
Dr. Raz Mohammed WALI Chief Migration Health Physician NTP National Seminar: 14-15 July 2014 Pukhra,...
18
Dr. Raz Mohammed WALI Chief Migration Health Physician NTP National Seminar: 14-15 July 2014 Pukhra, Nepal
-
Upload
randell-blankenship -
Category
Documents
-
view
217 -
download
0
Transcript of Dr. Raz Mohammed WALI Chief Migration Health Physician NTP National Seminar: 14-15 July 2014 Pukhra,...

Dr. Raz Mohammed WALIChief Migration Health Physician
NTP National Seminar: 14-15 July 2014Pukhra, Nepal
About IOM
Migration for the benefit of all Healthy migration in healthy community
International Organization for Migration (IOM) was established in 1951. The principal intergovernmental organization in the field of migration. IOM is committed to the principle that humane and orderly migration
benefit migrants and societies. Working in more than 151 countries globally, more than 480 main and sub-
offices, 9 regional hubs, 156 member states including Nepal, 10 states and organizations observers – over a billion USD budget annually.
Established in Nepal in 2006. Implementing several large and small projects in the country with the help
of more than 383 national and international staff
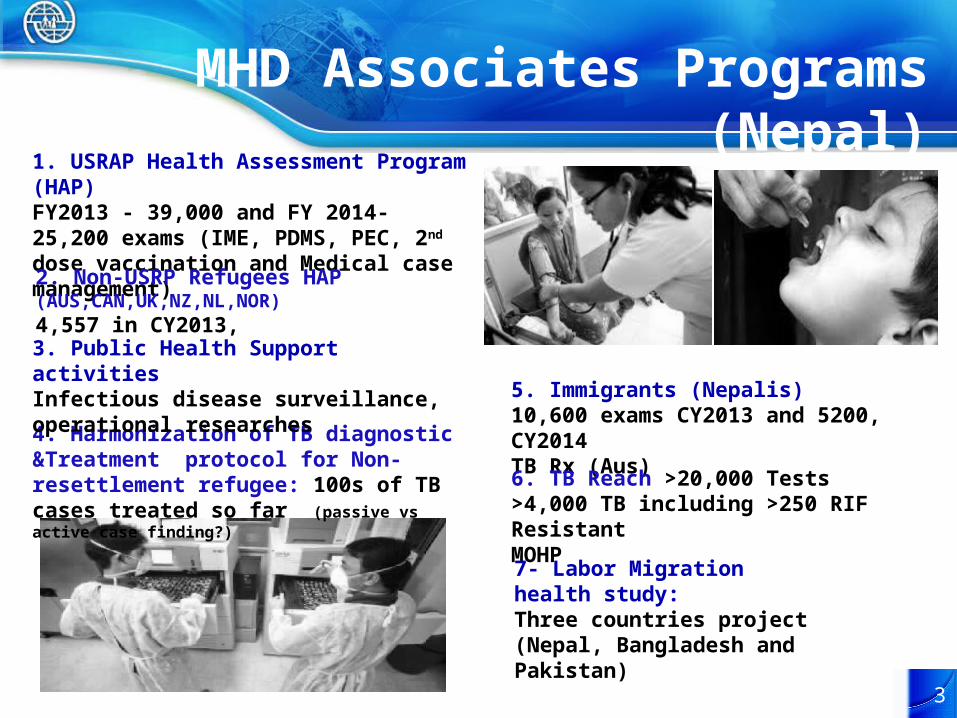
MHD Associates Programs (Nepal)
3
1. USRAP Health Assessment Program (HAP)FY2013 - 39,000 and FY 2014- 25,200 exams (IME, PDMS, PEC, 2nd dose vaccination and Medical case management)
5. Immigrants (Nepalis)10,600 exams CY2013 and 5200, CY2014TB Rx (Aus)
6. TB Reach >20,000 Tests>4,000 TB including >250 RIF ResistantMOHP
4. Harmonization of TB diagnostic &Treatment protocol for Non-resettlement refugee: 100s of TB cases treated so far (passive vs active case finding?)
