
Drug Therapy of Gout. What Is Gout? A medical condition caused by an increase in the level of uric...
54
Drug Therapy of Gout
-
Upload
deborah-horton -
Category
Documents
-
view
218 -
download
1
Transcript of Drug Therapy of Gout. What Is Gout? A medical condition caused by an increase in the level of uric...

Drug Therapy of Gout

What Is Gout?
A medical condition caused by an increase in the level of uric acid >> urate crystals , causing inflammatory responses around some joints of the body ( Gouty arthritis )

Case presentation ( Gouty arthritis)
• 55 y/o male• 12 hours “pain in my big toe & ankle”• went to bed last night feeling fine• felt as if had broken toe this morning• PMH of similar problems in right
ankle & left wrist

Gout - acute arthritis
acute synovitis, ankle & first MTP
joints
The metatarsophalangeal articulations are the joints between the metatarsal bones of the foot and the proximal bones
Redness and swelling are noticed around those joints in particular
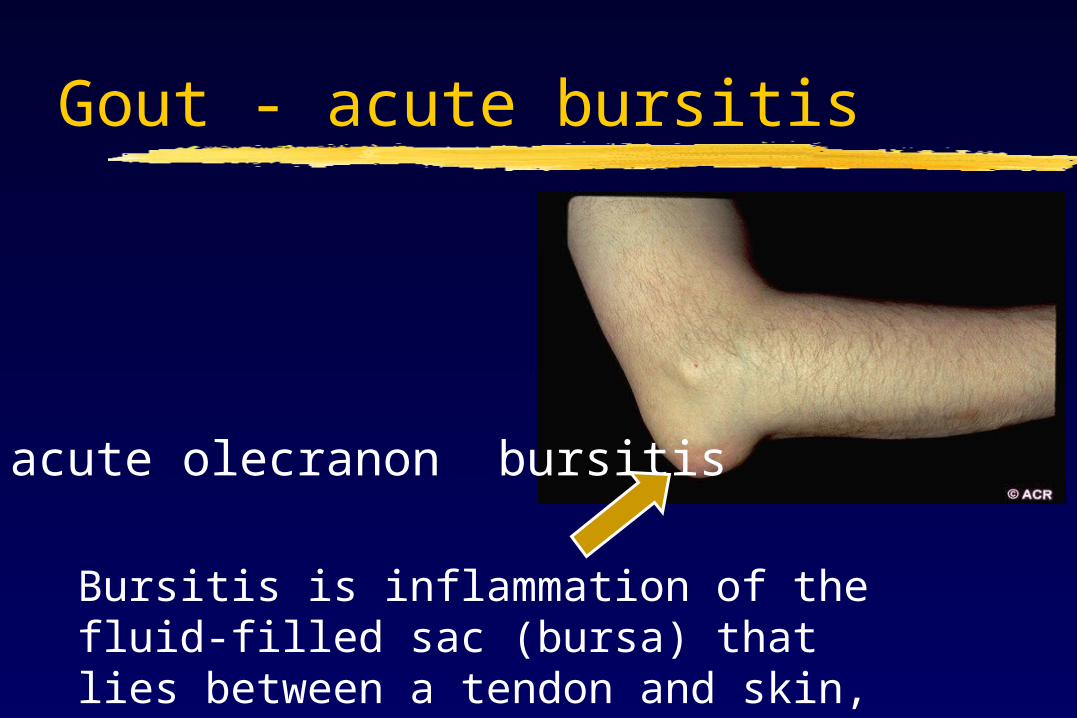
Gout - acute bursitis
acute olecranon bursitis
Bursitis is inflammation of the fluid-filled sac (bursa) that lies between a tendon and skin, or between a tendon and bone

Gouty arthritis - characteristics
• sudden onset• middle aged males• severe pain• distal joints• Intense
inflammation
• recurrent episodes• influenced by diet
( since uric acid level is influenced by our dietary intake of purines)
• bony erosions on Xray

Monosodium urate crystals
1-polarized light 2-red compensator
1-needle shape
2-negative birefringence (Birefringence: double streams of light, usually in prisms, etc)
Diagnosis is done by taking a biopsy from the synovial fluid and then examined either by:
These crystals show :

