

Dr l rajapaksa 16 10 2014 emtct college sessions
51
Overview of Elimination of MTCT of HIV programme in Sri Lanka
-
Upload
college-of-venereologists -
Category
Documents
-
view
215 -
download
0
description
Â
Transcript of Dr l rajapaksa 16 10 2014 emtct college sessions

Overview of
Elimination of MTCT of HIV
programme in Sri Lanka

Trend of Annual Reported HIV cases
Source: SIMU/NSACP
2 3 11 7 132737
2322303255
4254475068
91
129
95119
102
137121
146
186196
0
50
100
150
200
250
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
2007
2009
2011
2013
N. o
f HIV
cas
es re
port
ed
Males Females Total
Presenter
Presentation Notes
අල

Estimated number of HIV + pregnant women and who are in need of ART
for PMTCT, 2007-2015
3
26 3136
4249
54 5963
35
3136
43
50
57
6469
7477
0
10
20
30
40
50
60
70
80
90
2007 2008 2009 2010 2011 2012 2013 2014 2015
Num
ber
Pregnant women in need of ART for PMTCT
Source: National STD/AIDS Control Programme_Report on HIV Estimates and Projections 2009
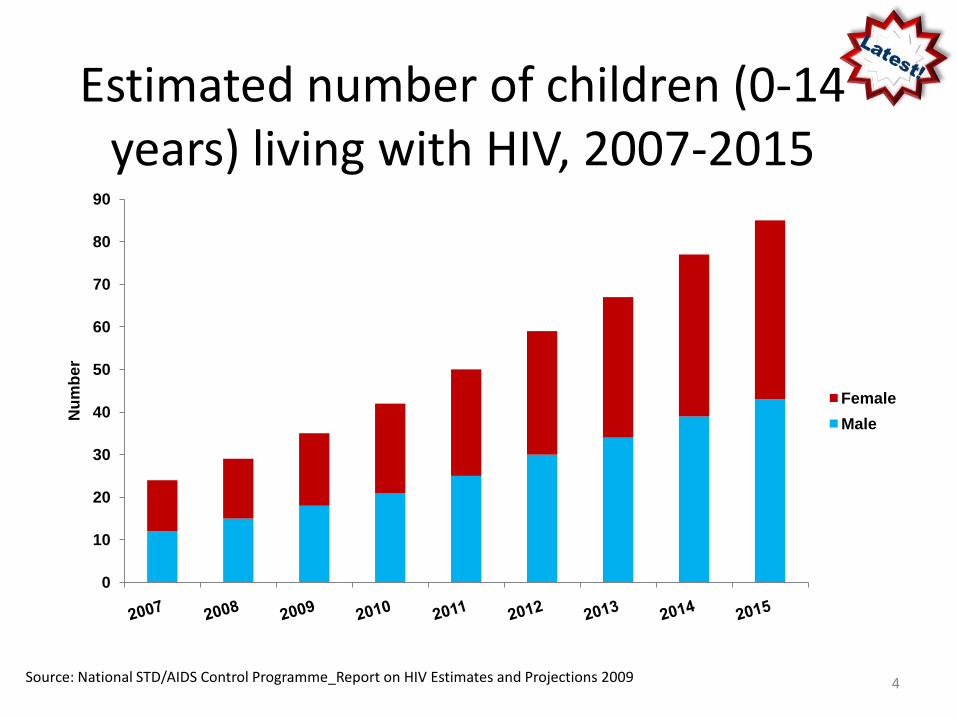
Estimated number of children (0-14 years) living with HIV, 2007-2015
4
0
10
20
30
40
50
60
70
80
90
Num
ber
FemaleMale
Source: National STD/AIDS Control Programme_Report on HIV Estimates and Projections 2009