2. Non-USRP Refugees HAP (AUS,CAN,UK,NZ,NL,NOR)4,557 in CY2013,
3. Public Health Support activitiesInfectious disease surveillance, operational researches
7- Labor Migration health study:Three countries project (Nepal, Bangladesh and Pakistan)

Health Assessment Program
Initial med exam (IME)•Counseling•Physical examination•CXR•Laboratory investigation•Vaccination
– 2nd dose vaccination (2013)– Hep B screening (2014)
On hold with regular follow up•TB suspects •TB Treatment•Drug abuse •Alcohol dependent•Psychiatric evaluation•Chronic disease
Re-med :Undergone the same IME procedure (except vaccination)
Medical Escort & Trv. Assistance•POE•Final destination
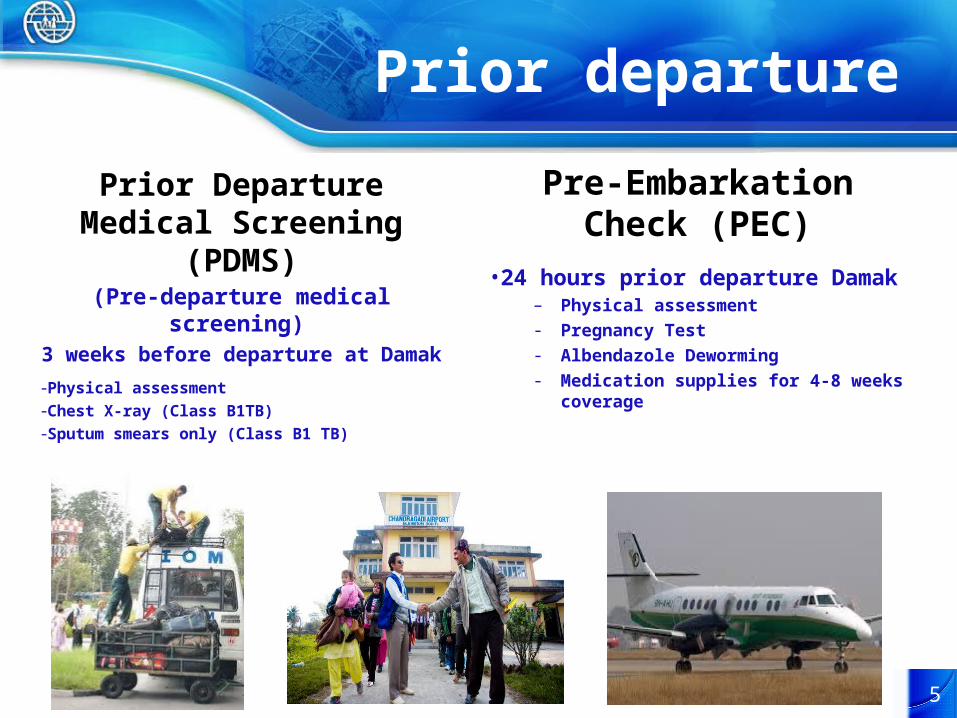
Prior departure
Prior Departure Medical Screening (PDMS)
(Pre-departure medical screening)
