Drug Abuse in Pregnancy
91
Substance Abuse in Pregnancy
-
Upload
crystal-gayle-nario-sabado -
Category
Documents
-
view
14 -
download
0
description
ppt on drug abuse
Transcript of Drug Abuse in Pregnancy

Substance Abuse in
Pregnancy

Title

Substance Abuse During Pregnancy (SAMHSA, 2005)
• Pregnant women are less likely to use substances than their peers.
• The exception is pregnant women aged 15 to 17; this substance use rate is 26 percent for pregnant women, compared with 19.6 percent for non-pregnant women.

• Women more prone to substance abuse:– Earn below poverty level – Were exposed to violence as a child– Have a history of domestic abuse – Have less than a high school education– Are unmarried– Are unemployed– Are involved with the criminal justice system– Suffer depression or other mental health
problems

Most Commonly Abused Substances During Pregnancy
• Alcohol• Tobacco• Caffeine – incidence unknown, purportedly very high• Benzodiazepines• Opiates• Cocaine• Ecstasy• Hallucinogens • Methamphetamine• Solvents• Other


Impact of Substance Abuse
Alcohol Tobacco Cannabis Amphetamine Cocaine Opioids
Miscarriage + + + + +
Fetal Morbidity + + + +
Perinatal Mortality + + +
IUGR + +
PROM + +
Preterm Delivery + + + +
LBW + + + + +
Neonatal Resp. +
Neonatal Withdrawal + +
Developmental + + + +

Alcohol use in Pregnancy
• There is no safe amount of alcohol consumption during pregnancy
(Jones & Chambers, 1999).

Alcohol Use in Pregnancy: Maternal Effects
• Cardiovascular and liver disease• Breast and gynecological cancer• Osteoporosis• Menstrual symptoms • Neurological and mental health
problems• Compromised ability to conceive • Spontaneous abortion
Alcohol Use in Pregnancy: Fetal Effects
• Abnormalities in brain and neuron development
• Growth deficiency • Structural changes• Prematurity• LBW • Decreased length and head circumference

Alcohol Use in Pregnancy: Neonatal Effects
• Fetal alcohol syndrome (FAS)
• Mental retardation
• Developmental, learning and behavior problems
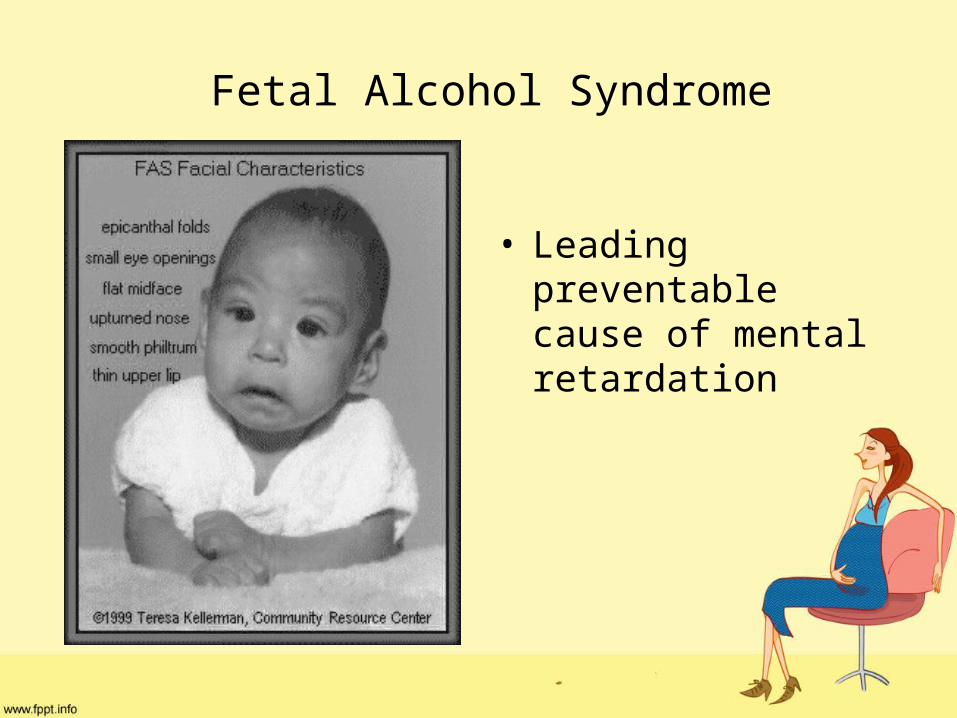
Fetal Alcohol Syndrome
• Leading preventable cause of mental retardation

