rosenthal M (1994) Trazodonefor antidepressant-associated insomnia. Am J Psychiatry 151:1069–1072.
Nierenberg AA, Husain MM, Trivedi MH, Fava M, Warden D, Wisniewski SR,Miyahara S, and Rush AJ (2010) Residual symptoms after remission of majordepressive disorder with citalopram and risk of relapse: a STAR*D report. PsycholMed 40:41–50.
Nilsen OG and Dale O (1992) Single dose pharmacokinetics of trazodone in healthysubjects. Pharmacol Toxicol 71:150–153.
Nilsen OG, Dale O, and Husebø B (1993) Pharmacokinetics of trazodone duringmultiple dosing to psychiatric patients. Pharmacol Toxicol 72:286–289.
Nishiyama K, Nishikawa H, Kato K, Miyamoto M, Tsukamoto T, and Hirai K (2014)Pharmacological characterization of M-II, the major human metabolite of ramel-teon. Pharmacology 93:197–201.
Nollet M, Gaillard P, Minier F, Tanti A, Belzung C, and Leman S (2011) Activation oforexin neurons in dorsomedial/perifornical hypothalamus and antidepressant re-versal in a rodent model of depression. Neuropharmacology 61:336–346.
Nutt DJ and Stahl SM (2010) Searching for perfect sleep: the continuing evolution ofGABAA receptor modulators as hypnotics. J Psychopharmacol 24:1601–1612.
Ochoa-Sanchez R, Comai S, Lacoste B, Bambico FR, Dominguez-Lopez S, Spadoni G,Rivara S, Bedini A, Angeloni D, Fraschini F, et al. (2011) Promotion of non-rapideye movement sleep and activation of reticular thalamic neurons by a novel MT2melatonin receptor ligand. J Neurosci 31:18439–18452.
Ochoa-Sanchez R, Comai S, Spadoni G, Bedini A, Tarzia G, and Gobbi G (2014)Melatonin, selective and non-selective MT1/MT2 receptors agonists: differentialeffects on the 24-h vigilance states. Neurosci Lett 561:156–161.
Oda T, Morikawa N, Saito Y, Masuho Y, and Matsumoto S (2000) Molecular cloningand characterization of a novel type of histamine receptor preferentially expressedin leukocytes. J Biol Chem 275:36781–36786.
Odagaki Y, Toyoshima R, and Yamauchi T (2005) Trazodone and its active metabolitem-chlorophenylpiperazine as partial agonists at 5-HT1A receptors assessed by[35S]GTPgammaS binding. J Psychopharmacol 19:235–241.
Ohayon MM (2002) Epidemiology of insomnia: what we know and what we still needto learn. Sleep Med Rev 6:97–111.
Olsen RW and Sieghart W (2009) GABA A receptors: subtypes provide diversity offunction and pharmacology. Neuropharmacology 56:141–148.
Otmani S, Demazières A, Staner C, Jacob N, Nir T, Zisapel N, and Staner L (2008)Effects of prolonged-release melatonin, zolpidem, and their combination on psy-chomotor functions, memory recall, and driving skills in healthy middle aged andelderly volunteers. Hum Psychopharmacol 23:693–705.
Pasquini M, Speca A, and Biondi M (2009) Quetiapine for tamoxifen-induced in-somnia in women with breast cancer. Psychosomatics 50:159–161.
Passani MB and Blandina P (2011) Histamine receptors in the CNS as targets fortherapeutic intervention. Trends Pharmacol Sci 32:242–249.
Paus S, Brecht HM, Köster J, Seeger G, Klockgether T, and Wüllner U (2003) Sleepattacks, daytime sleepiness, and dopamine agonists in Parkinson’s disease. MovDisord 18:659–667.
Perez DI, Gil C, and Martinez A (2011) Protein kinases CK1 and CK2 as new targetsfor neurodegenerative diseases. Med Res Rev 31:924–954.
Pompeiano M, Palacios JM, and Mengod G (1994) Distribution of the serotonin 5-HT2receptor family mRNAs: comparison between 5-HT2A and 5-HT2C receptors.Brain Res Mol Brain Res 23:163–178.
Popa D, Léna C, Fabre V, Prenat C, Gingrich J, Escourrou P, Hamon M, and Adrien J(2005) Contribution of 5-HT2 receptor subtypes to sleep-wakefulness and re-spiratory control, and functional adaptations in knock-out mice lacking 5-HT2Areceptors. J Neurosci 25:11231–11238.