Reported cases of Paediatric HIV due to MTCT
Year Male Female Total 1994 1 0 1 1995 - - - 1996 - - - 1997 0 1 1 1998 - - - 1999 - - - 2000 2 1 3 2001 4 0 4 2002 - - - 2003 3 - 3 2004 1 1 2 2005 6 4 10 2006 2 - 2 2007 3 1 4 2008 2 1 3 2009 4 6 10 2010 1 2 3 2011 3 2 5 2012 4 2 6 Total 36 21 57
2013 – 11 cases

File number ClinicAge at the time of diagnosis Family details
COF 832/13 Colombo 5y + 6 months Mother HIV + Father -
GP F 001/13 GPF 054/13 Gampaha 3y+ 6 monthsMother HIV + Died Father Not known
GP F 67/13 Gampaha 4y+ 6 monthsMother HIV + -Died Father +
IDF 48 IDH 4 years Mother HIV + Father -
COF 863/13 Colombo 5y + 4 months Mother HIV + -Died
COM 865/13 Colombo 5y + 6months Mother + Father +
GPF 138/13 Gampaha 4y+ 6 monthsMother + Father + brother +(GPF 139))
GPF 139/13 Gampaha 4y+ 6 monthsMother + Father + brother +( GPF 138)
COM 875/13 Colombo 5y + 4 monthsMother + Father + brother +(COM 905)
COM 891/13 Colombo 1y + 6 months Mother + Father +
COM 905/13 Colombo 2y + 6 monthsMother + Father + Sister + (COM 875)
Paediatric HIV cases in 2013

ART services for PMTCT initiated in 2002
Services were for identified pregnant females with HIV

PMTCT data2008 2009 2010
tested positive tested positive tested positive
Gampaha 2290 1 2259 0 1655 0
Kalutara 988 1 741 0 567 0
DMH 8961 1 10180 2 10373 3
CSHW - - - - 884 0
Total registered antenatal population per year – 350,000 – 400,000
ART services for PMTCT introduced in 2002
ConstraintsPilot project/ sentinel sites limited
Accessibility for •information and
•counselling and testing facilities

Number of antenatal samples screened for VDRL and HIV in government centres in 2012
Type of testing
Total number of deliveries
Number screened
Coverage Number positive
VDRL 320,518 194,153 60.6% 45
HIV 320,518 17,822 5.6% 3

Assess the situation
• Antenatal HIV screening coverage 5.6%• VDRL testing coverage close to 98% (60% through STD clinics)• Need to increase HIV testing coverage

Assess the situation
• High cost for testing• debate on cost effectiveness of universal
screening in a low prevalence setting• Lack of interest of others
Consultative Meeting held on 21.05.2013
• All venereologists agreed on universal testing and elimination of MTCT – May 2013
• Decisions taken to call the programme as “Elimination of Mother to child transmission of HIV and congenital syphilis programme”
• To scale up testing sevices for HIV to provide universal screening for all pregnant mothers in few years.

ELIMINATION OF MTCT OF
SYPHILIS
AND
HIV
PROGRAMME

Elimination of MTCT of STI
• Mile stones– Prevention of MTCT of syphilis – 1952– Prevention of MTCT of HIV - 2002– Elimination of congenital syphilis – 2009– Elimination of MTCT of HIV – 2013

Objectives of EMTCT of HIV programme by 2017
• >95% of ANC attendees received Provider Initiated Testing and counseling services for HIV
• 100% of identified HIV-positive pregnant women received antiretroviral medicines to reduce the risk of mother-to-child transmission
• 100% of infants born to identified HIV-infected mothers received ARV drugs
4 strategies were identified.

