Draft PIP of LUCKNOW - NATIONAL URBAN HEALTH …nuhm.upnrhm.gov.in/urban/pip/mahobapip.pdfof his...
33
Page | 1 Mahoba City Program Implementation Plan National Urban Health Mission Prepared by District Health Officials with support from Urban Health Initiative
Transcript of Draft PIP of LUCKNOW - NATIONAL URBAN HEALTH …nuhm.upnrhm.gov.in/urban/pip/mahobapip.pdfof his...

Page | 1
Mahoba City
Program Implementation Plan
National Urban Health Mission
Prepared by District Health Officials with support from Urban Health Initiative

Page | 2
NATIONAL URBAN
HEALTH MISSION
Programme Implementation Plan
MAHOBA
F.Y.2013-14

Page | 3
TABLE OF CONTENT
Preamble 3
Acknowledgement 4
Acronyms 5
City Profile 6-19
Health Scenario 20-23
Key Issues 24-26
Strategies, Activities & Work plan under NUHM 26-29
Programme Management Arrangements 30-31
City level targets & indicators 32

Page | 4
PREAMBLE
National Urban Health Mission aims to improve the health status of urban population in general and
the poor and other disadvantaged sections in particular. This would be made possible by facilitating
equitable access to quality health care through a revamped primary public health care system,
targeted outreach services and involvement of the community and urban local bodies. Under the
scheme, the government proposes to strengthen and enhance the health care service delivery in
urban areas with targeted focus on urban poor and the disadvantaged.
Mahoba with a population of 876055 (Census: 2011), is one small district in Uttar Pradesh (UP). An
estimated 95216 of the said population is poor. The current sex ratio for the urban areas is 901
females per thousand males which is an area of grave concern. The AHS-2010-11 reports that
institutional deliveries are around 59.7 % in the city and the IMR is 48% (AHS 2011-12) with MMR at
359 (AHS 2011-12) which again is a matter of concern. Complete immunization status of the district is
around 32.2 % (AHS 2010-11) . Unmet need for family planning services at the district level is 27.4
(AHS-10-11) and if we further examine the data, 18.4 % is for limiting and 9 % for spacing methods.
The health indicators for Mahoba show are way behind in so many aspects and the launch of
National Urban Health Mission, the efforts for improving the health parameters will complement
towards betterment of urban population and in particular to the urban poor & slum dwellers.
The NUHM planning for this financial year based on the data, surveys and available information at
city level and hoping that we will initiate the process very systematically so that we can make the
difference in improvement of quality life of urban people specially by reaching the unreached areas.
HUP – PFI deserves a very special mention for providing generous technical support in preparation of
City PIP.
Dr. Grish Kumar Kureel Anuj Kumar Jha (IAS)
Chief Medical Officer District Magistrate
Mahoba Mahoba

Page | 5
ACKNOWLEDGEMENT
Considerable efforts have been made by the team in preparing this Project Implementation Plan for
Mahoba under the newly announced National Urban Health Mission. This has been possible through
dedication, perseverance and hard work. This exercise of planning would not have been complete
without the help and support of the team.
We do not have hesitation in saying that this work would not have come up without the valuable
support and continuous encouragement of Shri Anuj Kumar Jha (IAS), District Magistrate, Mahoba
His great confidence in team and spurred us into action.
My special gratitude goes to Dr. G.K Kureel, Chief Medical Officer, Mahoba, a dynamic and
enthusiastic professional. He has always been a source of great encouragement for us. The initiation
and completion of this work has been possible due to his sincere and able guidance, expertise,
precious opinion, keen attention, constructive suggestions and constant help. His critical reading of all
the parts of the work has helped shape the NUHM planning in its present form.
I express my gratefulness to Shri. Amit Kumar Ghosh, IAS, Mission Director, National Health Mission
& Mr. Shashank Vikram, IFS, Additional Mission Director, NUHM for overarching support and
building the thoughts in our mind.
I own my sincere gratitude to Dr. M. R. Gautam (General Manager), Dr. Usha Gangwar, (Deputy
General Manager-NUHM) and HUP-PFI who have helped us immensely by providing relevant
information and valuable suggestions. This planning work got accomplished with their valuable
support and eagerness to help.
I am privileged to have such good city level team especially Shri Harit Saxena (Div.PMU), Smt.
Mamta Ahirwar (DPM NRHM), who have supported and helped in contributing their great efforts
towards planning of this city level plan under the NUHM.
I would also like to appreciate the precious help and motivation which I received from government line
department - DUDA, ICDS, Nagar Panchayat, Education department, CMS & DTO.
Last but not the least; I would like to thanks all those people who were involved in the planning
process directly or indirectly.
Dr. B.V.Verma
Add. CMO (RCH), Mahoba
September, 2013

Page | 6
Acronyms
ANM Auxiliary Nurse Midwife
ASHA Accredited Social Health Activist
AWC Aanganwari Center
AWW Aanganwari Worker
BSGY Bal Swasthya Guarantee Yojna
BSUP Basic services for urban poor
BSA Basic Shiksha Adhikari
CDPO Child Development Project Officer
DH District Hospital
DHS District Health Society
DUDA District Urban Development Authority
ICDS Integrated Child Development Scheme
IDSMT
Integrated Development of Small &
Medium Towns
IDSP Integrated Diseases Surveillance
Program
IHL Individual House level
IMR Infant Mortality Rate
KFA Key Focus Area
LHV Lady Health Visitor
LT Lab Technician
MAS Mahila Arogya Samiti
MMR Maternal Mortality Ratio
NHM National Health Mission
NPP Nagar Palika Parishad
NPSP National Polio Surveillance Program
NRHM National Rural Health Mission
NUHM National Urban Health Mission
OD Open Drainage
RSAP Remote Sensing Application Center
UA Urban Agglomeration
UCHC Urban Community Health Center
UFWC Urban Family Welfare Center
UHI Urban Health Initiative
UHP Urban Health Post
UPHC Urban Primary Health Center
SAM Severely acute Malnourishment

Page | 7
National Urban Health Mission- Programme Implementation Plan
Mahoba 2013-14
Mahoba Profile
Mahoba was the capital of the Chandel Rajputs, who ruled Bundelkhand from the 10th to the 16th
centuries. The Chandel king Vijaypal (1035–1045) built the Vijay-sagar reservoir, one of several
artificial lakes in Mahoba created by the Chandel rulers. During the reign of king Paramardi (c. 1165-?), the Chauhan king Prithviraj III of Delhi and Ajmer captured Mahoba c. 1182, despite the resistance of his generals Alha & Udal. The Chandelas recaptured Mahoba a few years later, but the city was
captured by the Muslim general Qutb-ud-din Aybak, later Sultan of Delhi, in 1203.
The Chandel ruler Keerat Pal Singh recaptured Mahoba in the 14th century. Emperor Sher Shah Suri campaigned against the Chandelas, and captured Mahoba before dying while besieging Kalinjar in
1545. The Mughal emperor Akbar captured Mahoba a few decades later.
The Bundela leader Maharaja Chhatrasal captured Mahoba in 1680, during the reign of the Mughal Emperor Aurangzeb. Upon his death in 1732, Chhatra Sal bequeathed Mahoba and the surrounding area to the Maratha Peshwa Baji Rao I in return for Baji Rao's assistance against the Mughals. The
Marathas ruled Mahoba until 1803, when it was ceded to British India by the Treaty of Bassein. Mahoba was made a subdivision of Hamirpur District.
The name Mahoba is derived from 'Mahotsav Nagar', the city of great festivals, which were celebrated
here by Chandra-Verman or Nannuka, The traditional founder of the Chandella Dynasty. The Bardic tradition preserves three other names of the City: Kekaipur, Patanpur and Ratanpur. These names are
said to have been current in the Treta and Dwapar Yugas. The existence of the sacred 'Ram-Kund' and 'Seeta-Rasoi' cave at the Gokhar hill here are said to be monumental to the visit of Rama who widely treated this hilly region while in 14-year exile at Chitrakoot.
Before the rise of Chandels, Mahoba was held by the Gahadvala and Pratihara clans of Rajputs. The
Chandela ruler Chandra-Verman, who hailed from Maniagarh, his birthplace near Panna, took it over from Pratihar rulers and adopted it as his Capital. Later, Vakpati, Jejja, Vijai Shakti and Rahila-deva
succeeded him.
Among the later Chandel rulers whose names are particularly associated with the local monuments are Vijai-pal (1035–1045) who built the Vijai-sagar lake, Keerti-Verman (1060-1100) built Keerat sagar tank and Madan-Verman (1128-1164) who built Madan Sagar. The last prominent Chandel ruler was
Parmardi-deva or Parmal whose name is still popular due to the heroic deeds of his two Generals 'Alha' and 'Udala' who own many battles. The court poet Jagnik Rao has made their names immortal
through his popular ballad (Veer-Kavya) 'Alha-Khand'. It is recited throughout the Hindi speaking masses in the country. In 1860, an English Officer of the East India Company, Mr. William Waterfield was so impressed with the ballad that he translated it into English under the title name of 'Lay of Alha'
which was published by the Oxford University Press of England. Another prominent scripture which