3 weeks before departure at Damak-Physical assessment-Chest X-ray (Class B1TB)-Sputum smears only (Class B1 TB)
Pre-Embarkation Check (PEC)
•24 hours prior departure Damak– Physical assessment- Pregnancy Test- Albendazole Deworming- Medication supplies for 4-8 weeks coverage
5
Facilities Group counseling and health education Clinic (clinical Evaluation) Radiology Laboratory, TB and Serology including media
preparations Vaccine and reagents storage facilities DOT and TB isolation centers Pool of medical escorts and escort bags Pharmacy for necessary medicines including 1st and
2nd line TB drugs

TB Laboratory Processing >120 sputum specimens/day Conc. smear read by Fluorescent Microscope MGIT960 Liquid & LJ Solid Culture Molecular Line Probe Assay (LPA) GeneXpert MTB/Rif First Line DST (S,H,R,E,Z) Second Line DST
(AMK,KM,OLF,LEV,PAS,ETO,PAS,CS)
7
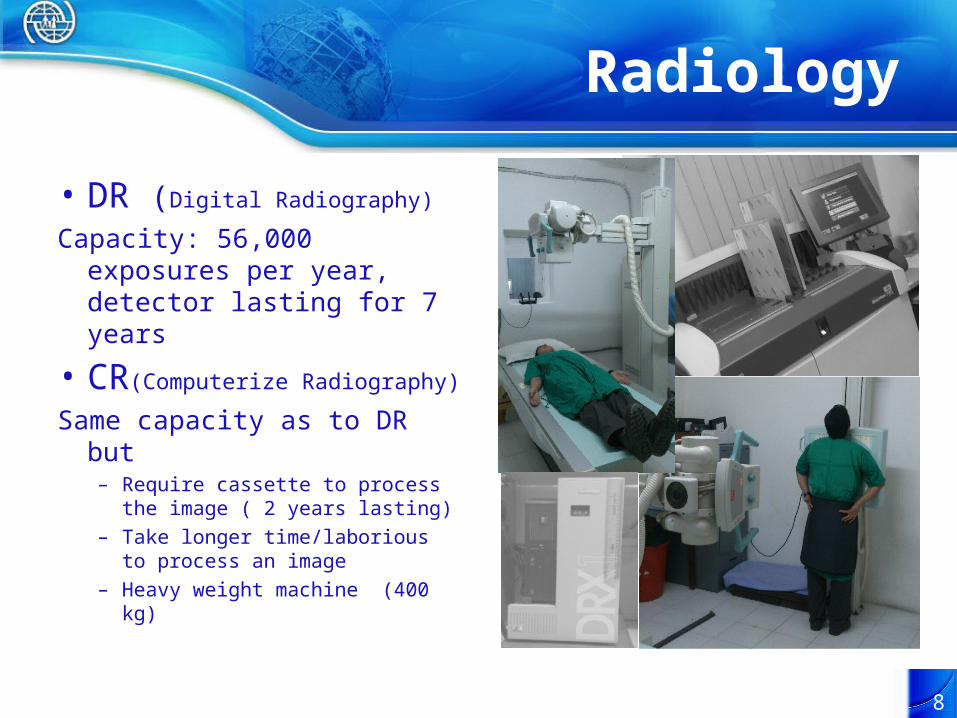
Radiology
• DR (Digital Radiography)
Capacity: 56,000 exposures per year, detector lasting for 7 years
• CR(Computerize Radiography)
Same capacity as to DR but– Require cassette to process the
image ( 2 years lasting)– Take longer time/laborious to
process an image– Heavy weight machine (400 kg)
8
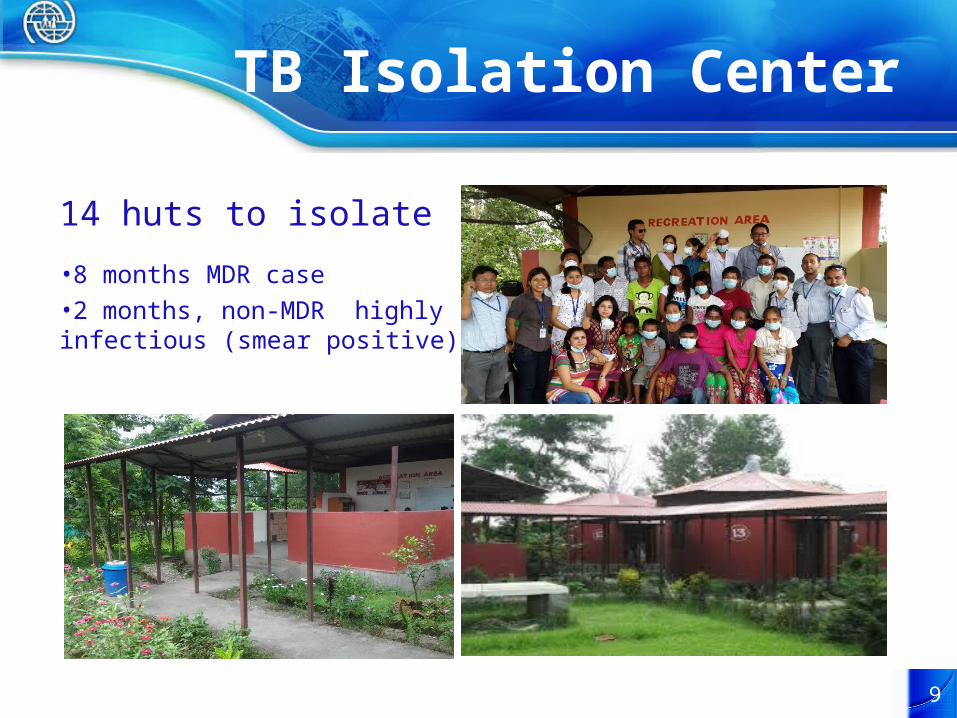
TB Isolation Center
14 huts to isolate
•8 months MDR case•2 months, non-MDR highly infectious (smear positive)
9

Active TB case findingProtocol of USRP
CDC migration Requirements: Technical Instructions for tuberculosis screening and treatment using cultures and DOT, (Oct 2009)
Applicant 2-14 years of age