Portaluppi F, Cortelli P, Avoni P, Vergnani L, Maltoni P, Pavani A, Sforza E, DegliUberti EC, Gambetti P, and Lugaresi E (1994) Progressive disruption of the cir-cadian rhythm of melatonin in fatal familial insomnia. J Clin Endocrinol Metab 78:1075–1078.
Portas CM, Thakkar M, Rainnie D, and McCarley RW (1996) Microdialysis perfusionof 8-hydroxy-2-(di-n-propylamino)tetralin (8-OH-DPAT) in the dorsal raphe nu-cleus decreases serotonin release and increases rapid eye movement sleep in thefreely moving cat. J Neurosci 16:2820–2828.
Pringsheim T and Gardner DM (2014) Dispensed prescriptions for quetiapine andother second-generation antipsychotics in Canada from 2005 to 2012: a descriptivestudy. CMAJ Open 2:E225–E232.
Purves D, Augustine GJ, Fitzpatrick D, Hall WC, Lamantia A-S, McNamara JO,and Williams SM (2004) Neuroscience, Sinauer Associates Inc, Sunderland, MA.
Qu W-M, Xu X-H, Yan M-M, Wang Y-Q, Urade Y, and Huang Z-L (2010) Essentialrole of dopamine D2 receptor in the maintenance of wakefulness, but not in ho-meostatic regulation of sleep, in mice. J Neurosci 30:4382–4389.
Quera-Salva M-A, Hajak G, Philip P, Montplaisir J, Keufer-Le Gall S, Laredo J,and Guilleminault C (2011) Comparison of agomelatine and escitalopram onnighttime sleep and daytime condition and efficacy in major depressive disorderpatients. Int Clin Psychopharmacol 26:252–262.
Quera-Salva MA, Lemoine P, and Guilleminault C (2010) Impact of the novel anti-depressant agomelatine on disturbed sleep-wake cycles in depressed patients.Hum Psychopharmacol 25:222–229.
Rajaratnam SM, Polymeropoulos MH, Fisher DM, Roth T, Scott C, Birznieks G,and Klerman EB (2009) Melatonin agonist tasimelteon (VEC-162) for transientinsomnia after sleep-time shift: two randomised controlled multicentre trials.Lancet 373:482–491.
Rechtschaffen A and Kales A (1968) A Manual of Standardized Terminology, Tech-niques, and Scoring Systems for Sleep Stages of Human Subjects, UCLA BrainInformation Service/Brain Research Institute, Los Angeles.
Richelson E (1979) Tricyclic antidepressants and histamine H1 receptors. Mayo ClinProc 54:669–674.
Richelson E and Souder T (2000) Binding of antipsychotic drugs to human brainreceptors focus on newer generation compounds. Life Sci 68:29–39.
Richer M, Hen R, and Blier P (2002) Modification of serotonin neuron properties inmice lacking 5-HT1A receptors. Eur J Pharmacol 435:195–203.
Rivara S, Vacondio F, Fioni A, Silva C, Carmi C, Mor M, Lucini V, Pannacci M,Caronno A, Scaglione F, et al. (2009) N-(Anilinoethyl)amides: design and synthesisof metabolically stable, selective melatonin receptor ligands. ChemMedChem 4:1746–1755.
Robert S, Hamner MB, Kose S, Ulmer HG, Deitsch SE, and Lorberbaum JP (2005)Quetiapine improves sleep disturbances in combat veterans with PTSD: sleep datafrom a prospective, open-label study. J Clin Psychopharmacol 25:387–388.
Robinson AA and Malow BA (2013) Gabapentin shows promise in treating refractoryinsomnia in children. J Child Neurol 28:1618–1621.
Rodríguez JJ, Noristani HN, Hoover WB, Linley SB, and Vertes RP (2011) Seroto-nergic projections and serotonin receptor expression in the reticular nucleus of thethalamus in the rat. Synapse 65:919–928.
Rosenberg RP, Hull SG, Lankford DA, Mayleben DW, Seiden DJ, Furey SA, Jaya-wardena S, and Roth T (2014) A randomized, double-blind, single-dose, placebo-controlled, multicenter, polysomnographic study of gabapentin in transient in-somnia induced by sleep phase advance. J Clin Sleep Med 10:1093–1100.