Page | 8
has an account of Mahoba's grandeur is the Jain text 'Prabhandh-kosh' which refers to its magnificence which could only be realized and not described.
The reign of Parmardi-deva or Parmal, the Fifteen ruler of the dynasty, witnessed the fall of Mahoba.
In 1182, differences arose between Parmala and Delhi king Prithviraj who gave an ultimatum lying certain conditions to be fulfilled by Parmala or to surrender. He made seize of Mahoba and his General
Chaumund Rai even made a surprise attack on the Kajli procession of queen Malhna who hadgone to Keerat Sagar tank to offer Kajli Pooja on the Raksha-Bandhan day. A grim fight ensued in which Mahoba warriors:Udala, Brahma, Ranjeet, and Abhai (son of Mahila) repulsed the attack and
Chaumund-Rai had to flee to his base camp at Pachpahara. The Kajli-Pooja was consequently celebrated the next day and that tradition continues to be followed even to this date. The third day is
observed as a Victory Day and a thanks-giving Pooja is performed to Lord Shiva, Gajantak Shiva idol on Gokhar hill.
Later, the Chauhan King Prithvi Raj captured Mahoba despite the brave fight put up by the Banafer
brothers, Alha and Udal. Other warriors of Mahoba, viz. Udal, Brahma, Malkhan, Sulkhan, Dheba and Tala Saiyyad, etc., laid down their lives in the battle. Parmala had to retreat to Kalinjar leaving Mahoba in the hands of the conqueror. Prithvi Raj appointed his Thanapati Pajjun Rai as his
administrator. A few years later, he was driven out by Samarjeet, son of Parmala. This, however, could not stop the beginning of the end of Chandella rule. Two decades later, Qutubuddin Aibek vanquised
Mahoba and Kalinjar in 1203. Aibk took away immense booty with thousands of artisans as prisoners. He deported most of them to Ghazni as slaves, who constructed beautiful buildings there. Later, Trailokya Verman, another son of Parmala, recovered Mahoba and Kalinjar but the Chandellas lost
their eminence. Mahoba lost its independence and became part of the Delhi Sultanate.
After about two centuries of obscurity a notable Chandel ruler Keerat Pal Singh rose to power and re-established his domain over Kalinjar and Mahoba. His illustrious daughter Durgavati was married to
Gond ruler Dalpat-shah of Garh Mandla(near Jabalpur) in 1543 . Later, Keerat Pal Singh battled bravely with Sher Shah Suri, while defending Kalinjar fort in 1545. Sher Shah, however, captured the fort after a prolonged fight but was killed in an explosion while directing final assault on the fort.
The account of Rani Durgavati's deeds is most glorious. She administered her territory admirably well
after the death of Raja Dalpat Shah and in 1564. gallantly resisted the unprovoked aggression of Mughal emperor Akbar, whose general Asif Khan attracted Garh Mandla to annex Rani's territory.
The Rani gave a brave fight but lost her life in the battle-field.
In the post Chandella period the history of Mahoba gets obscure. It was under the reign of Delhi Sultans. Local traditions ascribe and associate Bhars, Gonds and Khangar clans who held its administration from time to time. However, during the reign of akbar, it was constituted into a 'Mahal'
in the Sarkar of Kalinjar within the Suba of Allahabad. According to 'Aine-Akbari, it had an area of 82,000 Bighas yielding a revenue of over 40,42000 Dams[clarification needed] in addition to 12,000 Pans
(Betel-leaves) to the Moghal Darbar. Mahoba has been famous for its betal-leaves cultivation ever since the first Chandella ruler Chandra-Verman who adopted it as his capital. During the Moghal period the revenue assessment of Mahoba suggests a high degree of prosperity in comparison to the
neighbouring 'Mahals'.

Page | 9
Later, with the rise of Chhatrasal Bundela, Mahoba passed under his sway but failed to acquire and kind of pre-eminence. In the 17th century Chhatrasal declared independence and put a stiff resistance
against Aurangzeb. He established a Bundella Principality and Bahadur Shah Moghal had to confirm all his acquisitions in the area called 'Bundelkhand'. There was a revival of hostilities during the region
of reign of Farrukhsiyar when his general Mohammed Khan Bangash invaded Bundelkhand in the year 1729. and the aged ruler Chatrasal had to seek aid from Peshwa Baji rao. His 'Maratha' army of 70,000 men dashed from Indore (Malwa) and encamped at Mahoba. They surrounded forces of nawab
Banghash who had captured Jaitpur, Belatal, Mudhari and Kulpahar etc. The Peshwa inflicted a crushing defeat over the Nawab by annihilating his forces in the dense forests of Jaitpur, Mudhari and
Salat etc. In return for this help, Chhatrasal bequeathed one third of his dominion to the Maratha Chieftain. That part included Mahoba, Shri Nagar, Jaitpur, Kulpahar etc. Later, under the treaty Bessien in 1803 the marathas ceded Bundelkhand area to British rulers. Its administration was,
however, carried over by the subedar of Jalaun until 1858 when it was finally annexed by the East India Company. Mahoba was made the head-quarter of a sub-division in the district of Hamirpur. Its
later history is un-eventful except for the local revolt in the first freedom struggle of 1857 when the British Sub-divisional Magistrate, Mr Carne, had to flee and seek refuge in the nearby Charkhari estate which was being ruled by Raja Ratan Singh. The Rani of Jhansi, got annoyed over this betrayal of
Raja and deputed her general Tantia Tope to attack Charkhari and capture Mr. Carne. Raja Ratan Singh surrendered and entered into a treaty with Tantya Tope. Mahoba was then under the rule of
rebels whom the British General Whitloack defeated and restored British rule. He arrested a large number of local rebels and hanged some of the prominent men on the trees in the vicinity called Haveli Darwaza. A "Shaheed Mela" is now annually held there to commemorate the memory of those
rebels.
According to Bhavishya Puran , Mahoba was earlier known as 'Mahavati Nagar' . Mahavati nagar was established by Mahamaya , Devi jee. During the rule of Agni dynasty rulers in Kaliyug the people
have high moral values and follow the religion. In Kaliyug, morality of people should have been reduced because of Kaliyug, but Kaliyug's effect was neutralized by Agni dynasry rulers. Therefore, Kaliyug along with some Mlekshas went to Nilachal hills and worshipped the God Krishna for 12
years. Then Krishna appeared and blessed him that he will be incarnated as Ahla (Ahlad) and Udal (Udai Singh) and will weaken the Agni dynasty rulers by fighting with them and will do something so
that Mlekshas could conquer India and Kaliyug could have full effect among people of India. In Bhavishya Puran, Mahavati Nagar has been referred at least two times.
Mahoba is located at 25.28°N 79.87°E.[1] It has an average elevation of 214 metres (702 feet).
As of 2001 India census,[2] Mahoba had a population of 78,806. Males constitute 53% of the
population and females 47%. Mahoba has an average literacy rate of 66.94%, higher than the national average of 59.5%: male literacy is 67%, and female literacy is 51%. In Mahoba, 16% of the population is under 6 years of age.
Mahoba is well connected by roadways and railways to rest of the country. Mahoba is a railway
junction. National highways NH-76 and NH-86 passes through Mahoba.