Crystal-induced inflammation (from gout to gouty arthritis )
PMN is critical
component of crystal-induced
inflammation
crystal deposition
(blood stream)
hyperuricemia
protein binding
receptor binding
(Synovial joints )
cytokine release
influx of PMN’s
(Macrophages )
crystals engulfed
inflammation

Gouty arthritis - characteristics
• sudden onset• middle aged males• severe pain• distal joints• intense
inflammation
• recurrent episodes• influenced by diet• bony erosions on
Xray• Hyperuricemia
(always)
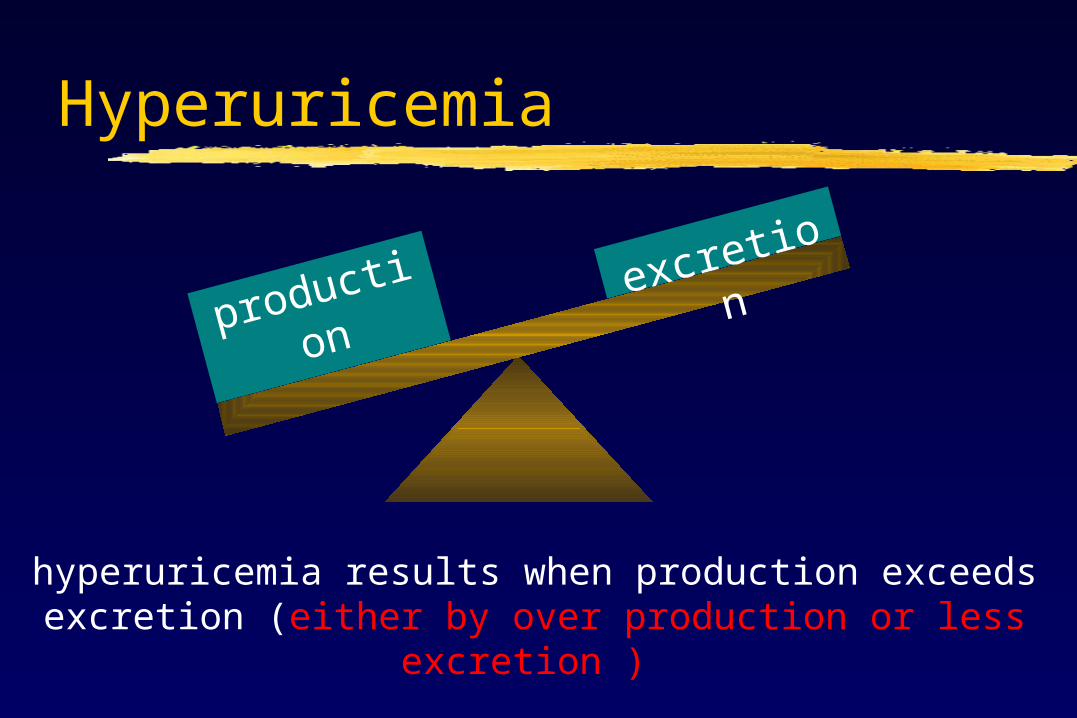
Hyperuricemia
productio
n
excretion
hyperuricemia results when production exceeds excretion (either by over production or less
excretion )

Hyperuricemia
productionexcretion
net uric acid loss results when excretion exceeds production

Chronic tophaceous gout
tophus = localized deposit of monosodium urate crystals
** could also be in several places in the
body

Gout - tophus
classic location of tophi on helix
of ear

Gout - X-ray changesDIP (Distal interphalangeal joint) joint destructionphalangeal bone cysts

Gout - X-ray changes
bony erosions

acute &
chronic
chronic
Gout - cardinal manifestations
Nephrolithiasis
(Kidney stones)
nephropathy
arthritis tophi
HYPERURICEMIA
*kidneys should be functioning well in order to use classical treatment

Drug therapy of gout
Treatment targets either :1- Decrease Uric Acid Formation 2- Increase Uric Acid Excretion

Uric acid metabolism
cell breakdown
dietary intake
purine bases
hypoxanthine
xanthine
uric acid
xanthine oxidase
catalyzes hypoxanthine to xanthine & xanthine to
uric acid
One method of reducing uric acid levels , is inhibition of the enzyme xanthine oxidase

Renal handling of uric acid
•glomerular filtration
•tubular reabsorption
•tubular excretion
•post-secretory reabsorption
•net excretion
Fate of uric acid in kidneys :Uric acid
Uric acid
Uric acid
Uric acid
The goal of some Gout Drugs, is to Increase the net excretion of uric acid from the kidneys.