Roth T, Heith Durrence H, Jochelson P, Peterson G, Ludington E, Rogowski R, ScharfM, and Lankford A (2010) Efficacy and safety of doxepin 6 mg in a model oftransient insomnia. Sleep Med 11:843–847.
Roth T, Rogowski R, Hull S, Schwartz H, Koshorek G, Corser B, Seiden D,and Lankford A (2007) Efficacy and safety of doxepin 1 mg, 3 mg, and 6 mg inadults with primary insomnia. Sleep 30:1555–1561.
Roth T, Seiden D, Sainati S, Wang-Weigand S, Zhang J, and Zee P (2006) Effects oframelteon on patient-reported sleep latency in older adults with chronic insomnia.Sleep Med 7:312–318.
Rotzinger S, Fang J, and Baker GB (1998) Trazodone is metabolized tom-chlorophenylpiperazine by CYP3A4 from human sources. Drug Metab Dispos 26:572–575.
Rudorfer MV and Potter WZ (1999) Metabolism of tricyclic antidepressants. Cell MolNeurobiol 19:373–409.
Russell IJ, Crofford LJ, Leon T, Cappelleri JC, Bushmakin AG, Whalen E, BarrettJA, and Sadosky A (2009) The effects of pregabalin on sleep disturbance symptomsamong individuals with fibromyalgia syndrome. Sleep Med 10:604–610.
�Sagud M, Mihaljevi�c-Peles A, Mück-Seler D, Jakovljevi�c M, and Pivac N (2006)Quetiapine augmentation in treatment-resistant depression: a naturalistic study.Psychopharmacology (Berl) 187:511–514.
Sakai K (2011) Sleep-waking discharge profiles of median preoptic and surroundingneurons in mice. Neuroscience 182:144–161.
Sakurai T, Amemiya A, Ishii M, Matsuzaki I, Chemelli RM, Tanaka H, Williams SC,Richardson JA, Kozlowski GP, Wilson S, et al. (1998) Orexins and orexin receptors:a family of hypothalamic neuropeptides and G protein-coupled receptors thatregulate feeding behavior. Cell 92:573–585.
Salin-Pascual RJ, Herrera-Estrella M, Galicia-Polo L, and Laurrabaquio MR (1999)Olanzapine acute administration in schizophrenic patients increases delta sleepand sleep efficiency. Biol Psychiatry 46:141–143.
Sanger DJ (2004) The pharmacology and mechanisms of action of new generation,non-benzodiazepine hypnotic agents. CNS Drugs 18 (Suppl 1):9–15; discussion 41,43–15.
Sansone RA and Sansone LA (2011) Agomelatine: a novel antidepressant. Innov ClinNeurosci 8:10–14.
Saper CB, Chou TC, and Scammell TE (2001) The sleep switch: hypothalamic controlof sleep and wakefulness. Trends Neurosci 24:726–731.
Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, and Heald JL (2017a) Clinicalpractice guideline for the pharmacologic treatment of chronic insomnia in adults:an American Academy of Sleep Medicine clinical practice guideline. J Clin SleepMed 13:307–349.
Sateia MJ, Sherrill WC Jr, Winter-Rosenberg C, and Heald JL (2017b) Payer per-spective of the American Academy of Sleep Medicine clinical practice guideline forthe pharmacologic treatment of chronic insomnia. J Clin Sleep Med 13:155–157.
Scammell TE, Arrigoni E, and Lipton JO (2017) Neural circuitry of wakefulness andsleep. Neuron 93:747–765.
Scharf M, Rogowski R, Hull S, Cohn M, Mayleben D, Feldman N, Ereshefsky L,Lankford A, and Roth T (2008a) Efficacy and safety of doxepin 1 mg, 3 mg, and6 mg in elderly patients with primary insomnia: a randomized, double-blind,placebo-controlled crossover study. J Clin Psychiatry 69:1557–1564.
Scharf MB and Sachais BA (1990) Sleep laboratory evaluation of the effects and efficacy oftrazodone in depressed insomniac patients. J Clin Psychiatry 51 (Suppl):13–17.
Schatzberg AF and Nemeroff CB (2009) The American Psychiatric Publishing Text-book of Psychopharmacology, American Psychiatric Pub, Washington, DC.