Page | 10
About Mahoba
As per census 2011, the urban population of Mahoba district is 95216 .About 38 % population of
Mahoba is urban. The urban sex ratio is 885 females per 1000 males. The average literacy rate in
Mahoba urban is 73.57% percent, 81.59 %for males and 64.49 % for females.
Table.1: Mahoba District and Mahoba Urban in Census 20111
Description Mahoba District
2011
Mahoba
Urban 2011
Actual Population 875,958 185,381
Male 466,358 98,349
1 2011 census (P)

Page | 11
Description Mahoba District
2011
Mahoba
Urban 2011
Female 409,600 87,032
Population Decadal Growth
rate 23.64%
Density/km2 279
Sex Ratio (Per 1000) 878 885
Child Sex Ratio (0-6 Age) 892 892
Average Literacy (%) 65.27% 73.57 %
Male Literacy (%) 75.83% 81.59 %
Female Literacy (%) 53.22% 64.49 %
Mahoba City
MAHOBA, A small district in Uttar Pradesh is famous for it's glorious history. It is known for its
bravery. The stories Of Veer ALHA and UDAL defines its importance in Indian history. There are
various Places which can create live glorious Moment of that previous time. . Mahoba is a city
located in the Indian state of Uttar Pradesh, in the Bundelkhand region. Mahoba is known for its
closeness to Khajuraho, Laundi and other historic places like Kulpahar, Charkhari, Kalinjar, Orchha,
and Jhansi. The name Mahoba is derived from Mahotsav Nagar, the city of great festivals. The Bardic
tradition preserves three other names of the city: Kekaipur, Patanpur and Ratanpur. The existence of
the sacred Ram-Kund and Seeta-Rasoi cave at the Gokhar hill here are said to be monumental to the
visit of Rama who widely treated this hilly region while in 14-year exile at Chitrakoot.

Page | 12
Table 2: Demographic profile of City- Mahoba
Total Population of city (in lakhs) 95216 Source: Census 2011
Slum Population (in lakhs) 37000 Source: RSAC
Slum Population as percentage of urban
population 38%
Number of Notified Slums 12 Source: DUDA
Number of slums not notified 0 Source: RSAC
No. of Slum Households 7500 Source: RSAC
No. of slums covered under slum improvement
programme (BSUP, IDSMT,etc.) NA
Number of slums where households have
individual water connections* NA
Number of slums connected to sewerage
network* NA
Number of slums having a Primary school
04 Source: BSA Deptt.
No. of slums having AWC 32 Source: ICDS Mahoba & BSUP
No. of slums having primary health care facility NA
Mahoba District Population Growth Rate
There was change of 23.64 percent in the population compared to population as per 2001. In the previous
census of India 2001, Mahoba District recorded increase of 21.33 percent to its population compared to 1991.
Mahoba District Density 2011
The initial provisional data released by census India 2011, shows that density of Mahoba district for 2011 is
279 people per sq. km. In 2001, Mahoba district density was at 233 people per sq. km. Mahoba district
administers 3,144 square kilometers of areas.
Mahoba Literacy Rate 2011
Average literacy rate of Mahoba in 2011 were 65.27 compared to 53.28 of 2001. If things are looked out at
gender wise, male and female literacy were 75.83 and 53.22 respectively. For 2001 census, same figures stood
at 67.74 and 36.41 in Mahoba District. Total literate in Mahoba District were 488,106 of which male and
female were 302,283 and 185,823 respectively. In 2001, Mahoba District had 305,662 in its district.

Page | 13
Mahoba Sex Ratio 2011
With regards to Sex Ratio in Mahoba, it stood at 878 per 1000 male compared to 2001 census figure of 866.
The average national sex ratio in India is 940 as per latest reports of Census 2011 Directorate. In 2011 census,
child sex ratio is 892 girls per 1000 boys compared to figure of 901 girls per 1000 boys of 2001 census data.
Mahoba Child Population 2011
In census enumeration, data regarding child under 0-6 age were also collected for all districts including
Mahoba. There were total 128,129 children under age of 0-6 against 134,725 of 2001 census. Of total 128,129
male and female were 67,720 and 60,409 respectively. Child Sex Ratio as per census 2011 was 892 compared
to 901 of census 2001. In 2011, Children under 0-6 formed 14.63 percent of Mahoba District compared to
19.02 percent of 2001. There was net change of -4.39 percent in this compared to previous census of India
Description 2011 2001
Actual Population 875,958 708,447
Male 466,358 379,691
Female 409,600 328,756
Population Growth 23.64% 21.33%
Area Sq. Km 3,144 3,144
Density/km2 279 233
Proportion to Uttar Pradesh Population 0.44% 0.43%
Sex Ratio (Per 1000) 878 866
Child Sex Ratio (0-6 Age) 892 901
Average Literacy 65.27 53.28
Male Literacy 75.83 67.74
Female Literacy 53.22 36.41
Total Child Population (0-6 Age) 128,129 134,725
Male Population (0-6 Age) 67,720 70,865
Female Population (0-6 Age) 60,409 63,860
Literates 488,106 305,662
Male Literates 302,283 209,207
Female Literates 185,823 96,455
Child Proportion (0-6 Age) 14.63% 19.02%

Page | 14
Boys Proportion (0-6 Age) 14.52% 18.66%
Girls Proportion (0-6 Age) 14.75% 19.42%
Mahoba District Urban Population 2011
Out of the total Mahoba population for 2011 census, 21.16 percent lives in urban regions of district. In
total 185,381 people lives in urban areas of which males are 98,349 and females are 87,032. Sex Ratio
in urban region of Mahoba district is 885 as per 2011 census data. Similarly child sex ratio in Mahoba
district was 892 in 2011 census. Child population (0-6) in urban region was 24,451 of which males and
females were 12,921 and 11,530. This child population figure of Mahoba district is 13.14 % of total
urban population. Average literacy rate in Mahoba district as per census 2011 is 73.57 % of which
males and females are 81.59 % and 64.49 % literates respectively. In actual number 118,390 people
are literate in urban region of which males and females are 69,699 and 48,691 respectively.
Description Rural Urban
Population (%) 78.84 % 21.16 %
Total Population 690,577 185,381
Male Population 368,009 98,349
Female Population 322,568 87,032
Sex Ratio 877 885
Child Sex Ratio (0-6) 892 892
Child Population (0-6) 103,678 24,451
Male Child(0-6) 54,799 12,921
Female Child(0-6) 48,879 11,530
Child Percentage (0-6) 15.01 % 13.19 %
Male Child Percentage 14.89 % 13.14 %
Female Child Percentage 15.15 % 13.25 %
Literates 369,716 118,390
Male Literates 232,584 69,699
Female Literates 137,132 48,691
Average Literacy 62.99 % 73.57 %
Male Literacy 74.26 % 81.59 %
Female Literacy 50.11 % 64.49 %
Urban Poor & Slums2
The UP Slum Areas (Improvement and Clearance) Act, 1962, considers an area a slum if the majority
of buildings in the area are dilapidated, are over-crowded, have faulty arrangement of buildings or
2 State of Urban Health in Uttar Pradesh, 2006