Symptoms of a baby with FAS
• Poor growth while the baby is in the womb and after birth
• Decreased muscle tone and poor coordination
• Delayed development and significant functional problems in three or more major
areas:
thinking, speech, movement, or social skills (as expected for the baby's age)

• Heart defects such as ventricular septal defect (VSD) or atrial septal defect (ASD)
Structural problems with the face, including: • Narrow, small eyes with large epicanthal fold• Small head• Small upper jaw• Smooth groove in upper lip• Smooth and thin upper lip


Fetal Alcohol Syndrome: Tests
• Blood alcohol level in pregnant women who show signs of being drunk (intoxicated)
• Brain imaging studies (CT or MRI) shows abnormal brain development
• Pregnancy ultrasound shows slowed growth of the fetus
• Toxicology screen

Alcohol Use Assessment
• Women are quite reliable in reporting alcohol use in pregnancy (Jacobson et al., 2002).
• The TWEAK is used to screen pregnant women for alcohol misuse.

TWEAK Alcohol Dependence Screening Tool
T Tolerance How many drinks does it take to make you feel high?
W Worry Have close friends or relatives worried or complained about your drinking in the past year?
E Eye-Opener
Do you sometimes have a drink in the morning when you firstget up?
A Amnesia
(blackouts)
Has a friend or family member ever told you about things yousaid or did while you were drinking that you could notremember?
K Cutting down
Do you sometimes feel the need to cut down on yourdrinking?


Smoking while Pregnant
• Cigarettes, cigars, pipes, “snuff,” “chew”
• Stimulant & relaxes
• Acute effects–Vasoconstriction secretions

• Lower the amount of oxygen available to you and your growing baby
• Increase your baby's heart rate
• Increase the chances of miscarriage and stillbirth
• Increase the risk that your baby is born prematurely and/or born with low birth weight
• Increase your baby's risk of developing
respiratory (lung) problems
• Elevates the risk of having a child with
excess, webbed or missing fingers and toes

• Chronic effects– Lung disease, heart disease– Cancer
• Very short-acting, so high-frequency use– Very reinforcing

Maternal Effects:
• Cigarette smoking is the most common form of substance abuse in pregnancy. It is linked to:
• Decreased fertility• Spontaneous abortion• Placenta previa• Placental abruption• Ectopic pregnancy• Preterm premature rupture of membranes
(PPROM)• Preeclampsia

Fetal Effects
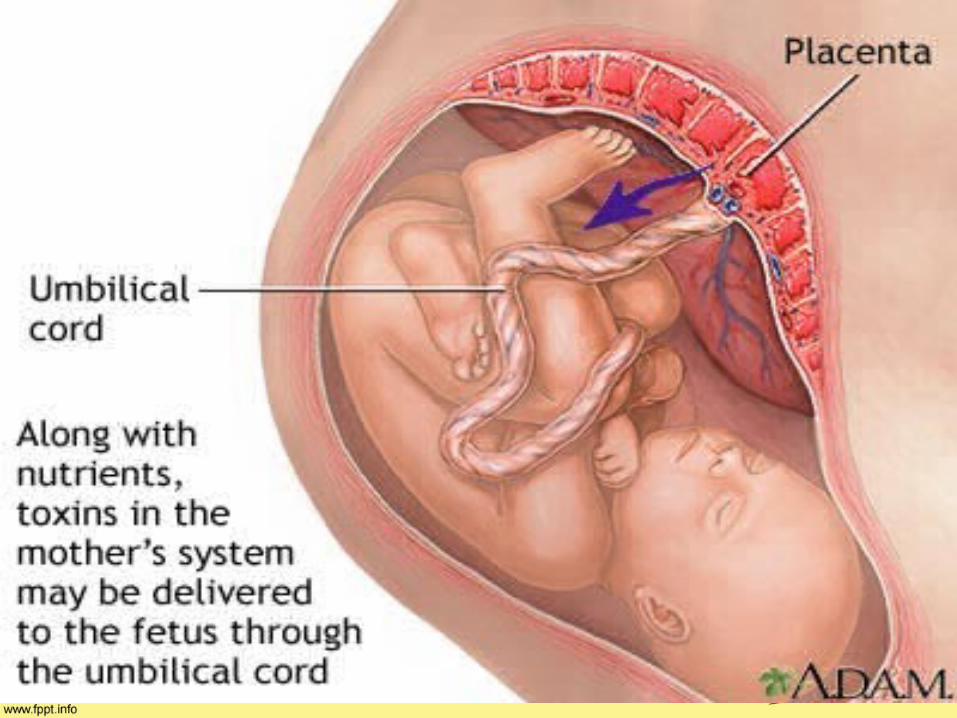
• Impaired transfer of oxygen and nutrition
• Long-term cognitive function and increased risk of brain damage
• Chronic low-level hypoxia
• Intrauterine growth restriction (IUGR)
• Preterm delivery
• Low birthweight (LBW) in term infants