The goal of some Gout Drugs, is to Increase the net excretion of uric acid from the kidneys
Non steroidal anti-inflammatory Drugs are sometimes used in the treatment of Gout ( cause increase in excretion )
Aspirin on the other hand is never used

Gout - problems
• excessive total body levels of uric acid
• deposition of monosodium urate crystals in joints & other tissues
• crystal-induced inflammation

Treating acute gouty arthritis
• colchicine• NSAID’s• steroids• rest, analgesia, ice, time

Drugs used to treat gout
allopurinol
probenecid
febuxostat?
steroids
NSAID’s
colchicine
Acute Arthritis Drugs
Urate Lowering Drugs
For chronic cases
rest + analgesia + time
It’s a new drug that’s being developed

NSAID’s
•Indomethacin (Indocin) 25 to 50 mg four times daily•Naproxen (Naprosyn) 500 mg two times daily•Ibuprofen (Motrin) 800 mg four times daily•Sulindac (Clinoril) 200 mg two times daily•Ketoprofen (Orudis) 75 mg four times daily
Drugs used to treat gout
*Don’t memorize the doses, just the names ** Remember that Aspirin is never used

Colchicine - plant alkaloid
colchicum autumnale
(autumn crocus or meadow
saffron)

Correction for the previous lecture
Colchicine is used to prevent the polymerization of the cell’s cytoskeleton by binding to TUBULIN ( not Actin)

Colchicine
• “only effective in gouty arthritis” ( it only works on the inflammation process , and has nothing to do with uric acid levels .)
• not an analgesic• does not affect renal excretion of uric acid• does not alter plasma solubility of uric acid• neither raises nor lowers serum uric acid

Colchicine
• Colchicine inhibits microtubule polymerization by binding to tubulin, one of the main constituents of microtubules
• reduces inflammatory response to deposited crystals
• diminishes PMN phagocytosis of crystals• blocks cellular response to deposited
crystals

Crystal-induced inflammation
PMN is critical
component of crystal-induced
inflammation
crystal deposition
hyperuricemia
protein binding
receptor binding
cytokine release
influx of PMN’s
crystals engulfed
inflammation

Colchicine - indications
Dose Indication
hightreatment of acute gouty arthritis
lowprevention of recurrent gouty arthritis
It’s better to use xanthine oxidase inhibitors for

Colchicine - toxicity
• gastrointestinal (nausea, vomiting, cramping, diarrhea, abdominal pain)
• hematologic (agranulocytosis, aplastic anemia, thrombocytopenia)
• muscular weaknessadverse effects dose-related & more common
when patient has renal or hepatic disease
Associated with high doses :

Gout - colchicine therapy
• more useful for daily prophylaxis (low dose)prevents recurrent attackscolchicine 0.6 mg qd - bid
• declining use in acute gout (high dose)

Colchicine - Cancers
• Promising studies have recently shown that Colchicine could be used for treating tumors
• HOW ?• Since Colchicine prevents the formation of
microtubules , this could be useful in limiting the mitotic activity of tumors cell : by preventing the formation of mitotic spindles (microtubules .)

Hyperuricemia - mechanisms
hyperuricemia
excessive production
inadequate excretion

Urate-lowering drugs
net reduction in total body pool of uric acid
block production
enhance excretion

Gout - urate-lowering therapy
• prevents arthritis, tophi & stones by lowering total body pool of uric acid
• not indicated after first attack• initiation of therapy can worsen or
bring on acute gouty arthritis• no role to play in managing acute gout
Xanthine Oxidase as an example

Drug therapy of gout
Drugs That Block Production of Uric Acid

Uric acid metabolism
cell breakdown
dietary intake
purine bases
hypoxanthine
xanthine
uric acid
xanthine oxidase
catalyzes hypoxanthine to xanthine & xanthine to
uric acid
Allopurinol (Zyloprim™)
• inhibitor of xanthine oxidase• effectively blocks formation of uric
acid• how supplied - 100 mg & 300 mg
tablets• pregnancy category C
allopurinol**Drugs are characterized according to their effects on pregnancy (fetus) into several categories A,B,C,D,X.A is the safest, X: completely dangerous and should not be given to pregnant women **benefits from taking the drug must outweigh it’s risks in order for it to be used.