Page | 15
streets, narrow streets, lack ventilation, light or sanitation facilities, and are detrimental to safety,
health or morals of the inhabitants in that area, or otherwise in any respect unfit for human habitation.
It mentions factors such as repairs, stability, extent of dampness, availability of natural light and air,
water supply; arrangement of drainage and sanitation facilities as considerations. Based on the
definition, estimates of slum population vary, so much so that the Census 2001 originally did not
report any slums and then later revised its findings. DUDA follows the definition as stated in the UP
Slum Areas (Improvement & Clearance) Act 1962; SUDA/UNCHS do not follow this definition but
define poverty in terms of vulnerability as does Oxfam.
DUDA’s estimation of slum population is a conservative increase over the Census estimation.
However, a survey report released by Oxfam Trust (India) in 2005 indicates that there are 787 poor
settlements in the city that can be categorized as slums - authorized and unauthorized (map
overleaf). This classification is on the basis of tenure. An authorized slum is one where there is
security of tenure with the cluster being either an outcome of a government resettlement programme
or being located on private/own land. Unauthorized settlements are those that have emerged on
available vacant plots, mainly railway land or on encroached areas. Slum clusters on the riverbanks
or on drains are classified as unauthorized. In 2009, NRHM did the GIS mapping through RSAC for
the planning of NUHM. The most recent information on slums available in Mahoba is from the RSAC
GIS mapping of 2009 and this plan has mainly used this information, partly on the advice of SUDA.
Other sources of information have been cited mainly to point out the range in the available data that
will impact the earmarking of resources for this group. Approximately 11 lakh 32 thousand people are
living in slums with few basic civic amenities.
3 DUDA Survey 2005
Table 5: Selected indicators of slum conditions in Mahoba3
Characteristic Percentage of people/families
Water Supply Facilities
Individual tap 28.68%
Community tap 18.84%
Others 5.06%
Sanitation
Individual toilet facility 10.12%
Community toilet facility 30.98%
Others 28.30%
Employment
Employed 9.78%
Unemployed 7.97%
Self employed 41.91%

Page | 16
S. No. Name of Slums Population 1 Nayapura,Naykana 3048
2 Fatepur,Bajariya 3442
3 Bhitar court 3065
4 Subhash Nagar 3022
5 Bhandhanward 3052
6 Bhatipura 3052
7 Raicout 2788
8 Mathuranpura ward 3183
9 Singhbhawani 3273
10 Naykanapura 2972
11 Magriyapura 3029
12 Jariganj 3080
Total 3006
The rapidly growing urban population poses great challenge to the efforts of the state government
towards improving the health of the urban poor.
Urban Governance4
There are multiple agencies responsible for urban governance and provision and management of
infrastructure and services. While, the Mahoba Nagar Palika Parisad (LPP), Mahoba Jal Sansthan
(LJS), Mahoba Development Authority (LDA) and UP Jal Nigam (UPJN) are the key urban service
providers, other agencies include the Housing Board, Central and State Public Works Departments
(CPWD and PWD), Transport Department, Industries Department and the Department of
Environment. There is significant overlap of roles and responsibilities and fragmentation in service
provision and management of infrastructure, which makes it difficult to hold institutions accountable
and to coordinate.
Table 6: Urban Governance and Service delivery institutions
City Level
Nagar Plika Prishad (NPP) Local level governance; Primary Collection of Solid Waste; Maintenance of
Storm Water Drains; Allotment of Trade Licenses under the Prevention of Food
Adulteration Act; O&M of internal sewers and community toilets; Street lighting;
O&M of water supply and sewerage assets; Collection of water tariff
Mahoba Development
Authority (LDA)
Preparation of Master Plans for land use; Development of new areas as well as
provision of housing and necessary infrastructure
District Urban Development Implementing agency for plans prepared by SUDA.
4 Mahoba City Development Plan 2006
Page | 17
Authority (DUDA) Responsible for the field work relating to community development – focusing on
the development of slum communities, construction of community toilets,
assistance in construction of individual household latrines, awareness
generation etc.
State Level
UP Jal Nigam (UPJN)
Water supply and sewerage including design of water supply and sewerage
networks. In the last two decades ‘pollution control of rivers’ has become one of
their primary focus areas
State Urban Development
Authority (SUDA)
Apex policy-making and monitoring agency for the urban areas of the state.
Responsible for providing overall guidance to the District Urban Development
Authority (DUDA) for implementation of community development programmes
UP Awas Vikas Parishad
(UPAVP)
Nodal agency for housing in the state. Involved in planning, designing,
construction and development of almost all types of urban development
projects in the state. Autonomous body generating its own resources through
loans from financial institutions
UP State Transport
Corporation (UPSTC)
Provides intra-city and state wide public transport; maintenance of buses, bus
stands
Public Works Department
(PWD)
Construction of main roads and transport infrastructure including construction
and maintenance of Government houses and Institutions
State Tourism Department
(STC)
Promotion of tourism
Archaeological Survey of
India (ASI)
Maintenance of heritage areas and monuments
UP Pollution Control Board
(UPPCB)
Pollution control and monitoring especially river water quality and regulating
industries
Town and Country Planning
Department (TCPD)
Preparation of Town Plans including infrastructure for the state (rural and
urban)
Access to Public Facilities5
Infrastructure development has not been commensurate with the growth of the city and there are
problems confronting the city in terms of access and coverage in key infrastructure sectors – water
supply, sewerage, housing, drainage, and transport. Overall service levels are inadequate and the
situation is worse for the urban poor.
5 Mahoba City Development Plan 2006

Page | 18
Housing
Mahoba has witnessed a radial growth – greater along the Faizabad Road and the Trans Gomti area
and in recent years, the city is witnessing a real estate boom with a large number of private
developers entering the market. The latter has not been factored into the Master Plan – the formal
basis for Government panning. Estimates of infrastructure requirements and population projections
are therefore likely to be conservative.
The position of the City as the only large urban centre amidst a number of small towns in the
surrounding districts makes it an attractive destination for job seekers and people in need of
education and health facilities. One of the features of the city’s growth has been an increase in the
number of slums but disagreements about the definition of slums and about data hamper efforts to
address service delivery challenges in these areas.
Table 7: Housing Characteristics6
INDICATOR %
Households living in a Pucca House (%) 44.3
Households living in a Kuchcha House (%) 28.9
Households living in a Rented House (%) 5.6
Households living in a Owned House (%) 93.5
Households treating water to make it safer for drinking (%) 6.9
Households having access to toilet facility (%) 33.4
Households sharing toilet facility (%) 7.0
Households having access to electricity (%) 52.7
Households using Electricity (%) 44.2
Households using Firewood/Crop Residues/Cow Dung Cake (%) 87.9
Households using LPG/PNG (%) 11.3
Availability of Kitchen
Households having a separate Kitchen (%) 37.2
Households having Computer/laptop with or without Internet Connectivity (%)
8.6
Households having Telephone/Mobile (%) 69.7
Health Infrastructure
Unlike in the rural areas, where the health department has a wide network of primary health care
facilities providing reproductive and child health services, the urban slums lack basic health
infrastructure and outreach services. Thus, they are often bypassed even by national programmes
providing immunization, safe motherhood and family planning services. The sparse health coverage
provided by health facilities like urban family welfare centers, health posts, and maternity homes in
cities is used more for emergencies and curative services. Often these facilities are far from their
service area, poorly staffed, with inadequate space and supply of medicines and equipment. Urban
6 AHS 2010-11