Neonatal Effects
• Impaired respiratory function in premature infants
• Low neurobehavior scores and higher withdrawal-symptom scores
• Asthma, respiratory illness and pneumonia
• Infections of the middle ear
• Increased risk of cancer and SIDS
Nicotine Withdrawal in mother
• craving for tobacco• irritability, frustration,
anger• anxiety• difficulty concentrating• restlessness
• decreased heart rate• increased appetite or
weight gain• depression• disrupted sleep• sedation
Smoking Treatment:
• Self-Determination Model
• The nurse uses motivational interviewing or autonomy-promoting counseling to elicit the woman’s personal values and goals.
• The nurse and woman explore the aspects of unhealthy behavior, focusing on the discrepancy between the desired goals and the behavior.

Smoking Treatment: The Five A’s (Fiore et al., 2000)
1. Ask about tobacco use.2. Advise to quit.3. Assess willingness to quit.4. Assist in attempting to quit.5. Arrange follow-up.
The Five A’s are recommended for patients who are willing to quit.

Smoking Treatment: The Five R’s (Fiore et al., 2000)
1. Relevance of quitting
2. Risks of continued smoking
3. Rewards of quitting
4. Roadblocks to quitting
5. Repetition
The Five R’s are recommended for patients who are unwilling to quit.

Smoking Treatment: Follow-up During Pregnancy
• Follow-up should focus on how the effort is going; support and reinforcement for even small successes; suggestions to overcome obstacles; and health progress reports.

Smoking Treatment: Bupropion (Zyban)
• Used as an antidepressant and as a smoking cessation aid
• Shows no harmful effects on pregnant women treated for depression (Kuller et al., 1996)

Opioids
• Morphine, heroin, OxyContin, methadone
• Analgesics: disconnect from pain
• Euphoria, disconnection, sedation
• Nausea, constipation, itching
• Oversedation, respiratory depression

• Obstetric complications increase up to six fold1,11: – SAB– LBW– IUGR– Preeclampsia– Placental abruption– PROM– PTB– Fetal distress– Fetal demise– Malpresentation, Low APGAR scores, PPH, septic
thrombophlebitis, Meconium aspiration, Chorioamnionitis

Effects on Fetus• No known fetal anomalies
• Intrauterine growth retardation
• Neonatal abstinence syndrome– Continuous exposure
– Use up to delivery

• Neonatal complications3,1:– Prematurity– Low birth weight– Postnatal growth deficiency– Microcephaly– Neurobehavioral problems*– Increased neonatal mortality– 74-fold increase in sudden infant death
syndrome (SIDS)– Neonatal abstinence syndrome (NAS)

• 60-90% of opiate
exposed infants develop
neonatal abstinence
syndrome (NAS).• Symptoms will • manifest within • 48 to 72 hours
after birth

S/S of Neonatal Abstinence Syndrome
– Withdrawal– Irritability– Tremors– High-pitched cry– Diarrhea & Vomiting– Respiratory Distress– Abrasions– Weight loss– Aberrant temp control– Lack of sucking– Sneezing
Signs of Neonate Withdrawal• Irritability• Tachypena• Tremors• Shrill Cry• Mottling• Hypertonicity of muscles• Frantic Sucking of hands• Temperature instability• Loose diarrheal stools• Seizures• Nasal stuffiness• Sleep Disturbances