Tuberculin Skin Test or IGRA
TST ≥ 10 mm or IGRA positive
Chest Radiograph
Medical History, examination, or CXR suggestive for tuberculosis
Individual known HIV infection
Medical HistoryPhysical Examination
Applicant ≥ 15 years of age
3 sputum smear & Culture
DST for all positive culture
Identification in the level of MTB-Complex
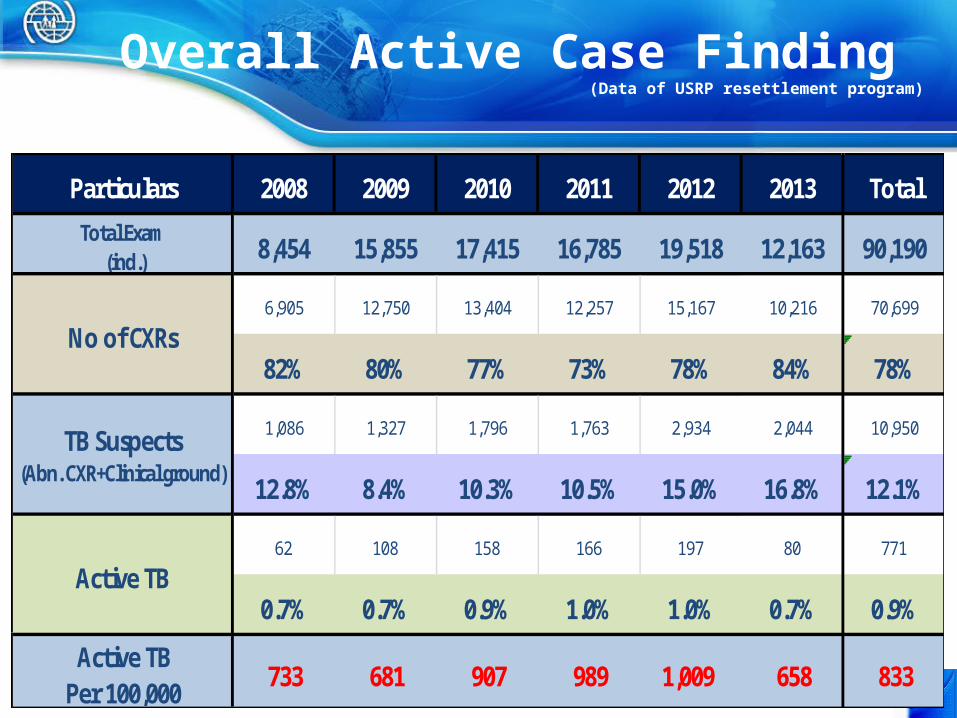
Overall Active Case Finding (Data of USRP resettlement program)
Particulars 2008 2009 2010 2011 2012 2013 Total
Total Exam (ind.) 8,454 15,855 17,415 16,785 19,518 12,163 90,190
6,905 12,750 13,404 12,257 15,167 10,216 70,699
82% 80% 77% 73% 78% 84% 78%
1,086 1,327 1,796 1,763 2,934 2,044 10,950
12.8% 8.4% 10.3% 10.5% 15.0% 16.8% 12.1%
62 108 158 166 197 80 771
0.7% 0.7% 0.9% 1.0% 1.0% 0.7% 0.9%
Active TBPer 100,000