Page | 19
local bodies like municipal corporations and nagar panchayats are also expected to provide health
care, but resource scarcity restricts them to only providing sanitation services. NGOs and private
trusts are also few and far between.
First and Second Tier Health Services
The Government of Uttar Pradesh has committed itself to make provisions for health care services to
its population. Though the efforts have been rural centric some efforts have also been made to
improve the delivery of primary health care services to the population living in urban areas. It has
established D Type health centers and dispensaries for providing family welfare services and OPD
facilities. The Urban Local bodies and Department of Health and Family Welfare are the two main
stakeholders for managing these services. In urban areas of UP, first tier health services are available
through D-type health centers, the family welfare centre, health post and PP centers7. Second tier
health services are provided in urban areas through District Male and Female or Combined Hospitals.
Table12: Health Structure in Mahoba
Sl. No.
Name & Type of Facility (DH,
Maternity Home, CHC, other ref. hospital UFWC,
UHP, PHC,Dispensary
etc.)
Managing Authority (Municipal Council,
State Health Department,
facilities functioning
on PPP basis)
Location of Health Facility
Population Covered by the Facility
Services Provided
Human Resources available (List Type
and Number of
HR available i.e. ANM, LT, SN, MOs,
Specialists etc.
No. and Type of
Equipment Available
(X-ray machine,
USG, autoclave
etc.)
1 DH,Mahoba State Health Department
District Head
Quater Near
,Roadvage
N/A Specialist and
Tertiary Care
Not Available
X-ray machine,
USG,
2 DWH,Mahoba State Health Department
District Head
Quarter,Near
Roadvage
N/A Specialist and
Maternaty Care
Not Available
Not Available
3 UHP,Bhatipura-
mahoba
State Health Department
Slum Area N/A Basic Health
Services
Not Available
Not Available
4 UHP,Bajriya-
Mahoba
State Health Department
Slum Area N/A Basic Health
Services
Not Available
Not Available
7 Ministry of Health and Family Welf are. 2005 Annual Report 2003-04. New Delhi : MoHFW.

Page | 20
5 Govt,Ayurvedic
Hospital,Alampura-
Mahoba
State Health Department
Near
Govt.Polytechnic
N/A Basic Health
Services
Not Available
Not Available
6 District
Homeophatic
Hospital,Mahoba
State Health Department
District Head
Quater Near
N/A Basic Health
Services
Not Available
Not Available
The data given in the table above reveals inadequacy of primary health care services. The first tier
health facilities were planned for a population of 50000 but as a result of rapid population growth they
are currently serving a population of more than 75000. The situation gets compounded due to lack of
adequate infrastructure, equipments and medicines. The staff mainly Doctors and ANM is also
inadequate. The high population- staff ratio results in poor service coverage with some areas being
entirely unserved. From the above assessment it becomes evident to consider the poor health
indicators for deciding the norms of staff population ratio. Uttar Pradesh has eight medical colleges
and one post-graduate institute which offer tertiary and superspecialty health services.

Page | 21
Health Scenario
Based on the results of DLHS the health scenario of Mahoba city is presented as below. The detailed
tables are given in the annexure.
Indicator %
Marrige below legal age (%)
Among females (below 18 Years) 9.1
Among males (below 21 Years) 19.6
CMW age ( 20-24 Years) married before age 18 years 41.9
CMM age ( 20-24 Years) married before age 21 years 40.7
Mean Age at Marriage
Male 23.3
Female 20.4
FERTILITY
Total Fertility Rate (TFR) 3.7
Women aged 20-24 reporting birth of order 2 & above (%) 50.7
Women reporting birth birth of order 3 & above (%) 46.7
Women with two children wanting no more children (%) 54.1
Median age at first live birth of Women aged 15-49 years 49.0
Median age at first live birth of Women aged 25-49 years 21.0
Women age 15-19 who were already mothers or pregnant at the time of the survey (%)
49.0
Mean number of children ever born to aged 15-49 3.1
Mean number of children surviving to Women aged 15-49 2.8
Mean number of children ever born to Women aged 45-49 4.84
Live Births taking place after an interval of 36 months (%) 48.5
ABORTION to EMW 15-49 Years (%)
Pregnancy resulting in abortion 7.2
Women who received any ANC before abortion 39.1
Married Women who went for Ultrasound before abortion 9.5
Average Month of pregnancy at the time of abortion 3.1
Abortion performed by skilled health personnel (%) 43.6
Abortion taking place in Institution (%) 40.9
Currently Married Pregnant Women aged 15-49 registered for ANC (%)
Current Usage Any method (%) 68.9
Any modern method (%) 50.4