CLINICAL SIGNS associated with Opiate Withdrawal in Newborns
• Central Nervous System Dysfunction
• Autonomic Dysfunction
• Respiratory Dysfunction
• Gastrointestinal Dysfunction
• Heroin– Passage through placenta to fetus within 1
hour of administration– Accumulates in amniotic fluid– Limited fetal detoxification due to immature
tissues– Fluctuation in drug levels causes placental
changes* placental insufficiency and IUGR
– More significant placental change and LBW than methadone or buprenorphine.

• Preferred over illicit substance abuse:
– less drug-seeking and criminal behavior, fewer relapses, decreased STDs, improved prenatal care and compliance, improved nutrition3
– Consistent maintenance opioid treatment prevents repeated fetal withdrawals.
HeroinMaternal Effects
•Heroin can cause severe physiological withdrawal symptoms, including fatal seizures when withheld for 12 to 48 hours.
Heroin: Fetal Effects• Opiates, such as heroin, methadone and
buprenorphine, have not been linked to fetal anomalies.
• Fetal withdrawal responses include arrhythmias, seizure activity and fetal demise.

Heroin: Neonatal Effects• Drug withdrawal • Suck-swallow difficulties • Central nervous system (CNS) irritability• Gastrointestinal upset• Yawning• Sneezing• Frantic sucking with uncoordinated feeding• High-pitched cry• Increased or decreased muscle tone
Heroin: Treatment• Methadone
–The most common treatment for heroin abuse in pregnant women
–During pregnancy, brings addicted women into agencies that promote prenatal care
• Buprenorphine –Linked to better treatment adherence with
fewer side effects and overdoses than methadone

Opioid Maintenance
• Methadone
• Subutex (Buprenorphine)
• Suboxone (Buprenorphine/Naloxone)
• Oral slow release morphine
1 g heroin ~ 8 mg buprenorphine ~ 80 mg methadone

Methadone
• Pregnancy Category C
• Full opioid agonist
• First-line treatment of opioid addiction in pregnancy in the US2,5,6, UK, and Australia1.
• Requires daily visits to methadone clinic.*

Methadone
• Higher infant BW and less IUGR than seen in heroin-addicted moms.1,8
• NAS in 60-100% of neonates
• Longer duration of NAS treatment vs. buprenorphine & heroin – 30 days vs. 11-12 days tx

Methadone
• However, some experts believe that, when compared to buprenorphine, methadone is the preferred medication:– They report buprenorphine has a “ceiling” dose, which
is surpassed by some woman…thus they require higher levels of opioid maintenance that can only be reached with methadone.
– Less structured regimen of buprenorphine tx vs. daily methadone dosing may lead to gaps in prenatal care, in addition to diversion or IVDA of buprenorphine.

• Standard of care for opioid-dependent pregnant women
• Stabilization of mother and fetus– Medical and social– Higher dose in 3rd trimester
• Improves growth of fetus & newborn
• Decreases practice of high-risk behaviors

Subutex
• Buprenorphine (Category C)• Long-acting partial mu opioid agonist & kappa
antagonist• While approved in the US for opioid detox &
maintenance, is not FDA-approved for use during pregnancy.*
• However, is considered safe in pregnancy.• First choice for opioid maintenance programs &
in pregnant women in Finland3 since 1996.
Subutex
• May have less placenta exposure than methadone
• Partial agonist profile may lower liability for NAS
• Cochrane Review6 favored buprenorphine over methadone in regards to:– Higher infant BW*– Shorter hospital stay

Subutex• Low rates of prematurity2 (ave 39.2
wks)• NAS occurs in 62%, but only half
require treatment• Less severe NAS than methadone
(though no RCTs yet*) with ↓ incidence and ↓ need for pharmacologic treatment vs. methadone.
• Shorter duration of NAS treatment vs. methadone
Subutex
• Preliminary MDFMR stats show:– None were low BW– All had APGARS of 8 or greater at 1 and 5
minutes– Possible dose-dependent relationship– Unable to draw conclusions about when
babies may develop withdrawal symptoms– High degree of variability in the frequency of
NAS scoring