Strategy 1 - Ensuring advocacy for a successful EMTCT programme
• Advocacy to give high priority to programmeand allocate resources
• Strengthen linkage betweenMCH and STI services
• Demonstrate the cost benefit of interventions
• Establish a national level steering committee

Advocacy -• Concept paper submitted to MOH• Meeting with Directors of major maternity units in the
country DMH, CSHW• Meeting with Director, FHB• Meeting on EMTCT at Kathmandu, Nepal organized by
UNICEF for MCH services and STI services – September 2013 –helped to improve links between MCH services and STI services
• Advocacy meeting - country programme to introduce EMTCT services – sensitization (UNICEF) at Hotel TajSamudra – with participation of all provincial MCH staff and STD staff
• sensitization of stakeholders including private sector
PROVIDER INITIATED TESTING FOR ALL PREGNANT WOMEN
IF NOT DONE IN PREGNANCYAT CHILD BIRTHDURING POST PARTUM PERIOD
WHO Recommendation for low prevalence settingsConsolidated guideline 2013 – August
• NAC meeting – October 2013 – Highlevelmeeting chaired by the secretary, ministry of Health
• Approved the programme.• Steering committee formed.• Target given to cover 50% of pregnant women
by end 2014.
National level steering committee, appointed by the Secretary
• Ministry of Health –, DGHS, DDG PHS 1, DDG PHS 2, DDG LS
• NSACP Director, PMTCT coordinator, Microbiologist
• FHB Director, PMTCT coordinator• Director MSD, Director private medical
institutions• Representatives from College of Obstetricans and
paediatricians• Funding agencies – UNICEF, WHO, WB

Linkages between MCH services and Provincial STI services
Provincial Administration
District STD Clinic
Medical Officer of Health (Primary health care Unit)
NSACPPolicy, guidelines,TOT programmes
TrainingTesting servicesPMTCT services
Obstetrician
FHB
MO MCH
RE
VENE/ MO STD
Coordination, administrative, logistic support

Linkages between MCH services and Provincial STI services
Provincial Administration
District STD Clinic
Medical Officer of Health (Primary health care Unit)
NSACP
Obstetrician
FHB
•Improve awareness•Promote PICT•Infant feeding
•Testing facilities•ART for mother•ART for baby•Care and support services for mother and baby
MO MCH
RE
VENE/ MO STD
Obstetric management

How to inform relevant authorities regarding decisions taken?
Ministry of health issued Circular
• All pregnant women are to be screened before 12 weeks of gestation for Syphilis and HIV.
• Antenatal clinic services have to arrange collection of 5cc of blood and transport to the STD clinic.
• STD clinics have to carry out Syphilis and HIV screening tests.
• The reactive VDRL reports and HIV positive reports need to be informed to the MO, MOH or VOG.
• The screening test positive pregnant women need to be referred to the STD clinic for further management.
• All pregnant women with Syphilis or HIV should be provided appropriate services.
• Programme need to be reviewed at the district level every six months.

Strategy 2
Increase access to and quality of syphilis and HIV services at maternal and child health services
– Expand provider initiated testing and counseling for HIV
– Ensure all antenatal mothers are screened– Maintain quality of testing– regular training of primary health care
workers– Non stigmatizing referral

Source: Strategic Information Management Unit, National STD/AIDS Control Programme, 2010. 27
Scaling up EMTCT services2013
Colombo GampahaMataraHambantotaGalle and Kandy

Source: Strategic Information Management Unit, National STD/AIDS Control Programme, 2010. 28
Scaling up EMTCT services2014
NothernprovinceNorth western provinceNorth central province

Countrywide services in 2016

Scaling up plan
• Year 2013 – cover Colombo, Gampaha, Galle, Matara, Hambantota and Kandy districts
(to start with HIV testing to be done in all samples sent to government STD clinics/ centres for VDRL testing)
• Year 2014 – scale up to Nothern, North Central, North Western provinces
• By year 2016 – to consider possibility to cover all the districts

Laboratory - Increase HIV testing services
• Procure test kits– WHO - US$10,000 – test kits– WB – US $ 200,000 – test kits
• Training of MLT when necessary
• Quality of testing
• ELISA machines – UNICEFNSACP, Matara, Badulla, Negombo
• Vacutainer tubes
• Protective gear kits –for the team involved in delivery
• carrier boxes – to transport samples to be distributed among MOH offices
Lack of human resourcesIncreased work loadOvertime approvalProtocol for testing
Logistics