Page | 22
Indicator %
Female sterilization (%) 31.8
Male sterilization (%) 0.1
Copper-T/IUD (%) 0.2
Pills (%) 4.7
Condom/Nirodh (%) 12.9
Emergency Contraceptive Pills (%) 0.3
Any traditional method (%) 18.5
Periodic abstinence (%) 7.7
Withdrawal (%) 0.8
LAM (%) 9.8
UNMET NEED FOR FAMILY PLANNING Unmet need for Spacing (%) 9.6
Unmet need for Limiting (%) 5.4
Total Unmet need (%) 15.1
Maternal Health Care ANTE NATAL CARE Mothers who received any antenatal check-up (%) 89.8
Mothers who had antenatal check-up in first trimester (%) 42.0
Mothers who received 3 or more antenatal care (%) 32.0
Mothers who received at least one tetanus toxoid (TT) injection (%) 88.1
Mothers who consumed IFA for 100 days or more (%) 7.1
Mothers who had Full Antenatal Check-up (%) 1.9
Mothers who received ANC from Govt. Source (%) 67.3
Mothers whose Blood Pressure (BP) taken (%) 42.4
Mothers whose Blood taken for Hb (%) 44.2
Mothers who underwent Ultrasound (%) 10.9
DELIVERY CARE Institutional Delivery (%) 70.3
Delivery at Government Institution (%) 61.4
Delivery at Private Institution (%) 8.9
Delivery at Home(%) 29.2
Delivery at home conducted by skilled health personnel (%) 16.0
Safe delivery *(%) 75.0
Caesarean out of total delivery taken place in Government Institutions (%) 1.2
Caesarean out of total delivery taken place in Private Institutions (%) 18.9
Less than 24 hrs. stay in institution after delivery (%) 79.2
Mothers who received Post-natal Check-up within 48 hrs. of delivery (%) 71.6
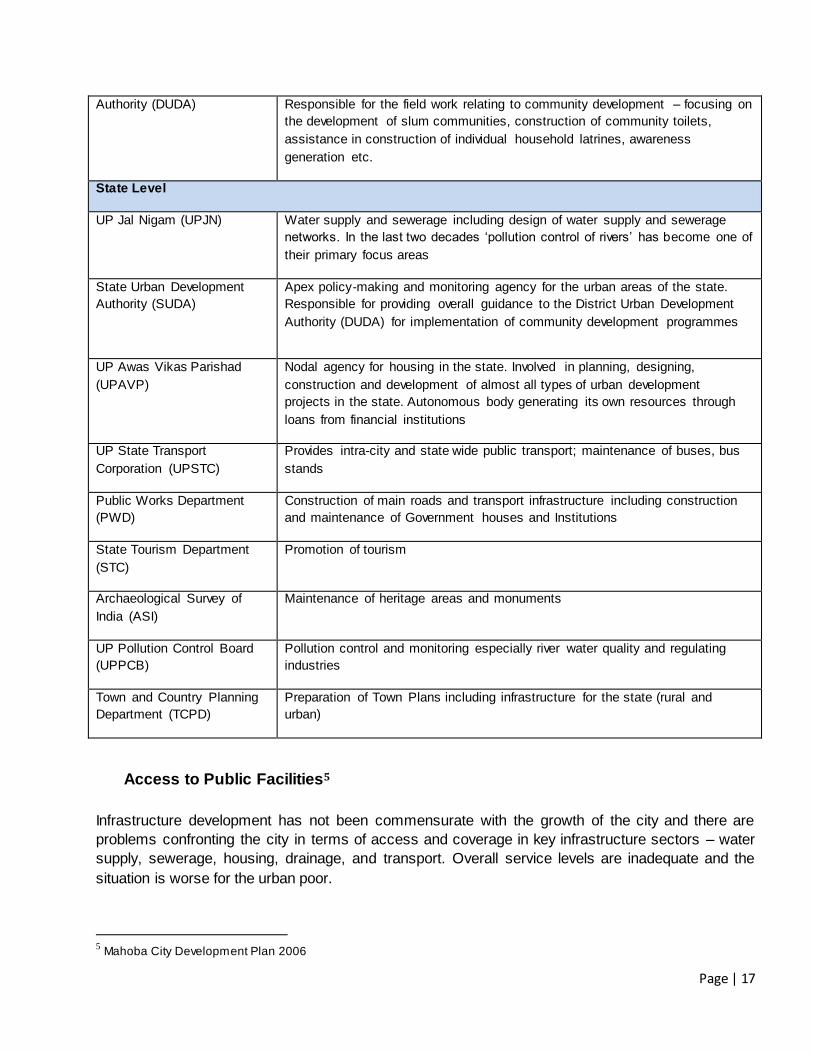
Page | 23
Indicator %
Mothers who received Post-natal Check-up within 1 week of delivery (%) 77.1
Mothers who did not receive any post-natal Check-up (%) 21.2
New borns who were checked up within 24 hrs. of birth (%) 73.1
JANANI SURAKSHA YOJANA (JSY)
Mothers who availed financial assistance for delivery under JSY (%) 59.5
Mothers who availed financial assistance for institutional delivery under JSY (%) 83.5
Mothers who availed financial assistance for government institutional delivery under JSY(%)
94.6
IMMUNIZATION (%)
No of Children age 12-23 months 71.9
Children aged 12-23 months who have received BCG 92.2
Children aged 12-23 months who have received 3 doses of Polio vaccine 67.7
Children aged 12-23 months who have received 3 doses of DPT vaccine 64.8
Children aged 12-23 months who have received Measles vaccine 64.5
Children aged 12-23 months Fully Immunized 50.9
Children who have received Polio dose at birth 76.7
Children who did not receive any vaccination 2.0
Children Vitamin A dose during last six months 38.4
Children (aged 6 months) who received IFA tablets/syrup during last 3 months
(%) 7.6
Children whose birth weight was taken (%) 45.6
Children with birth weight less than 2.5 Kg. (%) 15.8
CHILDHOOD DISEASES
Children suffering from Diarrhoea (%) 6.4
Children suffering from Diarrhoea who received HAF/ORS/ORT (%)
61.4
Children suffering from Acute Respiratory Infection (%) 1.3
Children suffering from Acute Respiratory Infection who sought treatment (%) 95.0
Children suffering from Fever (%) 9.8
Children suffering from Fever who sought treatment (%) 92.5
Child Feeding practices and nutritional staus of children (%)
Children under 3 years breastfed within one hour of birth 67.9
Children (aged 6-35 months) exclusively breastfed for at least six months (%) 14.8
Water 88.3
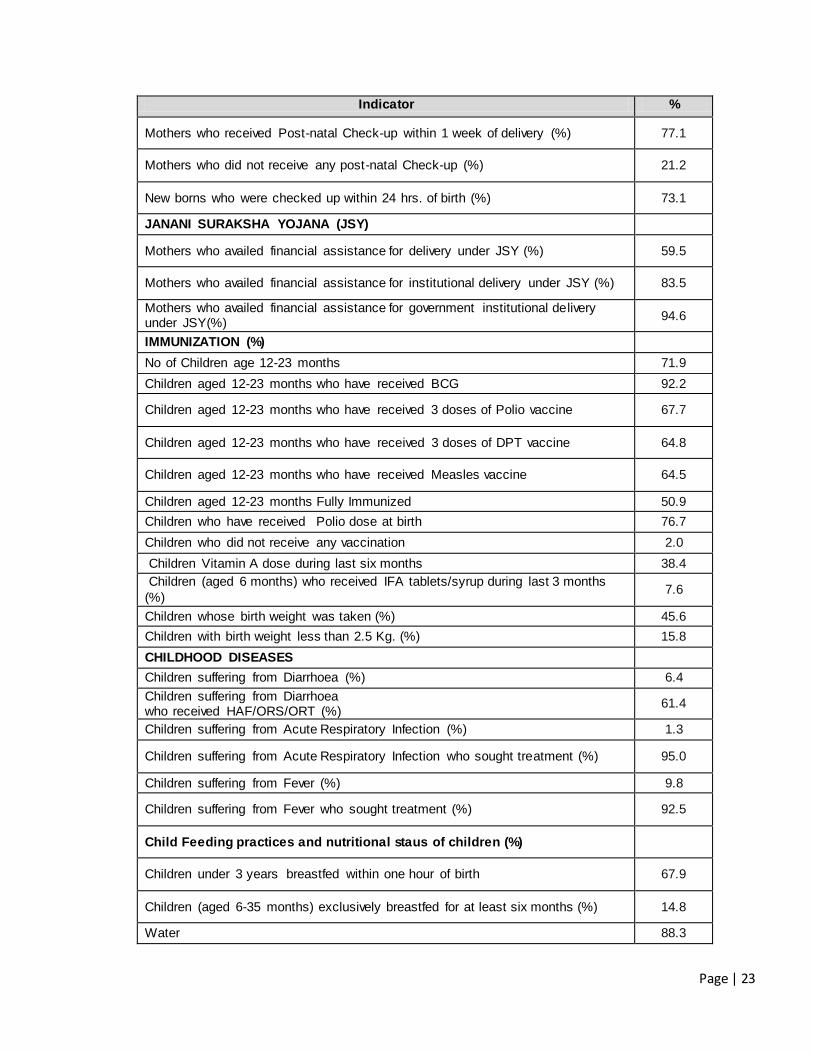
Page | 24
Indicator %
Animal/Formula Milk 69.3
Semi-Solid mashed food 5.7
Solid (Adult) Food 5.4
Vegetables/Fruits 7.0
Average month of receiving foods other than other than breast milk for
children under 3 years
Water 1.1
Animal/Formula Milk 1.2
Semi-Solid mashed food 2.6
Solid (Adult) Food 6.7
Vegetables/Fruits 9.4
BIRTH REGISTRATION
Birth registered (%) 52.2
Children whose birth was registered and received birth certificate (%) 37.8
AWARENESS ON HIV/AIDS
Women who are aware of HIV/AIDS (%) 46.5
Women who are aware of RTI/STI (%) 88.4
Women who are aware of HAF/ORS/ORT (%) 90.2
Women who are aware of danger signs of ARI/Pneumonia (%) 94.0
Amenities and Living Conditions
About 93.5% households were living in their own houses. About 28.9 % were still living in Kutcha or
Semi Pucca houses. Though almost all households had access to improved sources of drinking
water, but 6.9% were treating water to make it safer.
Whereas 18% were sharing toilets, still about 7% were defecating in open. About 97% had access to
electricity. Though 81% were using LPG for cooking, 15% were still using fire wood/dung cakes/ crop
residues for cooking. As high as 90% had telephones/ mobiles and 25% even had computers.
Following would be the issues for the cities to address: City Health Planning, Public Private
Partnership, Convergence, Capacity Building, Migration, Communitization, Strengthen Data,
Monitoring and Supervision, Health Insurance, Information Dissemination and Focus on NCDs/ Life-
Style Diseases.
After considering the available data, city scenario and analysis, the City planning team has identified issues at
both service delivery & demand generation level. Following are the details of issues which would be addressed
through NUHM at the city level:
1) Need of community volunteers (ASHAs) for taking up the community mobilization activities
2) Need of Mahila Arogya Samiti (MAS- a group of 10-12 women) for wider spread of information/ rights
and entitlements
3) Strengthening of ANC, PNC & identification of high risk pregnancies at community level