Schlicker E, Malinowska B, Kathmann M, and Göthert M (1994) Modulation ofneurotransmitter release via histamine H3 heteroreceptors. Fundam Clin Phar-macol 8:128–137.
Schmitt KC and Reith ME (2010) Regulation of the dopamine transporter: aspectsrelevant to psychostimulant drugs of abuse. Ann N Y Acad Sci 1187:316–340.
Drugs for Insomnia beyond Benzodiazepines 243

Schutte-Rodin S, Broch L, Buysse D, Dorsey C, and Sateia M (2008) Clinical guide-line for the evaluation and management of chronic insomnia in adults. J Clin SleepMed 4:487–504.
Sharpley AL, Elliott JM, Attenburrow M-J, and Cowen PJ (1994) Slow wave sleep inhumans: role of 5-HT2A and 5-HT2C receptors. Neuropharmacology 33:467–471.
Sharpley AL, Vassallo CM, and Cowen PJ (2000) Olanzapine increases slow-wavesleep: evidence for blockade of central 5-HT(2C) receptors in vivo. Biol Psychiatry47:468–470.
Sills GJ (2006) The mechanisms of action of gabapentin and pregabalin. Curr OpinPharmacol 6:108–113.
Smith MT and Wegener ST (2003) Measures of sleep: the insomnia severity index,medical outcomes study (MOS) sleep scale, Pittsburgh sleep diary (PSD), andPittsburgh sleep quality index (PSQI). Arthritis Care Res 49:S184–S196.
Snyder GL, Vanover KE, Zhu H, Miller DB, O’Callaghan JP, Tomesch J, Li P, ZhangQ, Krishnan V, Hendrick JP, et al. (2015) Functional profile of a novel modulator ofserotonin, dopamine, and glutamate neurotransmission. Psychopharmacology(Berl) 232:605–621.
Soldatos CR, Dikeos DG, and Whitehead A (1999) Tolerance and rebound insomniawith rapidly eliminated hypnotics: a meta-analysis of sleep laboratory studies. IntClin Psychopharmacol 14:287–303.
Song L, Du Q, Jiang X, and Wang L (2014) Effect of CYP1A2 polymorphism on thepharmacokinetics of agomelatine in Chinese healthy male volunteers. J ClinPharm Ther 39:204–209.
Springer Adis Insight (2017) Atagabalin, Adis Insight Drug Profiles Database.Srisurapanont M and Jarusuraisin N (1998) Amitriptyline vs. lorazepam in thetreatment of opiate-withdrawal insomnia: a randomized double-blind study. ActaPsychiatr Scand 97:233–235.
Stahl S (2008) Stahl’s Essential Psychopharmacology, Neuroscientific Basis andPractical Applications, Applications, 3rd ed. Cambridge University Press, NY.
Stahl SM (2009) Mechanism of action of trazodone: a multifunctional drug. CNSSpectr 14:536–546.
Stein MD, Kurth ME, Sharkey KM, Anderson BJ, Corso RP, and Millman RP (2012)Trazodone for sleep disturbance during methadone maintenance: a double-blind,placebo-controlled trial. Drug Alcohol Depend 120:65–73.
Stenberg D, Litonius E, Halldner L, Johansson B, Fredholm BB, and Porkka-Heis-kanen T (2003) Sleep and its homeostatic regulation in mice lacking the adenosineA1 receptor. J Sleep Res 12:283–290.
Steriade M, Contreras D, Curró Dossi R, and Nuñez A (1993) The slow (, 1 Hz)oscillation in reticular thalamic and thalamocortical neurons: scenario of sleeprhythm generation in interacting thalamic and neocortical networks. J Neurosci13:3284–3299.
Steriade M and Timofeev I (2003) Neuronal plasticity in thalamocortical networksduring sleep and waking oscillations. Neuron 37:563–576.
Sun H, Kennedy WP, Wilbraham D, Lewis N, Calder N, Li X, Ma J, Yee KL, Ermlich S,Mangin E, et al. (2013) Effects of suvorexant, an orexin receptor antagonist, on sleepparameters as measured by polysomnography in healthy men. Sleep 36:259–267.
Szabo ST and Blier P (2001) Functional and pharmacological characterization of themodulatory role of serotonin on the firing activity of locus coeruleus norepinephrineneurons. Brain Res 922:9–20.