733 681 907 989 1,009 658 833
Active TB
TB Suspects(Abn. CXR+Clinical ground)
No of CXRs
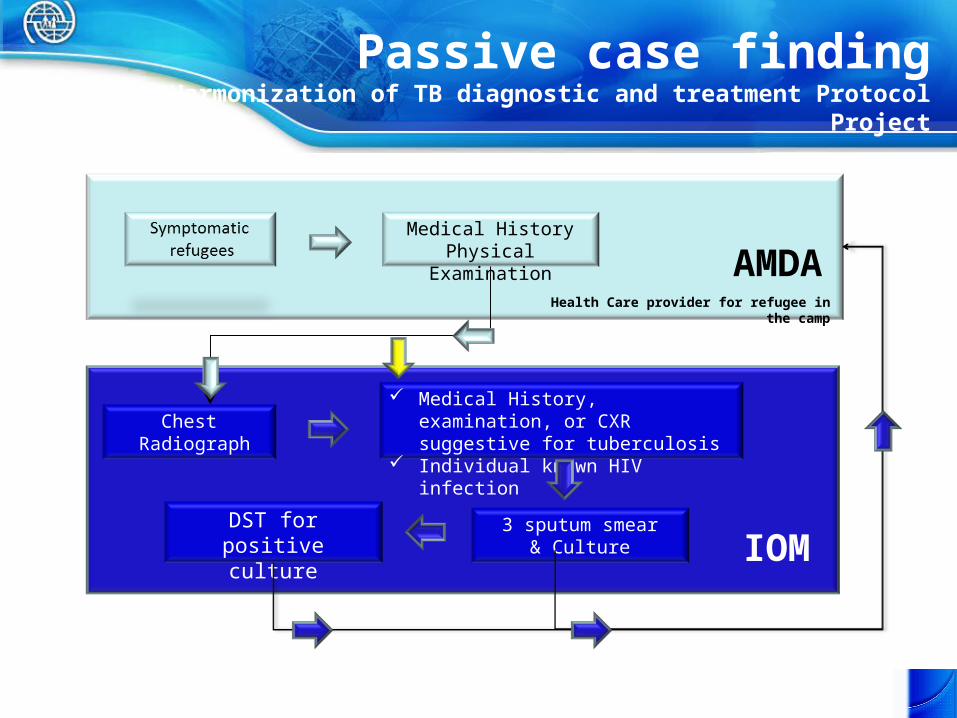
Passive case findingHarmonization of TB diagnostic and treatment Protocol Project
Chest Radiograph
Medical History, examination, or CXR suggestive for tuberculosis
Individual known HIV infection
Medical HistoryPhysical Examination
3 sputum smear& Culture
DST for positive culture IOM
Health Care provider for refugee in the camp
AMDA
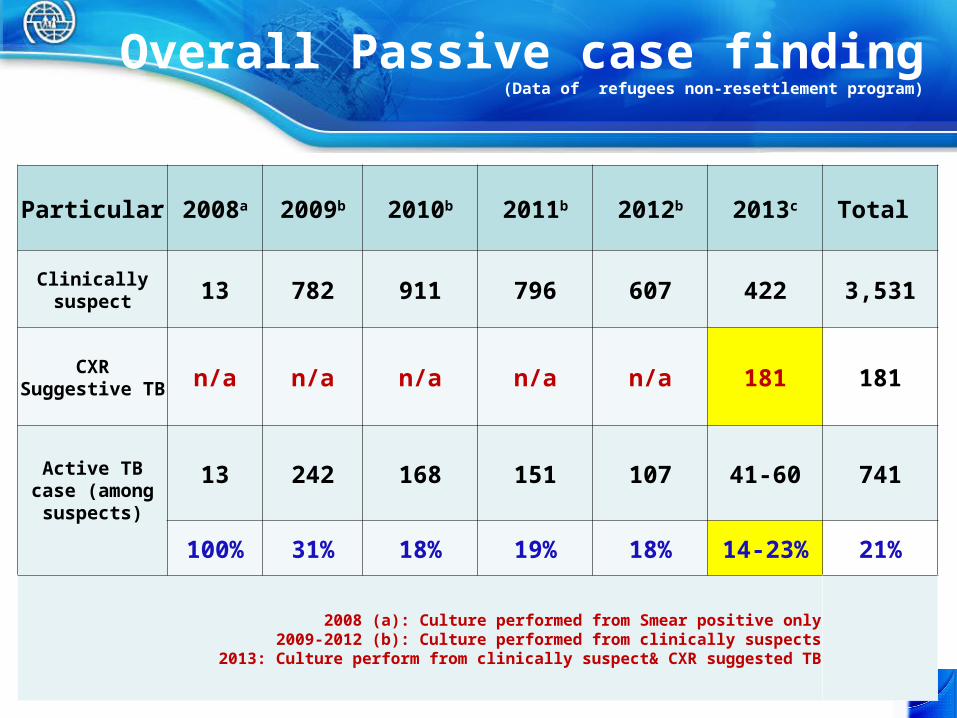
Overall Passive case finding(Data of refugees non-resettlement program)
Particular 2008a 2009b 2010b 2011b 2012b 2013c Total
Clinically suspect 13 782 911 796 607 422 3,531
CXR Suggestive TB n/a n/a n/a n/a n/a 181 181
Active TB case (among
suspects)
13 242 168 151 107 41-60 741