Page | 25
4) Home based care of neonates at community level
5) Promotion of institutional deliveries
6) Health education for all, especially for adolescent group
7) Complete immunization of pregnant women & children
8) Needs to strengthen the existing health care facilities by recruiting human resources
9) Need assessment of community in health scenario
10) Need a better convergence with other programs and wider determinants
11) Need of training & capacity building of human resources
12) Need of Strengthened program management structure at district level
13) Need of intensive baseline survey to start the community processes and identifying local needs
14) Involvement of local bodies in decision making and managing the program locally
15) Gap analysis of HR & recruitment
16) Promotion of family planning methods through basket of choice approach & counselling because unmet
need for family planning is high in Mahoba
17) Management of communicable & non- communicable diseases
18) Strengthening AYUSH
19) Constitution of BSGY team for urban areas.
20) Identification & management of SAM children
Strategies, Activities and Work plan
The key overarching strategies under NUHM for 2013-14 include data based planning, strengthening
of management and monitoring systems at the state and district level, improving the primary health
care delivery system and community outreach through ASHAs, MAS and Urban Health and Nutrition
Days(UHNDs).
The key activities at the district level will include convergence with key urban stakeholders,
sensitization of ULBs on their role in urban health, strengthening UPHCs for provision of primary
health care to urban poor, community outreach through selection, training and support to ASHAs and
MAS, conducting UHNDs and outreach camps to get services closer to the community and reach
complete coverage of slum and vulnerable populations.
With the aim to improve the health parameters of urban population in the city, structures and
strategies as recommended for the NUHM in its framework will be adopted and operationalized
rapidly over the years.
Listing and Mapping of Households in slums and Key Focus Areas
Listing and mapping of households will provide accurate numbers for population their family size and
composition residing in slums. Currently, estimates of population residing in slums are available from
District Urban Development Agency (DUDA) and National Polio Surveillance Project as the
immunization micro plans (under NPSP) provide updated estimates of s lum and vulnerable
populations and are expected to be fairly complete. The current plan for covering slums is based on
the currently available data of urban population of each city.

Page | 26
Once the ASHA are deployed they will list all households and fill the Slum Health Index Registers
(SHIR) including the number and details of family members in each household. This data will be
compiled for city and will provide the population composition of slums and key focus areas. This will
also help the urban ASHA know her community better and build a rapport with the families that will go
a long way in helping her advocate for better health behaviours and link communities to health
facilities under the NUHM. It is expected that once the household mapping is completed in cit ies, the
number of ASHAs will be reviewed and adjusted upwards or downwards and the geographical
boundaries of the coverage area for each ASHA would be realigned. This is due to the reason that
the actual population may be higher or lower than the original estimate used for planning.
Facility Survey for gaps in infrastructure, HR, equipment, drugs and consumables
Facility survey will be carried out in the public facilities to assess the gaps in infrastructure, human
resource, equipment, drugs and consumables availability as against expected patient load. Further
planning, particularly for UCHCs, will be based on these gaps. This work will be outsourced to a
research agency. Development Partners like Health of the Urban Poor project will technically support
this effort.
Baseline Survey
The state envisions monitoring progress in health indicators in urban areas and among urban poor
over the period of implementation of NUHM. This proposed Baseline survey will generate data on the
health and related indicators which will be reviewed during the course of implementation of the
program to assess the impact of implementation and necessary course corrections can accordingly
be made and use of resources can be optimised.
Training and Capacity Building
ULB, Medical and Paramedical staff, Urban ASHAs and MAS will be trained. The trainings will have
to be followed by periodic refresher trainings to keep these frontline health workers motivated. NUHM
will engage with development organisations to develop the training modules and facilitate the
trainings.
Monitoring & Evaluation
The M&E systems would also capture qualitative data to understand the complexities in health
interventions, undertake periodic process documentation and self evaluation cross learning among
the Planning Units to be made more systematic.
The Monitoring and Evaluation framework would be based on triangulation of information. The three
components would be Community Based Monitoring, HMIS for reporting and feedback and external
evaluations.

Page | 27
Strengthening of health facilities
Urban - Primary Health Centre (U-PHC) –
During the first year of implementation of the program, the total 2 U-PHC will be established , the
UHPs existing in rented accommodations will be shifted to adequately larger premises which would
help in rendering the mandated services. A provision of Rs. 15,000/- per month per UPHC is being
proposed for immediate service provision capacity enhancement, but over the period of time the said
rented accommodations will be shifted to owned premises for sustained services. Targeted
intervention for urban poor –
The process of listing of households in the KFAs, mapping of KFAs and health facilities and baseline
survey of the KFA households will help determine the scope and extent of services required for
targeting of the urban poor. A deliberate effort will be made to identify the vulnerable poor on the
basis of their residence status, occupational status and social status, besides other micro-level
indicators, which will further help focusing the health care services to the most deserving.
Mahila Arogya Samiti (MAS)-
MAS will act as community based peer education group in slums, involved in community mobilization,
monitoring and referral with focus on preventive and promotive care, facilitating access to identified
facilities and management of grants received. Existing community based institutions could be utilized
for this purpose. City planning team is proposing formation of only one MAS under each ASHA in the
first year and the identification of the remaining planned MAS will be undertaken in the subsequent
years.
ASHA-
For reaching out to the households ASHAs (frontline community worker) would serve as an effective
and demand–generating link between the health facility and the urban slum population. Each link
worker/ASHA would have a well-defined service area of about 1000-2,500 beneficiaries/ between
200-500 households based on spatial consideration.
Outreach services –
Outreach services will be provided to the slum areas and KFAs through ANMs who would be
responsible for providing preventive and promotive healthcare services at the household level through
regular visits and outreach sessions. Each ANM will organize a minimum of one routine outreach
session in her area every month.
Special outreach sessions (for slum and vulnerable population) will be organized once in a week in
partnership with other health professionals (doctors/ pharmacist/ technicians/ nurses – government or
private). It will include screening and follow-up, basic lab investigations (using portable /disposable
kits), drug dispensing, and counselling. The outreach sessions (both routine and special outreach)
could be organized at designated locations mentioned in the aforesaid paras in coordination with
ASHA and MAS members

Page | 28
Convergence –
Intra-sectoral convergence is envisaged to be established through integrated planning for
implementation of various health programmes like RCH, RNTCP, NVBDCP, NPCB, National Mental
Health Programme, National Programme for Health Care of the Elderly, etc. at the city level. Inter-
sectoral convergence with Departments of Urban Development, Housing and Urban Poverty
Alleviation, Women & Child Development, School Education, Minority Affairs, Labour will be
established through city level Urban Health Committees headed by the Municipal Commissioner/
Deputy Commissioner/ District Collector.
Activity Plan under NUHM for the state and cities
Act. No.
Activity
Responsibility Months : October'13 - March'14 Remarks
State level
City level O
ct.
No
v.
De
c
Ja
n
Fe
b
Ma
r
1
Establishment of Platform for Convergence at state level
Circular to be isued from state level to all their district level nodal officers
2 Preparation & Finalization of Guidelines for City Coord. Committee/ City Program Management Committee
These will be one time activities and will apply across the state
3 Preparation & Finalization of Guidelines for Urban ASHAs
4 Preparation & Finalization of Guidelines for Mahila Arogya Samiti
5 Preparation & Finalization of Guidelines for UHND
6 Preparation & Finalization of Guidelines for Outreach sessions/ School Health Programs
7 Preparation & Finalization of Job Descriptions for all district level NUHM positions
8 Preparation & Finalization of Guidelines for PPP
9 Induction of state level staff for Urban Health Cell
10 Induction of city level staff for Urban Health program
11 Meeting of DHS for establishment of City Program Management Committee (UH)
12 Sensitization of new probable members on NUHM
13 Identification of NGOs for their role under NUHM