Takahashi K, Suwa H, Ishikawa T, and Kotani H (2002) Targeted disruption of H3receptors results in changes in brain histamine tone leading to an obese phenotype.J Clin Invest 110:1791–1799.
Takeda Global Research & Development Center Inc. (2008) Clinical Trial Synopsis01-05-TL-375-067, NCT#00755495.
Takemura Y, Yamashita A, Horiuchi H, Furuya M, Yanase M, Niikura K, Imai S,Hatakeyama N, Kinoshita H, Tsukiyama Y, et al. (2011) Effects of gabapentin onbrain hyperactivity related to pain and sleep disturbance under a neuropathicpain-like state using fMRI and brain wave analysis. Synapse 65:668–676.
Tannenbaum C, Diaby V, Singh D, Perreault S, Luc M, and Vasiliadis HM (2015)Sedative-hypnotic medicines and falls in community-dwelling older adults: a cost-effectiveness (decision-tree) analysis from a US Medicare perspective. Drugs Aging32:305–314.
Tassniyom K, Paholpak S, Tassniyom S, and Kiewyoo J (2010) Quetiapine for pri-mary insomnia: a double blind, randomized controlled trial. J Med Assoc Thai 93:729–734.
Tatsumi M, Groshan K, Blakely RD, and Richelson E (1997) Pharmacological profileof antidepressants and related compounds at human monoamine transporters. EurJ Pharmacol 340:249–258.
Taylor CP (1997) Mechanisms of action of gabapentin. Rev Neurol (Paris) 153 (Suppl1):S39–S45.
Taylor CP, Angelotti T, and Fauman E (2007) Pharmacology and mechanism of ac-tion of pregabalin: the calcium channel alpha2-delta (alpha2-delta) subunit as atarget for antiepileptic drug discovery. Epilepsy Res 73:137–150.
Terán A, Majadas S, and Galan J (2008) Quetiapine in the treatment of sleep dis-turbances associated with addictive conditions: a retrospective study. Subst UseMisuse 43:2169–2171.
Theobald DE, Kirsh KL, Holtsclaw E, Donaghy K, and Passik SD (2002) An open-label, crossover trial of mirtazapine (15 and 30 mg) in cancer patients with painand other distressing symptoms. J Pain Symptom Manage 23:442–447.
Thomas RE (1998) Benzodiazepine use and motor vehicle accidents. Systematic re-view of reported association. Can Fam Physician 44:799–808.
Thompson W, Quay TAW, Rojas-Fernandez C, Farrell B, and Bjerre LM (2016)Atypical antipsychotics for insomnia: a systematic review. Sleep Med 22:13–17.
Todder D, Caliskan S, and Baune BT (2006) Night locomotor activity and quality ofsleep in quetiapine-treated patients with depression. J Clin Psychopharmacol 26:638–642.
Tsunematsu T, Ueno T, Tabuchi S, Inutsuka A, Tanaka KF, Hasuwa H, Kilduff TS,Terao A, and Yamanaka A (2014) Optogenetic manipulation of activity and tem-porally controlled cell-specific ablation reveal a role for MCH neurons in sleep/wake regulation. J Neurosci 34:6896–6909.
Uchimura N, Ogawa A, Hamamura M, Hashimoto T, Nagata H, and Uchiyama M(2011) Efficacy and safety of ramelteon in Japanese adults with chronic insomnia: arandomized, double-blind, placebo-controlled study. Expert Rev Neurother 11:215–224.
Uchiyama M, Hamamura M, Kuwano T, Nishiyama H, Nagata H, and Uchimura N(2011) Evaluation of subjective efficacy and safety of ramelteon in Japanese sub-jects with chronic insomnia. Sleep Med 12:119–126.
Urade Y, Eguchi N, Qu W-M, Sakata M, Huang Z-L, Chen J-F, Schwarzschild MA,Fink JS, and Hayaishi O (2003) Sleep regulation in adenosine A2A receptor-deficient mice. Neurology 61 (11, Suppl 6)S94–S96.
US FDA (2007a) Doxepin Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2007b) Remeron Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2009) Zyprexa Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2010a) Rozerem Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2010b) Silenor Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2014a) Belsomra Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2014b) Hetlioz Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2014c) Neurontin Prescribing Information. United States Food and DrugAdministration, Washington, DC.