Suboxone
• Buprenorphine (Category C) + Naloxone (Category B)
• Limited studies in pregnant women.• US DHHS Center for Substance Abuse Tx:
– cautious use of naloxone in opioid-addicted pregnant women may precipitate withdrawal in both mother & fetus.
– Recommends buprenorphine monotherapy, though admit it has great potential for abuse & diversion.
Opioid Maintenance – Monitoring in pregnancy
• UDS, UDS, UDS
• At increased risk for: anemia, malnutrition, HTN, hyperglycemia, STDs, TB, hepatitis, and preeclampsia.
– Regular Prenatal panel– LFTs, Renal function, PPD, glucose intolerance, anti-
HCV antibody– Consider repeat CBC, serology at 24-28 wks.
Opioid Maintenance dosing in pregnancy
• Varied opinion on monitored detoxification & abstinence during pregnancy.
• If attempt to wean, suggested in 1st vs. 2nd Trimester– 1st – theoretical risk of miscarriage11
– 3rd – risk of premature labor or fetal death11
• Generally not recommended– Higher methadone doses related to increased BW,
prolonged gestation11
– Attempt to decrease incidence of NAS by weaning may cause continued substance abuse11
Opioid Maintenance dosing in pregnancy
• In fact, increased dosage of maintenance therapy may be required in 2nd-3rd trimester:
– Increased maternal fluid volume + altered opioid metabolism in placenta & fetus same dose produces lower blood level of particular drug11

Pain Management during Labor & Delivery
o Opioid-dependent patients may require higher and more frequent doses of opioid analgesics to maintain pain control.
Methadone & buprenorphine suppress opioid withdrawal for 24-48 hours, but only provide analgesia for 4-8 hours.4

Pain Management during Labor & Delivery
• NO Stadol or Nubain!– Opioid agonist-antagonists, thus can displace
the maintenance opioid from the mu receptor, precipitating acute withdrawal4
• Epidural use reported in 73% of deliveries to opioid-dependent mothers.8
Cocaine
• Not teratogenic
• Neonatal complications– LBW– ↓ HC and birth length– IUGR– Increased incidence of infant infection with
hepatitis & HIV

Cocaine• Increase the risk of miscarriage• When the drug is used late in pregnancy, it may
trigger premature labor• It also may cause an unborn baby to die or to have a
stroke, which can result in irreversible brain damage• More likely to have a low birth-weight baby• More likely to have babies born with smaller heads
and smaller brains proportionate to body size• Twice as likely to have a premature baby• Placental abruption• Baby with a malformation of the urinary tract• Feeding difficulties and sleep disturbances in
newborn

• Early studies cited severe and irreversible consequences of prenatal cocaine exposure due to disruption of CNS of developing brain.
• However, more recent studies show little or no long term developmental effects of prenatal cocaine exposure.
• Lack of data on older children precludes any absolute statements that cocaine exposure in utero has no long term effects.
Cocaine
• Local anesthetic – blocks sodium channels
• Blocks reuptake of dopamine, norepinephrine and serotonin in CNS.
• Euphoria, hypertension, tachycardia, vasconstriction, coronary vasospasm, thrombosis.

Cocaine
• Increases vascular cell adhesion molecules (promoting white cell infiltration into tissues)
• Promotes thrombosis
• Cocaine is like obesity and hyperglycemia in this respect!

Cocaine: Maternal Effects
• Hypertension
• Tachycardia
• Cardiac events and maternal death
• Spontaneous abortion
• Placental abruption
• Premature rupture of membranes (PROM)

Cocaine: Fetal Effects
•Fetal effects of cocaine are caused by the drug’s direct effects (vasoconstriction and neuroexcitation) and by lifestyle issues that maternal drug use brings, including poor nutrition and avoidance of prenatal care.

Cocaine: Neonatal Effects
• Jitteriness• Hyperactivity• Inconsolability• Poor feeding and state regulation• No physiological withdrawal: Neonates are
not dependent on cocaine and do not need medication to lessen withdrawal.