Page | 29
14 Establishment & orientation of City Program Management Committee (UH)
15
Identification of groups, collectives formed under various govt. programs (like NHG under SJSRY, self help groups etc.) for MAS
16 Organize meetings with women in slums where no groups could be identified
17 Formation and restructuring of groups as per MAS guidelines
18 Orientation of MAS members
18 Selection of ASHAs
18a - Selection of local NGOs for ASHA selection facilitation
18b - Listing of local community members as facilitators by NGOs
18c - Listing of probable ASHA candidates and finalize selection
19 Convergence meeting with govt. Stakeholders
20 Mapping & listing exercise (for health facilities and slums)
20a
- Mapping of all urban health facilities (public & pvt.) for services
To continue in 2014-15
20b
- Mapping of slums (listed and unlisted)
To continue in 2014-15
20c
- Houselisting of slums/ poor settlements
To continue in 2014-15
21 Planning for strengthening of health facilites/ services
- Health Facility Assessment (of public facilities including listing of public facility wise infra & HR requirement)
To continue in 2014-15
22 Baseline survey of urban poor/ slums (KFAs)
(to determine vulnerability, morbidity pattern & health status)
23 Meetings of RKS for all the public health facilites under NUHM

Page | 30
24
Identification of alternate/ suitable locations for UPHCs under various urban devp. Programs
To continue in 2014-15
25 Strengthening of public health facilities
- Selection, training and deployment of HR in pub. health facilities
To continue in 2014-15
26 IEC activities
27 Outreach camps & UHNDs (from existing UHPs)
28
Empanelment of Private Health Facilities for health care provisioning
To continue in 2014-15
29 Involvement of CSR activities
Programme Management Arrangements
Districts Heath Society will be the implementing authority for NUHM under the leadership of the
District Magistrate. District Program Management Units have been further strengthened to provide
appropriate managerial and operational support for the implementation of the NUHM program at the
district level.
District Health Society under the chairmanship of the District Magistrate as the implementing authority for
NUHM
Fund flow mechanisms have been set up and separate accounts will be opened at in the district for
receiving the NUHM funds.
Urban Health will be included as a key agenda item for review by the District Health Society with
participation of city level urban stakeholders.
An Additional / Deputy CMO has been designated as the nodal officer for NUHM at the district level. The
District Program Management Unit will co-opt implementation of NUHM program in the district and the
District Program Manager will be overall responsible for the implementation of NUHM. To support this the
following additional staff and funds are proposed for strengthening the District Program Management Units
for implementing NUHM:

Page | 31
a. Urban Health Coordinator, Accountant and Data Entry Operators according to the following norms:
District total Urban
population
Additional Staff Proposed
1lakh to 10lakhs 1 Urban Health Coordinator,1 Accountant and 1 Data Entry Operator
b. District Programme Manager will be nodal for all NUHM activities so extra incentive and budget for
1 laptop to each DPM has been proposed for DPM for undertaking NUHM activities.
c. A onetime expense for computers, printer and furniture for the above staff has been budgeted along
with the recurring operations expenses.
d. Onetime expenses have been budgeted for up-gradation of the office of Additional/ Deputy CMO
and District Programme management Unit.
The City Program Management Committee will function as an Apex Body for management of the City
Health Plan, which will lead to delivery of Maternal, Newborn, Child Health and Nutrition (MNCHN)
and water, sanitation and hygiene (WASH) services to the urban poor and will work towards the
following objectives:
1. Establish a forum for convergence of city level stakeholders for the delivery of MNCHN and
WASH services to the urban poor.
2. Serve as the nodal body for the planning and monitoring of MNCHN and WASH service
delivery to the urban poor.
3. Provide a forum for exploring, reviewing and approving PPP initiatives and innovations to
address the gaps in MNCHN and WASH service delivery to the urban poor.
The structure proposed for the City Coordination Committee :
Chairperson - DM/ Municipal Commissioner
Convener - CMO
Members – Health - ACMO-Urban
Member – ICDS - CDPO
Member – Nagar Nigam - Sum Improvement Officer
Member – Water & Sanitation- Sup. En. / Ex.En. JalKal Vibhag, Nagar Nigam
Member DUDA & UD - Project Officer
Member – ESIC - ESIC Hosp. Supdt.
Members – School Education - BSA & DIOS
Members – Dev. Partners - Partners working in urban health sector ( HUP)
Coordinator - Lead Dev. Partner

Page | 32
Review Meetings at UPHC and City Level
Nature of Meeting Periodicity Meeting
Venue
Participants
Mahila Aarogya Samiti
Meeting
Once a month
for each MAS
Slum ANM, HV, Community
Organizer, Social Mobilization
officer
Review meeting with Link
workers and MAS
representatives
Once a month UPHC All ANMs, PHN, LMO,
Community Organizer, Social
Mobilization officer
Meeting of UPHC
Coordination Committee
Once a month UPHC LMO, PHN/Community
Organizer, Social Mobilization
officer, representative from 2nd
tier facility, and reps. From other
departments
Meeting with CMO & UH
Program Coordinator
Once a month CMO
Office
CMO, Program Coord., Asst.
Program Coordinator, LMO/
PHN/ Community Organizer,
Social Mobilization officer
City Task Force Meeting Once in two
months
DM’s
office
CMO, Program Coord. UH,
Various departments’ reps. ,
private partners, NGOs
City Level Indicators & Targets
Processes & Inputs
Indicators Baseline (as applicable)
Number Proposed (2013-14)
Number Achieved (2013-14)
Community Processes
1. Number of Mahila Arogya Samiti (MAS) formed * 0 38
2. Number of MAS members trained * 0 380
3. Number of Accredited Social Health Activists (ASHAs) selected and trained *
0 19
Health Systems
4. Number of ANMs recruited * 0 10
5. No. of Special Outreach health camps organized in the slum/HFAs * 0 4
6. No. of UHNDs organized in the slums and vulnerable areas * 0 37
7. Number of UPHCs made operational * 0 02
8. Number of UCHCs made operational * 0 0
9. No. of RKS created at UPHC and UCHC * 0 02
10. OPD attendance in the UPHCs 0 6895

Page | 33
11. No. of deliveries conducted in public health facilities 0 0
RCH Services
12. ANC early registration in first trimester 210
13. Number of women who had ANC check-up in their first trimester of pregnancy
210
14. TT (2nd dose) coverage among pregnant women 196
15. No. of children fully immunised (through public health facilities) 224
16. No. of Severely Acute Malnourished (SAM) children identified and referred for treatment
-
Communicable Diseases
17. No. of malaria cases detected through blood examination -
18. No. of TB cases identified through chest symptomatic -
19. No. of suspected TB cases referred for sputum examination -
20. No. of MDR-TB cases put under DOTS-plus
Non Communicable Diseases
21. No. of Diabetes cases screened in the city -
22. No. of Cancer cases screened in the city -
23. No. of Hypertension cases screened in the city -