100% 31% 18% 19% 18% 14-23% 21%
2008 (a): Culture performed from Smear positive only2009-2012 (b): Culture performed from clinically suspects
2013: Culture perform from clinically suspect& CXR suggested TB
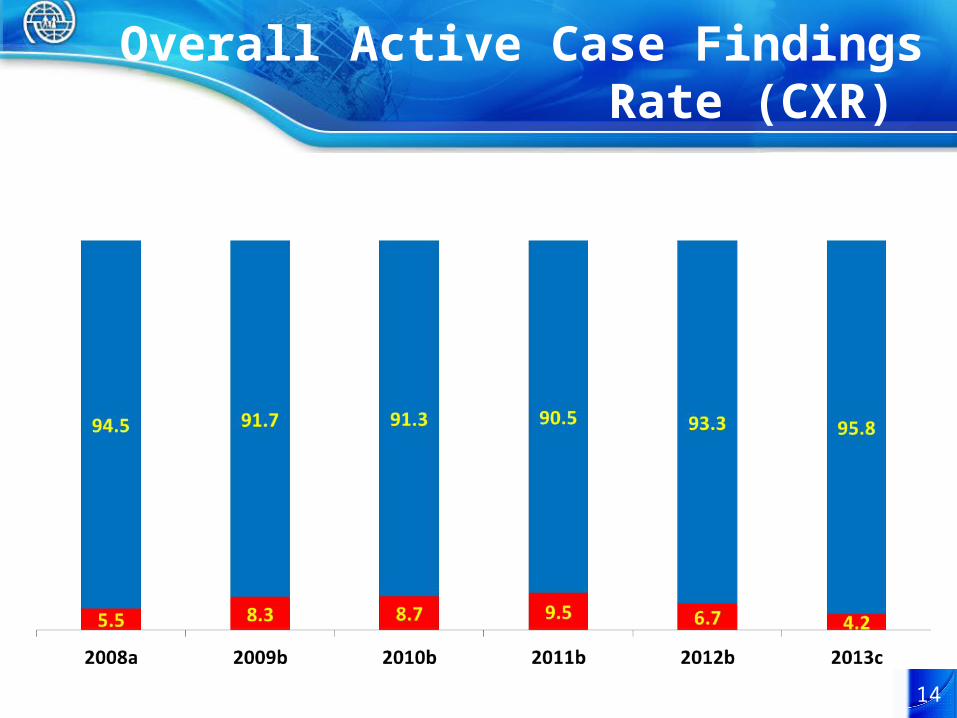
Overall Active Case Findings Rate (CXR)
14
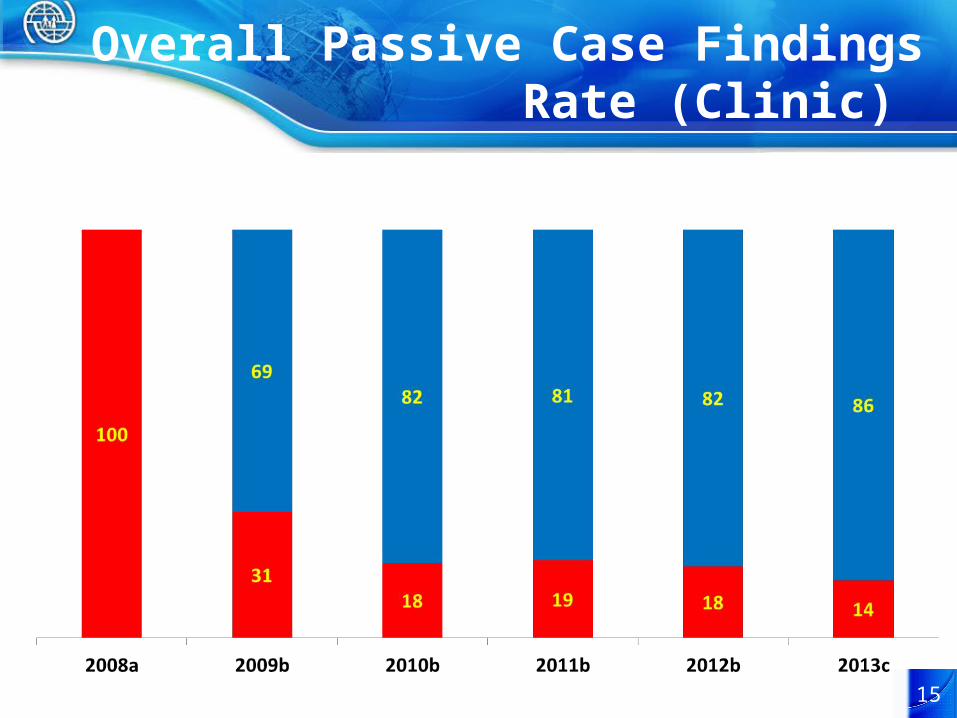
Overall Passive Case Findings Rate (Clinic)
15
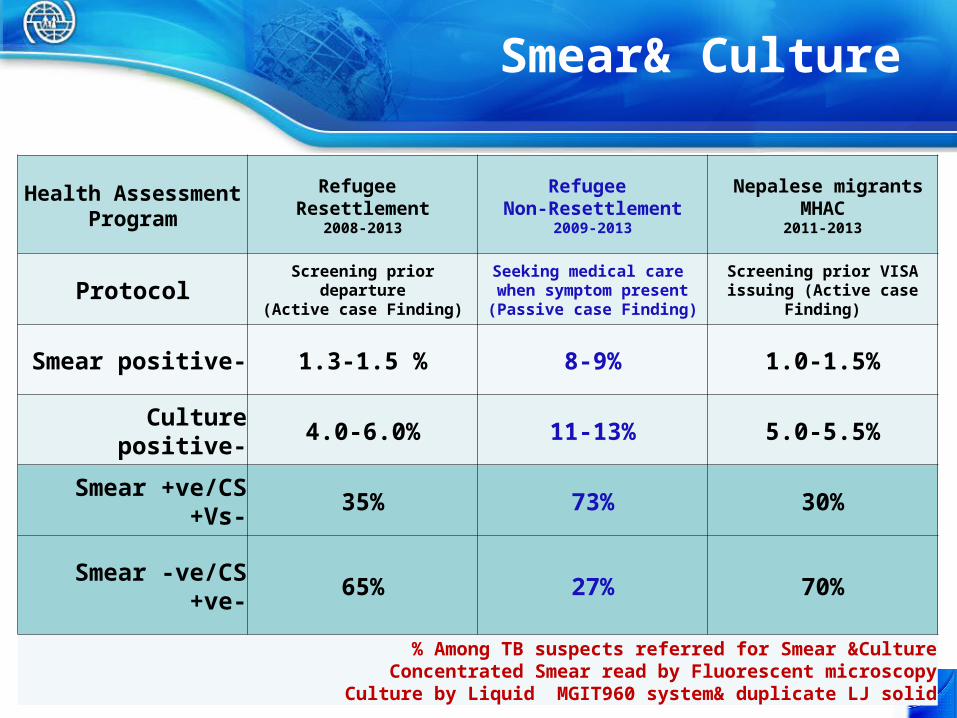
Smear& Culture
Health AssessmentProgram
Refugee Resettlement
2008-2013
Refugee Non-Resettlement
2009-2013
Nepalese migrants MHAC2011-2013
Protocol Screening prior departure(Active case Finding)
Seeking medical care when symptom present
(Passive case Finding)
Screening prior VISA issuing (Active case Finding)
Smear positive- 1.3-1.5 % 8-9% 1.0-1.5%