US FDA (2016) Lyrica Prescribing Information. United States Food and Drug Ad-ministration, Washington, DC.
US FDA (2017) Seroquel Prescribing Information. United States Food and DrugAdministration, Washington, DC.
Vaishnavi SN, Nemeroff CB, Plott SJ, Rao SG, Kranzler J, and Owens MJ (2004)Milnacipran: a comparative analysis of human monoamine uptake and transporterbinding affinity. Biol Psychiatry 55:320–322.
van Dyck CH, Tan PZ, Baldwin RM, Amici LA, Garg PK, Ng CK, Soufer R, CharneyDS, and Innis RB (2000) PET quantification of 5-HT2A receptors in the humanbrain: a constant infusion paradigm with [18F]altanserin. J Nucl Med 41:234–241.
Vanda Pharmaceuticals Inc. (Press release, June 26, 2008) Phase III data showVanda Pharmaceuticals’ tasimelteon (VEC-162) significantly improves sleep inpatients with chronic insomnia, Vanda Pharmaceuticals, Rockville, MD.
Vanda Pharmaceuticals Inc. (2014) VEC-162 Study in Adult Patients With PrimaryInsomnia National Library of Medicine, ClinicalTrials.gov.
Viola AU, Brandenberger G, Toussaint M, Bouhours P, Paul Macher J,and Luthringer R (2002) Ritanserin, a serotonin-2 receptor antagonist, improvesultradian sleep rhythmicity in young poor sleepers. Clin Neurophysiol 113:429–434.
Wade AG, Farmer M, Harari G, Fund N, Laudon M, Nir T, Frydman-Marom A,and Zisapel N (2014) Add-on prolonged-release melatonin for cognitive functionand sleep in mild to moderate Alzheimer’s disease: a 6-month, randomized,placebo-controlled, multicenter trial. Clin Interv Aging 9:947–961.
Wade AG, Ford I, Crawford G, McConnachie A, Nir T, Laudon M, and Zisapel N(2010) Nightly treatment of primary insomnia with prolonged release melatoninfor 6 months: a randomized placebo controlled trial on age and endogenous mel-atonin as predictors of efficacy and safety. BMC Med 8:51.
Wade AG, Ford I, Crawford G, McMahon AD, Nir T, Laudon M, and Zisapel N (2007)Efficacy of prolonged release melatonin in insomnia patients aged 55-80 years:quality of sleep and next-day alertness outcomes. Curr Med Res Opin 23:2597–2605.
Wafford KA and Ebert B (2008) Emerging anti-insomnia drugs: tackling sleepless-ness and the quality of wake time. Nat Rev Drug Discov 7:530–540.
Walsh JK (2004) Drugs used to treat insomnia in 2002: regulatory-based rather thanevidence-based medicine. Sleep 27:1441–1442.
Walsh JK, Erman M, Erwin C, Jamieson A, Mahowald M, Regestein Q, Scharf M,Tigel P, Vogel G, and Ware JC (1998) Subjective hypnotic efficacy of trazodone andzolpidem in DSMIII–R primary insomnia. Hum Psychopharmacol 13:191–198.
Wang-Weigand S, Watissée M, and Roth T (2011) Use of a post-sleep questionnaire-interactive voice response system (PSQ-IVRS) to evaluate the subjective sleep ef-fects of ramelteon in adults with chronic insomnia. Sleep Med 12:920–923.
Wang T-X, Yin D, Guo W, Liu Y-Y, Li Y-D, Qu W-M, Han W-J, Hong Z-Y, and HuangZ-L (2015) Antinociceptive and hypnotic activities of pregabalin in a neuropathicpain-like model in mice. Pharmacol Biochem Behav 135:31–39.
Ware JC, Rose FV, and McBrayer RH (1994) The acute effects of nefazodone, tra-zodone and buspirone on sleep and sleep-related penile tumescence in normalsubjects. Sleep 17:544–550.
What’s wrong with prescribing hypnotics? (2004) Drug Ther Bull 42:89–93.Wickwire EM, Shaya FT, and Scharf SM (2016) Health economics of insomniatreatments: the return on investment for a good night’s sleep. Sleep Med Rev 30:72–82.
Wiegand MH, Landry F, Brückner T, Pohl C, Veselý Z, and Jahn T (2008) Quetiapinein primary insomnia: a pilot study. Psychopharmacology (Berl) 196:337–338.