Training• Training programmes for health
care workers –MCH staff -• Colombo district• Kandy district• Southern province• Gampaha district
Consultative workshops - 3
Institutional staff• DMH, CSHW,CMC• Kalubowila, Homagama,
Awissawella hospital staff• STD clinic staff of SP, Kandy, WP
• 2014• Kalutara MCH staff• NSACP staff• NP, NWP, NCP staff
Only few get opportunity to participate
Need to do more training of HCW at district or MOH level
Use of local resource

UNICEF funds to improve facilitiesItem Unit Numbers
computers EMTCT unit, Reference laboratoryGalle, Gampaha, Kalutara, Kandy, Vavuniya, Jaffna,
8
multi media projectors - EMTCT unit, Matara 2
Fax machines EMTCT unitReference laboratory
2

IEC Material• Posters – To make public
aware of MTCT of HIV• Leaflets – To introduce
testing services package in ANC services, Hb, UFR, GTT, Blood gp and Rh, VDRL, HIV
• Laboratory form –improved to send ANC samples to STD laboratory
(currently being printed.)
CD –• Health talk for ANC mothers• Community awareness
programmes for women and girls
• Advocacy programmes for community leaders
• Management of pregnant women with HIV
• EMTCT scale up plan

Strategies 3:Elimination of HIV transmission from women living with HIV to their children by promotion and integration/linkage of EMTCT with related services
– Ensure that all positive mothers and partners are treated at the STD clinic.
– All babies be managed appropriately with the support of the venereologist/ MOIC of the STD clinic and paediatrician.
Guidelines
• MCH - guideline on antenatal care services for MCH staff
• Preconception services guidelines
• standard of care of management of pregnant women with syphilis or HIV
•
• NSACP - PMTCT guideline including paediatric care 2012
• ART guideline including paediatric care - 2014
• ECS strategy - 2009• EMTCT of syphilis and
HIV strategy – 2014 (to be printed)

Prevention of mother to child transmission of HIV
ART for baby for 6/52
Infant feeding (AFASS feeding)
Obstetric management according to guidelines LSCS/ vaginal
ART at 14 weeks /if diagnosed later, as soon as possible
Provider initiated Counselling and testing (PICT)

PMTCT Programme in Sri Lanka• Guidelines are developed.• ART for all eligible. • ART for PMTCT from 28 weeks.• Obstetric management with LSCS at 38-39
weeks• ART for baby• Infant feeding protocols are in place. • Free provision of formula feeding by an NGO• FP services for women with HIV

Rapid advice WHO - 2009 ART - B + option
Three drugs AZT+3TC+LPV/RtTDF+FTC+LPV/Rt
To continue ART after delivery for lifetime

Strategy 4:Strengthen surveillance, monitoring and evaluation systems
– Improve collection of data– Regular review of the programme

Indicators
• % pregnant women attending ANC in selected districts offered testing services for HIV
• % pregnant women attending ANC identified as having HIV infection
• % identified HIV infected pregnant women receiving PMTCT services according to national guidelines

Districts Pregnant mothers registered Number tested for syphilis Syphilis Coverage(%)
Ampara 5219 1917 36.73Anuradhapura 19572 12121 61.93Badulla 1672719943 81.4Monaragala 10577 2286Batticalloa 10983 1829 16.65Colombo 26779 +8816 (CMC)14559 43.23
829Puttalam 16336 15941 97.58Gampaha 312892983
104 53.71
13719Hambanthota 12976 8229 63.42Jaffna 10435 5864 56.20kalutara 16789 + 6033 (NIHS) 934 4.2Kalmunai 9399 4250 45.22Kandy 28187 13653 48.44Kegalle 15419 7191 46.64Kurunagala 30652 22197 72.42Galle 188633539 50.77
6038Mannar 2118 1941 91.64Matale 10245 5676 55.40Matara 15483 9918 64.06NuwaraEliya 14629 10099 69.03Polonnaruwa 8639 7514 86.98Ratnapura 20161 14971 74.26Trincomalee 9228 4644 50.33Vauniya 35064981 63.6Kilinichchi 2216Muuaitivu 2107
383,383 217870 56.8282892
ANC VDRL coverage 2013