Culture positive- 4.0-6.0% 11-13% 5.0-5.5%
Smear +ve/CS +Vs- 35% 73% 30%
Smear -ve/CS +ve- 65% 27% 70%
% Among TB suspects referred for Smear &CultureConcentrated Smear read by Fluorescent microscopy
Culture by Liquid MGIT960 system& duplicate LJ solid
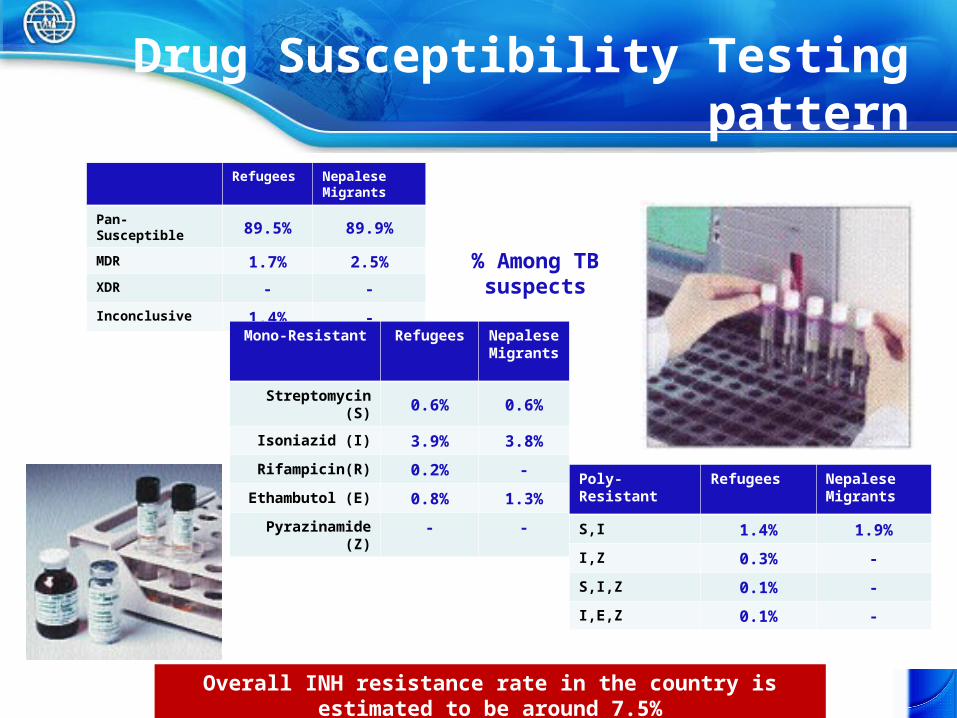
Drug Susceptibility Testing pattern
Refugees Nepalese Migrants
Pan-Susceptible 89.5% 89.9%
MDR 1.7% 2.5%
XDR - -
Inconclusive 1.4% -
Mono-Resistant Refugees Nepalese Migrants
Streptomycin (S) 0.6% 0.6%
Isoniazid (I) 3.9% 3.8%
Rifampicin(R) 0.2% -
Ethambutol (E) 0.8% 1.3%
Pyrazinamide (Z) - -
Poly-Resistant Refugees Nepalese Migrants
S,I 1.4% 1.9%
I,Z 0.3% -
S,I,Z 0.1% -
I,E,Z 0.1% -
% Among TB suspects
Overall INH resistance rate in the country is estimated to be around 7.5%

18


