Allopurinol - usage indications
• management of hyperuricemia of gout
• management of hyperuricemia associated with chemotherapy
• prevention of recurrent calcium oxalate kidney stones

Allopurinol - common reactions
• diarrhea, nausea, abnormal liver tests• acute attacks of gout• rash
*Manufactures are obliged to put a special indication on each leaflet ( a BLACK BOX) , that explains the serious side effect for that particular drug e.g Isotretinoin is a highly teratogenic Drug that should have a BLACK BOX
**For Allopurinol you might find that BLACK BOX sometimes , because certain people have shown to have allergy for it .
Allopurinol - serious reactions
• fever, rash, toxic epidermal necrolysis• hepatotoxicity, marrow suppression• vasculitis• drug interactions (ampicillin(antibiotic),
thiazides(diuretic ), mercaptopurine, azathioprine(anti-cancer)
• death

Stevens-Johnson syndrome
Mucocutaenous ulcerations
target skin lesions
mucous membrane erosions
epidermal necrosis with skin detachment
Another serious side effect , characterized by :
Those side effects are treated by systemic corticosteroids

Allopurinol hypersensitivity
• extremely serious problem• prompt recognition required• first sign usually skin rash• more common with impaired renal
function• progression to toxic epidermal
necrolysis & death

Febuxostat
• recently approved by FDA (not on market)• oral xanthine oxidase inhibitor• chemically distinct from allopurinol• 94% of patients reached urate < 6.0 mg/dl• minimal adverse events• can be used in patients with renal disease

PEG-uricase (Polyethelene Glycol)
• Uricase: enzyme that degrades uric acid
• investigational drug• PEG-conjugate of recombinant porcine
uricase• treatment-resistant gout• uricase speeds resolution of tophi• further research needed

Drug therapy of gout
Drugs That Enhance Excretion of Uric Acid

Uricosuric therapy
• probenecid• blocks tubular reabsorption of uric
acid• enhances urine uric acid excretion• increases urine uric acid level• decreases serum uric acid level

Uricosuric therapy
• moderately effective• increases risk of nephrolithiasis• not used in patients with renal
disease• frequent, but mild, side effects
Uricosuric therapy
• contra-indicationshistory of nephrolithiasiselevated urine uric acid levelexisting renal disease
• less effective in elderly patients

Choosing a urate-lowering drug
hyperuricemia
excessive production
inadequate excretion
xanthine
oxidase inhibito
r
uricosuric agent
Drug therapy of gout
Case Presentation
Refer to the third slide

Case presentation - therapy
NSAID
steroid
colchicine (low-dose)
allopurinol
NSAID
days 1-10 days 11-365 days 365+
Anti-inflammatory
Maintenance dose
Chronic condition

Done by Anas Khalil With the help of shaima shahin’s Notes
![· UU \ \ ]ùP ^ \ ]°P ^ \ &¶ &¶k ! \ &¶ W V \ðá Acute gout Chronic gout Uric Acid Monosodium urate crystal Purine Bu- &'EnND< • "G](https://static.fdocuments.net/doc/165x107/5e214ac52f885c72967c3a6b/uu-p-p-k-w-v-acute-gout-chronic.jpg)















![This student paper was written as an assignment in …Fig 2. Gout arthritis [from online sources] RN Rodionov Urate page 4 of 11 4. Chemistry of uric acid Uric acid, Mr 168.1, white](https://static.fdocuments.net/doc/165x107/5f2450aab1c9e17ae616d4ab/this-student-paper-was-written-as-an-assignment-in-fig-2-gout-arthritis-from-online.jpg)