Willie JT, Chemelli RM, Sinton CM, Tokita S, Williams SC, Kisanuki YY, MarcusJN, Lee C, Elmquist JK, Kohlmeier KA, et al. (2003) Distinct narcolepsy syn-dromes in orexin receptor-2 and orexin null mice: molecular genetic dissection ofNon-REM and REM sleep regulatory processes. Neuron 38:715–730.
Wilson S and Argyropoulos S (2005) Antidepressants and sleep: a qualitative reviewof the literature. Drugs 65:927–947.
Wilson S and Nutt D (2007) Management of insomnia: treatments and mechanismsi.Br J Psychiatry 191:195–197.
Winokur A, DeMartinis NA III, McNally DP, Gary EM, Cormier JL, and Gary KA (2003)Comparative effects of mirtazapine and fluoxetine on sleep physiology measures inpatients with major depression and insomnia. J Clin Psychiatry 64:1224–1229.
244 Atkin et al.

Winokur A, Sateia MJ, Hayes JB, Bayles-Dazet W, MacDonald MM, and Gary KA(2000) Acute effects of mirtazapine on sleep continuity and sleep architecture indepressed patients: a pilot study. Biol Psychiatry 48:75–78.
Winrow CJ, Gotter AL, Cox CD, Doran SM, Tannenbaum PL, Breslin MJ, Garson SL,Fox SV, Harrell CM, Stevens J, et al. (2011) Promotion of sleep by suvorexant-anovel dual orexin receptor antagonist. J Neurogenet 25:52–61.
Winrow CJ and Renger JJ (2014) Discovery and development of orexin receptorantagonists as therapeutics for insomnia. Br J Pharmacol 171:283–293.
Yamadera H, Nakamura S, Suzuki H, and Endo S (1998) Effects of trazodone hy-drochloride and imipramine on polysomnography in healthy subjects. PsychiatryClin Neurosci 52:439–443.
Yamashita T and Yamanaka A (2017) Lateral hypothalamic circuits for sleep-wakecontrol. Curr Opin Neurobiol 44:94–100.
Yeung W-F, Chung K-F, Yung K-P, and Ng TH-Y (2015) Doxepin for insomnia: a sys-tematic review of randomized placebo-controlled trials. Sleep Med Rev 19:75–83.
Yin J, Babaoglu K, Brautigam CA, Clark L, Shao Z, Scheuermann TH, Harrell CM,Gotter AL, Roecker AJ, Winrow CJ, et al. (2016) Structure and ligand-binding
mechanism of the human OX1 and OX2 orexin receptors. Nat Struct Mol Biol 23:293–299.
Yukuhiro N, Kimura H, Nishikawa H, Ohkawa S, Yoshikubo S, and Miyamoto M(2004) Effects of ramelteon (TAK-375) on nocturnal sleep in freely moving mon-keys. Brain Res 1027:59–66.
Zammit G, Erman M, Wang-Weigand S, Sainati S, Zhang J, and Roth T (2007)Evaluation of the efficacy and safety of ramelteon in subjects with chronic in-somnia. J Clin Sleep Med 3:495–504.
Zammit G, Wang-Weigand S, Rosenthal M, and Peng X (2009) Effect of ramelteon onmiddle-of-the-night balance in older adults with chronic insomnia. J Clin SleepMed 5:34–40.
Zammit GK, Weiner J, Damato N, Sillup GP, and McMillan CA (1999) Quality of lifein people with insomnia. Sleep 22 (Suppl 2):S379–S385.
Zhang Z, Ferretti V, Güntan _I, Moro A, Steinberg EA, Ye Z, Zecharia AY, Yu X,Vyssotski AL, Brickley SG, et al. (2015) Neuronal ensembles sufficient for re-covery sleep and the sedative actions of a2 adrenergic agonists. Nat Neurosci 18:553–561.
Drugs for Insomnia beyond Benzodiazepines 245



![Index [pharmrev.aspetjournals.org]pharmrev.aspetjournals.org/content/pharmrev/30/4/local/... · 2005-07-26 · INDEX 469 intissues withremote involvement withnervous system, 80 inbloodcells,93](https://static.fdocuments.net/doc/165x107/5f7f8afccf762d253719f201/index-2005-07-26-index-469-intissues-withremote-involvement-withnervous-system.jpg)