AmphetaminesMaternal Effects
• Stroke
• Cardiac problems
• Psychiatric emergencies
• Growth restriction
• Placental abruption
• Preterm delivery

Amphetamines: Fetal and Neonatal Effects
• Similar effects to cocaine, with decreased fetal growth
• Some researchers expect that, like with cocaine (Wouldes et al., 2004), effects can be seen early in life but are quickly overpowered by environmental factors.

MDMA (Ecstasy): Maternal Effects
• Anxiety
• Twitching
• Depression
• Impaired cognitive processing and memory performance

MDMA: Fetal and Neonatal Effects
• Animal studies do not show an increase in harmful fetal effects.
• A small, uncontrolled, retrospective study suggests a possible increase in ventricular septal defects (Bateman et al., 2004).
• Nurses should treat infants and families based on demonstrated health needs.

Introducing Social Issues
•The nurse should begin to explore the woman’s home situation, including:– Stress related to work, finances,
family and pregnancy– Satisfaction with the amount and
kind of support in her social network– Feelings about self-esteem and
ability to cope with stressors

• Benzodiazepines, barbiturates, other sleeping pills (Ambien, Lunesta)
• Sedation, anxiolytic• Respiratory
depression in overdose
• Withdrawal similar to alcohol DT’s

• Common to both:–Restlessness–Insomnia–Nausea/vomiting–High blood
pressure–Rapid heart rate–Rapid breathing–Seizures
• Seen in withdrawal, but not pregnancy:–Distractibility– Impaired memory–Agitation–Tremor–Fever–Sweating–Hallucinations
• Withdrawal symptoms may be life-threatening to mother and fetus
• Acute withdrawal treatment should be accomplished in an inpatient setting
• Risk to mother/fetus of untreated withdrawal is greater than risk from exposure to medications in a controlled setting
Marijuana• Marijuana, hashish,
hash oil
• active ingredient: THC
• relaxation, hallucination
• panic attacks
• short-term memory impairment, amnesia

Maternal Effects• Is the illicit drug most commonly used
during pregnancy, although only 3.6 percent of pregnant women report using it (SAMSHA, 2005)
• Does not cause a defined physical withdrawal syndrome
• Heavy use linked to lung problems

Effects on Fetus
• Intrauterine growth retardation
• Abnormal startle reflexes in newborns
• Reduced memory & verbal skills at age 4 years

Screening
• All pregnant women should be screened for drug and alcohol use– T-ACE: emphasizes tolerance
over guilt
• A positive screen indicates the need for further evaluation

Types of Treatment
• Detoxification• 12-Step groups• Outpatient counseling• Intensive outpatient• Inpatient• Residential• Opioid Maintenance
– Methadone– Buprenorphine

Addiction Counseling
• Network therapy• Family therapy• Supportive
psychotherapy• Contingency
management• Building Social
networks
• Twelve-Step facilitation
• Perceptual Adjustment therapy
• Rational Recovery• Medication
management• Brief intervention

Maintenance Pharmacotheraphy
• Long-acting medication in controlled setting– Counseling
– Social services
• Avoid withdrawal & craving• Reduce disease & crime• Maintenance vs. detoxification

• Pregnancy Category C• Use Subutex instead of
Suboxone to avoid naloxone
• NAS less intense than with methadone
• Studies ongoing, results encouraging
• Characterized by– Hyperactivity, irritable– Hypertonia– Difficulty/excessive sucking– High-pitched cries
• Begins 3h to 12d after delivery, depending on drugs used by mother
• Initial treatment is supportive–Swaddling, frequent feeding, IV fluids
• Assess regularly for symptoms and failure to thrive
• Pharmacotherapy–Usually opioids, occasionally sedative-hypnotic–Tincture of opium, paregoric, methadone,
phenobarbital

–Encourage involvement of significant other–Lack of support can lead to relapse
• Social services may need to be notified of unsafe living conditions
• Addicted pregnant woman often product of poor parenting
• Support network for new mother–Family, 12-Step group, health care workers

• Most common obstetrical effect of illicit drugs is low birthweight
• Methadone maintenance is treatment of choice for opioid-addicted pregnant women
• Breastfeeding is encouraged (as long as not actively using illicit drugs or alcohol)
• Support for mother is essential• Anticipate and educate to prevent relapse