DistrictsNumber tested for HIV Number positive HIV coverage(%)
Ampara 0 0
Anuradhapura 0 0
Badulla 772 0 4.62
Monaragala 0 0
Batticalloa 0 0
Colombo 20050 2 56.3
2 0
Puttalam 1263 0 7.73
Gampaha 240 0
0 0
2347 2 8.27
Hambanthota 0 0
Jaffna 0 0
kalutara 673 0 2.95
Kalmunai 0 0
Kandy 1911 0 6.78
Kegalle 793 0 5.14
Kurunagala 0
Galle 465 0 25.91
4422 0
Mannar 0 0
Matale 0 0
Matara 1016 0 6.56
NuwaraEliya 0 0
Polonnaruwa 0 0
Ratnapura 39 0 0.19
Trincomalee 57 0 0.62
Vauniya 55 0 0.7
KilinichchiMuuaitivu
34105 4 8.895803935
ANC HIV tests 2013

District No.tested No.positive No.tested No.positiveAmpara 0 0Anuradhapura 0 0Badulla 126 0Batticalloa 0 0Colombo 8628 8402 2
5 60Puttalam 2062 3275 2Gampaha 1 0
1515 20442933 4327994 1683
Hambanthota 2358 2237Jaffna 0 0Kalutara 758
773Kalmunai 1 0Kandy 6754 7176Kegalle 752 2004Kurunegala 0 0Galle 1252 1257
3009 2621Mannar 0 0Matale 0 0Matara 3591 2856Monaragala 0 335NuwaraEliya 0 0Polonnaruwa 0 0Ratnapura 25 17Trincomalee 11 8Vauniya 4 6
34779 39081
ANC HIV tests 2014 Q1, Q2
Targets by 2017
• Reduce mother to child transmission of HIV to <0.5 cases/1000 live births
• Reduce the incidence of congenital syphilis to <0.5 cases/1000 live births

Outcome of PMTCT servicesYear Positive
pregnant women
Known Newlyidentified
outcome Mode of delivery
2011 6 Abortion -2Negative babies - 4
LSCS - 4
2012 5 3 2 Negative babies - 5
LSCS – 4NVD - 1
2013 6 0 6 Negative babies - 6
LSCS
2014 8 4 4 Abortion – 15 delivered2 to deliver
LSCS – 4NVD - 1
Total 25 12 13 16 negative babiesNo positive babies

Challenges• Lack of human resources – MLT• Lack of facilities to transport samples• Delay in testing• Lack of storage facilities at STD clinics- refrigerators• Problems in labeling tubes – mix up• Uniformity in data collection• Local training of HCW – within the district • ?Stigma ?maintenance of confidentiality• PLHIV – reluctance to use FP services, need bigger
families• Management of paediatric HIV cases

Proposed• Training on EMTCT PLHIV 1 day programmes• Consultative workshops - 3 NP, NWP, NCP• Printing of strategy
• Regular training of MCH staff by the local resource• Introduce training of EMTCT into pre-service training - public health
staff - NIHS, PHM training, Doctors - undergraduate, postgraduate
• Regular reviews - National level, Provincial level
• Involvement of private sector• Involvement of professional colleges – obstetricians, paediatricians

Thank You
To all Who contributed to the success of the EMTCT programme



![MULHERES GRAVIDAS OPTION B+ PTV / EMTCT B PLUS MOZ_ [Read-Only].pdf · Remember that Prevention is the best step to EMTCT . STAGE 1 PRE-CONCEPTION. Case Mr. and Mrs Kamuzi have been](https://static.fdocuments.net/doc/165x107/5b7af66e7f8b9a184a8ba18e/mulheres-gravidas-option-b-ptv-b-plus-moz-read-onlypdf-remember-that.jpg)














